Embed Size (px)
Citation preview

Critical Challenges Critical Challenges in in CardiovascularCardiovascular MedicineMedicine
Advancing Management of Acute Coronary Syndromes(ACS)—Advancing Management of Acute Coronary Syndromes(ACS)—Establishing Interventional Cardiology & Emergency Medicine Establishing Interventional Cardiology & Emergency Medicine
Therapeutic Teams Therapeutic Teams
Linking Science and Landmark Studies to the Front Lines of Cardiology PracticeLinking Science and Landmark Studies to the Front Lines of Cardiology Practice
Critical Challenges Critical Challenges in in CardiovascularCardiovascular MedicineMedicine
Advancing Management of Acute Coronary Syndromes(ACS)—Advancing Management of Acute Coronary Syndromes(ACS)—Establishing Interventional Cardiology & Emergency Medicine Establishing Interventional Cardiology & Emergency Medicine
Therapeutic Teams Therapeutic Teams
Linking Science and Landmark Studies to the Front Lines of Cardiology PracticeLinking Science and Landmark Studies to the Front Lines of Cardiology Practice
A. Michael Lincoff, MD, FACCA. Michael Lincoff, MD, FACCVice Chairman for ResearchVice Chairman for Research
Department of Cardiovascular MedicineDepartment of Cardiovascular MedicineDirector, Cleveland ClinicDirector, Cleveland Clinic
Cardiovascular Coordinating CenterCardiovascular Coordinating CenterProfessor of MedicineProfessor of Medicine
Cleveland Clinic Lerner College of Medicine Cleveland Clinic Lerner College of Medicine of Case Western Reserve Universityof Case Western Reserve University
The Cleveland Clinic FoundationThe Cleveland Clinic Foundation
A. Michael Lincoff, MD, FACCA. Michael Lincoff, MD, FACCVice Chairman for ResearchVice Chairman for Research
Department of Cardiovascular MedicineDepartment of Cardiovascular MedicineDirector, Cleveland ClinicDirector, Cleveland Clinic
Cardiovascular Coordinating CenterCardiovascular Coordinating CenterProfessor of MedicineProfessor of Medicine
Cleveland Clinic Lerner College of Medicine Cleveland Clinic Lerner College of Medicine of Case Western Reserve Universityof Case Western Reserve University
The Cleveland Clinic FoundationThe Cleveland Clinic Foundation
EDICT for ACS SlideCASTEDICT for ACS SlideCAST

EDICT for ACS Mission Statement:
Bringing together interventional cardiologists and emergency medicine specialists to manage patients collaboratively and seamlessly in order to improve
clinical outcomes in ACS

CME-accredited symposium jointly sponsored by University of CME-accredited symposium jointly sponsored by University of Massachusetts Medical Center, office of CME and CMEducation Massachusetts Medical Center, office of CME and CMEducation Resources, LLCResources, LLC
Commercial Support:Commercial Support: Sponsored by an independent educational Sponsored by an independent educational grant from The Medicines Companygrant from The Medicines Company
Mission statement:Mission statement: Improve patient care through evidence-based Improve patient care through evidence-based education, expert analysis, and case study-based managementeducation, expert analysis, and case study-based management
Processes:Processes: Strives for fair balance, clinical relevance, on-label Strives for fair balance, clinical relevance, on-label indications for agents discussed, and emerging evidence and indications for agents discussed, and emerging evidence and information from recent studiesinformation from recent studies
COI:COI: Full faculty disclosures provided in syllabus and at the Full faculty disclosures provided in syllabus and at the beginning of the programbeginning of the program
Welcome Welcome

Educational ObjectivesEducational Objectives
► As a result of this session, cardiologists and emergency As a result of this session, cardiologists and emergency physicians will be able to assess and implement optimal physicians will be able to assess and implement optimal antithrombotic strategies for patients with acute coronary antithrombotic strategies for patients with acute coronary syndromes (ACS).syndromes (ACS).
► As a result of this session, attendees will understand impact As a result of this session, attendees will understand impact of specific pharmacologic agents on outcomes, including of specific pharmacologic agents on outcomes, including ischemic endpoints, bleeding, and mortality for patients with ischemic endpoints, bleeding, and mortality for patients with ACS.ACS.
► As a result of this session, attendees are able to discuss the As a result of this session, attendees are able to discuss the impact that new trials are likely to have on future impact that new trials are likely to have on future management of patients with ACS.management of patients with ACS.
► As a result of this session, ED physicians and cardiologists As a result of this session, ED physicians and cardiologists will learn to apply AHA/ACC, ACCP, and other national will learn to apply AHA/ACC, ACCP, and other national guidelines in order to optimize therapy ACS guidelines in order to optimize therapy ACS
► As a result of this session, cardiologists and emergency As a result of this session, cardiologists and emergency physicians will be able to assess and implement optimal physicians will be able to assess and implement optimal antithrombotic strategies for patients with acute coronary antithrombotic strategies for patients with acute coronary syndromes (ACS).syndromes (ACS).
► As a result of this session, attendees will understand impact As a result of this session, attendees will understand impact of specific pharmacologic agents on outcomes, including of specific pharmacologic agents on outcomes, including ischemic endpoints, bleeding, and mortality for patients with ischemic endpoints, bleeding, and mortality for patients with ACS.ACS.
► As a result of this session, attendees are able to discuss the As a result of this session, attendees are able to discuss the impact that new trials are likely to have on future impact that new trials are likely to have on future management of patients with ACS.management of patients with ACS.
► As a result of this session, ED physicians and cardiologists As a result of this session, ED physicians and cardiologists will learn to apply AHA/ACC, ACCP, and other national will learn to apply AHA/ACC, ACCP, and other national guidelines in order to optimize therapy ACS guidelines in order to optimize therapy ACS

Program FacultyProgram Faculty
A. Michael Lincoff, MD, FACCA. Michael Lincoff, MD, FACCVice Chairman for ResearchVice Chairman for ResearchDepartment of Cardiovascular Department of Cardiovascular MedicineMedicineDirector, Cleveland ClinicDirector, Cleveland ClinicCardiovascular Coordinating Cardiovascular Coordinating CenterCenterProfessor of MedicineProfessor of MedicineCleveland Clinic Cleveland Clinic Lerner College of Medicine of Case Lerner College of Medicine of Case Western Reserve UniversityWestern Reserve UniversityThe Cleveland Clinic FoundationThe Cleveland Clinic FoundationCleveland, OHCleveland, OH
A. Michael Lincoff, MD, FACCA. Michael Lincoff, MD, FACCVice Chairman for ResearchVice Chairman for ResearchDepartment of Cardiovascular Department of Cardiovascular MedicineMedicineDirector, Cleveland ClinicDirector, Cleveland ClinicCardiovascular Coordinating Cardiovascular Coordinating CenterCenterProfessor of MedicineProfessor of MedicineCleveland Clinic Cleveland Clinic Lerner College of Medicine of Case Lerner College of Medicine of Case Western Reserve UniversityWestern Reserve UniversityThe Cleveland Clinic FoundationThe Cleveland Clinic FoundationCleveland, OHCleveland, OH
Sunil V. Rao, MD, FACCSunil V. Rao, MD, FACCAssistant Professor of MedicineAssistant Professor of MedicineDuke University Medical CenterDuke University Medical CenterDirector, Cardiac Catheterization Director, Cardiac Catheterization LaboratoriesLaboratoriesDurham VA Medical CenterDurham VA Medical CenterDurham, NCDurham, NC
Charles V. Pollack, MD, FACEP, Charles V. Pollack, MD, FACEP, FAAEMFAAEMChairman, Department of Chairman, Department of Emergency MedicineEmergency MedicinePennsylvania HospitalPennsylvania HospitalProfessor of Emergency Medicine Professor of Emergency Medicine University of Pennsylvania School University of Pennsylvania School of Medicine of Medicine Philadelphia, PAPhiladelphia, PA
Sunil V. Rao, MD, FACCSunil V. Rao, MD, FACCAssistant Professor of MedicineAssistant Professor of MedicineDuke University Medical CenterDuke University Medical CenterDirector, Cardiac Catheterization Director, Cardiac Catheterization LaboratoriesLaboratoriesDurham VA Medical CenterDurham VA Medical CenterDurham, NCDurham, NC
Charles V. Pollack, MD, FACEP, Charles V. Pollack, MD, FACEP, FAAEMFAAEMChairman, Department of Chairman, Department of Emergency MedicineEmergency MedicinePennsylvania HospitalPennsylvania HospitalProfessor of Emergency Medicine Professor of Emergency Medicine University of Pennsylvania School University of Pennsylvania School of Medicine of Medicine Philadelphia, PAPhiladelphia, PA

Financial DisclosuresFinancial Disclosures
Sunil V. Rao, MD, FACCSunil V. Rao, MD, FACCGrant/Research Support: CordisGrant/Research Support: CordisConsultant: sanofi-aventis, The Medicines Co.Consultant: sanofi-aventis, The Medicines Co.Speaker’s Bureau: sanofi-aventis, Cordis, The Medicines Co.Speaker’s Bureau: sanofi-aventis, Cordis, The Medicines Co.
Charles V. Pollack, MD, FACEP, FAAEMCharles V. Pollack, MD, FACEP, FAAEMGrant/Research Support: GlaxoSmithKlineGrant/Research Support: GlaxoSmithKlineConsultant: The Medicines Co., Schering-Plough, sanofi-aventis, BMS, Consultant: The Medicines Co., Schering-Plough, sanofi-aventis, BMS, GenentechGenentechSpeaker’s Bureau: Schering-Plough, sanofi-aventis, BMS, GenentechSpeaker’s Bureau: Schering-Plough, sanofi-aventis, BMS, Genentech
Sunil V. Rao, MD, FACCSunil V. Rao, MD, FACCGrant/Research Support: CordisGrant/Research Support: CordisConsultant: sanofi-aventis, The Medicines Co.Consultant: sanofi-aventis, The Medicines Co.Speaker’s Bureau: sanofi-aventis, Cordis, The Medicines Co.Speaker’s Bureau: sanofi-aventis, Cordis, The Medicines Co.
Charles V. Pollack, MD, FACEP, FAAEMCharles V. Pollack, MD, FACEP, FAAEMGrant/Research Support: GlaxoSmithKlineGrant/Research Support: GlaxoSmithKlineConsultant: The Medicines Co., Schering-Plough, sanofi-aventis, BMS, Consultant: The Medicines Co., Schering-Plough, sanofi-aventis, BMS, GenentechGenentechSpeaker’s Bureau: Schering-Plough, sanofi-aventis, BMS, GenentechSpeaker’s Bureau: Schering-Plough, sanofi-aventis, BMS, Genentech

► AbraxisAbraxis► Alexion PharmaAlexion Pharma► AstraZenecaAstraZeneca► AtherogenicsAtherogenics► AventisAventis► Biosense WebsterBiosense Webster► BiositeBiosite► Boehringer IngelheimBoehringer Ingelheim► Boston ScientificBoston Scientific► Bristol-Myers Squibb Bristol-Myers Squibb
(BMS)(BMS)► CardionetCardionet► CentocorCentocor► Converge Medical Inc.Converge Medical Inc.► CordisCordis► Dr. Reddy’s LaboratoryDr. Reddy’s Laboratory
► Edwards Lifesciences Edwards Lifesciences ► EsperionEsperion► GE MedicalGE Medical► GenentechGenentech► GilfordGilford► GSKGSK► GuidantGuidant► J&JJ&J► Kensey-NashKensey-Nash► LillyLilly► Medicines CompanyMedicines Company► MedtronicMedtronic► MerckMerck► MytogenMytogen
► NovartisNovartis► Novo NordiskNovo Nordisk► Orphan Orphan
TherapeuticsTherapeutics► P&G PharmaP&G Pharma► PfizerPfizer► RocheRoche► SankyoSankyo► Sanofi-AventisSanofi-Aventis► Schering-PloughSchering-Plough► SciosScios► St. Jude MedicalSt. Jude Medical► TakedaTakeda► VasoGenixVasoGenix► ViacorViacor
Michael Lincoff, MD, FACCMichael Lincoff, MD, FACC Relationships with Industry Research Sponsors Relationships with Industry Research Sponsors Cleveland Clinic Cardiovascular Coordinating CenterCleveland Clinic Cardiovascular Coordinating Center
Financial DisclosuresFinancial Disclosures

NOTENOTE
There will be off-label discussions—indications and There will be off-label discussions—indications and dosing—during this CME symposium, and speakers dosing—during this CME symposium, and speakers will note such off-label information. This information will note such off-label information. This information
does not imply or constitute endorsement of such does not imply or constitute endorsement of such strategies, which must be evaluated on the basis of strategies, which must be evaluated on the basis of
evidence and expert analysis.evidence and expert analysis.
Off-Label Discussion and InformationOff-Label Discussion and Information

