Embed Size (px)
Citation preview

ELSEVIER Immunopharmacology 38 (1997) 51-62
Immunophannacology
Review article
Controlling the complement system in inflammation
M i c h a e l K i r s c h f i n k *
Institute of lmmunology, University of Heidelberg, Im Neuenheimer Feld 305, 69120 Heidelberg, Germany
Received 24 April 1997; accepted 5 May 1997
Abstract
Inappropriate or excessive activation of the complement system can lead to harmful, potentially life-threatening consequences due to severe inflammatory tissue destruction. These consequences are clinically manifested in various disorders, including septic shock, multiple organ failure and hyperacute graft rejection. Genetic complement deficiencies or complement depletion have been proven to be beneficial in reducing tissue injury in a number of animal models of severe complement-dependent inflammation. It is therefore believed that therapeutic inhibition of complement is likely to arrest the process of certain diseases. Attempts to efficiently inhibit complement include the application of endogenous soluble complement inhibitors (Cl-inhibitor, recombinant soluble complement receptor 1- rsCRl), the administration of antibodies, either blocking key proteins of the cascade reaction (e.g. C3, C5), neutralizing the action of the complement-derived anaphylatoxin C5a, or interfering with complement receptor 3 (CR3, CD18/1 lb)-mediated adhesion of inflammatory cells to the vascular endothelium. In addition, incorporation of membrane-bound complement regulators (DAF-CD55, MCP-CD46, CD59) has become possible by transfection of the correspondent cDNA into xenogeneic cells. Thereby, protection against complement-mediated inflammatory tissue damage could be achieved in various animal models of sepsis, myocardial as well as intestinal ischemia/reperfusion injury, adult respiratory distress syndrome, nephritis and graft rejection. Supported by results from first clinical trials, complement inhibition appears to be a suitable therapeutic approach to control inflammation. Current strategies to specifically inhibit complement in inflammation have been discussed at a recent meeting on the 'Immune Consequences of Trauma, Shock and Sepsis', held from March 4-8, 1997, in Munich, Germany. The Congress (chairman: E. Faist, Munich, Germany), which was held in close cooperation with various national and international shock and trauma societies, was attended by about 2000 delegates from 40 countries. The major objective of the meeting was to provide an overview on the most state-of-the-art methods to prevent multiple organ dysfunction syndrome (MODS)/multi- ple organ failure (MOF) following the systemic inflammatory response (SIRS) to severe trauma. One of the largest symposia held within the Congress was devoted to current aspects of controlling complement in inflammation (for abstracts see: Shock 1997, 7 Suppl., 71-75). After providing the audience with information on the scientific background by addressing the clinical relevance of complement activation (G.O. Till, Ann Arbor, MI, USA) and discussing recent developments in modern
Abbreviations: ARDS, adult respiratory distress syndrome; CD, cluster of differentiation; CPB, cardiopulmonary bypass; CR, complement receptor; CVF, cobra venom factor; C4bp, C4 binding protein; C8bp, C8 binding protein; DAF, decay accelerating factor; GPI, glycosyl-phosphatidyl-inositol; HRF, homologous restriction factor; ICAM, intercellular adhesion molecule; LAD, leukocyte adhesion deficiency; MASP, mannan binding ligand associated serine protease; MBL, mannan binding lectin; MCP, membrane cofactor protein; MODS, multiple organ dysfunction syndrome; MOF, multiple organ failure; rsCR1, recombinant soluble complement receptor l; SIRS, systemic inflammatory response syndrome
* Tel.: + 49-6221-564076; fax: + 49-6221-56-4030; e-mail: [email protected]
0162-3109/97/$17.00 © 1997 Elsevier Science B.V. All rights reserved. Pll S01 62-3 1 09(97)00057-X

52 M. Kirschfink / lmmunopharmacology 38 (1997) 51-62
complement diagnosis (J. KiShl, Hannover, Germany), B.P. Morgan (Cardiff, UK) introduced the symposium's special issue by giving an overview on complement regulatory molecules. Selected topics included overviews on the application of C1 inhibitor (C.E. Hack, Amsterdam, NL), sCR1 (U.S. Ryan, Needham, MA, USA), antibodies to C5 (Y. Wang, New Haven CT, USA) and to the anaphylatoxin C5a (M. Oppermann, GiSttingen, Germany), and a report on complement inhibition in cardiopulmonary bypass (T.E. Mollnes, Bod¢, Norway). The growing interest of clinicians in complement-directed anti-inflammatory therapy, and the fact that only some of the various aspects of therapeutic complement inhibition could be addressed on the meeting, has motivated the author to expand a Congress report into a short comprehensive review on recent strategies to control complement in inflammation. © 1997 Elsevier Science B.V.
Keywords: Inflammation; Complement inhibition; Therapy; Complement regulators; Antibodies
1. Introduction
The complement system (for review see MUller- Eberhard, 1988; Rother and Till, 1988) provides a rapid and efficient means to protect the host from invasive microorganisms. Due to its diverse biologi- cal activities, complement is a key mediator of in- flammation, a natural response of the host tissue to any injury. There is also increasing evidence that complement significantly contributes to the regula- tion of the immune response (Carroll and Fischer, 1997).
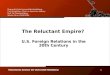
The complement system consists of about 30 proteins, acting within a cascade-like reaction se- quence (Fig. 1), serving as control proteins (Fig. 2) or as cellular receptors. Complement can be acti- vated by any of three pathways, either the antibody- dependent classical pathway, the alternative path-
[ classical pathway ] [ alternative pathway ]
Immune complex foreign surface y ~ y C 1 ~ MBL
~ " ~ [MASP 1 ~
,
C5 C5a @ ~ii: "4
~cs , c ~ 6 - ) ~i i "
Fig. I. Simplified schematic presentation of the complement activation pathways. In course of the reaction sequence proinflam- matory peptides are generated and the membrane attack complex is formed. MBL, mannan binding ligand; MASP, mannan binding ligand-associated serine protease.
MCP DAF
C8
CD59
CR1
~ _ . plasma
[ C linhibitor C4 bp
factor H factor I
clusterin S protein
carboxypeptidase N
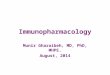
Fig. 2. Under physiological conditions the complement cascade reaction is controlled by fluid phase as well as membrane-associ- ated regulatory proteins.
way, or the recently discovered MBL/MASP (man- nan binding lectin/MBL-associated serine protease) pathway (Turner, 1996). Following complement acti- vation, proinflammatory peptides like the anaphyla- toxins C3a and C5a are generated and the membrane attack complex, C5b-9, is formed. Complement acti- vation products, especially the anaphylatoxins, elicit a number of biological effects such as chemotaxis of leukocytes, degranulation of phagocytic cells, mast cells and basophils, smooth muscle contraction and the increase of vascular permeability (Hugli, 1986). In addition, generation of toxic oxygen radicals and the induction of synthesis and release of arachidonic acid metabolites and cytokines lead to the amplifica- tion of the inflammatory response. Thus, effector functions arising from complement activation carry the potential for harming the host by directly and indirectly mediating inflammatory tissue destruction.
Under physiological conditions uncontrolled acti- vation of complement is prevented by a vast array of regulatory proteins, either circulating in the plasma,

M. Kirschfink / Immunopharmacology 38 (1997) 51-62 53
or expressed on the cell surface (Fig. 2). Host cells are protected against the deleterious attack of homol- ogous complement by the complement receptor 1 (CR1, CD35), the membrane cofactor protein (MCP, CD46) and by glycosylphosphatidylinositol (GPI)- anchored proteins such as the decay-accelerating fac- tor (DAF, CD55), the C8-binding protein/homolo- gous restriction factor (C8bp/HRF) and CD59 (De- vine, 1991).
