Embed Size (px)
Citation preview

International Journal of Infectious Diseases 18 (2014) 90–93
Short Communication
Hepatitis C virus genotypes in Tirana, Albania
Migena Haldeda a, Julien Baume b, Catherine Tamalet b,c, Melpomeni Bizhga a,Philippe Colson b,c,*a Laboratory of Virology, University Hospital Center ‘‘Mother Teresa’’, Tirana, Albaniab Institut Hospitalo-Universitaire (IHU) Mediterranee Infection, Pole des Maladies Infectieuses et Tropicales Clinique et Biologique, Federation de
Bacteriologie-Hygiene-Virologie, Centre Hospitalo-Universitaire Timone, Assistance Publique – Hopitaux de Marseille, 264 rue Saint-Pierre 13385, Marseille
Cedex 05, Francec URMITE UM 63 CNRS 7278 IRD 198 INSERM U1905, Aix-Marseille Univ., Facultes de Medecine et de Pharmacie, Marseille, France
A R T I C L E I N F O
Article history:
Received 22 May 2013
Received in revised form 29 August 2013
Accepted 30 August 2013
Corresponding Editor: Eskild Petersen,
Aarhus, Denmark
Keywords:
Hepatitis C
HCV genotype
HCV epidemiology
Albania
HCV NS3 protease
S U M M A R Y
Hepatitis C virus (HCV) infection is a worldwide concern. Knowledge of the HCV genotype is clinically
important because it predicts the rate of response to therapy and guides the treatment duration.
Moreover, it allows molecular epidemiology to be performed. To our knowledge, the prevalence of HCV
genotypes has been assessed only once in Albania, using a line probe genotyping assay. We determined
HCV genotypes by population sequencing of HCV-infected patients in Tirana, Albania. HCV genotype and
sequence analyses were performed for serum samples collected from January 2011 through May 2012
from 61 HCV-seropositive patients using population sequencing of the NS3 protease gene and
alternatively the NS5b gene and the 50 untranslated region (UTR). HCV RNA was retrieved from the blood
samples of 50 patients. The HCV NS3 protease gene was sequenced for 28 patients and NS5b and/or
50UTR fragments were sequenced for an additional 22 patients. The predominant genotype was 1b in 25
patients (50%), followed by genotypes 2c, 4a, 3a, and 1a in 18%, 14%, 8%, and 6% of cases, respectively. Best
matches for these HCV RNAs in GenBank were obtained in different countries worldwide. One NS3
protease naturally harbored an amino acid conferring minor drug resistance to newly available HCV
protease inhibitors. In conclusion, HCV-1b was predominant in the present Albanian population, as in
southeastern Europe.
� 2013 The Authors. Published by Elsevier Ltd on behalf of International Society for Infectious
Diseases.
Contents lists available at ScienceDirect
International Journal of Infectious Diseases
jou r nal h o mep ag e: w ww .e lsev ier . co m / loc ate / i j id
Open access under CC BY-NC-ND license.
1. Introduction
Hepatitis C virus (HCV) genotype identification is clinicallyimportant because it predicts the rate of sustained virologicalresponse and contributes to the determination of treatmentduration.1 In addition, HCV genotyping is a powerful tool todescribe HCV epidemiology.2 Very few data exist on HCV infectionin Albania. The prevalence of HCV antibodies was found to be 0.07%in blood donors, 2.3% and 0.3% in Albanian emigrant populations inGreece and southern Italy, respectively, and 14% and 11% in 1995and 2005, respectively, for patients with viral and/or alcoholic liverdisease at the University Hospital of Tirana, the capital city.3–5 Toour knowledge, HCV molecular epidemiology has been assessed
* Corresponding author. Tel.: +33 491 385 519.
E-mail address: [email protected] (P. Colson).
1201-9712 � 2013 The Authors. Published by Elsevier Ltd on behalf of International Soci
http://dx.doi.org/10.1016/j.ijid.2013.08.015
only once in Albania, using a line probe genotyping assay. Wedetermined HCV genotype prevalence in Albanian patients bysequencing.
2. Materials and methods
Serum samples collected from 61 HCV-infected patients fromJanuary 2011 through May 2012 at the University Hospital Center(UHC) of Tirana, Albania, were analyzed. The HCV-infected patientswere mostly on the following wards: hepatology (n = 22),nephrology including dialysis (n = 12), infectious diseases (n = 9),pediatrics (n = 4), and hematology (n = 2). Thirty-nine patientswere men (64%). HCV genotyping was performed using in-houseassays targeting initially the NS3 protease gene (543 nucleotides),2
then, in the case of negative PCR amplification of this gene, a 195-nucleotide-long fragment of the NS5b gene or an approximately200-nucleotide-long region of the 50 untranslated region (UTR).2
HCV sequences were retrieved using a 3130XL Genetic Analyzer(Applied Biosystems, Branchburg, NJ, USA) then analyzed usingSeqscape v2.5 (Applied Biosystems). HCV RNA sequences were
ety for Infectious Diseases. Open access under CC BY-NC-ND license.

