Embed Size (px)
Citation preview
THE BREAST
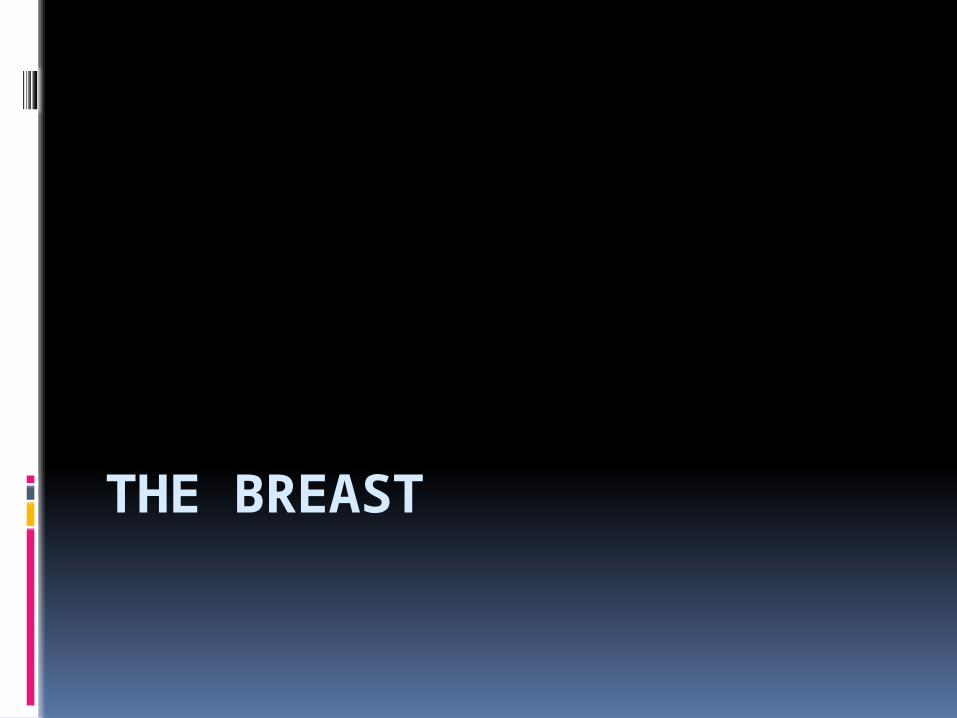
Introduction
Modified sweat glands.Lobes and lobules of gland in fat tissue stroma.Ducts emerge from acini of glandsSmaller ducts join to form lactiferous
ductsLactiferous ducts merge just beneath
the nipple to form a lactiferous sinus.Then individually open on nipple
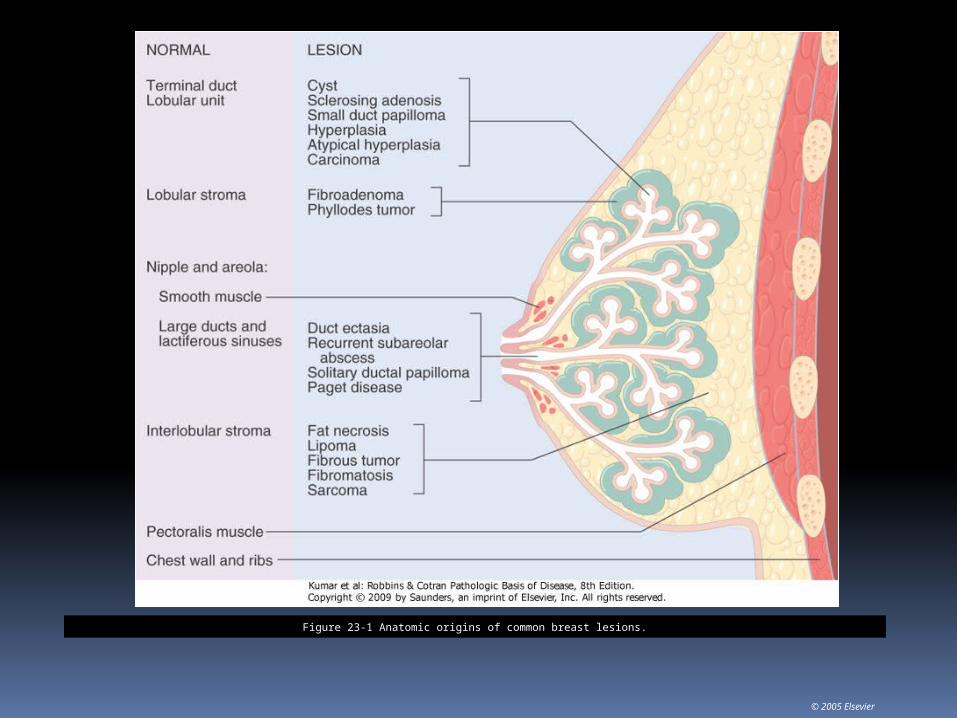
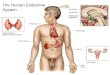
Figure 23-1 Anatomic origins of common breast lesions.
© 2005 Elsevier
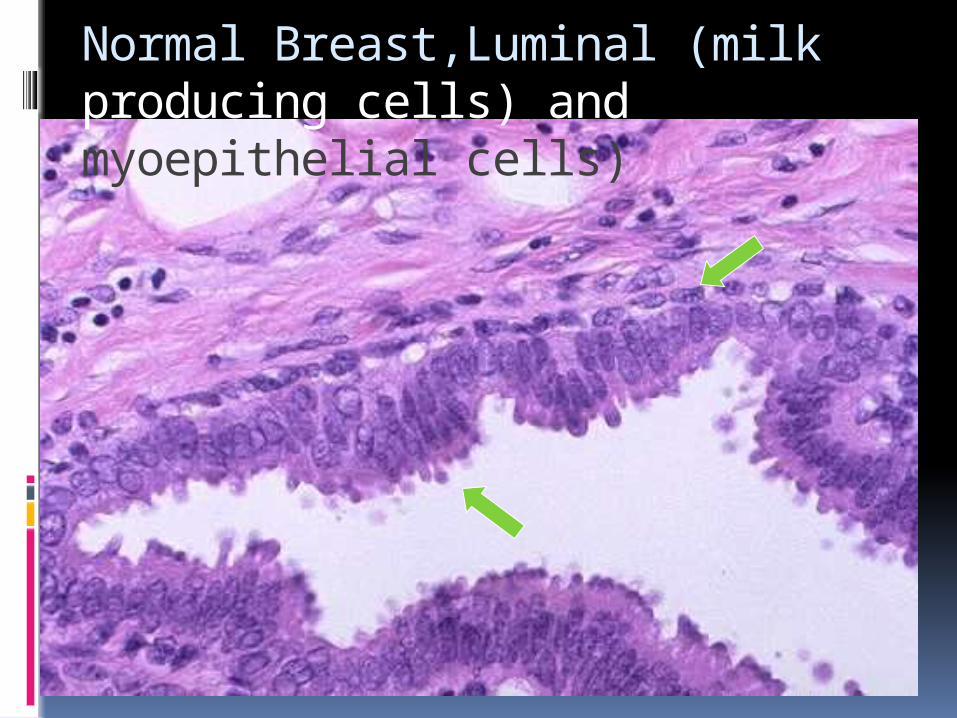
Normal Breast,Luminal (milk producing cells) and myoepithelial cells)
Disorders
Congenital Aplasia – turners, Juvenile
hypertrophy,Macromastia Inflammatory
Infections acute/chronic – Trauma Fat necrosis
Duct ectasia discharge, sinus Fibrocystic disease – common – painful
lumps Neoplastic
Benign - Fibroadenoma Malignant – Ca
Breast Symptoms
Pain(Most common symptom)Most are benign. Palpable Mass
Nipple discharge
Palpable masses 2nd most common breast symptom. A breast
mass becomes palpable when >2cm Distinguish a palpable mass from vague
nodularities or lumpinessLesions includes: Invasive carcinoma, fibroadenomas and cysts. 10% of palpable masses are malignant in
