-
8/16/2019 Intro to ECGs
1/63
An early Electrocardiograph
-
8/16/2019 Intro to ECGs
2/63
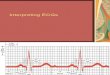
Einthoven’s first publishedEKG, 1902
-
8/16/2019 Intro to ECGs
3/63
“I do not however imagine that the
string galvanometer…is likely to
find any very extensive use in thehospital”
August D. Waller, 1909
-
8/16/2019 Intro to ECGs
4/63
The Electrocardiogram
(ECG/EKG)Most Commonly Utilized
Cardiovascular Lab Test100 Million Performed per Year$5 Billion
Cost per YearReimbursements have droppedKey to Therapy for
ACS/MI
Diagnosis of Arrhythmias
-
8/16/2019 Intro to ECGs
5/63
Indications For An ECGChest or EpigastricPain or Sensation
CHF Signs orSymptoms Abnormal
PulseHypotensionUnexplainedWeakness
Altered Mental State(Coma, CVA)
Drug OverdoseChest TraumaSyncope or NearSyncopeSystemic
IllnessMetabolic Disease
Screening??
-
8/16/2019 Intro to ECGs
6/63
P’s and Q’s of
Electrocardiography
Atrial
Depolarization
Ventricular
Depolarization
Ventricular
Repolarization
http://medstat.med.utah.edu
-
8/16/2019 Intro to ECGs
7/63RL/LL- side does not matter, place anywhere below
umbilicus
-
8/16/2019 Intro to ECGs
8/63
The Electrocardiogram
(ECG/EKG)
Rhythms
ST Segments
-
8/16/2019 Intro to ECGs
9/63
-
8/16/2019 Intro to ECGs
10/63
-
8/16/2019 Intro to ECGs
11/63
-
8/16/2019 Intro to ECGs
12/63
-
8/16/2019 Intro to ECGs
13/63
-
8/16/2019 Intro to ECGs
14/63
-
8/16/2019 Intro to ECGs
15/63
LAD 95%
1
-
8/16/2019 Intro to ECGs
16/63
LAD 95%
1
-
8/16/2019 Intro to ECGs
17/63
1
LAD 95%
-
8/16/2019 Intro to ECGs
18/63
1
-
8/16/2019 Intro to ECGs
19/63
1
LAD 0%
Post PCI
-
8/16/2019 Intro to ECGs
20/63
Basic Principles of ECGInterpretation
Place electrodes correctly (??)Be Careful to Get Correct
DataConsider Clinical Context/SettingChest pain? … consider ST
segments
Compare to Previous ECGBe Systematic
Rate, Rhythm, ?Pacemaker SpikesQRS duration, Other
intervals AxisQ waves
Pattern read
-
8/16/2019 Intro to ECGs
21/63
QRS Prolongation (=>120msec, 3 40 msec boxes)
Ventricular OriginPVCsVentricular TachycardiaVentricular
Electronic Pacemaker
SVT with Aberrant ConductionBundle Branch Block
Right (rabbit ears on the right)Left (rabbit ears on the
left)
WPW
IntraVentricular Conduction Delay
-
8/16/2019 Intro to ECGs
22/63
Why is QRS Prolongation so
important except for RBBB??? Q waves not diagnostic
ST Depression not diagnostic
Possibly Ventricular Origin
Usually High Risk
-
8/16/2019 Intro to ECGs
23/63
.000
.250
.500
.750
.000
0.0 2.0 4.0 6.0 8.0 10.0 12.0 14.
