Embed Size (px)
Citation preview


Alice Nelson Dinardo: “fm” — 2007/7/17 — 17:37 — page i — #1
Anesthesia for Cardiac Surgery

Alice Nelson Dinardo: “fm” — 2007/7/17 — 17:37 — page ii — #2
Dedication
To my wife Denée for her love, support and wisdom.To my daughter Isabel and her limitless potential.To my mother Josephine Ann who taught me the value of honesty and perseverance.
James A. DiNardo
Tomywife, Bharathi, and daughters, Alexandra, Jessica, Gracie andOlivia: each of you have inspiredme in ways that youwill never know. I love you and dedicate this book to you and your life’s dreams.
Go confidently in the direction of your dreams. Live the life you have imagined. (Henry David Thoreau)
David A. Zvara

Alice Nelson Dinardo: “fm” — 2007/7/17 — 17:37 — page iii — #3
Anesthesia forCardiac SurgeryThird Edition
James A. DiNardo, MDClinical Co-Director of Cardiac AnesthesiaDepartment of AnesthesiaChildren’s Hospital Bostan300 Longwood AvenueBoston, MA, 02115USA
David A. Zvara, MDJay J. Jacoby Professor and ChairDepartment of AnesthesiologyThe Ohio State University410 West 10th AvenueColumbus, Ohio, 43210USA

Alice Nelson Dinardo: “fm” — 2007/7/17 — 17:37 — page iv — #4
© 1990 and 1997 James A. DiNardo© 2008 James A. DiNardo and David A. ZvaraPublished by Blackwell PublishingBlackwell Publishing, Inc., 350 Main Street, Malden, Massachusetts 02148-5020, USABlackwell Publishing Ltd, 9600 Garsington Road, Oxford OX4 2DQ, UKBlackwell Publishing Asia Pty Ltd, 550 Swanston Street, Carlton, Victoria 3053, Australia
The right of the Author to be identified as the Author of this Work has been asserted inaccordance with the Copyright, Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrievalsystem, or transmitted, in any form or by any means, electronic, mechanical,photocopying, recording or otherwise, except as permitted by the UK Copyright, Designsand Patents Act 1988, without the prior permission of the publisher.
First published 1990Second edition 1997Third edition 2008
1 2008
Library of Congress Cataloging-in-Publication Data
DiNardo, James A.Anesthesia for cardiac surgery/James A. DiNardo, David A. Zvara. – 3rd ed.
p. ; cm.Includes bibliographical references and index.ISBN 978-1-4051-5363-8 (alk. paper)1. Anesthesia in cardiology. 2. Heart–Surgery. I. Zvara, David A. II. Title.
[DNLM: 1. Cardiac Surgical Procedures. 2. Anesthesia. WG 169 D583a 2007]
RD87.3.H43D5 2007617.9’67412–dc22
2007001204
ISBN: 978-1-4051-5363-8
A catalogue record for this title is available from the British Library
Set in 9/12pt Meridien byNewgen Imaging Systems (P) Ltd, Chennai, IndiaPrinted and bound in Singapore by Fabulous Printers Pte Ltd
Commissioning Editor: Stuart TaylorEditorial Assistant: Jennifer SewardDevelopment Editors: Adam Gilbert and Victoria PittmanProduction Controller: Debbie Wyer
For further information on Blackwell Publishing, visit our website:http://www.blackwellpublishing.com
The publisher’s policy is to use permanent paper from mills that operate a sustainableforestry policy, and which has been manufactured from pulp processed using acid-free andelementary chlorine-free practices. Furthermore, the publisher ensures that the text paperand cover board used have met acceptable environmental accreditation standards.
Blackwell Publishing makes no representation, express or implied, that the drug dosages inthis book are correct. Readers must therefore always check that any product mentioned inthis publication is used in accordance with the prescribing information prepared by themanufacturers. The author and the publishers do not accept responsibility or legal liabilityfor any errors in the text or for the misuse or misapplication of material in this book.

Alice Nelson Dinardo: “fm” — 2007/7/17 — 17:37 — page v — #5
Contents
Preface, vii
1 Introduction, 1
2 Myocardial Physiology and the Interpretation ofCardiac Catheterization Data, 20
3 Monitoring, 42
4 Anesthesia for Myocardial Revascularization, 90
5 Anesthesia for Valvular Heart Disease, 129
6 Congenital Heart Disease, 167
7 Anesthesia for Heart, Heart-Lung, and Lung Transplantation, 252
8 Pericardial Disease, 289
9 Anesthesia for Surgery of the Thoracic Aorta, 304
10 Management of Cardiopulmonary Bypass, 323
11 Mechanical Circulatory Support, 375
12 Myocardial Preservation during Cardiopulmonary Bypass, 409
13 Special Considerations during Cardiac Surgery, 425
Index, 439
v

Alice Nelson Dinardo: “fm” — 2007/7/17 — 17:37 — page vii — #7
Preface
Anesthesia for Cardiac Surgery originally published in1989, and revised in 1998, was written with theintention of filling the perceived void in cardiacanesthesia reference material between definitive,heavily referenced texts and outline-based hand-books. The updated 3rd Edition strives to do thesame. This book is intended to provide practi-cal recommendations based on sound principlesof physiology. The text provides a comprehensiveoverview of the contemporary practice of cardiacanesthesia. There is a place for this work as a compo-nent of a core curriculum in cardiac anesthesiologytraining as well as in the library of the busy, practic-ing clinician. We hope this work helps you in caringfor your patients.
JADDAZ
Acknowledgements
The authors would like to acknowledge Adela S.F.Larimore at the Wake Forest University School ofMedicine, Department of Anesthesiology for hereditorial support in the preparation of this textbook.Without her assistance this work would not bepossible.
vii

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 1 — #1
CHAPTER 1
Introduction
A complete evaluation of the patient’s medicalhistory, physical examination, and review of per-tinent laboratory and supportive tests is necessaryprior to any elective cardiac surgical procedure. Theintention of the preoperative evaluation is sever-alfold: define the status of the patient’s medicalcondition, identify areas of uncertainty that requirefurther evaluation, consultation or testing, devisea strategy to improve or stabilize ongoing medi-cal conditions prior to surgery, determine a prog-nostic risk classification, and provide informationto formulate an intraoperative and postoperativeplan. The anesthesiologist must clearly understandthe intended surgical procedure. This chapter willpresent a systems review of the common and sig-nificant features found preoperatively in the cardiacsurgical patient. There will be a special emphasis onthe methodology, limitations, and accuracy of thetests used most commonly in evaluation of cardiacsurgical patients.
Cardiovascular evaluation
A directed history and physical examination areessential before any cardiac surgical procedure.The information obtained, in the context ofthe anticipated surgical procedure, will deter-mine the requirement for subsequent evaluation,consultation or testing.
History and physical examinationThere are no controlled trials evaluating the effec-tiveness of the history and physical; however,
conditions discovered in the process help definethe anesthetic plan and are often associated withstrong prognostic value. For example, a history ofmyocardial infarction, unstable angina, congestiveheart failure, dyspnea, obstructive sleep apnea, andany number of other conditions may directly affectthe course of the preoperative evaluation, operativeoutcome, and patient satisfaction. There are manyalgorithms for quantifying patient risk, includingthe American Society of Anesthesiologists Physi-cal Status Classification. The Revised Cardiac RiskIndex is a clinically useful example of a preopera-tive scoring system to define perioperative cardiacrisk (Table 1.1).In most cardiac surgical procedures, the preanes-
thetic evaluation should take place prior to theday of surgery. This will allow time for additionaltesting, collection, and review of pertinent pastmedical records, and appropriate patient counsel-ing. The examination can be obtained on the dayof surgery for procedures with relatively low sur-gical invasiveness. The history provides insight intothe severity of the pathologic condition. For exam-ple, a history consistent with heart failure is mostalarming and requires careful deliberation beforeproceeding (Table 1.2). In evaluating a patient withangina, it is essential to determine if the symp-toms represent unstable angina (Table 1.3). TheCanadian Cardiovascular Society Classification ofAngina defines anginal symptoms (Table 1.4).At a minimum, the physical examination must
include the vital signs and an evaluation of
1

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 2 — #2
2 Chapter 1
Table 1.1 The Revised Cardiac Risk Index.
Ischemic heart disease: Includes a history of myocardialinfarction, Q waves on the ECG, a positive stress test,angina, or nitroglycerine use
Congestive heart failure (CHF): Includes a history of CHF,pulmonary edema, paroxysmal nocturnal dyspnea, rales,S3 gallop, elevated β-naturetic peptide, or imaging studyconsistent with CHF
Cerebrovascular disease: Includes a history of transientischemic attack or stroke
Diabetes mellitus treated with insulin:
Renal dysfunction (serum creatinine >2)
High-risk surgery: Includes any intraperitoneal,intrathoracic or suprainguinal vascular procedures
CABG, coronary artery bypass surgery; ECG, electrocardio-gram.0–2 risk factors = low risk.3 or more risk factors = high risk.
the airway, lungs and heart. Auscultation of thechest may reveal wheezing, rales, or diminishedbreath sounds. Auscultation of the heart is critical inuncovering new murmurs, S4 gallops, and rhythmabnormalities. In patients older than 40 years, newheart murmurs are found in upwards of 4% ofpatients. Further screening with echocardiographyreveals significant valvular pathology in 75% ofthese patients. Arterial hypertension is commonin the cardiac surgical patient; however, there islittle evidence for an association between admis-sion arterial pressures less than 180mmHg systolicor 110mmHg diastolic and perioperative compli-cations. In patients with blood pressures abovethis level, there is increased perioperative ischemia,arrhythmias, and cardiovascular lability.Once the history and physical examination are
complete, attention turns to what additional eval-uation, consultation or studies are indicated priorto the operative procedure. The decision regard-ing which test to order should be based uponan analysis of value of the information obtained,resource utilization and timeliness in regards tothe scheduled procedure. Several common tests arereviewed below.
ElectrocardiogramA preoperative electrocardiogram (ECG) should beobtained in all cardiac surgical patients. There is noconsensus on the minimum patient age for obtain-ing an ECG, although ECG abnormalities are morefrequent in older patients and those with multiplecardiac risk factors. The ECG should be examinedfor rate and rhythm, axis, evidence of left and rightventricular (RV) hypertrophy, atrial enlargement,conduction defects (both AV nodal and bundlebranch block (BBB)), ischemia or infarction, andmetabolic and drug effects.
Rate and rhythm abnormalitiesThere are a large number of rate and rhythm abnor-malitieswhichmay be present in the cardiac surgicalpatient. Tachycardia may be a sign of anxiety, drugeffect (i.e. sympathomimetics, β-adrenergic ago-nists, and cocaine intoxication), metabolic disorder(hypothyroidism), fever, sepsis or other condi-tions. Bradycardia is typically due to medications(β-adrenergic blocking agents), although a slowheart rate may by indicative of other pathol-ogy (hypothyroidism, drug effect, hypothermia,conduction defects). Arrhythmias are potentiallymore serious and require immediate evaluation.Electrolyte abnormalities are common in cardiacsurgical patients and may lead to premature ven-tricular contractions (PVCs). The actively ischemicpatientmay present with ventricular irritability, fre-quent ormultifocal PVCs, or ventricular tachycardia(VT). Atrial fibrillation is frequently observed inthe elderly cardiac surgical patient. The diagnosisof new atrial fibrillation requires evaluation prior tosurgery if time and the clinical condition permit.
AxisAxis refers to the direction of depolarization inthe heart. The mean QRS vector (direction ofdepolarization) is normally downward and to thepatient’s left (0–90). This axis will be displacedwith physical relocation of the heart (i.e. extrinsiccardiac compression from a mass effect), hypertro-phy (axis moves toward hypertrophy), or infarction(axis moves away from infarction). In the normalcondition, the QRS is positive in lead I and aVF.

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 3 — #3
Introduction 3
Table 1.2 American College of Cardiology/American Heart Association Classification of chronic heart failure.
Stage Description
A. High risk for developing heart failure Hypertension, diabetes mellitus, coronary artery disease, family history ofcardiomyopathy
B. Asymptomatic heart failure Previous myocardial infarction left ventricular dysfunction, valvular heartdisease
C. Symptomatic heart failure Structural heart disease, dyspnea and fatigue, impaired exercise tolerance
D. Refractory end-stage heart failure Marked symptoms at rest despite maximal medical therapy
Stage A includes patients at risk of developing heart failure but have no structural heart disease at present. A highdegree of awareness is important in this group
Stage B includes patients with known structural heart disease but no symptoms. Therapeutic intervention withangiotensin converting enzyme inhibitors or adrenergic beta-blocking agents may be indicated for long-term chronictreatment in this group
Stage C includes patients with structural heart disease and symptomatic heart failure. Operative risk is increased in thisgroup. Medical therapy may include diuretics, digoxin, and aldosterone antagonists in addition to ACE inhibitors andbeta-blockers depending upon the severity of symptoms. Cardiac resynchronization therapy also may be considered inselected patients
Stage D includes patients with severe refractory heart failure. These patients frequently present for heart transplantationor bridging therapy with ventricular assist devices. Acute decompensation is managed with inotropes and vasodilatortherapy
ACE, angiotensin-converting enzyme.
Table 1.3 The principal presentations ofunstable angina. Rest angina Angina occurring at rest and usually prolonged greater
than 20 minutes
New onset angina Angina of at least CCSC III severity with onset within2 months of initial presentation
Increasing angina Previously diagnosed angina that is distinctly morefrequent, longer in duration or lower in threshold(i.e. increased by at least one CCSC class within2 months of initial presentation to at least CCSC IIIseverity)
CCSC, Canadian Cardiovascular Society Classification.
Left atrial enlargementIn adults, left atrial enlargement (LAE) may befound in association with mitral stenosis, aorticstenosis, systemic hypertension, and mitral regur-gitation. In mitral stenosis, LAE occurs secondary tothe increased impedance to atrial emptying across
the stenotic mitral valve. In aortic stenosis andsystemic hypertension, an elevated left ventricu-lar (LV) end-diastolic pressure results in left atrialhypertrophy. In mitral regurgitation, LAE occursbecause of the large volumes of blood regurgitatedin the left atrium during systole.

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 4 — #4
4 Chapter 1
Table 1.4 The Canadian Cardiovascular Society Classification System of angina pectoris.
Class I: Ordinary physical activity, such as walking and climbing stairs does not cause angina. Angina occurswith strenuous, rapid, or prolonged exertion
Class II: Slight limitation of ordinary activity. Angina occurs on walking or climbing stairs rapidly, walkinguphill, walking or stair climbing after meals, in the cold or wind, under emotional stress or only during thefew hours after awakening. Angina occurs on walking more than two blocks on the level and climbing morethan one flight of ordinary stairs at a normal pace and under normal conditions
Class III: Marked limitations of ordinary physical activity. Angina occurs on walking one or two blocks on thelevel ground and climbing one flight of stairs in normal conditions and at a normal pace
Class IV: Inability to carry on any physical activity without anginal discomfort. Symptoms may be present at rest
Right atrial enlargementRight atrial enlargement (AAE) may be seen withRV hypertrophy secondary to pulmonary outflowobstruction or pulmonary hypertension. RAE alsomay be observed in patients with tricuspid stenosis,tricuspid atresia, or Epstein’s abnormality.
Left ventricular hypertrophyIn adults, left ventricular hypertrophy (LVH) com-monly occurs in LV pressure overload lesions suchas aortic stenosis and severe systemic hypertension.In children, LVHmay be present with coarctation ofthe aorta and congenital aortic stenosis.
Right ventricular hypertrophyRight ventricular hypertrophy (RVH) is a commonfinding in patients with congenital heart diseaseand may be seen in pulmonic stenosis, tetralogyof Fallot and transposition of the great arteries.In adults, RVH frequently results from pulmonaryhypertension.
Conduction defectsSimilar to rate and rhythm abnormalities, there area wide variety of conduction defects which maybe observed in the cardiac surgical patient. Atrio-ventricular (AV) block may be innocuous (1st and2nd degree type 1) or clinically significant requir-ing immediate evaluation of pacemaker placement(2nd degree type 2 and 3rd degree). BBB delaydepolarization in the effected ventricle andmay leadto ineffective ventricular contraction.
Ischemia and infarctionNew findings of active ischemia require immedi-ate attention. In the patient with known coro-nary artery disease (CAD) and unstable angina,ST segment abnormalities may be observed.In patients with diabetes, there may be episodes ofsilent ischemia during which the heart is ischemic,but due to autonomic dysfunction and a dimin-ished ability to perceive nociceptive signals, thepatient does not experience pain. The presence ofQ waves indicates an old transmural myocardialinfarction. Determining the timing of the Q wavefinding may be clinically relevant. For example,a Q wave not seen on an ECG 6months priorto the evaluation suggests a myocardial infarctionsometime during this recent interval. Periopera-tive cardiac morbidities are related to timing ofsurgery after a myocardial infarction, and there-fore this information requires attention and clinicalresolution.
Metabolic and drug effectsElevated serum potassium will flatten the P wave,widen the QRS complex, and elevate the T wave.Low serum potassium will flatten of invert theTwave. A Uwavemay appear.With elevated serumcalcium the QT interval shortens; whereas withhypocalcemia, the QT interval is prolonged. Digi-talis toxicity will cause a gradual down sloping ofthe ST segment. There may also be atrial and junc-tional premature beats, atrial tachycardia, sinus, andAV nodal blocks.

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 5 — #5
Introduction 5
It must be emphasized that a normal ECG doesnot preclude the presence of significant cardiac dis-ease in the adult, child, or infant. The ECG is normalin 25–50% of adults with chronic stable angina.Likewise, the ECG may be normal in children withLV pressure overload (aortic stenosis) and volumeoverload (patent ductus arteriosus or ventricularseptal defect) lesions.
Chest radiographObtaining a Chest radiograph (CXR) should bebased upon the necessity for the planned clini-cal procedure (i.e. a lateral chest film is essen-tial in a repeat sternotomy), or in assessing thepatient’s clinical condition. Clinical characteristicssuggesting a benefit to obtaining a CXR includea history of smoking, recent respiratory infection,chronic obstructive pulmonary disease (COPD), orcardiac disease. The posterior–anterior and lateralCXR provide a wealth of information including anassessment of pulmonary condition and maybe car-diovascular status. For example, radiographic evi-dence of pulmonary vascular congestion suggestspoor systolic function. For patients with valvu-lar heart disease, a normal CXR is more usefulthan an abnormal radiograph in assessing ventricu-lar function. The presence of a cardio-to-thoracicratio less than 50% is a sensitive indicator of anejection fraction greater than 50% and of a car-diac index greater than 2.5 L/min/m2. On the otherhand, a cardio-to-thoracic ratio greater than 50% isnot a specific indicator of ventricular function. Forpatients with CAD, an abnormal CXR is more usefulthan a normal radiograph in assessing ventricu-lar function. Cardiomegaly is a sensitive indicatorof a reduced ejection fraction, whereas a normal-sized heart may be associated with both normal andreduced ejection fractions.As with the ECG, efforts should be made to corre-
late radiographic findings with the clinical history.LAE is expected inmitral stenosis and regurgitation.Enlargement of the pulmonary artery and right ven-tricle occurs with disease progression. Eccentric LVhypertrophy results from mitral and aortic regur-gitation. Aortic stenosis results in concentric LVhypertrophy. In infants and children with increasedpulmonary blood flow (as with a large ventricular
septal or atrial septal defect), the pulmonary arteryand pulmonary vasculature is prominent. In con-trast, patients with reduced pulmonary blood flow(as with tetralogy of Fallot or pulmonary atre-sia) may manifest a small pulmonary artery anddiminished vascularity. Some congenital lesions areassociated with classic radiographic cardiac silhou-ettes: the boot-shaped heart of tetralogy of Fallot,the “figure 8” heart of total anomalous pulmonaryvenous return, and the “egg-on-its-side”-shapedheart seen in D-transposition of the great arteries.
Stress testingPatients presenting for cardiac surgery frequentlyundergo stress testing to establish the diagnosis ofCAD, assess the severity of known CAD, establishthe viability of regions of myocardium, or eval-uate anti-anginal therapy. Stress testing may useexercise or pharmacological agents. Pharmacolog-ical agents are useful for patients with physicaldisabilities that preclude effective exercise. It alsois useful for patients who cannot reach an optimalexercise heart rate secondary to their medicationregimen (i.e. patients on beta-blockers).
Pharmacological stress testingPharmacologic stress testing uses dipyridamole,adenosine, or dobutamine. Pharmacologic stresstesting can be performed in conjunctionwith myocardial perfusion scintigraphy orechocardiography.Adenosine and dipyridamole are potent coro-
nary vasodilators that increase myocardial bloodflow three to fivefold independent of myocardialwork. Adenosine is a direct vascular smooth musclerelaxant via A2-receptors; whereas, dipyridamoleincreases adenosine levels by inhibiting adenosinedeaminase. Dobutamine increases myocardial workthrough increases in heart rate and contractility viaβ1-receptors. The increased work produces propor-tional increases in myocardial blood flow. In thissense, dobutamine stress testing is similar to exercisestress testing.The hyperemic response to adenosine and dipyri-
damole produce increased myocardial blood flowin regions supplied by normal coronary arteries.In regions of myocardium supplied by steal prone

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 6 — #6
6 Chapter 1
anatomy or diseased coronary arteries, myocardialblood flow increases will be attenuated or decreasedbelow resting levels.Dipyridamole is infused at 0.56–0.84mg/kg for
4minutes, followed by injection of the radiophar-maceutical for myocardial perfusion scintigraphy3minutes later. If infusion produces headache,flushing, gastrointestinal (GI) distress, ectopy,angina, or ECG evidence of ischemia, the effectcan be terminated with aminophylline 75–150mgintravenously (IV). Adenosine is infused at140µg/kg/min for 6minutes with injection ofthe radiopharmaceutical for myocardial perfu-sion scintigraphy 3minutes later. Side effectsare similar to dipyridamole and are termi-nated by stopping the infusion (the half-life ofadenosine is 40 seconds). Dobutamine is infused at5µg/kg/min for 3minutes and then is increased to10µg/kg/min for 3minutes. The dose is increasedby 5µg/kg/min every 3minutes until a maximumof 40µg/kg/min is reached or until significantincreases in heart rate and blood pressure occur.Injection of the radiopharmaceutical for myocar-dial perfusion scintigraphy takes place 1minuteafter the desired dose is reached, and the infusionis continued for 1–2minutes after injection. Sideeffects of dobutamine (headache, flushing, GI dis-tress, ectopy, angina, or ECG evidence of ischemia)can be terminated by discontinuing the infusion(the half-life of dobutamine is 2minutes).
Exercise stress testingExercise stress testing increases in myocardialoxygen consumption to detect limitations in coro-nary blood flow. Exercise increases cardiac out-put through increases in heart rate and inotropy.Despite vasodilatation in skeletal muscle, exercisetypically increases arterial blood pressure as well.As a result, exercise is accompanied by increases inthe three major determinants of myocardial oxygenconsumption: heart rate, wall tension, and contrac-tility. Tomeet the demands of exercise, the coronaryvascular bed dilates. The ability of the coronarycirculation to increase blood flow tomatch exercise-induced increases in demand is compromised in thedistribution of stenosed coronary arteries becausevasodilatory reserve is exhausted in these beds.
All exercise tests increase metabolic rate andoxygen consumption (VO2). Isometric exercisemay be used to increase the workload, but morecommonly, dynamic exercise using either a tread-mill or a bicycle is used. VO2max is the maximalamount of oxygen a person can use while per-forming dynamic exercise. VO2max is influencedby age, gender, exercise habits, and cardiovascu-lar status. Exercise protocols are compared by usingmetabolic equivalents (METs). One MET is equal toa VO2 of 3.5mL oxygen(O2)/kg/min and representsresting oxygen uptake. Different exercise protocolsare compared by comparing the number of METsconsumed at various stages.The Bruce treadmill protocol is the most com-
monly used protocol for exercise stress testing.This protocol uses seven 3-minute stages. Eachprogressive stage involves an increase in boththe grade and the speed of the treadmill. Dur-ing stage 1 the treadmill speed is 1.7miles/h ona 10% grade (5 METs); during stage 5 the tread-mill speed is 5miles/h on an 18% grade (16 METs).The patient progressively moves through thestages until either exhausted, a target heart rateachieved without ischemia, or the detection ofischemic changes on the ECG. Exercise stress test-ing can be performed in conjunction with tradi-tional ECG analysis, myocardial perfusion scintig-raphy, or echocardiography. The details of stressmyocardial perfusion scintigraphy, stress radionu-cleotide angiography, and stress echocardiographyare discussed below.The following factors must be considered in
interpretation of an ECG exercise stress test:• Angina. Ischemia may present as the patient’stypical angina pattern; however, angina is not auniversal manifestation of ischemia in all patients.Ischemic pain induced by exercise is stronglypredictive of CAD.• VO2max. If patients with CAD reach 13 METs,their prognosis is good regardless of other fac-tors; patients with an exercise capacity of less than5 METs have a poor prognosis.• Dysrhythmias. For patients with CAD, ventricu-lar dysrhythmias may be precipitated or aggravatedby exercise testing. The appearance of reproduciblesustained (>30 seconds) or symptomatic ventricular

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 7 — #7
Introduction 7
tachycardia (VT) is predictive of multivessel diseaseand poor prognosis.• ST segment changes. ST segment depression is themost common manifestation of exercise-inducedmyocardial ischemia. The standard criterion for anabnormal response is horizontal or down sloping(>1mm) depression 80ms after the J point. Downsloping segments carry a worse prognosis than hor-izontal segments. The degree of ST segment depres-sion (>2mm), the time of appearance (startingwith<6 METs), the duration of depression (persisting>5minutes into recovery), and the number ofECG leads involved (>5 leads) are all predictive ofmultivessel CAD and adverse prognosis.• Blood pressure changes. Failure to increase systolicarterial blood pressure to greater than 120mmHg,or a sustained decrease in systolic blood pressurewith progressive exercise, is indicative of cardiacfailure in the face of increasing demand. This findingsuggests severe multivessel or left main CAD.
Comparison of stress test methodsThe sensitivity of detection of CAD with exer-cise myocardial perfusion scintigraphy or exerciseechocardiography is superior to that of exerciseECG testing. The superiority of these two modal-ities over ECG testing in detecting CAD is great-est for patients with single vessel CAD. Whencomparing myocardial perfusion scintigraphy tostress echocardiography, the data suggest a trendtoward greater sensitivity with myocardial per-fusion scintigraphy, particularly for patients withsingle-vessel disease. Moderate to large perfusiondefects by either stress echocardiography or thal-lium imaging predicts postoperative myocardialinfarction or death in patients scheduled for elec-tive noncardiac surgery. Negative tests assure theclinician of a small likelihood of subsequent adverseoutcome (negative predictive value = 99%). Unfor-tunately, however, the positive predictive value(i.e. the chance that a patient with a positive testwill have an adverse cardiovascular event) is poorranging from 4% to 20%. In a meta-analysis com-paring the two techniques, stress echocardiographyis slightly superior to thallium imaging in predictingpostoperative cardiac events. The choice of whichtechnique should be made based upon institutional
expertise and patient-specific attribute. In eithercase, angiography should be considered in patientswith moderately large defects.Limitations of exercise ECG testing are the inabil-
ity to accurately localize and assess the extentof ischemia. Furthermore, no direct informationregarding left ventricle function is available. Stressmyocardial perfusion scintigraphy, radionuclideangiography, and echocardiography provide thisinformation. On the other hand, these methods aremore expensive and technically more demandingthan exercise ECG testing.
Myocardial perfusion scintigraphyMyocardial perfusion scintigraphy assesses myocar-dial blood flow, myocardial viability, the numberand extent of myocardial perfusion defects, tran-sient stress-induced LV dilatation, and allows forrisk stratification. Myocardial perfusion scintigra-phy is performed most commonly in conjunc-tion with stress testing. Stress testing can beaccomplished with exercise or pharmacologicallywith dipyridamole, adenosine, or dobutamine.Withthis technology, it is possible to determine whichregions of myocardium are perfused normally,which are ischemic, which are stunned or hibernat-ing, and which are infarcted. The technique is basedon the use of radiopharmaceuticals that accumulatein the myocardium proportional to regional bloodflow. Single-positron emission computed tomogra-phy (SPECT) or planar imaging is used to imageregional myocardial perfusion in multiple viewsand at variousmeasurement intervals. Patients withsmall fixed perfusion defects have reduced periop-erative risk profiles, whereas patients with multiplelarger defects are at higher risk.The radiopharmaceuticals currently in use are
thallium-201 and technetium-99m methoxyiso-butyl isonitrile (Sestamibi). Thallium has biologicproperties similar to potassium and thus is trans-ported across the myocardial cell membrane bythe sodium–potassium adenosine triphosphatase(ATPase) pump proportional to regional myocar-dial blood flow. Sestamibi is not dependent onATP to enter myocardial cells because it is highlylipophilic but its distribution in myocardial tissue isproportional to blood flow.

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 8 — #8
8 Chapter 1
ThalliumThallium-201 is injected at the peak level of a mul-tistage exercise or pharmacological stress test. Scin-tillation imaging begins 6–8minutes after injection(early views) and is repeated again 2–4hours afterinjection (delayed or redistribution views). Identi-cal views must be used so the early and delayedimages can be compared. During stress, myocardialblood flow and thallium-201 uptake will increase inareas of the myocardium supplied by normal coro-nary arteries. Subsequently, thallium redistributesto other tissues, thus clearing from the myocardiumslowly. Areas of myocardium supplied by diseasedarteries are prone to ischemia during stress andhave a reduced ability to increase myocardial bloodflow and thallium-201 uptake. These areas willdemonstrate a perfusion defect when comparedwith normal regions in the early views. In thedelayed views, late accumulation or flat washoutof thallium-201 from the ischemic areas comparedwith the nonischemic areas results in equalizationof thallium-201 activity in the two areas. Thesereversible perfusion defects are typical of areas ofmyocardium that suffer transient, stress-inducedischemia. Nonreversible perfusion defects are presentin both the early stress and delayed redistributionimages. These defects are believed to represent areasof nonviable myocardium resulting from old infarc-tions. Reverse redistribution is the phenomenon inwhich early images are normal or show a defect andthe delayed images show a defect or a more severedefect. This is seen frequently in patients who haverecently undergone thrombolytic therapy or angio-plasty and may result from higher-than-normalblood flow to the residual viable myocardium in thepartially infarcted zone.Modified thallium scintigraphy protocols are use-
ful in detecting areas hibernating myocardium.Hibernating myocardium exhibits persistentischemic dysfunction secondary to a chronic reduc-tion in coronary blood flow, but the tissue remainsviable. Hibernating myocardium has been shownto exhibit functional improvement after surgicalrevascularization or angioplasty and restoration ofcoronary blood flow. Stunned myocardium, in con-trast, has undergone a period of transient hypop-erfusion with subsequent reperfusion. As a result,
these regions exhibit transient postischemic dys-function in the setting of normal coronary bloodflow. Stunned myocardium is detected by identify-ing regions of dysfunctional myocardium in whichno perfusion defect exists.Some regions of myocardium that do not
exhibit redistribution at 2.5–4.0 hours exhibit redis-tribution in late images at 18–24hours. Thislate redistribution represents areas of hibernatingmyocardium. Another approach to detecting hiber-nating myocardium is reinjection of thallium at restafter acquisition of the 2.5–4.0-hour stress images.Persistent defects that show enhanced uptake afterreinjection represent areas of viable myocardium.Finally, serial rest thallium imaging has proved use-ful in detecting hibernating myocardium. Imagesare obtained at rest after injection of thalliumand then are repeated 3hours later. Regionsof myocardium that exhibit rest redistributionrepresent areas of viable myocardium.Increased lung uptake of thallium is related to
exercise-induced LV dysfunction and suggests mul-tivessel CAD. Because increased lung uptake ofthallium is due to an elevated left atrial pressure(LAP), other factors besides extensive CAD andexercise-induced LV dysfunction (such as mitralstenosis, mitral regurgitation, and nonischemic car-diomyopathy) must be considered when few or nomyocardial perfusion defects are detected. TransientLV dilation after exercise or pharmacologic stressalso suggests severe myocardial ischemia.
SestamibiSestamibi, unlike thallium, does not redistribute.As a result, the distribution of myocardial bloodflow at the time of injection remains fixed overthe course of several hours. This necessitates twoseparate injections: one at rest and one at peakstress. The two studies must be performed so thatthe myocardial activity from the first study decaysenough not to interfere with the activity from thesecond study. A small dose is administered at restwith imaging approximately 45–60minutes later.Several hours later, a larger dose is administeredat peak stress, with imaging 15–30minutes later.Reversible and fixed defects are detected by com-paring the rest and stress images. As with thallium,

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 9 — #9
Introduction 9
late imaging after Sestamibi stress imaging may behelpful in detecting hibernating myocardium.Sestamibi allows high-count-density images to be
recorded, providing better resolution than thallium.In addition, use of Sestamibi allows performance offirst pass radionuclide angiography (see below) tobe performed in conjunctionwithmyocardial perfu-sion scintigraphy. Use of simultaneous radionuclideangiography and perfusion scintigraphy has proveduseful in enhanced detection of viable myocardium.Viable myocardium will exhibit preserved regionalperfusion in conjunction with preserved regionalwall motion.
Radionuclide angiographyRadionuclide angiography allows assessment ofRV and LV performance. Two types of cardiacradionuclide imaging exist: first-pass radionuclideangiography (FPRNA) and equilibrium radionu-clide angiography (ERNA), also known as radionu-clide ventriculography or gated blood pool imaging.ERNA is also known as multiple-gated acquisition(MUGA) ormultiple-gated equilibrium scintigraphy(MGES).FPRNA involves injection of a radionuclide bolus
(normally technetium-99m) into the central circu-lation via the external jugular or antecubital vein.Subsequent imaging with a scintillation camera in afixed position provides a temporal pictorial presen-tation of the cardiac chambers as the radiolabeledbolus makes its way through the heart. First-passstudies may be gated or ungated. Gated studiesinvolve synchronization of the presented imageswith the patient’s ECG such that systole and dias-tole are identified. Ungated studies simply present aseries of images over time.ERNA involves use of technetium-99m-labeled
red cells, which are allowed to distribute uniformlyin the blood volume. Radiolabeling of red cells isaccomplished by initially injecting the patient withstannous pyrophosphate, which creates a stannous-hemoglobin complex over the course of 30minutes.Subsequent injection of a technetium-99m bolusresults in binding of technetium-99m to thestannous-hemoglobin complex, thus labeling thered cells.
After equilibrium of the labeled red cells in thecardiac blood pool, gated imaging with a scintil-lation camera is performed. A computer dividesthe cardiac cycle into a predetermined number offrames (16–64). Each frame represents a specifictime interval relative to the ECG R wave. Datacollected from each time interval over the courseof several hundred cardiac cycles are then addedtogether with the other images from the same timeinterval. The result is a sequence of 16–64 images,each representing a specific phase of the cardiaccycle. The images can be displayed in an endlessloop format or individually. The procedure canthen be repeated with the camera in a differentposition.Below is a summary of the relative advantages
and disadvantages of first-pass and equilibrationstudies. Both types of studies currently are used foradults, infants, and children.• With both FPRNA and ERNA studies, the num-ber of radioactive counts during end systole andend diastole can be used to determine strokevolume, ejection fraction, and cardiac output.• Both types of studies allow reliable quantificationof LV volume using count-proportional methodsthat do not require assumptions to be made aboutLV geometry.• Although both studies allow determination of RVand LV ejection fractions, determination of RV ejec-tion fraction is more accurate with a first-pass studybecause the right atrium overlaps the right ventriclein equilibrium studies.• First-pass studies allow detection and quantifica-tion of both right-to-left and left-to-right intracar-diac shunts, whereas shunt detection is not possiblewith equilibration studies.• First-pass studies allow sequential analysis ofright atrial (RA), RV, left atrial (LA), and LV size,whereas equilibration studies do not. Abnormalitiesin the progression of the radioactive tracer throughthe heart and great vessels assist in the diagnosis ofcongenital abnormalities.• Equilibration studies provide better analysis ofregional wall motion abnormalities than first-passstudies due to higher resolution.• Both types of studies can be used with exer-cise. First-pass studies can be performed rapidly

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 10 — #10
10 Chapter 1
but do not allow assessment of ventricular wallmotion at different exercise levels, nor do they allowassessment of wall motion from different angles.• Mitral or aortic regurgitation is detectable withboth first-pass and equilibration studies by analysisof the stroke volume ratio. This method tends tooverestimate regurgitant fraction and is not reliablefor detection of minor degrees of regurgitation.
EchocardiographyTransthoracic and transesophageal echocardiogra-phy has revolutionized the noninvasive structuraland functional assessment of acquired and con-genital heart disease. Transthoracic echocardiogra-phy (TTE) and transesophageal echocardiography(TEE) often play a major role in the evaluationof cardiac surgical patients. Routine use of two-dimensional imaging, color flow Doppler, contin-uous wave Doppler, pulsed wave Doppler, andM-mode imaging allows the following:• Assessment of cardiac anatomy. Delineation of themost complex congenital heart lesions is feasi-ble. In many instances, information acquired froma comprehensive echocardiographic examinationis all that is necessary to undertake a surgicalrepair.• Assessment of ventricular function. A comprehen-sive assessment of RV and LV diastolic and systolicfunction is feasible.• Assessment of valvular abnormalities. Assessmentof the functional status of all four cardiac valvesis possible. In addition, quantification of valvularstenosis and insufficiency is accurate and reliable.Assessment of prosthetic valves also is feasible.• Characterization of cardiomyopathies. Hypertrophic,dilated, and restrictive cardiomyopathies can beidentified.• Assessment of the pericardium. Pericardial effusions,cardiac tamponade, and constrictive pericarditis arereliably identified.• Assessment of cardiac and extracardiac masses. Vege-tations, foreign bodies, thrombi, and metastatic andprimary cardiac tumors can be identified.• Contrast echocardiography. Contrast solutions con-taining microbubbles enhance the image allowingassessment of myocardial perfusion, intracardiac
shunts, enhancement of Doppler signals, andimproved assessment of regional and global LVfunction.• Stress echocardiography. Stress echocardiography isbased on the concept that exercise or pharmacolog-ically induced wall motion abnormalities developearly in the course of ischemia. Stress-inducedwall motion abnormalities occur soon after perfu-sion defects are detected by radionuclide imagingbecause, in the ischemic cascade, hypoperfusionprecedes wall motion abnormalities. Comparisonof resting and stress images allows resting abnor-malities to be distinguished from stress-inducedabnormalities. Resting abnormalities indicate priorinfarction, hibernating or stunned myocardium;whereas, stress-induced abnormalities are spe-cific for ischemia. Furthermore, dobutamine stressechocardiography may be useful in determin-ing myocardial viability. Regions that are hypo-kinetic, akinetic, or dyskinetic at rest and improvewith dobutamine administration probably containareas of stunned or hibernating myocardium. Suchareas demonstrate functional improvement aftermyocardial revascularization.
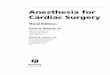
Computerized tomography and magneticresonance imagingAdvances in imaging techniques have played amajor role in defining anatomy in cardiac surgi-cal patients. Computerized tomography (CT) andmagnetic resonance imaging (MRI) now allow theclinician detailed anatomy, three-dimensional ren-dering, and functional assessment of myocardialperformance and blood flow (Fig. 1.1). It is likelythat new advances in imaging techniques will con-tinue to improve the quality and the anatomic detailafforded by these techniques. Molecular imaging,i.e. imaging of cellular function, is a developing areain cardiac imaging. The applications of these newtechnologies remain to be seen.
Cardiac catheterizationCardiac catheterization remains the gold standardfor evaluation of acquired and congenital heartdisease. Cardiac catheterization is covered in detailin Chapter 2.

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 11 — #11
Introduction 11
Fig. 1.1 Three dimension reconstruction of the heartand aorta
Respiratory evaluation
A preoperative assessment of pulmonary function(other than CXR) is required in all cardiac surgi-cal patients. The evaluation must include a historyof known pulmonary disease, current respiratorysymptoms, and a physical examination. Evalua-tion may include consultation with specialists andspecific pulmonary testing (pulmonary functiontesting, spirometry, pulse oximetry, arterial bloodgas analysis). The history should determine theextent and length of tobacco use, the presence ofCOPD, asthma, recurrent or acute pulmonary infec-tions, and the presence of dyspnea. Physical exam-ination should focus on the detection of wheezes,flattened diaphragms, air trapping, consolidations,and clubbing of the nails. A CXR is indicated innearly all cardiac surgical patients. Pulmonary func-tion tests (PFTs) play a limited role in preoperativeassessment. If there is confusion about whetherintrinsic pulmonary disease exists, its cause, andits appropriate treatment, then pulmonary func-tion testing may help guide the clinician. Spirom-etry measures lung volumes, capacities, and flow.Spirometry of expiratory flow rates allowsmeasure-ment of the forced expiratory volume in 1 second
(FEV1), the forced vital capacity (FVC), and theforced mid-expiratory flow (FEF 25–75%). Arterialblood gases should be obtained for patients inwhomcarbon dioxide (CO2) retention is suspected and forthose with severe pulmonary dysfunction as deter-mined by history, physical examination, PFTs, orcardiac catheterization.
Pulmonary assessment and congenitalheart diseaseLesions that produce excessive pulmonary bloodflow (large ventricular septal defect, truncus arte-riosus, dextrotransposition of the great arteries,and patent ductus arteriosus) are associated withpulmonary dysfunction. Occasionally, large airwaycompression occurs in response to enlargementof the pulmonary arteries. More commonly, how-ever, these lesions produce pulmonary vascularchanges that affect pulmonary function. The pul-monary vascular smooth muscle hypertrophy thataccompanies increased pulmonary blood flow pro-duces peripheral airway obstruction and reducedexpiratory flow rates characteristic of obstructivelung disease. In addition, smooth muscle hypertro-phy in respiratory bronchioles and alveolar ductsin patients with increased pulmonary blood flowcontributes to this obstructive pathology. Thesechanges predispose the patient to atelectasis andpneumonia. Children with Down syndrome havea more extensive degree of pulmonary vascularand parenchymal lung disease than other childrenwith similar heart lesions. This predisposes patientswith Down syndrome to greater postoperativerespiratory morbidity and mortality.Patients with lesions that reduce pulmonary
blood flow (pulmonary atresia or stenosis, tetralogyof Fallot) also have characteristic pulmonary func-tion changes. These patients have normal lung com-pliance as compared with the decreased complianceseen in patients with increased pulmonary bloodflow. However, the large dead space to tidal volumeratio in these patients greatly reduces ventilationefficiency, and large tidal volumes are required tomaintain normal alveolar ventilation. Finally, 3–6%of patients with tetralogy of Fallot will have anabsent pulmonary valve and aneurysmal dilata-tion of the pulmonary arteries. This aneurysmal

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 12 — #12
12 Chapter 1
dilatation produces bronchial compression andrespiratory distress at birth.
Pulmonary assessment and acquiredheart diseasePulmonary dysfunction ranks among the highestpredictors of postoperative pulmonary complica-tions. Pulmonary dysfunction is defined as a pro-ductive cough, wheeze, or dyspnea. Pulmonaryfunction testing consistent with pulmonary dys-function shows a FEV1 < 70% of predictedor FEV1/FVC < 65% of predicted, plus eithervital capacity (VC) < 3.0 L or maximum volun-tary ventilation (MVV ) < 80L/min. For patientsundergoing valvular surgery, the presence of pul-monary dysfunction is associated with up to a2.5-fold increase in perioperative mortality and a2.5-fold increase in postoperative respiratory com-plications. For patients undergoing only coronaryrevascularization, pulmonary dysfunction is lesspredictive of postoperative morbidity andmortality.
Pulmonary assessment and tobacco useChronic tobacco use has several physiologic effectsthat may complicate anesthetic management.Smoking accelerates the development of atheroscle-rosis. Further, smoking reduces coronary blood flowby increasing blood viscosity, platelet aggregation,and coronary vascular resistance. Nicotine, throughactivation of the sympathetic nervous system andelevated catecholamine levels, increases myocardialoxygen consumption by increasing heart rate, bloodpressure andmyocardial contractility. Furthermore,the increased carboxyhemoglobin level, which mayexceed 10% in smokers, reduces systemic andmyocardial oxygen delivery. This is particularlydetrimental to the patient with CAD due to the highextraction of oxygen that normally occurs in themyocardium. The threshold for exercise-inducedangina is reduced by carboxyhemoglobin levels aslow as 4.5%. Short-term abstinence (12–48hours)is sufficient to reduce carboxyhemoglobin and nico-tine levels and improve the work capacity of themyocardium.There is an increased incidence of postoperative
respiratory morbidity in patients who smoke. These
complications include respiratory failure, unantic-ipated intensive unit admission, pneumonia, air-way events during induction of anesthesia (cough,laryngospasm), and increased need for postopera-tive respiratory therapy. Smoking increases mucussecretion, impairs tracheobronchial clearance, andcauses small airway narrowing. For patients under-going coronary revascularization, abstinence fromsmoking for 2months may reduce the incidenceof postoperative respiratory complications. Absti-nence for less than 2months is ineffective inreducing the incidence of postoperative respiratorycomplications. Similar studies of patients under-going other surgical procedures have confirmedthe necessity of a 4–6-week abstinence period.Typically, tobacco-using patients presenting for car-diac surgery will not have had the recommendedabstinence period required to reduce complications.Acute cessation of smoking during the perioperativeperiod is not associated with elevated risk. Thereis no added cardiovascular risk for patients usingnicotine replacement therapy (NRT).
Pulmonary assessment and asthmaAsthma is characterized by paroxysmal or persis-tent symptoms of wheezing, chest tightness, dys-pnea, sputum production, and cough with airflowlimitation. There is hyper-responsiveness to endo-genous or exogenous stimuli. Preoperative evalua-tion of asthma confirms the diagnosis and evaluatesthe adequacy of treatment. Adequate control isdemonstrated when the patient reports normalphysical activity, mild and infrequent exacerba-tions, no missed school or work days, and lessthan four doses of β2-agonist therapy per week.Long-term treatment is largely preventive in nature.First-line pharmacologic treatment often incorpo-rates inhaled corticosteroids (ICSs). Beclometha-sone significantly improves FEV1, peak expiratoryflow, and reduces β-agonist use and exacerba-tions. Leukotriene receptor antagonists (LTRAs) aresometimes used as first-line therapy; however, theirrole is less clearly established when compared tothe ICS agents. Long-acting β2-agonists are safe andeffective medications for improving asthma controlin older children and adults when ICSs therapy doesnot adequately control the disease. Theophylline is

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 13 — #13
Introduction 13
less effective than ICSs and LTRAs in improvingasthma control.For patients in whom bronchospasm is well con-
trolled preoperatively, it is essential to continuetherapy during the perioperative period. Beta-2-agonist metered-dose inhaler or nebulizer therapycan be continued until arrival in the operating roomand can be restarted soon after emergence fromanesthesia. Metered-dose inhalation therapy can bedelivered via the endotracheal tube. For patients noton bronchodilator therapy who present for surgerywith bronchospasm, a trial of bronchodilators withmeasurement of PFTs before and after therapy isoften helpful. An increase in the FEV1 of 15% ormore after inhalation of a nebulized bronchodilatorsuggests a reversible component of bronchospasm.Surgery should be delayed until the asthma is con-trolled. If this is not possible, acute therapy withsteroids and β2-agonists is indicated. Therapy forthe cardiac surgical patient should be initiated witha β2-selective metered-dose inhaler or nebulizedsolution.
Renal function
Patients presenting for cardiac surgery may pos-sess varying degrees of renal dysfunction rangingfrommild elevations in creatinine to dialysis depen-dence. Assessing renal function preoperatively isvitally important in the cardiac surgical patient.Renal dysfunction after cardiac surgery is associ-ated with increased mortality, morbidity, resourceutilization and intensive care unit stay. Dependingon the definition of acute renal failure (ARF), any-where from 5% to 30% of patients demonstraterenal dysfunction after cardiac procedures. Renaldysfunction requiring dialysis is associated with a50–80% increased risk of death. ARF is among thestrongest predictors for death with an odds ratioof 7.9 (95% confidence interval 6–10) in cardiacsurgical patients. Identification of high-risk can-didates remains important for appropriate patientconsent, risk-benefit analysis, and hospital resourceutilization planning (Table 1.5).The dialysis-dependent patient will require dial-
ysis preoperatively. If dialysis is unobtainablepreoperatively, it can be managed intraoperatively.
Table 1.5 Risk factors for acute renal failure aftercardiac surgery.
Female genderCongestive heart failureLV ejection fraction <35%Preoperative use of an intraaortic balloon pumpChronic obstructive pulmonary diseasePrevious cardiac surgeryEmergency surgeryValve or valve+ CABG surgeryElevated preoperative creatinine
CABG, coronary artery bypass graft.
Dialysis will correct or improve the abnormalities inpotassium, phosphate, sodium, chloride, and mag-nesium. In addition, the platelet dysfunction thataccompanies uremia will be improved. L-deamino-8-D-arginine vasopressin (DDAVP) administrationmay improve uremia-induced platelet dysfunctionand should be considered if clinically significantpost-dialysis platelet dysfunction exists. Dialysiswill not favorably affect the anemia, renovascu-lar hypertension, or immune-system compromiseassociated with chronic renal failure.For nondialysis-dependent patients, preoperative
hydration is necessary to prevent prerenal azotemiafrom complicating the underlying renal dysfunc-tion. This is particularly important after proceduressuch as cardiac catheterization with arteriography.Creatinine clearance falls after contrast arterio-graphy; in patients with preexisting azotemia, thisreduction is much more likely to result in ARF.Hydration ameliorates contrast-induced renal dys-function. Treatmentwith acetylcysteine and sodiumbicarbonate reduce post-contrast ARF.Patients with renal transplants occasionally
present for cardiac surgical procedures. The extra-renal component of renal blood flow autoregula-tion is absent in the denervated kidney. Therefore,preoperative hydration and maintenance of sys-temic perfusion pressure are particularly importantto maintain renal perfusion. Sterile technique ismandatory in these immunocompromised patients.Renal dysfunction often results in electrolyte
imbalance. Potassium regulation is often difficultin the cardiac surgical patient. Hyperkalemia

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 14 — #14
14 Chapter 1
(>5.5mEq/L) is uncommon in patientswith normalrenal function; however, it may occur with injudi-cious potassium administration. Themajor causes ofhyperkalemia result from diminished renal excre-tion of potassium secondary to reduced glomerularfiltration rate (acute oliguric renal failure, chronicrenal failure). Reduced tubular secretion may leadto hyperkalemia as seen in Addison’s disease,potassium-sparing diuretics and angiotensin con-verting enzyme inhibitors. Other causes includetranscellular shifts of potassium as seen in acido-sis, trauma, burns, beta-blockade, rhabdomyolysis,hemolysis, diabetic hyperglycemia, and depolar-izing muscle paralysis with succinylcholine. Theclinical manifestations relate to alterations in car-diac excitability. Peaked T waves will appear with apotassium level of 6.5mEq/L. At levels of 7–8mEq/Lthe PR interval will prolong and the QRS complexwill widen. At 8–10mEq/L sine waves appear andcardiac standstill is imminent. Treatment is multi-modal and includes glucose, insulin, bicarbonateand β-agonists (shifting potassium to the intracel-lular compartment), diuretics, exchange resins anddialysis (enhancing potassiumelimination), and cal-cium (no change in serum potassium concentra-tion, but calcium counteracts the cardiac conductioneffects of hyperkalemia).Hypokalemia (<3.5mEq/L) is not uncommon in
the cardiac surgical patient. The most common eti-ology is chronic diuretic therapy, but other causessuch as GI loss (nasogastric suction, diarrhea, vom-iting), mineralocorticoid excess, acute leukemia,alkalosis, barium ingestion, insulin therapy, vita-min B12 therapy, thyrotoxicosis and inadequateintake must be considered. The clinical manifesta-tions of hypokalemia are observed in skeletal mus-cle, heart, kidneys, and the GI tract. Neuromuscularweakness is observed with levels of 2.0–2.5mEq/L.Hypokalemia leads to a sagging of the ST segment,depression of the T wave, and the appearance of aU wave on the ECG. In patients treated with digi-talis, hypokalemia may precipitate serious arrhyth-mias. Treatment of hypokalemia involves eitheroral or parenteral replacement. A deficit in serumpotassium reflects a substantial total body deficit.A decrease in plasma potassium concentration of1mEq/Lwith a normal acid-base balance represents
approximately 300mEq of total body potassiumdeficiency. In preparing the cardiac surgical patientfor surgery, it is reasonable to maintain serumpotassium higher than 3.5mEq/L for patients ondigitalis, those at high risk for myocardial ischemiaand those who have suffered acute reductions inserum potassium. Potassium replacement is notwithout risk (iatrogenic hyperkalemia). In gen-eral, potassium replacement should not exceed10–20mEq/h or 200mEq/day. Serum potassiummust be closely monitored during the replacementtherapy.
Endocrine evaluation
A careful evaluation for endocrine abnormalitiesshould be sought in the history and physical exami-nation. Diabetes mellitus (DM) and hypothyroidismdeserve special consideration.
Diabetes mellitusDiabetes mellitus is a risk factor for developmentof CAD; therefore, perioperative management ofDM is a common problem facing those who anes-thetize patients for cardiac surgery. Patients withinsulin-dependent diabetes have reduced or absentinsulin production due to destruction of pancre-atic beta cells. Patients with noninsulin-dependentdiabetes have normal or excessive production ofinsulin but suffer from insulin resistance. Thisresistance may be due to a reduction in insulinreceptors, a defect in the second messenger onceinsulin binds to receptors, or both. Patients withnoninsulin-dependent diabetes may be managedwith diet, oral hypoglycemic agents (agents thatincrease pancreatic insulin production), or exoge-nous insulin. Patients with insulin-dependent dia-betes must receive exogenous insulin.Cardiopulmonary bypass (CPB) is associated with
changes in glucose and insulin homeostasis in bothdiabetic and nondiabetic patients. During normoth-ermic CPB, elevations in glucagon, cortisol, growthhormone, and catecholamine levels produce hyper-glycemia through increased hepatic glucose produc-tion, reduced peripheral use of glucose, and reduced

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 15 — #15
Introduction 15
insulin production. During hypothermic CPB, hep-atic glucose production is reduced and insulin pro-duction remains low such that blood glucose lev-els remain relatively constant. Rewarming on CPBis associated with increases in glucagon, cortisol,growth hormone, and catecholamine levels and isaccompanied by enhanced hepatic production ofglucose, enhanced insulin production, and insulinresistance. The transfusion of blood preserved withacid-citrate-dextrose, the use of glucose solutions inthe CPB prime, and the use of β-adrenergic agentsfor inotropic support, further increase exogenousinsulin requirements. For nondiabetic patients,these hormonally mediated changes usually resultin mild hyperglycemia. For diabetic patients, thesechanges may produce significant hyperglycemiaand ketoacidosis.Management of perioperative glucose is directly
related to perioperative outcome. Uncontrolled, orpoorly controlled, perioperative glucose is associ-ated with increasedmortality, wound infection, andintensive care unit length of stay. This relationshipis true in cardiac and noncardiac surgical patientsadmitted to an intensive care unit setting. The ideallevel of glucose is unknown; however, if a targetof 130mg/dL can be achieved, this is associatedwith improved clinical outcome. Administration ofexogenous insulin should be administered early inthe perioperative period to achieve this goal. Theclinician must remember that achieving this goalmay be impossible in some patients. Insulin resis-tance and the physiologic conditions encouraginghyperglycemia may be too great in some patients.Similarly, the clinician must exercise caution whenadministering insulin. Serum glucose levels shouldbe checked as frequently as every 15–30minutesperioperatively while insulin therapy is utilized.Unrecognized hypoglycemia can adversely affectpatient outcome.Because of the varying insulin requirements dur-
ing cardiac surgery and the unreliable absorptionof subcutaneously administered insulin in patientsundergoing large changes in body temperatureand peripheral perfusion, insulin is best deliveredIV for patients undergoing cardiac surgery. Thegoal of therapy should be maintenance of normo-glycemia during the pre-CPB, CPB, and post-CPB
Table 1.6 Recommendations for insulin administration.
Bloodglucose(mg/dL)
Insulininfusionrate(U/kg/h)
Rate in100kgpatient(U/h)∗
150–200 0.02 2200–250 0.03 3250–300 0.04 4300–350 0.05 5350–400 0.06 6
∗ The actual rate of administration will vary from patientto patient and should be titrated against measured serumglucose levels and patient response.
periods. On the morning of surgery, the usualinsulin dose is withheld. On arrival in the operatingroom, the patient’s blood glucose is measured. Fortight control, a continuous regular insulin infu-sion can be started and adjusted to maintain bloodglucose between 100 and 150mg/dL during theoperative procedure. Determinations of blood glu-cose are made every 15–30minutes. Table 1.6provides guidelines for insulin administration. Itmust be emphasized that the alterations in glucosehomeostasis and the insulin resistance that accom-pany hypothermic CPB may necessitate alterationin infusion rates, and therefore insulin must betitrated against demonstrated patient response bymeasuring serial serum glucose levels.Patients taking oral hypoglycemic agents should
discontinue them at least 12hours before surgery.For patients managed with these agents andpatients managed with diet, blood glucose deter-minations should be made every 30–60minutesduring the operative procedure. These patientsfrequently require insulin infusions to maintainglucose homeostasis during surgery.
HypothyroidismHypothyroidism is characterized by a reduction inthe basal metabolic rate. In patients with hypothy-roidism cardiac output may be reduced by up to40% due to reductions in both heart rate and strokevolume. In addition, both hypoxic and hypercapnicventilatory drives are blunted by hypothyroidism.

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 16 — #16
16 Chapter 1
Furthermore, hypothyroidism may be associatedwith blunting of baroreceptor reflexes, reduced drugmetabolism, renal excretion, reduced bowel motil-ity, hypothermia, hyponatremia from syndrome ofinappropriate antidiuretic hormone (SIADH), andadrenal insufficiency. The hypothyroid patient maynot tolerate usual doses of antianginal drugs such asnitrates and β-adrenergic blocking agents. Hypothy-roid patients on beta-blockers typically require verylow anesthetic drug requirements.Despite these problems, thyroid replacement
for cardiac surgical patients, particularly thosewith ischemic heart disease, is not always desir-able. For hypothyroid patients requiring coronaryrevascularization, thyroid hormone replacementmay precipitate myocardial ischemia, myocar-dial infarction, or adrenal insufficiency. Coronaryrevascularization may be managed successfully inhypothyroid patients with thyroid replacementwithheld until the postoperative period. Mild tomoderate hypothyroid patients undergoing cardiacsurgery have perioperative morbidity and mortalitysimilar to euthyriod patients. Hypothyroid patientsmay experience delayed emergence from anesthe-sia, persistent hypotension, tissue friability, bleed-ing and adrenal insufficiency requiring exogenoussteroids. Hypothyroidism is preferentially treatedwith levothyroxine (T4). In healthy adults withoutCAD, a starting dose of 75–100µg/day is appro-priate. In elderly patients, and those with CAD,the initial dose is 12.5–25.0µg/day and is increasedby 25–50µg every 4–6weeks allowing for a slowincrease in metabolic rate thereby avoiding a mis-match in coronary blood supply and metabolicdemand.
Hematologic evaluation
By the nature of the surgery, and the associatedcardiovascular medications (heparin, clopidogrel),cardiac surgical patients are at higher periopera-tive risk of bleeding. A hemoglobin and hema-tocrit is indicated based on the invasiveness ofthe procedure (i.e. relative risk of blood loss andtransfusion), the history of liver disease, anemia,bleeding, other hematologic disorders or an extreme
in age. Serum chemistry (i.e. potassium, sodium,glucose, renal and liver function studies) are indi-cated in patients anticipating invasive surgery withpossible metabolic alterations, diabetic patients andother patients at specific risk of renal or liver dys-function. Plasma N-terminal pro-brain natureticpeptide (NTproBNP) is secreted by the left ven-tricle in response to wall stress. It is elevated inpatients with LV dysfunction and heart failure. Pre-operative NTproBNP levels greater than 450ng/Lare predictive of cardiac complications with a sen-sitivity of 100% and a specificity of 89%. Hence,an NTproBNP level may assist in preoperative riskassessment and resource management in selectedpatients. A urinalysis is usually not indicated unlessthere are specific urinary findings. A pregnancytest should be considered in all female patientsof childbearing age. Coagulation studies are indi-cated depending on the invasiveness of the proce-dure, a history of renal or liver dysfunction, and inpatients on anticoagulant medications.Medical management of acute coronary syn-
dromes, myocardial infarction, peripheral vasculardisease, atrial fibrillation, and stroke often includesantithromboticmedications such as aspirin, clopido-grel bisulfate, heparin, coumadin, and others. Thesemedications are common in patients presenting forcardiac surgery and may have a major impact onthemanagement and preoperative evaluation of thepatient. Patients may present with a long history ofaspirin or clopidogrel use. In the acute setting, hep-arin or shorter acting IIb/IIIa inhibiting agents suchas integrelin may be in use. These agents are ben-eficial in reducing the incidence of stent occlusion,myocardial infarction, or other thrombotic sequaelaof peripheral vascular disease or hyper-coagulation.A thoughtful plan regarding the continued admin-istration of these medications is required prior tothe operative procedure. In the case of clopido-grel, stable patients presenting for elective surgerymay be advised to stop the medication for 5 daysto reduce the risk of excessive bleeding duringthe operation. All of the agents, including aspirin,are associated with increased blood loss duringsurgery. The relative risk of stopping the agentversus the increased risk of excessive bleeding must

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 17 — #17
Introduction 17
be weighed in each patient. Consultation withsurgeon and cardiologist are recommended beforediscontinuing antithrombotic therapy.In addition to the medication history, all patients
scheduled for cardiac surgical procedures require acareful bleeding history with emphasis on abnor-mal bleeding occurring after surgical procedures,dental extractions and trauma. Signs of easy bruis-ing should be sought on physical examination.All patients should undergo laboratory screeningfor the presence of abnormalities in hemostasis.A platelet count, partial thromboplastin time (PTT),and prothrombin time (PT) should be obtained.Time permitting, all abnormalities should be eval-uated prior to surgery so that post-CPB hemostasisis not complicated by unknown or unsuspectedmedical conditions.
PT and PTT elevationsElevations in PT and PTT should be investigatedfor factor deficiencies, factor inhibitors, and thepresence of anticoagulants such as warfarin andheparin. It is important that documentation of anormal PTT and PT existing before warfarin orheparin administration is initiated so that othercauses of an elevated PTT and PT are not over-looked. Deficiencies of factors VIII, IX, and XIare most commonly encountered. These deficien-cies and their management are summarized in thefollowing sections.
Factor VIII deficiency (hemophilia A)The half-life of factor VIII in plasma is 8–12hours;normal persons have approximately 1unit offactor VIII activity per 1mLof plasma (100%activity).Patients with severe hemophilia A will have aslittle as 1% factor VIII activity, whereas mildlyaffected patients will have up to 50% activity.Patients present with an elevated PTT and varyingdegrees of clinical bleeding. The diagnosis is madeby a factor assay. Safe conduct of cardiac surgeryrequires 80–100% factor VIII activity during theoperative procedure, with maintenance of activitylevels in the 30–50% range for 7 days postopera-tively. An infusion of 1.0 unit of factor VIII perkilogram of body weight will increase the patient’s
factor VIII activity level by 2%. The 12-hour half-lifeof factor VIII requires that factor VIII be re-infusedevery 12hours during the perioperative period.Factor VIII may be provided with cryoprecipitate,which contains 100units of factor VIII per bag(10–20mL). Factor VIII concentrates that contain1000units of factor VIII in 30–100mL also mayprovide factor VIII.
Factor IX deficiency (hemophilia B)The half-life of factor IX in plasma is 24hours; nor-mal persons have approximately 1unit of factorIX activity per 1mL of plasma (100% activity).Factor IX deficiency is clinically indistinguishablefrom factor VIII deficiency. Diagnosis is made byfactor assay. Safe conduct of cardiac surgery requires60% factor IX activity during the operative pro-cedure, with maintenance of activity levels in the30–50% range for 7 days postoperatively. An infu-sion of 1.0 unit of factor IX per kilogram of bodyweight will increase the patient’s factor IX activ-ity level by 1%. The 24-hour half-life of factor IXrequires that factor IX be re-infused only every24hours during the perioperative period. Freshfrozen plasma (FFP) contains 0.8 units of all ofthe procoagulants per milliliter and generally isused to replace factor IX. A 250-mL bag of FFPwill provide 200 units of factor IX. For patients inwho factor IX replacement with FFP will requireinfusion of prohibitively large volumes, factor IXconcentrates are used.
Factor XI deficiency (Rosenthalsyndrome)The half-life of factor XI in plasma is 60–80hours;normal persons have approximately 1unit offactor XI activity per 1mLof plasma (100%activity).Factor XI deficiency is most common amongpatients of Jewish descent and is associated witha prolonged PTT. Many of these patients haveno symptoms or have a history of bleeding onlywith surgery or major trauma. The diagnosis ismade by factor assay. FFP administration replen-ishes factor XI. It is recommended that 10–20mLof FFP/kg/day be used during the preoperative andpostoperative periods to manage this deficiency.

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 18 — #18
18 Chapter 1
Platelet dysfunctionThrombocytopenia should be evaluated and treatedas necessary to avoid excessive operative bleeding.A platelet count and platelet function monitoringare important laboratory evaluations. The bleed-ing time is not a reliable predictor of perioperativeor postoperative bleeding. Other measurements ofplatelet dysfunction include thromboelastographyand assays of activated platelet aggregation (aggre-gometry). These evaluations provide informationon the functional integrity of platelet action. In thecase of thromboelastography, clot formation andfibrinolysis are observed. The information gainedprovides insight into both factor content and plateletfunction. The activated platelet aggregation assaysprovide both a total platelet count and a percent-age of active platelets. Platelet dysfunction can resultfrom a variety of causes.
ThrombocytopeniaThrombocytopenia may due to dilution (i.e. withmassive fluid replacement), increased peripheraldestruction (sepsis, disseminated intravascular coag-ulation, thrombotic thrombocytopenic prupura,prosthetic valve hemolysis or platelet antibodies)or sequestration (splenomegaly, lymphoma). Inthe cardiac surgical patient, dilutional thrombo-cytopenia is common. Thrombocytopenia is alsofrequently the result of platelet destruction from theCPB circuit and from activation of heparin inducedplatelet antibodies.Heparin-induced thrombocytopenia and throm-
bosis (HITT) occurs due to the presence of an anti-heparin-platelet factor 4 antibodies. The conditioncan be terminated by withdrawal of heparin ther-apy. Ideally, heparin therapy should not be restarteduntil in-vitro platelet aggregation in response toheparin no longer occurs. Heparin induced throm-bocytopeniamay re-occur up to 12months after theinitial episode. Patients with HITT requiring CPBbefore the antibody can be cleared present a man-agement problem. These patients may be treatedby a variety of alternate anticoagulation agents.Direct thrombin inhibitors such as danaparoid, lep-irudin, bivalirudin, and argatroban have all beenused with success. Other agents such as tirofibanand epoprostenol have been used in combination
with unfractionated heparin with good result. Inthe preoperative setting, identification of patientswho have experienced HITT is paramount. If HITTis diagnosed, then the surgery should either bedelayed long enough to clear the heparin antibodies(usually 90–100 days), or an alternate anticoagu-lation strategy devised. If heparin re-exposure isconsidered, testing for the presence of HITT anti-bodies, generally by enzyme-linked immunosobentassay (ELISA), is required.
Qualitative platelet defectsAbnormalities in platelet function are observedwithsome medications, renal failure, hepatic failure,paraproteinemias (i.e. multiple myeloma), myelo-proliferative disorders, and hereditary disorders ofplatelet function. In the cardiac surgical patient,medication related dysfunction, uremic dysfunctionare most common.There is an ever growing list of medications
that inhibit platelet function. Some medicationsaltering function and commonly observed in thecardiac surgical patient include aspirin, nonsteroidalanti-inflammatory drugs (NSAIDs), thienopyridineadenosine diphosphate (ADP) receptor antago-nists (clopidogrel, ticlopidine) and GP IIb/IIIaantagonists (abciximab, integrelin, and tirofiban),dextran, dipyridamole, heparin, plasminogen acti-vators, and beta-lactam antibiotics. NSAIDs inhibitplatelet function by blocking platelet synthesis ofprostaglandins and platelet function is normalizedwhen these drugs are cleared from the blood.Aspirin irreversibly acetylates prostaglandin syn-thase (cyclooxygenase) impairing platelet functionfor the life of the platelet (7–10 days). Like aspirin,the effects of clopidogrel are present for the lifeof the platelet. It is recommended that for elec-tive surgery, clopidogrel should be held for 5 daysallowing adequate time to reestablish a normalplatelet response to bleeding. Integrelin inhibitsfibrinogen from binding to the platelet surfaceGP IIb/IIIa receptor. Integrelin should be discon-tinued 12hours before surgery to ensure adequatereturn of platelet function.Renal dysfunction with uremia inhibits platelet
function. The cause of this effect is unknown. Inaddition to the qualitative defect there is often

Alice Nelson Dinardo: “ch01” — 2007/7/16 — 12:38 — page 19 — #19
Introduction 19
thrombocytopenia in these patients. The bleed-ing time is usually prolonged and there is asso-ciated anemia. Bleeding may be treated withplatelet transfusion or administration of DDAVP,or cryoprecipitate. DDAVP and cryoprecipitate raisethe levels of factor VIII (antihemophilic factor/von Willebrand factor). When DDAVP is used,0.3µg/kg is infused IV over 15minutes and thehalf-life of its activity is 8 hours.
Coagulopathy and congenital heartdiseaseCoagulopathies in children with congenital heartdisease are common. The etiology of these coag-ulopathies is multifactorial. Cyanosis has beenimplicated in the genesis of coagulation and fib-rinolytic defects particularly in patients wheresecondary erythrocytosis produces a hematocritgreater than 60%. Thrombocytopenia and qualita-tive platelet defects are common. Defects in bleedingtime, clot retraction, and platelet aggregation toa variety of mediators have all been described.Platelet count and platelet aggregation response toADP are inversely correlated with hematocrit andpositively correlated with arterial oxygen satura-tion. In cyanotic patients, generation of plateletmicroparticles, hypofibrinogenemia, low-grade dis-seminated intravascular coagulation (DIC), defi-ciencies in factors V and VIII, and deficiencies inthe vitamin-K-dependent factors (II, VII, IX, X) haveall been implicated in the genesis of coagulapathy.In patients who are cyanotic and erythrocytotic,the plasma volume and quantity of coagulation fac-tors are reduced, and this may contribute to thedevelopment of a coagulopathy. In some instances,erythrophoresis with whole blood removed andreplaced with fresh frozen plasma or isotonic salinemay be justified.
In addition to the defects induced by cyanosis,defects inherent to normal infants and to childrenwith congenital heart disease are present. Neonatalplatelets are hypo-reactive to thrombin (the mostpotent platelet agonist), epinephrine/ADP, colla-gen, and thromboxane A2. In addition, neonatalfibrinogen is dysfunction as compared to older chil-dren and adults. An acquired deficiency of thelarge von Willebrand multimers has been demon-strated in patients with congenital heart disease.Finally, factors synthesized in the liver may bereduced in both cyanotic and acyanotic patientsin whom severe right heart failure results in pas-sive hepatic congestion and secondary parenchymaldisease.
Suggested reading
Ashley EA, Vagelos RH. Preoperative cardiac evaluation:
mechanisms, assessment, and reduction of risk. Thorac
Surg Clin 2005;15:263–75.Katz RI, Cimino L, Vitkun SA. Preoperative medical con-
sultations: impact on perioperative management and
surgical outcome. Can J Anaesth 2005;52:697–702.Maurer WG, Borkowski RG, Parker BM. Quality
and resource utilization in managing preoperative
evaluation. Anesthesiol Clin North America 2004;22:155–75.
Practice Advisory for Preanesthesia Evaluation. A report
by the Society of Anesthesiologists Task Force
on Preanesthesia Evaluation. Anesthesiology 2002;96:485–96.
Schmiesing CA, Brodsky JB. The preoperative anesthesia
evaluation. Thorac Surg Clin 2005;15:305–15.Thakar CV, Arrigain S, Worley S, Yared JP, Paganini EP.
A clinical score to predict acute renal failure after cardiac
surgery. J Am Soc Nephrol 2005;16:162–8.Wesorick DH, Eagle KA. The preoperative cardiovascular
evaluation of the intermediate-risk patient: new data,
changing strategies. Am J Med 2005;118:1413.e1–9.

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 20 — #1
CHAPTER 2
Myocardial Physiology andthe Interpretation ofCardiac Catheterization Data
The ability to interpret cardiac catheterization datais essential to the cardiac anesthesiologist. Catheter-ization data provide information about the extentand distribution of coronary stenosis, the type andextent of valvular lesions, the location and quantifi-cation of intracardiac shunts, congenital lesions, andan assessment of systolic and diastolic function. Thisinformation contributes to a complete preoperativeevaluation and serves as a predictor of postoperativefunctional status.
Right heart catheterization
A fluid-filled catheter capable of making high-fidelity pressure measurements in the right atrium,right ventricle, pulmonary artery, and pulmonaryartery occlusion position is passed antegrade viaa basilic, cephalic, or femoral vein under fluoro-scopic guidance. In addition, the catheter may havethe capability of making thermodilution cardiacoutput and mixed venous oxygen saturation mea-surements. Angiography is performed by recordingseveral cardiac cycles on cine film while radio-graphic contrast material is injected into the rightheart chambers.
For infants and children, the femoral vein is theusual access site; however, right heart catheteri-zation via the umbilical vein may be possible inthe first few days after birth. Catheterization of theright ventricle and pulmonary arteries may be diffi-cult via the umbilical route because umbilical veincatheters tend to pass directly into the left atrium via
the foramen ovale. Right atrial, right ventricular,and pulmonary angiography may be performedon infants and children to delineate congenitallesions.
Left heart catheterization
A fluid-filled catheter capable of making high-fidelity systolic, diastolic, and mean pressure mea-surements and capable of allowing angiographic dyeinjection is used. The catheter may be passed retro-grade via the brachial or femoral artery to the aorticroot under fluoroscopic guidance where pressuresare recorded. In infants and children the femoralartery is the preferred route. The umbilical arteryis small and its course is tortuous; therefore, is notuseful except for pressure monitoring and angiogra-phy of the descending aorta. Left heart catheteriza-tion can be performed antegrade via the right atriumin patients in whom the atrial septum can be crossedvia a patent foramen ovale or an atrial septal defect.This is a common approach in infants and children.In patients in whom the retrograde approach tothe left ventricle is undesirable, and where an atrialor ventricular level communication does not exist,the atrial septum can be intentionally punctured togain access to the left atrium using a Brockenbroughneedle.
Pressures in the aorta, left ventricle, and leftatrium are recorded. Aortography may be per-formed by recording on cine film the injection ofradiographic contrast material into the aortic root.
20

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 21 — #2
Myocardial Physiology 21
(a) (b)1
2
3
4
5
Diastole Systole
LALA
mvmv
Ao
Ao
Fig. 2.1 Left ventriculogram in right anterior oblique (RAO) projection. End-diastolic image is shown in (a) whileend-systolic image is shown in (b). For purposes of comparison, end diastole is represented by dotted outline onend-systolic image. Numbers 1–5 refer to five segments analyzed for wall motion in RAO projection (see Fig. 2.12).Ao, aorta; LA, left atrium; mv, mitral valve.
This will allow detection of aortic regurgitation,congenital aortic arch abnormalities such as coarcta-tion or aortic arch interruption, and acquired aorticlesions such as aortic dissection. Left atrial and ven-tricular angiography allows detection of congenitalanomalies. Left ventriculography is performed byrecording several cardiac cycles on cine film asradiographic contrast material is injected into themid left ventricle. The left ventriculogram allowsdetection of mitral regurgitation as well as com-parison of both regional and global wall motion insystole and diastole (Fig. 2.1a,b). The left ventricu-logram also allows calculation of left ventricularend-diastolic volume (LVEDV) and left ventricu-lar end-systolic volume (LVESV). The innermostmargin of the left ventricular (LV) silhouette in sys-tole and diastole is determined. Computer assistedplanimetry calculates LV volumes from these two-dimensional pictures based on the assumption thatventricular shape is approximated by an ellip-soid. Angiographic stroke volume (SV) is thendefined as LVEDV – LVESV. Ejection fraction (EF)is defined as (LVEDV – LVESV)/LVEDV, which isSV/LVEDV.
Coronary angiography
Cine recordings of radiographic contrast materialselectively injected into the coronary ostia are made.Special catheters are used for the selective
Fig. 2.2 Left anterior oblique (LAO) projection of aortaillustrating use of Judkin’s technique to catheterize theright coronary ostia retrograde via femoral artery.
cannulization of the ostia and are advanced underfluoroscopic guidance via the same artery used forleft heart catheterization (Figs 2.2 & 2.3).
Cardiac output determination
Two complimentary methods are used to deter-mine cardiac output: the thermodilution techniqueand the Fick determination. Both methods measureforward cardiac outputs. Forward cardiac output

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 22 — #3
22 Chapter 2
Fig. 2.3 Left anterior oblique (LAO) projection ofaorta illustrating use of Judkin’s technique tocatheterize the left coronary ostia retrograde viafemoral artery.
and total cardiac output are equal only if there areno regurgitant lesions or shunt fractions.
Thermodilution cardiac output is a modificationof the indicator dilution method, in which flow isdetermined from the following relationship:
Known amount of indicator injected
Measured concentration of indicator× time
In the thermodilution method, cold water is theindicator. A predetermined volume of indicatorof known temperature is injected into the rightatrium, where the temperature of the blood alsois known. The subsequent change in temperatureover time is measured by a thermistor in the pul-monary artery. This method measures pulmonaryblood flow, which is equal to forward right heartoutput. It is not accurate at low cardiac outputs,in the presence of tricuspid regurgitation, or wherean intracardiac left-to-right shunt exists. Thermo-dilution cardiac outputs are discussed in detail inChapter 3.
The Fick determination is based on the rela-tionship:
O2 consumption/arterial− venous O2 content
difference
Oxygen uptake or consumption (Vo2) can bedetermined from calculations made on a 3-minuteexpired air sample collected in a Douglas bag. Thebag contents are analyzed for carbon dioxide and,using the respiratory quotient, VO2 is calculated.More commonly, an estimate of VO2 is obtainedfrom tables that relate VO2 to body surface area or toheart rate and age. Arterial–venous oxygen contentdifference (A–VO2 difference) is calculated from thedifference between the arterial and mixed venousoxygen contents where:
Content=(O2 saturation of arterial or mixed
venous blood×Hb concentration×(1.38))
+(0.003×PO2 of arterial or mixed venous blood)
This method measures systemic blood flow;which equals forward left heart output. It also can beused to measure pulmonary blood flow or forwardright heart output, when oxygen consumption isdivided by pulmonary arterial content subtractedfrom pulmonary venous content. The method ismore accurate at low cardiac outputs, where thearterial to venous oxygen difference is great. It alsois accurate in the presence of intracardiac shuntswhen the mixed venous oxygen content and pul-monary venous oxygen content are properly deter-mined. This will be discussed further in the sectionon intracardiac shunts.
Resistances
Systemic and pulmonary vascular resistances aremade using hemodynamic and cardiac output dataas follows:• Systemic vascular resistance (SVR)• Pulmonary vascular resistance (PVR)• Transpulmonary gradient (TPG)• Mean arterial blood pressure (MAP)• Mean pulmonary artery pressure (mPAP)• Pulmonary artery occlusion pressure (PAOP)• Central venous pressure (CVP)• Cardiac output (CO)
SVR = (MAP− CVP)80
CO
nl = 700–1600 dynes/s/cm5

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 23 — #4
Myocardial Physiology 23
SVR = (MAP− CVP)
CO
nl = 9–20 Wood units
PVR = (mPAP− PAOP)80
CO
nl = 20–130 dynes/s/cm5
PVR = (mPAP− PAOP)
CO
nl = 0.25–1.6 Wood units
TPG = mPAP− PAOP nl = 5–10 mmHg
The use of these parameters in evaluation ofpatients is discussed in detail in Chapters 4–9.
Saturation data
The oxygen saturation (%) of blood in the lowsuperior vena cava (SVC), the main pulmonaryartery, and the aorta are obtained to screen forintracardiac shunts. If an intracardiac shunt is sus-pected, multiple samples from locations in the greatvessels and cardiac chambers are necessary to local-ize the shunt and determine its magnitude anddirection.
Assessment of valve lesions
Analysis of the pressure data from right and leftheart catheterization, in combination with anal-ysis of ventriculography and aortography data,will delineate the extent and nature of valvularlesions.
Assessment of pulmonary vascularanatomy
For infants and children with congenital heartdisease, special procedures may be necessary toassess the pulmonary vasculature and the extent ofpulmonary vascular disease.
Pressure–volume loops
To fully understand catheterization data, it isnecessary to be familiar with ventricular pressure–volume loops. A normal LV pressure–volume loop
Pre
ssur
e
Volume
A
DC
B
SW = ∫ PdV
Fig. 2.4 Schematic representation of ventricularpressure–volume loop. Crosshatched area representsstroke work (SW) or total external mechanical work.Curve AB, diastolic filling; BC, isovolumiccontraction; CD, systolic ejection; DA, isovolumicrelaxation.
is illustrated in Fig. 2.4. Curve AB represents thediastolic pressure–volume relationship. Ventricularfilling begins when left atrial pressure (LAP) exceedsleft ventricular pressure at point A and the mitralvalve opens. Point B represents LVEDP and LVEDV.LVEDV is also known as Ved. Point B also repre-sents the onset of isovolumic contraction at whichLV pressure exceeds LAP and the mitral valve closes.Changes in diastolic function can be represented bychanges in the position and shape of the curve ABand will be discussed later.
Curve BC represents isovolumic contraction. LVpressure increases while LV volume remains con-stant. At point C, LV pressure exceeds aortic diastolicpressure and the aortic valve opens.
Curve CD represents the ejection phase ofventricular contraction. At point D, aortic pres-sure exceeds LV pressure and the aortic valvecloses. Point D represents the left ventricularend-systolic pressure (LVESP) and the left ventric-ular end-systolic volume (LVESV). LVESP is alsoknown as Pes.
Curve DA represents isovolumic relaxation. Atthis time there is constant LV volume and rapidlydecreasing LV pressure.

