Embed Size (px)
Citation preview

Interoperability:
Managing clinical diversity
Ian McNicoll
© Ocean Informatics 2011
“It must be kept in mind that interoperability implementation also depends on social, cultural and human factors within each organisation, region and country, each system and each time period.”
“Realising full interoperability is not necessarily a consensual goal in every place at any fixed time.”
SemanticHealth EU report
interoperability
© Ocean Informatics 2011
dysoperability
The „usual suspects‟ ?
Clinical ego, technophobia, vendor lock-in
Innovation, research
The consultant‟s MS-Access database
Information granularity
„Family history of breast cancer‟
GP, Breast Cancer unit, Research Genetics Unit
Organisational constraints
Health vs. social care
Financial constraints, Legal constraints
HB
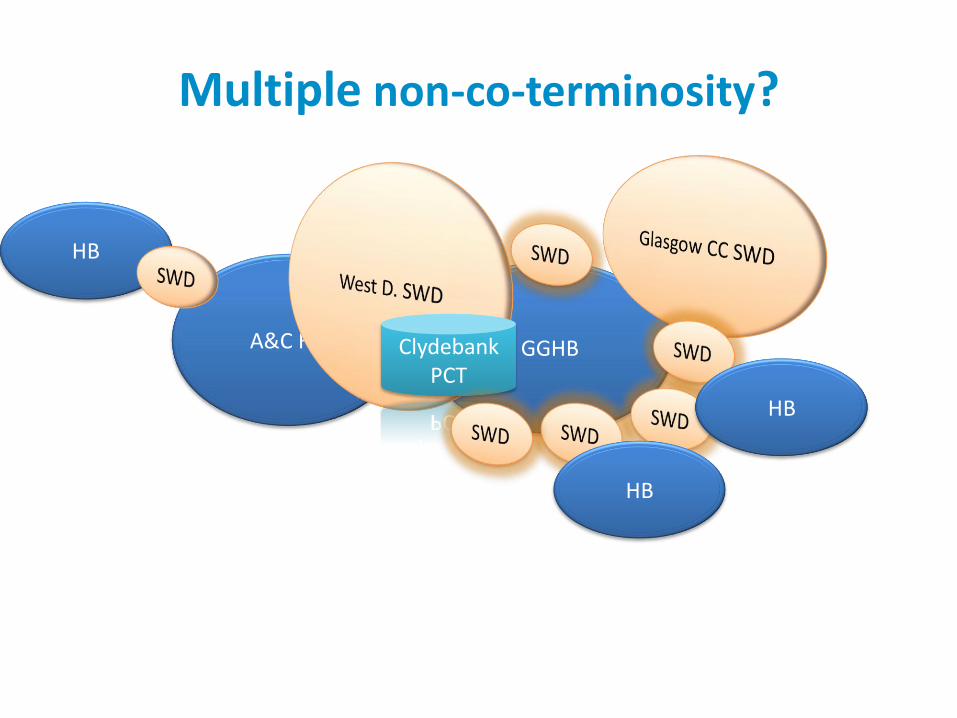
Multiple non-co-terminosity?
