Embed Size (px)
Citation preview

EDITOR’s NOTE: Welcome to IPQ’s “Monthly Update” on key CMC/GMP developments in the US, Europe, and internationally. The IPQ family of publications includes “The News in Depth” and”Updates in Brief” on our website as they occur, “Weekly News Alerts” sent via e-mail, and the “Monthly Update.” IPQ’s suite of offerings support our mission of helping readers under-stand, engage in and respond to the dialogue and developments around evolving and harmo-nizing the regulation of drug and biologic quality and manufacturing. Subscribers and license holders to IPQ have access to all of these sources of cutting-edge news and in-depth analysis as well as to the full IPQ archives. Visit IPQpubs.com for further information.
Bill Paulson, Editor-in-Chief
MONTHLY UPDATE - FEBRUARY 2014
IPQWWW.IPQPUBS.COM
INTERNATIONAL PHARMACEUTICAL QUALITY
Inside the Global Regulatory Dialogue
VOL. 5, NO. 2
CMC/REVIEW
• Post-approval Change Regulatory Burden Draws Heat atJapan Biotech CMC Strategy Forum............................................2
• International Panel of Regulators Spotlights Current BiotechCMC Regulatory Problems and Convergence Pathways.......19
• Global Quality Regulatory Maze Jeopardizes VaccineSupply, IFPMA is Stressing.........................................................25
• Industry Proposals for Addressing Post-Approval ChangeBurdens Include Harmonizing on Commitments and Classifications.................................................................................31
INTERNATIONAL UPDATES IN BRIEF - p. 45
U.S.: • OTC Overhaul Plan • ICH Photosafety Guide-line • FDA Transparency • Secure Supply Chain Pilot • Drug Tracing Standards • Generic Drug Inspections• Compounder DQSA Warning Letter
EUROPE: • Biosimilar Substitution in France • EDQM Counterfiet Medicines Webpage • EudraGMDP Non-compliance Listings
INTERNATIONAL: • China IT Standards • Australia Biosimilar MAb Guideline • Australia/New Zealand Agency • Hamburg in India •FDA/EMA Pharmaco-vigiilance Cluster
IPQ is now on Facebook and Twitter. Come join the global regulatory dialogue.
BREAKING NEWS AT YOUR FINGERTIPIPQ’S RSS FEED

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COMFEBRUARY 2014 �
MONTHLY UPDATE - FEBRUARY 2014
International Pharmaceutical Quality TM (ISSN 1937-6898) is dedicated to helping its readers understand, engage in and respond to the dialogue and developments around evolving and harmonizing the regulation of pharmaceutical and biologic qual-ity and manufacturing.
Subscriptions and licenses include full access to IPQ’s news up-dates and in-depth analysis plus the full archives. See IPQpubs.com for individual subscription and company/organization license rates.
© 2013. All rights reserved. IPQ Publications LLC. Content cannot be transmitted except for internal use by companies/organiza-tions that have licenses. For copies/reprints for other use, contact Wayne Rhodes ([email protected], 202-841-9470).
INTERNATIONAL PHARMACEUTICAL
QUALITY™
Editor-in-ChiefBill [email protected]
Senior EditorJerry [email protected]
Chief Financial OfficerRob [email protected] ext.105
Sales/Marketing Coordinator Wayne [email protected]
ReportersTed Seabright [email protected] 571-213-6318
Aaron Kozloff [email protected] 240-678-4637
Food and Drug Law AdvisorEve [email protected]
7920 Norfolk Ave., Suite 900,Bethesda, MD 20814
INTERNATIONALPost-Approval Change Regulatory Burden Draws Heat at Japan Biotech CMC Strategy ForumIndustry associations have been meeting with Japanese regulators to highlight the problems they are experiencing in Japan’s process for regulating post-approval manufacturing changes, including a lack of flexibility around biopharmaceutical manufacturing changes that results in most requiring prior approval as well as meetings with the agency to resolve unclear expectations.
The Japan Pharmaceutical Manufacturers Association (JPMA) met with Japan’s Pharmaceutical and Medical Device Agency (PMDA) and Ministry of Health, Labor and Welfare (MHLW) in the latter part of 2012 to highlight concerns its membership had raised regarding post-approval changes. Of primary concern were the requirements for reconfirming shelf life and the disparity between Japan’s requirements and those in the U.S. and EU.
A 2013 meeting also brought in the Pharmaceutical Research and Manufacturers of America (PhRMA) and the European Federation of Pharmaceutical Industries and Associations (EFPIA) to provide perspectives from outside of Japan.
The post-approval change regulatory process in Japan and how it compares to approaches in the rest of the world was a key focal point of a CASSS “CMC Strategy Forum Japan,” held in December in Tokyo, at which Japanese industry and regulators were well-represented. Also in attendance were
regulators and industry representatives from Asia as well as from Europe and the U.S.
The first of CASSS’ Japan CMC Strategy Forums was held in Tokyo in December, 2012 (see IPQ “Monthly Update” Jan./Feb. 2013, pp. 50-62). A third in the series will be held in December of 2014, also in Tokyo.
CASSS also hosts a strategy forum in Europe in the spring supported by European regulators, along with the strategy forums it holds in the U.S. in January and July. The Europe forum this spring will take place May 5-7 in Sorrento, Italy.
Changes are a Japanese and Global Problem
The session on biopharmaceutical post-approval changes at the 2013 Japan meeting included: ● a detailed look by PMDA’s Futaba Honda at Japan’s regulations regarding submissions and changes ● JPMA’s perspectives on the current post-approval change requirements, presented by Takeda’s Takao Kojima ● the difficulties and challenges faced by industry when making post-approval changes in multiple markets by Amgen’s Toshiko Mori-Bajwa, and ● Genentech’s Lynne Krummen on managing post-approval changes using risk-based comparability concepts.
[Editor’s Note: Honda’s, Kojima’s and Mori-Bajwa’s complete remarks are included on pp. 8-18].

MONTHLY UPDATE - FEBRUARY 2014MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 �
INSIDE THE GLOBAL REGULATORY DIALOGUE™
PMDA’s Honda explained that most post-approval changes in Japan for biopharmaceuticals need to be filed using a “partial change application” (PCA), which requires approval prior to implementation, takes one year to approve, and includes an on-site GMP compliance check.
Specified lower-risk changes under the two-tiered Japanese system can be implemented at the time a “minor change notification” (MCN) is filed. PMDA assesses the MCN at the time a subsequent PCA is filed or during the next GMP inspection, whichever comes first.
Honda explained that biological product changes typically require a PCA because biological syntheses are less defined than chemical ones, produce less homogeneity in the molecular structure, and require a multi-dimensional analysis when changes are made to ensure that safety and quality are not impacted.
Takeda’s Kojima also reviewed PMDA’s change categories en route to discussing JPMA’s concerns.
Kojima’s remarks encompassed: ● the results of a survey of JPMA’s member company concerns with how changes are administered ● the association’s meetings with PMDA to voice the concerns and present alternatives ● Japanese requirements vs. those in the U.S. and EU, which shows that, in general, Japan’s requirements are more onerous, and ● the case for international harmonization.
JPMA’s survey revealed that, of 48 post-approval changes that needed regulatory notifications in Japan, the U.S. and the EU, there were some that could be filed in the U.S. as an annual report and handled in the EU as Type 1A variation, but in Japan required pre-clearance through a PCA.
Amgen’s Mori-Bajwa provided a broader view of the problems international firms face when trying to make changes in multiple markets.
She presented a revealing case study showing how a single manufacturing change applied across global markets can take as long as five years to complete and require 100 or more separate supply chain strategies to ensure market supply while the changes are being approved.
Mori-Bajwa explained that Amgen’s model for filing in multiple countries includes three “waves:” ● The first wave of filings are in reference countries with approval cycle timelines of six and twelve months. ● The second wave of filings goes to countries that do not require approval from a reference country filing, with approval times between nine and 24 months. ● In the third wave are countries that require reference country approval prior to filing, further extending the global clearance process.
The Amgen exec pointed to a variety of reasons that prompt changes during the lifecycle of a product. She highlighted the difficulties of managing approvals in multiple countries, and the increased work load that multiple variations cause for regulators. “They have limited resources to support all the changes that we are filing,” she noted. “Sometimes this can lead to delays in approval.”
The last presenter in the post-approval change session – Genentech VP Krummen – provided further insights on strategies to manage global changes, emphasizing the importance of risk management in post-approval change filings and approvals.
Krummen made a case for: ● continued dialogue regarding the realities of global manufacturing and supply ● embracing and implementing risk-based approaches for product development and life-cycle management with an emphasis on enhanced product and process knowledge and patient risk/benefit, and ● continuing to strive towards regulatory convergence and facilitating risk-based requirements and shorter implementation timelines.
Post-approval changes were also a front-burner issue at the CASSS/FDA WCBP Symposium in late January in Washington, D.C.
A plenary session was held at the conclusion of the conference, which provided a wealth of additional insights into the post-approval regulatory quagmire in which global companies are currently immersed. (See story on pp. 31-44.)
Other Key Biopharma Topics Explored
In addition to the session on post-approval changes, the Japan CMC Strategy Forum included four other sessions on key topics with which the international biotech community is actively engaged.
Setting the stage at the opening session were presentations on the “recent trends in the regulation of biopharmaceutical products” and how various stakeholder collaborations are impacting them.
The current regulatory landscape in the various regions was explored from the perspective of: ● PMDA by Office of Cellular and Tissue-based Products Director Jun Sakamoto ● FDA by Office of Biotech Products Director StevenKozlowski ● EMA by Head of Quality Peter Richardson ● India by Indian Institute of Technology Department ofChemical Engineering Professor Anurag Rathore, and ● the Asia Partnership Conference on Pharmaceutical Associations (APAC) by JPMA’s Kozo Akasaka.

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 �
MONTHLY UPDATE - FEBRUARY 2014
Biosimilarity was among the regulatory topics addressed in the updates. Receiving attention was the first EU approval a few months earlier of two monoclonal antibodies (MAbs) – Celltrion’s Remsima and Hospira’s Inflectra – both determined to be biosimilar to Janssen’s Remicade (infliximab). Remicade was originally approved in the U.S. in 1999 for the treatment of rheumatoid arthritis and inflammatory bowel disease. The EU approval process was highlighted as an important step that can provide a template for other agency evaluations of biosimilarity for monoclonals.
The second session explored control strategies for aggregates and particles in biopharmaceuticals, including the challenges of identification and quantitation.
Esai’s Yasushi Shikata presented an overview of the issues. Discussions followed by Kyoto University’s Takayuki Yoshimori and Biogen Idec’s Robert Simler regarding recent advancements in technology used for aggregate and particle characterization.
Simler focused on the 0.1-1 micron size area that has proven the most challenging to characterize. He provided examples of both new applications of proven techniques and novel analytical methods, such as resonant mass spec and nanoparticle tracking analysis, which “allow for an ever increasing characterization of the aggregate/particle populations of protein solutions.”
On the second day, following the discussion of post-approval changes, a session was held to explore how quality by design (QbD) is advancing in Japan and internationally.
The PMDA perspective was provided by Office of Cellular and Tissue-based Products Reviewer Yasuhiro Kishioka. Chugai Pharma’s Mikio Suzuki then provided “lessons learned” from a QbD biologics application in Japan for breast cancer therapy Perjeta (pertuzumab). Chugai is licensed to distribute Roche’s Perjeta in Japan – the first cancer drug approved to treat breast cancer pre-surgery.
The CMC section of the Perjeta application has received considerable international attention, having undergone a joint review through the FDA and EU QbD parallel assess-ment pilot program. While the joint review was resource-intensive for the agency, it proved highly informative on highlighting some differences between the two regions and has led to important discussions around how to further harmonize and standardize the biotech CMC and QbD approaches.
FDA granted Perjeta priority review status and approved the drug in 2012, along with Switzerland and Mexico. Approvals were granted in 2013 in the EU, Russia, Canada, Australia, Brazil, Korea, Taiwan, Japan, New Zealand, and South Africa.
The concluding presentation at the session was given jointly by two former top biotech regulators now working in industry – Kowid Ho and Patrick Swann. Ho left the French agency AFSSAPS to join Roche in the latter part of 2013, and Swann left FDA mid-year to join Biogen Idec. The two provided their perspectives on the evolution of QbD for biotherapeutic products.
Ho focused on the learnings to date from the FDA/EMA parallel assessment process. Among them is that: ● The agencies do not support the use of the term “key process parameter” (KPP) since it is not an ICH term and may be used differently by companies ● All parameters that have an impact on a critical quality attribute (CQA) should be classified as critical; and that ● A risk judged to be “critical” remains critical even if it is mitigated.
The final session examined new technologies in MAb engineering and the scientific, structural, and regulatory complexities of antibody-drug conjugates (ADCs).
It was noted that the promise of ADCs to increase the effectiveness of the antibodies while decreasing adverse reactions, such as in chemotherapy, has gone beyond proof-of-concept and into commercialization – with more than 30 products approved and over 200 under development.
Receiving attention were the challenges of developing appropriate analytical methods. It was noted that the methods used for antibodies may not be generally reliable for ADCs – for example, charge-based methods will give different results depending on the linker – and often need to be modified to be effective.
Tokyo University Institute of Medical Sciences School of Engineering’s Kouhei Tsumoto provided an overview of new technologies that are being developed to analyze antibodies and ADCs. Further input on characterization of and control strategies for ADCs, with Genentech Protein Analytical Chemist Fred Jacobson addressing lysine-linked products and Seattle Genetics Quality VP Charles Smith focusing on cysteine-linked ADCs.
At the conclusion of the CASSS CMC Strategy Forum Japan in December in Tokyo, Roche Biologics Regulatory Policy Head Thomas Schreitmueller provided a summary of each of the five meeting sessions (see box on pp.5-7).

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 �
INSIDE THE GLOBAL REGULATORY DIALOGUE™
Trends in the Regulation of Biopharmaceutical Products
The first topic we discussed was recent trends in the regulation of biopharmaceutical products. I was happy to see the remarks and slides from [JPMA Executive Director Hideo Utsumi] regarding his definition of pharmaceutical regulation – that it is a collaboration between industry, academia, and regulators. Really, I could not agree more with this. In fact, this is what we discussed over the last two days. This was, to a certain extent, setting the stage.
We then heard what is going on in the agencies. There is a lot of activity, whether you look at Japan, the U.S., or Europe. This is necessary to cope with all the things that are going on in new product development, QbD, tighter review timelines, and so on.
What we also learned is that there are new guidances and new approval systems underway – for example, exchanges with academia are taking place more and more. Special groups are being implemented in agencies to cope with QbD and other challenges.
With respect to biosimilars, we saw that the number of consultations is really increasing. Eventually it might be good if there were more exchanges between the agencies, especially on a global level, to ensure proper implementation of the respective guidelines. This is especially true when we look at emerging markets.
QbD, like in every conference, was an important topic. I found [FDA Office of Biological Products Director Steve Kozlowski’s] elaboration very interesting in starting critical discussions and collaboration about critical attributes.
Also important are the activities which we have seen in APAC [Asia Partnership Conference of Pharmaceutical Associations]. This is an example of ongoing harmonization efforts that is recognized in other parts of the world.
We had quite an extensive discussion regarding QbD. There is still limited experience on the biotech side, but we are moving along. What regulators criticized is that a risk-based approach is often not very developed by companies, and immunogenicity is seen as a very critical thing.
Like always, when we discuss QbD, this is still evolving. If you ask five different people about a certain term, previously, you would get five different answers. Now you will get two or three. There is still room for improvement.
We heard today that QbD is progressing in the analytical areas as well.
Biosimilars were quite extensively discussed, focusing on changes in new regulation with respect to sourcing of the reference material. It was also recognized that the monoclonal antibody guideline in the EU is really setting the stage with respect to biosimilar concepts.
We discussed that the link to reference products is getting weaker over time, with new guidelines now clearly saying that the biosimilar will have its own life-cycle. What does this mean for interchangeability, for example?
In the context of emerging markets, clearly, I think, leading agencies should take more responsibility with respect to education of other agencies.
The regulatory framework regarding cellular therapy products was also discussed. I think the common-sense view was that a risk-based approach is key for these kinds of products. It is a fast-moving field, and therefore quite
Summary of �01� Japan CMC Strategy Forum
At the conclusion of CASSS’ biopharmaceutical CMC Strategy Forum Japan in December in Tokyo, Roche Biologics Regulatory Policy Head Thomas Schreitmueller provided a summary of the five forum sessions, which covered: ● trends in regulation ● control strategies for aggregates and particles ● post-approval changes ● how QbD is advancing in Japan and internationally, and ● new technologies for antibody engi-neering and ADCs.

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 �
MONTHLY UPDATE - FEBRUARY 2014
challenging with respect to guidance development.
Harmonization was also mentioned with respect to orphan drug designation, which might be something to consider. Regulatory convergence in Asia, as pointed out before, we think is really a good thing and should be taken further. I have to say I was extremely impressed looking at the improvement of the review timelines that were presented by PMDA over the time.
Control Strategies for Aggregates and Particles in Biopharmaceutical Products
We then discussed aggregates and particles and their importance for biopharmaceuticals. Clearly, we have methods in place, but they are interpreted in many different ways. The measurement itself, especially if you think about visible particles, is something that is highly subjective. We get more and more methods these days that allow more accurate detection of aggregates and particles, and even further characterization. What we also can say is that we really have made a lot of progress with respect to composition analysis of these mixtures. We can ask more questions, but are these academic questions? Or do they really add value with respect to product development?
With respect to immunogenicity, I think there is no clear evidence for the relationship to particles. We have certain hints that there might be something behind it, but we always have to keep in mind that there is not a very straightforward study that would show us that it is actually related.
Independent of this, aggregates have to be controlled as an impurity. I think we have a handle on this as well. The question now seems to be where and how to control the process and what method to apply.
Post-Approval Variations for Biopharmaceuticals
We had very interesting discussions around post-approval variation of pharmaceuticals. PMDA explained that a new API, strength, dosage form or brand name requires a new application. A partial change application [PCA] will be followed by a one-year compliance check. Process change categories are to be specified by the applicant. Details regarding how these compare to the U.S. and EU were discussed.
Then we also had a very interesting survey by JPMA, which I think is quite a solid piece of work, given the numbers of companies and variations that they examined. What was interesting was that most of the variations really related to the manufacturing process and analytical methods or specifications. The vast majority, of course, were handled as partial change applications. JPMA hopes that eventually there might be some relief with respect to that burden.
Most critical of these was how shelf-life is established after variations. There have been proposals developed by JPMA concerning this.
One proposal is that a more risk-based approach might be appropriate in cases where comparability has been demonstrated – that good comparability of the drug substance change should not impact the shelf-life of the drug product. Continuous dialogue between local and global stakeholders is helpful and essential….
We also saw some presentations concerning the global post-approval change situation, including some case studies where it became clear that for certain changes you actually need five years until you can have global implementation. I think it is clear to everybody that this is not an acceptable situation and we clearly have to work on this to improve the situation. The key is convergent harmonization. From my personal experience knowing many of these agencies, I have to say the way forward has to be mutual recognition and collaboration between the agencies in order to improve the situation.
We had a nice presentation on comparability and what we should do there. I think it became clear that this requires a risk-based approach. But it is not just doing an analytical comparison on the results and deciding what else to do. It is clear that you need to decide right away on the proper strategy of what you should really do. Again the message came out that in fact these different regulations that we have all over the world, rather than helping, eventually are putting more risk on the supply chain.

