Embed Size (px)
Citation preview
Novel HCV Agents
INTERFERON-FREE COMBINATION TREATMENT WITH THE HCV NS3/4A PROTEASE INHIBITOR FALDAPREVIR AND THE NON-NUCLEOSIDE NS5B INHIBITOR
BI 207127 ± RIBAVIRIN: FINAL RESULTS OF SOUND-C2 AND PREDICTORS OF RESPONSE
1Klinikum der J. W. Goethe-Universität, Frankfurt am Main, Germany; 2Department of Infectious Diseases,
Hospital Carlos III, Madrid, Spain; 3Hôpital Beaujon, Clichy, France; 4Hôpital de Brabois, Vandoeuvre Cedex,
France; 5University Hospital Hamburg-Eppendorf, Hamburg, Germany; 6University Hospital of Zurich,
Zurich, Switzerland; 7University Hospital Mainz, Mainz, Germany; 8Hopital Saint Joseph, Marseille, France; 9Hospital Vall d’Hebron and Ciberehd, Barcelona, Spain; 10Alfred Hospital, Department of Gastroenterology,
Melbourne, Australia; 11Auckland Clinical Studies, Auckland, New Zealand; 12Boehringer Ingelheim
Pharmaceuticals, Ridgefield, CT, USA; 13Boehringer Ingelheim Pharma RCV GmbH & Co KG, Vienna, Austria; 14Boehringer Ingelheim Pharma GmbH & Co KG, Ingelheim, Germany
Stefan Zeuzem1, Vicente Soriano2, Tarik Asselah3, Jean-Pierre Bronowicki4, Ansgar W. Lohse5, Beat Müllhaupt6, Marcus Schuchmann7, Marc Bourliere8, Maria Buti9, Stuart Roberts10, Ed Gane11,
Jerry O. Stern12, Richard Vinisko12, Ivona Herichova13, Wulf O. Böcher14, Federico J. Mensa12

SOUND-C2 Investigators
Australia
• Peter Angus
• Stuart Roberts
Austria
• Peter Ferenci
• Michael Gschwantler
• Andreas Maieron
France
• Tarik Asselah
• Marc Bourliere
• Jean-Pierre Bronowicki
• Dominique Larrey
• Joseph Moussalli
• Stanislas Pol
• Jean-Pierre Zarski
• Fabien Zoulim
Germany
• Keikawus Arastéh
• Thomas Berg
• Michael Geissler
• Ansgar Lohse
• Michael Manns
• Stefan Mauss
• Marcus Schuchmann
• Stefan Zeuzem
New Zealand
• Ed Gane
Portugal
• Filipe Calinas
• Guilherme Macedo
• Leopoldo Matos
• Célia Oliveira
• Cristina Valente
Romania
• Emanoil Ceausu
• Liliana Preotescu
• Adrian Streinu-Cercel
Spain
• Maria Buti
• José Luis Calleja
• Moises Diago
• Xavier Forns
• Javier Garcia-Samaniego
• Vicente Soriano
Switzerland
• Tilman Gerlach
• Markus Heim
• Darius Moradpour
• Beat Müllhaupt
• Jürg Reichen
Acknowledgments
• This work was supported by Böehringer Ingelheim.
• The authors met criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE) and were fully responsible for all content and editorial decisions, and were involved at all stages of poster/presentation development.
• The authors received no compensation related to the development of the poster, but are consultants for BIPI and did receive research grant support for this study.
• Editorial support, supported financially by Böehringer Ingelheim, was provided by Katharine Howe of Adelphi Communications Ltd.
Disclosures
• Stefan Zeuzem has served as a consultant for Abbot, Achillion, AstraZeneca, BMS, Böehringer Ingelheim, Gilead, Idenix, Janssen, Merck, Novartis, Presidio, Roche, Santaris, and Vertex; and has served on speakers’ bureaus for BMS, Böehringer Ingelheim, Gilead, MSD, Roche, and Janssen.
• Vicente Soriano has received grants from Gilead, Janssen, and Merck; has served on speakers’ bureaus for BMS, Böehringer Ingelheim, Gilead, Janssen, and Merck; and has received compensation for educational presentations from Abbott, Gilead, Janssen, and Merck.
• Tarik Asselah has served as a consultant, advisory board member, and/or speaker for Böehringer Ingelheim.
• Jean-Pierre Bronowicki has served as a consultant and received grants from Böehringer Ingelheim.
• Ansgar W. Lohse has received grants from Gilead, Janssen, and Merck; has served on speakers’ bureaus for BMS, Böehringer Ingelheim, Gilead, Janssen, and Merck; and has received compensation for educational presentations from Abbott, Gilead, Janssen, and Merck.
• Beat Müllhaupt has served as a consultant for Abbott, Bayer, Gilead, GSK, MSD, and Roche; and has served on speakers’ bureaus for AstraZeneca, Bayer, Gilead, MSD, and Roche.
• Marcus Schuchmann has received editorial assistance from Böehringer Ingelheim.
Disclosures (continued)
• Marc Bourliere has served as a board member for Abbott, BMS, Böehringer Ingelheim, Gilead, GSK, Janssen, MSD, Roche and Vertex.
• Maria Buti has served on speakers’ bureaus for Gilead, MSD, and Novartis.
• Stuart Roberts has served as an advisory board member for Janssen and Roche.
• Ed Gane has served as an advisory board member for Abbott, Gilead, Janssen, and Novartis; and on speakers’ bureaus for Gilead, Novartis, and Roche.
• Jerry O. Stern is an employee of Böehringer Ingelheim Pharmaceuticals, Ridgefield, CT.
• Richard Vinisko is an employee of Boehringer Ingelheim Pharmaceuticals, Ridgefield, CT.
