Embed Size (px)
Citation preview

April, 2006Volume 4, Issue 1
In This Issue
Innovations in Cardiac Surgery 1
Upcoming Events 2Market Report Highlights 3
Company Profiles Novadaq 4 Coronéo 5
Research Institution Profile CSTAR 6
Ask an Investor 7
Useful Links 7Patent Update 7
Ask a Regulatory Expert 8
Editor-in-Chief Katherine Taverner
Editors Denys Cooper Roxanne Deslauriers Landis Henry Vera Keown Graham North Louis Renaud Joe Wery
Ce bulletin est également disponible en français
ISSN: 1712-3518
http://www.medtechwatch.ca
Cardiology Issue
1
Innovations in Cardiac SurgeryInnovation is the operative word at the Montreal Heart Institute (MHI), in every sphere of cardiology, medical imaging, pharmacogenetic research, interventional cardiology, and heart surgery. Founded in 1954 by Dr. Paul Dav-id and affiliated with the Université de Montréal, the MHI is a highly specialized centre dedicated to tertiary and quaternary care, cardio-vascular disease preven-tion, as well as teaching and research. The MHI is a Canadian world leader in its field and a much sought-after partner. Its mission also includes the development and evaluation of new technologies and new forms of intervention in the field of cardiology. The MHI is now planning to ex-pand its surgery department to seven operating rooms equipped with the lat-est technology in the areas of service management and delivery, as well as audio-visual integration and telemedi-cine. The planning of the new surgery department provides an excellent op-portunity to examine current technol-ogy and to consider future standards in cardiac surgery It is in this context that we present a few specific innova-tions in the field of cardiac surgery.
In recent years, the field of cardiac surgery has seen the emergence of new, less invasive techniques that improve the quality of surgi-cal techniques through enhanced visualization of cardiac structures, and also reduce postoperative pain and complications, thus improving
patient recovery. The MHI plans to in-
troduce minimally invasive endoscopic mitral valve surgery at some point in 2006. The equipment re-
quired for such surgery is similar to laparoscopic
equipment, except that the endoscope is kept in
place with a supporting device and the surgeon must work with an instrument in each hand. The challenge consists of performing cardiopulmonary bypass procedures percutaneously. Instead of using an external aortal clamp, the aorta is obstructed with an inflatable balloon. An indispensable component of the procedure is the use of transesopha-geal echocardiotgraphy to verify the position of the balloon in the aorta. One of the operating rooms will be dedicated to research and de-velopment and will have a roboticContinued on page 2

April, 2006Volume 4, Issue 1
Upcoming Events
TechMedEdmonton - April 4, 2006Vancouver - May 16, 2006 (tentative)www.westlink.ca/techmed
NBIA’s 20th International Confer-ence on Business IncubationSt. Louis, MissouriApril 30-May 3, 2006www.nbia.org
3rd Annual National Research Forum for Young Investigators in Circulatory & Respiratory HealthMay 4-7, 2006Winnipeg, Manitobawww.yiforum.ca
29th Canadian Medical & Biological Engineering ConferenceJune 1-3, 2006Vancoucer, BCwww.cmbes.ca/MBCEC06
MD&M EastNew York, New YorkJune 6-8, 2006www.devicelink.com/expo/east06
AMT 2006June 19-21, 2006London, Ontariowww.amtcanada.ca//docs/gen_.htm
CanMedBio 2006June 19-20, 2006Toronto, Ontariowww.biotech.ca/canmedbio
World Society of Cardio-Thoracic Surgeons 16th World CongressAugust 17 - 20, 2006Ottawa, Ontariowww.wscts2006.com
A Global Symposium on the Future of Heart Health & DiseaseOctober 12 –15, 2006Winnipeg, Manitobawww.heartconference.com
2
Innovations in Cardiac Surgery(Continued)
surgery system for use in performing minimally invasive procedures (such as repairing mitral valves). Robots can perform more minute surgical gestures with a far greater degree of surgical freedom than human surgeons. The robotic surgical system com-prises a command console for the sur-geon and the robot itself. The robot is equipped with three robotic arms fitted with an endoscope and surgical instruments. It is designed to perform its work through small intercostal incisions. One robot arm introduces a 3-D camera into the thorax through the first (central) incision, while the other arms, which are fitted with minute cardiac surgery instruments, reach the surgical field through the other incisions. The cardiac surgeon “operates” from the console via two manipula-tors. A computerized system conveys the surgeon’s movements to the robot arms, after filtering out any tremors associated with fatigue. A screen enables the surgeon to visualize three-dimensional images of the operating field provided by the endoscope.
