Embed Size (px)
Citation preview
Integration of Clinical Enterprise
vs
Disintegration of the academic enterprise.
Switzerland
Decisions driven by market imperatives impose
challenges and risks to
University programs, missions and values.
Challenges for Academic Medicine
• Most schools, and certainly ours, rely on clinical revenue to support our research and educational missions.
• Nearly everyone agrees that the clinical revenue streams for teaching hospitals and practice plans will be less than they have been.
• After decades of doing more with more, and, here, doing more with less, can we adapt to a future where we will have to do less with less?
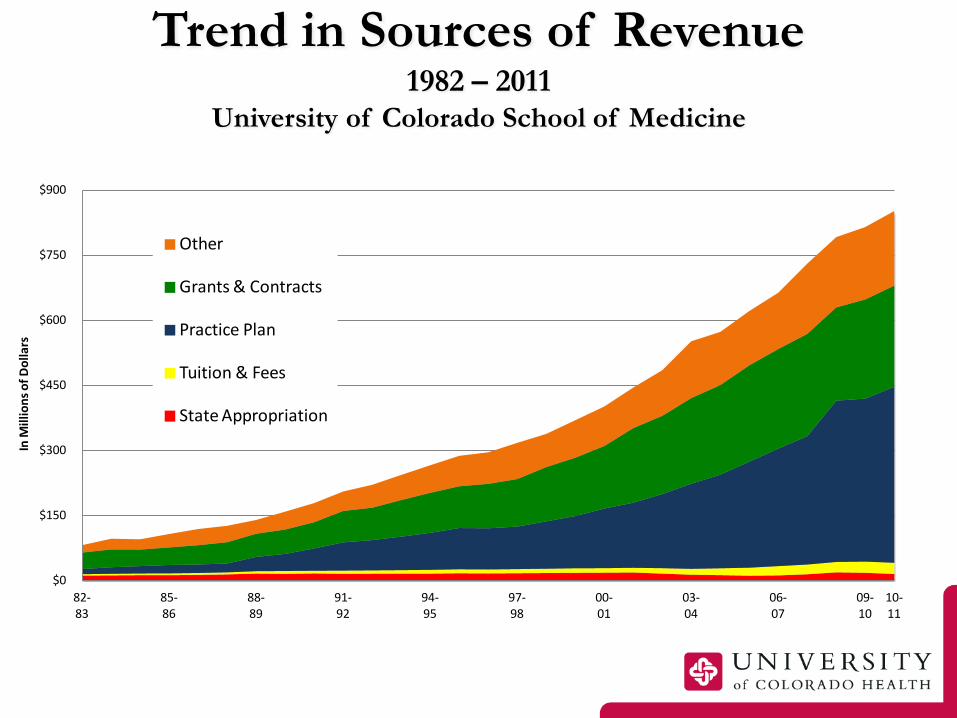
Trend in Sources of Revenue 1982 – 2011
University of Colorado School of Medicine
$0
$150
$300
$450
$600
$750
$900
82-83
85-86
88-89
91-92
94-95
97-98
00-01
03-04
06-07
09-10
10-11
In M
illio
ns o
f Dol
lars
Other
Grants & Contracts
Practice Plan
Tuition & Fees
State Appropriation
The Word of the Moment in Health Care Is “Unsustainable”
The size of the federal budget deficit is unsustainable
The annual increase in the Medicare budget is unsustainable
The percentage of health care spending to GDP is unsustainable
State Medicaid programs are unsustainable
The continued transfer of costs to employers and consumers is unsustainable
Copyrighted by Kaufman, Hall & Associates, Inc. 2012
6
The Solution that Worked for Us (so far)
• Made a decision that we could not stand alone – Systems are retaining patients
• Identified “like-minded” partners with shared
values
• Learned that a lot of give and take to create our vision
7

Benefits of Partnerships • Opens doors to bigger markets
• Creates larger geographic footprints
• Opportunities for economies of scale
• Drives efficiencies
• Adds market power
• Brings research and clinical trials to more patients
8
University of Colorado Health:
A 30,000 Foot View • Two high quality hospitals
• Only owned and operated Colorado based health system
• “Merger-like” in many respects: shared bottom line and a central board of directors