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 24 — #5
24 Chapter 2
The area encompassed by ABCD represents thestroke work (SW) that is external mechanical work.Preload is defined as the end-diastolic fiber lengthor volume and is represented by point B on thecurve AB. Augmented preload produces an increasein end-diastolic muscle fiber length represented bya point B further to the right on the curve AB.This increased fiber length enhances the velocityof muscle shortening for a given level of afterload(Frank–Starling mechanism).
A family of pressure–volume loops exists for anyventricle. Experimentally these loops are generatedby altering preload over a physiologic range usingpartial inferior vena cava (IVC) occlusion. Whenthe ventricular end systolic pressure volume points(point D) from each loop are connected a straightline is created. The slope of this line is ventric-ular elastance (Ees) and it uniquely defines thecontractile state of the ventricle (Fig. 2.5).
Afterload in this model can be defined simplyas Pes (point D) or as the stress (force per unitarea) encountered by ventricular fibers after theonset of shortening as represented by moving frompoint C to D.
Stress = pressure× radius
2hwhere h is wall thickness. Afterload, defined aswall stress, is constantly changing during ventric-ular ejection because ventricular pressure, radius,and thickness are all changing during ejection.
These definitions of afterload are incompletebecause they do not directly describe the charac-teristics of the arterial system. Because the ventricleproduces pulsatile ejection of a viscous fluid (blood)into a viscoelastic reservoir (the arterial system), it isworth considering the characteristics of the arterialsystem and of the blood, both of which consti-tute impedance to ventricular ejection. Pulsatile andnonpulsatile flow must be considered because bothexist in the intact arterial system. The nonpulsatilecomponent of afterload is measured as peripheralvascular resistance. This is a familiar concept and isdefined asMean arterial pressure− central venous pressure
cardiac output
Blood viscosity and the caliber of the arteriolesare the major determinants of peripheral vascular
LV p
ress
ure
(mm
Hg)
Ea
Ea
Ees
Pes
Ved
Ved
Pes
LV volume (mL)
Fig. 2.5 A family of four ventricular pressure–volumeloops have been generated by varying preload(ventricular end diastolic volume or Ved) in a ventriclewith fixed contractility (Ees) and fixed afterload (Ea).Joining the ventricular end-systolic pressure (Pes) andvolume points from the four loops defines the slope Ees.The ventricular end-systolic pressure and volume pointscorrespond to point D in Fig. 2.4. Ea is the slope of theline defined by joining Ved to Pes for each loop. Sinceafterload is fixed in this example the slope Ea is the samefor each loop. This can be seen in loops 2 and 4. Despitefixed afterload and fixed contractility, augmentation ofpreload results in an elevation of Pes. The intersectionpoint of Ees and Ea uniquely define Pes for each loop.Pes will remain constant with an augmentation ofpreload only if Ea simultaneously decreases (shallowerslope).
resistance. The pulsatile component of afterloadis measured as frequency-dependent aortic inputimpedance, which is determined by the elasticproperties of the proximal aorta and by the reflec-tion of pulse waves from the peripheral arterial tree.Effective arterial elastance (Ea) is defined as theratio of LVESP/SV (Pes/SV) and is the line that con-nects point B to D (see Fig. 2.5). This relationshipincorporates peripheral resistance, characteristicimpedance, and lumped total arterial compliance.Thus Ea can be used to define the hydraulic load(afterload) of the LV.
In the pressure–volume loop scheme, LVESVand Pes (point D) are uniquely determined by theintersection point of the contractile state (Ees) and

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 25 — #6
Myocardial Physiology 25
the afterload (Ea). Normally, the ratio of Ea/Ees
is 0.7–1.0. In this range, SW (external mechani-cal work) and efficiency (ratio of SW/myocardialoxygen consumption) are optimized. In heart fail-ure patients the ratio may be as high as 4.0 dueto simultaneous decreases in Ees and increasesin Ea.
For a given Ees with Ea constant an increase inpreload (LVEDV or Ved) will produce an increase inSV and an increase in LVESP (Pes) (see Fig. 2.5).This increase in the area ABCD is known as preloadrecruitable stroke work (PRSW). In reality the onlyway in which LVESP (Pes) could remain con-stant for a given Ees with an increase in preloadwould be for the slope of Ea to decrease. Statedanother way, an increase in preload for a givenEes will cause a parallel (no change in slope) shiftin Ea to the right resulting in an increase in Pes
and LVESV. With enhanced contractility (steep Ees
slope) the rise in Pes will be great and the reduc-tion in LVESP will be small; PRSW will be high.With diminished contractility (shallow Ees slope)the rise in Pes will be small and the reduction inLVESP will be great; PRSW will be limited. This isconsistent with the clinical observation that in thepresence of reduced contractility preload augmen-tation does not substantially improve SV and cardiacoutput.
For a given contractile state with fixed preload,an increase in afterload (steeper Ea slope) resultsin an increase in Pes and LVESV; representedby moving upward and to the right on the lineA decrease in afterload (shallower Ea slope) resultsin a decrease in Pes and LVESV; represented bymoving downward and to the left on the line(Fig. 2.6). Increased contractility is represented byan Ees that is steeper and shifted upward to the left.An increase in contractility with preload and after-load fixed obviously augments SV because of themarked decrease in LVESV with LVEDV (preload)constant (Fig. 2.7). Decreased contractility is rep-resented by an Ees that is shallower and shifteddownward to the right. With fixed preload (Ved)and afterload (Ea), SV is diminished when contrac-tility decreases (see Fig. 2.7). It is also obvious thatthe shallower the Ees slope (more depressed con-tractility) the more sensitive the ventricle will be to
LV p
ress
ure
(mm
Hg)
LV volume (mL)
Ved
Pes
Ea
Ea′
Ees
Ves′
Pes′
Fig. 2.6 Two ventricular pressure–volume loopsillustrating the effect of increased afterload (Ea′ ) withpreload (Ved) and contractility (Ees) fixed. Increasedafterload is represented by the line Ea′ which has asteeper slope than line Ea. Increased afterload (Ea′ )results in an increase in Pes (from Pes to Pes′ ) andan increase in end-systolic volume (from Ves to Ves′ ),which causes a reduction in SV (from Ved–Ves toVed–Ves′ ). EF = Ees/(Ees + Ea) and therefore EF falls asEa increases to Ea′ with Ees constant.
an increase in Ea as evidenced by a greater increasein LVESV.
Figure 2.8 serves to unify these concepts. Loop 1represents the control situation. Loop 2 representsan abrupt increase in afterload with contractilityconstant. The result is an increased LVESV and anunchanged LVEDV. The result is a reduction in SV.In subsequent beats (loop 3) of a normal heart,LVEDV is increased such that the original SV isnow maintained at the new increased afterload.The ability of the ventricle to maintain SV in theface of increasing afterload by increasing preloadis defined as preload reserve. Preload reserve isexhausted when the sarcomeres are stretched totheir maximum diastolic length. When this occurs,there will be no further augmentation of the veloc-ity of shortening and the ventricle behaves as ifpreload is fixed. For a given level of contractil-ity, after preload reserve is exhausted, additionalincreases in afterload will be accompanied by par-allel decreases in SV (loop 4). This is defined as astate of afterload mismatch. Afterload mismatch is

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 26 — #7
26 Chapter 2LV
pre
ssur
e (m
mH
g)
LV volume (mL)
Ved
Ved′
Pes′Ves′
PesVes
Ees′
Ees
Ea
Ea
Fig. 2.7 Two ventricular pressure–volume loopsillustrating effect of decreased contractility (Ees′ ) with Pes
and afterload (Ea) constant. Decreased contractility isrepresented by the line (Ees′ ) that has a shallower slopethan line Ees and is shifted downward to the left. Sinceafterload is fixed in this example, the slope Ea is the samefor both loops. Decreased contractility (Ees′ ) results in anincrease in end-systolic volume (from Ves to Ves′ ) whilePes = Pes′ . Since Pes and Ea are constant in this example,stroke volume (SV) must be constant as well asSV = Pes/Ea. As a result Ved′ increases by an amountequal to the increase in Ves′ . With Pes fixed SV willonly decrease with a decrease in contractility ifafterload (Ea) simultaneously increases (steeper slope).Progressive increases in Ea will result in a greaterincrease in Ves for Ees′ as compared to Ees. AlthoughSV is constant in this example EF decreases becauseEF = Ees/(Ees + Ea).
the inability of the ventricle at a given level of con-tractility to maintain SV in the face of an increasedwall stress.
Diastolic function
Normal diastolic function is dependent on normalventricular diastolic compliance, distensibility, andrelaxation. Both extrinsic and intrinsic factorsaffect ventricular diastolic function. It is necessaryto differentiate between compliance, distensibil-ity, and relaxation, and this is best accomplishedby examining diastolic pressure–volume diagrams
2404
SV
3
2
1
SV
Limit ofreserve
50 100
LV volume (mL)
150
180
120
LV p
ress
ure
(mm
Hg)
60
30
Fig. 2.8 Ventricular pressure–volume loops illustratingthe compensation of an intact ventricle for progressiveincreases in afterload with contractility fixed. Strokevolume (SV) can be maintained in the face of progressiveafterload increases until preload reserve is exhausted.
(Fig. 2.9a–d). Any or all of these abnormalities mayexist in a given patient.
ComplianceCompliance or distensibility is defined as theratio of a volume change to the correspond-ing pressure change or as the slope of thevolume–pressure (V /P) relationship. Elastanceor stiffness is the inverse of compliance (P/V ).Decreased compliance or increased stiffness isthus defined as an increase in the steepnessof the pressure–volume plot (see Fig. 2.9c).Strictly speaking, diastolic compliance is determinedby the intrinsic volume–pressure relationship ofcompletely relaxed myocytes. There are two causesof poor diastolic compliance.
Increased chamber stiffnessThis occurs in aortic stenosis or systemic hyper-tension. In these cases, there is an increase inthe amount of myocardial tissue due to concentric

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 27 — #8
Myocardial Physiology 27
Abnormalrelaxation
Increasedchamber stiffness
LV volume
Chamberdilatation
Pericardialrestraint
LV p
ress
ure
(a) (b)
(c) (d)
Fig. 2.9 A series of diastolic pressure–volume curves.The solid curve in each example represents a normaldiastolic pressure–volume relationship, whereas thedotted curve represents the altered diastolicpressure–volume relationship. (a) The diastolicpressure–volume relationship when ventricularrelaxation is impaired. (b) The diastolic pressure–volumerelationship when distensibility is reduced as withpericardial restraint. (c) The diastolic pressure–volumerelationship when ventricular chamber stiffness isincreased or ventricular chamber compliance is reduced.(d) The effect of chamber dilatation on a normal diastolicpressure–volume relationship.
LV hypertrophy. Diastolic compliance of the ven-tricle is diminished despite that fact that thecompliance of the individual muscle units isnormal.
Increased muscle stiffnessThis occurs in restrictive cardiomyopathies due toamyoidosis and hemochromatosis. In these cases,the compliance of the individual muscle units isdiminished due to an infiltrative process.
The diastolic pressure–volume relationship isdynamic. There is high compliance at low volumesand diminished compliance at higher volumes. Asa result, reduced diastolic compliance is not limitedto ventricles with altered pressure–volume slopes.A ventricle forced to make use of preload reserve to
maintain SV may function on the steep portion of anotherwise normal compliance curve (see Fig. 2.9d).
DistensibilityDecreased ventricular distensibility is defined asan increased diastolic pressure at a given volume.This would be represented in a diastolic pressure–volume diagram by a parallel upward shift of theentire pressure–volume relation (see Fig. 2.9b).Decreased distensibility can occur from intrinsic andextrinsic causes.
Intrinsic causesIt has been demonstrated clearly that pacing-induced ischemia in humans with coronary arterydisease (CAD) is responsible for diminished dia-stolic distensibility. Although impaired relaxationcertainly plays a role in diastolic dysfunction withischemia, the pressure–volume relation in ischemiamore closely resembles the pattern seen withpericardial restraint (see Fig. 2.9b). This dimin-ished diastolic distensibility often precedes systolicdysfunction. In addition, pacing-induced ischemiaelicits diminished diastolic distensibility in humanswith aortic stenosis without CAD. Differencesin the diastolic behavior of ischemic and non-ischemic segments of the same ventricle subjectedto pacing-induced ischemia have been demon-strated. An upward shift (diminished distensibility)in the pressure–length relationship is observed inischemic segments. For a given diastolic volume thisresults in an increase in diastolic pressure, whichcauses the nonischemic segments to move to asteeper (less compliant) portion of their originalpressure–length relationship.
Extrinsic causesDecreased distensibility may be caused by extrin-sic limitations to ventricular expansion in diastole.Diminished distensibility occurs due to ventricularinterdependence via an intact ventricular septumand the restraining effect of the pericardium(see Fig. 2.9b). For example, distension of theright ventricle with a leftward septal shift willresult in diminished distensibility of the leftventricle. In addition, reduced distensibility mayoccur due to restrictive pericarditis or pericardial

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 28 — #9
28 Chapter 2
tamponade a diseased or fluid-filled pericardium(see Chapter 7).
RelaxationVentricular relaxation is an energy consumptiveprocess. Adenosine triphosphate (ATP) is requiredfor calcium sequestration back into the sarcoplas-mic reticulum and for detachment of actin–myosincross-bridges. When isovolumic relaxation is delayed,early diastolic filling is impeded. When relax-ation is incomplete, filling is impeded through-out diastole (see Fig. 2.9a). Relaxation is impairedduring myocardial ischemia and in patients withhypertrophic and congestive cardiomyopathies.
Normally, the right ventricular end-diastolic pres-sure (RVEDP) is 1–2 mmHg greater than the meanright atrial pressure (RAP), and the left ventric-ular end-diastolic pressure (LVEDP) is 2–3 mmHggreater than the mean PAOP and the LAP. Thesesmall differences in pressure are due to the volumeadded to the ventricle by atrial systole. When LVcompliance is poor, the A wave produced by atrialsystole will be large and the additional volume pro-vided by the atrial kick in end-diastole will resultin a large increase in LVEDP. In these patients, thepeak A-wave pressure in the LAP or PAOP traceis a better measure of LVEDP than the mean LAPor PAOP because the mean LAP or PAOP pressurewill underestimate LVEDP. Even large A waves onlyslightly elevate mean LAP because their duration isshort. Thus, well-timed atrial contraction results ina large elevation of LVEDV with only a small ele-vation of mean LAP and limited pulmonary venouscongestion. For patients who chronically functionon a steep portion of the compliance curve, a largeA wave, left atrial enlargement on electrocardio-gram (ECG) and an S4 on physical examination areexpected findings.
Analysis of diastolicpressure–volume curves
Ideally, the diastolic pressure–volume curve shouldbe examined over its entire range and underbaseline and stress conditions. Unfortunately, thisinformation is not routinely available from cardiaccatheterization data. Typically, the A wave, V wave,
and mean pressures of the RAP and PAOP tracing,the RVEDP and LVEDP, and the left ventricular end-systolic and end-diastolic volume indices (LVESVIand LVEDVI) are provided. The LVESVI and theLVEDVI are simply the LVESV and LVEDV obtainedby planimetry of left ventricular end-systolic andend-diastolic angiograms divided by the patient’sbody surface area (BSA). Pressure and volume datafrom a representative catheterization report arereproduced in Figs 2.10 and 2.11.
One point on the LV diastolic pressure–volumecurve is obtained if the pressure and volume mea-surements are made under identical conditions ofpreload, heart rate, and ischemia. Thus, incompleteinformation must be used to draw inferences onoverall diastolic performance. Clinically, a dilatedheart would be expected in patients who are depen-dent on a large LVEDV to maintain an adequateforward SV. Patients with chronic volume over-load valvular lesions such as mitral regurgitationand aortic insufficiency are good examples. In thesepatients, a large LVEDV is needed because only aportion of the total SV becomes forward SV. Earlyin the disease, these patients operate on the flatportion of a diastolic pressure volume curve andhave enormous preload reserve. As the disease pro-gresses and systolic function deteriorates, a largerLVEDV is needed to maintain SV. Eventually, thesepatients operate on the steep portion of the diastolicpressure–volume relationship and are unable toaugment preload without large increases in diastolicpressure and subsequent pulmonary congestion. Inpatients with mitral regurgitation, this analysis ofdiastolic function is complicated by the presenceof regurgitant V waves in the LAP or PAOP traceduring ventricular systole. The electronically deter-mined mean LAP or PAOP will be increased in directproportion to the height and duration of the regurgi-tant V wave. This will cause the mean LAP or PAOPto overestimate LVEDP. An estimate of the LVEDPcan be obtained by examining a calibrated PAOP orLAP trace and determining the A-wave amplitude.In patients without atrial systole, the best estimateof LVEDP will be the PAOP or LAP at end diastole(see Chapter 3).
A normal LVEDV and diminished ventricularcompliance is seen most commonly in patients with

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 29 — #10
Myocardial Physiology 29
Fig. 2.10 Reproduction of portion ofcardiac catheterization report from61-year-old woman with severethree-vessel coronary artery disease(CAD) and systolic dysfunction. Rightand left ventricular pressuremeasurements, Fick cardiac output(CO) determination, and derivedhemodynamic variables are reported.
Fig. 2.11 Reproduction of portion ofcatheterization report from the patientdescribed in Fig. 2.10. Section reportsinformation obtained from leftventriculography. Left ventricularend-diastolic volume index (LVEDVI),left ventricular end-systolic volumeindex (LVESVI), stroke volume index(SVI) and ejection fraction (EF) arereported. In addition, qualitativedescriptions of left ventricular wallmotion in five wall segments seen inright anterior oblique (RAO) projectionare reported.

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 30 — #11
30 Chapter 2
LV pressure overload valve lesions such as aorticstenosis and, to a lesser degree, in patients with sys-temic hypertension. In these patients, the LVEDVnecessary to maintain an adequate SV is maintainedat the expense of a high LVEDP because complianceis poor. The volume contributed by atrial systolerepresents a larger proportion of the LVEDV than itdoes in ventricles with normal compliance becausethe early diastolic filling is compromised by lowcompliance and is compensated for by a well-timedforceful atrial systole. Loss of atrial systole in thesepatients is disastrous because LVEDV can only bemaintained by large elevations of mean LAP withconsequent pulmonary venous congestion.
A ventricle with abnormal LVEDV and dimin-ished distensibility is characteristic of patients withsevere CAD in which the energy requirements nec-essary to guarantee complete ventricular relaxationat rest are not met. Such diastolic dysfunctionprecedes the development of systolic dysfunction.
Systolic function
Systolic function is not synonymous with contrac-tility. Normal systolic function is the ability of theventricle to perform external work (generate a SV)under varying conditions of preload, afterload andcontractility. Any assessment of systolic functionmust take the contribution of these three factorsinto account.
Ejection fractionDefined as (LVEDV – LVESV)/LVEDV×100, theEF is an ejection-phase index and the most com-monly used assessment of global systolic function.The LVEDV and the LVESV are obtained fromplanimetry of LV end-diastolic and end-systolicangiograms (see Fig. 2.1). The normal value is50–80%. Determination of EF is dependent on vari-ations in preload, afterload, and contractility (seeFigs 2.5–2.7). This becomes obvious when EF isdescribed mathematically using the concepts of Ees,Ea, stroke volume (SV), and LVEDV (Ved):
EF = SV/Ved
EF = 1− Pes/Ved
Ees= 1− (Ea ∗ SV)/Ved
Ees
EF = Ees/(Ees + Ea)
Normal Ees and Ea are 1–3 mmHg/mL
These equations are consistent with a number ofclinical observations:• In the range of normal contractility (Ees), EF islargely insensitive to changes in afterload (Ea) andpreload (Ved).• EF is increasingly inversely related to afterload(Ea) as contractility (Ees) decreases with fixedpreload (Ved). In addition this inverse sensitivity isenhanced in the setting of reduced preload (Ved).• EF is increasingly inversely related to preload(Ved) as contractility (Ees) decreases with fixedafterload (Ea).• When preload (Ved) is very low, EF will bereduced in presence of normal contractility (Ees)and afterload (Ea).• If the Ea/Ees ratio is 1.0 (ideally matched) thenEF = 50%.• EF is most useful as screening tool with low EFidentifying those patients most likely to be sus-ceptible to alteration in preload, afterload, andcontractility.
As an example, an increase in LVEDVI from75 to 90 mL/m2 with LVESVI constant at 25 mL/m2,as would occur with afterload and contractilityconstant, would result in an increase in EF from66% to 72%. Thus, a 20% increase in preloadresults in a 9% increase in EF.
EF is not a very sensitive index of CAD becauseareas of regional myocardial dysfunction secondaryto ischemia may exist without depression of globalsystolic function. EF separates patients with normalLV function from those with LV dysfunction andis reliable in following changes in systolic functionin individual patients. An EF lower than 40% inthe absence of acute afterload elevations representsdepressed systolic function and corresponds clin-ically with New York Heart Association class 3symptoms. An EF lower than 25% represents severedepression of LV systolic function and correspondsto New York Heart Association class 4 symptoms(see Chapter 1).
EF may overestimate systolic function in mitralregurgitation because of the unique systolic loadingconditions in this lesion. The left ventricle is

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 31 — #12
Myocardial Physiology 31
presented with two outflow tracts in systole: theaortic valve and the incompetent mitral valve. Themitral valve provides a low impedance outflow tractand the aortic valve provides a normal-impedanceoutflow tract. EF may remain near normal in theface of depressed systolic function due to this lowmean afterload state. With mitral valve replace-ment and the elimination of the low-impedanceoutflow tract, the ventricle is presented with morenormal systolic loading conditions. EF may actu-ally decrease substantially postoperatively in suchpatients because depressed systolic function is nowunmasked.
Stroke workAnother ejection-phase index of systolic functionis stroke work (SW), or external LV work, repre-sented by the area ABCD in Fig. 2.4. When theshape of the LV pressure–volume loop is normal,as is true in the absence of pressure or volumeoverload conditions, left ventricular stroke work(LVSW) is a good measure of systolic function.Chronic volume and pressure overload conditionsalter the shape of the pressure–volume loop andthe calculated LVSW is increased above the normalvalue of 60–120 g-m/beat. LVSW is defined as:
(Mean LV systolic pressure
−mean LV diastolic pressure)× SV × 0.0136
When aortic and mitral regurgitation are absent, thiscan be simplified to:
(Mean arterial pressure−mean pulmonary artery
occlusion pressure)× SV × 0.0136
because mean arterial pressure approximates meanLV systolic pressure and mean pulmonary arteryocclusion pressure closely approximates mean LVdiastolic pressure. In direct contrast to EF, alter-ations in afterload have little effect on calculatedSW. SV declines or increases in proportion to theafterload elevation or reduction such that the area ofthe loop remains unchanged. SW, unlike EF, is verysensitive to changes in preload. The area of the loopis increased or decreased by increases or decreasesin preload. LVSW can be converted to LVSWI bydividing SV by BSA to get SVI.
LWSW is used in conjunction with Ved to describePRSW where PRSW=LWSW/Ved. PRSW is a mea-sure on myocardial contractility that is independentof preload and afterload. This method requires theability to simultaneously record LV pressures andvolumes and is not in routine clinical use.
Left ventriculographyQualitative analysis of regional wall motion byleft ventriculography is another index of systolicfunction. Ventriculography is performed by mak-ing cine recordings as contrast material is injecteddirectly into the mid-left ventricle. Left ventricu-lography is performed in the 30 right anterioroblique (RAO) projection or in the right and 60 leftanterior oblique (LAO) projections. The ventricle isdivided into segments (Fig. 2.12) and visual analy-sis of regional wall motion is made by comparisonof end-diastolic and end-systolic cineangiograms(see Fig. 2.1). Five segments are generally analyzedin the RAO projection: anterobasal, anterolateral,apical, diaphragmatic (inferior), and posterobasal.Five segments also may be analyzed in the LAOprojection: basal septal, apical septal, apical infe-rior, posterolateral, and superior lateral. These areasare graded qualitatively for wall motion. Normalareas exhibit concentric inward movement in sys-tole. Hypokinetic areas exhibit reduced concentricinward motion in systole. Akinetic areas exhibit nomotion with systole. Dyskinetic areas exhibit a para-doxical outward bulging with systole. Aneurysmalareas exhibit characteristic dilation with eitherhypokinesis or akinesis.
Areas of hypokinesis generally are composed ofischemic myocardium, whereas akinetic areas arecomposed of infracted or hibernating myocardium.Improvements in wall motion occur in hypokineticand akinetic areas when ischemic tissue has beensalvaged by revascularization or by pharmacologicinterventions to improve perfusion. The presenceof collaterals, the absence of surface ECG Q waves,and the presence of an associated proximal coro-nary stenosis less than 90% improve the likelihoodthat medical or surgical intervention will improvethe wall motion abnormalities. Dyskinetic andaneurysmal areas, respectively, represent regionswith little or no viable myocardium and rarely

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 32 — #13
32 Chapter 2
Anterobasal
LA
12
3
45
LVRAO
LVLAO
Anterolateral 610
9
78
Apical inferior
Posterolateral
Superior lateralLA
Apical
Posterobasal Diaphragmatic Apical septal
Basal septal
Fig. 2.12 Schematic delineation of the five wallsegments seen in right anterior oblique (RAO) and leftanterior oblique (LAO) projections duringleft ventriculography. The following is a summary ofcoronary arterial supply to these regions:1. Anterobasal – LMCA; proximal LAD; 1st diagonal.2. Anterolateral – LMCA; proximal or mid-LAD;1st diagonal. 3. Apical – LMCA; proximal, mid, or distalLAD; 2nd diagonal. 4. Diaphramatic (inferior) – proximal,mid, or distal RCA; PDA. 5. Posterobasal – proximal, mid,
or distal RCA; PDA. 6. Basal septal – LMCA; proximal ormid-LAD, 1st septal. 7. Apical septal – LMCA; proximal,mid, or distal LAD. 8. Apical inferior – proximal, mid, ordistal RCA. 9. Posterolateral – LMCA; proximal or distalCIRC marginals. 10. Superior lateral – LMCA; proximalCIRC marginals. CIRC, circumflex artery; LAD, leftanterior descending artery; LMCA, left main coronaryartery; PDA, posterior descending artery; RCA, rightcoronary artery.
show improvement in wall motion with surgical orpharmacologic intervention.
Regional wall motion abnormalities are a moresensitive indicator of CAD than is a reduction in aglobal ejection-phase index of systolic function suchas EF. This is because global systolic function can bemaintained in the presence of regional dyssynergyby compensatory increases in wall shortening inareas of normal wall motion as long as large areasof myocardium are not dyssynergic.
Coronary angiography
Coronary angiography delineates the normal andpathologic features of the coronary circulation.Normally, angiography is performed in the 60 LAOprojection and the 30 RAO projection with caudalor cranial angulated views if necessary.
Coronary anatomyDetermination of the areas of myocardium at riskwith a particular stenotic or vasospastic lesion
requires knowledge of the regional blood supplypattern. The right and left coronary anatomy is illus-trated in Figs 2.13 and 2.14. Most patients (85%)have a right dominant system of coronary circu-lation. Here, the right coronary artery extends tothe crux cordis in the atrioventricular groove andgives rise to the posterior descending branch, leftatrial branch, atrioventricular (AV) nodal branch,and one or more posterior LV branches. In a leftdominant system (8%), these branches are suppliedby the left circumflex artery and the right coronaryartery supplies only the right atria and ventricle. In7% of patients, the system is balanced, with the rightcoronary artery supplying the posterior descend-ing, left atria, and AV nodal branches, whereasthe left circumflex artery supplies the posterior LVbranches.
There is variation in the blood supply to variousregions of myocardium, but some generalizationscan be made. This information is summarized inFig. 2.12. Normally, a proximal branch of the leftcircumflex artery supplies the anterobasal region.

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 33 — #14
Myocardial Physiology 33
SA nodal
ProximalRCA
RV branch
Mid-RCA
Acutemarginal
Distal RCAPosterior descending
LV branch
AV nodal
Conus
RCA distal to posterior descending
Fig. 2.13 Anatomy of right coronary artery.AV, arterioventricular; LV, left ventricle; RCA, rightcoronary artery; RV, right ventricle; SA, sinoatrial.
Distal LAD
2nd diagonal
1st diagonalProximal LAD
Left mainProximal circumflex
Atrial branch1st septal perforator
Obtuse marginalDistal circumflex
Posterior lateral
Mid-LAD
Fig. 2.14 Anatomy of left coronary artery (rightoblique). LAD, left anterior descending.
The anterolateral region is supplied by contributionsfrom both the diagonal branch of the left anteriordescending (LAD) artery and the obtuse marginalbranch of the left circumflex. The terminal por-tion of the LAD artery supplies the apical region.The inferior region is a combination of the poste-rior lateral and diaphragmatic regions, which arebest seen in an LAO projection. The posterior lat-eral branch of the left circumflex artery supplies theposterior lateral region. The diaphragmatic region issupplied by the posterior descending artery, which,as previously discussed, is either a branch of theright coronary or left circumflex artery. The poster-obasal region is supplied by the proximal right coro-nary artery. The septal branches of the LAD arterysupply the anterior two-thirds of the ventricularseptum, and branches of the right coronary and
posterior descending arteries supply the posteriorone-third. A branch of the right coronary artery sup-plies the sinoatrial (SA) node in 55% of patientsand by a branch of the left circumflex artery in theother 45%.
The bulk of the right ventricle is located in thediaphragmatic and posterobasal regions suppliedby the right coronary artery in a right dominantsystem. Small portions of the right ventricle alsoare included in the apical and septal areas. It is forthis reason that involvement of the LAD results incompromise of perfusion to the anterior right ven-tricular wall near the ventricular septum and to theright ventricular apex. Conversely, involvement ofthe right coronary artery in a right dominant systemresults in compromise of perfusion to the portionsof the left ventricle located in the diaphragmatic andposterobasal regions. How severely the posteriorportion of the left ventricle will be compromised inthis setting will depend on how much of this regionis supplied by the distal branches of the circumflexartery.
Anatomic coronary lesionsCoronary atherosclerotic stenotic lesions are quan-titated visually from moving cineangiograms inseveral projections. Coronary arteriography froma representative catheterization report is repro-duced in Fig. 2.15. Stenotic areas of artery arecompared with adjacent normal areas and the per-cent reduction in lumen diameter caused by thestenosis is quantified. Thus, a 90% lesion refers toa stenosis that causes a 90% reduction in lumendiameter. It is generally acknowledged that rest-ing coronary blood flow does not decrease untilthere is an 85% reduction in lumen diameter. Thiscorresponds to a greater than 90% reduction inlumen cross-sectional area. By contrast, a 50%diameter reduction corresponds to a 75% reductionin cross-sectional area. Maximal coronary flow inresponse to a stimulus for vasodilation is bluntedwhen there is a 30–45% reduction in lumen diam-eter and is absent when the lumen diameter isreduced 90%. Inter-observer variability exists in thegrading of stenotic lesions. In addition, coronaryangiography typically underestimates the severityof stenotic lesions and may not accurately predictthe physiologic significance of a particular lesion.

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 34 — #15
34 Chapter 2
Fig. 2.15 Reproduction of a portion of a catheterizationreport from patient described in Fig. 2.10. This sectionreports information obtained from coronaryangiography. Morphology of stenoses, percent reductionin lumen diameter, and sources of collaterization arereported. A pictorial representation of coronary arterialanatomy also is given.
Coronary spasmTrue coronary spasm is diagnosed at the time ofcoronary angiography with a provocation test utiliz-ing methylergonovine, acetylcholine, or hyperven-tilation. The test is considered positive if focal spasmoccurs in the presence of clinical symptoms or ECGchanges.
Coronary thrombus formationA thrombus superimposed on an obstructive coro-nary lesion is often the pathogenesis of unsta-ble angina and is the direct cause of an acutetransmural myocardial infarction in most patients.Currently, protocols designed to intervene in theearly stages of myocardial infarction incorporate
thrombolytic therapy, percutaneous transluminalcoronary angioplasty, or both.
Coronary collateralsAn extensive network of coronary collaterals is nor-mally present at birth. However, these collaterals arenot demonstrable by angiography in normal heartsdue to their small diameter. It is only when thecollateral channels enlarge secondary to regionalmyocardial oxygen deprivation that they are visi-ble angiographically. The development of collateralpathways in patients with comparable degrees ofcoronary insufficiency is variable in both extentand time course. The presence of collaterals hasbeen identified as a determinant of reversible wallmotion abnormalities. LV function in the regionof an occluded coronary artery is better main-tained in the presence of collaterals than in theirabsence.
Interpretation of coronaryangiography dataTo properly interpret the coronary angiograms itis necessary to integrate data from the angiogramswith data from the right and left heart catheteri-zations and from the left ventriculograms. Severalquestions should be answered:• What is the status of systolic function? Globalfunction in the absence of mitral regurgitationis best evaluated with EF. Regional function isassessed by analysis of the ventriculogram. Patientswith an EF greater than 55% would be expected tohave limited areas of dyssynergy and no history ofa prior myocardial infarct. Patients with a historyof prior myocardial infarction or three-vessel coro-nary disease would be expected to have a reducedEF and more extensive areas of dyssynergy. EFsin the range of 40% are common in this subsetof patients. Patients with three-vessel disease anda history of myocardial infarction have EFs in therange of 35%. More extensive areas of dyssynergywould be expected. Patients with an EF lower than25% have poor ventricular function and will havelarge areas of akinesis and dyskinesis.• What is the status of diastolic function? It is nec-essary to determine whether myocardial ischemia isresponsible for diminished ventricular distensibility

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 35 — #16
Myocardial Physiology 35
as discussed in the section on diastolic function.An elevated LVEDP is characteristic of diastolicdysfunction; although this also may exist in con-cert with systolic dysfunction, an elevated LVEDP isnot synonymous with systolic dysfunction.• What regions of myocardium are jeopardized?Significant stenotic lesions jeopardize the myocar-dium in specific regions as discussed previously.A region is at high risk of developing ischemicdysfunction if it is poorly collaterized and distalto a severe stenosis. It also is necessary to deter-mine whether the regional myocardium distal toa stenosis is viable. If the area of myocardium isdyskinetic or aneurysmal with evidence of sur-face Q waves, pharmacologic and surgical effortsto salvage the area will likely be of no benefit.If the myocardium is viable, however, (hibernat-ing myocardium), then revascularization may leadto a dramatic improvement in regional systolicfunction.• What are the consequences of deteriorating func-tion in a given region? Deteriorating functionin a given region may cause major managementproblems. Continued compromise of flow to theAV node may cause progressive heart block withsubsequent hemodynamic compromise. A patientwith depressed global systolic function whose hypo-kinetic anterior lateral wall becomes akinetic maydevelop cardiogenic shock.
Evaluation of valvular lesions
The impressive technological advances in Dopplerechocardiography and nuclear cardiac imagingnow allow noninvasive assessment of valvularpathology. Evaluation via cardiac catheterization,however, provides important information.
Stenotic lesionsThe analysis of stenotic valve lesions is based onobtaining a valve orifice area from flow andpressure–gradient data. The Gorlin equation usesthe basic hydraulic formula: area = flow/velocity.Combining this with an equation that relatesvelocity to mean pressure gradient: velocity =k × √mean pressure gradient, where k is a spe-cific constant for either the aortic or mitral valve
allows a determination of valve area. For themitral valve, then, the equation is: valve area =flow/37.7×√mean pressure gradient. For the aorticvalve, the equation is: valve area = flow/44.5 ×√
mean pressure gradient. Obviously, flow occursacross the mitral valve only in diastole and acrossthe aortic valve only in systole. Therefore, car-diac output cannot be substituted for flow in theequations. The time per heartbeat during whichblood flows across the mitral valve is defined as thediastolic filling period. The diastolic filling period ismeasured from mitral valve opening to end dias-tole. The time per heartbeat during which bloodflows across the aortic valve is defined as the sys-tolic ejection period. The systolic ejection period ismeasured from aortic valve opening to aortic valveclosure.
Mitral valve flow (cm3/sec)
= Cardiac output (cm3/min)× diastolic filling period (sec/beat)
× heart rate (beat/min)−1
Mitral valve area (cm2)
= mitral valve flow (cm3/sec)× 37.7×√mean pressure gradient (cm/sec)−1
Aortic valve flow (cm3/sec)
= cardiac output (cm3/min)× systolic ejection period (sec/beat)
× heart rate (beat/min)−1
Aortic valve area (cm2)
= aortic valve flow (cm3/sec)× 44.5×√mean pressure gradient (cm/sec)−1
The mean pressure gradient for mitral stenosis isobtained by using planimetry to determine the areabetween simultaneous tracings of the left atrial orPAOP and the LV pressure during the diastolic fillingperiod and then dividing this area by the length ofthe diastolic filling period. Figure 2.16 illustrates thisarea during one diastolic filling period. Normally,the pressure gradients for several beats are deter-mined and the average is taken. For aortic stenosis,analogous measurements are made using planime-try to determine the area between simultaneous

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 36 — #17
36 Chapter 2
40
30
20
LV
Seconds
LA
ECG
mm
Hg
10
0
Fig. 2.16 One diastolic filling period in a patient withsevere mitral stenosis. Simultaneous tracings ofelectrocardiogram (EGG), left atrial (LA) pressure, andleft ventricular (LV) pressure are shown. The pressuregradient across the mitral valve is crosshatched and seento vary during diastolic filling period. The length of thediastolic filling period can be seen in seconds.
tracings of the proximal aortic pressure and theLV pressure during the systolic ejection period.Figure 2.17 illustrates this area during one ejec-tion period. The gradients for several beats aredetermined and averaged.
It is essential that proper assessment of flowbe used for lesions in which stenosis and regur-gitation coexist. A thermodilution or Fick cardiacoutput determination is an assessment of forwardflow across a valve orifice. If regurgitation exists,total flow across the valve orifice will be for-ward flow plus regurgitant flow. If forward flowinstead of total flow is used, the valve area fora given gradient will be underestimated and thedegree of stenosis will be exaggerated. Total flowis best obtained from angiographic determinationof cardiac output. Left ventriculography is used todetermine SV (as described previously) and SV ismultiplied by heart rate.
150
100
50
mm
Hg
0
LV
Ao
Fig. 2.17 One systolic ejection period in a patient withsevere aortic stenosis. Simultaneous recordings ofproximal aortic pressure and LV pressure are recorded.The pressure gradient across the aortic valve iscrosshatched and seen to vary during systolic ejectionperiod. Time scale for length of systolic ejection periodnot shown. Ao, aorta; LV, left ventricular.
It is important when evaluating stenotic lesionsthat the pressure gradient alone is not evaluated.At low flows (low cardiac output), it is possi-ble for a valve to be critically stenotic with asmall transvalvular pressure gradient. Several otherrelationships should be kept in mind. The meanpressure gradient is directly related to the squareof flow. Thus, if cardiac output doubles, the meanpressure gradient will increase by a factor of four.The mean pressure gradient is inversely related tothe square of the valve area. Thus, if valve area isreduced by one-half, the mean pressure gradientwill increase by a factor of four.
The normal mitral valve area in an adult is4–6 cm2. The mitral valve area must be reducedto 2.6 cm2 before symptoms occur. A valve areaof 1.5–2.5 cm2 is considered mild mitral stenosis,with symptoms occurring during exercise. A valvearea of 1.1–1.5 cm2 is considered moderate mitral

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 37 — #18
Myocardial Physiology 37
stenosis. In these patients an elevated LAP neces-sary to maintain cardiac output. A valve area of1.0 cm2 is considered severe mitral stenosis. A LAPof 25 mmHg is necessary to maintain even minimalcardiac output.
The normal aortic valve area is 2.6–3.5 cm2. Theaortic valve area must usually be reduced to 0.8 cm2
before angina, syncope, and congestive heart fail-ure occur. A valve area of 0.5–0.8 cm2 is consid-ered moderate aortic stenosis. Severe aortic stenosisexists when the valve area is less than 0.5 cm2.
For adults, valve areas usually are not normalizedfor body surface area (BSA). As a result, extremesof body size must be taken into consideration whendeciding whether a stenotic lesion is significant.A large person with higher cardiac output demandsmay have a large gradient and symptoms with avalve area that would be adequate for a smallerperson with reduced cardiac output requirements.Valve areas commonly are normalized for BSA ininfants and children.
Regurgitant lesionsQuantification of regurgitant lesions with catheter-ization techniques is more difficult and less accu-rate than for stenotic lesions. Two approaches areavailable. One method is qualitative; the other isquantitative. Qualitative analysis is based on assess-ing the amount of contrast material regurgitatedinto the left atrium during left ventriculographyfor mitral regurgitation (Fig. 2.18) or into the leftventricle during aortography for aortic regurgita-tion (Fig. 2.19). The degree of regurgitation is gradedfrom mild to severe (1+ to 4+). In mild aortic regur-gitation, a small amount of contrast enters the leftventricle during diastole but clears with each sys-tole. In mild mitral regurgitation, a small amountof contrast enters the left atrium during systole butclears in diastole. In severe aortic regurgitation, theleft ventricle is filled with contrast after the first dias-tole and it remains opacified for several systoles. Insevere mitral regurgitation, the left atrium is filledwith contrast after the first systole and becomesprogressively opacified with each beat. In addition,contrast is seen refluxing into the pulmonary veins.Similar qualitative analysis is used to grade tricuspidregurgitation.
Fig. 2.18 Long-axis cross-sectional view of left atrium,left ventricle, and aorta in severe mitral regurgitation.Injection of contrast material into left ventricledemonstrates regurgitation of contrast into left atriumand pulmonary veins.
The quantitative method of assessing regurgi-tation is based on calculation of the regurgitantfraction:
Regurgitant fraction = regurgitant stroke volume
total stroke volume
Regurgitant stroke volume
= total stroke volume− forward stroke volume
Angiographic or total SV is determined from leftventriculography as described previously and for-ward SV is determined by the Fick method. Aregurgitant fraction lower than 30% indicates mildmitral regurgitation, 30–60% indicates moderatemitral regurgitation, and higher than 60% indicatessevere mitral regurgitation. A regurgitant fractionof 10–40% indicates mild aortic regurgitation, 40–60% indicates moderate aortic regurgitation, andmore than 60% severe aortic regurgitation.
It is important to note that the height and dura-tion of V waves are not a direct assessment of thedegree of mitral regurgitation. Severe mitral regur-gitation can exist in the absence of a significant

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 38 — #19
38 Chapter 2
Fig. 2.19 Long-axis cross-sectional view of leftventricle, right ventricle, and aorta in severe aorticregurgitation. Injection of contrast material into proximalaorta demonstrates regurgitation of contrast into leftventricle.
V wave. It has been stated that, for an individualpatient, the height of the V wave correlates with thedegree of regurgitation under conditions of chang-ing afterload. Such conclusions must be drawncarefully however, as there are several factors thataffect the height and duration of V waves:• The degree of mechanical mitral valve impair-ment. Mechanical impairment occurs with a rup-tured papillary muscle, a torn prosthetic valveleaflet, or a perivalvular leak.• The degree of functional mitral valve impair-ment. Functional impairment occurs with papil-lary muscle ischemia or ventricular dilation withdeformation of the valvular annulus.• The compliance characteristics of the left atriumand pulmonary veins. For a given regurgitant vol-ume, a dilated, compliant left atrium will exhibita smaller V wave than a small, noncompliant leftatrium.• The relative impedance to ejection through theaortic valve versus that through the incompetent
mitral valve. An increase in the impedance to aorticejection will favor increased outflow through thelower impedance of the incompetent mitral valve.With all other variables constant, this will increasethe magnitude of the V wave.• The inotropic state of the left ventricle. Anincrease in LV contractility will tend to decrease LVdimensions, decrease the size of the valvular annu-lus, and thus decrease the amount of regurgitantflow.• The length of ventricular systole. A decrease inthe length of ventricular systole will reducethe time available for regurgitant flow to takeplace. However, forward SV may be compromisedas well.
Analysis of the V wave in tricuspid regurgitationis hampered by similar considerations. Nonethe-less, with severe tricuspid regurgitation, the rightatrial pressure trace takes on the shape of the rightventricular pressure trace.
Evaluation of cardiac shunts
A comprehensive discussion of the physiology ofshunts is provided in Chapter 6. Oxygen saturationmeasurements in multiple cardiac chambers andthe great vessels are used to localize and quantifycardiac shunts. Additionally, angiography duringcardiac catheterization may be used to locate cardiacshunts.
Shunt locationShunt localization is usually accomplished using acombination of angiography and measurement ofoxygen saturations in the pulmonary veins, SVCand IVC, right heart chambers, left heart chambers,aorta, and pulmonary artery. Oxygen saturationsampling is used to detect an oxygen saturationstep-up in the right heart in the case of a left-to-right shunt or an oxygen saturation step-down inthe left heart in the case of a right-to-left shunt.A step-up is defined as an increase in the oxygen sat-uration of blood in a particular location that exceedsthe normal variability in that location; whereas,a step-down is a greater-than-expected decrease insaturation for a given location.

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 39 — #20
Myocardial Physiology 39
Shunt quantificationShunt quantification is based on comparison ofsystemic and pulmonary blood flows. Systemic (QS)and pulmonary (QP) blood flows are calculated bythe Fick method previously described.
QP = VO2/(PVO2 content− PAO2 content)
PAO2 content is the pulmonary arterial oxygencontent. PVO2 content is pulmonary venous oxygencontent. Sampling blood from the left atrium (whenthe pulmonary veins return to the left atrium) willprovide a weighted average of the four pulmonaryveins oxygen content. If a right-to-left atrial levelshunt is present this sampling site will not providean accurate assessment of pulmonary vein oxygencontent. Each of the four pulmonary veins can beentered and sampled separately. When this is donesegmental areas of intra-pulmonary shunt and V /Qmismatch can be detected. The PaO2 or saturationof pulmonary venous blood from a lung segmentwith V /Q mismatch will improve with an increasein FiO2 while there will be no improvement if anintra-pulmonary shunt is present.
QS = VO2/(SAO2 content−MVO2 content)
SAO2 is systemic arterial oxygen content. MVO2
content is mixed venous oxygen content. Truemixed venous blood is a mixture of desaturatedblood from the IVC, SVC, and coronary sinus. Ina normal heart a mixed sample of venous bloodfrom these three locations can be obtained fromthe pulmonary artery. In the presence of an intracardiac left-to-right shunt, PAO2 saturation willoverestimate true MVO2 saturation because pul-monary arterial blood will be a mixture of mixedvenous blood and oxygenated pulmonary venousblood from the left heart. In this setting, true mixedvenous saturation must be determined from sam-ples taken from the SVC and IVC. If the very lowoxygen content low volume blood from the coro-nary sinus is ignored then a weighted average ofoxygen content of SVC and IVC blood can be usedto determine MVO2 content:
(3/4× superior vena cava O2 content)
+ (1/4× inferior vena cava O2 content)
This formula may be used to determine MVO2
in the catheterization laboratory when left-to-rightshunts exist. More commonly, particularly in chil-dren, SVC oxygen content is commonly used as asurrogate for MVO2 content. SVC blood has a loweroxygen content than IVC blood and a higher con-tent than coronary sinus blood and thus SVC bloodprovides a very close estimate of the mixture ofthe three samples. In addition, streaming of bloodof varying oxygen contents in the IVC hampersaccurate IVC oxygen content sampling.
After QP and QS have been calculated, shuntscan be quantified. For an isolated left-to-right shunt,the magnitude of the shunt is QP − QS. For an iso-lated right-to-left shunt, the magnitude of the shuntis QS − QP. The ratio QP:QS is also useful. It can becalculated from content data alone because the Vo2
terms cancel out:
QP:QS = (SAO2 content−MVO2 content)
(PVO2 content− PAO2 content)
Furthermore, if the blood is sampled using alow FiO2, the dissolved oxygen portion of thecontent equation (PO2 × 0.003) can be ignored.The hemoglobin × 1.34 term cancels out andthe equation can be simplified to one using justsaturation data from the four sites:
QP:QS = (SAO2 saturation−MVO2 saturation)
(PVO2 saturation− PAO2 saturation)
A QP:QS >2.0 constitutes a large shunt, whereasa QP:QS <1.25–1.5 constitutes a small shunt. Obvi-ously, a QP:QS <1.0 indicates a net right-to-leftshunt.
For bidirectional shunts, it is necessary to cal-culate effective pulmonary blood flow (QPeff) andeffective systemic blood flow (QSeff). QPeff is thequantity of desaturated systemic venous blood thattraverses the pulmonary capillaries to be oxy-genated. QSeff is the quantity of oxygenated pul-monary venous blood that traverses the systemiccapillaries to deliver oxygen to tissue.QSeff andQPeffare always equal. This concept is discussed in detailin Chapter 6.
Qseff=QPeff=VO2/(PVO2 content−MVO2 content)
The left-to-right shunt is defined as QP − QPeffwhile the right-to-left shunt is defined as QS−QSeff.

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 40 — #21
40 Chapter 2
The net shunt is the difference between these twocalculated shunts.
Evaluation of the pulmonaryvasculature
Marked increases or decreases in pulmonary bloodflow routinely occur in patients with congenitalheart disease. Obstructive pulmonary vascular dis-ease may occur as a consequence of increased pul-monary blood flow in patients with congenital heartdisease. The extent of pulmonary vascular diseasewill greatly influence the type of corrective or pal-liative operative procedure performed. For patientswith diminished pulmonary blood flow, an evalu-ation of the extent and caliber of the pulmonaryvessels is necessary to choose the proper correctiveor palliative operative procedure.
Pulmonary artery wedge angiogramThe pulmonary artery wedge angiogram is recordedon cine film while radiocontrast material is injectedinto a catheter that is in the pulmonary arterywedge position. Generally, the artery to the pos-terior basal segment of the right lower lobe isstudied. As obstructive pulmonary vascular diseaseprogresses, the wedge angiogram demonstrates pro-gressive increases in the diameter and tortuosity ofthe pulmonary arteries, a diminution in the blushseen as capillaries fill, and the abrupt termination ofthe dilated, tortuous arteries with a marked decreasein the number of supernumerary arterial branches.
Pulmonary vein wedge angiogramIn many congenital cardiac lesions with reducedpulmonary blood flow, the pulmonary vasculaturemay be well visualized with injection of contrastinto collaterals that arise off the aorta. For patientswith pulmonary atresia, pulmonary blood flow ismarkedly diminished and the pulmonary arteriesmay not be well visualized with contrast injec-tions into collateral vessels. In this instance, thepulmonary vein wedge angiogram may be used todelineate the pulmonary vasculature. Retrogradefilling of the parenchymal pulmonary vessels can beseen on cine recordings when contrast is handinjected into a catheter wedged in a pulmonary
vein. When antegrade pulmonary blood flow isseverely diminished, retrograde filling of even themain pulmonary artery can occur.
Assessment of pulmonary arterialhypertensionAssessment of pulmonary arterial hypertension(PAH) is defined as a PA systolic pressure>35 mmHg or mean pulmonary artery pressure(PAP) >25 mmHg at rest or mean PAP >30 mmHgwith exercise. While the causes of PAH are myr-iad the etiology of pulmonary hypertension relatedto cardiac disease can be divided into four generalcategories:
LA hypertensionElevated LAP can result from a number of causes(mitral valve disease, LV diastolic dysfunction, LVsystolic dysfunction, loss of AV synchrony). This isthe by far the most common cause of elevated PAPin adults with acquired heart disease.
Pulmonary venous obstructionThis may be the result of obstruction to pulmonaryvein entry into the venous circulation as with totalanomalous pulmonary venous return or as withcor triatriatum, or the result of obstructive diseaseinherent to the veins themselves.
Pulmonary vascular occlusive disease(PVOD)Chronic exposure of the pulmonary arterial bed tohigh flow and/or pressure leads to extensive struc-tural changes. There is progressive muscularizationof peripheral arteries, medial hypertrophy of mus-cular arteries and gradually reduced arterial numberdue to occlusive neointimal formation with fibrosis.Chronic LA hypertension can lead to developmentof a similar process thru chronic elevation of PAP.
High QP:QS
When a large nonrestrictive intracardiac communi-cation exists, particularly at the ventricular level,PAP may be systemic or just sub-systemic. Thequestion that must be answered is whether theelevated PAP is due to high flow into a low resis-tance pulmonary bed (high QP:QS, normal PVR,

Alice Nelson Dinardo: “ch02” — 2007/7/17 — 20:27 — page 41 — #22
Myocardial Physiology 41
Table 2.1 Characteristics findings in pulmonary hypertension from different etiologies.
Etiology Pressures LAP TPG PVR QP
LA hypertension PAD ≈ PAOP ≈ LAP(acute)
↑↑ ↔ ↔ ↔
PAD > PAOP ≈ LAP(chronic)
↑↑ ↑ ↑ ↔
Pulmonary veinobstruction
PAD ≈ PAOP LAP ↔ ↑↑ ↑↑ ↔sl ↓
Pulmonary vascularocclusive disease
PAD PAOP ≈ LAP ↔ ↑↑ ↑↑ ↔sl ↓
Large L–R shunt PAD ≈ PAOP ≈ LAP sl ↑ ↔sl ↑
↔sl ↑
↑↑
LAP, left atrial pressure; PAD, pulmonary artery diastolic pressure; PAOP, pulmonaryartery occlusion pressure; PVR, pulmonary vascular resistance (TPG/cardiac output) nL <
2 Wood units; QP, pulmonary blood flow; TPG, transpulmonary gradient (mPAP–LAP)nL 5–10mmHg.
large L–R shunt) or normal/low flow into a highresistance pulmonary bed (normal/low QP:QS, highPVR, PVOD).
Determination of the etiology of pulmonary hy-pertension requires measurement of the PAP, LAP,PAOP, TPG, and PVR as summarized in Table 2.1.
Suggested reading
Chemla D, Antony I, Lecarpentier Y, Nitenberg A. Contri-
bution of systemic vascular resistance and total arterial
compliance to effective arterial elastance in humans.
Am J Physiol Heart Circ Physiol 2003;285:H614–20.
Izzo JL, Jr. Arterial stiffness and the systolic hypertension
syndrome. Curr Opin Cardiol 2004;19:341–52.
Lock JE, Keene JF, Perry SB (eds). Diagnostic and Inteven-
tional Catheterization in Congenital Heart Disease, 2nd edn.
Boston: Kluwer Academic Publishers, 2000.
Maughan WL, Sunagawa K, Burkhoff D, Sagawa K.
Effect of arterial impedance changes on the end-
systolic pressure–volume relation. Circ Res 1984;54:
595–602.
Robotham JL, Takata M, Berman M, Harasawa Y. Ejection
fraction revisited. Anesthesiology 1991;74:172–83.
Segers P, Stergiopulos N, Westerhof N. Relation of effec-
tive arterial elastance to arterial system properties.
Am J Physiol Heart Circ Physiol 2002;282:H1041–6.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 42 — #1
CHAPTER 3
Monitoring
Basic monitoring of cardiopulmonary function isessential to the safe conduct of any anesthetic.For patients undergoing cardiac surgery, advancedmonitoring of cardiac, pulmonary, renal, and cere-bral function will allow measurement of the phys-iologic variables necessary to make sound clinicaldecisions. The extent of monitoring required fora given case should be individualized and basedupon the relative advantages and risks present.The consideration for advanced monitoring shouldinclude patient characteristics, the anticipated surgi-cal procedure, and the postoperative requirementsfor advanced monitoring. This chapter will providean overview of the monitoring systems used mostcommonly in the management of cardiac surgicalpatients.
Standard American Society ofAnesthesiologists (ASA) monitors
The ASA approved the Standards for Basic AnestheticMonitoring in 1986 and last amended the documentin 2005. This standard outlines the basic require-ments for all anesthetics including cardiothoracicand vascular procedures. There are two essentialstandards outlined in the text:• Standard I. Qualified anesthesia personnel shall bepresent in the room throughout the conduct of allgeneral anesthetics and monitored anesthesia care.• Standard II. During all anesthetics, thepatient’s oxygenation, ventilation, circulation, andtemperature shall be continually evaluated.
To ensure oxygenation, the standard prescribes thatinspired oxygen concentration will be monitoredwith an oxygen analyzerwith a low oxygen concen-tration limit alarm in use. The patient’s oxygenationwill be assessed using a quantitative method such aspulse oximetry. Further, when a pulse oximeter isused, the variable pitch pulse tone and a low thresh-old alarm shall be audible. Adequate exposure andillumination is required to assess patient color.Ventilation shall be continually evaluated for
adequacy. Means to determine adequacy includechest excursion, observation of the reservoir bag,auscultation, expired end-tidal carbon dioxide con-centration monitoring and qualitative monitoringof the volume of expired gas. Airway manipulationinvolving a laryngeal mask airway or endotrachealtube shall have the device position confirmed withcarbon dioxide monitoring. When ventilation iscontrolled by a mechanical ventilator, there shallbe a disconnection device in place with an audi-ble alarm. During regional anesthesia or monitoredanesthesia care, ventilation shall be evaluated bycontinual observation of qualitative clinical signsand/or monitoring for the presence of end-tidalcarbon dioxide.Circulation will be assessed with the use of on
electrocardiogram (ECG) continuously displayedduring the duration of the anesthetic. An arterialblood pressure and heart rate will be determinedat least every 5 minutes. Every patient shall fur-ther have at least one of the following continuallymonitored: palpation of a pulse, auscultation of
42

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 43 — #2
Monitoring 43
heart sounds, intra-arterial monitoring, ultrasoundperipheral pulse monitoring, or pulse plethysmog-raphy or oximetry.Finally, every patient shall have their tem-
perature monitored when clinically significantchanges in temperature are intended, anticipated,or suspected.These monitoring standards form the basis upon
which all advancedmonitoring of the cardiothoracicpatient occurs. Advanced monitoring in the cardio-thoracic patient involves both invasive and non-invasive strategies to assess circulation. In addition,the cardiothoracic patient may require advancedcerebral function monitoring. Finally, the cardio-thoracic anesthesiologist is required to monitoradvanced coagulation function monitoring. Theremainder of the chapter will review the variouscomponents of this advancedmonitoring stratagem.
Advanced electrocardiographic(ECG) monitoring
The Advanced electrocardiographic is a standardmonitor during cardiac surgical procedures formon-itoring heart rate, rhythm, and ischemia. A five-electrode ECG system capable of monitoring sevenleads (I, II, III, aVR, aVL, aVF, and V5) is typi-cal. In most operating room (OR) environments,leads II and V5 are simultaneously monitored. Thecombination of these two leads provides the bestsurveillance for ischemia and arrhythmia detection(Fig. 3.1).
Dysrhythmia detectionLead II usually allows P-wave identification andmorphology allowing for easy dysrhythmia iden-tification. In some tachydysrhythmias (paroxysmalatrial tachycardia, nodal rhythm, ventricular tachy-cardia), the P wave may be difficult or impossibleto see in any of the standard leads. In other tachy-dysrhythmias (atrial fibrillation, atrial flutter), theP wave is absent. In some cases of AV nodal blockor AV dissociation, the relationship between theP waves and the QRS complex may be difficult todiscern with standard ECG leads. In such instances,the bipolar esophageal or intra-atrial ECG may beuseful. Two electrodes are incorporated in either
50
40
30
20
Sin
gle
lead
sen
sitiv
ity (
%)
0I II III
ECG lead
aVR aVL aVF V1 V2 V3 V4 V5 V6
Fig. 3.1 The lead sensitivity in detecting myocardialischemia is displayed. The combination of lead II and V5provides the greatest ability to detect ischemia andrhythm disturbances. (From London MJ, Hollenberg M,Wong MF, et al. Anesthesiology 1988;69:232–41, withpermission.)
a 12-French esophageal stethoscope for pediatricpatients or a 15-French esophageal stethoscope foradults. Alternatively, two of the three atrial elec-trodes from a pacing pulmonary artery catheter(PAC) can be used to obtain a bipolar intra-atrialECG. The two leads from these electrodes are con-nected to the right arm and left arm jacks of astandard three-lead ECG system. The third lead ofthe three-lead ECG is connected to the patient viaa skin electrode and lead I monitored. Because theesophageal and intra-atrial ECG place electrodes soproximal to the atria, there is augmentation of atrialactivity such that the P wave is often larger than theQRS complex.
Ischemia detectionThe presence of ECG changes is useful in the detec-tion of myocardial ischemia. Specifically, ischemiaalters repolarization causing either downslopingor horizontal ST-segment depression. Transmu-ral ischemia and myocardial injury are associatedwith ST-segment elevation. In the case of coro-nary spasm, ST-segment elevations are likely to bethe initial manifestation seen on ECG. For ECGmonitoring to be effective in detecting ischemia,the appropriate leads must be monitored. Exercise

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 44 — #3
44 Chapter 3
treadmill testing has demonstrated that 89% ofthe significant ST-segment depressions occurringduring exercise can be detected in lead V5. Theaddition of leads II, AVF, V3, V4, and V6 to leadV5 increases the sensitivity of ischemia detectionto 100% during exercise testing. Combining leadsV5 and II increase the sensitivity for detectingischemic changes to 90%. This combination allowsthe most sensitive dysrhythmia and ischemia detec-tion and is therefore the preferred lead selection inmost OR environments.It is important to understand ECG mode selec-
tion and ischemia analysis. The monitoring mode(0.5–40.0Hz) filters out high and low frequencyartifacts thereby attenuating the effects of extrane-ous interference from 60 cycle interference, elec-trocautery, respiratory variation, and movement.Unfortunately, this mode makes analysis of sub-tle ST segment changes unreliable. The diagnosticmode (0.05–100.00Hz) reflects the true extent ofST segment changes but is more prone to interfer-ence. The monitoring mode is best selected whenthere is a low risk of ischemia; whereas, the diag-nostic mode should be employed when ischemia issuspected or anticipated.Automated ST-segment software is currently
available on many intraoperative monitoring sys-tems. These ST-segment analysis systems identifythe QRS complex and then identify the isoelectricpoint in the P–R interval and a measurement pointalong the ST-segment (80ms from the J-point).Mostmonitors analyze of two to three leads simulta-neously allowing a more complete examination forischemia. Alarms may be set for specific amounts ofST-segment deviation.
Arterial pressure monitoring
Arterial access allows beat-to-beat monitoringof arterial blood pressure as well as the ability toobtain arterial blood samples for analysis of partialpressure of oxygen (PO2), partial pressure of carbondioxide (PCO2), pH, bicarbonate, and other elec-trolytes. Themost common sites of arterial cannula-tion are the radial and femoral arteries in adults andchildren. In newborns the umbilical artery serves asan alternative to the radial or femoral arteries.
Radial artery cannulationRadial artery cannulation can be accomplished ininfants, children, and adults. A 24-gauge Teflonor polyurethane catheter is appropriate for infants<4–5 kg. A 22-gauge catheter is appropriate forinfants and children weighing less than 30 kg,whereas a 20-gauge catheter is used in larger chil-dren and adults. The wrist is dorsiflexed over a rollof towel or gauze and secured on a short arm board.The thumb is taped back to reduce the mobilityof the artery. Neither the dorsiflexion of the wristnor the taping of the thumb should be so severe asto compromise the radial pulse. The puncture siteshould be approximately 2 cm proximal to the sty-loid process of the radius. After appropriate sterileprepping, the area of proposed puncture is anes-thetized with 1–2mL of 1% lidocaine in the awakepatient. When using a 22-gauge catheter it is help-ful to nick the skin with a needle directly over theartery prior to catheter placement. The skin nickhelps prevent deformation of the catheter tip.The catheter is introduced at an angle of 30 to
the artery with the bevel of the needle directedupward. When blood flows freely out the end ofthe catheter, the angle between the catheter andthe artery is reduced and the catheter and needleare advanced approximately 1–2mm. At this point,both the catheter and needle should be within thevessel lumen, and the catheter can be advanced for-ward over the needle into the vessel. If there is noblood flow out the needle, it is likely that the pos-terior wall of the artery has been punctured. Theneedle and catheter are then intentionally advancedthrough the posterior wall. The needle is withdrawnpartly from the catheter and the catheter is thenwithdrawn until its tip is located within the lumenof the artery and free flow of blood is noted. At thispoint, the catheter is advanced into the artery. Alter-natively, a small guide wire (0.018) can be passedup a 24-, 22-, or 20-gauge catheter into the arteryand oftenwill facilitate advancement of the catheter(Fig. 3.2a–c).Radial arterial cannulation is associated with a
very low incidence of morbidity. An Allen’s test toassess collateral circulation to the hand via the ulnarartery and palmar arch is frequently performedbefore cannulation of the radial artery. There is

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 45 — #4
Monitoring 45
(a)
(c)10°
(b)30°
Fig. 3.2 Radial artery cannulation. (a) The wrist ispositioned. (b) The artery is cannulated approximately2 cm proximal to the styloid process of the distal radius.(c) The needle angle is reduced and the catheteradvanced. (From Lake CL. Cardiovascular Anesthesia.New York, Springer-Verlag, 1985:54, with permission.)
controversy regarding the specificity and sensitivityof an Allen’s test, however, and this examination isnot universally applied. The radial artery catheter ismost often placed into thewrist of the nondominanthand for patient comfort and convenience. In someinstances, however, the radial artery catheter mustbe introduced preferentially into one radial arteryor the other, as specified below:• Blalock–Taussig shunts. For children undergoingthese subclavian to pulmonary artery shunts, the
radial artery contralateral to the subclavian arterybeing used must be used for monitoring. Like-wise, for children with pre-existing Blalock–Taussigshunts, accurate arterial blood pressure will beobtained only in the contralateral arm.• Coarctation repair. Arterial blood pressure is bestmonitored in the right radial artery for a variety ofreasons: arterial blood pressure in the left arm maybe lower than that in the right arm in the presenceof hypoplasia of the aortic isthmus, a left subclavianartery patch may be used to repair the coarcta-tion, or left subclavian artery circulation may becompromised by placement of aortic cross-clampsduring the coarctation repair.• Thoracic aortic surgery. Left subclavian arteryflow may be compromised by surgical procedureson the distal arch or descending aorta; there-fore, blood pressure should be monitored in theright radial artery. For procedures involving theascending aorta, the left radial artery is a betterchoice.
Femoral artery cannulationA 22-gauge, thin-wall needle to puncture the arteryin infants and children weighing less than 30 kgcan be used for femoral artery cannulation. Afterfree flow of blood is obtained, a straight wire ispassed through the needle up into the artery. Forinfants, a 2-inch 20-gauge catheter is passed into theartery over thewire. For children, a 3-inch 20-gaugecatheter can be employed. For children weighingmore than 30kg, an 18-gauge thin-wall needle forarterial puncture and a 4-inch 18-gauge catheteris appropriate. For larger children and adults, an18-gauge thin-wall needle for arterial puncture anda 6-inch 16- or 18-gauge catheter is used.Femoral artery catheters have been used with
a low complication rate for infants, children andadults. Hesitation to use femoral artery cathetersin children stems from concern that damage tothe poorly encapsulated hip joint may occur eitherdirectly, from sepsis or arterial occlusion and throm-bosis. This does not seem to be a problem forinfants and children when proper insertion tech-niques and catheter sizes are used. However, forinfants younger than 1month of age, the inci-dence of transient perfusion-related complications

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 46 — #5
46 Chapter 3
(loss of distal pulse, limb coolness) has beenreported to be 25% when a 20-gauge catheter isused. This is higher than the rate associated withradial or umbilical artery catheterization in this agegroup.
Umbilical artery cannulationThe umbilical artery cannulation may be obtainedin the catheterization laboratory or in the inten-sive care unit (ICU) in neonates requiring invasivearterial pressure monitoring. A 3.5- or 5-Frenchcatheter is used for arterial monitoring. The cathetertip should lie just above the aortic bifurcation butbelow L3, or alternatively, above the diaphragm atthe T7–T8 level.
Central venous access
Access to the central venous circulation is essentialfor cardiac surgical patients for a variety of reasonsincluding secure intravenous (IV) access for volumeand medication administration and advanced mon-itoring of volume status and cardiac function. Theinternal and external jugular veins and the sub-clavian veins are commonly used for central venousaccess in infants, children, and adults. The rightinternal jugular vein offers fairly constant anatomywith a straight course to the right atrium and alow complication rate. Attempts at left internaljugular venous cannulation may lead to injury tothe thoracic duct, and for patients with congenitalheart disease, the left internal jugular may draininto a persistent left superior vena cava. The leftsubclavian vein provides an alternative for patientswith difficult or impossible internal jugular cannu-lation. For patients with communication betweenthe right and left heart chambers, all peripheral andcentral venous linesmust be kept clear of air bubblesto avoid potential systemic air embolization.A wide variety of central venous catheters are
available for use. For adults and large children,7- and 8-French double- and triple-lumen cathetersare available. For infants and children weighing<4kg, 4-French double-lumen catheters 5 cm inlength are available. For children weighing >4kg,5-French double-lumen catheters 5 or 8 cm inlength are used.
Internal jugular cannulationThree general approaches to the internal jugularusing anatomical landmarks have been described:central, anterior, and posterior. The centralapproach involves localization of the internal jugu-lar vein at the apex of the triangle formed by thetwo heads of the sternocleidomastoid muscle. Theapex is lateral to the carotid pulse and generally is atthe level of the cricoid cartilage (2–3 finger-breadthsabove the clavicle in adults). This approach appliesto infants and children. The anterior approachinvolves localization of the vein at the lateral borderof the medial head of the sternocleidomastoid at apoint halfway between the clavicle and themastoid.The posterior approach involves localization of thevein under the lateral border of the medial head ofthe sternocleidomastoid at the level of the cricoidcartilage. Regardless of the approach, extreme caremust be exercised to ensure that the jugular veinis cannulated and not the internal carotid artery(CA). Ultrasound imaging of the internal jugularvein demonstrates large anatomic variability in therelationship between the jugular vein and the CA(Figs 3.3 & 3.4). In about half of children and adults,more than 75% of the right CA is overlaid by theright internal jugular vein when the head is rotatedto the left. This overlap can be reduced somewhatby rotating the head less than 40% from the neu-tral position. Ultrasonic guidance facilitates catheterplacement and may reduce the complication rateof central venous catheter placement. The follow-ing is recommended for cannulation of the internaljugular vein:1 The patient is positioned with the head turnedaway from the intended cannulation site. Sup-plemental oxygen is supplied to nonanesthetizedpatients.2 For adults and older children, the pillow isremoved from beneath the head to produce aslightly extended neck position. For elderly patientswith limited neck mobility, removal of the pil-low may not be possible. For children, infants, andneonates, it may be necessary to place a small rollunder the shoulders to prevent cranial hyperflexiondue to the larger head size.3 The anatomic outline of the clavicle and of thetwo heads of the sternocleidomastoid muscle are

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 47 — #6
Monitoring 47
ICA
RIJ
Fig. 3.3 The internal carotid artery (ICA) is wellvisualized. In this patient with spontaneous respiration,the right internal jugular vein is collapsed (RIJ).
identified (some prefer to mark these structureswith a pen). In nonanesthetized patients, liftingthe head off the bed will help define these land-marks. An ultrasonic probe (5.0–7.5MHz) is placedon the neck using ultrasonic gel. The relationship ofthe internal jugular and CA relative to each otherand to the anatomic markings is noted. The depthof the vein below the skin surface also is deter-mined. Head position can be altered to providethe least amount of overlap of the internal jugularand CA without compromising access to the neck.Ultrasonography further allows one to determinewhether the internal jugular is small, absent, throm-bosed or compressed from extravascular structures(i.e. hematoma from previous attempts). This mayprompt a look at the contralateral internal jugularor move to a subclavian vein cannulation.4 The neck is prepped and draped using steriletechnique. The operator is gowned and gloved. Forawake patients, local anesthesia is accomplishedwith 1% lidocaine in the area of the intended needlepuncture. Deeper infiltration should be performed
RIJ
ICA
Fig. 3.4 In this same patient with a Valsalva maneuver,the right internal jugular vein (RIJ) is now engorged andprominent, anterior and lateral to the internal carotidartery (ICA).
with caution because the vein is not very deepbelow the skin. The patient is placed in a 10–15Trendelenberg position. This positioning increasesthe size of the internal jugular and reduces the riskof air embolus. It is best to wait until the last minuteto do this for patients with pulmonary venouscongestion or poor ventricular function becauseprolonged periods in the Trendelenberg positionmay exacerbate pulmonary venous congestion andheart failure. In nonanesthetized patients, this mayresult in patient discomfort, dyspnea, agitation andlack of cooperation.5 A 25-gauge 5/8-inch needle is used to locate thecenter of the vein in all but the largest of adults.A 112 -inch 22-gauge needle rarely is needed tolocalize the internal jugular. There is no need tokeep a hand on the CA after the vein position hasbeen localizedwith ultrasound. This maneuver onlyserves to compress the internal jugular.6 After the vein is localized, the finder needle canbe left in place or removed. The appropriate-sized

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 48 — #7
48 Chapter 3
thin-wall needle is inserted through the skin in thesame orientation as the finder needle. The thin-wallneedle is advanced. If the skin is depressed or dim-pled inward, the vein is at least partially compressed.When dimpling occurs, the skin should be allowedto “rebound.” This does not mean pulling the nee-dle back out of the skin, it means relieving pressureto allow the skin to return to a neutral position.Some compression of the vein by the larger thin-wall needle is inevitable, but when the needle isadvanced without compressing the skin, it is morelikely that the veinwill be entered on theway in andless likely that the veinwill be transfixed and the CAwill be punctured. Often, when the skin is allowedto rebound, free flow of internal jugular blood isobtained without any further advancement of theneedle.7 When free flow of internal jugular blood isobtained, the thin-wall needle is fixed in place withthe fingers of the left hand while the hypothenareminence rests on the patient. A flexible J-wire isadvanced into the thin-wall needle and vein. If thewire goes a short distance out the end of the nee-dle and resistance is met, advancement of the wirewhile spinning it with the right hand should beattempted. If resistance is still met, the wire canbe left in place and the thin-wall needle can beremoved. An appropriate-sized IV catheter is thenplaced over the wire and advanced into the vein.The guide wire is removed and a syringe is attachedto the catheter. The syringe is aspirated and thecatheter is withdrawn until free flow of blood isobtained. The catheter is then advanced into thevein and the guide wire is reintroduced.8 If there is any doubt that the thin-wall needleor catheter is in the internal jugular, the needleor catheter should be connected to the monitorand the venous (or arterial) waveform identified.Checking the color of the blood or the blood flowthrough the catheter are unreliable indicators ofarterial cannulation.9 When the guide wire is in place in the internaljugular (it is reassuring and common to see someventricular ectopy as the wire is advanced), a skinnick is made with a knife. The skin nick should becontiguous with the wire; that is, there should notbe a skin bridge between the wire and the incision
made with the knife. The dilator is passed over thewire. The dilator should only be passed once andonly deep enough to pass through skin, soft tissue,platysma, and into the vein. The dilator is removedand gentle pressure is held over the dilated puncturesite until the central venous pressure (CVP) catheteror PAC introducer is placed.10 For instances in which venous access is difficultor large transfusion requirements are anticipated,two catheters can be placed in the same inter-nal jugular. In this “double-stick” technique, oneguidewire is placed and then a second guidewire isplaced through a second puncture site 1–2 cm aboveor below the first one. The cannulation process isthen the same as described previously.The most common complication of the inter-nal jugular approach is carotid puncture (4%).Other potential complications of the internal jugu-lar approach include pneumothorax, thoracic ductinjury, brachial plexus injury, and air embolism.
External jugular cannulationThe external jugular approach is complicated bythe presence of a system of venous valves, whichcan make the placement of a guidewire and, sub-sequently, a catheter into the central circulation,difficult. The advantage of this approach is thatthere is little or no risk of carotid puncture, pneu-mothorax, thoracic duct injury, or brachial plexusinjury. For adults, the use of a guidewire with aflexible J-shaped tip increases the success rate ofthis approach to 75–95%, compared with 95% forthe internal jugular route. In children, the successrate of this approach is approximately 60%. Clini-cally silent venous thrombosis in pediatric patientsis high when the external jugular catheter does notreach the central circulation.
Central circulation pressuremonitoring
Pulmonary artery catheter monitoringPACs are multilumen, multipurpose cathetersavailable in a variety of sizes (5-, 7-, and7.5-French). A typical PAC contains the following

