Embed Size (px)
Citation preview

Introduzione: Come, Dove, QuandoIntroduzione: Come, Dove, Quando
La Terapia Occupazionale nell’Ictus
Francesco Landi Centro di Medicina dell’Invecchiamento Università Cattolica del Sacro Cuore, Roma
Guralnik JM, Simonsick EM. Physical disability in older Americans. J Gerontol. 1993;48:3-10.… functional disability has to be intended as the result of the interaction of different individual components of compromised functions: physical, emotional, and cognitive aspects usually interact to produce a comprehensive disability which is more than the simple addition of the single impairments, affecting the patient’s global function and his self-dependency …
Stucki G, Ewert T, Cieza A. Value and application of the ICF in rehabilitation medicine. Disability and Rehabilitation. 2003;25(11-12):628-34.... from a rehabilitation perspective, patients’ functioning and health are associated with, but not merely a consequence of, a condition or disease ...
DisabilitDisabilitàà FunzionaleFunzionale

ICFICF
World Health OrganizationWorld Health OrganizationClassification Assessment Surveys & Terminology GroupClassification Assessment Surveys & Terminology Group
as theas theNew Member in the New Member in the
WHO Family of WHO Family of International ClassificationsInternational Classifications
20012001

InterventionsInterventionsproceduresprocedures
Reasons forReasons forencounterencounter
ICDICD--1010International Statistical International Statistical
Classification of Classification of DiseasesDiseases & Related & Related
Health ProblemsHealth Problems
ICFICFInternational International
ClassificationClassification of of FunctioningFunctioning,, DisabilityDisability
and Healthand Health
INDINDNomenclature of Nomenclature of
DiseasesDiseases
SpecialitySpecialityadaptationsadaptations
Primary care Primary care adaptationsadaptations
WHO Family of WHO Family of International ClassificationsInternational Classifications
Associated ProductsAssociated Products Main ClassificationsMain Classifications AdaptationsAdaptations

Condizione di SaluteCondizione di Salute((trauma/malattiatrauma/malattia))
Fattori Fattori ambientaliambientali
Fattori Fattori personalipersonali
Funzione/Funzione/strutturastrutturadeldel corpo corpo
(Menomazione(Menomazione))
AttivitàAttività((DisabilitàDisabilità))
ParticipazioneParticipazione(Handicap)(Handicap)
RIABILITAZIONE(Fisioterapia, Terapie
riabilitative specialistiche)
TERAPIA OCCUPAZIONALE
L’intervento riabilitativo in ambito geriatrico deve essere organizzato sulla base di un modello concettuale di disabilità

ComorbiditàPoliterapiaStato funzionale
Stato cognitivoFunzione fisicaTono dell’UmoreStato sociale
Sd. geriatriche (incontinenza/cadute)
Modificazioni metabolismoModificazioni omeostasiAnemia/Osteoporosi/Sarcopenia
FRA
GIL
ITA
’FR
AG
ILIT
A’
I I -- Perché la riabilitazione in Perché la riabilitazione in geriatria è differente ?geriatria è differente ?

II II -- Quando iniziare ?Quando iniziare ?riab. “classica” ↔ riab. “geriatrica”
diagnosi diagnosi↓ +
trattamento trattamento↓ +
riabilitazione riabilitazione⇓ ⇓
in successione simultanea

III. Obiettivi differentiIII. Obiettivi differenti• giovane (PT): restitutio ad integrum• anziano (OT): restitutio ADL - IADL
Per questo tipo di malati il vero grande risultato è il Per questo tipo di malati il vero grande risultato è il “piccolo guadagno”: averlo capito è stata una conquista “piccolo guadagno”: averlo capito è stata una conquista almeno pari a quella del trapianto cardiaco.almeno pari a quella del trapianto cardiaco.
Kane RL. Looking for physical therapy outcomes. Phys Ther 1994;74:425-9
“piccolo guadagno”