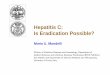
Figure 1. Phylogenetic tree based on partial sequences of the NS3 protease gene of the HCV genome (513 nucleotides; nucleotides 3420–3932 in reference to HCV genome
accession number AF011751). HCV sequences obtained in the present study are indicated with the black boxes. Sequences with the highest BLAST score recovered from the
NCBI GenBank nucleotide sequence database (indicated in boldface, underlined and labeled with BBH, GenBank accession number, country, and year of collection or
submission) for sequences obtained in the present study have been incorporated in the phylogeny reconstruction in addition to sequences with known genotypes and
subtypes (http://www.ncbi.nlm.nih.gov/projects/genotyping/view.cgi?db=3). Nucleotide alignments were performed using ClustalX v2.0 (http://www.clustal.org/
download/current/). The tree was constructed using MEGA v5.0 software (http://www.megasoftware.net/) and the neighbor-joining method. Branches with bootstrap
values �50%, obtained from 1000 resamplings of the data, are labeled on the tree. The HCV sequence EF108306 (genotype 7) was used as an outgroup. The scale bar indicates
the number of nucleotide substitutions per site. (BBH, best BLAST hit; Ref, reference sequence.).
M. Haldeda et al. / International Journal of Infectious Diseases 18 (2014) 90–93 91

Figure 2. Phylogenetic tree based on partial sequences of the NS5b encoding gene of the HCV genome (195 nucleotides; nucleotides 8287–8481 in reference to HCV genome
accession number AF011751). HCV sequences obtained in the present study are indicated with the black boxes. Sequences with the highest BLAST score recovered from the
NCBI GenBank nucleotide sequence database (indicated in boldface, underlined and labeled with BBH, GenBank accession number, country, and year of collection or
submission) for sequences obtained in the present study have been incorporated in the phylogeny reconstruction in addition to sequences with known genotypes and
subtypes (http://www.ncbi.nlm.nih.gov/projects/genotyping/view.cgi?db=3). Nucleotide alignments were performed using ClustalX v2.0 (http://www.clustal.org/
download/current/). The tree was constructed using MEGA v5.0 software (http://www.megasoftware.net/) and the neighbor-joining method. Branches with bootstrap
values �50%, obtained from 1000 resamplings of the data, are labeled on the tree. The HCV sequence EF108306 (genotype 7) was used as an outgroup. The scale bar indicates
the number of nucleotide substitutions per site. (BBH, best BLAST hit; Ref, reference sequence.).
M. Haldeda et al. / International Journal of Infectious Diseases 18 (2014) 90–9392

M. Haldeda et al. / International Journal of Infectious Diseases 18 (2014) 90–93 93
aligned using ClustalX v2.0 (http://www.clustal.org/download/current/) with sequences from the reference set of the NCBIgenotyping tool (http://www.ncbi.nlm.nih.gov/projects/genotyp-ing/view.cgi?db=3) and the two best matches obtained throughBLAST searches against the NCBI sequence database for eachsequence recovered here. Pairwise nucleotide similarities weregenerated using BioEdit (http://www.mbio.ncsu.edu/bioedit/page2.html). Phylogeny reconstructions were performed usingMEGA v5 (http://www.megasoftware.net/).
3. Results
HCV RNA was obtained from 50 blood samples, PCR amplifica-tion being negative in 11 cases. HCV NS3 protease sequences wereobtained for 28 sera (Figure 1) and the NS5b gene fragment(Figure 2) and 50UTR were obtained for 18 and four additional sera,respectively. The predominant genotype was 1b, found in 25patients (50%). Other genotypes, in decreasing prevalence, weregenotype 2c (n = 9, 18%), 4a (n = 7, 14%), 3a (n = 4, 8%), 1a (n = 3, 6%),and 2a and 4d (n = 1, 0.2% each). Best BLAST matches for HCV-1bhad been recovered in the USA, France, Switzerland, the UK, Brazil,Australia, and Japan (Figures 1 and 2). Best matches for HCV-2c hadbeen obtained in Japan, Argentina, Italy, the UK, and France, whilethose for HCV-4a had been obtained in Egypt, Cyprus, and France.
HCV-1b NS3 and NS5b sequences from the present studyshowed a mean � standard deviation identity of 91.3 � 1.6% and94.2 � 2.2%, respectively. HCV-1b NS3 RNA from two patients(numbers 860 and 639) were clustered together and showed 98.8%identity (Figure 1). These sequences had been recovered innephrology and dialysis units. In addition, HCV-1b NS5b RNA fromthree patients in a pediatrics unit (numbers 623, 188 and 290) wereclustered and showed 97.5–99.0% identity, and HCV-4a RNA fromfour patients including three dialysis patients (numbers 33p, 839,795, and 323) were clustered and showed 97.0–99.5% identity.Overall, five of eight patients (62%) sampled in the dialysis ward wereinfected with HCV-4a. Of note, amino acid substitution V55A withinthe HCV NS3 protease was observed in one patient naive to anti-HCVtherapy (number 369) and infected with HCV-1a.
