Embed Size (px)
Citation preview

Interventions for Children & Adolescents with Diabetes
Margaret Grey, DrPH, RN, FAAN
Dean & Annie Goodrich Professor
Yale School of Nursing

Objectives
• Review the development of
cognitive-behavioral interventions
for youth with diabetes
• Describe a program of research on
such interventions in type 1 diabetes

Type I Diabetes• Alterations in metabolism
– Carbohydrates– Fats– Proteins
• Complications– Microvascular– Macrovascular– Neurological
• Quality of Life

Epidemiology• Most common metabolic disease in
childhood
• 176,000 American youth
• 1 in 400-600 children
• 18 new cases per 100,000 annually
• Peak age - male: 12-14 years female: 10-12 years
www.diabetes.org, 2007

Age-Specific Incidence Rates
0
5
10
15
20
25
30
35
0 2 4 6 8 10 12 14 16 18
Age in years
100,000Rate

Treatment
• Insulin to achieve near-normal blood glucose levels
• Diet sufficient for growth• Monitoring of blood sugars• Regular physical activity• Glycosylated hemoglobin levels quarterly
to assess overall control• Maintain psychological well-being• Prevention of complications

Diabetes Control & Complications Trial
• Improved control associated with 50-75% reduction in complications
• HbA1c linearly associated with complications
• No adverse effects on:– Cognitive function– Quality of life– Psychological symptoms
DCCT Research Group. (1993). New England Journal of Medicine

RECOMMENDATION
“Most teenagers with IDDM should be treated with
intensive therapy since their long-term outcome should be
measurably improved.”
DCCT Research Group. (1994). Journal of Pediatrics
Educational Interventions
• Cornerstone of treatment• Necessary for self-management• Multiple approaches
– Individual– Structured self-management training– Technology
• Mixed results but limited effects beyond knowledge

Family Interventions
• Target family and child with diabetes• Newer approaches
– Satin, multi-family approach– Wysocki, behavioral family systems
therapy– Anderson, parent-child conflict
• Outcomes include individual functioning

Intervention to Maintain Parent-Adolescent Teamwork
• Pilot Project– Powered for conflict, not for HbA1c
• N=85, age 10-15 years• Intervention
– Office-based– Focus on importance of parent-teen
responsibility sharing– Ways to avoid conflict
Anderson, et al. (1999). Diabetes Care, 22, 713-721.

Teamwork Intervention
• N=105, age 8-17 years
• Teamwork intervention vs. standard care– Importance of parent-child
responsibility sharing– Ways to avoid conflict– Office-based
Laffel, et al. (2003). Journal of Pediatrics

Cognitive-Behavioral Interventions
• Growing awareness of the negative impact of diabetes on psychosocial functioning
• Need for more than educational approaches to improve outcomes

Cognitive-Behavioral Interventions
• Stress management & relaxation
• Social support groups & camps
• Coping skills training

Social Support
• Few studies
• Goal to enhance the environment• Peer group intervention (Anderson, et al,
1989)
– Clinic-based, prevent adolescent decline
– Improvement in multiple areas, including HbA1c
Stress Management & Relaxation
• Stress worsens metabolic control• 12 session program (Mendez & Belendez,
1997)– Improved knowledge, adherence, stress
• Camp-based stress management program (Smith, et al., 1991)
– Intent to use more problem-focused coping– Fewer diabetes-related stressors

Coping Skills Training

Preliminary Work
• Avoidance coping associated with poorer outcomes
• Depression common in diabetes
• Difficult to engage teens in intensive regimens
• Difficulties in management may be associated with social situations

Coping Skills Training
• Increase sense of mastery and competence by retraining non-constructive coping styles and forming more positive patterns of social behavior.– Focus on common social issues in
diabetes management– Role play, art, discussion

Coping Skills
• Social problem solving
• Communication skills training
– Social skills training, assertiveness
• Cognitive behavior modification
• Conflict resolution

Social Problem-Solving
• Designed to help youth look at ways of handling peer pressure and raises awareness of possible consequences of their decisions– Focus is on process of problem-solving,
not necessarily the content– Steps: Identify the problem, set goals,
develop alternative solutions, examine consequences, choose solution, & evaluate the outcome