• Ivona Herichova is an employee of Boehringer Ingelheim Pharma RCV GmbH & Co KG, Vienna, Austria.
• Wulf O. Böcher is an employee of Böehringer Ingelheim Pharma, Biberach, Germany.
• Federico Mensa is an employee of Boehringer Ingelheim Pharmaceuticals, Ridgefield, CT
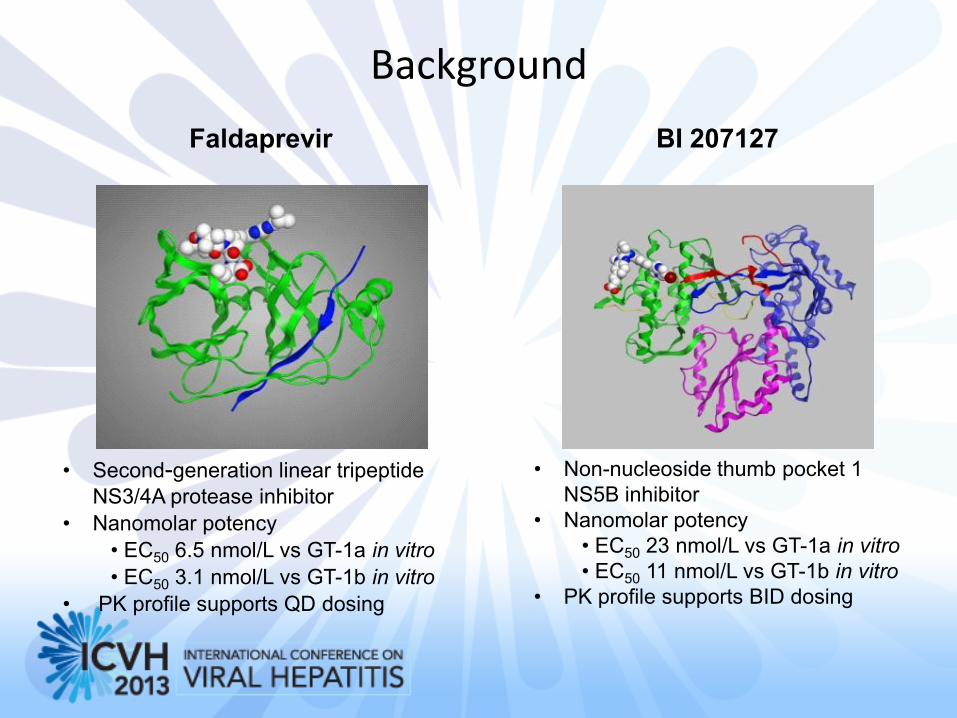
Background
BI 207127 Faldaprevir
• Second-generation linear tripeptide
NS3/4A protease inhibitor
• Nanomolar potency
• EC50 6.5 nmol/L vs GT-1a in vitro
• EC50 3.1 nmol/L vs GT-1b in vitro
• PK profile supports QD dosing
• Non-nucleoside thumb pocket 1
NS5B inhibitor
• Nanomolar potency
• EC50 23 nmol/L vs GT-1a in vitro
• EC50 11 nmol/L vs GT-1b in vitro
• PK profile supports BID dosing
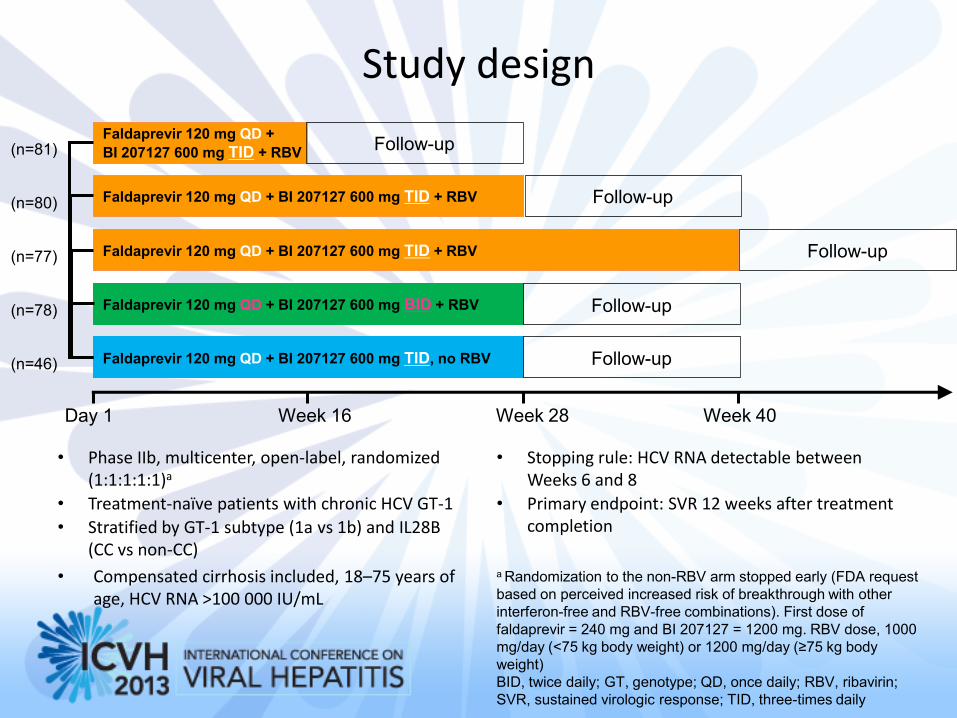
Study design
• Phase IIb, multicenter, open-label, randomized (1:1:1:1:1)a
• Treatment-naïve patients with chronic HCV GT-1
• Stratified by GT-1 subtype (1a vs 1b) and IL28B (CC vs non-CC)
• Compensated cirrhosis included, 18–75 years of age, HCV RNA >100 000 IU/mL
• Stopping rule: HCV RNA detectable between Weeks 6 and 8
• Primary endpoint: SVR 12 weeks after treatment completion