MONTHLY UPDATE - FEBRUARY 2014MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 �
INSIDE THE GLOBAL REGULATORY DIALOGUE™
We do a lot of things at manufacturing sites, and we heard comments from the agencies that they are not aware of all the data that we have. There certainly is a bit of mistrust, on both sides, which then also may lead to delays. But the key is once they go in the direction of global harmonization, then they really may be able to solve this.
The important role ICH members have was discussed because they are setting the stage. I think the whole world is looking at these ICH requirements and how the countries are implementing these regulations. I think the closer we work together, the closer we interpret things, the more impact this will have for all the other countries.
There was an interesting discussion talking about variation in guideline generation. Should they be more prescriptive? Should there be a lot of examples? Would this add clarity? I really did not sense the opinion going clearly in one direction or the other. And it is clear that there are advantages and disadvantages of both. You lose a lot of flexibility the more examples you put in, but then you also have clarity at the end, and you can plan for it.
QbD Case Study
Regarding QbD, I am still dizzy with respect to critical quality attributes, CQAs, CPPs, and I do not know how many other abbreviations have been used during this discussion. We still have open questions and there is still learning going on. This was, for me, the key message of the discussion. We have made a tremendous amount of progress over the last years. In fact, this resulted in the first approval of a QbD application including design space in the US for a biotech product.
Whether we like it or we do not like it, it will set the stage. It will set the development stage for the future, because people have recognized that this systematic approach really will lead to rational designs of control systems and so on. This is why, eventually even for orphan drugs or breakthrough products, there were will be no way around using the principles here.
As pointed out before, in using QbD for analytics, regulators are open for discussion. I think this was the key message. So let’s take this opportunity, and during the next forum have a session on this topic.
New Technologies for Antibody Engineering
Concerning ADCs [antibody drug conjugates], what was interesting to me is that there are now thirty-four ADCs in development – I was not thinking there were already that many. It is really great that that much work has been done. I think there are lots of challenges. We heard during the presentation and also during the discussions the challenges related to the formulation, the linker, stability issues, manufacturing changes, and so on. I think it is a challenge to make these ADCs. I think that was made very clear during the presentation.
The good news is that we have a lot of analytical methods, which we are using for characterization, and also for establishing a control system. The orthogonal method, for the complexity we are dealing with, is highly critical.
QbD principles might be applicable for individual components. It still might be difficult for the whole product, but eventually could be used for small molecules and for antibodies.
We also had discussions around starting materials for intermediates. The message here was that all these intermediates are practically treated as an individual API at the moment.
[Story continues on p. 8 with the presentations by Honda, Kojima and Mori-Bajwa.]

Best Practices for Managing Emerging Trends and Challenges of CMO Oversight and Other Service Providers
STRATEGY FORUM
ADVANCING BIOPHARMACEUTICAL DEVELOPMENT
July 21-22, 2014 Gaithersburg Marriott Hotel, Gaithersburg, MD
SCAN to browseC AS S S for program
updates at casss.org
Forum Co-chairs:
Siddharth Advant, ImClone Systems CorporationJulia Edwards, Genentech, a Member of the Roche GroupJeffrey Staecker, Genzyme, A Sanofi Company

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 �
MONTHLY UPDATE - FEBRUARY 2014
PMDA’S FUTABA HONDA ON REGULATIONS IN JAPAN I am from the office of in charge of review of biopharmaceuticals at PMDA [Pharmaceuticals and Medical Devices Agency]…. I would like to talk about the post-approval change regulations in Japan regarding the partial change applications in Japan, and what regulations apply here in Japan.
This is the agenda for today – there are four points:
● Number one is that in Japan within the application forms there is a part related to manufacturing methods and partial change applications.
● There are procedures to make the submissions, and the associated standard review periods and procedures for that.
● There are two types of change procedures here in Japan: There is a partial change approval application and a minor change notification.
● And number four is about making partial change applications and what sort of data would be expected from the regulatory authorities.
I will be using these abbreviations: PCA, for partial change approval applications; and MCN for minor change notifications.
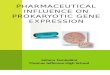
This is the CTD structure that is agreed upon within ICH (see box at right). Under M1, we have administrative and prescribing information related to manufacturing methods, the summary of which is given in M2.3, Quality Overall Summary, or QOS. M3 gives the manufacturing method information.
There is an application form for marketing approval. And within that, the items written there, include the brand name, ingredients and quantity, annex specifications, and manufacturing procedures. It also includes dosage administration, indications, storage conditions, periods of validity, spec and test methods, and manufacturing sites.
Within the application document are the requirements for the appropriate change procedures. It will be a PCA or an MCN.
Presentations from Post-Approval Change Session
The following are the complete remarks made by PMDA’s Futaba Honda, Takeda’s Takao Kojima, and Am-gen’s Toshiko Mori-Bajwa at the post-approval change session of the Japan CMC Strategy forum. Honda, a biopharmaceutical reviewer for PMDA, provided a detailed look at Japan’s post-approval change require-ments and procedures [see below]. Kojima focused on JPMA’s concerns with the current approach in Japan and how the requiresents differ from those in the U.S. and EU [see p. 11] . Amgen CMC Regulatory Affairs Director Mori-Bajwa provided a broader view of the problems international firms face when trying to make changes in multiple markets, including a revealing case study on the complexities and timelines for making the changes, and a “wave” model used by Amgen [see p. 15]. [Editor’s Note: Honda and Kojima delivered their presentations in Japanese. Provided below are the translations done simultaneously at the session.]
CTD Structure
M3:Information on Quality
M 4:N onclin ica l
S tudy R eports
M 5:C lin ica l
S tudy R eports
M2:S um m aries
2.3 quality Overall Summary
M1:Administrative Information
and Prescribing Information
Brand NameIngredients and Quan�ty Annex Specifica�ons Manufacturing procedures Dosage and Administra�on Indica�onsStorage Condi�ons
and Period of Validity Specifica�ons, Test Methods Manufacturing Sites
Application Formfor marke�ng approval
Any changes in the ma�ers entered in the Application Form shall be addressed in a PCA or a MCN.

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 �
INSIDE THE GLOBAL REGULATORY DIALOGUE™
So number one, under M3, as you may be aware, are the manufacturing methods, and the manufacturing site-related information for the drug substance [DS] and drug product [DP]. They will be put into the respective chapters in accordance to the ICH guideline.
In M2, the overview for development strategies will be provided based on the information in M3. In the application forms, there will be different items specified under which the essence of the critical information will be given. In Japan, information in the application form is what is approved. If there is a change applied, then you need to take up some procedures related to change regarding M3 and M2 when making the original submissions. If there is a PCA, it will need to be submitted, but they will not always require exhaustive change procedures.
For PCA and MCN, these are the standard periods and procedures (see box below).
After the PCA submission is made, one year is the standard review period, during which, of course, a review will be taking place. Within the review period there will be a GMP compliance check as well. This is not PMDA – the quality control office will be in charge of that GMP compliance check.
The check will probably happen six months before the expected approval time. You need to make an application for that GMP compliance check. Therefore, after the initial submission for change, within this period, you have to verify the application information. According to the information, the reviewers will also be preparing for GMP inspections. The approval will be expected at about one year’s time. After that, you will be able to ship the products with the changes.
In Japan, after the MCN change is applied – for example, if there is a change in manufacturing methods – the shipment of that first product with the change will be that day. And within thirty days of that you have to notify the regulatory authorities. The content of the notifications will not be subject to review right away. But if there is a new PCA, or if there is a periodic GMP inspection, the inspector will be reviewing or checking the contents of the MCN.
Comparing the change categories between the EU, US, and Japan MCNs: Between the EU and Japan, there are two major categories for applications and notifications, and in EU there is Type IA and Type IB. In the U.S., on top of that you have an annual report as well.
Regarding notifications in the EU, you have the notification before a change, and after a while, if there is no response, then you can affect the change. But in Japan, notification will happen only after the change is applied. So there are different categories by market regarding which one you should be applying. If it is critical, you need a PCA. If it is minor, then you can use the MCN.
As already mentioned regarding the MCN, there is no review happening right after that. It would happen only during the next GMP inspection or PCA submission. During the next periodic GMP inspection, if the MCN content was reviewed and it was found that it should have been a PCA, then the MCN will be invalidated. Once it has been invalidated, if the change was applied to the product and it was shipped, then according to the regulations there may be some administrative actions taken depending on the risks that such a change may have posed.
I would like to explain what sort of classifications there are regarding the general principles for deciding whether the change is a PCA or MCN.
Standard Periods and Procedures for PCA and MCN
Minor change no�fica�on
Par�al change approval applica�on
O ne year
A pprova l app lication A pp lication for G M P inspection A pproval
S hipp ingS ix m onths
N otificationNext PCA, GMP periodic inspection
S hipp ing
W ith in 30 days

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 10
MONTHLY UPDATE - FEBRUARY 2014
Regarding MCNs, the scope of an MCN are those other than specified here. This is very conceptual, by the way. If it does not fall under these definitions, you can use the MCN.
For biological products, according to the notifications issued in 2009, changes to items under manufacturing methods will require a PCA, in principle.
The reason for that is that biologics, unlike chemicals that are manufactured based on chemical synthesis, will utilize a biological synthesis process in biological bodies. Due to the mechanisms, there may be some inhomogeneity in the molecular structure. There are limitations to the physical chemical analysis. By changing the manufacturing method, the assessment to impact on quality and efficacy will require a multi-dimensional analysis. Therefore, there are many features, unlike the chemical synthesis products. That is the reason for the PCA.
Another aspect is that biological products consist of various kinds of materials such as proteins, glycoproteins, polypeptides and their derivatives, and there are extracts from biological bodies as well. Therefore, they require different controls. So unilaterally, we cannot specify what changes could use an MCN. So we think these changes require PCAs rather than MCNs.
The change of manufacturing site requires an adequate change control system. Therefore a PCA is required, because changing a biologics manufacturing method may impact quality. Changes related to facilities for inspection and testing would only require an MCN. Therefore, even if it was the same manufacturing method, once the manufacturing site changes, the impact needs to be assessed and reviewed by the regulatory authorities. When you submit the PCA, the process validation data at the new manufacturing site and the lot analysis results will be required to be submitted.
Regarding spec and test methods, this should be addressed, in principle, by PCAs, just like for a chemical synthesis product. However, if the acceptance criteria changes to become stricter, then such a change may be addressed in the MCN.
Regarding the expiration dating for biologics: In principle, you need to address it by means of PCA. When making submissions, you need long-term storage testing based on the real storage conditions.
Now I will talk about manufacturing methods, which is the main part of my talk. I will cover which changes will be a partial change, and which will be a minor change.
You need to include certain descriptions in the manufacturing method column in the application form. The processes required to ensure the quality of the drug shall be described. The control items should be clearly stated, and by doing that, GMP compliance can be verified. It is necessary to clarify all of the process operations and the manufacturing methods, including targets or set values, protocols and SOPs, and how they are controlled according to GMPs.
In actual production, if there are outliers, they should be handled as a deviation in terms of GMP compliance, and there are some considerations for the description and how you prepare the document. Where there is a change in a manufacturing method, whether that change will fall into a PCA category or not should be determined by the applicant and mentioned in the document.
The items should cover the flow of the manufacturing process – for example, raw materials, or cell banks, in the case bio-genetically modified protein products. Cell bank management should be described, including when they are updated and what procedures are to be followed. Also include the established criteria for proper process control and
Changes Requiring a PCA in Japan● Deletions or changes of specifications and test methods
● Change of the manufacturing processes regarding inactiva-tion or elimination of pathogens
● Additions , changes, or deletion of dosage, administration, and indications
● Any other change that may affect quality, efficacy or safety of the final product

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 11
INSIDE THE GLOBAL REGULATORY DIALOGUE™
the sources of the biological materials.
Regarding process parameters, what should be PCA and what should be MCN? If there is almost no impact on the product, it is MCN and no additional data would be needed. In other cases, applicants need to use their judgment to decide what to include in the PCA or MCN – for example, validation data, equipment operation procedures, risk-management, design of experiment results, or prior knowledge. Those pieces of information will be included in the M2 or M3 document.
Regarding target values and set values, those will be included in the MCN using『 『parentheses and in the PCA using << >> parentheses.
An allowable range for the target value or set value must be established in the product master formula or SOPs.
However, if these parameters are set for parametric release – for example, for homogeneity – or if the parameters can affect the quality significantly, it is necessary to specify an allowable range on the approval application form rather than a target value or set value.
In the event it is evident that there is an extremely low possibility of the change having an adverse impact on the quality or safety of the final product, an MCN may be applicable. For those cases, the applicant may make such a proposal when submitting an approval application. The proposal will be judged during the review as to whether it can be accepted. As an example of an applicable case – the allowable range for process parameters at the same manufacturing site – that is proposed at the time of application and may be changed during the review for approval or on the occasion of the actual production results.
Regarding changes in manufacturing method, regardless of the impact you would need adequate validation and change control, either for a PCA or an MCN, regardless of the magnitude of the impact of quality. You have to submit the changes based on Q5A and Q5E.
Regarding the documents that need to be prepared, you can have a simplified consultation with PMDA, and you can use that opportunity to decide if the protocol is adequate or not, and the agency judgment on whether there is an impact to quality and other items can be consulted through that formal process.
TAKEDA’S TAKAO KOJIMA ON JPMA’S PERSPECTIVE
The main topic of my presentation is a review of the current regulations in Japan regarding quality and our vision for the regulations.
In the biopharmaceutical committee, we discuss change management at the post-marketing stage. We have participation from each of our member companies. We talk about and research the issues and conduct questionnaires.
Today, based on the results of the questionnaires, I would like to present four topics:
● The first topic is the current status of administrative regulatory procedures. In the previous session, Ms. Honda explained the procedures in detail, so I would just like to briefly touch on this topic.
● The second one is a proposal on the administrative regulatory procedures based on the questionnaire results: I would like to cover the requests we gathered from the respective pharmaceutical companies.
● Number three is an overview of discussions on post-approval changes between JPMA, PMDA and EFPIA and what we have submitted to the authority.
● Last, for the biopharmaceuticals product development, to be able to facilitate product development, I would like to introduce what we are doing as a committee and our vision.

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 1�
MONTHLY UPDATE - FEBRUARY 2014
First of all, I would like to cover the current status of administrative regulatory procedures. [Kojima briefly reiterates Japan’s regulatory procedures, which Ms. Honda explained in detail above].
This does not incorporate all the items, but here are some examples of the items which are applicable for PCA and MCN for biotechnology products and synthetic products.
These are just some examples. For biopharmaceuticals compared to synthetic products, only limited changes are within the scope of minor change notifications….
As Ms. Honda explained, for the parameters within the scope of MCN, it is possible to use those marks listed here, and the legitimacy would be determined in the reviewing process. Compared to synthetic products, for bio-pharmaceuticals it is very limited.
Survey of Changes Shows Disparities
I would like to give some examples we collected as a result of the questionnaires. Here is the purpose or objective of this questionnaire: In the biopharmaceutical committee, we identified what kinds of administrative and regulatory procedures we have as challenges. That was the overarching objective – to list those challenges. We have listed some actual cases of those change variation cases and we have made a proposal to the authority.
This questionnaire took place from May to June of 2011, and involved 36 pharmaceutical companies, which are the members of the biopharmaceutical committee of JPMA. We received responses from 32 companies out of 36, so it was an 89% response rate. We had 21 Japanese companies and 11 non-Japanese companies respond.
For the change cases, we have gathered over two-hundred cases. Further analysis was based on 99 variations and 43 proposals, with detailed information provided by 18 companies.
Here is the breakdown of the products of those variations: ● mammalian cell culture products make up thirty-eight cases ● recombinant microorganisms thirty-five cases ● fourteen cases for recombinant vaccines, and ● twelve cases for animal cell products that were not recombinant.
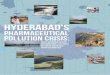
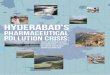
Here is the graph of the number of cases by the types of changes (see box below). Here are the actual changes that took place by ingredients and contents, manufacturing process, specification of API and drug product, storage and shelf life, manufacturing sites, and others. The parts in blue are handled as PCA, and the green represents the minor change notifications or MCNs.
The number of changes related to the manufacturing process is over fifty, so that was the most. Next were the changes related to specification and testing methods. What the MCN and PCA ratio tells us is that most of the cases you see are blue, so there are more cases that needed to be handled as PCA.
I would like to talk about what kind of specific cases we had within the MCN scope. For the minor change notification cases, there were seventeen cases. To give a breakdown, the changes related to the manufacturing process were seven, the specification and testing method was one, manufacturing sites had six, and the ‘other’ category three….
Here are some overseas cases. I have made some comparisons between Japan and overseas. In overseas markets, there were forty-eight cases reported for changes taking places. Out of those forty-eight cases, the sorts of changes
Examples of Japan Change Filing Categories: Biotech vs. Synthetic
Biotechnology products:Par�al Change Applica�on (PCA) Minor Change No�fica�on (MCN)Package form change/addi�on Tes�ng site change/addi�onSite change/addi�on (DS, DP, packaging, storage)
Manufacturing process change iden�fied in the applica�on form and jus�fied in the CTD
Ingredient changesManufacturing process changeTes�ng method change
Synthe�c products:
Par�al Change Applica�on (PCA) Minor Change No�fica�on (MCN)Package form change/addi�on Site elimina�on (one of several sites)Site change/addi�on (DS, DP) Site addi�on (storage, packaging, tes�ng)Ingredient changes Manufacturing process change iden�fied in
the applica�on form and jus�fied in the CTDManufacturing process change Tighten specsTes�ng method change

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 1�
INSIDE THE GLOBAL REGULATORY DIALOGUE™
that took place in the US are listed here on the top. Here is the number of actual cases listed next to it, and in the EU as well.
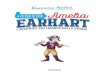
In Japan, it lists what kind of change procedures are needed to take place, either partial change or minor change. Comparing Japan and overseas, the measurable gap was observed in annual reports. In the US, some could be handled in the other parts of the annual report, but in Japan we needed to file a partial change. Those are the three cases. In the EU, it was handled as a Type 1A. But in Japan, we needed to file a partial change application for one case.
JPMA Members Request Simplification and Clarification
Now I would like to move on to the second topic of my presentation. We have done these surveys, and as a result we have identified requests that were expressed by the member companies. Altogether, forty-three proposals were identified in the questionnaire.
This is the breakdown of the requests: ● There were twelve proposals about the setting of shelf-life ● a simplification of administrative procedures had twelve proposals ● there were eight on clarification of administrative procedures requests; and ● eleven other requests.
Because of the limitation of time, I would like to focus on setting of shelf life and simplification of administrative procedures.
Regarding requests for the setting of shelf-life when changes are made to the production method, comparability needs to be established. There is a possibility of a reduced shelf life. For example, if three years was the shelf life with an older drug, and the manufacturing process changed, because of time limitation you may only have data for one or two years for stability. So the original shelf-life was three years, but was reduced to two years because the data submitted only covered two years. Approval is only given for the data which is available at the time of the submission.
With this as a background, member companies have made requests. The basic assumption is that before and after the change, if product comparability needs to be established, a high level of comparability should be established. If
Post-Approval Change Classifications in JapanThe following is a representation of data regarding post-approval change classifications in Japan collected by JPMA from its members.
0
10
20
30
40
50
Ingredient and Contents
Manufacturing SpecificationProcess and Testing
Type of Post-approval Change
Method (drug Method (drug Shelf life substance) product)
Storageand
Manufacturingsite(s)
Others
PCA: Partial Change Application
M CN: M inor Chang e Notification
16
45
22 23
14 14 15
1
7
1
5 3
Specificationand Testing
60
Num
ber o
f Cas
es

