Embed Size (px)
Citation preview
ManagingMedicalAlarms:A PracticalApproach toMeeting the JCAHO NationalPatient Safety Goal
Clinical Dynamics Corporation • 10 Capital Drive• Wallingford, CT • 203.269.0090 • Facsimile: 203.269.3402email:[email protected]
ManagingMedicalAlarms:A PracticalApproach toMeeting the JCAHO NationalPatient Safety GoalWritten by
Ode KeilOde Keil Consulting Group20497 Weatherstone RoadKildeer, IL 60047847-208-1173847-726-0137 [email protected]
Sponsored by
2
Clinical Dynamics Corporation • 10 Capital Drive • Wallingford, CT • 203.269.0090 • Facsimile: 203.269.3402email:[email protected]
Preface
The material in this guide is for informational purposes only and is subject tochange without notice. Ode Keil of Ode Keil Consulting Group assumes noresponsibility for any error or for consequential damages that may result fromthe misinterpretation of any content in this publication.
Ode Keil, is the President of The Ode Keil Consulting Group, which specializes inpreparing organizations for accreditation by the JCAHO. Areas of special expertiseinclude patient and workplace safety, performance improvement, emergencymanagement, and management of the environment of care. It is their mission toprovide clients with the skills and knowledge to provide very good patient care. TheOde Keil Consulting Group believes the best way to achieve this goal is to assess theneeds of individual organizations, design complete management processes, and workwith clients to hardwire the processes to assure safe, effective management of patientcare and the environment of care.
About the Author
Founded in 1990, Clinical Dynamics designs, manufactures and markets biomedicaltest equipment for biomedical engineers, independent service organizations andmedical device manufacturers worldwide. All Clinical Dynamics products include theindustry’s only standard three-year parts and labor warranty.
About Clinical Dynamics
3
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
IIIInnnnttttrrrroooodddduuuuccccttttiiiioooonnnn::::
Concerns about the function of alarms and timely and appropriate staff response toalarms are familiar issues to healthcare workers. Whether it is fire alarms, medical gasalarms, or medical equipment alarms there is a history of problems with both alarmfunction and staff response. Unfortunately, in some cases permanent injury or death hasresulted.
Beginning in July of 2002, the Joint Commission on Accreditation of HealthcareOrganizations (JCAHO) acted on this knowledge. The JCAHO issues a set of sixNational Patient Safety Goals (NPSG) that included one addressing the function and staffresponse to medical alarms. Through the NPSG, the JCAHO is using its leverage as arespected accrediting body to force healthcare organizations to evaluate whether they aremanaging medical alarms and the other issues addressed by the NPSG in an effectivemanner.
Clinical Dynamics has a strong commitment to patient safety and to maximizing theperformance of medical equipment. This monograph and the accompanying templates aredesigned to assist Clinical DynamicsÕ customers to develop effective medical alarmmanagement programs and to document reliable alarm function and staff performance. Itis the sincere desire of Clinical Dynamics management and staff to be more than anequipment seller. Through this and other efforts we want to demonstrate that we desire todevelop a partnership for patient care quality and safety with every Clinical Dynamicscustomer.
BBBBaaaacccckkkkggggrrrroooouuuunnnndddd::::
Beginning January 1, 2003 all JCAHO accredited healthcare organizations were requiredto demonstrate compliance with six NPSG. A seventh goal was added for 2004. TheNPSG are not accreditation standards. Rather, they are eligibility requirements. TheJCAHO Board of Commissioners and patient safety advisory panel felt so strongly thatthe NPSG represent such significant threats to patient safety that organizations are noteven eligible for accreditation unless they implement the recommended practices relatedto each NPSG. The JCAHO does allow organization to submit documentation of analternative solution to any of the recommendations. If the patient safety advisory panelapproves the alternative, it is considered equivalent to the NPSG.
The JCAHO does not want compliance with the NPSG to become a significant burden foraccredited organizations. The JCAHO believes that many organizations already haveaddressed this and the other NPSG to a significant degree. They also believe that thereare parts of the medical alarm system that are not managed effectively and organizationswill have to enhance existing efforts. The overall concern about medical alarms wastriggered by a JCAHO review of 23 ventilator incidents that resulted in patient injury ordeath. As documented in a Sentinel Event alert published February 26, 2002, more than
Written by Ode Keil for Clinical Dynamics
4
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
half the events were, at least in part, due to an alarm problem. Some instances of alarmmalfunction were identified, as were instances of staff failing to activate alarms andinstances where staff did not hear alarms due to environmental factors.
This wide variety of causes led the JCAHO to address the safety of medical alarms in amore comprehensive manner than they have addressed any other medical technology.Historically, the focus of the JCAHO standards and survey process for medicalequipment management has been primarily on preventive maintenance, safety testing,and performance testing of devices. The NPSG for medical alarms added the dimensionsof the environment of use and staff knowledge and performance. The NPSG addresses,for the first time, all the elements of a medical technology. The added dimensions are theareas that accredited organizations are most likely to improve.
A key point when addressing the medical alarm NPSG is to recognize that the issuesaddressed by the Goal are not wide spread. There is not a crisis of equipment reliabilityor staff performance that requires scheduling of additional tests or inspections. Rather, itrecognizes that in the increasingly complex environment of the modern healthcareorganization, managers and staff need to be aware that there are risks related to any typeof equipment or environment. They must develop processes to identify the risks and usethat knowledge to develop appropriate procedures and controls to eliminate or mange therisks. This paper and template document set provides a starting point for any accreditedorganization to meet these challenges.
A broad definition will be used to determine which equipment and systems are served bya medical alarm device or system. Medical alarms are sensing and indicating devices thatare integral parts of equipment or systems designed to diagnose, treat, or monitorpatients. In addition, medical alarms are sensing and indicating devices that are integralparts of equipment or systems designed for patient safety, security, or that supplyessential resources for patient care.
Based on this definition this document provides a general management summarytemplate, tools to assess alarm related risks, tools to assess alarm criticality, andrecommended practices for managing a variety of medical alarm related issues.
Alarm related problems occur for a variety of reasons. Some of the common findingsinclude deactivation of the alarms, settings that are not appropriate for the patient orparameter being monitored, excessive activation of alarms, poor staff training, andenvironmental conditions that made hearing the alarm difficult or impossible to hear.
All of these can be managed if they are identified and analyzed. For example, managingthe frequency with which alarms are not set appropriately can be managed by evaluationof equipment at the time of purchase to identify poor design. Minimizing the selection ofequipment that has alarms that can be turned off or muted significantly reduces onepotential problem related to alarm audibility. Evaluating audibility during equipment
Written by Ode Keil for Clinical Dynamics
5
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
trials and working with manufacturers to redesign alarms before purchase can help reduceproblems with environmental problems. An alternate is to limit use of critical devices toareas where there is a permanent staff presence. For example, limiting use of ventilatorsto critical care areas where high staffing rations and staff design help assure alarms willbe heard.
Meeting the JCAHO expectations is not impossible or burdensome. It does requireassessment, planning, design, implementation, measurement and evaluation of processesto reduce alarm related problems. The JCAHO does not require accredited organizationsto maintain any specific documentation of these activities. However, it is always prudentto be prepared to show surveyors documentation of any required activity. Using thematerials included in this report will provide all the information an organization shouldneed to demonstrate to surveyors what is done to manage alarm related problems.
Written by Ode Keil for Clinical Dynamics
6
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
AAAA TTTTeeeemmmmppppllllaaaatttteeee MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmm MMMMaaaannnnaaaaggggeeeemmmmeeeennnntttt PPPPrrrrooooggggrrrraaaammmm::::
MMMMaaaannnnaaaaggggeeeemmmmeeeennnntttt SSSSuuuummmmmmmmaaaarrrryyyy ooooffff tttthhhheeee MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmm MMMMaaaannnnaaaaggggeeeemmmmeeeennnntttt SSSSttttrrrraaaatttteeeeggggyyyy ooooffff<<<<<<<<OOOOrrrrggggaaaannnniiiizzzzaaaattttiiiioooonnnn NNNNaaaammmmeeee>>>>>>>>
Alarms are integral parts of many types of medical equipment. The alarms are providedto notify staff to check the status of the equipment or to assess and respond to changes inthe condition of a patient. <<Organization name>> is committed to assuring that allpatient care is provided in a manner that assures high quality and safety. Part of thiscommitment is assuring that medical alarms are managed in a manner that maximizes theeffectiveness of each system. The management of medical alarms includes assessment ofpatient care processes to determine which medical alarms play a role in detecting changesin the environment or the condition of the patient that may adversely affect the outcomeof care. The program for management of alarms then evaluates the criticality of thealarm. Based on the function and criticality of each identified medical alarm, appropriateprocedures and controls will be developed, education and training developed anddelivered, and a quality monitoring program will be implemented to maximize theeffectiveness of the alarms.
