Embed Size (px)
Citation preview
![Page 1: International Journal of Paleopathology Volume 1 issue 1 2011 [doi 10.1016_j.ijpp.2011.02.003] Lorna Tilley; Marc F. Oxenham -- Survival against the od.pdf](https://reader030.pdfslide.us/reader030/viewer/2022020713/56d6be511a28ab30169198b0/html5/thumbnails/1.jpg)
R
Ss
LS
a
ARRA
KPVHPKN
1
mhabspecbiswM(t
iveLP
1d
International Journal of Paleopathology 1 (2011) 35–42
Contents lists available at ScienceDirect
International Journal of Paleopathology
journa l homepage: www.e lsev ier .com/ locate / i jpp
esearch Article
urvival against the odds: Modeling the social implications of care provision toeriously disabled individuals
orna Tilley ∗, Marc F. Oxenhamchool of Archaeology & Anthropology, College of Arts and Social Sciences, Australian National University, Canberra, ACT 0200, Australia
r t i c l e i n f o
rticle history:eceived 9 October 2010eceived in revised form 15 February 2011ccepted 16 February 2011
eywords:
a b s t r a c t
Survival of an adult male (M9) with juvenile-onset quadriplegia in Neolithic Vietnam indicates provi-sion of continuous care from his community, and adds to the growing literature documenting survival ofdisabled individuals in prehistory. Although the role of care-giving in achieving survival is occasionallyacknowledged it is rarely elaborated, and a bioarchaeological model of care is missing. Contextualizedanalysis of specific instances of care can offer unique insights into contemporary culture, as the case of
alaeopathologyietnamealthcarearalysislippel-Feil Syndromeeolithic
M9 illustrates. The ‘bioarchaeology of care’ identifies likely functional impacts of the pathology; possibleand probable health challenges encountered; and nature of the support required to sustain life. Consider-ation of these factors in relation to lifeways practices and behaviours extends and enriches archaeologicalobservations of M9’s community. Additionally, M9’s survival of extreme disability suggests certain per-sonality traits touching on aspects of identity. Still under development, this new methodology promisesto be a valuable heuristic tool.
. Introduction
Between 3700–4000 years ago in northern Vietnam a youngan survived for approximately 10 years with disabilities so severe
e would have been dependent on assistance from others for everyspect of daily life. Paralysed from the waist down and with atest very limited upper body mobility (Oxenham et al., 2009), thekeletal remains of Man Bac Burial 9 (M9) provide evidence of aathological condition difficult to manage successfully in a mod-rn medical environment. In a subsistence Neolithic economy thehallenges to health maintenance and quality of life would haveeen enormous, yet M9 lived with minimally paraplegia and max-
mally quadriplegia from childhood into his third decade. M9’survival reflects high quality, continuous and time-consuming careithin a technologically unsophisticated prehistoric community.9’s pathology and its diagnosis are detailed in Oxenham et al.
2009). The current paper builds on this previous work to explorehe wider implications of M9’s survival.
A community’s response to the health care requirements ofts members is shaped by a combination of cultural beliefs andalues; collective knowledge, skills and experience; social and
conomic organisation; and access to resources (e.g. Bates andinder-Pelz, 1990; Hardey, 1998; Hofrichter, 2003; Mishler, 1981;ol and Thomas, 2001). In turn, and within physiological param-∗ Corresponding author. Tel.: +61 02 6125 3498/6247 2174; fax: +61 02 6125 2711.E-mail address: [email protected] (L. Tilley).
879-9817/$ – see front matter © 2011 Elsevier Inc. All rights reserved.oi:10.1016/j.ijpp.2011.02.003
© 2011 Elsevier Inc. All rights reserved.
eters, the way a person responds to the experience of a seriousdisease or injury reflects not only the treatment received, butindividual characteristics, beliefs and behaviours formed within aspecific socio-cultural environment (Bowling, 2002; Fábrega, 1997;Garro, 2006; Lieban, 1977). It follows from these observations thatanalysis of the functional impact of a significant pathology and themanner in which both the person affected and their communityrespond to the demands of this condition potentially offers insightsinto aspects of the contemporary society, and even a sense of thepersonality of the individual receiving care.
The provision and receipt of health care may therefore reflectsome of the most fundamental aspects of a culture. There existsa rich palaeoanthropological and bioarchaeological literature doc-umenting individual cases of palaeopathology, including those inwhich the likelihood of care is explicitly acknowledged if not elabo-rated (see for example Dickel and Doran, 1989; Hawkey, 1998; Lunaet al., 2008; Trinkaus and Zimmerman, 1982), and exploring inter-actions between lifeways, environment and evolution of diseaseand impact of these on population health status (e.g. Larsen, 2000;Ortner, 2003; Roberts and Manchester, 2005; Steckel and Rose,2002). However, archaeology has overlooked prehistoric healthcare provision as a specific focus for analysis, and a valuable sourceof information on past behaviours is being ignored. A ‘bioarchae-ology of care’ analytical framework, outlined below and illustrated
through application to the case of M9, is being developed to addressthis deficit.In the prehistoric setting, provision of health care is inferredfrom physical evidence in human remains which suggests that, at
![Page 2: International Journal of Paleopathology Volume 1 issue 1 2011 [doi 10.1016_j.ijpp.2011.02.003] Lorna Tilley; Marc F. Oxenham -- Survival against the od.pdf](https://reader030.pdfslide.us/reader030/viewer/2022020713/56d6be511a28ab30169198b0/html5/thumbnails/2.jpg)
3 l Journal of Paleopathology 1 (2011) 35–42
saItiridammono‘Citsrc
aotncatofeecictpsc
eucmaodoop
1
ars
pcibsea
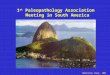
Fig. 1. Photograph of the modern day Man Bac landscape, looking southwest, withthe cemetery excavation site on the middle right (modern cemetery left foreground).
6 L. Tilley, M.F. Oxenham / Internationa
ome stage, an individual experienced a pathology that requirednd received assistance to enable or facilitate continued survival.ndicators of receipt of care comprise skeletal or preserved softissue evidence that (i) suggests survival over time with a continu-ng disability rendering functional independence impossible, or (ii)epresents healed or healing lesions associated with an illness ornjury necessitating care for recovery. ‘Health care’ is operationallyefined as the provision of assistance to an individual incapacitateds a result of a pathological condition who, without this assistance,ay have been unlikely to survive to age at death. Care provideday have lasted weeks, months or years, and could have consisted
f anything from basic supply of provisions, through dedicatedursing or direct medical intervention, to longer term modificationf group activity to enable community participation. In this paper
disability’, a contentious term in bioarchaeology (Dettwyler, 1991;ross, 1999; Molleson, 1999; Roberts, 1999, 2000), is employed
n accordance with the World Health Organisation (2008) usageo refer to a state arising from impairment in body function ortructure, associated with activity limitations and/or participationestrictions, and given specific meaning in relation to the lifewaysontext in which the pathology is experienced.