1 (130ms): N=61 (6.6%)
Follow-up (yrs)
S u r v i v
a l
-
8/16/2019 Intro to ECGs
24/63
-
8/16/2019 Intro to ECGs
25/63
Rabbit Ears
InvertedTwave
-
8/16/2019 Intro to ECGs
26/63
-
8/16/2019 Intro to ECGs
27/63
RBBB
-
8/16/2019 Intro to ECGs
28/63
LBBB
-
8/16/2019 Intro to ECGs
29/63
Rabbit Ears
InvertedTwave
-
8/16/2019 Intro to ECGs
30/63
IVCD
-
8/16/2019 Intro to ECGs
31/63
WPW
-
8/16/2019 Intro to ECGs
32/63
WPW
-
8/16/2019 Intro to ECGs
33/63
-
8/16/2019 Intro to ECGs
34/63
RAD
-
8/16/2019 Intro to ECGs
35/63
LAD
-
8/16/2019 Intro to ECGs
36/63
S1S2S3
-
8/16/2019 Intro to ECGs
37/63
Criteria For Infarction Q
WavesEqual or Greater than .04 seconds (onemillimeter box
horizontal width, 40
milliseconds)
Q Wave Amplitude must be 25% or
greater of following R Wave
Pathophysiology: no muscle to generateR wave
-
8/16/2019 Intro to ECGs
38/63
-
8/16/2019 Intro to ECGs
39/63
-
8/16/2019 Intro to ECGs
40/63
Basic Principles of ECGInterpretation
Place electrodes correctly (??)Be Careful to Get Correct
DataConsider Clinical Context/Setting
Chest pain? … consider ST segments Compare to Previous
ECGBe Systematic
Rate, Rhythm, ?Pacemaker SpikesQRS duration, Other
intervals AxisQ waves
Pattern read
-
8/16/2019 Intro to ECGs
41/63
inverted
Qw, P/Tup ordown
Rightventricularinvolvement:RVH, RBBB
Left ventricularinvolvement:LVH, LBBB
-
8/16/2019 Intro to ECGs
42/63
Pattern Reading of the ECG
Diagonal Line Rulebox around aVR (everything inverted)
line thru III, aVL, V1every thing else upright
Parallel Line RuleR waves increase then drop off in V6S
waves decrease from greatest in V1Rabbit ears on right side (V1-2)
for RBBB,
on left side for LBBB
Th 5 C d f ECG
-
8/16/2019 Intro to ECGs
43/63
The 5 Commandments of ECGInterpretation
• Be systematic
• Put into the clinical context
• Find an old ECG
• Watch out for bad data
– Strive for good data
• Do NOT be afraid to get help
Watch out for bad
data
-
8/16/2019 Intro to ECGs
44/63
-
8/16/2019 Intro to ECGs
45/63
RA/LA reversed
V1/V3 reversed
-
8/16/2019 Intro to ECGs
46/63
What happened?
-
8/16/2019 Intro to ECGs
47/63
-
8/16/2019 Intro to ECGs
48/63
Intervals, segments, and durations
-
8/16/2019 Intro to ECGs
49/63
Intervals
QRS durationPR interval QT IntervalNormal: .12-.20 sec
(3-5 small boxes)
Normal: .07-
.10 sec
Normal (corrected for
rate or QTc): .440-.470sec
• QT Interval
• PR Interval
• QRS Duration
-
8/16/2019 Intro to ECGs
50/63
Intervals: Conduction
System AbnormalitiesCongenital Syndromes
Electrolyte/Metabolic AbnormalitiesIntrinsic Cardiac
DiseaseMedicationsCNS Disorders
Systemic Illnesses
-
8/16/2019 Intro to ECGs
51/63
Electrolyte Abnormalities and
the ECGPotassiumHyper: tall, peaked T waves (also
ischemia), atrial arrestHypo: prominent U waves, low T wave
CalciumHyper: short QT
Hypo: long QT (also Quinidine, ischemia)MagnesiumHyper: short QT
interval
Hypo: long QT interval
-
8/16/2019 Intro to ECGs
52/63
L QT i t l
-
8/16/2019 Intro to ECGs
53/63
Long QT intervals(>50% of the RR interval)
• Congenital
HypoMg/CA
anti-arrhythmics
Myocarditis
Hypokalemia
Ischemia
Phenothiazines
Tricyclics
CNS--SubarachnoidHemorrhage
Torsades des Pointes
The QT interval
-
8/16/2019 Intro to ECGs
54/63
The QT intervalLong QT (>50% of the RR
interval) CongenitalHypomagnesiumHypocalcemiaIA
anti-arrhythmicsIschemiaTorsades de Pointes
PhenothiazinesTricyclicsMyocarditisHypokalemia
Short QT Hypercalcemia
HypermagnesiumHyperkalemiaDigoxinThyrotoxicosis
-
8/16/2019 Intro to ECGs
55/63
-
8/16/2019 Intro to ECGs
56/63
-
8/16/2019 Intro to ECGs
57/63
Other Patterns
• Atrial Abnormalities
• R>S V1
http://medstat.med.utah.edu
-
8/16/2019 Intro to ECGs
58/63
SANode
-
8/16/2019 Intro to ECGs
59/63
Atrial AbnormalitiesRight (P-pulmonale)Right atrium right heart
border, first hump
tall, peaked in inferior leads (>2.5mm)
Left (P-mitrale)Left atrium posterior, second hump
broad P wave (>120msec) with negativecomponent in V1-2 (>
1mm x 1mm)
Normal=2.5x2.5 boxes (100msec x .25Mv)
-
8/16/2019 Intro to ECGs
60/63
P pulmonale or
RAA
-
8/16/2019 Intro to ECGs
61/63
P mitrale or LAA
Computerized LAA with/without P wave prolongation
-
8/16/2019 Intro to ECGs
62/63
0.0
0.2
0.4
0.6
0.8
1.0
0.0 2.0 4.0 6.0 8.0 10.0
a. LAA (-), P duration 120ms n=4,476 (2.0%)
c. LAA (+), P duration 120ms n=407 (4.7%)
p p g
S u
r v i v a l
Years Follow up
-
8/16/2019 Intro to ECGs
63/63
R>S V1RVH
RBBBInferior Posterior MIWPWNormal Variant