Teams made up of appropriate representatives from the medical staff, nursing, facilitiesmanagement, administration, biomedical engineering, and, when appropriate,manufacturers will perform a risk assessment of each clinical area where medical alarmsare part of the environment or equipment used on patients to evaluate the function andcriticality of each alarm. Each team will then develop appropriate procedures andcontrols for assuring reliable performance of the alarm technology and the staffresponsible for managing the alarm. The evaluation will include the alarm device, theenvironment where it is installed or used and human factors that may affect the reliabilityor effectiveness of the alarm.
The procedures and controls will include, as appropriate, a program of plannedmaintenance, staff education and training, and monitoring of performance. All policies,procedures, educational materials, performance measures, and forms developed by theteams will be presented to the Environment of Care and Patient Safety Committees forapproval.
RRRRiiiisssskkkk aaaasssssssseeeessssssssmmmmeeeennnntttt
Risk assessment is a process designed to identify how a process or system might fail andwhat the consequences of the failure would be. The risk assessment for medical alarmsconsiders three issues. First is patient safety. The function of each alarm is evaluated andan assessment of what adverse outcomes of care could occur if an alarm is not managedproperly. Second is criticality. The severity of the identified consequences is evaluated todetermine if it is simply an inconvenience for the patient or there is an imminent threat ofpermanent injury or death. The third is evaluation of alarm design and environmental
Written by Ode Keil for Clinical Dynamics
7
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
Written by Ode Keil for Clinical Dynamics
factors that would contribute to an alarm related problem. The concurrent analysis of thesethree factors can lead to a rational approach to managing alarms.
The risk assessment will consist of the following activities:
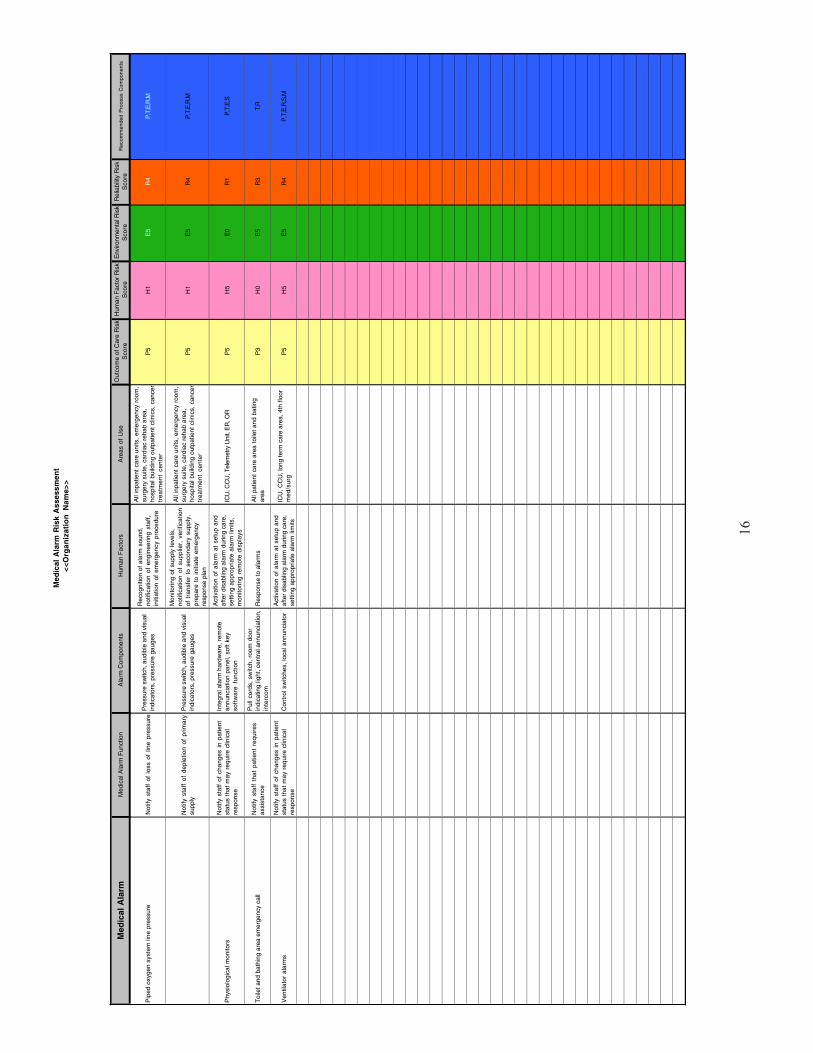
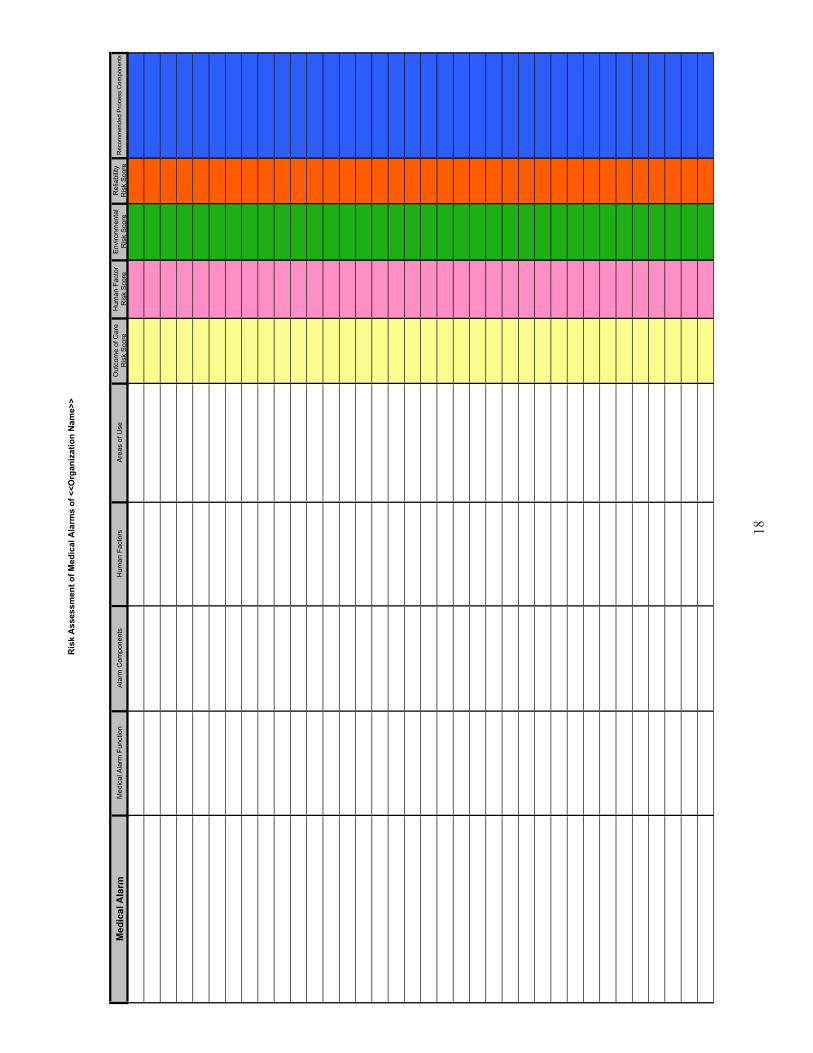
1. Development of a matrix of all medical alarms. The matrix will include the alarm,describe its purpose, identify the hardware and software components of the alarm,human factors related to setting and managing the alarm while in use, and areas wherethe equipment containing the alarm is used or installed.