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 1�
MONTHLY UPDATE - FEBRUARY 2014
system comparability is established, based upon the experiences and achievements in the previous years, and if it was determined that the change never had impact on the product after the change, and if the comparability can be demonstrated in terms of the safety and efficacy, instead of establishing a new shelf-life, the shelf life pre-change of the product should be able to be used for the product after the change.
Setting Shelf Life
This is the first request which we have identified from the questionnaire. Stability data will be gathered and it will be used for the internal purposes, but should not be required to be submitted to the health authority.
The second request that we identified has to do with when quality and efficacy and safety are not impacted as a result of the change. If you do not have enough experience with the performance of the previous site to demonstrate comparability, and if there is a need to gather long-term data to ensure comparability, then the shelf-life should be established based on product data at the new site. During the course of the review, we will commit to the authority that we will gather safety data, based upon the protocol, and when the long-term safety data is obtained, then we will go through the MCN instead of the PCA. Currently, this kind of approach is not accepted, but our expectation is that in such a case only a minor change notification will be required.
For the purpose of extension of the shelf life, these are the approaches taken by the rest of the world.
In the case of the United States, based on the approved safety protocol when the shelf life is expected to be extended, the annual report is enough. Likewise, in Europe, a Type IB will be required. However, here in Japan, based on the safety protocol, the safety study needs to be done, and when the shelf-life is to be extended, the PCA procedure has to take place. The review period will be twelve months.
Given this background, member companies asked us to request changes in how shelf-life is set.
Likewise, similar requests were expressed about site changes. If the sites are highly similar, the shelf life of the product produced at the new site should be the same as that for the product produced at the old site. Stability data would be used only for in-house purposes and would not be submitted.
Simplification of Administrative Procedures
The next request is about the simplification of administrative procedures. As was mentioned before, when there is a change made to the manufacturing method for biopharmaceuticals, the basic principle is to apply the PCA – the partial change application procedure. Even with appropriate change management and control, unlike the case of a chemical synthesis, we have to go through the partial change application. If the change has little impact to the biopharmaceutical, then we think it should be handled just like for chemically synthesized products.
There are differences between the procedures followed in Japan and the rest of the world. In Japan, a PCA is required for most of the cases. Currently, here in Japan, we only have two approaches – one is PCA, and the other is MCN. In the United States and Europe, there are CBE-30 or Type 1B approaches. And also in the United States, if the comparability protocol is submitted prior to the change, and if it is approved, then there is a possibility of reducing the level of the requirement. These are the main differences between Japan and the rest of the world in terms of the
Post-Approval Change Requirements in the U.S., EU, and Japan
The following is data representing 48 change proposals reported to JPMA from its members and the corresponding classification requirements in the U.S., EU, and Japan.
U.S. JapanPCA MCN
Annual Report 4 3 1CBE 2 2 0CBE-30 5 4 1PAS 18 17 1No answer 19 18 0
EU JapanPCA MCN
Type IA 2 1 0Type IB 3 2 1Type II 26 25 1Extension Applica�on
0 0 0
No answer 17 16 1

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 1�
INSIDE THE GLOBAL REGULATORY DIALOGUE™
procedures to be followed.
The third topic stems from requests that we looked into on the biopharmaceutical committee. When it comes to the administrative procedures associated with the changes for biopharmaceuticals, unlike the chemically synthesized product’s administrative procedures, there is not a very clear description of what we have to do, so a case-by-case approach has to be taken. As a result, we have to talk with the health authority every time we have to go through those changes.
Nowadays, the development of biopharmaceuticals has been advanced. As a result, the health authority has accumulated lots of experience reviewing biopharmaceutical products and changes. Based upon on those accumulated experiences, we would like to request to the authority to simplify and improve the administrative procedures. That is why we have decided to compile our requests and ask for an opinion exchange with the health authority.
We have had discussions with the health authority. The first meeting was with MHLW, PMDA, and JPMA’s Biopharmaceutical Committee and Regulatory Affairs Committee. That took place last year. When the second meeting took place, PMDA, JPMA, PhRMA, and EFPIA participated. The contents of the meetings cannot be described here in this room, because of limited time, but I would like to tell you that these meetings were very fruitful and productive….
Summary
In summary, we would like to further promote the development of pharmaceutical products. We have identified some of the issues and challenges. As far as biopharmaceutical products are concerned, unlike for chemically synthesized products, we have limited knowledge and experience. So what we have to do is promote collaboration between industry, academia, and the health authorities.
The first thing we have to do is to create an environment that will allow for collaboration among these three parties for the development of biopharmaceutical products. As an expert committee here in Japan, we would like to make a proposal to the health authorities and ask for the clarification, if possible. We would like to approach the health authority and have very fruitful and productive discussions with them at this CASSS CMC forum. We appreciate this kind of opportunity to discuss the improvement of procedures with the regulatory authorities.
AMGEN’S MORI-BAJWA ON THE GLOBAL PROBLEMS
Today I am going to go over some of the difficulties and challenges facing industry as we globalize and commercialize.
First I would like to review some of the types of changes that we make. As you know, there is a spectrum of changes, and some of them are minor in nature – such as changing a filter supplier – and carry very low risk. And the analytical data package supporting process studies that go with that, because they are lower risk, are essentially minimal.
But as we move up the spectrum into more complex changes that carry moderate risks, such as moving to a new production facility, the data package increases and the studies supporting that change also increase. As we move up the spectrum to the higher end – for example, when we introduce new cell lines or major formulation changes – we also need to have clinical studies to support those changes. All the changes that we make are typically governed by the fundamental basis of Q5E.
So why do we make changes? We make changes for a number of reasons throughout the development of the product. We make changes during the clinical phase of the product, and once we commercialize we make changes to the process, facility, and scale. We have new manufacturing technology. We may introduce a new media heat treatment platform to inactivate viruses that may be in our raw materials to prevent drug substance contamination as a risk mitigation program. We may introduce isolator filling technology to prevent drug product contamination.

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 1�
MONTHLY UPDATE - FEBRUARY 2014
We may also have new testing technologies…. We may introduce NMR to check for adulterated raw materials, or mass spec to do multi-attribute testing. We also have regulatory agency expectations – for example, serialization. Serialization is a new requirement that has been implemented across many countries and health authorities, and not all of the guidelines and regulations for serialization are the same.
Also, we need to add second sites for facility risk-mitigation. Or we need to add second sourcing for critical components or raw materials.
We make these changes throughout the development of a product. We make them during clinical development. And then we make changes during the post-approval phase.
We can make changes for a number of reasons that I have already mentioned. During development, we typically transfer the process from the clinical site to the commercial site. And we also introduce scale changes along the way to accommodate the market demands as we get prepared for launch.
All of the changes that we implement are governed by the quality system for change control. For each change that we have to make, we have to make an assessment whether it is reportable or not reportable. And if it is reportable, we need to know what kinds of restrictions will be placed on the product. For each and every application that we have in clinical trials, or in a marketing application, we have to make an individual assessment. It can be a complex process. Depending on your program, you can have hundreds of individual assessments that you have to make for one particular change.
Herein lies the problem. We make changes. We are going to continue to make changes. And as we make more changes throughout the development of our products, we increase the complexity in our supply planning. Where we have to manage the approvals in multiple countries, it creates a big burden on our supply chain management.
We also are increasing the burden on our regulators. We are making multiple changes, submitting multiple variations, and it increases their workload. They have limited resources to support all the changes that we are filing. Sometimes this can lead to delays in approval.
While we can increase inventory to cover the gap between approvals, it is not always an easy thing to do. It often creates increased costs, and there can be supply scrap risks where we have countries or products with limited stability to cover that gap in time. So when we start planning for changes, we ultimately have to decide how we are going to file
A Change/Risk Continuum
Change filter supplier
Move equipment within same facility
Move to new production facility (same company)
Change cell culture media
New celllineor major formulation change
Nature of Process Change
Risk Factor &Data Requirements Lower Risk
Commonly implemented- Analytical data- Process studies
Moderate Risk
- Analytical data- Process studies- Stability data
Higher RiskLess commonly implemented
- Analytical data- Process studies
- Stability data- Clinical data
Innovator Process ChangeGoverned by comparability guidance (ICH Q5E)
Fundamental Basis of Comparability Guidance (Q5E)
Same Manufacturer, Same Product …..Continuity of data, experience and knowledge about the product & process eg.� Access to retention samples� Ability to compare in-process parameters and samples� Access to the drug substance� Historical, data-based, understanding of critical quality and clinical attributes

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 1�
INSIDE THE GLOBAL REGULATORY DIALOGUE™
in many countries that we are going to file a change in, and what emerges is that there are three distinct waves.
The first wave is our core country or our reference country. And that is the first filing wave that we make. After we prepare the submissions, those approval cycle timelines can take between six and twelve months.
The second wave that emerges is for the non-reference countries. These are countries that do not require approval from a referenced core country before we start filing. But those data packages have country-specific requirements. They might have different formats. So it takes time to make those submissions. And those approval cycles for that second wave tend to be longer – between nine and 24 months.
That third wave that we encounter are the countries that require reference country approval. So we cannot even begin filing until we have approval in the core countries. That creates a bigger gap in time to implement a change. The wave three countries can be even longer in their approval cycles. Over time, you get an additive effect of increasing the time it takes to implement a single change.
Now I am going to test your math skills. We do not only make a single change, per year, per product – we make multiple changes for a product per year. This is a little bit of an extreme case, but I think it is a good example to show you how complex the process can be.
I talked about the waves. In wave one, say we have five jurisdictions. We are making four changes per year, and that jurisdiction’s review cycle is one year. That can lead to up to 10-20 different supply chain strategies for one product per SKU for one presentation.
Then we move into the wave two countries, and those can be up to 50 jurisdictions with a cycle time of two years. Doing the math, we see eight versions per jurisdiction, which can lead to 200-400 different supply chain strategies on top of the ones that we have from wave one.
In wave three, there is usually a smaller number of jurisdictions. But as I mentioned before, they have a longer cycle time. So we can end up with 12 versions per jurisdiction, and this is for CMC changes only. This calculates to around 108-216 different supply change strategies.
While this is an extreme example, you can see that our supply chain is completely maxed out and complicated by the number of changes that we are making, and by the review cycles and cycle times across the global regulatory environment.
Now I am going to give you an example of a real case study where we transferred the drug substance manufacturing site. This process took over five years. We went into 96 countries beginning in 2009 with this particular manufacturing site change.
One of the key challenges that we had to plan for when we were implementing this change and planning how we were going to file the change in the different waves was that the changes were not all equal in classification across countries. For some, it was only a minor change. For some, it may be a new registration. For others, it may be a prior approval.
I mentioned that the approval timelines across the regions are quite different and they add to the complexity. So we had to manage the approval times, and be able to manufacture the product with the original process, and create enough supply to cover the gap in time across the approval timelines.
We also had to keep in mind those countries requiring a certificate of pharmaceutical product. I mentioned that we have core countries that need to be approved prior to being able to file in those wave three markets. We also have to be cognizant of specific country requirements where, in some countries, for a drug substance change, we have to have twelve months of real-time stability data. Complicating that, there are countries where we also have to manufacture that drug substance into drug product, and we have to have an additional twelve months stability data on that drug product before we can even file.

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 1�
MONTHLY UPDATE - FEBRUARY 2014
Each country has different reporting requirements and specific content requirements. Some of them require executed batch records. Certificates of analysis are pretty typical across regions. Some require actual raw data, where we have to go back to the release results and copy all of the original analytical chromatograms and submit all of that. It creates very complex files that we have to manage for each individual country.
And then there is the matter of declarations, where there are statements from the company indicating stability, that the product is the same, that the quality of the product is the same, or regarding TSE [transmissible spongiform encephalopathy]. It just depends on the country what types of declarations we have to include in the package.
At the end of the day, in the major markets, the approval time lengths span over five years. When we begin to dispatch our wave one countries, there are gaps in the ability to file, as I mentioned, depending on the countries’ specific requirements.
You can see Brazil is one of our longest lead countries because it requires twelve months of drug substance and twelve months of drug product stability data, so we cannot file until we have all of that data available. There are also translations involved for different countries. So the whole process adds up to over five years….
And then by the time we dispatch in the Latin American, Asia-Pacific and Middle East countries, we are dispatching those regions and those submissions along with the major markets. But you can see again, the point is that we are really taking over five years to implement one single drug substance site change.
One of the key messages that we have from this example is that adding a manufacturing site submission takes over five years in some cases to get global approval. The regulatory environments are often dynamic and sometimes unpredictable and they may change in their expectations throughout this process. There may be different types of questions that we have to respond to, based on those different expectations from the health authorities.
On a positive note, most countries are accepting dual sourcing from drug substance sites. That is a good thing, where years ago dual sourcing was not allowed.
Harmonization Options
Given all these challenges that we have when we make a global change, are there ways that we can harmonize across the regions to make this process more efficient so we can facilitate world-wide drug availability?
For example, in the U.S. and the EU, we have the ability to have pre-approved comparability protocols, which allow us to shorten our review cycles and implementation of changes. Do we have an opportunity for those reference countries in the wave three markets to accept a CPP from a major market under mutual recognition? And can we leverage some of our organizations across WHO, ICH, ASEAN, and APEC to accept more a risk-based variation management plan? And is there potential to align those reporting categories across regions to align approval timelines and the notifications for prior approval in some cases?
And finally, where we have to implement a change immediately because there may be a safety risk or quality risk, is there a possibility we can have certain exceptions, where we submit the notification, we wait a certain period, and then we can implement because there is a high need due to risk to implement that change?
Approval Timelines in Major Markets
Switzerland
New Zealand

EXHIBITION: APRIL 7-8 POST-CONFERENCE WORKSHOP: APRIL 9-10
COURSES: APRIL 10-11
www.pdaannualmeeting.org
Biopharmaceutical and Sterile Manufacturing – Embracing Innovation to Meet Global Challenges
April 7-9, 2014 | JW MARRIOTT SAN ANTONIO HILL COUNTRY | SAN ANTONIO, TEXAS
PDA’s premier event, the 2014 PDA Annual Meeting will provide you with a one of a kind learning opportunity. This year the series of parallel sessions, a key and well liked feature of the annual meeting, will focus on issues and challenges related to Biological Sciences, Product Manufacturing, and Quality Systems as well as valuable peer-to peer networking events among many other benefits. Look no further than this must attend meeting, which has much to offer and will provide an excellent forum for learning and discussing recent innovations and interacting with industry and regulatory experts.
For the first time, this year’s agenda is filled with leading FDA experts:
Thomas Arista, Investigator,
CDER, FDA
Kalavati Suvarna, PhD, Microbiologist,
CDER, FDA
Karen Takahashi, Senior Policy
Advisor, CDER,
FDA
Alex Viehmann, Operations
Research Analyst,
CDER, FDA
Following the conference, there will be a post-conference workshop, PDA Biofilm and Bioburden Workshop on April 9-10. The workshop will provide the latest
science and best practices around microbial control for the pharmaceutical manufacturing environment. Presentations will be provided by technical experts from academia, industry, and FDA.
From April 10-11, the PDA Training and Research Institute will host six in-depth training courses. These courses for professionals involved in developing and manufacturing quality pharmaceutical products will cover a
range of topics from implementation of quality risk management to process validation and verification.
The PDA Training and Research Institute presents the...
What Are You Waiting For? Register Today!

Visit www.pdaannualmeeting.org/courses for more information and to register.
COURSE SERIESApril 10-11, 2014 | JW MARRIOTT SAN ANTONIO HILL COUNTRY | SAN ANTONIO, TEXAS
Biosimilars – Understanding the CMC Challenges of Meeting ‘Similarity’ – New Course (April 10)
Understand what the developing FDA biosimilar pathway might look like by examining the existing regulatory guidelines from the European Medicines Agency (EMA) and the World Health Organization (WHO).
Risk Based Product Development Basics for Combination Products: Harmonizing Design Controls and Quality-by-Design in Product Development and Market Authorization Development and Market Authorization Documents – New Course (April 10)
Gain a better understanding of combination product requirements and be prepared to streamline the transfer of knowledge from product development to regulatory submissions at their companies.
Implementation of Quality Risk Management for Commercial Pharmaceutical and Biotechnology Manufacturing Operations (April 10-11)
Learn to utilize the principles of quality risk management to strengthen the decision-making process and aid in allocating resources in a rational way.
Process Validation and Verification: A Lifecycle Approach (April 10-11)
Come away with an up to date understanding of the process validation strategies and approaches are consistent with current regulatory and quality system thinking.
Validation of Moist Heat Sterilization Processes: Cycle Design, Development, Qualification and Ongoing Control (April 11)
Learn more about sterilization science and apply it to the selection of a cycle design approach, process performance qualification and more.
Quality Control and Quality Assurance of Cell-Based Therapeutic Products (April 11)
Discover quality control testing for both in-process testing and for product release, including tests for purity, potency, reproducibility, and methods development considerations.
The PDA Training and Research Institute presents the...
Don’t miss these six courses hosted by PDA TRI immediately following the 2014 PDA Annual Meeting.

