Embed Size (px)
Citation preview

Iron Overload in NTDT
3rd Pan-European Conference on Haemoglobinopathies & Rare Anaemias
Limassol, 24 – 26 October 2012
Khaled M. Musallam, MD, PhDAmerican University of Beirut, Beirut, Lebanon
University of Milan, Milan, Italy

● Primary: Increased intestinal absorption
● Secondary: Blood transfusions
Excess Iron in NTDT
Musallam KM et al. Blood Rev 2012;26:16-9.

● Occasional
• Infection
• Pregnancy
• Surgery
● More regular
• Poor growth and development
• Specific complications (advanced age)
Leg ulcer, pulmonary hypertension, extramedullary hematopoietic psuedotumors, thrombotic disease
Transfusions in NTDT
Musallam KM et al. Cold Spring Harb Perspect Med 2012;2:a013482.

Primary Iron Overload
Musallam KM et al. Blood Rev 2012;26:16-9.Ginzburg Y and Rivella S. Blood 2011;118:4321-30.
Ineffective erythropoiesis, Anemia, Hypoxia
↓ Hepcidin↑ Erythropoietin
↓ Ferroportin↑ Intestinal absorption
↑ Release of recycled iron from reticuloendothelial system
↑ Liver iron concentration↓ Than expected serum ferritin level
GDF-15TWGF-1
HIFsTmprss6
? Other erythroid regulators

Primary Iron Overload (2)
r=0.63, P=0.0141 r=0.36, P=0.0022
1. Musallam KM et al. Blood Cells Mol Dis 2011;47:232-4.2. Taher AT et al. Br J Haematol 2009;146:569-72.

● Cumulative process
• Positive correlations between iron overload indices and advancing age1-5
● Slower than transfusional siderosis
• 3-4 mg/day or as much as 1,000 mg/year6
• Annual increase in liver iron concentration of 0.38 ± 0.49 mg Fe/g dry7
Iron Overload in NTDT
1. Taher A et al. Br J Haematol 2009;146:569-72.2. Taher AT et al. Br J Haematol 2010;150:486-9.3. Taher A et al. Haematologica 2008;93:1584-6.4. Lal A et al. N Engl J Med 2011;364:710-8.5. Chen FE et al. N Eng J Med 2000;343:544-50.6. Musallam KM et al. Blood Rev 2012;26:16-9.7. Taher AT et al. Blood 2012;120:970-7.
β-thalassemia intermedia2
Hemoglobin H disease5
r=0.65P<0.001

Considerable iron overload warranting concern?
● Iron overload as early as 5 years1
● Iron-related morbidities beyond 10 years2
● Mean LIC values at cross-sectional assessment of NTDT cohorts with a mean age in early-mid adulthood range between 7 and 15 mg Fe/g dw3-7
1. Cossu P et al. Eur J Pediatr 1981;137:267-71.2. Taher AT et al. Br J Haematol 2010;150:486-9.3. Origa R et al. Haematologica 2007;92:583-8.4. Musallam KM et al. Haematologica 2011;96:1605-12.5. Taher AT et al. Blood 2012;120:970-7.6. Lal A et al. N Engl J Med 2011;364:710-8.7. Pakbaz Z et al. Pediatr Blood Cancer 2007;49:329-32.

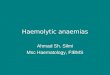
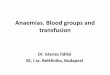
The Heart
20
25
30
35
40
45
50
55
60
65
0 500 1000 1500 2000 2500 3000 3500
Serum ferritin (ng/mL)
Ca
rdia
c T
2*
(ms
)
Normal LIC (< 3 mg Fe/g dry wt)
Mild LIC (3–7 mg Fe/g dry wt)
Moderate LIC (7–15 mg Fe/g dry wt)
Severe LIC (> 15 mg Fe/g dry wt)
Normal cardiac R2*
0
5
10
15
20
25
30
0 20 40 60 80 100
LIC
(m
g F
e/g
dry
wt)
Cardiac R2* (Hz)
1. Origa R et al. Haematologica 2008;93:1095-6.2. Roghi A et al. Ann Hematol 2010;89:585-9.3. Taher AT et al. Am J Hematol 2010;85:288-90.4. Mavrogeni S et al. Int J Cardiovasc Imaging 2008;24:849-54.
n=20 n=49
No evidence of cardiac siderosis even in NTDT patients with considerable iron overload1-4

The Liver
● Several case reports and case series suggest an association between iron overload and hepatocellular carcinoma in hepatitis C negative patients with NTDT1-4
1. Macaron J et al. Ann Hepatol 2012. In Press.2. Restivo Pantalone G et al. Br J Haematol 2010;150:245-7.3. Borgna-Pignatti C et al. Br J Haematol 2004;124:114-7.4. Mancuso A. World J Hepatol 2010;2:171-4.