The bioarchaeology of care approach is designed for applicationt a case-study level. Initial analysis focuses on the probable impactf a serious pathology upon an individual’s ability to operate withinheir immediate physical and social environments. Where diag-osis is relatively straightforward (pace Waldron, 1994), modernlinical literature can provide information on the range of associ-ted disease symptoms and likely outcomes. Even in cases wherehe exact diagnosis is uncertain, the physical evidence of pathol-gy may allow conclusions about minimum level and duration ofunctional impairment. It is taken as given that every individual’sxperience of a pathology is unique (Bowling, 2002; Martin Ginist al., 2005 in relation to spinal cord injury specifically) and thatomplete confidence in relation to the nature and extent of thempact of a pathology is not possible. However, a model of whatare-giving likely comprised may be derived from considering (i)he minimum range of disability/ies associated with the evidence ofathology in relation to (ii) the possible opportunities for, and con-traints on, the provision of support in the corresponding lifewaysontext.
The above principles are employed to explore what M9’sxtended period of survival, against all odds, may contribute tonderstanding the social and economic practices of the prehistoricommunity of Man Bac, and what it may suggest about this youngan as an individual. This study provides a demonstration of the
mount and quality of information obtainable through a bioarchae-logy of care analysis. In doing so it contributes to the growingiscussion in the bioarchaeological literature on social dimensionsf the past and, more broadly, helps to illustrate how case studiesf individual remains can contribute to achieving a fuller picture ofrehistoric society.
.1. The context for care
Identifying the range of care likely required for M9’s survival,nd how, and at what cost, this care might have been provided,equires an understanding of the Man Bac physical environment,ocio-cultural context and general level of health.
In summary, the Man Bac cemetery is located in Ninh Binhrovince of northern Vietnam, 100 km south of Hanoi. Excavationsarried out between 1999 and 2007 produced the remains of 95ndividuals, extending through three separate layers, all primary
urials, and comprising the first signs of human presence at theite. During occupation Man Bac was located at the mouth of anstuary of one of many rivers making up the Red River Delta, withlandscape of flat loess interspersed with sharply rising, rugged,In the Neolithic the lower ground would have been underwater, and the cemetery,which is slightly elevated, would have been on the bank of a tidal river.
limestone karsts (Fig. 1). The climate would have been similar tothat of the present, with cool, humid winters (minimum averagetemperature during January is 12 ◦C, frequently descending to 6 ◦C)and hot, wet summers (Sterling et al., 2006).
Archaeological evidence suggests a predominantly hunter-gatherer economy. Faunal remains indicate a focus on terrestrialand aquatic vertebrate resources (Sawada and Vu, 2005), withpreliminary stable isotopic data indicating over 50% of proteinintake derived from fish (Yoneda, 2008). While long grain ricehas been recovered from contemporaneous Red River Delta sites(Nguyen et al., 2004), confirmatory evidence for rice cultiva-tion/consumption has proved elusive at Man Bac. A preliminaryanalysis of the Man Bac pottery suggests extensive regional linksamong the Red River Delta communities (Nguyen, 2008), whilelithic evidence indicates trade routes extended as far as ShangDynasty China during this period (Higham, 1996).
A detailed description of M9’s pathologies, a brief review ofsome common health implications of immobility, and more infor-mation on the bio-cultural context for the discussion of care arepresented in the supplementary information section. Readers arestrongly encouraged to view this before continuing.
2. Caring for M9
M9, a male of between 20 and 30 years, was buried flexed,on his right side, and oriented north–south. This contrasts withstandard Man Bac mortuary practice (extended, supine, east–westorientation). Skeletal abnormalities suggestive of serious pathologywere immediately apparent on excavation, and are clearly visiblein Fig. 2.
M9’s remains manifest extreme disuse atrophy of lower andupper limbs, full ankylosis of all cervical and the first three thoracicvertebrae, a permanent torticollis, and bilateral temporomandibu-lar joint degeneration. A diagnosis of Klippel Feil Syndrome (KFS)Type III has been proposed (Oxenham et al., 2009). The severityof pathology leaves no doubt that M9 was dependent on othersfor survival from onset of paralysis in adolescence onwards. Theprecise nature of the support he required cannot be known, butthe constraints inherent in osteological analysis make it likely thatthe nature, duration and complications of his pathology will beunderestimated. Nevertheless, analysing the likely impact of M9’s
disabilities within the contemporary physical and cultural environ-ment of Man Bac is one way of identifying what – at a minimum –his care comprised.![Page 3: International Journal of Paleopathology Volume 1 issue 1 2011 [doi 10.1016_j.ijpp.2011.02.003] Lorna Tilley; Marc F. Oxenham -- Survival against the od.pdf](https://reader030.pdfslide.us/reader030/viewer/2022020713/56d6be511a28ab30169198b0/html5/thumbnails/3.jpg)
L. Tilley, M.F. Oxenham / International Journ
Fer
ipemfNtAtmmab
1po
•
•
iataucad
2
2
shcfmjc
ig. 2. Photograph of MB07H1M09 in situ immediately prior to removal; notextreme gracility of limbs. The single preserved grave good (a terracotta pot) wasemoved at an early stage of the excavation.
There are obvious caveats to this approach. Individual variabilityn response to disease has already been acknowledged. Similarly,alaeopathology relies on clinical experience to understand theffects of disease on physical and psychological function, and thisodern, usually Western, frame of reference refers to a very dif-
erent medico-cultural environment to that of the Vietnameseeolithic. More particularly, the manner in which M9’s condi-
ion emerged may have helped to shape the support he received.lthough making no difference to the practical aspects of long-
erm support required, the timing and nature of disability onsetay have had implications for the decision to provide care and forode of care-delivery. This information is not retrievable from the
rchaeological record, and the following analysis of M9’s care isased on evidence of disease present at time of death.
By referring to modern clinical literature (e.g. Bergman et al.,997; Martin Ginis et al., 2005) a minimum level of practical sup-ort required for M9’s survival can be identified under the headingsf:
Basic care: assistance with the daily necessities of life, such asprovision of food, water, shelter, transport, and help with dressingand other everyday activities; andAdvanced care: maintenance of personal hygiene, managingenvironmental and physical safety concerns, general healthmaintenance, monitoring to ensure continued well-being, anddedicated nursing and other medical interventions as needed.
This division does not imply that various tasks were necessar-ly carried out by different people or at different times. Caring for
person with severe handicaps is an integrated activity; the dis-inction between basic and advanced care is arbitrary, because allspects of care are critical to preserving life, and all interact to makep the standard of care provided. Arguably, however, the forms ofare listed as ‘advanced’ are more intimate, more labour intensivend demand a higher level of skill and/or commitment than thoseescribed as ‘basic’, and this is what these categories reflect.
.1. Basic care
.1.1. Food and water provisionM9 was incapable of obtaining food and water independently,
o these essentials must have been supplied by others. Upper limbandicap, combined with cervical ankylosis and a permanent torti-ollis, would have affected coordination, possibly posing problems
or M9 in feeding himself. Restrictions on head and neck move-ent, combined with those associated with temporomandibularoint osteoarthritis, may have been an obstacle to efficient masti-ation, although level of tooth wear observed in M9 appears normal
al of Paleopathology 1 (2011) 35–42 37
for age. It would have been more difficult for M9 to hold a drink-ing vessel at the correct angle for imbibing. It is probable that M9received assistance with both eating and drinking, but he wouldalmost certainly have required help in relation to the latter.