Advancing Management of Acute Coronary Syndromes Advancing Management of Acute Coronary Syndromes Linking Science and Landmark Studies to the Front Lines Linking Science and Landmark Studies to the Front Lines
of Cardiology Practiceof Cardiology Practice
Advancing Management of Acute Coronary Syndromes Advancing Management of Acute Coronary Syndromes Linking Science and Landmark Studies to the Front Lines Linking Science and Landmark Studies to the Front Lines
of Cardiology Practiceof Cardiology Practice
Introduction to EDICT for ACS ForumIntroduction to EDICT for ACS ForumIntroduction to EDICT for ACS ForumIntroduction to EDICT for ACS Forum
Critical Challenges in Cardiovascular Critical Challenges in Cardiovascular Disease—Introduction Disease—Introduction
A. Michael Lincoff, MD, FACCA. Michael Lincoff, MD, FACCVice Chairman for ResearchVice Chairman for Research
Department of Cardiovascular MedicineDepartment of Cardiovascular MedicineDirector, Cleveland ClinicDirector, Cleveland Clinic
Cardiovascular Coordinating CenterCardiovascular Coordinating CenterProfessor of MedicineProfessor of Medicine
Cleveland Clinic Lerner College of Medicine Cleveland Clinic Lerner College of Medicine of Case Western Reserve Universityof Case Western Reserve University
The Cleveland Clinic FoundationThe Cleveland Clinic Foundation
A. Michael Lincoff, MD, FACCA. Michael Lincoff, MD, FACCVice Chairman for ResearchVice Chairman for Research
Department of Cardiovascular MedicineDepartment of Cardiovascular MedicineDirector, Cleveland ClinicDirector, Cleveland Clinic
Cardiovascular Coordinating CenterCardiovascular Coordinating CenterProfessor of MedicineProfessor of Medicine
Cleveland Clinic Lerner College of Medicine Cleveland Clinic Lerner College of Medicine of Case Western Reserve Universityof Case Western Reserve University
The Cleveland Clinic FoundationThe Cleveland Clinic Foundation

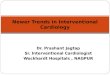
SYNERGY
LMWHLMWH
ESSENCEESSENCE
19941994 19951995 19961996 19971997 19981998 19991999 20002000 20022002 20032003 20042004 20052005 2006200620012001
CURECURE
ClopidogrelClopidogrel
Bleeding riskBleeding risk
Ischemic riskIschemic risk
GP IIb/IIIa GP IIb/IIIa blockersblockers
PRISM-PLUSPRISM-PLUS
PURSUITPURSUIT
ACUITYTACTICS TIMI-18TACTICS TIMI-18
Early invasiveEarly invasive
PCIPCI ~ 5% stents~ 5% stents ~85% stents~85% stents Drug-eluting stentsDrug-eluting stents
ISAR-REACT 2
Milestones in ACS Management
OASIS-5
[ Fondaparinux ][ Fondaparinux ]
Anti-Thrombin RxAnti-Thrombin Rx
Anti-Platelet RxAnti-Platelet Rx
Treatment StrategyTreatment Strategy
HeparinHeparin
AspirinAspirin
ConservativeConservative
ICTUS
BivalirudinBivalirudin
REPLACE 2REPLACE 2
Adapted from and with the courtesy of Steven Manoukian, MD.Adapted from and with the courtesy of Steven Manoukian, MD.Adapted from and with the courtesy of Steven Manoukian, MD.Adapted from and with the courtesy of Steven Manoukian, MD.

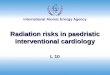
Sites of Antithrombotic Drug ActionSites of Antithrombotic Drug Action
Tissue factorTissue factor
Plasma clottingcascade
Plasma clottingcascade
ProthrombinProthrombin
ThrombinThrombin
FibrinogenFibrinogen FibrinFibrin
ThrombusThrombus
Platelet aggregationPlatelet aggregation
Platelet activationPlatelet activation
CollagenCollagen
Thromboxane A2Thromboxane A2
ADPADP
ATAT
ATAT
Aspirin
ClopidogrelPrasugrelCangrelor
EptifibatideAbciximabTirofiban
(GPI)BivalirudinHirudin
Argatroban
FactorXa
FactorXa
Heparin LMWHs
Fibrinolytics
FondaparinuxATAT

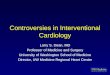
1992 1995 1998 2001 2004 2007
1997 1999
UFH
LMWH TIMI 11B
2004
SYNERGY
Bivalirudin
2003
REPLACE 2
ASA
IIb/IIIa antagonists
1995
2001
1998
EPISTENT
PURSUIT
2001
ESPRIT
GUSTO 42004
ISAR REACT
Clopidogrel CURE
2000
Anti-thrombotic agents
Anti-platelet agents
Evolving ACS Therapies and Patterns of Antithrombotic Use*
ACUITY
2006
ISAR-REACT 2
* Width of bar represents approximate degree of use of antiplatelet or anticoagulants at a particular time

A Science-to-Strategy Analysis of BleedingIssues in Acute Coronary Syndromes
A Science-to-Strategy Analysis of BleedingIssues in Acute Coronary Syndromes
BLEEDING IN THE SETTING OFACUTE CORONARY SYNDROMES (ACS)
Clinical Implications and Effects on Mortality and Resource Utilization
BLEEDING IN THE SETTING OFACUTE CORONARY SYNDROMES (ACS)
Clinical Implications and Effects on Mortality and Resource Utilization
Sunil V. Rao, MD, FACCSunil V. Rao, MD, FACCAssistant Professor of MedicineAssistant Professor of MedicineDuke University Medical CenterDuke University Medical Center
Director, Cardiac Catheterization LaboratoriesDirector, Cardiac Catheterization LaboratoriesDurham VA Medical CenterDurham VA Medical Center
Durham, NCDurham, NC
Sunil V. Rao, MD, FACCSunil V. Rao, MD, FACCAssistant Professor of MedicineAssistant Professor of MedicineDuke University Medical CenterDuke University Medical Center
Director, Cardiac Catheterization LaboratoriesDirector, Cardiac Catheterization LaboratoriesDurham VA Medical CenterDurham VA Medical Center
Durham, NCDurham, NC

Ischemic Complications Ischemic
Complications
► Death
► MI
► Urgent TVR
► Death
► MI
► Urgent TVR
Evolving Paradigm for Evaluating ACS Evolving Paradigm for Evaluating ACS Management StrategiesManagement Strategies
Composite Adverse Event EndpointsComposite Adverse Event Endpoints

Ischemic Complications Ischemic
Complications Hemorrhage HIT
Hemorrhage HIT
► Death
► MI
► Urgent TVR
► Death
► MI
► Urgent TVR
► Major Bleeding
► Minor Bleeding
► Thrombocytopenia
► Major Bleeding
► Minor Bleeding
► Thrombocytopenia
Composite Adverse Event EndpointsComposite Adverse Event Endpoints
Evolving Paradigm for Evaluating ACS Evolving Paradigm for Evaluating ACS Management StrategiesManagement Strategies
Evolving Paradigm for Evaluating ACS Evolving Paradigm for Evaluating ACS Management StrategiesManagement Strategies

Periprocedural
Complications
Periprocedural
Complications
Clinical BenefitClinical Benefit
► Death
► Major Disability
► Death
► Major Disability
► Cost
► Ease of Use
► Duration of Therapy
► Accounting for Bleeding and Ischemic Endpoints
► Cost
► Ease of Use
► Duration of Therapy
► Accounting for Bleeding and Ischemic Endpoints
Composite Adverse Event EndpointsComposite Adverse Event Endpoints
Evolving Paradigm for Evaluating ACS Evolving Paradigm for Evaluating ACS Management StrategiesManagement Strategies
Evolving Paradigm for Evaluating ACS Evolving Paradigm for Evaluating ACS Management StrategiesManagement Strategies

DeathDeath 4.3%4.3%
(Re)-Infarction(Re)-Infarction 2.5%2.5%
CHFCHF 8.0%8.0%
Cardiogenic ShockCardiogenic Shock 2.6%2.6%
StrokeStroke 0.8%0.8%
Non-CABG TransfusionNon-CABG Transfusion 9.9%9.9%
Bhatt DL, et al. Bhatt DL, et al. JAMAJAMA. 2004 Nov 3;292(17):2096-104. . 2004 Nov 3;292(17):2096-104.
CRUSADE In-Hospital OutcomesCRUSADE In-Hospital Outcomes

Bleeding in ACS - AgendaBleeding in ACS - Agenda
► Predictors of bleeding in ACSPredictors of bleeding in ACS
► Outcomes associated with bleedingOutcomes associated with bleeding Impact of definition on outcomesImpact of definition on outcomes
► Outcomes associated with blood Outcomes associated with blood transfusiontransfusion
► Special populations at riskSpecial populations at risk ElderlyElderly Chronic kidney diseaseChronic kidney disease AnemiaAnemia
► Cost implications of bleeding Cost implications of bleeding

What predicts bleeding among patients
with ACS ?
What predicts bleeding among patients
with ACS ?
Bleeding in ACS
Question to be answered:Question to be answered:

Independent Independent Predictors of Predictors of Major Bleeding Major Bleeding in Marker Positive in Marker Positive Acute Coronary Acute Coronary SyndromesSyndromes
Moscucci, GRACE Registry, Moscucci, GRACE Registry, Eur Heart JEur Heart J. 2003 Oct;24(20):1815-23. . 2003 Oct;24(20):1815-23.
Predictors of Major Bleeding in ACSPredictors of Major Bleeding in ACS
► Older AgeOlder Age
► Female GenderFemale Gender
► Renal FailureRenal Failure
► History of BleedingHistory of Bleeding
► Right Heart CatheterizationRight Heart Catheterization
► GPIIb-IIIa antagonistsGPIIb-IIIa antagonists

0 1 2 3
P-valueP-valueRR (95% CI)RR (95% CI)Risk ratio ± 95% CIRisk ratio ± 95% CIRisk ratio ± 95% CIRisk ratio ± 95% CI
Predictors of Major BleedingPredictors of Major Bleeding
Age Age >>75 (vs. 55-75)75 (vs. 55-75)
AnemiaAnemia
CrCl <60mL/minCrCl <60mL/min
DiabetesDiabetes
Female genderFemale gender
High-risk (ST / biomarkers)High-risk (ST / biomarkers)
HypertensionHypertension
No prior PCINo prior PCI
Prior antithrombotic therapyPrior antithrombotic therapy
Heparin(s) + GPI (vs. Bivalirudin)Heparin(s) + GPI (vs. Bivalirudin)
1.56 (1.19-2.04)1.56 (1.19-2.04) 0.00090.0009
1.89 (1.48-2.41)1.89 (1.48-2.41) <0.0001<0.0001
1.68 (1.29-2.18)1.68 (1.29-2.18) <0.0001<0.0001
1.30 (1.03-1.63)1.30 (1.03-1.63) 0.02480.0248
2.08 (1.68-2.57)2.08 (1.68-2.57) <0.0001<0.0001
1.42 (1.06-1.90)1.42 (1.06-1.90) 0.01780.0178
1.33 (1.03-1.70)1.33 (1.03-1.70) 0.02870.0287
1.47 (1.15-1.88)1.47 (1.15-1.88) 0.00190.0019
1.23 (0.98-1.55)1.23 (0.98-1.55) 0.07680.0768
2.08 (1.56-2.76)2.08 (1.56-2.76) <0.0001<0.0001
Manoukian SV, Voeltz MD, Feit F et al. TCT 2006.
Results: The ACUITY Trial PCI PopulationResults: The ACUITY Trial PCI PopulationResults: The ACUITY Trial PCI PopulationResults: The ACUITY Trial PCI Population

0 1 2 3 4 5
P-valueP-valueRR (95% CI)RR (95% CI)
Age Age >>75 (vs. 55-75)75 (vs. 55-75)
AnemiaAnemia
CrCl <60mL/minCrCl <60mL/min
DiabetesDiabetes
Female genderFemale gender
High-risk (ST / biomarkers)High-risk (ST / biomarkers)
HypertensionHypertension
HeparinHeparin(s)(s) + GPI + GPI (vs. Bivalirudin)(vs. Bivalirudin)
1.420 (1.055-1.910)1.420 (1.055-1.910) 0.00600.0060
3.764 (2.919-4.855)3.764 (2.919-4.855) <0.0001<0.0001
2.097 (1.568-2.803)2.097 (1.568-2.803) <0.0001<0.0001
1.560 (1.209-2.014)1.560 (1.209-2.014) 0.00600.0060
2.233 (1.739-2.867)2.233 (1.739-2.867) <0.0001<0.0001
1.754 (1.297-2.372)1.754 (1.297-2.372) 0.00030.0003
1.457 (1.051-2.020)1.457 (1.051-2.020) 0.02410.0241
1.728 (1.256-2.379)1.728 (1.256-2.379) 0.00070.0007
Predictors of TransfusionPredictors of Transfusion
Risk ratio ± 95% CIRisk ratio ± 95% CIRisk ratio ± 95% CIRisk ratio ± 95% CI
Manoukian SV, Voeltz MD, Feit F et al. TCT 2006.
Results: The ACUITY TrialResults: The ACUITY TrialResults: The ACUITY TrialResults: The ACUITY Trial

REPLACE-2REPLACE-2Multivariate Predictors of Major BleedingMultivariate Predictors of Major Bleeding
RISK FACTORSRISK FACTORS Odds RatioOdds Ratio 95% CI95% CI p-valuep-value
Baseline risk factorsBaseline risk factors
Age Age >> 75 75 1.4821.482 1.009 to 2.1761.009 to 2.176 0.0450.045
Gender (M vs. F)Gender (M vs. F) 0.6520.652 0.477 to 0.8900.477 to 0.890 0.00720.0072
Prior AnginaPrior Angina 1.5891.589 1.077 to 2.3451.077 to 2.345 0.01970.0197
Creatinine clearance* Creatinine clearance* 0.9930.993 0.987 to 0.9980.987 to 0.998 0.00610.0061
AnemiaAnemia 1.4031.403 1.015 to 1.9391.015 to 1.939 0.04010.0401
Peri-procedural risk factorsPeri-procedural risk factors
Treatment Group (BIV vs. H+GPI)Treatment Group (BIV vs. H+GPI) 0.5080.508 0.352 to 0.7330.352 to 0.733 0.00030.0003
Provisional GPI receivedProvisional GPI received 2.6792.679 1.591 to 4.5121.591 to 4.512 0.00020.0002
Procedure Duration >1hProcedure Duration >1h 2.0492.049 1.217 to 3.4491.217 to 3.449 0.00690.0069
Time to Sheath Removal >6hTime to Sheath Removal >6h 1.6141.614 1.064 to 2.4481.064 to 2.448 0.02440.0244
ICU stay (days)†ICU stay (days)† 1.251.25 1.183 to 1.3211.183 to 1.321 <0.0001<0.0001
IABPIABP 8.7058.705 3.433 to 22.0723.433 to 22.072 <0.0001<0.0001Feit F et al. Unpublished (in manuscript)

