Embed Size (px)
Citation preview

Iron Toxicity and Clinical Sequelae
John B. Porter, MA, MD, FRCP
ProfessorDepartment of HaematologyUniversity College LondonLondon, United Kingdom

Learning Objectives
• Analyze the mechanisms contributing to the development of iron overload and the clinical consequences of iron overload on the liver, heart, and endocrine system.
• Utilizing an understanding of the factors contributing to the development of iron overload, identify patients at risk in the practice setting.

Topics
• Causes of iron overload
• Mechanisms of iron-overload–mediated toxicity– Molecular level
– Non–transferrin-bound iron—extracellular
– Labile iron pool—intracellular
– Free radical formation Microscopic level Macroscopic level
• Clinical impact consequences of iron overload

Conditions Associated with Iron Overload
Transfusional Nontransfusional Age of onsetComplications
Thalassaemia major1 Type 2 haemochromatosis (rare)2 Childhood
Blackfan Diamond Anaemia1 2a hemojuvelin2 (Risks from HH)
Fanconi’s Anaemia1 2b hepcidin2
Early stroke with HbSS1
Severe haemolytic anaemias1
Aplastic anaemia1,2 Type 1 haemochromatosis1 Typically adult
Other transfusion in HbSS1 Thalassaemia intermedia1
Myelodysplasia (MDS)3
Repeated myeloablative chemotherapy1
1. Porter JB. Br J Haematol. 2001;115:239. 2. Brittenham G. In Hoffman R, et al, ed. Hematology: Basic Principles and Practice, 4th ed. Philadelphia, PA: Churchill Livingstone, 2004. 3. Taher A, et al. Semin Hematol. 2007;44:S2.
Slide courtesy of Dr. J. Porter.

*Dietary and hereditary components.
Bacon BR. In Goldman L, ed. Cecil’s Textbook of Medicine, 23rd ed. Philadelphia, PA: Saunders-Elsevier, 2008.
Acquired, Nontransfusional Forms of Iron Overload
• Chronic liver disease– Hepatitis C
– Alcoholic liver disease
– Nonalcoholic steatohepatitis
• Porphyria cutanea tarda
• Portacaval shunting
• Inappropriately high dietary intake – Latrogenic (eg, treatment of microcytosis)
– African (Bantu) siderosis*

Rare Abnormalities of Iron Distribution
Aceruloplasminaemia Plasma reductase Retina RetinopathyAR1,2 Basal ganglia Extrapyramidal
Pancreas Diabetes
Hallervorden-Spatz Pantotenate kinase Basal ganglia Extrapyramidal AR3 cysteine accumulation
Neuroferritinopathy Ferritin light chain Basal ganglia ExtrapyramidalAD4 Forebrain Parkinsonian
Cerebellum
Freidrich’s Ataxia5,6 Frataxin Mitochondrial AtaxiaAR oxidative stress Sensory neurons
Spinal cordDorsal root gangliaMyocardium Cardiomyopathy
Condition Cause Iron Distribution Effects
1. Mariani R, et al. Gut. 2004;53:756-8. 2. Hellman NE, et al. Gut. 2000;47:858-60. 3. Hayflick SJ. Curr Opin Pediatr. 2003;15:572-7. 4. Crompton DE, et al. Blood Cells Mol Dis. 2002;29:522-31. 5. Koepen A, et al. Acta Neuropahtol. 2007;114:163-73. 6. Michael, et al. Cerebellum. 2007;5:257-67.
AR = autosomal recessive; AD = autosomal dominant.

How Does Transfusional Iron Loading Develop?

Porter J. Hematol/Oncol Clinics. 2005;19(suppl 1):7.
Red
Erythron 2g
20–30 mg/day
Macrophages 0.6 g
1–2 mg/day
Gut
Transferrin
20–30 mg/day 2–3 mg/day
20–30 mg/dayOtherparenchyma
0.3 g
Hepatocytes1 g
Simplified Iron Turnover and Storage

1. Taher A, et al. Semin Hematol. 2007;44:S2.2. Porter JB. Br J Haematol. 2001;115:239.
Rate of Iron Loading from Transfusion
• Simple estimation1
– 1 unit contains 200 mg of iron
– Adult may receive 4–10 g/y from transfusion
• More-precise method2
– Volume of blood transfused x mean haematocrit of processed blood obtained from the transfusion centre x 1.08
• For exchange transfusion need to know– Volume and haematocrit transfused
– Volume and haematocrit removed