M9 may have been provided with a special diet, possibly involv-ing additional processing to encourage appetite and facilitatedigestion and absorption. Immobility is associated with adversegastrointestinal outcomes ranging from anorexia to constipation(McKinley et al., 2002; Olsen and Schroeder, 1967; Schnelle andLeung, 2004). Constipation and/or mechanical bowel obstructionare an almost inevitable corollary to prolonged immobility in theabsence of an appropriate diet, and the consequences can be severe(McKinley et al., 2002; Olsen and McCarthy, 1967; Teasell andDittmer, 1993); M9 may have received food(s) with known laxativeproperties to facilitate bowel movement. Immobility-associatedchanges in metabolic function also affect dietary requirements;high levels of dietary protein are needed to compensate for poornutritional absorption resulting from reduction in cell metabolismrates, and foods with an acid residue, such as fish, meat, poultryand cereals, may be beneficial in countering increases in systemalkalinity which affect urinary and other functions (Agarwal, 2002;Olsen and McCarthy, 1967; Olsen and Schroeder, 1967). M9’s car-ers may not consciously have been aware of developing an optimaldietary regime, but they probably arrived at one through trial anderror – aided by the fact that their normal diet was based on highprotein, low fat, marine foods.
It is critical for immobilised individuals to be kept well hydrated.Dehydration can be both an outcome of, and a contributor to, bodyorgan dysfunction (Bergman et al., 1997; Massagli and Reyes, 2008;Olsen and McCarthy, 1967). Attention must have been given toensuring not only that M9 had water within easy reach (particu-larly important in the hot months when sweating increases loss ofbody fluid), but that he was assisted in drinking if this was required.
Maintaining M9’s health must have involved establishing abalance between his digestive capabilities and his nutritionalrequirements; his continued survival suggests this was achieved.
2.1.2. TransportFollowing onset of paralysis it would have been impossible for
M9 to undertake significant independent movement. There is noevidence of contemporary draught animal domestication in thisregion, so if travel was undertaken M9 must have been transportedby others, possibly on a litter or even by water. Consideration oftransportation issues may offer an insight into the Man Bac econ-omy. It would not be impossible for a community undertakingseasonal movement to support a seriously handicapped individ-ual (e.g. Dickel and Doran, 1989), but it would be very unusual. Theextreme fragility of M9’s limbs would have rendered them vulnera-ble to fracture from even minor trauma. Given the lack of evidenceof antemortem injury it seems unlikely that M9 was involved intravel over long distances, supporting the independently derivedhypothesis that Man Bac was predominantly a sedentary commu-nity. Despite this, M9 must frequently have been moved over shortdistances, if only for the purposes of maintaining the standard ofhygiene necessary to avoid infection. He would have been depen-dent on the physical strength of others for his conveyance, and ontheir caution in carrying him for his safety.
2.1.3. ShelterThere is no direct evidence of dwellings from this period, but
it would have been impossible for M9 to have survived constantexposure to the elements for any period of time. A water, wind and
sun-resistant shelter must be assumed. M9’s continued survivalwould also have been dependent on both (i) a structure elevat-ing him off cold or wet ground, and possibly providing him withsupport for resting in a sitting position, and (ii) provision of a soft![Page 4: International Journal of Paleopathology Volume 1 issue 1 2011 [doi 10.1016_j.ijpp.2011.02.003] Lorna Tilley; Marc F. Oxenham -- Survival against the od.pdf](https://reader030.pdfslide.us/reader030/viewer/2022020713/56d6be511a28ab30169198b0/html5/thumbnails/4.jpg)
3 l Journ
shh(
2
iosiAtcctf
2
2
trMv
fircl2ihac(tc(b
2
dbelMeodiaare
2n
motm
8 L. Tilley, M.F. Oxenham / Internationa
urface upon which to lie. Failure in either of these areas wouldave resulted, at a minimum, in continuous challenges to M9’sealth from acquired pressure sores and respiratory tract infectionsAHCPR, 1992; McKinley et al., 2002; Olsen and McCarthy, 1967).
.1.4. DressingLimitations on upper body function would have been a serious
mpediment to self-dressing. In a modern clinical context the abilityf an individual with spinal cord injury to clothe and clean them-elves is given prominence because independence in these areass associated with psychological well being (Krause et al., 1997).lthough nothing has been recovered from the cemetery excava-
ions that sheds light on the specific dress customs of the Man Bacommunity, there is clear evidence for textile manufacture in theontemporary Phung Nguyen period (Cameron, 2002), and winteremperatures (Sterling et al., 2006) would have necessitated someorm of covering during this season at least.
.2. Advanced care
.2.1. Personal hygieneM9 would have been completely reliant on others for the main-
enance of personal hygiene, and this must have involved a regularegime of bathing and toileting. Although possibly bathed in situ,9 may have been moved elsewhere for, and/or assisted in, the
oiding of bowel and bladder.This care was fundamental to his survival. Had M9 been left
or any extended period lying in his own waste this would havencreased vulnerability to breaches of skin integrity and to bacte-ial and parasitic infection (AHCPR, 1992; Stillman, 2008). Similarly,hanges in metabolic function associated with immobility mayead to increased sweating (Campagnolo, 2006; McKinley et al.,002), and this physiological response would have intensified dur-
ng the humid summer season. Sweat-moistened skin would alsoave increased M9’s susceptibility to pressure sore developmentnd have required particular attention. All the above complicationsan have potentially fatal consequences for an immobile individualStillman, 2008; Thompson Rowling, 1967; Yeo et al., 1998). Assis-ance would have included removal and disposal of body wastes;ontinual observation and action to ensure M9 was clean and drywiping, bathing, towelling); and frequent replacement of soilededding.
.2.2. General supervisionIndividuals who suffer loss of sensation as a result of spinal cord
amage are vulnerable to acquired injury in affected areas of theirody because they are unable to tell when damage is occurring;ven immobile individuals who do not suffer sensory deficit willose an amount of sensation over time (Bergman et al., 1997). For
9, hazards probably included open fires; surfaces capable of pen-trating or tearing the skin; disease-carrying or poisonous insectsr reptiles; lengthy exposure to damp or cold; and the range ofomestic accidents that happen when people live in close prox-
mity. Support in this context would not only have entailed beingware of the location of M9 in relation to potential threats andcting to reduce risk, either by environmental management or byemoving M9 from danger, but also undertaking regular physicalxaminations to ensure absence of injury.
.2.3. Health maintenance, health monitoring, and dedicatedursing
Modern clinical experience suggests that care interventions
ust have occurred at various stages throughout the latter halff M9’s life. Characteristics of symptom onset would have shapedreatment approach. If M9 experienced a gradual decline in
obility and sensation, then the initial need for direct medical
al of Paleopathology 1 (2011) 35–42
intervention may have been minimal and support efforts concen-trated on compensation for functional restrictions. If paralysis wasof sudden onset, then intensive care would have been necessaryover the initial period of stabilisation (Lee and Green, 2002), fol-lowed by development and implementation of an ongoing supportregime. At a minimum, M9 probably experienced severe restric-tions on head and neck movement from birth, and he may also havemanifested other signature characteristics of KFS (Hensinger et al.,1974; Thomsen et al., 1997). Indeed, M9 may have been markedout as ‘different’ and possibly in need of assistance before paralysisoccurred.
Individuals with long term mobility constraints face an exten-sive range of possible secondary complications. Some, such asosteoporosis, are unavoidable, and many are potentially life-threatening (e.g. Anderson and Spencer, 2003; Dittmer and Teasell,1993; Marik and Fink, 2002; Teasell and Dittmer, 1993). M9 displaysextreme atrophy and bone demineralisation of both upper andlower limbs (Oxenham et al., 2009), but most other complicationshave no effect on bone. It is therefore impossible to say what otherhealth challenges M9 experienced, but it is hardly credible that heexperienced none at all (Corcoran, 1991; Lee and Ostrander, 2002;McKinley et al., 2002). Close monitoring of an immobile individualis required to ensure that symptoms associated with complicationsare addressed quickly. Consideration of what this monitoring mayhave comprised in relation to M9, and what sort of care may havebeen provided in direct response to an acute challenge, providesinsight into carers’ awareness of what constituted a health threatand their ability to respond effectively.
