Embed Size (px)
Citation preview

Archives of Gerontology and Geriatrics 57 (2013) 292–297
Interaction of white matter hyperintensities (WMHs) andapolipoprotein E (APOE) genotypes on cognition in patientswith amnestic mild cognitive impairment (aMCI)
Bora Yoon a, Yong S. Shim b, Hae-Kwan Cheong c, Yong-Duk Kim a, Kee Ook Lee a,Yun-Jeong Hong d, Yoon-Sang Oh b, Hae Ri Na e, Beoung-Chae Kim f,Seong Hye Choi g, Dong-Won Yang b,*a Department of Neurology, Konyang University College of Medicine, 685 Gasuwon-dong, Seo-gu, Daejeon, Republic of Koreab Department of Neurology, The Catholic University of Korea, College of Medicine, 505 Banpo-dong, Seocho-gu, Seoul, Republic of Koreac Department of Social and Preventive Medicine, School of Medicine, Sungkyunkwan University, 2066 Seobu-ro, Jangan-gu, Suwon, Republic of Koread Department of Neurology, Yong-in Hyoja Geriatric Hospital, 33 Sangha-dong, Giheung-gu, Yongin, Republic of Koreae Department of Neurology, Bobath Memorial Hospital, 310-8 Geumgok-dong, Bundang-gu, Seongnam, Republic of Koreaf Department of Neurology, Chonnam National University Medical School, 8 Hak-dong, Dong-gu, Gwangju, Republic of Koreag Department of Neurology, Inha University School of Medicine, 7-206 Sinheung-dong, Joong-gu, Incheon, Republic of Korea
A R T I C L E I N F O
Article history:
Received 15 November 2012
Received in revised form 12 February 2013
Accepted 18 April 2013
Available online 17 May 2013
Keywords:
WMHs
APOE
Mild cognitive impairment
Frontal executive function
Cognition
A B S T R A C T
The clinical implications of WMHs in aMCI are inconclusive. Moreover, clinical interactions between
APOE genotypes and WMHs remain unclear. This study was conducted to investigate the relationship
between WMHs and cognitive functions and how this relationship interacted with APOE genotype in
people with aMCI. This study included a total of 1472 patients with aMCI from the Clinical Research
Center for Dementia of South Korea (CREDOS) and divided them into 3 groups according to the severity of
WMHs as assessed by visual ratings of brain magnetic resonance images. The associations of WMHs with
the various cognitive domains and with APOE epsilon 4 (e4) status were evaluated. After multivariable
adjustments, the severity of WMHs was independently associated with semantic/phonemic verbal
fluency and Stroop test-color reading, while APOE e4 status was associated with verbal and visual
memory-immediate, delayed recall, and recognition. Moreover, there were interaction between WMHs
and APOE e4 status in semantic verbal fluency (animal, P = 0.033; supermarket, P = 0.047)/Stroop test-
color reading (P = 0.024). WMHs independently deleteriously affected frontal executive functions in
aMCI patients, regardless of APOE e4 presence. Furthermore, APOE e4 possession caused a rapid decline in
frontal executive functions with the increase in the WMHs severity (vs. absence), suggesting that WMHs
and APOE e4 genotypes synergistically contribute to frontal executive dysfunctions in aMCI.
� 2013 Elsevier Ireland Ltd. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Archives of Gerontology and Geriatrics
jo ur n al ho mep ag e: www .e lsev ier . c om / lo cate /ar c hg er
1. Introduction
The apolipoprotein E (APOE) epsilon 4 (e4) allele is a majorgenetic risk factor for late-onset Alzheimer’s disease (AD) and hasalso been implicated in cardiovascular diseases (Dik et al., 2000),white matter changes (Bronge et al., 1999; de Leeuw et al., 2004)and cognitive impairment (Dik et al., 2001). Moreover, somestudies have shown that APOE e4 affects conversion from amnesticmild cognitive impairment (aMCI) which is a subtype of MCI to AD
* Corresponding author at: Department of Neurology, The Catholic University of
Korea, College of Medicine, Seoul St. Mary’s Hospital, 505 Banpo-dong, Seocho-gu,
Seoul 137-040, Republic of Korea. Tel.: +82 2 2258 6077; fax: +82 2 599 9686.
E-mail address: [email protected] (D.-W. Yang).