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 1�
INSIDE THE GLOBAL REGULATORY DIALOGUE™
The limitations, constraints and disconnects in the current CMC regulatory processes around the world are emerging into high relief as the biopharmaceutical community wrestles with how to get new medicines that fill critical healthcare gaps more rapidly to patients and how to facilitate manufacturing adjustments that better assure the quality of marketed products.
The opening plenary session of the CASSS/FDA Well-Characterized Biotechnology Products (WCBP) Symposium in late January in Washington, D.C. brought together a panel of regulators from various agencies to review the regulatory obstacles that need to be addressed to achieve these public health goals, including the lack of international harmonization.
On the panel were: ● CDER Director Janet Woodcock ● ANVISA Research and Clinical Trial Manager Laura Gomes Castanheira ● EMA Quality of Biological Medicines Head Veronika Jekerle ● CBER Director Karen Midthun ● Health Canada Senior Regulatory Scientist Anthony Ridgway, and ● Japan Pharmaceuticals and Medical Devices Agency (PMDA) Division of Biological Chemistry and Biologicals Head Teruhide Yamaguchi. Genentech CMC Regulatory Director Kathleen Francissen served as the moderator for the session and was instrumental in guiding the discussions.
The panel’s focus encompassed the emerging expedited clearance strategies, such as FDA’s “breakthrough therapy” pathway, and the challenges they pose to the traditional CMC development and regulatory paradigm.
Also in focus was global regulatory convergence, and the need for furthering the alliances and collaborations among regulatory agencies – particularly in addressing the growing complexity and globalization of biologics and the availability and integrity of their supply worldwide.
Woodcock, who played a central role in the dialogue at the session, repeated her clarion call for evolving the quality regulatory paradigm to better accommodate process improvements and patient needs, and to do so in a larger global context (see IPQ Monthly Update June, 2013, pp. 2-11).
“I think it is important to match the resources to the problem,” she stressed. “It is important that we understand the need of the public, the people who are dying of these diseases, for speedy action on the part of the agency.” If trading off some CMC regulatory control up-front is needed, “so be it,” she
said. “I think this is the right thing to do.”
Woodcock referenced a recent email from a colleague and former biologics regulator, who said that while he understood the need for clinical trials and the importance of study data in making drug approval decisions, he now found himself “on the other side” with a relative suffering from a rare disease for which a therapy is in early trial stages. “Now it is all about urgency and how little time is left,” he wrote. Woodcock stressed that “we have to recognize those realities in the world and our society and respond to them.”
Woodcock Outlines Global Harmonization Pathway
In addressing the international component of the quality regulatory problem, Woodcock provided her thinking on what a pathway forward would entail. [Her full comments on this score are provided below.]
She stressed the importance of pursuing an economical and clearly targeted approach to the challenges of global harmonization that takes into account the resource constraints of national regulatory agencies.
While ICH “has stood up very well” as a harmonization vehicle, it has had the limitations of being “an exclusive club,” she observed.
The CDER director envisions moving toward an “international standard development organization” (SDO) that would allow for the broader participation of all competent authorities and associations in the process.
One problem in establishing a global framework is that the essential component of a rule of law in various of the world’s countries has not been established, she pointed out. The next required component for a country to participate is a legal framework for governing pharmaceutical regulatory activities and a funded, stable staff to carry them out.
Once countries have stable systems in place, the next step is to seek harmonization with other agencies, which can eventually lead to “universal worldwide reliance” on common review and inspection decisions, Woodcock maintained. While ad hoc efforts have made some strides forward, a more concerted global effort will be needed to achieve the desired outcomes, she stressed.
Stronger Foundation Needed for Harmonization
Woodcock also framed her thoughts on the need for
International Panel of Regulators Spotlights Current Biotech CMC Regulatory Problems and Convergence Pathways

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COMFEBRUARY 2014 �0
MONTHLY UPDATE - FEBRUARY 2014
international harmonization of quality regulation in terms of the stress and inefficiencies that multiple, redundant regulatory inspections cause for both industry and regulators. Company resources should be focused on quality science and process improvement rather than on trying to satisfy the divergent compliance expectations of various regulators.
She noted that the reorganization CDER is undergoing (see IPQ Monthly Update January, 2014, pp. 13-20) is intended to create a stronger foundation to support internal and international quality regulatory harmonization. The proposed Office of Pharmaceutical Quality (OPQ), in particular, would focus on the scientific basis of decisions and the risks involved and how they are mitigated, in the effort to shift away from a subjective assessment-based approach. “You just cannot harmonize subjective viewpoints,” the CDER director emphasized.
Rather than trying to build harmonization around the subjective, disparate expectations in the current GMP compliance-oriented system, Woodcock suggests that “quantitative assessments of things that can be described in a more rigorous manner” would provide a stronger foundation – in line with the quality metrics efforts at FDA (ibid., IPQ Monthly Update June, 2014, pp. 2-20).
The harmonized metrics, she emphasized, should be owned by industry and shift the focus away from compliance to the quality of production. They could also help address the deep gap between the growing continuous improvement expectations on the GMP side and the existing status quo-oriented, change-unfriendly CMC review paradigm.
NIH National Institute of Allergy and Infectious Diseases Scientific Director Kathy Zoon supported Woodcock’s assertion regarding the stress and inefficiencies that multiple, redundant regulatory inspections cause, and emphasized the need for good communications between the review and inspection functions. The former CBER director received an award at the symposium for “outstanding achievements in CMC regulatory science.”
She pointed out that a regulatory organization must both develop quality standards and assure that they are transmitted to the field force that is going to be required to enforce them.
“I think there is a disconnect” between the reviewers and the field force who go into the facilities to do the inspections, she cautioned. “I know at CBER over the years we have had folks who review the applications also be on the inspection team, at least for the pre-licensing inspection,” which helps strengthen the communication process.
Zoon also commented that forums such as the WCBP have played an important role in fostering international harmonization on the CMC side, but need to incorporate consideration of the GMP aspect for deeper solutions to be found.
“I think the WCPB has been a useful venue that involves IFPMA and all the regulatory authorities from both developed and developing countries.” She commented that she thinks the forum could be used in a broader context to bring more consistency from development through inspections of products. “I think it could be quite helpful as another vehicle to move things forward.”
Cell Tissue Arena Drawing International Dialogue
The other regulators on the panel at the opening WCBP session provided insights on how their respective agencies were seeking to refine their internal quality regulatory processes and why international harmonization was a critical factor in achieving their objectives.
ANVISA’s Castanheira explained the focus that her agency will have this year regarding internal coordination of advanced gene and cell therapy regulation with that of other biologic products.
The biologics review staff, now numbering eight, will grow over the next year to about 30 after its assumption of the gene and cell therapy responsibilities.
She characterized the effort as both the agency’s “first priority” and “a challenge.” In addition to the administrative issues, the team will need to be trained, and regulations for the gene and cell therapy products, which Castanheira characterized as “not strong,” will need to be revised.
Driving international harmonization efforts at ANVISA are inspections of its biologics operations by the World Health and Pan American Health Organizations (WHO and PAHO) scheduled for 2014.
“Part of the preparation is to strengthen all the harmonization initiatives that we have in ANVISA, especially the initiatives that involve PAHO and WHO,” Castanheira commented.
One of ANVISA’s recent harmonization efforts with PAHO is focused on the regulation of biologics, which she hopes will eventually “lead us toward parallel reviews and more convergence.”
CBER’s Midthun provided insight into the challenges FDA is facing with tissue-based products, in particular, and the challenges resulting from the

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 �1
INSIDE THE GLOBAL REGULATORY DIALOGUE™
lack of a “uniform framework” internationally on how to handle these emerging products.
“We have been working closely with other partners – for example, in cellular therapies, the so-called advanced therapies – and I think there that there is more of a commonality of the approach,” she said. FDA and ICH as well as international regulators through the Asia Pacific Economic Cooperation (APEC) Regulatory Harmonization Steering Committee (RHSC), she noted, have been involved in this effort to develop a more convergent approach.
Tissue-based products, however, have “unique challenges.” The CBER director explained that some tissues are regulated “to decrease any possibility for communicable disease,” but they are not regulated in terms of being a drug, or a biologic, or a device. “Our framework is somewhat unique, and everyone else in this novel area is developing their own framework.”
EMA’s Jekerle commented that in the areas of cell therapy and biosimilars, her agency has been working toward regulatory convergence by actively seeking comments from the U.S. and Japan to try to bring their viewpoints into the related EMA guidelines.
Broader Harmonization Efforts Explored
The regulators on the panel highlighted other harmonization and regulatory convergence activities and noted the organizations and associations that are facilitating them.
In addressing his agencies activities, Health Canada’s Ridgway pointed to the International Coalition of Medicines Regulatory Agencies (ICMRA) – a harmonization body formed under the auspices of WHO in mid-2013.
ICMRA will have its first meeting this year in Brazil. He commented that the coalition will be forthcoming with announcements “in the near future” that “may have an impact on the global approach to governance of regulatory approaches.”
Health Canada is also involved with APEC in the context of its current focus on training, capacity building, and promoting regulatory convergence and best practices, and has provided subject matter expertise and leadership in some areas.
Ridgway further commented on his agency’s participation in the Pan American Network for Drug Regulatory Harmonization (PANDRH), which is “now starting to have a greater focus on strengthening regulatory authorities and developing regulatory networks in the PANDRH area
and developing regulatory competencies and better use of international guidances that already exist.” PANDRH has also been focused on the development of guidances and tools on various tropics, such as good clinical practice.
Regarding clinical trial materials, Castanheira noted that ANVISA’s conducts “parallel reviews” with Cuba, “but only for some very specific products that are part of government programs.”
She said that having parallel reviews “is the way we need to go. It is impossible to do everything in every area in ANVISA. I think first it needs to happen in our region, and then we can think about other regions. We have a lot of differences.”
The Brazilian regulator also pointed to ANVISA’s increasing participation in ICH. “At the first WCBP, we had had no interaction with ICH,” she recalled. “Now we are observers in some groups. I think that maybe in the future we can join.”
A question to the panel from an attendee turned its attention to another recent initiative – the Transatlantic Trade and Investment Partnership (TTIP) agreement that is being negotiated between the U.S. and the EU. The TTIP agreement encompasses: ● market access between the two areas ● regulatory issues ● non-tariff barriers, and ● rules addressing shared global trade challenges.
EMA’s Jekerle commented that her agency has “a lot of interest” in the agreement and is “fully supportive” of the initiative, and pointed out that it is being driven in Europe by the European Commission, not by EMA.
Areas potentially impacted by the agreement, she said, include joint GMP inspections, parallel scientific advice, and biosimilars – “topics which we are interested in, and are already working on.”
CDER’s Woodcock commented that “we cannot talk about those discussions per se, since they are ongoing negotiations.”
Differing Review Timelines Complicate Global Submission Process
The TTIP should not be confused with a similarly-named initiative – the Transatlantic Administrative Simplification (TAS) initiative – which has involved US and EU regulators and industry (see IPQ Report Nov./Dec. 2008) and paved the way for joint inspection (IPQ Monthly Update August 2010, pp.33-34) and review pilots (IPQ Monthly Update February, 2011, pp. 42-43).

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
Noting her firm’s involvement in the joint QbD pilot, session moderator and Genentech CMC director Kathleen Francissen commented on how differing timelines among the various regulatory agencies impact parallel reviews and the global submission process.
“Sponsors are moving toward simultaneous global submissions,” she pointed out. “Let’s say you submit in the U.S., and you are under really rapid review. As you go through that review process and get the agency’s feedback, you are then updating the sections of that market application. So as you are doing that, what you initially submitted and what was finally approved are really two different things.”
Francissen explained that, since what was originally submitted in the U.S. was also submitted worldwide, by the time of U.S. approval, there is a disconnect between the approved process and what has been filed globally.
She also noted that another reason for the disparity between what is filed in various countries reflects differing or additional local requirements.
Trade Secrets are Problematic
Drawing discussion as one of the challenges that the international community faces on the way to harmonization was the issue of restrictions that countries have in sharing trade secret information unless permission is granted by the applicant. This lack of complete information among regulators can cause differing interpretations with no pathway to reconcile them.
Health Canada’s Ridgway emphasized that sponsors do have the ability to give permission to regulatory authorities to discuss trade secret information, and that it is a “great benefit for the sponsor to give us that permission.”
He explained that the interactions between agencies regar-ding information in an application “can be very helpful in cutting out delays and smoothing out any misunderstan-dings” between approaches and understanding why data judged acceptable by one agency may be looked at differently by another.
CBER’s Midthun agreed, noting that “one of the challenges is that the agreements we have allow us to share and discuss confidential commercial information but not trade secret information, and much of the nitty-gritty in the CMC is exactly that.”
With permission from the sponsor, she said, a “parallel scientific advice agreement” might be reached such that the manufacturer would submit the data to two agencies and allow them to discuss and compare their thinking and approaches, benefiting both the sponsor and the agencies.
EMA official Jekerle noted that her agency has a parallel scientific advice agreement with FDA, where the agencies “try to seek harmonization or explore those areas where we may have different views in the very early stage in development.” She commented that if the agencies know where else in the world a sponsor has submitted an application, certain information can be shared through confidentiality agreements with other agencies – for example, between EMA, FDA, Health Canada and PMDA.
CDER director Woodcock pointed out that agencies’ inability to share certain information up front without the permission of the applicant can result in different interpretations of the information by different agencies.
When this happens, she suggested that the companies involved should “take the bull by the horns” by pulling together the differing assessments and sharing them with regulators to get a clearer explanation of why the differences exist.
“If we do not share this information, if people are not confronted by their differences and they are unaware of them, we are never going to get improvements,” the CDER director emphasized.
“It would take some courage,” she said, “but I think it would be a tremendous improvement if companies actually said, ‘look, what are we supposed to do, have two separate lines?’ How important can it be if one country says it is satisfactory if you do it one way, but in another it is only satisfactory if you do it another way? These differences should be ironed out.”
The CDER official explained that internal harmonization of application assessments at FDA will be addressed in OPQ by a continuous improvement office and a policy office that will look at the advice given and compare it across applications to try and get more uniformity. “But I cannot look at what the other regulators told you, because that is a secret between you and them.”
Noting the sensitivity of trade secret information, Woodcock suggested that industry could form a consortium to take on the challenge of how to share the information, to “kind of take the individual sting out of it.”
[The story continues on p. 23 with Woodcock’s remarks on developing a global quality regu-latory pathway.]

NSF-DBA, NSF-Pharmalytica and Becker & Associates are changing their names to NSF Health Scienceson January 1, 2014.
NSF Health Sciences [email protected] www.nsf.org
Testing Auditing Consulting Training
••
•••
C
M
Y
CM
MY
CY
CMY
K
HS - Contract Pharma Ad_1_14_PRINT.pdf 1 1/7/2014 10:18:15 AM

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
CDER’s JANET WOODCOCK ON DEVELOPING A GLOBAL QUALITY REGULATORY PATHWAY
The following are the comments made by CDER Director Janet Woodcock at the WCBP symposium on de-veloping a global pathway for quality regulatory harmonization.
When you think back, we have come a long way from the start of ICH where we all just sat down and got to know each other, all the regulators.
We really have come a long way. The [QbD joint review] pilot was part of a series, and we are very interested in continuing to get to know one another at a deeper level. I think that is important. However, I believe all the efforts that we engage in like this are very time-consuming, and there are times that we do not have a lot of extra resources. At some point we are going to have to decide collectively what we are going to do and then do it.
I think these pilots are very helpful in informing where we should go, but at some point we are going to have to make a path and an objective on convergence. It is true that CDER is rather large. I have trouble achieving uniformity in standards amongst the CDER staff, and [CBER Director Karen Midthun] and I have efforts to ensure uniformity between drugs and biologics for similar products.
When we think about the world-wide regulators, and you also think about the language differences and the cultural differences, this is a very daunting set of challenges we have on the review side and on the inspection side….
We are going to have to do this in a way that is parsimonious of our resources. Otherwise, we will spend all our time on harmonization efforts, particularly if they are not coordinated and they do not have a single path that we have all agreed to. If there are a whole lot of one-off efforts, we could spend all our time doing that and not reviewing anybody’s application, and nobody wants that. Plus we have commitments that we have made to Congress that we have to do this.
I think everything that has happened so far has been tremendous, because first we have gotten to know each other, we have mechanisms to share, and so on. I can tell you CDER does not have an effort like this staffed in a way that I would need to do to really make it happen. It is going to take a fair number of dedicated full-time staff in my organization, so they really know what we are talking about here. If we commit to do this, we would have to dedicate resources to get it done over, say, a ten-year period – whatever it takes, whatever we decide this is. The pilots are great. But we should not think that doing a bunch of pilots is going to get us there….
I think we need an international SDO that everybody can agree upon that develops the standards. That is number one. These are my opinions, not necessarily FDA opinions.
I think ICH has stood up very well, but it has been an exclusive club. Theresa Mullin, who is our lead now, is trying – and I have been talking to her about the need – to move away from that model, which worked very well for twenty years, and move towards an international standard development organization that is really open to all competent authorities and other associations to join so that all the regions and regulators can participate in the development of standards through one body where the relevant expertise is at the table. Other people may have different ideas about how to do that. This is basically like the electrical engineers…they have their SDO. They agree upon international standards for things and they publish them and they get things done. That is one piece.
Another piece that we have just been talking about is we have regulatory capacity around the world at a variety of different levels of both being resourced and having experience. I think what we have just heard about Latin America, for those countries that do not have a lot of resources, banding together into a regional network makes a tremendous amount of sense, and sharing the load. Because those folks who are geographically adjacent to one another, relatively speaking, it makes it easier. Like you said, they have a common language. Then maybe we would not be dealing with how many countries there are in the world. We would be dealing with blocs of regulators from different regions, and they could also share the work in standards development.
There is another piece of that, which is regulatory capacity development. That has to do fundamentally in my mind

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COMFEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
– sorry if I am going on about this – basically you have to have rule of law first. In some places that is a problem. Ifyou do not have an established law, a legal system, a rule of law in a country – that comes first, before setting up what your CMC standards are, for example.
Then you have to have some kind of legal framework for your regulatory activities in pharmaceuticals. Some countries do have a rule of law, but they do not have that. Once you get that, you have to develop a tradition and experience and a body of people who are funded who then can execute whatever laws you have in that country. I think our rigorous analysis of this shows that we cannot do it just as, ‘oh, it would be nice if we could educate all these people,’ because there are really a lot of people out there. The more tumultuous, the less connection they have to rule of law, the more turnover they have. You may talk to some people and do some training and the next year it is all different people – it is a whole different regime.
That effort, which is being taken on by multiple different parties in a very uncoordinated manner, is another set of activities that needs to be done. To some extent, some of that kind of training can be done by ICH or by voluntary professional organizations and so forth. I can tell you that we are not funded to reach out to the entire world and provide that type of support.
Then you have standards, you have regulators, maybe you have various bodies of people, then how do you get to universal worldwide reliance or go toward that? There I think we need a plan.
What we are doing now is all these ad hoc efforts. There is nothing wrong with that. They have brought us to a lot of recognition and understanding. But I will tell you they are not going to get us there. We need some kind of plan about how you would actually achieve this type of thing.
It is bad in many ways right now. Not only is it bad that the regulators are short of resources, so we do not get where we need to go and we do not look at everything we want to look at. However, you may have five or eight different inspectorates in a plant in a given year. That is terrible. That is a recipe for errors and mistakes. That is not good.
Often, from what I hear, they all have different opinions about what you should correct and how fast you should correct it. That is just catastrophic as far as quality management goes, which is what we all should be aiming for – quality of the products that are put out on the world market.
I think we need a plan that takes that problem into account. It is not just that the regulators need help. It is that we should not be sending all these people into these plants all the time. We should be able to have a definitive evaluation every year by someone, then everybody should be able to look at that.
But to get there is going to require staffing on the part of the regulators. We are going to have to staff this effort, and we are going to have to agree on what the effort is, what the path is, perhaps over ten years or something, to get to where we need to go. That is what I think.


The use of statistics in PV continues to be one of the most debated aspects of the 2011 FDA PV Guidance. Work alongside FDA representatives and experienced statisticians to interpret and clarify expectations for the use of statistics to plan each stage of the Process Validation lifecycle.
REGISTER TODAY:www.ISPE.org/2014StatisticianForum
A unique opportunity for statisticians to share, discuss, and collaborate in finding optimal approaches to implement
statistical elements within the FDA PV Guidance
Forum Benefits:
• Examinethemeritsandlimitationsoftraditionalandalternatestatisticalap-proachestosupportthelifecycleapproachtoPVwithfellowparticipants.
• Evaluatevariousapproachesandcasestudiesandselectordevelopcom-pliantapproacheswhichbestmeetthespecificdosageformtypeandpro-cess.
• Gaugeyourcompany’sprogressandapproachesascomparedwithothers,includingindustryleaders.
• Identifyvalueaddedconceptsforcontinuedcollaboration.
One of a Kind Event!