‘Looking out for’ M9 must have included recognition of earlysymptoms of distress, even if these could not be attributed to aspecific cause. Cardiovascular dysfunction may manifest in dizzi-ness, rapid heart rate, excessive sweating and headaches (Claydonet al., 2006; Olsen and Thompson, 1967; Winslow, 1985) and respi-ratory system dysfunction in difficulties in breathing and coughing,or raised temperature (McKinley et al., 2002; Olsen and Johnson,1967). Urinary and renal dysfunction may manifest in raised tem-perature, pain, blood in the urine or nausea (Bergman et al., 1997;Olsen and Schroeder, 1967). Constipation or bowel obstructionmay manifest in loss of appetite, general discomfort, abdominalswelling, tangible mass in the colon, or abdominal pain (McKinleyet al., 2002; Olsen and McCarthy, 1967).
The community’s ability to treat these conditions aggressivelywas probably limited, but effective therapies may have existednonetheless. Modern clinical experience shows that physical ther-apy interventions can be very successful if applied in the earlystages of complications. Mobilisation, turning, repositioning, ele-vation, massage, percussion and postural drainage can improverespiratory and circulatory function, and repositioning, elevation,manual pressure, massage and manipulation can assist urinary flowand faecal elimination (McKinley et al., 2002; Olsen and Johnson,1967; Olsen and McCarthy, 1967; Olsen and Schroeder, 1967;Olsen and Thompson, 1967). Preventing dehydration and providingappropriate nutrition, previously discussed, is critical to maintain-ing the fitness levels necessary for overcoming health challenges.Historic and ethnographic research suggests that use of herbalremedies for treatment of fevers, pain and gastrointestinal com-plaints may have been common (e.g. Ferrence and Bendersky, 2004;Halberstein, 2005; Lieban, 1977). Direct evidence for the use ofbetel nut (Areca catechu) in Metal Age northern Vietnam is clear(Oxenham et al., 2002) and its use as medicament for children atMan Bac has been inferred (Oxenham et al., 2008a), but a generallack of palaeobotanical evidence from Man Bac precludes further
comment.When M9 experienced acute health complications, intensivecare over days or even weeks would have been necessary. The phys-ical therapies outlined above must have been applied at frequent
![Page 5: International Journal of Paleopathology Volume 1 issue 1 2011 [doi 10.1016_j.ijpp.2011.02.003] Lorna Tilley; Marc F. Oxenham -- Survival against the od.pdf](https://reader030.pdfslide.us/reader030/viewer/2022020713/56d6be511a28ab30169198b0/html5/thumbnails/5.jpg)
l Journ
icc
hmMllwiiio
2Cipfiabs(S
mraicl2i8aM
ahaolcpt
oomdatpwtsh
rvodje
L. Tilley, M.F. Oxenham / Internationa
ntervals, suggesting at least one, but probably more, dedicatedarers with the strength to lift, move and manipulate M9 withoutompromising his safety.
Even without an acute health condition as stimulus, M9 mustave received daily physical manipulation because this was theain risk mitigation strategy available to his carers. Protecting9 against the hazards of immobility must have involved regu-
ar repositioning and massage. At a theoretical level, there can beittle doubt that M9 received such prophylactic care and that this
as integral to his extended survival. At an empirical level, andn relation to two of the most common complications of prolongedmmobility (pressure sores and bone fracture), absence of evidencen the skeleton becomes possible evidence for receipt of care in itswn right.
.2.3.1. Absence of evidence: pressure sores and bone fracture.hanges in skin elasticity, vascular function and muscle tone result-
ng from prolonged immobility render the skin vulnerable to bothressure and shearing forces, and facilitate pressure sore (ulcer)ormation. When the skin’s surface is ruptured the risk of woundnfection is high; once established infection is difficult to control,nd unless contained will cause extensive deep tissue damage, mayecome systemic, may spread to bone, and may prove fatal. Pres-ure sores need early attention to achieve uncomplicated healingAHCPR, 1992; Margolis et al., 2003; Olsen and Edmonds, 1967;tillman, 2008).
To avoid sores the resting surface of an immobile individualust be soft but supportive, and the person must be regularly
epositioned to relieve areas of pressure (AHCPR, 1992; Olsennd Edmonds, 1967; Stillman, 2008). Monitoring skin conditions essential; damp conditions increase vulnerability to lesions, butracked, dry skin creates entry points for infection, and requiresubrication (AHCPR, 1992; Olsen and Edmonds, 1967; Stillman,008). In modern, sophisticated, clinical contexts the lifetime risk of
mmobile individuals experiencing pressure sores is approximately5% (Stillman, 2008, p. 1), and pressure sores are acknowledgeds an ever-present problem for this population (AHCPR, 1992;argolis et al., 2003; Olsen and Edmonds, 1967; Stillman, 2008).Had M9 suffered untreated pressure sores these lesions would
lmost certainly have led to long-term systemic infection, which,ad M9 survived, would likely have been expressed in bone. Thebsence of evidence for infection from pressure sores (or from anyther cause) in the recovered skeletal elements, combined withength of M9’s survival with paralysis, suggests a minimum level ofare comprising regular inspection and cleansing of skin surfaces,rovision of cushioning materials, and routine physical manipula-ion.
It is unlikely that M9 was able to avoid the initial stagesf pressure sore development, given their ubiquity in situationsf prolonged immobility (AHCPR, 1992; Stillman, 2008). Treat-ent would have required keeping the lesion clean, with possible
ebridement of necrotic tissue to promote healing. This man-gement of early stage pressure sores would have been withinhe technological capability of the Man Bac community, and it isossible that the site’s marine proximity encouraged the use of sea-eed dressings or saline washes, effective antiseptics used in some
herapies today (Stillman, 2008). Treatment would have requiredophisticated and dedicated effort, however, and again reflects theigh level of commitment to M9’s survival.
Absence of evidence of antemortem bone fracture in M9’semains, despite their gracility, also reflects the quality of care pro-ided. Immobility over a lengthy period results in osteoporosis; lack
f weight-bearing exercise leads to depletion of bone calcium andemineralisation and bones lose density, becoming brittle and sub-ect to fracture under minor stress (Bergman et al., 1997; McKinleyt al., 2002; Olsen and Edmonds, 1967), with such fractures occur-
al of Paleopathology 1 (2011) 35–42 39
ring most commonly in the femur, spine and wrist (Dittmer andTeasell, 1993). M9’s preserved lower and upper limbs display nosign of antemortem damage, despite extreme atrophy renderingthem potentially vulnerable.
3. Discussion
The case of M9 is perhaps the earliest and the most extremeprehistoric experience of long-term survival with total disability.Only one other instance of survival with such extensive paralysisis known; that of an individual from Hokkaido, dating to around,3500 years BP (Suzuki et al., 1984). The predicted outcome of acondition with such a severe functional impact and such a widerange of potential health complications would have been rapiddeath, long before the pathology had a chance to register in theskeleton. There can be no question that M9’s survival was dueto the care he received, and this enables certain observations tobe made about Man Bac as a community and about M9 as a per-son.