Faldaprevir 120 mg QD +
BI 207127 600 mg TID + RBV
Faldaprevir 120 mg QD + BI 207127 600 mg TID + RBV
Faldaprevir 120 mg QD + BI 207127 600 mg TID + RBV
Faldaprevir 120 mg QD + BI 207127 600 mg BID + RBV
Faldaprevir 120 mg QD + BI 207127 600 mg TID, no RBV
(n=81)
(n=80)
(n=77)
(n=78)
(n=46)
Day 1 Week 16 Week 28 Week 40
a Randomization to the non-RBV arm stopped early (FDA request
based on perceived increased risk of breakthrough with other
interferon-free and RBV-free combinations). First dose of
faldaprevir = 240 mg and BI 207127 = 1200 mg. RBV dose, 1000
mg/day (<75 kg body weight) or 1200 mg/day (≥75 kg body
weight)
BID, twice daily; GT, genotype; QD, once daily; RBV, ribavirin;
SVR, sustained virologic response; TID, three-times daily
Follow-up
Follow-up
Follow-up
Follow-up
Follow-up
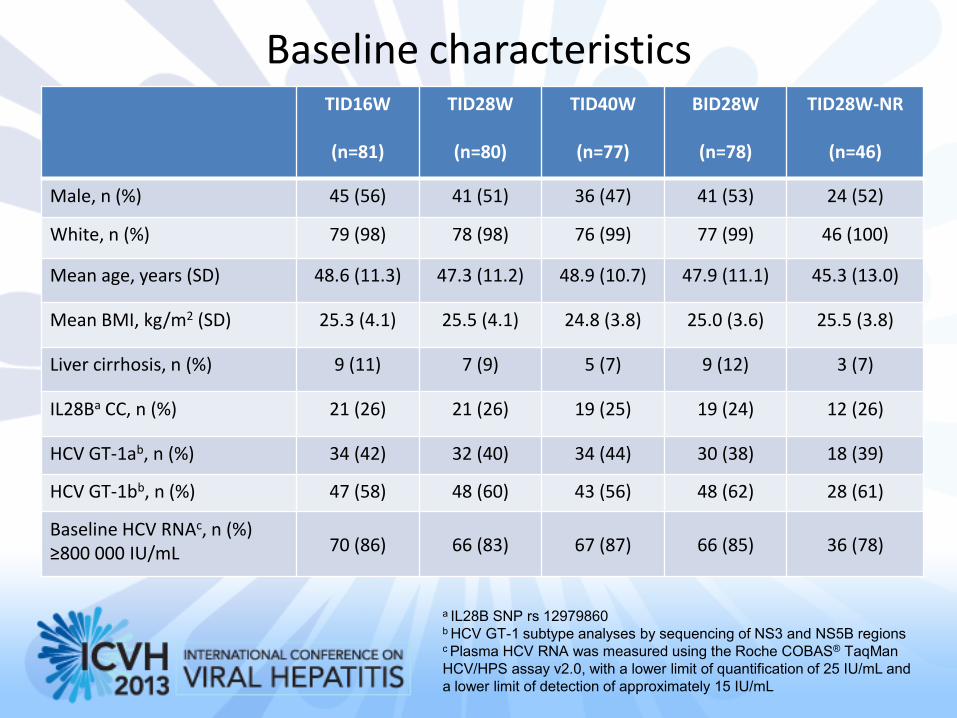
Baseline characteristics TID16W
(n=81)
TID28W
(n=80)
TID40W
(n=77)
BID28W
(n=78)
TID28W-NR
(n=46)
Male, n (%) 45 (56) 41 (51) 36 (47) 41 (53) 24 (52)
White, n (%) 79 (98) 78 (98) 76 (99) 77 (99) 46 (100)