0167-4943/$ – see front matter � 2013 Elsevier Ireland Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.archger.2013.04.008
(Aggarwal, Wilson, Beck, Bienias, & Bennett, 2005; Devanand et al.,2005). Distinct human APOE isoforms differ significantly in theirlong-term effects on neuronal integrity as well as in their ability toprotect against excitotoxicity, which could contribute to theincreased susceptibility and poor outcome of human APOE e4carriers to AD and other brain insults (Buttini et al., 1999).Although some studies have not demonstrated consistent resultsin terms of a relationship between WMHs and cognitive ability,most recent reports including evidence from the Leukoaraiosis AndDISability (LADIS) study have shown that WMHs are associatedwith worse cognitive performance, including processing speed,immediate and delayed memory and executive functions (Au et al.,2006; Debette & Markus, 2010; Murray et al., 2010; Poggesi et al.,2011; van der Flier et al., 2005) as well as mobility (Baezner et al.,2008; Moscufo et al., 2011), urinary control (Poggesi et al., 2008;

B. Yoon et al. / Archives of Gerontology and Geriatrics 57 (2013) 292–297 293
Wakefield et al., 2010) and activities of daily living (ADL) (Inzitariet al., 2007, 2009; Moon et al., 2011; Pantoni et al., 2006) in non-demented elderly and AD patients. The clinical relationshipbetween WMHs and APOE genotypes also still remains incongruentand unclear (Cherbuin, Leach, Christensen, & Anstey, 2007;Paternoster, Chen, & Sudlow, 2009). A previous study has shownthat a combination of WMHs and APOE e4 allele possessionincreases the risk of AD in an elderly population (de Leeuw et al.,2004). Additionally, a twin study has shown that the presence ofthe APOE e4 allele along with an unspecified cardiovascular orcerebrovascular disease increases the risk of WMHs (DeCarli et al.,1999). On the other hand, some previous studies failed to show anycorrelation between APOE e4 and WMHs in patients with AD orvascular dementia (Doody et al., 2000; Schmidt et al., 1996).Moreover, only one study included patients with aMCI known forthe prodromal stage of AD had been performed (Hirono, Yasuda,Tanimukai, Kitagaki, & Mori, 2000).
We hypothesized that the interaction between WMHs and APOE
genotypes could cause different impact on cognition in aMCIpatients, based on the evidence that APOE play a significant role inbrain protection and repair (Buttini et al., 1999). The purpose ofthis study was to evaluate the differences in cognition andfunctional measures depending on WMHs severity or APOE e4status in aMCI patients. In addition, we investigated the relation-ship between WMHs and APOE e4 status.
2. Subjects and methods
2.1. Participants
A total of 1472 aMCI patients were recruited from 43 dementiaclinics at university-affiliated hospitals in Korea between Novem-ber 2005 and March 2010. This study was performed as a part of anongoing, nationwide multicenter study on dementia: the ClinicalResearch Center for Dementia of South Korea (CREDOS) study(identifier on Clinical Trials: NCT01198093). Since 2005, theCREDOS study has developed common protocols, including its ownischemic scale, and recruited patients with subjective memoryimpairment, MCI, AD and vascular dementia. The study wasapproved by each Institutional Review Board of all participanthospitals and written informed consent was obtained from allpatients and their caregivers after a complete description of thestudy.
All patients were evaluated in the following respects: (1) fullclinical histories obtained from a reliable informant; (2) basicdemographic characteristics; (3) past medical histories includingvascular risk factors, such as hypertension, diabetes, hyperlipid-emia and heart disease; (4) neurological evaluations; (5) ClinicalDementia Rating Scale-Sum of Boxes (CDR-SB) (Morris, 1993); (6)the Korean version of the Mini-Mental State Examination (K-MMSE) (Kang, Na, & Hahn, 1997); (7) the Barthel ADL index (B-ADL) (Mahoney & Barthel, 1965) for the evaluation of basic ADL/Seoul-Instrumental Activities of Daily Living (S-IADL) (Ku et al.,2004) for IADL tasks; (8) a standard comprehensive neuropsycho-logical battery; (9) Korean version of the Geriatric Depression Scale(GDS) (Cho, Bae, & Suh, 1999); (10) laboratory tests; and (11) brainmagnetic resonance imaging (MRI) as outlined in the CREDOSstandard protocols.
We generally adhered to the diagnostic criteria for aMCI definedby Petersen et al. (2001) and Winblad et al. (2004). The inclusioncriteria for aMCI patients were as follows: (1) memory complaints;(2) cognitive impairment (at least �1.0 SD below age- andeducation-adjusted norms) in memory and/or �1 domain (execu-tive function, language or visuospatial) on standard neuropsycho-logical tests; (3) normal functional activities (informant’s report ofintact ADL); (5) a CDR of 0.5; and (6) lack of dementia according to
the DSM-IV criteria. In this study, we excluded patients withhemiparesis or who had suffered from a clinical stroke because itcould affect their physical activities. In addition, we excludedpatients with a history of neurological disorders (e.g., activeepilepsy or Parkinson’s disease), psychiatric illnesses (e.g.,schizophrenia, mental retardation, major depression or mania),psychotropic medication, or significant alcohol and/or othersubstance abuses. Furthermore, those who had the secondarycauses of cognitive deficits detected by laboratory findings,including complete blood count, blood chemistry, vitamin B12/folate, syphilis serology and thyroid function test, were excluded.We also excluded patients with large territory infarctions/hemorrhage, based on brain MRI for detecting organic brainlesions that affected cognitive impairment, and those exhibitinghigh MRI signal abnormality related to a brain tumor, radiationinjury, hippocampal sclerosis or multiple sclerosis.
2.2. Cognitive assessments
Cognitive functions were assessed by neuropsychologists usingthe standard comprehensive neuropsychological battery, whichincludes 5 specific cognitive domains: attention, visuospatialfunctions, language, verbal/visual memory and frontal executivefunctions. This battery tests attention by means of digit span andletter cancelation; visuospatial functions by means of the ReyComplex Figure Test (RCFT) copy; language functions by means ofthe Korean version of the Boston Naming Test; verbal memory bymeans of the Seoul Verbal Learning Test (SVLT; three free recalltrials of 12 words, a 20-min delayed recall trial of the same 12items, and a recognition test) (Kang, 1998); visuospatial memoryby means of delayed recall of the RCF; and frontal lobe functions bymeans of the contrasting program, go-no go, fist-edge-palm, Lurialoop, the Controlled Oral Word Association Test (COWAT) (Lee,Kang, Jin, Na, & Park, 2000) and the Stroop letter/color reading test.In this study, we used the scores of COWAT and Stroop test-colorreading among the frontal lobe function tests because other testscannot be calculated by scores.