Because the size and composition of the Man Bac communityis not known, it is impossible to tell whether carers came exclu-sively from M9’s family; whether carers were drawn from non-kincommunity members; or whether there existed dedicated heal-ers for particular aspects of treatment. It is possible to extrapolate,however, that the act of caring for M9 received general communityendorsement. At some stage following paralysis onset the extent offunctional impact, combined with failure to improve, would havemade it clear that M9 was not going to recover independence;that his health would probably deteriorate further; that he wouldnever be capable of making a substantive material contribution tothe community (whatever other contribution he was capable of);and that he would require continuing and labour intensive sup-port for the rest of his life. In practical terms, the costs to a smallcommunity of supporting M9 involved not only the provision ofresources necessary for his survival, but also compensation for thelabour foregone of those involved in meeting care requirements.The Man Bac environment was relatively resource rich – a situa-tion facilitating the full time support of a dependent individual andcompensating for community members taken out of mainstreamactivity to provide dedicated care. Nevertheless, in a small subsis-tence community it is usual for all members to participate in theeconomy as soon as they are old enough to do so (Oxenham et al.,2008a). In the case of M9, it is fair to assume that the adoption andmaintenance of support behaviours, resulting in reduced produc-tive capacity for the community over a period of years, would haverequired consent and cooperation from the group as a whole.
Consideration of the support likely received by M9 providesclues about behaviours in Man Bac for which there is no mate-rial evidence as yet. For example, essential tasks of bathing anddrying M9, as well as the need for covering in colder months, sug-gest textile production. Lack of antemortem injury to M9 suggests asedentary community lifestyle. Meeting M9’s dietary requirementssuggests a broad knowledge and range of food resources, foodprocessing skills capable of overcoming constraints on appetiteand digestion, and the ability to take the time needed for specialfood preparation. Furthermore, while prior experience of such anextreme condition as M9’s is unlikely, the effectiveness of the careenabling his long term survival suggests a community experiencedin looking after people incapacitated by disease or injury. The ele-vated level of general health stressors in Man Bac (Oxenham et al.,2008b), as well as ethnographic research into disease frequencies
and healthcare practices among hunter-gatherer and horticultur-alist societies in South America, Africa and Papua New Guinea (e.g.Frankel, 1986; Kaplan et al., 2000; Lewis, 1975; Sugiyama, 2004),indirectly support this observation.![Page 6: International Journal of Paleopathology Volume 1 issue 1 2011 [doi 10.1016_j.ijpp.2011.02.003] Lorna Tilley; Marc F. Oxenham -- Survival against the od.pdf](https://reader030.pdfslide.us/reader030/viewer/2022020713/56d6be511a28ab30169198b0/html5/thumbnails/6.jpg)
4 l Journ
cedntpcot
3
f4emedcbopn
coHmihtmcCottcw
wnSeciseOwmi(aoiZca1
aat
0 L. Tilley, M.F. Oxenham / Internationa
In summary, the effective and long-term response to M9’sondition argues for a socially stable and cohesive communityxperienced in nursing the sick; capable of assessing the likelyemands and costs of care-giving in relation to a serious and perma-ent pathology; able to develop a set of procedures for respondingo this situation successfully; and willing and able to maintain theserocedures over years. The Man Bac community made an informedommitment to the extended care of one of its members, probablyne reviewed and re-committed to in response to changes in – andhe inevitable decline of – M9’s health status.
.1. Caring for M9: cultural values in practice
Motivations for any substantive human behaviour are multi-aceted, ambiguous, often contradictory and, at a distance of around000 years, impossible to unravel completely. We can never knowxactly how the Man Bac society understood illness and how thisay have affected the decision to care for M9, but while acknowl-
dging the warnings of authors such as Dettwyler (1991) on theangers of retrospective attribution of motive (particularly that ofompassion) in the bioarchaeological context, it may still be possi-le to gain partial insight into the value placed by this communityn caring for others in need. For example, the considerable effortut into keeping M9 alive suggests that the people of Man Bac wereot fatalist in their views of disease and its origins.
Man Bac mortuary practice indicates that, in death at least, theommunity made little distinction between individuals on the basisf age, sex or other visible characteristics (Oxenham et al., 2008a).owever, individuals who are perceived as ‘different’ by their com-unity in life are frequently distinguished by different treatment
n death (Fay, 2009; Shay, 1985). Although M9 was buried withis contemporaries in the Man Bac cemetery, there were disposi-ional anomalies in his burial. His atypical position and orientation
ay have been an outcome of limitations imposed by his physicalondition; specifically, difficulty in breaking ankylosis and flexure.onversely, it is possible that this mortuary positioning was a markf M9’s difference, and had meaning in relation to either his posi-ion in the community or his passage into the afterlife. Whateverhe reason for differences in mortuary treatment, there is no indi-ation of careless handling and every sign of respect for someoneho was unique in his physical disability.
M9’s survival may reflect a high value placed on individual lifeithin the Man Bac community. While the culturally-mediatedature of psychological health is acknowledged (Lillard, 1998;cheper-Hughes and Lock, 2006), it is worth speculating on M9’sxperience in the context of modern clinical observations. Psy-hological depression, associated with loss of self esteem, socialsolation and social rejection, is a significant comorbidity of paraly-is resulting from spinal cord injury (Bockian et al., 2002; Boekampt al., 1996; Kennedy and Rogers, 2000; Krause et al., 1997;lsen, 1967). Direct (suicide) and indirect (e.g. failure to cooperateith treatment) self-destructive behaviours are a leading cause ofortality among this population, with perceived quality of life pos-
tively correlated with length of survival following disability onsetKrause et al., 1997). Additionally, psychological depression, medi-ted via physiological stress systems, is associated with a varietyf adverse impacts on physical health status, including reductionn general immune system function (O’Leary, 1990; Weisse, 1992;orrilla et al., 2001); increased risk of cardiovascular disease andongestive heart failure (Jagoda et al., 2003; Sherwood et al., 2007);nd increased incidence of respiratory tract pathologies (O’Leary,990).
It is impossible to make a direct comparison between modernnd prehistoric experience at a behavioural level, but it is reason-ble to assume that physiological responses to stress were the samehen as now. In a situation in which amenities were basic, had M9
al of Paleopathology 1 (2011) 35–42
suffered from clinical depression there is little doubt that he wouldhave quickly succumbed to health challenges in his environment.
It seems reasonable to conclude, therefore, that to have survivedwith his disabilities for more than 10 years M9 must have receivedextensive psychosocial as well as physical support. Modern expe-rience (Bockian et al., 2002; Krause et al., 1997) suggests that at anon-culturally specific level this must have included the creation ofa secure, emotionally-supportive, inclusive environment in whichcare was provided ungrudgingly, enabling M9 to grow to adulthood,to develop a role for himself within the group, to retain a sense ofself respect, and to interact with others in his community at what-ever level was possible. In view of the prolonged and particularlydemanding nature of the care provided, it seems justifiable to spec-ulate that the carers’ motivations included compassion, respect andaffection.
3.2. M9 – the individual
The past 15 years has seen growing interest in attempts to infer‘the individual’ from archaeological evidence of material culture(Meskell, 2000; Thomas, 2002). In most cases this focus has resultedin the production of a stereotype or cipher identified as the ‘actor’.It has rarely revealed any hint of a once-living human being.