The Liver (2)
Musallam KM et al. Blood Cells Mol Dis 2012;49:136-9.
ChelatedNon-chelated
● β-TI (n=42)
● Median age 38 yrs, 50% men
● Hepatitis C negative
● 28 non-chelated, 14 chelated
● Two consecutive Transient Elastography (FibroScan®) measurements (median 2 yrs, range 1-3 yrs)
R2: 0.836P<0.001

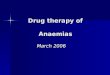
The Liver (3)
Musallam KM et al. Blood Cells Mol Dis 2012;49:136-9.
● ∆ TE in non-chelated patients:
4.4 to 5.7 kPa, P<0.001
● ∆ TE in chelated patients:
7.0 to 4.7 kPa, P=0.005
● ∆ TE/yr non-chelated vs. chelated:
+0.3 vs. -0.9 kPa/year, P<0.001
S <3 (n=11)
S 3 (n=1)
S 4 (n=1)
S 5 (n=1)
S <3 (n=11)
S 3 (n=3)
S <3 (n=28) S <3 (n=26)
S 3 (n=2)
First measurement
Lastmeasurement
Chelated
Non-chelated
Transient elastography values corresponding to fibrosis stages are: ≤7.9 kPa for S <3; >7.9 to 10.3 for S 3; >10.3 to 12.0 for S 4; and >12.0 for S 5.

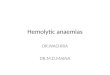
Other Morbidities
Musallam KM et al. Haematologica 2011;96:1605-12.
Morbidity absent
Morbidity present
p = 0.027
p = 0.490 p = 0.245 p = 0.682p = 0.002
p < 0.001 p < 0.001
p = 0.040
p < 0.001
p < 0.001
0
3
6
9
12
15
18
21
168 non-chelated β-TI, mean age 35.2 yrs, mean LIC 8.4 mg Fe/g dw
On multivariate analysis, a 1 mg Fe/g dw increase in LIC was significantly associated with higher odds of thrombosis, pulmonary hypertension,
hypothyroidism, osteoporosis, and hypogonadism
Adjusted for age, gender, splenectomy status, transfusion history, total hemoglobin level, fetal hemoglobin level, platelet count, NRBC count, and
serum ferritin level
On multivariate analysis, a 1 mg Fe/g dw increase in LIC was significantly associated with higher odds of thrombosis, pulmonary hypertension,
hypothyroidism, osteoporosis, and hypogonadism
Adjusted for age, gender, splenectomy status, transfusion history, total hemoglobin level, fetal hemoglobin level, platelet count, NRBC count, and
serum ferritin level

Other Morbidities (2)
Musallam KM et al. Haematologica 2011;96:1605-12.
MorbidityLIC cut-off(mg Fe/g dry wt)
AUC 95% CI p value Sensitivity Specificity AOR (95% CI)a
Thrombosis ≥ 7 0.669 ± 0.049 0.573–0.765 0.001 70.5% 61.3% 2.86 (1.22–5.91)
Pulmonary hypertension
≥ 6 0.684 ± 0.042 0.601–0.767 < 0.001 75% 58% 3.30 (1.54–7.08)
Vascularb ≥ 7 0.723 ± 0.039 0.647–0.800 < 0.001 66.3% 71.8% 3.76 (1.81–7.81)
Hypothyroidism ≥ 6 0.630 ± 0.056 0.521–0.739 0.025 76.7% 52.2% 2.65 (1.03–6.77)
Osteoporosis ≥ 9 0.796 ± 0.041 0.624–0.787 < 0.001 58.4% 81.3% 5.13 (2.46–10.71)
Hypogonadism ≥ 6 0.689 ± 0.053 0.585–0.793 0.002 78.6% 52.1% 3.35 (1.2–9.26)
Endocrinec ≥ 6 0.724 ± 0.039 0.647–0.801 < 0.001 71.3% 70.3% 4.05 (1.96–8.35)
aAdjusted for age, gender, splenectomy status, transfusion history, total hemoglobin level, fetal hemoglobin level, platelet count, NRBC count, and serum ferritin level. Model was built using forward-stepwise selection. p ≤ 0.1 was used as the criterion for inclusion. Multi-colinearity was absent in the model as evident from a variation inflation factor ≤ 3 (acceptable limit up to 10).bPatients having PHT or thrombosis.cPatients having hypothyroidism, osteoporosis, or hypogonadism.