2.3. Assessment of WMHs
All patients underwent MRI scans at each center using thestandard protocol. MRIs were set as ideal parameters of their own.MRI scans were performed in reference to the anterior-posteriorcommissure line. Axial T2, T1 and fluid attenuated inversionrecovery (FLAIR) images were obtained with 5-mm thicknesseswithout gaps. A neurologist and a radiologist, both of whomworked at participant centers, rated the severity of WMHs on theFLAIR sequence. If there was any disagreement between them inWMHs rating, central committee members finally decided on therating score after discussion. The CREDOS WMHs-rating scaleswere developed by the central committee for the CREDOS study bymodifying Fazekas’ (Fazekas, Chawluk, Alavi, Hurtig, & Zimmer-man, 1987) and Scheltens’ (Scheltens et al., 1993) scales. Thelongest diameter of WMHs around lateral ventricles (capping orbanding on periventricular areas) and the depth of WMHs(especially the centrum semiovale) were evaluated. Periventri-cular WMHs were rated as P1 (<5 mm), P2 (�5 mm, <10 mm), orP3 (�10 mm) and deep WMHs were rated as D1 (<10 mm), D2(�10 mm, <25 mm) or D3 (�25 mm). Periventricular and deepWMHs were combined to produce a final ischemia rating: mild,moderate or severe. The combination of D1 with P1 (D1P1) andthat of D1 with P2 (D1P2) were rated as ‘‘mild.’’ Combinations ofD2P1, D3P1, D2P2, D3P2, D1P3 and D2P3 were rated as‘‘moderate,’’ and D3P3 was rated as ‘‘severe.‘‘The inter-raterreliabilities for the periventricular WMHs (k = 0.595), deep WMHs(k = 0.787) and WMHs (k = 0.785) were high and the intra-rater

B. Yoon et al. / Archives of Gerontology and Geriatrics 57 (2013) 292–297294
reliabilities for WMHs, including periventricular and deep WMHs,(k = 0.694–0.979) were also high. We subdivided all patients into 3groups according to the severity of their WMHs: mild, moderateand severe. Several studies have already been conducted using thesame protocol (Kee Hyung et al., 2011; Ku et al., 2011; Moon et al.,2011; Shim et al., 2011).
2.4. APOE genotyping
APOE genotypes were analyzed, using the standard polymerasechain reaction method. The DNAs of all subjects were extractedfrom their peripheral blood samples using the phenol–chloroformprocedure, and APOE genes were amplified in the polymorphicregion. Frequencies of e2, e3 and e4 alleles were estimated by genecounting. We classified all patients into 2 groups, APOE e4 carrier vsnon-carrier group.
2.5. Statistical analysis
Categorical variables were analyzed using the chi-square test orFisher’s exact test. General characteristics were examined usinganalysis of variance (ANOVA) with the Tukey post hoc tests. Weconducted analysis of covariance (ANCOVA) to compare the resultsof neuropsychological tests according to the ratings of the WMHsand the APOE e4 status after adjustment for age, gender, educationlevel and hypertension. We performed a general linear model byentering interaction terms (WMHs � APOE e4 status) as a predictorand the results of cognitive tests as outcomes after controlling forage, gender, education level and hypertension. Bonferroni correc-tion was used for control type 1 error. The Statistical Package forthe Social Sciences (SPSS) for Windows ver. 17.0 (SPSS, Inc,Chicago, IL, USA) was used for data analysis. The statisticalsignificance level was set at P < 0.05.
3. Results
3.1. Demographics according to the ratings of WMHs
Of the 1472 patients, 1045 (71%) were female and 427 (29%)were male. Subjects were divided into 3 groups according to theseverity of WMHs: mild WMHs group (n = 1057; 71.8%), moderateWMHs group (n = 323; 21.9%) and severe WMHs group (n = 92;6.3%). Table 1 shows the demographics, K-MMSE and CDR-SBscores of the subjects according to the ratings of WMHs. There wasno significant association between APOE e4 allele possession and
Table 1Demographic data of patients according to the severity of WMHs.
Severity of WMHs Mild Moderate
Numbers 1057 323
Female, n (%) 745 (70.5) 229 (70.9)
APOEe4 carrier (%) 344 (32.5) 96 (29.7)
Age (yr) 68.7 � 8.2 73.4 � 6.2
Education (yr) 8.2 � 5.2 7.3 � 5.1
Diabetes, n (%) 215 (20.3) 83 (25.7)
Hypertension, n (%) 490 (46.4) 202 (62.5)
Hyperlipidemia, n(%) 198 (18.7) 54 (16.8)
Heart disease, n (%) 161 (15.2) 60 (18.6)
K-MMSE 25.1 � 3.6 24.2 � 3.9
CDR-SB 1.5 � 0.9 1.6 � 0.8
GDS 5.9 � 0.1 6.1 � 0.2
K-MMSE, Korean version Mini-Mental State Examination; CDR-SB, Clinical Dementia R
Values represent the mean � SD. P1 values were calculated by analysis of variance with t
P1 values < 0.05 obtained by post hoc tests were categorized into the following groups in
moderate and severe.
