Embed Size (px)
Citation preview

Introducing reflectance meters to hospital wards
L M Weedon RGN Diabetes Specialist Nurse, Diabetic Centre, Greenwich District Hospital P D Wills MSC BSC Senior Biochemist, Chemical Pathology, Greenwich District Hospital
Correspondence to: Ms LynneWeedon, Diabetic Centre, Greenwich District Hospital, Vanbrugh Hill, London SElO9HE
Abstract The introduction of Reflolux S blood glucose meters (BM UK Ltd) onto all
wards of a District General Hospital is described. We established a continuing, structured education programme and a laboratory-based quality assurance scheme (QA) and issued guidelines regarding safety and correct usage of the meter. A formal hospital policy on blood glucose monitoring together with
certification of user competence recorded on a database has enabled evaluation of nurse training and audit. The introduction of a QA scheme has allowed
assessment of meter results, identified areas where more education was needed and provided data to feed back to ward staff. Poor performers have benefited
from positive liaison with diabetic nurse specialists at an early stage.
Key words: Reflolux S, quality assurance, blood glucose monitoring
Introduction Accurate blood glucose monitoring is necessary in the management of diabetes. However, there have been con- cerns about the accuracy of using test strips at the bedside’ ‘. The speed and convenicnce is of particular benefit when intravenous insulin pumps are used to achieve “tight control”. Visually-read strips d o not give results which are as accurate as meter-read strips’: the former involve subjective judgements which may be influenced by whether therapeutic action is required. Also. timing is performed more accuratcly when a meter is used. Hutchison and Shcnkin reportcd thc accuracy of nurses making colour comparison with BM test strips (Boehringer Mannheim UK) and reported that 32.2% of readings was out- side of one strip rangc of the stated BM value and 12% was inaccurate enough to have led to inappropriatc clinical decision’.
Potentially serious errors are possible if meters are not used correctly. For example, inadequate covering of the reagent strip, smearing or failure to com- plctely remove blood, failing to recali- bratc when using a new batch o f strips and sticky fingers can all lead to inaccu- rate results; such errors are well documented’ ”. However, we felt that if used correctly, the advantages of a meter outweighed visually-read strips. The alarm on the meter ensures accurate timing and the meter may also serve to heighten the nurseS pcrception of the importance of accurate rcsults. The Department of Health and Social Security (DHSS) Hazard Warning in 1987 clearly identified the need for for-
mal training in the use of meters and a strict quality control programme’.
Reflolux I1 meters (BM) had pre- viously been introduced to 12 wards at Greenwich District Hospital in 1988, but the initiative had not proved successful. Problems expressed by the nurses were: difficulties in calibrating the Reflolux 11 and an unrealistic laboratory QA pro- gramme which was ward-initiated and felt to be too frequent and the use of an internal quality control solution was con- sidered to be too time-consuming, unnecessary and therefore rarely per- formed. Difficulty was also expressed in releasing ward staff for training in the Diabetic Day Care Centre (DDCC) and we identified a number of further prob- lems. Previously, only trained staff were permitted to use the meter though, in practice, junior nurses and auxiliaries often performed the majority of ward blood glucose measurements. There was no system of continuing education: this was an area of concern, as many wards have a rapid staff turnover. Too few people were able to train others; the two diabetes specialist sisters in the DDCC were the only identified assessors. In addition, there was no hospital policy or guidelines for capillary blood glucose measurement.
We chose to use Reflolux S meters (BM) because BM Stix strips were already used in the hospital and 12 wards were familiar with the Reflolux 11. Only one type of meter was used throughout the hospital to reduce confusion and simplify training. The Reflolux meter had been shown in clinical trials to be accurate and preeisc6.’.
At the time of the introduction of the
Reflolux S. only two of the original meters could be located and one area had purchased two meters indepen- dently. The majority of blood glucose monitoring was performed visually by nurses who had little or no training in the usc of the strips or in the interpretation of the results.
