-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
1/84
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
2/84
Marc Imhotep Cray, M.D.
The Electrocardiogram
Discussion Outline Propagation of Electrical Activity Through
the
Heart
The Cardiac Action Potential
Generation of the Cardiac Pacemaker
The Electrocardiogram
Cardiac Vectors
Section I
http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
3/84
Marc Imhotep Cray, M.D.
Electrical Conductivity in the Heart
3
Within the atria and ventriclesmyocardial cells are connected
bygap junctions
Gap junctions allow the cardiacaction potential to propagate
fromcell to cell through a lowresistance pathway
Thus, along with its
intercalated discarchitecture, cardiac muscleis able to contract
as asyncytial unit
The syncytial interconnecting
nature of cardiac muscle
http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
4/84
Marc Imhotep Cray, M.D.
Electrical Conductivity in the Heart (2)
Electrical activity can pass from cell to cell in atria and
ventricles
The atria and ventricles are electrically isolated by the
heartsfibrous skeleton theAnnulus fibrosus
The heart has specialized electrically active cells (conductive
tissue)in addition to contractile tissue
CONDUCTIVE TISSUE
These cells form the Sinoatrial (SA) node, Atrioventricular
(AV)node, Bundle of His and Purkinje Fibres
Electrical activity normally originates in the SA node
The AV node forms the only site of electrical connection
betweenthe atria and ventricles
4
http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
5/84
Marc Imhotep Cray, M.D.
Specialized Conductive Tissue in the Heart
5
See IVMS notes: N-Cardiac Myocyte & Conductive System
Chemical-Electrical Events with Clinical
Considerations.pdf
Click graphic for expandable view
https://drive.google.com/file/d/0B-tlCbPSHvfZNWJWcE1FY20waXc/edit?usp=sharinghttps://drive.google.com/file/d/0B-tlCbPSHvfZNWJWcE1FY20waXc/edit?usp=sharinghttps://docs.google.com/a/imhotepvirtualmedsch.com/file/d/0B-tlCbPSHvfZV1dZUDIyeHFkdTg/edithttp://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
6/84
Marc Imhotep Cray, M.D.
Autorhythmicity
Some heart cells (SA, AV node and Purkinje) show
automaticity, the ability to generate a heart beat
These cells have an intrinsic rhythmicity which generates a
pacemaker potential
The heart does not require nerve or hormonal input to
beat
The heart transplant patients the nerves are severed but
the heart beats on
6
http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
7/84Marc Imhotep Cray, M.D.
Propagation of the Cardiac Action Potential
7
Action potential (AP) starts at SA node.
AP conducted through atrial muscle,
interatrial band and internodal
pathways
The AP is delayed at the AV node
before entering the Bundle of His
Conduction through the Bundle of His
and Purkinje fibres is extremely rapid
The ventricles depolarise from endo to
epicardium and from apex to baseTransmission of cardiac impulse
through heart showing
time of appearance (in fractions of a second) of impulse in
different parts of heart
http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
8/84Marc Imhotep Cray, M.D.
The Cardiac Action Potential
8
The cardiac action potential has several distinct phases
The cardiac action potential is different in the ventricles,
atria
and conductive tissue
Cells in the specialised electoral pathways of the heart
are spontaneously active and show automaticity
These cells do not have a true resting membrane potential
http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
9/84Marc Imhotep Cray, M.D.
Cardiac versusSkeletal Muscle AP
9
http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
10/84Marc Imhotep Cray, M.D.
The Phases of
the Ventricular AP
10
The rapid depolarization is due to theopening of voltage gated
Na+channels
Inactivation of the Na+channels and
opening of slow Ca2+channels produces
the plateau
During the cardiac AP K+conductance
falls
Repolarization occurs by a return of the
Ca2+and K+permeability to resting
values
http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
11/84Marc Imhotep Cray, M.D.
Mechanism of the Pacemaker Potential
11
The rapid depolarization phase of the AP
in cardiac pacemaker cells is due to
opening of slow Ca2+channels
Repolarization after the AP is due toopening of K+channels
Spontaneous depolarization is produced
by a progressive fall in the K+permeability
combined with an inward current if(the
nature of ifis still under investigation)
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
12/84Marc Imhotep Cray, M.D.