Considerable clinical and experimental evidence implicate the role of complement in the pathogenesis of numerous inflammatory diseases (for review see Dalmasso, 1986; Morgan, 1990). These include not only immune complex and autoimmune disorders, but also organ failure subsequent to sepsis, multiple trauma and bums. The pivotal role of complement to a wide spectrum of diseases has been underlined by the study of genetic deficiencies (Rother and Rother, 1986) and the design and exploration of experimen- tal disease models.
In recent years great advances have been made in the use of complement measurements for the diagno- sis and assessment of disease severity, evolution and response to therapy. Complement analysis has also been shown to be of prognostic value in early recog- nition of patients at risk to develop multiple organ failure after trauma (Zilow et al., 1990) or with empeding graft rejection following renal transplanta- tion (Kirschfink et al., 1992). Modem diagnostic technologies which focus on the quantification of complement-derived split products or protein-pro- tein complexes provide a comprehensive insight into the activation state of the system (Cooper et al., 1983; Kirschfink, 1997). In his overview, Koehl (Hannover, Germany) focused on recent develop- ments in complement diagnosis, demonstrating that by applying a combination of affinity chromatogra- phy with immuno-assay procedures plasma concen- trations of anaphylatoxins can now be assessed within 20-30 min. This method fulfills the prerequisite for the introduction of complement analysis in intensive care units (Hartmann et al., 1993). Applying this novel assay to a recent polytrauma study (Hecke et al., 1997) and in patients with sepsis or SIRS (StiSve et al., 1996) it was demonstrated that C3a plasma levels correlated with the clinical outcome and helped to distinguish between patients with sepsis and those with SIRS.
2. Complement depletion by cobra venom factor
Cobra venom factor (CVF), a non-toxic protein in cobra venom, forms a stable bimolecular C3/C5 convertase (Fritzinger et al., 1994), which subse- quently leads to unrestricted complement consump- tion. For many years, complement depletion by CVF provided the only experimental means to analyse the significance of complement to inflammation (Coch- rane et al., 1970). As a 'gold standard', CVF is still used to comparatively evaluate the efficacy of most inhibitory molecules described in this overview. However, despite its capacity to exert significant protection in complement-mediated pulmonary in- jury (Ren et al., 1994; Dehring et al., 1987), experi- mental allergic neuritis (Vriesendorp et al., 1995), vasculitis (Mathieson et al., 1994) and hyperacute xenograft rejection (Gewurz et al., 1967; Chrupcala et al., 1994; Azimzadeh et al., 1996) the strong immunogenicity of purified CVF has hitherto pre- cluded its clinical application. The molecule has been cloned by Fritzinger et al. (1994) and modified recombinant forms of CVF may be generated which may become valuable for medical therapy.
3. Influence of synthetic compounds on comple- ment
A variety of synthetic compounds have been tested for their impact on the complement system. For example, 6-amidino-2-naphthyl-4-guanidinobenzoate (FUT-175), a synthetic serine proteinase inhibitor, was shown to also be a potent inhibitor of C ls, factor D and of C3/C5-convertase activity (Inagi et al., 1991). FUT-175 was successfully tested in ani- mal experiments of discordant xenotransplantation (Kobayashi et al., 1996), acute experimental pancre- atitis (Araida et al., 1995) and myocardial ischemia/reperfusion injury (Homeister and Lucch- esi, 1994). Upon administration of FUT-175 to glomerulonephritic patients with hypocomple- mentemia, serum complement levels improved and proteinuria was significantly reduced (Fujita et al., 1993). In a clinical trial on subarachnoid hemor- rhage, FUT-175 significantly reduced the incidence of cerebral infarction (Yanamoto et al., 1992). How- ever, it is not clear yet what the relative contribution

54 M. Kirschfink / lmmunopharmacology 38 (1997) 51-62
of complement inhibition is to an improvement of the clinical outcome.
The sulfonated dextran polymer (CMDBS25) in- terferes with the assembly of the classical and alter- native C3 convertases (Crepon et al., 1987). In a previous animal experiment the dextran derivative was shown to exhibit potent inhibitory activity to- wards complement activation in vivo (Thomas et al., 1995). In an in vitro model of hyperacute xenograft rejection porcine endothelial cells were protected against the deleterious attack of human complement (Thomas et al., 1996).
In general, most of the known synthetic comple- ment inhibitors are either toxic, not complement- specific, or require unrealistically high concentra- tions to inhibit complement in vivo (Asghar, 1984).
4. Immunogiobulins as a scavenger for activated complement
The intravenous application of immunoglobulin (IVIG) has been used as a therapy in various dis- eases, some of them known to be based on type II hypersensitivity reactions induced by antibody and complement (Mouthon et al., 1996). Supraphysiolog- ical doses of Ig have been shown to significantly increase the survival rate in experimental Forssman shock (Basta et al., 1989) and to prevent hyperacute rejection of porcine hearts transplanted into nonhu- man primates (Magee et al., 1995). It appears that lg in high concentration acts as a scavenger for acti- vated C3 and C4, thereby preventing the cascade reaction from taking place on the host tissue. The inhibitory activity appears to be most pronounced in a mixture of Igs of different isotypes (Miletic et al., 1996). High-dose intravenous Ig has been shown to be benefical in patients suffering from dermato- myositis. Immunohistochemical analysis revealed a significantly reduced deposition of C3b and C5b-9 in endomysial capillaries (Basta and Dalakas, 1994). According to Lutz et al. (1996), high dose IgG not only displaces C3b from its target, but also augments factor 1-dependent inactivation of C3b2-IgG com- plexes in vivo, thereby attenuating complement acti- vation via the amplification loop. There is increasing evidence that rapid clinical improvement in patients with systemic vasculitis (Gross, 1994), Kawasaki
syndrome (Newburger et al., 1986) or the bullous pemphigoid (Stiehm et al., 1987) may at least in part be due to the complement modulatory effect of high doses of immunoglobulin.
5. Support of physiologic complement regulation
Due to their high specificity and the absence of toxic side effects, the introduction of endogenous complement inhibitors appears to be a logical ap- proach to blocking the complement system in vivo.
Cl-inhibitor is a member of the superfamily of serine protease inhibitors (serpins, Carrell and Boswell, 1986). It is a major regulator of comple- ment (Clr, Cls) as well as of the contact phase of coagulation (factor XI, factor XII) and of kallikrein, thus controlling the generation of kinin-like molecules (Schapira et al., 1985).
Based on the hypothesis that in sepsis a relative deficiency of C 1-inhibitor might contribute to the development of fatal complications, substitution with this regulatory protein has been found to be of advantage for the clinical outcome. Hack (Amster- dam, Netherlands) summarized the development of C 1-inhibitor therapy from its primary indication as an acute treatment in hereditary angioedema (Gadek et al., 1980; Bork and Witzke, 1988) to its applica- tion in cases of fulminant inflammation. High doses of Cl-inhibitor were safely administered to patients with septic shock, or in cases of capillary leak syndrome associated with I1-2 therapy and this led to attenuation of complement system activation (Hack et al., 1993). Cl-inhibitor concentrate has also been applied successfully in capillary leak syndrome after bone marrow transplantation (Niirnberger and Gt~bel, 1996) as reported by Niirnberger (Diisseldorf, Ger- many). Administration of C 1-inhibitor to children undergoing open-heart surgery, who developed the capillary leak syndrome, substantially improved clin- ical, hemodynamic and respiratory parameters (Stieh et al., 1996). A cardioprotective effect of Cl-inhibi- tor was observed in a cat model of myocardial ischemia and reperfusion (Buerke et al., 1995) and was effective in animal models of endotoxin-induced organ dysfunction (Guerrero et al., 1993) and burn injury (Radke et al., 1995). Recent data from a clinical study in burn patients suggest a favorable

M. Kirschfink / Immunopharmacology 38 (1997) 51-62 55
effect of C 1-inhibitor treatment (A. Janssen, Mar- burg, Germany). The expanding field of clinical indications for Cl-inhibitor therapy has recently been discussed in a workshop held in Diisseldorf, Ger- many, 1996 (for overview see: Biomedical Progress, 9, Suppl. 1, 1996). Although the impact of Cl-inhibi- tor on complement is restricted to the classical path- way, its regulatory function in the coagulation sys- tem offers certain advantages in situations such as septic shock where activation of either system is associated with a poor clinical outcome (Nuijens et al., 1988).
