Embed Size (px)
Citation preview

Introduction: Cholesteatoma is an abnormal growth of squamous epithelium in the middle ear and mastoid which destroy important structures in the temporal bone. The presence of cholesteatoma requires surgical intervention and the main goal is to achieve a safe, dry ear and to improve the hearing. The extension of surgery depends on the size of the cholesteatoma. Methods: 875 patients were treated for cholesteatoma in our department between 2001 and 2011, 213 pediatric patients. We performed both, open and closed technique, depending on disease extension, bone erosion and complications, followed by second-look surgery in most of the closed-technique cases. Results: The closed technique was the treatment of choice in 69,2% of cases, most of them uncomplicated cholesteatomas. In 30,6% we've chose the open technique for different reasons. The second look surgery was done in 57,3% of cases after one and a half or two years. 27,1% of patients were lose of follow-up program after the first years. Residual cholesteatomas were noticed in 17% of cases and the recurrent cholesteatomas were operated in 32% of cases. After the surgery the air-bone gape has improved in 67.1% of cases because of tympanoplasty with autologous graft or different types of prosthesis. In some cases we've used the BAHA prosthesis with good results. Conclusions: Cholesteatoma is a serious condition which affects both children and adults. The second-look control in closed technique should be done after one-one and a half year. Closed technique is recommended in order to restore the function of the ear, the hearing, which is very important for a normal development and a proper quality of life.
It was a retrospective study of patients treated in Cluj-Napoca’s County Emergency Hospital, ENT Department , since 2001 to 2010 for chronic otitis media with cholesteatoma We found in our records 875 ear surgeries for chronic otitis media with cholesteatoma , 213 pediatric patients and 662 adults. Surgical techniques used:
Canal wall-down tympanomastoidectomy Canal wall-up tympanomastoidectomy
We included in our study only patients with cholesteatoma, or with deep and uncontrollable RP, with recurrent disease, and second-look surgeries for patients operated before in our department. We included also the primary cholesteatoma a very uncommon disease, with a low incidence. We excluded from our study the other types of chronic otitis media without cholesteatoma, or the cholesteatoma occurred after ear surgery.
Intraoperative findings Retraction pocket: 6.8±1.87% Retraction pocket + ossicular chain erosion: 12.4±5.42% Tympanic membrane perforation
Pars flaccida: 12.2±1.87% Posterior-superior quadrant 15.1±1.66% Total: 25±3.01%
Semicircular canal erosion 3.1±1.01% Facial nerve dehiscence: 9.10±1.28% Facial nerve palsy: 1.8±0.78% Sigmoid sinus thrombosis: 2.7±0.94% Subdural/cerebral abscess: 2.3±0.67% Good clinical results included dry open cavities or closed cavity with tympanoplasty. Recurrences occurred both in closed and in open techniques. In some cases second surgery was performed because of complications. Regarding the hearing, in closed techniques we used incus, cartilage or titanium prosthesis for ossicular chain reconstruction and perichondrium, cartilage or temporal fascia for tympanic membrane. In some cases we used BAHA prosthesis.
Our study reveals that in the last years the cholesteatoma was diagnosed in earlier stage than in the past, with less complication which allow us to perform more closed technique. This could been possible also as a result of an intensive and continuous training of surgeons. Recurrent disease was founded in 35.87% which is included in the interval reported in literature. Like in other studies we founded that closed technique had higher recurrence than open technique. In conclusion, cholesteatoma’s treatment need to be individualized, surgeons should to choose the procedure according to the localization and extension of disease, considering the hearing, the socio-economic status of the patient of which depends the follow-up and recurrence control.
1.Schuknecht HF. Pathology of the Ear. Cambridge Mass. Harvard University Press. 1974 2.Tran Ba Huy P et al. Otrites moyennes chroniques. Historire elemntaire et formes cliniques. Encycl
Méd Chir.Paris: Elsevier SAS; 2005 Oto-rhino-laryngologie, 3. Magnan J, et al. Anatomo-pathology of cholesteatoma. Acta OtorhinolaryngolBelg 1991;45:27–
34(1991) 4. Mitrovic M, Haralampiev K, Džinic M. Problems in diagnosis and treatment of cholesteatoma in
children. Int J Pediat Otorhinolaryngol .1991; 21:149–153 5. Mutlu C, Khashaba A, Saleh E, Karmarkar S, et al. Surgical treatment of cholesteatoma in children.