under 40 yr olds compared to 60 % malignancy rate for palpable masses in over 54 yr .olds
50 % of carcinomas arise in upper outer quadrant.20% in central quadrant and 10% each in the other quadrants
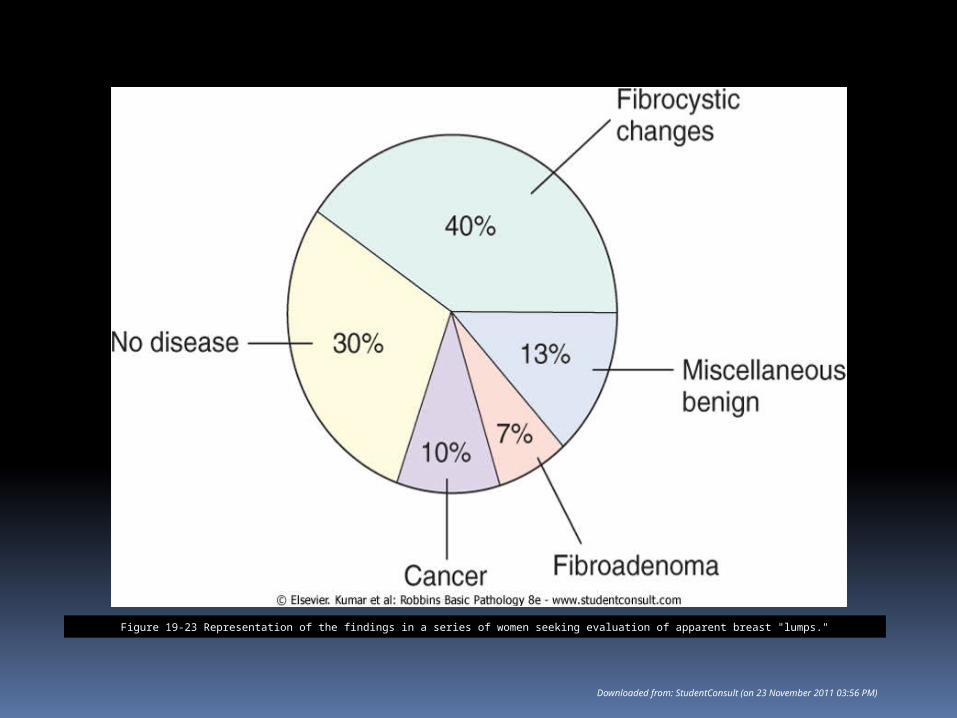
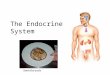
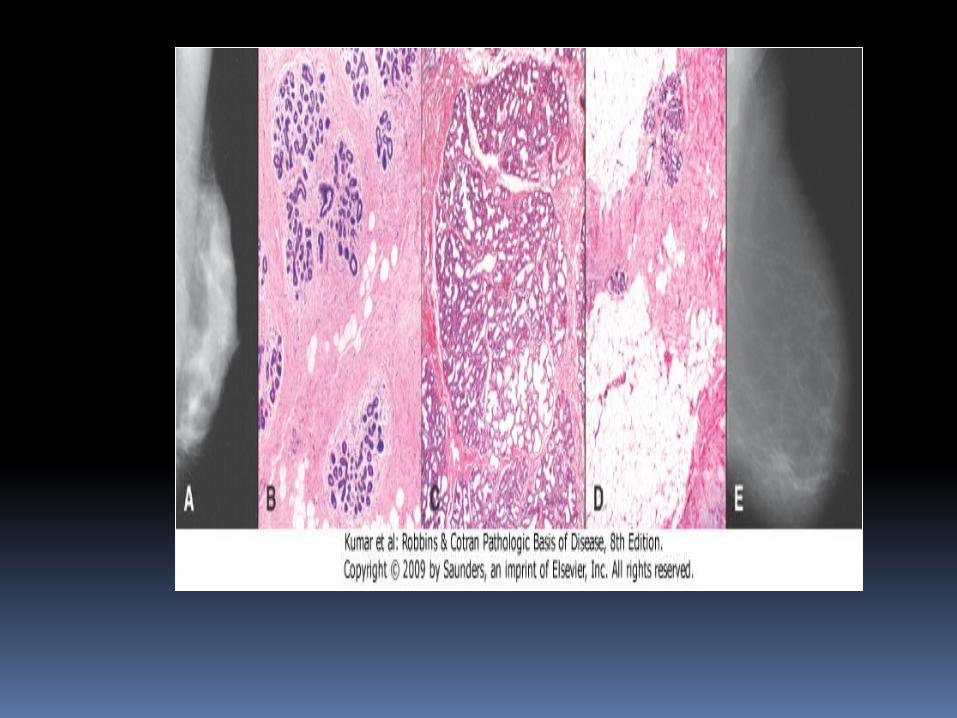
Figure 19-23 Representation of the findings in a series of women seeking evaluation of apparent breast "lumps."
Downloaded from: StudentConsult (on 23 November 2011 03:56 PM)
Nipple discharge
Note that galactorrhea is not associated with malignancies
Serous or bloody nipple discharge may be seen in a small percentage of breast cancers
The older the age, the higher the risk of a malignancy in a patient with bloody or serous discharge.
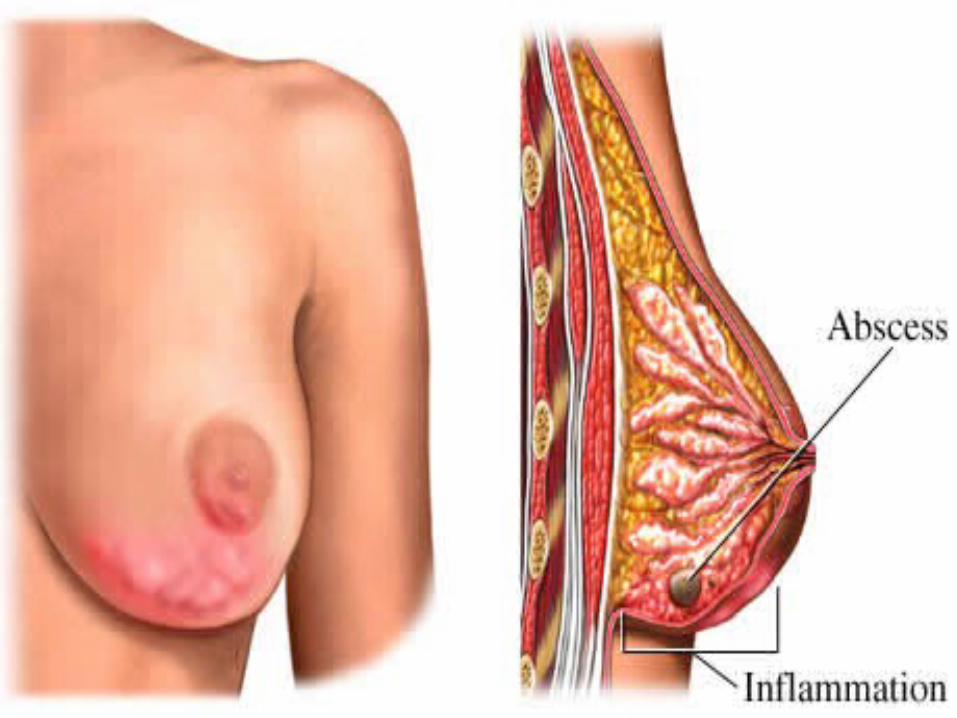
Mastitis Inflammation of the mammary gland Causes : 1. breast feeding (Acute mastitis) 2. Periductal mastitis 3. Mamary Duct EctasiaB 1. Breast feeding (Acute mastitis)A blocked milk duct Cracked or damaged skin or tissue around
the nipple Signs :red, hot, painful, or inflamed
breasts with flu-like symptoms such as headache, nausea, high temperature
• Staph aureus • Strept.

