Embed Size (px)
Citation preview
Section 1
Chapter
1Introduction
Clinical head and neck anatomyfor the ENT anesthesiologistNicole M. Fowler and Joseph Scharpf
IntroductionAn understanding of anatomy is paramount to theability to safely anesthetize the head and neck sur-gery patient. In contrast to other patient populations,the head and neck surgery patient's pathology mayobfuscate normal anatomy and impede or even pre-vent the anesthesiologist from being able to intubatethe patient. Furthermore, recognized anatomic vari-ations may complicate the anesthesiologist's man-agement of the patient. Cooperation among theentire operating team is the key to a successful oper-ation. The surgeon and anesthesiologist must discussthe particular patient's anatomy and specific proced-ural needs prior to each case. Potential airway man-agement options such as routine oral intubation,nasotracheal intubation, awake fiberoptic intubationand even awake tracheotomy must be considered.Contemporary technological advances can enhancethis discussion by including photography and video-graphy. For example, computerized imaging systemsin use in modern operating rooms can be synchron-ized to a server in the otolaryngology clinic to allowthe review of both photographs and videos ofpatients' airways and the extent that they have beenaltered through disease progression. While the addeddimension of visual review integrated into the dis-cussion can be an invaluable adjunct to this teamapproach, always bear in mind that conditions couldhave worsened significantly since the imaging wasperformed.
Patient safety concerns continue to be increasinglyrecognized as a vital component of modern healthcare. At the authors' institution we perform both anoperative “huddle” with the patient awake and a sur-gical “time-out” prior to performing any procedure.The huddle is an ideal time to review the intubation
plan including the use or avoidance of long-actingmuscle relaxants for the case. The huddle process alsoensures that both the anesthesiologist and surgeon arepresent and ready to handle any potential periopera-tive complications. The head and neck surgeonshould be considered an airway specialist and partnerwith the anesthesiologist.
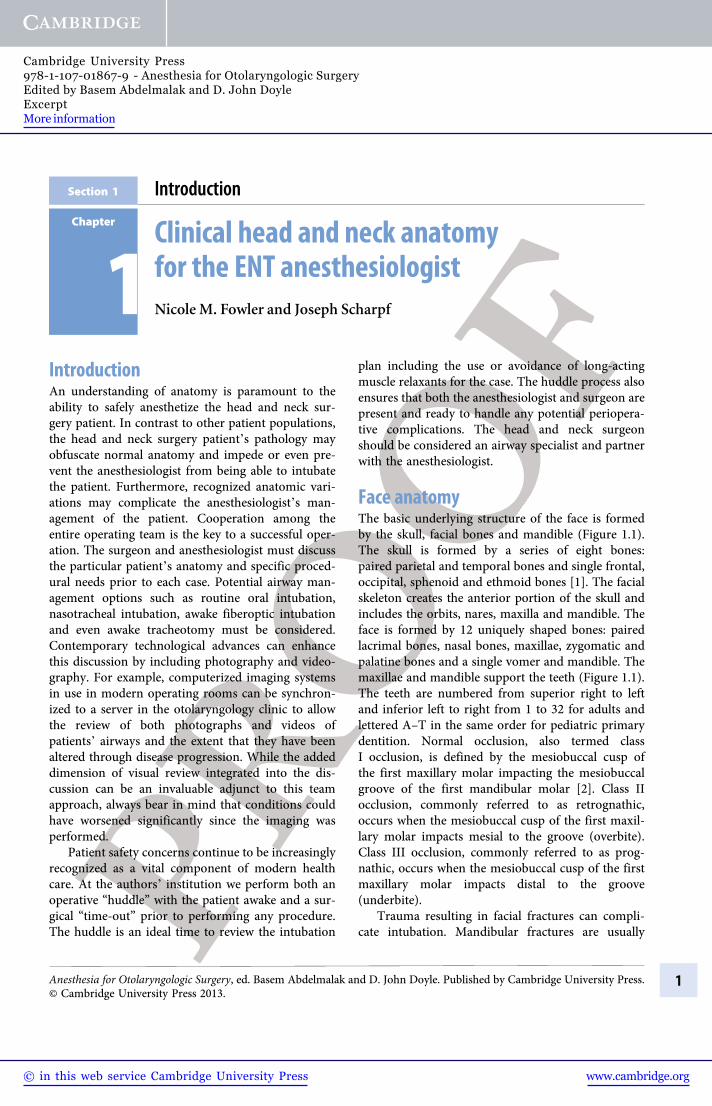
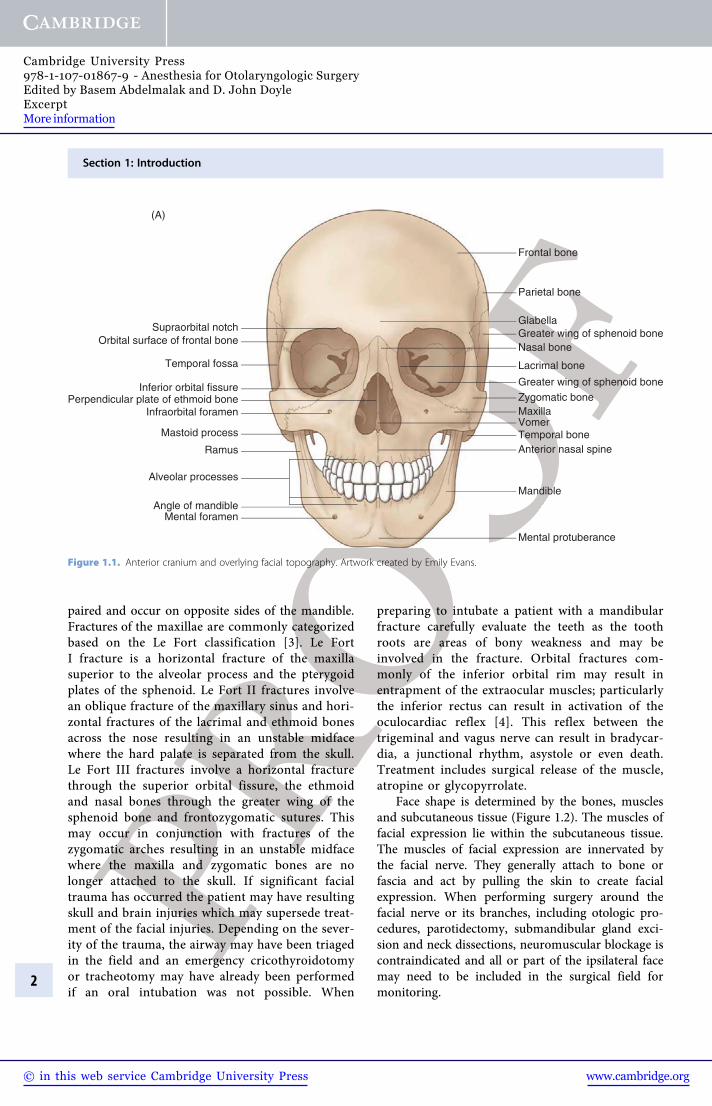
Face anatomyThe basic underlying structure of the face is formedby the skull, facial bones and mandible (Figure 1.1).The skull is formed by a series of eight bones:paired parietal and temporal bones and single frontal,occipital, sphenoid and ethmoid bones [1]. The facialskeleton creates the anterior portion of the skull andincludes the orbits, nares, maxilla and mandible. Theface is formed by 12 uniquely shaped bones: pairedlacrimal bones, nasal bones, maxillae, zygomatic andpalatine bones and a single vomer and mandible. Themaxillae and mandible support the teeth (Figure 1.1).The teeth are numbered from superior right to leftand inferior left to right from 1 to 32 for adults andlettered A–T in the same order for pediatric primarydentition. Normal occlusion, also termed classI occlusion, is defined by the mesiobuccal cusp ofthe first maxillary molar impacting the mesiobuccalgroove of the first mandibular molar [2]. Class IIocclusion, commonly referred to as retrognathic,occurs when the mesiobuccal cusp of the first maxil-lary molar impacts mesial to the groove (overbite).Class III occlusion, commonly referred to as prog-nathic, occurs when the mesiobuccal cusp of the firstmaxillary molar impacts distal to the groove(underbite).