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 49 — #8
Monitoring 49
components:1 A proximal lumen that terminates in a portlocated 30 cm (7- and 7.5-French) or 15 cm(5-French) from the distal end of the catheter.When the catheter is positioned properly, this prox-imal port will be located in the right atrium. Thislumen is used tomeasure right atrial pressure (RAP)and to inject fluid of a known volume and temper-ature for determination of a thermodilution (TD)cardiac output.2 A distal lumen that terminates in a port located atthe distal end of the catheter. This lumen measurespressures as the catheter is advanced into positionand, when the catheter is properly positioned, isused to measure pulmonary artery systolic pressure(PASP), pulmonary artery diastolic pressure (PADP)and pulmonary capillary wedge pressure (PCWP).3 A balloon located 1mm from the distal end ofthe catheter. This balloon is connected to the proxi-mal end of the catheter by a lumen that runs thelength of the catheter. The balloon can be filledwith air from a syringe located at the proximalend. The 7- and 7.5-French catheters have a 1.5-mLballoon, and the 5-French catheter has a 1-mL bal-loon. When the balloon is inflated, the catheter isdirected forward in the flow of blood. Balloon infla-tion is used whenever the catheter is advanced.When the catheter is positioned properly in the pul-monary artery, inflation of the balloon will result inthe balloon occluding a branch of the pulmonaryartery. The pressure tracing obtained from the dis-tal port at this point will be a measure of thePCWP. As described in Chapter 2 it is technicallythe pulmonary artery occlusion pressure (PAOP)that is measured.4 A thermistor is located at the distal end of thecatheter just proximal to the distal port and the bal-loon. The thermistor is connected to one or moreplugs at the proximal end of the catheter, whichare used to interface the thermistor with a cardiacoutput computer.5 The catheter is labeled in 10-cm increments fromthe distal end of the catheter.6 Optional features in PACs include:a An additional lumen for drug infusion.b An additional lumen for placement of a bipolarright ventricular endocardial pacing wire.
c Atrial and ventricular pacing electrodes for bipo-lar endocardial atrial, ventricular, and atrioventric-ular (AV) sequential pacing. These catheters containthree atrial electrodes and two ventricular elec-trodes. Two electrodes must be in contact withthe endocardium for successful pacing. Consider-ing the variations in patient size and the length ofcatheter necessary to properly position a PAC, thepresence of three atrial electrodes increases the like-lihood that two electrodeswill be in contact with theatrial endocardial surface. These catheters are 80%effective in establishing atrial, ventricular, and AVsequential pacing.d The addition of fiberoptic bundles, which allowcontinuous determination of mixed venous oxygensaturation by reflective spectrophotometry. Light ofselected wavelengths is transmitted down a fiber-optic bundle, the tip of which is located in thepulmonary artery. This light is transmitted throughblood flowing past the fiberoptic bundle and isreflected back to be transmitted down anotherfiberoptic bundle to be analyzed by a photodetector.The differential absorption of known wavelengthsof light by oxyhemoglobin and deoxyhemoglobin isused by a computer to determinemixed venous oxy-gen saturation. The use of continuousmixed venousoxygen saturation measurements will be discussedin detail later.e The ability to perform continuous cardiac outputdeterminations using a thermal filament.f The ability to measure right ventricular ejec-tion fraction using a rapid-response thermistor PAC(discussed in detail later).
PAC placementIn cardiac surgery, PACs usually are introduced per-cutaneously into the right heart and pulmonaryartery via an introducer placed in the right inter-nal jugular vein. For adults and large children, 7-,7.5-, and 8.0-French catheters are used and areplaced through an 8.5- or 9.0-French introducer.The 5-French catheter is used in smaller chil-dren (weighing 15–40 kg) and is placed through a6-French introducer.During placement, the patient should be moni-
tored with a continuous ECG display. A defibrilla-tor should be in the room and in working order.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 50 — #9
50 Chapter 3
The defibrillator should be capable of being syn-chronized with the ECG signal to allow cardiover-sion as well as defibrillation. The catheter must beplaced under sterile conditions by the operator. Thecatheter is placed in a sterile sheath, and the proxi-mal end of the catheter is handed off to an assistant,who uses the syringe to test balloon inflation. Thefully inflated balloon should protrude out over thedistal end of the catheter and inflate symmetrically.The assistant also should connect the proximal anddistal lumens to their respective transducer/flushsystems. The proximal lumen will be used to mea-sure the RAP while the distal lumen will be usedto measure the PASP, PADP, and PCWP. The distallumen trace must be visible on the monitor screenas the catheter is advanced. Finally, the TD car-diac output computer should be connected to theappropriate jack and the correction factor for thecatheter being used should be programmed intothe computer.The catheter is held, loosely coiled, in the opera-
tor’s hand with the tip pointed toward the patient’sleft (toward the right ventricle and pulmonary out-flow tract). The catheter is placed into the introducerand advanced 20 cm for older children and adultsand 10 cm for smaller children. At this point, theballoon is inflated and the catheter is advancedwith a smooth motion. For adults and older chil-dren, a RAP trace will be seen on the distal lumentrace at approximately 20–30 cm. For smaller chil-dren, this will occur at approximately 10–15 cm.Smooth catheter advancement with the ballooninflated continues until the right ventricular traceis seen, followed by the PASP trace and finally thePCWP trace.Catheter advancement stops when the PCWP
trace is seen. For adults and older children, thePCWP tracewill be seen at approximately 45–55 cm.In smaller children, the PCWP trace will be seen atapproximately 25–35 cm. Deflation of the balloonat this time should result in reappearance of thePASP trace. If the PCWP trace remains after bal-loon deflation, the catheter should be pulled back.The catheter should not remain in the PCWP posi-tion for any longer than it takes to measure PCWP.Excessive balloon inflation can lead to pulmonaryartery rupture or pulmonary infarction.
If the catheter is advanced more than 10–15 cm(5–10 cm for smaller children) before the trace fromthe next expected chamber or vessel is noted, thecatheter may be coiling in the right atrium or ven-tricle. At this point, the balloon should be deflated,the catheter should be drawn back into the sheath.The catheter can then be advanced again afterinflation of the balloon. Catheter coiling mayultimately lead to catheter knotting.If coiling occurs, several things can be tried to
advance the catheter out of the RA or RV:1 Remove the catheter from the introducer andmake certain that the balloon inflates properly.2 Orient the curve of the catheter so that it is moreanterior thanmedial as it enters the introducer. Thismay help direct it toward the tricuspid valve orifice.3 After multiple attempts, the catheter may soften.This can be remedied by flushing the distal portwith 2–3mL of iced saline or by gently twisting thecatheter as it is advanced.4 For awake patients, taking a deep breath mayenhance blood flow out the RA and the right ven-tricular outflow track. For anesthetized patients,release of a Valsalva maneuver may accomplish thesame thing.5 Putting the patient in the head-up positionand/or rotating the bed left or right may helpas well.Most patients with congenital heart disease are
not candidates for percutaneous placement of PACs.Some of the reasons and considerations in thesepatients include:1 Some patients (less than approximately 15 kg)are too small for the 5-French catheters.2 In some patients, percutaneous placement of aPAC may be difficult or impossible. For example,the presence of a large atrial septal defect or aventricular septal defect may make placement dif-ficult without the use of fluroscopy. Similarly, thepresence of tricuspid atresia, pulmonary atresia, orpulmonary stenosis make percutaneous placementimpossible.3 The PAC may interfere with the surgical repairand may have to be removed intraoperatively.4 If necessary, catheters can be placed directlyinto pediatric patients by the surgeon imme-diately before termination of cardiopulmonary

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 51 — #10
Monitoring 51
bypass (CPB). A thermistor probe (2.5-French) ora thermistor probe combined with a distal lumen(4-French) may be placed directly into the pul-monary artery via the right ventricular outflowtract. When combined with a directly placed rightatrial catheter (3.5-French), these will allow deter-mination of TD cardiac outputs. Because thesecatheters do not allow determination of PCWP, a leftatrial pressure (LAP) line may be placed by the sur-geon as well. These lines may be placed directly intothe left atrium or into the left atrium via the rightsuperior pulmonary vein. Caution must be exer-cised with left atrial lines to avoid introduction ofair into the systemic circulation.
Central venous and pulmonary arterypressure (PAP) measurements
Right and left atrial pressureRight atrial pressure (RAP) is monitored directlythrough the proximal lumen, whereas LAP is notdirectly measured by the PAC. The PCWP will bean accurate assessment of LAP, except for instancesin which there is pulmonary venous obstruction(rare) or in which the pulmonary alveolar pres-sure exceeds pulmonary venous pressure. In theseinstances, PCWP will reflect pulmonary alveolarpressure (Palv). Pulmonary alveolar pressure willexceed pulmonary venous pressure (Pv) when thedistal port lies in zone one (PAP < Palv > Pv) orzone two (PAP > Palv > Pv) of the lung. Fortu-nately, most catheters (93%) reside in zone three(PAP > Palv < Pv) portions of the right middle andlower lobes.The RAP trace usually is of higher quality than
the PCWP trace because the LAP changes aredamped as they are transmitted through the pul-monary vasculature to be detected by the distalport. The RAP and LAP traces normally contain A,C, and V waves as well as X and Y descents(Fig. 3.5).
A waveThe Awave reflects the atrial pressure increase seenduring atrial systole. Atrial systole occurs at ven-tricular end diastole and is commonly called theatrial kick. The peak of the right atrial A wave
40
20
0
ECG
A
Left atrial pressure
XC V Y
5 sI I
Fig. 3.5 Left atrial pressure (LAP) obtained from apatient undergoing left atrial pacing. Arrow shows pacerspike. The paper speed is 50mm/s and clearly showsthe A, C, and V waves as well as the X and Y descent.(From DiNardo JA. Monitoring. In: DiNardo JA (ed).Anesthesia for Cardiac Surgery, 2nd edn. Stamford, CT:Appleton & Lange, 1998:37–80, with permission.)
follows the peak of the P wave on the ECG by80ms when simultaneous RAP and ECG traces arecompared. The peak of the left atrial A wave followsthe peak of the P wave by 240ms due to the laterdepolarization of the left atrium compared withthe right atrium. The peak A-wave pressure is thebest estimate of ventricular end-diastolic pressure,particularly when ventricular compliance or disten-sibility is poor (Fig. 3.6). Obviously, no A wave willbe present when atrial systole is absent, as in atrialfibrillation and atrial flutter. For instances in whichatrial systole is not synchronous with ventriculardiastole, atrial contraction may occur in the pres-ence of a closed tricuspid or mitral valve duringventricular systole. This will result in productionof a large A wave (cannon A wave) because theatrium cannot empty via the closed tricuspid ormitral valve. Cannon A waves may be seen duringnodal rhythms with retrograde atrial depolarization(Fig. 3.7), re-entrant supraventricular tachycar-dia in which ventricular activation precedes atrialactivation, and heart block with nonconductedatrial activity occurring during ventricular systole.Cannon A waves also may be seen in instances inwhich atrial and ventricular contraction are syn-chronous but in which atrial outflow is preventedby tricuspid or mitral atresia.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 52 — #11
52 Chapter 3
40
20
0 PCWP
AX
VY
ECG
1 sI I
Fig. 3.6 Pulmonary capillary wedge pressure (PCWP)trace from a patient with aortic stenosis and concentricleft ventricular hypertrophy. A large A wave is clearlyseen. The peak A-wave pressure at end-expiration is18 mmHg; this is the best estimate of left ventricularend-diastolic pressure. (From DiNardo JA. Monitoring.In: DiNardo JA (ed). Anesthesia for Cardiac Surgery,2nd edn. Stamford, CT: Appleton & Lange, 1998:37–80,with permission.)
ECG
200
100
0
40
20
0 PCWP
AX C Y
Radial artery pressure
Fig. 3.7 Pulmonary capillary wedge pressure (PCWP)obtained from a patient in a nodal rhythm withretrograde atrial activation. Cannon A waves are present.(From DiNardo JA. Monitoring. In: DiNardo JA (ed).Anesthesia for Cardiac Surgery, 2nd edn. Stamford, CT:Appleton & Lange, 1998:37–80, with permission.)
C waveThe C wave reflects movement of the tricuspid ormitral valve annulus into the atrium during the iso-volumic phase of ventricular systole and is often notwell seen. The C wave follows the A wave by a timeinterval equal to the P–R interval and is seen bestwhen the P–R interval is prolonged.
V waveThe Vwave represents passive atrial fillingwhile thetricuspid and mitral valves are closed during ven-tricular systole. The peak V-wave pressure will bedetermined by the compliance of the atrium andthe volume of blood that enters the atrium duringpassive filling. In the right atrial trace, the V wavepeaks near the end of the ECG T wave, whereas theleft atrial V wave peaks after the T wave.A large V wave may be produced by tricuspid
or mitral regurgitation (Figs 3.8 & 3.9). In this set-ting, the Vwave represents a combination of passiveatrial filling and regurgitation of blood into theatrium via the incompetent valve during ventric-ular systole. Commonly, the height and duration ofthe V wave is used to quantitate tricuspid or mitralregurgitation. Such conclusions must be drawncarefully, however, because the duration of systole,the extent of mitral or tricuspid valve impairment,atrial compliance, the systolic performance of theventricle, and the impedance to ejection via the pul-monary artery or aorta all contribute to the heightand duration of V waves.It is important to note that other factors may be
responsible for production of a large Vwave. A largevolume of blood returning to the atrium and pooratrial compliance will both produce large V waves.For example, in the presence of a ventricular sep-tal defect with a two-to-one left-to-right shunt, leftatrial venous return will be twice that of right atrialreturn. Likewise, in the presence of poor ventric-ular systolic performance, preload reserve may beexhausted tomeet baseline cardiac output demands.In both instances, the large preload requirementswill result in atrial distension, with the atrium func-tioning on the steep portion of its compliance curve.This reduced atrial compliance will result in theproduction of a large V wave during passive atrialfilling.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 53 — #12
Monitoring 53
Fig. 3.8 Pulmonary artery pressure(PAP) and pulmonary capillary wedgepressure (PCWP) from a patient withmitral regurgitation. The presence ofthe large V wave may makedistinguishing PAP from PCWPdifficult. Close examination shows thatthe peak of the PAP trace occurs muchearlier in the electrocardiogram (ECG)cycle than the V wave in the PCWPtrace. (From DiNardo JA. Monitoring.In: DiNardo JA (ed). Anesthesia forCardiac Surgery, 2nd edn. Stamford, CT:Appleton & Lange, 1998:37–80, withpermission.)
1 s
ECG
Radial artery pressure
Pulmonary artery pressure
150
0
50
250 PCWP
AX VY
I I
ECG
50
25
0 Pulmonary artery pressure
Fig. 3.9 Pulmonary artery pressure (PAP) andpulmonary capillary wedge pressure (PCWP) in a patientwith mitral regurgitation. The PCWP V wave is clearlyseen. The arrow points to the end-diastolic pressure inthe PCWP trace. This pressure is approximately 18mmHgand is the best estimate of left ventricular end-diastolicpressure (LVEDP). (From DiNardo JA. Monitoring. In:DiNardo JA (ed). Anesthesia for Cardiac Surgery, 2nd edn.Stamford, CT: Appleton & Lange, 1998:37–80, withpermission.)
Differentiating the PAP trace from the PCWPcan be difficult in the presence of large V wavesbecause of the similarity of the two traces. Fail-ure to recognize the V wave of the PCWP canresult in over advancement of the PAC into a dis-tal pulmonary artery, increasing the likelihood ofa catheter-induced pulmonary artery perforation.Use of simultaneously obtained PAP and systemic
artery pressure or ECG traces can be used to differ-entiate the two traces. It has been demonstrated thatthe peak of the pulmonary artery trace normallyoccurs approximately 130ms after the upstroke ofa simultaneously recorded systemic arterial trace,whereas the peak of the V wave occurs approxi-mately 350ms after the systemic arterial upstroke.Similarly, the peak of the V wave will occur later inthe ECG cycle than the peak of the PAP wave.
X and Y descentThe X descent follows the A and C waves andreflects a combination of the downward displace-ment of the tricuspid and mitral valve with theonset of ventricular systole and atrial relaxationfollowing atrial systole. The Y descent follows theV wave and reflects rapid atrial emptying afteropening of the tricuspid and mitral valves. Thus,the Y descent also reflects early diastolic filling ofthe ventricle. In the presence of pericardial tam-ponade, the X descent usually will remain visiblewhile the Y descentwill be attenuated. In pericardialtamponade, diastolic filling of the heart chambers isimpeded because the potential space available forexpansion of the heart in the pericardium is largelyeliminatedwhen the pericardium is filledwith fluid.For this reason, passive filling and expansion of theventricle as reflected in the Y descent is attenuated.To the contrary, the X descent is preserved becauseit reflects a decrease in pericardial volume as atrialrelaxation and ventricular systole begin.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 54 — #13
54 Chapter 3
For patients with constrictive pericarditis, earlydiastolic filling of the ventricle is not compromisedas it is in pericardial tamponade. Constrictive peri-carditis is characterized by impairment of ventric-ular filling in late diastole. Because early diastolicfilling is not impaired and because atrial pressureis elevated, the Y descent is more prominent thannormal in constrictive pericarditis. As in pericardialtamponade, the X descent remains prominent. Thiscombination of prominent X and Y descents givesa characteristic shape to the atrial pressure curve,which is often referred to as the M or W sign.
Pulmonary artery pressureA determination of systolic, mean, and diastolicPAP can be made with a PAC. In the presence ofnormal pulmonary vascular resistance, the diastolicPAP will overestimate the PCWP by 2–3mmHg. Inthe presence of increased pulmonary vascular resis-tance, the diastolic PAPwill overestimate PCWP andcannot be used as a substitute measurement.
LimitationsThere are major limitations to accurate measure-ment and interpretation of intracardiac and PAPs.Common errors include a failure to properly zerothe transducers, placement of the transducer at aninappropriate level relative to the patient (trans-ducer too low reports a spuriously high pressure),catheter whip, and catheter dampening.
Determination of mean pressureMonitor systems designate systolic, diastolic, andmean pressures as the average highest, lowest, andmean pressures obtained during a preset time inter-val or a series of such intervals. The electronicallydetermined mean RAP and PCWP will be skewedupward by the presence of large V waves. This willcause mean RAP or PCWP to overestimate ven-tricular end-diastolic pressure. A device to providecalibrated paper printout of pressure traces is use-ful in analysis of pressure traces. These paper tracescan be used for accurate determination of A- andV-wave pressures as well as systolic and diastolicPAP. The best estimate of ventricular end-diastolicpressure will be the peak A-wave pressure. Forpatients without an atrial systole, the best estimate
of ventricular end-diastolic pressure will be the RAPor PCWP at end diastole. This can be determinedby obtaining simultaneous ECG and RAP or PCWPpaper traces. End-diastolic pressure in the RAP traceis determined at a point approximately 40ms beforethe start of upstroke of the QRS complex. End-diastolic pressure in the PCWP trace is determinedat the QRS ST-segment junction.
Changes in pleural pressureTransmural pressure, i.e. the pressure acting todistend a heart chamber, is determined by thepressure–volume relationship of the chamber.Intracardiac pressures (such as RAP and PCWP) areequal to the transmural pressure plus the juxtacar-diac pressure. Transmural and intracardiac pressurewill be equal as long as juxtacardiac pressure is zero.Pleural pressure is a major determinant of juxtac-ardiac pressure. Pleural pressure will be negativeduring spontaneous inspiration and positive dur-ing controlled inspiration and forced exhalation.Large fluctuations in pleural pressure will causeintracardiac pressure to over- and underestimatetransmural pressure and preload. Ideally, all intra-cardiac pressure determinations should be made atpassive end-expiration, when pleural pressure isclose to zero (atmospheric pressure).If positive end-expiratory pressure (PEEP) is
added to the ventilation circuit, the juxtacardiacpressure at end expiration may be greater thanatmospheric pressure; this will cause intracardiacpressure to overestimate transmural pressure andpreload. How much a given quantity of PEEPwill elevate juxtacardiac pressure depends on therelationship of lung and thoracic compliance. Undernormal circumstances, the juxtacardiac pressure isexpected to rise by approximately one half the valueof the added PEEP. Thus, if 10 cm H2O of PEEP isadded, the juxtacardiac pressure can be expectedto increase by 5 cm H2O. When lung compliance ishigh (emphysema) and thoracic compliance is low(obesity), a larger proportion of the added PEEP willbe added to the juxtacardiac pressure. A smallerproportion will be added in cases where lung com-pliance is poor (acute respiratory distress syndrome)and thoracic compliance is high (muscle relaxation).

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 55 — #14
Monitoring 55
Ventricular preload and pressuremeasurementsVentricular preload is defined as the ventricu-lar end-diastolic volume. Unfortunately, methodsof obtaining measurements of ventricular end-diastolic volume are not possible in a clinical envi-ronment. In the absence of tricuspid or mitralstenosis, the A wave of the RAP and LAP (as mea-sured by PCWP) traces are good estimates of theright and left ventricular end-diastolic pressures. Ifwe assume that the ventricular pressure–volumerelationship does not vary, then measurement ofventricular end-diastolic pressure is as good anassessment of preload as ventricular end-diastolicvolume. Unfortunately, the shape of the ventricularpressure–volume relationship is not linear. Fur-thermore, changes in ventricular distensibility andcompliance alter the relationship between ventric-ular pressure and volume. It is not surprising, then,that changes in PCWP and LAP have been shownto correlate poorly with changes in left ventricularend-diastolic volume in both the pre- and post-CPBperiods.
Thermodilution cardiac outputdeterminationThermodilution (TD) cardiac output is a modifica-tion of the indicator dilution method in which flowis determined from the following relationship:
Known amount of indicator injected
× time/measured concentration of indicatorIn the bolus TD method, the indicator is a crys-talloid injectate (usually 5% dextrose in water orisotonic saline) at a temperature lower than theblood temperature. Blood temperature is measuredby a thermistor in the pulmonary artery. Crys-talloid temperature is measured by separate ther-mistor. A predetermined volume of crystalloid isinjected into the right atrium. Adequate mixingof the crystalloid and blood occurs before passageinto the pulmonary artery, and the change in bloodtemperature over time after injection of the crys-talloid is measured by the thermistor in the pul-monary artery. Cardiac output in liters per minutecan be calculated with the aid of a computer and
the equation:
Cardiac output = V1 × S1 × C1 × (TB − T1)
× 60/SB × CB
∫TB(t) dt
where V1 is the volume of the injectate; S1 andSB are the specific gravity of the indicator and theblood, respectively; C1 and CB are the specific heatof the indicator and the blood, respectively; and T1and TB are the temperature of the indicator and theblood, respectively. (S1×C1)/(SB×CB) = 1.08whenisotonic saline or 5% dextrose is injected. TB(t)dtis the temperature–time curvemeasured by the pul-monary artery thermistor after indicator injection.∫TB(t) dt is the area under the temperature–timecurve.A computer extrapolates the exponential down
slope of the temperature–time curve to the base-line and then determines the area under thecurve. With all variables thus known or mea-sured the computer solves the equation for cardiacoutput.Two recent modifications of the bolus TD tech-
nique deserve attention: continuous cardiac output(CCO) monitoring and RV ejection fraction (EF)catheters.The CCO technique makes use of a thermal fil-
ament located between the 15- and 25-cm gra-dations on the PAC. No injectate is necessary.This filament infuses, on the average, 7.5W ofheat, heating the blood as it passes by. Althoughwarmed, the blood temperature always remainsbelow 44C. The resulting temperature change isdetected downstream in the pulmonary artery andcross-correlated with the input sequence to producea TD washout curve. This requires use of a signalprocessing systemwith an enhanced signal-to-noiseratio because the thermal input is low relative to thebackground PA thermal activity. The monitor dis-plays the average cardiac output from the previous3–7minutes updated every 30 seconds. In the Statmode, a new cardiac output can be obtained every45–60 seconds. In this mode, fast trend estimates ofcardiac output can be obtained when an unstablethermal signal is present. These catheters also canbe used to obtain standard bolus injectate cardiacoutputs.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 56 — #15
56 Chapter 3
Clinical studies have demonstrated a close cor-relation between TD cardiac output determinationsmade with the bolus and CCO techniques in a rel-atively stable ICU environment. A major advantageof the CCO technique would be the ability to mon-itor acute changes in cardiac output (CO) as theyoccur in real time. In the Stat mode, these changescan be tracked approximately every minute; in thestandard mode, changes are averaged over timeand show data more consistent with a trend overtime. In either mode, the changes in CCO lagbehind those seen with mixed venous saturationmonitoring.Right ventricular ejection fraction (RVEF)
catheters are another modification of the bolusinjectate catheter. RVEF catheters incorporate:• a rapid response thermistor, which has a reac-tion time of 50ms compared with the 300–1000msresponse time of standard bolus injectate PACs.• a multi-hole injectate port located 21 cm fromthe catheter tip to ensure complete mixing of theinjectate in the RV.• two ECG electrodes, which enable the computerto detect the R wave.• This arrangement allows beat-to-beat determina-tion of PA temperature changes. The injectatemixesand equilibrates with RV blood within two beats.There is an exponential decrease in the amountof indicator ejected with each subsequent beat. PAconcentrations of indicator for each beat are equalto the RV end-diastolic concentration of indicatorfor that beat. This produces a series of diastolictemperature plateaus that are identified by the com-puter. The RVEF is calculated as follows from threediastolic plateaus using the equation:
EF = 1− RFmeanwhere
RFmean = (RF1 − RF2)/2RF1 = (T2 − TB)/(T1 − TB)
RF2 = (T3 − TB)/(T2 − TB)
where T1, temperature at first diastolic plateau; T2,temperature at second diastolic plateau; T3, tem-perature at third diastolic plateau; and TB, bloodtemperature.
• Stroke volume (SV), right ventricular end-diastolic volume (RVEDV), and right ventricularend-systolic volume (RVESV) are calculated asfollows:
SV = CO/HR
RVEDV = SV/EF
RVESV = RVEDV − SVThenormal RVEF = 0.4. Good correlations betweenPACdeterminedRVEF and radionuclide determinedRVEF have been reported.• Several points regarding TD CO techniques(bolus, RVEF, and CCO) are worth emphasizing:a TD CO is a measure of pulmonary blood flow,which in the absence of shunting (both intracar-diac and systemic to pulmonary artery), is equal toforward right heart output.b Cardiac output is inversely proportional to thearea under the pulmonary artery temperature timecurve.c There are large cyclical variations in the TD deter-mination of cardiac output during the differentphases of mechanical ventilation. This seems to bedue to cyclic variations in pulmonary blood flowandtemperature. For this reason, bolus measurementsobtained at random during the ventilatory cycle willexhibit a great deal of variability, whereas thoseobtained during the same phase of the ventilatorycycle will have the greatest reproducibility. It hasbeen demonstrated thatmultiple cardiac output val-ues obtained at end expiration or peak inspirationin ventilated patients have high reproducibility. Thehighest measured TD CO occurs at peak inspiration,whereas the lowest occurs at end expiration. Tripli-cate TD CO determinations are commonly made atend-expiration because end-expiration is the easiestphase of respiration to detect clinically. This prac-tice provides excellent reproducibility but tends tounderestimate the average cardiac output over onefull cycle of mechanical ventilation.d Injectate temperatures from 0C to room temper-ature are used. The lower temperatures are obtainedby placing the injectate in an ice bath. The accuracyand variability of TD CO in adults is similar witheither 10mL of room temperature or iced injectate.Sinus bradycardia and atrial fibrillation have been

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 57 — #16
Monitoring 57
reported in conjunction with iced injectate for car-diac output determination. The slowing of the sinusrate is likely due to cooling of the sinus node.• TD cardiac output is inaccurate in thepresence of:a Low cardiac outputs. Cardiac output is overesti-mated because low flow allows the cold injectate towarm and reduces the area under the TD curve.b Left-to-right intracardiac shunts (atrial septaldefect, ventricular septal defect). Computer analysisof the temperature–time curve often is not possi-ble due to recirculation of indicator (cold water)through the pulmonary vasculature, which resultsin interruption of the exponential downslope ofthe temperature–time curve with a prolonged, flatdeflection. The larger the shunt, the earlier the recir-culation curve interrupts the normal downslope.Manual planimetry has been used to determine thearea under the two portions of these curves. Theratio of the area under the terminal deflection ofthe curve to the area under the entire curve hasbeen shown to be an accurate estimate of the ratioof pulmonary to systemic blood flow.c Tricuspid regurgitation. Regurgitation of a frac-tion of the cold injectate results in delayed clearanceof the indicator from the right heart. This causesthe TD curve to be broad and of low amplitude,which results in inaccurate assessment of forwardcardiac output. In the presence of TR TD cardiacoutput tends to underestimate true cardiac outputat high cardiac outputs and to overestimate it at lowcardiac outputs. Similar problems are encounteredwith CCO catheters.d Rapid infusion of volume via peripheral IVcatheters. Abrupt increases in the infusion rate ofIV solutions within 20 seconds of a bolus TD COdetermination have been shown to result in vari-ations of up to 80% in TD CO. The precise timingof the infusion rate increase relative to the TD COmeasurement determines whether the output willbe an over- or underestimate. It is recommendedthat volume infusions be terminated or held at aconstant rate for at least 30 seconds before a TD COdetermination. Likewise, rapid infusions of cold IVsolutions affect the accuracy of CCO catheters.The accuracy of bolus TD CO determinations in theperiod immediately following termination of CPB
is questionable. Bolus TD COs have been shownto underestimate true cardiac output by approx-imately 0.5 L/min in the first 10minutes aftertermination of CPB due to a downward drift ofthe temperature baseline in the pulmonary artery.Another source of bolus TD CO error in the first30minutes after termination of CPB is the presenceof respiratory variations or thermal noise in the pul-monary artery blood temperature. These thermalvariations in pulmonary artery blood temperaturemay cause large variations in the bolus TD COdeterminations made at the various points in therespiratory cycle. This problem can beminimized bymeasuring bolus TD CO at the same point in the res-piratory cycle or eliminated by holding ventilationduring bolus TD CO determination.Similar considerations may exist for the CCO
technique. In theory, the data processing of the CCOsystem should minimize the effects of baseline tem-perature shift and of thermal noise and improveperformance. There is a poor correlation betweenbolus TD CO and CCO during the first 45 minutesafter termination of CPB. The “stat” mode should beused during this interval.
Continuous mixed venous oxygensaturation (SvO2) monitoringSvO2 monitoring is available with some PACs. TheSvO2 is measured in the main pulmonary artery byoximetry. The main pulmonary artery is the loca-tion of the most reliable site of true mixed venous(SVC, IVC, and coronary sinus) blood. In infants andchildrenwhere SVC saturation is used as a surrogatefor mixed venous saturation surgically placed oxi-metric SVC catheters can be used. In either case, theSvO2 is used to determine total tissue oxygen bal-ance. It will not reflect regional oxygen imbalance(Table 3.1). Several definitions are in order:• Oxygen (O2) delivery (DO2) = cardiac output(CO) × O2 content.• Arterial oxygen content (CaO2) = (hemoglobin(Hgb)× 13.8) (SaO2)+ (0.003× PaO2).• Mixed venous oxygen content (CvO2) = (Hgb ×13.8) (SvO2)+ (0.003× PvO2).• Oxygen consumption (VO2) = the metabolic rateor the amount of oxygen consumed by the body.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 58 — #17
58 Chapter 3
Table 3.1 Limitations of mixed venous oxygensaturation monitoring. (From Marx G, Reinhard K. CurrOpin Crit Care 2006;12:263–8, with permission.)
SvO2 level Consequences
SvO2 > 75% Normal extraction;O2 supply > O2 demand
75% > SvO2 > 50% Compensatory extraction;increasing O2 demand ordecreasing O2 supply
50% > SvO2 > 30% Exhaustion of extraction;beginning of lactic acidosis;O2 supply < O2 demand
30% > SvO2 > 25% Severe lactic acidosis
SvO2 < 25% Cellular death
This is equal to the amount of oxygen delivered sys-temically (CO) (CaO2) minus the amount of oxygenreturned to the heart (CO) (CvO2).• If we ignore the small dissolved component ofoxygen in arterial (0.003×PaO2) and venous blood(0.003× PvO2) then (CO) (CaO2)− (CO) (CvO2) =[(Hgb× 13.8) (SaO2) (CO)]− [(Hgb× 13.8) (SvO2)(CO)] = (Hgb× 13.8) (CO)× (SaO2 − SvO2).This is simplified to:
SvO2 = SaO2 − [VO2/(Hgb× 13.8)(CO)]
Thus, mixed venous oxygen saturation as measuredcontinuously by a mixed venous saturation PACvaries directly with CO, Hgb, and SaO2 and variesinversely with VO2. If SaO2, Hgb, and VO2 remainconstant, then SvO2 will directly reflect changes inCO. Under these circumstances, continuous mea-surement of SvO2 is analogous to a continuous COmeasurement. The response time of SvO2 to acutechanges in CO under conditions of constant SaO2,Hgb, and VO2 has been demonstrated to be morerapid than CCOmeasurements. This is a reliable andsensitive indicator of function in the cardiac surgicalpatient.A normal SvO2 is 75%, which corresponds to
a mixed venous PO2 of 40–45mmHg. SvO2 is
a reflection of the adequacy of systemic oxygendelivery. A reduced SvO2 indicates inadequatesystemic oxygen delivery and increased peripheraloxygen extraction and should prompt an evalu-ation of SaO2, Hgb, VO2, and CO. Similarly, alow CO in the setting of a normal SvO2 indicatesthat systemic oxygen delivery is adequate to meetpresent metabolic needs and that, in reality, theCO is not low for the metabolic demand. Althougha high CO is reassuring, it does not guaranteeadequate systemic oxygen delivery under condi-tions of reduced Hgb and SaO2 or increased VO2.A SvO2 measurement allows this determination tobe made.
Hemodynamic profilesThe information obtained from a PAC can be usedin conjunction with arterial blood pressure moni-toring to obtain a number of derived hemodynamicparameters. The most commonly used parameters,their formula, and their units of measurement aregiven in Table 3.2.
Efficacy and complications ofpulmonary artery catheterizationRemarkably, demonstrating the efficacy of pul-monary artery catheterization is difficult. There areseveral studies indicating that PAC is not associatedwith improved outcome. Unfortunately, each studycarries certain limitations making a broad recom-mendation against use in specific patient popula-tions impossible. Published guidelines for PAC useindicate that PAC risk and benefit must be weighedin each patient in view of the specific patient char-acteristics, intended surgical procedure, and thepractice setting. PACs are indicated in patients atincreased risk of hemodynamic disturbance, clinicalevidence of cardiovascular disease, pulmonary dys-function, hypoxia, renal insufficiency, or other con-ditions associated with hemodynamic instability.Surgical procedures associated with increased riskinclude those with anticipated hemodynamic insta-bility, damage to the heart, vascular tree, kidneys,liver or brain. The decision to use a PAC should bebased upon the individual hemodynamic risk char-acteristics of the individual case rather than the type

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 59 — #18
Monitoring 59
Table 3.2 Hemodynamic parameters,derivation, and measurement.(From DiNardo JA. Monitoring. In:DiNardo JA (ed). Anesthesia for CardiacSurgery, 2nd edn. Stamford, CT:Appleton & Lange, 1998:37–80, withpermission.)
Formula Units Normal value
SV = CO/HR× 1000 mL/beat 60–90
SI = SV/BSA mL/b/m2 40–60
LVSWI = [1.36× (MAP− PCWP)/100]× SI [g-m/m2]/beat 45–60
RVSWI = [1.36× (PAP− CVP)/100]× SI [g-m/m2]/beat 5–10
SVR = (MAP− CVP/CO)× 80 dynes s/cm5 900–1500
PVR = (PAP− PCWP/CO)× 80 dynes s/cm5 50–150
BSA, body surface area; CO, cardiac output; CVP, central venous pressure;HR, heart rate; LVSWI, left ventricular stroke work index; MAP, mean arterialblood pressure; PAP, pulmonary artery; PCWP, pulmonary capillary wedge pres-sure; PVR, pulmonary venous return; RVSWI, right ventricular stroke work index;SI, stroke index; SV, stroke volume, SVR, systemic vascular resistance.
of procedure. Finally, PAC use may be indicatedfor postoperative management depending uponthe practice setting which should consider factorssuch as technical support and nursing training andskills.PAC insertion carries all the risks of central line
placement. There can be arterial injury, pneumoth-orax, arrhythmias, pulmonary artery hemorrhage,thromboembolism, sepsis, and endocardial dam-age. In addition, there may be misinterpretation ofinformation resulting in inappropriate patient care.Finally, unnecessary PAC placement is expensive.The incidence of catheter-induced transient pre-
mature ventricular contractions (PVCs) duringadvancement of PACs is approximately 65%;whereas, the incidence of persistent PVCs duringcatheter advancement is only approximately 3.0%.These persistent PVCs are generally self-limited.Removal of the catheter nearly always stops the per-sistent PVCs. If persistent, pharmacologic therapywith lidocaine (1.0–1.5mg/kg) may suppress thesePVCs. The prophylactic use of lidocaine doesnot reduce the incidence of these benign, tran-sient catheter-induced PVCS. The incidence ofcatheter-induced right bundle branch block is lessthan 0.05%. Although frequently mentioned, therisk of complete heart block in a patient with apre-existing left bundle branch block is rare. If con-cerned about arrhythmias, the PAC can be floated
after the sternum and pericardium are opened anddirect access to the heart obtained.The incidence of pulmonary artery rupture, a
potentially lethal complication, is less than 0.07%.The risk of pulmonary artery rupture is increasedby anticoagulation, pulmonary hypertension, distalcatheter placement, and eccentric balloon inflation.Pulmonary infarction is rare (<0.07%) and can beavoided by preventing the catheter from remainingin a continuous wedge position. Placement of pul-monary catheters has resulted in direct tricuspid andpulmonary valvular damage as well as tricuspid andpulmonary valvular endocarditis.
Transesophageal echocardiography
Transesophageal echocardiography (TEE) is anintraoperative diagnostic and monitoring modal-ity with wide use among cardiovascular anesthesi-ologists. The esophagus lies in direct proximity tothe heart and great vessels allowing extraordinarilyclear imaging windows. Furthermore, TEE allowsintraoperative use without disrupting the surgicalprocedure. It is a valuable tool in the ICU and inthe evaluation of trauma or other hemodynamicallyunstable or poorly responsive patients. Every car-diovascular anesthesiologist should be familiar withthe basic applications, advantages, and limitationsof TEE.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 60 — #19
60 Chapter 3
(a) (b) (c)
Fig. 3.10 Generation of longitudinal ultrasoundwave front production. (a) Single small element.(b) Multiple small elements (phased array). (c) Singlelarge element. The ultrasound waves travel in circularfashion away from a single element. Transesophageal
echocardiography (TEE) imaging typically employsphased array ultrasound wave generation. (FromFeigenbaum H. Echocardiography, 5th edn. Philadelphia:Lea & Febiger (Lippincott Williams & Wilkins), 1994:4,with permission.)
Basics of ultrasoundUltrasound is defined as sound waves above theaudible range in humans (above 20 000 cycles/s). Inechocardiographic equipment, piezoelectric crystalsin the distal transducer head generate and receivethe ultrasound waves (Fig. 3.10a–c). A high fre-quency electrical current is applied to the crystalcausing vibration and soundwave formation. As thegenerated soundwaves pass through tissue, they areeither absorbed, reflected, refracted, or scattered.The degree of ultrasound wave reflection (returnto the transducer) is enhanced when the struc-ture of interest is perpendicular to the ultrasoundwave. In order to identify two contiguous struc-tures, there must be a difference in density andimpedance between them altering beam absorption,reflection, refraction and scattering.The frequency of the ultrasound waves produced
by the piezoelectric crystals is important. Recallthat wavelength equals velocity (V ) divided by fre-quency (F): 1 = V /F. Because ultrasound travelsat 1540m/s through soft tissue, there is a constantrelationship between frequency andwavelength. Asthe frequency of the vibrations of the piezoelectriccrystals increases, the length of the waves produceddecreases. A smaller wavelength signal allows betterimage resolution but is prone to greater signal atten-uationwith increasing distance from the transducer.Likewise, greater wavelength will reduce resolu-tion, but will enhance visualization of structures atgreater depth from the transducer.When the piezoelectric crystal receives a reflected
sound wave, it vibrates and generates an electrical
signal. Because the wavelength, the frequency, andthe speed of the transmitted and reflected wavesare known, the time it takes for the signal to betransmitted and reflected back can be used to deter-mine the depth of the reflecting object (remember,ultrasound travels at a constant 1540m/s throughsoft tissue). With proper amplification and pro-cessing, these signals are converted to display thereal-time reflected wave activity (the image).Doppler echocardiography is based on the
Doppler principle, which states that when a wave ofa given frequency strikes a moving target it will bereflected with a frequency shift proportional to thevelocity of the target parallel to the path of the emit-ted wave. If the target is moving toward the emittedwave, the frequency of the returning reflected wavewill be higher. If the target is moving away fromthe emitted wave, the frequency of the reflectedreturning wave will be lower. Red blood cell mass isan excellent reflector in the heart and vascular sys-tem. Measuring the red blood cell flow velocity inthe heart is the application of Doppler technologyin echocardiography. The Doppler principle, whenused to calculate the velocity of red blood cell mass,can be summarized in the following equation:
V = c fd/2fo cos θ
where V , velocity of red cells; c, speed of sound intissue (1540m/s); fd, shifted or Doppler frequency;fo, transmitted frequency; θ , the angle of incidencebetween the transmitted wave and the velocityvector being interrogated.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 61 — #20
Monitoring 61
Recall that cosine 90 and cosine 270 = 0,the cosine 0 = 1 and cosine of 180 = −1;therefore, detection of velocity is most accuratewhen the transmitted beam and the velocity vec-tor are parallel (cosine 0 and 180). The detec-tion of velocity is impossible when the transmittedbeam and the velocity vector are perpendicular(cosine 90 and 270). In practice, aligning theDoppler beam and the velocity vector within 20produces acceptable results (6% underestimation ofvelocity). By convention, flow away from the trans-ducer (cosine 180) has a negative value and flowtoward the transducer (cosine 0) has a positivevalue.
M-mode echocardiographyM-mode echocardiography is the simplest echo-cardiographic imaging technique. Ultrasonic wavesof known frequency and wavelength are trans-mitted in a single beam path and recorded overtime. This provides a linear (“ice pick”) view ofthe imaging sector through which the beam passes(Fig. 3.11). M-mode is used in conjunction withtwo-dimensional (2-D) imaging and the cursor lineis used to direct the beam path through the desiredarea. The reflected waves are displayed in real timeas a time-motion study. The vertical axis displaysthe distance and intensity of the reflected from
Fig. 3.11 M-mode image through the left ventriclewith a measurement of fractional shortening (FS).The left ventricular internal dimension is measuredin both systole (LVIDs) and diastole (LVIDd). TheFS = LVIDd – LVIDs/LVIDd. Normal is 0.25–0.45.
the transducer, and time is on the horizontal axis.Blood-filled chambers with little or no reflectedwave activity appear black,whereas valve tissue andmyocardium with high wave reflectivity are gray orwhite.Ultrasound waves through a single beam path
are transmitted and received in 0.001 seconds. Asa result, the display is a real-time repetitive dis-play of cardiac activity along this single beam lineat 1000 frames/see. This M-mode feature allowsvery high-resolution images of moving cardiacstructures.
Two-dimensional (2-D) echocardiographyTwo-dimensional imaging is the display of reflectedimages obtained for transmission of waves not alonga single beam line but across a multiple beam linesector. This sector usually is 60–90wide (Fig. 3.12).Sector scanning is accomplished most frequentlyby use of a phased-array technology. In 2-D imag-ing, a set of piezoelectric crystals are activated inphased sequences to create a single beam througha defined sector. An analogy may help: For M-mode, imagine a man holding a flashlight in oneposition, looking at one object; in 2-D, imaginethe same man moving the flashlight beam backand forth across the horizon and putting the com-bined images together to create a picture of theobjects in the night. The resulting sector sweep in
Fig. 3.12 Two-dimensional (2-D) mid-esophageal fourchamber view of the heart. There is left ventricular septalhypertrophy.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 62 — #21
62 Chapter 3
2-D contains approximately 100 single scan lines.The computer assembles these scan lines and dis-plays the processed information as the echocardio-graphic image. Obviously, obtaining 100 scan linesis more time consuming than obtaining one scanline, as in M mode (hence, diminished spatial res-olution). Two-dimensional images are presented inreal timewith the sector scan updated 30–60 times/sas opposed to the 1000 times/s of M mode. As withM mode, distance of the reflected wave from thetransducer is displayed from the top of the scandown and the displayed brightness of the reflectedwave is proportional to its amplitude.
Pulsed-wave (PW) DopplerPW Doppler analyzes frequency shifts in a time-gated manner. The transducer intermittently trans-mits and then waits a specified time (t) to receivereflected ultrasonic signals. This pulse and receivepattern allows depth localization because the dis-tance of the reflecting object from the transducer isdefined by:
d = ct/2
where d, distance of the reflecting object from thetransducer; c, 1540m/s; t, time between emissionand reception of signal.In practice, the PW Doppler cursor and sample
volume are positioned on an updated 2-D image.After the Doppler cursor and sample volume arepositioned, only reflected signals from that positionare analyzed (Fig. 3.13). The sample volume alsocan be selected (usually from2 to 6mm). This allowsthe interrogated area to be expanded or contracted.Data are displayed as spectra, which are a real-timepresentation of velocity over time.There are limitations with PW Doppler. In order
to reliably detect the frequency shift (and hence thevelocity) of a reflecting object, the reflected ultra-sound wave must be sampled at a frequency atleast twice that of the object (Nyquist criterion). Thesampling frequency of PWDoppler is the pulse repe-tition frequency (PRF). Thus, the maximal detectedvelocity for a given PRF is PFR/2. This is the Nyquistlimit. Thus, the maximum velocity that can bedetected is limited. An additional problem is that the
Fig. 3.13 Pulse wave Doppler at the distal tips of themitral valve demonstrating an E and A wave.
PRF must decrease as the distance from the trans-ducer to the sampling site increases. This must occurbecause it takes longer for the emittedwave to reachthe increased depth and for the reflected wave toreturn.Exceeding the Nyquist limit causes aliasing or
wraparound. The signal literally wraps around thevelocity scale in the other direction. It then becomesdifficult or impossible to determine red cell velocityor direction. The trade-off is unambiguous distanceinformation but ambiguous velocity and direc-tion information. An analogy may help: recall oldWestern movies in which the wagon wheels appearto be rotating backwards as the wagon moves for-ward. This is due to the frame capture rate of thefilm as the spokes on the wagon wheel turn. Appro-priate film capture (altering the PRF) will capturethe forward progression of the spokes allowing theimage to portray the reality. There are two strategiesto deal with aliasing during PW Doppler interroga-tion. The first is to increase the available scale. Thesecond is to shift the baseline. If wraparound stilloccurs, then continuous-wave (CW) Doppler mustbe used to determine peak velocity and direction.PWDoppler is useful for measuring low velocities
at very specific locations such asmitral and tricuspidinflow or in the pulmonary and hepatic veins.
Continuous-wave DopplerIn CW Doppler, one transducer continuously emitssignals and a separate transducer continuously

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 63 — #22
Monitoring 63
receives reflected signals. These transducers are notthe same ones used to obtain 2-D images. Thisarrangement allows reliable measurement of veryhigh velocities because there is no lag betweenemission and reception of signals. In other words,the PRF is extremely high. Because reflected sig-nals returning from all points along the Dopplerbeam are recorded, the location of returning sig-nals is ambiguous. In addition, lower velocity signalsare buried in the higher velocity signals. Therefore,CW Doppler provides unambiguous peak velocityand direction information but ambiguous distanceinformation.In practice, the CW Doppler cursor is positioned
on an updated 2-D image just like PW except thatthere is no sample volume. A spectrum of data isdisplayed demonstrating a real time presentationof object velocity over time. CW Doppler is use-ful for measuring high velocities such as those seenwith aortic stenosis (Fig. 3.14) or with intracardiacshunts. With the baseline shifted, velocities up to600–800 cm/s are obtainable.
Color-flow DopplerColor-flow CF Doppler is a modification of PWDoppler called multigated PW Doppler. Samplingof object velocity occurs at several locations alongmany lines in a sector. The sample volumes are
Fig. 3.14 Continuous wave Doppler across the aorticvalve in the deep transgastric long-axis view. The peakvelocity is approximately 3m/s yielding a peak gradientof 36mmHg.
called packets. The average velocity and directionfor the spectra in a sample volume are deter-mined and assigned a predetermined color. Gener-ally, 8–16 samples per frame determine the averageobject velocity. The set of velocities that are aver-aged in a sample volume for a single frame is calleda packet or packet size. Object velocities are assignedspecific colors. A popular presentation is BART (blueaway, red toward). In this scheme, velocities towardthe transducer are red and those away are blue. Asvelocity increases, the intensity of color increasesas well. The CF Doppler image is presented in realtime as a sector displayed over a real-time 2-D image(Fig. 3.15).CF Doppler has some of the same limitations as
PW Doppler. There is no position ambiguity, butthe peak velocity is limited and decreases with thedistance from the transducer. Aliasing occurs andis presented as a color mosaic. Because the colorimage is presented over the real-time 2-D image,the direction of the aliased signal can be deter-mined easily. This is an obvious advantage whencomparing CF to PW Doppler. Because the averag-ing process loses valuable spectral data, CF Doppleris useful for detection of abnormal flows and thedirection and spatial extent of these flows. Reliabledetermination of peak velocities requires PW or CWDoppler spectral analysis.
Fig. 3.15 This color compare image shows thetwo-dimensional (2-D) image on the left and thecolor-flow Doppler image on the right. There is acentral jet of mitral regurgitation that is severe.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 64 — #23
64 Chapter 3
0%20%
60%
A
B
50% accuracy 94% accuracy
Fig. 3.16 The angle of interrogation has a great impacton the accuracy of Doppler measurement. (FromObeid AI. Echocardiography in Clinical Practice.Philadelphia: Lippincott Williams & Wilkins, 1992,with permission.)
Doppler spectra measurementsAs discussed previously, Doppler spectra representobject velocity data over time. Velocities toward thetransducer are presented above the zero velocityline or baseline and are assigned positive values.Velocities away from the transducer are presentedbelow the zero line or baseline and are assignednegative values. Accurate Doppler measurementsare dependent on the Doppler beam being paral-lel (or within 20 of parallel) to the interrogatedflow (Fig. 3.16). Several important Doppler spectrameasurements are discussed below.
Pressure gradientsA velocity measurement (m/s) can be converted toa pressure gradient (mmHg) using a modificationof the Bernoulli equation 4V 2 where V = velocityin meters per second. Peak instantaneous pressuregradients are determined by identifying the peakvelocity (Max V ) of the desired Doppler spectraand using the equation 4V 2. In practice, machinesoftware will calculate the peak pressure gradientusing a peak velocity identified by the operator (seeFig. 3.14). Peak instantaneous gradients are alwaysgreater than the peak-to-peak gradients determinedat catheterization.
Velocity–time integralVelocity–time integral (VTI) is determined by trac-ing (planimetry) the entire Doppler spectra over the
desired portion of the cardiac cycle (systole or dias-tole). Machine software integrates the area underthe traced spectra to determine VTI in centimeters.VTI can be used to determine themean gradient, thestroke volume, and orifice area using the continuityequation.Mean velocity (cm/s) is determined by the
machine software by dividing the VTI (cm) by theduration of flow (seconds). Mean velocity cannotbe used to calculate the mean gradient becausethe mean gradient is actually the average of mul-tiple instantaneous gradients within the VTI trace.Machine software determines, totals, and averagesthese individual pressure gradients to determine themean gradient.Stroke volume and cardiac output are determined
using the VTI as follows. The VTI can be used todetermine stroke volume (cm3) by multiplying theVTI (cm) obtained at a given location by the areaof the location (cm2). Cardiac output is then strokevolumemultiplied by heart rate (HR). This determi-nation can be done in the main pulmonary artery,in the right ventricular outflow tract (RVOT), at themitral valve annulus, in the left ventricular outflowtract (LVOT), or at the level of the aortic valve. Thefeasibility depends on two factors:• obtaining a Doppler spectra from the desired areawith the Doppler beam within 20 of parallel toblood flow, and• obtaining an accurate measure of the area fromwhich the Doppler sample was obtained.Diameter (D) is easilymeasuredwith ultrasound canbe converted to area using the equation:
Area = π(r)2 = π(D/2)2 = 0.785(D)2
Alternatively, a direct measurement of area can beobtained using planimetry.The continuity equation makes use of the VTI
to calculate valve areas. The conservation of massdemands that a stroke volume remain equal imme-diately upstream and downstream of a stenoticvalve. Although the velocities may be different, themass of ejected blood must be the same. Thus,
(A1)× (VTII) = (A2)× (VTI2)
where A1, area of region 1; A2, area of region 2;VTI1, VTI from area 1; VTI2, VTI from area 2.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 65 — #24
Monitoring 65
The concept can be extended to state that theflows across all valves in the heart must be equal,but this is true only in the absence of regurgitantlesions or shunts. Thus, in theory, the continuityequation could be used to determine aortic valvearea using mitral valve or pulmonary artery flowsor vice versa.
Deceleration time, acceleration time,pressure half-timeDeceleration time (D1) is the time it takes (ms)for the peak velocity of a Doppler spectra to fallto the zero baseline (Fig. 3.17). In instances inwhich the zero baseline is not reached, the natu-ral slope of the Doppler spectra is extended to thebaseline.The acceleration time (A1) is the time it takes (ms)
for the Doppler spectra to reach peak velocity fromthe zero baseline.The pressure half-time (PHT) is the time it takes
(ms) for the peak velocity gradient of a Dopplerspectra to decrease by one-half. In other words, itis the time it takes for the peak velocity to declineto the peak velocity divided by
√2. In addition, the
PHT (ms) is always 0.29 × DT. The PHT is impor-tant because it can be used to calculate mitral valvearea (MVA) over a wide range of values using theformula: MVA = 220/PHT.
TEE probesTEE probes consist of an echocardiographic trans-ducer or combination of transducers fitted to thedistal, flexible end of a gastroscope. The trans-ducer consists of an array of piezoelectric crys-tals. Most current adult TEE transducers have a64-crystal element, whereas pediatric probes havea 48-crystal element. Adult TEE transducers gen-erally operate at 5MHz, whereas pediatric probesoperate at 7.5MHz. Some adult TEE probes pos-sess frequency agility or the ability to functionat 3.7 and 5MHz, whereas some pediatric probescan function at 7.5 and 5.5MHz. The higher fre-quency transducers can be used without significantsignal attenuation because of the proximity of thetransducer to the heart. TEE probes allow 2-D,M-mode, PWDoppler, CWDoppler, andCFDopplerimagining.Hand controls allow flexion of the transducer
both side to side and anterior and posterior. Thesecontrols allow 70 of lateral mobility in each direc-tion (right and left) and 90 of anteflexion andretroflexion (Fig. 3.18). Presently, there are single-plane, biplane, and multiplane adult TEE probesavailable. Pediatric single plane and biplane probescan be used for neonates and infants as small as2–3 kg. With care, adult probes can be used forchildren as small as 15–20 kg.
Fig. 3.17 Schematic of a CW Dopplerspectra across a stenotic mitral valve. Thevelocity–time integral (VTI) is the shadedarea inside the spectra. The valuescalculated from the VTI are shown in theupper left hand corner. The decelerationtime is obtained by extending the slope ofthe spectra to the zero baseline. Thepressure half time (PHT) can bedetermined by calculating V2 andmeasuring the time between V1 and V2.The values calculated from the DT areshown in the bottom right corner. DT,deceleration time; MVA, mitral valve area.(From DiNardo JA. Monitoring. In:DiNardo JA (ed). Anesthesia for CardiacSurgery, 2nd edn. Stamford, CT:Appleton & Lange, 1998:37–80, withpermission.)
Max V = 250 cm/sMean V = 185 cm/sVTI = 200 cmMax PG = 25 mmHgMean PG = 13.7 mmHg
DT
DT = 600 msPHT = 174 msMVA = 1.26 cm2
PHT0
−100
− 200
−300
V2
V1

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 66 — #25
66 Chapter 3
Turn tothe left
Advance
Turn tothe right
Withdraw
Anterior Posterior
Anteflex Retroflex
Right Left
Flex tothe left
Flex tothe right
0°
90°
180°
Rotateforward
Rotateback
Fig. 3.18 Movement of the transesophagealechocardiography (TEE) probe allows extensivesectioning and imaging of the heart in a two-dimensional(2-D) plane. (From Shanewise JS, Cheung AT,Aronson S, et al. Anesth Analg 1999;89:870–84, withpermission.)
Single-plane probes have a single transducer thattransmits and receives ultrasonic signals in the0 plane (transverse or horizontal plane). Biplaneprobes have two transducers mounted one abovethe other. One transducer transmits and receivesultrasonic signals in the 0 plane and the othertransmits and receives ultrasonic signals in the 90(longitudinal or sagittal) plane. Changing planesrequires switching fromone transducer to the other.Because the transducers are at different levels, sub-tle (1.0–1.5 cm) advancement or withdrawal of theprobe is necessary after transducers are switchedto ensure imaging at the same anatomic level.Multiplane (omniplane) probes have the ability totransmit and receive ultrasonic signals in any planefrom 0 to 180. These probes use either mechan-ical rotation or phased-array activation (varyingsequential activation of the piezoelectric crystals inthe transducer) of a single transducer to accomplish
this. Activation of multiplane capability is obtainedwith a switch on the handle of the probe.
Insertion of the TEE probeInsertion of the TEE probe in the anesthetized adultor pediatric patient with an endotracheal tube (ET)in place is usually easy. The patient should have anorogastric tube placed and the stomach should beemptied as well as possible. Even a small volumeof air in the stomach can interfere with imagingfrom the transgastric position. The orogastric tubeshould be removed before probe insertion. Thepresence of a tube in the esophagus will interferewith imaging. The endotracheal tube should be wellsecured. The TEE probe is left in the unlocked posi-tion and is lubricated with ultrasonic gel. A biteblock is essential for TEE examinations in nonanes-thetized patients, but in anesthetized patients it isonly required in patients with jagged teeth or at theoperator’s discretion.The operator stands in the same position as if
to perform direct laryngoscopy. The patient’s headand neck should be in a neutral position. Thereshould be no positioning rolls under the patient’sshoulders. The thumb of the left hand is placedon the patient’s tongue and the left hand is usedto pull the jaw upward. The right hand is used toinsert the probe into the pharynx to the left sideof the ET with the probe transducer facing ante-rior. The remainder of the probe can be loopedaround the operator’s neck and shoulder, held byan assistant, or rested on the head of the bed nearthe patient. The probe is advanced with steadygentle pressure using a slight left to right rotatingmotion. The unlocked probe will follow the naturalcurve of the pharynx. At the pharyngeal-esophagealjunction (10 cm from the lips in neonates, 20 cmfrom the lips in adults), some mild resistance willcharacteristically be met. This can be overcomewith gentle, steady pressure. If undue resistance isencountered, it is possible that the probe is in thepiraform sinus or the vallecula. It should be with-drawn and advancement tried again. If there is anydoubt regarding probe position, the probe should beplaced under direct vision using a laryngoscope. Insome rare instances, it is impossible to place the TEEprobe.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 67 — #26
Monitoring 67
TEE viewsThe American Society of Echocardiography andthe Society of Cardiovascular Anesthesiologistsrecommended views for a comprehensive TEEexamination are shown in Fig. 3.19.Views available with a single-plane probe are
those obtained in the 0 plane. The basic viewsavailable with a biplane probe are those obtained
in both the transverse (0) and longitudinal (90)planes. Multiplane views are all of the viewsfrom 0 to 180. In fact, most of the viewsobtainable with a multiplane probe are obtain-able with a biplane probe. The difference isthat use of a biplane probe requires significantlymore probe manipulation than a multiplane probe.The following is useful when using a biplane
ME four chamber
(a) (b) (c) (d)
(e) (f) (g) (h)
(i) (j) (k) (l)
(m) (n) (o) (p)
(q) (r) (s) (t)
TG two chamber
ME AV LAX
ME RV inflow–outflow
desc aortic SAX desc aortic LAX UE aortic arch LAX UE aortic arch SAX
TG RV inflow ME asc aortic SAX ME asc aortic LAX
TG LAX deep TG LAX ME bicaval
TG basal SAX ME mitral commissural ME AV SAX
ME two chamber ME LAX TG mid SAX
Fig. 3.19 The 20 recommended views for a comprehensive transesophageal echocardiography (TEE) examination bythe American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. (From Shanewise JS,Cheung AT, Aronson S, et al. Anesth Analg 1999;89:870–84, with permission.)

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 68 — #27
68 Chapter 3
probe:• Angles 0–45: flex the transverse probe to thepatient’s left.• Angles 45–90: flex the longitudinal probe to thepatient’s right.• Angles 90–135: flex the longitudinal probe to thepatient’s left.• Angles 135–180: flex the transverse probe to thepatient’s right.In this text, rotation to the right always meansto the patient’s right (clockwise) and rotationto the left always means to the patient’s left(counterclockwise).Figure 3.20 shows views from the upper esopha-
gus. At this level, there can be interference from airin the right and left main stem bronchi. Good viewsof the proximal ascending aorta can be obtained.The view at 0 is useful for Doppler interrogation ofthe main pulmonary artery. For some patients, thepulmonic valve and a small portion of the RVOT canbe seen as well.CF Doppler interrogation just above this level but
at a level just below the aortic arch is useful for
0°RPA
SVCLPA
MPA
RPA LPA
MPA
LA
RA AoAo
30–40°
90–110°110–120°
Ao
Ao
RA
RV
Fig. 3.20 Transesophageal echocardiography (TEE)views at the base of the heart. Ao, aorta; LA, left atrium;LPA, left pulmonary artery; MPA, main pulmonaryartery; RA, right atrium; RPA, right pulmonary artery;SVC, superior vena cava. (From DiNardo JA. Monitoring.In: DiNardo JA (ed). Anesthesia for Cardiac Surgery,2nd edn. Stamford, CT: Appleton & Lange, 1998:37–80,with permission.)
detection of a patent ductus arteriosus (PDA). Gen-tle anteflexionmay be necessary to get good contactwith the esophagus at this level.Figure 3.21 shows views obtained with slight
advancement of the probe from the previous level.This level provides excellent views of the pulmonaryveins and allows Doppler interrogation. At 0 theleft lower pulmonary vein (LLPV) is lateral to andseen at a slightly deeper level (10–50mm) thanthe left upper pulmonary vein (LUPV). The LLPVusually is seen in conjunction with the descendingaorta. At 0, the right lower pulmonary vein is pos-terior to and at a slightly deeper level (10–50mm)than the right upper pulmonary vein (RUPV). TheRUPV is seen in conjunction with the superior venacava (SVC). The LUPV and LLPV usually can beseen in the same image at 100–110 while theRUPV and RLPV can usually be seen in the sameimage at 50–60. A persistent left superior venacava would appear as a vascular structure (circularin the sulcus between the left atrial appendage andthe LUPV).Figure 3.22 shows views obtained at a slightly
deeper level in the upper esophagus. Some of themost valuable views are obtained at this level. Bothlong- and short-axis views of the aortic valve areseen. In the short-axis views, the right coronarycusp is anterior, the noncoronary cusp is next to theright atrium, and the left coronary cusp is next to theleft atrial appendage (LAA). In the long-axis views,two cusps are seen: the right coronary cusp is ante-rior and the noncoronary cusp is in continuity withthe anterior mitral valve leaflet. A good long-axisview of the main pulmonary artery and two leafletsof the pulmonic valve are seen. Views of the tricus-pid valve suitable for Doppler interrogation are seenas well.Figure 3.23 shows views obtained at the mid-
esophageal level. Varying amounts of retroflexionare needed to prevent foreshortening of the leftventricle (LV) and right ventricle (RV). The clas-sic four-chamber view is seen at 0. These viewsallow good alignment for Doppler interrogation ofthe mitral valve. The anterior mitral valve leafletis seen in continuity with the ventricular septumat 0 and in continuity with the noncoronary cuspof the aortic valve at 130–150. The LAA also

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 69 — #28
Monitoring 69
Fig. 3.21 Transesophagealechocardiography (TEE) views of thepulmonary veins at the base of the heart.Ao, aorta; LA, left atrium; LAA, left atrialappendage; LLPV, left lower pulmonaryvein; LPA, left pulmonary artery; LUPV, leftupper pulmonary vein; MPA, mainpulmonary artery; RA, right atrium;RLPV, right lower pulmonary vein;RPA, right pulmonary artery; RUPV, rightupper pulmonary vein; SVC, superiorvena cava. (From DiNardo JA. Monitoring.In: DiNardo JA (ed). Anesthesia for CardiacSurgery, 2nd edn. Stamford, CT: Appleton &Lange, 1998:37–80, with permission.)
0° 0–30°
0–30°
100–110°
LA LPALUPVLLPV
LLPVLA
LA
AoPA
LAA
LUPV
RV
LV
35–40°
70–80°
RLPV
RUPV
RLPV
RUPVLA
SVC
RLPVSVC LA
Ao
Ao
RA
PA
RUPV
Fig. 3.22 Transesophagealechocardiography (TEE) views obtainedfrom the upper esophagus. Ao, aorta;AV, aortic valve; LA, left atrium; LV, leftventricle; MV, mitral valve; PA, pulmonaryartery; PV, pulmonic valve; RA, rightatrium; RV, right ventricle. (FromDiNardo JA. Monitoring. In: DiNardo JA(ed). Anesthesia for Cardiac Surgery, 2nd edn.Stamford, CT: Appleton & Lange,1998:37–80, with permission.)
130–150°
110°
90–100°LA
RA
RVPV
MV
Ao
LA
Ao
RV
40–60°
0–30°
60–75°
AV
RA
RV PA
LA
RA
LA
RV
LV
LALAA
AVRV
RV
is seen. Slight withdrawal and anteflexion will givea short-axis view of the aorta. The coronary arter-ies can be seen at this level. The left coronaryartery often can be seen dividing into the left ante-rior descending (LAD) and circumflex branches inthe area near the LAA. The right coronary arteryis anterior and usually requires very slight probeadvancement to be seen. Slight off angles (20–30)often will allow better visualization.Figure 3.24 shows views also obtained at the
midesophageal level. The probe is rotated tothe patient’s right to obtain these views fromthe previous angles. These views provide excellentvisualization of the atrial septum, which makesthem useful for detection of a patent foramen ovale
or atrial septal defect. Good visualization of the rightatrium/superior vena cava and right atrium/inferiorvena cava (IVC) junctions also is obtained.Figure 3.25 shows views obtained at the gas-
troesophageal junction (36–38 cm from the teeth).Gentle anteflexion usually is needed to obtain theseviews. The coronary sinus (CS) is seen entering theright atrium. A large CS should alert one to thepossibility of a persistent left superior vena cavaor anomalous pulmonary venous return. The rightatrium/inferior vena cava junction and eustachianvalve are seen as is the right atrial appendage.Figure 3.26 shows transgastric views of the left
heart structures. Varying degrees of anteflexion arerequired to obtain these views. These provide the

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 70 — #29
70 Chapter 3
130–150°
30–60°
0°
90°
LV LV
LV
LV
LARA
RV
LALAAAo
RV
Fig. 3.23 Transesophageal echocardiography (TEE)views obtained from the mid-esophagus. Ao, aorta; LA,left atrium; LAA, left atrial appendage; LV, left ventricle;PA, pulmonary artery; RA, right atrium; RV, rightventricle. (From DiNardo JA. Monitoring. In: DiNardo JA(ed). Anesthesia for Cardiac Surgery, 2nd edn. Stamford, CT:Appleton & Lange, 1998:37–80, with permission.)
115–130° 90°
30°
0°
IVCLA LA
LA
LA
IVC
RA RA
RA
RA
IAS
Ao
Ao
SVC
Fig. 3.24 Transesophageal echocardiography (TEE)views obtained from the mid esophagus. Ao, aorta; IAS,interatrial septum; IVC, inferior vena cava; LA, leftatrium; RA, right atrium; SVC, superior vena cava. (FromDiNardo JA. Monitoring. In: DiNardo JA (ed). Anesthesiafor Cardiac Surgery, 2nd edn. Stamford, CT: Appleton &Lange, 1998:37–80, with permission.)
0°
50°
90°110° LA
RA
RV
RAARA
IVC
CSRA
RV
LA
Ao
Ao
RA
RV
LV
Fig. 3.25 Transesophageal echocardiography (TEE)views obtained at the gastroesophageal junction.Ao, aorta; CS, coronary sinus; IVC, inferior vena cava;LA, left atrium; LV, left ventricle; RA, right atrium; RAA,right atrial appendage; RV, right ventricle; SVC, superiorvena cava. (From DiNardo JA. Monitoring. In:DiNardo JA (ed). Anesthesia for Cardiac Surgery, 2nd edn.Stamford, CT: Appleton & Lange, 1998:37–80, withpermission.)
0° 120° 90°
40–60°
0–30°
RV
MMVMV LVLV
AoAo
LALALA
LV
LV
RV
LAA
MV
RV
LA
Ao
Fig. 3.26 Transesophageal echocardiography (TEE)views at the transgastric position. Ao, aorta; IVC, inferiorvena cava; LA, left atrium; LAA, left atrial appendage;LV, left ventricle; MV, mitral valve; RA, right atrium;RV, right ventricle; SVC, superior vena cava. (FromDiNardo JA. Monitoring. In: DiNardo JA (ed). Anesthesiafor Cardiac Surgery, 2nd edn. Stamford, CT: Appleton &Lange, 1998:37–80, with permission.)