LALA SCELTA IN FUNZIONE DELL’OBIETTIVOSCELTA IN FUNZIONE DELL’OBIETTIVO
CD Multimediale PU Carbonin
IV. Valutazione risultatiIV. Valutazione risultati• fattori prognostici• outcomes• comparazioni
…… the the heterogeneity of functional and health problemsheterogeneity of functional and health problems experienced by elderly patients experienced by elderly patients makes it difficult to evaluate multiple outcomes of rehabilitatimakes it difficult to evaluate multiple outcomes of rehabilitation. Valid on. Valid negative negative predictorspredictors of functional recovery after acute events include of functional recovery after acute events include ageage, , urinary incontinence, urinary incontinence, cognitive impairmentcognitive impairment, , deliriumdelirium, , functional deficits present at admissionfunctional deficits present at admission, and, and level of level of social supportsocial support. . Other factorsOther factors, however, make it difficult to draw definitive conclusions , however, make it difficult to draw definitive conclusions about the about the efficacy and costefficacy and cost--effectiveness of rehabilitative programseffectiveness of rehabilitative programs. These include the . These include the characteristics of the studied populationcharacteristics of the studied population and of the and of the rehabilitation settingrehabilitation setting, the , the types of types of assessmentsassessments and/or and/or interventionsinterventions, and the , and the use of varying outcome measuresuse of varying outcome measures … … … … given the potential conflict between the increasing demand for rgiven the potential conflict between the increasing demand for rehabilitative ehabilitative programs and the development of health care services that limit programs and the development of health care services that limit the availability of the availability of rehabilitation beds, rehabilitation beds, identification of elderly patients who could potentially gain identification of elderly patients who could potentially gain improved function from such services is imperativeimproved function from such services is imperative …… Stroke. 2003;34:676-687

V. Strategie di interventoV. Strategie di intervento• fisioterapia• terapia occupazionale

Occupational therapy versus no Occupational therapy versus no routine input Outcome: ADLroutine input Outcome: ADL

Occupational therapy versus no Occupational therapy versus no routine input Outcome: IADLroutine input Outcome: IADL


PT activities: exercises and balance in standing and lying OT activities: sensory, perceptual training, cognition and
domestic activities. These findings reflect an implicit task division. Physiotherapists focus on mobility activities Occupational therapists on ADL and domestic trainingThe occurrence of selective movements, mobilization, and exercises and balance in sitting was similar in PT and OT. These activities are probably an essential preparation to a “higher level” profession-specific activity, such as ambulatory exercises and domestic activities. These findings also indicate the existence of role overlap between PT and OT.

The need for preventive and rehabilitative programs is steadily increasing with the growing proportion of the elderly in the population and the associated high rate of comorbidity and disability. Modern thought holds that the philosophy of rehabilitation should be the heart and primary aim of geriatrics.
… the emerging lack of resources for health care services in industrialized nations and the increasingly limited availabilityof rehabilitation services point to a critical need for evidencebased criteria that would determine which patients stand to benefit the most (recovery/stabilization) from specific rehabilitative programs. Further investigations are needed to define which parameters can predict the rehabilitative potential of various types of therapy that focus on physical, psychological, and social approaches, and whether the potential recovery of stroke subjects is influenced by different techniques - OT program


Landi F et al. Am J Phys Med Rehabil, 1997;76:38-42

Rehabilitation Program (PT + OT therapy)Rehabilitation Program (PT + OT therapy)
Landi F et al. Am J Phys Med Rehabil, 1997;76:38-42