Social Skills Training
• Allows youth to work with peers and adults in a manner leading to positive results for all
• Enhances self-confidence, peer acceptance, and adjustment
• Provide concrete instructions on handling certain situations, role play appropriate model behavior, practicing in group and in life

Assertiveness Training
• Express themselves in direct, honest, and appropriate ways
• Observation of others and to reflect on their own behavior and its effect on others
• Role-play helpful in teaching this skill

Cognitive Behavior Modification
• Help youth recognize their own thoughts and feelings
• Helps to recognize sources of stress and decrease negative responses to stress
• May help to identify thoughts that are not based in fact

Conflict Resolution
• Conflict may be positive or negative, constant in youth’s lives
• Skills to resolve conflicts in a win-win manner
• Focus on reworking situations, with the hope of finding a solution with better outcomes than the usual

CST Protocol
• Teens - 5 weekly sessions
– Use scenarios of common social issues
in diabetes management to begin
discussion
• Children & Parents – 6 sessions

Study 1
• To determine if coping skills training in conjunction with intensive diabetes management vs. intensive management with education enhances:– Metabolic control (serial HbA1c)– Psychosocial well-being (depression, self-
efficacy, quality of life)– Rate of adverse events (severe hypoglycemia,
weight gain)

Subjects
• Type I diabetes• Desire to improve metabolic control• Age: 12.5-20 years at entry• No other chronic illness• HbA1c in last year > 7.2 & < 14 %• No severe hypoglycemia in last 6 mos.• Appropriate grade for age

Baseline Data• Physiological data
– Height, weight– Tanner stage– HbA1c
• Psychosocial data• Intensification of therapy (MDI, pump)
– Intensive Education

Follow-up• Telephone follow-up
– Daily– Weekly
• Visits to outpatient CCRC– Diabetes management– HbA1c– Education
• Initial study follow-up x 1 year• Followed for up to 5 years
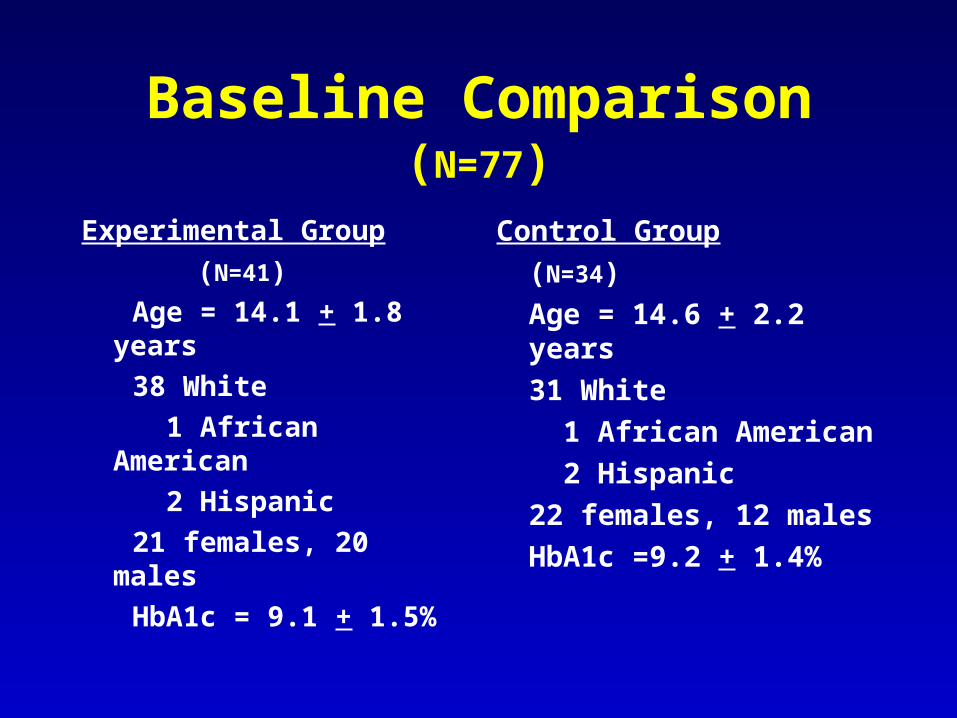
Baseline Comparison (N=77)
Experimental Group
(N=41)
Age = 14.1 + 1.8 years
38 White
1 African American
2 Hispanic
21 females, 20 males
HbA1c = 9.1 + 1.5%
Control Group
(N=34)
Age = 14.6 + 2.2 years
31 White
1 African American
2 Hispanic
22 females, 12 males
HbA1c =9.2 + 1.4%