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 71 — #30
Monitoring 71
0°
30°
90–100°110–130°
RVRVRA
RV
TVSVC
AoAoPAPA
RV
AoPA
TVAo
RVLV
Fig. 3.27 Transesophageal echocardiography (TEE)views of the right ventricle from the transgastric position.Ao, aorta; IVC, inferior vena cava; LV, left ventricle;PA, pulmonary artery; RA, right atrium; RV, rightventricle; SVC, superior vena cava; TV, tricuspid valve.(From DiNardo JA. Monitoring. In: DiNardo JA (ed).Anesthesia for Cardiac Surgery, 2nd edn. Stamford, CT:Appleton & Lange, 1998:37–80, with permission.)
short-axis views of the LV and RV used in regionalwall motion analysis. The anterior and posteriorpapillary muscles are seen. With manipulation, theview at or around 1200 can provide views of theLVOT and aortic valve amenable to Doppler interro-gation. A short-axis view of themitral valve suitablefor planimetry often is obtainable either by with-drawing the probe slightly or ante-flexing it to agreater degree.Figure 3.27 shows transgastric views of the right
heart structures. Varying degrees of anteflexion arerequired to obtain these views. They are obtained byrightward rotation of the probe from the previousposition. These views provide excellent visualiza-tion of the RVOT, which is very useful in thecongenital heart disease patient. They also providegood visualization of wall motion in the RV inferiorwall and free wall.Figure 3.28 shows the deep transgastric views.
These views are obtained by passing the probe ina neutral position all the way into the stomach.At this point, the probe is maximally flexed andwithdrawn until contact is made and resistance is
0°
120–140°
0°
RVLV
AV
AoRA
RARA
RVLV
PAPA
TVSVC
AoAoPAPA
RA
PA
AoPA
Fig. 3.28 Transesophageal echocardiography (TEE)views from the deep transgastric position. Ao, aorta;IVC, inferior vena cava; LA, left atrium; LV, left ventricle;PA, pulmonary artery; RA, right atrium; RV, rightventricle; SVC, superior vena cava. (From DiNardo JA.Monitoring. In: DiNardo JA (ed). Anesthesia for CardiacSurgery, 2nd edn. Stamford, CT: Appleton & Lange,1998:37–80, with permission.)
felt. Flexion of the probe to the left and rotation tothe patient’s right helps align the image so that theLVOT, aortic valve, and proximal ascending aortaare vertical. This location reliably provides views ofthe LVOT and aortic valve and of the RVOT and pul-monary valve amenable to Doppler interrogation.These views also provide images equivalent to thethose obtainable with subcostal transthoracic imag-ing which are valuable in children with congenitalheart lesions.Figure 3.29 shows the probe set in the transverse
plane and positioned as depicted in Fig. 3.23. Next,the probe is rotated 90–100 to the patient’s left andthe descending thoracic aorta is visualized. Once it islocated, it can be viewed from the arch (see below)to just below the diaphragm. Inability to see thedescending aorta to the left should arouse suspicionthat there is a right aortic arch. This can be localizedby rotating the probe to the patient’s right from theoriginal position.Figure 3.30 shows, with the descending tho-
racic aorta visualized, the probe being withdrawn,keeping the image of the aorta in the center of

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 72 — #31
72 Chapter 3
0–30°
30–60°
80–110°
Fig. 3.29 Transesophageal echocardiography (TEE)views of the descending thoracic aorta. (FromDiNardo JA. Monitoring. In: DiNardo JA (ed). Anesthesiafor Cardiac Surgery, 2nd edn. Stamford, CT: Appleton &Lange, 1998:37–80, with permission.)
0–30°
90°
90°
LCA
LSCA
Ao arch
Fig. 3.30 Transesophageal echocardiography (TEE)views of the aortic arch. Ao, aorta; LCA, left carotidartery; LSCA, left subclavian artery. (From DiNardo JA.Monitoring. In: DiNardo JA (ed). Anesthesia for CardiacSurgery, 2nd edn. Stamford, CT: Appleton & Lange,1998:37–80, with permission.)
the screen. As the arch is approached in the upperesophagus, the probe is rotated slightly to thepatient’s right. At this point, the inferior portion ofthe aortic arch is seen. At 90, a short-axis view ofthe arch is obtained. With slight further withdrawaland rotation to the patient’s right, the left CA canbe seen. With rotation to the left, the left subclavianartery can be seen curving off inferiorly.
TEE examinationThere is no one way to conduct a comprehensiveTEE examination. Each examiner has a particularprotocol. What is important is that the examinerconducts the same examination on every patientin a consistent format. This is the only way toavoid missing what may turn out to be critical find-ings. The examiner should concentrate on knowndiseases, but not to the exclusion of a completeexamination. This should include complete 2-Dimaging with a comprehensive Doppler examina-tion. When the TEE probe is not being used, itshould be left in the unlocked position and theimage should be frozen. Freezing the image will ter-minate ultrasound transmission. Some examinersadvocate advancing the probe to the stomach whenit is not being used to prevent undue pressure onthe esophagus from the probe tip.
LV systolic function, ejection fraction,and preloadOne of the most powerful applications of periop-erative TEE is the quick assessment of LV systolicfunction and regional wall motion abnormalities.LV systolic function can be determined by grossobservation or it can be calculated using severaldifferent parameters.Intraoperative changes in the shape and posi-
tion of the LV pressure–volume relationship makethe traditional pressure measurements used toassess LV preload unreliable, whereas hemody-namic assessment of LV ejection fraction is not pos-sible. Both qualitative and quantitative assessmentof LV end-diastolic area (EDA), end-systolic area(ESA), and fractional area change (FAC) are possibleusing TEE.Quantitative assessment of EDA using TEE pro-
vides an accurate assessment of preload in adults

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 73 — #32
Monitoring 73
and children. Quantitative assessment of LV EDA isfrequently performed using the short-axis view ofthe LV at the mid-papillary muscle level, althoughthe most accurate assessments are derived from acombination of several views. EDA is determinedby one of two ways:1 Computer planimetry – this method requiresfreezing the LV end-diastolic TEE image and trac-ing the endocardial border using a trackball. Thecomputer then calculates EDA. The short-axis EDAfor several cardiac cycles are obtained and averaged.This method also can be used to determine ESAusing the frozen end-systolic echocardiographicimage. ESA and EDA can be used for the FAC,whichis analogous to EF.
FAC% = (EDA − ESA)/EDA × 1002 Automated border detection (ABD) – also calledacoustic quantification (AQ), this method makesuse of backscattered signals from the blood–tissueinterface to outline the endocardial borders in realtime. When the data are gated to the ECG, a beat-to-beat display of EDA, ESA, and FAC is provided.Both methods can be performed online, but obvi-ously, the first method is more time consuming andis not a continuous real-time assessment. ABD is acontinuous real-time assessment but is cumbersomeand, for 20–30%of patients, is unreliable because ofpoor image quality. FAC obtained by both methodshas been shown to correlate well with EF obtainedby radionuclide angiography.Qualitative assessment of EDA, ESA, and FAC
requires no special techniques except a trained eye.In practice, clinicians must often make quick judg-ments for treatment plans based on limited informa-tion. TEE allows the ability for clinicians to quicklylook at the heart and determine if it is hypokinetic,normal or empty and hyperdynamic is invaluable. Itis quick and can be as continuous as desired. Severalcautions are in order, however. The development ofend-systolic cavity obliteration commonly is usedas one of the visual signs of a reduced EDA. How-ever, it has been demonstrated that although manyof the episodes of end-systolic cavity obliterationare associated with reduced EDA, end-systolic cav-ity obliteration does not always indicate reducedEDA. End-systolic cavity obliterationmay be caused
by increases in contractility or decreases in after-load. The clinician may also be fooled if using onlyone view to render an opinion or form judgment.Remember that the TEE slice represents only a lim-ited view of the heart. One area may appear grosslyhypokinetic, while the remainder of the heart func-tions normally. With experience, clinicians canestimate FAC or ejection fraction area (EFA) towithin 10% of offline values in 75% of cases.The assessment of EDA as either low or normalcorresponds well with offline assessment of EDAas well.
Regional wall motion analysisTEE analysis of regional wall motion abnormalities(RWMA) can be used to detect myocardial ischemicand has predictive value concerning adverse clinicaloutcomes.Intraoperative assessment of RWMA involves
imaging the heart in several planes to view all ofthe 17 wall segments (Table 3.3). The most pop-ular view for general surveillance, perhaps, is thetransgastric short-axis view of the LV at the level ofthemid-papillarymuscle level. This view is obtainedeasily and contains regions of myocardium suppliedby all three coronary arteries. Most data regardingintraoperative use of TEE to monitor for ischemiauses this viewwith analysis that has been performedoffline. One should not forget to assess RV wallmotion. The RV is imaged in many planes includ-ing the RV inflow–outflow view, the four-chamberview, and the transgastric short axis view.Wall motion is graded both on excursion andwall
thickening. Excursion is defined as inward move-ment along an imaginary radius to the center of
Table 3.3 Left ventricular 17 segment anatomic model.
Base Mid Apex
Anterior Anterior AnteriorAnterio-lateral Anterio-lateral LateralInfero-lateral Infero-lateral InferiorInferior Inferior SeptalInfero-septal Infero-septal Apical capAnterio-septal Anterio-septal

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 74 — #33
74 Chapter 3
the ventricular cavity. Both assessments are neces-sary because it is possible for an infarcted segmentof myocardium to move passively by surround-ing areas of normal myocardium; however, theinfarcted myocardium will not thicken. By concen-trating on both excursion and thickening, it is pos-sible to account for the translation (lateral motionof the entire heart) and rotation of the echocar-diographic image during contraction. Wall motionis graded as follows: 1, normal; 2, hypokinetic;3, akinetic; and 4, dyskinetic.A new wall motion abnormality is defined when
the wall motion score changes two or more grades.The recognition of a new RWMA is more diffi-cult than it sounds, particularly in the presenceof a preexisting RWMA. Furthermore, recogni-tion of mild degrees of RWMAs are more diffi-cult than recognition of normal wall motion orsevere RWMA.
LV diastolic functionLV diastolic function is characterized using an inte-grated approach, involving analysis of the mitralinflow pattern, the pulmonary venous blood flowpattern and tissue Doppler. Diastole commenceswith isovolumic relaxation. As ventricular relax-ation continues, LV pressure falls. LAP eventuallyexceeds LV pressure and the mitral valve opens,allowing early (E) rapid filling of the LV. Next, aperiod of diastasis occurs as LA and LV pressureequilibrate. Finally, atrial contraction (A) occursand augments LV filling as diastole terminates. Allof these events are detectable with Doppler spectra.
Isovolumic relaxation timeIsovolumic relaxation time (IVRT) is the time fromaortic valve closure to the commencement of flowacross the mitral valve. IVRT can be detected byplacing the CW Doppler cursor across the mitralinflow and aortic outflow tracts. The time from theaortic valve closure click to the commencement ofmitral flow is the IVRT.
Mitral inflowMitral inflow can be assessed with the PW Dopplersample volume placed at the tips of the mitral
MitralNormal
S
D
S
SDD D
AC ACAC
RestrictionAbnormalrelaxation
“Pseudo-normalization”
Pulmonaryvein
Fig. 3.31 Schematic of the relationship between mitralinflow and pulmonary venous flow patterns. (FromDiNardo JA. Monitoring. In: DiNardo JA (ed). Anesthesiafor Cardiac Surgery, 2nd edn. Stamford, CT: Appleton &Lange, 1998:37–80, with permission.)
Table 3.4 Normal values for mitral inflow parametersas well as those encountered with impaired relaxationand restriction. (From DiNardo JA. Monitoring. In:DiNardo JA (ed). Anesthesia for Cardiac Surgery, 2nd edn.Stamford, CT: Appleton & Lange, 1998:37–80, withpermission.)
Abnormalrelaxation
Normal Restriction
DT >240ms 160–240ms <160ms
E ↓ 0.8–1.5M/s ↔↑A ↑ 0.75M/s ↓E/A E < A E > A (>1.0) E A
IVRT ↑ 55–90ms <70ms
leaflets. The spectra will contain E and A veloci-ties, which correspond to passive (E) and atrial (A)filling of the LV (Fig. 3.31). Normal values for theparameters derived from the spectra are shown inTable 3.4.
Pulmonary venous flowPulmonary venous flow is measured by placing thePW sample volume 1.0–2.0 cm into the pulmonaryvein from its junction at the left atrium. Typically,the LUPV or LLPV is used. A typical pulmonaryvein spectra is shown in Fig. 3.31. The systolic (S)velocity occurs as a result of LA filling during LV sys-tole, whereas the diastolic (D) velocity occurs as theresult of LA filling during LV diastole. There is flowreversal seen with atrial systole (A). The D velocityusually mirrors the E velocity of mitral inflow. TheS velocity often is seen to have an early (S1) and

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 75 — #34
Monitoring 75
late (S2) velocity with S1 < S2. S1 is the result ofLA relaxation, whereas S2 is the result ofmovementof the mitral annulus toward the LV apex during LVcontraction.
Abnormalities of LV diastolic functionThe range of LV diastolic abnormalities is summa-rized in Fig. 3.32. With impaired relaxation, theE velocity is reduced, the A velocity is increased,and the mitral DT and IVRT are increased. The pul-monary venous spectra mirror these changes with areduction in the velocity and an increase in theDT ofthe diastolic component (D) of pulmonary venousreturn. These changes all are a consequence of pro-longed ventricular filling during early diastole. Thispattern is very common in patients with coronaryartery disease and in patients with left ventricularhypertrophy.
Pseudonormalization occurs due to an eleva-tion in mean LAP. This normalizes the passivemitral filling, mitral DT, and IVRT by increasing thepressure gradient between the LA and LV andmasking the impaired relaxation. This pattern isdistinguished from the normal pattern by analysisof the pulmonary venous blood flow and the tis-sue Doppler pattern. The systolic component (S)of pulmonary venous return is reduced becauseof the elevated LAP. In addition, the flow reversalwith atrial contraction ismore prominent because ofenhanced atrial contraction in the expanded atriumand reduced ventricular compliance.Rapidmitral DT and IVRT characterize the restric-
tive pattern. In this pathology, ventricular fillingis restricted resulting in rapid equilibration of LAPand LV pressure. The velocity of early filling (E)is high because of an elevated LAP. There is little
Transmitralflow velocity
Pulmonary veinflow velocity
Mitral annularvelocity(lateral wall)
NormalE ≥ A
DT 140–220IVRT 60–100
NormalS ≥ D
Ar < 25 cm/s
NormalEM/AM> 1
EM> 8cm/s
Mild dysfunction(delayed
relaxation)EM ≤ 8cm/s
Moderatedysfunction
(pseudonormal)EM < 8cm/s
Severedysfunction(restrictive)EM 8 cm/s
Delayedrelaxation
S > DAr < 25 cm/s
PseudonormalS < D
Ar >25 cm/sLAP increased
RestrictiveS < D
Ar > 25 cm/sLAP increased
Delayedrelaxation
E < ADT>200
IVRT>100
PseudonormalE < A
DT 140–220LAP increased
RestrictiveE A
DT< 140IVRT < 60
Fig. 3.32 Transmitral Doppler imaging, pulmonary view Doppler imaging, and tissue Doppler imaging profilescorresponding to normal, delayed relaxation, pseudonormal, and restrictive filling patterns. (From Groban L,Dolinsky SY Chest 2005;128:3652–63, with permission.)

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 76 — #35
76 Chapter 3
contribution to LV filling from atrial contraction,and thus, atrial filling velocity (A) is low The pul-monary veins exhibit marked reduction of the sys-tolic component (S) of filling due the high LAP. Thevelocity of the diastolic component (D) is high as itcorresponds to the early filling (E) velocity acrossthe mitral valve. There is pronounced flow reversalwith atrial contraction because of enhanced atrialcontraction and minimal antegrade flow across themitral valve with atrial systole. This restrictive pat-tern is common in patients with dilated cardiomy-opathies and in patients with ventricular volumeoverload.Unfortunately, the velocity patterns are load
dependent, which can make application difficult.A normal pattern can be converted to an impairedrelaxation pattern with hypovolemia or afterloadincreases. Similarly, an impaired relaxation patterncan be pseudonormalized with volume expansion.
Tissue DopplerTissue Doppler is the application of a PW Doppler inthe annular ring of the mitral valve and samplingfor the velocity of the heart tissue during relax-ation. There are two measured components: theearly diastolic movement (E′) and the atrial con-traction component of ventricular filling (A′). TheE′ and A′ correspond to the mitral inflow velocitiesof E and A. An E′ less than 8 cm/s is abnormal andindicates diastolic dysfunction.Figure 3.33 provides an easy step-by-step
algorithm to determine the degree of diastolicdysfunction.
Right ventricular functionGlobal RV function is assessed using the same tech-niques as described for the LV to determine EDA,ESA, and FAC. This usually is performed in a short-axis view, the four-chamber view, and the transgas-tric view. This allows all five wall segments of theRV to be analyzed: inferior wall, septal wall, lateralwall, anterior wall, and anterior wall of the RVOT.Use of the biplane and multiplane probes allows along view of both the RV inflow and outflow tractsand of the RV inferior wall and anterior wall ofthe RVOT. This view is valuable for assessing RVsize and systolic function.
Valvular heart diseaseAll four heart valves are well visualized with TEE.Although most cardiac surgical patients will presentto the operating room with a complete diagnosticwork up of anatomic structure, a comprehensiveexamination is required in all patients when a TEE isperformed. Heart valve structure and function mustbe observed and documented. It is not uncommonto find new pathology or new information that willhelp steer the planned operative procedure. Thereare many excellent textbooks detailing the varioustechniques and anatomic findings seen with TEE.In this next section, disease of the mitral, aortic andtricuspid valve are briefly reviewed.
Mitral valveThe mitral valve separates the LV from the leftatrium, pulmonary circulation and entire right sideof the heart. The valve is bicuspid with an anteriorand posterior leaflet. The anterior leaflet is the largerof the two leaflets, accounting for two-thirds of thesurface area of the valve. The posterior leaflet wrapsaround the anterior leaflet, accounting for only one-third of the valve’s surface area and two-thirds ofthe annular circumference. The mitral annulus is afibrous ring surrounding the mitral valve. Duringventricular systole, the contraction of the papillarymuscles prevent mitral leaflet prolapse. Rupturedchordae are a common cause of mitral insufficiency.The Carpentier classification divides the three scal-lops of the posterior leaflet into P1, P2, and P3;and the anterior leaflet into the three segments A1,A2, and A3, which oppose the corresponding scal-lops of the posterior valve. The coaptation of A1/P1at the annulus form the anterolateral commissure.The coaptation of A3/P3 at the annulus form theposteromedial commissure.
Mitral stenosis (MS)Normal mitral valve areas range from 4–6 cm2,and symptomatic stenosis is seen when the valveapproaches 1.5 cm2. Rheumatic heart disease is acommon cause ofMS and it is characterized by com-missural fusion with doming of the valve leaflets.Leaflet tip thickening and chordae tendineae thick-ening, fusion, and calcification result in restricted

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 77 — #36
Monitoring 77
EF ≥ 45%
TDI
Impairedrelaxation
normal fillingpressures
Impairedrelaxation
normal fillingpressures
Dopplerpulmonary
vein
Valsalvaand
mitral inflow
Impairedrelaxation
increased fillingpressures
Impairedrelaxation
increased fillingpressures
Normaldiastolicfunction
Normaldiastolicfunction
Highsuspicion ofpericardial
disease
Restrictivemyocardial
disease
Valsalvaand
mitral inflow
Reversible,restrictive
Fixed,restrictivePseudonormal
And/or
Dopplerpulmonary
vein
Ar wave<25 cm/s
Normal Pseudonormal
Ar wave≥ 25 cm/s
Ar wave≥ 25 cm/s
Ar wave< 25 cm/s
Pseudonormal
TDI
To doDiagnosis
TDI
DT>140 msDT>140 ms DT< 140 ms
EM> 8 cm/sEM≤ 8 cm/s EM≤ 8 cm/s EM> 8 cm/s EM≤ 8 cm/s
Dopplermitral inflow
E > AE < A
E/EM≤ 8 8 ≤E/EM≤ 15 E/EM>15 E/EM≤8 8≤E/EM≤15 E/EM>15 E/EM<8 E/EM>15
E >AE < AE > A E A(unchanged)
E A
Fig. 3.33 An algorithm to determine the degree of diastolic dysfunction using transesophageal echocardiography(TEE). A, atrial peak velocity; Ar, retrograde velocity; E, early filling peak velocity; EM, early filling; TDI, tissueDoppler imaging. (From Groban L, Dolinski SY. Transechocardiographic evaluation of diastolic function. Chest2005;128:3652–63, with permission.)
leaflet motion. MS increases transvalvular pres-sure gradients leading to increased left atrial (LA)pressures and LA distention. Increased LA pres-sures can lead to pulmonary hypertension withright ventricular dysfunction and tricuspid regur-gitation. The left atrium will be enlarged and hypo-kinetic and may be filled with spontaneous contrast(swirling, smoke-like contrast). Spontaneous con-trast is indicative of a low flow state and is predictiveof subsequent development of left atrial thrombus.The left atrium should be examined carefully forthrombus, particularly in the left atrial appendage.If there is atrial fibrillation or flutter, the atriumwillappear akinetic.
Two-dimensional (2-D) anatomyTwo-dimensional imaging of the stenotic mitralvalve typically demonstrates thickening and fibro-sis of the mitral valve leaflets, restricted leafletmotion, and mitral annular calcification. The MVarea can be estimated directly with planimetry inthe transgastric basal short-axis view.
DopplerCW Doppler is used to determine the mean velocityand mean grade using the VTI. Because the meangradient can underestimate the severity of MS withlow cardiac outputs and overestimate the severityin the presence of mitral regurgitation, the valve

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 78 — #37
78 Chapter 3
Table 3.5 Severity estimation of mitral stenosis.
Grade Mild Moderate Severe
Mean gradient (mmHg) <6 6–10 >10
PHT (ms) 100 200 >300
DHT (ms) <500 500–700 >700
MVA (cm2) 1.6–2.0 1.0–1.5 <1.0
area should be determined. MVA can be calculatedusing the PHT method. The summary of mean gra-dients, PHT, deceleration time, and MVA in MS areseen in Table 3.5. Color flow Doppler can be used tocalculate valve area using the proximal isovolemicsurface area (PISA) equation. The PHTwill overesti-mateMVA (underestimate severity) in conditions inwhich LV pressure rises quickly in diastole, such asaortic insufficiency (AI) or reduced LV compliance.PHT is unreliable when there ismerging of the E andA waves or an alteration in the E wave decay pat-tern due to tachycardia, atrioventricular (AV) block,or atrial flutter. In these instances, the continuityequation using the MVVTI and the LVOTVTI andLVOTAREA can be used to calculate MVA assumingthere is no MR. Details of the use of LVOTVTI andLVOTAREA are explained in the section on aorticstenosis.
Mitral regurgitationMitral regurgitation is commonly seen in thecardiac surgical patient. There are a myriad ofcauses including has including myxomatous degen-eration, rheumatic disease, endocarditis, Marfansyndrome, infiltrative diseases (amyloid, sarcoid,mucopolysaccharidosis), collagen-vascular disor-ders (SLE, rheumatoid arthritis), papillary musclerupture or dysfunction (ischemia), and cardio-myopathies. General anesthesia, changing hemo-dynamic conditions and volume status greatly affectmeasured mitral regurgitation. It is important forthe echocardiographer to quantify the degree of MRunder physiologic conditions if possible. It may benecessary to use phenylephrine to elevate afterloadand attempt to duplicate preoperative conditions forpatients in whom the intraoperative assessment of
MR is significantly different from the preoperativeassessment.
Two-dimensional (2-D) anatomyMitral leaflet motion is well visualized with TEEand will direct the echocardiographer to the cor-rect diagnosis. There can be excessive leafletmotion,restricted leaflet motion, or normal leaflet motionwith poor coaptation. Excessive leaflet motion canbe classified as billowing, prolapse or flail. A billow-ing mitral leaflet demonstrates bowing of part ofthe mitral valve leaflet above the level of the mitralannulus. The leaflet edge, however, still coapts well,and there is no MR. Prolapse occurs when theleaflet edge extends above the level of the annulus.Flail leaflet occurs when the supporting structures,the papillary muscle or chordae tendinae rupture,allowing leaflet movement into the left atrium dur-ing systole. MR due to excessive leaflet motion willresult in a regurgitant jet directed away from theaffected valve leaflet. Conversely, MR caused byrestricted leaflet motion results in a regurgitant jetdirected towards the affected valve leaflet. SevereMR is associated with a dilated left atrium andelevated pulmonary pressure.
DopplerComprehensive quantitative evaluation of MRshould be performed intraoperatively. Color flow(CF) Doppler analysis of the regurgitant jet (seeFig. 3.15) is performed in combination with PWDoppler interrogation of the pulmonary veins. Thearea of the regurgitant jet relative to the area of theLA is a useful CF Doppler technique. This shouldbe performed in as many planes as possible to gaina good understanding of the extent of the MR. Itshould be performed at the level of the mitral valveusing a full 180 sweepwith amultiplane probe or atmultiple angles using a biplane probe. Table 3.6 listsseveral measures one can use to assess MR severity.Regurgitant jets, which hug the atrial wall
(Coanda effect), are considered constrained jets andwill be 30–40% smaller than a free jet (such as acentral jet) under the same conditions of regurgi-tation. Jets that exhibit the Coanda effect usuallyare associated with moderate to severe MR. When

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 79 — #38
Monitoring 79
Table 3.6 Grading of mitral regurgitation severity.
Method Mild Moderate Severe
Jet area (cm2) <3 3–6 >6
Vena contracta (cm) <0.3 0.3–0.55 >0.55
Regurgitant fraction (%) <30 30–50 >50
Mitral orifice area (cm2) <0.2 0.2–0.39 ≥0.4Regurgitant volume (mL) <30 30–59 ≥60Pulmonary vein flow Blunted S wave S wave < D wave Systolic reversal
the MR jet width at the mitral leaflet (vena con-tracta) is greater than 0.6 cm, MR usually is severe.Quantitative methods to classify MR exist, suchas regurgitant fraction calculations and proximalisovelocity surface area (PISA), but they generallyare cumbersome and time consuming.Technical factors such as CF Doppler gain and
Nyquist limit will affect the imaging of the regur-gitant jet. Proper technique calls for turning thecolor gain up all the way, then reduce it untilthe “sparkling” disappears, and starting with thevelocity scale peak at 50–60 cm/s. Both right andleft pulmonary veins should be examined becauseeccentric jets may reverse flow in the pulmonaryveins on only one side of the atrium.
The aortic valveThe aortic valve consists of three semilunar valvesnamed according to their relationship to the coro-nary arteries: the right coronary cusp, the leftcoronary cusp, and the noncoronary cusp. At thecenter of the free-edge of each cusp is a tiny, ele-vated nodule commonly referred to as the noduleof Arantius. The aortic valve complex is composedof the sinotubular junction, the sinuses of Valsalva,the valve cusps, the junction of the aortic valvewith the ventricular septum, and the anterior mitralvalve leaflet. All of these structures are imaged easilywith TEE.
Aortic stenosisAortic stenosis occurs when there is a fixed obstruc-tion to left ventricular ejection of blood into theaorta. Normal aortic valve area is 2.5–3.5 cm2.The severity of aortic stenosis is divided into
three categories by valve area as follows: mild(1.5–1.0 cm2), moderate (1.0–0.8 cm2), or severe(<0.8 cm2). The classic triad of syncope, angina andcongestive heart failure are associated with the latestages of aortic stenosis and are ominous signs attheir onset.
Two-dimensional (2-D) anatomyA number of views of the aortic valve are avail-able, but the short- and long-axis views of the aorticvalve are most useful. Leaflet mobility should beobserved. A stenotic valve will have limited openingandheavy calcificationmay be present in the leafletsand commissures. A bicuspid aortic valve can beidentified easily in a short-axis view. Unfortunately,2-D imaging is limited by the occasional inabilityto evaluate the stenotic valve in the correct plane,thereby underestimating the true area of valvularstenosis. Therefore, it is imperative to examine thevalve until the narrowest area of stenosis is iden-tifiable and the stenotic area is reproducible withmultiple measurements. A secondary sign of aorticstenosis is left ventricular hypertrophy.
DopplerSeverity can also be quantified using Doppler mea-surements of the peak and mean gradients and thecalculated aortic valve area. The mean gradient andpeak instantaneous gradient are determined withthe VTI obtained by using CW Doppler aligned par-allel (or within 20) to the LVOT, aortic valve, andproximal ascending aorta. If the peak aortic veloc-ity is greater than 4.5m/s, the aortic stenosis issevere. Either the peak or the mean aortic veloc-ity can be substituted into the simplified Bernoulli

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 80 — #39
80 Chapter 3
equation that is used to calculate the transvalvularpressure gradient. The simplifiedBernoulli equationfor the peak gradient is calculated with the follow-ing equation: Peak Gradient (mmHg) = 4 (AorticPeak Velocity)2. Based on the peak aortic gradientvalue, the severity of aortic stenosis is graded asmild(<36mmHg), moderate (>50mmHg), or severe(>80mmHg). The simplified Bernoulli equation forthe mean gradient is calculated with either of thefollowing equations: Mean Gradient (mmHg) =4 (Mean Velocity)2 or 2.4 (Vmax)2. The valueof the mean aortic velocity grades the severityof aortic stenosis as mild (<20mmHg), moderate(20–50mmHg), or severe (>50mmHg). Unfortu-nately, this technique is sometimes difficult becausethe deep transgastric long-axis view can be veryelusive even for an experienced echocardiographer.Remember that gradients will underestimate theseverity of the stenosis when output is low and mayoverestimate it when output is high. If there is suspi-cion that the gradient is misleading, the aortic valvearea should be calculated or the dimensionless index(DI) should be used:
DI = peak velocity LVOT/peak velocity AoV orLVOTVTI/AoVVTI.
A DI < 0.2 indicates severe aortic stenosis. Becausethe peak velocity in the LVOT and across the aor-tic valve will change proportionally, this index isindependent of cardiac output.Doppler information can be used to calculate the
aortic valve area using the continuity equation:AoVAREA = (LVOTAREA) × (LVOTVTI)/AoVVTI.The LVOT area is determined using the diame-ter method. The long-axis view of the aortic valvecan be used to measure the diameter at the pointat which the aortic valve cusps abut the LVOT.AoVVTI is obtainedwith CWDoppler across the aor-tic valve in systolewith the views used to obtain VTI.LVOTVTI is obtained with PW Doppler in the LVOTjust below the aortic valve leaflets in systole withthe views used to obtain VTI.
Aortic regurgitation (AR)TEE can identify the presence of regurgitation,quantify its severity, determine the etiology, and
examine the secondary effects on other heartstructures (i.e. left ventricle, mitral valve). In gen-eral, the etiology of aortic regurgitation is classi-fied into two major groups: leaflet abnormalitiesand aortic root abnormalities. Leaflet abnormalitiesinclude congenital bicuspid valves, calcific valve dis-ease, rheumatic valve disease, myxomatous valvedisease, endocarditis, and nonbacterial thromboticendocarditis. Aortic root abnormalities are the mostcommon cause of aortic regurgitation. Aortic rootabnormalities include annular dilatation, hyper-tensive aortic root dilation, cystic medial necrosis,Marfan syndrome, and aortic dissection.
Two-dimensional (2-D) anatomySimilar to the evaluation of aortic stenosis, 2-Dexamination of the aortic valve will yield informa-tion on the etiology and extent of aortic regurgi-tation. In severe AR there may be fluttering of theanterior mitral valve leaflet in diastole when the ARjet is directed along it. There may be enlargementof the ascending aorta and aortic root causing poorcoaptation of the aortic leaflets and AR. Retrogradeaortic dissection can cause mechanical deformationof the aortic valve annulus and AR. The AR maybe associated with vegetations and leaflet perfora-tion. The presence of AR may alter the manner inwhich cardioplegia is delivered as infusion into theaortic root may not be effective when moderate orsevere AR is present. The LV may exhibit eccentrichypertrophy.
DopplerCF Doppler imaging of the aortic valve in the longaxis is used to measure the minimum width of theregurgitant jet (usually at the origin of the jet at theleaflets) relative to the width of the LVOT. AR isgraded, based on this assessment, as follows:• Trace: jet area/LVOT width <0.25• Mild: jet area/LVOT width 0.25–0.46• Moderate: jet area/LVOT width 0.47–0.64• Severe: jet area/LVOT width >0.65CFDoppler imaging of the aortic valve in the short
axis at or just below the level of aortic valve leafletsis used to measure the regurgitant jet area relativeto the circular LVOT area at this level (Fig. 3.34).

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 81 — #40
Monitoring 81
Fig. 3.34 M-mode color Doppler image just below theaortic valve in the left ventricular outflow trackdemonstrating aortic regurgitation.
AR is graded, based on this assessment, as follows:• Trace: jet area/LVOT width <0.20• Mild: jet area/LVOT width 0.20–0.40• Moderate: jet area/LVOT width 0.40–0.60• Severe: jet area/LVOT width >0.60CWDoppler is useful for quantifying AR by deter-
mining the PHT of the regurgitant spectra. A PHT<300ms is indicative of severe AR; whereas, a PHT>800ms is associated with mild AR. This occursbecause, in severe AR, there is more rapid equili-bration between aortic and LV pressure in diastoleand thus a more rapid decay in the velocity of theregurgitant spectra. In severe AR, the CW Dopplerspectra will be dense, whereas in mild AR, it will befaint. CF Doppler will help guide positioning of theCW cursor.PW Doppler of the mitral inflow will reveal
a restrictive pattern in severe or acute AR. PWDoppler of the proximal descending thoracic aortawill reveal holodiastolic flow reversal in severe AR.It is impossible to align the Doppler beam parallel tothe descending aorta, but it still may be possible todetect diastolic flow reversal.
Tricuspid and pulmonic valvesThe tricuspid valve consists of anterior, posteriorand septal cusps tethered by chordae tendinae andpapillary muscles all suspended by a fibromuscularannulus. The commisures of the tricuspid valve are
Fig. 3.35 Pulse wave Doppler in the hepatic veinsof a patient with severe tricuspid regurgitation (TR).There is reversal of hepatic venous flow indicatingsevere TR.
not as well defined as those of the mitral valve. Theorifice is larger than that of the mitral valve andis triangular in shape, as compared to the saddle-shape of the mitral valve. The pulmonic valve isanterior and superior to the aortic valve. Similarto the aortic valve, it is trileaflet and semilunar,consisting of anterior, left and right leaflets. Theplane of the valve is roughly perpendicular in ori-entation to the aortic valve. The pulmonic valve isisolated from the other three heart valves by theinfundibulum.Insignificant tricuspid insufficiency is very com-
mon and is often seen in patients with transvenouspacemaker leads and/or PACs. Moderate to severetricuspid insufficiency is most frequently the resultof dilation of the right ventricle and the tricuspidannulus. Any condition resulting in elevated rightventricular pressure (>55mmHg) or right ventricu-lar dilation can cause tricuspid insufficiency. Com-mon causes observed in surgical patients includemyocardial ischemia, cor pulmonale, pulmonaryembolism, left heart failure, pulmonic valve steno-sis and pulmonary hypertension. Significant mitralinsufficiency is a common cause of right ventric-ular dilation and secondary tricuspid insufficiency.Reversal of flow in the hepatic veins is associatedwithmore severe tricuspid regurgitation (Fig. 3.35).Tricuspid stenosis is much less common than
tricuspid insufficiency. Rheumatic heart disease

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 82 — #41
82 Chapter 3
is the most common cause of tricuspid stenosisand results in thickened, immobile valve leafletswith commissural fusion. Diastolic doming of theleaflets is usually present. In these cases, the mitralvalve is usually also involved. Other causes oftricuspid stenosis, although rare, include congeni-tal anomalies, endocarditis, carcinoid heart diseaseand endomyocardial fibrosis. Tricuspid valve areais estimated by the pressure half-time method orplanimetry.Pulmonary insufficiency is commonly observed
in cardiac surgical patients, especially if a PAC isin place. Severe pulmonary insufficiency is alwayspathologic and usually the result of dilation ofthe main pulmonary artery as seen in patientswith pulmonary hypertension from any etiology.The causes of pulmonary insufficiency includefenfluramine–phentermine valvulopathy and car-cinoid syndrome. These lesions result in short andthickened valves which fail to properly coapt. Infec-tious endocarditis can affects the tricuspid andpulmonic valves and presents as mobile massesattached to the valve leaflets.Pulmonic stenosis is categorized as valvular, sub-
valvular, or peripheral (supravalvular). Ninety per-cent of the lesions are valvular in nature and themajority of pulmonary stenosis in the adult popu-lation is from untreated or recurrent congenital dis-ease, such as tetralogy of Fallot. Pulmonary stenosisis more commonly seen as individuals with complexcongenital heart disease increasingly survive intoadulthood. Pressure gradients using CW Doppleracross the stenotic valve allow the quantificationof pulmonary stenosis as follows: Peak gradients<30mmHg are associated with mild stenosis, peakgradients between 30 and 65mmHg indicate mod-erate stenosis, and gradients >65mmHg are seenwith severe pulmonary stenosis. The continuityequation can be used to determine the area of thepulmonary valve to further assess disease severity.
TEE after valve repair or replacementAfter any valvular surgery, the repair or replace-ment must be assessed for both regurgitation andstenosis. The presence of trace to mild MR after MVrepair does not confer increased morbidity or mor-tality. The valve should be evaluated for stenosis
Fig. 3.36 Zoom view of a perivalvular leak after a mitralvalve replacement. Transesophageal echocardiography(TEE) evaluation after all valve repair and replacementprocedures must include an examination forregurgitation, perivalvular leak, and gradients across thevalve.
either directly by planimetry or indirectly with thePHT method. Systolic anterior motion (SAM) lead-ing to LVOT obstruction should be evaluated. Dis-cussion of all types of prosthetic valves is beyondthe scope of this presentation. However, severalimportant points deserve discussion. All mechani-cal valves have some small quantity of regurgitantflow built into their design to prevent thrombus for-mation. This regurgitant flow is characterized by lowvelocity, small area, and locationwithin the annulusof the valve. If a leaflet is stuck in the open posi-tion, the amount of regurgitation present will belarge. Tissue valves are not regurgitant unless theyhave degenerated. Perivalvular leaks generally havea high velocity and are located at the outer marginof the annulus or sewing ring (Fig. 3.36).Prosthetic valves should have transvalvular gradi-
ents that are physiologic for the particular position.If the gradient across a prosthetic valve is high,an aggressive examination to determine whetherthe leaflets are opening is warranted. A leafletmay be stuck closed because of impingement onsurrounding tissue.
Removing air from the heartAll procedures in which the heart is openedhave potential to introduce air into the systemiccirculation. In addition, closed procedures have

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 83 — #42
Monitoring 83
the potential to introduce air because of the place-ment of vents to decompress the left side of theheart. TEE can detect intracardiac air and guide airevacuation before termination of CPB. Air is par-ticularly likely to be retained in the LV apex, leftatrium, right coronary sinus, and the pulmonaryveins, particularly the right upper pulmonary vein.
Estimation of intracardiac pressures
Peak pressure gradientsThis method requires the presence of a regurgitantvalve or a communication between cardiac cham-bers. It is based on the premise that the peak velocityof a regurgitant jet can be used to determine thepressure gradient between two cardiac chambersduring either systole or diastole. Peak velocity isconverted to the peak pressure gradient using 4V2.For example, if there is a TR jet with a peak
velocity of 3.0m/s, then a peak pressure gradientof 36mmHg exists between the RV and RA duringsystole because TR is a systolic event. If we measurethe central venous pressure (CVP) to be 10mmHg(or assume that it is 10mmHg), then RV systolicpressure must be 36+ 10 = 46mmHg. If we know(or assume) that there is no RVOT obstruction, thenPA systolic pressure is also 46mmHg.Pulmonary regurgitation (PR) Doppler spectra
can be used in the same way. The peak PR veloc-ity (velocity at the beginning of diastole) is usedto calculate the pressure difference between thepulmonary artery (PA) and the RV at the time ofpulmonary valve closure in diastole which gives agood estimate of mean PA pressure (PAP).Mean PAP = 4(peak PR velocity)2 + RV end-
diastolic pressure (EDP); RV EDP = CVP, whichagain is measured or assumed. If the PR velocityat the end of diastole is used, PA EDP can be calcu-lated. PA EDP = 4(end-diastolic PR velocity)2 +RVEDP; RV EDP = CVP, which again is measured orassumed.The same arguments can be used with MR and
AR velocities.
Movement of the atrial septumThe shape of the atrial septum is determined by theatrial pressure gradient. Normally, LAP is greater
than RAP and the atrial septum is bowed towardthe RA. During the passive, expiratory phase ofmechanical ventilation, there is a transient mid-systolic reversal of inter-atrial septum position withbowing of the atrial septum into the LA fromthe RA. This finding is highly predictive of apulmonary capillary wedge pressure (PCWP) lessthan 15mmHg. Conversely, absence of this find-ing is highly predictive of a PCWP greater than15mmHg.The observation of an atrial septum continuously
shifted to the left would predict elevated RAP.
Pulmonary and hepatic venous bloodflow velocitiesReductions in the systolic portion of the hepaticvenous Doppler spectra relative to the diastolicportion are strongly correlated with increases inRAP. In fact, progressive decreases in the ratioVTIsystolic/(VTIsystolic + VTIdiastolic) are associ-ated with increasing RAP. Similar observationshave been made regarding pulmonary venousDoppler spectra and PCWP and LAP. When LVEDP>15mmHg the flow duration of pulmonary versusatrial flow reversal is more than 30ms longer thanthe duration of the mitral A wave.
Thoracic aortaTEE is useful for examination of the ascending aorta,aortic arch, and descending thoracic aorta. The dis-tal ascending aorta and proximal aortic arch arepoorly visualized because of interposed interfer-ence from air in the trachea and/or left main stembronchus. Unfortunately, this area encompasses theregion in which the aortic cannula, aortic cross-clamp, and proximal ends of the saphenous veingrafts are typically placed. Because of the higherincidence of stroke seen in patients with atheromain the ascending and descending aorta undergoingundergo cardiac surgery with CPB, there is con-cern about manipulation of the aortic if it containsatheroma. Presently, only epiaortic scanning (place-ment of a transducer directly on the aorta) canreliably visualize this area.Atheromatous disease of the aorta is graded I
to V as follows: I, normal; II, extensive intimalthickening; III, sessile atheroma protruding <5mm

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 84 — #43
84 Chapter 3
Fig. 3.37 Moderate plaque in the descending aorta.Such an image may prompt an epiaortic examination ofthe ascending aorta.
Fig. 3.38 An epiaortic scan of the ascending aortareveals grade III atheromatous disease.
into the aorta; IV, sessile atheroma protruding>5mm into the aorta; and V, mobile atheroma(Figs 3.37 & 3.38).Observation of atheroma in the aorta should
prompt attention to placement of the aortic cannula.Although TEE can rarely be used to visualize thesite of aortic cannulation, it can be used to visualizethe jet out of the aortic cannula. This is accom-plished using CF Doppler in conjunction with a 2-Dimage of the aortic arch. The direction of the jetout of the aortic cannula is important because thejet can dislodge plaque. Misdirection of the cannulajet down the left subclavian artery or left CA also
can be detected using CF Doppler in conjunctionwith 2-D images of those vessels. TEE also is usedextensively to diagnosis aneurysm, dissection, anddisruption of the ascending aorta, aortic arch, anddescending aorta. Ultrasound artifacts are found in50–60% of patients and may result in misdiagnosis.There are two classes of artifacts: linear and mirrorimage. Linear artifacts occur in the ascending aortaand are the result of reflections from either the leftatrium (LA) or right pulmonary artery (RPA). Theycan be distinguished from intimal flaps because theydo not display rapid oscillatory motion, do not dis-rupt the CF Doppler flow pattern, are parallel tothe posterior aortic wall, have movement (best seenwith Mmode) parallel to that of the posterior aorticwall, and are located twice as far from the posteriorwall of the LA or RPA as from the posterior wall ofthe aorta. Mirror image artifacts occur in the archand descending aorta and give the appearance of adouble barrelled aorta. They are caused by reflec-tions from the lung–aorta interface. They can bedistinguished from intimal flaps or false lumens bythe double-barrelled mirror image appearance andby the lack of interruption of the CF Doppler flowpattern.
Congenital heart diseaseA comprehensive treatment of the use of TEE of thewide variety of congenital lesions the pediatric car-diac anesthesiologist is likely to encounter is beyondthe scope of this chapter. However, by becom-ing familiar with some basic principles, the readershould be able to begin conducting a good qualityexamination in patients with congenital heart dis-ease. With a biplane or multiplane probe, a compre-hensive 2-D and Doppler examination of the heart,including the LVOT and RVOT can be obtained.The LVOT and RVOT are not well-oriented forperformance of a Doppler examination with stan-dard single-plane imaging. If only a single-planeprobe is available, the deep transgastric position willallow visualization of the LVOT and RVOT and theventriculo-arterial connections. In some situations,deep transgastric imaging may provide superiordelineation of anatomy than biplane examination.From a practical point of view, deep transgastricimaging with a biplane probe is difficult and much

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 85 — #44
Monitoring 85
less satisfactory because the extra transducer ele-ment makes the distance from the tip of the probeto the flexion point longer. This makes good tis-sue contact difficult, particularly in small infants.The following issues should be addressed while per-forming an examination of a patientwith congenitalheart disease.
Atrial identity and locationIdentity of the atrial chamber by examining theappendage is helpful. The right atrial appendage(RAA) is best seen in the transverse plane atthe level demonstrated in Fig. 3.22. Flexion of theprobe will allow better visualization. The RAA hasa broad junction to the RA which is short andblunt (Snoopy’s nose). The LAA is seen in multi-ple views. The LAA has a narrow junction to theLA, it is long, narrow, and crenulated (Snoopy’sear). The IVC almost always returns to the RA;whereas, the return patterns of the SVC and pul-monary veins are much less reliable. The RA willhave a eustachian valve and the LA septal surfacehas the flap of the fossa ovalis. The atrial situs soli-tus is the normal condition: the RA on the right sideof the heart, LA on the left side of the heart. Atrialsitus inversus occurs when the RA is on the left sideof the heart, and the LA on the right side of theheart.
Ventricular size and identityA chamber is considered a ventricle if it receivesmore than 50% of the ventricular inlet or fibrousring of anAVvalve. TheAVvalve need not be patentfor the chamber to be considered a ventricle, as isthe case with tricuspid or mitral atresia. Likewise,the chamber does not need to be large to be consid-ered a ventricle, as is the case with hypoplastic leftheart syndrome. The right and left ventricles havedifferent morphologies:1 RV:a has the tricuspid valve (three leaflets) with onethe leaflets having a chordal attachment to theseptum; there are three papillary muscles that arelocated apically.b the septal leaflet of the tricuspid valve insertsslightly lower on the intraventricular septum thanthe anterior leaflet of the mitral valve.
c the RV has a triangular shape and a trabeculatedendocardial surface.d the RV has the moderator band, a band of tissuethat stretches from lower intraventricular septumto the anterior RV wall and is best seen in thefour-chamber view with retroflexion of the TEEprobe.2 LV:a has themitral valve (two leaflets) with no chordalattachment to the septum; there are two papillarymuscles that are located at the junction of the apicaland middle two-thirds of the chamber.b has an ellipsoidal shape and a smooth endocardialsurface.
Great vessel orientation and identityNormally, the great vessels are oriented at 45 toeach other when they leave the heart with the pul-monary artery (PA) anterior to the aorta. Whenthey are viewed with echocardiography, one vesselwill be observed in the short axis and the other willhave a sausage shape. This is seen in the transverseplane image.When the great vessels are transposed,they are oriented parallel to each other when theyleave the heart. When they are viewed by TEE,both vessels will be observed in the same axis. Therule of thumb when viewing transposed vessels inthe short axis is that the anterior vessel is invari-ably the aorta. When the vessels are aligned side toside, the determination is more difficult and usuallyrequires finding the arch of the aorta or the branchpulmonary arteries to make the determination.After the great vessels are identified, their rela-
tionship to the ventricles must be delineated. Thisrequires creativity in finding the views that allowthis to be seen. This is an instance in whichdeep transgastric views are useful, although biplaneimaging also works well.
Presence of intracardiac shunts andobstructive lesionsCF Doppler is indispensable in identifying intra-cardiac shunts, including those not seen with 2-Dimaging. CW Doppler is useful in determiningvelocities and gradients across restrictive commu-nications or valves, whereas PW Doppler assessesless restrictive orifices as well as hepatic and

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 86 — #45
86 Chapter 3
pulmonary venous blood flow. The RVOT mustbe examined carefully for both dynamic and fixedobstructive lesions. Two-dimensional echocardio-graphy in combination with Doppler will clearlydelineate dynamic obstructive lesions. The use ofCW Doppler to determine intracardiac pressures asdescribed previously is also valuable.
Evaluation of the surgical repairA comprehensive preoperative intraoperative studyis the foundation of repair assessment. This allowsthe operator to focus the examination on therepaired lesions. Look for the common things:1 Patch leaks. After ventricular septal defect (VSD)and atrial septal defect (ASD) repairs, detectionof residual VSD leaks can be more difficult thanit sounds, because the VSD patch produces areasof echo attenuation in the RV and RVOT thatmay mask leaks. The use of multiplane imagingimproves detection but does not completely resolvethis problem.2 Regurgitant valves. After valvuloplasty but alsoafter transvalvular approaches to the lesion (suchas approach to a VSD via the tricuspid valve).3 Stenotic anastomoses. Pulmonary vein anasto-mosis to LA in total anomalous pulmonary venousreturn (TAPVR). SVC to PA in bidirectional cavopul-monary connections (bidirectional Glenn) and totalcavopulmonary connections (Fontan). PW Dopplerinterrogation of these cavopulmonary connectionswill reveal a phasic venous blood flow pattern withrespiratory variation.4 Residual outflow tract gradients. After tetralogyof Fallot repairs and repair of subaortic membranes.5 Residual gradients across ASD or VSD left openin the course of a staged repair (tricuspid atresia,double outlet RV, hypoplastic left heart syndrome).6 Ventricular function assessment. After all repairs.Particular attention paid to patients with reim-planted coronary arteries such as vessel switch fortransposition of the great vessels or Ross procedure(transplantation of the pulmonic valve to the aorticposition and creation of an RV-to-PA conduit) andto patients who may have had air in the coronaryarteries during the surgical process.7 Patency of aortopulmonary shunts. CW Dopplerwill detect a high velocity signal with flow in systole
and diastole. CF Doppler will help position the CWDoppler beam.
Saline-contrast echocardiographySaline-contrast echocardiography is a techniquethat can be used to detect intracardiac shunting. Thebasis of the technique is opacification of the rightheart chambers using agitated saline injected rapidlyinto a catheter.Microbubble formation occurs as thesolution leaves the catheter orifice as dissolved gasescapes from solution. The presence of micro bub-bles in high concentrations opacifies the RA andRV. The amount of opacification with a properlyperformed procedure is impressive.Saline-contrast studies are used most commonly
in conjunction with a provocative maneuver todetect right-to-left flow patency of the foramenovale. Agitated saline is produced by vigorouslytransferring 10mL of saline with a small amountof air between two syringes connected by a stop-cock. Alternatively, 8mL of saline and 2mL of thepatient’s blood can be used. The agitated mixturecan be injected peripherally or centrally.Detection of the right-to-left flow patency of the
patent foramen ovale (PFO) is dependent on tran-siently increasingRAP above that of LAP. The easiestway to accomplish this is by applying a Valsalvamaneuver (actually sustained positive inspiratorypressure) during positive-pressure ventilation. Thistransiently impedes venous return to the right heartand subsequently to the left heart. Upon release ofthe Valsalva, the rapid increase in venous returnto the right heart will precede the increase in returnto the left heart and the result will be a transient ele-vation in RAP above that of LAP. The atrial septummust bow into the LA for the test to be effective. Thetest is accomplished by injecting the saline contrastduring the Valsalva maneuver. After opacificationof the RA occurs, the Valsalva is released and theTEE is observed for appearance of saline contrast inthe LA. Appearance of three or more microbubblesin the LA within three cardiac cycles is indicative ofa flow-patent PFO.
Intracardiac and endovascular cathetersTEE can be used in a wide variety of ways toimage intracardiac and endovascular catheters and

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 87 — #46
Monitoring 87
devices. A few of the most common and importantare summarized here:• Intra-aortic ballon pump (IABP). TEE views of thedescending thoracic aorta can and should be usedto document that the tip of the IABP is below thelevel of the aortic arch and the takeoff of the leftsubclavian artery. In addition, inflation and defla-tion can be observed, which may aid in detection ofa ruptured balloon.• Coronary sinus cannula for cardioplegia. The coro-nary sinus is easily seen in most patients and isobliterated when the catheter is placed properly.• Ventricular assist devices. The inflow and outflowcannulas to the devices can be seen and should bechecked to rule out obstruction.• Venous cannulas for CPB. Position in the IVC andSVC can be checked. In particular, the IVC cannulashould not impinge on any hepatic veins. Diffi-culty in placing an IVC cannula can be caused bya prominent eustachian valve.• PACs. The position of a PAC can be documentedby sequential views of the RA, RV, and PA. Thismayhave some use if catheter placement is difficult.
Contraindications and complicationsThe relative and absolute contraindications to useof a TEE probe are summarized below:• Relative:a Recent gastroesophageal operationb Esophageal variciesc Upper gastrointestinal bleedd Cervical disk diseasee Severe cervical arthritisf Unexplained dysphagia or odynophagia• Absolute:a Esophageal obstruction (stricture, neoplasm)b Esophageal fistula, laceration, or perforationc Esophageal diverticulumd Cervical spine instabilityA number of complications have been reported inassociation with use of TEE probes. Most complica-tions in adults involve trauma to the upper gastro-intestinal (GI) tract ranging from minor lacerationsto perforation of the esophagus. The incidence ofswallowing complications after cardiac surgery inadults having undergone intraoperative TEE alsomay be higher.
The complications reported in infants and chil-dren involve hemodynamic or respiratory compro-mise. Vigilance is required when using TEE probesin a small child, even with the availability of pedi-atric probes. Airway obstruction may occur dueto compression of the small trachea or bronchusbetween surrounding tissue and the rigid probe.Likewise, aortic or aortic arch vessel compressionmay occur.Prophylactic antibiotic coverage for patients
undergoing TEE examinations is debated because itcarries a risk of inducing bacteremia like any otherendoscopic procedure. Most patients undergoingcardiac surgery receive prophylactic antibiotics ofsome kind, and many consider this sufficientprophylaxis for endocarditis.
Coagulation monitoringBy necessity, cardiac anesthesiologists must befamiliar with coagulation monitoring. CPB requiresanticoagulation, and reversal of the anticoagulatedcondition. In addition, the patient is often proneto bleeding disorders wither through their pre-operative medication regimen, thrombocyptope-nia or the inflammatory response associated withsurgery. Whether at the beginning of the case withheparinization or at the end of the case when theremay be excessive bleeding from an unknown cause,the anesthesiologist must be familiar with the toolsto treat the patient.
Activated coagulation timeThe Activated coagulation time (ACT) is most com-monly used to monitor for heparin effect. Wholeblood is added to a test tube containing eitherdiatomaceous earth (celite) or kaolin. This activatorinduces thrombosis which is measured in seconds.Normal ACT values range between 80–120 seconds.When aprotinin is used as an antifibrinolytic agent,kaolin ACT cartridges should be used; celite ACTcartridges are associated with falsely elevated ACTvalues (thereby making the patient appear fullyanticoagulated when, in fact, this is not the case).The ACT test can be modified by adding hepari-nase to one of the chambers. In this situation,heparin is revered with the heparinase, and there-fore any abnormality in ACT value is likely due to

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 88 — #47
88 Chapter 3
some factor other than inadequate heparin reversalwith protamine. The ACT is subject to variability,and there are elevated ACT values seen with bothhemodilution and hypothermia. Nonetheless, theACT is the standard monitor of coagulation in mostoperating rooms. The ACT should be checked atleast every half-hour while on CPB.
Heparin dose–response testThe Heparin dose–response test (HDR) allows theclinician to fine tune the patient variability inresponse to a heparin dose by constructing an indi-vidualized heparin dose–response curve. The HDRuses a known quantity of heparin in an ACT deter-mination, and an algorithm using the baseline ACTand the estimated blood volume to construct a dose–response curve. The advantage of this system is thegreater accuracy in dosing eliminating both underand over dosing with heparin. Further, this testprovides information on individualized protaminedoing at the termination of CPB.
Heparin concentration testingHeparin concentration can be measured using adevice that automatically titrates protamine inknown quantities in whole, heparinized blood.Protamine neutralizes heparin in the ratio of1mg/100units of heparin. With this information,a protamine–heparin titration can yield the circu-lation concentration of heparin. When monitoringheparin concentration, higher doses of heparin aretypically administered than when the ACT is mon-itored likely because of the effects of hypothermiaand hemodilution on the ACT. In side-by-side com-parisons between ACT and heparin concentrationmonitoring, the additional heparin administeredseems to have little effect on blood loss or bloodadministration outcomes.
High dose thrombin timeThe High dose thrombin time (HiTT) measures theconversion of fibrinogen to fibrin by thrombin. HiTTis not altered by hemodilution, hypothermia oraprotinin.
Standard blood tests of coagulationAfter CPB and reversal of heparin with protamine,there are some patients that continue to bleed
for unknown reasons. In these patients, stan-dard tests of coagulation are indicated. These testsinclude a prothrombin time (PT), activated partialthromboplastin time (aPTT), fibrinogen and plateletcount. The PT (normal 12–14 seconds) measuresthe extrinsic and common coagulation pathways.It is prolonged with factor VII deficiency, warfarintreatment, vitamin K deficiency and in the pres-ence of large heparin doses. The aPTT measuresthe intrinsic and final common pathway of coagula-tion. It is extremely sensitive to heparin, deficienciesof factors XII, XI, IX and VIII, and kallikrein. Nor-mal aPTT is 28–32 seconds. Fibrinogen and plateletlevels measure the quantitative amount of thesesubstances in the blood. Normal fibrinogen levelsrange from 180 to 220mg/dL.Cryoprecipitate (a source of concentrated
fibrinogen) is indicated when the fibrinogenlevel is below 150mg/dL. Thrombocytopenia isencountered when the platelet count falls below100000/µL. Platelet counts greater than 50000/µLhave no correlation with bleeding time or observedpostoperative bleeding in cardiac surgical patients.Qualitative defects in platelet function are oftenmore important than the platelet count.
Fibrin degradationEvidence of normal or abnormal fibrinolysis isobtained by measuring the end products of fib-rin degradation. When plasmin cleaves fibrin,dimeric units are released into the blood, andthese “d-dimers” can be quantified. The presenceof d-dimers in the blood signifies fibrin cross-link degradation and may represent a condition ofabnormal fibrinolysis.
Bleeding timeThe bleeding time is obtained by performing aprecisely measured incision in the patient’s fore-arm above which a cuff is inflated to 40mmHg.The wound is dabbed with an absorbent tissueand the time until clot formation is measured.The bleeding time has no predictive value in car-diac surgical patients and has largely fallen out offavor.

Alice Nelson Dinardo: “ch03” — 2007/7/17 — 20:28 — page 89 — #48
Monitoring 89
(a) (b) (c) (d) (e)
Fig. 3.39 Thromboelastograph tracings. (a) Normal.(b) Coagulation factor deficiency. (c) Platelet dysfunctionor deficiency. (d) Fibrinolysis. (e) Hypercoagulability.(From Mallett SV, Cox DJ. Br J Anaesth 1992;69:307–13,with permission.)
Platelet aggregometryActivated platelets aggregate. Aggregometry mea-sures platelet responsiveness to various agonists andprovides information on the quality of the circulat-ing platelets to respond to various stimuli. Variousagonists include epinephrine, adenosine diphos-phate and collagen. Impaired aggregation is seen inpatients taking aspirin and after exposure to CPB.
ThromboelastographyThromboelastography (TEG) is a method of mon-itoring blood viscosity that can be used to evalu-ate various components of the coagulation system.The device usually contains two identical chan-nels so that two blood samples can be run atonce. Each channel consists of a disposable cylin-drical plastic cup mounted in a base. The cup isfilled with a blood and maintained at 37C dur-ing testing. A piston is attached to a torsion wirethat generates a signal as the blood clots. Withthis presentation, the real-time development ofthe TEG pattern can be assessed. A TEG sam-ple trace is shown in Fig. 3.39. The test usually
takes between 15–30minutes to complete andallows diagnosis of a variety of pathologic conditionsincluding coagulation factor deficiency, platelet andfibrinogen function and fibrinolysis. In clinical prac-tice the TEG has been shown to function well asa predictor of abnormal bleeding. In some centers,TEGuse is associatedwith a reduction inmediastinalexploration for bleeding and transfusion of bloodproducts.
Suggested reading
American Society of Anesthesiologists. Standards for
Basic Anesthetic Monitoring. Available online at: http://
www.asahq.org/publicationsAndServices/standards/
02.pdf. Accessed June 28, 2006.
Cheitlin MD, Armstrong WF, Aurigemma GP, et al. ACC;
AHA; ASE. ACC/AHA/ASE 2003 Guideline Update for
the Clinical Application of Echocardiography: sum-
mary article. A report of the American College of
Cardiology/American Heart Association Task Force
on Practice Guidelines (ACC/AHA/ASE Committee to
Update the 1997 Guidelines for the Clinical Appli-
cation of Echocardiography). J Am Soc Echocardiogr
2003;16:1091–110.Groban L, Dolinski SY. Transesophageal echocardio-
graphic evaluation of diastolic function. Chest 2005;128:3652–63.
Practice Guidelines for Pulmonary Artery Catheteriza-
tion. American Society of Anesthesiologists, Inc. Avail-
able online at: http://www.asahq.org/publicationsAnd
Services/pulm_artery.pdf. Accessed June 28, 2006.
Shanewise JS, Cheung AT, Aronson S, et al. ASE/SCA
Guidelines For Performing a Comprehensive Intraop-
erative Multiplane Transesophageal Echocardiography
Examination: recommendations of the American Soci-
ety of Echocardiography Council for Intraoperative
Echocardiography and the Society of Cardiovascular
Anesthesiologists Task Force for Certification in Peri-
operative Transesophageal Echocardiography. Anesth
Analg 1999;89:870–84.

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 90 — #1
CHAPTER 4
Anesthesia for MyocardialRevascularization
Coronary artery bypass graft (CABG) surgeryaccounts for approximately 500 000 operativeprocedures per year in the United States. Althoughthere is great interest and development in alterna-tives to CABG, this operative procedure remains anappropriate, indicated therapy for a large number ofpatients. Patient outcome after percutaneous coro-nary intervention (i.e. stent placement, atherec-tomy, angioplasty, other) remains a moving targetas new therapies and technologies are developedand employed. Similar to this, outcome after CABGis evolving. The indications for CABG are period-ically reviewed by the American College of Cardi-ology (ACC) and the American Heart Association(AHA) (Tables 4.1 and 4.2). The reader is referredto the ACC’s website (www.acc.org) for the latestupdate.A firmunderstanding of the dynamics of coronary
blood flow, the determinants of myocardial oxygenbalance, and the consequences and treatment ofischemia are necessary to care for patients under-going coronary revascularization. This chapter willreview the physiology of coronary blood flow, theelements of myocardial oxygenation, the care andtreatment of patients with active ischemia, and theanesthetic care of patients presenting for CABG.
Control of coronary blood flow
Coronary perfusion pressureCoronary perfusion can only occur when aorticroot pressure exceeds subepicardial and subendo-cardial pressure. Myocardial back-pressure, which
is the summation of factors that tend to collapsemicrovessels, is important in determining coro-nary perfusion pressure (CPP). In clinical practice,myocardial back-pressure is equal to myocardialtissue pressure. The best estimate of myocardialtissue pressure is the ventricular pressure. In dias-tole, this will be the ventricular end-diastolic pres-sure. The best clinical estimate of left ventricularend-diastolic pressure (LVEDP) is the pulmonarycapillary wedge pressure (PCWP); whereas the bestestimate of right ventricular end-diastolic pres-sure (RVEDP) is the central venous or right atrialpressure (RAP).In the absence of obstruction to flow within
the coronary arterial system, left ventricular (LV)CPP is the driving force for blood going intothe myocardium – the resistance to blood flow.Physiologically, in the left ventricle, this relation-ship translates as CPP = aortic root diastolic bloodpressure – PCWP (Fig. 4.1). CPP will differ duringsystole and diastole. In the left ventricle, ventricularpressure during systole is equal to or, as in the caseof aortic stenosis, greater than aortic root pressure.For this reason, most coronary blood flow to the leftventricle occurs during ventricular diastole. In theright ventricle, in which right ventricular (RV) sys-tolic and diastolic pressures are both considerablyless than aortic root pressure, coronary blood flowis distributed evenly between systole and diastole.
AutoregulationChanges in coronary vascular resistance are nec-essary for the myocardium to regulate coronary
90

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 91 — #2
Anesthesia for Myocardial Revascularization 91
Table 4.1 The list of indications for coronary artery bypass graft surgery for patients with stable angina and unstableangina/Non-ST-segment elevation myocardial infarction (MI). The indications are assigned class and the level ofevidence provided for the recommendation. (From Eagle KA, Guyton RA, Davidoff R et al. ACC/AHA 2004Guideline Update for Coronary Artery Bypass Graft Surgery: summary article. A report of the American College ofCardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999Guidelines for Coronary Artery Bypass Graft Surgery). Circulation 2004;110:1168–76.)
Stable anginaClass I1 CABG is recommended for patients with stable anginawho have significant left main coronary artery stenosis (Level ofevidence: A)2 CABG is recommended for patients with stable angina who have left main equivalent: significant (≥70%) stenosis ofthe proximal LAD and proximal left circumflex artery (Level of evidence: A)3 CABG is recommended for patients with stable angina who have 3-vessel disease. (Survival benefit is greater whenLVEF is <0.50) (Level of evidence: A)4 CABG is recommended in patients with stable angina who have 2-vessel disease with significant proximal LAD stenosisand either EF <0.50 or demonstrable ischemia on noninvasive testing (Level of evidence: A)5 CABG is beneficial for patients with stable angina who have 1- or 2-vessel CAD without significant proximalLAD stenosis but with a large area of viable myocardium and high-risk criteria on noninvasive testing (Level ofevidence: B)6 CABG is beneficial for patients with stable angina who have developed disabling angina despite maximal noninvasivetherapy, when surgery can be performed with acceptable risk. If the angina is not typical, objective evidence of ischemiashould be obtained (Level of evidence: B)
Class IIa1 CABG is reasonable in patients with stable angina who have proximal LAD stenosis with 1-vessel disease.(This recommendation becomes Class I if extensive ischemia is documented by noninvasive study and/or LVEF is <0.50)(Level of evidence: A)2 CABG may be useful for patients with stable angina who have 1- or 2-vessel CAD without significant proximal LADstenosis but who have a moderate area of viable myocardium and demonstrable ischemia on noninvasive testing(Level of evidence: B)
Class III1 CABG is not recommended for patients with stable angina who have 1- or 2-vessel disease not involving significantproximal LAD stenosis, patients who have mild symptoms that are unlikely due to myocardial ischemia, or patients whohave not received an adequate trial therapy and the following:a Have only a small area of viable myocardium (Level of evidence: B) orb Have no demonstrable ischemia on noninvasive testing (Level of evidence: B)2 CABG is not recommended for patients with stable angina who have borderline coronary stenoses (50–60% diameterin locations other than the left main coronary artery) and no demonstrable ischemia on noninvasive testing (Level ofevidence: B)3 CABG is not recommended for patients with stable angina who have insignificant coronary stenosis (<50% diameterreduction) (Level of evidence: B)
Unstable angina/non-ST-segment elevation MIClass I1 CABG should be performed for patients with unstable angina/non-ST-segment elevation MI with significant left maincoronary artery stenosis (Level of evidence: A)2 CABG should be performed for patients with unstable angina/non-ST-segment elevation MI who have left mainequivalent: significant (≥70%) stenosis of the proximal LAD and proximal left circumflex artery (Level of evidence: A)
Continued p. 92

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 92 — #3
92 Chapter 4
Table 4.1 (Continued).
3 CABG is recommended for unstable angina/non-ST-segment elevation MI in patients in whom revascularization isnot optimal or possible and who have ongoing ischemia not responsive to maximal nonsurgical therapy (Level ofevidence: B)
Class IIa1 CABG is probably indicated in patients with unstable angina/non-ST-segment elevation MI who have proximal LADstenosis with 1- or 2-vessel disease (Level of evidence: A)
Class IIb1 CABG may be considered for patients with unstable angina/non-ST-segment elevation MI who have 1- or 2-vesseldisease not involving the proximal LAD when percutaneous revascularization is not optimal or possible. (If there is alarge area of viable myocardium and high-risk criteria are met on noninvasive testing, this recommendation becomesClass I) (Level of evidence: B)
Class I: Conditions for which there is evidence and/or general agreement that agiven procedure or treatment is useful and effective
Class II: Conditions for which there is conflicting evidence and/or a divergenceof opinion about the usefulness/efficacy of a procedure or treatmentIIa:Weight of evidence/opinion is in favor of usefulness/efficacyIIb: Usefulness/efficacy is less well established by evidence/opinion
Class III: Conditions for which there is evidence and/or general agreementthat the procedure/treatment is not useful/effective and in some cases may beharmful
Level of EvidenceLevel of Evidence A: Data are derived from multiple randomized clinical trialsor meta-analysesLevel of Evidence B: Data are derived from a single randomized trial, ornonrandomized studiesLevel of Evidence C: Only consensus opinion of experts, case studies, orstandard of care
Table 4.2 The classification ofrecommendations and level ofevidence used by the AmericanCollege of Cardiology and theAmerican Heart AssociationGuidelines for Coronary Artery BypassGraft Surgery. (From Eagle KA,Guyton RA, Davidoff R et al. ACC/AHA2004 Guideline Update for CoronaryArtery Bypass Graft Surgery: summaryarticle. A report of the AmericanCollege of Cardiology/American HeartAssociation Task Force on PracticeGuidelines (Committee to Update the1999 Guidelines for Coronary ArteryBypass Graft Surgery). Circulation2004;110:1168–76.)
blood flow in response to changes in myocardialoxygen consumption. Coronary autoregulation isthe intrinsic ability of the myocardium to main-tain coronary blood flow constant over a varietyof perfusion pressures. As illustrated in Fig. 4.2,coronary autoregulation maintains coronary bloodflow constant between perfusion pressures of60 and 140mmHg. Below and above these pres-sures, myocardial blood flow is pressure-dependent;that is, myocardial blood flow varies linearly withpressure and with the time available for perfusion
(diastole for the left ventricle, systole and diastolefor the RV).Autoregulation is dependent on changes in coro-
nary vascular resistance. The arterioles are theprimary source of resistance in the coronary arte-rial system. Autoregulation is tied to myocardialoxygen metabolism and coronary venous partialpressure of oxygen PO2, although the exact medi-ators at the vascular level are unknown. Duringexercise, reductions in coronary vascular resis-tance result in increased coronary blood flow

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 93 — #4
Anesthesia for Myocardial Revascularization 93
100B
P (
mm
Hg)
0Time
Sys
tole
MADBP
Aortic blood pressure
LAP or PCWP
Fig. 4.1 Left ventricular coronary perfusion pressure(CPP) is the difference between aortic diastolic bloodpressure and left ventricular end-diastolic pressure(LVEDP). Clinically, LVEDP is estimated by left atrialpressure (LAP) or pulmonary capillary wedge pressure(PCWP). Diastolic CPP is represented by cross-hatchedarea and can be seen to decrease as diastole progresses.Average diastolic CPP can be obtained by takingdifference between mean aortic diastolic blood pressure(MADBP) and LAP or PCWP. Length of time available forperfusion of left ventricle is dependent on length ofdiastole. Shortening diastole by increasing length ofsystole per beat or by increasing heart rate will decreasethe time available for left ventricular perfusion. (FromDiNardo JA. Anesthesia for myocardial revascularization.In: DiNardo JA (ed). Anesthesia for Cardiac Surgery,2nd edn. Stamford, CT: Appleton & Lange, 1998:81–108,with permission.)
(up to six-times normal). Likewise, as CPP falls,coronary vascular resistance decreases to main-tain coronary blood flow. At pressures <60mmHg,there is a progressive loss of autoregulation. Atsome point, the coronary arteries dilate maximallyand coronary blood flow now decreases linearlywith CPP. Autoregulation in the subendocardiumis exhausted before that of the subpericardium.
Collateral blood flowThe development of collateral blood flow inhumans is dependent on enlargement of pre-existing anastomoses between coronary arteries.These anastomoses may be either serial (pre-stenosis to post-stenosis in the same artery) orparallel (one artery to another). Collateral pathwaysenlarge in response to pressure gradients. After thecollateral pathways have enlarged, the direction andmagnitude of collateral blood flow remain pressuredependent. For this reason, collateral blood flow toa post-stenotic segment can be significantly reduced
Cor
onar
y bl
ood
flow
(m
L/m
in/1
00g)
150
100
50
0
Coronary perfusion pressure (mmHg)
0 40 80 120 160
Autoregulatoryvasodilator
reserve
Fig. 4.2 Coronary blood flow is seen to be constant(autoregulated) over coronary perfusion pressures from60–140mmHg. When coronary perfusion pressurereaches 60mmHg, there will be maximal autoregulatoryvasodilation to maintain coronary blood flow. Furtherdecreases in coronary perfusion pressure will result indecreases in coronary blood flow. At pressures higherthan 60mmHg, maximal autoregulatory vasodilation willprovide autoregulatory vasodilator reserve. This reserveprovides the increased coronary blood flow necessaryto meet increases in myocardial oxygen consumptionsuch as those induced by exercise. (From DiNardo JA.Anesthesia for myocardial revascularization. In:DiNardo JA (ed). Anesthesia for Cardiac Surgery, 2nd edn.Stamford, CT: Appleton & Lange, 1998:81–108, withpermission.)
if perfusion pressure at the origin of the collateral isreduced.There is evidence that coronary collateral flow
improves the outcome in patients with an acutemyocardial infarction (MI). This same relationshipis also true after CABG surgery. In a review of561 patients with a low-risk profile, the presenceof collaterals protects against cardiac death and MIat 1 year after coronary revascularization (Fig. 4.3).
Causes of increased myocardialoxygen demand
Three factors are primarily responsible for deter-mining myocardial oxygen consumption (MVO2):wall tension, contractility, and heart rate (HR).
Wall tensionMyocardial wall tension is determined by the rela-tionship between ventricular radius (r), ventricular

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 94 — #5
94 Chapter 4
6.0(a)
(b)
5.0
4.0
3.0
2.0
1.0
0.0
14.0
12.0
10.0
8.0
6.0
4.0
2.0
0.00 60 120 180 240 300 360 420
0
No. at riskCollaterals −Collaterals +
60 120 180 240Time since randomization (days)
Collaterals absent: 13.5%
Collaterals present: 5.7%
P < 0.01
00
191
211
222
222
222
222
232
300 360 420
P = 0.01
Collaterals absent: 5.3%
Collaterals present: 1.1%
Car
diac
dea
th o
r M
I (%
)A
ll ca
rdia
c ev
ents
(%
)
Time since randomization (days)
Fig. 4.3 Kaplan–Meier estimates of proportion of firstclinical events at 1 year after coronary revascularizationas stratified by collaterals. The P-values were calculatedusing the log–rank test. (a) Cardiac death or nonfatalmyocardial infarction (MI). (b) All-cause death, nonfatalstroke, nonfatal MI, or repeat coronary revascularization.(From Nathoe HM, Koerselman J, Buskens E et al.Determinants and prognostic significance of collateralsin patients undergoing coronary revascularization.Am J Cardiol 2006;98:31–5, with permission.)
pressure (P), and ventricular wall thickness (h)according to Laplace’s law: T = Pr/h. Ventricularwall tension constantly changes during the cardiaccycle. For example, during isovolumic contrac-tion, ventricular pressure and wall thicknesswill be increasing while ventricular radius remainsunchanged. During ventricular ejection, ventricularpressurewill remain relatively constantwhile radiusdecreases and wall thickness increases. Inherent inthe analysis of wall tension are the concepts of
preload, afterload, and hypertrophy. Increases inend-diastolic volume (EDV) (preload) will increaseventricular radius and will reduce wall thickness ifdilation is severe. These changes will increase walltension. Increases in the impedance to ventricularejection (afterload)will necessarily increase ventric-ular pressure and increase wall tension. Concentricventricular hypertrophywill increase wall thicknessand reduce wall tension.There are important differences between the
increase in MVO2 induced by increases in preloadand by those induced by increases in afterload.Work done in the isovolumic phase of ventricularcontraction is very energy-consumptive. Increasesin the impedance to ventricular ejection increasethe pressure required to begin ventricular ejection,and thus increase the work done in the isovolumiccontraction phase. The ejection phase of ventric-ular contraction, on the other hand, is a moreenergy-efficient process. Increases in preload induceejection of a larger stroke volume (SV) and anincrease in the work done in the ejection phase.For these reasons, when comparing equal work, theincrease in MVO2 induced by an increase in preload(volume work) is much less than that induced byan increase in afterload (pressure work).
ContractilityContractility is the state of myocardial performance(inotropy) independent of preload and afterload.Increasing the contractile state of the heart willincrease MVO2. However, an increase in contrac-tility may actually result in a reduced or unchangedMVO2 under certain conditions. For example, ifventricular dilation (increased ventricular radius)exists to maintain cardiac output (CO), wall ten-sion andMVO2 will be high. Improving contractilitythrough use of an inotropic agent can reduce ven-tricular radius while maintaining CO. The reductioninMVO2 that accompanies the reduction in ventric-ular radius may more than offset the increase thataccompanies an increase in contractility.
Heart rateHeart rate directly affects myocardial oxygen bal-ance. Tachycardia increases myocardial oxygendemand and reduces supply by diminishing the time

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 95 — #6
Anesthesia for Myocardial Revascularization 95
in diastole. Perhaps more importantly, one mustconsider the imbalance on a beat-to-beat basis.Myocardial ischemia does not occur with tachycar-dia simply because there are more beats per minute;rather, ischemia occurs with tachycardia becausesupply per beat is inadequate to meet demandper beat. Increases in HR increase MVO2 per beatby increasing contractility via the Bowditch effect.Normally, increasing HR decreases EDV. This reduc-tion in preload reduces wall tension and MVO2per beat. Thus, with tachycardia, the increase inMVO2 per beat caused by enhanced contractilityis offset by the reduction in MVO2 per beat thataccompanies reduced wall tension. On the otherhand, oxygen delivery is sometimes compromisedby tachycardia-induced reductions in the length ofdiastole per beat (discussed later).
Causes of reduced myocardialoxygen delivery
Adequate myocardial oxygen supply is dependenton delivery of the appropriate volume of oxy-genated coronary blood flow. The following sectionsdescribe factors that may compromise myocardialoxygen delivery.
Reduction in CPPLV CPP falls with either a reduction in diastolicblood pressure (DBP) or an increase in LV end-diastolic pressure. A commonly overlooked causeof reduced CPP is bradycardia. Bradycardia encour-ages diastolic runoff from the proximal aorta andmay result in a wide pulse pressure and reducedDBP. Furthermore, maintenance of CO with brady-cardia requires an increased SV. The increased SVoccurs primarily by an increase in left ventricularend-diastolic volume (LVEDV) and pressure. Thisfurther reduces CPP.
Reduction in time available forcoronary perfusionThe left ventricle receives most its perfusion dur-ing diastole; therefore, reductions in diastolic timeare potentially detrimental. Figure 4.4 illustratesthat as HR increases the length of time per beatspent in diastole falls while the length of systole
1000(a)
800
600
Tim
e (m
s)
400
200
0
80(b)
70
60
50
40
30
R–R
QS2
30
% D
iast
ole
40 50 60
30 50 70 90 110 130 150
70 80 90
Heart rate
100 110 120 130 140 150
Total diastolic period (R–R)–(QS2)
Heart rate
Fig. 4.4 (a) Increases in heart rate cause decreases inlength of each cardiac cycle (R–R interval). Decreasesin length of systole (OS2) with increases in heart rate arefar less dramatic than decreases in length of diastole(R–R–OS2). (b) Percent of each cardiac cycle(R–R interval) spent in diastole at various heart rates.Small changes in heart rate are seen to cause largedecreases in percent of time spent in diastole. (FromBoudoulas H. Changes in diastolic time with variouspharmacologic agents. Circulation 1979;60:165, withpermission.)
remains constant. Because MVO2 per beat is min-imally affected by tachycardia, the primary dis-advantage of tachycardia is a reduction in diastolicperfusion time per beat.
Obstruction to flowAny obstruction to flow in a coronary arteryresults in a pressure drop across the obstruction.The high velocity of blood flow in the area ofa stenosis (either stable, i.e. plaque disease; or

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 96 — #7
96 Chapter 4
dynamic, i.e. coronary spasm) necessarily resultsin the conversion of pressure energy to kineticenergy. On the distal side of the obstruction, tur-bulent eddies form and dissipate. The transfer ofkinetic energy to this turbulent energy and the sub-sequent dissipation of the turbulence reduce thequantity of kinetic energy available for conver-sion to pressure energy. This results in a pressuredrop across the obstruction. The pressure drop willincrease in direct proportion to any increase inflow across the obstruction as a greater propor-tion of kinetic energy dissipates as turbulence. Forthis reason, requirements for increased coronaryblood flow, such as those that accompany exercise,will increase the hemodynamic significance of anyobstructive lesion.Arteriolar dilatation distal to the obstruction will
help compensate for this pressure loss until thestenosis becomes critical. A stenosis is “critical”when the vasodilator reserve distal to the stenoticlesion is exhausted. This occurswith stenosis>90%.In the absence of autoregulation, coronary bloodflow distal to a stenotic lesion will fall linearly withdecreases in perfusion pressure. This places the dis-tal subendocardium at risk for ischemia. It followsthat in the presence of an obstructive coronarylesion, coronary perfusion is critically dependent onaortic DBP. The factors described in the followingsections deserve attention.
Atherosclerotic diseaseAtherosclerosis is a complex, heterogeneous dis-ease often starting in the very young and evolvingover several decades. There are both acute andchronic manifestations of the disease, the mostsignificant of which, involves the development ofcoronary occlusive disease, unstable coronary syn-dromes, MI, and death. Other systemic manifes-tations include progressive neurologic dysfunction(dementia), renal impairment, claudication,mesen-teric ischemia, hypertension, and stroke. The dis-ease is progressive in nature with a defined patternof morphologic evolution (Fig. 4.5).The fate of atheromatous lesions is dependent on
three additional factors:• Plaque disruption. Atheromatous lesions are lipidrich, soft, and prone to disruption from mechanical
forces. Plaque rupture may result in exposure ofsuperficial vascular wall elements or of deep fibrillarcollagen.• Thrombosis. Exposure of vascular wall elements isa stimulus for thrombus formation. Platelet depo-sition occurs at the site of disruption. Superficialplaque disruption is a much milder thrombogenicstimulus than deep plaque disruption. Thrombusformation at the site of a superficial injury is likelyto be labile and transient, whereas thrombus forma-tion associated with deep plaque disruption is likelyto be stable and permanent. This is often the causeof acute coronary syndromes.• Vasoconstriction. Transient vasoconstrictionaccompanies plaque disruption and thrombusformation. Injury to the endothelium producesthrombin-mediated vasoconstriction; whereas,subsequent platelet deposition mediates vasocon-striction via release of thromboxane-A2 and sero-tonin. In addition, endothelial injury may impairthe release of nitric oxide (NO).Using these concepts, one can understand the
spectrum of coronary artery disease (CAD) fromchronic stable angina to acute MI. Chronic stablestenotic lesions that cause angina develop as theresult of progression of atherosclerotic lesions.Progression of early lesions is more rapid in patientswith coronary risk factors. Progression is the resultof mural thrombus formation and fibrotic orga-nization, which follows minor plaque disruption.Initially, platelet thrombi form on the disruption.This is followed by migration of smooth musclecells from the media into the intima. During thefinal phase, intimal thickening and progression ofthe lesion occur. Repetition of this process leadsto gradual progression of the lesion. Ultimately, itmay lead to a chronic vessel occlusion. The slowprogression of the lesion allows time and providesstimulus for distal arteriolar collateral formation.This explains why thrombotic occlusion is frequentin patients with high-grade stenoses but does notlead to infarction.In unstable angina, a small plaque disruption
may change plaque morphology such that coro-nary blood flow is acutely reduced and anginaintensifies. Alternatively, plaque disruption may beassociated with labile thrombus, temporary vessel

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 97 — #8
Anesthesia for Myocardial Revascularization 97
LDL1
2
3
MCP-15
6
Smooth muscle mitogens
Foam cell
8
7
Cellapoptosis
Smooth muscleproliferation
Smooth musclemigration
IL-1
Oxidized LDL
Internal elasticlamina
Vascularendothelium
Monocytes Scavenger receptor
MacrophageCell adhesionmolecule
4
Fig. 4.5 Schematic of the evolution of theatherosclerotic plaque. 1. Accumulation of lipoproteinparticles in the intima. The modification of theselipoproteins is depicted by the darker color. Modificationsinclude oxidation and glycation. 2. Oxidative stress,including products found in modified lipoproteins,can induce local cytokine elaboration. 3. The cytokinesthus induced increase expression of adhesion moleculesfor leukocytes that cause their attachment andchemoattractant molecules that direct their migrationinto the intima. 4. Blood monocytes, upon entering theartery wall in response to chemoattractant cytokinessuch as monocyte chemoattractant protein 1 (MCP-1),encounter stimuli such as macrophage colony stimulatingfactor (M-CSF) that can augment their expression ofscavenger receptors. 5. Scavenger receptors mediate theuptake of modified lipoprotein particles and promote thedevelopment of foam cells. Macrophage foam cells area source of mediators such as further cytokines andeffector molecules such as hypochlorous acid, superoxide
anion (O−2 ), and matrix metalloproteinases. 6. Smoothmuscle cells in the intima divide other smooth musclecells that migrate into the intima from the media.7. Smooth muscle cells can then divide and elaborateextracellular matrix, promoting extracellular matrixaccumulation in the growing atherosclerotic plaque.In this manner, the fatty streak can evolve into afibrofatty lesion. 8. In later stages, calcification can occur(not depicted) and fibrosis continues, sometimesaccompanied by smooth muscle cell death (includingprogrammed cell death, or apoptosis) yielding arelatively acellular fibrous capsule surrounding alipid-rich core that may also contain dying or dead cellsand their detritus. IL-1, interleukin-1; LDL, low-densitylipoprotein. (From Libby P. The vascular biology ofatherosclerosis. In: Zipes DP, Libby P, Bonow RO,Braunwald E (eds). Braunwald’s Heart Disease: A Textbookof Cardiovascular Medicine, 7th edn. Philadelphia:Elsevier–Saunders, 2005:921–37, with permission.)
occlusion, and angina at rest. Coronary blood flowis further compromised by release of vasoconstrictorsubstances and impaired endothelial relaxation.In non-Q-waveMI, the process is similar to that in
unstable angina, except that the duration of vesselocclusion by labile thrombus is longer and there isresultant muscle injury and necrosis. Spontaneousthrombolysis or resolution of arterial spasm ulti-mately limits occlusion and prevents Q-wave MI(full thickness, or transmural MI). This process isresponsible for 75% of non-Q-wave MIs. The other25% occur when there is complete occlusion of theinfarct-related vessel with distal collateralization.
In a Q-wave MI, plaque disruption is associ-ated with formation of a fixed, persistent occlusion(usually by a thrombus, although this may occurwith an embolized vegetation or other material).This leads to cessation of blood flow and myo-cardial necrosis. The coronary lesion involvedusually is mild to moderate in severity with lim-ited distal collateralization. Thus, it is the intensityof plaque disruption and subsequent thrombus for-mation rather than the severity of the lesion that isthe determining factor.Further discussion is necessary to explain the
spectrum of anginal symptoms that can accompany

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 98 — #9
98 Chapter 4
a chronic, stable, stenotic coronary lesion. Themaincoronary artery epicardial branches have lumensthat are 2–4mm in diameter. In the absence ofcollaterals, exertional angina occurs when lumenarea is reduced to 1.0mm2 (50–60% reduction inlumen diameter or 75% reduction in cross-sectionalarea) and angina at rest occurs when lumen areais reduced to 0.65mm2 (75% reduction in lumendiameter or 90% in cross-sectional area).Figure 4.6 illustrates how changes in coronary
vascular tone can alter the clinical characteristicsof a chronic, stable stenotic lesion. Atheromatouslesions may be localized to one area of the arterialwall. As these eccentrically located lesions enlarge,they encroach upon the arterial lumen. Becausethe remainder of the arterial wall is free of plaque,it remains responsive to vasoactive stimuli and iscapable of contraction. Such contraction will causethe fixed atheromatous lesion to occupy a greaterportion of the arterial lumen and will result in alarger pressure drop across the lesion. Therefore,the severity of the stenosis is not static but isdynamic and dependent on the vasomotor activ-ity of the free arterial wall. This phenomenon isknown as dynamic coronary stenosis. As illustrated
in Fig. 4.6, a normal change in coronary vasomotortone resulting in a 10% circumferential shorteningof the outer arterial wall can convert an insignificant49% eccentric stenosis to a 76% stenosis, whichwill result in rest ischemia. Likewise, Fig. 4.6 illus-trates that a normal increase in arterial tone canconvert an eccentric stenosis, which causes ischemiaon exertion (60% stenosis), to one that also causesischemia at rest (76% stenosis).Atheromatous lesions may be static if the athero-
matous changes involve the entire circumferenceof the arterial wall. In this instance, the luminalarea is fixed and is unaltered by changes in arte-rial vasomotor activity. Figure 4.6 illustrates thata lesion that occupies the entire circumference ofthe arterial wall and causes exertional ischemia(60% stenosis) will be unaffected by changes inarterial vasoconstriction.
Variations in coronary vasomotor toneThere is a large variation in the extent of coro-nary vasomotor activity across a population. At oneend of the spectrum is the normal 10% reduc-tion in outer arterial wall circumference that occurswith α-adrenergic stimulation. At the other end of
Normal
Young, thinintima
Resting lumencross-section
“Normal”vasoconstriction(0% outercircumferentialshortening)
Diffuse intimalsmooth muscle
proliferation
Moderate sizedeccentric lumen plusintimal proliferation
Small eccentriclumen
Morphologic variants of atherosclerosis
Circumferentialatheroma
central lumen
17% 76%76% 76%76% 76%76%
47% 49%
1/3 fixed
Clinical syndrome: Asymptomatic Rest pain only Rest pain only Rest and exertional pain
Exertionalpain only
2/3 fixed 100% fixedcircumference
60% 60%
60%76% 76% 76%
Fig. 4.6 Cross-sections of normal and diseasedcoronary arteries. Morphologic state of arteries isillustrated. Percent reduction in lumen diameter for eachmorphologic state at rest and following normal degree ofvasoconstriction is also shown. Clinical syndromes
associated with both resting and vasoconstricted state ofnormal and diseased arteries are summarized at bottomof diagram. (From Brown BG. Dynamic mechanisms inhuman coronary stenosis. Circulation 1985;70:921, withpermission.)

