Embed Size (px)
Citation preview
Introduction to Psychological Assessment
of Children
Gregg Selke, Ph.D. PSY 4930
October 3, 2006
Purpose of Psych. Assessment
Goal Driven Broad Screening versus
Focused/Problem-Specific Diagnostic
Differential and Comorbid Conditions Therapy Oriented
Identify target problems Develop preliminary intervention plan
Progress evaluation How well are ongoing interventions
working?
Testing vs. Assessment
Both involve Identifying areas of concern Collecting data
Psychological Testing Administering tests Focuses solely on collection of data
Psychological Assessment More broad goals Involves several clinical tools Uses clinical skill to interpret data and interpret data and
synthesize resultssynthesize results
Psychological Testing
Require standardized proceduresstandardized procedures for behavior measurement Consistency and use of the same
Item content Administration procedures Scoring criteria
Designed to reduce personal differences and biases of examiners and other external influences on the child’s performance
Psychological Assessment
Main types of assessment1. Norm-referenced tests2. Interviews3. Observations4. Informal assessment procedures5. Non-norm referenced tests
Norm-Referenced Tests
Tests that are standardized on a clearly defined group Normative versus clinical reference groups
Goal: quantify the child’s functioning Scores represent a rank within the
comparison group Examples
Intelligence Academic skills Neurocognitive skills Motor skills Behavioral and emotional functioning
Norm-Referenced Tests
Psychometric properties Demographically representative
standardization sample Reliability
Internal consistency, test-retest stability Validity
Correlation with other tests measuring same construct
Ecological
Psychological tests are imperfect Examiner, the child, and the environment can
affect responses and scores
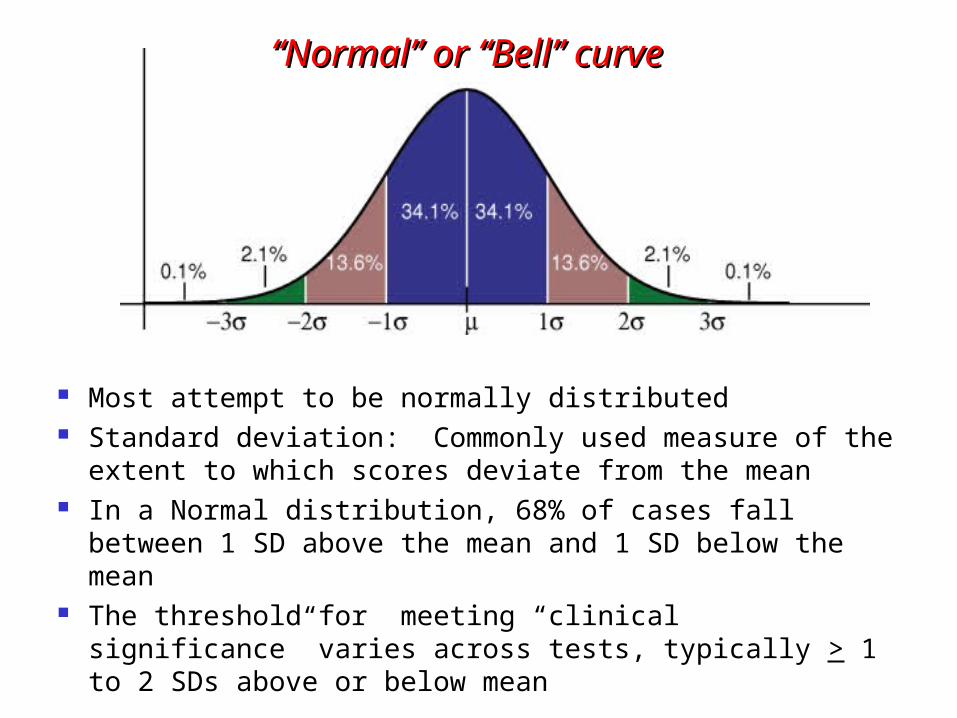
Most attempt to be normally distributed Standard deviation: Commonly used measure of the
extent to which scores deviate from the mean In a Normal distribution, 68% of cases fall between 1
SD above the mean and 1 SD below the mean The threshold for meeting “clinical significance”
varies across tests, typically > 1 to 2 SDs above or below mean
““Normal” or “Bell” curveNormal” or “Bell” curve
Norm-Referenced Tests
Percentile ranks Determines child’s position relative to the
comparison group Example: What does it mean when a child
is in the 35th %tile on an Intelligence test?? Age-Equivalent and Grade-Equivalent
scores Frequently used on academic achievement
tests Sometimes questionable validity
Variables Affecting Test Scores
Demand characteristics Child may give a certain type of response
in order to obtain a desired outcome Response bias
Child’s response to one item may influence how they respond to subsequent items