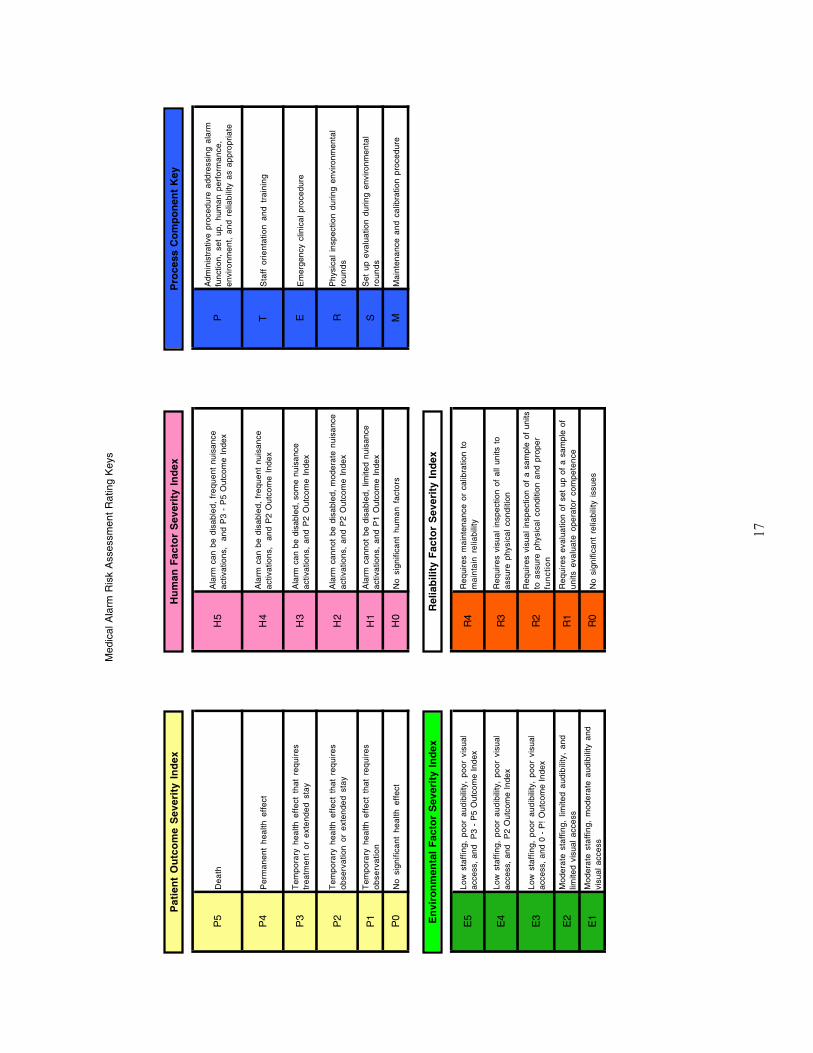
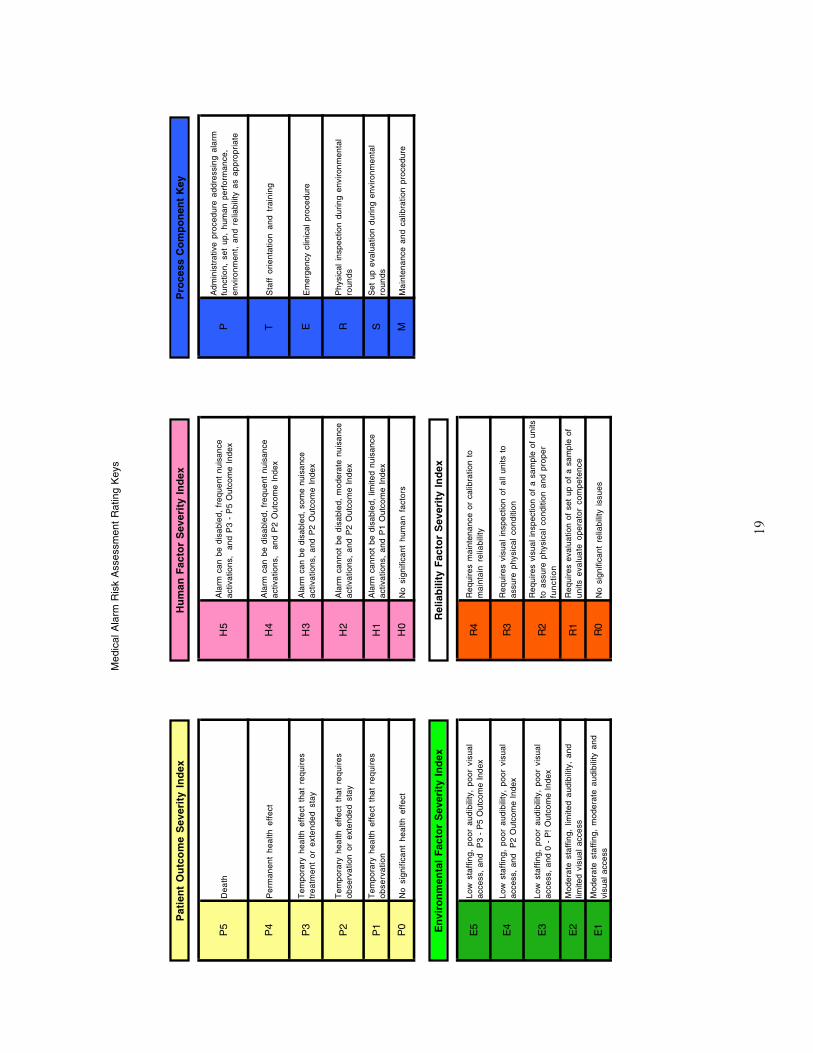
2. Determination of the potential severity of alarm related issues on patient outcomes.The rating should cover the spectrum of severity from nuisance to permanent injury ordeath of a patient.
3. Determination of the criticality of human factors. This step considers factors such assetting alarm limits and activation of alarms. This factor is used to determine whattraining and quality control activities are required to help assure appropriate operatorperformance.
4. Identification of environmental factors that would affect the probability that an alarmwill be heard. This factor is used to determine if the design of the alarm needs to bemodified, changes need to be made in a particular environment, or if use of devicesneeds to be restricted to specific locations when other changes cannot be made.
5. Assessment of field experience with the alarm to determine if there is a history ofdevice related problems reported in the literature or during use in the organization. Thisfactor is used to determine if a program of inspection or maintenance is required toassure proper functioning of the alarm.
Each factor is rated independently. Whenever any factor is considered significant, the teamwill design a strategy for managing the alarm related issues identified. It is possible thatdifferent strategies will be required for different locations using the same equipment.
In general, intermediate and general care areas present more challenges than intensivecare units. The intermediate and general care areas are spread out, staffing levels arelower, and staff is usually not as familiar with equipment containing alarms as staff incritical care areas. It is recommended that intermediate and general care areas whereequipment with alarms be given priority when there are limited resources.
A template risk assessment tool and a brief example are included with this document. Thetool is built as a Microsoft Excel® spreadsheet. Development of a complete risk assessmentis the first step in developing an effective alarm management strategy and plan.
8
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
MMMMaaaannnnaaaaggggiiiinnnngggg HHHHuuuummmmaaaannnn FFFFaaaaccccttttoooorrrrssss
Human performance is the most important variable in managing alarms. The key humanperformance issues include knowledge of how to set up alarms, management of alarmsduring use, and responding to alarms. Each of these issues is related to the managementof medical alarms through administrative and engineering controls, management of theenvironment where equipment or systems with alarms are used or installed, andmanagement of the reliability of alarms.
Staff knowledge of the operation of alarms plays a critical role in determining theeffectiveness of medical alarms. Generally, clinical staff working in critical care areas iswell trained and proficient in the set up and management of alarms. Clinical staffworking is intermediate or general care areas tend to be less familiar with alarm set upand function. This is also often true of clinical staff that ÒfloatsÓ between units to meetstaffing requirements.