Cardiopulmonary bypass (CPB), which can lead to postoperative complications by activating the im-mune system and the inflammation cascade, is also changing. A study to assess so-called mini-circuit CPB is currently underway. In some cases, the mini-circuit CPB is actually replacing conven-tional CPB methods. The mini-cir-cuit approach is designed to reduce the volume of extracorporeal blood by eliminating, among other things, the blood storage reservoir and re-ducing the total length of the circuit. Moreover, the circuit is entirely closed. The system aspirates the patient’s blood through a weakly hemolytic centrifugal pump; as a result, the oxygen machine can be placed at patient height. The system is small, approximately two-thirds of the size of a conventional device, and can be placed very close to the patient. A smaller circuit requires less priming solution and therefore less hemodilution. The circuits are coated with an antithrombogenic solution to protect the heart against inflammatory reactions. The MHI is also contributing to progress in hybrid procedures that call on the expertise of both cardiac surgeons and interventional cardi-ologists to treat pathologies of the thoracic aorta percutaneously under fluoroscopic guidance. We also im-plant thoracic aorta endoprostheses.Recently, a new type of aortic valve was implanted percutaneously in a patient who was unable to undergo a Continued on page 3
Cardiology Issue

Market Report Highlights
The Outlook for Medical Devices: Canada Espicom Business IntelligencePublished: December 2005 The Canadian medical equipment market is the seventh largest in the world and is largely supplied by imports from the USA. This report provides a comprehensive analy-sis of the medical device market, including five year market forecasts. Three quarterly updated reports are included, keeping you up to date with key market developments for a full year. US $795 View Table of Contents
Cardiovascular Disease Diagnostics: A Global Strategic Business ReportGlobal Industry Analysts IncPublished: October 2005
This report analyzes the worldwide markets for cardiovascular disease diagnostics in millions of US$. The major product segments analyzed are in vitro diagnostics and in vivo diagnostics. The report provides separate comprehensive analytics for the US, Canada, Japan, Europe, Asia-Pacific (excluding Japan), Middle East and Latin America. Annual forecasts are provided for each region for the period of 2000 through 2010. The report profiles 67 compa-nies including many key and niche players worldwide such as Abbott Diagnostics, Biosite, Inc., Cambridge Heart, Inc., Cholestech Corp., Dade Behring, Inc., EP Medsystems, GE HealthCare, Liposcience, Inc., Philips Medical Systems, Roche Diagnostics, Siemens Medical Solutions, and Spec-tral Diagnostics, Inc. US $3950View Table of Contents
Please contact CISTI if you would like to purchase sections of these reports.Email [email protected] or call 204-984-6027.
3
Innovations in Cardiac Surgery(Continued)
conventional operation – the first valve of this type to be implanted in North America. Hybrid procedures require an operating room environment that combines life support equipment, rig-orous asepsis and high-performance angiography equipment. The hybrid operating room is a conventional catheterization room designed to ac-commodate the instruments normally found in an operating room (anesthe-sia equipment, ECG equipment, heart-lung machine, etc.).
The room must also be designed to accommodate ceiling-suspended equipment, an arrangement that cre-ates a more comfortable environment for the patient. These rooms are equipped with articulated arms and integrated audio-visual systems so that considerable space is gained. In order to adapt to conventional forms of heart surgery, the room must also have an operating table in addition to an imaging table, since the latter is not suitable for conventional surgical procedures.
The field of ventricular assist-ance is also rapidly growing due to the difficulty in recruiting cardiac transplant donors. Ventricular assist-ance is achieved by installing a fairly large internal or external artificial valve which is controlled pneumati-cally or electromagnetically. New, completely implantable systems will soon be available in Canada. These consist of a rotating axial turbine, which is implanted directly at the apex of the left ventricle, with a sin-gle outflow conduit to the descend-ing thoracic aorta. Cardianove Inc., the company created when MHI surgeons joined forces with engi-neers from the École Polytechnique de Montréal, is currently develop-ing a miniature pump that will be entirely implantable in the heart as a treatment for heart failure. In tertiary cardiology, technolog-ical innovations abound, supporting as well as generating, new practices in cardiac surgery. In this context of constant change, the operating room of the future will need to be designed for versatility and adaptability in order to accommodate new technolo-gies and new surgical practices.