Landi F et al. Am J Phys Med Rehabil, 1997;76:38-42
I n t e r v e n t o(n = 6 7 )
C o n t r o l lo( n = 3 6 )
p
E t à 8 1 .7 ± 7 .8 8 0 .4 ± 8 .3 n .s .
S e s s o ( F ) 4 4 ( 6 5 .6 ) 2 1 ( 5 8 .3 ) n .s .
M M S E 2 1 .9 ± 6 .1 2 0 .9 ± 7 .2 n .s .
G D S 1 4 .4 ± 8 .4 1 5 .8 ± 7 .2 n .s .
A D L i n d i p e n d e n t i d i p e n d e n t i 1 - 3 d i p e n d e n t i 4 +
2 ( 2 .9 )4 0 ( 5 9 .7 )2 5 ( 3 7 .4 )
1 ( 2 .7 )2 0 ( 5 5 .7 )1 5 ( 4 1 .6 )
n .s .
Descriptive analysis of baseline demographic and Descriptive analysis of baseline demographic and functional parameters according to interventionfunctional parameters according to intervention
0
20
40
60
80
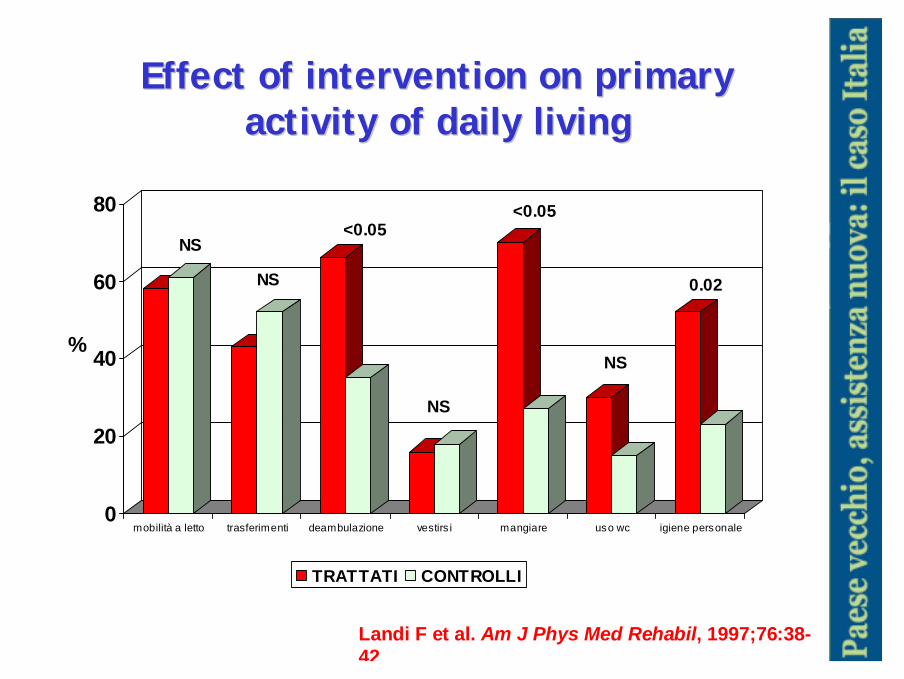
mobilità a letto trasferimenti deambulazione vestirs i mangiare uso wc igiene personale
TRATTATI CONTROLLI
NS
NS
<0.05
NS
<0.05
NS
0.02
%
Effect of intervention on primary Effect of intervention on primary activity of daily livingactivity of daily living
Landi F et al. Am J Phys Med Rehabil, 1997;76:38-42
EuropeanEuropeanJournal of Journal of NeurologyNeurology
2006, 13: 172006, 13: 17––2323
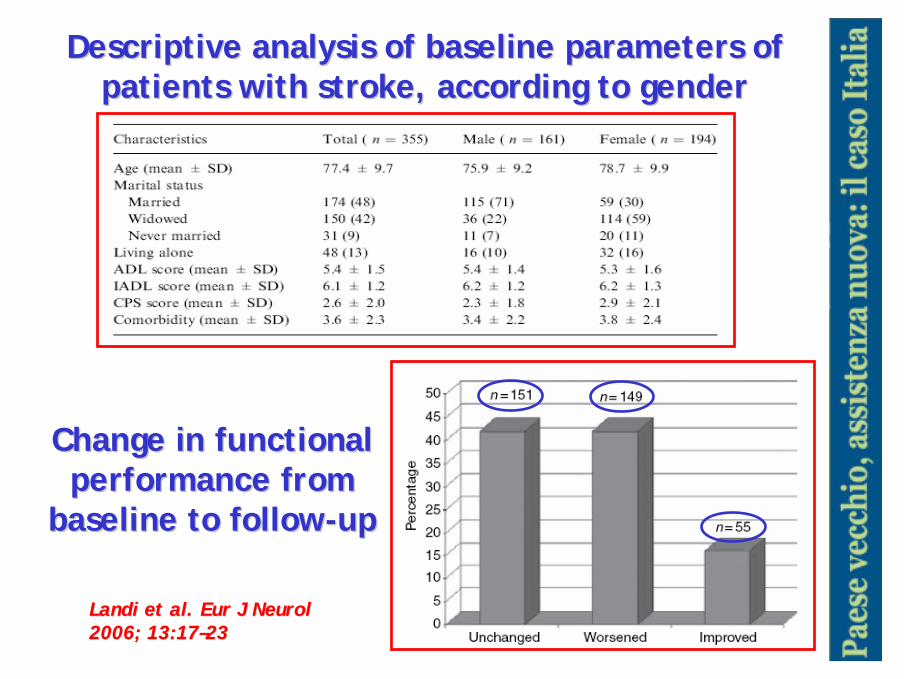
Descriptive analysis of baseline parameters of Descriptive analysis of baseline parameters of patients with stroke, according to genderpatients with stroke, according to gender
Change in functional Change in functional performance from performance from
baseline to followbaseline to follow--upup
LandiLandi etet al.al. EurEur J J NeurolNeurol2006; 13:172006; 13:17––2323