Complement receptor 1 (CR1, CD35) is a single- chain membrane-bound glycoprotein with a dual function. It mediates phagocytosis of C3b-opsonized targets and serves as a potent regulator of C3 and C5 activation (Fearon, 1979). CR1 binds C3b and C4b, exerts cofactor activity for factor-I mediated prote- olytic degradation of these molecules and accelerates the decay of both the classical and the alternative C3/C5 convertases. The extramembraneous part of CR1 was isolated from plasma and shown to retain full regulatory activity. A truncated soluble molecule, lacking the transmembrane and cytoplasmic domains was prepared from CHO cells transfected with a modified CR1 cDNA (Weisman et al., 1990). The recombinant soluble complement receptor 1 (sCR1) inhibits both the alternative and classical pathway activation in whole serum in a nanomolar concentra- tion range and was found to be 100-fold more effec- tive than the endogenous C3/C5 convertase in- hibitors C4bp and factor H (Fearon, 1991). Serving as a cofactor for the serum protease factor I, sCR1 further promotes the degradation of C3b and C4b to inactive forms which no longer bind to sCR1, releas- ing the regulator to recycle in the inactivation pro- cess.
U.S. Ryan (Needham, MA, USA) reviewed the abundant data on the application of sCR1 in various animal models of inflammatory diseases. After prov- ing that sCR1 is well tolerated by humans, phase II clinical trials are currently in progress to evaluate its therapeutical potential in patients with established adult respiratory distress syndrome, myocardial in- farction and to prove its efficacy in reperfusion injury subsequent to lung transplantation.
In numerous animal models, the application of sCR1 significantly reduced complement-mediated
tissue damage, as shown for myocardial (Weisman et al., 1990; Homeister and Lucchesi, 1994), intestinal (Hill et al., 1992) and hepatic (Jaeschke et al., 1993; Chavez Cartaya et al., 1995) ischemia/reperfusion injury. Benefical effects of sCR1 treatment were also reported for reverse passive Arthus reaction (Yeh et al., 1991), ARDS (Rabenovici et al., 1992), comple- ment-mediated experimental glomerulonephritis (Couser et al., 1995) and demyelinating experimental allergic encephalitis (Piddlesden et al., 1994).
Despite its rare occurrence, hyperacute graft rejec- tion, which is mediated by the action of natural antibodies and complement, is a significant problem in transplantation surgery. In addition, it represents the major barrier to xenotransplantation, which is frequently discussed as a potential solution to the shortage of human donor organs (Platt and Bach, 1991).
In several models of allogeneic and xenogeneic organ transplantation it could be demonstrated that pretreatment of the recipient with sCR1 significantly prolonged survival of heart (Pruitt and Bollinger, 1991) and kidney (Chrupcala et al., 1994) trans- plants.
The problem of a rapid clearance of therapeutic reagents like sCR1 from the blood may be solved by creating chimeric proteins of the inhibitory molecules and other proteins having longer half-lives, such as immunoglobulins (Kalli et al., 1991).
A simultaneous inhibition of complement and cell adhesion was suggested by U.S. Ryan (Needham) to improve anti-inflammatory therapy. The incorpora- tion into sCR1 of the seLe ~ oligosaccharide, the common carbohydrate ligand for the P-, E- and L-selectin adhesion molecules, would allow the com- bined inhibition of complement activation and se- lectin-mediated cellular interaction.
In order to overcome complement-mediated hy- peracute rejection of discordant xenografts (for re- view see: Dalmasso, 1992) human membrane-asso- ciated regulatory proteins have been transferred onto xenogeneic tissue. Dalmasso et al. (1991) were able to demonstrate that human DAF can be directly inserted by its GPI-anchor into porcine endothelial cell membranes, thereby preventing lysis of the cells by human complement. Subsequently, protection of xenogeneic cells was achieved by transfection with cDNA of human MCP, DAF or CD59. In a recent

56 M. Kirschfink / lmmunopharmacology 38 (1997) 51-62
series of experiments we demonstrated that transfec- tion of porcine endothelial cells with human CD59 by itself or in combination with soluble regulators effectively inhibited cell destruction by human serum complement (Heckl-Ostreicher et al., 1996). Kooy- man et al. (1995) were able to show that GPI-linked complement regulatory proteins expressed on the surface of transgenic mouse or pig erythrocytes can be transferred in an active form to vascular endothe- lium in vivo. A major step forward towards the clinical application of xenotransplantation was the generation of transgenic donor animals that express human complement inhibitor proteins on their tissue (Cozzi and White, 1995; Byrne et al., 1996; Kroshus et al., 1996). Quantitative analysis of the human regulator DAF in different pig organs displayed an expression level which was comparable or even higher than on normal human endothelium (Langford et al., 1994). Morphologic and functional analysis revealed that in xenoperfused hDAF/hCD59 trans- genic pig hearts (Schmoeckel et al., 1996; Kroshus et al., 1996; Byrne et al., 1997) and kidneys (Storck et al., 1997) the human regulators were sufficiently expressed to inhibit complement activation and to significantly reduce morphologic alterations indica- tive of hyperacute graft rejection.
6. Blocking complement components
By inhibition of the complement cascade reaction at C5, the formation of the membrane attack com- plex is blocked and the generation of the proinflam- matory peptide C5a is abolished. Y. Wang (New Haven, CT, USA) presented two murine preclinical models of systemic lupus erythematosus and rheuma- toid arthritis. Treatment with monoclonal anti-C5 antibodies resulted in a marked amelioration of the course of renal disease (Wang et al., 1996) and of joint inflammation (Wang et al., 1995), respectively. For clinical application, from the monoclonal anti- body N19-8, developed and characterized by Wiirzner et al. (1991), a humanized single chain anti-C5 anti- body (h5Gl.lscFv) has been constructed (Evans et al., 1995) and shown to be a potent inhibitor of complement as well as of platelet and leukocyte activation in an in vitro model of extracorporeal circulation relevant to cardiopulmonary bypass
(CPB). Pharmacokinetic and pharmacodynamic data from a phase I clinical trial indicate that a single bolus of the humanized anti-C5 scFv may suffi- ciently block complement activation during CPB (Rollins et al., 1997). Anti-C5 scFv may also provide an alternative approach to the treatment of immune complex mediated tissue inflammation. In previous experiments, Rollins et al. (1995) demonstrated that by the addition of monoclonal anti-C5 and anti-C8 IgG isolated rat hearts perfused with human serum were protected against complement-mediated organ damage. Addition of anti-C5 IgG to human blood used to perfuse porcine hearts ex vivo prevented acute tissue injury (Kroshus et al., 1995). Adminis- tration of various monoclonal antibodies against rat C3 led to increased survival time of guinea pig hearts transplanted into rats (Kemp et al., 1994).