Cardiac Pacemakers
The sinoatrial has the fastest pacemaker potential (~90-100
beats/min) and is the normal pacemaker
The atrioventricular node is the next fastest (~40-60
beats/min) followed by cells in the bundle of His (15-30).
The fastest pacemaker normally drives the heart and
suppresses other pacemakers (overdrive suppression).
A beat generated outside the normal pacemaker is an
ectopicbeat.
The site that generates an ectopic beat is known as an
ectopic focus(foci pl.) or ectopic pacemaker.
12
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
13/84Marc Imhotep Cray, M.D.
Physiology:
Neural Control of Heart Rate (1)
13
Norepinephrine (NE) from sympathetic nerves and circulating
adrenaline,
increase the heart rate and enhances conduction of the AP
Acetylcholine (ACh) released from parasympathetic nerves reduces
the
heart rate and conduction across the AV node
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
14/84Marc Imhotep Cray, M.D.
Physiology:
Neural Control of Heart Rate (2)
Agents that alter heart rate are chronotropic
Positive chronotropic agents increase heart rate
Epinephrine and Ne act onb-adrenergic receptors on heart
Isoproterenol is b-adrenergic agonist which increases heart rate
Propranolol is a b-adrenergic antagonist that blocks the actions
of
adrenaline, NA and Isoproterenol
Adrenergic stimulation increases the Na+and Ca2+permeability
of
cardiac cells, hypopolarizing them and increasing the
pacemakerpotential rise
At rest heart is under weak sympathetic tone
Predominate tone at rest is parasympathetic
14
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
15/84Marc Imhotep Cray, M.D.
Pharmacology:
Neural Control of Heart Rate (3)
Agents with negative chronotropic actions slow the heart
Acetylcholine acts on M-cholinergic (muscarinic) receptors
on
the heart
Methacholine, carbachol (carbamylcholine) and muscarine are
pharmacological stimulants of muscarinic receptors Atropine is a
muscarinic antagonist that blocks actions of ACh
and other muscarinic receptor agonists
ACh increases K+permeability of cardiac cell hyperpolarizing
them and reducing the rise in the pacemaker potential
AGAIN: At rest the heart is under parasympathetic tone which
slows the natural rhythm of the heart
15
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
16/84Marc Imhotep Cray, M.D.
Pharmacology:
Resting Autonomic Control of Heart Rate
16
At rest heart rate is under
both sympathetic and
parasympathetic tone
Normally the
parasympathetic inhibition
of rate is larger than the
sympathetic stimulation
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
17/84Marc Imhotep Cray, M.D.
Pharmacology (2)Some Other Agents
Nifedipine and Verapamil are calcium channel blocking agentsthat
reduce heart rate
Increased extracellular K+(hyperkalemia): hyperpolarizes
cardiac
myocytes, shortens the AP and slows the heart
Arrhythmia or heart block is often produced with fibrillation
athigher level
Only a 5-10mM rise in extracellular K+can cause death
Excessive extracellular Ca2+
(hypercalcemia) can produce spasticcontractions of the heart
Reduced Ca2+(hypocalcemia) concentrations inhibit heart
contraction and can trigger ectopic foci
17
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
18/84Marc Imhotep Cray, M.D.
The Electrocardiogram
(EKG/ECG)
18
P wave is due to atrialdepolarization
The QRS complex is due to
ventricular depolarization
T wave is Ventricular
repolarization
U wave is often seen in
hypokalemiaAn atrial T wave is occasionally
seen in complete heart block
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
19/84Marc Imhotep Cray, M.D.
Extracellular Action Potential
19
Recording the depolarization
wave and the repolarization wave
from a cardiac muscle fiber
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
20/84Marc Imhotep Cray, M.D.
EKG Intervals
20
P-R interval: delay between atrial
and ventricular depolarization
QRS: time for ventricular
depolarization
Q-T: Duration of electrical systole
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
21/84Marc Imhotep Cray, M.D.