• Each hospital continues to exist as a separate entity and controls operations at respective facilities
• Integration of central services, i.e., IT, Finance, Human Resources, Marketing, Legal
• Bottom Line: separate identities with shared values
9
The I-25 Corridor and UC Health
• 4.0 million of the 4.8 million people who call Colorado home live in an area adjacent to I-25 from Pueblo north to Cheyenne
• UC Health opens doors to research, clinical trials and education
• Brings residents to new areas of the state • History of economic success that is translatable
and replicable
10

The I-25 Corridor and UC Health
Poudre Valley Hospital
Medical Center of the Rockies
University of Colorado Hospital
Memorial Health North
Memorial Health Central
Ivinson Memorial Hospital
11
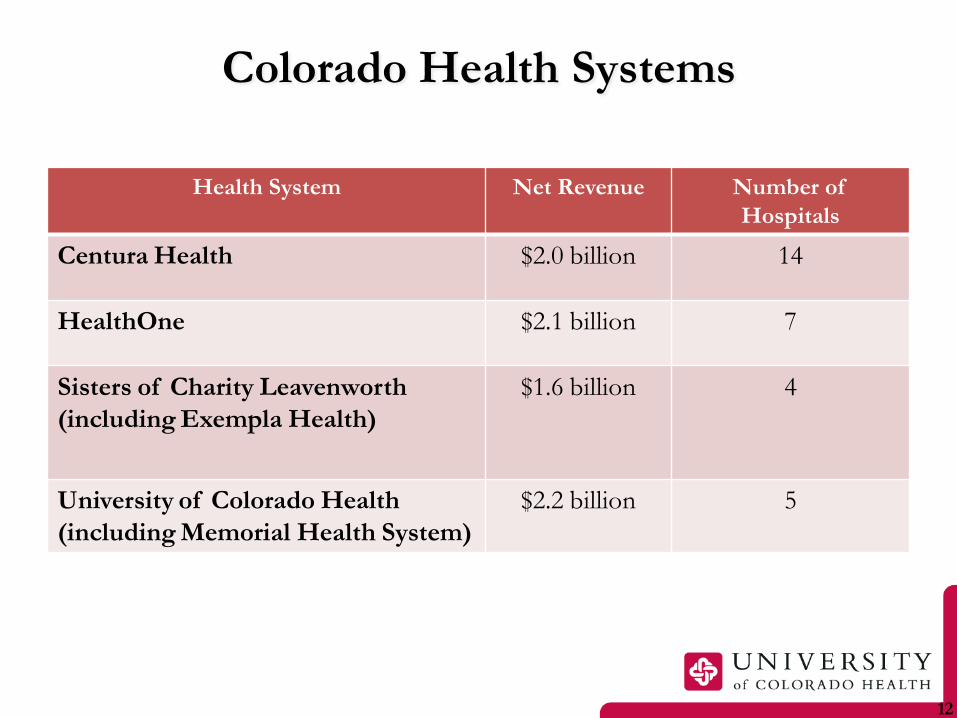
Colorado Health Systems
12
Health System Net Revenue Number of Hospitals
Centura Health $2.0 billion 14
HealthOne $2.1 billion 7
Sisters of Charity Leavenworth (including Exempla Health)
$1.6 billion 4
University of Colorado Health (including Memorial Health System)
$2.2 billion 5
The Challenges of Partnerships • Creating a new health care system can be a
distraction to the day-to-day work
• Academic world vs. Community Hospital world
• How do we balance it all?
• Is someone taking someone else over?
• Dealing with staff, physician and faculty anxieties
13
The Challenges of Partnership
• How to maintain the independence of each hospital while benefitting from being a part of a system
• Facing (and embracing) the ambiguity that exists on many levels
• Managing tension
• Appreciating the cultural and historical differences
14
The Challenges of Partnership for the Practice Plan and School
• The affiliation agreement between the School of Medicine and University of Colorado Hospital does not allow physician employment.
• The University of Colorado Health System does and will need to employ physicians
• How should the School support the System in this necessity?
• How should the system assure that the SOM physicians are not lured away?