Social desirability Tendency to present one’s self in a
positive light
Variables Affecting Test Scores
Misinterpretation of Items Misunderstanding directions
Format of instructions Oral vs. written
Response format True-false, written, oral, timed, untimed
Setting variables Location, time of day, medication status
Previous testing experience Practice effects
Variables Affecting Test Scores
Reactive effects Assessment procedure affects responses
Timed, anxiety provoking
Examiner-examinee variables Individual characteristics may affect
responses (e.g., gender, age, warmth) Research suggests that children of low
SES and/or ethnic minorities are more affected by examiner characteristics
Familiar vs. unfamiliar examiner
Administering Tests
Administering psychological tests to children requires specific skills Flexibility: breaks, time to warm up,
establishing rapport Vigilance: attend to child’s behavior
while still correctly administering the test
Self-awareness: how do children typically react to your style, body language, mannerisms
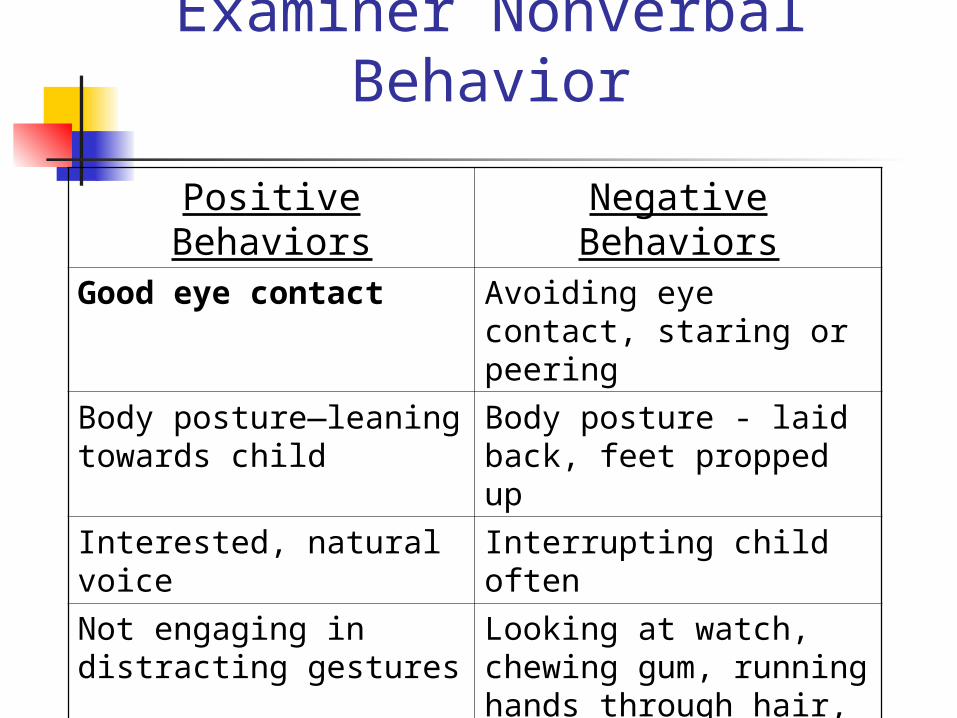
Examiner Nonverbal Behavior
Positive Behaviors Negative BehaviorsGood eye contact Avoiding eye contact,
staring or peering
Body posture—leaning towards child
Body posture - laid back, feet propped up
Interested, natural voice
Interrupting child often
Not engaging in distracting gestures
Looking at watch, chewing gum, running hands through hair, etc.
Taking minimal notes while continuing to make frequent eye contact
Taking excessive notes and seldom looking at child
Other Testing Issues
Introducing yourself to child Explaining what the child will be doing Letting them know where their parent
will be during the assessment Providing adequate expectations Developmental considerations
Younger children Older children
Praising effort NOT performance Setting limits on behavior
Establishing Rapport
“the sense of mutual trust and harmony that characterizes a good relationship”
Good rapport = child/family perceives the clinician as
caring, interested, competent, and trustworthy
Clinician feels positive regard, genuineness, and empathy
Necessary condition
Establishing Rapport
Use of communication skills Acknowledgements Descriptive Statements Reflections Praise Periodic Summaries Elaboration Clarification
Establishing Rapport
Avoid: Lack of interest or not attending Sarcasm Lecturing Interrupting Commands No eye contact Criticisms
Interviewing
Types of interviews: Unstructured—allow child/parent to “tell
their story” Semi-structured—provide flexible
guidelines, a starting point Structured—most often used to make
diagnoses or in research studies, standardized
May interfere with rapport Does not provide info on family interactions or a
functional analysis of behavior Which types of interview require the most
clinical skill??