Mastitis
Periductal mastitis (Zuska disease,recurent sub -areolar abscess)
Recurrent sub-areolar abscess Painful mass that resembles infection Not associated with lactation 90% of patients are smokers Keratinizing squamous metaplasia of
the nipple ducts. ? Vitamin A deficiency, Toxic
metabolites of tobacco.
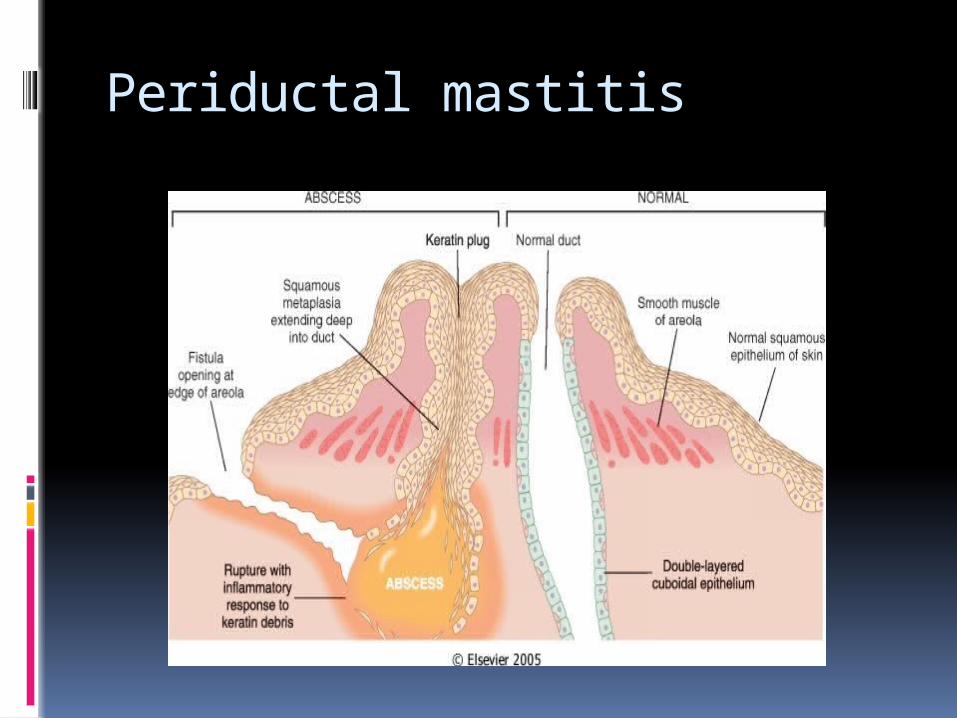
Periductal mastitis
Mammary duct ectasia
Nonbacterial chronic inflammation of the breast associated with inspissation of breast secretions in the main excretory ducts.
Multiparous women Ductal dilation with ductal rupture
leads to reactive changes in the surrounding breast substance.
40- 50 year old women Not Associated with smoking.
Fat Necrosis Trauma, Prior surgical intervention A zone of necrotic fat cells surrounded
by lipid-filled macrophages and an intense neutrophilic infiltration, foreign body giant cells, calcium salts.
Eventually the focus is replaced by scar tissue or is encysted and walled off by collagenous tissue
Match the following
Periductal fibrosis Acute mastitis Fat Necrosis
Smoking Breast feeding Trauma
Fibrocystic Changes Non proliferative type
Fibrosis, Cyst formation, apocrine metaplasia,
Proliferative type Papilloma(s), florid sclerosing adenosis, moderate to florid ductal hyperplasia,
Risk of malignancy increases from simple fibrocystic change to fibrocystic change with atypical hyperplasia
Family history of breast cancer increases the risk by up to 10%
Downloaded from: StudentConsult (on 23 November 2011 03:56 PM)© 2005 Elsevier

© 2005 Elsevier

Fibrocystic Changes
Symptoms and Signs Breast pain (mastodynia) and/or tenderness
is observed in the majority of patients. Mastodynia may start a few days or 1 to 2 weeks
before menstruation; it usually eases or subsides with the onset of or during menses
Nipple discharge is spontaneous or secretion can be expelled from the nipple
Diffuse lumpy feeling in the breast .
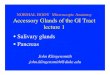
Fibroadenoma Firm, noncancerous tumor of the
breast. It is round, painless, feels firm
and rubbery, and can be easily moved around.
Peak age:20-30 Rapidly grow to a large size Present with Palpable mass or
mammographic density Malignant transformation rare