EEEEvvvvaaaalllluuuuaaaattttiiiioooonnnn ooooffff HHHHuuuummmmaaaannnn FFFFaaaaccccttttoooorrrrssss::::
Evaluation of the human factors should be done as part of the initiation of medical alarmmanagement program and whenever systems or equipment with alarms are purchased inthe future. Managing the human factors related to alarm effectiveness includes thefollowing steps:
1. Evaluation of alarm design
The evaluation should result in a list of issues that staff must be aware of andskills they must develop for the alarm to be effective. One key issue is thelocation and function of controls. The controls may be analog switches orsoftware functions activated through a touch screen or keyboard. Another is whatthe purpose the controls serve. For example, controls may activate or deactivatethe alarm or allow the alarm signal volume to be affected.
The product of the evaluation of the controls should be a listing of each control,its function, and the action required by the operator to assure proper function at alltimes the alarm is in use on a patient. The list should be used to develop aprotocol for setting up features such as limits and audio properties for each criticalmedical alarm.
2. Evaluation of the environment of use
Evaluation of the environment should include an assessment of the visibility andaudibility of alarm indicators under normal operating conditions. This assessmentmust take into account staffing levels, normal staff activities, the distinctivenessof the sound the alarm generates when activated, and the alarm signal intensity.For alarms such as the toilet and bathing area alarms activated by patients, theassessment must also consider accessibility of the activating mechanism.
Written by Ode Keil for Clinical Dynamics
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
9Written by Ode Keil for Clinical Dynamics
Staff Education:
Staff education addressing management of medical alarms must be based on theassessments described above. The manufacturer of each piece of equipment and eachsystem with an alarm function makes assumptions about the knowledge and skills ofoperators. The assessments described above are intended to identify these assumptions.The education process is intended to assure that staff develops the knowledge and skills tominimize the potential for human error that results in adverse patient outcomes. Theeducation needs to focus on alarm function. Operators must understand how the alarmcontrols are manipulated to achieve the desired alarm function, the logic of the alarmsystem, and how to set alarm features including alarm limits. The education must alsofocus on environmental and reliability factors that must be managed in a specific manner tominimize the potential for the occurrence of alarm related incidents.
The product of the environmental evaluation should be a listing of all the identifiedfactors and elements of the procedures and protocols staff must learn to adapt toshortcomings in the environment. For example, if stand-alone alarms serve a criticalfunction, a policy that doors cannot be closed in some areas may be required toassure staff can hear an alarm. Alternatively, the evaluation may determine thatsome equipment with stand-alone alarms is not suitable for use in some areas. Ifequipment with stand alone alarms must be used in areas where there is pooraudibility or visual access, the alarm or the space may have to be reengineered orthe equipment may have to be replaced when there is no way to overcome theidentified challenges operationally.
3. Evaluation of Reliability
Evaluation of reliability should assess what steps staff must take to check thefunction of alarms and the frequency of reliability checks. The product of thisassessment may be simple operator “pre-flight” checks performed using self testfeatures of alarm systems that is performed as part of the alarm managementprotocol. The product may also be a technical protocol for performing calibration,inspection, or maintenance activities. The protocol may be part of a largerpreventive maintenance protocol for an entire piece of equipment or a system. Theprotocol should specify the frequency for performing the required activities, the testmethod, required test equipment, and required documentation.
Any technical test protocol must conform to the general requirements of the JCAHOmedical equipment management standards found in the Management of theEnvironment of Care® 1 standards.
1Comprehensive Accreditation Manual for Hospitals, 2004 JCAHO, Oakbrook Terrace, IL 2004.
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
SSSSttttaaaaffffffff PPPPeeeerrrrffffoooorrrrmmmmaaaannnncccceeee MMMMeeeeaaaassssuuuurrrreeeemmmmeeeennnntttt aaaannnndddd EEEEvvvvaaaalllluuuuaaaattttiiiioooonnnn::::
Measurement and evaluation of staff performance is a key part of assuring alarmreliability. Design of the staff education protocols must include a method for assessingstaff knowledge and competence at the time of the education and on an ongoing basis.
Evaluation at the time of education can be done using written or oral tests of knowledgeand return demonstrations of alarm operation. The return demonstrations can be enhancedby use of simulators. Some sophisticated simulated patients can mimic critical bodyfunction parameters in a manner that requires effective set up of equipment, setting oralarms, and response to alarms to prevent ÒdeathÓ. It this type of technology is available,it can greatly enhance the effectiveness of training.
Measurement and evaluation of performance over time can be done in a variety of ways.It can be evaluated using return demonstration as part of a Òskills dayÓ. It can also bedone using written knowledge evaluations as part of performance appraisals. It isrecommended that the measurement be done by incorporating observation of the settingsof equipment serving patients into the environmental rounds process. This can be donewithout undue disturbance of patients and is a highly reliable indicator of both theknowledge of staff about equipment function and the diligence with which staffimplements equipment operation protocols. For example, performance of staff on specificclinical care units can be evaluated, staff performance related to a particular type ofequipment or a system can be studied, or the performance of a particular staff disciplinecan be studied.
Whichever approach is chosen, the measurement and evaluation procedure must bedesigned in a manner that provides enough data to get a good picture of how well staff isperforming. A performance measurement and evaluation template and a simple exampleare included as part of this monograph.
MMMMaaaannnnaaaaggggiiiinnnngggg EEEEnnnnvvvviiiirrrroooonnnnmmmmeeeennnnttttaaaallll FFFFaaaaccccttttoooorrrrssss
The environment in which equipment or a system with integral alarms is used or installedcan play a pivotal role in the effectiveness. The issues introduced earlier in thismonograph must be assessed for all current equipment and systems with integral alarms.In addition, the environment must be considered when contemplating the purchase ofnew equipment and systems. The key considerations include audibility, visibility, andaccessibility. Evaluation of these factors as part of the risk assessment process isessential.
Audibility is one of the most frequently reported alarm related problems. Assessingaudibility requires consideration of several variables. They include the distance that staffcan be from the source of an alarm. In addition, the path the alarm signal must travel to
10Written by Ode Keil for Clinical Dynamics
11
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
reach a staff member must be evaluated. Obstructions to sound such as angled surfacesand doors play a significant role in the attenuation of sound. It is important to rememberthat sound waves are a physical phenomenon. The intensity of the sound wave decreasesas the square of the distance from the source. In addition, sound is easily reflected orredirected by hard surfaces and is absorbed by soft surfaces such as carpet and curtains.The entire path of travel for alarm signals must be evaluated. Limiting the evaluation towhether doors can be closed to obstruct transmission of the sound waves is important butis not the only consideration.
Some alarm systems include visible indicators. A common example is an indicator lightactivated by a toilet or bathing area alarm. The assessment of any alarm system thatincludes a visible indicator must consider how critical the visible indicator is to locatingthe source of the alarm. If the visible indicator is a critical part of locating a patient indistress, then the risk assessment must determine if the indicators can be seen at all timesby a qualified staff member. If staffing levels or the layout of an area preventvisualization of an alarm indicator at all times, a potential solution is to install remoteindicating panels in areas that are continuously attended. This is a common practice withcardiopulmonary emergency alarm systems. A signal is transmitted to a remote locationsuch as a communication systems center that is staffed continuously. The staff in theremote location has paging or other communication systems that are designed to alertappropriate response staff wherever they are located.
Accessibility is a key characteristic of emergency alarms that require activation bypatients or staff. Examples of such alarms are medical emergency alarms, toilet andbathing area alarms, and staff distress alarms. The assessment for accessibility requiresevaluation of whether or not the individual who must activate the alarm can move to analarm activating device. In general, the urgent need for help related to the activation ofany of the listed types of alarms precludes significant movement to an alarm activationstation. In cases such as these, a determination needs to be made of the best way toprovide an activation point close to the individual in need.
Medical distress alarms should be located in the immediate vicinity of patient beds ortreatment stretchers in high risk patient care areas. They should be visibly marked andoperable with little effort. Assessment of the activation switches for medical distressalarms should include visibility, accessibility from normal work positions, and ease ofoperation.