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 99 — #10
Anesthesia for Myocardial Revascularization 99
the spectrum, is the intense vasoconstriction thatoccurs with variant or Prinzmetal’s angina. Theexaggerated coronary spasm seen in these patientsresults in total or near total occlusion in responseto stimuli that cause only minimal constriction inindividuals who do not have variant angina. Forpatients with coronary spasm, myocardial ischemiamay develop in the absence of coronary stenosis.For patients with normal coronary vasoconstriction,myocardial ischemia will occur only if coronarystenoses also exist.
Coronary stealCoronary steal refers the physiologic conditionwhereby blood flow is directed away from ischemicprone areas of the myocardial dependant uponupstream coronary artery anatomy (Fig. 4.7).Coronary steal occurs in some patients with specificcoronary artery lesions upon the exposure of coro-nary vasodilators. Approximately one-fourth ofpatients with CAD meet these anatomical criteria.In these patients, the administration of an arterio-lar dilator, such as dipyridamole or adenosine, mayproduce a steal.In the mid-1980s a series of reports suggested
that isoflurane induced coronary steal by abnor-mally redistributing flow away from ischemic areasof the myocardium. Subsequent work and clinicalexperience, however, have refuted this proposition.Although isoflurane-induced hypotension may
reduce myocardial perfusion, true coronary stealdoes not occur when CPP is maintained. Furtherstudies demonstrate that the volatile agentsdo not abnormally reduce or redistribute coronarycollateral flow.In contrast to these initial concerns regarding
isoflurane, recent evidence suggests a myocardialprotective benefit with volatile agent use (Fig. 4.8).These protective benefits extend beyond a favor-able alteration in the oxygen supply and demandbalance. The benefits may be related to physiologicalterations in response to ischemia and reperfu-sion. Many of these actions are similar to thosefound with ischemic preconditioning, and are infact, termed, anesthetic-induced preconditioning(discussed later).
AnemiaMyocardial oxygen delivery is the product ofcoronary blood flow and the oxygen content ofthe transported blood. Anemia reduces myocardialoxygen delivery by reducing the oxygen-carryingcapacity of blood. The degree of anemia that an areaof myocardium can tolerate without developingischemia is dependent on the relationship betweenregional MVO2 and regional coronary blood flow.In the absence of coronary stenoses, hematocritlevels <15% result in subendocardial ischemiain anesthetized canines. In the presence of theincreased MVO2 that accompanies large increases
Coronaryarteriolar
vasodilatorPreferentialvasodilatationincreases flow tononischemicarea
Stenosis>50%
Blockedepicardialcoronary
Area ADependent on collateralsNo autoregulatory reserveMaximally dilated
Area BNormal autoregulation
Area AIschaemic as collateralperfusion diverted away
Area BNormal regulation lostLuxury perfusion
Collateral flow Reducedcollateral
flow
Fig. 4.7 Schematic diagram illustrating coronary steal. Arrows represent coronary blood flow. (From Agnew NM,Pennefather SH, Russell GN. Isofurane and coronary heart disease. Anaesthesia 2002;57:338–47, with permission.)

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 100 — #11
100 Chapter 4
10
8
6
4
2
0Control T0 T3 T12 T24 T36
14
12
10
Tro
poni
n I (
ng/m
L)T
ropo
nin
I (ng
/mL)
8
6
4
2
0Control T0 T3 T12 T24 T36
Control T0 T3 T12 T24 T36 Control T0 T3 T12 T24 T36
Propofol Desflurane Sevoflurane10
8
6
4
2
0
14
12
10
8
6
4
2
0
10
8
6
4
2
0
14
12
10
8
6
4
2
0Control T0 T3 T12 T24 T36 Control T0 T3 T12 T24 T36
Fig. 4.8 Coronary artery patients (n = 45) wererandomly assigned to receive either target controlledinfusion of propofol or inhalational anesthesia withdesflurane or sevoflurane. After coronary artery bypass(CPB), the cardiac index was lower in the propofolgroup. Cardiac troponin I concentrations in the threegroups before surgery (control), at arrival in the intensivecare unit (T0), and after 3 (T3), 12 (T12), 24 (T24), and36 (T36) hours. The upper panel show the median values
with 95% confidence intervals. The lower panels showthe evolution of the individual values. Concentrationswere significantly higher with propofol anesthesia. (FromDe Hert SG, Cromheecke S, ten Broecke PW et al. Effectsof propofol, desflurane, and sevoflurane on recovery ofmyocardial function after coronary surgery in the elderlyhigh-risk patients. Anesthesiology 2003;99:314–23, withpermission.)
in afterload, hematocrit levels <30% producesubendocardial ischemia in the same canine model.There is great debate about the ideal hematocrit
in any patient and especially in the patient withknown CAD. Recent investigation in a medical pop-ulation after MI reveals that a hematocrit of atleast 33% is associated with improved outcome.Hematocrit levels must be individualized for eachpatient; however, lowhematocrit levels (<30%) arepotentially dangerous in awake patients with CADfor the following reasons:• Increased CO necessarily accompanies normo-volemic anemia to maintain systemic oxygentransport; this CO increase results in an increasedMVO2.• Increases in coronary blood flow to main-tain coronary oxygen delivery result in increasedpressure drops across stenoses and potential forsubendocardial hypoperfusion.
Myocardial ischemia
Regional or global imbalances inmyocardial oxygensupply and demand result in myocardial ischemia.The metabolic consequences of ischemia are dis-cussed in detail in Chapter 12. The clinical manifes-tations of myocardial ischemia are varied. Anginapectoris, with or without signs of ventricular fail-ure or dysrhythmias, is the classic manifestationof myocardial ischemia. However, it is importantto remember that angina is not a universal mani-festation of ischemia. In fact, myocardial ischemiamay present as ventricular failure or dysrhyth-miaswithout angina. In some individuals, especiallydiabetics, ischemiamay remain clinically silent. Fur-thermore, patients have varying thresholds for thedevelopment of ischemia during the course of a day.The dynamic nature of coronary stenoses accountsfor the changes in the caliber of a stenosis that

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 101 — #12
Anesthesia for Myocardial Revascularization 101
may produce rest pain at one time and angina withvarying degrees of exercise at other times.Despite these varied clinical presentations, the
progression of hemodynamic and electrocardio-graphic changes with ischemia tends to follow aconsistent pattern in a given patient. Myocardialischemia is heralded by a decrease in regionalventricular diastolic distensibility (see Chapter 2),which usually results in an elevation in LVEDP orRVEDP, and central venous pressure (CVP). Thisis followed by systolic dysfunction, electrocardio-gram (ECG) changes, and finally by angina duringsymptomatic episodes. Patients manifesting eleva-tions in PCWPwith symptomatic episodes are likelyto do so with asymptomatic episodes as well. Somepatients will not manifest wedge pressure changeswith either symptomatic or asymptomatic episodes.
Symptomatic versus asymptomaticmyocardial ischemiaAmbulatory Holter monitoring of patients withchronic stable angina demonstrates that 83% ofischemic episodes with ST-segment depression of1–2mm are asymptomatic, and 63% of ischemicepisodes with ST-segment depression of 3 mmor more are asymptomatic. Of the ischemic ECGchanges seen in elective CABG surgery patientsmonitored for 48hours in the preoperative period,up to 80% are asymptomatic. The reasons whysome episodes of ischemia are symptomatic whileothers are not remain unclear. There is some evi-dence that asymptomatic episodes are of shorterduration and lesser severity than symptomaticepisodes, but this is not consistently true. There isalso evidence to suggest that patients with asymp-tomatic episodes have a higher pain tolerance,but this is not uniformly true. Diabetic patientswith autonomic dysfunction are at higher risk forasymptomatic ischemia.
Incidence of perioperative ischemiaEfforts to prevent myocardial ischemia usuallytarget control of the readily obtainable hemody-namic determinants of myocardial oxygen demandsuch as HR and blood pressure (BP). Contrary tothis practice, however, most ischemic episodes arenot preceded by increases in HR or rate-pressure
product (RPP) (the product of HR and systolic BP).In fact, most episodes are clinically silent. The sameis true in cardiac surgical patients in the preopera-tive period. Approximately 40% of cardiac surgicalpatients will experience ST-segment evidence ofischemia sometime in the 48hours prior to elec-tive cardiac surgery. Less than one-fourth of theseepisodes are preceded by a HR increase of 20%or more. In addition, most of these episodes areclinically silent.As with preoperative ischemic events, approxi-
mately half of intraoperative ischemic events areunrelated to changes in HR and BP. This unpro-voked ischemia suggests that decreases in myocar-dial oxygen supply may be important in the genesisof intraoperative ischemia. In the cardiac sur-gical patient, ischemia consists of a backgroundof hemodynamically unrelated silent ischemia,upon which is superimposed episodes of hemo-dynamically related ischemia. Rigorous intraoper-ative hemodynamic control will not worsen thepreoperative ischemic pattern and may actuallyimprove it.In the noncardiac surgical population, the post-
operative period is the most common time forST-segment myocardial ischemia. In addition tothe underlying propensity towards silent ischemia(as described above), the postoperative period issubject to increasing metabolic demands, increasedMVO2, and a hypercoagulable state. There may beplaque fissure and subsequent thrombus formation.In the patient recovering from CABG, one antic-ipates a reduction in the incidence of ischemia.After all, the coronary artery stenoses are bypassed,and myocardial blood flow normalized. In reality,however, CABG patients may suffer postoperativeischemia for a number of reasons including acutegraft occlusion, coronary air or debris embolism,technical anastomoses failure or disruption, tam-ponade with graft obstruction, or myocardialoxygen supply–demand mismatch. CABG patientsrequire close monitoring for ischemia in the hoursafter surgery.
Outcome after myocardial ischemiaThe most significant consequence of pre- andintraoperative ischemia is postoperative myocardial

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 102 — #13
102 Chapter 4
infarction (PMI). The risk of PMI is approxi-mately 7% in CABG patients who had preoper-ative ischemia, intraoperative ischemia, or both,and 2.5% in patients who did not have ischemia.The risk of PMI correlates with the severity ofischemia. In patients with ST-segment depressions>2mV, the PMI incidence is 9%; whereas thosewith ST-segment depressions between 1.0–1.9mV,the incidence is 6%.There aremany factors well beyond the control of
the anesthesiologist that are responsible for increas-ing the incidence of PMI. An aortic cross-clamp timein excess of 40minutes increases the incidence ofPMI from 2.6 to 10.9%. PMI occurs in 14.3% ofpatients in whom the distal anastomoses were ratedby the surgeon as poor as compared with 3.4% ofpatients in whom the anastomoses were consideredof good quality.
Diagnosing myocardial ischemia
ECG changesThe gold standard for diagnosis of myocar-dial ischemia is the presence of ECG changes.Unfortunately, ECG changes occur relatively late inthe temporal sequence of myocardial ischemia afterdeterioration of ventricular diastolic and systolicfunction. Lead selection greatly enhances ischemicdetection. Simultaneous monitoring of leads II andV5 is commonly used because of the high sensi-tivity of this combination in detecting myocardialischemia.
PCWP traceThe PCWP trace of the pulmonary artery catheter(PAC) can assist in the early diagnosis of LVischemia. Reduction in LV compliance occurs inthe early stages of LV ischemia because of dias-tolic dysfunction. In particular, LVEDP is elevated.Under these circumstances, left atrial pressure (LAP)will be elevated to maintain LV diastolic filling.Movement of the left atrium (LA) to a steeperpotion of its pressure–volume relationship willresult in magnification of the normal LAP wave-forms. In addition, dilation of the LA may result ina more forceful atrial contraction and productionof an enlarged A wave. The peak of this A wave
will reflect LVEDP. LV ischemia, which produces LVdilation or papillary muscle dysfunction, may causemitral regurgitation with generation of a prominentV wave. If there is inferior ischemia with RV dys-function, some of these same observations may beseen on the CVP waveform.The PCWP trace is a reflection of LAP. However,
because the PCWPwaveform is transmitted throughthe compliant pulmonary venous system, it is adamped version of the LAP. In particular, the leftatrial A wave may be poorly seen. As a result, it hasbeen demonstrated that mean PCWP reflects meanLVdiastolic pressure andmayunderestimate LVEDPby 10–15mmHg during ischemia.Changes in PCWP and the PCWP waveform have
poor sensitivity and specificity in detecting episodesof myocardial ischemia. This is true for a number ofreasons:• PCWP does not necessarily reflect LVEDP aspreviously described.• When only a small region of LV wall developsdiminished compliance with an ischemic episode,overall LV functionmay be onlyminimally affected.This will reduce the observed changes in LVEDP asreflected by the PCWP.• The quantitative change in PCWP and the qual-itative change in the PCWP waveform neces-sary to define an ischemic event have not beensystematically defined.• Acute elevations in afterload in the absence ofischemia can produce elevations in PCWP. This maylead to a false positive interpretation of the PCWPtracing.Myocardial ischemia does not result in PCWP
chances in all patients, and therefore, PCWP cannotbe relied upon as the sole indicator of ischemia. Forthis reason, it is important to emphasize that sus-picious ECG or transesophageal echocardiography(TEE) changes cannot be ignored simply becausethere is no change in the PCWP or the PCWPwaveform.
Transesophageal echocardiographyRegional wall motion abnormalities (RWMA)during systole (diminished inward excursion andthickening) occur with ischemia. These RWMAprecede ECG changes. The development of severe

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 103 — #14
Anesthesia for Myocardial Revascularization 103
hypokinesis, akinesis, or dyskinesis is more specificfor ischemia than mild hypokinesis. Changes inwall thickening are more sensitive for detectingischemia than changes in wall excursion. Typically,wall motion abnormalities and ECG changes occurwithin 60 seconds of each other. However, in a sit-uation in which ischemia is less severe, RWMAmay precede ECG changes by several minutes. Infact, numerous studies have shown intraoperativeTEE qualitative analysis of regional wall excursionand thickening to be a more sensitive detector ofmyocardial ischemia than ECG changes and to becapable of detecting ischemia before ECG changes.As with all monitors, there are occasional dis-
crepancies between ischemia detected by ECGand that detected by TEE. There are both TEE-detected ischemic episodes not detected by ECGand ECG-detected ischemic episodes not detectedby TEE. This may be due to several factors:• Normally, the TEE probe is placed at the mid-LVlevel (level of the papillary muscles), at which wallsegments in the distribution of all three coronaryarteries can bemonitored. Because a short-axis viewof the left ventricle can only be obtained at one levelat a time, ischemic changes occurring in the basal orapical ventricular levels will be missed. Obtainingmultiple TEE windows, allowing visualization of all17 segments of the heart will reduce or eliminatethis as a source of error.• Ischemic episodes may be missed because qual-itative wall motion analysis is difficult for patientswith preexisting wall motion abnormalities.• Some RWMA (particularly in areas tethered toscar) may not be ischemic in origin. Changes inafterload may unmask areas of previous scarring.• Ventricular pacing or a bundle-branch block maymake detection of RWMA more difficult because ofasynchronous contraction.• Stunned myocardium may exhibit continuedRWMA despite adequate perfusion.• The ECG may detect ischemia with small areas ofsubendocardial ischemia undetectable by TEE.
Predicting myocardial ischemiaThe ability to predict hemodynamic alterations thatare likely to result in myocardial ischemia in indi-vidual patients would allow prompt treatment and
avoidance of events initiating ischemia. Unfortu-nately, the diverse nature of myocardial oxygenimbalance in patients leaves the anesthesiolo-gist with no predictor of myocardial ischemiathat is reliable in all circumstances. The indicesdescribed in the next sections all have limitedusefulness.
Rate-pressure product and triple indexThe RPP is the product of HR and systolic BP,whereas the triple index (TI) is the product ofHR, systolic BP, and PCWP. The RPP provides auseful assessment of MVO2 and predicts ischemiain patients undergoing stress testing. Most patientsexperience the onset of ischemia at an RPP of20 000. However, its usefulness in assessing MVO2and predicting ischemia in anesthetized patients isnot reliable. In fact, it is common for a patient underanesthesia to have a low RPP and yet be at highrisk for ischemia (tachycardia and hypotensionwithacute blood loss).The TI is subject to the same criticisms as the
RPP. The addition of PCWP to the product adds thevariable of wall radius to the assessment of MVO2.However, the TI still fails to account for large reduc-tions in myocardial oxygen delivery in the genesisof ischemia.
Myocardial supply–demand ratio(DPTI:SPTI)Efforts to account for beat-to-beat variations in bothmyocardial supply and demand in the genesis ofischemia led to development of the supply–demandratio. In this evaluation, supply is defined by thediastolic pressure time index (DPTI): DPTI = (meandiastolic pressure – LVEDP) × duration of diastole.Demand is defined as the systolic pressure timeindex (SPTI): SPTI = (mean arterial pressure) ×duration of systole. Ratios below 0.5 may result insubendocardial ischemia. Unfortunately, use of thisratio is also unreliable for several reasons:• Increases in MVO2 due to increased contractil-ity are not reflected in BP and HR changes andtherefore are not accounted for by SPTI.• A higher ratio is required in the presence of ane-mia to compensate for the reduced oxygen carryingcapacity of blood.

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 104 — #15
104 Chapter 4
• The presence of pressure drops across coronarystenoses makes the DPTI an unreliable index ofdistal coronary perfusion.• Changes in coronary vascular resistance makeDPTI an unreliable index of distal coronaryperfusion.• Use of the ratio is cumbersome because it requirescalculation of the areas under the diastolic andsystolic pressure curves, respectively.
Mean arterial blood pressure–heart rate(BP–HR) quotientAnimal work demonstrates that ischemia occursin the distribution of a critical coronary stenosisand in collateral-dependent myocardium when thepressure rate quotient (PRQ), defined as mean arte-rial pressure (MAP)/HR, is <1. This relationshipis valid over a wide range of pressures and HRs.An increase in HR can cause or worsen ischemicdysfunction at any mean arterial BP; however, theabsolute HR at which ischemia occurs is dependenton the pre-existing MAP. In other words, higherHRs are tolerated without ischemia at higher MAPs.For patients undergoing coronary revascularization,PRQ < 1.0 has poor sensitivity and specificity inpredicting myocardial ischemia as detected by bothECG and TEE.In summary:• The combination of hypertension and tachycar-dia may result in myocardial ischemia by increasingmyocardial oxygen demand.• The combination of hypotension and tachy-cardia is particularly detrimental to myocardialoxygen balance because it reduces both the timeand the pressure gradient available for myocardialperfusion.• Tachycardia, in and of itself, is detrimental tomyocardial oxygen balance. Experimentally, tachy-cardia causes or worsens ischemic dysfunction atany given mean arterial BP. Clinically, tachycar-dia is associated with the development of ischemiain patients undergoing coronary revascularizationwhereas hypertension per se is not a risk factor.In particular, HRs >110 b/min are associated witha dramatically increased incidence of intraoper-ative ischemia in patients undergoing coronaryrevascularization.
Treatment of ischemiaThe most effective ischemic therapy involvesidentification of the cause of ischemia and tar-geted treatment of this causative factor or factors.In some cases, the specific cause for new ischemiais unclear.
TachycardiaNo single value of HR is uniformly detrimentalto myocardial oxygen balance in a given patient.As already discussed, the HR at which ischemia islikely to occur will vary with mean arterial BP andthe other determinants of myocardial oxygen bal-ance. When an increase in HR results in ischemiaor is likely to result in ischemia, immediate therapyis necessary.Eliminating inadequate anesthetic depth as a
cause is among the first and immediate steps inthe patient undergoing surgery. Preload must beadequate. This is particularly important for patientswith diminished ventricular compliance. In thesepatients, a higher-than-normal end-diastolic pres-sure is necessary to ensure an adequate ventricularEDV. Once anesthetic depth and volume status areeliminated as a cause of the tachycardia, treat-ment with a beta-blocker may be necessary. Manypatients taking beta-blockers preoperatively mayhave plasma concentrations that are too low toblunt the hemodynamic responses to surgery andwill require supplemental medication. Propranololin incremental doses of 0.5–1.0mg IV to a total of0.1mg/kg may be used for patients without severeventricular systolic dysfunction. For patients with ahistory of bronchospasm or reactive airway disease,a β1 selective agent such as metoprolol is useful.Incremental doses of 2.5–5.0mg IV to a total of0.5mg/kg can be used. Because elevations in PCWPwill reduce CPP, concomitant intravenous (IV) ther-apy with nitroglycerin 0.5–1.0µg/kg/min is indi-cated in the presence of an elevated PCWP. Theclinician must titrate drug use against anticipatedor observed hypotension.In some instances, the ultra-short-acting beta-
blocker esmolol may be useful. Esmolol has anelimination half-life of 9minutes due tometabolismby red-cell esterases and is β1 selective. Esmololis started with a bolus of 0.5mg/kg given over

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 105 — #16
Anesthesia for Myocardial Revascularization 105
several minutes followed by an infusion of50µg/kg/min and titrated up to 300µg/kg/minas necessary. In a patient under general anesthe-sia, however, the initial dose should be signifi-cantly reduced (10–50µg). Esmolol is useful inpatients with poor ventricular function or bron-chospastic disease. A striking advantage to thismedication is the short half-life. If the drug ispoorly tolerated, therapy can be quickly termi-nated. Furthermore, unlike longer-acting beta-blockers, esmolol can be used aggressively in thepre-cardiopulmonary bypass (CPB) period with-out fear that it will compromise terminationof CPB.
HypotensionMany patients with coronary disease will toler-ate brief episodes of hypotension without ischemicsequelae, but otherswill not. The extent of hypoten-sion that can be tolerated before ischemia developsis dependent on several variables. For example,a reduction in arterial BP may reduce MVO2by reducing afterload (decreasing demand); how-ever, at the same time, aortic perfusion pressuremay fall to a critical level (decreasing supply).Furthermore, as discussed previously, at higherHRs, hypotension adversely effects perfusion. In anycase, the source of hypotensionmust be quickly andaccurately determined. Determination of CO andsystemic vascular resistance (SVR) will help directtherapy.When hypotension is due to a reduction in
CO, HR and preload should be optimized. Ifthese measures fail to correct the fall in CO, oneshould consider starting an inotrope and eliminat-ing or reducing any inhalational anesthetic agents(eliminating their negative inotropic properties).A fall in SVR can be treated with an α-adrenergicagonist such as phenylephrine in incremental dosesof 40–100µg IV. It should be kept in mindthat α-adrenergic agonists may constrict coronaryarteries with dynamic stenoses and should there-fore be titrated carefully. Because elevations inPCWP will reduce CPP (increasing ventricular walltension), concomitant therapy with nitroglycerin0.5–1.0µg/kg/min is indicated in the presence ofan elevated PCWP.
HypertensionHypertension is classically associated with tachy-cardia in the genesis of myocardial ischemia.Treatment, in this instance, is directed towarddeepening of anesthesia. If hypertension is persis-tent despite adequate anesthetic depth, vasodilatortherapy is warranted. Many agents reduce systemicBP. Sodiumnitroprusside is an easily titrated, potentarteriolar dilator that effectively treats hyperten-sion. An infusion can be started at 0.25µg/kg/minand titrated upward. However, because sodiumnitroprusside is a potent arteriolar dilator, it has thepotential to induce a coronary steal in the presenceof the appropriate anatomy. Another concern isover treating the patient and inducing acute, severehypotension.Nitroglycerin preferentially dilates large coronary
vessels and is not implicated in the steal phe-nomenon. Nitroglycerin has its greatest dilatingeffect on the venous beds and arterial dilatationoccurs only at higher doses. Despite this, when usedin appropriate doses, nitroglycerin and nitroprus-side have been shown to be equally effective intreatment of hypertension associated with coronaryartery bypass surgery. Both agents have comparableeffects on HR, CO, and PCWP. With compara-ble reductions in systolic BP, nitroglycerin causesless reduction in diastolic BP than does nitroprus-side. Therefore, CPP may be better preserved withnitroglycerin thanwith nitroprusside. For these rea-sons, nitroglycerin may be the preferred agent fortreatment of hypertension associated with myocar-dial ischemia. For treatment of hypertension,start nitroglycerin at 0.5µg/kg/min and titrate toeffect.
Dynamic stenosisEvidence of myocardial ischemia may occur withlittle or no initial change in HR or BP. In theseinstances, acute reductions in coronary blood flowmay occur due to vasoconstriction in the area of acoronary stenosis or due to true coronary spasm inan area free of a stenosis. The mainstays of ther-apy are nitroglycerin and calcium channel blockersto reduce coronary vasomotor tone. Nitroglycerincan be started at 0.5µg/kg/min and titrated upward.When an elevated PCWP accompanies the ischemic

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 106 — #17
106 Chapter 4
episode, nitroglycerin effectively reduces PCWPthrough both vasodilation (reducing preload) andtreatment of the underlying ischemia. Nifedipine isa calcium channel blocker and systemic vasodilatorthat can be administered sublingually in a 10-mgdose to reduce coronary vasomotor tone.Systemic hypotension may occur with adminis-
tration of these agents. CPP improves when thepressure drop across the stenosis diminishes withvasodilation in the area of the stenosis and whenvasodilation reduces PCWP. However, extremediastolic hypotension offsets any potential improve-ment of CPP. For this reason, administration ofphenylephrine in addition to nitroglycerin acts topreserves diastolic BP and CPP.
Anesthetic management forCABG surgery
Goals• Avoid increases in myocardial oxygenconsumption.• Avoid tachycardia; it compromises oxygendelivery at any MAP.• Appreciate that the patient’s baseline ischemicpattern will continue into the preoperative andintraoperative periods; these episodes must betreated when recognized.
Preoperative cardiac assessmentPreoperative evaluation is discussed in detail inChapter 1. Careful review of the cardiac catheteriza-tion data is also an essential part of the preoperativevisit. The important features of the catheterizationreport are reviewed here and discussed in detail inChapter 2.
Diastolic functionTo varying degrees, many patients with CAD man-ifest diminished ventricular compliance. In manypatients with diastolic dysfunction, an elevatedLVEDP is necessary for adequate LVEDV. The mea-surement of LVEDP at the time of cardiac catheter-ization will provide some index of the degree ofdiastolic impairment. In addition to diminisheddistensibility, patients with long-standing systemichypertensionmayhave concentric hypertrophy and
diminished ventricular compliance. Patients func-tioning on the steep portion of their diastolicpressure–volume curve will be dependent on awell-timed atrial systole (the A wave in the atrialpressure trace) to adequately fill the ventricle at enddiastole.Echocardiography offers another avenue for eval-
uation of diastolic dysfunction. This noninvasivemodality allows precise quantification of dias-tolic parameters. The function can be character-ized as normal, delayed relaxation, pseudo-normaland restrictive. These quantifications represent acontinuum of disease (Figs 4.9 and 4.10).For patients undergoing repeat coronary revascu-
larization procedures, elevated right heart pressuresincrease the risk of inadvertent right atriotomiesand ventriculotomies during sternotomy. Similarly,if the pericardium was left open after the origi-nal surgical procedure, the anterior surface of theRV is more likely to be adherent to the sternum(Fig. 4.11). The hemorrhage induced by these trau-matic atriotomies, and ventriculotomies can be lifethreatening. A femoral vein and artery are oftenexposed before sternotomy in redo patients so thatpartial bypass can be initiated emergently if hem-orrhage occurs with sternotomy. Partial bypass pro-vides the circulatory support and the decompressionof the right heart that may be necessary for surgicalrepair.
Systolic functionEjection fraction (EF) and assessment of wallmotion are the most commonly obtained assess-ments of systolic function (Fig. 4.12). Because EFis an ejection-phase index, it is dependent on load-ing conditions. For this reason, the presence of alow-impedance outflow tract, such as that whichexists via the mitral valve in mitral insufficiency,will cause the EF to overestimate systolic func-tion. EF is an assessment of global systolic functionand will not be depressed until a relatively largeportion of ventricle exhibits compromised systolicfunction. An EF lower than 40% is abnormal. Wallmotion abnormalities are seen with ventriculogra-phy, advanced magnetic resonance imaging (MRI)or computed tomography (CT) imaging, or com-monly, with echocardiography.When large areas of

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 107 — #18
Anesthesia for Myocardial Revascularization 107
NormalE ≥ A
DT 140–220IVRT 60–100
Transmitralflow velocity
Pulmonary veinflow velocity
Mitral annularvelocity(lateral wall)
NormalS ≥ D
Ar < 25 cm/s
NormalEM/AM> 1
EM> 8cm/s
Mild Dysfunction(Delayed
relaxation)EM ≤ 8cm/s
ModerateDysfunction
(Pseudonormal)EM < 8cm/s
SevereDysfunction(restrictive)EM 8 cm/s
Delayedrelaxation
S > DAr < 25 cm/s
PseudonormalS < D
Ar >25 cm/sLAP increased
RestrictiveS < D
Ar > 25 cm/sLAP increased
DelayedRelaxation
E < ADT>220
IVRT>100
PseudonormalE < A
DT 140–220LAP increased
RestrictiveE A
DT< 140IVRT < 60
Fig. 4.9 Transmitral Doppler imaging, pulmonary view Doppler imaging and tissue Doppler imaging (TDI) profilescorresponding to normal, delayed relaxation, pseudonormal, and restrictive filling patterns. (From Groban L,Dolinski SY. Transechocardiographic evaluation of diastolic function. Chest 2005;128:3652–63, with permission.)
akinesis and dyskinesis exist, systolic function willbe severely compromised.RV EF and wall motion analysis generally are not
obtained at the time of catheterization. For patientswith suspected RV systolic dysfunction, either first-pass or equilibrium noninvasive radionuclear imag-ing can be used to determine EF.
Coronary anatomy and coronary lesionsThe surgeon and anesthesiologist must know theextent of coronary disease and the presence orabsence of collateral flow. This will allow intelligentassessment of the areas most at risk for developingischemia. This knowledge will help guide monitor-ing decisions (i.e. ECGmonitoring selection and TEEwindow).
The coronary angiograms guide the surgeonin target vessel location. Distal disease in smallvessels makes the technical success of the operativeprocedure less likely. Furthermore, bypassinga vessel supplying a dyskinetic or aneurysmal areaof ventricle may yield little in terms of improvedsystolic function postoperatively because such areashave little salvageable myocardium. There arestrong data to suggest that bypassing areas of hiber-nating myocardium result in improved LV func-tion at 1 year after surgery. In some patients, theEF% may dramatically improve from 20 to 40% orbetter.The term “left main equivalent” is commonly
used and deserves clarification. A high-grade leftmain coronary artery lesion potentially jeopardizes

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 108 — #19
108 Chapter 4
EF ≥ 45%
E > AE < A
E/EM≤ 8 8 ≤E/EM≤ 15 E/EM>15 E/EM≤8 8≤E/EM≤15 E/EM>15 E/EM<8 E/EM>15
TDI
Impairedrelaxation
normal fillingpressures
Impairedrelaxation
normal fillingpressures
Dopplerpulmonary
vein
Valsalvaand
mitral inflow
Impairedrelaxation
increased fillingpressures
Impairedrelaxation
increased fillingpressures
Normaldiastolicfunction
Normaldiastolicfunction
Highsuspicion ofpericardial
disease
Restrictivemyocardial
disease
Valsalvaand
mitral inflow
Reversible,restrictive
Fixed,restrictive
E >AE < A
Pseudonormal
And/or
Dopplerpulmonary
vein
Ar wave< 25
Normal Pseudonormal
Ar wave≥ 25
E > AAr wave≥ 25 cm/s
Ar wave< 25 cm/s
E A(unchanged)
Pseudonormal
TDI
E A
= To do= Diagnosis
TDI
DT>140 msDT>140 ms DT< 140 ms
EM> 8 cm/sEM≤ 8 cm/s EM≤ 8 cm/s EM>8 cm/s EM≤ 8 cm/s
Dopplermitral inflow
Fig. 4.10 Algorithm for the assessment of diastolic function in the patient with a normal or near-normal ejectionfraction (EF) (i.e. ≥45%). A, atrial peak velocity; Ar, retrograde velocity; E, early filling peak velocity; EM, early filling;TDI, tissue Doppler imaging. (From Groban L, Dolinski SY. Transechocardiographic evaluation of diastolic function.Chest 2005;128:3652–63, with permission.)
Fig. 4.11 Lateral andposterior/anterior chest radiographs ofa woman presenting for a re-dosternotomy. Note the sternal wires andthe heart adherent to the sternum.This woman has a thoracoabdominalaortic aneurysm.

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 109 — #20
Anesthesia for Myocardial Revascularization 109
(a)
(b)
Fig. 4.12 Systolic function is easily assessed withtransesophageal echocardiography (TEE). (a) Ejectionfraction (EF) is determined by the modified method ofdisk. Capturing the image in both end systole and enddiastole allows the echocardiographer to trace theendocardial border and determine ejection fraction.The EF in this patient is normal (65%). (b) M-modeDoppler allows determination of wall motion andfractional shortening. In this patient, there is significantinferior wall hypokinesis as evidenced by a lack ofthickening and movement during systole. Comparethe thickening and movement of the anterior wall(far field) to that of the inferior wall.
most of the LV muscle mass. Likewise, high-gradestenoses of both the left anterior descending (LAD)and circumflex arteries jeopardize the same ter-ritory. As a result, this combination of lesions isfunctionally the same as a left main lesion; hence,the designation left main equivalent. The differenceis that with the true left main lesion, only one vessel(the left main) must become completely occludedto compromise LV blood flow. In the case of theLAD and circumflex lesions, both vessels wouldhave to be occluded simultaneously to producethe same effect. Another high-risk combination
of lesions occurs when collaterals from a vesselwith a high-grade stenosis supply myocardium dis-tal to an occluded vessel. An example would bemyocardium distal to an occluded LAD suppliedby collaterals from a right coronary artery (RCA)with a high-grade proximal stenosis. In this setting,complete occlusion of the remaining vessel (RCA)compromises most of the LV.For patients undergoing redo procedures, evalua-
tion of the extracardiac conduits (internalmammaryarteries and reverse saphenous veins) is required.These grafts may now have varying degrees ofstenosis. Inadvertent compromise (i.e. transec-tion, laceration, kinking) of these conduits dur-ing the difficult dissection that often accompa-nies a redo procedure may severely compromisemyocardial perfusion. Likewise, surgical manipula-tion of these conduits may result in embolization ofatherosclerotic plaques into the distal coronary vas-cular bed with subsequent transmural myocardialischemia.
PremedicationReassurance and allowing time to address thepatient’s concerns are perhaps the best anxiolytic.This is especially import when one considers therelative risk CABG surgery involves. In the verybest of hands, the risk of mortality is approximately1–3%, and there is a further risk of neurocognitivedeficit, stroke, renal failure and respiratory failure.Our patients are facing a major risk which inducessignificant anxiety. It is our obligation to treat themwith care, compassion and patience.There are a number of safe premedication pre-
scriptions than a clinician may chose. Patients withpreserved ventricular function can be premedicatedwith morphine 0.10–0.15mg/kg intramuscularly(IM), scopolamine 0.005mg/kg IM, and diazepam0.15mg/kg or lorazepam 0.04mg/kg orally (PO)approximately 1.5 hours before scheduled induc-tion time. Alternatively, morphine 0.10–0.15mg/kgIM and midazolam 0.03–0.05mg/kg IM may beused. The dysphoric effects of scopolamine may betroublesome for elderly patients. For elderly patientsor patients with poor ventricular function, the dosescan be reduced and supplemental premedicationcan be given in the operating room holding area

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 110 — #21
110 Chapter 4
under direct observation. Supplemental oxygenwith a face mask should be started at the timeof premedication. Most prudently, premedicationcan be held until the patient arrives in the pre-operative holding area. At this time, the physicianor nurse anesthetist can administer either fen-tanyl or midazolam under direct supervision andobservation.All cardiac medications should be continued
on schedule until the time of surgery. Preop-erative beta-blocker therapy has been shown toblunt the hemodynamic responses to surgical stim-ulation during coronary revascularization and toreduce the incidence of HR-related intraoperativeischemic events. Continuation of preoperative beta-blockade therapy does not compromise myocardialperformance during the post-CPB period. Further-more, abrupt withdrawal of beta-blockade therapyhas been associated with myocardial ischemia,hypertension, and tachydysrhythmias secondaryto a beta-blockade induced increase in β-receptordensity. In fact, continuation of beta-blockers inpatients undergoing surgery who are receiving themedication for angina, symptomatic arrhythmias,hypertension or other ACC/AHA class I indicationscarries a class I level recommendation.Some preoperative medications require addi-
tional comment. Patients treated with diltiazemand nifedipine preoperatively demonstrate a dimin-ished response to phenylephrine. Thus, treatmentof intraoperative hypotension may require higherthan usual doses of phenylephrine for patients con-tinued on preoperative calcium channel blockers.The incidence of perioperative ischemia duringcoronary revascularization is greater in patientsreceiving just calcium channel blockers (nifedipine,diltiazem, or verapamil) preoperatively than inpatients receiving beta-blockers or a combination ofcalcium channel and beta-blockers. This is probablydue to better attenuation of tachycardia-inducedischemia in patients receiving beta-blockers. Theangiotensin converting enzyme inhibiting drugs areassociated with refractory hypotension after CPBin some patients. These medications should beheld on the morning of surgery. If hypotension isencountered, treatment is most effective using IVvasopressin (2 units IV bolus titrated to effect or
an infusion of 2–6units/h). The antiplatelet med-ications pose an unusual management problem.Patients on clopidogrel should have the medicationheld for 3–5 days before elective surgery. Surgeryin patients on clopidogrel is associated with exces-sive bleeding and transfusion of blood and bloodproducts.
PreinductionAfter arrival in the operating room, all patientsshould be attached to an ECG system capable ofmonitoring leads I, II, III, aVR, aVL, AVF, andV5. Baseline recording of all seven leads shouldbe obtained for comparative purposes. Normally,two leads (II and V5) are monitored simultane-ously intraoperatively. However, if the areas ofmyocardium at risk are better assessed in otherleads, then those leads should be monitored.All patients should have a radial arterial
catheter and adequate peripheral IV access (14- or16-gauge). Alternatively, if peripheral IV accessis poor, a peripheral IV suitable for inductioncan be started and a large-bore multilumen (16- or14-gauge) central venous line can be placed at thesame time as the PAC. For patients who are to havean internal mammary artery (IMA) harvested, thearterial waveform obtained in the ipsilateral radialor brachial artery may be compromised during IMAdissection. This occurs when the patient’s arm istucked at the side and is compressed between thebody and the retractor used for IMA dissection. Thisresults in compression of the brachial artery againstthe humerus and is particularly common in largepatients. The arterial line may be placed in the con-tralateral arm or the ipsilateral arm can be abductedto avoid this problem.When the arm is tucked at theside, care should be taken to provide ample paddingbetween the arm and the retractor. Many surgeonsharvest the radial artery for additional arterial con-duit. In these cases, the nonsurgical arm is onlysite available for radial artery cannulation. If can-nulation is impossible, a femoral artery catheter isrequired.The use of PACs for all patients undergoing coro-
nary revascularization is controversial. PACs allowmeasurement of thermodilution CO; pulmonaryartery, right atrial, and PCWPs; systemic and

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 111 — #22
Anesthesia for Myocardial Revascularization 111
pulmonary vascular resistances (PVRs); and LV andRV stroke work. Some PACs monitor continuousCO, mixed venous oxygen saturation, right heartEF, and RV diastolic volume. Analysis of the PCWPand RAP traces may be helpful in the early diag-nosis of ischemia. There are several reviews ofoutcome and pulmonary artery catheterization. It isextremely difficult to demonstrate a benefit in plac-ing a PAC, and in many studies, the PAC is associ-ated with worse outcome. Nonetheless, PAC use iscommon during cardiac surgery.The PAC may be safely placed either before or
after the induction of anesthesia. If placed before,the information can be used during the inductionsequence. However, some patients may experienceundue anxiety, or if sedated, potential respira-tory compromise during line placement. If placedafter induction, the patient will be under gen-eral anesthesia and paralyzed thereby facilitatingrapid and safe placement. As with any central lineplacement, certain precautions are required. Allof the equipment and medications for treatmentof dysrhythmias should be on hand before place-ment of the catheter is attempted. In particular, adefibrillator with demonstrated consistent synchro-nization to the patient’s ECG signal must be in theroom in case cardioversion is necessary. In addi-tion, strict sterile technique is required to reducethe incidence of perioperative line colonization andsepsis.The information obtained at cardiac catheteriza-
tion about LVdiastolic function and LV end-diastolicpressure can be used in conjunction with thePCWP to optimize LV preload. Patientswith reducedcompliance may require a PCWP in the rangeof 12–15mmHg to ensure an adequate preload(LVEDV). When preload is inadequate, SV and COwill be reduced and systemic BP and CPP willbe maintained by increases in SVR. Subsequentreductions in SVR (as with induction) may lead tohypotension and potentially to tachycardia. In thissetting, any advantage of a low PCWP in terms ofCPP is offset by systemic hypotension.For patients with poor systolic function, preload
reservewill be limited or exhausted tomeet baselineCO demands. Any increase in afterload will pro-duce afterload mismatch and result in progressive
reductions in SV and CO. Because poor systolicfunction associated with ischemic heart diseaseis accompanied by reduced diastolic distensibility,maintenance of an adequate preload will requirea PCWP in the range of 12–18mmHg.All episodes of ischemia in the preinduc-
tion period require aggressive therapy. Therapyshould be directed toward the specific cause of theischemic episode. A high proportion of ischemicepisodes are likely to be asymptomatic and to occurin the absence of hemodynamic changes, the ECG,RAP, and PCWP traces are important in diagnosingischemia in these patients.
Induction and maintenanceNo one anesthetic technique is superior to anotherfor patients presenting for coronary artery bypassgrafting. Two types of techniques are discussed:a traditional high-dose narcotic technique and a“fast-track” technique geared toward shorter post-operative ventilation and earlier discharge from theintensive care unit (ICU).
High-dose narcotic techniqueFentanyl and sufentanil generally provide the stablehemodynamics essential in preventing imbalancein myocardial oxygen supply and demand. Theseagents have no effect on myocardial contractilityand cause a reduction in peripheral vascular resis-tance only through a diminution in central sym-pathetic tone. In a high-dose narcotic technique,50–75µg/kg of fentanyl, or 10–15µg/kg of sufen-tanil serve as the primary anesthetic for inductionand maintenance before CPB. A benzodiazepinemust be included to avoid awareness.Sufentanil is associated with greater decreases in
arterial BP and SVR on induction than fentanyl.However, sufentanil is more effective than fen-tanyl in blunting the hypertensive responses toskin incision, sternotomy, sternal spread, and aor-tic manipulation. To avoid hypotension on induc-tion with either narcotic, adequate preload isessential.The choice of muscle relaxant influences the
hemodynamic stability of a high-dose narcotic anes-thetic. Pancuronium has a vagolytic effect as wellas the capacity to enhance sympathetic outflow by

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 112 — #23
112 Chapter 4
blockade of sympathetic postganglionic muscarinicreceptors, inhibition of catecholamine reuptake,and stimulation of release of catecholamine fromnerve terminals. Vecuronium and cisatracurium aredevoid of these effects. Induction with fentanyl–pancuronium provides stable induction hemo-dynamics without ischemia. In some patients,induction with fentanyl–vecuronium or sufentanil–vecuronium results in bradycardia and hypoten-sion. Induction with sufentanil–pancuroniumprovides stable induction hemodynamics and HR.Caution is urged in any case in a patient receiv-ing beta-blocking agents preoperatively. In thesepatients, a high-dose narcotic is more likely to beassociated with significant bradycardia.Preoxygenation is important in cardiac surgical
patients. The induction sequence must be tailoredto the individual patient. A system of graded stimu-lation is used to individualize the narcotic dose foreach patient. After loss of consciousness, the hemo-dynamic response to insertion of an oral airway, fol-lowed by insertion of a urinary catheter, can gaugethe need for additional narcotic to blunt the antic-ipated hemodynamic response to tracheal intuba-tion. If an upward trend in HR or BP is noted duringlaryngoscopy, additional narcotic should be admin-istered. If there is poor visualization of the trachea,laryngoscopy should be terminated and intubatingconditions should be improved by changing headposition, using a stylet, or changing blades. Thisapproach will help prevent long, stimulating laryn-goscopies that compromise hemodynamics. Afterthe airway is secure, the stomach should be evac-uated with an oral-gastric tube, after which, a TEEprobe can be placed.It is sometimes helpful to administer a priming
dose of muscle relaxant prior to the narcotic admin-istration. Vecuronium or pancuronium 0.02mg/kgor cisatracurium0.04mg/kg are appropriate approx-imately 1–2minutes before starting the narcoticinfusion. As the patient loses consciousness, theremainder of the total dose of 0.1mg/kg of vecuro-niumor pancuroniumor 0.2mg/kg of cisatracuriumis administered and controlled ventilation with100% oxygen is initiated. This technique minimizesthe risk of narcotic-induced rigidity without unduestress to the patient.
Bradycardia with hypotension requires prompttreatment. A small dose of pancuronium (1–3mg) isoften effective if vecuronium or cisatracurium hasbeen used. Glycopyrrolate, ephedrine, or atropinemay be appropriate alternatives. Atropine should beused cautiously. Atropine administration may ini-tiate tachycardia. Atropine, unlike β1-adrenergicagents, increases HR without any reduction in theduration of systole. Thus, for equal increases inHR, atropine will cause a greater reduction in theduration of diastole and will compromise suben-docardial perfusion to a greater degree than willa β1-adrenergic agent. Ephedrine (a direct- andindirect-acting β- and α-agonist), 5mg, is a reli-able agent to increase HR without compromisingdiastole. In addition, the augmentation in dias-tolic BP obtained is beneficial when hypotensionaccompanies bradycardia.Tachycardia requires aggressive treatment to
avoid subendocardial ischemia and hemodynamiccompromise. The first strategy should be to termi-nate any noxious stimuli, assure proper intravas-cular volume and increase the depth of anesthesiawhen necessary. Failing this, a short- or long-actingbeta-blocker is usually appropriate therapy.Should hypotension due to reduced SVR occur,
small doses of phenylephrine (40–120µg) andvolume infusion to increase preload to preinduc-tion levels usually will correct the problem. A doseof phenylephrine reliably causes an increase in SVRwith a concomitant increase in wall stress and areduction in ejection phase indices of contractility inCABG patients. The peak effect of a phenylephrinedose occurs 30–40 seconds after injection.If surgical stimulation (skin incision, sternotomy,
sternal spreading, and aortic manipulation) pro-duces hypertension, additional doses of sufentanil(1–5µg/kg) or fentanyl (5–25µg/kg) may be nec-essary. If this fails to control the hypertension, theuse of additional agents will be necessary. As dis-cussed previously, treatment of hypertension withvasodilator therapy must take into account theeffect of these agents on regional myocardial bloodflow and on their ability to improve concomitantischemia.As mentioned, this technique requires the
administration of benzodiazepines and possibly

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 113 — #24
Anesthesia for Myocardial Revascularization 113
inhalational anesthetics to reduce the incidenceof operative recall. Diazepam, midazolam, andlorazepam administered in conjunction with fen-tanyl or sufentanil may decrease peripheral vascu-lar resistance resulting in subsequent hypotension.Therefore, theymust be titratedwith caution.Mida-zolam in increments of 1–2mg or lorazepam inincrements of 0.5–1.0mg are reasonable.Nitrous oxide (N2O), in association with high-
dose opiates, causes systolic dysfunction in patientswith CAD, particularly those with an LVEDP>15mmHg. N2O combined with high-dose opiatesalso elevates PVR, particularly in the presence ofpre-existing pulmonary hypertension. The potentinhalational agents, isoflurane, sevoflurane anddesflurane are safe in patients undergoing coronaryrevascularization. The role of anesthetic precondi-tioning with inhalational agents is discussed later inthis chapter.
Fast-track techniqueThe “fast track” is a comprehensive programdesigned to improve perioperative outcome andreduce costs by reducing hospital stay for patientsundergoing coronary revascularization. Early extu-bation (<8hours) is the hallmark of this program.Anumber of anesthetic techniques allow early extu-bation without increasing the risk of adverse car-diac and noncardiac outcomes. Generally, patientsselected for inclusion in the protocol are low-riskcoronary revascularization patients, but more cen-ters are including all cardiac surgical patients. Riskfactors contributing to prolonged postoperative ven-tilation in coronary revascularization patients arefemale sex, advanced age, congestive heart fail-ure (CHF) requiring preoperative diuretic therapy,and unstable angina. Both the anesthetic tech-nique and the maintenance of normothermia areimportant with this technique; however; the mostimportant element for success in a hospital sys-tem is the adoption of a “fast-track extubationprotocol.” Using such a protocol identifies appro-priate patients, alerts the care team of the clini-cal pathway, and facilitates a scheduled weaningprocess.The following is an example of a fast-track pro-
tocol. There are many approaches, however, and
the clinician will soon master a technique suitablefor his or her practice.• Premedication with midazolam 1–2mg IV in thepreoperative holding area.• Fentanyl 15–20µg/kg and etomidate 0.20–0.30mg/kg for induction in combination withcisatracurium or vecuronium. The considerationsused in choosing a relaxant are the same used inthe high-dose narcotic technique.• Maintenance of anesthesia with isoflurane0.5–1.0%.• Either Propofol 75–100µg/kg/min, or isofluraneis administered while on CPB.• Intermediate-acting neuromuscular blockingagent (Fig. 4.13).
RocuroniumPancuronium
120
100
80
60
40
20
0
TOF
fade
rat
io
0 1 2Hours
Postoperative recovery
Variable Rocuronium
90 (40–315)335 (185–1290)0.99 (0.87–1.21)
180 (50–180)460 (225–1350)0.14 (0.00–1.11)
<0.05<0.05<0.05
Pancuronium P value
Duration of ventilatory weaning (min)ICU arrival until extubation (min)TOF ratio at initiation of ventilatory weaning
Data are median (range).ICU, intensive care unit; TOF, train-of-four.
3 4
Fig. 4.13 The use of pancuronium (0.08–0.10mg/kg) orrocuronium (0.6–0.8mg/kg) was evaluated in 82 patientsundergoing coronary artery bypass grafting surgery. Thebar graph shows the train-of-four ratios were measuredupon arrival to the intensive care unit and then eachhour for the next 4 hours. Significant differences werenoted between groups at all time intervals (P < 0.05).The postoperative recovery profiles are shown below inthe figure. Data are median (range). ICU, intensive careunit; TOF, train-of-four. (From Murphy GS, Szokol JW,Marymont JH et al. Recovery of neuromuscular functionafter cardiac surgery: pancuronium versus rocuronium.Anesth Analg 2003;96:1301–7, with permission.)

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 114 — #25
114 Chapter 4
• Post-CPB, the isoflurane is maintained andno additional narcotic is administered. Eitherpropofol, 20–50µg/kg/min or dexmedetomidine0.1–0.7mg/kg/min is started prior to transport tothe ICU.
Off-pump coronary artery bypassgraftingOff-pump coronary artery bypass (OPCAB) graftsurgery offers an alternate technique to traditionalon-pump CABG. Advantages of this techniqueinclude potentially decreased postoperativemorbid-ity in some patients and reduced resource utilizationand total cost. CPB is avoided in this technique, andtherefore, so are all of the potential problems withmyocardial preservation. Various investigators havedemonstrated better myocardial energy preserva-tion, less oxidative stress, and minimal myocar-dial damage with this technique. New advances inmyocardial stabilizing devices allow a still opera-tive field and excellent surgical conditions (themainadvantage of CABG with cardioplegia and a flac-cid heart). There are several reports in the literaturecomparing outcome between on-pump CABG andOPCAB. As expected, the results vary; however, itappears that there is no difference in outcome in lowrisk patients with either technique (Fig. 4.14). Thereis a consistent cost savings with OPCAB. The anes-thetic management of these patients is strikinglydifferent from traditional on-pump CABG. Thesedifferences are reviewed below.In contrast to on-pump CABG, brief periods of
ischemia are necessary during the operative pro-cedure. These ischemic periods may be reducedin some patients with the placement of a tempo-rary coronary stent, however, there remains sometime of interrupted blood flow. The ischemic bur-den is usually of such short duration, that there islittle risk of significant long-term damage; however,there may be some element of stunning and imme-diate myocardial dysfunction. In addition, theremay be a cumulative global dysfunction after severalsequential occlusions in multiple graft procedures.In fact, it is common for a patient to toleratea one-or-two vessel OPCAB bypass, but a three-or-four-vessel procedure often results in signifi-cant support required to complete the procedure.Because ischemia is anticipated, monitoring for
P = 0.48
On pump (90.6%)
Off pump (88.0%)
1.00
0.98
Eve
nt-f
ree
surv
ival 0.96
0.94
0.92
0.90
0.88
0.860
0 60 120
Days since randomization
No. at riskOn pumpOff pump
139142
130132
128 131
127 128
127 127
127 126
126125
180 240 300 360
Fig. 4.14 Kaplan–Meier estimates of survival free fromstroke, myocardial infarction, and repeated coronaryrevascularization. P = 0.48 by log-rank test. Results froma multicenter, randomized evaluating off pump coronaryartery bypass grafting to traditional on-pump coronaryartery bypass grafting. In this investigation, 139 patientswith single or double vessel coronary disease wererandomly assigned to on-pump surgery and 142 patientsto off-pump surgery. At 1 year, the rate of freedom fromdeath, stroke, myocardial infarction and coronaryreintervention was 90.6% after on-pump surgery and88.0% after off-pump surgery (absolute difference, 2.6%;95% confidence interval, −4.6−9.8). The graft patencywas similar between groups. On-pump surgery wasassociated with $1839 in additional direct costs perpatient compared to off-pump surgery. (FromNathoe HM, van Dijk D, Jansen EW et al. A comparisonof on-pump and off-pump coronary bypass surgery inlow risk patients. N Engl J Med 2003;348:394–402, withpermission.)
significant ischemia is essential. During the occlu-sion and anastomoses, the anesthesiologist shouldmonitor the appropriate ECG leads highlighting thetarget area, the TEE for new RWMA, continuousCO, and mixed venous oxygen saturation. It isimportant to note that OPCAB procedures requireextensive positioning of the heart, and this posi-tioning changes the observedmonitoring (especiallyTEE windows); nonetheless, following trends willallow the clinician opportunity to intervene whenappropriate in these complex procedures.OPCAB procedures are associated with hemo-
dynamic instability. These hemodynamic changes

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 115 — #26
Anesthesia for Myocardial Revascularization 115
may be secondary to the ischemic episodes aswell as the positioning requirements of the heartand resultant preload alterations. In general, main-taining systemic BP (and, hence, CPP) is essen-tial. Techniques to maintain BP include adequatevolume loading prior to ischemia, Trendelenburgposition, norepinephrine or phenylephrine infu-sions, and atrial pacing if bradycardia occurs.Placement of a coronary stent allows blood flowduring much of the anastomoses and is helpful inreducing ischemic time. Occasionally, the patientmay require inotropic support during the OPCABprocedure. In some patients, ischemic mitral regur-gitation develops of worsens with heart manipula-tion, positioning and ischemia. In addition to thesteps outlined above to support the systemic BP,milrinone may be effective in this circumstance.Obviously, the quicker the operative procedure andthe less time the heart is ischemic, the better thepatient will tolerate the procedure. One last cau-tion involves the occurrence of sudden, significantdysrhythmias during OPCAB. Occasionally, uponreperfusion, the heart may respond with multi-focal premature contractions, ventricular tachy-cardia, or even ventricular fibrillation. Awarenessof this potential and prompt intervention for fib-rillation is essential. In most cases, the ventriculardysrhythmias are self-limiting.There are many potential methods to reduce
the impact of the obligate ischemic insult. Main-taining a normal acid-base balance and electrolyteprofile are important. In addition, pharmacologicinterventions may include nitroglycerin infusion,magnesium supplementation, use of calcium antag-onists (with the anticipated ischemic-reperfusioninjury and possible calcium overload), tight glu-cose control, and choice of anesthetic and ischemicpreconditioning.
Ischemic preconditioning andanesthetic preconditioningIschemic preconditioning is process whereby short,transient periods of tissue ischemia render the tissueresistant to subsequent usually lethal periods ofischemia. This process exists in many organ systemsin the body including the heart, kidneys, lungs,brain and spinal cord. In the myocardium, ischemiaresults in an immediate reduction in contractile
effort, with cellular death ensuing after approxi-mately 15minutes. If the ischemic episode is pre-ceded by one or more sub-lethal ischemic episodes,the myocardium is altered in such a way as to limittissue injury and prolong the interval of ischemictolerance. In experimental models, infarct size ismeasured with and without ischemic precondition-ing. With ischemic preconditioning, the infarct sizeis approximately 25% smaller. This protective ben-efit is seen immediately after the preconditioningevent, and again at 24hours (a “second window”of protection). There are several proposed mecha-nisms for both acute and late preconditioning. In theacute phase, the preconditioning involves an alter-ation of the Katp channel. Late protection involvesheat shock protein synthesis.Several pharmacologic agents can induce ischemic
preconditioning like effects. Recent work sug-gests that some anesthetic agents may possesspharmacologic ischemic preconditioning properties.Anesthetic preconditioning (APC) is defined as theadministration of a volatile anesthetic before theperiod of myocardial ischemia. In animal studies,contractility is preserved and infarct size is reducedapproximately 40%. The mechanism of the APCeffect is likely multifactorial and includes preser-vation of adenosine triphosphate (ATP) and highenergy phosphates, decreased polymorphonuclearneutrophil (PMN) adhesion during reperfusion,reduced calcium loading and alteration of the Katpchannel (Fig. 4.15).There are compelling animal data in multiple
studies affirming the anesthetic preconditioningeffects of the volatile anesthetics. In clinical prac-tice, the data remains indirect and there is currentlyno clear translated therapeutic approach utiliz-ing APC. Anesthetic preconditioning is difficultto demonstrate clinically because of the compli-cated patient scenario, the hemodynamic alter-ations during surgery, and the uncontrolled mix ofanesthetic, analgesics and vasoactive medicationsused during surgery. In vitro, isoflurane, sevoflu-rane, and desflurane all enhance muscle recov-ery in atrial tissue after an ischemic-reperfusionevent. Isoflurane immediately before aortic cross-clamping in patients undergoing CABG decreasesthe troponin I and creatine kinase-MB releasepostoperatively. There is reduced ST segment

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 116 — #27
116 Chapter 4
G-protein-coupledreceptors
Volatileanesthetics
Volatileanesthetics
Extracellular
G
PKC
ROS
K+
K+
Fig. 4.15 Multiple endogenous signaling pathwaysmediate volatile anesthetic-induced myocardialprotection. A trigger initiates a cascade of signaltransduction events, resulting in the activation of anend-effector that promotes resistance against ischemicinjury. Mitochondrial adenosine triphosphate-sensitivepotassium (KATP) channels have been implicated as theend-effector in this protective scheme, but sarcolemmalKATP channels may also play a role. Volatile anestheticssignal through adenosine and opioid receptors, modulateG proteins, stimulate protein kinase C (PKC) and other
intracellular kinases, or have direct effects onmitochondria to generate reactive oxygen species (ROS)that ultimately enhance KATP channel activity. Volatileanesthetics may also directly facilitate KATP channelopening. Dashed arrows delineate the intracellular targetsthat may be regulated by volatile anesthetics; solid arrowsrepresent potential signaling cascades. (From Tanaka K,Ludwig LM, Kersten JR et al. Mechanisms ofcardioprotection by volatile anesthetics. Anesthesiology2004;100:707–21, with permission.)
changes and preservation of cardiac index com-pared to inpatients who did not receive pre-treatment with a volatile anesthetic. In off-pumpCABG, patients randomized to sevoflurane had lesstroponin I release compared to those randomized topropofol.In summary, ischemic preconditioning and anes-
thetic preconditioning are new and exciting areas ofinvestigation. The full clinical impact of these phys-iologic and pharmacologic mechanisms remains tobe determined.
Intrathecal and epidural anesthesia andanalgesia for cardiac surgeryPain after cardiac surgery may be severe and limitpatient recovery. Traditionally, pain treatment iswith IV opioids; however, there is recent interest
in advanced techniques of pain control includingintrathecal and epidural analgesia. In the acutesetting, pain is largely surgical in origin; persistentpain may be due to tissue destruction, intercostalnerve trauma, rib fractures, wound infection, thesternal wires, or nonunion of the sternum. Thetechniques for postoperative analgesia are manyincluding local anesthetic infiltration, nerve blocks,opioids, nonsteroidal anti-inflammatory agents,α-adrenergic drugs, and intrathecal and epiduraltechniques. Each technique has unique advantagesand disadvantages.Intrathecal analgesia has beenwidely investigated
since the 1980s. Intrathecal opioids (morphine, fen-tanyl, sufentanil) reliably extend the duration ofanalgesia without significant impact on extubationtimes. The addition of clonidine to the opioid further

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 117 — #28
Anesthesia for Myocardial Revascularization 117
enhances the opioid effect. Some authors haveadministered hyperbaric bupivacaine (20–30mg),hyperbaric lidocaine (150mg), or both with mor-phine to induce a “total spinal” and completethoracic cardiac sympathectomy. This techniquereduces β-receptor dysfunction and lowers the stressresponse (as measured by circulating epinephrine,norepinephrine and cortisol levels) during CABGsurgery. As predicted, the fall in HR and BP inthe majority of these patients required pharmaco-logic intervention. The role of total spinal anesthesiafor CABG is controversial and remains undefinedat this time. In summary, although safe, intra-thecal administration of analgesics reliably producesanalgesia, however, there is no additional clinicalbenefit.The same is true of epidural analgesia. Multiple
clinical reports demonstrate that thoracic epiduralanalgesia is associated with good pain control, butthere is limited benefit beyond this single measure.For both intrathecal and epidural techniques, thereis no evidence of improved outcome in mortalityor MI.Both techniques carry risk. Hypotension is com-
mon and can be significant. Administration oflocal anesthetics always carries the risk of IVabsorption and myocardial depression. Dense anal-gesia may mask postoperative myocardial ischemia.Neuroaxial opioids are associated with pruritus,nausea and vomiting, urinary retention, and res-piratory depression. Finally, and perhaps mostconcerning, is the risk of spinal hematoma for-mation. The incidence of hematoma formation isapproximately 1:220 000 for intrathecal instrumen-tation and 1:150 000 for epidural instrumentation.This risk increases in the cardiac surgical patientbecause of the systemic heparinization; however,it is difficult to quantify this risk.In summary, intrathecal and epidural techniques
are practiced in some hospitals with good results.The data affirm reliable analgesia, but there is noimprovement in mortality or MI. Other parame-ters, such as dysrhythmias, respiratory failure andearly extubation may be improved with regionaltechniques (Table 4.3). There remains significantcontroversy regarding the role of these techniquesin adult cardiac surgical practice.
Glucose management duringcoronary artery bypass surgeryRecent data suggest that tight perioperative controlof blood glucose in diabetic patients improvesoutcome after cardiac surgery (Fig. 4.16). Hyper-glycemia has several adverse effects on the heartafter an ischemic-reperfusion injury. In animalmodels, blood glucose correlates with infarct sizeand the beneficial effects of ischemic precondi-tioning are abolished with hyperglycemia. Further,hyperglycemia reduces coronary collateral bloodflow through a nitric-oxide-mediated mechanism.Effective treatment with insulin during the peri-operative period is enhanced with a continuousinfusion of insulin as compared to intermittentbolus insulin. Most agree that maintaining a glucoselevel <200mg/dL is appropriate. Some evidencesuggests that insulin therapy should be initiatedwhen the glucose level is >110–150mg/dL.
Emergency coronary arterybypass surgeryAnesthesia for emergency coronary artery bypasssurgery provides some unique challenges. Thesepatients typically are those suffering from complica-tions of cardiac catheterization or of catheter-basedinterventional techniques to treat coronary stenosis.Patients presenting with failed coronary angioplastyprocedures fall into three categories:1 Hemodynamically stable, nonischemic patients.Some of these patients will have sustained noendothelial damage and can be managed as electivecoronary revascularization patients. Some patientswill have sustained endothelial damage and are atrisk for subsequent thrombus formation and vesselclosure. These patients may require surgical revas-cularization but can afford to wait several hours.This is time enough to complete a comprehensiveanesthetic evaluation and to allow further gastricemptying if necessary.2 Hemodynamically stable, ischemic patients. Thesepatients require urgent revascularization. Theischemic interval should be limited to <3hoursto avoid infarction. An intra-aortic balloon pumpmay be in place to temporize this condition. Anes-thetic evaluation should be concise and focused.Communication with the cardiologist is essential to

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 118 — #29
118 Chapter 4
Table 4.3 Outcomes for thoracic epidural analgesia (TEA) and intrathecal analgesia (IT) versus general anesthesia(GA) for cardiac surgery. A meta-analysis of 15 trials enrolling 1178 patients having neuroaxial analgesia aftercardiac surgery demonstrates no differences in the rates of mortality or myocardial infarction after coronary arterybypass grafting with central neuroaxial analgesia. There were associated improvements in faster time until trachealextubation, decreased pulmonary complications and cardiac dysrhythmias in reduced pain scores. The majority ofthese benefits, however, may be reduced or eliminated with changing cardiac practice using fast track techniques,use of beta-blocking agents, amiodarone, or nonsteroidal anti-inflammatory drugs for postoperative analgesia.(From Liu SS, Block BM, Wu CL. Effects of perioperative central neuraxial analgesia on outcome after coronaryartery bypass surgery. Anesthesiology 2004;101:155–61.)
Outcome No. TEA GA OR or WMD(95% confidence interval)
P-value
Death 1178 0.7% 0.3% 1.56 (0.35–6.91) 0.56Myocardial infarction 1026 2.3% 3.4% 0.74 (0.34–1.59) 0.44Dysryhthmias 913 17.8% 30% 0.52 (0.29–0.93) 0.03Pulmonary complications 644 17.2% 30.3% 0.41 (0.27–0.60) <0.00001Time to tracheal extubation (h) 905 6.9∗ 10.4∗ −4.5 (−7 to −2) 0.0005VAS pain score at rest (mm) 392 12.4∗ 19.6∗ −7.8 (−15 to −0.6) 0.03VAS pain score with activity (mm) 222 14∗ 27.6∗ −11.6 (−19.7 to −3.5) 0.005Death 668 0.3% 0.6% 0.88 (0.13–5.72) 0.89Myocardial infarction 290 3.9% 5.7% 0.75 (0.24–2.31) 0.61Dysryhthmias 204 24.8% 29.1% 0.81 (0.42–1.53) 0.51Time to tracheal extubation (h) 588 10.4∗ 10.9∗ −0.85 (−1.83 to 0.12) 0.09Time to tracheal extubation forsmall-dose IT (h)
189 7.1∗ 9.3∗ −1.2 (−1.8 to −0.7) <0.0001
Morphine use per day (mg) 816 14∗ 22∗ −11 (−15 to −7) <0.00001VAS pain score (mm) 315 13.4∗ 23.4∗ −16 (−27 to −4.9) 0.005Pruritus 506 10.1% 2.5% 2.9 (1.2–6.7) 0.01Nausea/vomiting 490 31.3% 28.5% 1.27 (0.81–2.0) 0.3
Random effects model used for all analyses.∗Weighted by number of subjects.GA, general anesthesia; IT, intrathecal analgesia; OR, odds ratio; TEA, thoracic epidural analgesia; VAS, visual analogscale; WMD, weighted mean difference (inverse variance method).
determine the extent of jeopardized myocardium,current vasoactive agents, anticoagulation methods(heparin, streptokinase, tissue plasminogen activa-tor (tPA), clopidogrel, and abciximab), NPO status,current laboratory values, and vascular access. Thearterial access used for the catheterization proce-dure (femoral artery) should be left in place andused for monitoring in the operating room. Femoralvein sheaths can be used for venous access. A PACis commonly placed via the femoral vein and can beused as well. Induction can be accomplished eas-ily and safely using the high-dose narcotic tech-nique described previously. For patients deemed at
high risk for aspiration, a nonparticulate antacid andmetoclopramide 10–20mg IV can be administered.A rapid sequence induction can be accomplishedwith etomidate 0.15–0.30mg/kg and succinyl-choline 1.0–1.5mg/kg, in conjunction with fen-tanyl (10µg/kg) or sufentanil (1µg/kg). Etomidateproduces minimal cardiovascular effects at thisdosage when administered in conjunction withnarcotics. Alternatively, sufentanil 5µg/kg and suc-cinylcholine 1.0–1.5mg/kg can be used in a rapid-sequence technique. Hypotension and ischemiamust be aggressively treated. After induction, place-ment of additional intravascular catheters can be

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 119 — #30
Anesthesia for Myocardial Revascularization 119
70
60
50
40
30
20
10
0Total CV Resp.
Poor intraoperative glycemic control
Tight intraoperative glycemic control
% o
f pat
ient
s w
ith m
orbi
dity
Inf. Renal Neuro. Others
∗
∗
∗
∗ ∗ ∗
Fig. 4.16 Incidence of severe in-hospital morbiditybetween patients in whom intraoperative glycemiccontrol was poor or tight. Two hundred consecutivediabetic patients undergoing on-pump heart surgerywere enrolled. A standard insulin protocol based onsubcutaneous intermediary insulin was given themorning of the surgery. Intravenous insulin therapy wasinitiated intraoperatively from blood glucoseconcentrations of 180mg/dL or greater and titratedaccording to a predefined protocol. Poor intraoperativeglycemic control was defined as four consecutive bloodglucose concentrations >200mg/dL without any decreasein despite insulin therapy. Postoperative blood glucoseconcentrations were maintained below 140mg/dL byusing aggressive insulin therapy. The main endpointswere severe cardiovascular, respiratory, infectious,neurologic, and renal in-hospital morbidity. Insulintherapy was required intraoperatively in 36% of patients,and poor intraoperative glycemic control was observed in18% of patients. Poor intraoperative glycemic controlwas significantly more frequent in patients with severepostoperative morbidity (37 vs. 10%; P < 0.001). Theadjusted odds ratio for severe postoperative morbidityamong patients with a poor intraoperative glycemiccontrol as compared with patients without was 7.2(95% confidence interval, 2.7–19.0). CV, cardiovascularmorbidity; Inf., infectious morbidity; Neuro., neurologicmorbidity; Resp., respiratory morbidity (see text fordefinitions of different morbidities). ∗P < 0.05 vs. tightcontrol. (From Ouattara A, Lecomte P, Le Manach Y et al.Poor intraoperative blood glucose control is associatedwith a worsened hospital outcome after cardiac surgeryin diabetic patients. Anesthesiology 2005;103:677–94,with permission.)
accomplished in parallel with the surgical prepara-tion. In particular, a PAC can be placed via the rightinternal jugular vein. This substantially improvesthe ability to manipulate and position the PACand to infuse vasoactive agents at a proximal site.
The femoral vein PAC often is not in a sterilesheath and is distant from the head of the bed. Ifperipheral venous access is poor, a large-bore dou-ble lumen (16- or 14-gauge) central venous linecan be placed at the same time as the PAC. Becausethese patients usually are anticoagulated with atleast heparin, placement of these catheters usingultrasonic guidance should be considered.3 Hemodynamically unstable, ischemic patients.These patients require emergent revascularization.Evaluation must often be performed in the hallwayon the way to the operating room. Communicationwith the cardiac catheterization team is essential.Some of these patients are mildly hypotensive,requiring minimal cardiovascular pharmacologicsupport; whereas, others may be intubated andreceiving cardiopulmonary resuscitation (CPR). Thegoal is to establish CPB as expeditiously as possible.Vascular access for monitoring and volume infusioncan be obtained on the surgical field if necessary.All existing intravascular access should be used.For more stable patients, the induction techniquesdescribed above are applicable. For patients receiv-ing CPR, scopolamine 0.005mg/kg or midazolam0.05–0.1mg/kg in conjunction with a nondepolar-izing muscle relaxant may be all that is necessary.Although the in-hospital mortality is high (approxi-mately 50%), there are good data demonstrating abenefit to emergency surgical intervention (surgeryor angioplasty) versus initial medical stabilization inpatients presenting in cardiogenic shock after a MI(Fig. 4.17).
Post-CPB managementThe assumption that coronary revascularizationwillproduce a patient with normal myocardial func-tion after CPB is erroneous. Immediate improve-ments in LV systolic and diastolic function mayoccur within the first 10minutes after terminationof CPB; however, many patients require inotropicand vasoactive support. There may be depression ofboth RV and LV systolic function (reduced EF, LVstroke work index (SWI), cardiac index (CI)) withthe nadir occurring approximately 4hours aftertermination of CPB.Coronary revascularization may be less than
complete for technical reasons, such as occurs with

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 120 — #31
120 Chapter 4
100
80
60
Per
cent
age
40
20
0IMS ERV
2 weekspost-discharge
6 monthspost-MI
1 yearpost-MI
IMS ERV IMS ERV
Fig. 4.17 Outcome of 126 SHOCK trial hospitalsurvivors with at least one interview, 69 assigned to theemergency revascularization (ERV) group and 57assigned to the initial medical stabilization (IMS) group.There were significant differences between treatmentgroups at 6months (P = 0.035) and 1 year (P = 0.014).White bars = New York Heart Association (NYHA)functional class I/II; ruled bars = NYHA functional classIII/IV; black bars = deceased. MI, myocardial infarction.(From Sleeper LA, Ramanathan K, Picard MH et al.Functional status and quality of life after emergencyrevascularization for cardiogenic shock complicatingacute myocardial infarction. J Am Coll Cardiol2005;46:266–73, with permission.)
small distal vessels. Communication with the sur-geon is necessary to determine the success of theoperative procedure. The sense of security thataccompanies a “successful” operative proceduremust be temperedwith the knowledge that a signifi-cant number of patients (35–50%) continue to haveevidence of myocardial ischemia in the post-bypassperiod after apparently successful revascularization.Most episodes occur in the immediate (0–8hours)postoperative period. The development of post-CPB RWMA and the development of ECG-detectedischemia in the immediate postoperative period areboth associated with adverse clinical outcome.There may be alterations in the vascular tone
of the native coronary circulation during the post-CPB period. Coronary vasospasm may occur distalto bypass grafts or in segments of artery that havenot been bypassed. This usually is heralded by thepresence of elevated ST segments in the absenceof a precipitating hemodynamic event. Spasm iseffectively treated with IV nitroglycerin.Vasoactive substances used during the post-CPB
period may affect flow through the IMA and
saphenous vein grafts. In humans, infusion ofepinephrine to increase systemic BP during thepost-CPB period increases IMA graft flow, nore-pinephrine infusion does not change IMA graftflow, and phenylephrine infusion reduces IMAgraft flow. Some animal models suggest that suchchanges are due to the effects of vasoactive sub-stances on IMAvascular tone,whereas others impli-cate changes in systemic BP. In humans, vasopressorassociated increases in systemic BP are accompa-nied by increases in saphenous vein graft flows.Additional work is required to determine moreprecisely how changes in graft vascular resistance,systemic BP, and myocardial oxygen consumptioncontribute to these flow variations. Nonetheless, itshould be kept in mind that the choice of vasopres-sor may affect flow through engrafted arteries andveins.Inadequate myocardial protection during the
procedure will adversely affect LV systolic function.This is particularly likely if the patient has suffereda preoperative ischemic event or has poor preop-erative ventricular function. In these patients, opti-mization of preload and HR are necessary first stepsin obtaining hemodynamic stability. Patients withcompromised systolic function are often dependenton HR for increases in CO. In addition, patients withreduced ventricular compliance and distensibilitywill be dependent on atrial systole to provide an ade-quate LVEDVwithout a highmean PCWP. For thesereasons, pacing of the atrium (with intrinsic con-duction via the atrioventricular (AV node) or of theatrium and ventricle (when AV nodal dysfunctionexists) may be necessary.Attention to the metabolic condition of the
patient is required in the postoperative period.These patients often require electrolyte supplemen-tation (potassium and magnesium), as well as strictventilatory management to control acid-base bal-ance in the immediate hours after CABG. Thereare significant issues regarding continued ther-mal regulation, coagulation and glycemic control.There is a growing body of research in the areaof strict glycemic control. Several authors havepublished data suggesting that tight control of glu-cose (110–150mg/dL) is associated with superioroutcome in both critically ill patients and those

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 121 — #32
Anesthesia for Myocardial Revascularization 121
after CABG. A regular insulin infusion (2–8units/h)is indicated when the glucose is >150mg/dL.Optimization of preload after termination of CPB
requires careful attention and is facilitated by useof TEE and the PCWP and CVP. Preload reserve(preload recruitable stroke work) can be assessedby infusion of blood from the CPB circuit in incre-ments of 10–15mL/kg (“give a hundred”). Oneof three distinct hemodynamic responses will beobserved:• Intact preload reserve. Infusion of volume producesan increase in MAP with little or no change inPCWP or CVP. TEE demonstrates normal LV andRV chamber volume. CO increases. For this subsetof patients, further infusion of volume to improvehemodynamics is warranted.• Optimized preload. Infusion of volume produces lit-tle or no change in MAP with no change or a smallincrease in PCWP or CVP. TEE demonstrates a LVor RV at the upper limits of size for the particularpatient. Obviously, pre-CPB assessment of LV andRV dimensions is necessary to take full advantage ofthis modality. CO may increase slightly or remainunchanged. For this subset of patients, no furtherinfusion of volume to improve hemodynamics iswarranted.• Exhausted preload reserve. Infusion of volume willproduce no change or a fall in MAP with a substan-tial increase in PCWP or CVP. TEE will demonstratea distended LV or RV. CO may decrease slightlyor should remain unchanged. For this subset ofpatients, no further infusion of volume to improvehemodynamics is warranted. Initiation of inotropicsupport will improve hemodynamics and reduceventricular dimensions.Several risk factors are associated with an
increased incidence of inotropic agent use afterCPB. Factors related to inotrope use include lowEF<55%, older age, cardiac enlargement, femalesex, and higher baseline and post-contrast LVEDP.For patients with an EF>55%, the presence ofpreoperative wall motion abnormalities and anincrease of >10mmHg in LVEDP with contrastinjection is associated with the need for inotropes.In addition, for patients with an EF > 45%, pro-longed duration of CPB is associated with the needfor inotropes.
The most commonly used inotropic agents aredescribed below. Use of inotropic agents post-CPBshould be used with the knowledge that both adultsand children exhibit uncoupling of β-adrenoceptorsfrom the Gs-protein-adenylate cyclase complexafter CPB. This desensitization may contribute to arelative catecholamine resistance in the post-CPBperiod.
DopamineDopamine possesses β1-adrenergic, α1-adrenergic,and dopaminergic activities. Some of the α activ-ity is due to release of endogenous norepinephrine.At doses of 2–3µg/kg/min, the dopaminergic activ-ity is maximal, resulting in preferential dilationof renal, mesenteric, and coronary vasculature.Alpha-agonists do not antagonize this dopaminer-gic activity. This makes dopamine a useful agentfor preservation of renal blood flow in the pres-ence of α-agonists. β1-Induced enhanced inotropyoccurs at doses between 1 and 10µg/kg/min; how-ever, at doses above 4–6µg/kg/min dopamine’sα-adrenergic activity increases such that SVR, PVR,and PCWP increase with little concomitant increasein CO. This combination of increased ventricularwall radius and afterload may cause detrimen-tal increases in myocardial oxygen consumption.At doses >10µg/kg/min, the α-adrenergic effectsof dopamine predominate, producing vasoconstric-tion. Dopamine’s chronotropic and dysrhythmiceffects increase as the dose increases.
DobutamineDobutamine possesses β1-, β2-, and α1-adrenergicactivities. The predominant effect is enhancedinotropy through βl stimulation. The β2 and α1activities are balanced such that mild vasodi-lation occurs at the commonly used dosesfrom 5–20µg/kg/min. Dobutamine decreases PVR,blunts hypoxic pulmonary vasoconstriction, andincreases coronary blood flow. Dobutamine mayactually reduce myocardial oxygen consumption inthe failing heart. Although dobutamine increasescontractility, it reduces LV radius and end-diastolicpressure while increasing arterial pressure andmaintaining HR. Dobutamine is less likely to causetachycardia than dopamine.