MONTHLY UPDATE - FEBRUARY 2014MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
The International Federation of Pharmaceutical Manufacturers and Associations (IFPMA) is throwing a spotlight on the impact that the current tangled global regulatory web is having on the ability to supply vaccines to the people who need them.
Significant obstacles for vaccine manufacturers in meeting the global need, IFPMA is stressing, include: ● the complexities, disharmonies and extended timelines for clearance of marketing applications and post-approval changes around the world ● the need for transferring high-tech processes to meet localized production requirements, and ● the time required for redundant regulatory lot clearance.
The effort by the global non-profit, non-governmental organization (NGO) to create broader awareness around these problems in the vaccine arena reflects IFPMA’s mission to “advocate for policies that encourage discovery of and access to life-saving and life-helping medicines to improve the health of people everywhere.”
IFPMA has published a brochure explaining the significant role vaccines play in global health and the obstacles that the current disparate regulatory processes place in the way of their availability, and the organization is adding its voice at public forums to the call for an international effort to find a harmonized pathway forward.
Speaking for IFPMA at the final plenary session of the CASSS/FDA WCBP Symposium in late January in Washington, D.C., Merck Biologics VP and Biologics/Vaccines Regulatory CMC Executive Director David Robinson stressed that, “new, increasingly complex vaccines, high quality standards, and the volatile regulatory environment are combining to create what is an essentially non-sustainable situation. In order to sustain access to vaccines, the regulatory environment does need to adapt.”
The final plenary WCBP session was focused on the challen-ges of managing the global quality regulatory complexities that biotech products face.
Along with Robinson’s, compelling presentations on the post-approval change dimension of the problem were made by Bristol-Myers Squibb (BMS) Global Regulatory Sciences CMC Executive Director Annie Sturgess and Roche Head of Marketed Biologics for the EU Ralf Gleixner. Both shed a hard light on the quagmire that global manufacturers, and biotech producers in particular, face in trying to make
process improvements (see story on pp. 31-44).
The post-approval change concerns also drew front-burner attention at the CMC strategy forum Japan held in Tokyo in December, which focused on problems in Japan’s post-approval change system, including a lack of flexibility around biopharmaceutial manufacturing changes that results in most requiring prior approval as well as meetings with the agency to resolve unclear expectations (see story on pp. 2-19). Presentations were given there by a Japanese reviewing official as well as by a JPMA representative and an Amgen executive that compared Japan’s system to the rest of the world.
The Implementation Quandary and Inventory Hell
At the WCBP symposium, Robinson discussed: ● the “tremendous” impact that vaccination programs have had on the public health worldwide ● the complexities of manufacturing vaccines and their regulatory approval ● case studies illustrating the difficulties and time-consuming nature of global post-approval change clearance and the “inventory hell” it creates ● the disparity between lot release testing performed for vaccines vs. other products, and ● possible solutions (Robinson’s full remarks are provided below).
Many vaccines contain multiple components – in some cases as many as 23 – in order to provide more complete and robust protection, he pointed out. Each component is prepared as an individual active substance and combined to produce the final product. Each requires its own unit operations with multiple steps, and changes to any step to increase manufacturing efficiency or product quality requires regulatory approval.
Robinson provided case studies that highlight the regulatory hurdles manufacturers face in: ● increasing capacity to enhance global access to vaccines ● adding a vaccine product facility to increase productivity ● changing a lyophilization cycle to increase productivity, and ● filing all three changes at the same time.
In the case of making all three changes for a product that is marketed in 130 different countries, Robinson noted that the approval can be done in one year in 80% of the countries.
Additional data requirements in the remaining countries can stretch the approval time globally to six years. This extended
Global Quality Regulatory Maze Jeopardizes Vaccine Supply, IFPMA is Stressing

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
timeline reflects practices by some countries to only review one change at a time, requiring the three changes to be submitted sequentially.
This extended approval timeline presents the manufacturer with the quandary of when to start implementing a change.
In the three-change scenario, one option is to wait six years “until you get approval for all three changes,” Robinson said.
Implementing the changes as they are approved in different countries rather than waiting is another option. However, doing so will result in the firm “managing dozens upon dozens of different products in inventory and essentially living in something like inventory hell.” Also at issue is the compliance tightrope that is created by having to track multiple versions of a product and ensure they are only released to the countries in which they are approved.
Testing Delays Jeopardize Vaccine Supplies
Requirements for repeat testing of vaccine lots by government agencies can further jeopardize supply reliability.
Each lot of a vaccine is first tested by the manufacturer prior to release, then again by the domestic national control lab,
and possibly a third time in the importing country. Unique compendial requirements can further complicate the release process.
“All that takes time,” the Merck exec pointed out. “And a vaccine, like any biologic, has a limited shelf-life.” After the redundant testing, “there may be very little time left to distribute the vaccine to the patients that actually need it.”
The additional testing beyond that that is conducted by the manufacturer, he maintained, “adds little contribution to the assurance of the safety of the product.”
Robinson concluded his remarks with suggestions from IFPMA on how the regulatory maze could be made less onerous and more navigable.
Harmonization of regulatory requirements, partnerships on review of applications, alignment of compendial methods with input from industry, and the reduction of redundant testing and inspection, he maintained, would go a long way toward helping ensure the supply of and access to vaccines globally.
DOWNLOAD FROM THE STORY: • IFMPA’s “The Complex Journey of a Vaccine”
[The story continues on p. 27. with Robinson’s full presentation]
WASTED ENOUGH TIME SEARCHING THE
INTERNET?
Come to IPQpubs.com to find all the important CMC/review and GMP/inspection developments in the US, Europe and internationally.
All the stories that appear in IPQ’s real-time “In the News” web coverage and in our“Monthly Update” are indexed and searchable on our website
--with the relevant document links you need ready at hand.
We do the work so you don’t have to.Visit IPQpubs.com and relax.

PAREXEL Internationalwww.PAREXEL.com
A proactive approach to achieving and sustaining
compliance is ideal. But, if the unforeseen occurs,
you need to make well-informed decisions to
overcome a product crisis.
PAREXEL has a rapid response staff consisting of
more than 25 former regulators in the U.S. and Europe.
Among this group are ex-FDA investigators and compli-
ance experts who have an average 25 years of FDA
experience, plus many years of worldwide compliance
consulting experience.
When knowledgeable, experienced advice is needed
to minimize regulatory enforcement risk and achieve
your objectives, we can help.
To learn more, please visit:
www.parexel.com/strategic-compliance
Sustainable compliance demands a proactive approach
PAREXEL CONSULTING

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
MERCK’S DAVID ROBINSON ON GLOBAL VACCINE REGULATORY ISSUES
Speaking for IFPMA at the CASSS/FDA WCBP Symposium in late January, Merck Biologics VP and Biolog-ics/Vaccines Regulatory CMC Executive Director David Robinson discussed: ● the “tremendous” impact that vaccination programs have had on the public health worldwide ● the complexities of manufacturing vaccines and their regulatory approval ● case studies illustrating the difficulties and time-consuming nature of global post-approval change clearance and the “inventory hell” it creates ● the disparity between lot re-lease testing performed for vaccines vs. other products, and ● possible solutions.
I am very delighted to be speaking here today on behalf of IFPMA [the International Federation of Pharmaceutical Manufacturers and Associations]. I will start with an introduction of the impact of vaccines on human health. I will discuss the complexity of vaccines, including the manufacturing pathways and regulatory approvals.
Vaccine Impact on Human Health
Vaccines have tremendous positive impacts on human health, and access to vaccines remains very important because of that health impact. I will give you a few illustrations. Here is a series of graphs that are all laid out exactly the same showing cases or incidence rates for a particular disease over the course of time. You can see in the case of measles, looking at the U.S., that in the 50s and 60s there were probably 500,000 cases of measles per year. Upon introduction of the first vaccine in 1964, there is a dramatic drop in the incidence rate of measles.
One can see the same thing for mumps. Upon introduction of the mumps vaccine in the U.S., you can see a dramatic drop in disease rates. Similarly for rubella, the same thing – the disease drops dramatically. And for my last example, Haemophilus influenza B, you can see the same kind of thing: Introduction of the vaccine leads to a dramatic drop in incidence rate.
The Dramatic Impact of Vaccines on Human HealthHiB-United States, 1981-1995
Mumps-United States, 1968-1996
Rubella-United States, 1966-1996
http://www.hhs.gov/nvpo/concepts/intro6.htm

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
This is not limited to just the United States. I can give you a series of slides, but here I will just go over the first one. Here is how vaccine efforts helped reduce the instance rates in various parts of the world: Focusing on Africa, this looks at diphtheria, pertussis, neo-natal tetanus, total tetanus, measles, and polio [showing disease reduction of 100%, 96%, 33%, 73%, 93%, and 83%, respectively]. This was gathered from 1980 to 2009 in Africa with very similar results in the Americas. There were also very similar results in Southeast Asia. I could keep going on to other regions of the world, but I imagine you get the point.
Despite this, access to vaccines and robust vaccination progress remain very important. We still see outbreaks of vaccine-preventable diseases throughout the world – for example, polio. We can celebrate the fact that India has gone three years without a single case of polio. However, there were 500 cases of polio reported in Kazakhstan in 2010. Just this month, in one week of this month, there were 60 cases reported in Pakistan.
For mumps, in an 18-month period, there were 16,000 cases reported in Macedonia. This happens throughout the world. We can see the same thing for measles: In about an18-month period there were 200 cases in Barcelona. In the United States just last year, in an eight-month period, there were nearly 160 cases, despite the fact that measles was actually declared officially eradicated in the United States in 2000. Access to vaccines remains very important to protect human health.
Vaccine Product and Manufacturing Complexity
Vaccines are actually quite complex. Manufacturing them with consistent quality is also complex. One of the things that is unique about vaccines is that many of them are multi-component. I will give a few examples.
In terms of complexity, one can look at something like simvastatin, which some of my colleagues think was a fairly complex molecule to synthesize, with multiple chiral centers. Of course, that pales in comparison to a monoclonal antibody with a molecular weight of 150,000 Daltons. But, as all my vaccine colleagues like to point out, the human papilloma virus [HPV] vaccine has a molecular weight of 20,000,000 Daltons.
Many vaccines contain multiple components in order to provide more complete and robust protection. There are two licensed vaccines for HPV, which causes cervical cancer in women. Here is an example of the quadrivalent vaccine, but these same two strains are in the bivalent vaccine. They provide protection against the strains of the virus that cause 70% of cervical cancer worldwide. An investigational product out now contains nine different HPV vaccines and provides protection now for up to 90% of the strains that cause cervical cancer worldwide. So you can see that adding an additional five strains can give significantly increased coverage. Each of those nine HPV types is prepared as a separate drug substance and combined into one vaccine.
There is also vaccine available for immunization and prevention of pneumococcal disease. That vaccine actually contains 23 different polysaccharides in order to provide robust coverage. And each of those 23 polysaccharides is manufactured as a separate drug substance.
When producing a biological product like a vaccine, everyone knows that there are multiple steps required to do that, and each of those steps has multiple unit operations. Each of those unit operations needs to be individually optimized, demonstrated, and executed. When we are looking at a multi-complement vaccine, you are talking now about doing this either four times, nine times, or 23 times. You introduce changes, of course, when you are trying to improve the vaccine, in any one of those steps.
Regulatory approval of vaccines can be very complex. Vaccines are licensed generally in multiple countries – for example, anywhere from ten to 130 countries. So multiple filings will be required. Previous speakers have already touched on the various ways in which we might want to improve a vaccine to increase access. We could optimize the manufacturing process or increase the capacity. We may have analytical changes, we may have unplanned changes outside the sponsor’s control.
In many cases, for vaccines, there is strong market preference for local manufacturing. So you have to transfer the process and manufacture the product in the country. That also requires certain filings and submissions, and there may be new regulatory requirements.

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
Case Studies
I will provide three case studies about attempts by a manufacturer to increase capacity and enhance global access to vaccines. This could be by adding a vaccine product facility to increase productivity, changing the lyophilization cycle to increase productivity, or multiple improvements in order to increase capacity.
In this case I will look at products available that are marketed in about 130 different countries…. Each line, each row is a different country, and we are looking at the filing requirements of that country for this change. So we can see that for many countries we have to file the same document, but each country is somewhat individualized. This means that we are preparing 130 different files for submission, which does take time and effort to do. In addition, we find that the data requirements and the length of time for approval will vary in the countries.
Looking at a product that is available in 20 countries, in this case there was a change in the lyophilization cycle to increase productivity. For some countries, pre-approval is not required, and one can essentially implement as soon as the data is ready, with no requirements for stability data and no review. For other countries, there is no stability data required for submission, but the review period can take anywhere from a few months to ten months. For other countries, we cannot file until we have three months of stability data, and again the review period varies. Others require six months of stability data.
As the previous speaker pointed out, some countries require the CPP [certificate of pharmaceutical product] either during the review or before filing. This means that kind of change can take up to 24 months for one change.
In the third case study, I will talk about trying to do all three of these things: ● adding a drug product facility to increase productivity ● changing the lyophilization cycle to increase productivity, and ● changing the facility design to comply with new regulations.
In this case we are looking at a product that is marketed in a 130 different countries. For the first 80% of those countries you can get the approval done relatively quickly – in about a year. But the last 20% of the countries could take an extra two years.
So you stagger your submissions because you need additional data to support the next change. You see now this starts to cause about a three-year period for approval. But at the time of the third change, that approval cycle could be stretching out to six years. That is because in some cases there are countries that only review one change at a time. So this could add that extra three-year period, because you have to wait for that country to get the change approved before you can submit your next change, wait again, and then submit the third change.
The question you are faced with as a manufacturer is, when do you actually start to implement the change in the facility? Do you wait until you get approval for all three changes, in six years? You can consider in this case that you could implement and start marketing in the first 80% of the countries. Now you are managing two different products. If you repeat this again for the second change, you are now managing three different versions in inventory. By the third change you are managing four different versions in inventory.
For some of the older products that have been on the market for ten, 20, or 30 years, if you start to add in the fact that there are also local countries that have requirements for unique images or strengths in that country, we can be managing dozens upon dozens of different products in our inventory and essentially be living in something like inventory hell. And certainly this represents a compliance issue – just trying to track and make sure you are releasing the right product to all markets, and you have the right product available for all markets to avoid drug shortages.
Vaccine Testing
Next is testing of vaccines. Vaccines undergo multiple tests. Some countries require lot-specific testing prior to release, and in some case unique compendial requirements. Vaccines, like any biologic, will undergo a number of different test methods and you have to transfer each of those test methods to the different labs around the world.

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COMFEBRUARY 2014 �0
MONTHLY UPDATE - FEBRUARY 2014
Each lot of vaccines is, of course, first tested by the manufacturer prior to release. The same tests need to be repeated by the official national control lab prior to your ability to export it. These same tests may again be repeated by the importing countries. And so vaccines may well be undergoing repeated testing three times using the exact same tests. All that takes time. And a vaccine, like any biologic, has a limited shelf-life. So by the time you actually get it into that country and available on the market place, there may be very little time left to distribute that vaccine to the patients that actually need it….
Next I will touch on compendial changes. There are WHO reports looking at 148 countries that show something greater than 30 different pharmacopeias, if you include national, regional, and international requirements. There is certainly a lack of consistent communication on those, and a lack of industry representation during the process of revising many of those compendia. The impact across a range of drug products may not be well understood without input from industry. This could potentially impact compliance and disrupt the drug supply chain.
I propose that for a small molecule perhaps much of this would be acceptable, as you have a much simpler molecule to characterize and analyze, and perhaps simpler test methods. But as you move to increasingly complex products like biologics – and perhaps one could argue that live virus vaccines are among the most complex – adding a compendial requirement that may be a minor change for a small molecule has a greater impact to a live virus vaccine due to its increased complexity.
On the other hand, I am not trying to argue against having the review process. I believe quite strongly that high rigor in regulatory standards and high rigor in reviews helps to ensure the quality of vaccines around the world. But I think, and many of the health authority representatives would agree, that the complexity of those files is increasing – the sheer size of the file and the complexity of the information that is in them. At the same time, health authorities around the world are facing resource constraints that limit their ability to quickly review these increasingly complex submissions and to quickly conduct multiple testing.
Proposals and Conclusions
The proposal is that these redundant reviews may not greatly increase the assurance of product quality, and additional testing beyond that that is conducted by the manufacturer, and is internationally recognized by the health authorities, adds little contribution to the assurance of the safety of the product.
So to help reduce this complexity and enhance access to vaccines, we recommend efforts to be made to: ● harmonize the compendial requirements ● provide systems to update the compendia that includes input from industry ● harmonize the data and information requirements to streamline the submission preparation, and ● engage in a level of mutual recognition of internationally recognized health authorities output for most of these redundant reviews, redundant testing, and redundant facility inspections.
Vaccines are an important component in improving the public health around the globe. New, increasingly complex vaccines, high quality standards, and the volatile regulatory environment are combining to create what is an essentially non-sustainable situation. In order to sustain access to vaccines, the regulatory environment does need to adapt. The proposal is that harmonization of regulatory requirements, partnerships on review of applications, alignment of compendial methods, and reduction of redundant testing and inspection would help facilitate access.
Vaccines help save lives. This is a quote from Stanley Plotkin, an emeritus professor at the University of Pennsylvania: “With the exception of safe water, no other modality, not even antibiotics, has had such a major effect on mortality reduction and population growth” as vaccines. It is important that we can maintain and increase access to vaccines.
I will close with an introduction of IFPMA, which is a global non-profit, non-governmental organization which has a mission to advocate for policies that encourage discovery and access to life-saving and life-helping medicines to improve the health of people everywhere.
We have prepared a very simple brochure that can be used for education on the complexity of what we are doing, called “The Complex Journey of a Vaccine”, and you are welcome to come up and get that brochure or to visit the IFPMA website.

www.usp.orgGAMS292F_ 2014-1
Future USP Global Education and Training Courses, Meetings, Workshops and More!
Global Education and Training Courses
Featured Classroom Courses
§ Brazil: Excipient Performance; Developing and Validating Dissolution Methods
§ China: Essentials of Compendial Microbiology Testing; Analysis of Elemental
Impurities; Pharmaceutical Waters; Dissolution: Theory and Best Practices
§ Europe: In-Vivo In-Vitro Correlation (IVIVC); HPTLC for Identification
of Articles of Botanical Origin
§ India: Pharmaceutical Stability; Effectively Using USP–NF; Practical
Applications of Chapter <467> Residual Solvents
§ United States: Effectively Using FCC; Good Manufacturing Practices;
Analysis of Elemental Impurities; Dissolution: Theory and Best Practices
Webinars Increase your knowledge of compendial activities!
The USP Global Education and Training Department has launched a series of webinars to increase distance learning opportunities for the pharmaceutical industry. These sessions are conducted by USP Scientific Liaisons or Expert Committee Members who are directly involved in the standards-setting process.
For Classroom Course Information and Schedules Contact [email protected], or visit www.usp.org/meetings-courses/courses and click on the appropriate language if other than English. All Europe offerings are available in English. For India offerings, contact George Mathew at [email protected].
FOR MORE MEETING AND WORKSHOP INFORMATIONVisit www.usp.org/meetings, contact [email protected] or call +1-301-816-8130.
NOTE: Events held at USP Headquarters, Rockville, MD (U.S.) unless otherwise indicated. Courses, symposia, workshops and dates subject to change.
USP Workshop Series
March 24–25, 2014
§ Dissolution Testing of Capsules
June 2–3, 2014§§ 6th Bioassay Workshop
August 2014 (Date–TBA) § DNA Barcoding of Botanical Articles
September 8–9, 2014 § Alternative Microbiological Methods
October 1, 2014 § Synthetic Therapeutic Peptide—Regulations,
Standards and Quality
November 5–6, 2014 § Contaminants in Foods–Compendial
Approaches to Protect Public Health