Mean age, years (SD) 48.6 (11.3) 47.3 (11.2) 48.9 (10.7) 47.9 (11.1) 45.3 (13.0)
Mean BMI, kg/m2 (SD) 25.3 (4.1) 25.5 (4.1) 24.8 (3.8) 25.0 (3.6) 25.5 (3.8)
Liver cirrhosis, n (%) 9 (11) 7 (9) 5 (7) 9 (12) 3 (7)
IL28Ba CC, n (%) 21 (26) 21 (26) 19 (25) 19 (24) 12 (26)
HCV GT-1ab, n (%) 34 (42) 32 (40) 34 (44) 30 (38) 18 (39)
HCV GT-1bb, n (%) 47 (58) 48 (60) 43 (56) 48 (62) 28 (61)
Baseline HCV RNAc, n (%) ≥800 000 IU/mL 70 (86) 66 (83) 67 (87) 66 (85) 36 (78)
a IL28B SNP rs 12979860 b HCV GT-1 subtype analyses by sequencing of NS3 and NS5B regions c Plasma HCV RNA was measured using the Roche COBAS® TaqMan
HCV/HPS assay v2.0, with a lower limit of quantification of 25 IU/mL and
a lower limit of detection of approximately 15 IU/mL
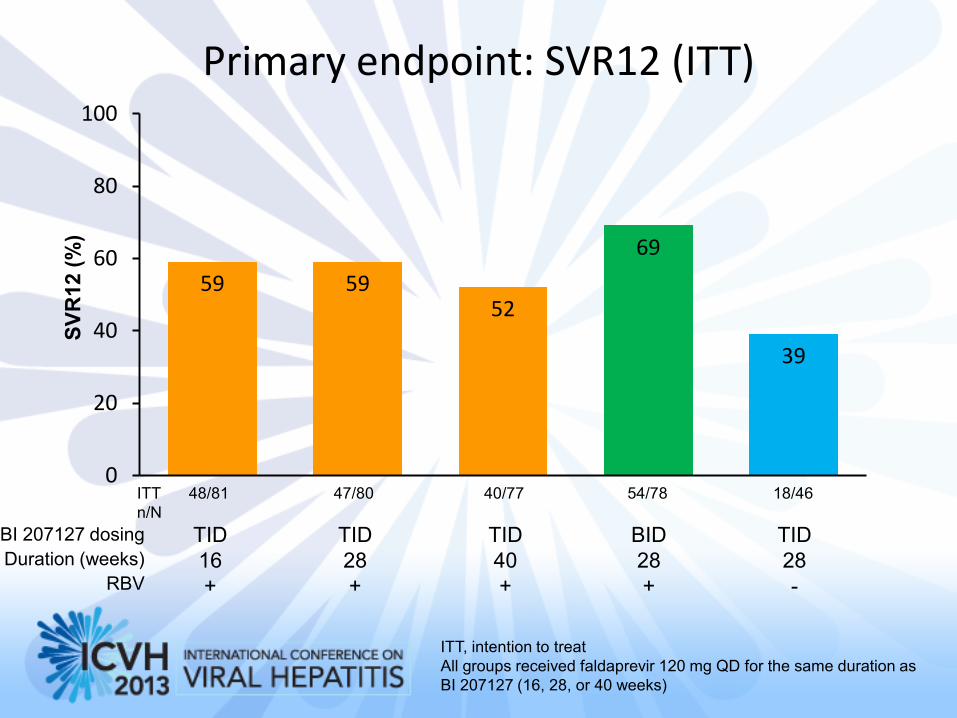
Primary endpoint: SVR12 (ITT)
59 59 52
69
39
0
20
40
60
80
100
SV
R12 (
%)
TID
16
+
TID
28
+
TID
40
+
BID
28
+
TID
28
-
BI 207127 dosing
Duration (weeks)
RBV
40/77 48/81 47/80 54/78 18/46 ITT
n/N
ITT, intention to treat
All groups received faldaprevir 120 mg QD for the same duration as
BI 207127 (16, 28, or 40 weeks)
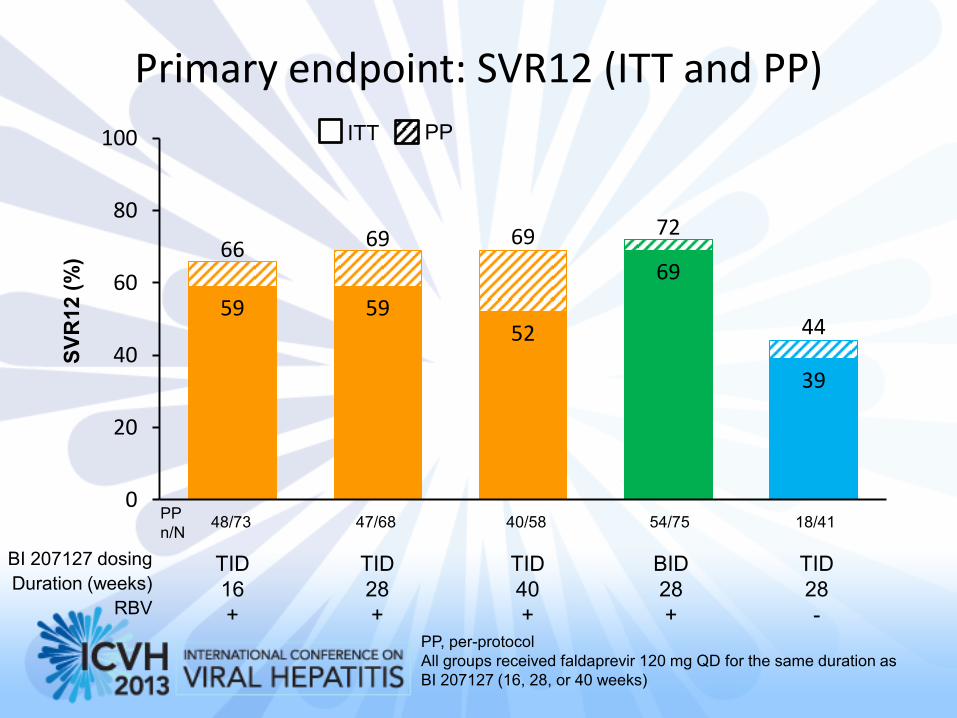