Osteological evidence can enrich approaches to understandingthe individual within their archaeological context, although thispotential is rarely exploited in practice (Sofaer, 2006). Considerableinformation can be extracted from skeletal remains, including sex(implications for gendered behaviour); age at death (implicationsfor rites of passage); general physical demands of correspondinglifeways; and place of origin, travel undertaken, and diet (Oxenhamand Tayles, 2006; Robb, 2002; Sofaer, 2006).
Palaeopathological analysis contributes an intensely personalperspective – there is little that has more immediacy than experi-encing a pathology severe enough to leave markers on bone. Whereaspects of individual response to pathology can be inferred, thismay provide clues to personality.
For a minimum of the last 10 years of his life M9 would have beenunable to take on the normal role of those in his cohort. He couldonly watch on as his peers participated in the activities of late child-hood/early adolescence in Man Bac. He experienced the hormonalchanges of adolescence as a severely disabled individual (althoughthe impact of these may have been mitigated by immobility-relatedchanges in metabolic function [Olsen and Wade, 1967]). M9’s peersmoved through adolescence to adulthood, being admitted intothe roles and responsibilities associated with achieving differentage-related stages in life (Robb, 2002), while he remained with-out prospect of attaining ‘normal’ development. Although M9 mayhave contributed to his group in many ways – for example, thevery success of M9’s continued survival may have been a source ofstrengthened community identity and cohesion – none of these isarchaeologically accessible. All that can be concluded with certaintyis that M9 was reliant on others for every aspect of his physical andsocial existence.
M9’s prolonged survival with disability suggests an extraordi-narily strong will to live; a robust psychological adaptation; a selfesteem capable of overcoming the complete loss of independence;and a personality capable of inspiring others to maintain high qual-ity and costly care over time.
4. Conclusion
The bioarchaeology of care approach uses evidence of care-giving to explore details of past behaviour that may be impossibleto retrieve through other means. It does this by providing a focusand a framework for synthesising information from archaeological,
![Page 7: International Journal of Paleopathology Volume 1 issue 1 2011 [doi 10.1016_j.ijpp.2011.02.003] Lorna Tilley; Marc F. Oxenham -- Survival against the od.pdf](https://reader030.pdfslide.us/reader030/viewer/2022020713/56d6be511a28ab30169198b0/html5/thumbnails/7.jpg)
l Journ
aTocaawetntitg
temcuEwsat
A
HJoD
A
t
R
A
A
A
B
B
B
B
B
C
C
C
L. Tilley, M.F. Oxenham / Internationa
nthropological, palaeopathological and modern clinical sources.he methodology is based on individual case studies. As the numberf case studies increase these will undoubtedly contribute signifi-antly to the broader theoretical debate on the origins of care, butt present generalisation from one situation of caring for a dis-bled individual to another such situation should be undertakenith extreme caution. Although there may be points of similarity,
ach case of care-giving is unique. The example of M9 illustrateshe methodology’s potential for achieving a more detailed and moreuanced understanding of aspects of contemporary prehistoric cul-ural practice and social relations in a specific small community, andn this instance consideration of M9’s experience of pathology overime also allows speculation on aspects of personality, allowing alimpse, if only partial, of a real person.
By definition, the bioarchaeology of care approach is restrictedo instances in which care-giving can be inferred. Although in thexample of M9 the level of disability involved was extreme, theethodology employed in this study can be used in less dramatic
ases of pathology where the evidence suggests that the individ-al affected required assistance from others over a period of time.ven when it is only possible to use this approach in a limiteday, the perspective it offers should enrich more general analy-
es. The analytical framework is still undergoing development, buts demonstrated in this paper it promises to be a valuable heuristicool.
cknowledgements
We thank the Institute of Archaeology, Hanoi, Vietnam, andirofumi Matsumura of the Sapporo Medical School, Hokkaido,
apan, for their cooperation in the excavation of MB07H1M09. Partf this research was funded under an Australian Research Counciliscovery Grant.
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at doi:10.1016/j.ijpp.2011.02.003.
eferences
garwal, N., 2002. Nutrition in spinal cord injured patients. In: Lee, B., Ostrander,L.E. (Eds.), The Spinal Cord Injured Patient: Comprehensive Management. DemosPublishing, New York, pp. 317–324.
HCPR, 1992. Panel on the Prediction and Prevention of Pressure Ulcersin Adults. Pressure Ulcers in Adults: Prediction and Prevention.Quick Reference Guide for Clinicians. AHCPR Publication No. 92-0050. Agency for Health Care Policy and Research, Public HealthService, U.S. Department of Health and Human Services, Rockville, MD,http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.chapter.9026 (accessed21.06.08).
nderson, F.A., Spencer, F.A., 2003. Risk factors for venous thromboembolism. Cir-culation 107, 9–16.
ates, E., Linder-Pelz, S., 1990. Health Care Issues, second ed. Allen and Unwin,Sydney.
ergman, S.B., Yarkony, G.M., Stiens, S., 1997. Spinal cord injury rehabilitation. 2.Medical complications. Archives of Physical Medicine and Rehabilitation 78,S53–S58.
ockian, N.R., Fidanque, C.S., Lee, A., 2002. Psychosocial aspects of spinal cord injury.In: Lee, B., Ostrander, L.E. (Eds.), The Spinal Cord Injured Patient: ComprehensiveManagement. Demos Publishing, New York, pp. 326–329.
oekamp, J.R., Overholser, J.C., Schubert, D.S., 1996. Depression following a spinalcord injury. International Journal of Psychiatry in Medicine 26, 329–349.
owling, A., 2002. Research Methods in Health: Investigating Health and HealthServices, second ed. Open University Press, Buckingham.
ameron, J., 2002. Textile Technology in the Prehistory of Southeast Asia. Unpub-lished PhD thesis. Australian National University.
ampagnolo, D., 2006. Autonomic dysreflexia in spinal cord injury. eMedicine.
http://emedicine.medscape.com/article/322809-overview (accessed Septem-ber 2008).laydon, V.E., Steeves, J.D., Krassioukov, A., 2006. Orthostatic hypotension follow-ing spinal cord injury: understanding clinical pathophysiology. Spinal Cord 44,341–351.
al of Paleopathology 1 (2011) 35–42 41
Corcoran, P.J., 1991. Use it or lose it – the hazards of bed rest and inactivity. Reha-bilitation medicine – adding life to years [Special Issue]. Western Journal ofMedicine 154, 536–538.
Cross, M., 1999. Accessing the inaccessible: disability and archaeology. Archaeolog-ical Review from Cambridge 15, 7–30.
Dettwyler, K.A., 1991. Can paleopathology provide evidence for “compassion”?American Journal of Physical Anthropology 84, 375–384.
Dickel, D.N., Doran, G.H., 1989. Severe neural tube defect syndrome from the EarlyArchaic of Florida. American Journal of Physical Anthropology 80, 325–334.
Dittmer, D.K., Teasell, R., 1993. Complications of immobilization and bed rest. Part 1:musculoskeletal and cardiovascular complications. Canadian Family Physician39, 1428–1437.
Fábrega, H., 1997. Evolution of Sickness and Healing. University of California Press,Berkeley.
Fay, I., 2009. Text, space and the evidence of human remains in English late Medievaland Tudor disease culture: some problems and possibilities. In: Gowland, R.,Knüsel, C. (Eds.), Social Archaeology of Funerary Remains. Oxbow Books, Oxford,pp. 190–207.