Trauma resulting in facial fractures can compli-cate intubation. Mandibular fractures are usually
Anesthesia for Otolaryngologic Surgery, ed. Basem Abdelmalak and D. John Doyle. Published by Cambridge University Press.© Cambridge University Press 2013.
1
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
paired and occur on opposite sides of the mandible.Fractures of the maxillae are commonly categorizedbased on the Le Fort classification [3]. Le FortI fracture is a horizontal fracture of the maxillasuperior to the alveolar process and the pterygoidplates of the sphenoid. Le Fort II fractures involvean oblique fracture of the maxillary sinus and hori-zontal fractures of the lacrimal and ethmoid bonesacross the nose resulting in an unstable midfacewhere the hard palate is separated from the skull.Le Fort III fractures involve a horizontal fracturethrough the superior orbital fissure, the ethmoidand nasal bones through the greater wing of thesphenoid bone and frontozygomatic sutures. Thismay occur in conjunction with fractures of thezygomatic arches resulting in an unstable midfacewhere the maxilla and zygomatic bones are nolonger attached to the skull. If significant facialtrauma has occurred the patient may have resultingskull and brain injuries which may supersede treat-ment of the facial injuries. Depending on the sever-ity of the trauma, the airway may have been triagedin the field and an emergency cricothyroidotomyor tracheotomy may have already been performedif an oral intubation was not possible. When
preparing to intubate a patient with a mandibularfracture carefully evaluate the teeth as the toothroots are areas of bony weakness and may beinvolved in the fracture. Orbital fractures com-monly of the inferior orbital rim may result inentrapment of the extraocular muscles; particularlythe inferior rectus can result in activation of theoculocardiac reflex [4]. This reflex between thetrigeminal and vagus nerve can result in bradycar-dia, a junctional rhythm, asystole or even death.Treatment includes surgical release of the muscle,atropine or glycopyrrolate.
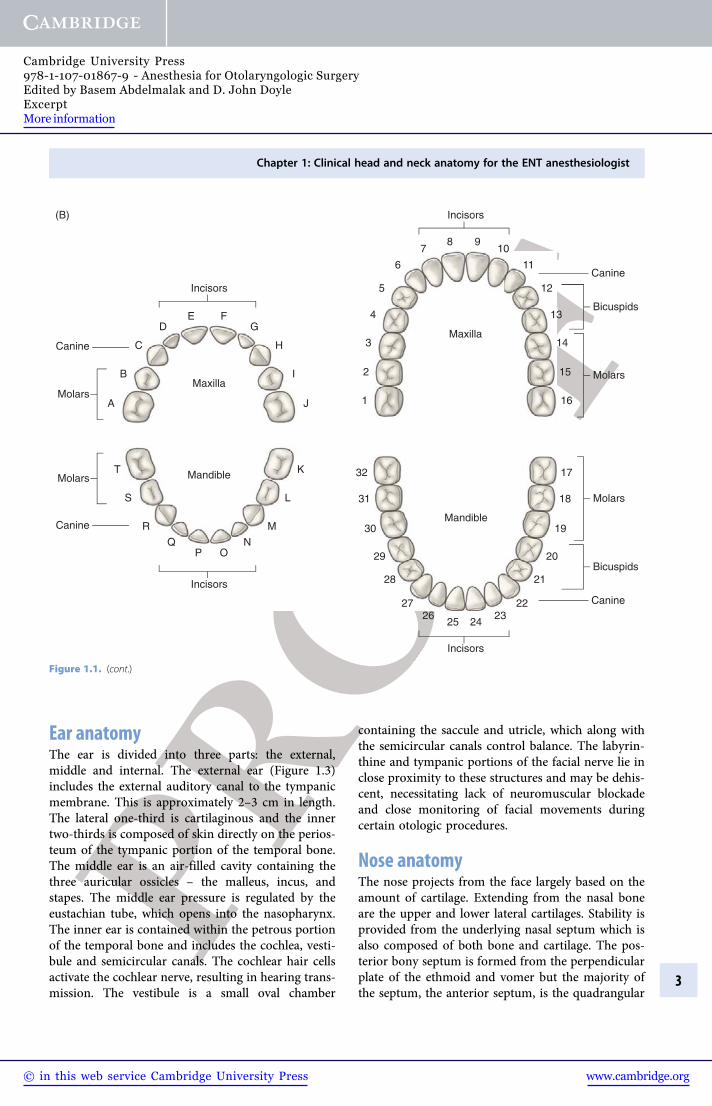
Face shape is determined by the bones, musclesand subcutaneous tissue (Figure 1.2). The muscles offacial expression lie within the subcutaneous tissue.The muscles of facial expression are innervated bythe facial nerve. They generally attach to bone orfascia and act by pulling the skin to create facialexpression. When performing surgery around thefacial nerve or its branches, including otologic pro-cedures, parotidectomy, submandibular gland exci-sion and neck dissections, neuromuscular blockage iscontraindicated and all or part of the ipsilateral facemay need to be included in the surgical field formonitoring.