7. Inhibition of the anaphylatoxin C5a
With respect to its diverse biological functions, the complement-derived anaphylatoxin C5a is con- sidered to be one of the most potent phlogistic peptides (Hugli, 1986). Inflammatory cells react to nanomolar concentrations of C5a with chemotaxis, upregulation of adhesion molecules and the release of destructive oxygen radicals and lysosomal pro- teases. Mice, defective in C5 and thereby unable to generate C5a upon complement activation, have been shown to be protected in septic shock (Hsueh et al., 1990). M. Oppermann (Gottingen, Germany) sum- marized current data on anti-C5a treatment, pointing to conflicting results from different animal studies. In two models of septic shock, by the prophylactic administration of anti-C5a antibodies, the mortality rate was significantly reduced and the animals showed a considerable improvement of their hemo- dynamic condition (Stevens et al., 1986; Smedegard et al., 1989). In contrast, monoclonal antibodies di- rected against a porcine C5a/C5adesArg neoepitope had no beneficial effect on mortality and organ function in a pig septic model. However, upon anti- C5a treatment, significantly less 11-6 was generated, supporting the notion of an immunoregulatory role of C5a (Htipken et al., 1996). As outlined by G.O. Till (Ann Arbor, MI, USA), anti-rat C5a efficiently blocked complement (C5a)-mediated upregulation of

M. Kirschfink / Immunopharmacology 38 (1997) 51-62 57
lung vascular ICAM-1 and P-selectin in two rat models of lung vascular injury (Mulligan et al., 1997).
Synthetic C5a analogues are considered valuable tools in analyzing C5a-mediated cell activation. However, the design of low molecular weight antag- onists generated to interfere with the high affinity binding of C5a to its receptor (CD88) is still a challenging problem (Kaneko et al., 1995). Neutral- izing anti-C5a antibodies (Ames et al., 1994; Opper- mann et al., 1993; Kola et al., 1996), anti-C5a receptor antibodies (Morgan et al., 1993), or in- hibitors of C5a receptor binding, such as substituted 4,6-diaminoquinolines (Lanza et al,, 1992), may pro- vide further avenues for reducing the impact of the anaphylatoxin on inflammation.
8. Interference with leukocyte adhesion
The complement receptors CR3 and CR4 (CD18/CDllb,c) , members of the /32 integrin fam- ily, promote adhesive interactions of leukocytes with the vascular endothelium. As an 'experiment of na- ture' the leukocyte adhesion deficiency syndrome (LAD), caused by an inherited deficiency of the leukocyte /32 integrin receptor CD11/CD18 in man (Harlan, 1993) and cattle (Kehrli et al., 1990), has provided important insights into the molecular basis of leukocyte recruitment from the circulation to ex-
travascular sites of inflammation. Adhesion molecules are recognized as key determinants of the inflammatory response (Mulligan et al., 1993a,b) and have therefore gained considerable interest as targets of antiphlogistic therapy.
The role of /32 integrins in lung injury has been determined by the application of blocking antibodies. Anti-CD18 and anti-CD1 lb antibodies reduced com- plement-mediated lung injury either induced by CVF or by immune complexes (Mulligan et al., 1993a,b). Early treatment with anti-CDllb also substantially increased survival of rats with experimental allergic encephalitis (Huitinga et al., 1993) and protected dogs from myocardial reperfusion injury (Simpson et al., 1988). Furthermore, monoclonal antibodies di- rected against CD18 were shown to reduce vascular rejection in a rabbit heterotopic heart transplant model (Sadahiro et al., 1993).
9. Complement inhibition on blood-interacting biomaterials
The inflammatory response induced by artificial surfaces in hemodialysis and extracorporeal circuits may lead to organ dysfunction. Complement activa- tion has been shown to be associated with transient neutropenia, pulmonary vascular leukostasis and oc- casionally anaphylactic shock of varied severity in patients undergoing hemodialysis (Johnson, 1994) or cardiopulmonary bypass (Chenoweth, 1986; Gardi-
Table l Strategies of complement inhibition
Reagent Clinical application (man)/animal models
CVF IgG Dextran derivatives FUT-175 C 1-inhibitor rsCR1
rsDAF Anti-C3 Anti-C5 Anti-C5a Anti-CD18/1 lh,c (Anti- CR3/CR4) DAF, CD59 (genetransfer)
ARDS, experimental allergic neuritis, hyperacute graft rejection (xenotransplantation) dermatomyositis, pemphigoid (man), Forssman shock, hyperacute graft rejection (xenotransplantation) hyperacute graft rejection (xenotransplantation) glomernlonephritis, ischemia/reperfusion injury, hyperacute graft rejection (xenotransplantation) septic shock, burn, capillary leak syndrome (man), hyperacute graft rejection (xenotransplantation) ARDS, lung transplantation (man), hyperacute graft rejection (xenotransplantation) Guillain-Barr6 syndrome, multiple sclerosis, ischemia/reperfusion injury, reverse passive Arthus reaction, cardiopulmonary bypass reverse passive Arthus reaction hyperacute graft rejection (xenotransplantation) glomerulonephritis, rheumatoid arthritis, SLE, cardiopulmonary bypass septic shock, lung injury lung injury, hyperacute graft rejection
hyperacute graft rejection (xenotransplantation)

58 M. Kirschfink / lmmunopharmacology 38 (1997) 51-62
classical pathway _ __ alternative pathway I I I D A F g , M c p g I I _ _
~ . P
CSa
C5b-9 anti-C5a C5aRAntag.
Fig. 3. Therapeutic control of the complement reaction may be possible by the application of physiological regulatory proteins, the administration of blocking antibodies, or, with respect to xenotransplantation, by genetransfer (e.g. CD59g). C5aRAntag., C5a receptor antagonist.
nali et al., 1986). Biomedical polymers considerably differ in their capacity to activate complement (Janatova et al., 1991). It is therefore accepted that evaluation of biocompatibility of artificial surfaces has to include the analysis of activation of both the coagulation and complement systems (Cheung, 1994; Mollnes et al., 1995). Heparin with its well-known anticoagulatory effect is also considered a potent inhibitor of the complement system, especially if it is bound to the surface of an activator (Cheung et al., 1992; Edens et al., 1993). Mollnes (Bode, Norway) summarized data on the substantial improvement of biocompatibility of CPB devices upon end-point at- tachment of heparin to the surfaces of a extracorpo- real circuit as tested in animal experiments and in vitro with human blood in closed circuits (Kirschfink et al., 1993; Redmond et al., 1993; Mollnes, 1997). A recent clinical study with patients randomized to operation with either uncoated or heparin-coated sur- faces demonstrated a significant reduction of com- plement activation accompanied by an attenuation of the leukocyte integrin and selectin response (Moen et al., 1997). Alternatively or in addition, complement activation by CPB devices may be reduced by the application of anti-C5 scFv (Rollins et al., 1997) or sCR1 (Gillinov et al., 1993
10. Conclusion
Stimulated by promising results from experimen- tal and first clinical studies (Table 1), research insti-
tutions and industry are pursuing strategies to inhibit complement activation as a novel therapeutic ap- proach for many inflammatory diseases. Further- more, effective complement inhibition may provide an avenue for successful xenotransplantation. How- ever, drug designers and clinicians must take into consideration that the effective systemic inhibition of complement will deprive the patient of an important immunological defense system.
Double-blinded controlled clinical trials are needed to definitively prove the therapeutic potential of targeted complement inhibition (Fig. 3) to reduce morbidity and mortality.
References
Ames, R.S., Tometta, M.A., Jones, C.S., Tsui, P., 1994. Isolation of neutralizing anti-C5a monoclonal antibodies from a fila- mentous phage monovalent Fab display library. J. Immunol. 152, 4572-4581.