The Advantage ofUnrivaled Quality...by Design
Components
Ensuring a drug product maintains its safety and ef� cacy from concept to commercialization while reducing total cost of ownership requires high-quality packaging components.
West designed NovaPure components within a Quality by Design framework. Our data-driven process provides a deeper understanding of our product development and manufacturing processes. We apply this knowledgeto components that can help customers build quality, safety and ef� cacy into their drugs.
Our holistic approach encompasses a thorough process review, from raw materials to commercial manufacturing to transportation of components to the customer’s facility.
NovaPure serum stoppers, lyophilization stoppers and syringe plungers are globally available with a reduced lead time, and are providedin optimized packaging that helps ease the transition through manufacturing environments.
West NovaPure®
#6731
The New Definition of High-Quality Components
West and the diamond logo and NovaPure® are registered trademarks of West Pharmaceutical Services, Inc., in the United States and other jurisdictions.
© Copyright 2012 West Pharmaceutical Services, Inc.
Unrivaled Quality…by Design
To learn more about West’s NovaPure technology, call your West account manager or a Technical Customer Support representative.
Contact West today.
North America +1 800-345-9800Europe +49 2403 7960Asia Paci� c +65 6860 5879
www.westpharma.com
6731 NovaPure Advert.indd 1 3/29/2012 8:46:01 AM

MONTHLY UPDATE - FEBRUARY 2014MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 �1
INSIDE THE GLOBAL REGULATORY DIALOGUE™
Biopharmaceutical firms are calling for a global effort to decrease their heavy post-approval change filing burdens that would clarify and harmonize change classification and submission requirements on a risk-based foundation.
High on the priority list are a common definition of what information in marketing applications is a regulatory commitment and a broader adoption of “do and tell” mechanisms for notification of minor, low-risk changes.
The regulatory quagmire global companies face in trying to make post-approval adjustments to their manufacturing and control processes received front-burner attention at the CASSS/FDA WCBP Symposium in late January in Washington, D.C.
A plenary session was held at the conclusion of the conference to focus specifically on the post-approval change problem and pathways to address it. Highlighted were the amount of valuable resources that the problem consumes, the extended and varying clearance timelines, and the product distribution complexities that ensue.
The result, the participants noted, is that manufacturing and control improvements are not being made that should be and the supply of products to patients is being jeopardized.
Bristol-Myers Squibb (BMS) Global Regulatory Sciences CMC Executive Director Annie Sturgess set the stage by providing background and context regarding why post-approval changes need to be made for biopharmaceuticals, and how the regulatory complexities play out in long approval timelines and inventory issues.
Following Sturgess to the podium, Roche’s Head of Marketed Biologics in the EU Ralf Gleixner delved further into the consequences of the divergent expectations among regulators for CMC submissions and post-approval changes. He provided a handful of case studies revealing the hurdles and extended approval timelines that firms encounter in pursuing even minor changes.
The session also included a presentation by Merck Biologics VP and Biologics/Vaccines Regulatory CMC Executive Director David Robinson. Speaking for the International Federation of Pharmaceutical Manufacturers and Associations (IFPMA), Robinson offered insights on the impact that the global quality regulatory maze is having in the vaccine arena, in particular – including complicating vaccine approval, discouraging innovation, and jeopardizing patient supplies (see story on pp. 25-30).
The discussions that followed the three presentations revolved around how the current CMC paradigm discourages transparency and putting information in applications that is not strictly necessary for approval, since the additional information can decrease the room for making needed post-approval adjustments.
However, participants noted that the applications are getting more detailed, particularly on the biotech side, reflecting the increasing complexity of the products and processes, further exacerbating the problem. In turn, the learning curve is getting steeper, and technology moving faster, enhancing the need for regulatory flexibility around changes.
At issue was how the paradigm could be adjusted on the international level such that more transparent, information-rich applications were rewarded with lessened post-approval burdens.
The closing session extended discussions that had begun in the opening session of the WCBP symposium three days earlier (see story on pp. 19-24).
The opening session brought together a panel of regulators from the U.S., Europe, Brazil, Canada, and Japan to review the regulatory CMC obstacles that need to be addressed to facilitate getting new medicines that fill critical healthcare gaps more rapidly to patients and the pathways being explored among the various regulatory agencies, such as FDA’s breakthrough therapy initiative. The discussion encompassed the problems in the post-approval change arena which come into play in making the needed regulatory adjustments.
Post-approval change concerns also drew front-burner attention at CASSS’ CMC Strategy Forum Japan, held in Tokyo in December (see story on pp. 3-18). Presentations were given there by a Japanese review official, who explained Japan’s system, as well as by a Japan Pharmaceutical Manufacturers Association (JPMA) representative and an Amgen expert that focused on the post-approval change constrictions in Japan and how they compare and interface with those confronting firms across the global regulatory landscape.
Differing Change Expectations Pose Challenges
After providing some background and context, Sturgess discussed: ● the challenges in interpreting regulations and timelines ● the concept of a “living license” or “living
Industry Proposals for Addressing Post-Approval Change Burdens Include Harmonizing on Commitments and Classifications

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
dossier” ● the implications of implementing global changes ● the inventory problems that the current system fosters, and ● mitigation strategies (Sturgess’ complete remarks are provided on pp. 36-39).
She concluded that managing post-approval changes is complex and time-consuming, with long approval times that cause inventory issues, delay implementation of changes, and hinder innovation and continuous improvement.
The BMS exec emphasized that “post-approval changes are essential. We want to stay current. We want to innovate. We want to improve. We learn new things. We are learning them every day. We don’t want to hold back change.”
Her recommendations on how to improve the current system include better guidelines that are harmonized globally. “I think we all recognize that each country has its own legislation,” Sturgess said. However, harmonized guidelines could “help to bring clarity and consistency in interpretation for better risk-based decisions.”
She explained that a change that may be the right one to make may not be made by manufacturing if the regulatory burden is judged to be excessive. “I never want my manufacturing colleagues to make a decision” based on the change category assessment, she commented. “That is not where we should be going.”
Gleixner illustrated the post-approval change problems using case studies that focused on three different low-risk changes. These involved a laboratory method and drug substance and drug product technical transfers (Gleixner’s complete remarks are provided on pp. 40-44).
In his first example, Gleixner detailed how a change in preparing a laboratory reagent used in an upstream in-process test that had no impact on the associated method took a total of over two years for approval in all of the countries where the product was registered. The drug substance and drug product change cases took even longer.
“What results in the end is a very complex supply situation which is very difficult to plan for, including needing high bridging stocks, which you have to have in case something goes wrong,” he emphasized. “That then leads…to drug shortages. And you hinder innovation and continued improvements of the process and product because you think very, very carefully before you submit one of these changes. And that, of course, has an impact on quality and safety to the patient.”
Gleixner echoed Sturgess in recommending the harmoniza-
tion of change classifications, submission requirements, review timelines and the development of common guidelines to help remedy the situation – potentially through regulator collaborations involving PIC/S, WHO or ICH. Mutual recognition of decisions by reference countries would also benefit both regulators and industry, he said.
Another approach that would “greatly reduce” the number of change filings, the Roche official maintained, would be harmonizing the documentation requirements and removing the GMP elements, such as analytical SOPs and batch records, from the scientific documentation, and verifying these elements, instead, on inspections.
“Changes that innovate or improve the quality of the product could be fast tracked to drive progress,” he proposed, and “their categorization should be driven by their potential to influence patient safety and efficacy.”
Disincentives for Transparency
Central concerns addressed in the discussions that followed the presentations at the closing session were the lack of consistency and clarity around what information provided in an application constitutes a commitment requiring change notification and the relationship between the level of detail provided and the change burden it engenders.
Industry consultant and WCBP program committee member Nadine Ritter opened up the discussion in the context of lab methods.
Ritter explained that she has clients who want to file information that is “as vague as possible” to allow changes without agency notification, while she generally recommends filing enough detail such that a “knowledgeable reviewer” would understand how the method is conducted. The failure to include sufficient analytical method information in IND and BLA submissions has been cited by CBER Division of Biological Standards and Quality Control Analytical Chemistry Team Leader Alfred Del Grosso as a key inadequacy he has seen (see IPQ “Monthly Update” January 2014, pp. 2-13).
Ritter noted, however, that she is “torn,” she said, because “some places in the world would interpret it in a much more rigorous way that would trigger a whole level of things that we don’t anticipate.”
BMS’ Sturgess acknowledged the level of uncertainty regarding what to file and pointed to the lack of clear guidance. She noted that “many” agencies in less established markets do not have a review process that looks at the potential implications of a change. Given this situation, company regulatory personnel tend to “take a conservative view,” and say, “if you change it, thou shalt file it, and it is

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
a PAS.”
An audience participant pointed out that the issue of what to file is related to the level of trust that the agency reviewers have in the applicant and their understanding of why more or less detail is being provided. She further noted that less detail may be perceived as not being transparent. However, she pointed out that in the reagent preparation example cited by Gleixner, more detail in the application resulted in “a two-year or three-year regulatory approval cycle that is just dreaded.”
Another participant referenced the discussions at an earlier workshop at the WCBP on analytical methods in which a suggestion was made to provide information such that the regulators can see that the firm has control over its lab operations rather than provide more detail on individual methods.
Regarding the level of detail to include, Sturgess recommended a summary, potentially equivalent to an abstract in a scientific paper. She said that she has seen a summary that worked well in which examples were given rather than specific data. “You can talk about system suitability and criteria in general terms so that they know what controls you have, but not give enough detail so that every time you update a positive control, you have to do a global filing.”
The discussions at the close of the WCBP symposium extended those that had begun in the opening session regarding the appropriate venue for advancing post-approval change harmonization.
It was noted that WHO has a draft guideline on post-approval changes for vaccines, and that IFPMA is “encouraging” the organization to draft a similar guide for biopharmaceuticals.
Amgen’s Jason Hampson commented that while ICH advocates risk-based approaches, the relevant post-approval legislation “is not written with that in mind.”
Hampson recommended “a stepwise, disruptive change to the legislation to really put in the appropriate degree of oversight for the major changes, and allow sponsors to make certain risk-based decisions as to what gets reported, and move beyond what you have actually written into your dossier.” He noted that there is precedent for such an approach in the European clinical trial application system.
Prior Workshop Also Tackled Change Problems
A workshop that preceded the final session was also focused on how to tackle the problems with the current post-approval change systems.
At issue, Sturgess commented in the workshop, is what drives the reporting of changes. “Is the basis of when I need to report a change the potential to impact quality, safety, and efficacy? Or is it, for lack of a better term, based on the text of the license? It is always a debate.”
She said that she has had discussions in her company where a change was “clearly reportable by the change guideline,” but she received pushback saying it need not be reported because it was not a commitment made in the application. “Well, that is not where we should be as an industry,” she emphasized – hiding behind the text of the application to avoid reporting important changes.
Sturgess also commented that, “on the flip side,” she has seen situations “mainly in some of the smaller countries” where everything in the license is viewed as a commitment. “I have had some interesting conversations around if you put in the detailed SOP – and they ask for the detailed SOP in your module three – then any update to that document that requires a version number update is a prior-approval, because they have no other criteria.”
Commenting on the issue of the level of detail that should be provided in applications at the plenary session that followed, Sturgeon remarked that the regulators themselves are interested in industry striking a balance “because many of them don’t want to review those changes either.”
What is needed, she proposed, are different mechanisms – for example, a biannual report for minor changes, like those involving methods – which would allow for a risk-based approach so that “it wouldn’t really matter if the detail was in there or not.”
Hampson, who lead the workshop, commented on the impact of quality by design (QbD) on post-approval changes and what information regulators need to do a good change assessment. “QbD is extending the gray zone of what is a compliance commitment and what is not,” he said.
The application of QbD in actual submissions is bringing to the surface the disconnects between the review and inspection process – “particularly in the EU, where the review division and the inspection division may be in different countries, and may not even talk to each other.” In that situation, Hampson commented, it is important for the reviewers to have “at least a high level overview” of the firm’s quality management system to be able to judge the potential impact of proposed changes and to have confidence in the company’s ability to manage changes internally.
He cited an example of a proposal to reduce the number of reject limits in favor of increasing the number of associated

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
action limits, which would be managed in the quality system. In that situation, understandably “the regulators are interested to know more about that system.”
Hampson maintained that “with the right dossier construction, with the right information in the right sections, and the right definitions of what an action limit is versus a reject limit” the regulators
could agree to allow some changes to be managed internally and others to be reported.
“I think that is an ongoing journey,” he commented. “We are still, maybe, not even half-way through in terms of understanding that and fitting it within the regulations. I think that many regulations were written for black and white compliance, and the regulations may not align with having effectively some degree of self-regulation.”
POST-APPROVAL CHANGE CHALLENGES AND REGULATORY PROPOSALS TO HELP ADDRESS THEM
The following are discussion points prepared for a workshop on how “divergent regulatory requirements and approval timelines are driving complexity, risk and cost for industry, and potentially hindering continu-ous improvement,” which was held on the last day of the CASSS/FDA WCBP symposium. The discussion points focus on strategies for proactively managing such challenges, and potential changes to the global regulatory framework that would facilitate more efficient change implementation and encourage innovation. Questions addressing the key concerns are followed by some of the relevant considerations.
What regulations are inhibiting innovation and/or risk mitigation? ● Limitations on number of authorized manufacturing facilities and back-up facilities (consequences for inspection scheduling) ● Strict time requirements on change implementation ● Legal definitions of “registered details,” “conditions of approval” and “compliance obligations”
What strategies are companies employing to manage and mitigate the complexity of managing changes into the global supply chain? ● Dual manufacturing processes ● Dual analytical methods ● Rejection of change proposals if costs of filing and implementation do not meet required threshold ● Submission of differing levels of technical details to different territories
What should an ICH-Q topic on change management address? ● Risk-based implementation of changes ● Broader adoption of practical “do and tell” and “tell, wait and do” mechanisms ● Alignment of reportability of changes across ICH regions, without adopting the “lowest common denominator” reporting criteria
What would industry like to see from ICH-observer and non-ICH countries/regions? ● Adoption of future ICH provisions ● Reduction in review periods ● Removal of requirement for proof of reference country approval ● Greater “mutual recognition” of reference country approval ● Broader adoption of practical “do and tell” and “tell, wait and do” mechanisms ● Greater use of regional mechanisms (e.g. GCC centralized process) to drive regional consistency and review speed & efficiency

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
Rethinking the CMC Review Paradigm
The need for a rethinking of the current CMC submission paradigm at the international level to better accommodate manufacturing and control improvements and better align with the advancing GMP quality systems/continuous improvement concepts was clear from the discussions of the current change constraints at the opening and closing WCBP plenary sessions.
Emerging into relief was the vision of a CMC review approach in which transparent, information-rich QbD-oriented applications, incorporating a solid control strategy, would leave more room, not less, for the “self-regulation” of change that Hampson proposed.
Rather than oriented toward preserving the status quo, a revamped CMC filing could provide a control strategy roadmap for continuous improvement as the applicant’s knowledge base increased and the technology improved post-approval. The focus would be on transparency in the CTD around where the applicant was on the knowledge/technology curve and how the additional knowledge would be gained and incorporated post-approval. The application could become, in effect, a commitment to change rather than to maintain the status quo.
IPQ Editor-in-Chief Bill Paulson suggested during the final session discussions that the post-approval change problems highlighted at the WCBP Symposium point back to a larger problem with “the whole CMC review paradigm,” and would not be resolved by “tweaks” in post-approval regulation alone.
“We are changing the way with think about GMPs to allow for continuous improvement. But on the CMC side, we haven’t really seen that same push to change the basic paradigm,” Paulson pointed out.
Rather than focusing on committing to “where you are now,” the application could include “a commitment to change and improve from where you are now, and indicate how you are going to do that.”
The comparability protocol approach is a step in that direction, “but that is really a one-off for each company,” Paulson commented. A deeper-seated approach, he suggested, would be to “get ICH to change the CTD to reflect a continuous improvement kind of modality with a control strategy orientation that would change the paradigm.”
The conversation continued at the session around the use of comparability protocols and the limitations of that approach as a global solution to the change regulation burdens described in the presentations.
It was noted that the comparability protocol requires a prior-approval supplement and does not exist as an option in many places.
Genentech’s Julia Edwards, who co-chaired the session, explained that her company has “had quite a bit of experience with comparability protocols and expanded change protocols for drug substance manufacturing site changes.” She commented that the approach “is great for the US market, but as you start looking at the practicalities of it [in view of] the fragmentation of the supply chain…the benefits start to get smaller. And it is a huge amount of effort to bring something like that through.”
Edwards proposed that “a regulatory agreement structure that can be implemented and executed globally would be the vision there.” However, she recognized the hurdles that would have to be worked through “among the various regulatory authorities from around the world to make something like that happen.”
Medimmune’s Tim Schofield commented that repeatedly doing post-approval comparability protocols for a standard change doesn’t make a lot of sense. “There are so many things that we know we have to do, and we know exactly what we are going to put in the prior-approval supplement, so why don’t we have it licensed ahead of time?”
In a pithy summary of the thrust of the three-days of discussions at the WCBP Symposium, Schofield pointed to a “disconnect between potential quality issues leading to harm to patients and the amount of work that you have to do take care of insignificant changes.”
Pfizer’s Stephanie Pluschkell, who co-chaired the closing plenary session with Edwards, concluded the session by noting that “we have in many ways come full circle and reconnected to the opening regulatory panel where there were a lot of excellent discussions about how to assure access to medicines for people across the globe. It is a very complex issue. There are a lot of players involved. We talked about breakthrough therapies. We talked about what to do when things move very quickly. And we are not going to solve all of this today, or in the next few years. But I think the dialogue that we have had here was excellent.”
[Story continues on p. 36 with Sturgess’ full remarks at the WCBP symposium.]

INTERNATIONAL PHARMACEUTICAL QUALITY
Inside The Global Regulatory DialogueWWW.IPQPUBS.COM
From breaking news to in-depth analysis —
the quality regulatory intelligence you need
at your fingertips!
IPQ tracks the major industry/regulator conferences and forums to keep you informed on the critical CMC/review and GMP/inspection developments in the US, Europe and internationally.
All the stories that appear in IPQ’s real-time “In the News” web coverage and in our “Weekly Alerts,” “Monthly Updates” and “Special Reports” are text searchable on our website
– with the relevant document links you need ready at hand.
We do the work so you don’t have to. Subscribe to IPQpubs.com and relax.