Perpendicular plate of ethmoid boneInferior orbital fissure
Temporal fossa
Orbital surface of frontal boneSupraorbital notch
(A)
Mental foramenAngle of mandible
Alveolar processes
Ramus
Mastoid process
Infraorbital foramen
Frontal bone
Parietal bone
Greater wing of sphenoid boneGlabella
Nasal bone
Lacrimal bone
Greater wing of sphenoid boneZygomatic boneMaxillaVomerTemporal bone
Mandible
Anterior nasal spine
Mental protuberance
Figure 1.1. Anterior cranium and overlying facial topography. Artwork created by Emily Evans.
2
Section 1: Introduction
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
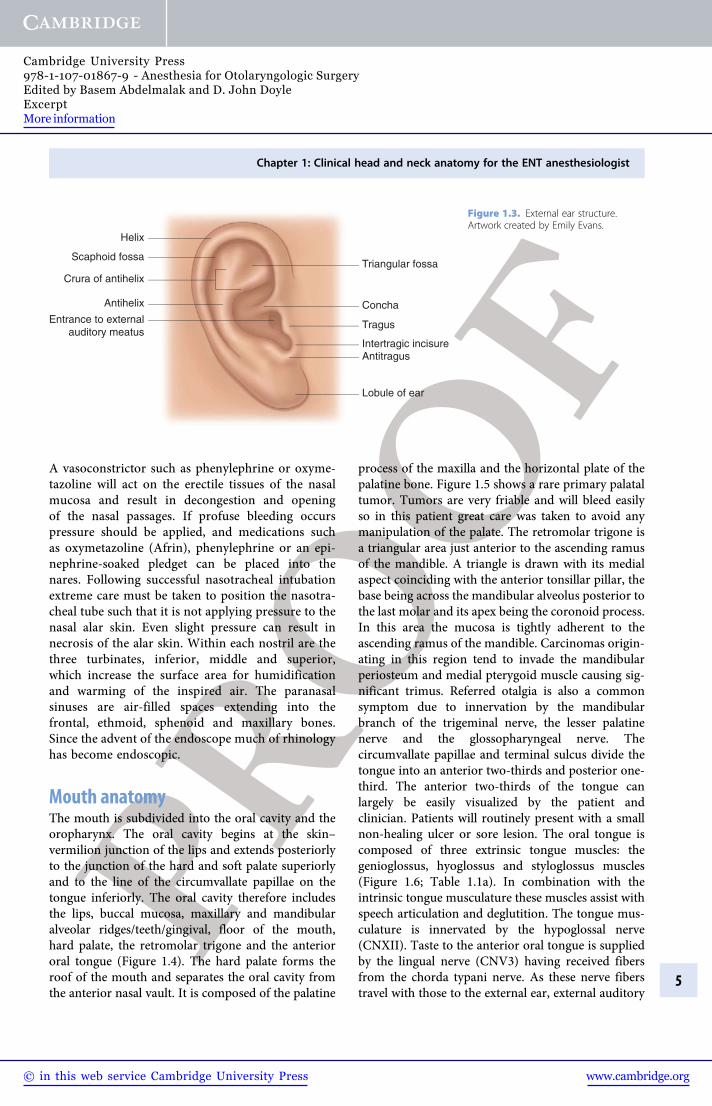
Ear anatomyThe ear is divided into three parts: the external,middle and internal. The external ear (Figure 1.3)includes the external auditory canal to the tympanicmembrane. This is approximately 2–3 cm in length.The lateral one-third is cartilaginous and the innertwo-thirds is composed of skin directly on the perios-teum of the tympanic portion of the temporal bone.The middle ear is an air-filled cavity containing thethree auricular ossicles – the malleus, incus, andstapes. The middle ear pressure is regulated by theeustachian tube, which opens into the nasopharynx.The inner ear is contained within the petrous portionof the temporal bone and includes the cochlea, vesti-bule and semicircular canals. The cochlear hair cellsactivate the cochlear nerve, resulting in hearing trans-mission. The vestibule is a small oval chamber
containing the saccule and utricle, which along withthe semicircular canals control balance. The labyrin-thine and tympanic portions of the facial nerve lie inclose proximity to these structures and may be dehis-cent, necessitating lack of neuromuscular blockadeand close monitoring of facial movements duringcertain otologic procedures.
Nose anatomyThe nose projects from the face largely based on theamount of cartilage. Extending from the nasal boneare the upper and lower lateral cartilages. Stability isprovided from the underlying nasal septum which isalso composed of both bone and cartilage. The pos-terior bony septum is formed from the perpendicularplate of the ethmoid and vomer but the majority ofthe septum, the anterior septum, is the quadrangular
1
2
3
4
5
6
78
16
17
15
18
14
19
13
20
21
2223
24
32
31
30
29
28
2726
25
A
B
C
DE
J
KT
LS
MR
NQOP
I
H
GF
12
11
109
Maxilla
Maxilla
Incisors
Incisors
Incisors
Incisors
Canine
Canine
(B)
Canine
Canine
Bicuspids
Bicuspids
Molars
Molars
Molars
Molars
Mandible
Mandible
Figure 1.1. (cont.)