Fibroadenoma
Fibroadenomas may enlarge during late menstrual period and tends to calcify or regress by menopause
Lobular stromal cells are the neoplastic component in fibro-adenomas
© 2005 Elsevier
© 2005 Elsevier
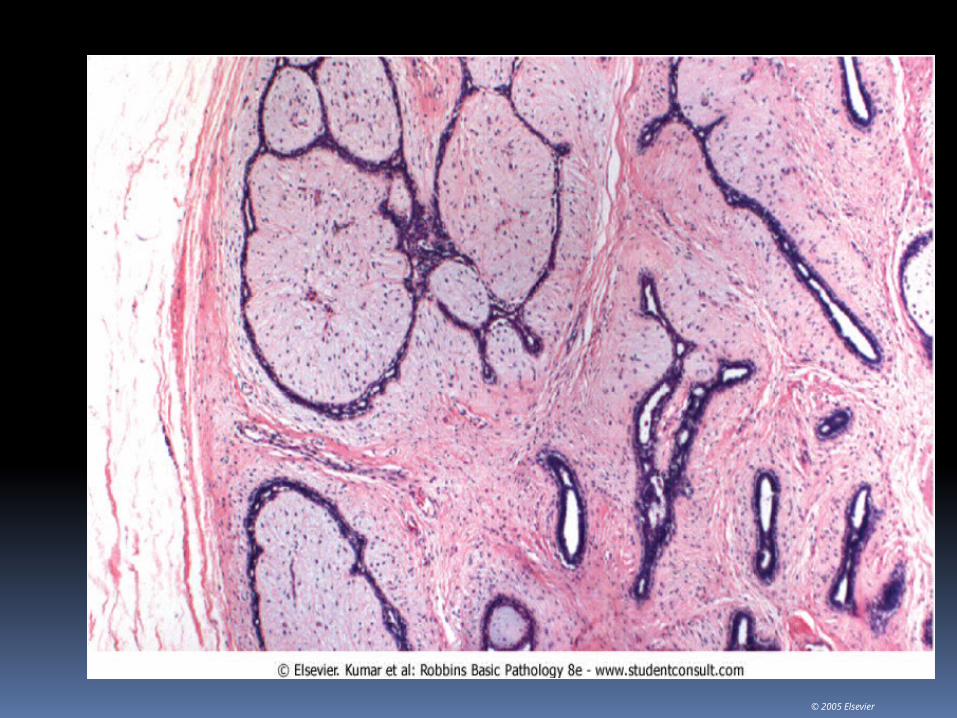
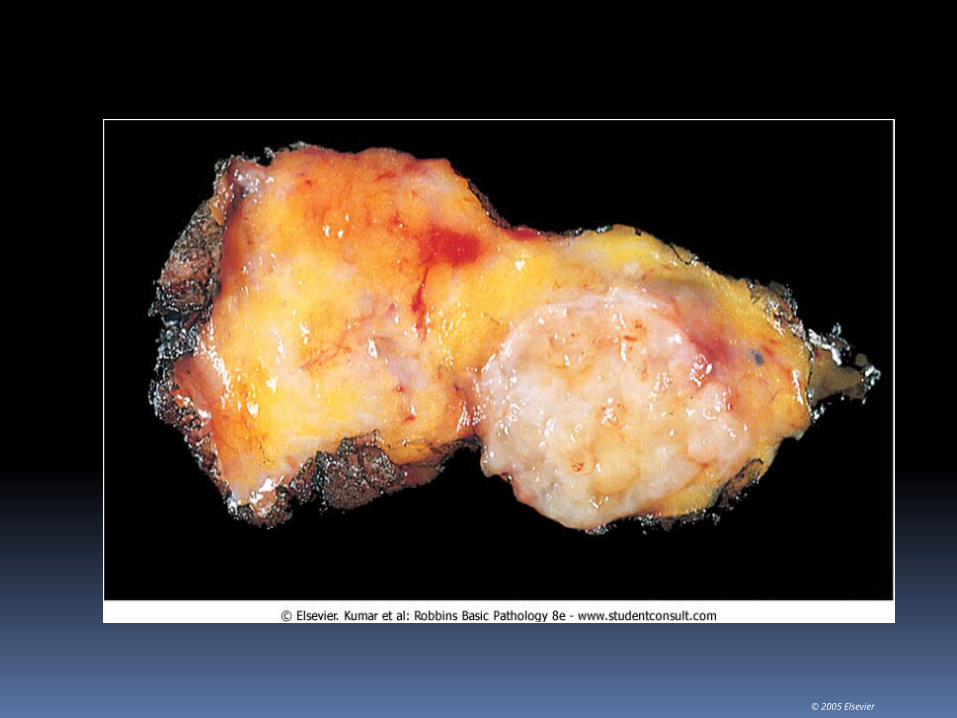
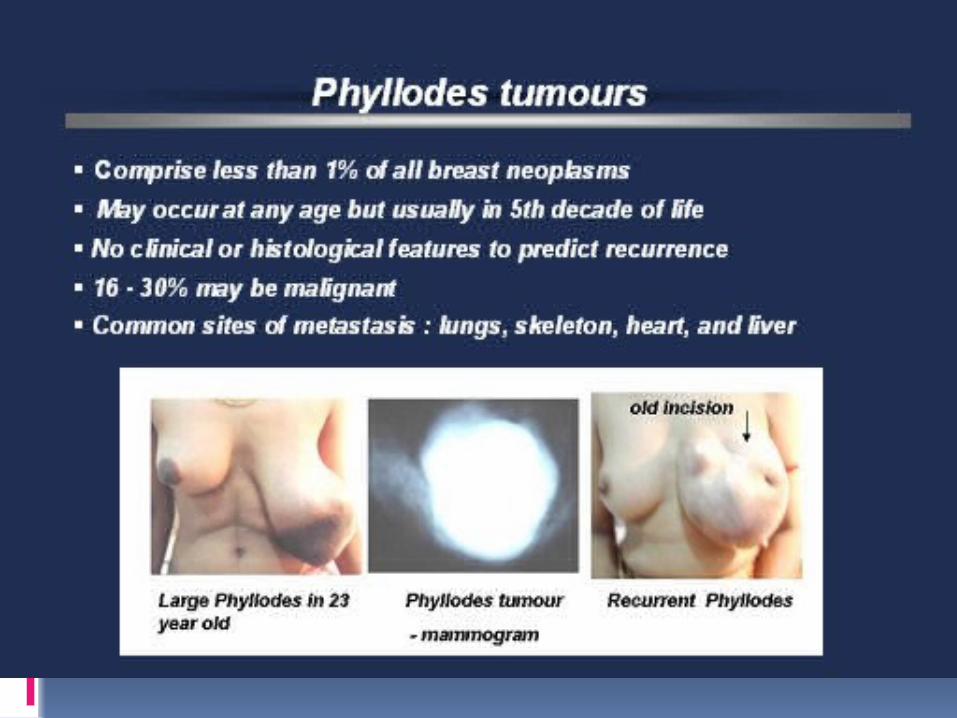
Phyllodes tumorCystosarcoma phyllodes• epithelial-stromal neoplasms with
dominating stroma and leaf-like structure
• Most are benign lesions.• 15% are malignant.• 0.3% of all breast tumors• 30% recurrence; 10% metastasis• Age: older than with FA (average 45)• Well defined, uncalcified, lobulated,
round or oval• Commonly with thin irregular cystic
spaces
Quiz A 30 year old woman complained that
she has noticed a firm ,painless , freely mobile mass located in the upper –outer quadrant of her left breast. The mass increases in size towards the end of her menstrual flow. Which of the following is the most likely diagnosis?
A. MelanomaB. FibroadenomaC. Fibrocystic changeD. Breast cancer
INTRADUCTAL PAPILLOMA: Benign solitary lesions within the
ducts. EPIDEMIOLOGY: Middle-aged and older
women. SYMPTOMS: Serous or Bloody Nipple discharge,
nipple retraction. Lump beneath nipple. papillary clonal proliferations of duct
epithelia cells composed of multiple branching papillae
Benign and are not the precursors of papillary carcinoma
TREATMENT: Surgical excision.
Breast Carcinoma
20% of all cancers in women
Commonest cause of death - 35-55y
1 in 8 women in US Less incidence in Asia Majority of cancers
arise in the ducts. Very rare before age
25
Risk Factors:Female ..!, Age, Obesity, high
fat ,low fibre diet Maternal relative with breast cancer. Longer reproductive span. Nulliparity, Oral contraceptivesLater age at first pregnancy. Atypical epithelial hyperplasia. Previous breast cancer/Endometrial
Ca. Geographic factors –Western
countriesBRCA1 and BRCA2 genesPostmenopausal hormone
replacement
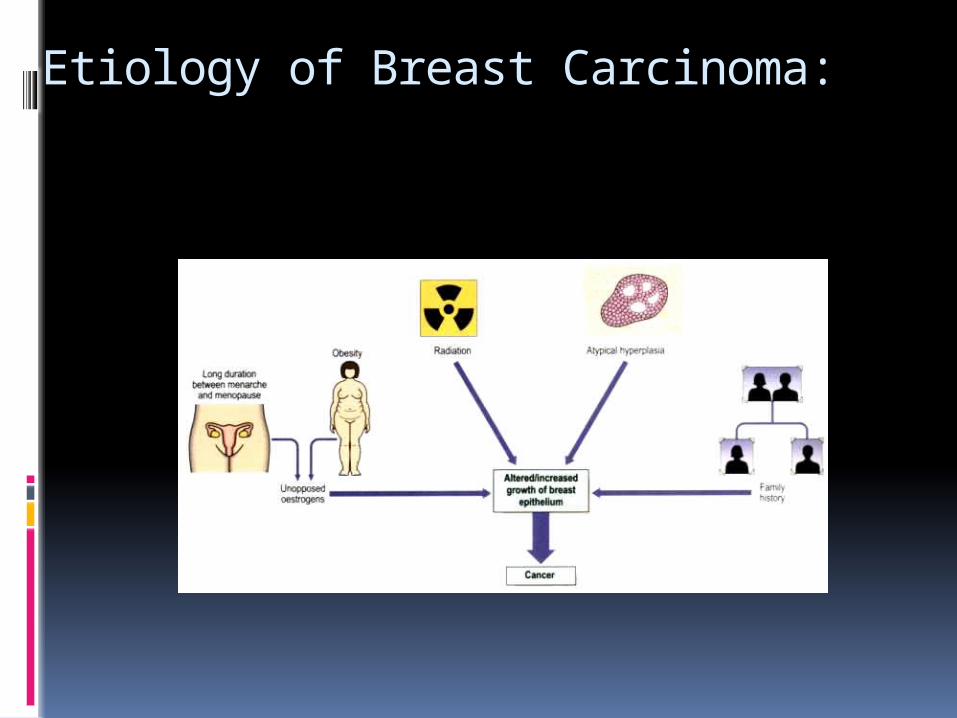
Etiology of Breast Carcinoma:
Genetics/Hereditary BRCA-1(Also ovarian
cancer,Pancreatic cancer)
BRCA-2(Also pancreatic cancer)
BRCA-1 and 2 have an autosomal dominant pattern of inheritance.