► Older age, chronic kidney disease, female gender are consistently associated with bleeding and blood transfusion
► Analysis of large randomized trials have also identified novel risk factors for bleeding such as diabetes and anemia
► Procedural characteristics such as procedure duration and sheath dwell time also predict bleeding complications
► Older age, chronic kidney disease, female gender are consistently associated with bleeding and blood transfusion
► Analysis of large randomized trials have also identified novel risk factors for bleeding such as diabetes and anemia
► Procedural characteristics such as procedure duration and sheath dwell time also predict bleeding complications
Bleeding Predictors—Conclusions

Does bleeding influence the prognosis
of ACS patients ?
Does bleeding influence the prognosis
of ACS patients ?
Bleeding in ACS
Question to be answered:Question to be answered:

Moscucci M et al. Moscucci M et al. Eur Heart JEur Heart J 2003;24:1815-23. 2003;24:1815-23.
P<0.001
5.13.0
5.37.0
18.616.1 15.3
22.8
0.0
10.0
20.0
30.0
40.0
No Bleed
Bleed
Overall Unstable NSTEMI STEMIOverall Unstable NSTEMI STEMI ACS AnginaACS Angina
Pat
ien
ts (
%)
Pat
ien
ts (
%)
Major Bleeding Predicts Mortality in ACSMajor Bleeding Predicts Mortality in ACSMajor Bleeding Predicts Mortality in ACSMajor Bleeding Predicts Mortality in ACS
24,045 ACS patients in the GRACE registry, in-hospital death24,045 ACS patients in the GRACE registry, in-hospital death24,045 ACS patients in the GRACE registry, in-hospital death24,045 ACS patients in the GRACE registry, in-hospital death

log rank p-value for all four categories <0.0001log-rank p-value for no bleeding vs. mild bleeding = 0.02log-rank p-value for mild vs. moderate bleeding <0.0001log-rank p-value for moderate vs. severe <0.001
Bleeding & OutcomesBleeding & Outcomes
Rao SV, et al. Rao SV, et al. Am J CardiolAm J Cardiol. 2005 Nov 1;96(9):1200-6. Epub 2005 Sep 12 . 2005 Nov 1;96(9):1200-6. Epub 2005 Sep 12 Rao SV, et al. Rao SV, et al. Am J CardiolAm J Cardiol. 2005 Nov 1;96(9):1200-6. Epub 2005 Sep 12 . 2005 Nov 1;96(9):1200-6. Epub 2005 Sep 12
Kaplan Meier Curves for 30-Day Death, Stratified by Bleed SeverityKaplan Meier Curves for 30-Day Death, Stratified by Bleed Severity
N=26,452 ACS patients from GUSTO IIb, PARAGON A, PARAGON B, & PURSUIT N=26,452 ACS patients from GUSTO IIb, PARAGON A, PARAGON B, & PURSUIT

26,452 patients from PURSUIT, PARAGON A, 26,452 patients from PURSUIT, PARAGON A, PARAGON B, GUSTO IIb NSTPARAGON B, GUSTO IIb NST
Bleeding severity and adjusted hazard of deathBleeding severity and adjusted hazard of death
*p<0.0001*p<0.0001
Bleeding and Outcomes in NSTE ACS Bleeding and Outcomes in NSTE ACS
Bleeding SeverityBleeding Severity 30d Death30d Death 30d Death/MI30d Death/MI 6 mo. Death6 mo. Death
Mild*Mild* 1.6 1.6 1.31.3 1.41.4
Moderate*Moderate* 2.7 2.7 3.33.3 2.12.1
Severe*Severe* 10.610.6 5.65.6 7.57.5
*Bleeding as a time-dependent covariate*Bleeding as a time-dependent covariate
Rao SV, et al. Rao SV, et al. Am J CardiolAm J Cardiol. 2005 Nov 1;96(9):1200-6. Epub 2005 Sep 12 . 2005 Nov 1;96(9):1200-6. Epub 2005 Sep 12 Rao SV, et al. Rao SV, et al. Am J CardiolAm J Cardiol. 2005 Nov 1;96(9):1200-6. Epub 2005 Sep 12 . 2005 Nov 1;96(9):1200-6. Epub 2005 Sep 12

9.3%
3.0%
17.1%
5.4%
24.2%
5.5%7.8%
0.8%
IschemicComposite
Death MI (all) UnplannedRevasc
30 d
ay e
ven
ts (
%)
Major Bleeding (N=462, 5.9%) No Major Bleeding (N=7327, 94.1%)
Major Bleeding, Ischemic Endpoints, Major Bleeding, Ischemic Endpoints, and Mortalityand Mortality
9.3%
3.0%
17.1%
5.4%
24.2%
5.5%7.8%
0.8%
IschemicComposite
Death MI (all) UnplannedRevasc
30 d
ay e
ven
ts (
%)
Major Bleeding (N=462, 5.9%) No Major Bleeding (N=7327, 94.1%)
P<0.0001 for all
Manoukian SV, Voeltz MD, Feit F et al. TCT 2006.
Results: The ACUITY Trial PCI Population (N=7,789)Results: The ACUITY Trial PCI Population (N=7,789)Results: The ACUITY Trial PCI Population (N=7,789)Results: The ACUITY Trial PCI Population (N=7,789)

4.8%
12.6%
17.1%
0.8%
5.5% 4.8%
MI (all) Non-Q MI Q-MI
30 d
ay e
ven
ts (
%)
Major Bleeding (N=462, 5.9%) No Major Bleeding (N=7327, 94.1%)
Major Bleeding and Myocardial InfarctionMajor Bleeding and Myocardial Infarction
4.8%
12.6%
17.1%
0.8%
5.5% 4.8%
MI (all) Non-Q MI Q-MI
30 d
ay e
ven
ts (
%)
Major Bleeding (N=462, 5.9%) No Major Bleeding (N=7327, 94.1%)
P<0.0001 for all
Manoukian SV, Voeltz MD, Feit F et al. TCT 2006.
Results: The ACUITY Trial PCI Population (N=7,789)Results: The ACUITY Trial PCI Population (N=7,789)Results: The ACUITY Trial PCI Population (N=7,789)Results: The ACUITY Trial PCI Population (N=7,789)

Major and Minor Bleeding in PCIMajor and Minor Bleeding in PCIBleeding Increases Mortality and EventsBleeding Increases Mortality and Events
Kinnaird TD et al. AM J Cardiol 2003;92:930-5.
10,974 patients undergoing PCI, Washington Hospital Center, 1991-2000.
In-Hospital Clinical EventsIn-Hospital Clinical Events
MajorMajor(n=588)(n=588)
MinorMinor(n=1,394)(n=1,394)
NoneNone(n=8,992)(n=8,992)
DeathDeath 7.5%*7.5%*†† 1.8%*1.8%* 0.6%0.6%
Q-wave myocardial infarctionQ-wave myocardial infarction 1.2%*1.2%* 0.7%0.7%‡‡ 0.2%0.2%
Non-Q-wave myocardial infarctionNon-Q-wave myocardial infarction 30.7%*30.7%*†† 16.8%*16.8%* 11.8%11.8%
Repeat lesion angioplastyRepeat lesion angioplasty 1.9%*1.9%*§§ 0.8%0.8%‡‡ 0.3%0.3%
Major adverse cardiac eventMajor adverse cardiac event 6.6%*6.6%*†† 2.2%*2.2%* 0.6%0.6%
Bleeding ComplicationBleeding Complication
* p<0.001 versus none † p<0.001 versus minor ‡ p<0.01 versus none § p<0.05 versus minor

► Bleeding is associated with adverse short- and long-term outcomes among patients with ACS and those undergoing PCI
Mortality rates are higher among those who bleed
MI rates are higher among those who bleed
► The risk is “loss-dependent” with worse bleeding associated with worse outcomes
► This relationship is persistent after robust statistical adjustment for confounders
► Bleeding is associated with adverse short- and long-term outcomes among patients with ACS and those undergoing PCI
Mortality rates are higher among those who bleed
MI rates are higher among those who bleed
► The risk is “loss-dependent” with worse bleeding associated with worse outcomes
► This relationship is persistent after robust statistical adjustment for confounders
Bleeding and Outcomes—Conclusions

How does one assess bleeding
severity?
How does one assess bleeding
severity?
Bleeding in ACS
Question to be answered:Question to be answered:

Bleeding Incidence in ACS Clinical TrialsBleeding Incidence in ACS Clinical Trials
0.4
10
1.2
4
1.5
3.7
9.1
0
2
4
6
8
10
12
GUSTO IIb OASIS-2 PRISM-PLUS PURSUIT PRISM CURE SYNERGY
%
Rao SV, et al. J Am Coll Cardiol. 2006 Feb 21;47(4):809-16. Epub 2006 Jan 26 Rao SV, et al. J Am Coll Cardiol. 2006 Feb 21;47(4):809-16. Epub 2006 Jan 26

Bleeding DefinitionsBleeding Definitions
► TIMI DefinitionTIMI Definition MajorMajor
• ICHICH• Associated with Hgb decrease ≥ 5 g/dl or Associated with Hgb decrease ≥ 5 g/dl or
HCT decrease ≥ 15%HCT decrease ≥ 15% MinorMinor
• Observed blood loss associated with Hgb Observed blood loss associated with Hgb decrease ≥ 3 g/dl or HCT decrease ≥ 10%decrease ≥ 3 g/dl or HCT decrease ≥ 10%
• No identifiable source but Hgb decrease No identifiable source but Hgb decrease ≥ 4 g/dl or HCT decrease ≥ 12%≥ 4 g/dl or HCT decrease ≥ 12%
MinimalMinimal• Overt hemorrhage with Hgb drop < 3 g/dl or Overt hemorrhage with Hgb drop < 3 g/dl or
HCT drop < 9%HCT drop < 9%
Chesebro JH. Chesebro JH. CirculationCirculation 1987. Jul;76(1):142-54. 1987. Jul;76(1):142-54. Chesebro JH. Chesebro JH. CirculationCirculation 1987. Jul;76(1):142-54. 1987. Jul;76(1):142-54.

N Engl J MedN Engl J Med. 1993 Nov 25;329(22):1615-22. Erratum in: . 1993 Nov 25;329(22):1615-22. Erratum in: N Engl J MedN Engl J Med 1994 Feb 17;330(7):516 1994 Feb 17;330(7):516 N Engl J MedN Engl J Med. 1993 Nov 25;329(22):1615-22. Erratum in: . 1993 Nov 25;329(22):1615-22. Erratum in: N Engl J MedN Engl J Med 1994 Feb 17;330(7):516 1994 Feb 17;330(7):516
Bleeding DefinitionsBleeding Definitions
► GUSTO DefinitionGUSTO Definition Severe or life threateningSevere or life threatening
• ICH or hemodynamic compromise ICH or hemodynamic compromise requiring treatmentrequiring treatment
ModerateModerate• Requiring transfusionRequiring transfusion
MildMild• Not meeting criteria for Severe or Not meeting criteria for Severe or
ModerateModerate

Bleeding Incidence Among 15,858 NSTEBleeding Incidence Among 15,858 NSTEACS Patients: Impact of DefinitionACS Patients: Impact of Definition
8.5 8.2
12.7
1.2
11.4
19.2
0
5
10
15
20
25
GUSTOMild
GUSTOMod
GUSTO Sev TIMI Mini TIMI Min TIMI Maj
%
Rao SV, et al. J Am Coll Cardiol. 2006 Feb 21;47(4):809-16. Epub 2006 Jan 26 Rao SV, et al. J Am Coll Cardiol. 2006 Feb 21;47(4):809-16. Epub 2006 Jan 26

Bleeding Scales Among Bleeding Scales Among NSTE ACS PatientsNSTE ACS Patients
Rao SV, et al. J Am Coll Cardiol. 2006 Feb 21;47(4):809-16. Epub 2006 Jan 26 Rao SV, et al. J Am Coll Cardiol. 2006 Feb 21;47(4):809-16. Epub 2006 Jan 26
TIMI and GUSTO – Adjusted Hazard of 30 d Death/MI N=15,858TIMI and GUSTO – Adjusted Hazard of 30 d Death/MI N=15,858TIMI and GUSTO – Adjusted Hazard of 30 d Death/MI N=15,858TIMI and GUSTO – Adjusted Hazard of 30 d Death/MI N=15,858

► Clearly defining bleeding severity can be difficult, but there are definitions that have been used in clinical trials and registries
► Not all of these definitions have been validated in terms of prognosis
► TIMI and GUSTO are 2 of the most commonly used definitions
► Bleeding definitions that include clinical events (e.g. GUSTO) are better at predicting outcomes
► Clearly defining bleeding severity can be difficult, but there are definitions that have been used in clinical trials and registries
► Not all of these definitions have been validated in terms of prognosis
► TIMI and GUSTO are 2 of the most commonly used definitions
► Bleeding definitions that include clinical events (e.g. GUSTO) are better at predicting outcomes
Bleeding Definitions—Conclusions