Ferrence, S.C., Bendersky, G., 2004. Therapy with saffron and the goddess at Thera.Perspectives in Biology and Medicine 47, 199–226.
Frankel, S., 1986. The Huli Response to Illness. Cambridge University Press, Cam-bridge.
Garro, L.C., 2006. Cultural meaning, explanations of illness, and the development ofcomparative frameworks. In: Whitaker, E. (Ed.), Health and Healing in Compar-ative Perspective. Pearson Prentice Hall, New Jersey, pp. 296–315.
Halberstein, R., 2005. Medicinal plants: historical and cross-cultural usage patterns.Annals of Epidemiology 15, 686–699.
Hardey, M., 1998. The Social Context of Health. Open University, Buckingham.Hawkey, D.E., 1998. Disability, compassion and the skeletal record: using muscu-
loskeletal stress markers (MSM) to construct an osteobiography from Early NewMexico. International Journal of Osteoarchaeology 8, 326–340.
Hensinger, R.N., Lang, J.E., MacEwan, G.D., 1974. Klippel-Feil Syndrome: a con-stellation of associated anomalies. The Journal of Bone and Joint Surgery 56,1246–1253.
Higham, C.F.W., 1996. The Bronze Age of Southeast Asia. Cambridge University Press,Cambridge.
Hofrichter, R. (Ed.), 2003. Health and Social Justice: Politics, Ideology and Inequityin the Distribution of Disease. John Wiley and Sons, San Francisco.
Jagoda, P., Levy, W.C., Sullivan, M.D., 2003. Cytokines in depression and heart failure.Psychosomatic Medicine 65, 181–193.
Kaplan, H., Hill, K., Lancaster, J., Hurtado, A.M., 2000. A theory of human life his-tory evolution: diet, intelligence and longevity. Evolutionary Anthropology 9,156–185.
Kennedy, P., Rogers, B.A., 2000. Anxiety and depression after spinal cord injury:a longitudinal analysis. Archives of Physical Medicine and Rehabilitation 81,932–937.
Krause, J.S., Sternberg, M., Lottes, S., Maides, J., 1997. Mortality after spinal cordinjury: an 11 year prospective study. Archives of Physical Medicine and Reha-bilitation 78, 815–821.
Larsen, C.S., 2000. Skeletons in our Closet: Revealing our Past through Bioarchaeol-ogy. Princeton University Press, Princeton.
Lee, T.T., Green, B.A., 2002. Immediate management of the spinal cord injuredpatient. In: Lee, B.Y., Ostrander, L.E. (Eds.), The Spinal Cord Injured Patient:Comprehensive Management. Demos Publishing, New York, pp. 1–6.
Lee, B.Y., Ostrander, L.E. (Eds.), 2002. The Spinal Cord Injured Patient: ComprehensiveManagement. Demos Publishing, New York.
Lewis, G., 1975. Knowledge of Illness in a Sepik Society: A Study of the Gnau. TheAthlone Press, University of London, New Guinea, London.
Lieban, R.W., 1977. The field of medical anthropology. In: Landy, D. (Ed.), Culture,Disease and Healing: Studies in Medical Anthropology. Collier Macmillan, NewYork, pp. 13–31.
Lillard, A., 1998. Ethnopsychologies: cultural variations in theories of mind. Psycho-logical Bulletin 123, 3–32.
Luna, L.H., Aranda, C.M., Bosio, L.A., Beron, M.A., 2008. A case of multiple metas-tasis in Late Holocene hunter-gatherers from the Argentine Pampean Region.International Journal of Osteoarchaeology 18, 492–506.
Margolis, D.J., Knauss, J., Bilker, W., Baumgarten, M., 2003. Medical conditions as riskfactors for pressure ulcers in an outpatient setting. Age and Ageing 32, 259–264.
Marik, P.E., Fink, M.P., 2002. One good turn deserves another! Critical Care Medicine30, 2146–2148.
Martin Ginis, K.A.M., Latimer, A., Hicks, A.L., Craven, B.C., 2005. Development andevaluation of an activity measure for people with spinal cord injury. Medicineand Science in Sports and Exercise 37, 1099–1111.
Massagli, T.L., Reyes, M.R., 2008. Hypercalcemia and spinal cord injury. eMedicine.http://emedicine.medscape.com/article/322109-overview (accessed 13.10.08).
McKinley, W.O., Gittler, M.S., Kirshblum, S.C., Stiens, S.A., Groah, S.L., 2002. Medicalcomplications after spinal cord injury: identification and management. Archivesof Physical Medicine and Rehabilitation 83, S58–S64.
Meskell, L.M., 2000. Writing the body in archaeology. In: Rautman, A.E. (Ed.), Readingthe Body: Representations and Remains in the Archaeological Record. Universityof Pennsylvania Press, Pennsylvania, pp. 13–21.
Mishler, E.G., 1981. The health-care system: social contexts and consequences. In:Mishler, E.G. (Ed.), The Social Consequences of Health, Illness and Patient Care.Cambridge University Press, Cambridge, pp. 195–217.
Molleson, T., 1999. Archaeological evidence for attitudes to disability. ArchaeologicalReview from Cambridge 15, 69–77.
![Page 8: International Journal of Paleopathology Volume 1 issue 1 2011 [doi 10.1016_j.ijpp.2011.02.003] Lorna Tilley; Marc F. Oxenham -- Survival against the od.pdf](https://reader030.pdfslide.us/reader030/viewer/2022020713/56d6be511a28ab30169198b0/html5/thumbnails/8.jpg)
4 l Journ
N
N
O
O
O
O
O
O
O
O
O
O
O
O
O
O
P
R
R
R
R
S
2 L. Tilley, M.F. Oxenham / Internationa
guyen, K.S., Pham, M.H., Tong, T.T., 2004. Northern Vietnam from the Neolithic tothe Han Period. In: Glover, I., Bellwood, P. (Eds.), Southeast Asia from Prehistoryto History. Routledge Curzon, London, New York, pp. 177–201.
guyen, K.D., 2008. The scientific cooperation program at Man Bac (2004–2007):results and questions. A paper presented at the International Forum on the Pre-historic Man Bac Site, held on 19th July at the Institute of Archaeology, VietnamAcademy of Social Sciences Institute, 61 Phan Chu Trinh, Ha Noi.
’Leary, A., 1990. Stress, emotion, and human immune function. American Psycho-logical Bulletin 108, 363–382.
lsen, E.V., 1967. The hazards of immobility: effects on psychosocial equilibrium.The American Journal of Nursing 67, 794–796.
lsen, E.V., Edmonds, R.E., 1967. The hazards of immobility: effects on motor func-tion. The American Journal of Nursing 67, 788–790.
lsen, E.V., Johnson, B.J., 1967. The hazards of immobility: effects on respiratoryfunction. The American Journal of Nursing 67, 783–784.
lsen, E.V., McCarthy, J.A., 1967. The hazards of immobility: effects on gastrointesti-nal function. The American Journal of Nursing 67, 785–787.
lsen, E.V., Schroeder, L.M., 1967. The hazards of immobility: effects on urinaryfunction. The American Journal of Nursing 67, 790–792.
lsen, E.V., Thompson, L.F., 1967. The hazards of immobility: effects on cardiovas-cular function. The American Journal of Nursing 67, 781–782.
lsen, E.V., Wade, M., 1967. The hazards of immobility: effects on metabolic equi-librium. The American Journal of Nursing 67, 793–794.