Normal EKG Intervals
P-R interval is normally 0.12-0.20 sec, most of this time is
delay atthe AV node
An increased P-R interval (>0.28 sec) is characteristic of
1stdegree
heart block
QRS complex normally lasts less than 0.10 sec.
Increased width of the complex is a characteristic of defects
in
the branch bundles or Purkinje fibres i.e. branch bundle
block
Q-T interval varies inversely with heart rate21
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
22/84Marc Imhotep Cray, M.D.
The Cardiac Vector
22
The heart is a three dimensionalobject so the mean axis of
polarity in the heart exists as a
vector
A vector has both an orientationand a magnitude
Both the direction and
magnitude of the cardiac vector
change during the heart beat
A mean vector through the
partially depolarized heart
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
23/84
Marc Imhotep Cray, M.D.
The Cardiac Vector (2)
23
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
24/84
Marc Imhotep Cray, M.D.
EKG Limb Leads
24
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
25/84
Marc Imhotep Cray, M.D.
25
Dependence of speed of depolarization on resting potential
ANormal resting potential (RP) and normal rapid -50 rise of
phase 0
depolarization.B Less negative RP results in slower rise of
phase O, and lower
maximal amplitude of the action potential.
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
26/84
Marc Imhotep Cray, M.D.
Normal EKG recorded on the
Bipolar Limb Leads
26
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
27/84
Marc Imhotep Cray, M.D.
Uses of the EKG
Heart Rate
Conduction in the heart
Arrhythmias
Direction of the cardiac vector Damage to the heart muscle
Provides NO (direct) information about pumping
or mechanical events in the heart
27
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
28/84
Marc Imhotep Cray, M.D.
EKG Interpretation
Section II
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
29/84
Marc Imhotep Cray, M.D.
The Basics
PQRST
Rate
Rhythm
Axis
Intervals
Ischemia
29
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
30/84
Marc Imhotep Cray, M.D.
PQRST waves
30
Name the waves
P T
Q
R
Name the intervals
PR QT
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
31/84
Marc Imhotep Cray, M.D.
PQRST waves
31
Name the waves
Name the intervals
P
TS
R
PR QT
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
32/84
Marc Imhotep Cray, M.D.
RateThe Paper
32
Measure the rate by the distance between QRS complexes
300
150
100
75
60
Or look at the right upper corner for the rate
or look at the monitor for the rate
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
33/84
Marc Imhotep Cray, M.D.
RateThe Paper
33
What are the time intervals between lines?
0.2 sec
200 msec
0.04 sec
40 msec
Normal paper speed is 25 mm/sec
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
34/84
Marc Imhotep Cray, M.D.
Rhythm Questions
Is this sinus rhythm?
Are there P waves present?
If notAtrial fibrillation
Is this sinus rhythm?
P before every QRS PR interval the same for every beat
PR less than 0.2 sec (one big box)
Not sinus rhythm
AV block Tachydysrhythmia
Bradydysrhythmia
34
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
35/84
Marc Imhotep Cray, M.D.
Is this sinus rhythm?
1. P in front of every QRS?
2. PR interval > 0.12 and < 0.20 sec?
3. P upright in I, II, and III?
Yes to all 3 indicates sinus rhythm
35
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
36/84
Marc Imhotep Cray, M.D.
The AV Blocks
1stDegree AVB
PR interval fixed
PR interval > 200 msec
36
Note: A TRACINGS INTERPRATION REVIEW AND QUIZ IS PROVIDED IN THE
LAST
(HIGH- YIELD ) SECTION OF THIS PRESENTATION
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
37/84
Marc Imhotep Cray, M.D.
The AV Blocks
Type 1 Second Degree Block
Wenkebach
Watch for grouped beating
PR lengthens
RR shortens
Dropped beat
37
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
38/84
Marc Imhotep Cray, M.D.
The AV Blocks
Type 2 Second Degree Block
PR interval fixed
P without QRS
Dropped beat often in a fixed ratio
38
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
39/84
Marc Imhotep Cray, M.D.
