Embed Size (px)
Citation preview
I N T R O D U C T I O N T O H E A L T H H O M E S & Q C C P C O L L A B O R A T I O N
J A N U A R Y 2 6 , 2 0 1 7
P R E S E N T E D B Y :
V A L E N T I N E H E R N A N D E Z
G U I L L E R M O G A R C I A G O L D W Y N
What is a Health Home ?
Opening Activity
• Write down the definition of a Health Home
• Write Down the Role of a Care Manager
Group Discussion
What is a Health Home?
• Health Homes are an administrative oversight agency that oversees Care Management Agencies who provide case management services.
• Case Management is a service model that aims to increase communication among all
members of the care team. • A Care Manager connects the care providers and coordinates referrals and access to
the services a members requires.
• A mutually agreed upon Care Plan (goals) address the patient’s medical, behavioral health and social service needs.
• Partnerships are important! Healthcare providers, health plans, community based organizations • It is a voluntary service- no impact on current services if a patient doesn’t enroll
Eligibility
▶ Active Medicaid status -(Includes: dual eligible, managed care, SNP, MLTC,HARP, FIDA) ▶ 2 Diagnosed chronic medical conditions OR one of the below, -HIV/AIDS -Serious mental illness ▶ Demonstrated need for care management services -(e.g. Inadequate social supports, non-adherence, frequent hospital/ED use, homeless)
Health Home Goals
• Improve overall health outcomes • Helps patients address socioeconomic concerns • Reduce preventable hospitalizations & emergency room visits • Avoid unnecessary costs Help patients become self advocates and self sufficient!
Current Contracted Partners: Operating Agreement /Governing Partners Community Healthcare Network Mount Sinai Queens MediSys New York Presbyterian Queens iHealth
1. ACQC 2. Apicha 3. Bailey House 4. BOOM! Health 5. GMHC 6. Harlem United 7. HeartShare 8. BrightPoint Health 9. LIAAC/Tri Care Systems 10. NADAP
Downstream Providers ACMH Family Services of New York Federation of Organizations Mental Health Providers of
Western Queens Puerto Rican Family Institute Argus (formerly Steinway) The Bridge Transitional Services for New
York, Inc. New Horizon Creedmoor (ACT and Care
Management) VNS ACT Team
Six Core Services
Comprehensive Care Management (Assessing, Care Plans & Team
Consulting) Care Coordination & Health Promotion (Services in Place & Adherence to
Treatment) Comprehensive Transitional Care (Use of other Systems of Care w/i the
Hospital & Review discharge summary) Patient & Family Support (Peer Support Groups & Involving Natural
Resources) Referral to Community & Social Support Services (Identifying/
Linkage/Referral to Community Based Organizations) Health Information Technology (Utilizing electronic information for