Primary endpoint: SVR12 (ITT and PP)
59 59 52
69
39
66 69 69 72
44
0
20
40
60
80
100 ITT PP
TID
16
+
TID
28
+
TID
40
+
BID
28
+
TID
28
-
BI 207127 dosing
Duration (weeks)
RBV
PP
n/N 40/58 48/73 47/68 54/75 18/41
SV
R12 (
%)
PP, per-protocol
All groups received faldaprevir 120 mg QD for the same duration as
BI 207127 (16, 28, or 40 weeks)
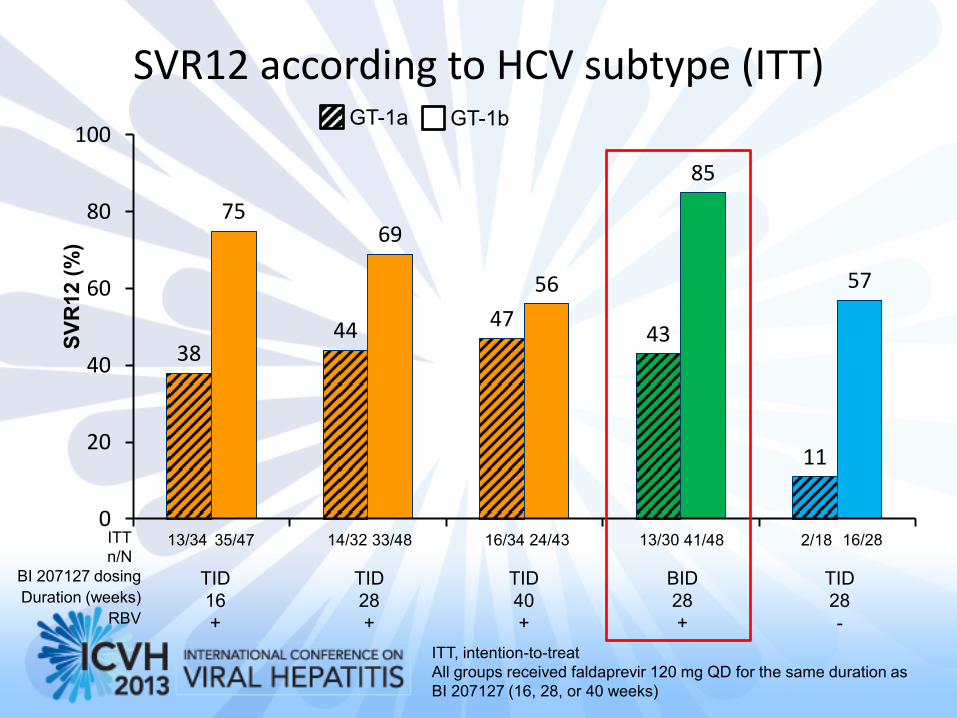
SVR12 according to HCV subtype (ITT)
38 44 47
43
11
75 69
56
85
57
0
20
40
60
80
100
ITT, intention-to-treat
All groups received faldaprevir 120 mg QD for the same duration as
BI 207127 (16, 28, or 40 weeks)
TID
16
+
TID
28
+
TID
40
+
BID
28
+
TID
28
-
BI 207127 dosing
Duration (weeks)
RBV
13/34 ITT
n/N 35/47 14/32 33/48 16/34 24/43 13/30 41/48 2/18 16/28
GT-1a GT-1b
SV
R12 (
%)
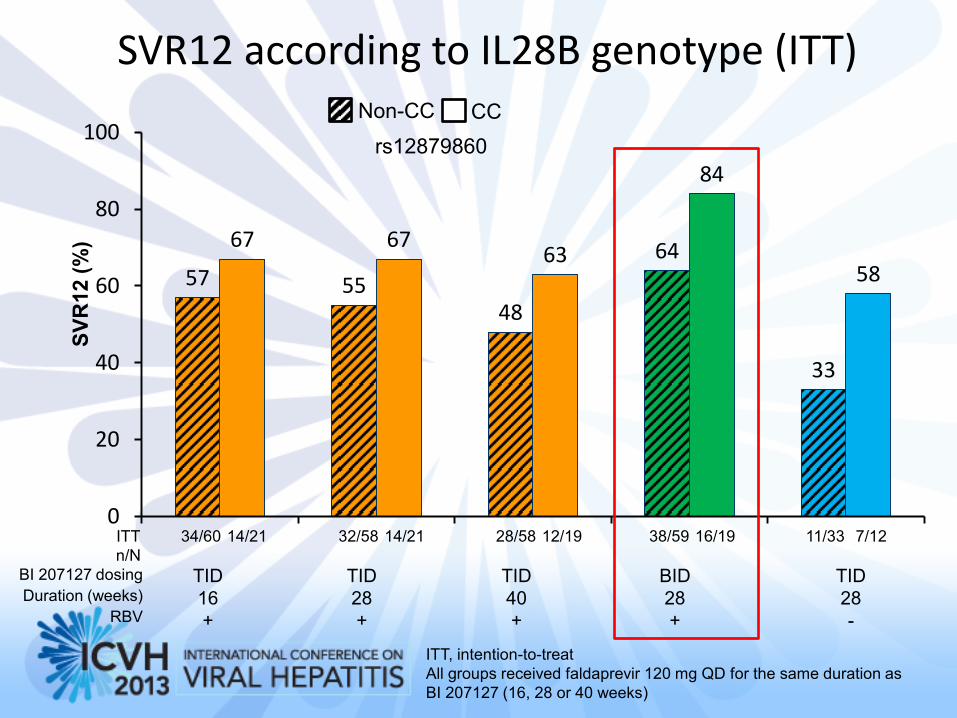
SVR12 according to IL28B genotype (ITT)
57 55 48
64
33
67 67 63
84
58
0
20
40
60
80
100
34/60 ITT
n/N
14/21 32/58 14/21 28/58 12/19 38/59 16/19 11/33 7/12
TID
16
+
TID
28
+
TID
40
+
BID
28
+
TID
28
-
BI 207127 dosing
Duration (weeks)
RBV
Non-CC CC
rs12879860
SV
R12 (
%)
ITT, intention-to-treat