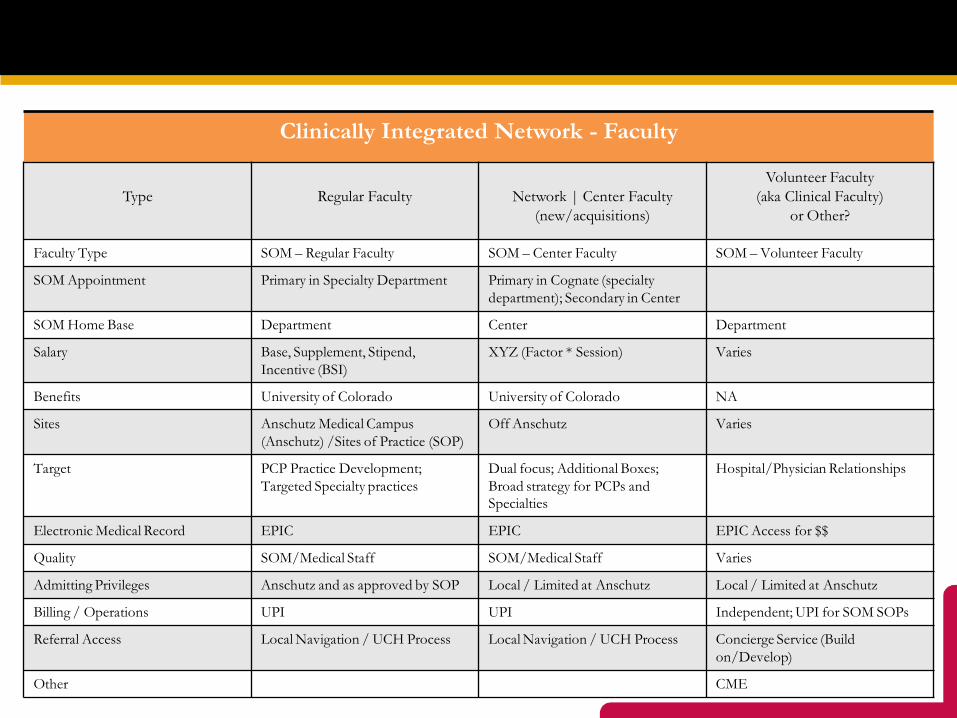
Physician Alignment and Integration
Clinically Integrated Network - Faculty
Type
Regular Faculty
Network | Center Faculty
(new/acquisitions)
Volunteer Faculty (aka Clinical Faculty)
or Other?
Faculty Type SOM – Regular Faculty SOM – Center Faculty SOM – Volunteer Faculty
SOM Appointment Primary in Specialty Department Primary in Cognate (specialty department); Secondary in Center
SOM Home Base Department Center Department
Salary Base, Supplement, Stipend, Incentive (BSI)
XYZ (Factor * Session) Varies
Benefits University of Colorado University of Colorado NA
Sites Anschutz Medical Campus (Anschutz) /Sites of Practice (SOP)
Off Anschutz Varies
Target PCP Practice Development; Targeted Specialty practices
Dual focus; Additional Boxes; Broad strategy for PCPs and Specialties
Hospital/Physician Relationships
Electronic Medical Record EPIC EPIC EPIC Access for $$
Quality SOM/Medical Staff SOM/Medical Staff Varies
Admitting Privileges Anschutz and as approved by SOP Local / Limited at Anschutz Local / Limited at Anschutz
Billing / Operations UPI UPI Independent; UPI for SOM SOPs
Referral Access Local Navigation / UCH Process Local Navigation / UCH Process Concierge Service (Build on/Develop)
Other CME
Questions for the group
• How will the academic mission be supported in the future when all revenue streams slow? – How is it done in a system integrated like UC Davis? – How is it done at non-integrated systems/places?
• Wash U? Hawaii?
• Whose responsibility is it to support the research mission of basic and clinical scientists? – How will we protect faculty’s time?
Questions for the group
• When you are chronically fiscally hungry, can you maintain good table manners?
• If you are not a completely integrated health system with direct accountability to a single person and/or board, how do you assure that people will get along with each other well enough to have everyone succeed?