Aims The study attempted to produce a stan- dardised hospital policy for capillary blood glucosc measurement that fulfills DHSS recommendations to include:
Careful and appropriate selection of equipment 0 Quality assurance based on the routine involvement of the pathology department
A written hospital policy for the measurement of blood glucose and a pro- cedure for using the Reflolux metcr, including guidelines for appropriatc action to be taken when problems are encountered - both the policy and the procedure to be evaluated and revised as necessary
Adequate ongoing staff training with evaluation using the database, QA results and fcedback from the nursing staff which is revised accordingly.
Thc study also attempted to increase the accuracy of capillary blood glucose measurements and heighten staff aware- ness of the consequences of incorrect results in the management of diabetes.
Methods Initially, we arranged a meeting for all nurses in charge of wards and depart- ments and this was attended by a repre- sentative from BM.
228 Practical Diabetes November/December Vol8 No 6

Original Articles ________ -_F_____
The aim was to discuss the merits and problems of the previous procedure and develop a scheme acceptable to ward staff, RM and ourselves. The Reflolux S was demonstratcd and an opportunity was given for staff to use the mcter and ask questions.
A hospital policy for the measurement of capillary blood glucose was drawn up with the cooperation of nursing manage- ment. This included guidelines for both visual and meter readings with a prefer- ence expressed for the use of meters whenever possible. This document is now included in ward procedure filcs.
The procedure outlines the QA pro- gramme, routine maintenance, certifica- tion, initial training in the use of the meter, the action to be taken if problems arise and the need for retraining. It iden- tifics the ward sister or charge nurse as responsible for the training on herhis ward. All grades of nurses are able to use the meter and are issued with certifi- cates, but only qualified staff trained in the use of the meter are to be involved in the training and asscssment of others.
Both the procedure and certificate, which incorporates the training checklist (see Appendix), were drawn up with nurs- ing management. They were based on analysis of comments made at the sisters’ meeting, guidelines from BM and the diabetic literature’,’.
The documents were distributed when the meters were introduced to the wards and comments and suggestions for mod- ification were encouraged. Both empha- sise the nurse’s individual responsibility, the nurse only signing the certificate when shelhe felt competent in the use of the meter.
As a result of this meeting, the patho- logy department agreed to be involved in devising a QA programmc. A senior biochemist was identified as responsible for this and standard QA solutions were sent from the laboratory to the wards, thus transferring rcsponsibility from the ward to the laboratory: this was carried out at approximately fortnightly intervals.
Commercially available control sera (and mixtures at various levels) which had been screened for hepatitis B sur- face antigen and which were in routine use in the laboratory were distributed in 0.5mI aliquots in labelled plastic tubes. The tubes were contained in sealable polythene bags together with 3ml dispos- able transfer pipettes (LIP Ltd). It was sent to the nurse-in-chargc with a short letter requesting early attention. A “tear-off‘’ strip was included which required minimal information to be entered by the nurse - namely the ward, serial number of meter, the sample result with the batch code of sticks used and date of analysis.
introducing reflectance meters to hospital wards
Table 1 Problems encountered and action taken
Meter Became blocked with blood and cotton wool Reasons: a) Poor user technique
Modification: Ongoing education b) Debris difficult to remove with cold water
Policy now recommends cleaning with 70% alcohol
Certificates Nurses using meters without certificates Reasons: a) Trained by ward staff but no certificate issued
b) Certificate locked in sister‘s drawer cl Difficult to complete three copies d) Unaware of existence of policy Certificate adapted into three “tear-off” sections (see appendix) Modification:
Samples a) Difficulty in obtaining enough blood b) Needle stick injuries Reasons:
Modification:
a) N o “finger pricking” devices provided by hospital b) Poor user technique Autolet multi-patient devices (Owen Mum ford) purchased Protocol devised by infection control and occupational health nurse
Recording Blood glucose meter results inappropriately recorded Reason: Inappropriate ward diabetic charts Modification: New ward charts devised
Table 2 Range of co-efficients of variation (CV)
Low Medium High
Range (mmolil) 3.0-4.6 6.6- 10.9 13.0-20.1 SD range (mmolll) 0.3-0.6 0.5-0.9 0.7-1.8 CVrange (‘7”) 10.0-16.7 5.6 11.3 5.0- 11.7 Median CV 12.1 8.7 6.3 Number of distributions 4 9 6
It was agreed that some form of feed- back should be given to the participants to maintain their interest and enthusiasm‘. The laboratory agreed to be responsible for the individual written feedback to the wards. Early response to the distribution of elementary statistics suggested that ward staff merely wished to be informed whether or not their result was acceptable. Under laboratory conditions, a range of k one standard deviation (SD) is acceptable.