Chapter 1: Clinical head and neck anatomy for the ENT anesthesiologist
3
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
cartilage. The nasal ala are supported by U-shapedalar cartilage which is free and mobile, allowing thedilatation or constriction of each nostril. In prepar-ation for a nasotracheal intubation or a fiberopticintubation the nares should be examined for anyseptal deviation. The degree and site of deviationmay help decide which nostril to use for the intub-ation. Care must be taken when placing any foreignobject into the nose because of its robust blood
supply. The anterior nasal septal area is referred toas Kiesselbach's plexus and is the site of a capillaryanastomosis from the sphenopalatine artery, anteriorand posterior ethmoid arteries, greater palatine arteryand the superior labial artery. Any object placed intothe nose should be directed along the floor of thenose, which is wider than the roof. In preparationfor any nasal manipulation the nasal mucosa shouldbe treated with a vasoconstrictor and anesthetic.
Orbicularis oculiOrbital part
Palpebral part
Levator labii superioris
Levator labii superiorisaleque nasii
Zygomaticus minor
Zygomaticus major
Platysma
Sternocleidomastoid
Orbicularis oris
Procerus
Depressor anguli oris Depressor labii inferioris
Frontalis
Temporalis
Nasalis
Risorius
Mentalis
Masseter
Figure 1.2. Muscles of facial expression. Artwork created by Emily Evans.
Section 1: Introduction
4
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
A vasoconstrictor such as phenylephrine or oxyme-tazoline will act on the erectile tissues of the nasalmucosa and result in decongestion and openingof the nasal passages. If profuse bleeding occurspressure should be applied, and medications suchas oxymetazoline (Afrin), phenylephrine or an epi-nephrine-soaked pledget can be placed into thenares. Following successful nasotracheal intubationextreme care must be taken to position the nasotra-cheal tube such that it is not applying pressure to thenasal alar skin. Even slight pressure can result innecrosis of the alar skin. Within each nostril are thethree turbinates, inferior, middle and superior,which increase the surface area for humidificationand warming of the inspired air. The paranasalsinuses are air-filled spaces extending into thefrontal, ethmoid, sphenoid and maxillary bones.Since the advent of the endoscope much of rhinologyhas become endoscopic.
Mouth anatomyThe mouth is subdivided into the oral cavity and theoropharynx. The oral cavity begins at the skin–vermilion junction of the lips and extends posteriorlyto the junction of the hard and soft palate superiorlyand to the line of the circumvallate papillae on thetongue inferiorly. The oral cavity therefore includesthe lips, buccal mucosa, maxillary and mandibularalveolar ridges/teeth/gingival, floor of the mouth,hard palate, the retromolar trigone and the anteriororal tongue (Figure 1.4). The hard palate forms theroof of the mouth and separates the oral cavity fromthe anterior nasal vault. It is composed of the palatine
process of the maxilla and the horizontal plate of thepalatine bone. Figure 1.5 shows a rare primary palataltumor. Tumors are very friable and will bleed easilyso in this patient great care was taken to avoid anymanipulation of the palate. The retromolar trigone isa triangular area just anterior to the ascending ramusof the mandible. A triangle is drawn with its medialaspect coinciding with the anterior tonsillar pillar, thebase being across the mandibular alveolus posterior tothe last molar and its apex being the coronoid process.In this area the mucosa is tightly adherent to theascending ramus of the mandible. Carcinomas origin-ating in this region tend to invade the mandibularperiosteum and medial pterygoid muscle causing sig-nificant trimus. Referred otalgia is also a commonsymptom due to innervation by the mandibularbranch of the trigeminal nerve, the lesser palatinenerve and the glossopharyngeal nerve. Thecircumvallate papillae and terminal sulcus divide thetongue into an anterior two-thirds and posterior one-third. The anterior two-thirds of the tongue canlargely be easily visualized by the patient andclinician. Patients will routinely present with a smallnon-healing ulcer or sore lesion. The oral tongue iscomposed of three extrinsic tongue muscles: thegenioglossus, hyoglossus and styloglossus muscles(Figure 1.6; Table 1.1a). In combination with theintrinsic tongue musculature these muscles assist withspeech articulation and deglutition. The tongue mus-culature is innervated by the hypoglossal nerve(CNXII). Taste to the anterior oral tongue is suppliedby the lingual nerve (CNV3) having received fibersfrom the chorda typani nerve. As these nerve fiberstravel with those to the external ear, external auditory
Helix
Scaphoid fossa
Crura of antihelix
Antihelix
Antitragus
Triangular fossa
Tragus
Concha
Intertragic incisure
Lobule of ear
Entrance to externalauditory meatus
Figure 1.3. External ear structure.Artwork created by Emily Evans.