Otolaryngol Head Neck Surg .1995;113:56–60; 6. Sanna M, Zini C, Gamoletti R, Delogu P, Russo A, et al. The surgical management of chilhood
cholesteatoma. J Laryngol Otol. 1987;101:1221-6 7. Rosenfeld RM, Moura RL, Bluestone CD. Predictors of residual- recurrent cholesteatoma in children.
Arch. Otolaryngol. Head Neck Surg. 1992;118:384-91
Cholesteatoma Scaled keratin inside the middle ear or any pneumatized area in the temporal bone deriving from a keratinized squamous epithelium¹ Malphigien descuamant epithelim in the tympanic cavity ² Skin in the wrong place³ Destructive lesion of the skull base that can erode and destroy important structures within the temporal bone. In children - more aggressive than in adults - more extensive and it has a higher rates of residual and recurrent disease. Treatment - Surgical intervention - Main goals:
- a safe and dry ear by removing disease with the preservation of normal anatomy; - to preserve/restore the hearing; - to prevent residual/recurrent disease The extent and effectiveness of surgery depends upon the size of the cholesteatoma.
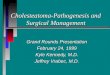
Hearing loss and otorrhea were the main symptoms both in adults and children, followed by otalgia in children or dizziness in adults. Adult complains also about headache. Although the complications had a low rates, both in adults and children, almost every year we founded some complicated cases like cerebral abscess, meningitis, sigmoid sinus thrombosis, labyrinthine fistulae or facial palsy. At physical examination we found (Fig 1,6, Table 1): - Granulation tissue, purulent discharge - Tympanic membrane perforation - Deep retraction pocket – pars flaccida/posterior quadrant - Complications like abscess in the neck, sigmoid sinus thrombosis, epidural/cerebral abscess, meningitis, facial palsy
62 69 76 63 54 72 67 75 56 68
17 19 22 21 23
18 26 23 20
24
-30
20
70
120
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Children
Adults
Figure 2. Patients distribution over the studied period, adults and children.
Symptoms Adults Children
Otorrhea Hearing loss - ABG Otalgia Dizziness Headache Facial palsy Fever
62.2% 100% 17.5% 30.8% 20.7% 14.6% 12.7%
88.7% 100% 47.4% 19.2% 6.6% 0.5% 26.3%
Complications
Epidural/cerebral abscess Facial palsy Meningitis Sigmoid sinus thrombosis Abscess in the neck
4.4% 4.7% 5.1% 4.4% 1.8%
2.4% 3.8% 4.2% 2.4% 1.4%
Figure 3. Surgical techniques: At first operation: - Close technique was used in 47% of adults and in 46% of children. - Open technique was used in 52.5% in adults and in 54% in children. 19% of adults missed the follow-up and 35% had dry open cavity or they did not have any complains In children about 9 % missed the follow-up and about 25% had dry open cavity or no complains Second surgery was performed in about 46% of adults, where one third were open cavities, and in 65% of children, where about 44% were open cavities. At second surgery in adults about 58% were close techniques which include also the reconstructed open cavities; in children about 44% had close techniques, including the reconstructed cavities. About 24% of all patients needed more than 2 surgeries.
0
10
20
30
40
50
60
2000 2002 2004 2006 2008 2010 2012
Adults CWU
Children CWD
Children CWU
Adults CWD
Figure 4. Both, in adults and in children, the CWU surgery tend to replace the CWD surgery
0
5
10
15
20
2000 2002 2004 2006 2008 2010 2012
Adults CWU
Children CWU
Adults CWD
Children CWD
Figure 5. In the revision surgery we reconstructed the ear structures all over when the disease allowed it.
Figure 1. Preoperative finding: otorhea (a), tympanic membrane perforation in pars flaccida (b) and retroauricular abscess (c)
Table 1. Symptoms and complications
Figure 6. Preoperative and intraoperative findings
ABG Adults Children
Preoperative 29.49±1.94 dBHL 29.30±1.40 dBHL
Postoperative 16.08±2.72 dBHL 17.79±2.36 dBHL
Improvement 13.41±2.79 dBHL 11.51±1.73%
Postoperative profound hearing loss 2.0±1.33% 0.20±0.42%
Figure 7. Functional outcomes
Figure 8. Postoperative aspects