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
BMS’ ANNIE STURGESS ON MANAGING CHANGE IN GLOBAL OPERATIONS
In the final plenary session at the WCBP symposium on managing the global complexity of post-approval changes, Bristol-Myers Squibb (BMS) Global Regulatory Sciences CMC Executive Director Annie Sturgess set the stage by providing background and context regarding why changes need to be made for biophar-maceuticals, and how the general regulatory and country-specific requirements play out in long approval timelines and inventory issues. After providing some background and context, Sturgess discussed: ● the challenges in interpreting regulations and timelines ● the concept of a “living license” or “living dossier” ● the implications of implementing global changes ● the inventory problems that the current system fosters, and ● mitigation strategies.
I am going to be focusing on everyone’s favorite topic, particularly my manufacturing friends – change control. Prior to the meeting, the presenters got together and we decided it would be good if we could start with the first presenter giving an overview of the issue. So you are going to find mine isn’t a detailed example, it is going to be framing the questions and the topics.
I will talk about why we do post-approval changes and go over some general regulatory expectations and some country-specific requirements so it is put into context. Often we get asked what the terms mean. I will explain them. Then I am going to talk a little about challenges, global implications, and maybe some ideas of what we can do as a collective community to start mitigating those challenges. Then I will end with some key messages.
Reasons for Post-approval Changes
I think we have heard this week that our manufacturing processes are complex, our assays are complex, and the technology is evolving. So we anticipate after the launch of a new biotech product that we are going to need to make changes to stay up with the times. Innovation is a big driver. Efficiency improvements – sometimes you hear your productivity isn’t as high as you would like it to be when you first start because you are trying to get the new medicine to patients quickly. So as you go through, you want to make it more efficient.
Some of the changes are driven by changing regulations or items that come up in inspections. Some of them are GMP-driven changes, but they are still affecting information in our approved dossier. Another one is when your equipment becomes outdated or a vendor no longer makes a reagent. It becomes critical, and sometimes you don’t get a lot of advance notice.
General Regulatory Expectations
So what happens then? We have to report it…. The bottom line is, it is the law. But most importantly, it is the law in every country where you have licensed the product, and every country has its own unique interpretations and requirements….
The types of changes that are prior approval are the big ones. We all know them when we see them. They are a major filing in most countries. The big thing is, you have to get the data, submit to the health authority, and wait for approval before you can put product on the market.
Below that there are different categories. The tell, wait, and do: I get the data, I submit it, and then I get approval, but have to wait for a fixed period of time before I can start releasing product to the market. There is a tell and do. There are a few examples of that. Then there is do and tell, where you can implement the change, start making it available to patients,
Examples of Country-Specific Reportable ChangesType of Change ExamplesPrior Approval � US: Prior Approval Supplement (4 month FDA review �me)
� EU: Type II; Type IB (60 days)� Japan: Par�al Change Applica�on (3-12 months)� Switzerland: Varia�on that does not meet the condi�ons for
no�fica�on (140-270 days)� Mexico: CMC Varia�on 12 – 15 months
Tell, Wait, & Do � US: CBE-30 (30 day wait)� Switzerland: Varia�on Requiring No�fica�ons (30 days)� Saudi Arabia: Type IB
Tell and Do � US: CBE (no�fy, then implement)Do & Tell � US: Annual Report
� EU: Type IA� Canada: Annual No�fica�on� Brazil: Annual Report� Japan: No�fica�on - within 30 days a�er implementa�on

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
and then within a fixed time frame and communicate that to the health authority.
I don’t have every market’s requirement or terms here. I have some examples of each (see box above).
Prior approval is generally self-explanatory. In Europe there are two categories of review clocks. I have a few here. Tell, wait, and do – most people always think it is CBE-30. In other countries, I always explain that it is like a CBE-30, just go with that.
The U.S. also has a CBE. Some countries have annual reports or annual notifications, and some just have a notification process. The biggest challenge is that there are many countries that don’t have anything below the prior approval line.
Challenges Interpreting Regulations and Timelines
The next challenge we face is interpreting the regulations and the timelines.
Regarding submission categories for change, I think anyone in the regulatory framework knows the question: ‘If I do this, what is the reporting category?’ We are asked that on a daily basis. Well, it is not always clearly defined.
Some countries do a better job than others. I know Health Canada has some great guidelines. What happens is, when it is ambiguous, there are different interpretations. Even within companies, I am amazed. Someone will bring forward a change, and within the people on my team, you will have one person saying ‘annual report’ and the other saying ‘PAS.’
The biggest challenge is the tendency sometimes to say, ‘submit everything as a prior approval.’ It is not just a challenge for industry. I have seen differences in interpretations from health authorities. It is not clear, and it depends on your understanding of the change and your perception and maybe some past experiences.
Review times can differ drastically around the globe. There are countries that lack defined review periods. So you don’t know. You know what the last few have been like, and you know kind of a general expectation, but they are not defined.
There are countries that still require approval by a reference authority. So you have to get approval in the first country, and then submit in the second country, which can take 12 months. You can see that staggers it, and it prevents us from being able to submit globally at one time. Overall, and I have seen and felt this number – some changes require three to five years to get global approval. The big impact of that is the supply chain impact, and it can lead to drug shortages.
The Living License/Dossier
The other challenge, and I bring this term up, because it is an interesting one: I have benchmarked in the past from at least three or four companies, and it is the term ‘living license’ or ‘living dossier.’ Most regulators don’t know exactly what I mean by that, but they can kind of guess it, because it is self-explanatory.
In theory, a living dossier consists of the quality module, and a very conservative approach is to continually update it such that every section and every word is representative of the current condition. That is the strict definition. Some people use that. Some countries expect that. It is not always clear who does. I have heard people say, ‘that is not a living section.’ I ask, ‘who defines what a living section is? Where is it written?’ It is not written anywhere.
The one advantage of keeping it living is that it is always easy to see what is approved. And if it comes up during a health authority inspection, you can show that it was approved.
The challenge is mainly in those countries that don’t have categories below a simple PAS or a simple notification – in that middle ground. Everything, even those that are classified in other countries as minor, not just the manufacturer’s interpretation of minor, ends up being a prior approval. You see this particularly with facility changes a lot, and with

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
some analytical changes.
One of the questions I have seen recently, if you are implementing a new system for managing your analytical methods, is ‘do you have to do that because the method number changed?’ I keep asking people, ‘help me understand. What will you do tomorrow differently than what you did today?’ Absolutely nothing. The only change is the number. But guess what? It is on your spec table. It is in your specs. It is on your C of A [certificate of analysis].
I have seen mixed practices happen. But in some countries, if you query the local manager, they will say ‘prior approval.’ The potential impact on patient safety or efficacy? None. Nothing has changed. I am doing the same thing, but the number has changed. But there could be a situation where I am waiting for health authority approval and it is impacting drug availability. Or it could delay getting a new and better quality system to be able to manage it.
Regulatory expectations for having or keeping a living license are not clear. In fact, many agencies have never said that they need this. It is industry interpreting – we cause our own pain at times. But there are periods where inspectors will do a side-by-side comparison. And if they do, you can get an observation, because you are not in accordance with your license.
Some countries are clear. PMDA is very clear. But if you ask a lot of people, ‘well, what does that mean?’ I talked about the quality module. Most people think of that as Module 3, right? No, the one they manage is Module 1. We talked about that in the workshop earlier. Module 1 is a legally binding document.
Global Implementation Implications
What is implementation? If you are in manufacturing, you will have one perspective, and if you are out in the world, in industry or in regulatory, you may have a different one. There are two different opinions on that. It is when the change is introduced into routine manufacturing. But from a health authority standpoint, they want to know when that change is entering the market place. That is when they want to see and maybe monitor AEs [adverse events], and pharmacovigilance starts coming up in discussions.
Many countries require the introduction of product manufactured with the change at a specified time after approval. That can be challenging. You make the change. Globally it can take three to five years to get approval. And if one of the countries you need as a reference member state is the first one, and they expect that in a year, then you have two types of supply. And I know I am introducing a lot of terms to some people, but you start seeing these in industry because that is what manufacturers deal with. It is fragmentation of inventory and potential supply shortage. I find the term fragmentation interesting. I have been in regulatory for eight years, and I did not hear it until I switched to a new job.
In my old world, they were managing it through material numbers in SAP, and they called it proliferation. You had proliferation of your versions. It is a different term that means the same thing. Whatever term you use, it is basically when not all of your inventory is available to supply all countries for which the product is approved. Pretty simple. Pretty basic challenge. What is amazing is that the inventory may be impacted differently for each change and for each country.
This is just a hypothetical situation – an example (see box at right). I wish it were this simple. This is a case where there could be six potential changes that came on at different periods of time. Some are requests from health authorities. Some are vendor changes. Some are continuous improvement. What we tried to do, where it says ‘lots impacted by the change,’ you may have lots in the A category that are only impacted by one of those changes. Then you have lots in the B
Inventory Fragmentation Example
Change Reason for the changeDrug Lots Impacted by the Change
A B C D EEnhancement to method “A”
Request from health authority “A”
X X
Drug substance facility modifica�on
Inspec�on commitment (health authority “B”)
X X
Raw material change Vendor change X X XEnhancement to method “B”
Con�nuous improvement X X X X X
Expiry extension Availability of addi�onal data
X X X
Drug substance process change
Process consistency X X X X

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
category that are impacted by two of them. You can see the complexity. So I have multiple different groups of products that can go to some countries but not others.
Managing that inventory can be quite challenging. The inventory will consist of lots manufactured with different combinations of the changes. But most importantly, they change over time. So you saw the scenario with the lots available that only had the ‘A’ change. Supply goes down over time. And if you haven’t planned for it well, it could be a situation where you are talking about having to plan around a shortage and shuffle things around.
It is not ideal. So at any time, supply may be limited for some companies due to pending regulatory approvals. Now companies will sometimes manage that by saying, ‘I am holding this supply to meet the global market, and I will start switching over as they approve.’ It is not an easy task.
Mitigation
So, what can we do to make the process more efficient? We would like to update existing guidelines to reflect current expectations, to try to get a more consistent interpretation. It is really challenging, even for me, when I am talking to people with regulatory experience, and I will mention it, and they have such extreme, diverse experiences.
It would also be good – and I don’t have this listed – to define the expectations for what sections in that license must be maintained as living. We had great discussions on this during the workshop.
It would be good if we could harmonize and define the change control categories based on the potential to impact quality, safety, and efficacy, so we can make risk-based decisions rather than document-based text decisions.
For countries that do not have it, it would be good to create options for notifications for minor changes so there is less of a supply impact for minor changes.
We need to align on what is minor. I always laugh when any change control I get from manufacturing says, ‘minor change.’ I so, ‘no. That is a subjective term. Take that out. That is for us and the regulators to decide.’ There will be some big ones that will say ‘minor change,’ but is a PAS.
Continue to improve the timelines. I will put in a plug for many of the health authorities around the world for what they have done – they are getting better. When I first came into industry, compared to what I see now, it is improved. Let’s continue in that direction.
Key Messages
Post-approval changes are essential. We want to stay current. We want to innovate. We want to improve. We learn new things. We are learning them every day. We don’t want to hold back change.
I never want my manufacturing colleagues to make a decision based on, ‘Annie, if I do this, what is the filing category?’ ‘It is a PAS.’ ‘What about if I do this?’ Well, they just made a decision that may not be the best one long-term. That is not where we should be going. That happens frequently.
Managing post-approval changes is complex and time-consuming. Longer approval times can result in depleting of inventory that meets a particular market’s license. Sometimes it delays implementation. It can hinder innovation and continuous improvement. As I said, ‘we don’t want to implement it now even though it is an improvement, because we need to build inventory.’ That is not where we want to be.
We need better and harmonized guidelines. I think we all recognize that each country has its own legislation. But maybe they can help to bring clarity and consistency in interpretation for better risk-based decisions.

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 �0
MONTHLY UPDATE - FEBRUARY 2014
ROCHE’S RALF GLEIXNER ON POST-APPROVAL REQUIREMENTS FOR MINOR CHANGES
Following Sturgess to the podium at the final WCBP plenary session, Roche’s Head of Marketed Biologics in the EU Ralf Gleixner delved further into the consequences of the divergent expectations among regula-tors for CMC submissions and post-approval changes. His talk encompassed: ● the elements of life-cycle complexity ● a handful of telling case studies showing that even minor changes have extended approval timelines, and ● “reflections on pragmatic solutions.”
I am pleased that I can talk to you about something that really cries for convergence. What I will try to do in the next 20 minutes or so – bear with me if it takes a little longer – is summarize the current challenges of global life-cycle management, more from a regulatory perspective. To illustrate this, what I will be telling you, will be some examples that are actually random. I just told my group to give me a few examples that have a green flag that can be implemented, and then I looked up what I would do with it. I will include some reflections on how we can improve that with some more or less pragmatic solutions.
As a little bit of background, pharmaceutical companies on a bigger scale usually operate globally and have global manufacturing operations. That means they will have to follow global regulations and submit a global registration that meets the requirements of all health authorities where they operate. And they have to manage a global supply chain, which often means they have to have a multiple sourcing strategy for risk-mitigation.
I have split the rest of my talk into three parts: ● the elements of life-cycle complexity ● some examples, and ● reflections on pragmatic solutions.
Elements of Lifecycle Complexity
The content differences from original submissions are the first main cause of life-cycle complexity. There are approximately 192 recognized states. In the case of Roche, we are active in about 140 of them. In general, there will be two types of registration dossiers and packages. One is an ICH type, where you give lots of technical documentation. And the second category is one where you are allowed to give a little bit less detail.
Unfortunately, there is a trend of introducing more individual country-based details. I get requests for declarations that have to be hand-signed. I get requests for raw data. I get requests for paper-based inspections where GMP documents have to be put into the submissions. That obviously complicates things.
There is also a difference in the submission approval timelines that adds complexity on top. And some of them are homemade, because we have a tendency to submit applications in waves. One reason for that is because some countries need the so-called CPP, or certificate of pharmaceutical product, which means they have to wait for the approval in the country of origin or another country where the manufacturing is done.
Some of it is internal. As I said, there may be prioritization in the affiliates. They say, ‘we already have ten submissions
One Global Submission: Multiple Local Registrations
Each pin reflects a dossier with separate regulatory commitments for one
product application…..24 separate registrations for one product

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 �1
INSIDE THE GLOBAL REGULATORY DIALOGUE™
to do, this one goes to the end of the tube.’ And that can be based on purely logistical problems and resource problems, but it can also have reasons in terms of reimbursement – ‘I have to submit here first, because otherwise I will not get a good reimbursement in one of my neighboring countries.’
And then, of course, the international approval timelines differ vastly. You can get an approval in the U.S. in six months, or in ten months, but it may take 36 months to get the approval elsewhere.
I borrowed this slide from an ISPE annual meeting in November 2013, because it I thought it is a nice way to show what can happen to you: One submission had 24 different approved files (see box above).
Here is an attempt to summarize what I have just told you. To the workshop participants, my apologies as you have seen this before.
You start off with documentation with more or less detail depending on the country that it is submitted to. So far, everything is fine. And then you get an approval after question and answer, and the situation may look completely different, because some countries will have modified your file. By question and answer, and the commitments you have to make, [the number of different versions increases].
That is not the end of the story, because so far you have not submitted in your CPP countries yet, because you get the CPP on the basis of a modified dossier that is approved in the country of origin. It may not necessarily be the same certificate that you get for the country where your manufacturing takes place. These come much later. That is basically a situation that you face even before you market your drug.
So now we are getting into the area of post-approval changes, and that complicates things even further, because some of these countries don’t have any classification guidelines. They don’t tell you if they are minor or major. You just simply don’t know. They may be completely different. It may be that I have a change that is annual reportable in the United States, but it is a minor submission somewhere else – for example, a type IB submission in Europe. In the extreme of all cases, you may need a new license in a country like Indonesia.
Change Review TimelineThe following illustrates the time a single, minor change can take from submission to approval when filed in multiple countries:
D oc R ev iew 0-10 m
D oc R eviews 6-20 m
R eview 6-24 m
0 2 4 12 24 36
DataCPP
Time Elapsed, Months
Wave 1: “ICH dossier” countries
Wave 2: Non-CPP
Wave 3: CPP countries

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
On top of all that, you may have country-specific requirements. Some countries want to have 12 months of stability data before you even do the submission. In other countries you can submit with three months data. This, combined with very long, unpredictable timelines, makes things even more complex.
What results in the end is a very complex supply situation which is very difficult to plan for, including needing high bridging stocks, which you have to have in case something goes wrong. That then leads to what Annie already told you, to drug shortages. And you hinder innovation and continued improvements of the process and product because you think very, very carefully before you submit one of these changes. And that, of course, has an impact on quality and safety to the patient.
So after the first approval – and I am not talking about the second one, because then it becomes messy and I couldn’t get it on the slide anyway – it may look like this (see box above).
Because, again, in your approval of the change, there will be subsequent changes introduced during the review. And this is why post-approval changes – and this is a theory – should be approximately a three-year endeavor.
Change Examples
I went to my group out and said, ‘okay, give me some examples. I want a minor change.’ I wanted something that is a little bit more complex, let’s say a drug substance tech transfer, and I wanted a drug product tech transfer, because that is the most complicated situation I can think of, because it has to be submitted virtually in all countries. That is what I did.
Before I get there, when you get out of here and you don’t remember anything I said, just remember that life-cycle complexity is resource-intensive for both the industry and for the agencies, because these changes pile up and make a lot of work.
So the first case study is something that I have thought was seemingly very minor and should not be a big deal to implement. It was an IPC [in-process control] method, and we just made a little modification in the way the method was run. It was not a change of the method, but it was a change in how a reagent was prepared. Unfortunately, it was registered in a few countries. So what was the situation?
Okay, so the product – I won’t name it, it doesn’t really matter – was registered in 127 countries…. 108 said that no submission was needed. So there were only a few countries, around 20, where we had to actually do the submission.
I was also interested in how many of the problems that we have were caused internally. So I looked at when I dispatched the files – which happened in May 2011 – and how long it took to get all the submissions in. To my surprise, there were a few countries that actually said, ‘you don’t have to submit this, we misinterpreted the change.’ In others, however, we submitted this within 30 days, and then there were a few exceptions that took up to six months. So I thought this was not bad – half a year for the entire submission was okay.
So then I looked at what happened from submission to approval, and how long that took.
This went pretty well in most countries. Within 30 days we got approval in North America and Europe. Within six months we got a few other countries – we got Australia and Central America. But then unfortunately there were a few outliers in which it took more than 12 months to get the approval. That dragged out the change to a total approval time in the last country to 20 months, and then closure only after 26 months, for a change that was very minor. So it took more than two years for this change.
Let’s look at something a little bit more interesting, where we have to do more countries – a drug substance change. This was a technology transfer from one site to another, and the documentation had to be dispatched into 88 countries. We are moving from 20 to 88. I have summarized a little bit: ● 20 countries gave “active approvals” ● three countries were submitted notifications without supporting documentation ● 51 confirmed that submission was not required, and

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
● 14 countries never confirmed anything.
So again, the same story. Here the dispatch happened in several waves, because we had to wait for CPPs in this case. So the first wave was in April and July 2010. The second wave had many countries in September and October. Some countries did not require submission…. And there were a few countries that we did later because they didn’t have approval at the time we wanted to submit the drug substance transfer, we actually had to wait for those approvals before we could submit. That happened in 2011 and 2012.
So now for time from dispatch to submission – it is the same picture roughly. The majority of countries were submitted within the first 12 months, but some took more than 12 months. The situation on submission to approval was also a mixed bag. Some approvals came in within 30 days – those that only required notifications. Others came in within the first six months. The majority were actually done after 24 months. But overall the longest approval was 24 months, and the time to closure was 33 – almost three years for this change.
Here is my last example, a drug product change. I had to choose another product for this one, unfortunately, because we didn’t have a corresponding change for the first one. And again, the documentation was dispatched in 120 countries. 13 countries including the EU, which is another 28, were in the first wave. 87 countries were in the second wave, which was partially caused by the need for CPP, which 37 countries actually wanted. Up to today, 101 countries have now completed it.
We will take a little bit of a step back. How long did it actually take to get the CPP? Because that is obviously the starting point for many countries. For Europe, it was about six months. For Switzerland, it was about 12. So you would
expect if you submit somewhere in 2006, 12 months later you would see the second wave, and that is exactly what happened. The product was registered in 120 countries, and obviously there were two waves of submissions: One was in March to June 2006, and the other was in May to July 2007. There were only three countries where we didn’t
Global Application Approval TimelinesThe following is Gleixner’s depiction of the approval times for a drug product change submitted in 120 coun-tries. It is color-coded as follows: ● yellow, submission not required. ● blue, approved within 30 days. ● light red, approved within 12 months. ● green, approval exceeded 12 months, and ● dark red, not submitted or not yet completed.
Submission not required Within 30 daysMore than 12 months
Not submitted / completed Within 12 months

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
have to submit in this case.
So the actual submission, where I could find the data, was actually performed in ten months in the vast majority of countries. But there were several, the green and yellow ones, where I couldn’t find the actual submission date. Luckily, I could find all the approval dates and the dispatch dates so I could do some calculations (see box below).
Here is the outcome of the time for submission for approval: Some were between two and 12 months. Again there were a few, mainly in the Asia region, that took more than twelve months. Overall, I think I can say we are roughly in the area of around twelve months for that change.
Now what does this look like when you look at the data of date of dispatch to actual approval? This is where I had the shock of my life: The last countries actually came on board only after 36 to 41 months. These are the ones that are approved today, and there are still a few countries pending where we live on bridging stocks right now. I can give you the example of Iran, where it took 71 months to approval.
The essence of this section is that global change requires multiple years until complete implementation.
Reflections on Pragmatic Solutions
So now a few reflections on what could be done to improve the situation.
I think it would be very good if we could have a defined change classification, procedures and document requirements, because that would accelerate implementation massively. You would just have to prepare one dossier for all of the countries and not multiple dossiers for multiple countries.
It would mean a convergence in change classification and at least a vague agreement on review timelines. This may actually include a ban on applicants not responding within a certain timeframe, because that also sometimes happens. That is homemade, of course. And maybe convergence of document requirements – in particular, the elimination of GMP documents and declarations that are not very useful, and the elimination of raw data that can always be checked on inspection.
If you want to take this a step further, you can say that the workload of the agencies, who very often complain about the lack of resources, could be actually diminished by mutual recognition of certain things – for example, inspections. Why is it not possible that we have a PIC/S country that is inspecting other countries that are also PIC/S members accept it? It is just a thought.
And QC samples, if they are tested in one state lab, why do we have to retest them in several other countries again?
In the European Union there is a procedure that is called ‘mutual recognition.’ Why don’t they install this in the LATAM region and the APEC region and the EMA region? Maybe that is possible. Maybe we can distribute different dossiers and different changes to the different countries and then they just do one assessment, and then the other countries review their regional parts and mutually recognize the decision by the first one. Who could actually coordinate the writings of guidelines? It could be WHO. Or maybe it could be orchestrated by the ICH global coordination group.
It will be important that there is a lot of sense in this, that there is a risk-based approach to writing those guidelines so that we get a risk-based approach to the classifications, the timelines, and in particular, also the document requirements without any GMP documents.
The last message here is that conversion of requirements and mutual recognition can reduce the complexity of life-cycle changes. A global conversion of national change regulations would substantially improve planning and execution of changes and ensure patient supply of high-quality drugs globally. Convergence could include change classification, reporting procedures, documentation requirements and timelines, and mutual recognition of inspections and sample testing results. This would reduce the work of both agencies and companies alike.