Chapter 1: Clinical head and neck anatomy for the ENT anesthesiologist
5
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
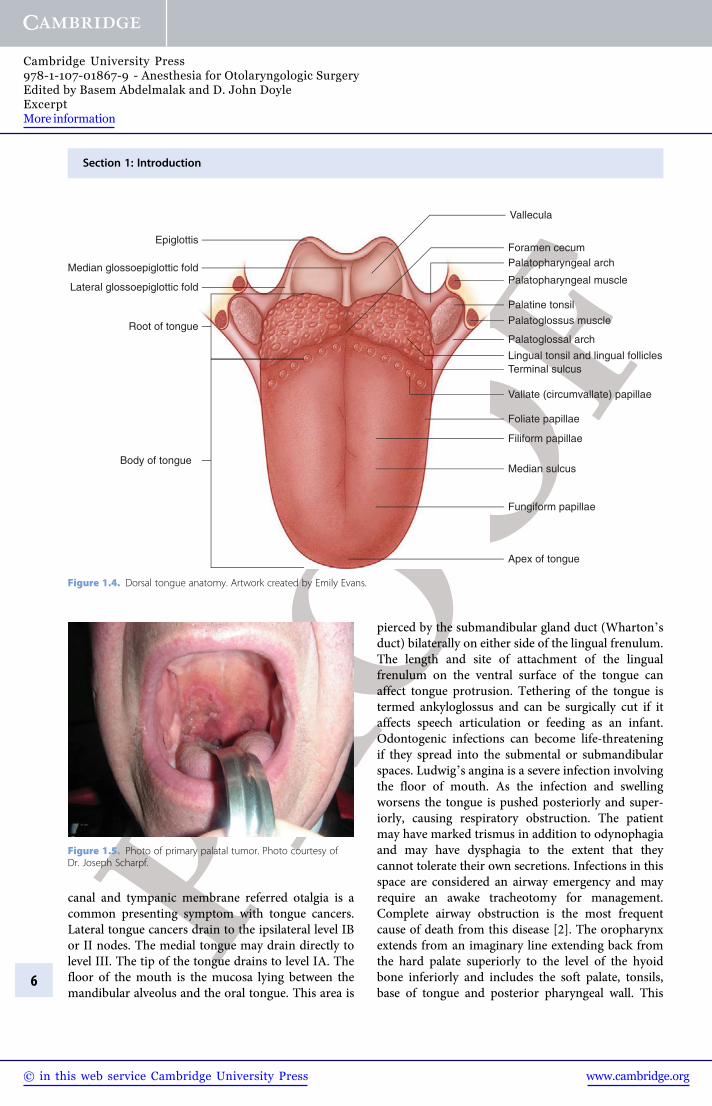
canal and tympanic membrane referred otalgia is acommon presenting symptom with tongue cancers.Lateral tongue cancers drain to the ipsilateral level IBor II nodes. The medial tongue may drain directly tolevel III. The tip of the tongue drains to level IA. Thefloor of the mouth is the mucosa lying between themandibular alveolus and the oral tongue. This area is
pierced by the submandibular gland duct (Wharton'sduct) bilaterally on either side of the lingual frenulum.The length and site of attachment of the lingualfrenulum on the ventral surface of the tongue canaffect tongue protrusion. Tethering of the tongue istermed ankyloglossus and can be surgically cut if itaffects speech articulation or feeding as an infant.Odontogenic infections can become life-threateningif they spread into the submental or submandibularspaces. Ludwig's angina is a severe infection involvingthe floor of mouth. As the infection and swellingworsens the tongue is pushed posteriorly and super-iorly, causing respiratory obstruction. The patientmay have marked trismus in addition to odynophagiaand may have dysphagia to the extent that theycannot tolerate their own secretions. Infections in thisspace are considered an airway emergency and mayrequire an awake tracheotomy for management.Complete airway obstruction is the most frequentcause of death from this disease [2]. The oropharynxextends from an imaginary line extending back fromthe hard palate superiorly to the level of the hyoidbone inferiorly and includes the soft palate, tonsils,base of tongue and posterior pharyngeal wall. This
Epiglottis
Median glossoepiglottic fold
Lateral glossoepiglottic fold
Root of tongue
Body of tongue
Vallecula
Foramen cecumPalatopharyngeal arch
Palatopharyngeal muscle
Palatine tonsil
Palatoglossus muscle
Palatoglossal arch
Lingual tonsil and lingual folliclesTerminal sulcus
Vallate (circumvallate) papillae
Foliate papillae
Filiform papillae
Median sulcus
Fungiform papillae
Apex of tongue
Figure 1.4. Dorsal tongue anatomy. Artwork created by Emily Evans.
Figure 1.5. Photo of primary palatal tumor. Photo courtesy ofDr. Joseph Scharpf.
Section 1: Introduction
6
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
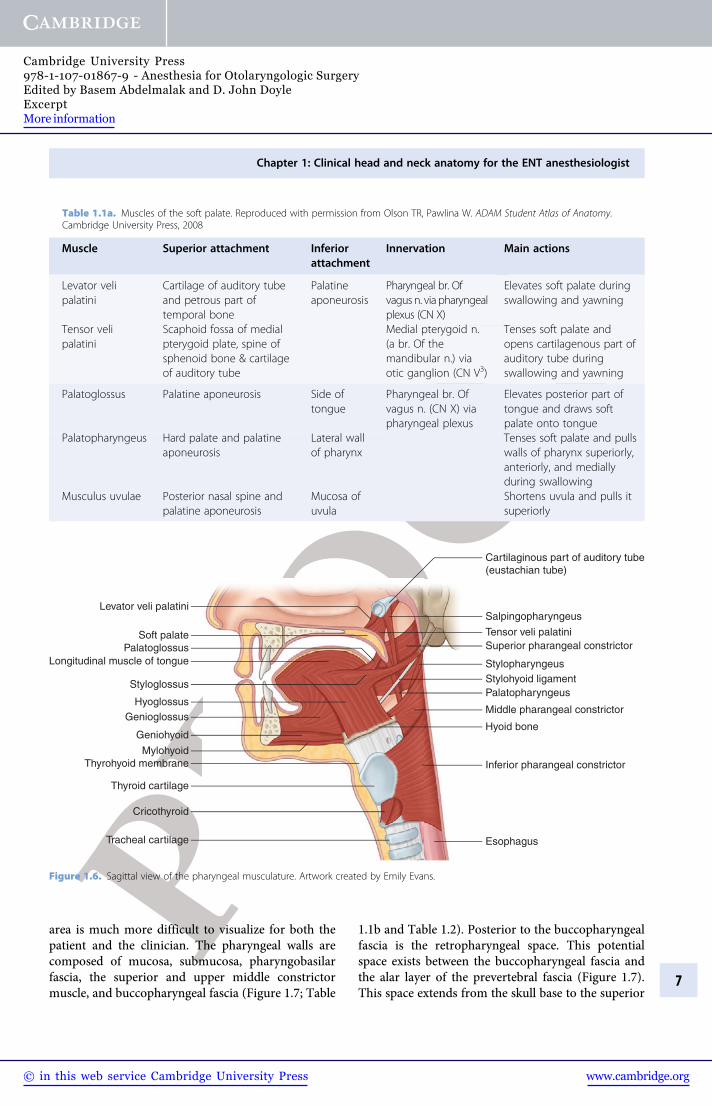
area is much more difficult to visualize for both thepatient and the clinician. The pharyngeal walls arecomposed of mucosa, submucosa, pharyngobasilarfascia, the superior and upper middle constrictormuscle, and buccopharyngeal fascia (Figure 1.7; Table
1.1b and Table 1.2). Posterior to the buccopharyngealfascia is the retropharyngeal space. This potentialspace exists between the buccopharyngeal fascia andthe alar layer of the prevertebral fascia (Figure 1.7).This space extends from the skull base to the superior
Cartilaginous part of auditory tube(eustachian tube)
Salpingopharyngeus
Palatopharyngeus
Stylopharyngeus
Superior pharangeal constrictor
Middle pharangeal constrictor
Inferior pharangeal constrictor
Hyoid bone
Esophagus
Stylohyoid ligament
Levator veli palatini
Tensor veli palatini
PalatoglossusSoft palate
Longitudinal muscle of tongue
HyoglossusGenioglossus
Geniohyoid
Cricothyroid
Thyroid cartilage
Tracheal cartilage
Thyrohyoid membraneMylohyoid
Styloglossus
Figure 1.6. Sagittal view of the pharyngeal musculature. Artwork created by Emily Evans.