Alarms in toilet and bathing areas should be accessible from waist to floor level. This isgenerally accomplished by connecting a cord to a switch that is activated by a gentle tug.Assessment of the alarm activation switches and cords needs to include evaluation ofobstructions to reaching the cord and obstructions to pulling the cord. Obstructions couldinclude walls, grab bars, and shower doors or curtains. If switches or cords areobstructed, changes in the environment need to be made to eliminate or reduce thepotential that the alarms can be disabled.
Written by Ode Keil for Clinical Dynamics
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
Personal distress alarms are becoming more prevalent in emergency care and behavioralhealth areas. They are primarily used by staff to alert security or other personnel todangerous situations that may include violent behavior. Some personal distress alarms arealso used by staff to notify security or other personnel of conflict between patients.Assessment of the environment where personal distress alarms are deployed needs toinclude the same considerations listed in the medical distress alarm paragraph. Aspersonal distress alarms must often be activated while physically engaged with a patientor other individual, strong consideration should be given to placing the activation deviceon the person facing potential danger.
In summary, managing the environment of medical alarms can be far m ore complex thansimply establishing policies requiring keeping doors open. The environment includesphysical and functional considerations. The primary problem with the environment iscreation of obstructions that prevent or delay activation and awareness of alarms. If theenvironment disrupts the function of any alarm, it is as if no alarm was ever present. Thisis a severe problem and requires diligent analysis and ongoing field assessment todetermine if any changes in staffing or the layout of space degrade alarm performanceover time.
MMMMaaaannnnaaaaggggiiiinnnngggg RRRReeeelllliiiiaaaabbbbiiiilllliiiittttyyyy
Medical alarms devices have proven to be very reliable. Current medical equipmentmanagement programs generally include activation of alarms and checking alarmfunctions as part of scheduled safety and functional testing procedures. As with theenvironment, managing reliability includes more than simple testing of alarm functions.The reliability of staff is a critical part of alarm function. If staff is not skilled inunderstanding the operation and concept of alarms and does not respond to alarms, thevalue of the affected alarm is negated.
Managing the reliability of staff has two phases. The first is determining if staff ismanaging alarms currently in place effectively. This can be done as part of the riskassessment. The risk assessment needs to evaluate the level of staff knowledge of currentalarms and whether they respond appropriately when alarms sound. The level ofknowledge can be measured by direct observation of staff skills, written or oral exams ora similar approach. Not all staff members need to be evaluated. A random selection ofstaff in clinical areas can be used to evaluate the general level of current knowledge.Similarly, the level of response can be measured by observation or physical testing. Theobservation can be incorporated into scheduled management or environmental rounds.The testing can also be part of the rounds. The testing is performed by activating alarmsand evaluating staff response. The effectiveness of response can be evaluated bymeasuring the time of response and whether appropriate staff responds.
Measurement of staff for future equipment purchases begins at the time of evaluation.Staff expected to operate the equipment should be included in the evaluation. Throughparticipation in the evaluation and clinical trials of equipment, front line staff can helpidentify design related or functional problems that may affect staff reliability.
12Written by Ode Keil for Clinical Dynamics
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
Based on the findings of the evaluation, initial education and training can be developed.The education and training can include a Òpreventive maintenanceÓ component. ThePreventive maintenance component could be scheduled refresher training at intervals.The intervals can initially be hardwired at specific times. Through performancemeasurement and assessment the level of staff reliability can be assessed. Once the levelof reliability is stabilized at an acceptable level, the reinforcement intervals can becontrolled by the results of measurement.
SSSSuuuummmmmmmmaaaarrrryyyy
There is no program that will eliminate all alarm related problems. The approachdescribed in this monograph is intended to focus on alarms that have the greatestpotential for affecting patient outcomes. As indicated earlier, based on availableinformation, the greatest risks exist in intermediate and general care areas. These areas donot have the high nurse-to-patient ratios found in intensive care areas. The intermediateand general care areas are often served by long hallways and the patient rooms aredesigned to provide privacy and dignity for patients. The long hallways and the potentialthat doors are closed virtually guarantees that staff will not be able to hear alarms in somerooms in such areas.
Another key factor is the level of preparation related to working with equipment. Staff incritical care areas is generally more familiar with the use and function of alarms. Thetraining they receive is reinforced by daily exposure. The staff in intermediate andgeneral care areas generally has intermittent exposure to equipment with alarms.
Development of an effective program requires development of an action plan. Theelements of the plan are listed in figure 1.
Figure 1.Each listed step is critical. This monograph presents a broad description of each. Thedetails must be worked through at each organization. A final brief description of eachstep is designed to provide a roadmap for getting started.
1. Create teams for major groupings of alarms2. Conduct a risk assessment3. Establish priorities4. Determine the current baseline of performance5. Develop correction action plans6. Design management protocols for alarm groupings7. Implement corrective actions8. Implement protocols for future alarms9. Measure and evaluate performance10. Improve programs based on findings
13Written by Ode Keil for Clinical Dynamics
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
14Written by Ode Keil for Clinical Dynamics
Create teams for major alarm groupings
The JCAHO lists a wide variety of specific alarms in the FAQ’s posted on its’ website www.jcaho.org. The list includes alarms as diverse as ventilators and infantabduction systems. Two general major groupings can be created based on the list.One is direct clinical the other is indirect clinical/environmental.
The direct clinical alarms include all alarms that directly monitor patientparameters. For example, physiological monitors and pulse oximeters. The indirectclinical/environmental includes alarms that monitor utility systems andenvironmental situations. Examples include medical air and oxygen andelopement alarms.
Two teams are recommended because the responsibilities of the individuals thatinteract with the alarms are different.
Conduct a Risk Assessment
The risk assessment examines current alarms and the processes in place tomange them. The risk assessment considers direct patient risk, environmentalrisk, reliability, and human factor risks. The product of the risk assessment is aroad map for correcting current issues and designing protocols for managing eachtype of alarm.
It may not be practical to develop a single protocol for managing all the types ofalarms addressed by the NPSG. As with the teams, at least two protocols arerecommended to manage direct clinical and indirect clinical/environmental alarms.
Establish Priorities
The key to establishing priorities is evaluation of the environment. When alarmsare used in areas that are geographically large, thinly staffed, and the alarms arenot present on a frequent basis, the areas should be considered higher prioritythan areas that are concentrated, heavily staffed, and technology intensive.
Determine baseline performance
Determining baseline performance is important as part of managing performanceimprovement activities. Unless the baseline is known it is difficult to focusimprovement efforts on areas of need. Determination of the baseline ofperformance should assess the current level of performance in high priority areasand whether there are general patterns of deficiencies. For example, recognitionof the medical gas alarm might be a general issue where audibility of ventilatoralarms is an issue in a specific location.
1.
2.
3.
4.
MMMMaaaannnnaaaaggggiiiinnnngggg MMMMeeeeddddiiiiccccaaaallll AAAAllllaaaarrrrmmmmssssAAAA PPPPrrrraaaaccccttttiiiiccccaaaallll AAAApppppppprrrrooooaaaacccchhhh ttttoooo MMMMeeeeeeeettttiiiinnnngggg tttthhhheeee JJJJCCCCAAAAHHHHOOOO NNNNaaaattttiiiioooonnnnaaaallll PPPPaaaattttiiiieeeennnntttt SSSSaaaaffffeeeettttyyyy GGGGooooaaaallll
5555.... DDDDeeeevvvveeeelllloooopppp AAAAccccttttiiiioooonnnn PPPPllllaaaannnnssss
Action plans should be identified as either short term action to address specificissues or longer term improvement projects to make changes in processes. Shortterm actions would most likely be related to the physical environment. Forexample, limiting treatment of ventilator dependent patients to intensive care unitsto address audibility concerns can be done immediately. A change in processcould be a redesign of the medical equipment selection and acquisition process toassure comprehensive evaluation of JCAHO and other patient safety concernsprior to purchase.
6666.... DDDDeeeessssiiiiggggnnnn MMMMaaaannnnaaaaggggeeeemmmmeeeennnntttt PPPPrrrroooottttooooccccoooollllssss ffffoooorrrr AAAAllllaaaarrrrmmmm GGGGrrrroooouuuuppppiiiinnnnggggssss
If alarms are grouped by risk, protocols addressing restriction of use of equipmentto specific areas, staff education and competence assessment related to specifictypes of alarms, and calibration, inspection, maintenance, or testing requirementsshould be developed for each alarm grouping. This approach is recommended toassure all elements of the system that must work for each type of alarm to beeffective are addressed in an appropriate manner.