P2 values of K-MMSE and CDR-SB were calculated by analysis of covariance after adjustm
P values of <0.05 are italicized.
WMHs severity. Age, education, frequency of hypertension, the K-MMSE score and CDR-SB were significantly different between the 3groups. After adjustment for age, gender and education, there wereno significant differences in K-MMSE scores (P = 0.634) and CDR-SB (P = 0.340).
3.2. Clinical differences according to WMHs severity or APOE e4 status
and interaction between WMHs and APOE e4 status
WMHs severity revealed statistically significant negativeassociation with neuropsychological tasks such as in the RCFT-copy (P = 0.025), COWAT-animal (P = 0.003), COWAT-phonemictotal score (P = 0.048), and Stroop test-color reading score(P < 0.001) after adjustment for age, gender, education andhypertension (Table 2). APOE e4 carrier group showed worseperformances on SVLT-immediate recall (P = 0.008), delayed recall(P < 0.001), recognition (P < 0.001), RCFT-immediate recall(P < 0.001), delayed recall (P < 0.001), and recognition(P = 0.031) than non-carrier group after adjustment for samecovariates (Table 2).
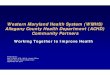
The interactions between WMHs severity and APOE e4 status oncognitive test scores were evaluated after adjustment for theaforementioned covariates. There were close relationships be-tween WMHs and APOE e4 status in COWAT-animal (P = 0.033),supermarket (P = 0.047) and Stroop test-color reading (P = 0.024)(Table 2). The higher the severity of the WMHs became, the morerapidly the slope of cognitive functions declined in the APOE e4carriers vs. non-carriers (Fig. 1). Moreover, the slopes of semanticverbal fluency tests decreased more rapidly from the moderate tosevere state of WMHs, while Stroop test-color reading scoresshowed a rapid decline from the mild to moderate WMHs states, inall the APOE e4 carrier group (vs. non-carrier group; see Fig. 1).
4. Discussion
The aim of this study was to examine the association betweenWMHs and APOE e4 status or cognitive functions in aMCI patients.The results of this study revealed significant differences incognitive test scores between mild, moderate and severe WMHsgroups as well as between APOE e4 carriers and non-carriers. Wealso observed an interactive effect on cognitive tasks of frontalexecutive functions, where WMHs were associated with signifi-cantly worse scores in APOE e4 carriers vs. non-carriers, afteradjustment for various confounding factors. Our results – namelythat WMHs were associated with frontal executive functions –
Severe P1 P2
92 1472
71 (77.2) 0.398
24 (26.1) 0.324
74.0 � 5.3 <0.001*y
7.1 � 5.4 0.006*
16 (17.4) 0.059
63 (68.5) <0.001
12 (13.1) 0.563
22 (23.9) 0.171
24.3 � 4.0 <0.001* 0.643
1.7 � 0.9 0.014y 0.340
5.7 � 0.4 0.350 0.705
ating-Sum of Boxes; GDS, Geriatric Depression Scale.
he Tukey post hoc tests.
terms of WMHs: *between mild and moderate, ybetween mild and severe, zbetween
ent for age, gender and education.

Table 2Results of neuropsychological assessments according to the severity of WMHs.
WMHs severity Noncarrier Carrier WMHs APOE e4 status WMH*APOE
e4 status
Mild Moderate Severe Mild Moderate Severe P1 P2 P3
Attention
Digit span_F 5.29 � 0.05 5.48 � 0.09 5.56 � 0.16 5.50 � 0.07 5.52 � 0.13 5.22 � 0.26 0.205 0.273 0.176
Digit span_B 3.21 � 0.03 3.18 � 0.08 3.07 � 0.11 3.27 � 0.05 3.26 � 0.09 3.25 � 0.18 0.667 0.854 0.764
Language
K_BNT 38.56 � 0.30 38.65 � 0.54 37.54 � 0.96 39.15 � 0.44 37.54 � 0.80 39.14 � 1.64 0.504 0.340 0.125
Visuospatial function
RCFT_copy 27.57 � 0.24 27.83 � 0.43 25.89 � 0.77 28.09 � 0.35 27.99 � 0.65 24.23 � 1.32 0.025 0.425 0.528
Memory
SVLT_IR 15.32 � 0.15 15.51 � 0.26 15.25 � 0.48 15.16 � 0.21 15.10 � 0.40 14.70 � 0.79 0.888 0.008 0.789
SVLT_DR 3.45 � 0.09 3.48 � 0.16 3.43 � 0.28 2.96 � 0.13 2.96 � 0.24 2.11 � 0.47 0.661 <0.001 0.601
SVLT_Rec 18.95 � 0.09 18.89 � 0.16 18.99 � 0.29 18.40 � 0.13 18.73 � 0.24 18.47 � 0.49 0.995 <0.001 0.622
RCFT_IR 8.58 � 0.20 8.79 � 0.36 7.55 � 0.65 6.93 � 0.29 7.89 � 0.54 6.06 � 1.10 0.156 <0.001 0.716
RCFT_DR 8.85 � 0.20 8.81 � 0.35 7.87 � 0.63 6.61 � 0.28 7.95 � 0.53 5.74 � 1.07 0.212 <0.001 0.301
RCFT_Rec 18.27 � 0.08 17.99 � 0.15 17.62 � 0.27 17.76 � 0.12 17.71 � 0.23 17.73 � 0.46 0.103 0.031 0.371
Frontal executive function
COWAT_A 12.34 � 0.14 11.83 � 0.24 11.21 � 0.44 12.12 � 0.20 12.07 � 0.37 10.23 � 0.73 0.003 0.059 0.033