Taking account of the greater number of variables which may contribute to errors in bedside chemistry, we decided a range of k 1.5 S D to be appropriate with- out the risk of masking poor performcrs. Results of > 2.0 SD were excluded from the calculations. Results within range were reported as “acceptable”, while
those greater than rf: 1.5 SD were reported as “outside acceptable limits”. The sisters in the DDCC were respon- sible for visiting any wards that per-
.formed poorly to check the meters and the nurse’s technique and identify and solve problems.
The procedure clearly states the appropriate clinical situations for the meter’s use and its unsuitability for diag- nostic or stress tests. Clear guidelines were given regarding action to be taken if readings are >25 or (3 as well as the importance of verification of hypo- glycaemia and hyperglycaemia by labor- atory measurement.
A computer database was set up to keep a record of all nurses assessed, the date assessed, name of assessor, grade, ward and department. Continuedonp232
Practical Diabetes NovembedDecember Vol8 No 6 229
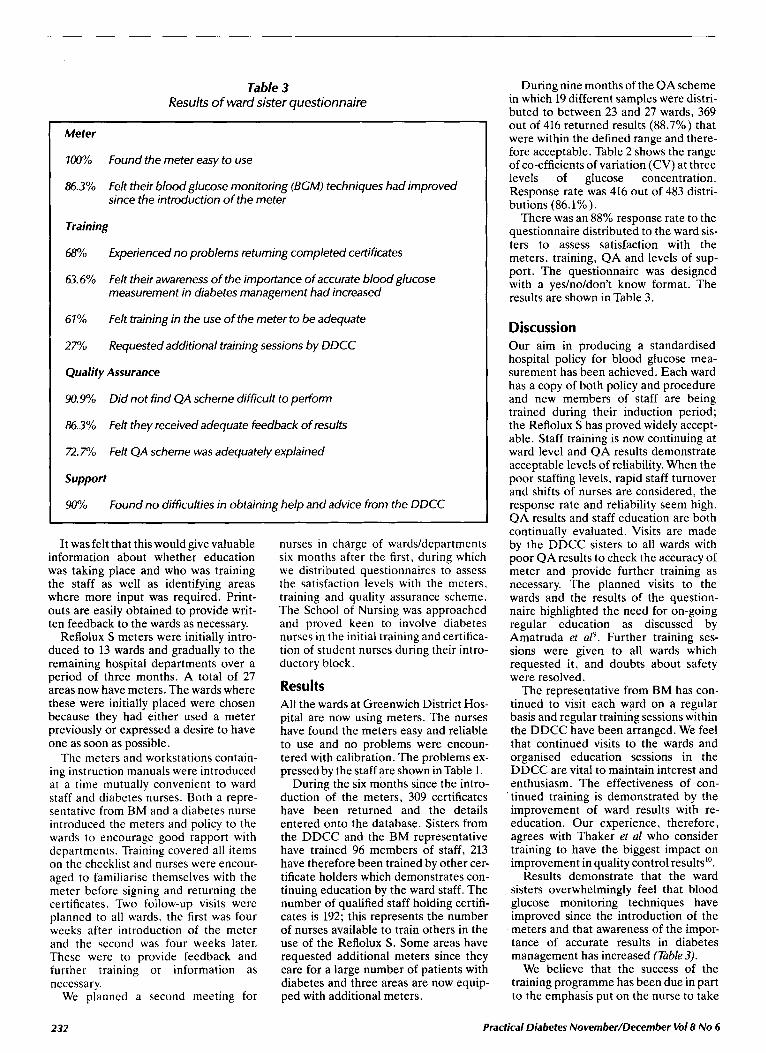
Table 3 Results of ward sister questionnaire
Meter
700%
86.3%
Found the meter easy to use
Felt their blood glucose monitoring (BGM) techniques had improved since the introduction of the meter
Training
68%
63.6%
Experienced no problems returning completed certificates
Felt their awareness of the importance of accurate blood glucose measurement in diabetes management had increased
Felt training in the use of the meter to be adequate
Requested additional training sessions by DDCC
61%
27%
Quality Assurance
90.9%
86.3%
R.7?/o
Support
Wh
Did not find Q A scheme difficult to perform
Felt they received adequate feedback of results
Felt Q A scheme was adequately explained
Found no difficulties in obtaining help and advice from the DDCC
It was felt that this would give valuable information about whether education was taking place and who was training the staff as well as identifying areas where more input was required. Print- outs are easily obtained to provide writ- ten feedback to the wards as necessary.