Sophie Le Bail M.Sc.A, Biomedical Technology Consultant, Montreal Heart Institute
Cardiology Issue

4
Novadaq® TechnologiesCoronary artery bypass graft (CABG) surgery is the most common form of heart surgery, with approximately 400,000 procedures performed an-nually in the United States and over 750,000 worldwide. Yet despite the prevalence and effectiveness of the procedure in the treatment of coro-nary artery disease (CAD), there has not been a way to routinely assess bypass graft quality and functionality during the course of surgery. Novadaq® Technologies, a Canadian-based medical device company specializing in the develop-ment and marketing of diagnostic and therapeutic procedures for human vascular, ophthalmic, and neurologic diseases and conditions, has em-ployed a proprietary imaging technol-ogy platform to address this unmet need in cardiac operating rooms. The roots of Novadaq can be traced back the National Research Council of Canada Institute for Bio-diagnostics (NRC-IBD) where NRC-IBD scientists spent three years de-veloping the intra-operative imaging technique upon which the Novadaq technology is based. Novadaq’s technology platform leverages the in-tegration of three technologies: laser, high-speed imaging, and a fluoresc-ing agent. The integration of these technologies provides Novadaq with the capability to visualize natural blood flow in real-time, in vessels as small as five microns in diameter, at a speed of up to 30 frames per second. The technology produces superior, real-time images through a simple
Company Profiles
operating room by commercial-izing disease-specific procedures that set the gold standard for safety, efficacy, and quality.
* LIMALeft Internal Mammary Artery
** LADLeft Anterior Descending Artery
Visit Novadaq Technologies online at:http://www.novadaq.com
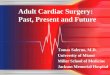
and safe two-minute process, and has the potential to increase pro-cedural efficiencies and improve outcomes and procedural safety. With this platform at its core, Novadaq has successfully devel-oped and is globally commercial-izing the SPY® Imaging System. SPY was cleared by the Food and Drug Administration (FDA) in early 2005 and is being used for the intra-operative visual assess-ment of coronary vasculature and bypass grafts during coronary artery bypass graft procedures in leading centres throughout the US. SPY provides surgeons the ability to identify the unpredictable need to perform graft revisions; thereby potentially achieving technical graft perfection during the course of surgery while the patient is still in the operating room – an oppor-tunity that can increase a patient’s quality and length of life. Novadaq continues to develop the system and advance the adoption of this new technology as the standard of care in cardiac surgery. The technology platform utilized with the SPY System is now being applied to additional applications where image-guided therapy may enable enhanced procedure and treatment outcomes. Technology developments for treatment areas such as visualiza-tion of the retina, nerves, and lym-phatic system are being explored. Novadaq strives to provide the imaging system of choice in the
LIMA* to LAD**No flow through graft
Vein Graft Good flow through graft

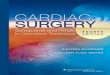
Swift-Loop with Occluding Pledget
Extra-Aortic Annuloplasty Ring
Cor-Valv Aortic Retractor
Extra-Aortic Annuloplasty Ring (pre-implantation)
Extra-Aortic Annuloplasty Ring (post-implantation)
Cor-Valv Mitral Retractor
5
Company Profiles(Continued)
CORONÉO, a Montreal-based medical device company, develops instruments and enabling technologies that render cardiac surgery less invasive and more cost-effective. Working closely with leading Canadian and international surgeons during all stages of product development – from problem state-ment to concept design to product validation – CORONÉO has been able to quickly respond to the “real needs” of the healthcare industry. Possessing its own prototype facilities, plastic injection, and clean room capabilities, CORONÉO can expediently introduce prototypes and rapidly converge design iterations dur-ing market sensitive product develop-ment. The company is certified to ISO 13485:2003. Since its inception in 1998, the company’s ongoing developments have led to the successful marketing of six surgical platforms, and differen-tiated CORONÉO as a responsive and noteworthy provider of novel surgi-cal solutions. The company’s four reusable titanium and two single-use plastic products feature patented or patent-pending innovations, and allow adult or pediatric interventions through either sternotomy or intercostal ap-proaches. All products have received FDA and CE mark approval, and are currently commercialized in thirteen countries In recent years, CORONÉO has undertaken to grow its business in the field of implantable devices by lever-aging its established infrastructure and competence network. The company’s first implantable device, the Extra-Aortic Ring, is a unique annuloplasty device allowing surgeons to repair a dilated aortic root by restoring valve leaflet contact. The expansible nature of the aortic ring allows preservation
of the physiology of the aortic root, and more importantly, by sparing the patient’s valve leaflets it avoids the need to replace the entire valve with a prosthetic mechanical valve. No such device presently exists on the market. The European launch of the Extra-Aortic Ring is planned by last quarter 2006, with the use of the device in a prospective, multi-centre randomized trial in France entitled CAVIAAR (Conservation Aortique Valvulaire dans les Insuffisances Aortiques Dystrophiques et les Anévrismes de la Racine Aortique). CORONÉO’s second implantable device, presently in R&D, focuses on providing an effective surgical treat-ment for ischemic mitral valve disease. It is estimated that the current treat-ment for repairing ischemic valves through mitral annuloplasty is charac-terized by a thirty percent recurrence of valve insufficiency within one year of surgery. CORONÉO’s longer-term plans involve validating and exploiting a novel biomaterial having anatomi-cally representative mechanical prop-erties. Suitable applications for this biomaterial include pulsatile vascular conduits and compliant heart valves. One of CORONÉO’s objectives from the onset was to create a medical engineering discipline that brings to-gether the high-tech design experience of creative engineers with the medi-cal expertise of prominent surgeons. CORONÉO is continuously forging new alliances with Canadian medical doctors and Canadian universities to complement its current skills base and expertise.