Li Fraumeni syndrome P53 Her-2/neu, c-erB2

Sporadic Breast carcinoma Majority of breast CA is sporadic Hormonally and environmental
factors Most are ER positive and occur
in Postmenopausal women.
Breast Carcinoma
Epithelial Non-invasive
Ductal carcinoma in situ (DCIS) Lobular carcinoma in situ (LCIS)
Invasive Ductal (85%) Lobular (1%) Mucinous (5%) Papillary (<5%) Medullary (<5%)
Mixed Connective tissue and Epithelial
Miscellaneous
CLASSIFICATIONAll Breast CA arise from epithelial cells
in the TDLU>90% are adenocarcinomas and are
divided into:1.1. Carcinoma in situ(DCIS,LCIS) Intact basement membrane Carcinoma is limited to the lobule or
ducts22. Invasive carcinoma Basement membrane is breached Tissue invasion and metastasis is
possible.
CLASSIFICATION
The classification into ductal or Lobular refers to the histological appearance and the biologic properties of the tumor rather than to the cell of origin.
Lobular carcinoma refers to a distinct subtype while the term Ductal refers to any histological type that is not otherwise specified.
© 2005 Elsevier
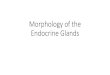
Direct precursor of invasive ductal carcinoma• Visible on mamography because of calcification• Most often picked up via mamography• Clonal proliferation of cells in the ducts and lobules
limited by basement membrane.• Five subtypes:• Comedone, Solid, cribriform, papillary and micro
papillary• Mastectomy is usually curative(95%)• Incidence of DCIS increases with increase uptake of
mamographic screening in any population.
DUCTAL CARCINOMAIN-SITU
DUCTAL CARCINOMAIN-SITU
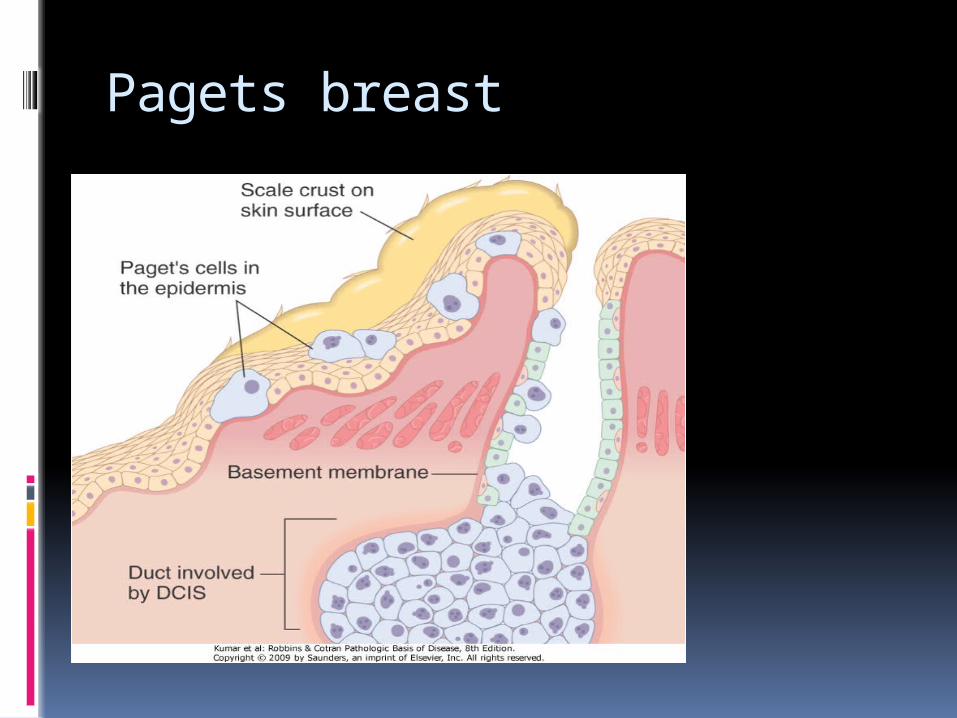
Paget disease of the nipple Rare manifestation of breast cancer (1%
to 4% of cases) Unilateral erythematous eruption with
scaly crust and Pruritus. Malignant cells (Paget cells) extend from
DCIS via the lactiferous sinuses, into nipple skin without crossing the basement membrane.
60% of women with the lesion would have an underlying mass and invasive cancer.
Pagets breast
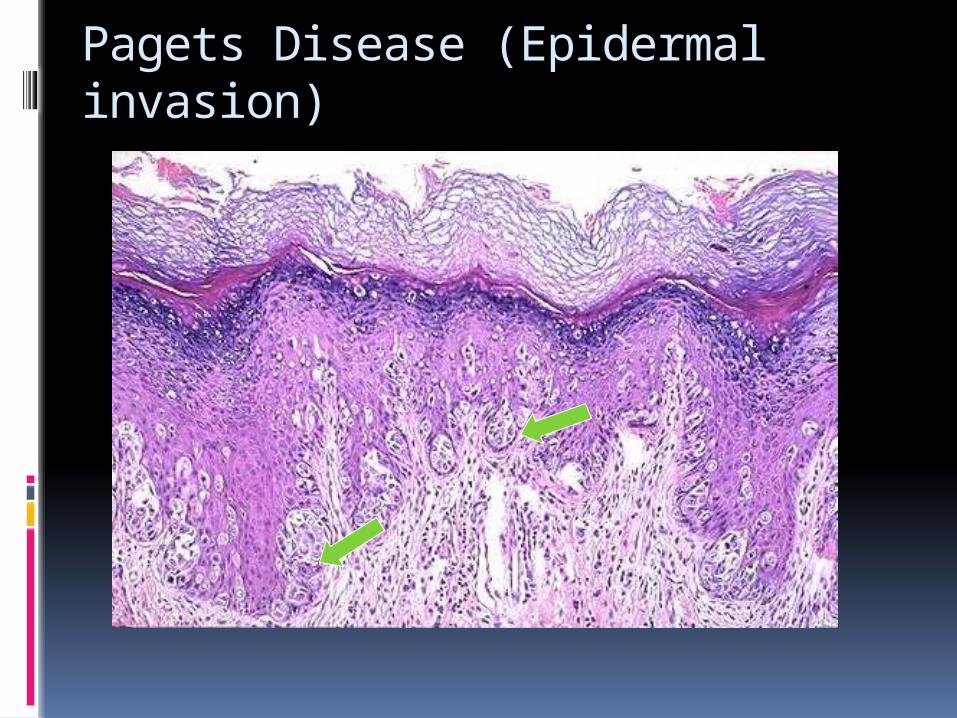
Pagets Disease (Epidermal invasion)
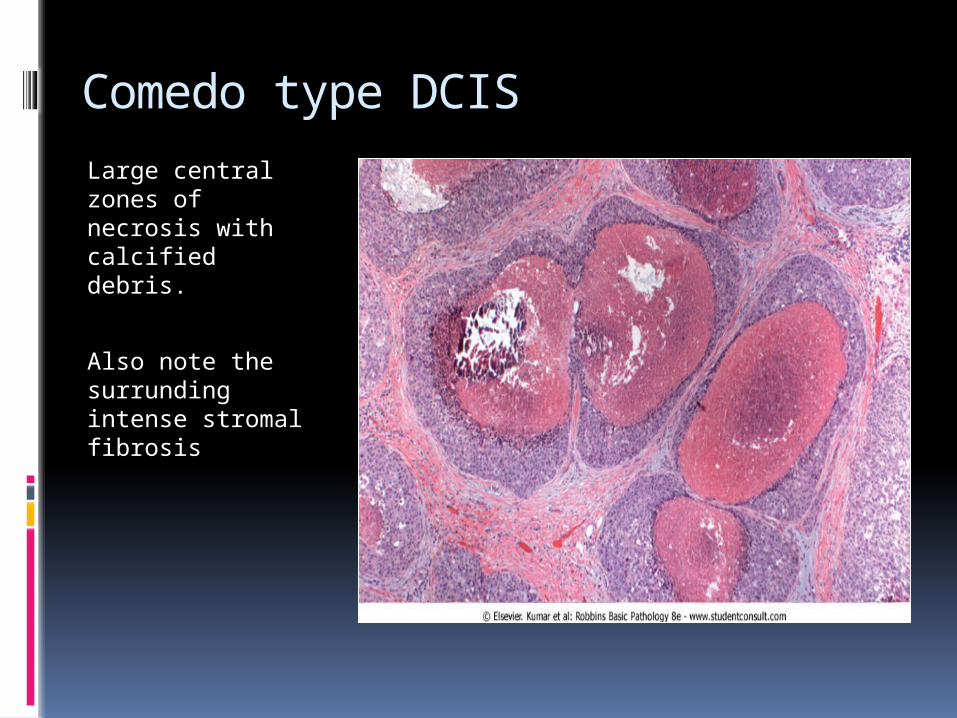
Comedo type DCIS
Large central zones of necrosis with calcified debris.