Protecting Patients WorldwideProtecting Patients WorldwideProtecting Patients WorldwideProtecting Patients WorldwideProtecting Patients Worldwide®®
+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org+1 (202) 230-5608 • [email protected] • www.rx-360.org
We the undersigned members of Rx-360 fully support the mission of Rx-360 which is to:
PROTECT PATIENT SAFETY BY SHARING INFORMATION AND
DEVELOPING PROCESSES RELATED TO THE INTEGRITY OF THE
HEALTHCARE SUPPLY CHAIN AND THE QUALITY OF MATERIALS WITHIN THE SUPPLY CHAIN.
ABBVIE • AMGEN • AMPAC FINE CHEMICALS • ASH STEVENS • ASTRAZENECA • AURISCO PHARMACEUTICAL CO. LTD. • AVANTOR • BASF • BAXTER • BAYER • BEND RESEARCH • BIOGEN IDEC • BO
EHR
ING
ER IN
GELH
EIM • B
RISTO
L-MYER
S SQU
IBB
• CA
MB
RID
GE M
AJO
R LA
BO
RATO
RIES • C
AR
DIN
AL H
EALTH
• CO
DEX
IS • DA
IICH
I SAN
KYO
• DK
SH IN
TERN
ATION
AL • D
OE &
ING
ALLS • D
SM N
UTR
ITION
AL P
RO
DU
CTS • ELI LILLY • FO
REST LA
BO
RATO
RIES • FU
JIFILM • G
E HEA
LTHC
AR
E • GLA
XO
SMITH
KLIN
E • HIKAL • HOSPIRA • HOVIONE • JOHNSON & JOHNSON • LABOCHIM • LIFECONEX • LIFE TECHNOLOGIES • LIGAND • MERZ • MERCK & CO. • MERCK KGaA • MYLAN • MYODERM • NOVARTIS • N
OV
OZ
YM
ES
BIO
PH
AR
MA
•
PE
RR
IGO
•
PR
OC
TE
R &
GA
MB
LE
• P
FIZ
ER
•
OS
O B
IOP
HA
RM
AC
EU
TIC
ALS
•
RO
CH
E/G
EN
EN
TE
CH
•
SA
NO
FI
•
SA
RT
OR
IUS
•
SIG
MA
ALD
RIC
H
• S
PE
CT
RU
M C
HE
MIC
AL
MF
G
• T
AK
ED
A
• T
EM
PT
IME
•
TE
VA
•
UC
B
• V
WR
•
WA
TS
ON
•
WE
ST
•
YO
RK
CO
NTA
INE
R
•
We support our suppliers and colleagues who share our support of Rx-360 and its critical mission to protect patient safety. And, recognizing the power of leadership by example, we
invite others who share our patient safety goals to join us in this important endeavor.
Wes SchmidtVP, Quality Systems
AbbVie
William ReisVP, Global Strategic Sourcing
Amgen Inc.
Martin VanTriesteSVP QualityAmgen Inc.
Gary A. BakerVP, QARA
Ash Stevens, Inc.
Ashley ReadshawChief Procurement Offi cer
Astrazeneca
Peng ZhienPresidentAurisco
Richard M SiberskiGlobal Director of Quality
Avantor Performance Materials
Jaspreet GillVP, Global Quality & ComplianceBaxter Healthcare Corporation
Dr. Paul Heiden SVP QHSE
Bayer HealthCare
Richard SpoorSVP ProcurementBayer HealthCare
Debra KatterVP, Corporate Quality
Bend Research
Melissa Stoutt SeymourSr. Director, Corporate Quality
Biogen Idec, Inc.
Robert PantanoSVP, Warehouse Operations and
Operational ExcellenceCardinal Health
John NicolsPresident and CEO
Codexis, Inc.
Allen WelsherGlobal Head QA
Daiichi Sankyo Co., Ltd.
Jennifer Finnegan McCafferty
VP External QualityGlaxoSmithKline
Luisa PauloCompliance Director
Hovione
Vincent AntleSr. Director of Technical Operations and Quality
AssuranceLigand Pharmaceuticals, Inc.
Robert NassVP Quality and Regulatory
Management Merck Millipore Merck KGaA
Matt AndersonVP Quality
Merz North America, Inc.
Patricia M. LatzoSVP Global Quality and Strategic
SourcingMylan Inc.
Michael CohenManaging Director
Myoderm
Michael HoffmanVP Global Procurement
Pfi zer Inc.
Heiko HackelVP Global Sourcing
Sartorius
Thomas PaustVP Supply Chain Management
Sartorius
Tom BeilVP, Quality and Regulatory
AffairsSigma-Aldrich
Tom TynerVP Quality & Technical Service
Spectrum Chemicals and Laboratory Products
Steve FeldmanVP Quality & Regulatory Affairs
Temptime Corporation
Angélique KlootwijkDirector Quality Management &
Quality AssuranceVWR International
Pfi zer Inc.
Heiko HackelVP Global SourcingVP Global Sourcing
Robert Pantano
Thomas Paust
Richard M Siberski Melissa Stoutt Seymour
GlaxoSmithKline
Luisa PauloCompliance Director
William Reis
Robert NassRobert NassVP Quality and Regulatory
Management Merck Millipore
Wes Schmidt
Tom BeilDebra Katter
Allen Welsher
Hovione
Vincent Antle
Patricia M. Latzo
Ashley Readshaw
Temptime Corporation
Angélique KlootwijkDirector Quality Management & Director Quality Management &
Michael Cohen
Peng ZhienPresidentAurisco
Martin VanTriesteSVP Quality
Myoderm
John Nicols
Sigma-Aldrich
Tom TynerVP Quality & Technical Service
Spectrum Chemicals and
Gary A. BakerVP, QARA
Ash Stevens, Inc.
Jaspreet Gill
Jennifer Finnegan McCafferty

You Can Count On Our Expertise To Realize Your Goals.
We help put your plan in motion… And then we f inish it with you.Our unique focus is helping you meet your development and commercialization needs by bringing your product to market quickly and successfully, while maximizing the expertise and resources you already have on board. With decades of experience and involvement in dozens of products that have been filed and approved in the United States and across the globe, we’re the experts you need to shape and execute your biopharmaceutical manufacturing and CMC needs.
Contact us for the resources to start delivering on your goals.Peter Dellva: (847) [email protected]
Or Visit: www.biotechlogic.comwww.processvalidation.com
Our approach is tailored to meet the requirements of your project. We can integrate into your development efforts, augment your team resources, or provide hands-on support.Our areas of expertise include:
Our success has been our ability to serve as your technical expert and be the additional resource that helps you drive and execute your plan.
Process Validation Regulatory Submissions Quality Assurance

MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
Updates in Brief
CMC/REVIEW
FDA To Hold Hearings on OTC Overhaul Plan FDA will hold public hearings on March 25-26 at its White Oak, MD campus on a plan to strengthen its oversight of OTC products and align it more closely with the prescription drug process. Comments will be accepted until May 12, 2014.
FDA Implements ICH Photosafety Evaluation Guideline (S10)
In early February, FDA announced its implementation of ICH’s photosafety evaluation guideline (S10). The guideline addresses the toxicity resulting from drug exposure to light. In order to better address safety concerns, a distinction has also been made between phototoxicity and photoallergy.
FDA to Move Toward More Transparency
In line with the White House digital strategy initiative, FDA has opened up a number of its document related datasets for direct download access from its website. Among these are adverse event reports. It also gives access to an Application Programming Interface (API) allowing the data to be accessed directly by software.
GMP/INSPECTION
Congressional Hearing on Counterfeit Drugs and Supply Chain
A February 27th hearing was held by the House of Representatives’ Committee on Energy and Commerce to discuss the FDA effort to combat counterfeit drugs and what additional authorities may be needed to aid this effort. Appearing at the hearing were FDA Deputy Commissioner Howard Sklamberg, Elizabeth Jungman of Pew Charitable Trusts, as well as leading industry experts. [Video of hearing.]
FDA Begins Secure Supply Chain Pilot
FDA has begun its Secure Supply Chain Pilot Program, which will permit 13 participating companies to import up to five products into the U.S. with an expedited clearance. Announced last August, the pilot is intended to allow the agency to focus its surveillance on shipments that are at higher-risk of adulteration or counterfeiting (see IPQ “Monthly Update” September 2013, pp. 24-28).
FDA Asking for Comments on Standards for Tracing Rx Drugs
FDA is establishing a public docket to receive information and comments on the standards needed to comply with the track and trace provisions in Title II of the Drug Quality and Safety Act (see IPQ “Monthly Update” January 2014, pp. 13-20). A February 20 Federal Register announcement explains that the agency wants to figure out how to confirm that all transaction information, including histories and statements, is interoperable in both paper and electronic formats.
FDA to Report on Generic Drug Inspections in 2014
An HHS 2014 work plan calls for FDA to report on its inspections of generic drug manufacturers and related enforcement actions by the end of the year.
DQSA Title I Cited in Warning Letter to Pharmacy Compounder
A warning letter issued to Triangle Compounding Pharmacy is the first to cite Title 1 compounding provisions of the Drug Quality Security Act (see IPQ “Monthly Update” Nov./Dec. 2013, pp. 28-30). The letter, issued in the wake of a February/March 2013 inspection, states that the sterile drug compounder does not “qualify for the exemptions in section 503A of the FDCA” due to the findings that patients receiving the firm’s products were not individually identified.
UNITED STATES

MONTHLY UPDATE - FEBRUARY 2014
WWW.IPQPUBS.COM FEBRUARY 2014 ��
MONTHLY UPDATE - FEBRUARY 2014
EUROPE CMC/REVIEW France to Allow Biosimilar Substitution
Pharmacists in France are now allowed to substitute a biosimilar for a prescribed biologic as long as the prescribing physician has not marked the prescription as “non-substitutable.” A law concerning France’s Social Security budget, which came into ef-fect on January 1, has provisions that allow the substitution. [See IPQ “Monthly Update” August 2012 pp. 34-38 for an analysis of global regulatory pathways for biosimilars.]
GMP/INSPECTION
EDQM Launches Webpage on Counterfeit Medicines
EDQM has launched a new website capturing its activities in the field of “Counterfeit Medicines and Similar Crimes.” The website covers risk communication, facts, and practical advice regarding counterfeit issues. The website also lays out legislative, public health, and criminal legal strategies.
New EudraGMDP Database lists 87 Non-Compliant Companies
As of the end of February, EMA’s EudraGMDP database, recently made publicly available, lists 87 companies as having received non-compliance statements. The list extends from a Genzyme statement issued in 2009 through a statement regarding Smurthi Organics Limited issued in January. The statements include a brief explanation of the main GMP problem areas uncovered at the firms.
INTERNATIONAL
CMC/REVIEW China Issues Regulatory IT Standards
CFDA issued IT standards in late February facilitating interoperability between different parts of the agency. The IT standards focus on food and drug classification and coding, regulatory infrastructure information, a common regulatory support plat-form, and a software development process specification.
Australia to Adopt EMA Biosimilar MAb Guideline
Australia’s Therapeutic Goods Administration (TGA) announced in mid-February that it is carrying out public consultations on its adoption of the EMA 2012 guideline for biosimilar Mabs.
Update Provided on Australia/New Zealand Agency
Australia and New Zealand’s regulatory agencies have provided an update on their progress in developing the Australia New Zealand Therapeutic Product Agency (ANZTPA). The combined agency will cover pre-market evaluation and assessment, product licensing, controls on manufacture, post-market monitoring and surveillance, and setting standards.

MONTHLY UPDATE - FEBRUARY 2014MONTHLY UPDATE - FEBRUARY 2014 MONTHLY UPDATE - FEBRUARY 2014
FEBRUARY 2014 ��
INSIDE THE GLOBAL REGULATORY DIALOGUE™
GMP/INSPECTION
Hamburg Addresses Drug Quality Regulation During India Visit
In mid-February, FDA Commissioner Margaret Hamburg traveled to India to meet with government officials on quality and other regulatory topics. This visit included the signing of a “Statement of Intention” to clarify the points on which both countries will cooperate, such as: ● sharing of CGMP compliance and facility information, ● India observing FDA inspections, and ● enhancing communication and public meeting collaboration. [Hamburg’s Feb. 14 and Feb. 21 blogs on the trip. See IPQ “Monthly Update” July/Aug. 2013 pp. 2-8 for an analysis of FDAs inspection findings of data integrity problems in India.]
FDA and EMA Create Pharmacovigilance Cluster
EMA and FDA announced a new pharmacovigilance “cluster” to provide a forum to share information on the safety of medicines. The “cluster” will involve monthly meetings via teleconference, during which agency representatives will discuss “areas that have been identified as requiring an intensified exchange of information and collaboration.” Representatives from Canada and Japan will participate in these meetings as observers. [See IPQ “Monthly Update” Nov./Dec.2013 pp. 44-53 for an analysis of the industry effort to empower pharmacovigilance programs to find GMP root causes.]
IPQ wishes to thank the following sponsors:
For subscription and sponsorship information visit IPQpubs.comor contact Wayne Rhodes — [email protected], Tel: �0�-��1-���0.

International Pharmaceutical Excipients Council Of The Americas
3138 N. 10th Street, Suite 500, Arlington, VA 22201 • Phone: (571) 814-3449 [email protected]
IPEC-Americas QbD Webinar Series Excipient Variability: Design & Lifecycle Implications
Speakers:
§ Brian Carlin (Director of Open Innovation (Pharma), at FMC BioPolymer, and Chair of the IPEC Quality by Design and Excipient Composition Committees)
§ David R. Schoneker (Director of Global Regulatory Affairs at Colorcon, and Vice Chair of IPEC-Americas Maker and Distributor Relations)
§ R. Christian Moreton, Ph.D (Formulation Scientist, Principal, FinnBrit Associates, and past Chair, IPEC-Americas)
§ Tim Cabelka (USP Expert Committee, Consultant, previously with Dow Wolffe Cellulosics) § Joseph Kushner, IV, Ph.D. (Principal Scientist, Pfizer, Inc - Drug Product Design)
I. February 11, 2014 (Webinar I: 3 part)
1) Introduction to IPEC Americas and Total Excipient Control (TEC) – D. Schonekera. Workshop Objectivesb. Background on IPEC Americasc. The Need for Improved Controlsd. IPEC Guidelines and Initiativese. TEC Elements
2) Manufacturing of Materials that are Useful (Fortunately) as Pharmaceutical Excipients – T. Cabelkaa. Intended primary market for the material (excipients may be minor use)b. Scale of manufacture/practical limitationsc. Types of Manufacturingd. Continuous and batch processinge. Hypromellose Manufacturing Processf. Ethylcellulose Manufacturing Process
3) Types and Sources of Excipient Variability – C. Moretona. Backgroundb. Why excipient variability is important?c. How excipient variability can arise?d. Options for addressing excipient variability
II. March 19, 2014 (Webinar II: 2 part)
4) Excipients: The Unknown Unknown as Unforeseen Failure Mode – B. Carlina. Case Study 1 – The Unforeseen Failure Modeb. Case study 2 – Microcrystalline Cellulosec. (Un)Predictability of Excipient Performanced. Process Capabilitye. Application Criticalitiesf. Closing the Knowledge Gap

International Pharmaceutical Excipients Council Of The Americas
3138 N. 10th Street, Suite 500, Arlington, VA 22201 • Phone: (571) 814-3449 [email protected]
5) Issues with Variance in Measured Properties of Excipients – T. Cabelkaa. Characterization of Excipientsb. Why are we concerned with Variance?c. Real World Data for Methocel K100Md. Effects on Execution and Interpretation of Designed Experimentsa. Backgroundb. Why excipient variability is important?c. How excipient variability can arise?d. Options for addressing excipient variability
III. April 16, 2014 - (Webinar III: 2 part)
6. Excipient Composition and Performance-Related Properties of Excipients – C. Moreton a. How excipient performance arisesb. Excipient compositionc. Excipient formd. Excipient performance examples
7. QbD and Excipient Variability: A Perspective from a User Company – J. Kushnera. What are the challenges for the user?b. Understanding Excipient Variability
i. Case study 1 - using vendor CoA datasets to assess variabilityii. Case study 2 - experimental investigation of excipient variability and drug product
performancec. Managing Excipient Variabilityd. Some approaches to manage variability
i. Case Study 3 - using Advanced Process Control to manage excipient variabilitye. Regulatory interactions
IV. May 7, 2014 - (Webinar IV: 3 part)8. Misunderstandings of what types of Samples will be available for Experimentation – D. Schoneker
a. Excipient Selection Choicesb. Robustness of Formulationc. Sample Limitations
i. Mid, Min, and Max samples are typically not availabled. Excipient Realitiese. Opportunities
i. Concepts for QbD Sample sets
9. Integration of Excipients into the Design of Experiments for Pharmaceutical Product Development& Design Space Development – C. Moreton
a. Incorporating excipients into the DoEb. Single grade excipientsc. Multiple grade excipientsd. Examplese. Conclusions
10. Some Future Developments – B. Carlina. Variable pharmaceutical product batch sizeb. Continuous manufacture of finished pharmaceutical productsc. Formulation flexibility