Reflolux S meters were initially intro- duced to 13 wards and gradually to the remaining hospital departments over a period of three months. A total of 27 areas now have meters. The wards where these were initially placed were chosen because they had either used a meter previously or expressed a desire to have one as soon as possible.
Thc meters and workstations contain- ing instruction manuals were introduced at a time mutually convenient to ward staff and diabetes nurses. Both a repre- sentativc from BM and a diabetes nurse introduced thc meters and policy to the wards to encouragc good rapport with dcpartments. Training covered all items on the checklist and nurses were encour- aged to familiarise themselves with the meter before signing and returning the certificates. Two follow-up visits wcrc planncd to all wards, the first was four weeks after introduction of the meter and the second was four weeks later. These were to provide feedback and further training or information as nccessary.
We planned a second meeting for
nurses in charge of wards/departmcnts six months after the first, during which we distributed questionnaircs to assess the satisfaction levels with the mcters, training and quality assurance schcme. The School of Nursing was approachcd and proved keen to involve diabetes nurses in the initial training and certifica- tion of student nurses during their intro- ductory block.
Resu I ts All the wards at Greenwich District Hos- pital are now using meters. The nurses have found the meters easy and reliable to use and n o problems were encoun- tered with calibration. The problems ex- pressed by the staff are shown inTable 1.
During the six months since the intro- duction of the meters, 309 certificates have been returned and the details entered onto the database. Sisters from the DDCC and the BM representative have trained 96 members of staff, 213 have therefore been trained by other cer- tificate holders which demonstrates con- tinuing education by the ward staff. The number of qualified staff holding certifi- cates is 192; this represents the number of nurses available to train others in the use of the Reflolux S. Some areas have requested additional meters since they care for a large number of patients with diabetes and three areas are now equip- ped with additional meters.
During nine months of the QAscheme in which 19 different samples were distri- buted to between 23 and 27 wards, 369 out of 416 returned results (88.7%) that were within the defined range and there- fore acceptable. Table 2 shows the range of co-efficients of variation (CV) at three levels of glucose concentration. Response rate was 416 out of 483 distri- butions (86.1%).
There was an 88% response rate to the questionnaire distributed to the ward sis- ters to assess satisfaction with the meters, training, QA and levels of sup- port. The questionnaire was designed with a yeslnoldon’t know format. The results are shown in Table 3.
Discussion Our aim in producing a standardised hospital policy for blood glucose mea- surement has been achieved. Each ward has a copy of both policy and procedure and new members of staff are being trained during their induction period; the Reflolux S has proved widely accept- able. Staff training is now continuing at ward level and QA results demonstrate acceptable levels of reliability. When the poor staffing levels, rapid staff turnover and shifts of nurses are considered, the response rate and reliability seem high. QA results and staff education are both continually evaluated. Visits are made by the DDCC sisters to all wards with poor QA results to check the accuracy of meter and provide further training as necessary. The planned visits to the wards and the results of the question- naire highlighted the need for on-going regular education as discussed by Amatruda et aZ9. Further training ses- sions were given t o all wards which requested it, and doubts about safety were resolved.