Also note the surrunding intense stromal fibrosis
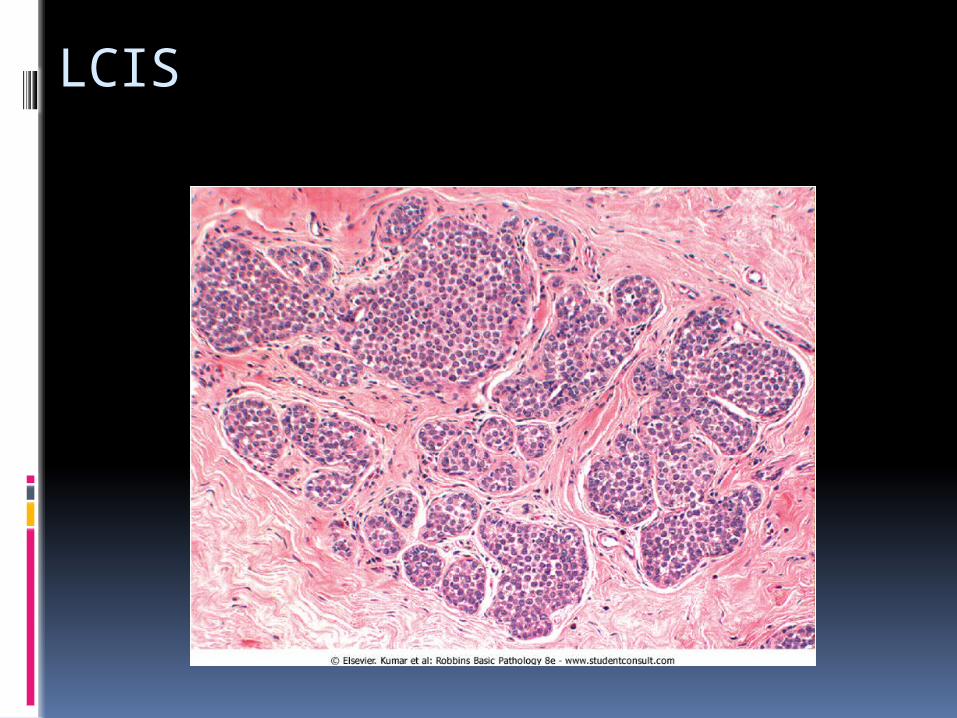
LOBULAR CARCINOMA IN SITU Incidental biopsy finding, No calcifications or stromal
reactions that produce mammographic densities.
Incidence is not affected by mamographic screening.
Bilateral in 20% to 40% of cases, compared with 10% to 20% of cases of DCIS.
LCIS is more common in young women, 80% to 90% of cases occurring before menopause.
LOBULAR CARCINOMA IN SITU
The cells of LCIS and invasive lobular carcinoma are identical.
Loss of expression of E-cadherin
LCIS
DCIS/LCIS
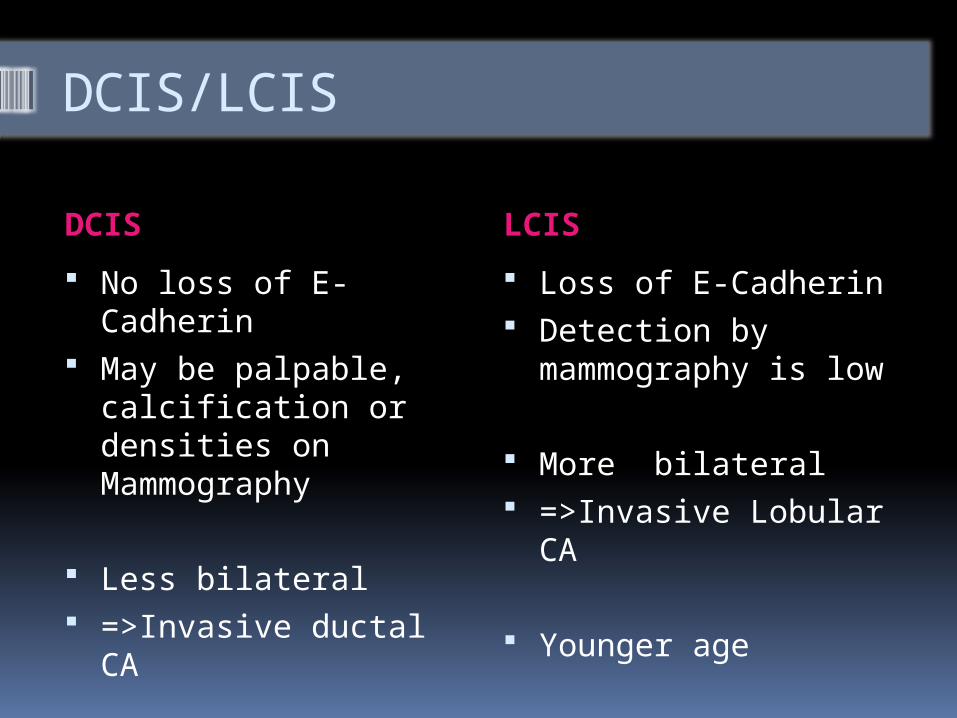
DCIS LCIS
No loss of E-Cadherin May be palpable,
calcification or densities on Mammography
Less bilateral =>Invasive ductal CA
Loss of E-Cadherin Detection by
mammography is low
More bilateral =>Invasive Lobular
CA
Younger age

INVASIVE BREAST CARCINOMA
INVASIVE BREAST CARCINOMA Without mammographic screening,
invasive carcinoma presents as a palpable mass.
Palpable tumors are associated with axillary lymph node metastases in over 50% of patients.
Larger carcinomas may be fixed to the chest wall or cause dimpling of the skin=> Nipple retraction
Lymphedema and thickening of the skin may occur as a result of lymphatic blockade Leading to peau d'orange.
Inflammatory carcinoma refers to tumors that present with a swollen, erythematosus breast. They tend to have poor prognosis.(Commoner with African ancestry)
BREAST CANCER
• Most common histologic type• 70 - 80% of all breast cancer• Diagnosis of exclusion• Breast cancer NOS or NST.