Developing separate activities for the different elements of an alarm system islikely to result in over laps or gaps in assessing the performance of the alarmhardware and software and the human element.
7777.... IIIImmmmpppplllleeeemmmmeeeennnntttt CCCCoooorrrrrrrreeeeccccttttiiiivvvveeee AAAAccccttttiiiioooonnnnssss
This step includes three activities. The first is self explanatory. The changes madeto current practices are initiated. The second activity is active removal of allunwanted or unacceptable practices or conditions. Elimination of unwanted orunacceptable practices is essential to the overall success of the medical alarmimprovement project. The third activity is initiation of measurement andevaluation to determine if improved performance is attained.
8888.... MMMMeeeeaaaassssuuuurrrreeee aaaannnndddd EEEEvvvvaaaalllluuuuaaaatttteeee PPPPeeeerrrrffffoooorrrrmmmmaaaannnncccceeee
Measurement and evaluation of performance against the previously determinedbaselines of performance must be continued until it is clear that a stable,sustainable, and acceptable level of performance has been attained.
9999.... IIIImmmmpppprrrroooovvvveeee PPPPrrrrooooggggrrrraaaammmmssss BBBBaaaasssseeeedddd oooonnnn FFFFiiiinnnnddddiiiinnnnggggssss
Measurement and evaluation of the changes in the program may reveal areas ofcontinued weakness. These should be addressed in an iterative fashion until anacceptable level of performance is attained and maintained.
15Written by Ode Keil for Clinical Dynamics
16
Med
ical
Ala
rm R
isk
Ass
essm
ent
<<
Org
aniz
atio
n N
ame>
>
Med
ical
Ala
rmM
edic
al A
larm
Fun
ctio
nA
larm
Com
pone
nts
Hum
an F
acto
rsA
reas
of
Use
Out
com
e of
Car
e R
isk
Sco
reH
uman
Fac
tor
Ris
k S
core
Env
ironm
enta
l Ris
k S
core
Rel
iabi
lity
Ris
k S
core
Rec
omm
ende
d P
roce
ss C
ompo
nent
s
Pip
ed o
xyge
n sy
stem
line
pre
ssur
eN
otify
sta
ff of
los
s of
lin
e pr
essu
reP
ress
ure
switc
h, a
udib
le a
nd v
isua
l in
dica
tors
, pre
ssur
e ga
uges
Rec
ogni
tion
of a
larm
sou
nd,
notif
icat
ion
of e
ngin
eerin
g st
aff,
initi
atio
n of
em
erge
ncy
proc
edur
e
All
inpa
tient
car
e un
its,
emer
genc
y ro
om,
surg
ery
suite
, car
diac
reh
ab a
rea,
ho
spita
l bui
ldin
g ou
tpat
ient
clin
ics,
can
cer
trea
tmen
t ce
nter
P5
H1
E5
R4
P,T
,E,R
,M
Not
ify s
taff
of d
eple
tion
of p
rimar
y su
pply
Pre
ssur
e sw
itch,
aud
ible
and
vis
ual
indi
cato
rs, p
ress
ure
gaug
es
Mon
itorin
g of
sup
ply
leve
ls,
notif
icat
ion
of s
uppl
ier,
ver
ifica
tion
of t
rans
fer
to s
econ
dary
sup
ply,
pr
epar
e to
initi
ate
emer
genc
y re
spon
se p
lan
All
inpa
tient
car
e un
its,
emer
genc
y ro
om,
surg
ery
suite
, car
diac
reh
ab a
rea,
ho
spita
l bui
ldin
g ou
tpat
ient
clin
ics,
can
cer
trea
tmen
t ce
nter
P5
H1
E5
R4
P,T
,E,R
,M
Phy
siol
ogic
al m
onito
rsN
otify
sta
ff of
cha
nges
in
patie
nt
stat
us t
hat
may
req
uire
clin
ical
re
spon
se
Inte
gral
ala
rm h
ardw
are,
rem
ote
annu
ncia
tion
pane
l, so
ft ke
y so
ftw
are
func
tion
Act
ivat
ion
of a
larm
at
setu
p an
d af
ter
disa
blin
g al
arm
dur
ing
care
, se
tting
app
ropr
iate
ala
rm li
mits
, m
onito
ring
rem
ote
disp
lays
ICU
, CC
U, T
elem
etry
Uni
t, E
R, O
RP
5H
5E
0R
1P
,T,E
,S
Toi
let a
nd b
athi
ng a
rea
emer
genc
y ca
ll N
otify
sta
ff th
at p
atie
nt r
equi
res
assi
stan
ce
Pul
l cor
ds,
switc
h, r
oom
doo
r in
dica
ting
light
, cen
tral
ann
unci
atio
n,
inte
rcom
Res
pons
e to
ala
rms
All
patie
nt c
are
area
toi
let
and
batin
g ar
eaP
3H
0E
5R
3T,
R
Ven
tilat
or a
larm
sN
otify
sta
ff of
cha
nges
in
patie
nt
stat
us t
hat
may
req
uire
clin
ical
re
spon
seC
ontr
ol s
witc
hes,
loca
l ann
unci
ator
Act
ivat
ion
of a
larm
at
setu
p an
d af
ter
disa
blin
g al
arm
dur
ing
care
, se
tting
app
ropr
iate
ala
rm li
mits
ICU
, CC
U, l
ong
term
car
e ar
ea, 4
th fl
oor
med
/sur
gP
5H
5E
5R
4P
,T,E
,R,S
,M
17
Med
ical
Ala
rm R
isk
Ass
essm
ent
Rat
ing
Key
s
P5
De
ath
H5
Ala
rm c
an b
e di
sabl
ed,
freq
uent
nui
sanc
e ac
tivat
ions
, a
nd P
3 -
P5
Out
com
e In
dex
PA
dmin
istr
ativ
e pr
oced
ure
addr
essi
ng a
larm
fu
nctio
n, s
et u
p, h
uman
per
form
ance
, en
viro
nmen
t, a
nd r
elia
bilit
y as
app
ropr
iate
P4
Per
man
ent
heal
th e
ffec
tH
4A
larm
can
be
disa
bled
, fr
eque
nt n
uisa
nce
activ
atio
ns,
and
P2
Out
com
e In
dex
TS
taff
ori
enta
tion
and
trai
ning
P3
Tem
pora
ry h
ealth
eff
ect
that
req
uire
s tr
eatm
ent
or e
xten
ded
stay
H3
Ala
rm c
an b
e di
sabl
ed,
som
e nu
isan
ce
activ
atio
ns,
and
P2
Out
com
e In
dex
EE
mer
genc
y cl
inic
al p
roce
dure
P2
Tem
pora
ry h
ealth
eff
ect
that
req
uire
s ob
serv
atio
n or
ext
ende
d st
ayH
2A
larm
can
not
be d
isab
led,
mod
erat
e nu
isan
ce
activ
atio
ns,
and
P2
Out
com
e In
dex
RP
hysi
cal
insp
ectio
n du
ring
envi
ronm
enta
l ro
un
ds
P1
Tem
pora
ry h
ealth
eff
ect
that
req
uire
s o
bse
rva
tion
H1
Ala
rm c
anno
t be
dis
able
d, l
imite
d nu
isan
ce
activ
atio
ns,
and
P1
Out
com
e In
dex
SS
et u
p ev
alua
tion
durin
g en
viro
nmen
tal
rou
nd
s
P0
No
sign
ifica
nt h
ealth
eff
ect
H0
No
sign
ifica
nt h
uman
fac
tors
MM
aint
enan
ce a
nd c
alib
ratio
n pr
oced
ure
E5
Low
sta
ffin
g, p
oor
audi
bilit
y, p
oor
visu
al
acce
ss,
and
P3
- P
5 O
utco
me
Inde
xR
4R
equi
res
mai
nten
ance
or
calib
ratio
n to
m
aint
ain
relia
bilit
y
E4
Low
sta
ffin
g, p
oor
audi
bilit
y, p
oor
visu
al
acce
ss,
and
P2
Out
com
e In
dex
R3
Req
uire
s vi
sual
ins
pect
ion
of a
ll un
its t
o as
sure
phy
sica
l co
nditi
on
E3
Low
sta
ffin
g, p
oor
audi
bilit
y, p
oor
visu
al
acce
ss,
and
0 -
P!