A&C HB GGHB Clydebank PCT
HB
HB
© Ocean Informatics 2011
• National clinical datasets
• National forms libraries
• National Care pathways
National clinical consensus
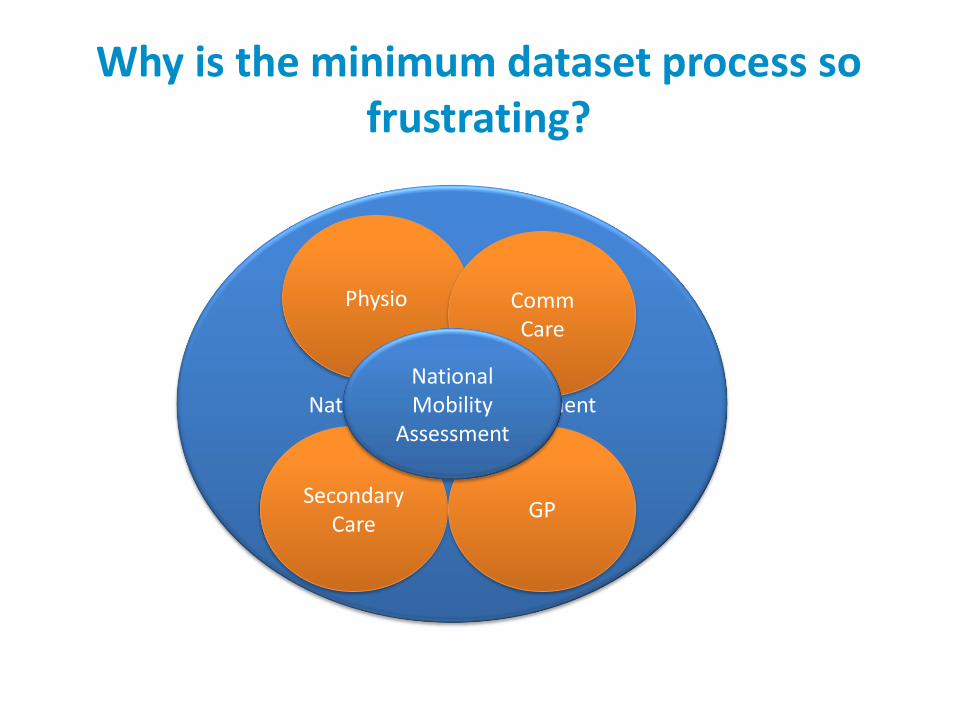
National Mobility Assessment
Why is the minimum dataset process so frustrating?
Physio
Secondary Care
GP
Comm Care
National Mobility
Assessment
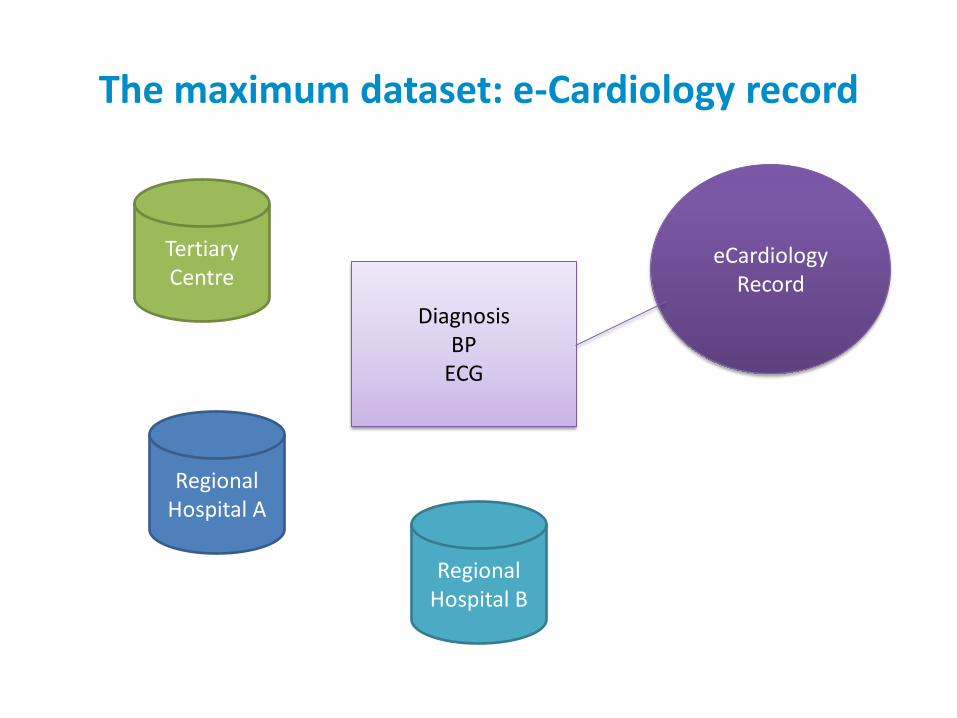
The maximum dataset: e-Cardiology record
Tertiary Centre
Regional Hospital A
Regional Hospital B
eCardiology Record
Diagnosis BP
ECG
Diagnosis BP
ECG
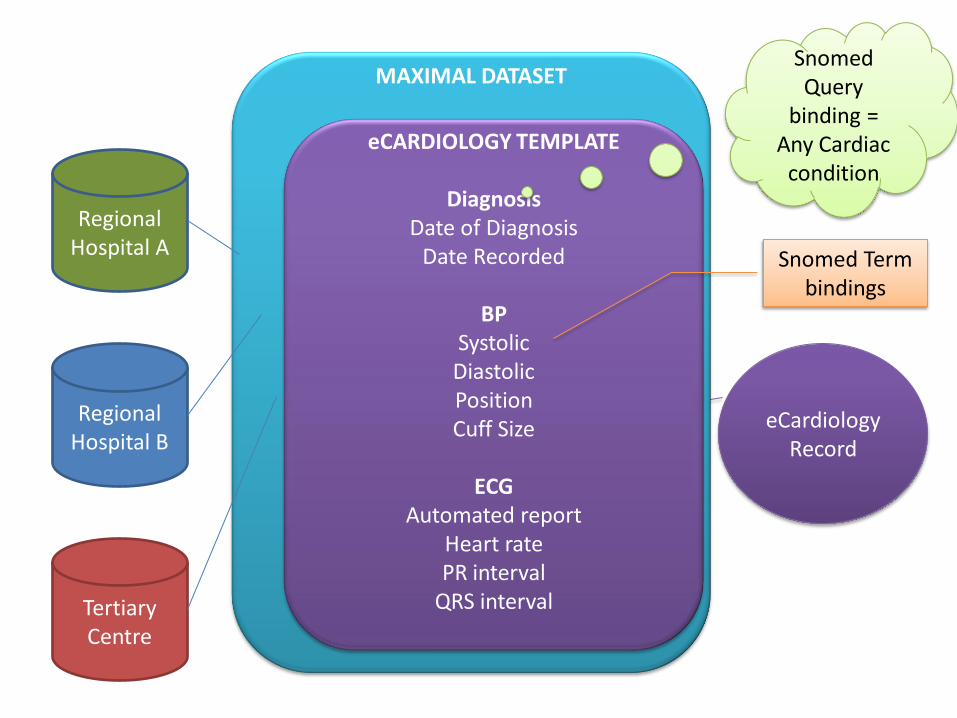
eCARDIOLOGY TEMPLATE
Diagnosis
Date of Diagnosis Date Recorded
BP
Systolic -163030003 Diastolic - 163031004
Position Cuff Size - 246153002
ECG
Automated report Heart rate PR interval
QRS interval
Diagnosis Date of Diagnosis
BP
Systolic Diastolic
Coded finding – “normal” Exertion level
Cuff size Position
ECG
Multimedia Automated report
Regional Hospital A
Regional Hospital B
Tertiary Centre
eCardiology Record
Diagnosis Date recorded
BP
Systolic Diastolic Cuff size Position
ECG
Automated report
Diagnosis Event Date
BP
Systolic Diastolic
ECG
Heart rate PR interval
QRS interval
MAXIMAL DATASET
Diagnosis Date of Diagnosis (Event Date)
Date Recorded
BP Systolic Diastolic
Coded finding – “normal” Exertion level
Cuff size Position
ECG
Multimedia Automated report
Heart rate PR interval
QRS interval
eCARDIOLOGY TEMPLATE
Diagnosis Date of Diagnosis
Date Recorded
BP Systolic
Diastolic Position Cuff Size
ECG
Automated report Heart rate PR interval
QRS interval
Snomed Term bindings
Snomed Query
binding = Any Cardiac
condition
© Ocean Informatics 2011
What does not work?