► Do blood transfusions have predictive
value?
► Do blood transfusions correct negative
impact of bleeding?
► Do blood transfusions have predictive
value?
► Do blood transfusions correct negative
impact of bleeding?
Bleeding in ACS
Questions to be answered:Questions to be answered:

30-Day Survival By Transfusion Group30-Day Survival By Transfusion Group
Rao SV, et. al., Rao SV, et. al., JAMAJAMA 2004;292:1555–1562 2004;292:1555–1562Rao SV, et. al., Rao SV, et. al., JAMAJAMA 2004;292:1555–1562 2004;292:1555–1562
Transfusion in ACSTransfusion in ACS
N=24,111N=24,111N=24,111N=24,111

*Transfusion as a time-dependent covariate*Transfusion as a time-dependent covariate
PRBC Transfusion Among NSTE ACS Patients:PRBC Transfusion Among NSTE ACS Patients:Cox Model for 30-day DeathCox Model for 30-day Death
Rao SV, et. al., Rao SV, et. al., JAMAJAMA 2004;292:1555–1562 2004;292:1555–1562Rao SV, et. al., Rao SV, et. al., JAMAJAMA 2004;292:1555–1562 2004;292:1555–1562
N=24,111N=24,111N=24,111N=24,111

Adjusted Risk of In-Hospital Outcomes Adjusted Risk of In-Hospital Outcomes
By Transfusion Status*By Transfusion Status*
*Non-CABG patients onlyYang X, Yang X, J Am Coll CardiolJ Am Coll Cardiol 2005;46:1490–5. 2005;46:1490–5.Yang X, Yang X, J Am Coll CardiolJ Am Coll Cardiol 2005;46:1490–5. 2005;46:1490–5.
N=74,271 ACS patients from CRUSADEN=74,271 ACS patients from CRUSADE

9.4%
2.3%
18.8%
11.0%
29.2%
4.8%7.1%
1.3%
IschemicComposite
Death MI (all) UnplannedRevasc
30 d
ay e
ven
ts (
%)
Transfusion (N=319, 2.3%) No Transfusion (N=13500, 97.7%)
Transfusion, Ischemic Endpoints, and Transfusion, Ischemic Endpoints, and MortalityMortality
9.4%
2.3%
18.8%
11.0%
29.2%
4.8%7.1%
1.3%
IschemicComposite
Death MI (all) UnplannedRevasc
30 d
ay e
ven
ts (
%)
Transfusion (N=319, 2.3%) No Transfusion (N=13500, 97.7%)
P<0.0001 for all
Manoukian SV, Voeltz MD, Feit F et al. TCT 2006.
Results: The ACUITY Trial (N=13,819)Results: The ACUITY Trial (N=13,819)Results: The ACUITY Trial (N=13,819)Results: The ACUITY Trial (N=13,819)

5.3%
13.8%
18.8%
0.9%
4.8% 3.8%
MI (all) Non-Q MI Q-MI
30 d
ay e
ven
ts (
%)
Transfusion (N=319, 2.3%) No Transfusion (N=13500, 97.7%)
Transfusion and Myocardial InfarctionTransfusion and Myocardial Infarction
5.3%
13.8%
18.8%
0.9%
4.8% 3.8%
MI (all) Non-Q MI Q-MI
30 d
ay e
ven
ts (
%)
Transfusion (N=319, 2.3%) No Transfusion (N=13500, 97.7%)
P<0.0001 for all
Manoukian SV, Voeltz MD, Feit F et al. TCT 2006.
Results: The ACUITY Trial (N=13,819)Results: The ACUITY Trial (N=13,819)Results: The ACUITY Trial (N=13,819)Results: The ACUITY Trial (N=13,819)

Increased 1-year mortality in transfused patientsIncreased 1-year mortality in transfused patientsAdjusted Odds Ratio 4.26 (2.25–8.08)Adjusted Odds Ratio 4.26 (2.25–8.08)
Transfusion Post PCI:Transfusion Post PCI:REPLACE 2 One Year MortalityREPLACE 2 One Year Mortality
1.9%
13.9%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
Non-Transfused Transfused
P<0.0001
Manoukian SV, Voeltz MD, Attubato MJ, Bittl JA, Feit F, Lincoff AM. CRT 2005. Abstract.

► Although there has never been a randomized trial of blood transfusion in patients with ACS, the available observational data consistently supports a relationship between blood transfusion and increased adverse outcomes, including death, MI, and unplanned revascularization
► Blood transfusion is best avoided in ACS patients whenever possible
► Although there has never been a randomized trial of blood transfusion in patients with ACS, the available observational data consistently supports a relationship between blood transfusion and increased adverse outcomes, including death, MI, and unplanned revascularization
► Blood transfusion is best avoided in ACS patients whenever possible
Blood Transfusion—Conclusions

Are there certain ACS subpopulations
at especially high risk for bleeding,
transfusion, and morbidity/mortality?
Are there certain ACS subpopulations
at especially high risk for bleeding,
transfusion, and morbidity/mortality?
Bleeding in ACS
Question to be answered:Question to be answered:

4.5
10.3
14.1
18.517.9
9.7
0
5
10
15
20
<65 yrs 65–75 yrs > 75 yrs
% R
BC
Tra
nsf
usi
on
Non-CABG Overall
Bleeding Risks—Transfusions by AgeBleeding Risks—Transfusions by Age
Alexander KA, Alexander KA, JAMAJAMA 2005;294:3108–16. 2005;294:3108–16. Alexander KA, Alexander KA, JAMAJAMA 2005;294:3108–16. 2005;294:3108–16.

6,002 patients in REPLACE-26,002 patients in REPLACE-2806 patients (13.4%) classified as elderly, >75 years of age806 patients (13.4%) classified as elderly, >75 years of age
p<0.0001 p=0.0001
2.7%
1.7%
5.0%
6.7%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
Major Bleeding Transfusions
REPLACE-2:REPLACE-2:Elderly Patients Have Increased Major Bleeding and Elderly Patients Have Increased Major Bleeding and
TransfusionsTransfusions
= Not Elderly, <75
= Elderly, >75
Voeltz MD, Lincoff AM, Feit F, Manoukian SV. Circulation 2005;112(17):II-613. Abstract.

0.5%0.4%
13.0%
15.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
Major Bleeding Transfusions
30
-Da
y M
ort
ali
ty
No
Yes
p<0.0001 p=0.0001
6,002 patients in REPLACE-2.6,002 patients in REPLACE-2. 806 patients (13.4%) classified as elderly, >75 years of age.806 patients (13.4%) classified as elderly, >75 years of age.
Elderly Patients in REPLACE-2:Elderly Patients in REPLACE-2:Increased 30-Day Mortality With Major Bleeding and TransfusionsIncreased 30-Day Mortality With Major Bleeding and Transfusions
Voeltz MD, Lincoff AM, Feit F, Manoukian SV. Circulation 2005;112(17):II-613. Abstract.

Excessive Dosing ofExcessive Dosing ofAnticoagulants by AgeAnticoagulants by Age
Alexander KA, Alexander KA, JAMAJAMA 2005;294:3108–16. 2005;294:3108–16. Alexander KA, Alexander KA, JAMAJAMA 2005;294:3108–16. 2005;294:3108–16.
12.5
28.7
8.5
33.137
12.5
64.5
38.5
16.5
0
10
20
30
40
50
60
70
LMW Heparin UF Heparin GP Iib/IIIa
% R
BC
Tra
nsf
usi
on
<65 yrs 65Š75 yrs >75 yrs

RBC Transfusions by Excess DosingRBC Transfusions by Excess Dosing
8
6.7
4.4
13.3
8.8
10.4
0
3
6
9
12
15
UF Heparin LMWH GP llb-llla
% R
BC
Tra
nsf
usi
on
Recommended Excess
Alexander KA, Alexander KA, JAMAJAMA 2005;294:3108–16. 2005;294:3108–16. Alexander KA, Alexander KA, JAMAJAMA 2005;294:3108–16. 2005;294:3108–16.

Cumulative Effects of Dosing Errors: Cumulative Effects of Dosing Errors: Combined Use of Heparin and GP IIb-IIIaCombined Use of Heparin and GP IIb-IIIa
4.1
9
18.5
0
5
10
15
20
Both Right 1 Excessive Both Excessive
% R
BC
Tra
nsf
usi
on
Alexander KA, Alexander KA, JAMAJAMA 2005;294:3108–16. 2005;294:3108–16. Alexander KA, Alexander KA, JAMAJAMA 2005;294:3108–16. 2005;294:3108–16.

Excess Dosing of Gp IIb/IIIa Excess Dosing of Gp IIb/IIIa and Bleeding in Womenand Bleeding in Women
OverallOverallOverallOverall
WomenWomenWomenWomen
MenMenMenMen
1.46 (1.22, 1.73)1.46 (1.22, 1.73)1.46 (1.22, 1.73)1.46 (1.22, 1.73)
1.72 (1.30, 2.28)1.72 (1.30, 2.28)1.72 (1.30, 2.28)1.72 (1.30, 2.28)
1.27 (0.97, 1.66)1.27 (0.97, 1.66)1.27 (0.97, 1.66)1.27 (0.97, 1.66)
0.50.50.50.5 1.01.01.01.0 1.51.51.51.5 2.02.02.02.0 2.52.52.52.5
Excess Dosing More Likely to BleedExcess Dosing More Likely to BleedExcess Dosing More Likely to BleedExcess Dosing More Likely to Bleed
Alexander KP, et. al. Circulation 2006Alexander KP, et. al. Circulation 2006
N=32,601 patients from CRUSADEN=32,601 patients from CRUSADEN=32,601 patients from CRUSADEN=32,601 patients from CRUSADE

Bleeding is Increased in Patients With Bleeding is Increased in Patients With Impaired Renal Function Undergoing PCIImpaired Renal Function Undergoing PCI
≥≥ 60 ml/min60 ml/min N=4824 N=4824
< 60 ml/min< 60 ml/min N=886 N=886 p valuep value
30-d Death30-d Death 5 (0.1%)5 (0.1%) 14 (1.6%)14 (1.6%) < 0.001< 0.001
30-d Myocardial infarction30-d Myocardial infarction 305 (6.3%)305 (6.3%) 75 (8.5%)75 (8.5%) 0.0180.018
30-d urgent revascularization30-d urgent revascularization 61 (1.3%)61 (1.3%) 10 (1.1%)10 (1.1%) 0.7380.738
Triple ischemic endpointTriple ischemic endpoint 338 (7.0%)338 (7.0%) 84 (9.5%)84 (9.5%) 0.0100.010
In-hospital protocol major In-hospital protocol major bleedingbleeding 123 (2.5%)123 (2.5%) 54 (6.1%)54 (6.1%) < 0.001< 0.001
TIMI major + minor bleedingTIMI major + minor bleeding 114 (2.4%)114 (2.4%) 46 (5.2%)46 (5.2%) < 0.001< 0.001
Creatinine ClearanceCreatinine Clearance
Chew DP et al. Am J Cardiol 2005;95:581–585.

Anemia Identifies High-RiskAnemia Identifies High-RiskThe Unrecognized Risk FactorThe Unrecognized Risk Factor
► OlderOlder
► FemaleFemale
► Lower BMILower BMI
► Fewer CaucasiansFewer Caucasians
► Lower Hemoglobin (11.7 vs. 14.3 g/dL)Lower Hemoglobin (11.7 vs. 14.3 g/dL)
► Lower Hematocrit (34.6 vs. 41.8%)Lower Hematocrit (34.6 vs. 41.8%)
► Less Tobacco useLess Tobacco use
► More Diabetes MellitusMore Diabetes Mellitus
► More history of CHF, MI, PCI, CABGMore history of CHF, MI, PCI, CABG
REPLACE-2 Anemic Patient Baseline Characteristics:REPLACE-2 Anemic Patient Baseline Characteristics:(Anemia in 22.7%)(Anemia in 22.7%)
Voeltz MD, Attubato MJ, Feit F, Lincoff AM, Manoukian SV. J Am Coll Cardiol 2005;45(3)[Suppl A]:1037-Voeltz MD, Attubato MJ, Feit F, Lincoff AM, Manoukian SV. J Am Coll Cardiol 2005;45(3)[Suppl A]:1037-13-31A. Abstract.13-31A. Abstract.

Major Bleeding is IncreasedMajor Bleeding is Increasedin Anemic Patients Undergoing PCIin Anemic Patients Undergoing PCI
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
Non-Anemic Anemic
6,010 patients in REPLACE-2.1,362 patients (22.7%) classified as anemic based upon WHO definition.
Major bleeding = 3.2%
Major Bleeding
2.8%
4.9%
P=0.0001
Protocol definition: >3g/dL drop in HgB,
intracranial, retroperitoneal,
2U transfusion
Voeltz MD, Attubato MJ, Feit F, Lincoff AM, Manoukian SV. J Am Coll Cardiol 2005;45(3)[Suppl Voeltz MD, Attubato MJ, Feit F, Lincoff AM, Manoukian SV. J Am Coll Cardiol 2005;45(3)[Suppl A]:1037-13-31A. Abstract.A]:1037-13-31A. Abstract.