Table 1.1a. Muscles of the soft palate. Reproduced with permission from Olson TR, Pawlina W. ADAM Student Atlas of Anatomy.Cambridge University Press, 2008
Muscle Superior attachment Inferiorattachment
Innervation Main actions
Levator velipalatini
Cartilage of auditory tubeand petrous part oftemporal bone
Palatineaponeurosis
Pharyngeal br. Ofvagus n. via pharyngealplexus (CN X)
Elevates soft palate duringswallowing and yawning
Tensor velipalatini
Scaphoid fossa of medialpterygoid plate, spine ofsphenoid bone & cartilageof auditory tube
Medial pterygoid n.(a br. Of themandibular n.) viaotic ganglion (CN V3)
Tenses soft palate andopens cartilagenous part ofauditory tube duringswallowing and yawning
Palatoglossus Palatine aponeurosis Side oftongue
Pharyngeal br. Ofvagus n. (CN X) viapharyngeal plexus
Elevates posterior part oftongue and draws softpalate onto tongue
Palatopharyngeus Hard palate and palatineaponeurosis
Lateral wallof pharynx
Tenses soft palate and pullswalls of pharynx superiorly,anteriorly, and mediallyduring swallowing
Musculus uvulae Posterior nasal spine andpalatine aponeurosis
Mucosa ofuvula
Shortens uvula and pulls itsuperiorly
Chapter 1: Clinical head and neck anatomy for the ENT anesthesiologist
7
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
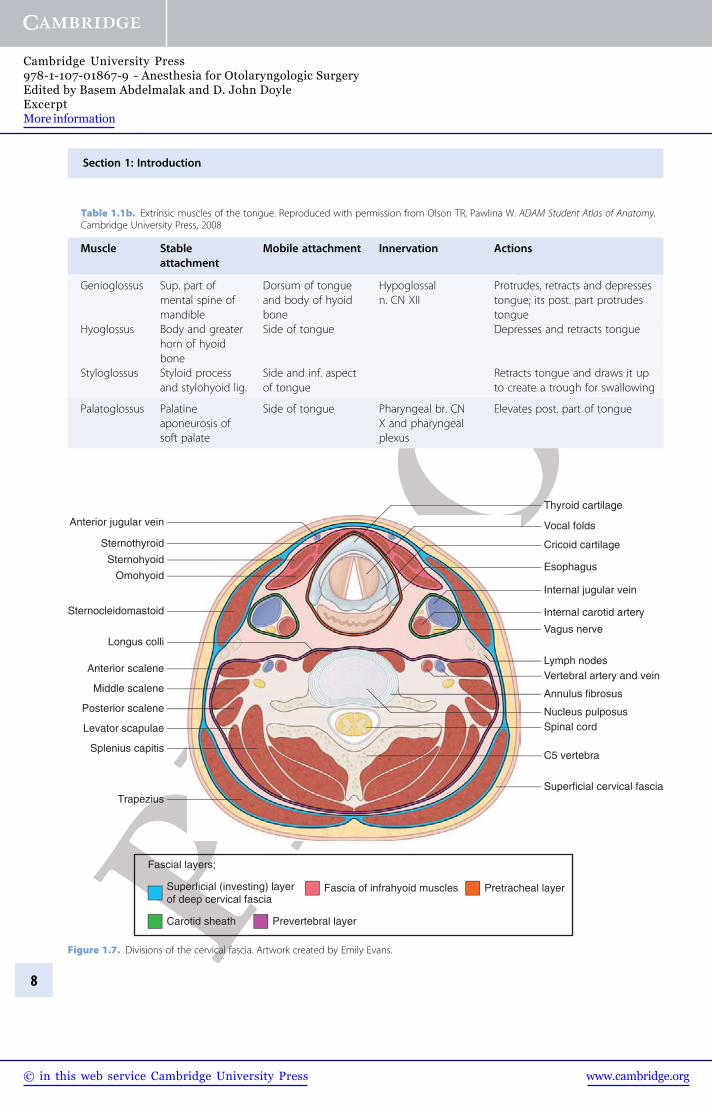
Table 1.1b. Extrinsic muscles of the tongue. Reproduced with permission from Olson TR, Pawlina W. ADAM Student Atlas of Anatomy.Cambridge University Press, 2008
Muscle Stableattachment
Mobile attachment Innervation Actions
Genioglossus Sup. part ofmental spine ofmandible
Dorsum of tongueand body of hyoidbone
Hypoglossaln. CN XII
Protrudes, retracts and depressestongue; its post. part protrudestongue
Hyoglossus Body and greaterhorn of hyoidbone
Side of tongue Depresses and retracts tongue
Styloglossus Styloid processand stylohyoid lig.
Side and inf. aspectof tongue
Retracts tongue and draws it upto create a trough for swallowing
Palatoglossus Palatineaponeurosis ofsoft palate
Side of tongue Pharyngeal br. CNX and pharyngealplexus
Elevates post. part of tongue
Thyroid cartilage
Esophagus
Cricoid cartilage
Vocal folds
Sternothyroid
Anterior jugular vein
Sternohyoid
Omohyoid
Sternocleidomastoid
Anterior scalene
Middle scalene
Posterior scalene
Levator scapulae
Splenius capitis
Trapezius
Longus colliVagus nerve
Annulus fibrosus
Spinal cord
C5 vertebra
Superficial cervical fascia
Nucleus pulposus
Vertebral artery and veinLymph nodes
Internal jugular vein
Internal carotid artery
Fascial layers;
Prevertebral layerCarotid sheath
Superficial (investing) layerof deep cervical fascia
Pretracheal layerFascia of infrahyoid muscles
Figure 1.7. Divisions of the cervical fascia. Artwork created by Emily Evans.