All groups received faldaprevir 120 mg QD for the same duration as
BI 207127 (16, 28 or 40 weeks)
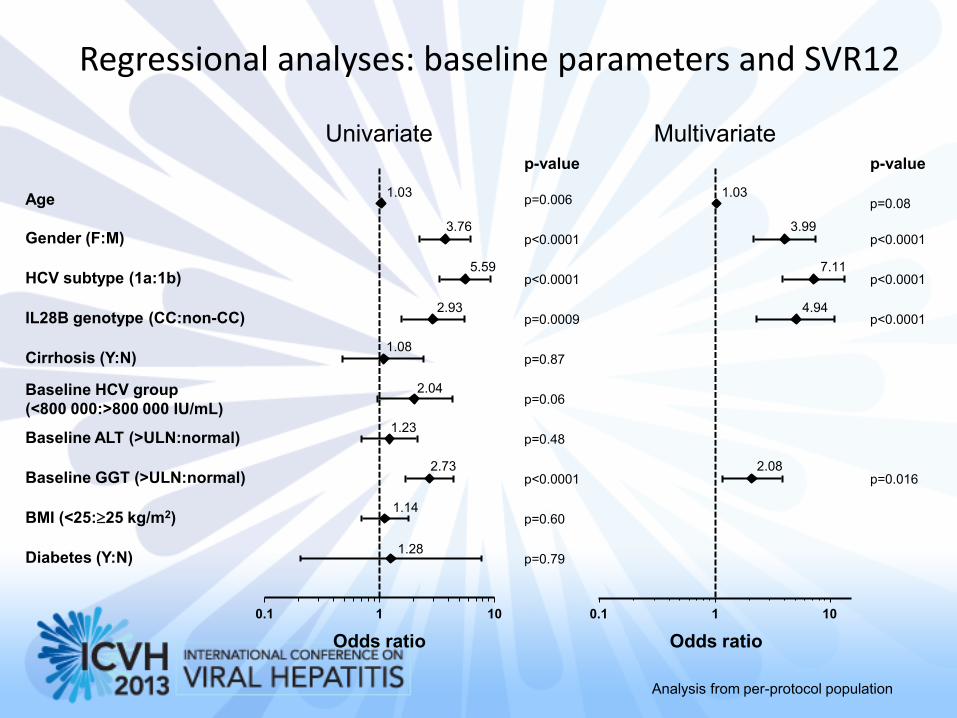
Age
Gender (F:M)
HCV subtype (1a:1b)
Baseline HCV group
(<800 000:>800 000 IU/mL)
Baseline ALT (>ULN:normal)
Cirrhosis (Y:N)
BMI (<25:25 kg/m2)
Diabetes (Y:N)
IL28B genotype (CC:non-CC)
Baseline GGT (>ULN:normal)
p-value p-value
Univariate
p=0.006
p<0.0001
p<0.0001
p=0.0009
p=0.87
p=0.06
p=0.48
p<0.0001
p=0.60
p=0.79
p<0.0001
p<0.0001
p<0.0001
p=0.016
Multivariate
Regressional analyses: baseline parameters and SVR12
Odds ratio Odds ratio
0.1 1 10 0.1 1 10
p=0.08 1.03
3.76
5.59
2.93
1.08
2.04
1.23
2.73
1.14
1.28
1.03
3.99
7.11
4.94
2.08
Analysis from per-protocol population
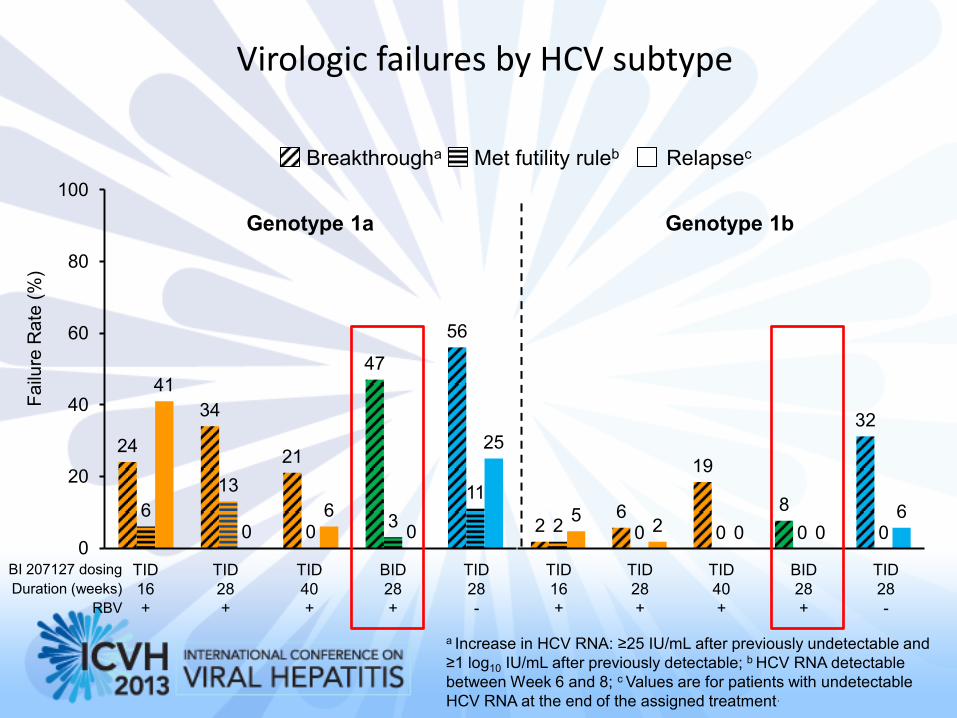
Virologic failures by HCV subtype
24
34
21
47
56
6
13
0 3
11
41
0 6
0
25
0
20
40
60
80
100
Fa
ilure
Ra
te (
%)
a Increase in HCV RNA: ≥25 IU/mL after previously undetectable and
≥1 log10 IU/mL after previously detectable; b HCV RNA detectable
between Week 6 and 8; c Values are for patients with undetectable
HCV RNA at the end of the assigned treatment.