For additional information, please contact: Anthony PaolittoTelephone: (514) 336-9230Facsimile: (514) 334-9778E-mail: [email protected]

6
CSTAR
An inter-disciplinary medical team at CSTAR (Canadian Surgical Technolo-gies & Advanced Robotics) is seeing a marked increase in the number of refer-rals of patients from across Canada for a relatively new innovation to treat heart disease. In 2004, the team became the first in North America to complete two different procedures to clear blocked ar-teries, minimally-invasive robot-assisted heart bypass surgery and angioplasty with stenting, at the same time in the operating room.
Although the individual procedures are not new, the fact that they are combined into one episode of care is unique. Before the hybrid surgery, pa-tients needing both procedures would have bypass surgery first and then angioplasty a day or two later, or vice versa. Advanced technology, such as 3-D imaging in CSTAR’s specialized Hybrid Operating Room/Angiosuite at London Health Sciences Centre (LHSC), one of a few such facilities in the world, has made this intervention possible. “Combining heart bypass surgery and angioplasty in one operating room opens up an entirely new op-
Research Institution Profile
tion to treat select patients with heart disease,” says Bob Kiaii, leader of CSTAR’s Robotic Coronary Artery Bypass research project and cardiac surgeon at the LHSC. “The benefits of this new hybrid procedure include a reduced hospital stay by approxi-mately two days compared to the traditional approach to treatment, and a faster recovery, which benefits patients as well as the health care system.” With continued positive results for patients, the team has been able to successfully complete thirty hybrid procedures since September 2004 at LHSC. Dr. Kiaii says the number of referrals is continuing to grow as word of the procedure’s success spreads. “Robotics has actually become 80% of my practice now with pa-tients being referred to us from across Canada.” Dr. Kiaii, using the four-armed da Vinci robot, bypasses a sin-gle blocked coronary artery through small incisions instead of cutting the breast bone in half. The surgery is also performed without stopping the heart as opposed to traditional bypass surgery where the heart is stopped and the heart/ lung machine is used to circulate the blood supply. According to Dr. Kiaii, “When we use what we call an ‘off pump’ procedure, patients may experience a reduced risk of developing com-plications such as increased inflam-mation, neurological side effects and bleeding.” This procedure also avoids cutting the breast bone and reduces post operative wound complications and infections.
Immediately following the surgery, the intervention cardiologists com-plete the percutaneous coronary in-tervention (PCI) or angioplasty with stenting to open additional narrowed arteries. According to Dr. Kostuk, interventional cardiologist at LHSC, “The one procedure allows us to do a PCI on patients at a reduced risk.” PCI involves the advancing of a small tube (catheter) from the groin to the mouth of the artery. Through this tube a smaller catheter with a balloon on the tip is passed across the narrowed segment. The balloon is inflated, which presses the fat deposits against the artery wall and increases the opening. A stent (wire mesh) is then placed across the nar-rowed opening. The stent is pressed into the wall of the vessel by inflat-ing a balloon. The end result is a wide open blood vessel and normal blood flow. Patients who would be consid-ered for the hybrid research protocol are those with blocked heart arteries who would benefit from a minimal-ly-invasive bypass with robotic as-sistance and who also have blocked arteries not accessible through a minimally-invasive approach that would be treated with interventional cardiology. Research at CSTAR is supported by grants from the Canada Founda-tion for Innovation and the Ontario government. CSTAR is a collabora-tive research program of London Health Sciences Centre and the Lawson Health Research Institute and is affiliated with the University of Western Ontario.
Success breeds interest in combined innovative method to treat heart disease
Dr. Bill Kostuk (left) and Dr. Bob Kiaii consult about a patient’s case prior to the angioplasty being completed by Dr. Kostuk in CSTAR’s Hybrid Operating Room.