Section 1: Introduction
8
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
mediastinum. Contingent upon the patient, his or herclinical history, and the location of a retropharyngealspace abscess in relation to the great vessels (carotidartery, internal jugular vein), the abscess may beamenable to transoral drainage versus a more trad-itional transcervical drainage. The tonsils are housedwithin a fossa created by two muscles, the anteriortonsillar pillar formed from the palatoglossus muscleand the posterior tonsillar pillar by the palatopharyn-geal muscle. A small primary tonsillar or base oftongue tumor may be asymptomatic and present withmetastatic cervical lymphadenopathy. Careful exam-ination of the oral excursion is advised in any patientwith a tonsillar tumor as invasion into the lateralpterygoid muscle may result in trismus, which willnot improve with muscular relaxation. The soft palateis composed of the levator veli palatini, tensor velipalatini, musculus uvulae and tonsillar pillars musclesas above. The base of the tongue extends fromthe circumvallate papillae to the glossoepiglottic fold.The lingual tonsils are found laterally and lie in a
superficial plane creating an irregularity to thesurface. Alternatively, base of tongue tumors maygrow to very large sizes with minimal symptoms.Patients with a large base of tongue tumor may beable to maintain their airway but extreme cautionshould be taken prior to induction. An awake trache-otomy should be considered based on the anesthesiol-gist's experience and comfort with awake fiberopticintubation.
The throat or pharynx is subdivided into thelarynx and the hypopharynx. The larynx is furthersubdivided into three spaces: the supraglottis,glottis and subglottis. Furthermore the larynx is com-posed of nine cartilages joined by ligaments andmembranes: three single cartilages: thyroid, cricoidand epiglottic; and three paried cartilages: arytenoid,corniculate and cuneiform (Figure 1.8). The largest ofthe cartilages, the thyroid cartilage, was so namedfrom the Greek word thyreos, or shield, due to itsshield-like appearance and its main function beingthat of protection of the vocal cords. It is composed
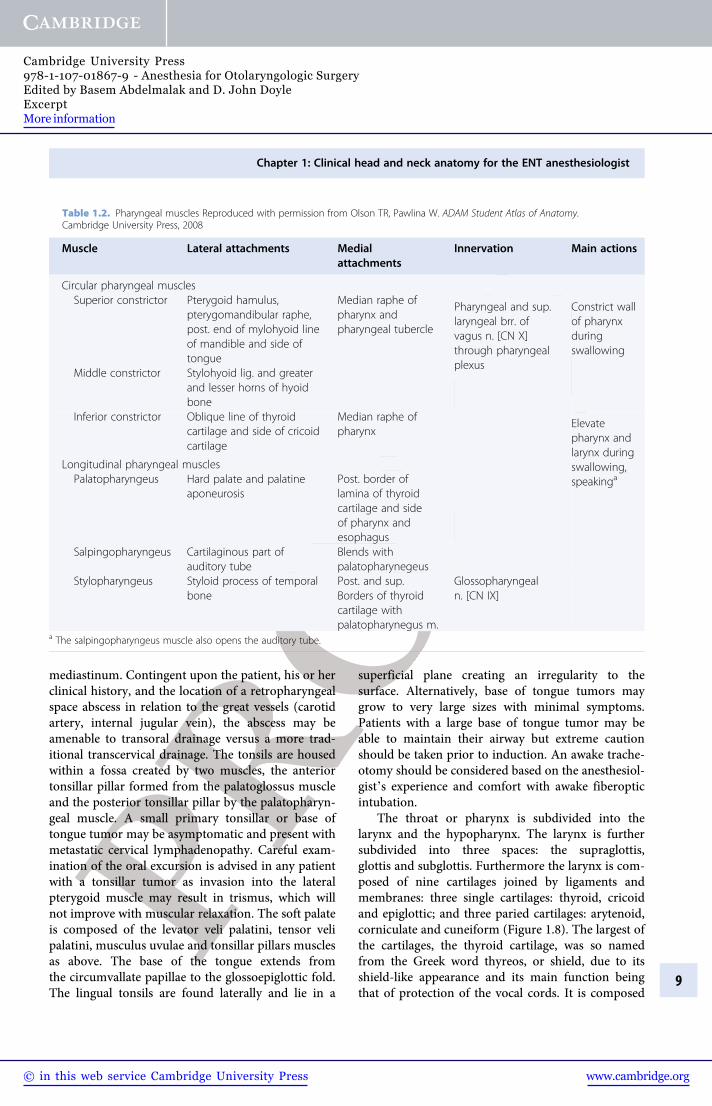
Table 1.2. Pharyngeal muscles Reproduced with permission from Olson TR, Pawlina W. ADAM Student Atlas of Anatomy.Cambridge University Press, 2008
Muscle Lateral attachments Medialattachments
Innervation Main actions
Circular pharyngeal musclesSuperior constrictor Pterygoid hamulus,
pterygomandibular raphe,post. end of mylohyoid lineof mandible and side oftongue
Median raphe ofpharynx andpharyngeal tubercle
Pharyngeal and sup.laryngeal brr. ofvagus n. [CN X]through pharyngealplexus
Constrict wallof pharynxduringswallowing
Middle constrictor Stylohyoid lig. and greaterand lesser horns of hyoidbone
Median raphe ofpharynx
Inferior constrictor Oblique line of thyroidcartilage and side of cricoidcartilage
Elevatepharynx andlarynx duringswallowing,speakinga
Longitudinal pharyngeal musclesPalatopharyngeus Hard palate and palatine
aponeurosisPost. border oflamina of thyroidcartilage and sideof pharynx andesophagus
Salpingopharyngeus Cartilaginous part ofauditory tube
Blends withpalatopharynegeus
Stylopharyngeus Styloid process of temporalbone
Post. and sup.Borders of thyroidcartilage withpalatopharynegus m.
Glossopharyngealn. [CN IX]
a The salpingopharyngeus muscle also opens the auditory tube.