COWAT_S 12.96 � 0.18 12.94 � 0.32 12.68 � 0.57 12.82 � 0.26 13.35 � 0.49 10.86 � 0.96 0.289 0.103 0.047
COWAT_Ph 17.29 � 0.33 16.46 � 0.61 14.97 � 1.11 18.90 � 0.48 17.25 � 0.91 17.53 � 1.74 0.048 0.055 0.075
Stroop test-color 66.71 � 0.86 61.42 � 1.57 61.05 � 2.88 68.75 � 1.24 57.29 � 2.37 57.15 � 4.70 <0.001 0.322 0.024
F/B, forward/backward; K-BNT, Korean version Boston Naming Test; RCFT, Rey Complex Figure Test; SVLT, Seoul Verbal Learning Test; IR/DR/Rec, immediate recall/delayed
recall/recognition; COWAT, Controlled Oral Word Association Test; A/S/Ph, animal/supermarket/phonemic total score.
Values represent the estimated mean � SE using ANCOVA after adjustment for age, gender, and education.
P1, P2, P3 values were calculated by ANCOVA adjusted by age, gender, education level and hypertension.
WMHs � APOE e4 status means the interaction term. P-values of <0.05 are italicized.
B. Yoon et al. / Archives of Gerontology and Geriatrics 57 (2013) 292–297 295
are consistent with previous studies reporting that WMHs areassociated with cognitive impairment, particularly executivedysfunction (Bombois et al., 2007; Debette et al., 2007). WMHscorrespond to ischemic tissue injuries, including incompleteinfarction, gliosis, and the rarefaction and loss of myelin, whichcan cause disconnection of functionally related cortical andsubcortical structures that are important in cognitive functions(Kalaria, 2002; Wen & Sachdev, 2004) APOE e4 status wasassociated with verbal and visual memory, which is in agreementwith the results of previous studies (Packard et al., 2007; Swan,Lessov-Schlaggar, Carmelli, Schellenberg, & La Rue, 2005). WMHswere not associated with MMSE or CDR-SB, after adjustment forconfounders. It was presumed that MMSE and CDR-SB were notsensitive enough to detect subtle cognitive impairment caused byWMHs due to floor effects in aMCI patients. Moreover, MMSE hasthe limitation that it does not reflect executive dysfunctions indetail, compared with other more domain-specific cognitive tasks.Another major finding of this study was the interaction betweenWMHs and APOE e4 status in aMCI patients. In other words, we
Fig. 1. Regression model illustrating the estimated marginal means of specific cognitive d
(c) Stroop test-color reading. The solid line represents APOE e4 carrier and the dot line
found that carriers of the APOE e4 allele showed a greater decline inperformance on executive function tasks with increasing WMHsseverity (compared with non-carriers). From this, it can beconcluded that WMHs and APOE e4 status synergisticallycontribute to impairment in frontal executive functions. Amongthe executive function tests, the semantic verbal fluency testsshowed rapid decline from moderate to severe WMHs state, whilethe Stroop test-color reading was changed severely from mild tomoderate WMHs state. The semantic verbal fluency tests could bebetter than the phonemic verbal fluency test to detect the frontalexecutive dysfunctions related to WMHs in APOE e4 carriers. Ourresults are consistent with a previous report which showed thatthe APOE genotype is an effect-modifier of the relationshipsbetween the cerebral changes and cognitive deterioration which isexacerbated in APOE e4 carriers (Godin et al., 2010). The resultscoincide well with that of a previous study which indicated thatAPOE e4 carrier patients had a greater subcortical WM lesionvolume than those with the e3/e3 genotype (de Leeuw et al., 2004)as well as with the results of other previous studies which
omains in the 3 groups according to WMHs. (a and b) semantic verbal fluency tests;
represents APOE e4 non-carrier.

B. Yoon et al. / Archives of Gerontology and Geriatrics 57 (2013) 292–297296
suggested a positive association between the presence of an e4allele and greater WM lesion volume (Hirono et al., 2000; Kulleret al., 1998). These interactive effects might be explained byseveral mechanisms. First, the presence of an APOE e4 allele mayincrease vulnerability to mild chronic hypoperfusion of the WM byreducing the range of mechanical and chemical flexibility of theglial cytoskeleton (Szolnoki, 2007). Second, the APOE e4 allelepromotes vascular b-amyloid peptide accumulation; therefore,cerebral amyloid angiopathy and vascular amyloid deposition mayalter WM perfusion due to vascular stenosis (Godin et al., 2009;Gurol et al., 2006).