Predictors of functional declinePredictors of functional decline
Impedire la Impedire la comparsa di una comparsa di una ulcera da pressione ulcera da pressione è un problema di è un problema di tutti i giorni del tutti i giorni del geriatra; ma è geriatra; ma è anche un esempio anche un esempio utile per capire il utile per capire il vero significato del vero significato del “piccolo guadagno”“piccolo guadagno”in funzione della in funzione della qualità della vita. qualità della vita.
LandiLandi etet al.al. EurEur J J NeurolNeurol2006; 13:172006; 13:17––2323

2002;50:679-684
North AmericaCanada
US
Nordic CountriesIceland, Norway, Sweden, Denmark, Finland
EuropeNetherlands, Germany,
Switzerland,France, UK
Italy, Spain,
Czech Republic
AustralasiaJapan, South Korea, Taiwan, Hong Kong
Australia, New Zealand
Middle EastIsrael
interinterRAIRAI –– MDSMDS--PACPAC

Descriptive analysis of baseline socioDescriptive analysis of baseline socio--demographic, functional and clinical parameters demographic, functional and clinical parameters
according to ageaccording to age
LandiLandi etet al.al. JAGS 2002;50:679JAGS 2002;50:679--684684

LandiLandi etet al.al. JAGS 2002;50:679JAGS 2002;50:679--684684
Predictors of functional Predictors of functional recoveryrecovery

J Am Med Dir Assoc J Am Med Dir Assoc 2007;8:2332007;8:233––242242

J Am Med Dir Assoc 2007;8:233J Am Med Dir Assoc 2007;8:233––242242
Structure of health staff of participating PAC Structure of health staff of participating PAC Departments, in terms of average number of staff Departments, in terms of average number of staff
and beds (Staff Burden) in Israel and Italyand beds (Staff Burden) in Israel and Italy

J Am Med Dir Assoc 2007;8:233J Am Med Dir Assoc 2007;8:233––242242
Multiple Logistic Regression of Predictors of Multiple Logistic Regression of Predictors of Functional Recovery (1 Point in ADL) in Israel and Functional Recovery (1 Point in ADL) in Israel and
Italy (Israel, n=364; Italy, n=351)Italy (Israel, n=364; Italy, n=351)


Clinical and functional characteristics of subjects Clinical and functional characteristics of subjects in the intervention and control groupsin the intervention and control groups

Effect of occupational therapy on Effect of occupational therapy on primary activity of daily livingprimary activity of daily living
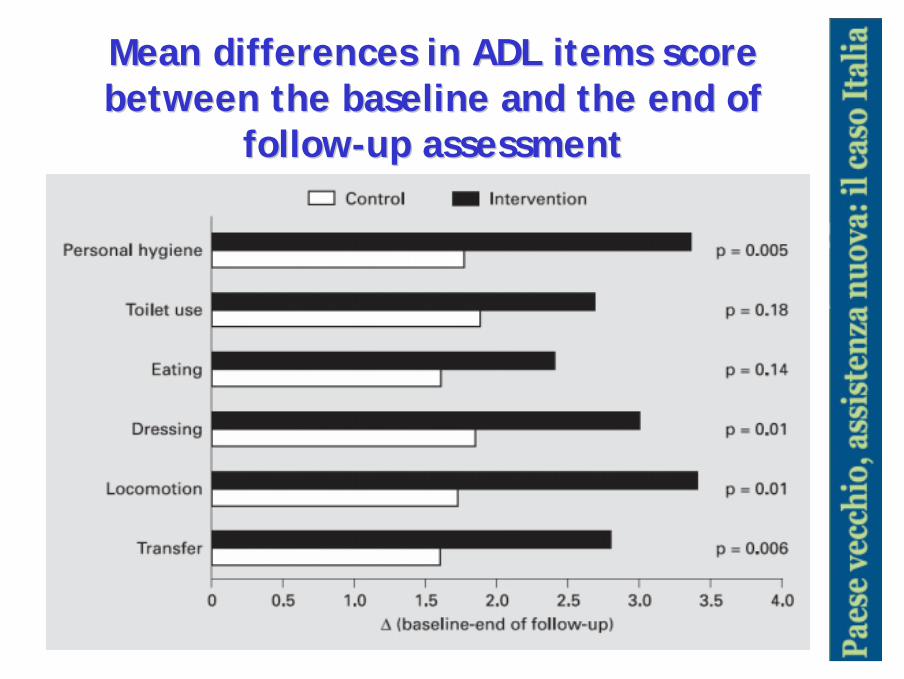
Mean differences in ADL items score Mean differences in ADL items score between the baseline and the end of between the baseline and the end of
followfollow--up assessmentup assessment

