Embed Size (px)
Citation preview

Inverclyde Telehealth

‘Telehealthcare is defined as: “the convergence of telecare and telehealth to provide a technology enabled and integrated approach to the delivery of effective, high quality health and care services’

The National Telecare Development Programme was introduced in 2006 with partnerships across Scotland being invited to participate in the introduction and development of the use of telecare equipment.In 2009 the Inverclyde Partnership agreed to identify people with Chronic Obstructive Pulmonary Disease who were at risk of readmission to hospital to pilot the use of specialist telehealth equipment.The objective being to assist them to manage and better understand their condition by monitoring and supporting these people in their own homes in order to achieve the following
To facilitate further mainstreaming of telecare at a local partnership level, within the policy contexts of shifting the balance of care and promotion of telehealth/telecare convergence promoting self management.In order to treat individuals with long term conditions more proactively, nearer home, and earlier in the course of their disease, NHS Greater Glasgow & Clyde (Inverclyde CHP) in partnership with Inverclyde Council, patients, carers and other relevant agencies has piloted a model for long term conditions that delivers care to match the level of need. A fundamental aspect of improving care delivery is the facilitation of multidisciplinary collaboration and effective information sharing.

The principal aim of the project was to improve the care of patients with Chronic Obstructive Pulmonary Disease (COPD) by early identification and treatment of exacerbations, facilitated by an alternative The principal aim of the project was to improve the care of patients with Chronic Obstructive Pulmonary Disease (COPD) by early identification and treatment of exacerbations, facilitated by an alternative pathway of care.

Project objectives
Evaluate the use of telehealth in the management of long term conditions (in this case, COPD.
Promote supported self care empowering patients to manage their own condition
Install and monitor Doc@Home Hubs (home hub) to provide early indicators of a COPD exacerbation.
Devise and implement an electronic COPD patient record to allow care managers and other
health care professionals to remotely track and record the relevant information across the integrated care pathway.
Develop the role of District Nurses to provide early interventions in the event of COPD exacerbations with the support of Respiratory Clinical Nurse Specialist

Recruitment The number of patients identified in Inverclyde with a
COPD diagnosis is 1095. Patients were recruited via their GP practices, which identified eligible patients for assessment using Scottish Patients at Risk of Readmission (SPARRA) data.
A cohortof 94 patients at risk of readmission was identified. Practices contacted patients to inform them of the pilot, and to invite expressions of interest in participating. Details of patients who were willing to be involved were passed to the RNS who arranged an initial home visit appointment (as detailed in the Standard Operating Procedure).

Baseline Assessment
Activities at the initial visit included: Taking of social, past medical, drug, smoking and exacerbation histories Observations made – respirations / blood pressure / pulse / pulse oximetry Taking of symptom history and breathlessness assessed using the MRC Dyspnoea
Scale Assessment of inhaler use and education on correct technique given, if necessary Provision of the Chronic Respiratory Disease Questionnaire for completion by the
patient, as far as possible independently. Knowledge gaps were assessed and education around self care was carried out to a
level appropriate for the patients needs before acceptance into the pilot. All patients received education on controlling their breathlessness at the initial
visit. British Lung Foundation (BLF) self management booklet was provided for every
patient and prescribed home medication packs were issued to all patients suitable for this level of self management. Home medication packs consisted either of Amoxicillin 500mg or Clarithromycin 500mg (7 days supply) and Prednisolone 30mgs (7 days supply) (NHS GG&C COPD guidelines)

doc@ HOME is a solution that enables clinicians to manage the care of patients with long term conditions in their own homes. The service can be easily tuned to the specific and changing needs of patients and their clinical support requirements. Information, collected each day, is available on the server and can be reviewed at any time, courses of treatment adjusted as necessary and messages and advice sent to patients using only a standard web browser. Each patient has a personal health envelope which is automatically tracked. Individual patient alert criteria can be defined and assessment questions customised by the clinician. A default ‘general question set’, based on the outcomes of clinical studies, is available as standard. Motivation feed back is provided to the patient and alert calls sent to nurse led support when key parameters go outside the envelope.

TECHNOLOGICAL INFRASTRUCTURE
The Inverclyde telehealth pilot has been run on a technological platform utilising both telephony and the internet.
Hardware and software has been supplied by Docobo. The home hub enables the patient to remotely input symptoms and signs of their COPD at regular intervals.
These are then uploaded to the secure server and archived. The daily data is downloaded via a secure internet connection to the Respiratory Nurse Specialist’s (RNS) computer.
The RNS reviews the data and using the assessment criteria decides if any intervention is required.
Data from all patients is then regularly transmitted back to the remote server and incorporated into a database which can then be interrogated.