meaningful use)
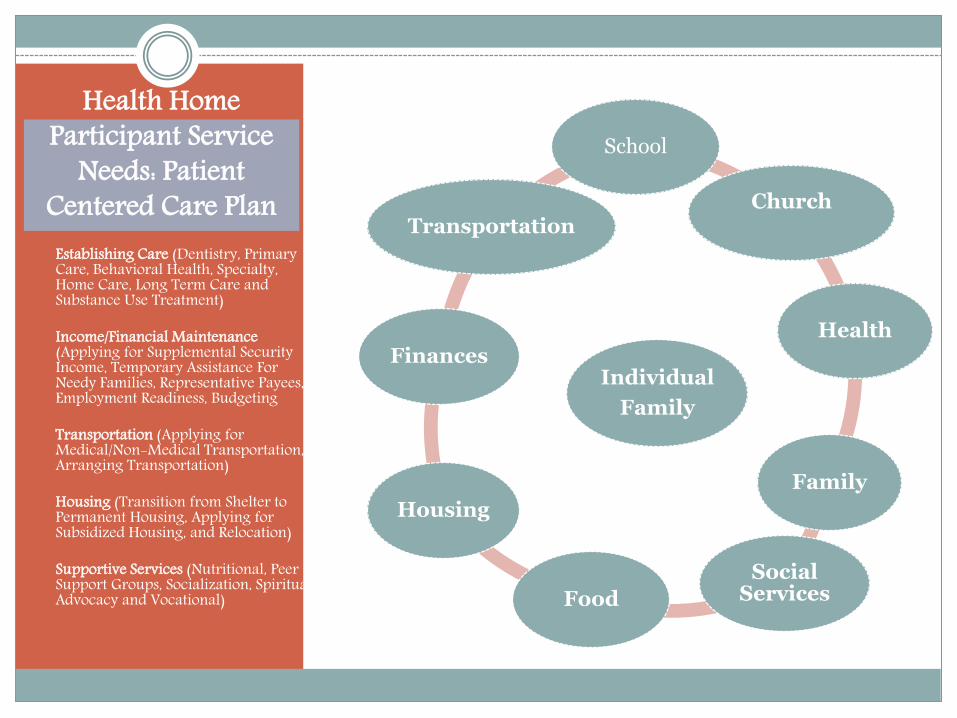
Health Home Participant Service
Needs: Patient Centered Care Plan
Establishing Care (Dentistry, Primary
Care, Behavioral Health, Specialty, Home Care, Long Term Care and Substance Use Treatment)
Income/Financial Maintenance (Applying for Supplemental Security Income, Temporary Assistance For Needy Families, Representative Payees, Employment Readiness, Budgeting
Transportation (Applying for Medical/Non-Medical Transportation, Arranging Transportation)
Housing (Transition from Shelter to Permanent Housing, Applying for Subsidized Housing, and Relocation)
Supportive Services (Nutritional, Peer Support Groups, Socialization, Spiritual, Advocacy and Vocational)
Individual
Family
School
Church
Health
Family
Social Services Food
Housing
Finances
Transportation
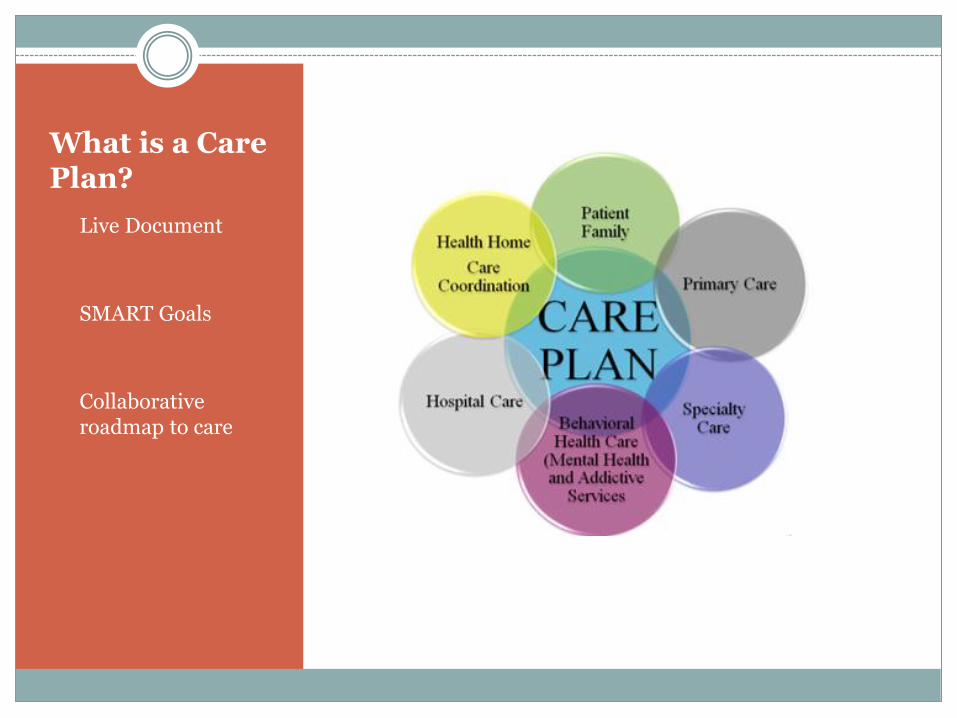
What is a Care Plan?
• Live Document
• SMART Goals
• Collaborative roadmap to care
Disconnections with clients and providers
Clients: -The care managers purpose is to focus on
psychosocial needs such as transportation, housing, and entitlements, the clinical goals of care coordination are seen as secondary.
- The care manager must establish a
relationship so that clients understand the holistic approach to care and gradually incorporate clinical goals as priorities without making the patient feel the care manager is not understanding there needs.
Providers:
Communication with Care Managers takes away from the time they need to provide direct services
Health Homes can make bulk referrals
to clinical agencies after a linkage or partnership is formed
The Mystical Care Plan is an administrative burden
that holds no value….

Barriers to Collaboration
• HIPAA rights are vital to protecting patients PHI and they are important … however, providers often misunderstand HIPAA regulations… as they relate to care coordination and the NYS Health Home Consent.
Early data across New York State shows: o 14 %increase in primary care visits o 23 % decrease in hospital admissions and emergency
department visits.
Health Homes provide: o Connectivity between providers o Increase compliance with patient care plans o The staff connect the patient to additional services o Support in medication management and compliance o Psycho-social supports to improve patient outcomes
Despite it ALL!!!! Positive Outcomes
Requirements o Medicaid o Two or more chronic conditions or one qualifying (HIV, SMI)
QCCP Contacts o Oscar Laluyan: Warm Hand Offs! [email protected] 718.906.6243
o Guillermo Goldwyn Garcia [email protected] 718.906.6246 (Direct/Office) 347-640-1406 (Cell)
o Secure Email & Referral Form
How Do I Refer patients or clients?
We are all on the same journey to improve people’s health!!!!!!!!!!!!!