Explaining Confidentiality
Parents sign releases of information Review concept of confidentiality and its
limits early in clinical interaction Limits to confidentiality:
Specific threat to someone else (homicidal ideation)
Self-harm is threatened (suicidal plan/intent) Sexual and physical abuse (history or current) Insurance requests Courts Generally referral source
Interviewing Techniques
Establishing rapport is crucial Moving from open-ended to closed-
ended questions (general to specific) Tell me about why you’re here today? What about school is most difficult for you? Are you failing math because you didn’t
hand in your homework….not studying……didn’t understand the material?
Avoid Double-barreled questions (“and”, “or”) Long, multiple questions Leading questions Psychological jargon
Example Developmental Interview
A. History of presenting problemB. Prenatal, perinatal, and early postnatal
historyC. Medical historyD. Acquisition of age-related milestonesE. School historyF. Personality, social, emotional, behavioral
historyG. Family historyH. Expectations about assessment visit
Example Developmental Interview
A. History of presenting problem Parental description of problem Child’s view of problem Onset Duration Interventions attempted Prior assessments Parents sense of effects of problem,
and sense of child’s understanding
Example Developmental Interview
B. Prenatal, perinatal, and early postnatal history
Pregnancy Labor and delivery Birth weight Apgar scores Complications post-birth
Example Developmental Interview
C. Medical history Across all ages Accidents & injures Major illnesses Ear infections Neurological conditions Congenital and genetic conditions Hearing and eyesight
Example Developmental Interview
D. Acquisition of age-related milestones Motor Language Toileting
E. School history Preschool experiences to present – Settings Achievement, grades, strengths and
weaknesses Behavioral, emotional, social functioning IEPs, 504 Plans, accommodations, modifications What teachers think
Example Developmental Interview
F. Personality, social, emotional/mood, behavioral history across development
Temperament as an infant and toddler 2.5-5 years: Development of play, aggression,
interests 5-11 years: Hobbies, activities, friendships,
family relationships 11 to adolescence: Development of interest in
opposite sex, dating and sex, activities, drug and alcohol use, family relationships, self-concept, goals and aspirations
Example Developmental Interview
G. Family history Parental history: marriage(s), # children Demographics, ages, education,
occupation, SES Siblings: ages, problems, school history Medical, genetic, developmental,
psychological, abuse problems
H. Expectations about assessment visit
Developmental Considerations
Young children tend to think in concrete ways, while teens may reflects more on feelings and motivations
While age is an obvious indicator of developmental level, language and cognitive levels may also vary with age
Interview format should be adjusted to the individual child’s level Open vs. Closed questions
Developmental Considerations
6 year olds might be asked about the difference between preschool and kindergarten
Young teens might be asked about the transition to individualized school schedules and homework, and peer pressures.
Older teens might be asked about college, vocational plans, or separating from parents
Format of the Interview
Who will be interviewed is often a question with young patients e.g., Children under 6 typically are
generally interviewed with parents, then sometimes parents are seen alone
e.g., Older children and adolescents are often seen as a family first and then later may be interviewed alone
Sex abuse may be an exception
Format of the Interview
If the clinicians sees family together it allows for: Observation of interactional patterns Areas of agreement and disagreement
Tell family how their time will be structured Allow them to know if they can save
sensitive topics for when they are alone
Closing the Interview
Summarize what has been learned Make sure you understand what the
interviewee has reported Helps determine what additional
information might be needed Ask the child/family if they have
questions “Is there anything else I didn’t ask
about that you think it would be important for me to know?”
Behavioral Observations
Psychological assessments always include observations about the patient’s behavior during the assessment
Collected throughout the assessment Areas assessed/observed:
Orientation (person, place, time) General appearance and behavior
Gait, posture, dress, personal hygiene, activity level
Speech and thought Coherence, speed, open vs. guarded
Behavioral Observations
General response style Mood and affect
Euthymic vs. dysthymic Labile, blunted, etc.
Reactions to being evaluated Response to encouragement Attitude towards self Unusual habits, mannerisms,
vocalizations
Behavioral Observations
How child relates to parent? How child relates to examiner? How child reacts to test materials
or toys? Is the child age appropriate in
behavior? How is the child’s concentration?
Behavioral Observations
Are tantrums seen? Does the child cooperate? What is the extent of child’s
responses? short vs. elaborate
How is the child’s speech and language development?
Informal Assessment
Self-monitoring records Report cards Personal documents
Diaries, poems, stories Role playing
Multimodal Assessment
Obtaining information from several sources Integrate information from several
sources Recognize limitations of any one source
Using several assessment methods Assessing several areas of
functioning Strengths and weaknesses
Interpreting Results
Are test results congruent with other information obtained?
How can you account for discrepancies in teacher, parent, child reports?
Do findings appear to be reliable and valid?
INTEGRATING results from multiple sources is a critical clinical skill
Final Steps in Assessment
Develop intervention strategies and recommendations
Write a report Provide feedback Follow-up
Key Ingredients
Successful assessment requires knowledge of: Psychological tests Psychopathology Interviewing Statistics Development Hypothesis testing Your self