Embed Size (px)
Citation preview

Internal Medicine Board Review: Cardiology
Acute Coronary Syndrome
Christine Nardi
May 20, 2009

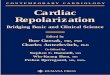
Hospitalizations in the U.S. Due to ACS
Acute Coronary Syndromes*
1.57 Million Hospital Admissions - ACS
UA/NSTEMI† STEMI
1.24 million Admissions per year
0.33 million Admissions per year
*Primary and secondary diagnoses. †About 0.57 million NSTEMI and 0.67 million UA.Heart Disease and Stroke Statistics – 2007 Update. Circulation 2007; 115:69–171.
Incidence rate of MI
has not
changed but survival has

Acute Coronary Syndrome
• Clinical syndromes caused by acute myocardial ischemia– Unstable angina
• Angina at rest or new onset angina, accelerating symptoms• No detectable increase of biomarkers
– Non-ST-elevation MI• Angina at rest or new onset angina, accelerating symptoms• Detectable release of biomarkers
– ST-elevation MI• Clinical presentation of acute myocardial infarction with EKG
evidence of ST-segment elevation

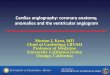
Timing of Release of Various Biomarkers After Acute Myocardial Infarction
Shapiro BP, Jaffe AS. Cardiac biomarkers. In: Murphy JG, Lloyd MA, editors. Mayo Clinic Cardiology: Concise Textbook. 3rd ed. Rochester, MN: Mayo Clinic Scientific Press and New York: Informa Healthcare USA, 2007:773–80. Anderson JL, et al. J Am Coll Cardiol 2007;50:e1–e157, Figure 5.

Pathophysiology: unstable angina and NSTEMI
• Spontaneous rupture of lipid-laden, macrophage rich atherosclerotic plaques leading to platelet activation and thrombosis
• Leads to episodic cessation of coronary blood flow, ischemia and pain
• Rarely, caused by vasospasm (Prinzmetal’s or cocaine)

Causes of UA/NSTEMI*
• Thrombus or thromboembolism, usually arising on disrupted or eroded plaque– Occlusive thrombus, usually with collateral vessels†– Subtotally occlusive thrombus on pre-existing plaque– Distal microvascular thromboembolism from plaque-
associated thrombus – Thromboembolism from plaque erosion
• Non–plaque-associated coronary thromboembolism• Dynamic obstruction (coronary spasm‡ or
vascoconstriction) of epicardial and/or microvascular vessels
• Progressive mechanical obstruction to coronary flow• Coronary arterial inflammation• Secondary UA• Coronary artery dissection§
*These causes are not mutually exclusive; some patients have 2 or more causes. †DeWood MA, et al. N Engl J Med 1986;315:417–23. ‡May occur on top of an atherosclerotic plaque, producing missed-etiology angina or UA/NSTEMI. §Rare. Modified with permission from Braunwald E. Circulation 1998;98:2219–22. Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157, Table 3.

Pathophysiology of STEMI
• Occlusive thrombus that develops on a dissected or ulcerative atherosclerotic plaque, resulting in complete epicardial coronary artery occlusion
• Moderately sized plaques are more common than those causing severe stenosis

Evaluation
• History
• Physical exam
• EKG
• Cardiac biomarkers

•Age ≥ 65 years
•At least 3 risk factors for CAD
•Prior coronary stenosis of ≥ 50%
•ST-segment deviation on ECG presentation
•At least 2 anginal events in prior 24 hours
•Use of aspirin in prior 7 days
•Elevated serum cardiac biomarkers
Variables Used in the TIMI Risk Score
The TIMI risk score is determined by the sum of the presence of the above 7 variables at admission. 1 point is given for each variable. Primary coronary stenosis of 50% or more remained relatively insensitive to missing information and remained a significant predictor of events. Antman EM, et al. JAMA 2000;284:835–42.TIMI = Thrombolysis in Myocardial Infarction.
0-2 low risk (5%)3-4 intermediate risk5-7 high risk (40%)

Selection of Initial Treatment Strategy: Initial Invasive Versus Conservative Strategy
Invasive Recurrent angina/ischemia at rest with low-level activities despite intensive medical therapy
Elevated cardiac biomarkers (TnT or TnI)
New/presumably new ST-segment depression
Signs/symptoms of heart failure or new/worsening mitral regurgitation
High-risk findings from noninvasive testing
Hemodynamic instability
Sustained ventricular tachycardia
PCI within 6 months
Prior CABG
High risk score (e.g., TIMI, GRACE)
Reduced left ventricular function (LVEF < 40%)
Conservative
Low risk score (e.g., TIMI, GRACE)
Patient/physician presence in the absence of high-risk features
angiography
Stress testing

