Embed Size (px)
Citation preview

In partnership with:
Supporter of:
Intracranial Pressure
Terry Coyne MBBS, FRACS
In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Raised ICP • Definitions
• Causes
• Consequences
• Therapy

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
What its all about
• Cerebral blood flow (CBF) sufficient to meet cerebral metabolic oxygen demand (CMRO2)

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Cerebral Perfusion Pressure (CPP)
= Mean Arterial Pressure (MAP) – ICP
Normal ICP <10-15 mm Hg
Normal CPP > 50 mm Hg

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Cerebral Autoregulation
In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Monro-Kellie Doctrine
• The skull is an inelastic closed compartment
• Intracranial compartment contains
brain
blood (intra- & extra-vascular)
CSF
other – tumour, abscess, etc
- extracellular fluid (vasogenic
edema)
• Sum of these is constant – if one increases, another must decrease, or else ICP increases

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
ICP Curve

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Consequences of Raised ICP
• Global - CPP
• Compartment - herniation

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Causes of Raised ICP
• Too much:
brain – cytotoxic edema
blood – intracranial haemorrhage
- venous sinus thrombosis
CSF – hydrocephalus
• Other – tumour, abscess

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Effects of Raised ICP
Early on
Headache – positional
val salva
early morning
Nausea/vomiting
Changed level of consciousness
Any focal symptom/deficit
Papilloedema

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Effects of Raised ICP
• Generalised – low CPP, generalised loss of brain function – decreased level of consciousness
• Herniations

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Herniations
• Subfalcine – not generally clinically significant
• Tentorial – 3rd nerve palsy (dilated pupil)
- lateral brainstem (pyramidal tracts) compression – contralateral weakness
- PCA occlusion - hemianopia
- cardio-respiratory centre
destruction - death

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
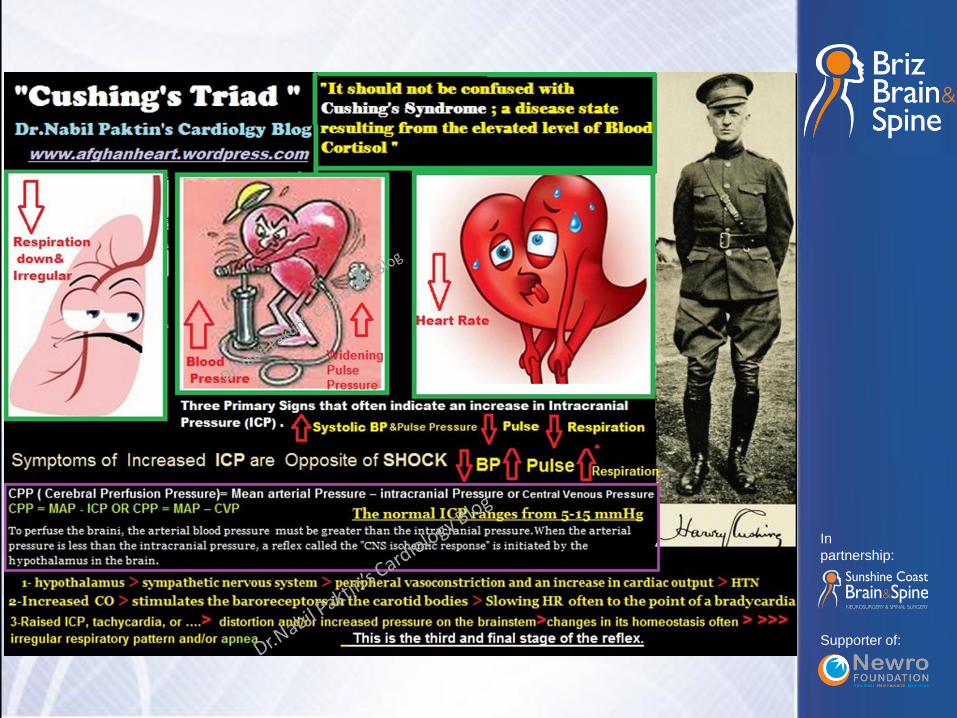
Herniations
• Foramen magnum
“Cushing’s triad”
bradycardia
hypertension
irregular respirations
(decreased level of consciousness)
In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Raised ICP Management
• Treat cause (remove clot/tumour, V-P shunt for hydrocephalus)
• Less blood volume – head up
- neck not kinked
- low pCO2 (hyperventilation)
• less brain – mannitol
- dexamethasone (vasogenic edema)
• less CSF – CSF drain

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Extradural haematomas
In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Raised ICP Management
More sophisticated (Neuro ICU)
• Change the rigid box (decompressive craniotomy)
• Modulate CPP
• Reduce CMRO2 – sedation
- thiopentone

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:

In partnership with:
Supporter of:
In partnership with:
In
partnership:
Supporter of:
Raised ICP Management
• GP management
• ABC’s – prevent hypoventilation
- maintain pO2, BP (CPP)
dexamethasone if vasogenic edema
eg 4mg q6h
- 20% mannitol (eg 300 mls)

In partnership with:
Supporter of:
Thank you




























![Brazilian Industrial and Innovation Complex in Health: H ... · Monro-Kellie doctrine is not valid." Acta Neurochir Suppl 114: 117-120. [2] Mascarenhas, S. and G. H. F. Vilela (2012)](https://img.pdfslide.us/doc/110x75/5b39b0897f8b9a310e8eaeeb/brazilian-industrial-and-innovation-complex-in-health-h-monro-kellie-doctrine.jpg)