Out
com
e In
dex
R2
Req
uire
s vi
sual
ins
pect
ion
of a
sam
ple
of u
nits
to
ass
ure
phys
ical
con
ditio
n an
d pr
oper
fu
nct
ion
E2
Mod
erat
e st
affin
g, l
imite
d au
dibi
lity,
and
lim
ited
visu
al a
cces
sR
1R
equi
res
eval
uatio
n of
set
up
of a
sam
ple
of
units
eva
luat
e op
erat
or c
ompe
tenc
e
E1
Mod
erat
e st
affin
g, m
oder
ate
audi
bilit
y an
d vi
sual
acc
ess
R0
No
sign
ifica
nt r
elia
bilit
y is
sues
Pat
ien
t O
utc
om
e S
ever
ity
Ind
ex
En
viro
nm
enta
l F
acto
r S
ever
ity
Ind
exR
elia
bili
ty F
acto
r S
ever
ity
Ind
ex
Hu
man
Fac
tor
Sev
erit
y In
dex
P
roce
ss C
om
po
nen
t K
ey
Ris
k A
sses
smen
t o
f M
edic
al A
larm
s o
f <<
Org
aniz
atio
n N
ame>
>
Med
ical
Ala
rmM
edic
al A
larm
Fun
ctio
nA
larm
Com
pone
nts
Hum
an F
acto
rsA
reas
of U
seO
utco
me
of C
are
Ris
k S
core
Hum
an F
acto
r R
isk
Sco
reE
nviro
nmen
tal
Ris
k S
core
Rel
iabi
lity
Ris
k S
core
Rec
omm
ende
d P
roce
ss C
ompo
nent
s
18
19
Med
ical
Ala
rm R
isk
Ass
essm
ent
Rat
ing
Key
s
P5
De
ath
H5
Ala
rm c
an b
e di
sabl
ed,
freq
uent
nui
sanc
e ac
tivat
ions
, a
nd P
3 -
P5
Out
com
e In
dex
PA
dmin
istr
ativ
e pr
oced
ure
addr
essi
ng a
larm
fu
nctio
n, s
et u
p, h
uman
per
form
ance
, en
viro
nmen
t, a
nd r
elia
bilit
y as
app
ropr
iate
P4
Per
man
ent
heal
th e
ffec
tH
4A
larm
can
be
disa
bled
, fr
eque
nt n
uisa
nce
activ
atio
ns,
and
P2
Out
com
e In
dex
TS
taff
ori
enta
tion
and
trai
ning
P3
Tem
pora
ry h
ealth
eff
ect
that
req
uire
s tr
eatm
ent
or e
xten
ded
stay
H3
Ala
rm c
an b
e di
sabl
ed,
som
e nu
isan
ce
activ
atio
ns,
and
P2
Out
com
e In
dex
EE
mer
genc
y cl
inic
al p
roce
dure
P2
Tem
pora
ry h
ealth
eff
ect
that
req
uire
s ob
serv
atio
n or
ext
ende
d st
ayH
2A
larm
can
not
be d
isab
led,
mod
erat
e nu
isan
ce
activ
atio
ns,
and
P2
Out
com
e In
dex
RP
hysi
cal
insp
ectio
n du
ring
envi
ronm
enta
l ro
un
ds
P1
Tem
pora
ry h
ealth
eff
ect
that
req
uire
s o
bse
rva
tion
H1
Ala
rm c
anno
t be
dis
able
d, l
imite
d nu
isan
ce
activ
atio
ns,
and
P1
Out
com
e In
dex
SS
et u
p ev
alua
tion
durin
g en
viro
nmen
tal
rou
nd
s
P0
No
sign
ifica
nt h
ealth
eff
ect
H0
No
sign
ifica
nt h
uman
fac
tors
MM
aint
enan
ce a
nd c
alib
ratio
n pr
oced
ure
E5
Low
sta
ffin
g, p
oor
audi
bilit
y, p
oor
visu
al
acce
ss,
and
P3
- P
5 O
utco
me
Inde
xR
4R
equi
res
mai
nten
ance
or
calib
ratio
n to
m
aint
ain
relia
bilit
y
E4
Low
sta
ffin
g, p
oor
audi
bilit
y, p
oor
visu
al
acce
ss,
and
P2
Out
com
e In
dex
R3
Req
uire
s vi
sual
ins
pect
ion
of a
ll un
its t
o as
sure
phy
sica
l co
nditi
on
E3
Low
sta
ffin
g, p
oor
audi
bilit
y, p
oor
visu