Doc@homehealthhub

Overview of telehealth system



Pre Pilot Data
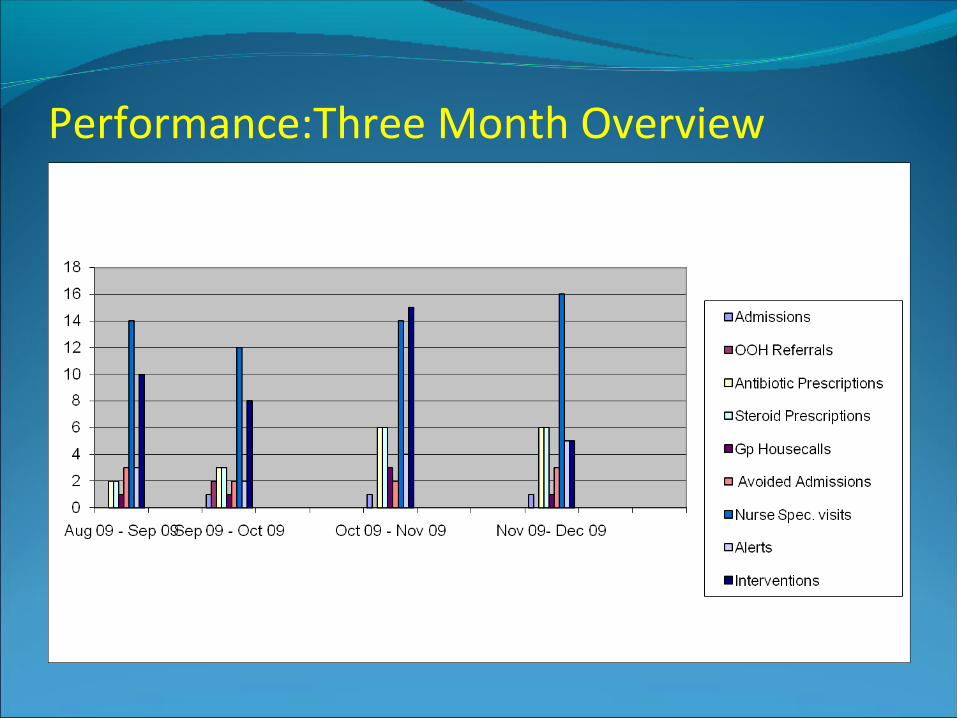
Performance:Three Month Overview

Performance

Performance

Performance

Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May-10 Jun-10 Jul-10|Aug-10 Total
Admissions 0 1 1 1 0 0 0 0 0 1 1 0 5
OOH Referrals 0 2 0 0 0 0 0 0 0 0 0 0 2
Antibiotic Prescriptions
2 3 6 6 2 3 2 4 3 2 6 7 46
Steroid Prescriptions
2 3 6 6 4 2 2 4 3 2 6 7 47
GP Housecalls 1 1 3 1 2 1 2 0 2 4 2 3 22
Spec Nurse visit 0 0 14 12 16 14 2 5 7 4 11 15 100
Avioded Admissions 3 2 2 3 3 2 0 0 1 0 1 2 19
Alerts 6 5 0 8 7 3 2 4 5 4 16 22 82
Interventions 18 15 0 9 9 9 2 2 5 2 12 18 101
Data Failure 1 2 0 0 1 0 0 0 1 3 0 0 8
Average Compliance 94% 93% 93% 94% 91% 95% 85% 93% 95% 95% 94% 94% 93%
Performance
After a period of stabilisation Patient A, was provided with a Homehub connected to telehealthsystem. In the period August 2009- August 2010, Patient A was successfully monitored at home. Timely interventions using telehealth monitoring, has seen Patient A’s admissions reduce to zero during the pilot period. Patient A states that he’s ‘never had such care’ until commencing on telehealth monitoring. ‘I feel that someone is really interested in keeping me out of hospital’

In terms of understanding and managing their condition, people commented that knowing that HPs are looking at the data “makes you feel more secure”; “someone else is looking at it, highlighting needs”.One said that it was helping them to manage their condition, “although it’s not very cheerful”. One person reported that they used to worry about what their BP was “and now I get the reading and know its okay”. Others commented that they are able to adjust their activities in the light of the readings, and one that they know how their body reacts to different things. One person said that it “lets me know how far I can go, I can push myself more”, and one that it “keeps me calm – I look at the readings and know I need to calm down. A reminder to calm down and relax”, and another that “I use the figures, and know not to worry when they are normal”. Whilst one person suggested that “I know better what I can expect of myself on any given day”, there were a coupe of people who felt that they had understood their condition well previously.

No-one reported anything unexpected happening during he early stages of the pilot, nor of concerns going unaddressed. One person’s final comment was” If I can use it anyone can - I'm intelligent but not technical, and this is easy. Another commented, I Feel closer to CM - he's wonderful, nothing's a bother”(thanks mum!, Myra, Clare , Alison ,Thelma et al)
Patients were asked if having the Hub has changed the way they use other parts of the service. All now said that they contact their GP less – one said they hadn’t been in touch that much before – and cited being able to contact CM as a reason. Some thought that having the Hub meant that they were generally less in contact with HPs.