This study has several limitations. First, the incidence of WMHsincreases with aging. Thus, samples were imbalanced with regardto age. We, therefore, corrected all analyses by using patient age asa covariate. Second, this study focused on WMHs, but not on otherdifferences (e.g., lacunar infarcts and hippocampal atrophy) thatmay also have affected the cognitive and functional performancesof the study groups. Third, we used FLAIR images obtained fromdifferent MRI scanners because of the multicenter study design.However, we demonstrated high inter-rater and intra-raterreliabilities for visual ratings of WMHs used in this study andminimized inconsistent rating results by using the centralcommittee. Lastly, this study used a cross-sectional design. Thegeneral applicability of our results may be limited. Therefore,longitudinal studies are needed to have a better understanding ofthe relationships between APOE genotypes and WMHs on MRI.Nevertheless, the strengths of this study include its relatively largesample size, the standardized assessment of WMHs and itsdetailed clinical evaluations.
In summary, WMHs would be an additive, potential imagingbiomarker to predict frontal executive dysfunctions regardless ofAPOE genotypes in aMCI. WMHs and APOE e4 alleles interacted inaffecting performance on executive function – namely there was asignificantly more deleterious effect of increased WMHs severity inAPOE e4 carriers (vs. non-carriers). The semantic verbal fluency andStroop test-color reading test were more sensitive to theinteraction between APOE genotype and WMHs severity, com-pared with memory tasks. It would be desirable to utilize not onlyWMHs but also APOE genotype to predict cognition in aMCIpatients with severe WMHs. Future research therefore couldconsider whether other frontal lobe function tests, such asreasoning, process/motor speed, and concept formation, aresimilarly sensitive.
Conflict of interest
None.
Acknowledgement
This study was supported by a grant of the Korea Healthcaretechnology R&D Project, Ministry of Health and Welfare, Republicof Korea (A102065).
References
Aggarwal, N. T., Wilson, R. S., Beck, T. L., Bienias, J. L., & Bennett, D. A. (2005). Mildcognitive impairment in different functional domains and incident Alzheimer’sdisease. Journal of Neurology, Neurosurgery and Psychiatry, 76, 1479–1484.
Au, R., Massaro, J., Wolf, P., Young, M., Beiser, A., Seshadri, S., et al. (2006). Association ofwhite matter hyperintensity volume with decreased cognitive functioning: TheFramingham Heart Study. Archives of Neurology, 63, 246–250.
Baezner, H., Blahak, C., Poggesi, A., Pantoni, L., Inzitari, D., Chabriat, H., et al. (2008).Association of gait and balance disorders with age-related white matter changes:The LADIS study. Neurology, 70, 935–942.
Bombois, S., Debette, S., Delbeuck, X., Bruandet, A., Lepoittevin, S., Delmaire, C., et al.(2007). Prevalence of subcortical vascular lesions and association with executivefunction in mild cognitive impairment subtypes. Stroke, 38, 2595–2597.
Bronge, L., Fernaeus, S. E., Blomberg, M., Ingelson, M., Lannfelt, L., Isberg, B., et al.(1999). White matter lesions in Alzheimer patients are influenced by apolipopro-tein E genotype. Dementia and Geriatric Cognitive Disorders, 10, 89–96.
Buttini, M., Orth, M., Bellosta, S., Akeefe, H., Pitas, R. E., Wyss-Coray, T., et al. (1999).Expression of human apolipoprotein E3 or E4 in the brains of Apoe�/� mice:Isoform-specific effects on neurodegeneration. Journal of Neuroscience, 19, 4867–4880.
Cherbuin, N., Leach, L. S., Christensen, H., & Anstey, K. J. (2007). Neuroimaging and APOEgenotype: A systematic qualitative review. Dementia and Geriatric Cognitive Dis-orders, 24, 348–362.
Cho, M., Bae, J. N., & Suh, G. H. (1999). Validation of geriatric depression scale. Koreanversion (GDS) in the assessment of DSM-III-R major depression. Journal of KoreanNeuropsychiatric Association, 38, 48–63.
de Leeuw, F. E., Richard, F., de Groot, J. C., van Duijn, C. M., Hofman, A., Van Gijn, J., et al.(2004). Interaction between hypertension, apoE, and cerebral white matter lesions.Stroke, 35, 1057–1060.
Debette, S., Bombois, S., Bruandet, A., Delbeuck, X., Lepoittevin, S., Delmaire, C., et al.(2007). Subcortical hyperintensities are associated with cognitive decline inpatients with mild cognitive impairment. Stroke, 38, 2924–2930.
Debette, S., & Markus, H. S. (2010). The clinical importance of white matter hyper-intensities on brain magnetic resonance imaging: Systematic review and meta-analysis. British Medical Journal, 341, c3666.
DeCarli, C., Reed, T., Miller, B. L., Wolf, P. A., Swan, G. E., & Carmelli, D. (1999). Impact ofapolipoprotein E epsilon4 and vascular disease on brain morphology in men fromthe NHLBI twin study. Stroke, 30, 1548–1553.
Devanand, D. P., Pelton, G. H., Zamora, D., Liu, X., Tabert, M. H., Goodkind, M., et al.(2005). Predictive utility of apolipoprotein E genotype for Alzheimer disease inoutpatients with mild cognitive impairment. Archives of Neurology, 62, 975–980.