Invasive Ductal Carcinoma
BREAST CANCER
•Grossly forms hard and stellate mass
• Used to be call “scirrhous” ca
• Typically metastasize to bone, liver and lung
Invasive Ductal Carcinoma
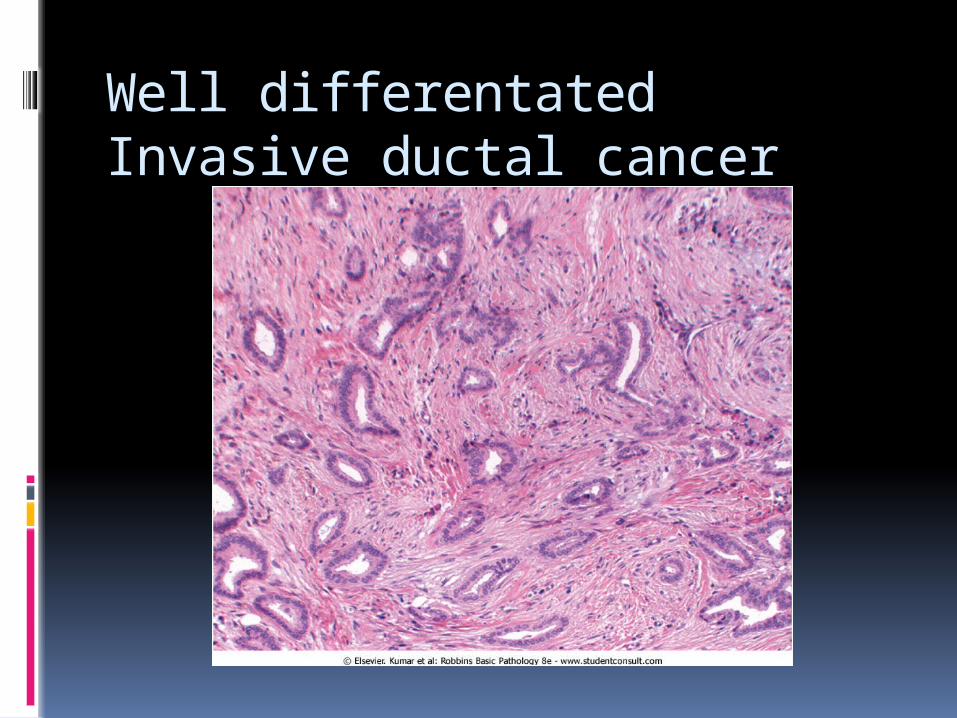
Well differentated Invasive ductal cancer
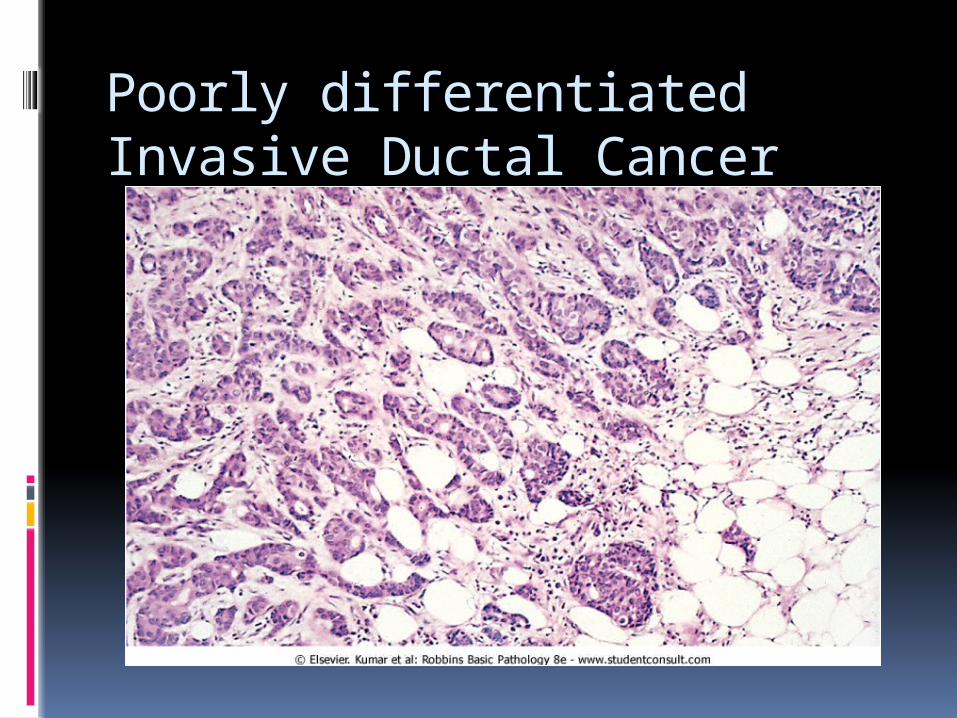
Poorly differentiated Invasive Ductal Cancer
Invasive Lobular Carcinoma• Composed of small cells with linear arrangement
• Commonly forms multifocal and multicentric lesions
• Metastasize to meninges(carcinoma meningitis), serosal
surfaces, ovaries and retroperitoneum.
E-Cadherin mutationsSignet ring cells.
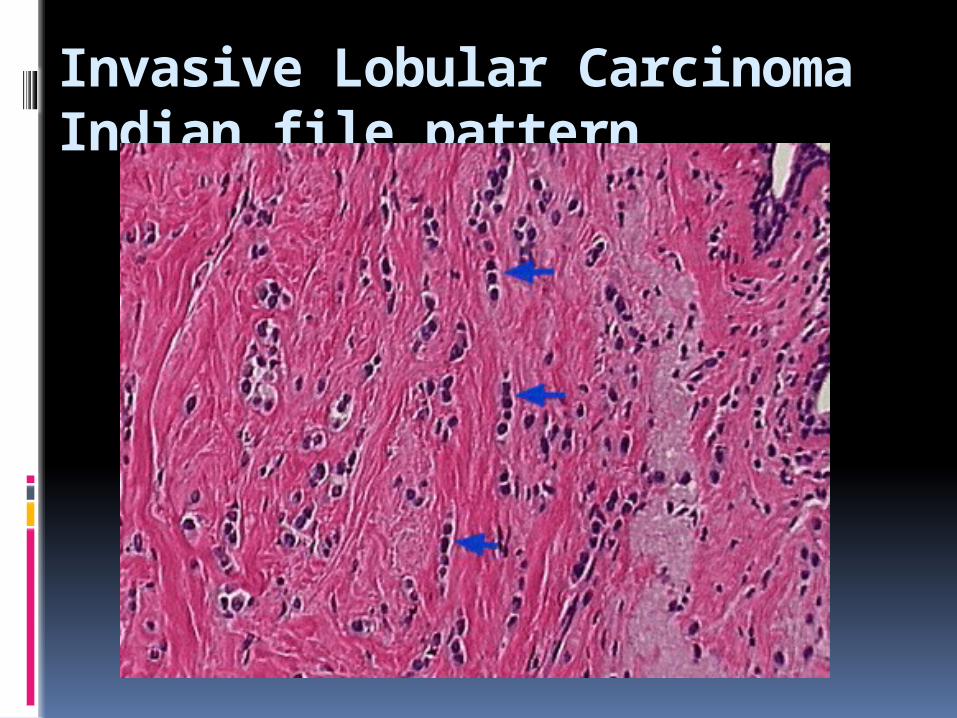
Invasive Lobular CarcinomaIndian file pattern
BREAST CANCER
Tubular Carcinoma
• Variant of ductal carcinoma• Usually small lesion detected by mammogram• 5 - 10% of all breast cancers• Better prognosis• Small tubules composed of neoplastic cells with low grade nuclei.