Araida, T., Frey, C.F., Ruebner, B., Carlson, J., King, J., 1995. Therapeutic regimens in acute experimental pancreatitis in rats: Effects of a protease inhibitor, a beta-agonist, and antibi- otics. Pancreas 11, 132-140.
Asghar, S.S., 1984. Pharmacological manipulation of complement system. Pharm. Rev. 36, 223-244.
Azimzadeh, A., Wolf, P., Dalmasso, A.P., Odeh, M., Belier, J.P., Fabre, M., Charreau, B., Thibaudeau, K., Cinqualbre, J., Soulillou, J.P., Anegon, I., 1996. Assessment of hyperacute rejection in a rat-to-primate cardiac xenograft model. Trans- plantation 61, 1305-1313.
Basta, M., Dalakas, M.C., 1994. High-dose intravenous immuno- globulin exerts its beneficial effect in patients with dermato-

M. Kirschfink / lmmunopharmacology 38 (1997) 51-62 59
myositis by blocking endomysial deposition of activated com- plement fragments. J. Clin. Invest. 94, 1729-1735.
Basta, M., Kirschbom, P., Frank, M.M., Fries, L.F., 1989. Mecha- nism of therapeutic effect of high-dose intravenous immuno- globulin. Attenuation of acute complement-dependent immune damage in a guinea pig model. J. Clin. Invest. 84, 1974-1981.
Bork, K., Witzke, G., 1988. Long-term prophylaxis with Cl-in- hibitor (C1 INH) concentrate in patients with recurrent an- gioedema caused by hereditary and acquired Cl-inhibitor defi- ciency. J. Allergy Clin. Immunol. 63, 677-682.
Buerke, M., Murohara, T., Lefer, A.M., 1995. Cardioprotective effects of a C1 esterase inhibitor in myocardial ischemia and reperfusion. Circulation 91,393-402.
Byrne, G.W., McCurry, K.R., Martin, M.J., Platt, J.L., Logan, J.S., 1996. Development and analysis of transgenic pigs ex- pressing the human complement regulatory protein CD59 and DAF. Transplant. Proc. 28, 759.
Byrne, G.W., McCurry, K.R., Martin, M.J., McClellan, S.M., Platt, J.L., Logan, J.S., 1997. Transgenic pigs expressing human CD59 and decay-accelerating factor produce an intrin- sic barrier to complement-mediated damage. Transplantation 63, 149-155.
Carrell, R.W., Boswell, D.R., 1986. Serpins: The superfamily of plasma serine protease inhibitors. In: Barret, A.J., Salvese, G. (Eds.), Proteinase Inhibitors. Elsevier, Amsterdam, pp. 403- 420.
Carroll, M.C., Fischer, M.B., 1997. Complement and the immune response. Curr. Opin. Immunol. 9, 64-69.
Chavez Cartaya, R.E., DeSola, G.P., Wright, L., Jamieson, N.V., White, D.J., 1995. Regulation of the complement cascade by soluble complement receptor type 1. Protective effect in exper- imental liver ischemia and reperfusion. Transplantation 59, 1047-1052.
Chenoweth, D.E., 1986. Anaphylatoxin formation in extracorpo- real circuits. Complement 3, 152-165.
Cheung, A.K., 1994. Complement activation as index of hemodialysis membrane biocompatibility: The choice of meth- ods and assays. Nephrol. Dial. Transplant. 9, 96-103.
Cheung, A.K., Parker, C.J., Janatova, J., Brynda, E., 1992. Modu- lation of complement activation on hemodialysis membranes by immobilized heparin. J. Am. Soc. Nephrol. 2, 1328-1337.
Chrupcala, M., Pomer, S., Staehler, G., Waldherr, R., Kirschfink, M., 1994. Prolongation of discordant renal xenograft survival by depletion of complement. Comparative effects of systemi- cally administered cobra venom factor and soluble comple- ment receptor type 1 in a guinea pig-to-rat model. Transplant. Int. 7, 650-653.
Cochrane. C.G., Miiller-Eberhard, H.J., Aikin, B.S., 1970. Deple- tion of plasma complement in vivo by a protein of cobra venom: Its effect on various immunologic reactions. J. Im- munol. 105, 55-69.
Cooper, N.R., Nemerow, G.R., Mayes, J.T., 1983. Methods to detect and quantitate complement activation. Springer Semin. Immunopathol. 6, 195-212.
Couser, W.G., Johnson, R.J., Young, B.A., Yeh, C.G., Toth, C.A., Rudolph, A.R., 1995. The effects of soluble recombinant
complement receptor 1 on complement-mediated experimental glomerulonephritis. J. Am. Soc. Nephrol. 5, 1888-1894.
Cozzi, E., White, D.J., 1995. The generation of transgenic pigs as potential organ donors for humans. Nat. Med. 1,964-966.
Crepon, B., Maillet, F., Kazatchkine, M.D., Jozefonvicz, J., 1987. Molecular weight dependency of the acquired anti-comple- mentary and anticoagulant activities of specifically substituted dextrans. Biomaterials 8, 248-253.
Dalmasso, A.P., 1986. Complement in the pathophysiology and diagnosis of human diseases. Crit. Rev. Clin. Lab. Sci. 24, 123-183.
Dalmasso, A.P., 1992. The complement system in xenotransplan- tation. Immunopharmacology 24, 149-160.
Dalmasso, A.P., Vercellotti, G.M., Platt, J.L., Bach, F.H., 1991. Inhibition of complement-mediated endothelial cell cytotoxic- ity by decay-accelerating factor. Transplantation 52, 530-533.
Dehring, D.J., Steinberg, S.M., Wismar, B.L., Lowery, B.D., Carey, L.C., Cloutier, C.T., 1987. Complement depletion in a porcine model of septic acute respiratory disease. J. Trauma 27, 615-625.
Devine, D.V., 1991. The regulation of complement on cell sur- faces. Transfusion Med. Rev. V, 123-131.
Edens, E.R., Linhardt, R.J., Weiler, J.M., 1993. Heparin is not just an anticoagulant anymore: Six and one-half decades of studies on the ability of heparin to regulate complement activity. In: Cruse, J.N., Lewis, R.E., Jr. (Eds.), Complement Today. Karger, Basel, pp. 96-120.
Evans, M.J., Rollins, S.A., Wolff, D.W., Rother, R.P., Norin, A.J., Therrien, D.M. et al., 1995. In vitro and in vivo inhibi- tion of complement activity by a single chain Fv fragment recognizing human C5. Mol. Immunol. 32, 1183-1195.
Fearon, D.T., 1979. Regulation of the amplification C3 convertase of human complement by an inhibitory protein isolated from human erythrocyte membranes. Proc. Natl. Acad. Sci. USA 76, 5867-5871.
Fearon, D.T., 1991. Anti-inflammmatory and immunosuppressive effects of recombinant soluble complement receptors. Clin. Exp. Immunol. 86, 43-46.
Fritzinger, D.C., Bredehorst, R., Vogel, C.W., 1994. Molecular cloning and derived primary structure of cobra venom factor. Proc. Natl. Acad. Sci. USA 91, 12775-12779.
Fujita, Y.. Inoue, I., Inagi, R., Miyata, T., Shinzato, T., Sugiyama, S., Miyama, A., Maeda, K., 1993. Inhibitory effect of FUT-175 on complement activation and its application for glomerulo- nephritis with hypocomplementemia. Nippon Jinzo Gakkai Shi 35, 393-397.
Gadek, J.E., Hasea, S.W., Gelfand, J.A., Santaella, M., Wicker- hauser, M., Triantaphyllopoulos, D.C., Frank, M.M., 1980. Replacement therapy in hereditary angioedema. Successful treatment of acute episodes of angioedema with partly purified CI inhibitor. N. Engl. J. Med. 302, 542-546.