Dik, M. G., Deeg, D. J., Bouter, L. M., Corder, E. H., Kok, A., & Jonker, C. (2000). Stroke andapolipoprotein E epsilon4 are independent risk factors for cognitive decline: Apopulation-based study. Stroke, 31, 2431–2436.
Dik, M. G., Jonker, C., Comijs, H. C., Bouter, L. M., Twisk, J. W., van Kamp, G. J., et al.(2001). Memory complaints and APOE-epsilon4 accelerate cognitive decline incognitively normal elderly. Neurology, 57, 2217–2222.
Doody, R. S., Azher, S. N., Haykal, H. A., Dunn, J. K., Liao, T., & Schneider, L. (2000). DoesAPO epsilon4 correlate with MRI changes in Alzheimer’s disease? Journal ofNeurology, Neurosurgery and Psychiatry, 69, 668–671.
Fazekas, F., Chawluk, J., Alavi, A., Hurtig, H., & Zimmerman, R. (1987). MR signalabnormalities at 1.5 T in Alzheimer’s dementia and normal aging. American Journalof Roentgenology, 149, 351–356.
Godin, O., Tzourio, C., Maillard, P., Alperovitch, A., Mazoyer, B., & Dufouil, C. (2009).Apolipoprotein E genotype is related to progression of white matter lesion load.Stroke, 40, 3186–3190.
Godin, O., Tzourio, C., Rouaud, O., Zhu, Y., Maillard, P., Pasquier, F., et al. (2010). Jointeffect of white matter lesions and hippocampal volumes on severity of cognitivedecline: The 3C-Dijon MRI study. Journal of Alzheimer’s Disease, 20, 453–463.
Gurol, M. E., Irizarry, M. C., Smith, E. E., Raju, S., Diaz-Arrastia, R., Bottiglieri, T., et al.(2006). Plasma beta-amyloid and white matter lesions in AD, MCI, and cerebralamyloid angiopathy. Neurology, 66, 23–29.
Hirono, N., Yasuda, M., Tanimukai, S., Kitagaki, H., & Mori, E. (2000). Effect of theapolipoprotein E epsilon4 allele on white matter hyperintensities in dementia.Stroke, 31, 1263–1268.
Inzitari, D., Pracucci, G., Poggesi, A., Carlucci, G., Barkhof, F., Chabriat, H., et al. (2009).Changes in white matter as determinant of global functional decline in olderindependent outpatients: Three year follow-up of LADIS (leukoaraiosis and dis-ability) study cohort. British Medical Journal, 339, b2477.
Inzitari, D., Simoni, M., Pracucci, G., Poggesi, A., Basile, A. M., Chabriat, H., et al. (2007).Risk of rapid global functional decline in elderly patients with severe cerebral age-related white matter changes: The LADIS study. Archives of Internal Medicine, 167,81–88.
Kalaria, R. N. (2002). Small vessel disease and Alzheimer’s dementia: Pathologicalconsiderations. Cerebrovascular Diseases, 13(Suppl. 2), 48–52.
Kang, Y. (1998). Samsung neuropsychological battery. Seoul: Korean Dementia Asso-ciation.
Kang, Y. W., Na, D. L., & Hahn, S. H. (1997). A validity study on the Korean Mini-MentalState Examination (K-MMSE) in dementia patients. Journal of the Korean Neuro-logical Association, 15, 300–307.
Kee Hyung, P., Lee, J. Y., Na, D. L., Kim, S. Y., Cheong, H. K., Moon, S. Y., et al. (2011).Different associations of periventricular and deep white matter lesions withcognition, neuropsychiatric symptoms, and daily activities in dementia. Journalof Geriatric Psychiatry and Neurology, 24, 84–90.
Ku, B. D., Na, D. L., Moon, S. Y., Kim, S. Y., Seo, S. W., Cheong, H. K., et al. (2011).Neuropsychological correlates of the proportional impact of white matter hyper-intensities on mild to moderate dementia: The MRI 300 Study. Dementia andGeriatric Cognitive Disorders, 31, 397–405.
Ku, H., Kim, J., Kwon, E., Kim, S., Lee, H., Ko, H., et al. (2004). A study on the reliabilityand validity of Seoul-instrumental activities of daily living (S-IADL). Journal of theKorean Neurological Association, 43, 189–199.
Kuller, L. H., Shemanski, L., Manolio, T., Haan, M., Fried, L., Bryan, N., et al. (1998).Relationship between ApoE, MRI findings, and cognitive function in the Cardio-vascular Health Study. Stroke, 29, 388–398.
Lee, J., Kang, H., Jin, Y., Na, J. H., & Park, D.L.J.S. (2000). A normative study of the Koreanversion of Controlled Oral Word Association Test (COWAT) in the elderly. KoreanJournal of Clinical Psychology, 19, 385–392.
Mahoney, F. I., & Barthel, D. W. (1965). Functional evaluation: The Barthel index.Maryland State Medical Journal, 14, 61–65.

B. Yoon et al. / Archives of Gerontology and Geriatrics 57 (2013) 292–297 297
Moon, S. Y., Na, D. L., Seo, S. W., Lee, J. Y., Ku, B. D., Kim, S. Y., et al. (2011). Impact ofwhite matter changes on activities of daily living in mild to moderate dementia.European Neurology, 65, 223–230.