Chapter 1: Clinical head and neck anatomy for the ENT anesthesiologist
9
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information
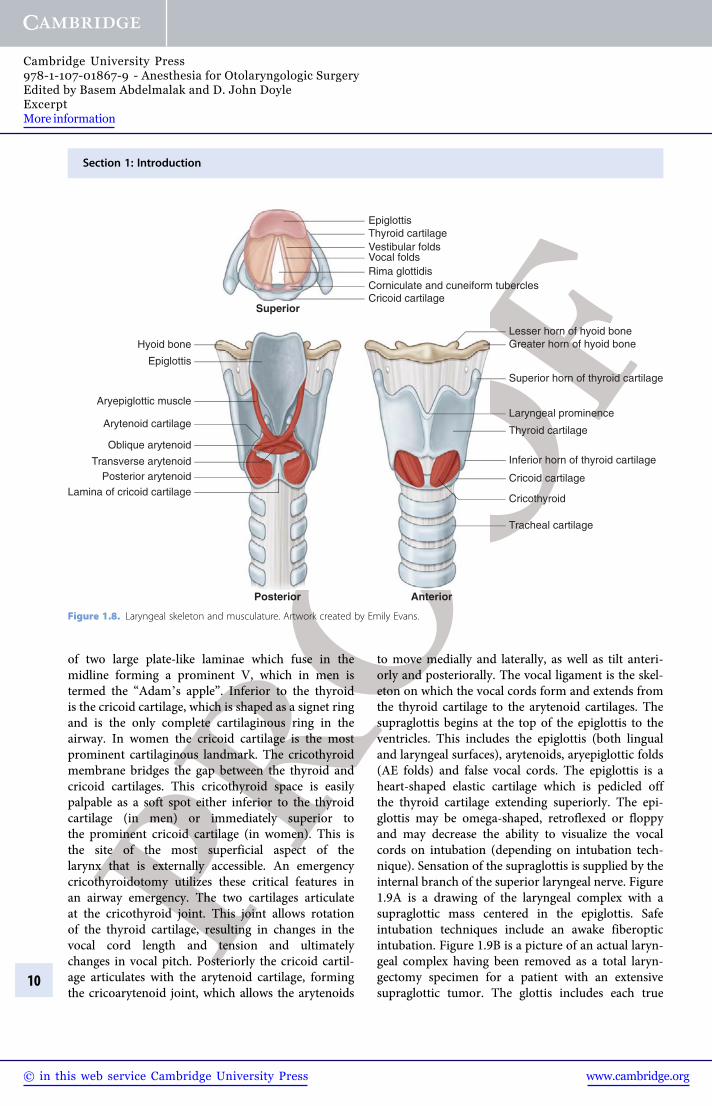
of two large plate-like laminae which fuse in themidline forming a prominent V, which in men istermed the “Adam's apple”. Inferior to the thyroidis the cricoid cartilage, which is shaped as a signet ringand is the only complete cartilaginous ring in theairway. In women the cricoid cartilage is the mostprominent cartilaginous landmark. The cricothyroidmembrane bridges the gap between the thyroid andcricoid cartilages. This cricothyroid space is easilypalpable as a soft spot either inferior to the thyroidcartilage (in men) or immediately superior tothe prominent cricoid cartilage (in women). This isthe site of the most superficial aspect of thelarynx that is externally accessible. An emergencycricothyroidotomy utilizes these critical features inan airway emergency. The two cartilages articulateat the cricothyroid joint. This joint allows rotationof the thyroid cartilage, resulting in changes in thevocal cord length and tension and ultimatelychanges in vocal pitch. Posteriorly the cricoid cartil-age articulates with the arytenoid cartilage, formingthe cricoarytenoid joint, which allows the arytenoids
to move medially and laterally, as well as tilt anteri-orly and posteriorally. The vocal ligament is the skel-eton on which the vocal cords form and extends fromthe thyroid cartilage to the arytenoid cartilages. Thesupraglottis begins at the top of the epiglottis to theventricles. This includes the epiglottis (both lingualand laryngeal surfaces), arytenoids, aryepiglottic folds(AE folds) and false vocal cords. The epiglottis is aheart-shaped elastic cartilage which is pedicled offthe thyroid cartilage extending superiorly. The epi-glottis may be omega-shaped, retroflexed or floppyand may decrease the ability to visualize the vocalcords on intubation (depending on intubation tech-nique). Sensation of the supraglottis is supplied by theinternal branch of the superior laryngeal nerve. Figure1.9A is a drawing of the laryngeal complex with asupraglottic mass centered in the epiglottis. Safeintubation techniques include an awake fiberopticintubation. Figure 1.9B is a picture of an actual laryn-geal complex having been removed as a total laryn-gectomy specimen for a patient with an extensivesupraglottic tumor. The glottis includes each true
Epiglottis
Posterior arytenoid
Lamina of cricoid cartilage
Aryepiglottic muscle
Oblique arytenoid
Arytenoid cartilage
Transverse arytenoid
Epiglottis
Hyoid boneLesser horn of hyoid boneGreater horn of hyoid bone
Superior horn of thyroid cartilage
Inferior horn of thyroid cartilage
Tracheal cartilage
AnteriorPosterior
Superior
Cricothyroid
Cricoid cartilage
Thyroid cartilage
Thyroid cartilage
Cricoid cartilageCorniculate and cuneiform tubercles
Vocal foldsVestibular folds
Rima glottidis
Laryngeal prominence
Figure 1.8. Laryngeal skeleton and musculature. Artwork created by Emily Evans.
Section 1: Introduction
10
www.cambridge.org© in this web service Cambridge University Press
Cambridge University Press978-1-107-01867-9 - Anesthesia for Otolaryngologic SurgeryEdited by Basem Abdelmalak and D. John DoyleExcerptMore information





![1 Introduction - Cambridge University Pressassets.cambridge.org/97811070/37267/excerpt/...1 Introduction Bird,bat,andinsectflighthasfascinatedhumansformanycenturies.Asenthusiasti-callyobservedbyDial[1],mostspeciesofanimalsfly.Basedonhisacuteobservation](https://img.pdfslide.us/doc/110x75/5ad5c8627f8b9a6d708d4aa8/1-introduction-cambridge-university-introduction-birdbatandinsectighthasfascinatedhumansformanycenturiesasenthusiasti-callyobservedbydial1mostspeciesofanimalsybasedonhisacuteobservation.jpg)