Metabolic Control Over 12 Months(CST vs. Routine, N=72)
6
7
8
9
10
0 6 12
Hb
A1c
% CST
RC
MonthsF (groupxtime) = 5.3, df=2, p<.01

Diabetes Treatment by Group (N=77)
• MDI vs. CSII, p=.4– MDI=> 3 injections– CSII=pump
• Total Daily Dose:– 1.3+0.4 vs. 1.3+0.7
Units/Kg 0
5
10
15
20
25
30
N
I P
RC
CST
All comparisons, p>.05

Adverse Events by Group
0
5
10
15
20
25
30
Severe DKA Wt Gain
N
Cnt-M CST-M Cnt-F CST-F
* difference CST vs. control, p<.02
*
*

Quality of Life: Impact (N=77)
4042444648505254565860
Baseline 6 Months 12 Months
CST
Control
F(group x time)=5.4, df=2, p=.005; F(time)=12.5, df=2, p<.001

Diabetes Self-Efficacy(N=77)
80
90
100
110
Baseline 6 Months 12 Months
CST
Control
F(groupxtime)=5.4, df=2, p=.005; F(time)=14.1, df=2, p=.001

Impact of CST
• Improved metabolic control• Better self-efficacy• Less negative impact of diabetes on
quality of life• Fewer worries about diabetes• In females, fewer severe
hypoglycemic events and less weight gain

Building Evidence-From Efficacy to Effectiveness
• CST for pre-adolescents and their parents
• CST as an addition to nutrition and exercise for young adolescents at high risk for type 2 diabetes
• Moving to dissemination

CST for School-Aged Children and A Parent
• Can we improve the transition to
adolescence with CST?
– Children age 8-12 years and a parent
– RCT
– Child and parent outcomes

Parents and Children Together

Metabolic Control (N=41)
6.5
7
7.5
8
8.5
9
9.5
Baseline 3 Months 6 Months 12 Months
Control
CST
HbA1c
%
F=2.3, p=.1

Family Adaptability (N=41)
40
44
48
52
56
60
Baseline 3 Months 6 Months
CSTControl
F=5.33, df=2, p=.007

Parent’s Depressive Symptoms (N=41)
6
8
10
12
14
16
18
Baseline 3 Months 6 Months
CST
Control
F=3.91, df=2, p=.02

Diabetes-Related Conflict
10
15
20
25
30
35
Baseline 3 Months 6 Months
CSTControl
F =3.13, df=2,
p=.04

Next Steps:Moving to Dissemination

Problems with Previous Studies
• 50-60% enrollment of eligible subjects
• Conducted in a single tertiary medical center
• Less than 15% minority youth
• Small group format limited clinical applicability

Conceptual Framework
AgeGenderSESDevelopmental statusType 1 diabetes
Depressive Sx
StressCopingSelf-efficacySocial competenceFamily support
Family Adaptation Conflict resolution
Individual Adaptation Metabolic control Quality of life
Pre-existing Characteristics Individual Responses & Context Level of Adaptation
CST

Web Design
• Team approach– CST trainers, Research team, Web
development staff
• Initial focus group– Youth and parents– Likes and dislikes in web sites
• Web sites developed – CST & Education– Interactive with CST staff

Think Aloud Usage
• 3 adolescents
• 2 prototype sessions
• What they were thinking as they went through
• What they didn’t like
• Anything else that came to mind