4. Discussion
To our knowledge, we have provided the first HCV sequencesfrom patients in Albania. Half of these patients were infected withHCV-1b. In a previous study conducted on 18 patients with chronicliver diseases in Tirana using a line probe genotyping assay, HCV-1b was identified in 11 cases (61%), then HCV-2a/2c and HCV-3awere identified in five and two patients, respectively.5 Thisdistribution of HCV genotypes is similar to that observed here.In addition, the predominance of HCV-1b has been reported inother southeastern European countries, including Greece, Serbia,Montenegro, Slovenia, Croatia, and Bosnia and Herzegovina.6–10
(http://hcv.lanl.gov/components/sequence/HCV/geo/geo.comp).Best matches for HCV RNA obtained here were obtained in multiple
countries on the five continents, but not in southeastern Europe,apart from Cyprus. This finding may be explained by the smallnumber of HCV sequences available from southeastern Europe,especially when regarding the NS3 protease region.
The population studied here may not be fully representative ofthat of HCV-infected patients in Albania. Notably, only a fewpatients likely acquired HCV through intravenous drug use, as thispopulation is managed in other centers. In one HCV-1a-infectedpatient, amino acid 55A was observed within the NS3 protease inthe absence of any prior anti-HCV therapy. The HCV NS3-V55Asubstitution was associated with minor drug resistance to linearHCV NS3 protease inhibitors and compromised viral fitness.11
Further studies, conducted on larger and different populations andin different regions, are needed to strengthen knowledge on HCVgenotypes that circulate in Albania.
Acknowledgements
We are grateful to the team of the Virology Laboratory at IHUMediterranee Infection, Centre Hospitalo-Universitaire Timone,Marseille, France for technical help.
Conflict of interest: No potential conflict of interest or financialdisclosure for all authors.
References
1. Kamili S, Drobeniuc J, Araujo AC, Hayden TM. Laboratory diagnostics forhepatitis C virus infection. Clin Infect Dis 2012;55(Suppl 1):S43–8.
2. Colson P, Bregigeon S, Tourres C, Solas C, Poizot-Martin I, Tamalet C. Relapse ofhepatitis C virus after 14 months of sustained virological response followingpegylated-interferon alpha plus ribavirin therapy in a human immunodeficien-cy virus type 1 infected patient. J Clin Virol 2013;58:309–14.
3. Roussos A, Goritsas C, Pappas T, Spanaki M, Papadaki P, Ferti A. Prevalence ofhepatitis B and C markers among refugees in Athens. World J Gastroenterol2003;9:993–5.
4. Durro V, Koraqi A, Saliasi S. Trends in the prevalence of transfusion-transmis-sible infections among blood donors in Albania. Clin Lab 2010;56:591–5.
5. Kondili LA, Cuko L, Chionne P, Candido A, Madonna E, Dentico P, et al. HepatitisB, C and delta virus infections in Albanian patients with chronic liver disease:evaluation of possible changes during the last 10 years. Eur J GastroenterolHepatol 2010;22:167–71.
6. Stamouli M, Panagiotou I, Kairis D, Michopoulou A, Skliris A, Totos G. Genotypedistribution in chronic hepatitis C patients in Greece. Clin Lab 2012;58:173–6.
7. Katsoulidou A, Sypsa V, Tassopoulos NC, Boletis J, Karafoulidou A, Ketikoglou I,et al. Molecular epidemiology of hepatitis C virus (HCV) in Greece: temporaltrends in HCV genotype-specific incidence and molecular characterization ofgenotype 4 isolates. J Viral Hepat 2006;13:19–27.
8. Svirtlih N, Delic D, Simonovic J, Jevtovic D, Dokic L, Gvozdenovic E, et al.Hepatitis C virus genotypes in Serbia and Montenegro: the prevalence andclinical significance. World J Gastroenterol 2007;13:355–60.
9. Seme K, Vrhovac M, Mocilnik T, Maticic M, Lesnicar G, Baklan Z, et al. Hepatitis Cvirus genotypes in 1,504 patients in Slovenia, 1993-2007. J Med Virol2009;81:634–9.
10. Ahmetagic S, Salkic N, Cickusic E, Zerem E, Mott-Divkovic S, Tihic N, et al.Hepatitis C virus genotypes in chronic hepatitis C patients and in first timeblood donors in northeastern Bosnia and Herzegovina. Bosn J Basic Med Sci2009;9:278–82.
11. Welsch C, Schweizer S, Shimakami T, Domingues FS, Kim S, Lemon SM, et al.Ketoamide resistance and hepatitis C virus fitness in val55 variants of the NS3serine protease. Antimicrob Agents Chemother 2012;56:1907–15.