NSTE-ACS MortalityNSTE-ACS MortalityStratified by HemoglobinStratified by Hemoglobin
Sabatine MS. Circulation 2005
UnadjustedUnadjusted
Hb (g/dL)Hb (g/dL) nn OROR (95% Cl)(95% Cl) OROR (95% Cl)(95% Cl) P P valuevalue
>17>17 216 216 1.471.47 (1.03–2.10)(1.03–2.10) 1.451.45 (0.94–2.23)(0.94–2.23) 0.0930.093
16–1716–17 812 812 1.211.21 (0.97–1.51)(0.97–1.51) 1.271.27 (0.98–1.65)(0.98–1.65) 0.0660.066
15–1615–16 21302130 1.0 1.0 referencereference 1.0 1.0 referencereference
14–1514–15 33903390 1.061.06 (0.89–1.22)(0.89–1.22) 1.111.11 (0.93–1.33)(0.93–1.33) 0.2510.251
13–1413–14 35203520 1.021.02 (0.88–1.19)(0.88–1.19) 1.041.04 (0.86–1.24)(0.86–1.24) 0.7090.709
12–1312–13 23312331 1.091.09 (0.92–1.28)(0.92–1.28) 1.071.07 (0.88–1.30)(0.88–1.30) 0.5140.514
11–1211–12 976 976 1.201.20 (0.97–1.47)(0.97–1.47) 1.041.04 (0.81–1.34)(0.81–1.34) 0.7550.755
10–1110–11 343 343 1.411.41 (1.05–1.89)(1.05–1.89) 1.291.29 (0.92–1.82)(0.92–1.82) 0.1450.145
9–109–10 342 342 2.442.44 (1.88–3.18)(1.88–3.18) 2.692.69 (2.01–3.60)(2.01–3.60) <0.001<0.001
8–98–9 306 306 2.242.24 (1.69–2.96)(1.69–2.96) 2.452.45 (1.80–3.33)(1.80–3.33) <0.001<0.001
<8<8 137 137 3.973.97 (2.76–5.70)(2.76–5.70) 3.493.49 (2.35–5.20)(2.35–5.20) <0.001<0.001
Abbreviations: CI, confidence interval; Hb, hemoglobin; OR, odds ration. Adapted with permission.Abbreviations: CI, confidence interval; Hb, hemoglobin; OR, odds ration. Adapted with permission.
Unadjusted and adjusted odds ratios for cardiovascular mortality in patientsUnadjusted and adjusted odds ratios for cardiovascular mortality in patientswith non-ST elevation acute coronary syndromes at 30 days stratefied by hemoglobinwith non-ST elevation acute coronary syndromes at 30 days stratefied by hemoglobin
Adjusted for baseline characteristicsAdjusted for baseline characteristics

► Certain ACS patient populations are at especially high risk for bleeding and mortality
Elderly, females, CKD, anemia
► Improper dosing of anticoagulants is a common error and is associated with bleeding risk in the elderly, females, and those with CKD
► Anemia places patients at risk for both bleeding and mortality
► Certain ACS patient populations are at especially high risk for bleeding and mortality
Elderly, females, CKD, anemia
► Improper dosing of anticoagulants is a common error and is associated with bleeding risk in the elderly, females, and those with CKD
► Anemia places patients at risk for both bleeding and mortality
High-Risk Populations—Conclusions

Does bleeding influence the cost of
care for patients with ischemic heart
disease?
Does bleeding influence the cost of
care for patients with ischemic heart
disease?
Bleeding in ACS
Question to be answered:Question to be answered:

8800
27349
1300
5900
0
10000
20000
30000
$$$
Urgent PCI UrgentCABG
Minor bleed Major bleed
Costs Abciximab versus Placebo
ischemic costs: $523
major bleed costs: $458
Abciximab versus Placebo
ischemic costs: $523
major bleed costs: $458
Mark DB, et al. Mark DB, et al. CirculationCirculation. 2000 Feb 1;101(4):366-71 . 2000 Feb 1;101(4):366-71 Mark DB, et al. Mark DB, et al. CirculationCirculation. 2000 Feb 1;101(4):366-71 . 2000 Feb 1;101(4):366-71
Calculating Costs of Ischemia and Bleeding:Calculating Costs of Ischemia and Bleeding:EPIC EQOL Study (Abciximab in PCI)EPIC EQOL Study (Abciximab in PCI)

► The available costs data confirms that a balance must be struck between ischemia reduction and bleeding.
► Both ischemic complications and bleeding are associated with increased costs.
► The available costs data confirms that a balance must be struck between ischemia reduction and bleeding.
► Both ischemic complications and bleeding are associated with increased costs.
Bleeding and Costs—Conclusions

Bleeding Among Patients with ACSBleeding Among Patients with ACSConclusionsConclusions
► Antithrombotic therapies are cornerstone RxAntithrombotic therapies are cornerstone Rx Must balance thrombosis and hemostasisMust balance thrombosis and hemostasis
► Certain patient and PCI procedure Certain patient and PCI procedure characteristics predict bleedingcharacteristics predict bleeding Age, female gender, CKD, procedure time, Age, female gender, CKD, procedure time,
sheath dwell timesheath dwell time
► Diabetes and anemia are newly identified risk Diabetes and anemia are newly identified risk factors for bleeding among ACS patientsfactors for bleeding among ACS patients

Conclusions—Bleeding Conclusions—Bleeding
►Bleeding is associated with worse short and Bleeding is associated with worse short and long-term outcomes including death and MIlong-term outcomes including death and MI
►Assessing bleeding severity is important Assessing bleeding severity is important
► Many definitions have been usedMany definitions have been used
► Definitions that include clinical events Definitions that include clinical events appear to be more useful than those that appear to be more useful than those that include only laboratory parametersinclude only laboratory parameters
►Blood transfusion is associated with increased Blood transfusion is associated with increased mortality in ACS patients mortality in ACS patients
►Bleeding is associated with worse short and Bleeding is associated with worse short and long-term outcomes including death and MIlong-term outcomes including death and MI
►Assessing bleeding severity is important Assessing bleeding severity is important
► Many definitions have been usedMany definitions have been used
► Definitions that include clinical events Definitions that include clinical events appear to be more useful than those that appear to be more useful than those that include only laboratory parametersinclude only laboratory parameters
►Blood transfusion is associated with increased Blood transfusion is associated with increased mortality in ACS patients mortality in ACS patients

Conclusions—Bleeding Conclusions—Bleeding
► In addition to clinical outcomes, bleeding is In addition to clinical outcomes, bleeding is associated with increased cost of careassociated with increased cost of care
► Bleeding costs can offset the savings Bleeding costs can offset the savings realized by reduced ischemic realized by reduced ischemic complicationscomplications
►Given the body of evidence related to bleeding Given the body of evidence related to bleeding and transfusion, therapies that can reduce and transfusion, therapies that can reduce ischemia while minimizing the risk for bleeding ischemia while minimizing the risk for bleeding have the potential to further improve outcomes have the potential to further improve outcomes among patients with ACSamong patients with ACS
► In addition to clinical outcomes, bleeding is In addition to clinical outcomes, bleeding is associated with increased cost of careassociated with increased cost of care
► Bleeding costs can offset the savings Bleeding costs can offset the savings realized by reduced ischemic realized by reduced ischemic complicationscomplications
►Given the body of evidence related to bleeding Given the body of evidence related to bleeding and transfusion, therapies that can reduce and transfusion, therapies that can reduce ischemia while minimizing the risk for bleeding ischemia while minimizing the risk for bleeding have the potential to further improve outcomes have the potential to further improve outcomes among patients with ACSamong patients with ACS

Non-ST-Segment ElevationNon-ST-Segment ElevationAcute Coronary Syndrome:Acute Coronary Syndrome:
Initial Presentation and Implications for Selecting Initial Presentation and Implications for Selecting Treatment StrategiesTreatment Strategies
Does One Size Fit All?Does One Size Fit All?
The Emergency Medicine PerspectiveThe Emergency Medicine Perspective
Charles V. Pollack, MD, FACEP, FAAEMCharles V. Pollack, MD, FACEP, FAAEMChairman, Department of Emergency MedicineChairman, Department of Emergency Medicine
Pennsylvania HospitalPennsylvania HospitalProfessor of Emergency Medicine Professor of Emergency Medicine
University of Pennsylvania School of Medicine University of Pennsylvania School of Medicine Philadelphia, PAPhiladelphia, PA
Charles V. Pollack, MD, FACEP, FAAEMCharles V. Pollack, MD, FACEP, FAAEMChairman, Department of Emergency MedicineChairman, Department of Emergency Medicine
Pennsylvania HospitalPennsylvania HospitalProfessor of Emergency Medicine Professor of Emergency Medicine
University of Pennsylvania School of Medicine University of Pennsylvania School of Medicine Philadelphia, PAPhiladelphia, PA

Changing the Calculations for Changing the Calculations for Assessing Guidelines AdherenceAssessing Guidelines Adherence
Anderson HV, Bach RG, J Am Coll Cardiol 2005;46:1488-9. Anderson HV, Bach RG, J Am Coll Cardiol 2005;46:1488-9.
““We need to invert the current equation to We need to invert the current equation to
calculate an opportunity score for ACS patients calculate an opportunity score for ACS patients
rather than a risk score. Patients with higher rather than a risk score. Patients with higher
baseline risks, such as the elderly, would have baseline risks, such as the elderly, would have
higher opportunity scores for benefit, even higher opportunity scores for benefit, even
allowing for some of the greater risks from the allowing for some of the greater risks from the
treatment.”treatment.”

The Challenge: The Challenge: Balancing Efficacy and SafetyBalancing Efficacy and Safety
► CCurrent guidelines (2002) emphasize reduction urrent guidelines (2002) emphasize reduction of ischemic risk in NSTE ACS—especially for of ischemic risk in NSTE ACS—especially for upstream therapy initiated in the EDupstream therapy initiated in the ED
► Updated guidelines (2007) are expected to Updated guidelines (2007) are expected to include data on the harm that bleeding events include data on the harm that bleeding events cause, diminishing ischemic efficacy in some cause, diminishing ischemic efficacy in some patientspatients
► Emergency physicians are comfortable with Emergency physicians are comfortable with the goal of reducing ischemic risk . . . and the goal of reducing ischemic risk . . . and traditionally have left concern over bleeding to traditionally have left concern over bleeding to “downstream providers”“downstream providers”

The Challenge: The Challenge: Balancing Efficacy and SafetyBalancing Efficacy and Safety
► Emergency physicians are accustomed to Emergency physicians are accustomed to assessing ischemic risk . . . but have little assessing ischemic risk . . . but have little data to guide them in assessing “bleeding data to guide them in assessing “bleeding risk”—a task not previously considered to risk”—a task not previously considered to be in their domainbe in their domain
► More than ever, “balanced” More than ever, “balanced” pharmacotherapy will require pharmacotherapy will require multidisciplinary collaboration, pathways, multidisciplinary collaboration, pathways, anticipation of consistent care (especially anticipation of consistent care (especially time from ED to cath), and individualized time from ED to cath), and individualized patient assessmentpatient assessment

Ischemic Risk StratificationIschemic Risk Stratification
► Three levels of risk strat are pertinent to the Three levels of risk strat are pertinent to the ED:ED:
lowlow, , intermediate, or highintermediate, or high risk that ischemic risk that ischemic symptoms are a result of CADsymptoms are a result of CAD
low, intermediatelow, intermediate, or , or high riskhigh risk of short-term of short-term death or nonfatal MI from ACSdeath or nonfatal MI from ACS
dynamic, ongoing risk-oriented evaluation of dynamic, ongoing risk-oriented evaluation of low- or intermediate-risk patients for low- or intermediate-risk patients for “conversion” to high-risk status “conversion” to high-risk status that is linked that is linked to intensity of treatmentto intensity of treatment

Ischemic Risk Stratification ToolsIschemic Risk Stratification Tools
History and PhysicalHistory and Physical Standard EKG and Non-standard EKG leadsStandard EKG and Non-standard EKG leads
15-lead ECGs should perhaps be 15-lead ECGs should perhaps be “standard” in all but very-low-risk patients“standard” in all but very-low-risk patients
MarkersMarkers CPK-MB, Troponins I and T, MyoglobinCPK-MB, Troponins I and T, Myoglobin Markers of ischemia and inflammation?Markers of ischemia and inflammation?
Non-Invasive ImagingNon-Invasive Imaging EchocardiogramEchocardiogram Stress testingStress testing Technetium-99m-sestamibi Technetium-99m-sestamibi
Predictive Indices/SchemesPredictive Indices/Schemes better as research tools than for real-time better as research tools than for real-time
clinical decisionmakingclinical decisionmaking

Guidelines Call for Therapeutic Response to Guidelines Call for Therapeutic Response to Identification of Ischemic RiskIdentification of Ischemic Risk
Anti-ischemic therapyAnti-ischemic therapy Oxygen, nitroglycerin, beta-blockers, Oxygen, nitroglycerin, beta-blockers,
morphinemorphine
Anti-thrombotic therapyAnti-thrombotic therapy ASA, anticoagulantASA, anticoagulant
Anti-platelet therapyAnti-platelet therapy Anti-activation therapy with clopidogrel, anti-Anti-activation therapy with clopidogrel, anti-
aggregation therapy with a GP IIb/IIIa receptor aggregation therapy with a GP IIb/IIIa receptor antagonistantagonist
lowrisklowriskmod
riskmodrisk
highriskhighrisk