UA/NSTEMI
StatinASA and/or clopidogrelB-blocker
NitrateHeparin/LMWH
TIMI 5-7 TIMI 3-4 TIMI 1-2
GP IIb/IIIa inhibitor Stress imaging study
Recurrent anginaElevated trop
New ST depressionCHF
Prior CABGPCI within 6 moSustained VT
Hemodynamic instability
PositiveOr EF<40
normal
Medical therapycath
yes no

Feature
High Risk
≥ 1 of the features
below must be present:
Intermediate RiskNo high-risk features, but must
have 1 of the following:
Low RiskNo high- or
intermediate- risk features but may have any features
below:
History Accelerating tempo of ischemic sx in preceding 48 h
Prior MI, peripheral or cerebrovascular disease, or CABG; prior ASA use
Character of pain
Prolonged ongoing (> 20 min) rest pain
• Prolonged (> 20 min) rest angina, now resolved, w/ moderate/high likelihood of CAD
• Rest angina (> 20 min) or relieved with rest or sublingual NTG
• Nocturnal angina• New-onset or progressive
CCS class III/IV angina in past 2 wks w/o prolonged (> 20 min) rest pain but with intermediate/high likelihood of CAD
• ↑ Angina frequency, severity or duration
• Angina provoked at lower threshold
• New onset angina with onset 2 wks to 2 mos prior to presentation
Short-Term Risk of Death/Nonfatal MI in Patients With UA/NSTEMI

Feature
High risk Intermediate risk Low risk
Clinical findings
• Pulmonary edema, most likely due to ischemia
• New/worsening MR murmur
• S3 or new/worsening rales
• Hypotension, bradycardia, tachycardia
• Age > 75 y
Age > 70 y
ECG •Angina @ rest with transient ST-segment changes > 0.5 mm
•BBB, new/presumed new
•Sustained VT
• T-wave changes • Pathological
Q-waves/resting ST-depression < 1 mm in multiple lead groups (anterior, inferior, lateral)
Normal or unchanged ECG
Cardiac markers
↑ Cardiac TnT, TnI, or CK-MB (e.g., TnT/TnI > 0.1 ng/mL)
Slightly ↑ cardiac TnT, TnI, or CK-MB (e.g., TnT > 0.01, but < 0.1 ng/mL)
Normal
Estimation of the short-term risk of death and nonfatal cardiac ischemic events in UA/NSTEMI is a complex multivariable problem that cannot be fully specified in a table such as this; this table is mean to offer general guidance & illustration rather than rigid algorithms. Braunwald E, et al. AHCPR Publication No. 94-0602:1–154. Anderson JL, et al. J Am Coll Cardiol 2007;50:e1–e157, Table 7.
Short-Term Risk of Death/Nonfatal MI in Patients With UA/NSTEMI, Continued

Long-Term Antithrombotic Therapy at Hospital Discharge after UA/NSTEMI
Medical Therapy without Stent
Bare Metal Stent Group
Drug Eluting Stent Group
ASA 162 to 325 mg/d for at least 1 month, then 75 to 162 mg/d indefinitely
(Class I, LOE: A)
&Clopidogrel 75 mg/d for at least 1 month and up to 1
year (Class I, LOE:B)
Add: Warfarin (INR 2.0 to 2.5) (Class IIb, LOE: B)
Continue with dual antiplatelet therapy as
above
Yes
No
Indication for Anticoagulation?
ASA 75 to 162 mg/d indefinitely (Class I,
LOE: A)
&
Clopidogrel 75 mg/d at least 1 month (Class I, LOE: A) and up to 1 year (Class I, LOE: B)
ASA 162 to 325 mg/d for at least 3 to 6
months, then 75 to 162 mg/d indefinitely (Class I, LOE: A)
&
Clopidogrel 75 mg/d for at least 1 year (Class I, LOE: B)
Anderson JL, et al. J Am Coll Cardiol 2007;50:e1–e157, Figure 11. INR = international normalized ratio; LOE = level of evidence.
UA/NSTEMI Patient
Groups at Discharge

Management of STEMI
• PCI– Higher vessel patency,
lower reinfarction and stroke rates, immediate risk stratification
– Should be performed if presenting within 12 hours of symptom onset if a skilled PCI lab is available
• Fibrinolytic therapy– Highly available, ease
of use– If no contraindications
and no PCI available, fibrinolytics should be administered within 30 minutes from arrival to ED (if symptoms started within the last 12 hours)

