Embed Size (px)
Citation preview

Innovative Approach of Managing High Risk Chronic Opioid Users in a Residency Practice
Erin Inglis, MDa, Jessie Burch, PharmDb, Nida Awadallah, MDc, ,Vanessa Rollins, PhDd, Myra Bodegahl, MSWe
aAssistant Professor, Division of Family Medicine, University of Colorado School of Medicineb Assistant Professor, University of Wyoming School of Pharmacy
c Assistant Professor, Division of Family Medicine, University of Colorado School of Medicined Assistant Professor, University of Colorado School of Medicine, The Colorado Health Foundation,
Doctorate of Psychology, Rose Family Medicinee Masters of Social Work, The Colorado Health Foundation, Rose Family Medicine
Collaborative Family Healthcare Association 15th Annual ConferenceOctober 10-12, 2013 Broomfield, Colorado U.S.A.
Session #E2cFriday, October 11, 2013

Faculty Disclosure
We have not had any relevant financial relationships during the past 12 months.
Objectives
• Describe challenges to managing chronic opioid therapy in primary care and residency education.
• Describe elements of multidisciplinary chronic pain treatment.
• Describe development and implementation of our committee.
• Describe typical interventions, preliminary outcome data, challenges to implementation of committee recommendations, and effect on physician satisfaction and education.
Introduction
• Burden of chronic pain can not accurately be estimated but it is a significant social and economic problem
• Challenging to treat, especially in a residency setting
• Providers and patients often dissatisfied with treatment process
• Safety concerns with opioid abuse and overdose

Chronic pain treatment in a residency setting
What was the problem?• Wide variation of training experience and
comfort level• Lack of continuity of care• Little to no access to pain management
specialists• Patients with multiple co-morbidities • Insurance limitations

Preliminary Intervention
• Developed a pain management policy to include:– Initial patient evaluation guidelines– Chronic opioid treatment agreement– Evaluation tool for patient’s risk of abuse– Pain level assessment tool– Intermittent urine drug testing

Initial Patient Evaluation

Opioid Risk Tool

Calculating Morphine Equivalents• Morphine is the standard for equianalgesic
comparison• Determine the total daily dose (TDD) of each
opioid the patient takes and convert to oral morphine equivalents (ME)
• Example equianalgesic conversion– Oxycodone 20 mg = 30 mg ME– Percocet 10/325 mg PO q6h PRN and patient takes
4 tabs daily – TDD = oxycodone 40 mg = 60 mg ME

Patient Case
• Casey is a 45 yr old female that presents to your office with a history of chronic pain looking to establish care with you
• PMH: hypertension and depression, fibromyalgia, low back pain since a MVA 5 years ago
• Current medications: HCTZ, Vicodin, citalopram• FMHx: EtOH and cocaine abuse by her father • SH: 2-3 EtOH drinks most days of the week but denies
having an EtOH problem

Patient Case
• How would you assess her risk for opioid abuse?
• Which of the following risk categories would you place her in with regards to opioid prescribing?
A) Low RiskB) Medium RiskC) High Risk

Patient Case
• Casey is a 45 yr old female that presents to your office with a history of chronic pain looking to establish care with you
• PMH: hypertension and depression, fibromyalgia, low back pain since a MVA 5 years ago
• Current medications: HCTZ, Vicodin, citalopram• FMHx: EtOH and cocaine abuse by her father • SH: drinks 2-3 EtOH drinks most days of the week but
denies having an EtOH problem

Patient Case
• How would you assess her risk for opioid abuse?– Variety of validated risk tools– Our practice uses the Opioid Risk Tool (ORT)
• Which of the following risk categories would you place her in with regards to opioid prescribing?
A) Low RiskB) Medium RiskC) High Risk

Initial Outcomes
• Improvement but adherence to policy limited by lack of continuity
• Continued frustration with the process• Physicians found it difficult to make long-term
decisions because of lack of continuity• Lack of time during busy clinic days to review
drug testing and PDMP data

Follow-Up Interventions• Formed Pain Management Committee (PMC)– Consists of residents, attending physicians, pharmacist,
social worker, and psychologist– Generated a pain management registry– Monthly meetings: review of 5-7 patient charts
followed by open discussion• Patients are chosen for review based on provider request or
policy guidelines
– Review of clinic visit notes, drug screens, self management goals, PDMP data, and aberrancies
– Generate recommendations for future management to PCP or next visit provider

Follow-Up Interventions
• Created a‘Pain Management Toolbox’that is easily accessible to entire practice– Pain management policy– Additional guidelines– Supporting documents – List of resources
• Increased resident/physician education on pain management