Selection of Therapy in the ED is Traditionally Selection of Therapy in the ED is Traditionally Based on Reducing Ischemic RiskBased on Reducing Ischemic Risk
► Escalation of therapy for ischemia in this setting is Escalation of therapy for ischemia in this setting is associated with increased risk of bleedingassociated with increased risk of bleeding
► This “price to be paid” has generally been accepted This “price to be paid” has generally been accepted and tolerated, especially in patients at high ischemic and tolerated, especially in patients at high ischemic risk, who benefit disproportionately from advanced risk, who benefit disproportionately from advanced therapytherapy Enox superior to UFH in patients with higher TIMI Risk Enox superior to UFH in patients with higher TIMI Risk
ScoresScores Clopidogrel + ASA superior to ASA alone in patients with Clopidogrel + ASA superior to ASA alone in patients with
higher TIMI Risk Scoreshigher TIMI Risk Scores GP IIb/IIIa receptor antagonists benefit troponin positive GP IIb/IIIa receptor antagonists benefit troponin positive
patients more than troponin negative patientspatients more than troponin negative patients

Selection of Therapy in the ED Should Selection of Therapy in the ED Should Include Consideration of Bleeding RiskInclude Consideration of Bleeding Risk
► Just as in the Cath Lab and the CCU, we must Just as in the Cath Lab and the CCU, we must also be attentive to the impact of bleeding riskalso be attentive to the impact of bleeding risk
► In the ED, bleeding risk is impacted byIn the ED, bleeding risk is impacted by Choice of therapyChoice of therapy Dosing Dosing Duration and reversibility of therapy and Duration and reversibility of therapy and
impact on selection of downstream therapyimpact on selection of downstream therapy

Selection of Therapy in the ED Must Selection of Therapy in the ED Must Include Consideration of Bleeding RiskInclude Consideration of Bleeding Risk
► AgeAge
► GenderGender
► Renal insufficiencyRenal insufficiency
► Baseline anemiaBaseline anemia
► Expectation of prolonged medical therapyExpectation of prolonged medical therapy

How Do We Balance? One Guy’s Opinion of How Do We Balance? One Guy’s Opinion of Choices for Upstream TherapyChoices for Upstream Therapy
► Pertinent data since 2002 ACC/AHA Guidelines:Pertinent data since 2002 ACC/AHA Guidelines: INTERACTINTERACT SYNERGYSYNERGY OASIS-5OASIS-5 ISAR-REACT-2ISAR-REACT-2 REPLACE-2REPLACE-2 ACUITYACUITY CRUSADE and NRMI dataCRUSADE and NRMI data

How Do We Balance? One Guy’s Opinion of How Do We Balance? One Guy’s Opinion of Choices for Upstream Therapy: AntithromboticsChoices for Upstream Therapy: Antithrombotics
OptionOption PatientPatient Ease of UseEase of Use Ischemic Ischemic EfficacyEfficacy
Reduction of Reduction of Bleeding RiskBleeding Risk
UFHUFH Low riskLow risk not indicatednot indicated
Mod riskMod risk BB BB BB
High riskHigh risk BB BB BB
EnoxEnox Low riskLow risk not indicatednot indicated
Mod riskMod risk AA B*B* CC
High riskHigh risk AA B*B* CC
Bival (not yet Bival (not yet approved in approved in
ED)ED)
Low riskLow risk not indicated upstreamnot indicated upstream
Mod riskMod risk B-B- BB AA
High riskHigh risk B-**B-** B to C+B to C+ AA
* If medical management only, enox is ++++** ease of use higher if no IIb/IIIa is used* If medical management only, enox is ++++** ease of use higher if no IIb/IIIa is used

How Do We Balance? One Guy’s Opinion of How Do We Balance? One Guy’s Opinion of Choices for Upstream Therapy: AntiplateletsChoices for Upstream Therapy: Antiplatelets
OptionOption PatientPatient Ease of UseEase of Use Ischemic Ischemic EfficacyEfficacy
Reduction of Reduction of Bleeding RiskBleeding Risk
ASAASA Low riskLow risk AA AA BB
Mod riskMod risk AA AA BB
High riskHigh risk AA AA BB
clopidogrelclopidogrel Low riskLow risk not indicatednot indicated
Mod riskMod risk AA BB BB
High riskHigh risk AA AA B-C*B-C*
GP IIb/IIIaGP IIb/IIIa Low riskLow risk not indicatednot indicated
Mod riskMod risk not indicatednot indicated
High riskHigh risk BB AA B-B-
* CABG concern* CABG concern

► Braunwald E, Antman EM, Beasley JW, et al: ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients with Unstable Angina). J Am Coll Cardiol 2000;36:970-1062 (2002 update at www.acc.org; summary in Circulation 2002;106:1893-1900)
► Pollack CV, Roe MT, Peterson ED: 2002 Update to the Pollack CV, Roe MT, Peterson ED: 2002 Update to the ACC/AHA guidelines for the management of patients with ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation unstable angina and non-ST-segment elevation myocardial infarction: Implications for emergency myocardial infarction: Implications for emergency department practice. department practice. Ann Emerg MedAnn Emerg Med 2003;41:355-69. 2003;41:355-69.
ACC/AHA Guidelines for TherapyACC/AHA Guidelines for Therapy

Hospital CareHospital CareAnti-Thrombotic TherapyAnti-Thrombotic Therapy
Immediate aspirinImmediate aspirin
Clopidogrel, if aspirin contraindicatedClopidogrel, if aspirin contraindicated
Heparin (IV unfractionated, LMW) with Heparin (IV unfractionated, LMW) with antiplatelet agents listed aboveantiplatelet agents listed above
Enoxaparin preferred over UFH unless Enoxaparin preferred over UFH unless CABG is planned within 24 hoursCABG is planned within 24 hours
Immediate aspirinImmediate aspirin
Clopidogrel, if aspirin contraindicatedClopidogrel, if aspirin contraindicated
Heparin (IV unfractionated, LMW) with Heparin (IV unfractionated, LMW) with antiplatelet agents listed aboveantiplatelet agents listed above
Enoxaparin preferred over UFH unless Enoxaparin preferred over UFH unless CABG is planned within 24 hoursCABG is planned within 24 hours
IIII IIaIIaIIaIIa IIbIIbIIbIIb IIIIIIIIIIII

Hospital CareHospital CarePlatelet GP IIb/IIIa InhibitorsPlatelet GP IIb/IIIa Inhibitors
Any GP IIb/IIIa inhibitor + ASA/Heparin Any GP IIb/IIIa inhibitor + ASA/Heparin for all patients, if cath/PCI plannedfor all patients, if cath/PCI planned
Eptifibatide or tirofiban + ASA/Heparin Eptifibatide or tirofiban + ASA/Heparin for high-risk* patients in whom early for high-risk* patients in whom early cath/PCI is not plannedcath/PCI is not planned
Any GP IIb/IIIa inhibitor for patients Any GP IIb/IIIa inhibitor for patients already on ASA + Heparin + clopidogrel, already on ASA + Heparin + clopidogrel, if cath/PCI is plannedif cath/PCI is planned
Any GP IIb/IIIa inhibitor + ASA/Heparin Any GP IIb/IIIa inhibitor + ASA/Heparin for all patients, if cath/PCI plannedfor all patients, if cath/PCI planned
Eptifibatide or tirofiban + ASA/Heparin Eptifibatide or tirofiban + ASA/Heparin for high-risk* patients in whom early for high-risk* patients in whom early cath/PCI is not plannedcath/PCI is not planned
Any GP IIb/IIIa inhibitor for patients Any GP IIb/IIIa inhibitor for patients already on ASA + Heparin + clopidogrel, already on ASA + Heparin + clopidogrel, if cath/PCI is plannedif cath/PCI is planned
II IIaIIa IIbIIb IIIIII
* High-risk: Age > 75; prolonged, ongoing CP; hemodynamic instability; rest CP w/ ST ; VT; positive cardiac markers * High-risk: Age > 75; prolonged, ongoing CP; hemodynamic instability; rest CP w/ ST ; VT; positive cardiac markers

Hospital CareHospital CarePlatelet GP IIb/IIIa InhibitorsPlatelet GP IIb/IIIa Inhibitors
Eptifibatide or tirofiban + ASA/Heparin Eptifibatide or tirofiban + ASA/Heparin for patients without continuing for patients without continuing ischemia in whom PCI is not planned ischemia in whom PCI is not planned
Abciximab for patients in whom PCI is Abciximab for patients in whom PCI is not plannednot planned
Eptifibatide or tirofiban + ASA/Heparin Eptifibatide or tirofiban + ASA/Heparin for patients without continuing for patients without continuing ischemia in whom PCI is not planned ischemia in whom PCI is not planned
Abciximab for patients in whom PCI is Abciximab for patients in whom PCI is not plannednot planned
II IIaIIa IIbIIb IIIIII

0 1 2
ACUITY—Primary Endpoint Measures (ITT)ACUITY—Primary Endpoint Measures (ITT)ACUITY—Primary Endpoint Measures (ITT)ACUITY—Primary Endpoint Measures (ITT)
Bivalirudin alone betterBivalirudin alone betterBivalirudin alone betterBivalirudin alone better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa better
Risk ratioRisk ratio±95% CI±95% CI
Risk ratioRisk ratio±95% CI±95% CI
PrimaryPrimaryendpointendpoint
BivalBivalalonealone
UFH/EnoxUFH/Enox+ IIb/IIIa+ IIb/IIIa
RR (95% CI)RR (95% CI)
Net clinical Net clinical outcomeoutcome
Ischemic Ischemic compositecomposite
Major bleedingMajor bleeding
Upp
er b
oun
dary
non
-infe
riorit
y11.7%11.7%10.1%10.1% 0.86 (0.77-0.97)0.86 (0.77-0.97) <0.001<0.001
0.0150.015
7.3%7.3%7.8%7.8% 1.08 (0.93-1.24)1.08 (0.93-1.24)0.020.020.320.32
5.7%5.7%3.0%3.0% 0.53 (0.43-0.65)0.53 (0.43-0.65) <0.001<0.001<0.001<0.001
p valuep value(non inferior)(non inferior)
(superior)(superior)
UFH/Enoxaparin + GPI vs. Bivalirudin AloneUFH/Enoxaparin + GPI vs. Bivalirudin Alone
Stone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16. Stone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16.

0 1 2
ACUITY—Net Clinical Outcome CompositeACUITY—Net Clinical Outcome Composite
UFH/Enoxaparin + IIb/IIIa vs. Bivalirudin AloneUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone
Men (n=6444)Women (n=2771)
Diabetes (n=2585)No diabetes (n=6630)
CrCl ≥60 (n=6993)CrCl <60 (n=1644)
Age <65 (n=5051)Age ≥65 (n=4164)
Risk ratio±95% CI
Risk ratio±95% CI
BivalAlone
UFH/Enox+ IIb/IIIa
7.8%12.9%
US (n=5224)OUS (n=3991)
10.6%9.5%
8.9%16.1%
10.8%9.8%
9.5%11.6%
9.2%14.7%
11.8%11.5%
10.4%16.8%
13.7%10.9%
10.9%13.5%
P Pint
0.86 (0.71-1.03)0.88 (0.75-1.02)
0.90 (0.77-1.05)0.82 (0.68-0.98)
0.86 (0.74-0.99)0.96 (0.77-1.19)
0.79 (0.64-0.97)0.90 (0.78-1.04)
0.87 (0.75-1.00)0.86 (0.70-1.04)
0.090.09
0.160.03
0.030.71
0.020.16
0.050.12
0.89
0.47
0.43
0.28
0.91
RR (95% CI)
Bivalirudin alone betterBivalirudin alone better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa betterStone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16. Stone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16.