Parenchyma
Hepatocytes
Hepatocytes
Parenchyma
Red
Erythron
Macrophages
Gut
Transfusion
20–40 mg/day(0.3–0.7 mg/kg/day)
Transferrin
Adapted from Porter JB. Hematol/Oncol Clinics. 2005;19(suppl 1):7-12.
NTBI
NTBI = non–transferrin-bound iron.
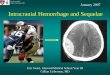
Transfusional Iron Overload

50403020100
50
100
150
200
250Thalassaemia major
HH homozygote
HH heterozygote
Age (years)
Hep
atic
Iro
n (
µm
ol/
g w
et w
eig
ht)
50
40
30
20
10
0
Hep
atic
Iro
n (
mg
/g,
dry
wei
gh
t)
Threshold for cardiac disease and early death
Increased risk of complications
Normal
Olivieri N, Brittenham G. Blood. 1997;89:739.
Liver Iron and Risk from Iron Overload
0
HH = hereditary haemochromatosis.

How Do Inherited Nontransfusional Forms of Iron Loading Develop?

Effect of Hepcidin on Iron Turnover
Erythron
20–30 mg/day
1–2 mg/day
Gut
Transferrin20–30 mg/day2–3 mg/day
20–30 mg/dayHepatocytes
IL6Iron
Prohepcidin
Hepcidin
Hypoxia
+ - Macrophages
Adapted from Porter JB. Hematol/Oncol Clinics. 2005;19(suppl 1):7.

Factors Affecting Hepcidin Expression?
• TfR21
• HJV2
• Oral iron1
• Iron stores1,2
• LPS2 • IL-62
• HFE1
+ -• Erythropoiesis1 • Anaemia1
• Hypoxia1
• NTBI?
Hepcidin
Tf = transferrin; TfR = transferrin receptor; HJV = hemojuvelin; LPS = lipopolysaccharide; IL = interleukin; NTBI = non–transferrin-bound iron.
1. Leong W, Lönnerdal B. J Nutr. 2004;134:1.2. Lee P, et al. Proc Natl Acad Sci U S A. 2004;101:9263.

Type 1 Type 2A Type 2B Type 3 Type 4
Gene HFE HJV HAMP (hepcidin)
TFR2 Ireg1Ferroportin 1
Function Interact with TfR1
Unknown Regulates iron export
Iron uptake Iron export
InheritanceIncidence
RecessiveCommon
RecessiveRare
RecessiveRare
RecessiveRare
DominantRare
Tissues affected
Liver;hepatocytesmacrophages
Skeletal muscle, heart,liver
Liver hepatocyte
Liver hepatocyte
DuodenumMacrophage
Clinical presentation
Late variable Early onsetSevere
Early onsetSevere
Severe Variable
Hepcidin levels ??
With permission from Worwood M. Blood Rev. 2005;19:69.
Classification of Haemochromatosis

Why Is Iron Overload Toxic?

Fe 2+
Fe 3+
+ e- - e-
Redox Cycling of Iron
Slide courtesy of Dr. J. Porter.

Porter J. Hematol/Oncol Clinics 2005;19(suppl 1):7.
Hydroxyl Radical (HO.) Generation
Haber Weiss Reaction
O2.- + H2O2 -----> O2 + OH- + HO.
Catalysed by Iron in two steps; (Fenton reaction)
Fe3+ + O2.- -----> Fe2+ + O2
Fe2+ + H2O2 -----> Fe3+ + OH- + HO.

OO
OOH
Hydrogen abstraction ( H.)
Molecular rearrangement
Oxygen uptake
Lipid hydroperoxide
Peroxyl radical propagates peroxidation by abstracting H.
from another fatty acid
+ O2.
.
.
H2O
Decompositioneg, to MDA
Porter J. Hematol/Oncol Clinics 2005;19(suppl 1):7.With permission from Gutteridge JM, Halliwell B. Baillieries Clin Haematol. 1989;2:195.
Lipid Peroxidation by HO.

20
Consequences of Iron-Mediated Toxicity
Increased free iron
Hydroxyl radical generation
Lipid peroxidation
Organelle damage
Lysosomal fragilityEnzyme leakage
Cell death
Collagensynthesis
TGF-b1
Fibrosis
Gutteridge JMC, Halliwell B. Bailleres Clin Haematol. 1989;2:195-256. Bacon BR, et al, J Clin Invest. 1983;71:429-439.Myers BM, et al. J Clin Invest. 1991;88:1207-1215. Tsakamota H, et al. J Clin Invest. 1995;96:620-630.Houglum K, et al. Hepatology.1997;26:605-610.