Clean–room, top-down technical modelling
Diktat by government
Late vendor involvement in model harmonisation
Message or „domain‟ driven modelling
Secondary uses driven modelling
Project-driven modelling without reusable clinical
concepts
© Ocean Informatics 2011
Embrace diversity
Break the endless strategic cycling between
central „ruthless standardisation‟
unconstrained local variation
Develop methodologies and tools that embrace
both
central standards and local variation
Allow standards to develop
Organically
by diktat (where circumstances are favourable)
in a controlled and cooperative environment
© Ocean Informatics 2011
Positively manage diversity Democratise clinical content modelling
Non-proprietary approach, widest natural community
possible
Modelling tools and methodologies must be
Clinically orientated, non-technical, minimise demands on
clinical time
Web 2.0 “social network” applications
Capture content at all organisational levels
Include diverse models
Today‟s outlier may be tomorrow‟s standard
Communicate who is modelling what
Federated approach “Subsidiarity”
© Ocean Informatics 2011
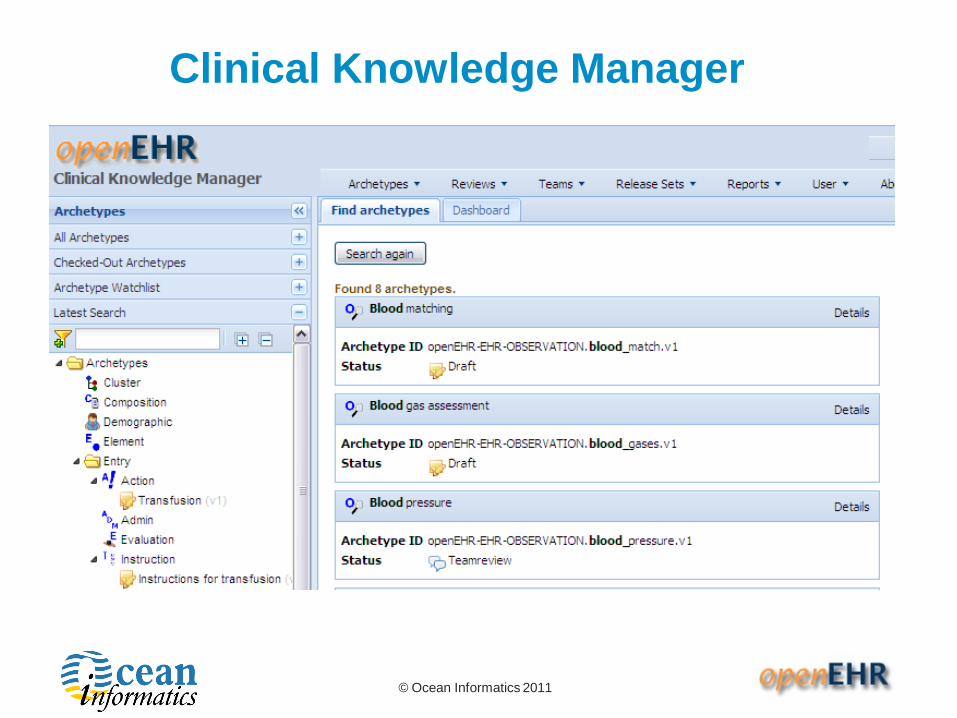
Web 2.0/3.0 collaboration
Clinical Knowledge Manager
Web based collaborative archetype/template/termset
reviews
Governed „authoring‟ environment
Community-led „archetype incubator‟
To encourage early, informal collaboration
Communication with clinical/technical stakeholders
Feeds CKM with early drafts
Lightly governed
© Ocean Informatics 2011
Clinical modelling capacity I
Core modelling team with clinical informatics
leadership Good understanding of openEHR paradigm and
appropriate use of terminology
Close involvement with international modelling efforts
Web- based collaborative authoring
Formal - CKM
Informal
© Ocean Informatics 2011
Clinical Knowledge Manager
© Ocean Informatics 2011
Building modelling capacity II
Good 2-way communications + relationships
Vendors (esp. clinical champions/ designers)
Professional clinical bodies
Academic units
Public health and reporting bodies
Ground level clinicians
build informatics expertise
Education and dissemination of skills
Who is doing what?
Who do I contact if I need new content?
Agile response to change request
© Ocean Informatics 2011
The risk of losing control…
“Let's look at a laboratory test result for example. Using
the HL7 RIM…. there are at least 7 ways within the
published standards to say the same thing….”
* Care Record
* Clinical Genomics Pedigree
* Clinical Document Architecture
* Clinical Statement
* Common Message Element Types
* Public Health Reporting: Individual Case Safety Report
* Periodic Reporting of Clinical Trials
* Laboratory Results
Keith Boone : http://motorcycleguy.blogspot.com/2009/07/at-rim-of-dam-or-edge-of-precipice.html
© Ocean Informatics 2011
In modern farming terms?
…combine the productivity and efficiency of high yield
„standardised‟ monoculture
… with the necessity of local bio-diversity
A semantic ecology?





