Other Morbidities (3)
Musallam KM et al. Eur J Haematol 2011;87:539-46.
>0.8<0.7<0.5<0.3<0.1
Probability
Total Hemoglobin (g/l)
NTBI (µmol/l)
1.0
0.8
0.6
0.4
0.2
40 50 60 70 80 90 100 110 120 130 140
12
10
8
6
4
2
0
● 29 β-TI
● Splenectomized
● Mean age 32 yrs
● Significant association between the occurrence of large-vessel cerebrovascular disease (MRA) and high NTBI levels

Other Morbidities (4)
Musallam KM et al. Ann Hematol 2012;91:235-41.
● 30 β-TI
● Splenectomized
● Mean age 32 yrs
● Significant association between decreased neuronal function (PET-CT) and high LIC
1.0
LIC (mg Fe/g dry wt)
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0 5 10 15 20 25 30 35 I I I I I I
II
II
II
II
I
0

Association with vascular disease truly causal?
Splenectomyn (%)
Transfusion n (%)
LIC (mg Fe/g dw) n (%)
Vascular morbidity n (%)
+
P<0.001
P=0.016
P=0.001
N=168
No47 (28)
Yes121 (72)
Yes103 (85.1)
No18 (14.9)
Yes21 (44.7)
No26 (55.3)
<723 (88.5)
≥73 (11.5)
<727 (69.2)
≥712 (30.8)
<739 (37.9)
≥764 (62.1)
47 (73.4)
16 (41)
7 (58.3)
9 (33.3)
1 (33)
3 (13)
P=0.020
P<0.001
Mild phenotype (neither splenectomized nor transfused)
Moderate phenotype (either splenectomized or transfused)Severe phenotype (both splenectomized and transfused)
Musallam KM et al. Haematologica 2011;96:1605-12.

*p < 0.05; **p < 0.01; ***p < 0.001.
1.0
0.8
0.6
0.4
0.2
0
Pro
ba
bil
ity
of
va
sc
ula
r m
orb
idit
y
0 10 20 30 40 6050 70
Age (years)
LIC < 7 mg Fe/g dry wtLIC ≥ 7 mg Fe/g dry wt
*
**
Mild phenotype (neither splenectomized nor transfused)
Moderate phenotype (either splenectomized or transfused)
Severe phenotype (both splenectomized and transfused)
1.0
0.8
0.6
0.4
0.2
0
Pro
ba
bil
ity
of
va
sc
ula
r m
orb
idit
y
0 10 20 30 40 6050 70
Age (years)
LIC < 7 mg Fe/g dry wtLIC ≥ 7 mg Fe/g dry wt
**
Association with vascular disease truly causal? (2)
Musallam KM et al. Haematologica 2011;96:1605-12.

Musallam KM et al. Thromb Res 2012;130:695-702.
Hemoglobin
Denaturation Degradation
Excess α-chains
Hemichromes
Inclusion bodies
Band 3 clustering
Oxidation
ROS
Fe++
Spectrin & Band 3 abnormalities
PS exposure
PS
PSThrombin
FVa, FXa, FII
↓ Protein C & S
↑ RBC adhesion & aggregation
↑ Platelet activation& adhesion
↑ WBC activation
Fibrin
Endothelial damage/activation
Tissue factor, ELAM-1, ICAM-1, VCAM-1, VWF
Thrombus formation
RBC

Assessment of Iron Overload
● Serum ferritin
● Liver iron concentration● SQUID
● MRI
● Biopsy
● Cardiac MRI?
● Other markers (NTBI, Transferrin Sat)?
Musallam KM et al. Blood Rev 2012;26:16-9.

Spot Serum Ferritin Measurement
● Caution with interpreting spot serum ferritin values to tailor iron chelation therapy in NTDT
● The 1000 and 2500 ng/ml thresholds are used in thalassemia major patients as they predict survival and cardiac outcomes -> less relevant in NTDT and no similar predictive assessment exists
● Although serum ferritin correlates with LIC in NTDT1-4, the ratio of serum ferritin to LIC is lower relative to patients with β-thalassemia major1,4-6
1. Taher A et al. Haematologica 2008;93:1584-6.2. Lal A et al. N Engl J Med 2011;364:710-8.3. Taher AT et al. Blood 2012;120:970-7.4. Pakbaz et al. Pediatr Blood Cancer 2007;49:329-32.5. Origa R et al. Haematologica 2007;92:583-8.6. Taher AT et al. Am J Hematol 2010;85:288-90.

Serum Ferritin vs. LIC in TI and TM
1,0002,000
3,0004,0005,0006,0007,000
8,0009,000
10,000
0 5 10 15 20 25 30 35 40 45 50LIC (mg Fe/g dry wt)
Ser
um
fer
riti
n l
evel
(μ
g/L
)
TI TMLinear (TI) Linear (TM)
0
Taher A et al. Haematologica 2008;93:1584-6.

Conclusions
● NTDT patients show considerable iron overload despite their transfusion-independence
● Ineffective erythropoiesis leading to hepcidin suppression and increased intestinal iron absorption is the primary implicated mechanism
● Iron overload in this patient population is associated with morbidities involving several organs and organ systems
● Timely detection is warranted, and caution regarding serum ferritin level interpretation is essential