Evans R et al. J Biol Inorg Chem. 2007;13:57.
Nature of NTBI
• Nature of NTBI– Citrate iron
Polymeric Slowly chelated Oligomeric Dimeric Monomeric Rapidly chelated
• Protein-bound iron– Binds weakly to albumin
– As citrate oligomers bound to albumin
• OtherNTBI = non–transferrin-bound iron.

1.Bacon BR. In Goldman L, ed. Cecil’s Textbook of Medicine, 23rd ed. Philadelphia, PA: Saunders-Elsevier, 2008. 2. Oudit GY, et al. Circulation. 2004;109:1877. 3. Rafique et al. Blood. 2006;108:1542a.
Uptake of NTBIReceptors
• Divalent metal transporter (DMT1)1
– Enterocytes
– Erythron (negatively regulated by iron loading)
– ? Other
• L-type calcium-dependent channels2
– Myocardium (positively induced by iron loading)
– Anterior pituitary (positively induced by iron loading)
• T-type calcium channels3
– Hepatocytes (positively induced by iron loading)

Antioxidant Capacity in Iron Overload
806040200
Vitamin C
B-carotene
Vitamin A
Vitamin E
Ubiquinone
Ubiquinol
Lycopene
% Decrease of Control
• 48 thalassaemia major (age 11–22 years) • Vitamin E and NTBI negatively correlate (r = -0.81)
• No correlation with serum ferritin
De Luca C, et al. Free Radic Res. 1999;30:453.
Slide courtesy of Dr. J. Porter.

Intracellular Iron-Mediated Toxicityfrom Labile Intracellular Iron
Transferriniron
Lysosomaldegradation
LV
DC
CNon-transferriniron
Organelle damage
Ironproteins
Free-radical generation
Ferritin
LVDCC = L-type voltage-dependent calcium channel.Porter JB. Am J Hematol. 2007;82:1136.
Labile iron pool
(LIP)

Where Is Iron Toxic ?

Adapted from Porter JB. Hematol/Oncol Clinics 2005;19(suppl 1):7.
Parenchyma
Hepatocytes
Hepatocytes
Parenchyma
Erythron
Macrophages
Gut
Transfusion
20–40 mg/day(0.3–0.7 mg/kg/day)
Transferrin
NTBI
NTBI = non–transferrin-bound iron.
Transfusional Iron Overload

1. Porter JB. Hematol/Oncol Clinics 2005;19(suppl 1):7.2. Taher A, et al. Semin Hematol. 2007;44:S2.
Iron Distribution in Transfusional Overload
• Transfusional overload distribution differs from absorption distribution at early stages1
• Why great variability in iron distribution in different tissues?– Liver, endocrine glands, anterior pituitary1
– Very little in brain, skeletal muscle1
– Liver iron correlates with units transfused2

Adapted from Modell B, Mathews R. Birth Defects Orig Artic Ser. 1976;12:13.
86420
Fe % d.w.
Minimum
Maximum
Skeletal muscle
Testes
Kidney
Heart
Adrenal
Salivary gland
Thyroid
Pancreas
Liver
Parathyroid
Distribution of Body Iron at Postmortem in TM in Prechelation Era
Tm = thalassaemia major; d.w. = dry weight.

Liver Heart
Liver and Iron Content Postmortem in Thalassaemia Major

0–4 5–9 10–14 15–19 >20 Total
Heart disease 0 6 39 35 16 96
Infection 2 6 9 3 0 20
Liver disease 0 0 2 7 1 10
Malignancy 2 2 1 1 2 8
Endocrine disease 0 0 2 1 1 4
Accident 0 0 2 2 0 4
Thromboembolism 0 0 2 1 1 4
Anaemia 2 0 0 0 0 2
Other 0 1 1 0 1 3
Unknown 0 1 3 3 1 8
Total 6 16 61 53 23 159
Zurlo MG, et al. Lancet. 1989;2:27.
Causes of Death in Thalassaemia
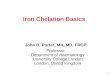
n = 1078
Age (years)

131 transfused adult patients
• 101 leukaemias
• 30 other anaemias
0–25 26–50 51–75 76–100 101–200 201–3000
20
40
60
80
100
Units of Blood Transfused
Pat
ien
ts w
ith
Car
dia
c Ir
on
(%
)
Buja LM, Roberts WC. Am J Med. 1971;51:209.
Blood Transfusion and Cardiac Iron Deposits at Postmortem in the Prechelation Era
Slide courtesy of Dr. J. Porter.

Blood Transfusion Predicts Heart Iron in Unchelated Patients
0
2
4
6
8
10
12
14
16
18
20
Est
imat
ed H
eart
Iro
n (
µm
ol/
g)
25 50 75 100
125
150
Blood Units Transfused
Jensen PD, et al. Blood. 2003;101:4632.
Upper Normal Limit
Slide courtesy of Dr. J. Porter.