Absolute Contraindications to Fibrinolytics
• Prior intracranial hemorrhage• Known structural cerebral vascular lesion (AVM)• Known malignant intracranial neoplasm• Ischemic stroke without 3 months• Suspected aortic dissection• Active bleeding (excluding menses)• Significant closed-head injury or facial trauma
within 3 months

Mortality Predictors in STEMI
• Age > 65 years
• Clinically evident heart failure
• Diabetes
• Renal failure
• Previous myocardial infarction
• Time of presentation (reperfusion less successful 12 hours after symptom onset)

Complications during STEMI
• Hypotension– Hypovolemia, increased vagal tone, low CO, hypoxia,
rhythm disturbances
• Pulmonary congestion– O2, nitrates, morphine, diuretics when appropriate
• RV infarction– Hypotension, elevated JVP, inferior STEMI,
bradcardia– ST-elevation in V4R– Treatment: fluids, temporary pacemaker

Complications after STEMI
• Occur in 0.1% of STEMI patients 2-7 days after infarction– Ventricular septal defect– Papillary muscle rupture (acute MR)– Left ventricular free wall rupture (tamponade)– pericarditis
• New systolic murmur (VSD or MR)• Diagnosed with echo or Swan-Ganz catheter
– VSD: O2 saturation step-up– Tamponade: equalization of diastolic pressures in all
heart chambers

Key Points
• Intermediate and high risk patients with UA or NSTEMI benefit from an early invasive strategy with angiography
• Early management of UA or NSTEMI includes ASA, heparin, nitrates, b-blocker, GP IIb/IIIa inhibitor, clopidogrel and statin
• LMWH (enoxaparin) is a suitable alternative to unfractionated heparin for patients with acute coronary syndrome or STEMI and those undergoing early PCI

Key Points
• Clinical predictors of mortality in patients with acute STEMI are time to presentation after symptom onset, age>65, heart failure, DM, renal failure and previous MI
• Immediate reperfusion, preferable with PCI, should be performed for any STEMI
• Most patients with STEMI should be started early on oral b-blocker
• STEMI patients with anterior infarction, pulmonary congestion, or a LVEF<40% should be started on an ACE inhibitor

Differential Diagnosis
• Aortic dissection
• Pulmonary embolus
• Perforating ulcer
• Tension pneumothorax
• Esophageal rupture (Boerhaave’s syndrome)

Key Points
• In patients with STEMI, successful fibrinolysis is suggested by resolution of chest pain and ST-segment elevation and/or transient ventricular arrhythmias early after reperfusion.
• In patients with STEMI, reperfusion arrhythmias usually do not require therapy.
• Immediate coronary angiography is not indicated unless recurrent ischemia, persistent ST elevation or hemodynamic instability (including CHF) occurs.

Key Points
• Patients with STEMI should undergo coronary reperfusion in the most expeditious manner
• STEMI patients who cannot be reperfused by direct coronary intervention within 90 to 120 minutes should receive fibrinolytic therapy if there are no contraindications

Key Points
• Ascending aortic dissection may involve the coronary arteries, most commonly the RCA
• Ascending aortic dissection may lead to disruption of the aortic valve, leading to aortic regurgitation

Key Points
• Glycoprotein receptor blockade is indicated for patients with acute coronary syndrome who will undergo coronary angiography and intervention

Key Points
• Medical therapy for acute, recent myocardial infarction includes B-blocker, aspirin, ACE-inhibitor and statins
• This is an uncomplicated (based on the absence of further symptoms and EKG changes) anterior STEMI
• Late fibrinolysis is not beneficial for most patients and may be associated with an increase of transformation to a hemorrhagic zone of infarction
• A glycoprotein IIb/IIIa blocker in addition to aspirin and heparin is indicated for patients with continuing ischemia, elevated troponin level or other high-risk features including angina at rest with ST changes and CHF

Key Points
• In patients with chest pan and intermediate risk of CAD, non-invasive testing is indicated
• Patients with chest pain and low coronary artery disease risk with a normal EKG and a normal exercise EKG can be discharged without coronary angiography
• Immediate coronary angiography would be appropriate if there were high risk markers: – Elevated enzymes– Hypotension– Decreased LVEF– New EKG changes in a patient with unstable angina or NSTEMI

Key Points
• Right ventricular infarction is a cause of hypotension following inferior infarction and typically requires appropriate volume infusion
• Right ventricular infarction should be suspected as a cause of hypotension when findings of right heart failure coincides with an absence of evidence of pulmonary congestion

Key Points
• Papillary muscle rupture and ventricular septal defect are recognized mechanical complications that occur early after myocardial infarction
• Both papillary muscle rupture and ventricular septal defect present with hypotension and acute dyspnea