0 1 2
UFH/Enoxaparin + IIb/IIIa vs. Bivalirudin AloneUFH/Enoxaparin + IIb/IIIa vs. Bivalirudin Alone
Yes (n=3197)No (n=6008)
Low (0-2) (n=1291)Intermed (3-4) (n=4407)
High (5-7) (n=2449)
Elevated (n=5368)Normal (n=3841)
Risk ratio±95% CI
Risk ratio±95% CI
BivalAlone
UFH/Enox+ IIb/IIIa
9.2%11.3%
12.2%11.1%
P Pint
0.76 (0.65-0.89)1.02 (0.86-1.21)
12.2%7.1%
13.3%9.4%
0.92 (0.80-1.06)0.75 (0.61-0.93)
0.230.01
<0.0010.83
0.35
0.02
0.18
13.0%8.6%
13.7%10.6%
0.96 (0.80-1.14)0.81 (0.69-0.95)
0.610.01 0.42
Biomarkers (CK/Trop)
ST Deviation
TIMI Risk Score
Pre Thienopyridine
6.4% 10.2% 0.63 (0.43-0.91) 0.019.4% 10.2% 0.92 (0.77-1.10) 0.34
13.9% 15.2% 0.92 (0.76-1.11) 0.36
Yes (n=5192)No (n=4023)
RR (95% CI)
Bivalirudin alone betterBivalirudin alone better UFH/Enox + IIb/IIIa betterUFH/Enox + IIb/IIIa betterStone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16. Stone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16.
ACUITY—Net Clinical Outcome CompositeACUITY—Net Clinical Outcome Composite

Hospital CareHospital CareClopidogrel TherapyClopidogrel Therapy
Aspirin + clopidogrel, for up to 1 month*Aspirin + clopidogrel, for up to 1 month*
Aspirin + clopidogrel, for up to 9 months*Aspirin + clopidogrel, for up to 9 months*
Withhold clopidogrel for 5-7 days for CABGWithhold clopidogrel for 5-7 days for CABG
Aspirin + clopidogrel, for up to 1 month*Aspirin + clopidogrel, for up to 1 month*
Aspirin + clopidogrel, for up to 9 months*Aspirin + clopidogrel, for up to 9 months*
Withhold clopidogrel for 5-7 days for CABGWithhold clopidogrel for 5-7 days for CABG
IIII IIaIIaIIaIIa IIbIIbIIbIIb IIIIIIIIIIII
* For patients managed with an early conservative strategy, and * For patients managed with an early conservative strategy, and those who are planned to undergo early PCIthose who are planned to undergo early PCI* For patients managed with an early conservative strategy, and * For patients managed with an early conservative strategy, and those who are planned to undergo early PCIthose who are planned to undergo early PCI
Guidelines do not specify initial timing of using Guidelines do not specify initial timing of using clopidogrel when coronary anatomy is unknownclopidogrel when coronary anatomy is unknown

CURE: Ischemic Endpoints Were Reduced CURE: Ischemic Endpoints Were Reduced within 24h of Randomizationwithin 24h of Randomization
Adapted from Adapted from Yusuf S, et al. Yusuf S, et al. Circulation.Circulation. 2003;107:966-972. 2003;107:966-972.
Hours After RandomizationHours After Randomization
Cu
mu
lati
ve H
azar
d R
ates
Cu
mu
lati
ve H
azar
d R
ates
0.00.0
0.0050.005
0.0100.010
0.0150.015
0.0200.020
0.0250.025
00 22 44 66 88 1010 1212 1414 1616 1818 2020 2222 2424
RR = 0.67RR = 0.67P P = 0.003= 0.003
PlaceboPlacebo+ ASA+ ASA
ClopidogrelClopidogrel+ ASA+ ASA
33%33%RRRRRR

Bleeding Among CABG Patients Receiving ClopidogrelBleeding Among CABG Patients Receiving ClopidogrelExcludes transfers out within 48 hours and contraindicationsExcludes transfers out within 48 hours and contraindications
95% CI Odds Ratio
1.0 2.00.5Clopidogrel WorseClopidogrel Better
Clopidogrel>5 days 1.30 (0.95, 1.78)
Risk-adjusted AnalysesRisk-adjusted Analyses
ClopidogrelWithin 5 days 1.33 (1.12, 1.58)
unpublished CRUSADE data, www.crusadeqi.comunpublished CRUSADE data, www.crusadeqi.com

Factors that Should Influence Choice of Factors that Should Influence Choice of Upstream Therapy for NSTE ACSUpstream Therapy for NSTE ACS
► AgeAge Older patients more likely to have ischemic Older patients more likely to have ischemic
eventsevents Older patients more likely to have bleeding Older patients more likely to have bleeding
eventsevents
► GenderGender Women more likely to present late and atypicallyWomen more likely to present late and atypically Women more likely to have bleeding eventsWomen more likely to have bleeding events
► DiabetesDiabetes Diabetics more likely to present atypically and Diabetics more likely to present atypically and
have ischemic eventshave ischemic events

Factors that Should Influence Choice of Factors that Should Influence Choice of Upstream Therapy for NSTE ACSUpstream Therapy for NSTE ACS
► Renal statusRenal status Without appropriate adjustment for CrCl, may Without appropriate adjustment for CrCl, may
increase bleeding events associated with UFH, increase bleeding events associated with UFH, enox, and GP IIb/IIIa agentsenox, and GP IIb/IIIa agents
► Anticipated downstream managementAnticipated downstream management PCI, CABG capability and time to cathPCI, CABG capability and time to cath
► TroponinTroponin Troponin + shown to respond better to Troponin + shown to respond better to
• early (vs later) cathearly (vs later) cath• enox (vs UFH)enox (vs UFH)• clopidogrel + ASA (vs ASA monotherapy)clopidogrel + ASA (vs ASA monotherapy)• GP IIb/IIIa therapyGP IIb/IIIa therapy

Factors that Should Influence Choice of Factors that Should Influence Choice of Upstream Therapy for NSTE ACSUpstream Therapy for NSTE ACS
► H / HH / H Anemic patients more likely to have bleeding Anemic patients more likely to have bleeding
eventsevents
► WeightWeight Smaller patients more likely to be overdosedSmaller patients more likely to be overdosed Larger patients more likely to be underdosed and Larger patients more likely to be underdosed and
may have renal issuesmay have renal issues
► Perceived CABG risk (short-term)Perceived CABG risk (short-term) Impacts timing of clopidogrel dosingImpacts timing of clopidogrel dosing Among GP IIb/IIIa agents, mitigates against Among GP IIb/IIIa agents, mitigates against
abciximababciximab

► Chest Pain or ACS CommitteeChest Pain or ACS Committee
► Meets quarterly or PRNMeets quarterly or PRN PRN means after . . .PRN means after . . .
• Pertinent, “practice-changing” new study Pertinent, “practice-changing” new study publishedpublished
• ACC / AHA / TCT meetingsACC / AHA / TCT meetings• M & M or sentinel eventM & M or sentinel event• New guidelines publishedNew guidelines published
Optimal Management of NSTE ACS: Optimal Management of NSTE ACS: ED to Cardiology: A Functional ModelED to Cardiology: A Functional Model

► Chest Pain or ACS Committee comprised ofChest Pain or ACS Committee comprised of Emergency physiciansEmergency physicians Interventional cardiologistsInterventional cardiologists Medical cardiologistsMedical cardiologists HospitalistsHospitalists CT surgeonsCT surgeons ED nursingED nursing Cath lab nursingCath lab nursing CCU nursingCCU nursing LabLab imagingimaging
Optimal Management of NSTE ACS: ED Optimal Management of NSTE ACS: ED to Cardiology: A Functional Modelto Cardiology: A Functional Model

► Chest Pain or ACS Committee discusses:Chest Pain or ACS Committee discusses: Protocols / standing ordersProtocols / standing orders Practice variations vs evidencePractice variations vs evidence Reduction of medical errors in ACS careReduction of medical errors in ACS care DTB timesDTB times QI issues (CRUSADE / NRMI / ACTION)QI issues (CRUSADE / NRMI / ACTION) Transfers in, transfers outTransfers in, transfers out New data - - should it impact our protocols New data - - should it impact our protocols
before it is added to guidelines?before it is added to guidelines?
Optimal Management of NSTE ACS: Optimal Management of NSTE ACS: ED to Cardiology: A Functional ModelED to Cardiology: A Functional Model

We in the ED should be using optimal medical We in the ED should be using optimal medical therapy for NSTE ACS, just as in the CCU or the cath therapy for NSTE ACS, just as in the CCU or the cath lab. lab.
We in the ED must work with our colleagues in We in the ED must work with our colleagues in Cardiology to develop pathways for proper use of Cardiology to develop pathways for proper use of antithrombotic and antiplatelet therapy at all levels, to antithrombotic and antiplatelet therapy at all levels, to facilitate early invasive management whenever facilitate early invasive management whenever feasible, and to address issues related to bleeding feasible, and to address issues related to bleeding risk as well as ischemic risk. A seamless transition of risk as well as ischemic risk. A seamless transition of care is most likely to result in good outcomes.care is most likely to result in good outcomes.
We in the ED should be using optimal medical We in the ED should be using optimal medical therapy for NSTE ACS, just as in the CCU or the cath therapy for NSTE ACS, just as in the CCU or the cath lab. lab.
We in the ED must work with our colleagues in We in the ED must work with our colleagues in Cardiology to develop pathways for proper use of Cardiology to develop pathways for proper use of antithrombotic and antiplatelet therapy at all levels, to antithrombotic and antiplatelet therapy at all levels, to facilitate early invasive management whenever facilitate early invasive management whenever feasible, and to address issues related to bleeding feasible, and to address issues related to bleeding risk as well as ischemic risk. A seamless transition of risk as well as ischemic risk. A seamless transition of care is most likely to result in good outcomes.care is most likely to result in good outcomes.
Optimal Management of NSTE ACS: Optimal Management of NSTE ACS: ED to CardiologyED to Cardiology

Case Studies inCase Studies inAcute Coronary SyndromesAcute Coronary Syndromes
Moderated by:Moderated by:
Interventional Cardiology Co-ChairmanInterventional Cardiology Co-ChairmanEmergency Medicine Co-ChairmanEmergency Medicine Co-Chairman
Regional Expert Panel MembersRegional Expert Panel Members
Moderated by:Moderated by:
Interventional Cardiology Co-ChairmanInterventional Cardiology Co-ChairmanEmergency Medicine Co-ChairmanEmergency Medicine Co-Chairman
Regional Expert Panel MembersRegional Expert Panel Members

Case Studies in Acute Coronary SyndromesCase Studies in Acute Coronary Syndromes
Acknowledgement is made to Dr. Steven Manoukian, Acknowledgement is made to Dr. Steven Manoukian, MD and CMEducation Resources, LLC for patient cases MD and CMEducation Resources, LLC for patient cases
studies, cineangiograms, and/or assistance in studies, cineangiograms, and/or assistance in preparation of case studies for this segment of the preparation of case studies for this segment of the
program program
Acknowledgement is made to Dr. Steven Manoukian, Acknowledgement is made to Dr. Steven Manoukian, MD and CMEducation Resources, LLC for patient cases MD and CMEducation Resources, LLC for patient cases
studies, cineangiograms, and/or assistance in studies, cineangiograms, and/or assistance in preparation of case studies for this segment of the preparation of case studies for this segment of the
program program

Case #1: History and FindingsCase #1: History and Findings
► A 76 year-old white male with h/o stent to LAD 1 A 76 year-old white male with h/o stent to LAD 1 year agoyear ago
► Presents with multiple episodes of recurrent Presents with multiple episodes of recurrent chest pain including rest pain over 2 dayschest pain including rest pain over 2 days
► Pain similar to time of PCI in pastPain similar to time of PCI in past► Symptoms relieved in ED with sl NTGSymptoms relieved in ED with sl NTG► PMH: IDDM, HTN, CHOL elevationPMH: IDDM, HTN, CHOL elevation► PE: benign (weight 84 kg).PE: benign (weight 84 kg).► Labs: Labs: Hgb 10.7Hgb 10.7, , Cr 1.9,Cr 1.9, CK 173/2, Tr <0.03. CK 173/2, Tr <0.03.► ECG (next slide)ECG (next slide)
► A 76 year-old white male with h/o stent to LAD 1 A 76 year-old white male with h/o stent to LAD 1 year agoyear ago
► Presents with multiple episodes of recurrent Presents with multiple episodes of recurrent chest pain including rest pain over 2 dayschest pain including rest pain over 2 days
► Pain similar to time of PCI in pastPain similar to time of PCI in past► Symptoms relieved in ED with sl NTGSymptoms relieved in ED with sl NTG► PMH: IDDM, HTN, CHOL elevationPMH: IDDM, HTN, CHOL elevation► PE: benign (weight 84 kg).PE: benign (weight 84 kg).► Labs: Labs: Hgb 10.7Hgb 10.7, , Cr 1.9,Cr 1.9, CK 173/2, Tr <0.03. CK 173/2, Tr <0.03.► ECG (next slide)ECG (next slide)

Case #1: ECGCase #1: ECG
New anterior and lateral ST / T changes.

Based on your clinical assessment, this patient’s risk of Based on your clinical assessment, this patient’s risk of short-term (30-Day) ischemic events is:short-term (30-Day) ischemic events is:
A.A. LowLow
B.B. ModerateModerate
C.C. HighHigh
D.D. Very highVery high
Case #1Case #1

Which of this patient’s baseline factors do you Which of this patient’s baseline factors do you consider most important for determining this patient’s consider most important for determining this patient’s
ischemic risk?ischemic risk?
A.A. Advanced age Advanced age
B.B. Anginal pattern Anginal pattern
C.C. ECG findings ECG findings
D.D. Biomarkers Biomarkers
*
Case #1Case #1

Based on your clinical assessment, this patient’s risk of Based on your clinical assessment, this patient’s risk of incurring a short-term (30-Day) hemorrhagic event related incurring a short-term (30-Day) hemorrhagic event related
to PCI is:to PCI is:
A.A. LowLow
B.B. ModerateModerate
C.C. HighHigh
D.D. Very highVery high
Case #1Case #1

Which of this patient’s baseline factors do you consider Which of this patient’s baseline factors do you consider most important for determining hemorrhagic risk?most important for determining hemorrhagic risk?
A.A. Advanced age Advanced age
B.B. Hypertension Hypertension
C.C. Impaired creatinine clearance Impaired creatinine clearance
D.D. Anemia Anemia
*
Case #1Case #1

In ACS patients, do you alter your choice of In ACS patients, do you alter your choice of anticoagulant/ antithrombotic therapy based upon an anticoagulant/ antithrombotic therapy based upon an
assessment of the individual patient’s risk of assessment of the individual patient’s risk of hemorrhagic complications?hemorrhagic complications?
A.A. Yes Yes
B.B. No No
*
Case #1Case #1

Among those of you who Among those of you who wouldwould alter or customize alter or customize antithrombotic therapy based on an ACS patient’s risk antithrombotic therapy based on an ACS patient’s risk
for hemorrhage in the setting of PCI, which of the for hemorrhage in the setting of PCI, which of the following baseline characteristics would you consider following baseline characteristics would you consider
most important in supporting the use of a “hemorrhage-most important in supporting the use of a “hemorrhage-minimizing” anithrombotic regimen:minimizing” anithrombotic regimen:
A.A. Elderly and femaleElderly and female
B.B. Renal insufficiency and positive Renal insufficiency and positive biomarkersbiomarkers
C.C. Anemia and high risk ischemic featuresAnemia and high risk ischemic features
*
Case #1Case #1