TID
16
+
TID
28
+
TID
40
+
BID
28
+
TID
28
-
BI 207127 dosing
Duration (weeks)
RBV
Breakthrougha Relapsec Met futility ruleb
2 6
19
8
32
2 0 0 0 0 5
2 0 0 6
Genotype 1a Genotype 1b
TID
16
+
TID
28
+
TID
40
+
BID
28
+
TID
28
-
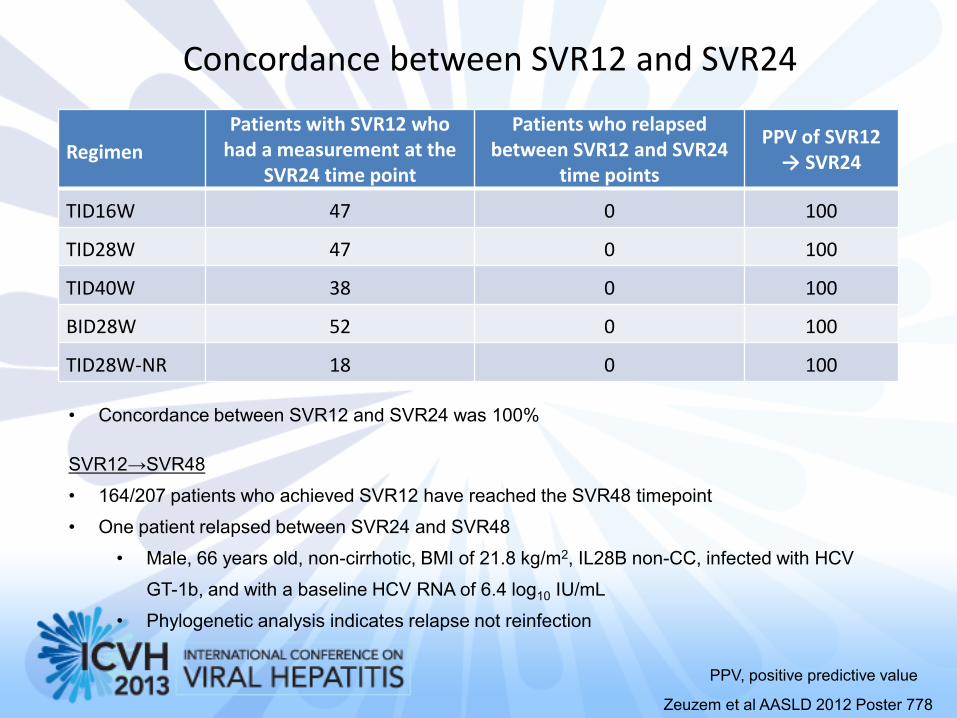
Concordance between SVR12 and SVR24
Regimen
Patients with SVR12 who had a measurement at the
SVR24 time point
Patients who relapsed between SVR12 and SVR24
time points
PPV of SVR12 → SVR24
TID16W 47 0 100
TID28W 47 0 100
TID40W 38 0 100
BID28W 52 0 100
TID28W-NR 18 0 100
PPV, positive predictive value
• Concordance between SVR12 and SVR24 was 100%
SVR12→SVR48
• 164/207 patients who achieved SVR12 have reached the SVR48 timepoint
• One patient relapsed between SVR24 and SVR48
• Male, 66 years old, non-cirrhotic, BMI of 21.8 kg/m2, IL28B non-CC, infected with HCV
GT-1b, and with a baseline HCV RNA of 6.4 log10 IU/mL
• Phylogenetic analysis indicates relapse not reinfection
Zeuzem et al AASLD 2012 Poster 778
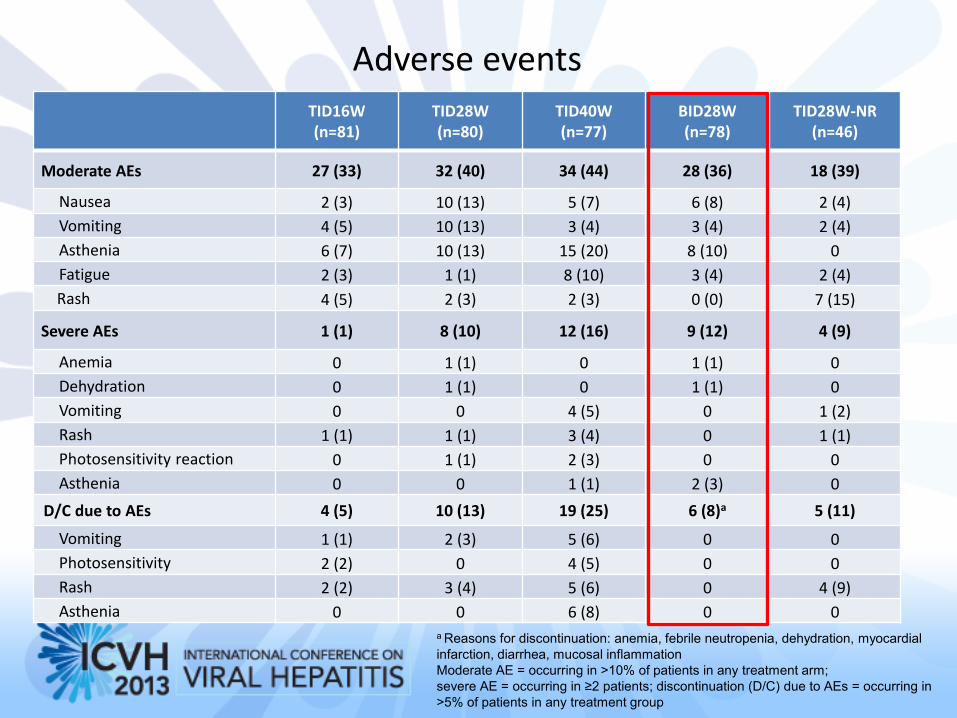
Adverse events TID16W (n=81)
TID28W (n=80)
TID40W (n=77)
BID28W (n=78)
TID28W-NR (n=46)
Moderate AEs 27 (33) 32 (40) 34 (44) 28 (36) 18 (39)
Nausea 2 (3) 10 (13) 5 (7) 6 (8) 2 (4)
Vomiting 4 (5) 10 (13) 3 (4) 3 (4) 2 (4)
Asthenia 6 (7) 10 (13) 15 (20) 8 (10) 0
Fatigue 2 (3) 1 (1) 8 (10) 3 (4) 2 (4)
Rash 4 (5) 2 (3) 2 (3) 0 (0) 7 (15)
Severe AEs 1 (1) 8 (10) 12 (16) 9 (12) 4 (9)
Anemia 0 1 (1) 0 1 (1) 0
Dehydration 0 1 (1) 0 1 (1) 0
Vomiting 0 0 4 (5) 0 1 (2)
Rash 1 (1) 1 (1) 3 (4) 0 1 (1)
Photosensitivity reaction 0 1 (1) 2 (3) 0 0
Asthenia 0 0 1 (1) 2 (3) 0
D/C due to AEs 4 (5) 10 (13) 19 (25) 6 (8)a 5 (11)
Vomiting 1 (1) 2 (3) 5 (6) 0 0
Photosensitivity 2 (2) 0 4 (5) 0 0
Rash 2 (2) 3 (4) 5 (6) 0 4 (9)
Asthenia 0 0 6 (8) 0 0
a Reasons for discontinuation: anemia, febrile neutropenia, dehydration, myocardial
infarction, diarrhea, mucosal inflammation
Moderate AE = occurring in >10% of patients in any treatment arm;