The representative from BM has con- tinued to visit each ward on a regular basis and regular training sessions within the DDCC have been arranged. We feel that continued visits to the wards and organised education sessions in the DDCC are vital to maintain interest and enthusiasm. The effectiveness of con-
‘ tinued training is demonstrated by the improvement of ward results with re- education. Our experience, therefore, agrees with Thaker et ul who consider training to have the biggest impact on improvement in quality control resultslO.
Results demonstrate that the ward sisters overwhelmingly feel that blood glucose monitoring techniques have improved since the introduction of the meters and that awareness of the impor- tance of accurate results in diabetes management has increased (Table 3).
We believe that the success of the training programme has been due in part to the emphasis put on the nurse to take
232 Practical Diabetes November/December Vol8 No 6
Original Articles _------~________--__----____-----
Introducing reflectance meters to hospital wards
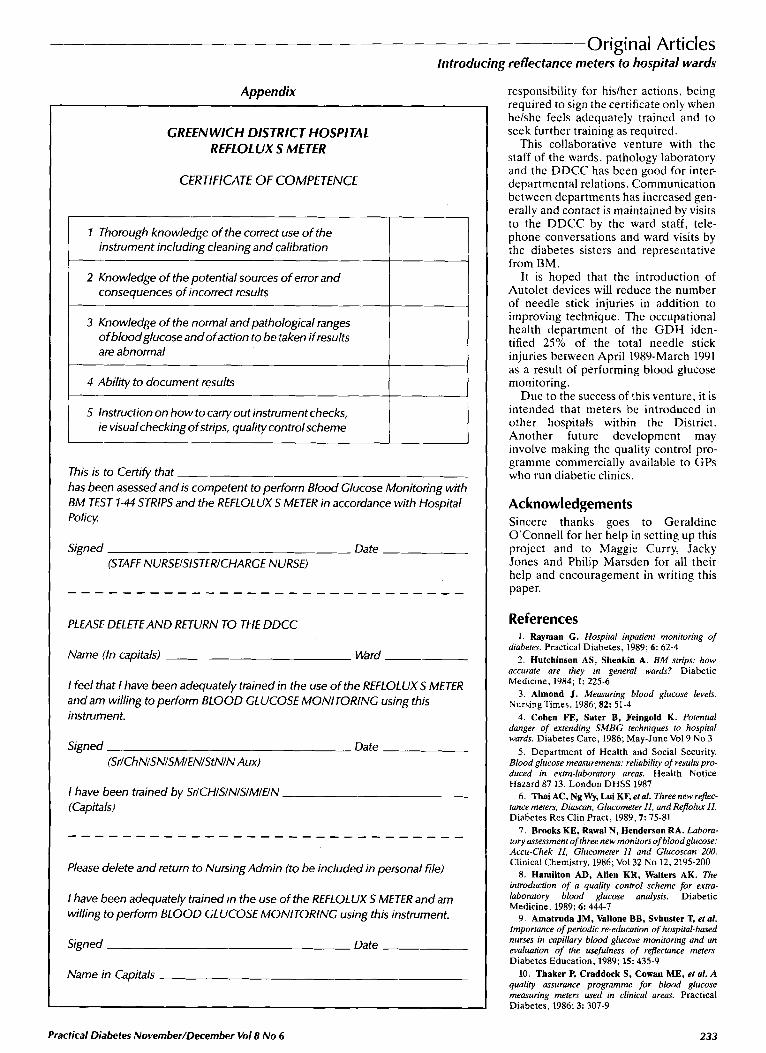
Appendix
GREENWICH DISTRICT HOSPITAL REFLOLUX S METER
CERTlFlCATE OF COMPETENCE
I Thorough knowledge of the correct use of the instrument including cleaning and calibration
2 Knowledge of the potential sources of error and consequences of incorrect results
3 Knowledge of the normal and pathological ranges of bloodglucose and ofaction to be taken if results are abnormal
4 Ability to document results 1 I 5 Instruction on how to carry out instrument checks,
ie visualchecking of strips, quality controlscheme --
This is to Certify that -- has been asessed and is competent to perform Blood Glucose Monitoring with BM TEST 1-44 STRIPS and the REFLOLUX S METER in accordance with Hospital Policy
Signed -- Date - (STAFF NURSEISISTERICHARGE NURSE)
PLEASE DELETEAND RETURN TO THE DDCC
Name (In capitals) ~- Ward -~
I feel that I have been adequately trained in the use of the REFLOLUX S METER and am willing to perform BLOOD GLUCOSE MONITORING using this instrument.