Patents Update
Prosthetic heart function evalua-tion method and apparatusUnited States Patent Application 20060047209A1ViewAbstractMarch 2, 2006
Device for shaping infarcted heart tissue and method of using the deviceUnited States Patent Application 20060025838A1View AbstractFebruary 2, 2006
Useful Links
Top Advances in Cardiovascular Disease and Strokehttp://www.americanheart.org/pre-senter.jhtml?identifier=220 US Clinical Trials Databasehttp://www.clinicaltrials.gov Pharmalicensinghttp://pharmalicensing.com/ Medical Device Manufacturers As-sociation: Reimbursement sectionhttp://www.medicaldevices.org/public/issues/reimbursement.asp FDA Cardiovascular Devices Clas-sification http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?CFRPart=870 Clinical Device Forumhttp://www.clinicaldeviceforum.com/
7
How do I approach a VC?
The best way to approach a VC is with a very short non-confidential executive summary (1-2 pages max). This should be presented after a brief introduction by phone or in person (have a 30-60 second pitch ready at all times). If you believe Malcom Gladwell’s book BLINK, your fate is decided in that first interaction so you need to prepare for that initial contact and ensure that it is a high quality in-teraction. VCs are busy like the rest of us and will generally pay more atten-tion to those people with whom they have some sort of connection. So if you know someone who knows a VC, an introduction is a good way to get in the door. One of the biggest mistakes you can make is providing your full business plan in the first interaction. It probably won’t get picked up, and if it does, it will likely move to the bot-tom of the pile unless the VC happens to have a particularly strong interest in your technology or knows of your company from some other source.
Do you have questions on invest-ment options? Send your questions to Katherine Taverner [email protected]
What are the essential pieces I need to have before approaching an investor?
There needs to be a unique value proposition for most VCs. This usually encompasses having an “unfair” competitive advantage. You will need some way to protect your idea (patents are generally considered the most effective way to do this), a better solution to whatever problem you are tackling, and a growing market. In addi-tion to having a good protected idea, you need to have a plan for how you will commercialize your product, how you will sell it, to whom you will sell it, and for how much. You also need to be aware of who else is out there compet-ing with you. In short, you need a viable business plan that lays out what you plan to do. Be aware, though, that your plan will need to be constantly updated as you obtain more and better information about your product and its market.
Ask an Investor
Darren Fast, Ph.D.PresidentSolalta Advisors49 Nutley CircleWinnipeg, MB R2N [email protected]

A note from the Editor Thanks for checking out our new and improved newsletter! We hope you enjoy the new features, including a revamped look and format, Q & A columns on regulatory and investment issues, and specialty-themed issues.
We’re also delighted to invite you to visit the new Medical Technology Watch website www.medtechwatch.ca where you will find archived past issues, information about upcoming issues, biographies of members of the Editorial Board, and more!
We welcome your feedback. Please send your comments or suggestions to [email protected] We look forward to hearing from you.
Sincerely,
Katherine Taverner, Editor-in-Chief
8
What can you do to ensure control over outsourced processes?
Most medical device companies will find themselves at some time hav-ing to consider outsourcing, whether it is the entire manufacturing or a specific process for which the company does not have the expertise or resources. Developing a comprehensive quality agreement with the subcontractor is critical to a successful relationship, and provides a medical device company with confidence that the subcontractor can meet their requirements. The qual-ity agreement provides a standard to which the medical device company can evaluate the subcontractor’s perform-ance and demonstrate control over their outsourced processes under their Quality Management System.
What information should be included in a subcontractor quality agreement?
The quality agreement should clearly define the responsibilities of both parties, and performance requirements and expectations. Depending on the scope of the agreement and nature of the ac-tivities involved, items included in the quality agreement can range from specifying a date of delivery to defining quality and/or industry standards and/or regulations ap-plicable to services provided by a subcontractor. Requirements for performance should be clearly defined to prevent any misinterpre-tation, be specific, measurable and periodically subject to an audit.
Do you have questions on regula-tory issues? Send questions to Katherine Taverner [email protected]
Ask a Regulatory Expert
Jerry Holatko, H.B.Sc., Chem.Senior Director, Consultative ServicesPharmEng Technology Inc.Suite 201 3760 – 14th Ave.Markham, ON L3R [email protected]
DisclaimerOpinions and statements in the publication attributed to named authors do not necessarily reflect the policy of the National Research Council Canada or the Government of Canada. Al-though we strive to make the information helpful and accurate, neither the National Research Council Canada, nor any of its employees, makes any guarantee, express or implied, regard-ing the accuracy of information or fitness for a particular purpose. The National Research Council Canada disclaims all liability of any kind whatsoever arising out of the use of, or inability to use, this information.