Gardinali, M., Cicardi, M., Agostoni, A., Hugli, T.E., 1986. Complement activation in extracorporeal circulation: Physio- logical and pathological implications. Pathol. Immunopathol. Res. 5, 352-370.
Gewurz, H., Clark, D.S., Cooper, M.D., Varco, R., Good, R.A.,

60 M. Kirschfink / lmmunopharmacology 38 (1997) 51-62
1967. Effect of cobra venom-factor induced inhibition of complement activity on allograft and xenograft rejection reac- tions. Transplantation 5, 1296-1303.
Gillinov, A.M., Devaleria, P.A., Winkelstein, J.A., Wilson, I_ Curtis, W.E., Shaw, D. et al., 1993. Complement inhibition with soluble complement receptor type 1 in cardiopulmonary bypass. Ann. Thorac. Surg. 55, 619-624.
Gross, W.L., 1994. New developments in the treatment of sys- temic vasculitis. Curr. Opin. Rheumatol. 6, 11-19.
Guerrero, R., Velasco, F., Rodriguez, M., Lopez, A., Rojas, R., Alvarez, M.A., Villalba, R., Rubio, V., Torres, A., del Castillo, D., 1993. Endotoxin-induced pulmonary dysfunction is pre- vented by C l-esterase inhibitor. J. Clin. Invest. 91, 2754-2760.
Hack, C.E., Ogilvies, A.C., Eisele, B., Eerenberg, A.J.M., Wagstaff, J., Thijs, L.G., 1993. Cl-inhibitor substitution ther- apy in septic shock and in the vascular leak syndrome induced by high doses of interleukin-2. Intensive Care Med. 19, 19-28.
Harlan, J., 1993. Leukocyte adhesion deficiency syndrome: In- sights into the molecular basis of leukocyte emigration. Clin. Immunol. Immunopathol. 67, 16-24.
Hartmann, H., LUbbers, B., Casaretto, M., Bautsch, W., Klos, A., Ktihl, J., 1993. Rapid quantification of C3a and C5a using a combination of chromatographic and immunoassay procedure. J. Immunol. Methods 166, 35-44.
Hecke, F., Schmidt, U., Kola, A., Bautsch, W., Klos, A., K~ihl, J., 1997. Analysis of complement proteins in polytrauma pa- tients-correlation with injury severity, sepsis, and outcome. Shock 7, 74.
Heckl-Ostreicher, B., Wosnik, A., Kirschfink, M., 1996. Protec- tion of porcine endothelial cells from complement-mediated cytotoxicity by the human complement regulators CD59, CI inhibitor and soluble complement receptor 1: Analysis in a pig-to-human in vitro model relevant to hyperacute rejection. Transplantation 62, 1-3.
Hill, J., Lindsay, T.F., Ortiz, F., Yeh, C.G., Hechtman, H.B., Moore, F.D. Jr., 1992. Soluble complement receptor type 1 ameliorates the local and remote organ injury after intestinal ischemia-reperfusion in the rat. J. lmmunol. 149, 1723-1728.
Homeister, J.W., Lucchesi, B.R., 1994. Complement activation and inhibition in myocardial ischemia and reperfusion injury. Annu. Rev. Pharmacol. Toxicol. 34, 17-40.
Hrpken, U., Mohr, M., Struber, A., Montz, H., Burchardi, H., GiStze, O., Oppermann, M., 1996. Inhibition of interleukin-6 synthesis in an animal model of septic shock by anti-C5a monoclonal antibodies. Eur. J. Immunol. 26, 1103-1109.
Hsueh, W., Sun, X., Rioja, L.N., Gonzalez-Crussi, F., 1990. The role of the complement system in shock and tissue injury induced by tumor necrosis factor and endotoxin. Immunology 70, 309-314.
Hugli, T.E., 1986. Biochemistry and biology of anaphylatoxins. Complement 3, 111-127.
Huitinga, 1., Damoiseaux, J.G.M.C., Drpp, E.A., Dijkstra, C.D., 1993. Treatment with anti-CR3 antibodies ED7 and ED8 suppresses experimental allergic encephalomyelitis in Lewis rats. Eur. J. Immunol. 23, 709-715.
Inagi, R., Miyata, T., Maeda, K., Sugiyama, S., Miyama, A., Nakashima, I., 1991. FUT-175 as a potent inhibitor of C5/C3
convertase activity for production of C5a and C3a. Immunol. Lett. 27, 49-52.
Jaeschke, H., Farhood, A., Bautista, A.P., Spolarics, Z., Spitzer, J.J., 1993. Complement activates Kuffer cells and neutrophils during reperfusion after hepatic ischemia. Am. J. Physiol. 264, 801 - 809.
Janatova, J., Cheung, A., Parker, C.J., 1991. Biomedical polymers differ in their capacity to activate complement. Complement Inflamm. 8, 61-69.
Johnson, R.J., 1994. Complement activation during extracorporeal therapy: Biochemistry, cell biology and clinical relevance. Nephrol. Dial. Transplant. 9, 36-45.
Kalli, K.R., Bartow, T.J., Hsu, P., Klickstein, L.B., Ahearn, J.M., Matsumoto, A., Fearon, D.T., 1991. Mapping of the C3b-bind- ing site of CR1 and construction of a chimeric complement inhibitor. Complement Inflamm. 8, 171.
Kehrli, M.E., Schmalstieg, F.C., Anderson, D.C., van der Marten, M.J., Hughes, B.J. et al., 1990. Molecular definition of the bovine granulocythopathy syndrome: Identification of defi- ciency of the Mac-1 (CDIlb/CD18) glycoprotein. Am. J. Vet. Res. 51, 1826-1836.
Kemp, R.E., Dieperink, P., Leth, P., Jesenius, J.C., Nielsen, B., Lillevang, S.T., Salomon, S., Steinbriichel, D., Larsen, S., Koch, C., White, D., 1994. Monoclonal antibodies to comple- ment C3 prolong survival of discordant xenografts: guinea pig heart to rat transplantation. Transplant. Proc. 26, 1011-1015.
Kirschfink, M., 1997. The clinical laboratory: Testing the comple- ment system. In: Rother, K., H~insch, G.M., Till, G. (Eds.), The Complement System. Springer, Heidelberg/New York, in press.
Kirschfink, M., Kovacs, B., Mottaghy, K., 1993. Extracorporeal circulation: In vivo and in vitro analysis of complement activation by heparin-bonded surfaces. Circ. Shock 40, 221- 226.
Kirschfink, M,, Wienert, T., Rother, K., Pomer, S., 1992. Comple- ment activation in renal allograft recipients. Transpl. Proc. 24, 2556-2557.
Kaneko, Y., Okada, N., Baranyi, L., Azuma, T., Okada, H., 1995. Antagonistic peptides against human anaphylatoxin C5a. Im- munology 86, 149-154.
Kobayashi, T., Neethling, F.A., Koren, E,, Taniguchi, S., Ye, Y., Niekrasz, M., Takagi, H., Hancock, W.W., Cooper, D,K., 1996. In vitro and in vivo investigation of anticomplement agents FUT-175 and K76COOH, in the prevention of hypera- cute rejection following discordant xenotransplantation in a nonhuman primate model. Transplant. Proc. 28, 604.
Kola, A.. Baensch, M., Bautsch, W., Hennecke, M., Klos, A., Casaretto, M., KiShl, J., 1996. Epitope mapping of a C5a neutralizing mAb using a combined approach of phage dis- play, synthetic peptides and side-directed mutagenesis. Im- munotechnology 2, 115-126.