The AV Blocks
Third Degree Block AV dissociation
Escape beat
AV nodalrate normal Narrow complex
Junctionalrate 40-60s
Narrow complex
Ventricularrate 30-40s Wide complex, bizarre shape
39
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
40/84
Marc Imhotep Cray, M.D.
Fill in the table with the correct
rhythms (Ans. next slide)
Narrow Wide
Regular
Irregular
40
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
41/84
Marc Imhotep Cray, M.D.
Filled in the Table
41
Narrow Wide
Regular
Sinus rhythmSupraventricular tachy (SVT)
Re-entrant tachycardia
(WPW)
Ventriculartachycardia
SVT with BBB
SVT with aberrancy
Irregular
Atrial fibrillation (AF)Multifocal Atrial Tachy (MAT)
AF with BBBAF with aberrancy
Torsade du Pointes
The Normal Axis
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
42/84
Marc Imhotep Cray, M.D.
42
The Normal Axis
-30to 90
-30
90
Note: You will not be able to appreciate the full learning
impact of the following slides unless youhave the PowerPoint, as I
am sequencing activity moving forward via slide transition
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
43/84
Marc Imhotep Cray, M.D.
The AxisLead I
43
0
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
44/84
Marc Imhotep Cray, M.D.
44
The AxisLead II
60
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
45/84
Marc Imhotep Cray, M.D.
45
The AxisLead III
120
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
46/84
Marc Imhotep Cray, M.D.
46
The AxisLead aVF
90
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
47/84
Marc Imhotep Cray, M.D.
47
The AxisLead aVL
-30
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
48/84
Marc Imhotep Cray, M.D.48
The AxisLead aVR
-150
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
49/84
Marc Imhotep Cray, M.D.49
0I
60II120III
90aVF
-30aVL-150aVR
The Axis
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
50/84
Marc Imhotep Cray, M.D.
How to find the axis
Find the most isoelectric limb lead (R=S)
The mean axis is perpendicular to this lead
If the QRS is positive then the axis is in that direction
If the QRS is negative then the axis is away from thatlead
50
A i P i Wh i h i ?
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
51/84
Marc Imhotep Cray, M.D.
Axis PracticeWhat is the axis?
51
Most isoelectric lead? Lead aVF
Positive or negative? Positive
aVF is 90 The axis is perpendicular to this and is 0
A i P i Wh i h i ?
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
52/84
Marc Imhotep Cray, M.D.52
Axis PracticeWhat is the axis?
Most isoelectric lead?
Positive or negative?
and is -30
Lead II
Positive
II is +60 The axis is perpendicular to this
A i P i Wh i h i ?
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
53/84
Marc Imhotep Cray, M.D.53
Axis PracticeWhat is the axis?
Positive or negative?
Lead aVR
Negative
aVR is -150 The axis is perpendicular to this
Most isoelectric lead?
and is -60
SUMMARY SHEET
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
54/84
Marc Imhotep Cray, M.D.54
SUMMARY SHEET
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
55/84
Marc Imhotep Cray, M.D.
Intervals
55
PR interval
Normal range0.12 to 0.20 sec
QT interval
Normal range
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
56/84
Marc Imhotep Cray, M.D.
QT interval
The normal QT interval will
vary with heart rate and acorrected score is the most
accurate measure.
56
QTc = QT preceding RR interval
RR interval
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
57/84
Marc Imhotep Cray, M.D.
Bundle Branch Blocks
Left (LBBB)
Right (RBBB)
Left Anterior Fascicular Block (LAFB)
Left Posterior Fascicular Block (LPFB)
57
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
58/84
Marc Imhotep Cray, M.D.
Wide QRS = Bundle Branch Block
RBBB Rabbit ears in V1
Tall R in V6 with slurred S
Normal or right axis (90 to 110)
LBBB
V1small R and deep, wide S
V6Tall, wide, slurred R Normal or left axis (-30 to -90)
58
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
59/84
Marc Imhotep Cray, M.D.