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 122 — #33
122 Chapter 4
EpinephrineEpinephrine possesses β1-, β2-, and α1-adrenergicactivities. At doses of 1–3µg/min, epinephrine hasa potent inotropic effect mediated through β1 stim-ulation, with little effect on vasomotor tone due tothe balance of β2 and α1 stimulation. As thedose increases above 3µg/min, progressively moreα1 activity occurs, with resultant mixed inotropicand vasoconstrictive effects. Doses above 3µg/minalso cause progressive decreases in renal blood flow.Above 10µg/min, epinephrine is primarily a vaso-constrictor. Epinephrine’s vasoconstrictive effectsalso reduce venous capacitance. Although coronaryblood flow is maintained, epinephrine may not befavorable to myocardial oxygen balance, because inaddition to increasing contractility, it increases sys-tolic BP, increases LVEDV and pressure, and reducesdiastolic BP while increasing HR.Epinephrine is often the agent of choice to ter-
minate CPB. The potent inotropic and balancedperipheral vascular effects allow prompt, reliabletermination of CPB while avoiding the ventriculardistension and systemic hypotension that compro-mise subendocardial perfusion. Critics point outthat the potent inotropic effects of epinephrinemay not be necessary in every instance, and thus,epinephrine’s potentially deleterious effects on themyocardial and renal blood flow can be avoided ifanother agent is selected.
NorepinephrineNorepinephrine possesses βl- and α1-adrenergicactivity. The α1 effects of norepinephrine are man-ifest at low doses (1–2µg/min) and predominate asthe dose increases. Norepinephrine reduces renalblood flow, elevates both systolic and diastolicBP, reduces venous capacitance, and generallycauses a reflex decrease in HR. Although coro-nary blood flow is maintained, norepinephrine maynot be favorable to myocardial oxygen consump-tion, because there is increased contractility andafterload.
MilrinoneMilrinone is a potent inotropic agent that acts byinhibiting phosphodiesterase III (PDE III) to increaseintracellular cyclic adenosine monophosphate
(cAMP). In addition, milrinone possesses vasodila-tor activity by virtue of PDE III inhibition in vascularsmooth musc1e. Milrinone increases cardiac index,reduces LVEDP and LVEDV, reduces systolic BP,and has little effect on HR. Like dobutamine in thefailing heart, this increase in cardiac index may beassociated with a decrease in myocardial oxygenconsumption due to the concomitant reduction inwall stress. Milrinone reduces PVR.Milrinone does not act via βl-receptors, and is
synergistic with βl-agents in augmenting inotropy.Evidence demonstrates that PDE III inhibitors areat least as effective as epinephrine in improvingpost-CPB function and that the combination of thetwo agents produces effects at least as large as thesum of the two agents individually. The benefit ofthe two agents together is particularly marked forthe RV.Milrinone requires a 50µg/kg loading dose fol-
lowed by an infusion of 0.375–0.500µg/kg/min.Loading milrinone while on CPB just beforetermination attenuates the effects of the acutevasodilation.
LevosimendanThe catecholamines and PDE III inhibiting drugsact through different pathways to increase inotropyby ultimately increasing intracellular calcium con-centration (Fig. 4.18). Levosimendan is a newinotropic agent that acts without increasing intra-cellular calcium concentration. There is increasedinotropy without impairment of diastolic function.Levosimendan is a myofilament calcium sensitizerthat increases myocardial contractility by stabiliz-ing the calcium bound conformation of troponin C.The systolic interaction of actin and myosin is pro-longed. The enhanced calcium binding is dependenton the intracellular calcium concentration, withaugmentation occurring in the presence of highersystolic calcium concentrations; however, the aug-mentation is unaffected by the lower calcium con-centrations during diastole. This selective actionpreserves diastolic relaxation and diastolic function.In addition to the inotropic effects, levosimendaninhibits PDE III in higher concentrations. The drugcauses vasodilation and an increase in HR. Finally,levosimendan stimulates ATP-sensitive potassium

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 123 — #34
Anesthesia for Myocardial Revascularization 123
β-AR
Catecholaminesvoltage-gated
L-type Ca2+-channel
Calcium-inducedCa2+ release
Ca2+
Ca2+K+
Ca2+Na+
Na+
SRPKA
Ca2+Ca2+
Ca2+
Ca2+
PPL
ATP
SERCA2
RyR2
Levosimendan
Myosin
TnC
Actin
PTnl
ATP cAMPPDE III
PDE III-inhibitors P Digoxin
ATP
AC
Gs
Fig. 4.18 Schematic illustration mechanism of action ofpositive inotropic drugs. β-adrenergic stimulation(catecholamines) and phosphodiesterase (PDE) IIIinhibition increase cyclic adenosine monophosphate(cAMP), which acts via protein kinase A (PKA) tophosphorylate calcium channel protein, phospholamban(PL), and troponin I (TnI). Phosphorylation (P) ofcalcium channel protein enhances sarcolemmal inwardmovement of Ca2+, which subsequently increases Ca2+movement from the sarcoplasmic reticulum (SR)through the calcium release channel (ryanodine receptortype 2, RyR2) to the cytosol (calcium-induced Ca2+release). Digoxin increases cytosolic Ca2+ by inhibitionof sarcolemmal Na+–K+–adenosine triphosphatase andNa+–Ca2+ exchange. Cytosolic Ca2+ binds to
troponin C (TnC) and initiates contraction (inotropiceffect). Phosphorylation of PL enhances relaxation byincreased reuptake of Ca2+ back into the SR by the SRCa2+ adenosine triphosphatase isoform 2 (SERCA2)(lusitropic effect). Phosphorylation of TnI enhances therate of relaxation by decreasing the sensitivity ofmyofilaments to Ca2+. Levosimendan binds to TnCduring systole and thereby increases the sensitivity ofmyofilaments to Ca2+ without alteration of Ca2+ levels.AC, adenylate cyclase; ATP, adenosine triphosphate;β-AR, β-adrenoceptor; Gs, stimulatory guaninenucleotide binding proteins. (From Toller WG, Stranz C.Levosimendan, a new inotropic and vasodilator agent.Anesthesiology 2006;104:556–69, with permission.)
channels, which improves coronary blood flow,reduces preload and afterload, and may have rel-evant anti-ischemic actions.At the time of this writing, levosimendan is
approved for use in over 30 countries world-wide,and there are ongoing trials in the United States andEurope. Indications for the drug include treatmentfor the acute decompensation of CHF, inotropicsupport during myocardial ischemia, cardiogenic
shock, and use in the perioperative period in cardiacsurgical patients. Currently the drug is approvedfor 24-hour administration due to its metabolismyielding biologically active metabolites (OR-1896, aweak calcium sensitizing agent and PDE III inhibitorwith an elimination half life of 96hours). Inplacebo-controlled trials of cardiac surgical patients,levosimendan effectively increased HR, MAP, andCO. There were decreases in SVR, SV, and PVR.

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 124 — #35
124 Chapter 4
Levosimendan was administered in either an 18 or36µg/kg bolus and 0.2–0.3µg/kg/h infusion.
CalciumCalcium chloride 5–10mg/kg is a commonlyused adjuvant during termination of CPB. Recentevidence, however, suggests that calcium admin-istration may be no better than placebo in aug-menting LV function, RV function, and CI afteremergence from CPB. Calcium administration doesincrease MAP, however.The higher doses of calcium (10mg/kg) can
attenuate the effects of inotropic agents that areβ-adrenergic receptor agonists, such as dobutamineand epinephrine. No such effects are seen with mil-rinone. A recent investigation suggests that entryof calcium ions through calcium channels atten-uates adenylyl cyclase, which may explain theobservation.Ionized calcium levels decrease during CPB but
approach normal before separation from CPB.Hypocalcemia is rarely present as an indication forcalcium administration, except perhaps in neonatesand infants, who are more prone to hypocalcemia.In addition, because loss of calcium homeostasis isone of the hallmarks of ischemia, the administrationof calcium in the vulnerable reperfusion intervalafter aortic cross-clamp removalmay exacerbate cellinjury and death.For routine termination of CPB in which
SVR is in the normal range and inotropic sup-port is needed, epinephrine, 0.015–0.05µg/kg/min,dopamine, 1–5µg/kg/min, or dobutamine,5–10µg/kg/min, are reasonable choices becausethey provide inotropic support with little concomi-tant vasoconstriction and afterload increase. Forsituations in which cardiac index is low and SVR iselevated, therapy with a vasodilator such as nitro-prusside may be all that is necessary to relieveafterload mismatch. If an inotrope is necessary inthis situation, dobutamine is a good choice becauseit possesses some vasodilatory activity.When the CI remains low (<2.0 L/min/m2), it is
appropriate to increase the inotrope dose or adda second agent. Dobutamine may be increasedto 15–20µg/kg/min; however, the progressivedecrease in SVR may require the addition of
a small dose (0.5–1.0µg/min) of norepinephrineto normalize SVR. As the doses of epinephrineand dopamine are increased, SVR may increase,and the addition of nitroprusside to the inotropicmay be necessary to reduce afterload and improvesystolic performance. Epinephrine in combina-tion with nitroprusside is a reliable approach tosevere ventricular failure. Elevations of PCWPabove 15–18mmHg should be treated with nitro-glycerin to prevent ventricular dilatation and pul-monary congestion and to improve subendocardialblood flow.The addition of milrinone is useful when these
measures fail to produce acceptable hemodynam-ics (CI > 2L/min/m2, PCWP<18mmHg, CVP <
15mmHg, systolic BP>90mmHg, or MAP >
50mmHg). More specific guidelines for treatmentof RV dysfunction are addressed in Chapter 7.Continued LV and RV dysfunction in the setting ofaggressive inotropic and vasodilator support is anindication for placement of amechanical circulatoryassist device, as discussed in Chapter 11.
Long-term outcome after CABGMore than 800000 patients undergo CABG surgeryeach year around the world. The patient populationis changing (older patients with more significantmorbidities), and the pharmacologic and surgicalinterventions are ever evolving. Nonetheless, CABGremains a mainstay therapy. The long-term adverseevents after CABG are many and reflect the mor-bidities and insult seen in this population. In arecent review of 176 studies (205 717 patients)the in-hospital adverse events were death (1.7%);nonfatal MI (2.4%); nonfatal stroke (1.3%); gastro-intestinal bleeding (1.5%); and renal failure (0.8%).The 30-day mortality was 2.1%. Meta-analysesshow that age greater than 70 years, female sex, lowEF, history of stroke, MI, or heart surgery, and thepresence of diabetes or hypertension are all asso-ciated with increased 30-day mortality after CABG(Table 4.4).Longer-term outcome is also a subject of great
interest. Recent work in patients with multivesseldisease demonstrates that there is no difference inmortality between stenting and surgery (Fig. 4.19).There is no difference in stroke or MI between these

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 125 — #36
Anesthesia for Myocardial Revascularization 125
Table
4.4Post-coronaryarterybypassgraftsurgery(CABG)adverseeventincidenceandmortalityin205717patients.
In-hospitaladverseeventincidence
MI
Non-fatalMI
Stroke
Non-fatal
stroke
GIbleeding
Renal
failure
Mortality
30-day
mortality
AllCABG
Mean%(SE)
3.89(0.66)
2.44(0.28)
2.24(0.27)
1.32(0.15)
1.46(0.29)
0.79(0.15)
1.65(0.14)
2.06(0.16)
Median%
2.94
2.44
1.8
1.29
1.23
0.67
1.54
1.99
n(k)
69487(52)
11973(52)
26750(21)
31132(52)
12897(8)
22798(23)
75933(105)
81136(70)
NorthAmerica
Mean%(SE)
3.56(0.59)
2.82(0.58)
2.29(0.39)
1.25(0.19)
1.11(0.14)
0.88(0.16)
1.96(0.20)
2.00(0.19)
Median%
3.30
2.83
1.71
1.06
1.01
0.86
2.00
1.98
n(k)
49969(32)
2454(18)
13777(12)
25555(28)
7332(3)
21410(14)
59014(49)
47158(39)
Europe
Mean%(SE)
2.59(0.33)
2.55(0.36)
2.42(1.18)
1.30(0.27)
1.33(0.91)
0.99(0.74)
1.30(0.22)
2.21(0.40)
Median%
2.53
2.52
1.66
0.67
1.66
0.49
1.00
2.08
n(k)
13418(15)
8389(24)
6515(4)
4256(13)
220(2)
625(5)
12893(33)
21156(21)
Multinational/other
Mean%(SE)
9.81(5.54)
1.94(0.51)
2.43(0.22)
1.27(0.31)
1.93(0.62)
0.06(0.16)
1.38(0.33)
1.72(0.38)
Median%
3.92
1.66
2.18
1.96
1.32
0.00
1.52
1.61
n(k)
6100(5)
1130(10)
6458(5)
1321(11)
5345(3)
763(4)
4026(23)
13240(10)
ElectiveCABG
Mean%(SE)
2.84(0.81)
2.32(0.40)
2.35(0.60)
1.01(0.21)
1.18(0.48)
0.45(0.18)
1.48(0.19)∗
1.50(0.29)∗
Median%
2.17
2.00
1.59
0.64
1.23
0.22
1.00
1.23
n(k)
3313(17)
3371(32)
1680(7)
9170(24)
510(2)
1333(6)
7912(47)
7764(21)
MixedCABG
Mean%(SE)
4.32(0.89)
2.64(0.36)
2.21(0.31)
1.51(0.20)
1.50(0.35)
0.89(0.18)
1.81(0.18)∗
2.23(0.19)∗
Median%
3.22
2.59
1.86
1.56
1.24
0.89
1.89
2.07
n(k)
66174(35)
8602(20)
25070(14)
21962(28)
12387(6)
21465(17)
68021(58)
73372(49)
RCTs Mean%(SE)
6.26(1.66)∗
2.64(0.42)
2.73(0.98)
1.00(0.16)∗∗
1.23(0.41)
0.39(0.23)∗
1.51(0.21)∗
1.57(0.28)
Median%
4.21
2.94
1.86
1.78
1.23
0.05
0.98
1.69
n(k)
3449(22)
2604(34)
1111(5)
3790(19)
730(4)
2189(10)
4949(48)
4913(23)
Cohortstudies
Mean%(SE)
2.70(0.22)∗
2.21(0.38)
2.15(0.27)
1.52(0.18)∗∗
1.53(0.40)
0.98(0.14)∗
1.80(0.18)∗
2.21(0.19)
Median%
2.51
1.75
1.67
0.61
1.24
0.89
1.83
2.03
n(k)
66038(30)
9369(18)
25639(16)
27342(33)
12167(4)
20609(13)
70984(57)
76223(47)
Continuedp.126

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 126 — #37
126 Chapter 4Table
4.4
(Continued).
In-hospitaladverseeventincidence
MI
Non-fatalMI
Stroke
Non-fatal
stroke
GIbleeding
Renal
failure
Mortality
30-day
mortality
Singlecentre
Mean%(SE)
2.77(0.26)∗∗
2.34(0.28)
2.17(0.37)
1.29(0.16)
1.06(0.23)
0.97(0.19)
1.47(0.15)∗
1.87(0.16)∗
Median%
2.55
2.37
1.60
1.40
1.16
0.84
1.30
1.83
n(k)
48655(40)
11742(49)
11728(16)
26977(47)
1977(4)
6472(15)
45572(93)
54218(54)
Multicentre
Mean%(SE)
7.87(2.66)∗∗
6.10(3.50)
2.43(0.30)
1.43(0.41)
1.60(0.40)
0.62(0.22)
2.52(0.26)∗
2.68(0.38)∗
Median%
4.04
6.45
2.59
1.18
1.31
0.51
2.63
2.65
n(k)
20832(12)
231(3)
15022(5)
4155(5)
10920(4)
16326(8)
30361(12)
26918(16)
MeanEF
<50%
Mean%(SE)
2.79(0.92)
1.82(0.58)
3.81(3.02)
0.82(0.48)
1.47(0.29)
1.09(0.41)
1.45(0.38)
1.56(0.42)
Median%
2.20
1.82
4.03
0.00
1.42
0.89
2.00
1.92
n(k)
4722(8)
698(5)
256(2)
2824(7)
1697(1)
2758(5)
7622(15)
5338(9)
MeanEF
>50%
Mean%(SE)
5.99(1.85)
2.37(0.46)
1.69(0.26)
1.21(0.24)
1.02(0.24)
0.48(0.17)
1.68(0.25)
1.61(0.35)
Median%
3.07
2.41
1.67
1.18
1.16
0.49
1.51
1.23
n(k)
22213(18)
8100(18)
10186(9)
7973(15)
1757(2)
6567(7)
29121(40)
8535(17)
Meanage≤60yrs
Mean%(SE)
3.19(0.94)
2.49(0.54)
2.75(0.82)
1.41(0.42)
N/A
0.00(2.80)
1.21(0.27)
1.15(0.44)∗∗
Median%
2.37
2.68
2.33
0.80
N/A
0.00
1.00
0.78
n(k)
4303(12)
2540(13)
1613(5)
1273(6)
N/A
25(1)
5885(25)
3260(12)
Meanage
>60yrs
Mean%(SE)
4.14(0.84)
2.44(0.36)
1.94(0.23)
1.28(0.16)
1.46(0.29)
0.75(0.16)
1.77(0.16)
2.26(0.17)∗∗
Median%
3.18
2.51
1.67
1.45
1.23
0.6
1.59
2.07
n(k)
63035(39)
9219(37)
24681(15)
26524(44)
12897(8)
13926(20)
45921(76)
74288(54)
NopriorCABG
Mean%(SE)
2.73(0.72)
1.99(0.46)
1.82(0.40)
0.99(0.31)
2.63(1.84)
1.23(1.10)
1.18(0.28)
1.66(0.35)
Median%
3.33
1.83
1.27
0.66
2.63
1.00
1.00
1.81
n(k)
2606(11)
2115(18)
1097(4)
3240(10)
76(1)
270(4)
27625(25)
8390(14)
Somepatientswith
priorCABG
Mean%(SE)
6.47(1.83)
2.57(0.88)
2.19(0.34)
1.80(0.15)
1.53(0.40)
0.86(0.22)
1.92(0.25)
2.27(0.23)
Median%
3.32
1.86
1.8
1.74
1.24
0.9
2.01
2.52
n(k)
45306(18)
6986(6)
19252(12)
17619(15)
12167(4)
16263(9)
32177(30)
48599(28)
∗ P<0.05.∗∗P
<0.01.
CABG,coronaryarterybypassgraftsurgery;EF,ejectionfraction;GI,gastrointestinal;MI,myocardialinfarction;N/A,notavailable;RCT,randomizedcontrolledtrial;SE,standarderror.
(FromNalysnykL,FahrbachK,ReynoldsMW
etal.Adverseeventsincoronaryarterybypassgraft(CABG)trials:asystematicreviewandanalysis.Heart2003;89:767–72.)

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 127 — #38
Anesthesia for Myocardial Revascularization 127
100%
90%
80%
Sur
vlva
l for
dea
th
0%p(log-rank)=0.810
(a) (b)
(c) (d)
0 150 300 450 600 750 900 105012001350
Days since randomization
Pat. At riskCABGStent
1 year588585
2 years583582
3 years577576
4 years568567
5 years559552
1500165018001950
Bypass surgery
Stented angioplasty
Pat. At riskCABGStent
1 year553543
2 years544536
3 years535 521
4 years523507
5 years515 491
100%
90%
80%
70%
60%
50%
40%
Eve
nt fr
ee s
urvi
val
0%
p(log-rank)=0.810
0 150 300 450 600 750 900 105012001350
Days since randomization
1500165018001950
Bypass surgery
Stented angioplasty
Pat. At riskCABGStent
1 year532441
2 years515 417
3 years502393
4 years483375
5 years473350
100%
90%
80%
70%
60%
50%
40%
Eve
nt fr
ee s
urvi
val
0%0 150 300 450 600 750 900 105012001350
Days since randomization
1500165018001950
Bypass surgery
Stented angioplasty p(log-rank) = 0.0001
Pat. At riskCABGStent
1 year566 464
2 years552 441
3 years541 422
4 years523 408
5 years511 382
100%
90%
80%
70%
60%
50%
40%
Eve
nt fr
ee s
urvi
val
0%0 150 300 450 600 750 900 105012001350
Days since randomization
1500165018001950
Bypass surgery
Stented angioplasty
Fig. 4.19 (a) Kaplan–Meier curves showing freedomfrom death. (b) Kaplan–Meier curves showing freedomfrom death/cerebrovascular accident/myocardialinfarction or revascularization. (c) Kaplan–Meier curvesshowing freedom from death/cerebrovascularaccident/myocardial infarction or revascularization.(d) Kaplan–Meier curves showing freedom fromrevascularization. A total of 1205 patients with thepotential for equivalent revascularization were randomlyassigned to coronary artery bypass graft (CABG) surgery(n = 605) or stent implantation (n = 600). The primaryclinical end point was freedom from major adversecardiac and cerebrovascular events (MACCE) at 1 year;MACCE at 5-year follow-up constituted the finalsecondary end point. At 5 years, there were 48 and 46deaths in the stent and CABG groups, respectively (8.0vs. 7.6%; P = 0.83; relative risk (RR), 1.05; 95%confidence interval (CI), 0.71–1.55). Among 208 diabetic
patients, mortality was 13.4% in the stent group and8.3% in the CABG group (P = 0.27; RR, 1.61; 95% CI,0.71–3.63). Overall freedom from death, stroke, ormyocardial infarction was not significantly differentbetween groups (18.2% in the stent group vs. 14.9% inthe surgical group; P = 0.14; RR, 1.22; 95% CI,0.95–1.58). The incidence of repeat revascularization wassignificantly higher in the stent group (30.3%) than inthe CABG group (8.8%; P < 0.001; RR, 3.46; 95% CI,2.61–4.60). The composite event-free survival rate was58.3% in the stent group and 78.2% in the CABG group(P < 0.0001; RR, 1.91; 95% CI, 1.60–2.28). (FromSerruys PW, Ong AT, van Herwerden LA et al. Five-yearoutcomes after coronary stenting versus bypass surgeryfor the treatment of multivessel disease: the final analysisof the Arterial Revascularization Therapies Study (ARTS)randomized trial. J Am Coll Cardiol 2005;46:575–81, withpermission.)

Alice Nelson Dinardo: “ch04” — 2007/7/17 — 20:30 — page 128 — #39
128 Chapter 4
two groups. The stenting group had a significantlyhigher incidence of repeat revascularization.
Suggested reading
Chaney MA. Intrathecal and epidural anesthesia and
analgesia for cardiac surgery. Anesth Analg 2006;102:45–64.
Eagle KA, Guyton RA, Davidoff R et al. ACC/AHA 2004
Guideline update for coronary artery bypass graft
surgery: summary article. Circulation 2004;110:1–9.Groban L, Dolinski SY. Transesophageal echocardio-
graphic evaluation of diastolic function. Chest 2005;128:3652–63.
Lan Kwak Y. Reduction of ischemia during off-pump coro-
nary artery bypass graft surgery. J Cardiothorac Vasc
Anesth 2005;19:667–77.Nalysnyk L, Fahrbach K, Reynolds MW et al. Adverse
events in coronary artery bypass graft (CABG) trials:
a systematic review and analysis.Heart 2003;89:767–72.Tanaka K, Ludwig LM, Kersten JR et al. Mechanisms of
cardioprotection by volatile anesthetics. Anesthesiology
2004;100:707–21.Van Mastrigt GA, Maessen JG, Heijmans J et al. Does fast
track treatment lead to a decrease of intensive care unit
and hospital length of stay in coronary artery bypass
patients? A meta-regression of randomized clinical
trials. Crit Care Med 2006;34:1624–34.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 129 — #1
CHAPTER 5
Anesthesia for Valvular Heart Disease
While the number of cardiac procedures forcoronary artery bypass grafting (CABG) is falling inthe USA, the number operations for heart valve dis-ease is increasing. Over 5 million persons have mod-erate to severe valvular regurgitation in the USAalone. The aging population, expanding indicationsfor surgery, improvements in valve construction,and improvements in patient morbidity and mortal-ity after surgical intervention all suggest that valvesurgery is likely to increase in coming years. Thischapter will review anesthesia for patients with avariety of valvular heart conditions. There will bespecial emphasis on the more common lesions ofthe aortic and mitral valves.
General considerations
Preoperative evaluationIn valvular heart disease, there are a number of his-tory and physical findings that directly influenceanesthetic management. Posting a case as “aorticvalve replacement” or “mitral valve replacement”provides no information on whether this is for aor-tic stenosis (AS), aortic regurgitation (AR), or both;mitral stenosis (MS), mitral regurgitation (MR), orboth. The anesthesiologist must dig further and findout the specific valvular pathology. This knowledgeis essential in preparing hemodynamic goals for theinduction, maintenance, and postoperative care ofthese patients.
Additional information is required unrelated tothe valve pathology. For example, will there be
other procedures during this repair (i.e. carotidendarterectomy, CABG, septal myomectomy,a Maze procedure (a series of surgical incisionsin the atrium intended to interrupt the circularpattern of electrical activity associated with atrialfibrillation), or other intervention)? What is theclinical condition of the patient? Is the patient ina compensated or uncompensated state? With ASthe timing of surgery will have a great impacton outcome depending on the patient’s condition.For example, a patient in the early to mid-stagesof AS will have a hyperdynamic, hypertrophiedheart that will likely perform well after cardiopul-monary bypass (CPB). In contrast, a patient in thelate stages of AS will be in congestive heart fail-ure (CHF), have a reduced ejection fraction (EF),and will likely require extensive inotropic supportafter CPB.
Review of imaging and laboratory studies isessential prior to moving the patient to the oper-ating room. Imaging of the heart will give thediagnosis and degree of the structural abnormality.Preoperative echocardiography will establish thetype of lesion (stenotic versus regurgitant), the heartfunction, and the valve gradients. The valve area isof critical importance in assessing any stenosis. Inpatients with normal left ventricular (LV) function,aortic valve gradients in severely stenotic lesionsmay be very high (Fig. 5.1). In patients with poorventricular performance, there may be anatomicallycritical lesions (aortic valve area <0.7 cm2) and alow gradient. These patients are especially prone to
129

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 130 — #2
130 Chapter 5
Fig. 5.1 Deep transgastric long-axis transesophagealechocardiographic image in a patient with severe aorticstenosis. The velocity of flow is very high at 5 m/s witha peak gradient of 101 mmHg and a mean gradient of67 mmHg. This is clearly severe aortic stenosis.
intraoperative instability with the induction of gen-eral anesthesia and may require significant inotropicsupport post-CPB. Other important imaging studiesinclude coronary angiography to rule out concur-rent coronary artery disease, a chest radiograph, andperhaps, thoracic computed tomography (CT) ormagnetic resonance imaging (MRI) to evaluate tho-racic anatomy. A chest X-ray is essential in “redo”operations involving the heart and mediastinum.The heart may be adhered to the posterior margin ofthe sternum rendering sternotomy quite hazardous.All precautions including adequate venous access,immediate availability of blood products, and intra-operative awareness and vigilance are required inthese situations.
Atrial natriuretic peptides are useful markerswhen following patients with heart failure dueto valvular pathology. In severe AS, natriureticpeptides increase with increasing New York HeartAssociation (NYHA) functional classes and decreas-ing LV EF. Natriuretic peptide levels fall aftersuccessful aortic valve surgery.
MonitoringMonitoring during valvular surgery varies littlefrom monitoring required during other types ofheart surgery. In addition to the American Society
of Anesthesiologists (ASA) standard monitors, a uri-nary Foley catheter, and arterial and central linesare essential. Many institutions routinely use pul-monary artery catheters to monitor cardiac out-put (CO), mixed venous oxygenation, pulmonaryartery pressures, and pulmonary capillary wedgepressures (PCWPs). Although this is standard prac-tice by many clinicians, outcome data supportingpulmonary artery catheterization are lacking.
Intraoperative transesophageal echocardiogra-phy (TEE) is rapidly becoming an essential compo-nent of anesthesia for all heart valve procedures.Extensive preoperative evaluation by TEE oftenreveals previously unknown structural or func-tional defects. In addition, TEE can provide instantassessment of the status of a valve repair proce-dure. TEE may also diagnose perivalvular leaksafter valvular replacement requiring prompt inter-vention. The assessment of air in the left side ofthe heart is important after an open-heart proce-dure. TEE may assist in locating the air therebyfacilitating direct venting procedures. TEE is help-ful in guiding post-CPB hemodynamic interventionand treatment. In recognition of this tool’s util-ity in cardiac surgical procedures, the AmericanSociety of Echocardiography and the AmericanHeart Association provide a class 1 recommendationfor TEE use in all heart valve surgical procedures(Table 5.1).
Other special monitoring devices in heart valvesurgery may include processed electroencephalo-gram (EEG) monitoring for either patient awarenessor for EEG activity during procedures in which it isdesirable that all electrical activity stop (i.e. deephypothermic circulatory arrest). Cerebral oximetryhas no special application in surgery for heart valvedisease.
PremedicationGreat caution is advised when prescribing pre-medication in patients with valvular heart disease.In patients with preserved LV function, morphinesulfate 0.1 mg/kg intramuscularly (IM) and orallorazepam 1.5 hours before scheduled incision timeare appropriate. Supplemental oxygen should beinstituted at the time of premedication. Reducingdosing, or no premedication at all, is indicated for

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 131 — #3
Anesthesia for Valvular Heart Disease 131
Table 5.1 Recommendations for intraoperative echocardiography. (Reprinted from Cheitlin MD, Armstrong WF,Aurigemma GP et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography–summaryarticle: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines(ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography). J Am CollCardiol 2003;42:954–70.)
Class I1 Evaluation of acute, persistent, and life-threatening hemodynamic disturbances in which ventricular function and itsdeterminants are uncertain and have not responded to treatment2 Surgical repair of valvular lesions, hypertrophic obstructive cardiomyopathy, and aortic dissection with possible aorticvalve involvement3 Evaluation of complex valve replacements requiring homografts or coronary re-implantation, such as the Ross procedure4 Surgical repair of most congenital heart lesions that require cardiopulmonary bypass5 Surgical intervention for endocarditis when preoperative testing was inadequate or extension to perivalvular tissue issuspected6 Placement of intracardiac devices and monitoring of their position during port-access and other cardiac surgicalinterventions7 Evaluation of pericardial window procedures in patients with posterior or loculated pericardial effusions
Class IIa1 Surgical procedures in patients at increased risk of myocardial ischemia, myocardial infarction, or hemodynamicdisturbances2 Evaluation of valve replacement, aortic atheromatous disease, the Maze procedure, cardiac aneurysm repair, removal ofcardiac tumors, intracardiac thrombectomy, and pulmonary embolectomy3 Detection of air emboli during cardiotomy, heart-transplant operations, and upright neurosurgical procedures
Class IIb1 Evaluation of suspected cardiac trauma, repair of acute thoracic aortic dissection without valvular involvement, andanastomotic sites during heart and/or lung transplantation2 Evaluation of regional myocardial function during and after off-pump coronary artery bypass graft procedures3 Evaluation of pericardiectomy, pericardial effusions, and pericardial surgery4 Evaluation of myocardial perfusion, coronary anatomy, or graft patency5 Dobutamine stress testing to detect inducible demand ischemia or to predict functional changes after myocardialrevascularization6 Assessment of residual duct flow after interruption of patent ductus arteriosus
Class III1 Surgical repair of uncomplicated secundum atrial septal defect
elderly or debilitated patients, patients with poorventricular function, or patients with poor pul-monary function. Most prudently, premedicationcan wait until the patient arrives in the preopera-tive holding area. At this time, the anesthesiologistmay administer intravenous (IV) midazolam and/orfentanyl while directly observing and monitoringthe patient.
All cardiac medications may be continued untilthe time of surgery. There is debate on holdingangiotensin converting enzyme inhibitors (ACE-I)
prior to surgery. These medications are associatedwith significant hypotension during and after CPBin some patients. Data on the harmful effects ofwithholding ACE-I medications are undetermined.Consultation with the cardiologist and surgeon isrequired before stopping any antiplatelet agentsprior to surgery. In many centers, patients withstable symptoms will wait 3–5 days after stoppingclopidogrel. It is common for patients with valvularheart disease to present with atrial fibrillation or amechanical valve, and thus require anticoagulation.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 132 — #4
132 Chapter 5
Coordination regarding the administration of thesemedications during the perioperative period isessential.
Induction and maintenance ofanesthesiaNo specific agents or techniques are indicated foreither induction or maintenance of anesthesia inany specific valvular condition. Rather, adherenceto preset hemodynamic goals will provide appro-priate guidance when choosing anesthetic agents.There are a number of ways to achieve thesegoals safely in the patient presenting for valvesurgery.
Patient awareness during cardiac surgical proce-dures requires special attention. Awareness occursin approximately 0.13% of surgical patients. Multi-variate logistic regression identified increasing ASAstatus, and type of procedure as risk factors forrecall. For cardiac surgical procedures, the odds ratiofor recall is 3.58 with a 95% confidence intervalof 0.72–17.9. As with any procedure, attention tohemodynamic signs, depth of anesthesia, the use ofbenzodiazepines, and inhalational agents will likelyreduce the risk of operative recall.
There are good data to support the concept of“fast-track” or early extubation protocols in thecare of patients presenting for CABG surgery. Thesebenefits include reduced hospital stay, intensivecare unit stay, and reduced cost of care. Data onearly extubation protocols in valve surgery are lesscommon, although one might expect similar ben-efit as observed in CABG surgery. One should beaware, however, that many valvular procedures arecomplex in nature, requiring extended CPB time,potential deep hypothermic circulatory arrest, andincreased requirements for blood and blood prod-uct transfusion. All of these factors may limit theopportunity for early extubation.
There are limited reports of regional anesthesiafor valvular heart surgery. Most reports providedata on combined general anesthesia and thoracicepidural anesthesia. When applied, upwards of 65%of these patients may be extubated in the operat-ing room. Typically, an epidural catheter is placedat T1–3 on the day of surgery. A rigid anticoagu-lation protocol must be followed both before and
after surgery. There are case reports of aortic valvereplacement in conscious patients under regionalanesthesia without intubation. Given the signifi-cant issues with anticoagulation, it is unlikely thatregional anesthesia will replace traditional generalanesthesia for valvular surgery.
Weaning from bypass andthe post-bypass periodRepairing or replacing the valve may fundamentallychange the hemodynamic goals of the patient fromthe pre-bypass period. A normal valvular profilemay be observed immediately after CPB (Fig. 5.2).The anticipation is that the heart will now per-form normally; however, that does not necessarilyfollow. The heart suffers an acute insult with thesurgical intervention, aortic cross-clamping, and themyocardial depressant effects of the various anes-thetic agents. As with any cardiac surgical proce-dure, there may be evidence of new regional wallmotion abnormalities, global cardiac dysfunction,and peripheral vascular dysfunction. In valvularheart surgery, the heart requires time to remodelbefore significant improvement is observed.
In some patients, however, hemodynamics maybe greatly improved post-bypass. In simple, com-pensated AS, the patient may be hyperdynamic
Fig. 5.2 This is the same patient as seen in Fig. 5.1 afteraortic valve replacement with a stentless freestyle aorticvalve. The deep transgastric long axis view through theaortic valve now shows a peak gradient of 9 mmHg anda mean gradient of 4 mmHg. Both of these gradients arenow normal.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 133 — #5
Anesthesia for Valvular Heart Disease 133
and hypertensive after weaning from bypass. Itmay also be possible, however, that due to the LVhypertrophy, cardioplegia may have been incom-plete for total myocardial protection, and the patientmay emerge from bypass with transient myocar-dial dysfunction. In complex repairs, or multiplevalve surgery, an extended bypass run may berequired, thereby increasing the risk of immediatepostoperative cardiac dysfunction and the require-ment of inotropic support. EF and LV functionmay decline after surgery to repair MR; this iscommonly thought to be due to the new load-ing conditions of the heart after removal of the“pop-off” mitral regurgitant outflow. This is likelyuntrue, as emerging data on mitral valve repair pro-cedures, in which there is sparing of the mitral valveapparatus, show little alteration in EF. This preser-vation of mitral annular integrity stabilizes LV shapeand contractility, thereby preserving function. Thediminished performance is likely secondary to otherfactors including extended cross-clamp time, inade-quate myocardial protection, and myocardial stun-ning. Combined CABG and valvular heart surgeryis associated with inotrope use during separationfrom CPB.
TEE is especially useful in the immediate post-bypass period. TEE will facilitate the assessment ofmyocardial function and filling parameters, render-ing important information affecting decisions aboutinotropes and volume management. TEE can alsoassess the condition of the valve repair or replace-ment. On every case in which TEE is used, acomplete evaluation of valve structure and func-tion is required. In a valve repair, the degree ofresidual regurgitation must be documented. Deter-mination of the Doppler gradient across the repairedvalve is required, and images of the valve move-ment are necessary. In a valve replacement, all ofthe above are essential, and a further evaluation fora perivalvular leak is required. After mitral valverepair, an assessment for systolic anterior motion(SAM) of the mitral valve is required. These imagesmust be stored as a part of the patient record anda note made in the patient’s chart or anestheticrecord.
The post-bypass period may be a time of unsta-ble hemodynamics. The heart is adjusting to a new
conditions of preload, afterload, and inotropy. Thereis usually ongoing bleeding, which in many patients,and especially in “re-do” procedures, may be severe.Constant vigilance regarding hemodynamics, bloodvolume, blood gas chemistry, and metabolic state(i.e. ionized calcium, glucose concentrations, andurine output) is required. There may be newrhythm disturbances. Patients with preoperativeatrial fibrillation may now be in sinus rhythmafter mitral valve repair and a Maze procedure.These patients may be dramatically improved. Otherpatients, however, may suffer from third-degreeheart block, bradycardia, tachycardia, or other rateand rhythm abnormalities making managementdifficult.
In the intensive care unit, these patients willlikely remain intubated for some hours. Theusual considerations of temperature management,metabolic and hemodynamic management, vigi-lance for excessive chest tube bleeding and evidenceof cardiac tamponade must be performed. Elderlypatients and those with additional risk factors mayrequire additional support.
Special considerations andlong-term prognosisCardiac anesthesia for valvular heart surgery carriesnumerous special considerations not found in otheraspects of cardiothoracic anesthesiology. Amongthese considerations is familiarity with the type ofvalve used in the operative repair. There are a num-ber of valve types including allografts, autografts,xenografts, mechanical, and bioprosthetic valves.The choice of valve is up to the surgeon; how-ever, the anesthesiologist is frequently consultedto provide TEE measurements that may guide thesurgeon in valve choice. For example, the measure-ment of the aortic valve annulus size is importantwhen determining the size of a prosthetic valve.In the assessment for a possible Ross procedure(pulmonary valve moved to the aortic position andpulmonary allograft placement), the pulmonaryannulus size and the degree of pulmonary insuf-ficiency are important factors before committing tothe procedure. After the repair, it is important toassess the new valve function. Bioprosthetic valvesall come with a complete hemodynamic profile in

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 134 — #6
134 Chapter 5
their packaging and this information is importantwhen rendering a decision on the function of a newvalve. The expected gradients are sometimes higher,and the calculated valve area may be less thanone might expect. The impact of valve prosthesis-patient mismatch (VP-PM) on mortality is as highas 25% in those patients with a severe VP-PM mis-match. Reference to the packaging insert will guidethe clinician as to whether intraoperative gradi-ents and calculated valve areas are acceptable. Invalve repair procedures, one must not only lookfor the cessation of regurgitation, but one mustensure that there is no new stenosis. Measurementof valve gradients and orifice areas will help in thisregard.
Valve repair for patients with endocarditis presentall of the aforementioned hemodynamic considera-tions in addition to the frequently septic conditionof the patient. Patients with endocarditis usuallyhave acute regurgitant lesions and present in heartfailure. The in-hospital mortality for acute endo-carditis is 20%. The early predictors of in-hospitalmortality include embolic events, diabetes melli-tus, Staphylococcus aureus, and APACHE II score. Theuse of intraoperative TEE is especially helpful inthe diagnosis of endocarditis and quantification ofthe valve defect. Valve surgery reduces 6-monthmortality.
There are solid data to support valve repair andreplacement in patients with heart valve diseaseover medical management. After surgery for ASthere is initial remodeling of the heart, with sub-sequent LV mass reduction. In MR, there is symp-tomatic relief, and improvement in LV EF. Althoughthere is a known early mortality with heart valvesurgery, the long-term benefit remains superior tomedical management. As the population extendslongevity, more patients will present for valve pro-cedures. Although advancing age is associated withworse outcome, there is no upper limit of agecontraindicating valvular surgery.
It is unknown what impact percutaneous valvesand other nonsurgical valve repair procedures willhave on the volume of valvular surgery. It is likely,that anesthesiologists will provide sedation and/orgeneral anesthesia in patients presenting for per-cutaneous valve procedures. In such cases, all of
the hemodynamic principles described below apply.In addition, TEE will be required for percutaneousmitral annular reduction for MR, and endovascularmitral valve repair (Alfieri procedure).
The aortic valve
Aortic valve anatomyThe aortic valve consists of three semilunar valvesnamed according to their relationship with theappropriate coronary arteries: the right coronarycusp, the left coronary cusp, and the noncoronarycusp. At the center of the free-edge of each cusp is atiny, elevated nodule commonly referred to as thenodule of Arantius. All three nodules coapt at thecenter of a normal, closed aortic valve (Fig. 5.3).The lunulas are the free-edges of the cusps and spanfrom the nodule of Arantius to the wall of the aorta.When the lunulas of the cusps are apposed and thenodules of Arantius are coapted in a normal aorticvalve, the valve is completely closed.
Figure 5.4 demonstrates normal subvalvular,valvular, and ascending aortic anatomy in the mid-esophageal aortic valve long-axis view. In thisimage, the left ventricular outflow tract (LVOT),aortic valve annulus, sinuses of Valsalva, sinotubu-lar junction, and proximal ascending aorta are wellvisualized. Measurements of these structures are
Fig. 5.3 This is a mid-esophageal short axistransesophageal echocardiographic image of a normalaortic valve in the color compare mode. To the left thetrileaflet valve is seen during systole. To the right, colorDoppler demonstrates a normal flow pattern.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 135 — #7
Anesthesia for Valvular Heart Disease 135
Fig. 5.4 This is the same patient as in Fig. 5.3. This is amid-esophageal long axis view of the aortic valve in thecolor compare mode. To the left one can clearly identifythe left ventricular outflow tract, aortic valve, sinus ofValsalva, sinotubular ridge, and the aortic root. To theright, color Doppler demonstrates a normal flow patternwith aliasing as the blood accelerates through the aorticvalve.
part of a complete examination and are integral indetermining annular dilatation and aortic aneurysmpathology. AR can be quantified in this view.The aortic valve complex, including the junctionof the aortic valve with the ventricular septum andthe anterior mitral valve leaflet, is easily visualizedin this imaging plane.
Aortic stenosis (AS)AS is the most common valvular lesion in the USA.The incidence is increasing due to the aging pop-ulation and the presence of calcific degenerativechanges in the aortic valve with time. This pro-cess was once viewed as simply a byproduct of theageing process; however, new data suggest that cal-cific AS is the result of an inflammatory process.Isolated AS in adults is more common in malesthan females and is usually nonrheumatic in origin.Most commonly, AS is degenerative with calcifica-tion of the valve leaflets. Congenital bicuspid valvesdevelop the same degenerative changes seen innormal tricuspid aortic valves.
In rheumatic AS, the valve commissures are fusedand aortic valve leaflet excursion is limited. Theresult is a stenotic valve orifice. This stenosis isusually accompanied by regurgitation. In rheumatic
heart disease, the mitral valve is usually involved inaddition to the aortic valve.
Pathophysiology and adaptation in ASAS is a chronic LV pressure overload lesion. Thenatural history of the lesion involves a gradualreduction in the aortic valve area from the normal2.6–3.5 cm2 to <1.0 cm2 occurring over severalyears. Replacement is generally considered beforethe aortic valve area is <0.7 cm2 or the peak systolicpressure gradient is >50 mmHg. The relationshipof valvular gradient to orifice area is given by theGorlin formula: gradient = (CO)2/(aortic valvearea)2. Using this relationship, one can immediatelyappreciate that reducing the aortic valve area whilemaintaining CO has a huge impact on the valvulargradient. In a valve with a gradient of 60 mmHg, theLV must generate a systolic pressure of 180 mmHg inorder to maintain a normal aortic systolic pressureof 120 mmHg.
As the disease progresses, there is an increasingpressure load on the left ventricle. This pressureload is compensated by ventricular hypertrophy.Under these circumstances, left LV stress (afterload)is greatly elevated. The law of LaPlace providesthe relationship between wall stress and pressure:Load or stress in the myocardium = (ventricularpressure) (radius)/2 (wall thickness), or T =Pr/2h where P = peak ventricular pressure,r = ventricular radius, and h = wall thickness).Therefore, as the afterload increases (the pres-sure in the numerator), the myocardial tension iscompensated by increasing wall thickness (in thedenominator). The increased wall stress results inconcentric ventricular hypertrophy. The degree ofthickening parallels the increased ventricular pres-sure demands. The result is normalization of ven-tricular wall stress despite greatly elevated peakventricular pressure (Fig. 5.5a,b). This normaliza-tion of wall stress allows maintenance of EF despitethe high impedance to ejection found in AS. Even-tually, the valve orifice narrows to the point atwhich stroke volume (SV) and EF fall (Fig. 5.6).
Concentric hypertrophy has several hemody-namic implications. There is reduced ventricularcompliance which results in diastolic dysfunctionwith reduced early diastolic filling of the ventricle.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 136 — #8
136 Chapter 5
250
200
LV p
ress
ure
(mm
Hg)
LV w
all s
tres
s
150
100
50
050 100 150
LV volume (mL)50 100 150
(a) (b)
B
A B
A
Con
cent
ricH
yper
troph
yCon
trol
Fig. 5.5 (a) Left ventricular pressure–volume loopsdemonstrating adaptation to chronic pressure overload.Loop A represents a normal ventricle before thedevelopment of aortic stenosis. Loop B represents thesame ventricle after prolonged exposure to elevatedafterload and development of concentric hypertrophy.End-systolic and end-diastolic volumes in loop B areunchanged from those in loop A, but left ventricularsystolic pressure is greatly elevated. (b) The same loopsillustrated in (a) are shown again here, except that wallstress is plotted against volume. It is obvious thatelevated ventricular systolic pressure seen in loop A doesnot result in elevated wall stress compared with loop B.Development of concentric hypertrophy allowsnormalization of wall stress in the face of chronicallyelevated left ventricular systolic pressure. LV, leftventricular. (From Ross J Jr. Afterload mismatch in aorticand mitral valve disease: implications for surgical therapy.J Am Coll Cardiol 1985;5:811–26, with permission.)
Normal end-diastolic volumes are maintained withnormal sinus rhythm. In patients with severe AS,atrial systole contributes nearly 30% of the left ven-tricular end-diastolic volume (LVEDV), whereas inpatients without AS, atrial systole contributes 20%.This late diastolic filling occurs on the steep portionof the diastolic pressure–volume curve. The well-timed atrial systole allows late diastolic filling tooccur with minimal elevation in mean left atrialpressure (LAP). With loss of atrial systole (atrialfibrillation), normal end-diastolic volume is main-tained by increasing mean LAP to equal or exceedleft ventricular end-diastolic pressure (LVEDP).When compliance is poor, a normal LVEDV mayoccur at a LVEDP in excess of 25 mmHg. Acuteincreases in mean LAP may result in pulmonary
LV w
all s
tres
sLV volume (mL)
50 100 150
Limit of preloadreserve
EFx 33%
EFEFx 60% 60%EFx 60%
Compe
nsat
ed
Mild
dys
func
tion
EFx 52%Post-op.
Fig. 5.6 Left ventricular wall stress–volume loops inprogressive aortic stenosis (AS). The dotted looprepresents a ventricle with concentric hypertrophy andpreserved systolic function. As systolic dysfunctiondevelops, stroke volume (SV) and ejection fraction (EF)can be maintained by making use of the preload reserve(EF = 60%). Further progression of systolic dysfunctionresults in exhaustion of preload reserve. At this point,further progression of AS results in afterload mismatchand reduction in SV and EF (EF = 33%). Surgicaltherapy for replacement of the stenotic aortic valveresults in a reduction in afterload, the abolition ofafterload mismatch, and the ability of the ventricle todeliver nearly normal SV and EF despite the presence ofsystolic dysfunction (EF = 52%). Post-op., postoperative.(From Ross J Jr. Afterload mismatch in aortic and mitralvalve disease: implications for surgical therapy. J Am CollCardiol 1985;5:811–26, with permission.)
congestion. Unfortunately, in AS with atrial fibril-lation, low mean LAP results in diminished LVEDVand, therefore, SV and CO.
Diminished ventricular compliance also limits theuse of preload reserve. With the ventricle operatingon the steep portion of its diastolic pressure–volumecurve, incremental increases in end-diastolic vol-ume result in prohibitive increases in end-diastolicpressure. Hence, even with preserved atrial systole,it may be impossible to augment preload unlessmean LAP is above 20–25 mmHg. Again, at these

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 137 — #9
Anesthesia for Valvular Heart Disease 137
Table 5.2 Myocardial oxygen supply and demand in aortic stenosis.
Myocardial oxygen consumption is increased by:• The increased mass of myocardium• The demands of LV pressure work, which is much more energy-consumptive than volume work. A large portion ofthe total myocardial workload is devoted to the isovolumic contraction phase because of the high intraventricularpressures necessary to commence the ejection phase (see Fig. 5.5). Recall that the isovolumic contraction phase is a veryenergy consumptive process• The prolonged ejection phase
Myocardial oxygen delivery is compromised by:• Elevated LVEDP secondary to diminished ventricular compliance• An aortic diastolic pressure that is low relative to the elevated LVEDP• Diminished diastolic coronary perfusion time secondary to the prolonged ejection phase• Compression of subendocardial vessels by hypertrophied myocardium• Absence of any systolic coronary perfusion because LV systolic pressure greatly exceeds aortic systolic pressure
LV, left ventricle; LVEDP, left ventricular end-diastolic pressure.
pressures the patient is a risk for pulmonary conges-tion. In this end-stage disease, increases in preloadonly minimally increase SV. Thus, for a givencontractile state, SV is nearly fixed.
Patients with AS are especially susceptibleto ischemia. Several factors are responsible forthe myocardial oxygen supply–demand imbalanceseen in AS (Table 5.2). This combination of factorsexplains why 30% of patients with AS experienceangina in the absence of significant coronary arterydisease.
In general, global ventricular function (EF%) isnormal in AS. The mechanism for depressed EFin patients with severe AS is not entirely clear.Concentric hypertrophy, inadequate to normalizewall stress, will result in excessive afterload andreduced EF. Subendocardial ischemia may also playa role. In patients without myocardial infarction,irreversible myocardial damage is relatively uncom-mon, and there is remarkable improvement in EFafter uncomplicated aortic valve replacement. Manypatients with depressed function preoperatively willexhibit a normal EF postoperatively. The patientwith a low gradient, low CO and low EF is at highestrisk for surgery. These patients have lost their abil-ity to compensate for the disease process. Survivalin these patients depends on medical versus surgi-cal treatment and the presence of inotropic reserve(Fig. 5.7).
100
75
Pat
ient
sur
viva
l (%
)
50
25
0
0 50Follow-up (months)
Group I, valve replacement
Group II, valve replacement
Group I, medical treatment
Group II, medical treatment
100
Fig. 5.7 Survival for aortic stenosis patients with lowgradient and low ejection fraction. Group I patientsdemonstrated inotropic reserve and had a better outcomewith aortic valve replacement (AVR) than did similarpatients treated medically, and better than group IIpatients who lacked inotropic reserve. (From Monin JL,Quere JP, Monchi M et al. Low-gradient aortic stenosis:operative risk stratification and predictors for long-termoutcome. A multicenter study using dobutamine stresshemodynamics. Circulation 2003;108:319–24, withpermission.)
In patients with systolic dysfunction, there isa progressive increase in LVEDV so that SV andEF are maintained through use of preload reserve(see Fig. 5.6). Reduced ventricular compliance limitsthe increase in end-diastolic volume and the pres-sure tolerated without pulmonary congestion. Withsevere systolic dysfunction, the maximal wall stress

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 138 — #10
138 Chapter 5
that the ventricle can generate is severely limited. Inthis situation, afterload mismatch may limit mainte-nance of SV and EF despite use of preload reserve. Inthese patients, the aortic valve gradient may be lowsecondary to the reduced flow across the stenoticvalve. The calculated valve area will give a muchbetter indication of the severity of the stenosis.
Severe AS does not directly affect right ventricu-lar (RV) function until the occurrence of pulmonaryartery hypertension. In patients with severe AS andan EF <50%, a reduced SV and CO is maintainedat the expense of elevated left atrial and pulmonaryartery pressures. Pulmonary artery pressures beginto rise through passive pulmonary venous con-gestion when LAPs exceed 18 mmHg. Ultimately,pulmonary artery fibrosis develops and pulmonaryarterial hypertension follows. As the mean pul-monary artery pressure gradually rises to exceed50 mmHg, the right ventricle, which normally func-tions with low impedance to ejection, fails. Patientswith AS and an EF < 40% have CO maintained bya gradual increases in mean LAP to 25–30 mmHg,with mean pulmonary artery pressure in excessof 50 mmHg. These patients may have clinical evi-dence of RV failure with peripheral edema and livercongestion.
Increases in heart rate normally result in a markeddecrease in the time of diastole, whereas the lengthof systole remains largely unchanged (Fig. 5.8a,b).Over the heart rate range of 50–110 b/min, thelength of systole decreases from 441 to 315 ms;whereas, the time of diastole decreases from 759 to230 ms. Hence, tachycardia in patients with AS isdetrimental because, although there is adequatetime in systole to allow ejection across the stenoticvalve, diastolic time and subendocardial perfusionare drastically reduced.
Bradycardia in these patients is also detrimen-tal. Recall that the valve gradient increases as thesquare of the flow across the valve. MaintainingCO at a reduced heart rate requires increased SV(CO = HR × SV). Because SV is flow, the gra-dient must increase. Figure 5.9(a–c) demonstratesthat for a given CO, progressive decreases in heartrate result in large increases in the transvalvulargradient. With aortic valve areas <0.5 cm2, gra-dients in excess of 150 mmHg are possible, even
1000(a)
800 R–R
Total diastolic period (R–R)−(QS2)
600
400Tim
e (m
s)
200
80(b)
70
60%
Dia
stol
e
50
40
3030 50 70 90
Hour
110 130 150
30 40 50 60 70 80 90
Hour
100 110 120 130 140 150
OS2
Fig. 5.8 (a) Increases in heart rate cause decreases inlength of each cardiac cycle (R–R interval). Decreases inlength of systole (OS2) with increases in heart rate arefar less dramatic than decreases in the length of diastole(R–R–QS2). (b) Percent of each cardiac cycle (R–Rinterval) spent in diastole at various heart rates. Smallchanges in heart rate cause large decreases in percent oftime spent in diastole. (From Boudoulas H, Rittgers SE,Lewis RP et al. Changes in diastolic time with variouspharmacologic agents: implication for myocardialperfusion. Circulation 1979;60:164–9, with permission.)
with low normal SVs. Because the left ventricle iscapable of generating peak pressures in the rangeof 250–300 mmHg, maximal ventricular pressuresare needed to maintain a systolic blood pressure>100 mmHg. In this setting, bradycardia with anincrease in the gradient will result in systemichypotension. The result is poor subendocardialperfusion and ischemia. In addition, diminisheddiastolic compliance may prohibit the increase inend-diastolic volume necessary to augment SV in

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 139 — #11
Anesthesia for Valvular Heart Disease 139
(c) Aortic stenosis10000
7500
Car
diac
out
put (
cc/m
in)
5 000
2500
Assumption: HR= 68 b/min, SEP=0.32 s/beat
00 75 150
Mean gradient (mmHg)225 300
4.02.0
1.0
0.7
0.5
0.3
(b) Aortic stenosis10000
7500
Car
diac
out
put (
cc/m
in)
5000
2500
Assumption: HR = 76 b/min, SEP = 0.34 s/beat
00 75 150
Mean gradient (mmHg)225 300
4.04.02.0
1.00.7
0.5
0.3
Aortic stenosis10000
(a)
7500
Car
diac
out
put (
cc/m
in)
5 000
2500
Assumption: HR = 88 b/min, SEP = 0.32 s/beat
00 75 150
Mean gradient (mmHg)225 300
4.04.02.0
1.00.7
0.5
0.3
4.0 4.0
Fig. 5.9 The relationship of heart rate (HR), cardiacoutput (CO), aortic valve area, and systolic pressuregradient across the aortic valve is illustrated for patientswith aortic stenosis. CO is plotted against the systolicpressure gradient for aortic valve areas ranging from0.3–4.0 cm2. (a) This plot illustrates these relationshipsfor HR of 88 b/min and systolic ejection period (SEP) of0.32 s/beat. (b) This plot illustrates these relationships forHR of 76 b/min and SEP of 0.34 s/beat. (c) This plotillustrates these relationships for HR of 68 b/min and SEPof 0.32 s/beat. Clearly, for a given CO and HR, systolicpressure gradient increases as aortic valve area decreases.
Furthermore, for a given CO and aortic valve area,systolic pressure gradient increases as HR decreases.Increases in HR in the range examined here have littleeffect on length of SEP. Therefore, for CO to remainconstant as HR decreases, larger stroke volume (SV) mustbe ejected across stenotic aortic valve in relativelyconstant time period. This results in larger systolicpressure gradient. (From Carabello BA, Grossman W.Calcification of stenotic valve orifice areas. In: Baim DS,Grossman W (eds). Cardiac Catheterization, Angiographyand Intervention, 5th edn. Baltimore: Williams & Wilkins,1996:151–65, with permission.)
bradycardic states without prohibitive increasesin mean LAP.
Contrary to what might be expected, decreasingafterload by reducing systemic vascular resistancedoes not always have a beneficial effect for patientswith AS. A reduction in afterload should enhanceLV ejection and thus increase SV. However, theimpedance to LV ejection is largely due to the
fixed outflow obstruction at the aortic valve orifice.Reductions in systemic vascular resistance (SVR)are offset by the large increases in the transvalvulargradient that accompany increased flow across thestenotic valve orifice. Thus, SVR reduction resultsin very little augmentation of CO in patients withsignificant AS. Furthermore, agents used to reduceafterload, such as nitroprusside and hydralazine,

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 140 — #12
140 Chapter 5
decrease aortic diastolic pressure and compromisethe tenuous subendocardial blood flow in thesepatients. In contrast, increases in afterload result inan elevation of LVEDV and LVEDP with mainte-nance of SV in patients with good ventricular func-tion and some preload reserve. In patients with poorventricular function, increasing afterload may resultin a progressive decline in SV and EF secondary toafterload mismatch (see Fig. 5.6).
The term “critical aortic stenosis” commonly isused in association with severe aortic valve disease.This is a poorly defined term, but it is most appropri-ate when describing a pathophysiologic state ratherthan an absolute valve area. Critical AS exists whenpreload reserve is exhausted and EF is reduced suchthat further reductions in aortic valve area will pro-duce increased pulmonary vascular congestion orfurther reductions in SV. Critical AS can exist witha larger valve area in patients with severe concomi-tant diastolic or systolic dysfunction or in patientswith atrial fibrillation.
Anesthetic technique in AS
Goals• Sinus rhythm is essential. Atrial contraction maycontribute up to 40% of LV filling.• Maintain heart rate at 70–90 b/min.• Maintain a PCWP high enough to ensureadequate LVEDV; more full rather than less full.• Maintain afterload. Decreases in diastolic bloodpressure reduce coronary perfusion.• Maintain contractility.
PreinductionAll patients should have adequate IV and centralaccess. ECG monitoring should allow assessmentof leads V5, I, II, III, aVR, aVL, and aVF. Baselinerecording of all seven leads should be obtained forcomparative purposes. Normally, two leads (II andV5) are monitored simultaneously intraoperatively.
A radial artery catheter is placed with local anes-thesia and adequate sedation before induction ofanesthesia. A pulmonary artery catheter can beplaced either before or after induction of anesthe-sia. All of the equipment and medications necessaryfor treatment of dysrhythmias must be available
before placement of the pulmonary artery catheter.In particular, a defibrillator with demonstrated con-sistent synchronization to the patient’s electro-cardiogram (ECG) signal must be in the room if lossof sinus rhythm requires immediate cardioversion.Placement of the pulmonary artery catheter beforeinduction allows optimization of preload and after-load before induction of anesthesia. Placement afterinduction is not associated with poor outcome andmay be better tolerated by the compromised patient.
The presence of compensatory LV concentrichypertrophy will cause LV compliance to be con-siderably less than RV compliance. This will causethe right atrial pressure to underestimate the PCWPand LVEDP. Therefore, the peak A-wave pressureof the PCWP trace is used. The LVEDP measured atthe time of cardiac catheterization is a useful guideas to the PCWP that will be necessary to obtainthe end-diastolic volume that will optimize SV. Ingeneral, for patients with significant AS, a PCWPA-wave pressure of 15–25 mmHg is appropriate. Inthe absence of RV failure, the mean right atrialpressure will be 5–8 mmHg. If necessary, volumeinfusion before induction can optimize LVEDV.
Induction and maintenanceThere is no one anesthetic technique superior toanother. Induction agents must be chosen basedupon the ability to achieve the anesthetic goals out-lined above. Etomidate, barbiturates, or high dosenarcotics are appropriate. Propofol may cause asevere reduction in blood pressure and should beused with great caution in patients with AS. A highdose narcotic induction is indicated in some criti-cally ill patients. Generally, a balanced technique ofnarcotics and inhalational agents for maintenanceof anesthesia is appropriate. Fentanyl (10–25 µg/kg)or sufentanil (2–5 µg/kg) can be used as the pri-mary anesthetic for maintenance before CPB. Theseagents have no effect on myocardial contractilityand cause a reduction in peripheral vascular resis-tance only through a diminution in central sympa-thetic tone. Compared with fentanyl, sufentanil ismore likely to cause a fall in mean arterial pressuresecondary to a reduced peripheral vascular resis-tance in patients with valvular heart disease. On

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 141 — #13
Anesthesia for Valvular Heart Disease 141
the other hand, patients with valvular heart dis-ease receiving sufentanil are less likely to requiresupplemental anesthesia or vasodilator therapy forskin incision, sternotomy, sternal spread, or aorticmanipulation.
After preoxygenation, with the patient breathing100% oxygen, induction begins with a deliberateinfusion of a hypnotic, midazolam, and fentanyl orsufentanil. Compared with patients with coronaryartery disease, patients with valvular heart dis-ease have a lower narcotic requirement to achieveunconsciousness. This is probably due to a lower COwith a relative greater distribution of output to thebrain and spinal cord. After loss of consciousness,the hemodynamic response to insertion of an oralairway followed by insertion of a urinary cathetercan gauge the need for additional narcotic to bluntthe hemodynamic response to tracheal intubation.Laryngoscopy is performed carefully and should notbe prolonged. If an upward trend in heart rateor blood pressure occurs, laryngoscopy should beterminated and additional narcotic administered.If there is poor visualization of the larynx, laryn-goscopy should be terminated and intubating con-ditions improved by changing head position, usinga stylet, or changing blades. This approach will helpprevent long stimulating laryngoscopies that com-promise hemodynamics. A TEE probe can be placedafter tracheal intubation.
To optimize heart rate, the choice of musclerelaxant is critical. For patients who are poorlybeta-blocked and for those not taking beta-blockers,fentanyl or sufentanil in combination with vecuro-nium is a good choice. Vecuronium 0.02 mg/kgor cisatracurium 0.04 mg/kg can be administeredapproximately 1–2 minutes before starting the nar-cotic infusion. As the patient loses conscious-ness, the remainder of the total dose of 0.1 mg/kgof vecuronium or 0.2 mg/kg of cisatracuriumis administered, and controlled ventilation with100% oxygen initiated. For patients who are wellbeta-blocked, fentanyl or sufentanil in combina-tion with pancuronium works well. Sufentanil incombination with vecuronium or cisatracurium ina well beta-blocked patient may result in signif-icant bradycardia. Pancuronium 0.02 mg/kg canbe administered approximately 1–2 minutes before
starting the narcotic infusion. As the patient losesconsciousness, the remainder of the 0.1 mg/kg doseis administered and controlled ventilation is initi-ated. Using this “priming dose” of neuromuscularblockade minimizes the risk of narcotic-inducedrigidity without undue stress to the patient.
Bradycardia with hemodynamic compromiserequires immediate treatment. A small dose of pan-curonium (1–3 mg) can be effective if vecuroniumwas the neuromuscular blocking agent. Atropineis not a good choice for two reasons: its effecton heart rate, even in small doses (0.2 mg), isunpredictable; and tachycardia may be initiated bylarger doses. Atropine, unlike β1-adrenergic agents,increases heart rate without any reduction in theduration of systole. Thus, for equal increases inheart rate, atropine will cause a greater reductionin the duration of diastole and will compromisesubendocardial perfusion to a greater degree thana β1-adrenergic agent. Ephedrine (a direct- andindirect-acting β- and α-agonist) is a reliable agentto increase heart rate without compromising dias-tole. In addition, the augmentation in diastolic bloodpressure obtained is beneficial when hypotensionaccompanies bradycardia.
Tachycardia requires aggressive treatment toavoid subendocardial ischemia and hemodynamiccompromise. The first strategy should be to termi-nate any noxious stimuli and increase the depthof anesthesia if appropriate. Esmolol is an excel-lent agent to acutely reduce heart rate in a patientwith AS. Esmolol is a β1 selective agent with anelimination half-life of 9 minutes. This short half-life renders esmolol quite useful for patients withpoor ventricular function or bronchospastic diseasebecause, if it is not tolerated, therapy is terminatedquickly. Furthermore, unlike longer acting beta-blockers, esmolol can be used aggressively in thepre-CPB period without fear that it will compromisetermination of CPB.
If hypotension due to reduced peripheral vascu-lar resistance occurs during induction, small dosesof phenylephrine (40–120 µg) and volume infusionto increase preload to preinduction levels usuallywill correct the problem. TEE is very useful at thispoint. If TEE reveals a dilated, hypokinetic LV or ifthe patient fails to respond with a prompt increase

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 142 — #14
142 Chapter 5
in aortic blood pressure, an inotropic agent may beindicated. Dobutamine 5–10 µg/kg/min is a reason-able choice because it is unlikely to cause tachy-cardia. IV nitroglycerin should be started to treatthe elevated PCWP that inevitably accompanies thisdownward spiral. The infusion can be started at0.15–0.30 µg/kg/min and titrated as necessary.
If surgical stimulation (skin incision, sternotomy,sternal spreading, or aortic manipulation) pro-duces hypertension, additional doses of sufentanil(1–3 µg/kg) or fentanyl (5–15 µg/kg) may be neces-sary. If this fails to control the hypertension, the useof additional agents will be necessary. Vasodilationwith increasing inhalational agents may resolve theissue. Alternatively, sodium nitroprusside can betitrated easily and terminated quickly. This makesit an ideal choice for treatment of transient ele-vations in peripheral vascular resistance. Althoughrelatively large doses of nitroglycerin may be neededto control systemic hypertension, nitroglycerin is abetter choice than nitroprusside for cases in whichmyocardial ischemia exists.
Benzodiazepines are an essential componentof the anesthetic, and midazolam is the mostcommonly used. Doses range from 5 to 15 mg.Administration in conjunction with fentanyl orsufentanil may cause decreases in peripheral vascu-lar resistance with subsequent hypotension. There-fore, caution is necessary. Midazolam in incrementsof 1–2 mg or lorazepam in increments of 0.5–1.0 mgare reasonable.
In recent years, there has been movement awayfrom a pure high-dose narcotic anesthetic. Inhala-tional anesthetics are now common in all types ofcardiac surgery. Nitrous oxide (N2O) in associationwith high-dose opiates causes systolic dysfunctionin patients with coronary artery disease, particularlythose with an LVEDP > 5 mmHg. N2O combinedwith high-dose opiates elevates pulmonary vascularresistance (PVR), particularly in the presence of pre-existing pulmonary hypertension. Because of thepotential for altered myocardial oxygen balance inall patients with AS, and the presence of an elevatedPVR in some patients, N2O must be used with cau-tion, if at all. Isoflurane is a potent vasodilator thatcauses little depression of systolic function. Sevoflu-rane and desflurane have similar effects. However,
care must be taken to avoid decreases in peripheralvascular resistance and hypotension when they areused in patients with AS. Controversy exists regard-ing whether isoflurane in the presence of coronarystenosis is responsible for producing a coronary stealphenomena leading to ischemia. There may be ben-eficial effects of inhalational anesthetics as pharma-cologic preconditioning agents. There is a growingbody of evidence demonstrating that inhalationalagents reduce the markers of myocardial injury afteran ischemic-reperfusion injury.
Post-CPB managementAfter aortic valve replacement, the obstruction toforward flow is eliminated. With allograft replace-ment, the valve gradients are usually normal, andwith mechanical valves there is a small peak gra-dient of 10–20 mmHg. The reduced transvalvulargradient allows the hypertrophied LV to signifi-cantly decrease left ventricular end systolic vol-ume (LVESV); thus, augmenting SV and EF (seeFig. 5.6). In addition, the ventricle can now respondto further reductions in afterload with an increasein SV.
As with any procedure requiring cardiople-gia, the LV systolic function may be compro-mised by inadequate myocardial protection duringCPB. It may, therefore, be necessary to relyon inotropic agents for augmentation of sys-tolic function despite the dramatic reduction inafterload. This is particularly true if there iscoexisting coronary artery disease. Epinephrine0.015–0.030 µg/kg/min, dopamine 1–5 µg/kg/min,or dobutamine 5–10 µg/kg/min are reasonablechoices, providing inotropic support with littleconcomitant vasoconstriction and afterload increase.
Because there is no significant regression of con-centric hypertrophy for 6–12 months after aorticvalve replacement, the compliance characteristics ofthe LV will be unchanged in the post-CPB period.In fact, poor subendocardial myocardial protectionduring aortic cross-clamping may result in ischemicdiastolic dysfunction. Sinus rhythm enhances fill-ing. The peak A-wave pressure must be high enoughto ensure adequate LVEDV. In general, becauseLVESV will be lower because of the reductionin impedance to ventricular ejection, LVEDV, and