Morris, J. C. (1993). The Clinical Dementia Rating (CDR): Current version and scoringrules. Neurology, 43, 2412–2414.
Moscufo, N., Guttmann, C., Meier, D., Csapo, I., Hildenbrand, P. G., Healy, B. C., Schmidt, J.A., & Wolfson, L. (2011). Brain regional lesion burden and impaired mobility in theelderly. Neurobiology of Aging, 32, 646–654.
Murray, M. E., Senjem, M. L., Petersen, R. C., Hollman, J. H., Preboske, G. M., Weigand, S.D., et al. (2010). Functional impact of white matter hyperintensities in cognitivelynormal elderly subjects. Archives of Neurology, 67, 1379–1385.
Packard, C. J., Westendorp, R. G., Stott, D. J., Caslake, M. J., Murray, H. M., Shepherd, J.,et al. (2007). Association between apolipoprotein E4 and cognitive decline inelderly adults. Journal of the American Geriatrics Society, 55, 1777–1785.
Pantoni, L., Poggesi, A., Basile, A. M., Pracucci, G., Barkhof, F., Chabriat, H., et al. (2006).Leukoaraiosis predicts hidden global functioning impairment in nondisabled olderpeople: The LADIS (leukoaraiosis and disability in the elderly) study. Journal of theAmerican Geriatrics Society, 54, 1095–1101.
Paternoster, L., Chen, W., & Sudlow, C. L. (2009). Genetic determinants of white matterhyperintensities on brain scans: A systematic assessment of 19 candidate genepolymorphisms in 46 studies in 19,000 subjects. Stroke, 40, 2020–2026.
Petersen, R. C., Stevens, J. C., Ganguli, M., Tangalos, E. G., Cummings, J. L., & DeKosky, S. T.(2001). Practice parameter: Early detection of dementia: Mild cognitive im-pairment (an evidence-based review). Report of the Quality Standards Subcom-mittee of the American Academy of Neurology. Neurology, 56, 1133–1142.
Poggesi, A., Pantoni, L., Inzitari, D., Fazekas, F., Ferro, J., O’Brien, J., et al. (2011). 2001–2011: A decade of the LADIS (Leukoaraiosis and DISability) study: What have welearned about white matter changes and small-vessel disease? CerebrovascularDiseases, 32, 577–588.
Poggesi, A., Pracucci, G., Chabriat, H., Erkinjuntti, T., Fazekas, F., Verdelho, A., et al.(2008). Urinary complaints in nondisabled elderly people with age-related white
matter changes: The Leukoaraiosis And DISability (LADIS) Study. Journal of theAmerican Geriatrics Society, 56, 1638–1643.
Scheltens, P., Barkhof, F., Leys, D., Pruvo, J. P., Nauta, J. J., Vermersch, P., et al. (1993). Asemiquantative rating scale for the assessment of signal hyperintensities onmagnetic resonance imaging. Journal of the Neurological Sciences, 114, 7–12.
Schmidt, H., Schmidt, R., Fazekas, F., Semmler, J., Kapeller, P., Reinhart, B., et al. (1996).Apolipoprotein E e4 allele in the normal elderly: Neuropsychologic and brain MRIcorrelates. Clinical Genetics, 50, 293–299.
Shim, Y. S., Youn, Y. C., Na, D. L., Kim, S. Y., Cheong, H. K., Moon, S. Y., et al. (2011). Effectsof medial temporal atrophy and white matter hyperintensities on the cognitivefunctions in patients with Alzheimer’s disease. European Neurology, 66, 75–82.
Swan, G. E., Lessov-Schlaggar, C. N., Carmelli, D., Schellenberg, G. D., & La Rue, A. (2005).Apolipoprotein E epsilon4 and change in cognitive functioning in community-dwelling older adults. Journal of Geriatric Psychiatry and Neurology, 18, 196–201.
Szolnoki, Z. (2007). Pathomechanism of leukoaraiosis: A molecular bridge between thegenetic, biochemical, and clinical processes (a mitochondrial hypothesis). Neuro-molecular Medicine, 9, 21–33.
van der Flier, W. M., van Straaten, E. C., Barkhof, F., Verdelho, A., Madureira, S., Pantoni,L., et al. (2005). Small vessel disease and general cognitive function in nondisabledelderly: The LADIS study. Stroke, 36, 2116–2120.
Wakefield, D. B., Moscufo, N., Guttmann, C. R., Kuchel, G. A., Kaplan, R. F., Pearlson, G.,et al. (2010). White matter hyperintensities predict functional decline in voiding,mobility, and cognition in older adults. Journal of the American Geriatrics Society, 58,275–281.
Wen, W., & Sachdev, P. (2004). The topography of white matter hyperintensities onbrain MRI in healthy 60- to 64-year-old individuals. Neuroimage, 22, 144–154.
Winblad, B., Palmer, K., Kivipelto, M., Jelic, V., Fratiglioni, L., Wahlund, L. O., et al.(2004). Mild cognitive impairment-beyond controversies, towards a consensus:Report of the International Working Group on Mild Cognitive Impairment. Journalof Internal Medicine, 256, 240–246.