Fascicular Blocks
LAFB Left axis (-30 to -90)
I and aVL = small Q
II, III, aVF = small R and deep S
q1r3
LPFB
Right axis (110 to 180)
I, aVL, V5-6 = no Q, small R, deep S
II, III, aVF = small Q, tall R
q3r1
59
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
60/84
Marc Imhotep Cray, M.D.
Ischemia or Infarction
ST segment = depression Infarction
ST segment = elevation Ischemia
60
Wh d EKG h f th
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
61/84
Marc Imhotep Cray, M.D.
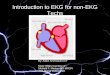
Where do you see EKG changes for the
following areas of ischemia? (1)
Anterior
Septal
Anteroseptal
Inferior
Lateral
PosteriorRight ventricular
61
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
62/84
Marc Imhotep Cray, M.D.
Anterior Ischemia
ST segment elevation
V3 and V4
Reciprocal changes (ST depression)
II, III, AVF
62
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
63/84
Marc Imhotep Cray, M.D.
Septal Ischemia
ST segment elevation
V1 and V2
63
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
64/84
Marc Imhotep Cray, M.D.
Anteroseptal
ST segment elevation
V1 through V4
Reciprocal changes (ST depression)
II, III, AVF
64
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
65/84
Marc Imhotep Cray, M.D.
Inferior Ischemia
ST segment elevation
II, III, aVF
Reciprocal changes (ST depression)
V1 through V4
65
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
66/84
Marc Imhotep Cray, M.D.
Lateral Ischemia
ST segment elevation
I, aVL, V5 and V6
Often associated with anterior ischemia
Reciprocal changes (ST depression)
II, III, AVF
66
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
67/84
Marc Imhotep Cray, M.D.
Posterior Ischemia
Easy to miss!
Tall R wave in V1 and V2
ST segment depression in V1 through V4
If you hold the EKG up to a bright light and
turn it over you will see the classic ST
elevation.
67
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
68/84
Marc Imhotep Cray, M.D.
Right Ventricular
ST segment elevation II, III, aVF
Tall R
II, III, aVF
Reciprocal changes (ST depression)
I and aVL
Check right sided leads
Expect hypotension with nitroglycerine or morphine
68
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
69/84
Marc Imhotep Cray, M.D.
Which coronary artery?
69
Where do you see EKG changes for
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
70/84
Marc Imhotep Cray, M.D.
y g
the following areas of ischemia? (2)
70
The idea is that you should be able to look at an EKG pattern of
ischemia or
infarction and know the coronary lesion location that will show
at cardiac cath.
Of course this means you must memorize the previous slides
information
The next slide provides more details related to this graphic
Source: Tao Le T and Bhushan V,
Cardiovascular, In First Aid for the USMLE
Step 1 The McGraw-Hill 2013; 2013:253
Where do you see EKG changes for the
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
71/84
Marc Imhotep Cray, M.D.
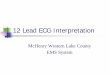
Where do you see EKG changes for the
following areas of ischemia? (3)
71
SA and AV nodes a re usually supplied by RCA
Right-dominant circulation = 8 5 %= PD arises from RCA
Left-dominant circulation = 8 % = PD arises fro m LCX.
Codominant circulation = 7% = PD arises from both LCX and
RCA.
Coronary artery occlusion most commonly occurs in the
LADCoronary arteries fill during diastole
The most posterior part of the heart is the left atrium ;
enlargement can cause dysphagia
(due to compression of the esophagus) or hoarseness (clue to
compression of the left
recurrent laryngeal nerve, a branch of the vagusTransesophageal
echocardiography is useful for diagnosing left atrial enlargement,
aortic
dissection , and thoracic aortic aneurysm
Modified after Tao Le T and Bhushan V, Cardiovascular, In First
Aid for the
USMLE Step 1, The McGraw-Hill 2013; 2013:253
Section III
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
72/84
Marc Imhotep Cray, M.D.72
High Yield Summary Data,
ECG Tracings andGreat External Resources
For more on slides 73-81 see:
Tao Le T and Bhushan V, Cardiovascular, In First Aid for the
USMLE Step 1, The McGraw-Hill 2013; 2013:260-65
Further study resources at the end of this presentation
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
73/84
Marc Imhotep Cray, M.D.73
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
74/84
Marc Imhotep Cray, M.D.74
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
75/84
Marc Imhotep Cray, M.D.75
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
76/84
Marc Imhotep Cray, M.D.76
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
77/84
Marc Imhotep Cray, M.D.77
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
78/84
Marc Imhotep Cray, M.D.78
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
79/84
Marc Imhotep Cray, M.D.79
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
80/84
Marc Imhotep Cray, M.D.80
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
81/84
Marc Imhotep Cray, M.D.81
For more on slides 73-81 see:
Tao Le T and Bhushan V, Cardiovascular, In First Aid for the
USMLE Step 1, The McGraw-
Hill 2013; 2013:260-65
Further study resources at the end of this presentation
MAKE THE DIAGNOSIS
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
82/84
Marc Imhotep Cray, M.D.