severe AE = occurring in ≥2 patients; discontinuation (D/C) due to AEs = occurring in
>5% of patients in any treatment group
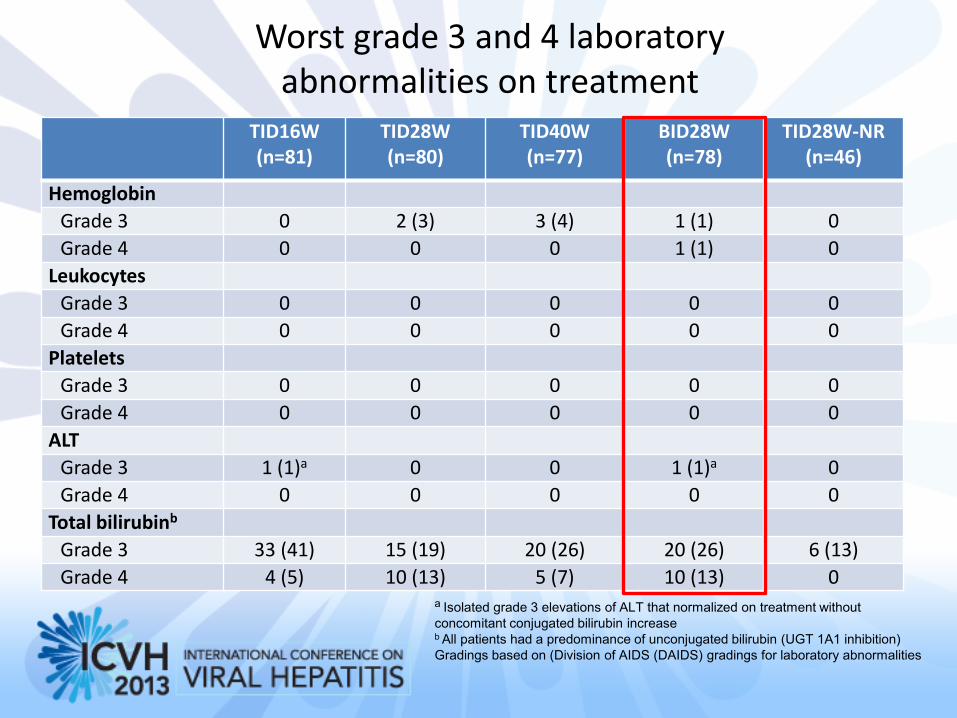
Worst grade 3 and 4 laboratory abnormalities on treatment
TID16W (n=81)
TID28W (n=80)
TID40W (n=77)
BID28W (n=78)
TID28W-NR (n=46)
Hemoglobin
Grade 3 0 2 (3) 3 (4) 1 (1) 0
Grade 4 0 0 0 1 (1) 0
Leukocytes
Grade 3 0 0 0 0 0
Grade 4 0 0 0 0 0
Platelets
Grade 3 0 0 0 0 0
Grade 4 0 0 0 0 0
ALT
Grade 3 1 (1)a 0 0 1 (1)a 0
Grade 4 0 0 0 0 0
Total bilirubinb
Grade 3 33 (41) 15 (19) 20 (26) 20 (26) 6 (13)
Grade 4 4 (5) 10 (13) 5 (7) 10 (13) 0 a Isolated grade 3 elevations of ALT that normalized on treatment without
concomitant conjugated bilirubin increase b All patients had a predominance of unconjugated bilirubin (UGT 1A1 inhibition)
Gradings based on (Division of AIDS (DAIDS) gradings for laboratory abnormalities
Conclusions
• Faldaprevir plus BI 207127 plus RBV achieved SVR rates of up to 69% in this study,
including patients with compensated cirrhosis
SVR12 rates up to 85% in GT-1b with BI 207127 BID
SVR12 successfully predicted SVR24 with this interferon-free regimen
BI 207127 BID had the most favorable tolerability profile with a low rate of discontinuation and no
moderate or severe skin reactions
• In GT-1b patients receiving the TID (+RBV) regimens, treatment durations >16 weeks
did not increase SVR
• GT-1a patients had lower SVR12 rates than GT-1b patients, possibly due to the lower
activity of BI 207127 in this population1,2
GT-1a patients also had a lower barrier to resistance than GT-1b patients3
• RBV remains a necessary component of treatment
• Phase III studies evaluating the combination of faldaprevir 120 mg QD and
BI 207127 600 mg BID with RBV began in 2012
1Larrey et al., Hepatology 2009;50(Suppl 4): 267A 2Beaulieu et al., J Hepatol 2012;56(Suppl 2): S321
3Sarrazin et al., Gastroenterol 2010;138:447–62