Kooyman, D.L., Byrne, G.W., McClellan, S., Nielsen, D., Tone, M., Waldmann, H., Coffman, T.M., McCurry, K.R., Platt, J.L., Logan, J.S., 1995. In vivo transfer of GPI-linked comple- ment restriction factors from erythrocytes to the endothelium. Science 269, 89-92.
Kroshus, T.J., Bolman, R.M. III, Dalmasso, A.P., Rollins, S.A.,

M. Kirschfink / lmmunopharmacology 38 (1997) 51-62 61
Guilmette, E.R., Williams, B.L., Squinto, S.P., Fodor, W.L., 1996. Expression of human CD59 in transgenic pig organs enhances organ survival in an ex vivo xenogeneic perfusion model. Transplantation 61, 1513-1521.
Kroshus, T.J., Rollins, S.A., Dalmasso, A.P., Elliott, E.A., Matis, L.A., Squinto, S.P., Bolman, R.M., 1995. Complement inhibi- tion with an anti-C5 monoclonal antibody prevents acute cardiac tissue injury in an ex vivo model of pig-to-human xenotransplantation. Transplantation 60, 1194-1202.
Langford, G.A., Yannoutsos, N., Cozzi, E., Lancaster, R., Elsome, K., Chen, P., Richards, A., White, D.J.G., 1994. Production of pigs transgenic for human decay accelerating factor. Trans- plant. Proc. 26, 1400-1401.
Lanza, T.J., Durette, P.L., Rollins, T., Siciliano, S., Cianciarulo, D.N., Kobayashi, S.V., Caldwell, C.G., Springer, M.S., Hag- mann, W.K., 1992. Substituted 4,6-diaminoquinolines as in- hibitors of C5a receptor binding. J. Med. Chem. 35, 252-258.
Lutz, H.U., Stammler, P., Jelezarova, E., Nater, M., Sp~ith, P.J., 1996. High doses of immunoglobulin G attenuate immune aggregate-mediated complement activation by enhancing phys- iologic cleavage of C3b in C3bn-IgG complexes. Blood 88, 184-193.
Magee, J.C., Collins, B.H., Harland, R.C., Lindman, B.J., Bollinger, R.R., Frank, M.M., Platt, J.L., 1995. Immunoglobu- lin prevents complement-mediated hyperacute rejection in swine-to-primate xenotransplantation. J. Clin. Invest. 96, 2404- 2412.
Mathieson, P.W., Qasim, F.J., Thiru, S., Oldroyd, R.G., Oliveira, D.B., 1994. Effects of decomplementation with cobra venom factor on experimental vasculitis. Clin. Exp. Immunol. 97, 474-477.
Miletic, V.D., Hester, C.G., Frank, M.M., 1996. Regulation of complement activity by immunoglobulin. I. Effect of immuno- globulin isotype on C4 uptake on antibody-sensitized sheep erythrocytes and solid phase immune complexes. J. Immunol. 156, 749-757.
Moen, O., H0gasen, K., Fosse, E., Dregelid, E., Brockmeier, V., Heggen, G. et al., 1997. Attenuation of changes in leukocyte surface markers and complement activation with heparin- coated cardiopulmonary bypass. Ann. Thorac. Surg., in press.
Mollnes, T.E., 1997. Biocompatibility: Complement as a mediator of tissue damage and an indicator of incompatibility. Clin. Exp. Immunogenet. 14, 24-29.
Mollnes, T.E., Riesenfeld, J., Garred, P., NordstrOm, E., H0gasen, K., Fosse, E., G&ze, O., Harboe, M., 1995. A new model for evaluation of biocompatibility: Combined determination of neoepitopes in blood and on artificial surfaces demonstrates reduced complement activation by immobilization of hepafin. Artif. Organs. 19, 909-917.
Morgan, B.P., 1990. Complement. Clinical Aspects and Relevance to Disease. Harcourt Brace Jovanovich, London/New York.
Morgan, E.L., Ember, J.A., Sanderson, S.D., Scholz, W., Buch- ner, R., Ye, R.D., Hugli, T.E., 1993. Anti-C5a receptor anti- bodies. Characterization of neutralizing antibodies specific for a peptide, C5aR-(9-29), derived from the predicted amino- terminal sequence of the human C5a receptor. J. Immunol. 151,377-380.
Mouthon, L., Kaveri, S.V., SpaRer, S.H., Lacroix Desmazes, S.,
Lefranc, C., Desai, R., Kazatchkine, M.D., 1996. Mechanisms of action of intravenous immune globulin in immune-mediated diseases. Clin, Exp. Immunol. 104 (Suppl. 1), 3-9.
Miiller-Eberhard, H.J., 1988. Molecular organization and function of the complement system. Ann. Rev. Biochem. 57, 321-347.
Mulligan, M.S., Smith, C.W., Anderson, D.C., Todd, R.F., Miyasaka, M., Tamatani, T., Issekutz, T.B., Ward, P.A., 1993a. Role of leukocyte adhesion molecules in complement-induced injury. J. Immunol. 150, 2401-2406.
Mulligan, M.S., Wilson, G.P., Todd, R.F., Smith, C.W., Ander- son, D.C., Varani, J., lssekutz, T.B., Miyasaka, M., Tamatani, T., Rusche, J.R., Vaporciyan, A.A., Ward, P.A., 1993b. Role of /31 and /32 integrins and ICAM-1 in lung injury following deposition of IgG and IgA immune complexes. J. Immunol. 150, 2407-2417.
Mulligan, M.S., Schmid, E., Till, G.O., Hugli, T.E., Friedl, H.P., Roth, R.A., Ward, P.A., 1997. C5a-dependent up-regulation in vivo of lung vascular P-selecfin. J. Immunol. 158, 1857-1861.
Newburger, J.W., Takahashi, M., Bums, J.C., Beiser, A.S., Chung, K.J., Duffy, C.E. et al., 1986. The treatment of Kawasaki syndrome with intravenous gamma globulin. N. Engl. J. Med. 315, 341-347.
Niirnberger, W., Gtibel, U., 1996. Capillary leak syndrome follow- ing bone marrow transplantation. Biomed. Progr. 9, 8-11.
Nuijens, J.H., Huijbregts, C.C., Eerenberg-Belmer, A.J., Abbink, J.J., Strak van Schijndel, R.J., Felt-Bersma, R.J., Thijs, L.G., Hack, C.E., 1988. Quantification of plasma factor XIIa-Cl-in- hibitor and kallikrein-Cl-inhibitor complexes in sepsis. Blood 72, 1841-1848.
Oppermann, M., Raedt, U., Hebell, T., Schmidt, B., Zimmermann, B., Gtitze, O., 1993. Probing the human receptor for C5a anaphylatoxin with site-directed antibodies. Identification of a potential ligand binding site on the NH2-terminal domain. J. Immunol. 151, 3785-3794.
Piddlesden, S.J., Storch, M.K., Hibbs, M., Freeman, A.M., Lass- mann, H., Morgan, B.P., 1994. Soluble recombinant comple- ment receptor 1 inhibits inflammation and demyelination in antibody-mediated demyelinating experimental allergic en- cephalomyelitis. J. Immunol. 152, 5477-5484.
Platt, J.L., Bach, F.H., 1991. The barrier to xenotransplantation. Transplantation 52, 937-947.
Pruitt, S.K., Bollinger, R.R., 1991. The effect of soluble comple- ment receptor type 1 on hyperacute allograft rejection. J. Surg. Res. 50, 350-355.
Rabenovici, R., Yeh, C.G., Hillegass, L.M., Griswold, D.E., DiMartino, M.J., Vernick, J., Fong, K.L.L., Feuerstein, G., 1992. Role of complement in endotoxin/platelet-activating factor-induced lung injury. J. Immunol. 149, 1744-1750.