Monitoring Guidelines

Urine Drug Testing • Guidelines established for frequency of
monitoring in-house urine drug screens• When urine drug screen not what was
expected then sample sent for confirmatory testing
• Frequently the test ordered from the lab was only another screen and not confirmatory
• Challenge identifying CPT codes for specific confirmatory tests
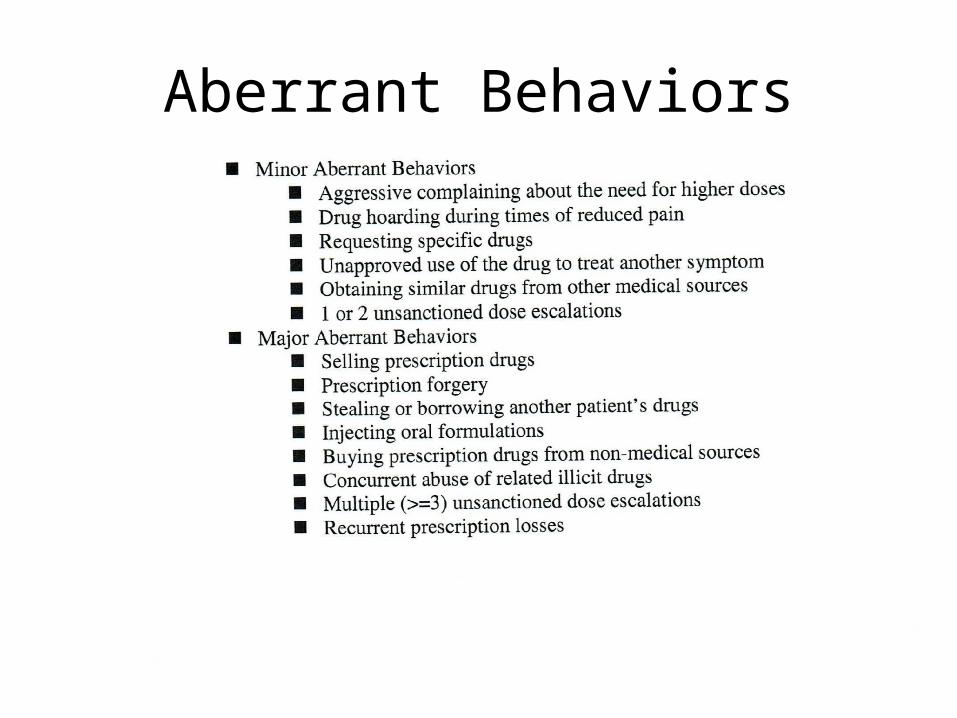
Aberrant Behaviors


Patient Case Continued• After careful assessment, the decision was made accept Casey as a
patient and prescribe her Vicodin• She agrees to and signs the Chronic Opioid Treatment Agreement • At 3rd monthly visit, her in-office urine drug test is negative for
hydrocodone despite stating she is taking the medication as prescribed • You send out a confirmatory urine drug test, which is also negative for
hydrocodone• When you discuss the results over the phone, she admits to increasing
her dose without discussing it with you and running out of her Vicodin 1 week early
• You review the agreement again and see her the following month • At this visit, you review the PDMP and see that she has received other
prescriptions for Vicodin from 2 outside providers over the past month

Patient Case Continued
• What would you do? A. Continue to prescribe her Vicodin regularlyB. Tell patient she has had at least 2 minor aberrancies,
refer to a pain management specialist and stop prescribing Vicodin
C. Discuss the aberrancies and try to come to a resolution with patient that you both agree on

Typical PMC Interventions• No concerns:– Continue current treatment plan– Reassess in 12 months
• Moderate or high risk with no aberrancies:– Consider tapering to a lower risk dose– Adjuvant treatments– Assess for psychosocial barriers and comorbid disease
states– Consider referral to pain management specialist– Reassess in 3-6 months

Typical PMC Interventions
• 2 minor or 1 major aberrancies:– Dismissal from pain management program with or
without taper and referral to pain management specialist

PMC Outcome Data
• Registry of 130 patients taking chronic opioids• To date: 35 have been tapered off• Continue to monitor other high risk patients

Resident/Physician Education
• Monthly meetings of the PMC • Bimonthly PMC meetings with entire practice• Chronic pain modules (AMA)– https://cme.ama-assn.org/Education.aspx
• First year residents receive several PM talks during their first few months of residency
• Methadone management talk in the second year of residency
Physician Satisfaction• Overall improved significantly– More comfortable with managing chronic pain
than before the PMC existed– Residents feel more comfortable managing
chronic pain after graduation
• Pressure taken off individual providers as major decisions made by the PMC
• Safer prescribing given routine review by PMC
Future Direction
• Develop a policy for chronic pain patients with concomitant use of benzodiazepines
• Review validated risk tools for patients with active substance abuse receiving chronic opioids
• Improve utilization of self-management goals• Evaluate patient satisfaction

Conclusions
• Developing a chronic pain registry, pain management committee, and toolbox can help manage complex chronic pain patients in a residency or large practice setting– Improved patient safety– Improved provider satisfaction

Questions?

Session Evaluation
Please complete and return theevaluation form to the classroom monitor
before leaving this session.
Thank you!












![Fall 2013 - PDF [New Window] - Inglis](https://img.pdfslide.us/doc/110x75/62063e138c2f7b173005c7dd/fall-2013-pdf-new-window-inglis.jpg)
