Signed - - Date - (SrlChNlSNlSMlENlStNlN Aux)
I have been trained by SrICHlSlNlSlMIEIN (capitals)
Please delete and return to Nursing Admin (to be included in personal file)
I have been adequately trained in the use of the REFLOLUX S METER and am willing to perform BLOOD GLUCOSE MONITORING using this instrument.
Signed Date -
Name in Capitals
responsibility for hislhcr actions, being required to sign the certificate only when helshc fecls adequately trained and to seek further training as required.
This collaborative venture with the staff of the wards. pathology laboratory and the DDCC has bcen good for inter- departmental relations. Communication between departments has increased gen- erally and contact is maintained by visits to the DDCC by the ward staff, tele- phone conversations and ward visits by thc diabetes sistcrs and representative from BM.
It is hoped that the introduction of Autolet devices will rcducc the number of needle stick injuries in addition to improving technique. The occupational health department of the G D H iden- tified 25% of the total needle stick injuries between April 1989-March 1991 as a result of performing blood glucose monitoring.
Due to the succcss of this venture, it is intended that meters be introduced in other hospitals within the District. Another future development may involve making the quality control pro- gramme commercially available to GPs who run diabetic clinics.
Acknowledgements Sincere thanks goes to Geraldine O'Connell for her help in setting up this project and to Maggie Curry, Jacky Jones and Philip Marsden for all their help and cncouragement in writing this paper.
Ref ere n ces 1 . Raymnn G. Hospital inpatient monitoring of
diabetes. Practical Diabetes, 1989; 6: 62-4 2. Hutchinsun AS, Shenkia A. BM strips: how
accurate are they in general wards? Diabetic Medicine, 1984; 1: 225-6
3. Almond J. Measuring blood glucose levels. Nursing'f'imes, 1986; 82: 51-4
4. Cohen FE, Sater B, Feingold K. Potential danger of extending SMBG techniques to hospital wards. Diabetes Care, 1986; May-June Vol9 No 3
5 . Department of Health and Social Security. Blood glucose meawrements: reliability of results pro- duced in extra-laboratory areas. Health Notice Hazard 87 13. London DHSS 1987
6. ThaiAC,NgWy, LuiKF,etal. Threenewrdec- tunce meters; Diuscan, Glucometer 11, and R@olu II. Diabetes Rcs Clin Pract, 1989,7: 75-81
7. Brooks KE, Rawal N, Hendersun RA. Labora- tory assessment of three new monitors of bloodglucose: Accu-Chek II, Glucometer II and Glucoscan 200. Clinical Chemistry, 1986; Vol32 No 12,2195-200
8. Hamilton AD, Allen KR, Walters AK. The introduction of a quality control scheme for extra- laboratory blood glucose analysir. Diabetic Medicine. 1989; 6: 444-7
9. Amatruda JM, Vnllone BB, Svhuster T, et al. Importance of periodic re-education of hospital-based nurses in capillury blood glucose monitoring and an evaluation of the usefulness of reftectunce meter.s. Diabetes Education. 1989; 15: 435-9
10. Thaker P, Crnddock S , Cowan ME, et d. A qualitj assurance programme for blood glucose measuring meters used in clinical areas. Practical Diabetes. 1986; 3: 307-9
Practical Diabetes November/December Vol8 No 6 233