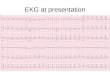
MAKE THE DIAGNOSISYou should go back to determine the answers if
you are not sure.
Or *click here to view the source graphic which includes
interpretations and explanations.
82
* ONCE YOU LAND DOUBLE TO EXPAND, HOLD LEFT MOUSE AND DRAG TO
NAVIGATE
MAKE THE DIAGNOSIS (2)
https://drive.google.com/file/d/0B-tlCbPSHvfZZDVKazA4R2RmQ2s/edit?usp=sharinghttps://drive.google.com/file/d/0B-tlCbPSHvfZZDVKazA4R2RmQ2s/edit?usp=sharinghttp://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
83/84
Marc Imhotep Cray, M.D.
MAKE THE DIAGNOSIS (2)
83
THE END THANK YOU FOR YOUR ATTENTION
http://www.imhotepvirtualmedsch.com/http://www.imhotepvirtualmedsch.com/
-
8/13/2019 Introduction to Review of | EKG Interpretation w
Physiology and Pharmacology of Cardiac Conductivity
84/84
THE END, THANK YOU FOR YOUR ATTENTION
Electrocardiogram, EKG, or ECGExplanation of what an ECG is, who
needs one, what to
expect during one, etc. Written by the National Heart Lung and
Blood Institute (a division of
the NIH)
University of Maryland School of Medicine Emergency Medicine
Interest GroupIntroduction to EKG's as written by a medical student
and a cardiologist
ECGpedia: Course for interpretation of ECG
12-lead ECG library
Simulation tool to demonstrate and study the relation between
the electric activity of the
heart and the ECG
EKG Review: ArrhythmiasA guide to reading ECG's written by a
college (not medical school)professor
CyberHeartTutorial to experiment with cardiac function... (but
try to avoid causing cardiac
arrest!)
Resources for Further Study: remarkable and challenginglearning
tools. Just dont have a Cardiac Arrest
http://www.nhlbi.nih.gov/health/dci/Diseases/ekg/ekg_what.htmlhttp://davidge2.umaryland.edu/~emig/ekgtu01.htmlhttp://en.ecgpedia.org/http://www.ecglibrary.com/http://www.ecgsim.org/http://www.ecgsim.org/http://www.gwc.maricopa.edu/class/bio202/cyberheart/ekgqzr0.htmhttp://www.gwc.maricopa.edu/class/bio202/cyberheart/cybrhart49.htmhttp://www.gwc.maricopa.edu/class/bio202/cyberheart/cybrhart49.htmhttp://www.gwc.maricopa.edu/class/bio202/cyberheart/ekgqzr0.htmhttp://www.gwc.maricopa.edu/class/bio202/cyberheart/ekgqzr0.htmhttp://www.ecgsim.org/http://www.ecgsim.org/http://www.ecglibrary.com/http://www.ecglibrary.com/http://www.ecglibrary.com/http://en.ecgpedia.org/http://en.ecgpedia.org/http://davidge2.umaryland.edu/~emig/ekgtu01.htmlhttp://www.nhlbi.nih.gov/health/dci/Diseases/ekg/ekg_what.htmlhttp://www.imhotepvirtualmedsch.com/