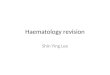
0 20 40 60 80
Thalassaemia major (n = 108)
Thalassaemia intermedia (n = 23)
Congenital sideroblastic (n = 4)
PK deficiency (n = 9)
Diamond Blackfan (n = 7)
Myelodysplasia (n = 7)
Sickle (n = 37)
Patients (%, n) with T2* < 20 ms
UCLH patients with cardiac MRI
Glanvillle J, et al. Presented at ASH 2006. Blood. 2006;108:abstract 1553.
Is the Heart Equally at Risk of Iron Loading in All Forms of Transfusional Iron?

Shah F. Presentation at ASH Dec 2002. Blood 2002;100:668a.
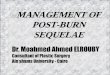
-2
-1
0
1
2
3
4
5
6
7
8
Thalassaemia majorHbSS
NT
BI (
µM
)Patients Treated at UCLH
3.38 ± 2.4
0.17 ± 1.8
P = 0.0001
LIC = 4.34 LIC = 4.22
NTBI in Sickle Cell or Thalassaemia Major Matched for Liver Iron Concentration
Slide courtesy of Dr. J. Porter.

Which Forms of Iron Are Most Toxic?

Porter J. Hematol/Oncol Clinics. 2005;(suppl 1):S7.
Labile Toxic Iron Pools?
• NTBI in plasma?– Correlates with antioxidant depletion
– Promotion of lipid peroxidation in vitro
– BUT which species?
• Labile iron pools (LIP) in cells?– In vitro: clear evidence linking free iron to lipid peroxidation and
organelle damage
• Clinical evidence?– Improvement in cardiac performance with intravenous
desferrioxamine precedes changes in cardiac iron
– BUT direct link of NTBI or LIP to clinical damage not established

1. Olivieri NF, et al. N Engl J Med. 1994;331:574.2. Brittenham GM, et al. N Engl J Med. 1994;331:567. 3. Porter JB. Hematol/Oncol Clinics. 2005;19(suppl 1):S7.
Absolute Tissue Levels?
• Evidence (serum ferritin) >2500 µg/L & cardiac disease-free survival1
• Liver iron association with cardiac death2
Of 15/53 thalassaemia major patients with cardiac disease, all had liver iron >15 mg/g dry weight3
– Association or causation?
• But– Iron in different tissues at postmortem does not
correlate with damage to those organs3
– Link of cardiac iron to damage & death not known3

Intracellular Iron Levels and Toxicity
• Concepts– “Safe iron”
No toxicity in heterozygotes of hereditary haemochromatosis where liver levels < 7mg/g dry weight.1
– “Dangerous iron” High risk of cardiac death if liver >15 mg/g dry weight.1
• Limitations– Uneven distribution within and between tissues2
– Relationship between heart iron and mortality unknown2
1. Porter JB. Br J Haematol. 2001;115:239.
2. Porter J. Hematol/Oncol Clinics. 2005;19(suppl 1):7.

1. Porter JB. Hematol/Oncol Clinics. 2005;19(suppl 1):S7.2. Brittenham G. In Hoffman R, et al, ed. Hematology: Basic Principles and Practice, 4th ed.
Philadelphia, PA: Churchill Livingstone, 2004.
Functional Consequences of Transfusional Iron Overload
• Liver1
• Heart1
• Endocrine system1
• Cancer
• Other potential sequelae – Arthropathy2
– Hyperpigmentation2

Diabetes1Pancreas
Gonads
Cirrhosis, carcinoma1Liver
Cardiomyopathy1Heart
Hypoparathyoidism1Parathyroid
Hypothyroidism1Thyroid
Hypogonadotrophic hypogonadism1Pituitary
ConsequencesOrgan
Joints Arthropathy2
Skin Pigmentation2
Hypogonadotrophic hypogonadism1
1. Taher A, et al. Semin Hematol. 2007;44:S2.2. Brittenham G. In Hoffman R, et al, ed. Hematology: Basic Principles and Practice, 4th ed.
Philadelphia, PA: Churchill Livingstone, 2004.
Organ Systems Affected by Iron Overload

Conclusions
• Conditions associated with iron overload include transfusional iron overload as well as hereditary and acquired nontransfusional iron overload
• Because the body has no mechanism for excretion of excess iron, iron can accumulate
• Iron accumulation results in– Increased free iron
– Hydroxyl radical generation
– Lipid peroxidation
• This results in cell death and fibrosis, with impact on a variety of organ systems and functional consequences – Heart
– Liver
– Endocrine system