BREAST CANCER
Mucinous Carcinoma
• 5% of all breast cancers• Older age group• Abundant accumulation of extracellular mucin• Low grade tumor, grows slowly
BREAST CANCER
Medullary Carcinoma• 5% of all breast carcinoma
• Younger age group• Well circumscribed mass• Sheaths of tumor cells with high nuclear grade and intense lymphoplasmacytic infiltrateNo Hormone receptors ,no over expression of her-2 neu. (similar to basal type cancers) better prognosis than NST
Hormone receptors and Her -2/neu
Hormone receptor positive tumors have good response to anti-estrogen therapy such as Tamoxifen but have poor response to chemotherapy.
Tumors arising from the basal group of cells are usually negative for ER,PR and HER-2 /Neu(Triple Negative).This tumors tend to have good prognosis.

Peu d ‘orange

Breast Carcinoma - Schirrous
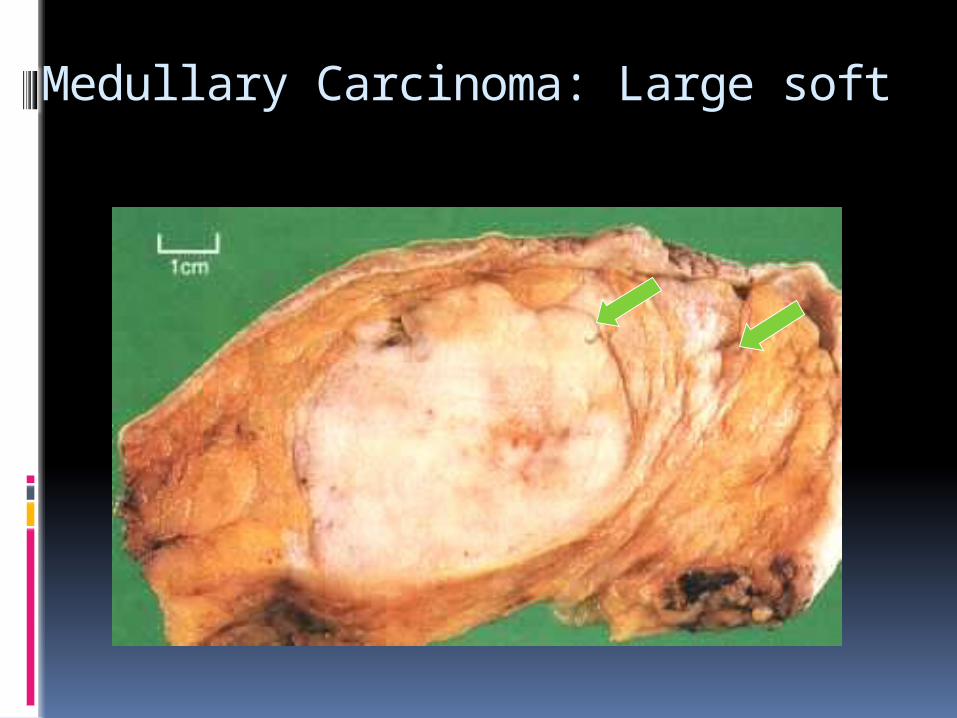
Medullary Carcinoma: Large soft
Stage 1
Tumor < 2.0 cm in greatest dimension
No nodal involvement (N0)
No metastases (M0)
Stage II
Tumor > 2.0 < 5 cm
or Ipsilateral
axillary lymph node (N1)
No Metastasis (M0)
Stage III
Tumor > 5 cm (T3)or ipsilateral axillary lymph nodes
fixed to each other or other structures (N2)
involvement of ipsilateral internal mammary nodes (N3)
Inflammatory carcinoma (T4d)
Stage IV (Metastatic breast cancer)
Any T Any N Metastasis (M1)
PROGNOSTIC FACTORS
• Examination of the primary carcinoma and the axillary lymph nodes. correlated with survival : Invasive carcinoma versus in situ disease.
Cure is possible when the carcinoma has not crossed the basement membrane.
Distant metastases. Cure is rare in the presence of distant metastasis.
Lymph node metastases. Axillary lymph node status (sentinel biopsy) .Most Important prognostic factor for non metastatic disease.
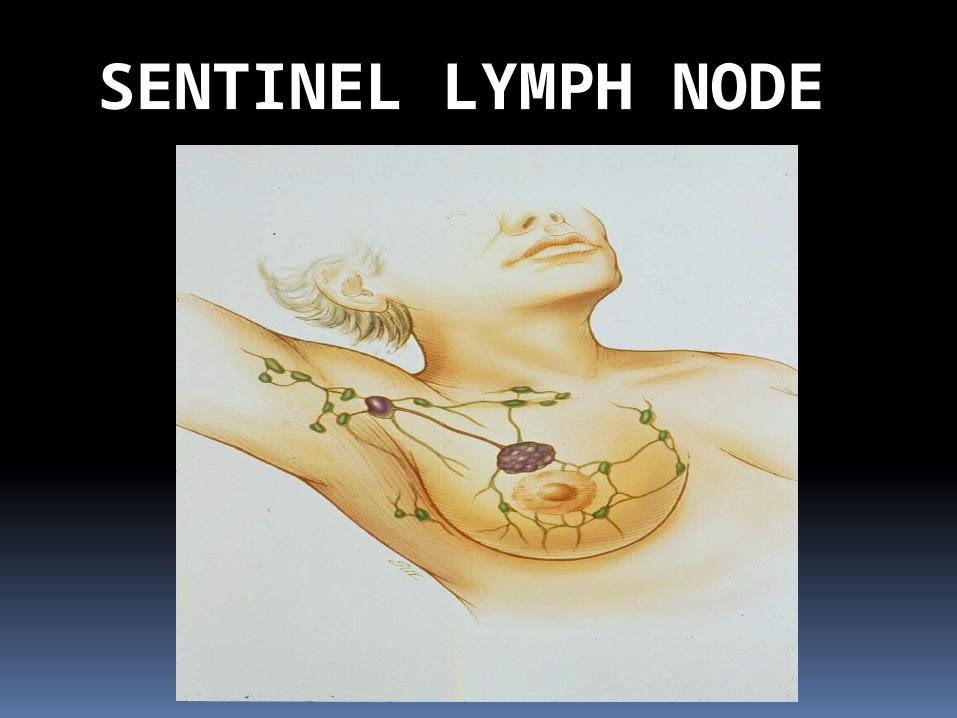
SENTINEL LYMPH NODE
PROGNOSTIC FACTORS
Tumor size. Size of an invasive carcinoma is
the second most important prognostic factor for non metastatic disease.
Risk of axillary lymph node metastases increases with the size of the primary tumor carcinomas <1 cm in size have a 10-year survival rate of over 90%, this drops to 77% survival for cancers >2 cm.Mammographically detected cancers are smaller and less likely to have metastasized.
PROGNOSTIC AND PREDICTIVE FACTORS
Locally advanced disease. Large carcinomas with invasion into skin and muscle are usually beyond surgical salvage.
Inflammatory carcinoma. Presenting with swelling and skin
thickening due to dermal lymphatic involvement have a poor prognosis.
3-year survival rate is only 3% to 10%.
Higher incidence with African descent and younger women

Other prognostic factors
Histology subtypes
Allsubtypes(Tubular,Mucinous,medullary,Lobular,papillary) have a better prognosis compared to the NST or invasive ductal carcinoma.
30 year year survival rate of >60% COMPARED TO <30% OF DUCTAL TUMORS.
Hormone receptors and Her -2/neu Progesterone, Estrogen and Over-
expression of Human epidermal growth factor receptors( HER-2 /neu)
Well differentiated/low grade tumors usually express ER,PR and do not over express HER-2 /neu
Poorly differentiated /high grade tumors do not express ER/PR but usually over express HER-2/neu.
Demonstrated by Immunoperoxidase special stain.
Response to hormonal therapy or targeted Therapy Estrogen and Progesterone receptor
positive tumors have good response to hormonal manipulation.
Tumors that are HER 2/neu positive have shown good response to Trastuzumab (Herceptin)