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 143 — #15
Anesthesia for Valvular Heart Disease 143
therefore the A-wave pressure, need not be ashigh in the post-bypass period. A-wave pressuresof 10–20 mmHg are usually adequate. Subendocar-dial perfusion will remain compromised in diastoleand, therefore, aortic diastolic blood pressure mustremain high enough to ensure perfusion.
Tachycardia remains detrimental because of itseffects on subendocardial perfusion. Slower heartrates are now better tolerated because of the dra-matic reduction in the transvalvular gradient withsurgery.
Because the surgical procedure requires an aorto-tomy with subsequent repair, it is helpful to avoidhypertension, which places undue stress on theaortic suture line. The atrioventricular (AV) nodelies proximal to the aortic valve annulus and maybe transiently or permanently damaged after valvereplacement. Ventricular pacing may be necessary.
Aortic regurgitationAortic regurgitation (AR) may result from dam-age to the aortic valve leaflets or from dilatation ofthe aortic root. Damage to the aortic valve leafletsresults in a mechanical valve defect, whereas aor-tic root dilatation results in functional aortic valveimpairment. AR may be acute or chronic in nature.Infective endocarditis with destruction of the valveleaflets is a cause of acute AR. There may be actualdestruction of the valve leaflet by the infective pro-cess. Alternatively, the infective process may causeperforation of a leaflet or the presence of vegetationsmay prevent proper apposition of the leaflets.
Trauma with cusp rupture or laceration mayresult in acute AR. Aortic dissection may causeAR through a variety of mechanisms. Dilation ofthe proximal aortic root and valve annulus resultsin poor apposition of the leaflets and functionalvalvular incompetence. Dissection with intramuralhematoma formation may distort the valve. Dissec-tion can result in mechanical incompetence whenthe valvular annulus is involved.
Connective tissue diseases such as Marfan syn-drome, Ellers–Danlos syndrome, and pseudoxan-thoma elasticum produce chronic AR. Progressiveaortic root dilation with subsequent dilation of thevalve annulus results in functional AR. As timepasses, the poorly apposed valve leaflets begin to
bow, thicken, and shorten; resulting in worseningregurgitation. These patients may also suffer frommitral valve incompetence. A congenital bicuspidaortic valve is present in approximately 0.5% of thepopulation. This condition is associated with AR.Bicuspid aortic valves with a genetic mutation inthe fibrillin gene are seen in Marfan syndrome.
Inflammatory diseases of the aorta, such assyphilis, rheumatoid disease, ankylosing spondyli-tis, and Takayasu’s aortitis, may produce chronicAR. These diseases cause distortion of the aorticroot as well as destruction of valve cusps and annu-lar support structures. MR is common in theseconditions.
Aortic valve leaflet damage due to rheumaticfever is a common cause of chronic mechanicalAR. However, isolated AR-secondary to rheumaticfever is rare. In rheumatic fever, there is infiltra-tion of fibrous tissue in the valve cusps causingretraction. This results in poor valve apposition indiastole with subsequent regurgitation. At the sametime, commissure fusion results in AS. Mitral valveinvolvement is common in rheumatic heart disease.
Pathophysiology and adaptation in ARAR is a volume overload lesion that may be acuteor chronic in nature. The extent of regurgitationdepends on the diastolic pressure gradient betweenthe aorta and the left ventricle, the time availablefor regurgitation (diastole), and the effective regur-gitant orifice area. The pressure gradient is deter-mined by the aortic diastolic pressure, ventricularearly diastolic pressure, and ventricular compliance.Regurgitation ceases when the ventricular diastolicand aortic diastolic pressures equalize. The dura-tion of diastole is inversely related to heart rate asdemonstrated in Fig. 5.8.
Chronic volume overloading of the left ventri-cle results in eccentric ventricular hypertrophy orincreased ventricular radius. The details of this pro-cess are summarized in Fig. 5.10a. Whereas bothLVESV and LVEDV increase, LVEDV increases to agreater extent. This results in an enhanced SV withno need for an increased EF. The slope of the dias-tolic pressure–volume curve is little changed andcompliance is only slightly increased. The entirepressure–volume loop is shifted to the right. This

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 144 — #16
144 Chapter 5
Wal
l str
ess
(a)
Volume
EFx 60%
EFx 55%
Norm
alEc
cent
ric h
yper
troph
y
(b)
Wal
l str
ess
Volume
Pre-op.EFx 45%Po
st-o
p.Com
pens
ated Mild
dys
func
tion
Mild
dys
func
tion
Post opPost opEFEFx 55% 55%Post-op.EFx 55%
Mild
dys
func
tion
Fig. 5.10 Left ventricular wall stress–volume loops forpatient with progressive aortic stenosis. (a) Wallstress–volume loops of normal ventricle and of ventriclehaving developed eccentric hypertrophy in response tochronic volume overload of aortic regurgitation (AR) areshown. The ventricle with eccentric hypertrophy has areduced isovolumic contraction phase and has its entirewall stress–volume relationship shifted to the right. Theseadaptations allow the ventricle to deliver large strokevolume with nearly normal ejection fraction (EF) despiteelevation of end-systolic wall stress. (b) Wallstress–volume relationships in a ventricle with chronicaortic regurgitation and mild systolic dysfunction.Progressive systolic dysfunction leads to exhaustion ofpreload reserve and elevation of wall stress due to largeventricular radius. This, in turn, results in reduced strokevolume (SV) and EF (EF = 45%). After surgicalreplacement of aortic valve, ventricular radius and wallstress are reduced and near-normal SV and EF existdespite the presence of systolic dysfunction (EF = 55%).(From Hurst JW. The Heart, 5th edn. New York:McGraw–Hill, 1985:818, with permission.)
rightward shift of the diastolic pressure–volumecurve allows low diastolic pressures at very largeend-diastolic volumes. The large increase in ventric-ular radius that accompanies eccentric hypertrophyelevates wall stress and stimulates some degree ofconcentric hypertrophy. This compensation is notcomplete and wall stress remains elevated both inend systole and end diastole (see Fig. 5.10a).
Unique LV pressure loading exists in AR, as illus-trated in Fig. 5.10a. The isovolumic phase of ven-tricular systole is of very short duration and limitedpressure generation. This allows a greater portionof myocardial energy expenditure directed towardejecting a large volume and less toward overcomingimpedance to begin ejection.
In acute AR, there is not ample time for com-pensatory eccentric hypertrophy to occur. With-out increased diastolic compliance and the rightshift of the pressure–volume loop, the regurgitatedvolume results in a very high LVEDP. BecauseLVEDP rises rapidly to equal aortic end-diastolicpressure, the gradient for regurgitation is abolishedquickly. As a result, the aortic end-diastolic pressuregenerally is higher and the regurgitant volumegenerally is smaller in acute versus chronic AR.Ventricular dilation from acute AR may result infunctional MR. For other patients, the rapid risein diastolic pressure may result in early diastolicequalization of left atrial and LV pressures such thatpremature mitral valve closure occurs. In this set-ting, the PCWP or LAP will greatly underestimatethe LVEDP.
In chronic AR, the increased compliance andthe rightward shift of the diastolic pressure–volumecurve allows passive filling of the left ventriclein early and mid-diastole. Therefore, LVEDV ismaintained even without an atrial kick, exceptin end-stage AR, in which preload reserve isexhausted and the ventricle operates on the steepportion of its diastolic pressure volume curve(Fig. 5.10b).
In acute AR, increased ventricular complianceand a rightward shift of the diastolic pressure–volume curve are absent. In this setting, an atrialsystole may be necessary to increase the left atrialto LV pressure gradient enough to allow filling ofthe left ventricle. If premature mitral valve closure

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 145 — #17
Anesthesia for Valvular Heart Disease 145
occurs due to rapid rise of LVDP, diastolic fillingfrom the left atrium (LA) will be reduced.
Eccentric hypertrophy and the altered pressure–volume relationship allow large increases in LVEDVwith minimal increases in LVEDP in patients withchronic AR. This affords a great deal of preloadreserve. Stroke volume can be increased by preloadaugmentation without pulmonary congestion. Incontrast, in acute AR preload reserve is nearlyexhausted. Without adequate time for adaptation,the left ventricle operates on the steep portion of itsdiastolic pressure–volume curve.
The alterations in myocardial oxygen consump-tion in AR are shown in Table 5.3. Patients withchronic AR may remain symptom-free for manyyears despite progressive decreases in systolic func-tion. The enormous preload reserve available tothese patients allows preservation of SV by pro-gressive increases in LVEDV in the face of declin-ing contractile function. When preload reserve isexhausted, SV falls. At this point, systolic func-tion is compromised and symptoms of reduced COmanifest (see Fig. 5.10b).
As contractility decreases, LVEDV increases: SV ismaintained, but EF falls. EF will remain in the lownormal range until significant systolic dysfunction
occurs. In fact, valve replacement is recommendedfor patients with AR without symptoms whenventricular dilation and a depressed EF are present.
As with AS, RV function is not directly affectedby AR until pulmonary arterial hypertension devel-ops. In chronic AR, ventricular dilation may lead tofunctional MR. This, in turn, may lead to a gradualelevation in left atrial and pulmonary artery pres-sures. If this situation persists, pulmonary arterialhypertension will soon develop. RV failure devel-ops if the pulmonary arterial hypertension becomessevere.
In acute AR, functional MR from ventricular dila-tion is tolerated poorly. Acute ventricular dilationand functional MR leads to an immediate and pro-found elevation in LAP. Pulmonary vascular con-gestion with interstitial pulmonary edema ratherthan secondary pulmonary artery hypertension andRV failure ensues.
The relationship between heart rate and CO inAR is complex. Recall that the regurgitant volumeis in large part determined by the length of dias-tole. Figure 5.8 illustrates the inverse relationshipbetween heart rate and the length of diastole.Bradycardia (heart rate < 60 b/min) is detrimen-tal in AR for several reasons. It increases the
Table 5.3 Myocardial oxygen consumption in aortic regurgitation.
Myocardial oxygen consumption is increased by:• The large mass of myocardium• The enormous volume of work done by the left ventricle. Volume work increases oxygen consumption, but to a muchlesser extent than pressure work. The isovolumic contraction phase is highly energy consumptive. Because of the lowaortic diastolic blood pressures present in AR, the isovolumic contraction phase is very brief and represents only a smallportion of the total work done by the ventricle (see Fig. 5.10a). A greater portion of the total workload is devoted to thegeneration of volume ejection, which is an energy-efficient process• Despite the development of eccentric hypertrophy and some degree of concentric hypertrophy, wall stress remainsslightly elevated in both systole and diastole (see Fig. 5.10a). Recall that wall stress determines oxygen consumption in theejection phase of ventricular contraction
Myocardial oxygen delivery is compromised by:• The low diastolic aortic pressure characteristic of AR reduces the gradient for coronary blood flow (coronary perfusionpressure = aortic diastolic blood pressure− LVEDP). This is particularly true in acute AR, in which precipitous increases inLVEDP occur. Bradycardia can exacerbate the situation. Bradycardia increases the regurgitant volume and thus increasesLVEDP• In acute AR due to aortic dissection, one or both of the coronary ostia may be involved in the dissection. This mayacutely and drastically reduce coronary blood flow
AR, aortic regurgitation; LVEDP, left ventricular end-diastolic pressure.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 146 — #18
146 Chapter 5
regurgitant volume per beat, which tends to loweraortic diastolic blood pressure and increase LVEDP.This decreases the gradient for subendocardial oxy-gen delivery. Simultaneously, the large SV thataccompanies bradycardia increases wall tension andoxygen consumption. Forward SV and CO fallbecause the regurgitant volume represents a largeportion of the total SV (the regurgitant fraction ishigh).
With tachycardia, the regurgitant volume perbeat falls, whereas the regurgitant volume perminute may remain unchanged. The relationshipbetween regurgitant volume and total SV (theregurgitant fraction) does not remain constant asheart rate increases. Therefore, CO may decrease,remain unchanged, or increase with a heart rateincrease. A change in rate of 75–85 b/min increasesCO significantly. Further increases in heart ratefrom 85–110 b/min show a trend toward a slightadditional increase in CO. Little additional change,or a slight decrease in CO, occurs when the heartrate is in excess of 110–120 b/min. Therefore,extremes of tachycardia offer no advantage overmore moderate rates of 75–85 b/min in improvingCO. Furthermore, in patients with coronary dis-ease, the elevated heart rates increase demand anddecrease oxygen supply.
Increased afterload is detrimental to patients withboth acute and chronic AR because it increases theregurgitant volume per beat. Recall that one of thedeterminants of the regurgitant volume is the gradi-ent between the aorta and the left ventricle in earlydiastole. It is important, then, to avoid agents andto blunt stimuli that increase afterload.
Efforts to actively decrease afterload in patientswith AR are not uniformly helpful. In chronic AR,vasodilators benefit patients who have a depressedEF, high LVEDP, decreased forward CO, and higharterial pressure. Patients who do not meet thesecriteria may actually experience diminished for-ward CO with vasodilator therapy due to preloadreduction from venodilation. In acute AR, vasodila-tor therapy is usually warranted. Recall that theabsence of adequate ventricular compensation cre-ates a very high LVEDP and that a low forwardCO exists despite preserved systolic function. After-load reduction will reduce LVEDP and increase
forward CO. In addition, functional MR due to ven-tricular dilation improves in these patients with areduction in ventricular size by vasodilators.
In properly selected patients, vasodilator ther-apy enhances ventricular performance in two ways.Reduced aortic impedance enhances systolic per-formance and the regurgitant volume is reducedby a reduction in the diastolic aortic to LV gradi-ent. It is important to ensure that the reductionin aortic diastolic blood pressure that accompaniesvasodilator therapy is not so severe as to jeopardizesubendocardial perfusion.
Anesthetic technique in AR
Goals• Maintain sinus rhythm (although this is not asimportant as in AS).• Maintain heart rate at 75–85 b/min; faster betterthan slower.• Avoid afterload increases; pursue afterload reduc-tion in acute AR and in chronic AR when LVEDPand arterial blood pressure are elevated, and CO andEF are depressed.• Maintain a PCWP high enough to guaranteeadequate LVEDP.• Maintain contractility.
PreinductionThe preinduction routine and monitoring is thesame as for AS.
In chronic AR, a large LVEDV is necessary toensure an adequate forward CO in the face ofregurgitation. Because of the increased ventricularcompliance and the right shift of the pressure–volume relationship, the peak A-wave pressure willdiffer little from mean PCWP. Likewise, LVEDV willbe supplemented with only small increases in themean PCWP. For patients with preserved LV func-tion, a mean PCWP in the range of 10–15 mmHgwill ensure optimal LVEDV. Serial COs obtainedin conjunction with volume infusion will pro-vide a Frank–Starling relationship curve to identifyoptimal preload.
For patients with depressed ventricular func-tion who have exhausted preload reserve, optimalpreload will occur with a peak A-wave pressure

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 147 — #19
Anesthesia for Valvular Heart Disease 147
in the range of 20–25 mmHg. For these patients,afterload reduction is indicated. Sodium nitroprus-side is the agent of choice. It is easy to titrateowing to its very short half-life. Start the infu-sion at 0.15–0.30 µg/kg/min and titrated to effectwith careful attention CO, arterial blood pressure,and LVEDP. Although nitroprusside is primarily anarterial vasodilator, it has some vasodilatory effectson the venous system. It is important not to letreductions in preload offset the beneficial effects ofarterial dilation. If necessary, volume infusion canmaintain PCWP in the range of 10–15 mmHg.
In acute AR in which premature closure of themitral valve occurs, mean PCWP will underestimateLVEDP. When mitral incompetence from ventricu-lar dilation occurs, mean PCWP will overestimateLVEDP in direct proportion to the amplitude andduration of the regurgitant V wave. These patientsare very ill and may require pharmacologic sta-bilization before induction. Due to the lack ofcompensatory alterations in the pressure–volumerelationship, these patients may have a PCWP in therange of 20–25 mmHg to maintain a low normal car-diac index. Afterload reduction with nitroprusside isindicated. Inotropic support should be added if thecardiac index remains depressed (<2.2 L/min/m2)
or functional MR persists due to a dilated ventricle.Either dopamine (1–5 µg/kg/min) or dobutamine(5–10 µg/kg/min) can be used; neither will causean elevation of afterload.
Use of an intra-aortic balloon pump is contraindi-cated in AR because balloon inflation and augmen-tation of diastolic blood pressure will worsen theregurgitation.
Induction and maintenanceInduction of anesthesia can be accomplished with anumber of agents as long as the primary hemody-namic goals are obtained. In stable patients, sodiumthiopental or etomidate are appropriate. Alterna-tively, a high dose narcotic and benzodiazepineinduction is safe. In the critically ill patient withacute AR, great caution is advised. Many of thesepatients require inotropic and vasodilatory supportprior to induction of anesthesia. The addition ofthe anesthetic agents may reduce systemic bloodpressure and inotropy to a critically dangerous level.
Muscle relaxants are chosen with optimization ofheart rate in mind. In the absence of beta block-ade, the vecuronium–fentanyl or vecuronium–sufentanil combination is a good choice if a smallheart rate decrease is desired. The pancuronium–fentanyl or pancuronium–sufentanil combination ismore likely to cause a heart rate increase, which isadvantageous for those patients with bradycardia.
Bradycardia with hemodynamic compromisemust be treated promptly. A small dose of pancuro-nium (1–3 mg) is often effective if vecuronium orcisatracurium has been used. Atropine 0.4–0.8 mgis a reasonable choice despite the risk of tachy-cardia because tachycardia is well tolerated bythese patients. Ephedrine is a poor choice becausethe concomitant increase in afterload may bedetrimental.
Hypotension must not be treated routinely withvasopressors because these arterial vasoconstrict-ing agents may increase the regurgitant volumeworsening the situation. If heart rate and preloadare optimized, then augmentation of SV withan inotropic agent should be initiated. Dopamine1–5 µg/kg/min or dobutamine 5–10 µg/kg/min willboth augment CO without increasing afterload.When AR occurs in conjunction with an aortic dis-section, inotropic agents may worsen the dissectionby increasing shear forces on the aortic wall.
In emergency patients deemed at high-risk foraspiration, the induction sequence can be safelymodified. Preoxygenation and cricoid pressureare indicated. Induction agents include etomidate0.15–0.30 mg/kg, succinylcholine 1.0–1.5 mg/kg,in conjunction with fentanyl 10 µg/kg or sufen-tanil 1 µg/kg. Alternatively, sufentanil 5 µg/kg andsuccinylcholine 1.0–1.5 mg/kg can be used safely.
Post-CPB managementAfter aortic valve replacement for chronic AR,the impedance to ventricular ejection increases.The ventricle that has undergone compensationfor a volume overload lesion is now faced witha relative pressure overload. The competent aor-tic valve causes an elevation of ventricular pres-sure during the isovolumic contraction phase (seeFig. 5.10b). The elimination of regurgitation viathe competent valve greatly reduces the need for

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 148 — #20
148 Chapter 5
a large total SV. Therefore, a greater proportion oftotal myocardial oxygen consumption goes towardthe more energy-consumptive process of pressuregeneration to begin ejection and less toward vol-ume ejection. Although there is an increase in LVpressure generation, wall stress does not increasesubstantially because ventricular radius is greatlyreduced by elimination of the regurgitant vol-ume. Nonetheless, if poor myocardial protection isobtained during bypass and aortic cross-clamping,or if depressed systolic function exists preopera-tively, inotropic support of systolic function maybe necessary in the post-bypass period. Epinephrine0.015–0.030 µg/kg/min, dopamine 1–5 µg/kg/min,or dobutamine 5–10 µg/kg/min are good choicesbecause they provide inotropic support with littlevasoconstrictor activity at these doses.
After valve replacement in acute AR, the elimi-nation of the regurgitant fraction allows the ven-tricle to maintain CO with a much lower LVEDV;therefore, LVEDP drops precipitously. Wall stressfalls. Inotropic support may be necessary when pre-operative systolic and diastolic dysfunction existsdue to subendocardial ischemia or where myocar-dial preservation on bypass is poor. Epinephrine,dopamine, or dobutamine are good choices.
All LV diastolic filling occurs via the mitral valvewhen regurgitation is abolished. Therefore, atrialsystole becomes more important in ensuring ade-quate LVEDV. Maintenance of sinus rhythm or AVsequential pacing becomes necessary. Bradycardiawill be better tolerated in the post-bypass period.
In chronic AR, there are no significant alterationsin the pressure–volume relationship and eccentrichypertrophy for 6–12 months after valve replace-ment (see Fig. 5.10b). Therefore, LVEDP will remainlow, even for large LVEDV. This low LVEDP in com-bination with the elevation in aortic diastolic bloodpressure will greatly improve myocardial oxygendelivery. The temptation when CO is low will beto use the large preload reserve available in thesepatients. Because ventricular pressure is elevatedduring the prolonged isovolumic contraction phase,wall stress for a given LVEDV will be greater in thepost-bypass period. Efforts to increase preload tocontend with poor systolic function or high after-load states will result in afterload mismatch and
declining systolic function. A mean PCWP or LAP of10–15 mmHg usually is adequate. A better approachwould be inotropic support with epinephrine orafterload reduction with sodium nitroprusside asdescribed previously.
In acute AR, there is little or no alterationin the pressure–volume relationship or eccentrichypertrophy and postoperative preload reserve willresemble that of a normal ventricle.
Because the surgical procedure requires an aorto-tomy with subsequent repair, it is helpful to avoidhypertension, which places undue stress on theaortic suture line. The AV node lies proximal tothe aortic valve annulus and may be transientlyor permanently damaged after valve replacement.Ventricular pacing may be necessary.
The mitral valve
AnatomyThe mitral valve acquired its name in the sixteenthcentury because of its resemblance to a bishop’smitre. In a normal heart, the mitral valve separatesthe left ventricle from the LA, pulmonary circula-tion, and entire right side of the heart. The valveis bicuspid with an anterior and posterior leaflet.The anterior leaflet is the larger of the two leaflets,accounting for two-thirds of the surface area of thevalve. The anterior leaflet base-to-coaptation dis-tance is longer than that of the posterior leaflet. Theposterior leaflet wraps around the anterior leaflet,accounting for only one-third of the valve’s surfacearea and two-thirds of the annular circumference.The mitral annulus is a fibrous ring surroundingthe mitral valve. The anterior leaflet portion of theannulus is part of the heart’s fibrous skeleton. Thisskeleton also has a common attachment to the leftcoronary and noncoronary cusps of the aortic valve.The coaptation points of the anterior and posteriorleaflets at the annulus are called the anterolateraland posteromedial commissures. The leaflets them-selves are attached to the anterolateral and postero-medial papillary muscles via the chordae tendineae.During ventricular systole, the contraction of thepapillary muscles prevent mitral leaflet prolapse.The American Society of Echocardiography and theSociety of Cardiovascular Anesthesiologists have

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 149 — #21
Anesthesia for Valvular Heart Disease 149
adopted the Carpentier classification of the mitralvalve. This classification divides the three scallopsof the posterior leaflet into P1, P2, and P3. Theanterior leaflet is similarly divided into the threesegments A1, A2, and A3, which oppose the corre-sponding scallops of the posterior valve. The coapta-tion of A1/P1 at the annulus form the anterolateralcommissure. The coaptation of A3/P3 at the annulusform the posteromedial commissure.
Mitral stenosisMitral stenosis (MS) is almost always rheumaticin origin. Rheumatic fever results in fusion ofthe mitral valve apparatus in various locations.The site of valve apparatus involvement deter-mines whether the valve will be primarily stenoticor incompetent in nature. Fusion of the cuspsand commissures results in a stenotic valve orifice(Fig. 5.11a,b). The valve leaflets may become sorigid that they are incapable of closing, in whichcase MS and incompetence coexist.
Pathophysiology and adaptation in MSThe left ventricle in MS is typically under filled. Thenatural history of the disease is a gradual reductionin the mitral valve area from a normal of 4–6 cm2
to <1 cm2 over 3–4 decades. The length of diastole,the pressure gradient between the LA and the leftventricle and the mitral valve area, determine LVfilling. As the mitral valve orifice decreases in size,there is a gradual increase in impedance to LV filling,and a pressure gradient develops across the valvesuch that LAP exceeds LV diastolic pressure.
Early in the disease process, complete LV fillingoccurs without an elevation of mean LAP if dias-tole is long enough and if an atrial systole exists. Asthe valve area decreases and the transvalvular gradi-ent rises, a long diastole and an elevated mean LAPare necessary to ensure ventricular filling. Eventu-ally, the valve orifice narrows to the point at whichthese compensatory mechanisms fail. The pressure–volume loop for MS is illustrated in Fig. 5.12.
Because MS presents a fixed resistance to ven-tricular inflow and because the atrial systole is ofshort duration, a large portion of the kinetic energyproduced by atrial systole is dissipated in overcom-ing resistance to inflow. The role of atrial systole in
(a)
(b)
Fig. 5.11 (a) This is a patient with rheumatic mitralvalve disease. There is commissural fusion with a classic“hockey stick” deformity of the anterior mitral valveleaflet (arrow) seen in diastole. (b) In systole this samepatient now exhibits significant mitral regurgitation. Theleft atrium is severely dilated. Mixed lesions, mitralstenosis with regurgitation, are common in patientswith rheumatic valvular disease.
augmenting LVEDV in MS is less dramatic than inAS but important nonetheless. At heart rates of80–110 b/min, the loss of atrial systole results in a20% decrease in diastolic flow per beat and CO inpatients with moderate and severe MS. However, inmoderate and severe MS, the presence of an atrialsystole alone will not maximize LV filling, and anelevation of mean LAP is necessary.
The high LAP that develops as a result of thestenotic mitral valve orifice results in left atrialhypertrophy and left atrial distention. This dis-tension results in the development of atrial dys-rhythmias, the most common of which is atrialfibrillation. In severe MS, atrial fibrillation gener-ally is the rule. When atrial systole is lost, diastolicflow is dependant on mean LAP. The higher the

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 150 — #22
150 Chapter 5
Wal
l str
ess
Normal
Mitral stenosis
Volume
Fig. 5.12 Pressure–volume loop from a patient withmitral stenosis. The left-ventricular end-diastolic volume(LVEDV) is severely limited compared to a normalpatient. This preload reduction results in reduced strokevolume and cardiac output. (From DiNardo JA.Anesthesia for valve replacement in patients withacquired valvular heart disease. In: DiNardo JA (ed).Anesthesia for Cardiac Surgery, 2nd edn. Stamford, CT:Appleton & Lange, 1998:109–40, with permission.)
mean LAP, the more complete the LV filling. MeanLAP is limited by the development of pulmonarycongestion, and pressures >25 mmHg are rarely tol-erated without symptoms. For a given valve areaand LAP, ventricular inflow is determined by thelength of diastole.
Ventricular diastolic function and complianceremain unchanged in MS. Despite this, preloadreserve is severely limited in this lesion. Maxi-mal LVEDV in moderate and severe MS is wellbelow that seen in patients with normal mitralvalves. Mean LAP must be elevated (often to thepoint of pulmonary congestion) to obtain an LVEDVlarge enough to meet baseline CO demands. Fur-ther increases in mean LAP only slightly augmentLVEDV due to the large pressure gradient across thevalve. In addition, this further elevation of meanLAP leads to progressive pulmonary congestion andpulmonary edema.
There are no special considerations regardingmyocardial oxygen balance in patients with MS. Itis important, however, to keep in mind the relation-ship between the length of diastole, aortic diastolicpressure, and LVEDP on subendocardial perfusion.It is also important to determine the extent of coro-nary artery disease in patients with MS and anginapectoris.
Myocardial fibrosis in the posterobasal regionof the LV may result in segmental wall motionabnormalities and reduced systolic performance inpatients with rheumatic MS. Patients with MShave normal indices of LV contractility, but havea reduced EF due to limited preload.
The prolonged elevations of LAP seen in progres-sive MS have profound effects on the pulmonaryvasculature and RV function. Early in the dis-ease, elevated LAP is transmitted to the pulmonaryvenous system, and there is reversible passive ele-vation of the pulmonary artery pressures while PVRremains normal (Fig. 5.13). RV function remainsunchanged.
As the disease progresses, reactive changes occurin the pulmonary vasculature. Prolonged perivas-cular edema results in arterial intimal fibroelastosisand nonreversible elevations in PVR. Progression ofthis process presents a large increase in RV after-load or a “second stenosis” (see Fig. 5.13). The RV ispoorly adapted to generate pressures that approachsystemic. As a result, afterload mismatch occurs,the RV invariably fails, and the RV output falls.Peripheral edema and hepatic congestion ensue. RVfailure and dilation also may lead to functional tri-cuspid regurgitation and worsening symptoms ofright heart failure. In the steady-state, RV outputand LV output must be equal. Therefore, LV out-put is limited by RV failure. Efforts to reduce RVafterload and improve RV output with nitroprussidesignificantly improve systemic output in patientswith elevated PVR.
Figure 5.8 illustrates the reduction in diastolic fill-ing time that accompanies an increase in heart rate.If CO is to remain constant as heart rate increases,then the flow rate across the mitral valve in dias-tole must increase. Recall that as flow rate increasesacross the stenotic valve, the gradient across thevalve will increase by the square of the flow. Thus,the requirement for increased flow can result inprohibitive increases in mean LAP.
Figure 5.14(a–c) illustrates the effect of heart ratechanges in MS. Higher heart rates can potentiallyimprove CO when SV is small. However, in MS,the transvalvular gradient increases so dramaticallywith tachycardia that prohibits increases in meanLAP ensue. At slower rates, more diastolic filling

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 151 — #23
Anesthesia for Valvular Heart Disease 151
Normal
SVC
IVC
5 5 20/5 20/8 (12)
Without pulmonaryvascular disease
With pulmonaryvascular disease
RA RV PA PV LA LV Ao
MVA – 4.0 cm2
MVA – 0.5cm2
MVA – 1.0 cm2
PC
6 6 6
5 5 45/5 45/25 (32) 25 25 25 120/5
20 20 130/20 130/80 (100) 30 30 30 110/5
120/6 120/80
Flow6L/min
Flow5L/min
Flow3 L/min
Tightmitral stenosis
Tightmitral stenosis
Fig. 5.13 Illustration of changes seen with progressionof mitral stenosis (MS). Pressure in each of cardiacchambers and great vessels is indicated.
In MS without pulmonary vascular disease, there isreversible passive elevation of pulmonary vein (PV),pulmonary capillary (PC), and pulmonary artery (PA)pressures while pulmonary vascular resistance remainsnormal. These elevations are secondary to elevation ofleft atrium (LA) pressure, which is necessary to maintainleft ventricle (LV) filling across stenotic mitral valve.Right ventricle (RV) pressure is elevated in response toelevated PA pressure, and RV concentric hypertrophymay result. RV systolic dysfunction usually is not present.
In MS with pulmonary vascular disease, PA pressure iselevated far in excess of LA, PC, and PV pressuresbecause of the presence of pulmonary arterial occlusivedisease with elevated pulmonary vascular resistance. This
results in a second stenosis at the level of the PA.This second stenosis causes dramatic elevations in RVpressure. This RV pressure elevation may result inreduced RV stroke volume due to afterload mismatchand to tricuspid regurgitation due to RV dilation.Reduction in RV stroke volume results directly in adecrease in systemic cardiac output. Similar changeswould be expected over time in patients with sustainedelevations in LA pressure due to mitral regurgitation.Ao, aorta; IVC, inferior vena cava; LA, left atrium; LV,left ventricle; MVA, mitral valve area; PA, pulmonaryartery; PC, pulmonary capillary; PV, pulmonary vein;RA, right atrium; RV, right ventricle; SVC, superior venacava. (From Grossman W. Profile of heart disease. In:Baim DS, Grossman W (eds). Cardiac Catheterization,Angiography and Intervention, 5th edn. Baltimore:Williams & Wilkins, 1996:735–56, with permission.)
time is available to augment LVEDV, but CO iscompromised by bradycardia unless LVEDV is large.Large LVEDVs require a further increase in meanLAP as ventricular compliance diminishes at higherLVEDVs. For these reasons, heart rates between 70and 90 b/min are optimal.
Most patients with moderate and severe MS arein atrial fibrillation. In these patients, control ofheart rate is dependent on adequate control of theventricular response rate to the fibrillating atrium.Drugs used to control the ventricular response rate
by producing AV nodal block such as digoxin,diltiazem, and beta-blockers must be continued.
Patients with MS have severely limited preloadreserve, as discussed previously. Some patients mayhave depressed systolic function due to posterobasalwall motion abnormalities. In addition, high base-line afterload states may limit SV in other patients.For these reasons, patients with MS tolerate largeincreases in afterload poorly because it is likelyto cause afterload mismatch. LV afterload reduc-tion is fraught with hazard because of the limited

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 152 — #24
152 Chapter 5
10000
(a) Mitral stenosis
4.02.0
1.0
0.7
0.5
Assumption: HR = 72 b/min, DFP = 0.58 s/beat
7500
5000
Car
diac
out
put (
cc/m
in)
2500
00 5 10 15 20 25 30 35
Mean gradient (mmHg)40 45 50 55 60
(b)
10000Mitral stenosis
4.02.0
1.0
0.7
0.5
Assumption: HR = 88 b/min, DFP = 0.43 s /beat
7500
5000
Car
diac
out
put (
cc/m
in)
2500
00 15 30
Mean gradient (mmHg)45 60
(c)
10000Mitral stenosis
4.02.0
1.0
0.7
0.5
Assumption: HR = 100 b/min, DFP = 0.32 s/beat
7500
5000
Car
diac
out
put (
cc/m
in)
2 500
00 15 30
Mean gradient (mmHg)45 60
Fig. 5.14 The relationship of heart rate (HR), cardiacoutput (CO), mitral valve area, and diastolic pressuregradient across the mitral valve is illustrated for patientswith mitral stenosis. CO is plotted against diastolicpressure gradient for mitral valve areas ranging from0.5–4.0 cm2. (a) Plot illustrates these relationships forHR of 72 b/min and diastolic filling period (DFP) of0.58 s/beat. (b) Plot illustrates these relationships forHR of 88 b/min and DFP of 0.43 s/beat. (c) Plot illustratesthese relationships for HR of 100 b/min and DFPof 0.32 s/beat.
It is clear that for given CO and HR, diastolic pressuregradient increases as mitral valve area decreases.Furthermore, for a given CO and mitral valve area, thediastolic pressure gradient increases as HR increases.
With CO constant, an increase in HR requires that asmaller volume cross the stenotic mitral valveduring the DFP. This should result in reduction indiastolic pressure gradient. However, increases in HR inthe range examined here progressively shorten thelength of DFP. Reduction in DFP requires thatvolume move across stenotic mitral valve in lesstime, which increases diastolic pressure gradient.Shortening of DFP is the more important determinantof diastolic pressure gradient at HRs illustrated here.(From DiNardo JA. Anesthesia for valve replacement inpatients with acquired valvular heart disease. In:DiNardo JA (ed). Anesthesia for Cardiac Surgery, 2nd edn.Stamford, CT: Appleton & Lange, 1998:109–40,with permission.)
preload reserve in these patients. Recall that after-load reduction will increase SV by reducing LVESVif LVEDV is maintained. Recall also that LVEDV isbelow normal in these patients and small decreasesin mean LAP will result in large decreases in LVEDV
due to the mitral valve gradient. Because afterloadreduction invariably results in some preload reduc-tion due to venodilation, great care must be taken tomaintain preload in these patients when afterloadreducing agents are used.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 153 — #25
Anesthesia for Valvular Heart Disease 153
Critical MSThe term “critical mitral stenosis” commonlydescribes mitral valve disease. Typically, it is used todescribe patients with mitral valve areas <1.0 cm2.As with AS, the term “critical MS” properlydescribes a specific pathophysiologic state, ratherthan an absolute valve area. Critical MS existswhen LA pressure is elevated producing pulmonaryvenous congestion at rest. In the presence of dias-tolic and systolic dysfunction or poorly controlledatrial fibrillation or flutter, critical MS may existwith larger valve areas.
Anesthetic technique in MS
Goals• Maintain sinus rhythm when possible; controlventricular rate in atrial fibrillation.• Maintain heart rate at 70–90 b/min; slower betterthan faster.• Maintain PCWP high enough to ensure as largean LVEDV as possible without pulmonary edema.• Maintain a normal LV afterload; increases arepoorly tolerated. Decreasing afterload is warrantedwhen LV systolic function is poor and afterload ishigh. In this instance, preload must be maintained.• Maintain contractility.• When PVR is high and RV systolic performanceis poor, RV afterload reduction will improve RVand LV output. Caution must be exercised so thatexcessive systemic vasodilation does not result.• Avoid hypercarbia, hypoxemia, and acidemiathat tend to cause pulmonary hypertension andmay result in acute RV decompensation.
PreinductionStandard monitoring and IV access is required.Although placement of a pulmonary artery cathetercan be safely performed after the induction of gen-eral anesthesia, placement of the pulmonary arterycatheter before induction allows recording baselinevalues and optimization of preload and afterload.The insertion distance necessary to obtain a wedgepressure trace is greater (5 cm more via the rightinternal jugular route) in patients with pulmonaryhypertension than in normal patients. The risk ofpulmonary artery perforation is greater in patients
with pulmonary hypertension. Pulmonary arteryrupture may be due to eccentric balloon inflationforcing the catheter tip into the wall of vessel, ves-sel rupture from balloon over-inflation, or distalcatheter migration during balloon deflation.
Patients in sinus rhythm will have a very largeA wave on the PCWP trace, which can be used toestimate LVEDP. Patients in atrial fibrillation haveno A wave, and mean PCWP can be used. It must beremembered that both the A-wave pressure and themean PCWP will overestimate the LVEDP. The erroris compounded (overestimated) with a smaller valvearea and elevated heart rate. The cardiac catheter-ization report will provide information as to therelationship between mean PCWP and LVEDP in agiven patient. In general, for patients with moder-ate to severe MS, a mean PCWP of 20–30 mmHgwill optimize LVEPV. Some patients may present inheart failure and require diuresis preoperatively.
The pulmonary artery catheter allows calculationof PVR and measurement of pulmonary artery andcentral venous pressures (CVPs). This informationis essential in treating RV afterload and improvingRV systolic performance.
For patients with severe RV failure, pulmonarycongestion, and systemic hypotension (systolicblood pressure below 90 mmHg), efforts to improveRV function with vasodilator therapy may be unsuc-cessful due to worsening systemic hypotension.For these patients, the addition of inotropic sup-port is necessary. Dobutamine 5–10 µg/kg/min is agood choice because it has no α-adrenergic activ-ity and little chronotropic activity, and it tends toreduce pulmonary artery pressures. Therefore, itwill not exacerbate pulmonary artery hyperten-sion or cause tachycardia. Other agents of benefitinclude epinephrine 0.03 µg/kg/min or milrinone0.5 µg/kg/min.
Induction and maintenanceAdherence to the hemodynamic goals rather thana specific agent is the most important considerationin choosing an induction and maintenance plan foranesthesia.
Hypotension may be treated initially with volumeinfusion if PCWP has decreased and with cautioususe of phenylephrine 40–80 µg. After preload and

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 154 — #26
154 Chapter 5
heart rate are optimized, it may be necessary touse an inotropic agent. As discussed previously,dobutamine, epinephrine and milrinone are allappropriate choices.
If surgical stimulation (skin incision, sternotomy,sternal spreading, or aortic manipulation) pro-duces hypertension, additional doses of sufentanil(1–2 µg/kg) or fentanyl (5–10 µg/kg) may be nec-essary. If this fails to control the hypertension,the use of additional agents will be necessary.Benzodiazepines and inhalational agents in com-bination with narcotics will cause vasodilation inpatients and reduce blood pressure. Vasodilationwith sodium nitroprusside can be titrated easily andterminated quickly. This makes it an ideal choicefor treatment of transient elevations in peripheralvascular resistance.
Post-CPB managementAfter mitral valve replacement for MS, a small meangradient of 2–5 mmHg usually exists across theprosthetic valve. Mechanical valves exhibit a smallamount of regurgitant flow in systole (Fig. 5.15a,b).Repaired mitral valves may exhibit some residualmild regurgitation and stenosis. TEE allows theanesthesiologist and surgeon an excellent oppor-tunity to evaluate the new valve structure andfunction. A full examination of the valve includ-ing color Doppler and pressure gradients is required.A dramatic improvement in LV filling via the LAafter replacement or repair is expected. As a result,preload reserve is greatly improved. This makes LVafterload mismatch less likely and allows augmen-tation of CO via increases in preload even whenpreoperative systolic dysfunction exists. A meanPCWP or LAP of 10–15 mmHg usually is adequateto take advantage of this increased preload reserve.
Patients in atrial fibrillation with large left atriararely convert to sinus rhythm postoperatively.Although the reduction in the transvalvular gra-dient allows greater hemodynamic tolerance withtachycardia, control of the ventricular response rateis important to allow adequate time in diastole to fillthe LV.
The management of RV function and the pul-monary vasculature can be problematic in thepost-bypass period. In all patients with elevated
(a)
(b)
Fig. 5.15 (a) Replacement of the mitral valve with aSt. Jude mechanical valve yields a characteristicregurgitant pattern. The regurgitant “flames” are normalbackwash from the valve closure (arrows). (b) In thispatient there is a significant perivalvular leak around theSt. Jude valve (arrow). Note the normal regurgitantbackwash next to the perivalvular leak.
pulmonary artery pressures, there will be a dra-matic reduction in pulmonary artery pressures dueto the reductions in the mean LAP and passive pul-monary congestion after valve replacement. Despitethis, some patients will continue to have elevatedPVR due to reversible (reactive pulmonary vasocon-striction) and nonreversible (morphologic changesin the pulmonary vasculature) causes. For thesepatients, careful management is necessary. LV SVdepends on proper RV function. In RV failure, thereis inadequate transit of blood to the left heart andCO falls. The hallmarks of this syndrome are a highright atrial pressure (RAP) (>10 mmHg) and PVR(over 150 dynes/s/cm5), coupled with a low LAP(<5 mmHg) and cardiac index (<2.2 L/min/m2).The clinician should aggressively strive to keep

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 155 — #27
Anesthesia for Valvular Heart Disease 155
PVR as low as possible by avoiding hypercar-bia, hypoxemia, and acidemia, and by avoidingpulmonary vasoconstrictors. If pulmonary hyper-tension persists despite these efforts, then activepulmonary vasodilation will be necessary. Nitro-glycerin has been shown to be effective in reducingpulmonary artery pressures and increasing pul-monary blood flow after mitral valve replacement.Nitroglycerin can be started at 0.15–0.30 µg/kg/minand titrated upward as needed. Sodium nitroprus-side started at the same dosage and titrated upwardalso is effective. Other effective pulmonary vasodila-tors include inhaled nitric oxide (NO) and prostacy-clin (PGI2). These agents are discussed in detail inChapter 7.
In some patients, inotropic support of theRV may be necessary in addition to pulmonaryvasodilation. Inotropic support without increasedPVR is ideal. Epinephrine 0.015–0.030 µg/kg/min,dopamine 1–5 µg/kg/min, or dobutamine5–10 µg/kg/min all meet this goal. Increased dosesof epinephrine and dopamine may result in pro-gressive pulmonary vasoconstriction from increasedα-adrenergic activity. In situations in which increas-ing demand for inotropic support is required, mil-rinone 0.5–0.75 µg/kg/min after a loading dose of50–75 µg/kg may be added. Milrinone, a phospho-diesterase III inhibitor, provides potent inotropicsupport and pulmonary vasodilation. Isoproterenol,a potent β1-agonist offers can improve inotropy andinduce pulmonary vasodilation; however, isopro-terenol is associated with an increase in heart rate,myocardial oxygen consumption, and the incidenceof ventricular dysrhythmias, all of which may limitits usefulness. The combination of prostaglandin E1
(PGE1) and norepinephrine is effective in treat-ing refractory pulmonary hypertension and RVfailure after mitral valve replacement. PGE1 is apotent pulmonary and systemic vasodilator. PGE1
30–150 ng/kg/min is infused into the right heartin combination with norepinephrine in doses upto 1–2 µg/kg/min infused via a left atrial line.The norepinephrine is infused via the left atrialline to minimize its vasoconstricting effects on thepulmonary vasculature, provide inotropic support,and counteract the profound systemic vasodilatoryeffects of PGE1. Management of RV dysfunction,
including TEE findings are discussed in detail inChapter 7.
A rare but potentially lethal complication ofmitral valve replacement is ventricular disruption.This complication has been described after mitralvalve replacement for a variety of lesions, but ismost common in patients undergoing replacementfor chronic MS. Three types of ventricular ruptureare described. Type 1 involves rupture of the mitralannulus or of the ventricle at the atrioventricularjunction due to a diseased annulus or posterior ven-tricular wall. Type 2 rupture occurs at the site of theexcised papillary muscle due to surgically-inducedthinning of the ventricular wall. Type 3 rupture ortransverse mid-ventricular disruption (TMD) occursmidway between type 1 and 2 ruptures. Type 3ruptures are secondary to a variety of causes. Endo-cardial injury from inadvertent surgical trauma orthe valve prosthesis may be involved. Total exci-sion of the mitral valve apparatus may result inloss of longitudinal support, which predisposes theventricle to transverse disruption when ventriculardilation occurs.
Goals• Maintain the ventricular response rate to atrialfibrillation below 100 b/min in absence of normalsinus rhythm.• Maintain LAP high enough to take advantage ofthe increased preload reserve.• Avoid pulmonary artery hypertension by treatinghypercarbia, hypoxemia, and acidemia.• Aggressively treat pulmonary artery hyperten-sion with vasodilator therapy to avoid RV failure.If RV failure does occur, inotropic support of the RVand pulmonary vasodilation may be necessary.• Maintain awareness of potential for LV rupture.
Mitral regurgitation (MR)Any abnormality of the mitral valve apparatus maycause MR. The most common cause in the west-ern countries is myxomatous mitral valve disease(Barlow syndrome). This condition is character-ized by a prolapse of one or more valve seg-ments into the LA. There is elongated or rupturedchordae, a thickened valve, and dilated annulus.Other causes include mechanical impairment due to

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 156 — #28
156 Chapter 5
Fig. 5.16 Severe ischemic mitral regurgitation in thecolor compare mode. Note the dilated left ventricle andthe central mitral regurgitation jet.
rheumatic fever, trauma, or infective endocardi-tis. Calcification of the valve annulus may resultin mechanical impairment of leaflet apposition.Functional impairment of leaflet apposition due toannular dilation may result from ventricular dila-tion caused by ischemia or a dilated cardiomyopathy(Fig. 5.16). Mechanical impairment may result fromrupture of the chordae tendinae. Infective endocardi-tis, rheumatic fever, trauma, or long-standing strainfrom mitral valve prolapse may result in chordaetendinae rupture.
Ischemia may cause ventricular wall motionabnormalities or papillary muscle dysfunction lead-ing to regurgitation. The posterior papillary musclesare more vulnerable to ischemia than the anteriorpapillary muscles. This occurs because the poste-rior papillary muscle is supplied with blood solelyfrom the posterior descending artery; whereas theanterior papillary muscle derives its blood supplyfrom branches of both the left anterior descendingand circumflex arteries. With continued ischemia,papillary muscle dysfunction may progress to necro-sis and rupture of the papillary muscle. Classically,rupture of one or more of the papillary mus-cle heads from necrosis occurs 2–7 days after aninferior myocardial infarction. This leads to acute,severe MR.
Pathophysiology and adaptation in MRMR is an LV volume overload lesion that can beeither acute or chronic. In essence, a double-outlet
left ventricle exists. There is a low-impedance out-flow tract into the low-pressure LA via the incom-petent mitral valve, and a high-impedance outflowtract into the high-pressure aorta via the aorticvalve. The extent of regurgitation depends on thesize of the mitral valve orifice, the time availablefor regurgitation (systole), and the pressure gradi-ent between the LA and LV. The area of the mitralvalve orifice is determined, in part, by the size ofthe LV. Dilation of the LV will result in distortionand enlargement of the valve orifice. Ventricularsystolic pressure, LA pressure, and LA complianceall contribute to the valve gradient.
Regurgitant flow ceases when the LV and LA pres-sures equalize. Equalization of pressure will occurmore rapidly when a small, noncompliant LA exists,because LA pressure will rise more rapidly than ina large compliant atrium. Equalization of pressurealso occurs more rapidly when the impedance to LVejection in the aorta is low. When aortic impedanceis low, there is a larger forward SV, and equalizationof pressure will occur quickly.
Chronic volume overloading of the left ventricleresults in eccentric ventricular hypertrophy similarto that seen in AR. The results of this process aresummarized in Fig. 5.17. As in AR, both LVESV andLVEDV increase, but LVEDV increases to a greaterextent. This results in an enhanced SV with noneed for an increased EF. The slope of the dias-tolic pressure–volume curve is little changed, andthus, compliance is only slightly increased. Theentire pressure–volume loop is shifted to the right.This rightward shift of the diastolic pressure–volumecurve allows low diastolic pressures at very largeend-diastolic volumes. The large increase in ventric-ular radius that accompanies eccentric hypertrophyelevates wall stress and stimulates some degree ofconcentric hypertrophy. Unlike AR, this compen-sation is complete and wall stress is normalized inboth end systole and end diastole (Fig. 5.17a).
Unique LV pressure loading exists in chronic MR,as illustrated in Fig. 5.17a. The isovolumic phaseof ventricular systole is of very short duration andlimited pressure generation. In fact, because theimpedance to ejection into the LA is so low, theisovolumic phase is shorter and lower in pressurethan that seen in AR. This allows a greater portion

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 157 — #29
Anesthesia for Valvular Heart Disease 157
Wal
l str
ess
Wal
l str
ess
Norm
al
Norm
al
Depre
ssed
Ecce
ntric
hyp
ertro
phy
Ecce
ntric
hyp
ertro
phy
EFx 60%
Volume Volume
EFx 65%
Post-op.EFx 37%
EFx 50%
(a) (b)
Fig. 5.17 Left ventricular wall stress–volume loops fora patient with progressive mitral regurgitation (MR).(a) Wall stress–volume loops of normal ventricle and ofventricle having developed eccentric hypertrophy inresponse to chronic volume overload of MR. Theventricle with eccentric hypertrophy has reducedisovolumic contraction phase and has its entire wallstress–volume relationship shifted to the right. Theisovolumic contraction phase is even shorter than seen inaortic regurgitation (see Fig. 5.10). In addition,end-systolic wall stress is normalized. These adaptationsallow the ventricle to deliver large stroke volume (SV)with high normal ejection fraction (EF). (b) Wallstress–volume relationships in ventricle with chronicmitral regurgitation and systolic dysfunction.
Low-impedance outflow tract to the left atriumprovided by an incompetent mitral valve allows wallstress to remain low during early and late ventricularsystole. Thus, despite the presence of systolicdysfunction, EF is maintained near normal (EF = 50%).After surgical replacement of mitral valve, thelow-impedance outflow tract to the left atrium isabolished. This results in an elevation of wall stressduring early and late systole. Under these loadingconditions, afterload mismatch occurs and ventricularsystolic dysfunction manifests as reduced EF (EF = 37%).Post-op., postoperative. (From Ross J Jr. Left ventricularfunction and the timing of surgical treatment in valvularheart disease. Ann Intern Med 1981;94:498–504, withpermission.)
of myocardial energy expenditure directed towardejecting a large volume and less toward overcomingimpedance to begin ejection.
In chronic MR, the sustained high LAP results inleft atrial hypertrophy and eventually left atrial dis-tension. This distension results in the developmentof atrial dysrhythmias, the most common of whichis atrial fibrillation. In severe MR, atrial fibrillationrather than sinus rhythm generally is the rule.
In acute MR, there is not ample time for ven-tricular eccentric hypertrophy to occur. As a result,the ventricle does not have the enormous preloadreserve available in chronic MR. Of greater impor-tance, is the status of the LA. In acute MR, a small,noncompliant LA exists. Regurgitation of volumeinto a small LA results in high LA pressures, whichmanifests as a regurgitant V wave. The height of theV wave does not quantify the regurgitant volumebut rather is an indicator of the relationship between
regurgitant volume and LA compliance. Nonethe-less, this elevation of LA pressure results in acutepulmonary congestion.
In chronic MR, as in AR, a large total SV is neces-sary to maintain forward SV when the regurgitantvolume is large. An atrial kick is helpful in augment-ing LVEDV; however, the increased compliance andrightward shift of the diastolic pressure–volumecurve allows passive filling of the LV in early andmid-diastole when atrial fibrillation exists.
In acute MR, increased ventricular complianceand a rightward shift of the diastolic pressure–volume curve are absent. In this setting, an atrialsystole may be necessary to increase the left atrialto LV pressure gradient enough to complete fillingof the left ventricle via the LA.
In chronic MR, eccentric hypertrophy and aright shift in the pressure–volume curve allowlarge increases in LVEDV with minimal increases

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 158 — #30
158 Chapter 5
in LVEDP. This affords a great deal of preloadreserve. Unfortunately, the ventricular dilation thataccompanies increases in LVEDV results in enlarge-ment of the mitral annulus and an increase in theregurgitant fraction.
In contrast, in acute MR preload reserve is nearlyexhausted. Without adequate time for adaptation,the left ventricle operates on the steep portion ofits diastolic pressure–volume curve. Again, preloadaugmentation may result in ventricular dilation anda worsening of the regurgitation.
Myocardial oxygen consumption is altered in MR.There is an increase in oxygen consumption due tothe large mass of myocardium that must be suppliedwith oxygen and the enormous volume work doneby the left ventricle. Volume work increases oxy-gen consumption, but to a much lesser extent thanpressure work. The isovolumic contraction phaseis highly energy-consumptive. Because of the lowimpedance to ejection into the LA, the isovolumiccontraction phase is very brief and represents onlya small portion of the total work done by the ven-tricle (see Fig. 5.17a). A greater portion of the totalworkload is devoted to the generation of volumeejection, which is an energy efficient process.
In addition to the increased myocardial oxygendemands, oxygen supply is compromised whenthere are coexistent coronary artery stenoses. Thisis particularly important for patients with acute MRfrom papillary muscle rupture or dysfunction. For-tunately, unlike AR, aortic diastolic blood pressureis normal, which helps maintain the gradient forcoronary blood flow. Further impairment of sup-ply occurs because of the high LV end-diastolicpressures that accompany acute MR. In acute MR,eccentric hypertrophy has not had time to occur,and large LVEDV is accompanied by large LVEDP.
Patients with chronic MR may remain symptom-free for years despite progressive decreases insystolic function. The enormous preload reserveavailable to these patients allows maintenance ofSV by progressive increases in LVEDV in the faceof declining contractile function and increasingLVESV. When preload reserve is exhausted, fur-ther diminution in systolic function goes uncom-pensated and SV falls. At this point, symptoms ofreduced CO and CHF appear (Fig. 5.17b). There is
usually significant systolic impairment in patientswith acute MR secondary to ischemia.
EF will greatly overestimate systolic function inMR because a portion of the SV is ejected backwardsas mitral regurgitant volume. Recall that EF deter-minations are very afterload-dependent. In MR, theimpedance to ejection via the incompetent mitralvalve is low. Therefore, EF may remain in thenormal range despite severe systolic dysfunction.This severe dysfunction may only become appar-ent after mitral valve repair or replacement whenthe low-impedance outflow tract is eliminated (seeFig. 5.17b).
The large, compliant LA that develops in chronicMR tends to shield the pulmonary circulation fromelevated LA pressures. With time, however, pul-monary artery hypertension will develop from pas-sive pulmonary venous distension. If LA pressuresremain elevated over a long period, reactive changesoccur in the pulmonary vasculature. Prolongedperivascular edema results in arterial intimal fibroe-lastosis and nonreversible elevations in pulmonaryartery pressures and PVR. RV dysfunction fromafterload mismatch may develop, as occurs in MS(see Fig. 5.13). In the most severe instances, tricus-pid regurgitation from RV distension will complicatethe picture. Pulmonary vasodilators may reduce RVafterload and improve RV output in patients withelevated PVR.
In acute MR the small, noncompliant LA ispoorly adapted to shield the pulmonary vascula-ture from the regurgitant volume. Regurgitation ofvolume into the noncompliant LA results in pro-found and immediate elevation of LAP with a verylarge V wave. Pulmonary vascular congestion withinterstitial pulmonary edema rather than secondarypulmonary artery hypertension is the issue here.RV systolic dysfunction may exist because reduc-tions in posterior descending coronary artery per-fusion severe enough to produce posterior papillarymuscle dysfunction or infarction also may produceRV ischemia or infarction.
Bradycardia (heart rate < 60 b/min) is detri-mental in MR because it prolongs systole, whichincreases the time available for regurgitation.In addition, bradycardia prolongs diastole allow-ing a large LVEDV to develop. This may result

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 159 — #31
Anesthesia for Valvular Heart Disease 159
in LV distension, particularly in acute MR, inwhich eccentric hypertrophy and pressure–volumecompensation are absent. LV distension leads toenlargement of the mitral annulus and worseningregurgitation. Finally, when the regurgitant fractionis large (50–60%), total SV will be large but forwardSV low. Elevating the heart rate enhances forwardflow in this situation.
Efforts to increase heart rate into the opti-mal range of 80–100 b/min are balanced withthe increased oxygen demand and decreased oxy-gen supply with tachycardia. This is particularlyimportant for patients who have MR secondaryto papillary muscle rupture or dysfunction fromischemia.
Most patients with moderate and severe MR arein atrial fibrillation. In these patients, control ofheart rate is dependent on adequate control of theventricular response rate to the fibrillating atrium.Drugs used to control the ventricular response rateat the AV node, such as digoxin, diltiazem, andbeta-blockers, must be continued.
Increased afterload is poorly tolerated by patientswith acute and chronic MR because it increasesthe regurgitant fraction. Increased afterload tends toincrease the size of the LV by increasing LVESV, fol-lowed by a compensatory increase in LVEDV. ThisLV dilation increases the size of the mitral orifice.Increased afterload also increases the impedance toaortic ejection. This favors ejection into the LA viathe lower impedance outflow tract.
Unlike AR, in which afterload reduction must beused selectively, afterload reduction is uniformlyadvantageous in both acute and chronic MR. After-load reduction improves forward CO by promotingejection via the aorta and reducing the regurgi-tant fraction. This is because the incompetent mitralvalve provides such low impedance to ejection thatany decrease in the impedance to ejection via theaortic valve will augment forward flow.
Anesthetic technique in MR
Goals• Maintain sinus rhythm when possible.• Maintain heart rate at 80–100 b/min; faster betterthan slower.
• Maintain end-diastolic PCWP high enough toguarantee a large LVEDV without ventriculardistension and increased valve area.• Decrease LV afterload; increases are poorlytolerated. Decreasing afterload will improve COby decreasing regurgitation but preload must bemaintained.• Maintain contractility; there may be significantLV dysfunction.• When PVR is high or when RV systolic dys-function exists RV afterload reduction will improveRV and subsequently LV output. The concur-rent systemic vasodilation also will directly reduceregurgitation.• Avoid hypercarbia, hypoxemia, and acidemiawhich tend to cause pulmonary hypertension andmay result in acute RV decompensation.
PremedicationFor patients with acute MR, severe hemodynamiccompromise usually is the rule. It is dangerous tosedate these patients before surgery. All sedativesand narcotics should be given with careful obser-vation of the fully monitored patient. In chronicMR, the usual cautions are appropriate whenconsidering premedication.
PreinductionThe V wave and the mean PCWP are not good esti-mates of LVEDP in patients with MR. Recall thatthe V wave occurs during early ventricular systoleand quantifies the relationship between the regur-gitant volume and left atrial compliance. The meanPCWP is skewed upward by a large V wave and will,therefore, overestimate the LVEDP by an amountproportional to the amplitude and duration of theV wave. The best estimate of LVEDP is the end-diastolic PCWP. In patients in sinus rhythm, this willbe the A-wave pressure. In patients in atrial fibrilla-tion, it will be the PCWP just before the onset of theV wave. The cardiac catheterization report will pro-vide information regarding the optimal LVEDP in agiven patient. The pulmonary artery catheter allowsPVR to be calculated as well as measurement of theCVP. Therapy to reduce RV afterload and improveRV systolic performance cannot be initiated safelywithout this information.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 160 — #32
160 Chapter 5
In chronic MR, because of the increased ventric-ular compliance and the right shift in the pressure–volume relationship, LVEDV will be supplementedwith only small increases in the mean PCWP. Inpatients with preserved LV function, a mean PCWPin the range of 10–15 mmHg will usually ensureoptimal LVEDV. In patients with depressed ventric-ular function and exhausted preload reserve, PCWPwill be in the range of 20–25 mmHg are sometimesrequired for optimal loading conditions.
In acute MR, there will be large V waves andLVEDP will be elevated because of the lack of com-pensatory atrial and ventricular enlargement. Itmay be necessary to have an end-diastolic PCWPof 20–25 mmHg to ensure an adequate LVEDV inpatients with acute MR.
For patients in whom afterload reduction isrequired before induction, sodium nitroprusside isthe agent of choice. It is easily titratable with avery short half-life. The infusion can be startedat 0.15–0.30 µg/kg/min and titrated with care-ful attention paid to CO, arterial blood pressure,and PCWP. Nitroprusside is primarily an arterialvasodilator; however, it has vasodilatory effects onthe venous system as well. It is important not to letreductions in preload offset the beneficial effects ofarterial dilation. If necessary, volume infusion canmaintain PCWP in the optimal range.
For patients with severe RV failure, pulmonarycongestion, and systemic hypotension (systolicblood pressure < 90 mmHg), efforts to improve RVfunction and reduce regurgitation with vasodila-tor therapy may be unsuccessful due to worsen-ing systemic hypotension. For these patients, theaddition of inotropic support of the RV and LV isnecessary. Dobutamine 5–10 µg/kg/min is a goodchoice because it has no α-adrenergic activity, littlechronotropic activity and it tends to reduce pul-monary artery pressures. Therefore, it will not exac-erbate pulmonary artery hypertension or increaseLV afterload and regurgitation.
In patients with myocardial ischemia, efforts mustbe directed toward lowering LVEDP, decreasingventricular radius, improving aortic diastolic bloodpressure, and decreasing heart rate as much as ispossible without worsening the regurgitant pro-cess. IV nitroglycerin is a mainstay of therapy.
Dobutamine 5–10 µg/kg/min is a good choice if aninotropic agent is necessary. It reduces LV radiusand end-diastolic pressure while increasing aorticblood pressure and causing little change in heartrate. In patients with MR, the resultant reductionin wall stress and the valve orifice area will serveto decrease both myocardial oxygen consumptionand the regurgitant volume. When pharmacologicinterventions fail, the use of the intra-aortic balloonpump (IABP) may be indicated.
Induction and maintenancePatients with chronic, stable MR usually tolerateinduction without significant hemodynamic com-promise. Etomidate, pentothal, ketamine, or propo-fol are all appropriate agents. Hypotension maybe treated with vasopressors; however, caution isurged because in some patients, increasing after-load will increase the regurgitant volume whichworsens the situation. In all patients heart rateand preload must be optimal. If inotropic supportis required, dobutamine 5–10 µg/kg/min can aug-ment CO without increasing afterload or worseningpulmonary artery hypertension.
Many patients with acute MR from myocardialischemia or infarction will be in cardiogenic shockwith possible respiratory distress from pulmonaryvascular congestion. These patients may arrive fromthe cardiac catheterization laboratory or ICU intu-bated, on inotropes, and supported with an IABP.Narcotics, small dose benzodiazepines, and musclerelaxants are appropriate in this group of patients.In nonintubated patients with acute MR, the induc-tion sequence should be modified to account forthe hemodynamic condition and the higher risk ofaspiration. After preoxygenation and with cricoidpressure applied, etomidate 0.15–0.30 mg/kg, suc-cinylcholine 1.0–1.5 mg/kg, in conjunction withfentanyl 10 µg/kg or sufentanil 1 µg/kg can beadministered. Alternatively, sufentanil 5 µg/kg andsuccinylcholine 1.0–1.5 mg/kg can be used.
Post-CPB managementRepaired mitral valves may exhibit some residualmild regurgitation and stenosis. TEE is essential inevaluating valvular repairs.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 161 — #33
Anesthesia for Valvular Heart Disease 161
After mitral valve replacement or repair forchronic MR, the ventricle is now faced with arelative pressure overload. The competent mitralvalve eliminates the low-impedance outflow intothe LA. Ejection of the SV is now directed outthe high-impedance outflow tract into the aorta.This causes a substantial elevation of ventricularpressure during the isovolumic contraction phase.The elimination of regurgitation by the competentvalve greatly reduces the need for a large total SV.Therefore, a greater proportion of total myocardialoxygen consumption goes toward the more energy-consumptive process of pressure generation to beginejection and less toward volume ejection. There isan elevation of early and late systolic wall stress.This occurs despite the dramatic reduction in ven-tricular radius that accompanies elimination of theregurgitant volume (see Fig. 5.17b). This results in astate of afterload mismatch such that postoperativesystolic function is compromised. The temptationwhen CO is low will be to use the large preloadreserve available in these patients. Because ven-tricular pressure is already elevated, during theprolonged isovolumic contraction phase wall stressfor a given LVEDV will be greater in the post-bypassperiod. Efforts to increase preload to contend withpoor systolic function or high afterload states willonly worsen afterload mismatch. A mean PCWP orLAP of 10–15 mmHg usually is adequate.
For these reasons, particularly if poor myocar-dial protection is obtained during bypass and aor-tic cross-clamping or if depressed systolic functionexists preoperatively, management of these patientspost-CPB is challenging. The mainstays of therapyare afterload reduction and inotropic support of sys-tolic function. The goal of vasodilator therapy is toreduce afterload.
An inotrope is indicated when systolic bloodpressure is low (<90 mmHg) and the cardiacindex is low (<2.0 L/min/m2). Epinephrine0.015–0.030 µg/kg/min is a good choice becauseit is a potent inotrope with little vasoconstrictoractivity at this dose. When afterload reduction isneeded, as determined by a high SVR or meanaortic pressure, nitroprusside can be added. It iseasily titratable with a short half-life. The infusioncan be started at 0.15–0.3 µg/kg/min and titrated
with careful attention paid to cardiac index, arte-rial blood pressure, and PCWP. Volume infusionmay be necessary to keep PCWP in the optimalrange. If the PCWP remains elevated (>18 mmHg)with inotrope infusion, then nitroglycerin startedat 0.15–0.30 µg/kg/min and titrated upward is thevasodilator of choice. Alternatively, a phosphodi-esterase inhibitor can be used. Milrinone providesboth inotropy and vasodilation.
The management of RV function and the pul-monary vasculature can be problematic in thepost-bypass period. Management of this problem isdescribed in detail in the section on MS.
Patients in atrial fibrillation with large left atriawill rarely convert to sinus rhythm postoperatively.Therefore, the ventricular response rate will have tobe controlled. Bradycardia is better tolerated afterreplacement of the incompetent mitral valve thanbefore replacement.
Goals• Maintain the ventricular response rate to atrialfibrillation <100 b/min if sinus rhythm cannot bemaintained.• Avoid reliance on a large LVEDV; wall stresswill be greatly elevated and systolic function maydecline.• Aggressively use inotropic support and afterloadreduction of the LV.• Avoid pulmonary artery hypertension by treatinghypercarbia, hypoxemia, and acidemia.• Aggressively treat pulmonary artery hyperten-sion with vasodilator therapy to avoid RV failure.If RV failure does occur, inotropic support of the RVand pulmonary vasodilation may be necessary.
The tricuspid valve
The tricuspid valve (TV) consists of anterior, pos-terior, and septal cusps tethered by chordae ten-dinae and papillary muscles all suspended by afibromuscular annulus. The commissures of theTV are not as well defined as those of the mitralvalve. The orifice is larger than that of the mitralvalve and is triangular in shape, as compared tothe saddle-shape of the mitral valve. The ante-rior leaflet is the largest and is tethered to the

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 162 — #34
162 Chapter 5
Table 5.4 The primary and secondary causes oftricuspid insufficiency.
Primary Secondary
Infective endocarditis Myocardial ischemia/Carcinoid tumor infarctionRheumatic heart disease Cor pulmonaleTrauma Pulmonary embolismPapillary muscle dysfunction Left heart failureFen-Phen valvulopathy Pulmonic stenosisEbstein anomaly Pulmonary hypertensionConnective tissue disorders Mitral insufficiency
Pulmonary arterycatheter/pacemaker
anterior papillary muscle which arises from themoderator band. The moderator band is composedof muscular tissue arising from the intraventric-ular septum and can sometimes be seen on theechocardiogram. The posterior leaflet is the smallestand is anchored by the posterior papillary muscle.The septal leaflet attaches to the ventricular sep-tum and is in very close proximity to the bundleof His.
Tricuspid valvular disease is almost always regur-gitant in nature. The defect may be either functionalor anatomic. The result is RV dilation, elevationof RV systolic and diastolic pressures, and tricuspidannular dilatation. Left-sided valvular lesions withpulmonary hypertension, RV infarction, pacemakermalfunction, or RV failure from any cause can resultin tricuspid regurgitation (TR). Other causes of tri-cuspid abnormalities include rheumatic valvulitis,endocarditis, carcinoid, radiation therapy, trauma,or congenital lesions. Ebstein’s anomaly is seenwhen the TV is displaced toward the apex in the RV(Table 5.4). Tricuspid stenosis (TS) is less commonand most likely secondary to rheumatic heart dis-ease. Other causes of TS include congenital abnor-malities or endocarditis. Right atrial masses may actas functional stenotic lesions and impede TV inflow.
There is a giant a wave on the CVP waveformin TS, and abnormal c and v waves with TR. TEEis most helpful in the diagnosis of TS and TR(Fig. 5.18). It is common for TR to present in con-junction with other valvular heart lesions (i.e. MS
Fig. 5.18 A mid-esophageal four-chamber viewtransesophageal echocardiographic image demonstratingsevere tricuspid regurgitation. Note the large right atriumand the bulging intra-atrial septum indicating high rightatrial pressures (arrow).
or MR). If there is RV failure, the medical prog-nosis is worse. The anesthetic management shouldconsider the degree of RV failure. Most frequently,the surgical intervention for TR is a repair with aring annuloplasty.
The pulmonary valve
The pulmonary valve (PV) is anterior and supe-rior to the aortic valve. Similar to the aortic valve,it is trileaflet and semilunar, consisting of ante-rior, left and right leaflets. The plane of the valveis roughly perpendicular in orientation to the aor-tic valve. The pulmonic valve is isolated from theother three heart valves by the infundibulum. Pul-monary valvular disease is usually congenital innature. Stenosis is more common than regurgi-tation although a wide spectrum of pathology ispossible (Fig. 5.19). Congenital pulmonary steno-sis is usually treated with balloon valvuloplasty.Mild pulmonary regurgitation occurs in nearly allcardiac surgical patients in whom a pulmonaryartery catheter has been placed. Significant pul-monary regurgitation is rare, and is usually welltolerated. In some patients, RV dysfunction mayoccur secondary to pulmonary regurgitation andshould be surgically corrected. Pulmonary allograftsare usually chosen when replacing a pulmonary

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 163 — #35
Anesthesia for Valvular Heart Disease 163
Fig. 5.19 Transesophageal echocardiography (TEE)color compare image of severe pulmonary arteryaneurysm with pulmonary hypertension and mildpulmonary insufficiency. On the left image the aneurysmis indicated by the arrow. In the right image, thepulmonary insufficiency is seen with color Doppler.LA, left atrium; PA, pulmonary artery; PR, pulmonaryregurgitation; RA, right atrium; RV, rightventricle.
valve; pulmonary valvular repair is typically notperformed.
Multiple valve lesions
It is not uncommon for patients with valvular heartdisease to have both a stenotic and regurgitant pro-cess affecting one valve or to have involvement oftwo or more valves. There are several importantpoints to keep in mind when evaluating patientswith multiple valve lesions.
It is possible for a valve to be stenotic and incom-petent; however, a severely stenotic valve can allowonly minimal regurgitation because of the profoundreduction in valve area. Likewise, a severely incom-petent valve can offer only minimal impedanceto flow across its large area. It is possible for aprosthetic valve to possess high-grade stenosis andregurgitation if it has a large perivalvular leak.
When a valve is not clearly primarily stenoticor incompetent, it is necessary to determine whichlesion has the most pronounced effect on thepatient’s hemodynamics. If a patient with MS andMR has a large LVEDV, it follows that MR is thepredominant lesion. Likewise, if a patient with ASand AR is found to have a normal LVEDV with left
atrial enlargement and a large A-wave pressure, itfollows that AS is the predominant lesion.
When two valves are involved, it is necessary toknow which features of each lesion exacerbate orameliorate the effects of the other lesions.
AR and MSThe under-loading of the LV characteristic of MSwill be offset by the regurgitation of the aortic valvelesion. Increased LAP and pulmonary artery hyper-tension characteristic of MS will be present. Theincreased heart rate so beneficial in AR will causeprecipitous increases in LAP with subsequent pul-monary congestion. Therapy for both RV and LVafterload reduction will be necessary.
AS and MSThe LV under-loading characteristic of MS willseverely limit the preload reserve of the LV becauseLV compliance in AS will be diminished, LAP willhave to be greatly elevated to ensure adequate fill-ing of the LV with the gradient across the mitralvalve. This will exacerbate pulmonary congestion.LV afterload reduction will be poorly toleratedbecause of the large gradient across the aortic valveand the limited ability to increase LVEDV. Efforts toreduce RV afterload will be severely limited by theconcomitant systemic vasodilation.
AR and MRThe pathophysiology of LV volume overload willbe predominant. Efforts to reduce LV afterload willbe of benefit in the management of both lesions.Likewise, a relatively fast heart rate will be advan-tageous. High LAP and pulmonary artery hyperten-sion not normally seen in AR may be a feature here.If the MR is secondary to ventricular dilation fromAR, then only replacement of the aortic valve willbe necessary.
AS and MRHigh ventricular pressure in AS will cause dramaticMR if the mitral valve is incompetent. The com-bination of concentric and eccentric hypertrophywill allow the LV to maintain a relatively largeSV. With a larger than normal preload reserveavailable, some LV afterload reduction might be

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 164 — #36
164 Chapter 5
tolerated in an effort to reduce regurgitation ifthe AS is mild. Efforts to increase heart rate toreduce the regurgitant process will have detrimen-tal effects on the subendocardial perfusion of thehypertrophied LV. Pulmonary congestion and pul-monary artery hypertension with RV failure arelikely. Reduction of pulmonary arterial pressure willbe difficult for patients with severe AS, becausethe concomitant systemic vasodilation may resultin profound systemic hypotension. In instances inwhich MR is mild to moderate and AS is severe,replacement of the aortic valve may reduce ventric-ular pressures and ventricular dilatation such thatmitral valve replacement or repair is unnecessary.
Pulmonary autograft for aortic valvereplacementIn some patients with aortic valve disease, mov-ing the pulmonary valve to the aortic position andimplantation of a pulmonary homograft is benefi-cial (Ross procedure). In children, the pulmonaryautograft will increase in size as the child growsand there is no need for anticoagulation. Hemo-dynamics seen across the new aortic valve areexcellent and the development of new AR is low.The freedom from autograft replacement is approx-imately 50–75% at 20 years. This procedure is tech-nically more complicated and requires an extendedCPB time.
Table 5.5 Indications for aortic valve replacement. (Reprinted with permission from Bonow RO, Carabello BA,Chatterjee K et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of theAmerican College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee toDevelop Guidelines for the Management of Patients with Valvular Heart Disease). J Am Coll Cardiol 2006;48:e1–148.)
Class I1 AVR is indicated for symptomatic patients with severe AS (Level of evidence: B)2 AVR is indicated for patients with severe AS undergoing coronary artery bypass graft surgery (CABG) (Level ofevidence: C)3 AVR is indicated for patients with severe AS undergoing surgery on the aorta or other heart valves (Level of evidence: C)4 AVR is recommended for patients with severe AS and LV systolic dysfunction (ejection fraction <0.50) (Level ofevidence: C)
Class IIaAVR is reasonable for patients with moderate AS undergoing CABG or surgery on the aorta or other heart valves (seeSections on Combined multiple valve disease and on AVR in patients undergoing CABG) (Level of evidence: B)
Class IIb1 AVR may be considered for asymptomatic patients with severe AS and abnormal response to exercise (e.g. developmentof symptoms or asymptomatic hypotension) (Level of evidence: C)2 AVR may be considered for adults with severe asymptomatic AS if there is a high likelihood of rapid progression (age,calcification, and CAD) or if surgery might be delayed at the time of symptom onset (Level of evidence: C)3 AVR may be considered in patients undergoing CABG who have mild AS when there is evidence, such as moderate tosevere valve calcification, that progression may be rapid (Level of evidence: C)4 AVR may be considered for asymptomatic patients with extremely severe AS (aortic valve area less than 0.6 cm2, meangradient >60mmHg, and jet velocity >5.0m/s) when the patient’s expected operative mortality is 1.0% or less (Level ofevidence: C)
Class IIIAVR is not useful for the prevention of sudden death in asymptomatic patients with AS who have none of the findingslisted under the class IIa/IIb recommendations (Level of evidence: B)
AS, aortic stenosis; AVR, aortic valve replacement; CABG, coronary artery bypass graft; CAD, coronary artery disease; LV, leftventricle.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 165 — #37
Anesthesia for Valvular Heart Disease 165
Previously undiagnosed valvedisease found during CABG
Occasionally, patients presenting for CABG arefound to have significant AS during the TEE exam-ination. The new lesion should be fully evaluatedby TEE and the indications for replacement are thesame as in any other patient (Table 5.5). If theAS is moderate to severe, the aortic valve shouldbe replaced. Controversy exists when mild AS isuncovered.
MR is also a common unexpected finding inpatients having CABG surgery. The MR requires fullevaluation by TEE. If there is a structural defectsuch as valve prolapse or flail, the valve shouldbe repaired or replaced. Ischemic MR is due to LVremodeling and apical tenting of the chordae. TheMR jet us usually central in nature as compared tothe more eccentric MR jets seen with either restric-tive disease or valve prolapse. Severe ischemic MRshould be surgically corrected. Controversy existsabout mild to moderate ischemic MR. Ischemic MR
Table 5.6 Indications for mitral valve surgery. (Reprinted with permission from Bonow RO, Carabello BA,Chatterjee K et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report ofthe American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committeeto Develop Guidelines for the Management of Patients with Valvular Heart Disease). J Am Coll Cardiol 2006;48:e1–148.)
Class I1 MV surgery is recommended for the symptomatic patient with acute severe MR (Level of evidence: B)2 MV surgery is beneficial for patients with chronic severe MR and NYHA functional class II, III, or IV symptoms in theabsence of severe LV dysfunction (severe LV dysfunction is defined as ejection fraction <0.30) and/or end-systolicdimension >55mm (Level of evidence: B)3 MV surgery is beneficial for asymptomatic patients with chronic severe MR and mild to moderate LV dysfunction,ejection fraction 0.30–0.60, and/or end-systolic dimension ≥40mm (Level of evidence: B)4 MV repair is recommended over MV replacement in the majority of patients with severe chronic MR who requiresurgery, and patients should be referred to surgical centers experienced in MV repair (Level of evidence: C)
Class IIa1 MV repair is reasonable in experienced surgical centers for asymptomatic patients with chronic severe MR withpreserved LV function (ejection fraction >0.60 and end-systolic dimension <40mm) in whom the likelihood of successfulrepair without residual MR is >90% (Level of evidence: B)2 MV surgery is reasonable for asymptomatic patients with chronic severe MR, preserved LV function, and new onset ofatrial fibrillation (Level of evidence: C)3 MV surgery is reasonable for asymptomatic patients with chronic severe MR, preserved LV function, and pulmonaryhypertension (pulmonary artery systolic pressure >50mmHg at rest or >60mmHg with exercise) (Level of evidence: C)4 MV surgery is reasonable for patients with chronic severe MR due to a primary abnormality of the mitral apparatus andNYHA functional class III–IV symptoms and severe LV dysfunction (ejection fraction <0.30 and/or end-systolic dimension>55mm) in whom MV repair is highly likely (Level of evidence: C)
Class IIbMV repair may be considered for patients with chronic severe secondary MR due to severe LV dysfunction (ejectionfraction <0.30) who have persistent NYHA functional class III–IV symptoms despite optimal therapy for heart failure,including biventricular pacing (Level of evidence: C)
Class III1 MV surgery is not indicated for asymptomatic patients with MR and preserved LV function (ejection fraction >0.60 andend-systolic dimension <40mm) in whom significant doubt about the feasibility of repair exists (Level of evidence: C)2 Isolated MV surgery is not indicated for patients with mild or moderate MR (Level of evidence: C)
LV, left ventricular; MR, mitral regurgitation; MV, mitral valve; NYHA, New York Heart Association.