rtner, D.J., 2003. Identification of Pathological Conditions in Human SkeletalRemains. Academic Press, New York.
xenham, M.F., Locher, C., Nguyen, L.C., Nguyen, K.T., 2002. Identification of Arecacatechu (betel nut) residues on the dentitions of Bronze Age inhabitants of NuiNap, Northern Vietnam. The Journal of Archaeological Science 29, 909–915.
xenham, M.F., Tayles, N. (Eds.), 2006. Bioarchaeology of Southeast Asia. CambridgeUniversity Press, Cambridge.
xenham, M.F., Matsumura, H., Domett, K., Nguyen, K.T., Nguyen, K.D., Nguyen, L.C.,Huffer, D., Muller, S., 2008a. Health and the experience of childhood in lateNeolithic Vietnam. Asian Perspectives 47, 190–209.
xenham, M.F., Ross, K.W., Nguyen, K.D., Matsumura, H., 2008b. Children throughadult eyes: subadult identity in Neolithic Vietnam. A paper presented at the 6thWorld Archaeological Congress, Peopling the Past, Individualizing the Present:Bioarchaeological Contributions in a Global Context: A Cast of Thousands: Chil-dren in the Archaeological Record, 29th June–4th July, Dublin, Ireland.
xenham, M.F., Tilley, L., Matsumura, H., Nguyen, L.C., Nguyen, K.T., Nguyen, K.D.,Domett, K., Huffer, D., 2009. Paralysis and severe disability requiring intensivecare in Neolithic Asia. Anthropological Science 117 (2), 107–112.
ol, L.G., Thomas, R.K., 2001. The Demography of Health and Health Care, second ed.Kluwer Academic/Plenum Press, New York.
obb, J., 2002. Time and biography: osteobiography of the Italian Neolithic. In:Hamilakis, Y., Pluciennik, Y., Tarlow, M.S. (Eds.), Thinking Through the Body:Archaeologies of Corporeality. Kluwer Academic/Plenum Publishers, London, pp.153–171.
oberts, C.A., 1999. Disability in the skeletal record: assumptions, problems andsome examples. Archaeological Review from Cambridge 15, 79–97.
oberts, C.A., 2000. Did they take sugar? The use of skeletal evidence in the study ofdisability in past populations. In: Hubert, J. (Ed.), Madness, Disability and SocialExclusion: The Archaeology and Anthropology of “Difference”. Routledge, NewYork, pp. 46–59.
oberts, C., Manchester, K., 2005. The Archaeology of Disease, third ed. Cornell Uni-
versity Press, New York.awada, J., Vu, The Long, 2005. Animal remains from the late Neolithic Man Bac site.In: Matsumura, H. (Ed.), Anthropological and Archaeological Study on the Originof Neolithic People in Mainland Southeast Asia, (Unpublished) Report of Grant-in-Aid for International Research (2003–2005 No. 15405018), pp. 351–353.
al of Paleopathology 1 (2011) 35–42
Scheper-Hughes, N., Lock, M.M., 2006. The mindful body: a prolegomenon to futurework in medical anthropology. In: Whitaker, E. (Ed.), Health and Healing inComparative Perspective. Pearson Prentice Hall, New Jersey, pp. 296–315.
Schnelle, J.F., Leung, F.W., 2004. Urinary and fecal incontinence in nursing homes.Gastroenterology 126, S41–S47.
Shay, T., 1985. Differential treatment of deviancy at death as revealed in anthropo-logical and archaeological material. Journal of Anthropological Archaeology 4,221–241.
Sherwood, A., Blumenthal, J.A., Trivedi, R., Johnson, K.S., O’Connor, C.M., Adams, K.F.,Dupree, C., Waugh, R.A., Bensimhon, D.R., Gaulden, L., Christenson, R.L., Koch,G.G., Hinderliter, A.L., 2007. Relationship of depression to death or hospitaliza-tion in patients with heart failure. Annals of Internal Medicine 167, 367–373.
Sofaer, J.R., 2006. The Body as Material Culture. Cambridge University Press, Cam-bridge.
Steckel, R.H., Rose, J.C. (Eds.), 2002. The Backbone of History: Health and Nutritionin the Western Hemisphere. Cambridge University Press, Cambridge.
Sterling, E.J., Hurley, M.M., Minh, L.D., 2006. Vietnam: A Natural History. Yale Uni-versity Press, New Haven, London.
Stillman, R.M., 2008. Wound care. eMedicine. http://www.emedicine.com/med/topic2754.htm#PressureUlcers (accessed 27.06.08).
Sugiyama, L.S., 2004. Illness, injury and disability among Shiwiar forager-horticulturalists: implications of health-risk buffering for the evolutionof human life history. American Journal of Physical Anthropology 123,371–389.
Suzuki, T., Mineyama, I., Mitsuhashi, K., 1984. Paleopathological study of an adultskeleton of Jomon period from Irie shell mound, Hokkaido. Journal of the Anthro-pological Society of Nippon 92, 87–104.
Teasell, R., Dittmer, D.K., 1993. Complications of immobilization and bed rest. Part2: other complications. Canadian Family Physician 39, 1440–1446.
Thomas, J., 2002. Archaeology’s humanism and the materiality of the body. In:Hamilakis, Y., Pluciennik, M., Tarlow, S. (Eds.), Thinking Through the Body:Archaeologies of Corporeality. Kluwer Academic/Plenum Publishers, London, pp.29–46.
Thompson Rowling, J., 1967. Paraplegia. In: Brothwell, D., Sandison, A.T. (Eds.),Diseases in Antiquity: A Survey of the Diseases, Injuries and Surgery of EarlyPopulations. Charles C Thomas, Springfield, Illinois, pp. 272–278.
Thomsen, M.N., Schneider, U., Weber, M., Reiner, J., Neithard, F.U., 1997. Scoliosis andcongenital anomalies associated with Klippel-Feil Syndrome Types I–III. Spine22, 396–401.
Trinkaus, E., Zimmerman, M.R., 1982. Trauma among the Shanidar Neandertals.American Journal of Physical Anthropology 57, 61–76.
Waldron, T., 1994. Counting the Dead: the Epidemiology of Skeletal Populations.John Wiley and Sons, London, pp. 28–39.
Weisse, C.S., 1992. Depression and immunocompetence: a review of the literature.Psychological Bulletin 111, 475–489.
Winslow, E.H., 1985. Cardiovascular consequences of bed rest. Heart Lung 14,236–246.
World Health Organisation, 2008. http://www.who.int/topics/disabilities/en/(accessed 30.10.08).
Yeo, J.D., Walsh, J., Rutkowski, S., Soden, R., Craven, M., Middleton, J., 1998. Mortalityfollowing spinal cord injury. Spinal Cord 36, 329–336.
Yoneda, M., 2008. Dietary reconstruction of ancient Vietnamese based on carbonand nitrogen isotopes. A paper presented at the International Forum on the Pre-historic Man Bac Site, held on 19th July at the Institute of Archaeology, Vietnam
Academy of Social Sciences Institute, 61 Phan Chu Trinh, Ha Noi.Zorrilla, E.P., Luborsky, L., McKay, J.R., Rosenthal, R., Houldin, A., Tax, A., McCorkle, R.,Seligman, D.A., Schmidt, K., 2001. The relationship of depression and stressors toimmunological assays: a meta-analytic review. Brain, Behavior, and Immunity15, 199–226.