al
acce
ss,
and
0 -
P!
Out
com
e In
dex
R2
Req
uire
s vi
sual
ins
pect
ion
of a
sam
ple
of u
nits
to
ass
ure
phys
ical
con
ditio
n an
d pr
oper
fu
nct
ion
E2
Mod
erat
e st
affin
g, l
imite
d au
dibi
lity,
and
lim
ited
visu
al a
cces
sR
1R
equi
res
eval
uatio
n of
set
up
of a
sam
ple
of
units
eva
luat
e op
erat
or c
ompe
tenc
e
E1
Mod
erat
e st
affin
g, m
oder
ate
audi
bilit
y an
d vi
sual
acc
ess
R0
No
sign
ifica
nt r
elia
bilit
y is
sues
Pat
ien
t O
utc
om
e S
ever
ity
Ind
ex
En
viro
nm
enta
l F
acto
r S
ever
ity
Ind
exR
elia
bili
ty F
acto
r S
ever
ity
Ind
ex
Hu
man
Fac
tor
Sev
erit
y In
dex
P
roce
ss C
om
po
nen
t K
ey
20
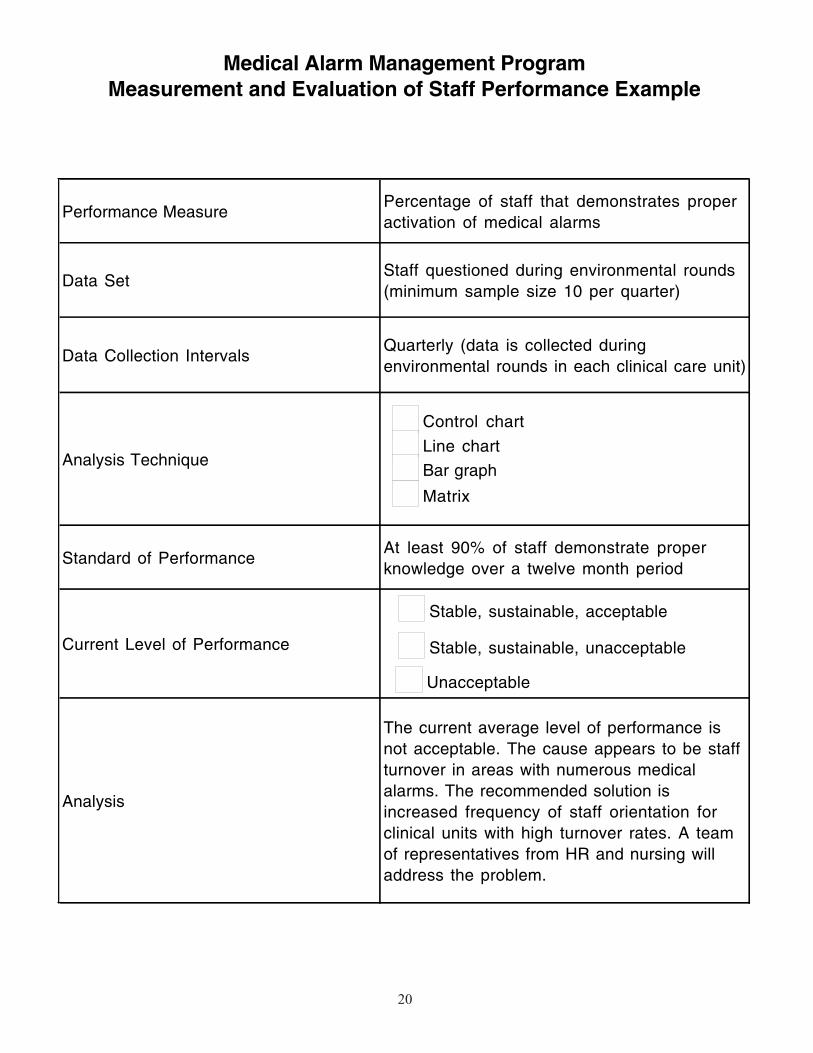
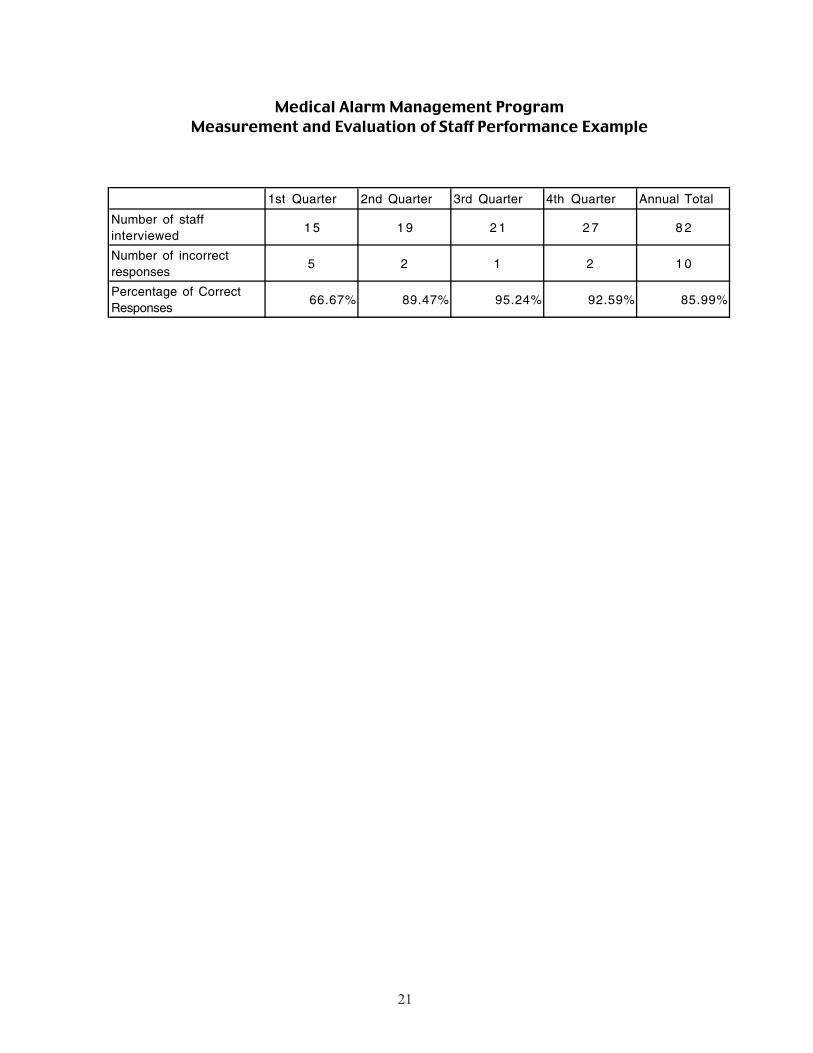
Medical Alarm Management ProgramMeasurement and Evaluation of Staff Performance Example
Performance MeasurePercentage of staff that demonstrates proper activation of medical alarms
Data SetStaff questioned during environmental rounds (minimum sample size 10 per quarter)
Data Collection IntervalsQuarterly (data is collected during environmental rounds in each clinical care unit)
Analysis Technique
Standard of PerformanceAt least 90% of staff demonstrate proper knowledge over a twelve month period
Current Level of Performance
Analysis
The current average level of performance is not acceptable. The cause appears to be staff turnover in areas with numerous medical alarms. The recommended solution is increased frequency of staff orientation for clinical units with high turnover rates. A team of representatives from HR and nursing will address the problem.
Stable, sustainable, unacceptable
Unacceptable
Stable, sustainable, acceptable
Control chart
Line chart
Bar graph
Matrix
21
���������������� �������� ��
����������������������������������������������������
1st Quarter 2nd Quarter 3rd Quarter 4th Quarter Annual Total
Number of staff interviewed
1 5 1 9 2 1 2 7 8 2
Number of incorrect responses
5 2 1 2 1 0
Percentage of Correct Responses
66.67% 89.47% 95.24% 92.59% 85.99%
22
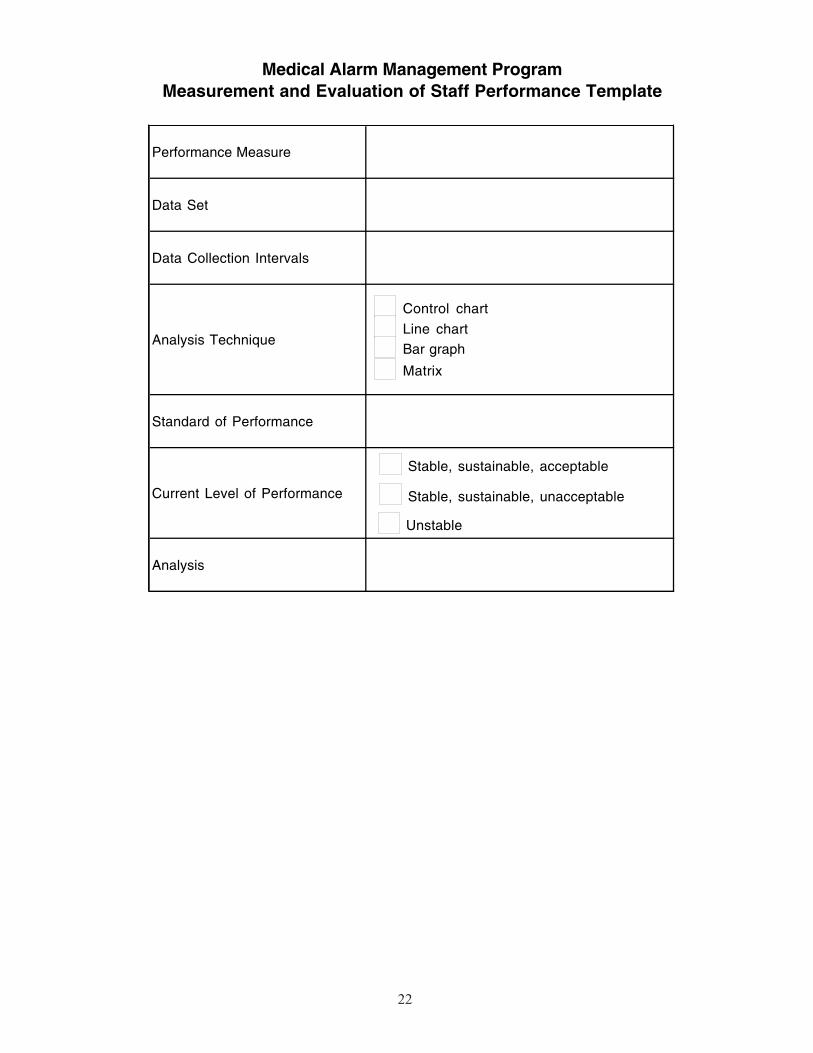
Medical Alarm Management ProgramMeasurement and Evaluation of Staff Performance Template
Performance Measure
Data Set
Data Collection Intervals
Analysis Technique
Standard of Performance
Current Level of Performance
Analysis
Stable, sustainable, unacceptable
Unstable
Stable, sustainable, acceptable
Control chart
Line chartBar graph
Matrix






















![Car Alarms & Smoke Alarms [Monitorama]](https://img.pdfslide.us/doc/110x75/54b6cdf94a7959d84d8b45a5/car-alarms-smoke-alarms-monitorama.jpg)