Radke, A., Mottaghy, K., Goldmann, Ch., Eisele, B., Hettich, R., Kirschfink, M., 1995. The protective effect of Cl-inhibitor on thermal trauma: First results from an animal study. In: Rous- sos C. (Ed.), 8th European Congress of Intensive Care Medicine. Mundozzi Editore, Bologna, pp. 761-769.
Redmond, J.M., Gillinov, M.A., Stuart, R.S., Zehr, K.J., Winkel- stein, J.A., Herskowitz, A. et al., 1993. Heparin-coated bypass circuits reduce pulmonary injury. Ann. Thorac. Surg. 56, 474-479.
Ren, X.D., Huang, S.J., Sun, J.J., Zhu, Z.G., 1994. Protective

62 M. Kirschfink / lmmunopharmacology 38 (1997) 51-62
effect of cobra venom factor on pulmonary injury induced by oleic acid. Int. J. Immunopharmacol. 16, 969-975.
Rollins, S.A., Matis, L.A., Springhorn, J.P., Setter, E., Wolff, D.W., 1995. Monoclonal antibodies directed against human C5 and C8 block complement-mediated damage of xenogeneic cells and organs. Transplantation 60, 1284-1292.
Rollins, S.A., Rinder, H.M., Rinder, C.S., Fitch, J.C.K., Smith, B.R., Hines, R.L., Alford, B.L., Matis, L.A., 1997. A human- ized anti-C5 scFv blocks platelet and leukocyte activation and exhibits prolonged pharrnacokinetics and pharmacodynamics in humans. Exp. Clin. Immunogenet. 14, 36.
Rother, K., Till, G.D., 1988. The Complement System. Springer, Berlin/Heidelberg/New York.
Rother, K., Rother, U., 1986. Hereditary and acquired comple- ment deficiencies in animals and man. Progress in Allergy, vol. 39. Karger, Basel/London/New York.
Sadahiro, M., McDonald, T.O,, Allen, M.D., 1993. Reduction in cellular and vascular rejection by blocking leukocyte adhesion molecule receptors. Am. J. Pathol. 142, 675-683.
Schapira, M., Agostoni de, A., Schifferli, J.A., Colman, R.W., 1985. Biochemistry and pathophysiology of human CI in- hibitor: Current issues. Complement 2, 111-126.
Schmoeckel, M., Nollert, G., Shahmohammadi, M., Young, V.K., Knig, W., White, D.J., Hammer, C., Reichart, B., 1996. Human decay accelerating factor successfully protects pig hearts from hyperacute rejection by human blood. Transplant. Prec. 28, 768-769.
Simpson, P.J., Todd, R.F. IlL Fantone, J.C., Mickelson, J.K., Griffin, J.D., Lucchesi, B,R., Adams, M.D., Hoff, P., Leeh, K., Rogers, C.E., 1988. Reduction of experimental canine reperfusion injury by a monoclonal antibody (anti-Mol, anti- CDIlb) that inhibits leukocyte adhesion. J. Clin. Invest. 81, 624-629.
Smedegard, G., Cui, L., Hugli, T.E., 1989. Endotoxin-induced shock in the rat. A role for C5a. Am. J. Pathol. 135, 489-497.
Stevens, J.H., O'Hanley, P., Shapiro, J.M., Mihm, F.G., Satoh, P.S., Collins, J.A., Raffin, T.A., 1986. Effects of anti-C5a antibodies on the adult respiratory distress syndrome in septic primates. J. Clin. Invest. 77, 1812-1816.
Stieh, J., Harding, P., Scheewe, J., Diitschke, P., Kramer, H.H., 1996. Capillary leak syndrome after open heart surgery lbr congenital heart defects: Therapy with Cl-inhibitor. Biomed. Progr. 9, 13-16.
Stiehm, E.R., Ashida, E., Kim, K,S., Winston, D.J., Haas, A., Gale, R.P., 1987. Intravenous immunoglobulins as therapeutic agents (clinical conference). Ann. Int. Med. 107, 367-382.
Strive, S., Welte, T., Wagner, T.O.F., Kola, A., Kits, A., Bautsch, W., K~hl, J., 1996, Circulating complement proteins in pa- tients with sepsis or systemic inflammatory response syn- drome. Clin. Diagn. Lab. Immunol. 3, 175-183.
Storck, M., Abendroth, D., Prestel, R., Pino-Chavez, G., Miiller- H~Sker, J., White, D.J.G., Hammer, C., 1997. Morphology of
hDAF (CD55) transgenic pig kidneys following ex-vivo hemoperfusion with human blood. Transplantation 63, 304- 310.
Thomas, H., Maillet, F., Letourneur, D., Jozefonvicz, J., Kazatchkine, M.D., 1995. Effect of substituted dextran deriva- tive on complement activation in vivo. Biomaterials 16, 1163- 1167.
Thomas, H., Maillet, F., Letourneur, D., Jozefonvicz, J., Fischer, E., Kazatchkine, M.D., 1996. Sulfonated dextran inhibits com- plement activation and complement-dependent cytotoxicity in an in vitro model of hyperacute xenograft rejection. Mol. Immunol. 33, 643-648.
Turner, M.W., 1996. Mannose-binding lectin: The pluripotent molecule of the innate immune system, lmmunol. Today 17, 532-540.
Vriesendorp, F.J., Flynn, R.E., Pappolla, M.A., Koski, C.L., 1995. Complement depletion affects demyelination and inflamma- tion in experimental allergic neuritis. J. Neuroimmunol. 58, 157-165.
Wang, Y., Hu, Q., Madri, J.A., Rollins, S.A., Chodera, A., Matis, L.A., 1996. Amelioration of lupus-like autoimmune disease in NZB/WFI mice after treatment with a blocking monoclonal antibody specific for complement component C5. Proc. Natl. Acad. Sci. USA 93, 8563-8568.
Wang, Y., Rollins, S.A., Madri, J.A., Matis, L.A., 1995. Anti-C5 monoclonal antibody therapy prevents collagen-induced arthri- tis and ameliorates established disease. Proc. Natl. Acad. Sci. USA 92, 8955-8959.
Weisman, H.F., Bartow, T., Leppo, M.K., Marsh, H.C. Jr., Car- son, G.R., Concino, M.F., Boyle, M.P., Roux, K.H., Weis- feldt, M.L., Fearon, D.T., 1990. Soluble human complement receptor type 1: In vivo inhibitor of complement suppressing post-ischemic myocardial inflammation and necrosis. Science 249, 146-151.
Wtirzner, R., Schulze, M., Happe, L., Franzke, A., Bieber, F.A., Opermann, M., GtJtze, O., 1991. Inhibition of terminal com- plement complex formation and cell lysis by monoclonal antibodies. Complement Inflamm. 8, 328-340.
Yanamoto, H., Kikuchi, H., Sato, M., Shimizu, Y., Yoneda, S.. Okamoto, S., 1992. Therapeutic trial of cerebral vasospasm with the serine protease inhibitor, FUT-175, administered in the acute stage after subarachnoid hemorrhage. Neurosurgery 30, 358-363.
Yeh, C.G., Marsh, H.C. Jr., Carson, G.R., Berman, L., Concino, M.F., Scesney, S.M., Kuestner, R.E., Skibbens, R., Donahue, K.A., Ip, S.H., 1991. Recombinant soluble human complement receptor type 1 inhibits inflammation in the reversed passive Arthus reaction in rats. J. Immnnol. 146, 250-256.
Zilow, G., Sturm, J.A., Rother, U., Kirschfink, M., 1990. Comple- ment activation and the prognostic value of C3a in patients at risk of the adult respiratory distress syndrome. Clin. Exp. Immunol. 79, 151-157.