What would you likely use for anticoagulation in this What would you likely use for anticoagulation in this patient, prior to catheterization, if you anticipated patient, prior to catheterization, if you anticipated catheterization would occur in catheterization would occur in 4 hours or less?4 hours or less?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. FondaparinuxFondaparinux
*
Case #1Case #1

What would your choice of upstream anticoagulation What would your choice of upstream anticoagulation therapy be, if you anticipated cardiac catheterization therapy be, if you anticipated cardiac catheterization the the
same day (within 12 hours)?same day (within 12 hours)?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. FondaparinuxFondaparinux
*
Case #1Case #1

What would your choice of upstream anticoagulation What would your choice of upstream anticoagulation therapy be, if you anticipated cardiac catheterization therapy be, if you anticipated cardiac catheterization the the
next day (within 24 hours)?next day (within 24 hours)?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. FondaparinuxFondaparinux
*
Case #1Case #1

At this point, your anticoagulation regimen for PCI in At this point, your anticoagulation regimen for PCI in this patient would be?this patient would be?
A.A. Additional heparin Additional heparin
B.B. Switch to enoxaparin Switch to enoxaparin
C.C. Switch to bivalirudin Switch to bivalirudin
D.D. Additional heparin plus GP IIb/IIIa inhibitor Additional heparin plus GP IIb/IIIa inhibitor
*
Case #1Case #1

Case #2: HistoryCase #2: History
► 77 year-old white female without prior cardiac 77 year-old white female without prior cardiac historyhistory
► Multiple short episodes of chest pain todayMultiple short episodes of chest pain today
► Unrelieved with NTG sl and IV; metoprolol IVUnrelieved with NTG sl and IV; metoprolol IV
► PMH: DM, HTN, CHOLPMH: DM, HTN, CHOL
► PE: benign (weight 65 kg).PE: benign (weight 65 kg).
► Labs: Hgb 11.7, Cr 1.1, CK 285/9, Labs: Hgb 11.7, Cr 1.1, CK 285/9, Tr 2.7.Tr 2.7.
► ECG.ECG.

Case #2: ECGCase #2: ECG
New inferior changes New lateral changes

Based upon this patient’s overall profile, when selecting Based upon this patient’s overall profile, when selecting an antithrombotic regimen, you are more likely be an antithrombotic regimen, you are more likely be
concerned about:concerned about:
A.A. Ischemic risk Ischemic risk
B.B. Hemorrhagic risk Hemorrhagic risk
*
Case #2Case #2

Which of the following factors would you consider most Which of the following factors would you consider most important when evaluating the need for immediate important when evaluating the need for immediate
catheterization in this patient?catheterization in this patient?
A.A. Advanced age Advanced age
B.B. Positive biomarkers Positive biomarkers
C.C. ECG findings ECG findings
D.D. Refractory discomfort Refractory discomfort
*
Case #2Case #2

Would a plan of immediate versus delayed Would a plan of immediate versus delayed catheterization influence your choice of anticoagulation catheterization influence your choice of anticoagulation
therapy?therapy?
A.A. YesYes
B.B. NoNo
*
Case #2Case #2

If this patient was going for immediate catheterization If this patient was going for immediate catheterization (now), which of the following regimens would you start?(now), which of the following regimens would you start?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. FondaparinuxFondaparinux
*
Case #2Case #2

If catheterization had to be delayed 2-4 hours If catheterization had to be delayed 2-4 hours (availability of lab, transfer, etc.), which of the following (availability of lab, transfer, etc.), which of the following
regimens would you start?regimens would you start?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. Fondaparinux Fondaparinux
*
Case #2Case #2

Case #3: HistoryCase #3: History
► 82 year old white-female with history of MI, 82 year old white-female with history of MI, PTCA/LAD in 1997PTCA/LAD in 1997
► Presents with exertional chest pain as well as Presents with exertional chest pain as well as chest pressure at rest x 72 hours, but is now chest pressure at rest x 72 hours, but is now pain-free in EDpain-free in ED
► PMH: IRDM, HTN, CHOLPMH: IRDM, HTN, CHOL
► PE: 2/6 murmur at apex (weight 58 kg)PE: 2/6 murmur at apex (weight 58 kg)
► Labs: Hgb 11.1, Labs: Hgb 11.1, Cr 1.6Cr 1.6, CK 37/1, , CK 37/1, Tr <0.03Tr <0.03
► ECG.ECG.

Case #3: ECGCase #3: ECG
No notable findings compared to old ECG.

What would you use for upstream anticoagulation in this What would you use for upstream anticoagulation in this patient whose catheterization is planned for the next patient whose catheterization is planned for the next
day: i.e., within 24 hours?day: i.e., within 24 hours?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. FondaparinuxFondaparinux
*
Case #3Case #3

In general, in an ACS patient with moderate or high risk In general, in an ACS patient with moderate or high risk ischemic features, at what point in the patient’s course would ischemic features, at what point in the patient’s course would
you administer clopidogrel?you administer clopidogrel?
A.A. In the ED, immediately. In the ED, immediately.
B.B. In the catheterization lab, prior to In the catheterization lab, prior to catheterization.catheterization.
C.C. In the catheterization lab, after In the catheterization lab, after catheterization and decision to proceed catheterization and decision to proceed with PCI, but prior to PCI.with PCI, but prior to PCI.
D.D. In the catheterization lab, post-PCI. In the catheterization lab, post-PCI.
*
Concluding QuestionsConcluding Questions

In general, based on my interpretation of the current In general, based on my interpretation of the current evidence for selecting anticoagulation therapy in ACS evidence for selecting anticoagulation therapy in ACS
patients, therapy is best guided by:patients, therapy is best guided by:
A.A. Ischemic risk (reduction of ischemic Ischemic risk (reduction of ischemic endpoints) endpoints)
B.B. Bleeding risk (reduction of bleeding Bleeding risk (reduction of bleeding endpoints)endpoints)
C.C. Balance of ischemic and bleeding risk, and Balance of ischemic and bleeding risk, and selection of a strategy that optimizes “net selection of a strategy that optimizes “net clinical benefit” (optimizes aggregate clinical benefit” (optimizes aggregate reduction of both ischemic and bleeding reduction of both ischemic and bleeding endpoints)endpoints)*
Concluding QuestionsConcluding Questions

INTERACTIVE FORUMApplying Evidence, Trials, and
Clinical Realities to Multidisciplinary ACS Care
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

1.1. How should interventional cardiologists and How should interventional cardiologists and emergency physicians collaborate to deliver optimal emergency physicians collaborate to deliver optimal care for ACS?care for ACS?
• Can and should EDICT therapeutic teams be • Can and should EDICT therapeutic teams be organized, and if so, what form should they take? organized, and if so, what form should they take? Who should be on these teams? Who should be on these teams?
• What are the responsibilities and mandates of such • What are the responsibilities and mandates of such
a team? Policies? Pathways? Therapeutic a team? Policies? Pathways? Therapeutic consistency? consistency?
• How should protocols for EDICT for ACS be • How should protocols for EDICT for ACS be generated? generated?
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

2.2. Understanding the “mind sets” and action drivers of Understanding the “mind sets” and action drivers of EDICT for ACS team members, i.e., interventional EDICT for ACS team members, i.e., interventional cardiologists (ICs) versus emergency physicians cardiologists (ICs) versus emergency physicians (EPs):(EPs):
• Are emergency physicians “guideline-driven?” Are • Are emergency physicians “guideline-driven?” Are they more likely to adhere strictly to AHA/ACC they more likely to adhere strictly to AHA/ACC guidelines than ICs? Why do they adopt strategies? guidelines than ICs? Why do they adopt strategies?
• Are IC decisions, practices, and protocols driven • Are IC decisions, practices, and protocols driven more by clinical experience, and trial-based data? more by clinical experience, and trial-based data?
• Does this lead to a divergence of treatment • Does this lead to a divergence of treatment approaches for ACS? How can and should these approaches for ACS? How can and should these differences be reconciled? differences be reconciled?
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

3. In which patient types are IC and EP care strategies 3. In which patient types are IC and EP care strategies for ACS patients most closely aligned currently?for ACS patients most closely aligned currently?
• Medical therapy for low risk groups?• Medical therapy for low risk groups? Where is there agreement? Disagreement? Where is there agreement? Disagreement?
• Moderate or high risk patients going to• Moderate or high risk patients going to catheterization/PCI within 4 hours (relatively catheterization/PCI within 4 hours (relatively immediately)? Agreement? Disagreement? immediately)? Agreement? Disagreement?
• Moderate or high risk groups with anticipated• Moderate or high risk groups with anticipated catheterization within 12-24 hours? catheterization within 12-24 hours? Agreement? Disagreement? Agreement? Disagreement?
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

4. What clinical outcome measures would an EDICT for 4. What clinical outcome measures would an EDICT for ACS team or review panel follow to evaluate success ACS team or review panel follow to evaluate success or failure of their NSTE-ACS protocols, processes, or failure of their NSTE-ACS protocols, processes, and therapies?and therapies?
• Door to catheterization/PCI time? Measure against• Door to catheterization/PCI time? Measure against CRUSADE findings and benchmarks? Other CRUSADE findings and benchmarks? Other benchmarks? benchmarks?
• Time to onset of antithrombotic therapy?• Time to onset of antithrombotic therapy?
• Length of hospitalization? Cost of hospitalization?• Length of hospitalization? Cost of hospitalization?
• Bleeding complications? Ischemic complications?• Bleeding complications? Ischemic complications?
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

5.5. Can EDICT for ACS teams develop a quick checklist Can EDICT for ACS teams develop a quick checklist or risk stratification tool to determine importance of or risk stratification tool to determine importance of bleeding risk?bleeding risk?
• What risk factors should suggest bleeding-sparing• What risk factors should suggest bleeding-sparing strategies as dominant antithrombotic strategy? strategies as dominant antithrombotic strategy?
• What are bleeding reduction strategies? When• What are bleeding reduction strategies? When should they take precedence? should they take precedence?
• How should this be incorporated into protocol?• How should this be incorporated into protocol?
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

6. What specific ACS strategies can this group agree 6. What specific ACS strategies can this group agree upon as it relates to NSTE-ACS, and therefore, upon as it relates to NSTE-ACS, and therefore, recommend for adoption by an EDICT for ACS team?recommend for adoption by an EDICT for ACS team?
• Timing of invasive strategy? ASAP? Depending• Timing of invasive strategy? ASAP? Depending on risk group? on risk group?
• Clopidogrel use: When? In Whom? How much? • Clopidogrel use: When? In Whom? How much? Caveats? Caveats?
• GPIIb/IIIa receptor antagonist: When? Upstream?• GPIIb/IIIa receptor antagonist: When? Upstream? At catheterization? Routine? Provisional? At catheterization? Routine? Provisional?
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

6. Recommendations for EDICT for ACS strategies 6. Recommendations for EDICT for ACS strategies (continued)?(continued)?
• Direct thrombin inhibitor (bivalirudin)? In which • Direct thrombin inhibitor (bivalirudin)? In which patient populations? Monotherapy? When to patient populations? Monotherapy? When to initiate? Crossovers? When not to initiate? initiate? Crossovers? When not to initiate?
• How should new ACC/AHA guidelines impact • How should new ACC/AHA guidelines impact decisions about bivalirudin? Where would EPs and decisions about bivalirudin? Where would EPs and ICs introduce bivalirudin into process-of-care ICs introduce bivalirudin into process-of-care pathway for ACS? pathway for ACS?
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

6. Recommendations for ACS strategies (continued)?6. Recommendations for ACS strategies (continued)? • Enoxaparin? When to use? When not to use?• Enoxaparin? When to use? When not to use? What if consistency cannot be maintained? What if consistency cannot be maintained? Crossovers? Crossovers?
• Heparin? When to use? When not to use?• Heparin? When to use? When not to use? What if consistency cannot be maintained? What if consistency cannot be maintained? Crossovers? Crossovers?
• Fondaparinux?• Fondaparinux?
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

6.6. Recommendations for EDICT for ACS clinical Recommendations for EDICT for ACS clinical strategies (continued)?strategies (continued)?
• Statins: Should they be initiated in ED as part of • Statins: Should they be initiated in ED as part of EDICT strategy? If so, at what point? What agent? EDICT strategy? If so, at what point? What agent? At what dose? At what dose?
• Beta-blockers?• Beta-blockers?
• ACEIs or ARBs? In certain subsets? Diabetics? • ACEIs or ARBs? In certain subsets? Diabetics? Heart failure? Heart failure?
*
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants

7. Practical and process-oriented recommendations for 7. Practical and process-oriented recommendations for and EDICT for ACS program:and EDICT for ACS program:
• How often should EDICT for ACS leadership• How often should EDICT for ACS leadership committee meet within an institution? committee meet within an institution?
• What should its goals be? Protocols? • What should its goals be? Protocols? Compliance? Measuring outcomes? Compliance? Measuring outcomes?
• How should findings and recommendations• How should findings and recommendations be disseminated? be disseminated?
• Education? EdictforACS.com? How should it • Education? EdictforACS.com? How should it be used? be used?
*
EDICT for ACS INTERACTIVE FORUMEDICT for ACS INTERACTIVE FORUMFaculty, Expert Panel, and ParticipantsFaculty, Expert Panel, and Participants