(...) "the defining feature of geriatric medicine is not age, but rather the intense focus on the preservation and restoration of function. Because optimizing function is central to persons of all age groups who are afflicted with chronic disease or disability, many of the fundamental principles and practices of geriatric medicine are broadly applicable across disciplines and subspecialty areas. The underlying premise of this commentary is that geriatric medicinerepresents more than caring for old people; it is a mind-set, a way of thinking that can be incorporated into clinical practice to improve the health and well-being of patients with chronic disease or disability across the continuum of age." (...) "The overall goal of chronic care is not to cure, but rather to help persons with chronic conditions maintain independence and a high level of functioning. Geriatricians bring special expertise to the management of patients with chronic conditions across multiple sites of care. (...) Gill TM, Am J Med 2002;113:85-90


Nell'affrontare i problemi del malato anziano fragile si può essere all'inizio colti da un senso di impotenza. Avendo presenti i successi ottenuti dalla medicina in tutti gli altri campi, può venir da pensare: “Tanto è vecchio, non vi è nulla da fare!“
Rendere indipendente un soggetto emiplegico nella propria casa, evitandone l’istituzionalizzazione o impedire le piaghe da decubito in un anziano allettato sono i problemi di tutti i giorni del geriatra; ma sono anche esempi utili per capire il vero significato del “piccolo guadagno” in funzione della qualità della vita. Se tutto ciò non è servito a convincere il lettore, è bene che egli non diventi mai un geriatra!
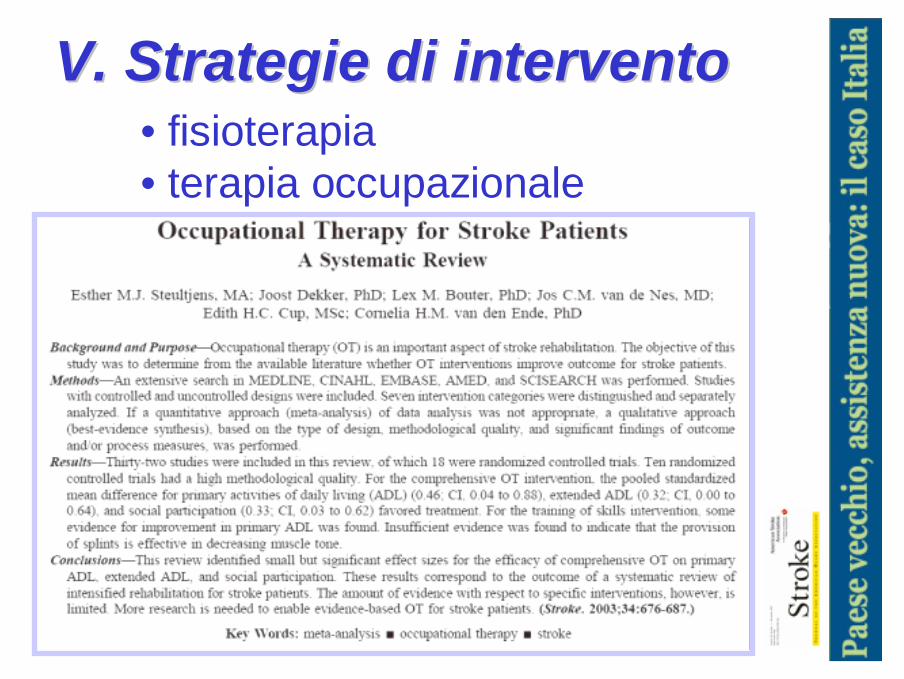
V. Strategie di interventoV. Strategie di intervento• fisioterapia• terapia occupazionale



Participation Participation oror Handicap?Handicap?

7%7%
10%10%
LandiLandi F, F, EurEur J J PhysPhys MedMed RehabilRehabil, 1996, 1996
0
600
1200
1800
2400
3000
Fisioterapia Terapia Occupazionale
TUTTI GERIATRIA
Letteratura riabilitazione Letteratura riabilitazione geriatricageriatrica anni anni
19901990--19961996

Letteratura riabilitazione Letteratura riabilitazione geriatricageriatricaanni 1997anni 1997--20072007
(Landi F, Personal data)(Landi F, Personal data)
0600
120018002400300036004200480054006000
Fisioterapia Terapia Occupazionale
TUTTI GERIATRIA
44%44%
32%32%