Think Aloud Results
• “This is really cool. I love the characters. I want to name them. I like that you can see the (insulin) pumps”. “I can definitely relate (to the characters).” “I really like the graphic novels.”
• “The body questions really make me aware of how much my body is affected by stress.” “Great stress relieving examples – I would try them all.”
• Suggestions for improvement– Clarify directions– More about stressors– Provide better alternatives for some of the character
dialogue.

https://transact.med.yale.edu/teencope/Login.asp
Pilot/Feasibility Study
• 12 subjects assigned randomly by computer– 58% Female, 14.4 +.9 yrs.
• All data collection online
• Usage Patterns
• Preliminary outcomes to 3 months to date

Usage Patterns
• Excellent participation• Decreased slightly over time• 120 logins over 6 weeks of active intervention• TEENCOPE 2x as many logins as Education• High CDI (> 12) at baseline logged into the
website with the greatest frequency• TEENCOPE program engaged adolescents to a
greater extent and may be particularly appealing to adolescents with high levels of depressive symptoms.
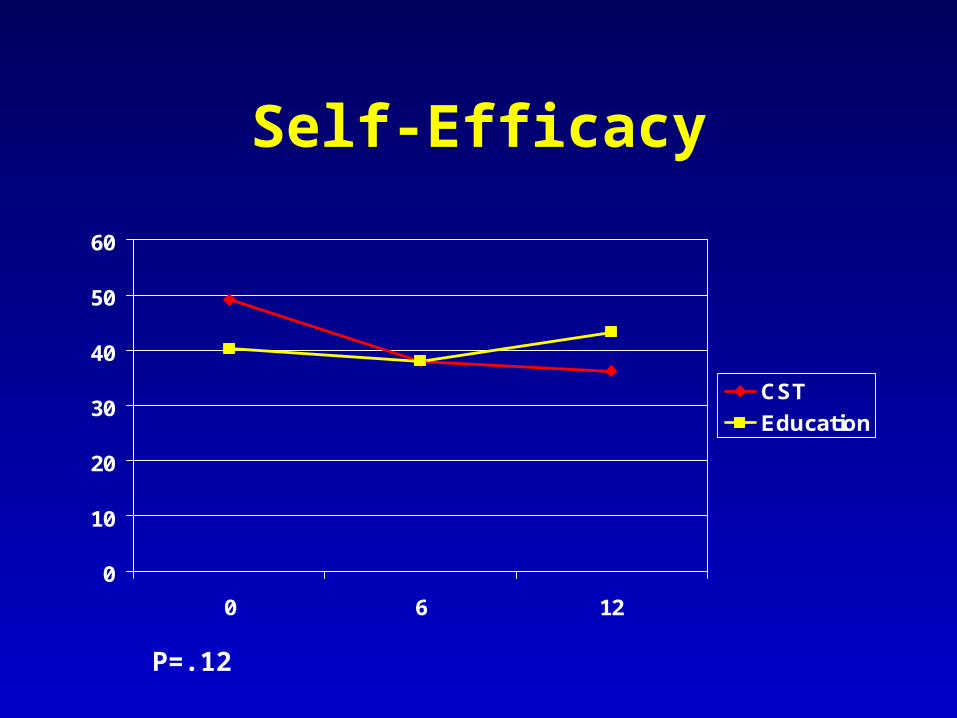
Self-Efficacy
0
10
20
30
40
50
60
0 6 12
CST
Education
P=.12

Quality of Life
68
70
72
74
76
78
80
82
84
0 6 12
CST
Education
P=.02

Proposed Study
• Enhance TEENCOPE with animation• Online data collection• Multi-site clinical trial
– Yale (mostly White)– CHOP (Black and Hispanic)– Arizona (Hispanic and White)
• 12 month follow-up• Mediators & Moderators

What we know…
• Incorporate behavioral approaches into standard diabetes care for youth with & at risk for diabetes
• CST is a useful adjunct to usual clinical care
• Goals of treatment involve not only enhancing metabolic outcomes but functional and quality of life

Acknowledgements
• Great research teams
• Funding– 1 & 2 R01NR04009– 1R21DK59248– 1R01NR008244


Thank You