Alice Nelson Dinardo: “ch05” — 2007/7/16 — 12:39 — page 166 — #38
166 Chapter 5
(a) (b)
Fig. 5.20 (a) Schematic of the endovascular repairsystem guide catheter across the atrial septum. The clipdelivery system is positioned through the guide. The clipis in the open position in the left ventricle, ready to beretracted to grasp the mitral leaflets. (b) The distal end ofthe delivery system and the polyester-covered clip shownin the open position. (From St. Goar FG, Fann JL,Komtebedde J et al. Endovascular edge-to-edge mitralvalve repair: short term results in a porcine model.Circulation 2003;108:1990–3, with permission.)
is dynamic and is responsive to pharmacologic alter-ations in loading conditions and LV remodeling. Theindications for mitral valve repair or replacementare given in Table 5.6.
Alternatives to surgical repair
For some patients, alternatives to surgical repairexist. Techniques are now available for percuta-neous replacement of the pulmonary and aor-tic valve. There is active work on percutaneousendovascular end-to-edge repair of the mitralvalve (Fig. 5.20a,b). The coronary sinus wrapsaround the mitral valve and allows an opportu-nity for positioning of an annular constraint device,which may reduce mitral annular size and MR(Fig. 5.21). Finally, there is some enthusiasm for
Coronary sinus Mitral annularconstraint device
Mitral valve
Fig. 5.21 The position of the mitral annular constraintdevice in the coronary sinus and its relation to theposterior aspect of the mitral valve. Elements of thedevice, including proximal and distal anchors and anintervening cable, are depicted. (From Kaye DM,Byrne M, Alferness C, Power J. Feasibility and short-termefficacy of percutaneous mitral annular reduction for thetherapy of heart failure-induced mitral regurgitation.Circulation 2003;108:1795–7, with permission.)
a surgical edge-to-edge annuloplasty of the mitralvalve (Alfieri stitch); although late outcome datasuggest that long-term benefit is lacking. In anycase, the techniques and indications for percuta-neous repair and replacement of valvular heartdisease will likely only increase in the next years.
Suggested reading
Bonow RO, Carabello BA, Chatterjee K et al. ACC/AHA
2006 guidelines for the management of patients with
valvular heart disease. J Am Coll Cardiol 2006;48:
1–148.
Carabello BA. Is it ever too late to operate on the
patient with valvular heart disease? J Am Coll Cardiol
2004;44:376–83.
Rahimtoola SH. Choice of prosthetic heart valve for adult
patients. J Am Coll Cardiol 2003;41:893–904.
Rahimtoola SH. The year in valvular heart disease. J Am
Coll Cardiol 2005;45:111–22.
Vahanian A, Acar C. Percutaneous valve procedures: what
is the future? Curr Opin Cardiol 2005;20:100–6.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 167 — #1
CHAPTER 6
Congenital Heart Disease
The incidence of congenital heart is approximately7–10 per 1000 live births. Environmental factorssuch as drugs, viral infection, maternal diabetes,or maternal alcohol abuse may account for spe-cific lesions. Most congenital heart defects are theresult of an interaction of genetic predisposition andenvironmental factors.The anesthesiologist who cares for patients with
congenital heart disease (CHD) faces myriad chal-lenges in the perioperative management of thesecomplex individuals. In major pediatric cardiac cen-ters, almost every lesion is amenable to surgicalintervention. The pathophysiology of a wide varietyof congenital heart defects can be best understoodby applying certain basic principles to each patient.This chapter outlines those principles. The anesthe-siologist who understands the dynamics of theselesions and the planned surgical interventionwill beable to conduct an appropriate anesthetic. Althoughyounger, smaller, and sicker patients are presentingfor more complex, innovative surgical treatment, itis encouraging and impressive that there has beena concomitant decrease in surgical and anestheticmorbidity and mortality.
Pediatric cardiovascularphysiology
Dramatic circulatory changes occur within minutesof birth, there and continue over the first few daysand weeks of life. These changes have profoundeffects on neonatal cardiovascular physiology. It is
not coincidental that 50% of the neonates bornwith CHD will become ill enough during the firstdays or weeks of life to require medical or surgi-cal intervention. Optimal anesthetic managementof the neonate with CHD must be based on a firmunderstanding of these developmental changes.
Fetal circulationThe placenta provides gas exchange in the fetus.Changes at birth are directly related to the exclu-sion of the placenta and the establishment of thelungs as the unit of gas exchange. Fetal circulatorychannels shunt blood away from the lung, result-ing in a parallel circuit in which both ventriclessupply systemic circulation. This parallel circulationpermits normal fetal growth and development evenin fetuses with cardiac malformations. Fetal shuntspermit alternate pathways and provide adequatesystemic blood flow.Oxygenated blood from the placenta returns to
the fetus via the umbilical vein, which enter theportal venous system (Fig. 6.1). The ductus veno-sus connects the left portal vein to the left hepaticvein at its junction with the inferior vena cava(IVC). This allows approximately 50% of umbili-cal venous blood to bypass the hepatic sinuses. Theremainder of umbilical venous flow passes throughthe liver and enters the IVC via the hepatic veins.Fetal IVC blood is a combination of blood from thelower fetal body, umbilical vein, and hepatic veins.The stream of blood from the ductus venosus hasa higher velocity in the IVC than the stream from
167

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 168 — #2
168 Chapter 6
Upper bodyand brain
DA
Ao PA
LungsRV LV
LA
RA
Liver
DV
Placenta
Lower body
Gastrointestinal
Fig. 6.1 Schematic of the fetal circulation. Ao, aorta;DA, ductus arteriosus; DV, ductus venosus; LA, leftatrium; LV, left ventricle; PA, pulmonary artery;RA, right atrium; RV, right ventricle.
the lower body and hepatic veins. This higher veloc-ity facilitates delivery of this higher oxygen contentblood across the foramen ovale (FO) into the leftatrium (LA).IVC blood enters the right atrium (RA) and due
to the position of the Eustachian valve, Chiarinetwork, and FO enters the LA during 80% of thecardiac cycle. During the other 20% (atrial systole)IVC blood crosses the tricuspid valve and enters theright ventricle (RV). The overwhelming majority ofsuperior vena cava (SVC) crosses the tricuspid valveand enters the RV as well. Blood from the RV isejected into the pulmonary artery (PA). Approxi-mately 10–15%of blood from the PApasses throughthe lungs to reach the LA the rest is shunted tothe distal aorta via the ductus arteriosus (DA). Asa result, two-thirds of total fetal cardiac output isprovided by the RV with the remaining one-thirdprovided via the left ventricle (LV).The dynamics of shunting at the level of the
ductus venosus, FO, and DA result in preferentialdelivery of the most highly oxygenated blood to
the coronary and cerebral circulations. Obviously,this preferential delivery of oxygenated blood iscompromised in utero by cardiac lesions that preventor reduce LV output.At birth, a series circulation is established in
which each ventricle pumps into a specific vascu-lar bed (RV to PA; LV to aorta). The removal of theplacenta and the initiation of alveolar ventilationat birth have the immediate effect of establish-ing this series circulation. To maintain the adultseries circulation, the fetal channels must be closed.Complex neurochemical and hormonal influencesaffect the closing of these fetal shunts. Acidosis,sepsis, hypothermia, hypoxia, and hypercarbia maycause reopening of the shunts and persistence ofthe fetal circulation (PFC). Most neonates who arecritically ill from CHD have one or more of theseinciting factors at the time of presentation. In someinstances, persistence of fetal circulatory channelsmay be beneficial or even mandatory for survival.
Closure of the ductus arteriosusIn the fetus, patency of the ductus arteriosus (DA) ismaintained by high levels of prostaglandin (prosta-cyclin (PGI2) and prostaglandin E1 (PGE1)). Thereare two stages of ductal closure in the newborn:functional closure and permanent anatomic clo-sure. Functional closure occurs by contraction ofthe smooth muscle of the ductal wall and usuallyoccurs within the first day of life. An increase inpartial pressure of oxygen (PO2) and a decreasein prostaglandins contribute to functional closure.Oxygen is a dose-dependent ductal constrictor thatacts by increasing the rate of oxidative phosphory-lation within smooth muscle cells. In addition, theresponse to oxygen may be age-related; full-termneonates have a more dramatic response to oxygenthan an immature newborn. Norepinephrine andepinephrine, by changing pulmonary and systemicvascular resistances, may secondarily contribute toductal closure. Acetylcholine has a direct constrictoreffect on ductal tissue. Permanent anatomic closureof the duct usually is accomplished by 2–3weeksof life in the normal full-term neonate. The lumenis sealed by fibrous connective tissue, leaving thevestigial structure, known as the ligamentum arte-riosum (Fig. 6.2a–c).

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 169 — #3
Congenital Heart Disease 169
(b)
m3850 30
PA
68
97DA
70
97
9767
60
RA 97
IVC
65
m2 m4
RV LV
LA PVSVC
Ao
705
7045
m55
50 3
IVC
Ao
65
DA55
55 65
60
PV
m55
RV LV
SVC
40
RA
70
m3 m2
LA
m557045
PA
(a)
704
703
7045
(c)
99
65PA
Ao
99
9965
RV
SVC
60RA
LA
65
IVC
99
m4m2
LV
PV
m60
65m1830
12
805
8050
303
Fig. 6.2 Hemodynamics of the fetus and neonate.Circled figures are oxygen saturations. Systolic, diastolic,and mean (m) pressures appear near their respectivechambers and vessels. (a) Circulation of the term fetus.(b) Transitional circulation less than 1 day after birth.
(c) Circulation several days after birth. Ao, aorta;DA, ductus arteriosus; DV, ductus venosus; IVC, inferiorvena cava; LA, left atrium; LV, left ventricle; PA,pulmonary artery; PV, pulmonary vein; RA, right atrium;RV, right ventricle; SVC, superior vena cava.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 170 — #4
170 Chapter 6
Survival of some neonates with congenital car-diac lesions is dependent on ductal patency. Becausefunctional closure is a reversible event, the useof PGE1 infusions (0.01–0.05µg/kg/min) has beenone of the major medical advances in stabilizationof neonates with ductal-dependent heart lesions.Preterm neonates are at risk of delayed ductalclosure. This may be due to decreased degradationof PGE1, increased production of PGE1, or dimin-ished sensitivity to the ductal constricting effectsof oxygen. In instances in which delayed ductalclosure is disadvantageous, prostaglandin inhibitorssuch as indomethacin (0.1–0.3mg/kg orally (PO)or intravenously (IV)) have been used successfullyto promote ductal closure and establish normalpatterns of pulmonary blood flow.
Closure of the foramen ovaleIn utero, the right atrial pressure is higher thanleft atrial pressure (LAP) IVC blood flows in sucha manner as to keep the foramen ovale (FO)open. Removal of the placenta causes a significantdecrease in venous return to the right heart, caus-ing a decrease in right atrial pressure. In addition,ventilation causes a marked increase in pulmonaryarterial and venous blood flow resulting in anincrease in LAP. This elevation of left atrial relativeto right atrial pressure causes the flap-like valve ofthe FO to functionally close. In instances in whichright atrial pressure remains elevated, right-to-left(R–L) shuntingmay persist. Functional closure usu-ally progresses to anatomic closure. However, probepatency of the FO may persist in 30% of normaladults and 50% of children younger than 5 yearsof age.
Closure of the ductus venosusThe umbilical vessels constrict strongly aftermechanical stimulation and high oxygen tensionsfacilitate this process. The resultant decrease inumbilical venous blood flow causes passive closureof the ductus venosus. The ductus venosus does notappear to be as sensitive as the DA to the arterialpartial pressure of oxygen (PaO2), the arterial par-tial pressure of carbon dioxide (PaCO2), or pH. Highlevels of norepinephrine also cause constriction. Theductus venosus is functionally closed by 1week
of life and anatomically closed by 3months. Theremaining structure is the ligamentum venosum.In addition to the establishment of the adult
series circulation, dramatic alterations in pulmonarycirculation, cardiac output and distribution, myo-cardial performance, and myocardial cell growthand hypertrophy continue to occur during the firstweeks, months, and even years of life. In the pres-ence of CHD, these changes may be pathologicallyaffected.
Pulmonary vascular changesThe fetus has low pulmonary blood flow secondaryto a high pulmonary vascular resistance (PVR). Theminimal blood flow that reaches the pulmonarybed has a very low PaO2, which may cause hypoxicpulmonary vasoconstriction and contributes to theelevated pulmonary resistance seen in the fetus.Morphologic examinations of the small arteries ofthe fetal and newborn lung show a thick medialsmooth muscle layer. The fetal pulmonary vas-culature is reactive to a number of stimulants.Vasoconstriction is induced by decreases in PaO2,pH, and leukotrienes. Acetylcholine, histamine,bradykinin, PGE1, PGE2, PGI2 (prostacyclin), andprostaglandin D2 and β-adrenergic catecholaminesare potent vasodilators of fetal pulmonary ves-sels.At birth, alveolar ventilation commences. This
reduces mechanical compression of small pul-monary vessels and increases PaO2. The result is adramatic reduction in PVR. During the followingweeks and months, remodeling of the pulmonaryvessels occurs; themost notable change is a thinningof the medial smooth muscle layer. By 6months oflife, this process results in reduction of PVR to nearnormal adult levels. The normal process of postnatalpulmonary maturation may be altered significantlyby pathologic conditions, such as those associatedwith CHD.
Myocardial performance inthe neonateIn utero, the RV has a cardiac output of approxi-mately 330mL/kg/min compared with the LV out-put of 170mL/kg/min. At birth, both RV and LVeject an output of approximately 350mL/kg/min.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 171 — #5
Congenital Heart Disease 171
This requires minimal stroke volume increase forthe RV but a considerable increase in stroke volumefor the LV. The high output state of the new-born effectively limits further increases in cardiacoutput. This high output state decreases to about150mL/kg/min by 8–10weeks of life.Myocardial morphology and performance is
notably different in the neonate. These differencesare summarized as follows:• Afterload mismatch. The neonatal heart is moresusceptible to afterload mismatch, and therefore,stroke volume is poorly maintained in the face ofincreasing outflow resistance.• Limited preload reserve. The neonatal heart haslimited preload reserve. Augmentation of strokevolume via the Frank–Starlingmechanism is limitedas compared with an adult.• Reduced contractile capacity. Neonatal cardiac cellscontain more water and fewer contractile elementsthan mature myocardium.• Reduced ventricular compliance. The compliance ofthe neonatal myocardium is reduced because a defi-ciency of elastic elements parallels the deficiency ofcontractile elements.• Increased intraventricular dependence. Changes inventricular pressure are transmitted to the oppositeventricle via the ventricular septum more read-ily in the immature myocardium. Left ventricu-lar diastolic filling is disproportionately impairedin the neonate by high right ventricular end-diastolic pressure. This is due to a leftward shiftof the intraventricular septum and a reductionin left ventricular distensibility. Right ventricu-lar diastolic filling is impaired to an equal extentby high left ventricular end-diastolic pressure inneonates. This enhanced ventricular interactionis caused by reduced ventricular compliance andbecause, at birth, the LV and RV are of equal mass.The increased volume and pressure load experi-enced by the LV after birth produces relative LVhypertrophy. The normal adult LV to RV massratio of 2:1 is not seen until several months afterbirth.• Incomplete autonomic innervation. Sympatheticinnervation, which is responsible for increasingheart rate and contractility, is incompletely devel-oped at birth. As a result, local myocardial release
of norepinephrine contributes less to increasesin contractility than do increases in circulatingcatecholamine levels. For this reason, inotropicagents such as dopamine, the effects of whichare partially mediated through release of nor-epinephrine from myocardial nerve endings, mayhave to be used in higher doses to be effective inyounger patients. On the other hand, the parasym-pathetic system, which reflexly slows the heart, isfully functional at birth.• Immature myocardial metabolism. The neonatalmyocardium is more dependent on anaerobicmetabolism than the adult heart. This may havea somewhat protective effect, making the neo-natal myocardium more tolerant to the effects ofhypoxia.
Pathophysiology of CHD
While some congenital heart defects involve purelyobstructive or regurgitant valvular lesions, the pres-ence of shunts (both physiologic and anatomic)is the hallmark of CHD. Anesthetic managementof the patient with CHD is dependent on a clearunderstanding of:• The concepts of shunting (both physiologicand anatomic), single ventricle physiology, andintercirculatory mixing.• The types of anatomic shunts and the dynamicsof the anatomic shunting process.• The effects of congenital lesions on thedevelopment of the pulmonary vascular system.• The factors that influence pulmonary andsystemic vascular resistance.• The factors responsible for producing myocardialischemia.
The concepts of shunting,single ventricle physiology, andintercirculatory mixing
ShuntingShunting is the process whereby venous returninto one circulatory system is recirculated throughthe arterial outflow of the same circulatory sys-tem. Flow of blood from the systemic venousatrium or RA to the aorta produces recirculation

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 172 — #6
172 Chapter 6
of systemic venous blood. Flow of blood fromthe pulmonary venous atrium or LA to the PAproduces recirculation of pulmonary venous blood.Recirculation of blood produces a physiologic shunt.Recirculation of pulmonary venous blood producesa physiologic left-to-right (L–R), whereas recircu-lation of systemic venous blood produces a physi-ologic R–L shunt. A physiologic R–L or L–R shuntcommonly is the result of an anatomic R–L or L–Rshunt. In an anatomic shunt, bloodmoves from onecirculatory system to the other via a communica-tion at the level of the cardiac chambers or greatvessels. Physiologic shunts can exist in the absenceof an anatomic shunt. Transposition physiology isthe primary example of this process.Effective blood flow is the quantity of venous
blood from one circulatory system reaching thearterial system of the other circulatory system.Effective pulmonary blood flow is the volume ofsystemic venous blood reaching the pulmonary cir-culation, whereas effective systemic blood flow isthe volume of pulmonary venous blood reach-ing the systemic circulation. Effective pulmonaryblood flow and effective systemic blood flows arethe flows necessary to maintain life. Effective pul-monary blood flow and effective systemic bloodflow are always equal, no matter how complex thelesions. Effective blood flow usually is the result ofa normal pathway through the heart, but it mayoccur as the result of an anatomic R–L or L–Rshunt.Total pulmonary blood flow (QP) is the sum of
effective pulmonary blood flow and recirculatedpulmonary blood flow. Total systemic blood flow(QS) is the sum of effective systemic blood flow andrecirculated systemic blood flow. Total pulmonaryblood flowand total systemic blood flowdonot haveto be equal. Therefore, it is best to think of recir-culated flow (physiologic shunt flow) as the extra,noneffective flow superimposed on the nutritiveeffective blood flow. These concepts are illustratedin Figs 6.3 and 6.4.
Single ventricle physiologySingle ventricle physiology is used to describethe situation wherein complete mixing of pul-monary venous and systemic venous blood occurs
at the atrial or ventricular level and the ventricle(s)then distribute output to both the systemic andpulmonary beds. As a result of this physiology the:• Ventricular output is the sum of pulmonary bloodflow (Qp) and systemic blood flow (Qs).• Distribution of systemic and pulmonary bloodflow is dependent on the relative resistances to flow(both intra and extracardiac) into the two parallelcircuits.• Oxygen saturations are the same in the aorta andthe PA.• This physiology can exist in patients with onewell-developed ventricle and one hypoplastic ven-tricle as well as in patients with two well-formedventricles.In the case of a single anatomic ventricle there
is always obstruction to either pulmonary or sys-temic blood flow as the result of complete or nearcomplete obstruction to inflow and/or outflow fromthe hypoplastic ventricle. In this circumstance theremust be a source of both systemic and pulmonaryblood flow to assure post-natal survival. In someinstances of a single anatomic ventricle, a direct con-nection between the aorta and the PA via a patentductus arteriosus (PDA) is the sole source of sys-temic blood flow (hypoplastic left heart syndrome(HLHS)) or of pulmonary blood flow (pulmonaryatresia with intact ventricular septum or PA/IVS).This is known as ductal dependent circulation.In other instances of a single anatomic ventricle,intracardiac pathways provide both systemic andpulmonary blood flow without the necessity of aPDA. This is the case in tricuspid atresia (TA) withnormally related great vessels, a nonrestrictive ven-tricular septal defect (VSD) and minimal or absentpulmonary stenosis.Single ventricle physiology can exist in the pres-
ence of two well-formed anatomic ventricles whenthere is complete or near complete obstruction tooutflow from one on the ventricles:• Tetralogy of Fallot (TOF) with PA where pul-monary blood flow is supplied via a PDA or majoraortopulmonary collateral arteries (MAPCAs).• Truncus arteriosus.• Severe neonatal aortic stenosis and interruptedaortic arch; in both lesions a substantial portion ofsystemic blood flow is supplied via a PDA.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 173 — #7
Congenital Heart Disease 173
Saturations(%)
98
80
65
65
LA RA
LA
LV
Ao
Qs
1.5 1.8
3.3
PA
Qp
1.5 1.3
2.8
2.8 3.3Vena cavae
RA
RV
Effective pulmonaryand systemic bloodflow
Physiologic shuntflow
80 80
LV RV
Pulmonary veins Vena cavae
Flow(L/min/m2)
Flow(L/min/m2)
Pressures(mmHg)
Pressures(mmHg)
A = 5V = 7
100/4 25/5
Total systemicblood flow
Total pulmonaryblood flow
10/6100/60
SVR = 22.7 mmHg/L/min /m2 PVR = 1.4 mmHg/L/min /m2
4
Saturations(%)
Pulmonaryveins
–
8–
A = 10V = 5 5
–
80 Ao80
PA80
—
Fig. 6.3 Depiction of saturations, pressures, and bloodflows in type 1B tricuspid atresia with a mildly restrictiveatrial septal defect (ASD), a small restrictive ventricularseptal defect (VSD), and mild pulmonic stenosis (PS).Complete mixing or blending occurs at the atrial level.This complete mixing is the consequence of an obligatoryphysiologic and anatomic right-to-left (R–L) shuntingacross the ASD. Effective pulmonary and effectivesystemic blood flow are equal (1.5 L/min/m2). Effectivesystemic blood flow occurs via a normal pathwaythrough the heart. Effective pulmonary blood flow is theresult of an anatomic R–L shunt at the atrial level and ananatomic left-to-right (L–R) shunt at the ventricularlevel. This illustrates the concept that when completeoutflow obstruction exists and there is obligatoryanatomic shunting, a downstream anatomic shunt must
exist to deliver blood back to the obstructed circuit. Totalpulmonary blood flow (QP) is 2.8 L/min/m
2 and is thesum of effective pulmonary blood flow (1.5 L/min/m2)and a physiologic and anatomic L–R shunt(1.3 L/min/m2) at the VSD. Total systemic blood flow(QS) is 3.3 L/min/m2 and is the sum of effective systemicblood flow (1.5 L/min/m2) and a physiologic andanatomic R–L shunt (1.8 L/min/m2) at the ASD.In this depiction, there is a small pressure gradient at
the atrial level and a large pressure gradient at theventricular level. In addition, there is a small additionalgradient at the level of the pulmonic valve. Ao, aorta; LA,left atrium; LV, left ventricle; PVR, pulmonary vascularresistance; RA, right atrium; RV, right ventricle; SVR,systemic vascular resistance.
• Heterotaxy syndrome where there are compo-nents of systemic venous (SVC, IVC, hepatic veins,azygous veins) and pulmonary venous return toboth right and left sided atria. In addition, atrialmorphology is ambiguous.Despite the fact that patients with totally anoma-
lous pulmonary venous return (TAPVR) have com-plete mixing of pulmonary and systemic venousblood at the atrial level they do not manifest theother features necessary to create single ventri-cle physiology. This holds true as well for lesionsin which a common atrial or ventricular cham-ber exists due to bidirectional (both L–R and R–L)anatomic shunting across a large defect (atrialseptal or ventricular septal) and where there is
no obstruction to ventricular outflow. Table 6.1 listsa number of single ventricle physiology lesions.All patients with single ventricle physiology who
have severe hypoplasia of one ventricle will ulti-mately be staged down the single ventricle pathwayto Fontan physiology. This will be discussed indetail later. Patients with single ventricle physiol-ogy and two well-formed ventricles will be ableto undergo a two-ventricle repair. In some casesthe two-ventricle repair will be complete. In others,significant residual lesions (VSD, aortopulmonarycollaterals) may remain.With single ventricle physiology, the arterial sat-
uration (SaO2) will be determined by the relativevolumes and saturations of pulmonary venous and

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 174 — #8
174 Chapter 6
Saturations(%)
99
95
50
70
LA RA
LA
LV
PA
Qp
9.0 1.1
10.1
Ao
Qs
1.1 1.2
2.3
10.1 2.3Vena cavae
RA
RV
Effective pulmonaryand systemic bloodflow
Physiologic shuntflow
94 72
LV RV
Pulmonary veins Vena cavae
Flow(L/min/m2)
Flow(L/min/m2)
Pressures(mmHg)
Pressures(mmHg)
Pulmonaryveins
A = 3V = 6
35/5 90/4
Total pulmonaryblood flow
Total systemicblood flow
90/5018/10
PVR = 0.8 mmHg/L/min/m2 SVR = 28.7 mmHg/L/min/m2
4
Saturations(%)
Pulmonaryveins
–
70—
A = 7V = 3 4
–
12 PA94
Ao72
—
Fig. 6.4 Depiction of saturations, pressures, and bloodflows in transposition of the great arteries with anonrestrictive atrial septal defect (ASD) and a small leftventricular outflow tract gradient. Intercirculatorymixing occurs at the atrial level. Effective pulmonary andeffective systemic blood flows are equal (1.1 L/min/m2)and are the result of a bidirectional anatomic shunt at theatrial level. The physiologic L–R shunt is 9.0 L/min/m2;this represents blood recirculated from the pulmonaryveins to the pulmonary artery. The physiologic R–Lshunt is 1.2 L/min/m2; this represents blood recirculatedfrom the systemic veins to the aorta. Total pulmonary
blood flow (QP = 10.1 L/min/m2) is almost five timestotal systemic blood flow (QS = 2.3 L/min/m2). The bulkof pulmonary blood flow is recirculated pulmonaryvenous blood. In this depiction, pulmonary vascularresistance is low (approximately 1/35 of systemicvascular resistance) and there is a small (17mmHg peakto peak) gradient from the left ventricle to thepulmonary artery. These findings are compatible withthe high pulmonary blood flow depicted. Ao, aorta;LA, left atrium; LV, left ventricle; PVR, pulmonaryvascular resistance; RA, right atrium; RV, right ventricle;SVR, systemic vascular resistance.
systemic venous blood flows that have mixed andreach the aorta. This is summarized in the followingequation:
Aortic saturation = [(systemic venous saturation)
× (total systemic venous blood flow)
+ (pulmonary venous saturation)
× (total pulmonary venous blood flow)]
÷ [total systemic venous blood flow
+ total pulmonary venous blood flow].
This is illustrated in Fig. 6.3 where:
SaO2 = [(65)(3.3)+ (98)(2.8)]/(3.3+ 2.8) = 80%From this equation, it is apparent that with singleventricle physiology, three variables will determinearterial saturation:1 The ratio of total pulmonary to total systemicblood flow (Qp:Qs). A greater proportion of
the mixed blood will consist of saturated blood(pulmonary venous blood) than of desaturatedblood (systemic venous blood) when Qp:Qs ishigh. Figure 6.5 demonstrates the increase in arte-rial saturation that occurs with increases in pul-monary blood flow relative to systemic blood flow.Figure 6.5 also demonstrates that an arterial satu-ration approaching 100% is possible only with anextremely large Qp:Qs.2 Systemic venous saturation. For a given QP:QS andpulmonary venous saturation, a decrease in sys-temic venous saturation will result in a decreasedarterial saturation. Decreases in systemic venoussaturation occur as the result of decreases in sys-temic oxygen delivery or increases in systemicoxygen consumption. Recall that systemic oxygendelivery is the product of systemic blood flow andarterial oxygen content. Arterial oxygen content isdependent on the hemoglobin concentration andthe arterial saturation.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 175 — #9
Congenital Heart Disease 175
Table 6.1 Anatomic subtypes of single ventricle physiology.
Aortic bloodflow from
Pulmonary arteryblood flow from
HLHS PDA RV
Severe neonate aortic stenosis PDA RV
IAA LV (proximal)PDA (distal)
RV
PA/IVS LV PDA
Tetralogy of Fallot with pulmonary atresia LV PDA, MAPCAs
Tricuspid atresia, NRGA, with pulmonaryatresia (type 1A)
LV PDA, MAPCAs
Tricuspid atresia, NRGA, with restrictive VSDand pulmonary stenosis (type 1B)
LV LV thru VSD to RV
Tricuspid atresia, NRGA, with non-restrictiveVSD and no pulmonary stenosis (type 1C)
LV LV thru VSD to RV
Tricuspid atresia, D-TGA, with non-restrictiveVSD and pulmonary atresia (type 2A)
LV thru VSD to RV PDA, MAPCAs
Tricuspid atresia, D-TGA, with non-restrictiveVSD and pulmonary stenosis (type 2B)
LV thru VSD to RV LV
Tricuspid atresia, D-TGA, with non-restrictiveVSD and no pulmonary stenosis (type 2C)
LV thru VSD to RV LV
Tricuspid atresia, D-loop ventricles, L-TGA,subpulmonic stenosis (type 3A)
LV LV thru VSD to RV
Tricuspid atresia, L-loop ventricles, L-TGA,subaortic stenosis (type 3B)
LV thru VSD to RV LV
Truncus arteriosus LV and RV Aorta
DILV, NRGA LV LV thru VSD to BVF
DILV, L-loop ventricles, L-TGA, restrictive BVF LV thru VSD toBVF, PDA
LV
BVF, bulboventricular foramen; D, dextro; DILV, double inlet left ventricle; HLHS, hypoplastic leftheart syndrome; IAA, interrupted aortic arch; L, levo; LV, left ventricle;MAPCAs,multiple aortopul-monary collateral arteries; NRGA, normally related great arteries; PA/IVS, pulmonary atresia withintact ventricular septum; PDA, patent ductus arteriosus; RV, right ventricle; TGA, transpositionof the great arteries; VSD, ventricular septal defect.
3 Pulmonary venous saturation. In the absence oflarge intrapulmonary shunts and/or V /Q mis-match, pulmonary venous saturation should beclose to 100% breathing room air. In the presenceof pulmonary parenchymal disease, pulmonary
venous saturation may be reduced. The V /Qmismatch component of pulmonary venous desat-uration will be largely eliminated with a fractionalinspired oxygen concentration (FiO2) of 1.0 whilethe intrapulmonary shunt contribution will not be

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 176 — #10
176 Chapter 6
0
10
20
30
40
50
60
70
80
90
0 2 4 6 8 10QP:QS
SaO
2
300 mL /min/kg450 mL /min/kg
Fig. 6.5 Graph of systemic SaO2 versus QP:QS for twodifferent systemic ventricular outputs (300mL/kg/minand 450mL/kg/min) in single ventricle physiology.In this example oxygen (O2) consumption isassumed to be 9mL/kg/min and SpvO2 = 95%. It isclear that SaO2 peaks at or near a QP:QS of 1:1. Furtherincreases in QP:QS produce minimal to no increasesin SaO2.
eliminated. For any given systemic venous sat-uration and QP:QS a reduction in pulmonaryvenous saturation will result in a decreased arterialsaturation.
Intercirculatory mixingIntercirculatory mixing is the unique situation thatexists in transposition of the great arteries (TGA)(see Fig. 6.4). In TGA, two parallel circulations existdue to the existence of atrioventricular (AV) concor-dance (RA to RV, LA to LV) and ventriculoarterialdiscordance (RV to aorta, LV to PA). This producesa parallel rather than a normal series circulation.In this arrangement, blood flow will consist of par-allel recirculation of pulmonary venous blood inthe pulmonary circuit and systemic venous bloodin the systemic circuit. Therefore, the physiologicshunt or the percentage of venous blood from onesystem that recirculates in the arterial outflow ofthe same system is 100% for both circuits. Unlessthere are one or more communications (atrialseptal defect (ASD), patent foramen ovale (PFO),VSD, PDA) between the parallel circuits to allowintercirculatory mixing, this lesion is incompatiblewith life.
An anatomic R–L shunt is necessary to pro-vide effective pulmonary blood flow, whereasan anatomic L–R shunt is necessary to provide effec-tive systemic blood flow. Effective pulmonary bloodflow, effective systemic blood flow, and the volumeof intercirculatory mixing must always be equal.Total systemic blood flow is the sum of recirculatedsystemic venous blood plus effective systemic bloodflow. Likewise, total pulmonary blood flow is thesum of recirculated pulmonary venous blood pluseffective pulmonary blood flow. Recirculated bloodmakes up the largest portion of total pulmonary andtotal systemic blood flow with effective blood flowscontributing only a small portion of the total flows.This is particularly true in the pulmonary circuitwhere the total pulmonary blood flow (QP) and thevolume of the pulmonary circuit (LA to LV to PA) is2–3 times larger than the total systemic blood flow(QS) and the volume of the systemic circuit (RA toRV to aorta). The net result is transposition physi-ology, in which the PA oxygen saturation is greaterthan the aortic oxygen saturation.Arterial saturation (SaO2) will be determined by
the relative volumes and saturations of the recircu-lated systemic and effective systemic venous bloodflows reaching the aorta. This is summarized in thefollowing equation:
Aortic saturation = [(systemic venous saturation)
× (recirculated systemic venous blood flow)
+ (pulmonary venous saturation)
× (effective systemic venous blood flow)]
÷ [total systemic venous blood flow
].
This is illustrated in Fig. 6.4 where:
SaO2 = [(50)(1.2)+ (99)(1.1)]/2.3 = 73%.
Obviously, the greater the effective systemic bloodflow (intercirculatory mixing) relative to the recir-culated systemic blood flow, the greater the aorticsaturation. For a given amount of intercirculatorymixing and total systemic blood flow, a decrease insystemic venous or pulmonary venous saturationwill result in a decrease in arterial saturation.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 177 — #11
Congenital Heart Disease 177
Table 6.2 Simple shunts (no obstructivelesions).
Restrictive(small communication)
Nonrestrictive(large communication)
1 Large shunt pressure gradient 1 Small shunt pressure gradient2 Direction and magnitude ofshunt are relatively independentof PVR:SVR
2 Direction and magnitude of shuntare largely dependent on PVR:SVR
3 Shunt is less subject to controlby ventilatory or pharmacologicinterventions
3 Shunt is subject to control byventilatory or pharmacologicinterventions
Examples: Small VSD, small PDA,modified Blalock–Taussig shunt,small ASD
Examples: Large VSD, large PDA, CAVC
ASD, atrial septal defect; CAVC, complete atrioventricular canal defect; PDA,patent ductus arteriosus; PVR, pulmonary vascular resistance; SVR, systemicvascular resistance; VSD, ventricular septal defect.
Classification of anatomic shuntsAnatomic shunts can be characterized as simple orcomplex.
Simple shuntsIn an anatomic shunt, a communication (orifice)exists between pulmonary and arterial vessels orheart chambers (Table 6.2). In a simple shunt, thereis no fixed obstruction to outflow from the vesselsor chambers involved in the shunt. When the shuntorifice is small (restrictive shunt), a large pressuregradient exists across the orifice, and variationsin outflow resistance (PVR; and systemic vascularresistance (SVR)) have little effect on shunt magni-tude and direction. In this instance, the magnitudeof the shunt is affected by the size of the shuntorifice. However, when the shunt orifice is large,the shunt becomes nonrestrictive, and the outflowresistance becomes the primary determinant of themagnitude and direction of shunting. These shunts,in which the ratio of PVR to SVR determines themagnitude of shunting, are known as dependentshunts. When the communication is very large,no pressure gradient exists between the vessels orchambers involved. In this instance, bidirectionalshunting occurs, resulting in complete mixing anda functionally common chamber. Net systemic andpulmonary blood flow is then determined by theratio of systemic to PVR (Fig. 6.6a–c).
Complex shuntsIn complex anatomic shunt lesions there is obstruc-tion to outflow in addition to a shunt orifice(Table 6.3). The obstruction may be at the valvular,subvalvular, or supravalvular level. The obstruc-tion may be fixed (as with valvular or infundibularstenosis) or variable (as with dynamic infundibu-lar obstruction). In complex shunts, outflow resis-tance is a combination of the resistance across theobstructive lesions and the resistance across the pul-monary or systemic vascular bed (Fig. 6.7). Whenan obstruction is severe, the SVR or PVR distalto the obstruction will have little effect on shuntmagnitude or direction.TOF is a good example of a complex shunt
in which there is partial obstruction to out-flow. There is a fixed component of right ven-tricular outflow obstruction in TOF secondary toinfundibular, valvular, and possibly supravalvu-lar obstruction. A dynamic component of rightventricular obstruction is produced by changesin the caliber of the right ventricular infundibu-lum. These two components of right ventricularoutflow obstruction can produce a R–L shunt.Because right ventricular outflow obstruction isincomplete, increases in PVR will also increasethe total right ventricular outflow resistance andincrease R–L shunting. Similarly, a decrease inSVR relative to PVR will increase R–L shunting

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 178 — #12
178 Chapter 6
Outflow = PVRresistance
SVR = Outflow resistance
Increased PVR
Pulmonaryflow
PVR
Systemicflow
Pulmonaryflow
SVRPVR
SVR
Systemicflow
Increased SVR
2) Balance of:
1) Orifice size
Pulmonary sideSystemic side
Chamber or great vessel(a)
(b) (c)
Fig. 6.6 Influence of orifice size and the pulmonaryvascular resistance:systemic vascular resistance(PVR:SVR) ratio on the magnitude and direction ofa dependant shunt. (a) PVR and SVR are balancedresulting in equal pulmonary and systemic blood flows.
(b) PVR is reduced relative to SVR, resulting in anincrease in pulmonary blood flow and a decrease insystemic blood flow. (c) PVR is elevated relative to SVR,resulting in a decrease in pulmonary blood flow and anincrease in systemic blood flow.
Partial outflow obstruction Complete outflow obstruction
1 Shunt magnitude and directionis largely fixed due to theobstruction
1 Shunt magnitude and directionis totally fixed
2 Shunt dependence on PVR:SVRis inversely related to the severityof the obstructive lesion
2 All flow is thru the shunt,independent of PVR:SVR
3 Shunt pressure gradient isdetermined by both the shuntorifice and the obstructive lesion
3 Shunt pressure gradient isdetermined only by the shuntorifice
Examples: TOF, VSD andpulmonary stenosis, VSD withcoarctation
Examples: Tricuspid atresia, mitralatresia, pulmonary atresia, aorticatresia
PVR, pulmonary vascular resistance; SVR, systemic vascular resistance; TOF,tetralogy of Fallot; VSD, ventricular septal defect.
Table 6.3 Complex shunts (shunt anddownstream obstructive lesion).

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 179 — #13
Congenital Heart Disease 179
Fig. 6.7 Influence of orifice size andtotal outflow resistance on themagnitude and direction of a complexshunt. Total outflow resistance will bea combination of pulmonary vascularresistance (PVR) or systemic vascularresistance (SVR) and the resistanceoffered by the obstructive lesion.
Systemic obstruction
Chamber or great vessel
Systemic side Pulmonary side
Orifice size
Orifice size
outflowresistance
= outflow resistance
= PVR
outflowresistance
SVR =
SVR + outlet obstruction
= outflow resistance
PVR + outlet obstruction
Pulmonary obstruction
Systemicflow
Systemicflow
Pulmonaryflow
Systemic side Pulmonary side
Pulmonaryflow
without any increase in right ventricular outflowresistance.Another form of complex shunt is present in
patients who have single ventricle physiology. Inthese lesions, changes in SVR or PVR play norole in determining shunt magnitude or direction.The entire shunt flow is fixed and obligatory acrossthe communication and complete mixing results.For flow of this mixed blood to reach the obstructedcircuit, an additional downstream shunt, such asa VSD or PDA must be present. The downstreamshunt may be simple or complex and is dependanton the ratio of PVR to SVR.These concepts are critical to a clear understand-
ing of the pathophysiology involved in patients withCHD. Describing a lesion as cyanotic or acyanoticmay be misleading and simplistic. For example, in apatient with TOF, there may be minimal valvular orinfundibular obstruction to pulmonary blood flowat baseline, and the patient may not be cyanotic.In fact, this type of patient (“pink Tet”) may havea large L–R shunt through the VSD with increasedpulmonary blood flow. During anesthesia, hyper-carbia and hypoxemia may develop resulting in
an increase in both PVR and the dynamic compo-nent of infundibular obstruction. This will producea net R–L shunt and cyanosis (“Tet spell”). Similarly,a cyanotic episode (a net R–L shunt) may be precip-itated in the same patient by the SVR reduction thataccompanies a febrile illness.
Pulmonary vascular pathophysiologyPulmonary vascular occlusive disease (PVOD) mayoccur as the result of congenital heart lesions.Unfortunately of late PVOD has been used asan abbreviation for pulmonary veno-occlusive dis-ease, a different process. PVOD as described inthe context of CHD produces obstruction to pul-monary blood flow due to structural changesin the pulmonary vasculature. The morphologicchanges have three components: increased mus-cularity of small pulmonary arteries, small arteryintimal hyperplasia, scarring, and thrombosis andreduced numbers of intra-acinar arteries. Thesechanges produce progressive obstruction to pul-monary blood flow and result in progressive andirreversible elevations of PVR and PA pressure.These changes may be graded morphologically

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 180 — #14
180 Chapter 6
using lung biopsy or angiographically using the PAangiogram. Ultimately, these changes elevate PVRand reduce pulmonary blood flow. The increasedmuscularity of the small pulmonary arteries thataccompanies development of PVOD enhancesthe response of the pulmonary vasculature topulmonary vasoconstrictors.The stimulus for development of PVOD is expo-
sure of the pulmonary vascular system (both in uteroand after birth) to abnormal pressure and flow pat-terns associated with CHD. In particular, three cate-gories of abnormalities predispose the developmentof PVOD:1 Exposure of the pulmonary vascular circuit tosystemic arterial pressures and high pulmonaryblood flows. Patients for whom the pulmonaryvasculature is exposed to high flows and systemicarterial pressures typically have very early devel-opment of PVOD. This classically occurs in thepresence of a large (nonrestrictive) VSD.2 Exposure of the pulmonary vascular circuit tohigh pulmonary blood flow in the absence of highPA pressures. The progression of PVOD is typi-cally much slower in this situation than when PApressure is also elevated. A large ASD or a small(restrictive) PDA are examples of this type of lesion.3 Obstruction of pulmonary venous drainage. Thiswill lead to elevation of pulmonary arterial pres-sure and will predispose to development of PVOD.Pulmonary venous obstruction may result fromstenotic pulmonary veins, which can exist in TAPVRor cor triatriatum. Pulmonary venous obstructionalso may occur as the result of high LAPs (mitralatresia, congenital aortic stenosis, severe coarctationof the aorta) or high right atrial pressures (TAPVR).
Control of PVRAlterations in PVR may be an important determi-nant of shunt magnitude and direction in someshunt lesions. Furthermore, the patient with CHDis likely to have an enhanced response of the pul-monary vasculature to vasoconstricting substances.It is therefore necessary to be familiar with theinterventions that will alter PVR in the patientwith CHD:• PaO2. Both alveolar hypoxia and arterial hypox-emia induce pulmonary vasoconstriction. A PaO2
lower than 50mmHg increases PVR over a widerange of arterial pH; however, this effect is enhancedwhen pH is lower than 7.40. Conversely, high levelsof inspired oxygen can reduce an elevated PVR.• PaCO2. Hypercarbia increases PVR, independentof changes in arterial pH. Hypocarbia, on the otherhand, reduces PVR only through production of analkalosis. In fact, reliable reductions in PVR andincreases in pulmonary blood flow and PaO2 areseen in children with R–L shunts when hyperventi-lation to a Paco2 near 20mmHg and a pH near 7.60is obtained.Similarly, post-cardiopulmonary bypass(CPB) hyperventilation to a Paco2 of 20–33mmHgand a pH of 7.50–7.56 in patients with preoperativepulmonary hypertension results in a reduction inPVRwhen comparedwith ventilation that producesnormocarbia or hypercarbia.• pH. Both respiratory and metabolic alkalo-sis reduce PVR, whereas both respiratory andmetabolic acidosis increase PVR.• Variation in lung volumes. At small lung volumes,atelectasis results in compression of extra-alveolarvessels, whereas at high lung volumes, hyper-inflation of alveoli results in compression of intra-alveolar vessels. Therefore, PVR is normally lowestat lung volumes at or near the functional residualcapacity. Positive end-expiratory pressure (PEEP)may cause an increase in PVR by increasing alve-olar pressure through hyperinflation. However, insituations in which PEEPworks to recruit atelectaticalveoli and increase arterial PaO2, a decrease in PVRgenerally is seen.• Anesthetic agents. This topic will be discussed atlength in the section on anesthetic agents.• Vasodilator agents. Most IV pulmonary vasodila-tors (PGE1, nitroglycerin, sodiumnitroprusside, andtolazoline) induce systemic vasodilation as well.A number of inhaled agents (of which nitric oxide(NO) is the prototype) capable of providing selec-tive pulmonary vasodilatation are now available.NO generated by endothelial NO synthase (eNOS)is an endogenous vasodilator. Awide variety of sub-stances that increase intracellular calcium stimulateproduction of NO from L-arginine via eNOS. Afterit has been formed, NO diffuses from endotheliumto vascular smooth muscle (VSM), where it bindsto and activates guanylate cyclase to produce cyclic

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 181 — #15
Congenital Heart Disease 181
guanosine monophosphate (cGMP). cGMP acts asa second messenger to catalyze reactions that leadto a reduction of VSM calcium by reduced cal-cium influx, increased calcium efflux, and reducedrelease of intracellular calcium. This produces relax-ation of VSM and vasodilation. NO is involved inmodulation of basal VSM tone as well. This modula-tion capacity is lost in vessels in which endotheliumis removed or damaged.Inhaled NO selectively reduces pulmonary hyper-
tension and improves ventilation/perfusion match-ing in a variety of disease states. Pulmonaryselectivity is based on three characteristics of NO:• Its gaseous state allows delivery to ventilatedalveoli by inhalation.• Its small size and lipophilicity allows readydiffusion into the appropriate cells.• Its avid binding to and rapid inactivation byhemoglobin prevents systemic vasodilatation. NObinds to oxyhemoglobin (Fe2+) to form nitro-sylhemoglobin which is rapidly converted tomethemoglobin (Fe3+) and NO−3 .Inhaled NO has been used to treat pulmonary
hypertension in both the pre- and post-CPB periodin a variety of congenital heart lesions and intreatment for persistent pulmonary hypertension ofthe newborn. Generally, approximately 20–40 ppminhaled NO has been used. Some caution is war-ranted because both NO dependency and reboundpulmonary hypertension following NO discontinu-ation has been reported. No may not be effective intreating pulmonary hypertension when there is adownstream obstruction to pulmonary blood flowsuch as:• Pulmonary vein obstruction.• LA hypertension from LV dysfunction or mitralvalve disease.• A small LV where an increase in pulmonaryvenous return is likely to elevate LAP.In these situations NO is unlikely to reduce pul-monary artery pressure (PAP) and will likely causeinterstitial pulmonary edema.An alternative to inhaled NO is aerosolized
prostacyclin (PGI2) and aerosolized PGE1. PGI2and its analogues (iloprost, epoprostenol or Flolan)and PGE1 act by binding to prostacyclin receptorsand activating cyclic adenosine monophosphate
(cAMP). This activates protein kinase A, whichleads to a reduction of VSM intracellular cal-cium, causing vasorelaxation. PGI2 also stimu-lates endothelial release of NO. Aerosolized PGI2(2–50ng/kg/min) is useful in selectively loweringPVR after congenital cardiac surgery. There is lessexperience with aerosolized PGE1 but at doses of150–300ng/kg/min it has been proved useful intreatment of neonatal respiratory failure.Sildenafil is cGMP-specific phosphodiesterase
(PDE5) inhibitor that also works to increase cGMPlevels. Oral, IV, and aerosolized sildenafil is effectivein reducing PVR.
Sympathetic nervous system stimulationSympathetic stimulation results in increases inboth pulmonary and systemic vascular resistance.In children with PA medial hypertrophy, this mayresult in a hyperactive pulmonary vasoconstrictorresponse. Blunting of sympathetic outflow duringa stress response attenuates increases in PVR inchildren predisposed to pulmonary hypertension.
In summary, control of ventilation with manip-ulation of PaO2, PaCO2, pH, and lung volumes arethe best methods for altering PVR independently ofSVR. A combination of a high inspired FiO2, a PaO2higher than 60mmHg, a PaCO2 of 30–35mmHg,a pH of 7.50–7.60, and low inspiratory pressureswithout high levels of PEEP, will produce reliablereductions in PVR. Conversely, a reduced FiO2, aPaO2 of 50–60mmHg, a PaCO2 of 45–55mmHg, andthe application of PEEP, can be used to increase PVR.Inhaled NO and prostacyclin are valuable selectivepulmonary vasodilators in some patients.
Myocardial ischemiaPatients with CHD are more at risk for the develop-ment of subendocardial ischemia than is commonlyappreciated. In some congenital lesions there areabnormalities in the coronary circulation predispos-ing to ischemia but in many others forms of CHDischemia occurs in the presence of normal coronaryarteries secondary to myocardial oxygen supply anddemand imbalance.Subendocardial perfusion is largely determined
by coronary perfusion pressure (CPP), which is

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 182 — #16
182 Chapter 6
the mean aortic diastolic pressure minus the ven-tricular end-diastolic pressure. In addition the timeinterval available for perfusion (predominately dias-tole) is critical. As a result, the relationship betweenheart rate, diastolic blood pressure, and ventricu-lar end-diastolic pressure will determine whethersubendocardial ischemia occurs. These factors asthey apply to patients with CHD are consideredbelow.
Aortic diastolic pressureSubendocardial perfusion in a ventricle withsystemic pressure occurs predominately in earlydiastole. In normal children, some subendocardialperfusion of the pulmonary or RV can occur insystole as well as in diastole because pulmonaryventricular systolic pressure is low. However, inmany congenital lesions systolic pressure in bothventricles is systemic, and in some cases the pul-monary ventricle may have suprasystemic pres-sures. As a result perfusion of both ventriclesmay be dependent on the rapid increase in earlydiastolic flow.Aortic diastolic pressure, which is normally low
in neonates and infants, is further compromisedin single ventricle physiology lesions because theselesions promote diastolic runoff of aortic blood intothe lower resistance pulmonary circuit. The sub-group of patients with ductal dependent systemicblood and patients with truncus arteriosus are par-ticularly at risk for enhanced aortic diastolic runoff.In addition, coronary perfusion is further compro-mised in patients with HLHS because the coronaryostia are perfused retrograde down a segment ofatretic ascending aorta.
Subendocardial pressureSubendocardial pressure is elevated and subendo-cardial perfusion is compromised in the pres-ence of elevated ventricular end-diastolic pressure.Elevated end-diastolic pressure may be the resultof impaired diastolic function (both reducedventricular compliance and impaired ventricularrelaxation), impaired systolic function, increasedventricular end-diastolic volume, or a combinationof all three. For example, elevated ventricular
end-diastolic pressure occurs as the result of theventricular volume overload that accompaniessingle ventricle lesions, lesions with a high QP:QS,and regurgitant AV and semilunar valve lesions.The ventricular hypertrophy that accompanies pres-sure overload lesions is particularly detrimentalto subendocardial perfusion. Ventricular hypertro-phy reduces ventricular compliance and elevatesventricular end-diastolic pressure. In addition, theextravascular compressive forces that accompany ahigh external pressure workload further compro-mise myocardial perfusion by reducing transmuralcoronary vascular reserve (CVR). CVR is the ratioof hyperemic myocardial blood flow to baselinemyocardial blood flow.
Heart rateThe duration of diastole diminishes geometricallyas heart rate increases while the duration of sys-tole remains relatively constant. As a result, thetime available for diastolic coronary artery perfu-sion falls as heart rate increases. Consequently,a higher diastolic pressure is necessary to main-tain subendocardial perfusion at higher heart rates.Hence, subendocardial perfusion is maintained inthe presence of a low diastolic blood pressure if theheart rate is slower. In an infant with HLHS andan aortic diastolic pressure of 25mmHg a heart rateof 130–140 b/min may well be tolerated withoutevidence of subendocardial ischemia whereas it isunlikely that a heart rate of 170–180 b/min will betolerated at the same diastolic pressure.
Anatomic coronary artery lesionsAnatomic coronary artery abnormalities compli-cate the management of patients with a numberof congenital cardiac lesions such as PA/IVS andWilliams–Beurin syndrome.
Preoperative evaluation
Psychological considerationsThe anesthesiologist who evaluates the patient withCHD must be aware of the considerable effect thatappropriate psychological preparation may haveduring the preoperative and postoperative period.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 183 — #17
Congenital Heart Disease 183
The pediatric patient has unique psychologicalconcerns that depend on age and previous surgi-cal and anesthetic experience. In addition, the effectthat serious heart disease has on parents and otherfamily members cannot be minimized and mustbe addressed sensitively during the preoperativeevaluation. Although neonates require no psycho-logical preparation, the perioperative process canoverwhelm the parents.The preoperative psychological preparation must
be appropriate to the age of the patient. Fear ofseparation from parents (“stranger anxiety”) can bemanifest in the infant at 8–12months with anintense aversion to strangers. Very few toddlers,even if playful and cooperative in the presenceof the parent, will leave their parent happily togo to the operating room. Older children havefears of disfigurement or that they will “wake up”or feel pain during and after surgery. Even thewithdrawn, seemingly complacent adolescent oftenis in great turmoil regarding impending surgery.Previous surgery and anesthesia will influence evena young child’s ability to cope with the newestoperative experience. Psychological issues influencenot only the conduct of the physical examina-tion but also how much detail is discussed withparents in the presence of the patient. Obtaininginformed consent from the parent in the presenceof a school-aged child may create undue stress forthe child. On the other hand, weak promises of “noneedles” or little discussion about what the childcan expect is equally unpleasant and counterpro-ductive. Most experienced pediatric anesthesiolo-gists, aware of the spectrum and unpredictabilityof children’s behavior, prudently plan for alterna-tive approaches to physical examination and, mostimportantly, how to pleasantly and safely sepa-rate the child from the parent for the induction ofanesthesia.
Clinical historyClinical history should include medications, aller-gies, past hospitalizations and operations (includ-ing prior anesthetic experiences), and a thoroughreview of systems. Performance of age-appropriateactivities will aid in the evaluation of cardiac
function and reserve. The infant in cardiac fail-ure will manifest symptoms of low cardiac reserveduring feeding. A parent might report that sweat-ing, tiring, dyspnea, and circumoral cyanosis duringfeeding. The observation by a parent that the patientcannot keep the same pace as siblings often is a reli-able clinical sign that cyanosis or congestive heartfailure is worsening. Frequent pulmonary infectionsmay occur as a result of increased pulmonary bloodflow in otherwise asymptomatic patients. Cardiaccatheterization data may be several months old bythe time the patient presents for surgery, and thenewly observed clinical signs may more accuratelyreflect the patient’s current cardiac status.
Physical examinationInterpretation of vital signs is age-specific. Heartrate decreases and blood pressure increases withage (Figs 6.8 and 6.9). Growth curves also areuseful. Congestive heart failure will sequentiallyinhibit age-appropriate gains in weight, height andhead circumference. It is not unusual for patientswith severe congestive heart failure to weigh less at4months of age than at birth. Interestingly, cyan-otic children often do not manifest this failure tothrive.Physical examination may reveal cyanosis, club-
bing, or signs of congestive heart failure similar tothose seen in adults (hepatomegaly, ascites, edema,or tachypnea). Rales may not be heard in infantsand children with congestive heart failure, and thedegree of heart failure may be determined morereliably by some of the signs and symptoms out-lined above. Cyanosis is visibly detectable whenthe deoxyhemoglobin concentration is >5 g/dL andanemia masks detection of cyanosis. Differentia-tion between congestive heart failure and a upperrespiratory tract infection can be difficult. The phys-ical examination in both conditions may show mildtachypnea,wheezing, and upper airway congestion.Abnormal laboratory findings may help distinguishbetween the two. The decision to proceed to surgerymay be necessary even when the differentiationbetween worsening congestive heart failure anda respiratory tract infection cannot be made withcertainty.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 184 — #18
184 Chapter 6
190
= Heart rate= ± 2 Standard deviations
170
150
130
Ave
rage
hea
rt r
ate
(b/m
in)
110
90
70
50Birth 1st
month1–6
months6–12
months1–2
years
Age
2–4years
6–10years
10–14years
14–18years Fig. 6.8 Variation in average heart rate
with age.
150
125
100
75
Nor
mal
blo
od p
ress
ure
(mm
Hg)
50
25
0Newborn 6
months1
year2
years3
years4
years5–6
years
Age
6–7years
7–8years
8–9years
9–10years
10–11years
11–12years
12–13years
13–14years
= Systolic blood pressure= ±2 Standard deviations= Diastolic blood pressure= ±2 Standard deviations= Point of muffling taken as diastolic pressure
Fig. 6.9 Variation in normal blood pressure with age.
Physical examination should include an evalua-tion of the limitations to vascular access and moni-toring sites. A child who has undergone a previouspalliative shunt procedure may have a diminishedpulse or unobtainable blood pressure in the arm inwhich the subclavian artery has been incorporated
into the shunt. This obviously has implications forarterial catheter placement, blood pressure moni-toring, and use of pulse oximetry during surgery.Finally, the child who has undergone multiple pal-liative procedures may have poor venous access,which will influence the mode of induction.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 185 — #19
Congenital Heart Disease 185
Approximately 8% of children with CHD haveother congenital abnormalities. Preoperative eval-uation must define these defects. For example,conotruncal lesions (TOF, interrupted aortic arch,truncus arteriosus, VSDs) are commonly associ-ated with a 22q11.2 chromosomal deletion. Thisdefect is associated with DiGeorge syndrome, velo-cardiofacial syndrome, and conotruncal anomalyface syndromes. These syndromes are associatedwith hypocalcemia, immunodeficiency, facial dys-morphia, palate anomalies, velopharyngeal dys-function, renal anomalies, and speech and feedingdisorders. ASDs, VSDs, and TOF are seen in childrenwith VACTERL (vertebral, vascular, anal, cardiac,tracheoesophageal, renal, and limb anomalies) andCHARGE (coloboma, heart anomaly, choanal atre-sia, retardation, and genital and ear anomalies)association. Tracheal stenosis must be consideredin patients with VATER (vertebral defects, imper-forate anus, transesophageal fistula, and radial andrenal dysplasia) association who have undergonetracheoesophageal fistula repair. The incidence ofCHD (primarily AV canal defects) in patients withtrisomy 21 is approximately 50%. As they agethese patients may present with problematic air-ways due to a large tongue and atlanto-occipitalinstability.
Laboratory dataA review of pertinent laboratory data and correla-tion with the clinical findings is necessary. The childin congestive heart failure may have mild iron defi-ciency because of chronically increased metabolicneeds. The cyanotic child will be erythrocytoticin direct relation to the degree of arterial desat-uration. Hematocrit levels higher than 65% areassociatedwith amarked increase in blood viscosity.To avoid possible neurologic sequalae from suchextreme viscosity, exchange transfusion should beconsidered before surgery. This is especially impor-tant if the proposed surgery is palliative and CPBwith hemodilution is not employed. Patients withsevere cyanosis and anemia may require transfu-sion. Cyanosis also affects the coagulation process,and it is not unusual to observe prolongation ofprothrombin time (PT), partial thromboplastin time(PTT), and bleeding times. Thrombocytopenia or
functional platelet defects also may exist. In the faceof reoperation with extensive dissection, the anes-thesiologist should plan adequate blood componenttherapy for each patient.Plasma electrolyte concentrations should be
screened, especially in patients receiving digitalisand diuretic therapy. Hypocalcemia may beobserved in patients with congestive heart fail-ure as well as patients with DiGeorge syndrome.Severe congestive heart failuremay be accompaniedby jitteriness and irritability. It is important to ruleout hypoglycemia as an alternative cause of thesefindings.The chest radiograph serves to confirm other clin-
ical and diagnostic findings, such as cardiomegaly,the quantity of pulmonary blood flow, previoussurgical procedures, and the presence of acute pul-monary infections. The electrocardiogram (ECG)similarly confirms chamber enlargement and thepresence of dysrhythmias. Review of the catheter-ization and echocardiographic data is critical to aclear understanding of the pathophysiology andsurgical plan. The following information shouldbe obtained routinely from a review of thecatheterization data:• Anatomic diagnosis.• Interpretation of saturation data. Saturation step-upsor step-downs between vessels and chambers areused to detect shunts. Likewise, saturation data areused to calculate the ratio of pulmonary to systemicblood flow (QP:QS). Saturation data also are usedto differentiate intrapulmonary shunting and V /Qmismatch (atelectasis, hypoventilation, pulmonarydisease) from intracardiac shunting.• Interpretation of pressure data. Pressure data areused to compare right and left heart pressures andsystemic and pulmonary arterial pressures. In addi-tion, pressure gradients across valve and shuntorifices are measured. Pressure data can be usedto assess ventricular diastolic function (distensibilityand compliance).• Interpretation of angiographic data. Cineangiogramscan be used to assess ventricular wall motion(systolic function) and to assess intracardiac andgreat vessel blood flow patterns.• Functional status and location of prior surgical inter-ventions. This information will allow intelligent

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 186 — #20
186 Chapter 6
decisions regarding monitor placement andanesthetic management to be made.• Effect of interventions. Interventions made in thecatheterization laboratory to palliate congenitalheart lesions (balloon valvuloplasty, balloon sep-tostomy, balloon angioplasty) are common. Theeffects of these interventions on the underlyinglesion must be assessed. Furthermore, a trial of100% inspired oxygen or NO may be used to assessthe reversible component of PA hypertension.Two-dimensional echocardiography has revolu-
tionized the field of pediatric cardiology over thelast decade. Unlike adults, who may have limitedtransthoracic echocardiographic windows, imagesin pediatric patients are easily obtained. Mostneonates proceed to surgerywithout catheterizationstudies. In rare instances catheterization is necessaryto clearly delineate coronary or aortopulmonarycollateral anatomy. Although angiocardiographicstudies often complement echocardiographic find-ings, it is not unusual for the echocardiographic datato be a superior diagnostic tool and offer the surgeonmore valuable anatomic information.
Preoperative preparation
The routine preoperative preparation of the anes-thesia equipment is not noticeably different for thepediatric patient. It is important to have various-sized airway equipment so that there can bequick selection of appropriate airways, masks, andendotracheal tubes. A pediatric circle system withhumidification can be used for older children.The resistance to airflow created by the unidirec-tional valves is not an issue for patients receivingmechanical ventilation. Generally, pressure-limitedventilation is used to avoid inadvertent baro-trauma. This mode of ventilation requires vigilancein that changes in chest wall or lung compli-ance will lead to instantaneous changes in tidalvolumes.Appropriate emergency medications should be
available in doses consistent with the patient’sweight (Tables 6.4 and 6.5). For critically ill patientsand patients with marginal reserve, selected infu-sions should be prepared in anticipation of their use.Careful attention should be paid to dosages because
Table 6.4 Vasoactive agents.
Agent Dosage (IV)
Calcium chloride 10–20mg/kgCalcium gluconate 50–100mg/kg
Epinephrine 0.05–0.50µg/kg/min
Norepinephrine 0.05–0.50µg/kg/min
Phenylephrine 0.1–0.50µg/kg/min
Isoproteronol 0.01–0.05µg/kg/min
Dobutamine 5–10µg/kg/min
Dopamine 3–15µg/kg/min
Milrinone Bolus 50µg/kg then0.3–1.0µg/kg/min
Nitroglycerin 0.5–5.0µg/kg/min
Nitroprusside 0.5–5.0µg/kg/min
Fenoldopam 0.1–0.5µg/kg/min
PGE1 Initiate at 0.05–0.10µg/kg/minthen 0.01–0.05µg/kg/min
IV, intravenous; PGE1, prostaglandin E1.
Table 6.5 Antiarrythmic agents.
Agent Dosage (IV)
Lidocaine Bolus 1mg/kg then20–50µg/kg/min
Procainamide Bolus 2–5mg/kg then20–50µg/kg/min
Diltiazem Bolus 0.1–0.2mg/kg then1–3µg/kg/min
Amiodarone Slow bolus of 2–5mg/kg with extremecaution in neonates/infants then7µg/kg/min
Esmolol Bolus 300–500µg/kg then50–300µg/kg/min
Adenosine 50–200µg/kg
Magnesium 10–25mg/kg
IV, intravenous.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 187 — #21
Congenital Heart Disease 187
the dose per kilogram may vary significantly fromthose used for adults.Appropriate IV catheters are placed with air-trap
filters in line to avoid the potential for air embolismin every patient (not just those with R–L shunts).
Preoperative fluid therapyPreoperative fluid and NPO (nothing by mouth)orders are routinely geared to the age-specific needsof the pediatric patient. Generally speaking therule of two, four, six, eight can be used as theNPO interval for neonates, infants and childrenwith CHD:• Two hours for clear liquids.• Four hours for breast milk.• Six hours for formula.• Eight hours for solid food.Obviously, in the absence of IV hydration infants
should remain NPO for the shortest possibleinterval. Because dehydration may have poten-tially deleterious effects on hemodynamics or onthe degree of blood viscosity in the polycythemicpatient, IV hydration with maintenance fluidsbefore surgery should be considered for certainpatients (i.e. cyanotic patients with hematocritlevels of 60% or higher).Maintenance caloric requirements in the awake
neonate and infant are 100 kcal/kg/day or4 kcal/kg/h. This caloric requirement can be metwith glucose 25 g/kg/day or 1 g/kg/h. From a prac-tical point of view this glucose requirement can bemet with 10% dextrose (100mg/mL) adminis-tered at maintenance volume replacement rate of4mL/kg/h. Ten percent dextrose administered athalf this rate (2mL/kg/h) is usually sufficient tomeet the caloric requirements of an anesthetizedinfant while avoiding both the hyper- and hypo-glycemia that can be detrimental to neurologicoutcome following deep hypothermic circulatoryarrest (DHCA). These dextrose infusions should bediscontinued prior to commencement of CPB asCPB generally produces mild hyperglycemia. Somepatients receive nutritional support as part of med-ical stabilization prior to surgery. High calorie totalparenteral nutrition and intralipid therapy shouldbe discontinued and replaced with a 10% dex-trose infusion several hours prior to transport to
the operating room. Continued administration ofthese high calorie infusions makes intraoperativeserum glucose management problematic. In thesepatients, higher dextrose infusion rates may benecessary pre-CPB to avoid rebound hypoglycemia.
Preoperative medicationsPremedication prior to induction can be used tofacilitate a number of objectives. In older chil-dren it can be used to alleviate anxiety prior toan IV or inhalation induction. In younger children,premedication can ease separation of the child fromthe parents. In infants, judicious premedicationalone, or in combination with inhaled nitrous oxidecan greatly simplify placement of an IV catheter.One must always consider how stressful it is to par-ents to see their child being taken to the operatingroom crying or upset.Current induction techniques do not justify rou-
tine administration of atropine or glycopyrrolateeither IV or intramuscularly (IM) as a premedi-cant. Midazolam 1.0mg/kg (20mg as a maximumdose) orally in infants and younger children whohave not had prior cardiac surgery is useful. Inpatients who have undergone previous operativeprocedures midazolam alone may be insufficient.These patients are remarkably tolerant to midazo-lam as the result of either heightened anxiety orprevious intra- and postoperative exposure to ben-zodiazepines. Oral ketamine (3–5mg/kg for infants,5–10mg/kg for children>1 year old) can be given inconjunction with the midazolam to these patients.In circumstances in which the child will not takeoral medication the IM route can be used. Ketamine2–3mg/kg and glycopyrrolate (8–10µg/kg) aloneor in combination with midazolam 0.1mg/kg isappropriate.Age-appropriate premedication dosages are out-
lined in Table 6.6. Premedication requires individu-alization of dosage to avoid respiratory depression.Lower doses are best used for smaller children andchildren in congestive heart failure. Premedicationshould always be administered and assessed in thecontinuous presence of the anesthesiologist. Olderchildren may opt for placement of an IV.Digoxin, diuretics, and angiotensin-converting
enzyme (ACE) inhibitors are generally withheld

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 188 — #22
188 Chapter 6
Table 6.6 Premedication guidelines.
Age Medication
0–6months NoneorMidazolam 0.5–1.0mg/kg POorMidazolam 0.5–1.0mg/kg POKetamine 3–5mg/kg
6–12months NoneorMidazolam 0.5–1.0mg/kg POorMidazolam 0.5–1.0mg/kg POKetamine 3–5mg/kg
>12months Midazolam 0.5–1.0mg/kg POorMidazolam 0.5–1.0mg/kg POKetamine 5–10mg/kgorPentobarbital 4mg/kg POMeperidine 3mg/kgorMidazolam 0.5–1.0mg/kg POMeperidine 3mg/kgorKetamine 3mg/kgMidazolam 0.1mg/kg IMGlycopyrrolate 8–10µg/kg
IM, intramuscular; PO, by mouth.
the morning of surgery. ACE inhibitors exacerbatehypotension occurring with anesthetic induction.Inotrope and prostaglandin infusions are continuedinto the operative period for critically ill neonatesand children.
MonitoringIf the infant or child is awake or minimally sedated,application of multiple monitors can prevent asmooth induction, even for an initially calm patient.Minimizing stimulation, including distracting dis-cussion in the operating room, will avoid dis-turbing the child. Ideally, preinduction monitoringshould include a noninvasive automated bloodpressure cuff, ECG, pulse oximeter, and an end-tidalcarbon dioxide monitor. In some cases, a pulse
oximeter and an ECG may be all that is practicalin the early stages of induction. Other monitors arethen quickly added as induction progresses.
ECG and blood pressureA 5-lead ECG with leads II and V5 displayed allowsrhythm and ischemia monitoring. Intra-arterialaccess is obtained following induction, howevermany neonates who have been medically stabi-lized in the intensive care unit (ICU) preoperativelywill have an arterial catheter in place. Generally,percutaneous arterial access can be accomplishedin even the smallest neonates. Radial and femoralarteries are the sites most commonly utilized. Poste-rior tibial and dorsalis pedis arteries may be usedas well; however these sites often do not reflectcentral aortic pressure during and immediately fol-lowing hypothermic CPB in neonates and infants.Brachial arteries are not used given the high riskof distal limb ischemia. Consideration is given toany previous or proposed surgical procedure whichmay compromise the reliability of ipsilateral upperextremity intra-arterial pressuremonitoring such asa Blalock–Taussig shunt, modified Blalock–Taussigshunt, subclavian artery patch repair of aorticcoarctation, or sacrifice of an aberrant subclavianartery. Previous catheterization procedures particu-larly those of an interventional nature may resultin femoral or iliac artery occlusion. Occasionally,surgical access to a peripheral artery is necessary.Umbilical artery catheters may be used intra-
operatively but are generally replaced with aperipheral arterial catheter and removed postop-eratively. Blood pressure monitoring consists ofan intra-arterial catheter as well as upper andlower extremity noninvasive blood pressure cuffs.This arrangement allows detection of residualcoarctation or aortic arch/isthmus obstruction viacomparison of upper and lower extremity bloodpressures.
Systemic oxygen saturationOxygen saturation (SaO2) monitoring is accom-plished with pulse oximeter probes on both anupper and a lower extremity; these can be placedin pre- and post-ductal locations if the physiologywarrants.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 189 — #23
Congenital Heart Disease 189
End-tidal carbon dioxideEnd-tidal carbon dioxide (ETCO2)monitoring is rou-tinely employed with the caveat that the differencebetween PaCO2 and ETCO2 will vary as physio-logic dead space varies and that in some circum-stances the difference may be large (>10–15 torr).Any acute reduction in pulmonary blood flow(decreased cardiac output, pulmonary embolus,increased physiologic intracardiac R–L shunting)will increase this gradient. In patients with singleventricle physiology (most commonly those withHLHS or truncus arteriosus) with high QP:QS priorto initiation of CPB, the right PA may be partially,or completely, occluded by the surgeon to mechan-ically limit pulmonary blood flow. This maneuverdramatically increases physiologic dead space andETCO2 will vastly underestimate PaCO2.
Central venous pressure (CVP)Percutaneous central venous access offers numer-ous advantages and can be reliably obtained evenin small neonates. The use of ultrasound bothreal-time and off-line has helped improve the suc-cessful placement rate to 90–95% in neonates.The preferred access sites are the internal jugularand femoral veins. Four-French 5 cm double lumencatheters are available for use in neonates andinfants, 5-French 5 cm double lumen catheters areavailable for use in young children and 6–9-Frenchcatheters are available for use in older children. Pre-operative use of PA catheters for pediatric patients isuncommon. In patients where postoperative assess-ment of PAP is important the surgeon may chooseto place a transthoracic PA catheter.Central venous access is not without risks par-
ticularly in neonates and infants and therefore thedecision to place a percutaneous central venouscatheter must involve consideration of the relativerisks and benefits. In particular, the risk of inter-nal jugular or SVC thrombosis must be consideredas this complication can be devastating in patientswho are to be staged to a superior cavopulmonaryconnection. The relative risk and benefits of centralvenous cannulation are outlined in Table 6.7. Therisk of thrombosis and infection can be reduced bymaintaining a heparin infusion (2units/h) throughthe central line lumens postoperatively and by
Table 6.7 Advantages and disadvantages of centralvenous pressure monitoring in neonates, infants andchildren.
Advantages• Central venous pressure monitoring• Infusion site for vasoactive and inotropic agents• Infusion site for blood products and intravascularvolume replacement• Sampling of SVC blood for measurement of SVCoxygenation saturation to determine the adequacy ofcardiac output and to determine QP:QS (internal jugular)• Cardiac rhythm analysis (detection of cannon A wavesmay accompany loss of atrial-ventricular synchrony)• Detection of inadequate SVC drainage leading tocerebral venous hypertension during CPB (internal jugular)
Disadvantages• Pneumothorax (internal jugular)• Hematoma with vascular or trachealcompression/displacement• Thoracic duct injury (left internal jugular)• Air embolus• Internal jugular and/or SVC thrombosis• Femoral vein thrombosis• Infection
CPB, cardiopulmonary bypass; SVC, superior vena cava.
removing the lines as soon as possible (typically1–2 days).In some institutions neonates and infants are
managed prior to CPB without central venous lines.Transthoracic intracardiac lines (RA, LA, PA) placedby the surgeon prior to termination of CPB can beused for pressure monitoring, infusion of vasoactiveand inotropic agents, and blood product and volumereplacement. In older children particularly thoseundergoing reoperation with adhesion of the aortaor of the RV to PA conduit to the sternum largebore central venous catheters are used in conjunc-tion with a rapid infusion system. In these chil-dren, transthoracic intracardiac lines while suitablefor pressure monitoring and infusion of drugs areinsufficient for rapid volume replacement.
TemperatureRectal, esophageal and tympanic membrane tem-peratures are monitored for all CPB cases.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 190 — #24
190 Chapter 6
Rectal temperature is considered a peripheral tem-perature site and equilibration of rectal tempera-ture with tympanic and esophageal temperatureserves as the best index of homogenous somaticcooling and rewarming. Rectal temperature lagsbehind esophageal and tympanic membrane tem-perature during both cooling and rewarming. Bothesophageal and tympanic membrane are core tem-perature monitoring sites and temperature changesat these sites generally mirror brain temperaturechanges. Even so, esophageal and tympanic mem-brane temperatures may over- or under-estimatebrain temperature by asmuch as 5C during coolingand rewarming. This observation underscores theimportance of providing an adequately long periodof core cooling prior to commencement of low-flow CPB or DHCA. The likelihood that target braintemperature (15–18C) will be reached is greatlyincreased if core cooling is utilized to bring tym-panic, esophageal, and rectal temperatures to thistarget temperature.
Near infra-red spectroscopyThis is an evolving technology that holds promise asa real-time, on-line monitor of cerebral tissue oxy-genation. All commercially available NIRS devicesutilize continuous wave (cwNIRS) reflectance tech-nology. With this technology the transmission anddetection optodes are placed a few centimeters(3–6 cm) apart on the same side of the head. Thereare two closely placed (1–2 cm apart) detectionoptodes. The more proximal optode receives light,which passes primarily through extracranial tissue(skin, bone) while the distal optode receives light,which also passes through brain tissue. The dif-ference between the two signals represents lightpassing through brain tissue.Near infra-red spectroscopy (NIRS) technology
is particularly suited to analysis of cerebral tissueoxygenation because wavelengths of light in thenear infra-red range (650–900nm) contain photonscapable of penetrating tissue far enough to reachthe cerebral cortex and because the peak absorp-tion spectra of the chromophores best suited toreflect tissue oxygenation – oxyhemoglobin (HbO2),deoxyhemoglobin (Hb), and oxidized cytochromeaa3 (CytOx) reside in this wavelength range.
Cerebral oxygen saturation (SCO2) as measuredby NIRS is the combined oxygen saturation of anuncertain mix of arterioles, capillaries, and venules.Commercially available NIRS monitors assume thatSCO2 represents contributions of cerebral arterialand venous blood in a ratio of 25:75 with thecontribution of capillary blood felt to be negli-gible. Traditional pulse oximetry differs in thisrespect from NIRS because it is capable of isolatingand measuring the arteriole component by gatingmeasurements to pulsatility.Investigations utilizing NIRS devices in neonates
and infants are limited and both normal and criticalvalues for cerebral oxygenation have yet to be deter-mined. Nonetheless, it is clear that the technologyhas an emerging role in detecting cerebral deoxy-genation and in guiding appropriate correctiveinterventions.
Transcranial DopplerThe role of Transcranial Doppler (TCD) monitor-ing in the care of pediatric cardiac surgical patientsis evolving. TCD allows measurement of cerebralblood flow velocity as well as detection of cere-bral microemboli and is a technology ideally suitedto use in neonates and infants. The thin skull ofneonates/infants combined with a low-frequencyultrasonic transducer allows transmission of ultra-sonic energy into brain tissuewith little signal atten-uation. Placement of a 2MHz pulsed wave (PW)Doppler probe over the temporal bone allows theultrasonic signal to be aligned parallel to the prox-imal (M1) segment of the middle cerebral artery(MCA). The ability of PW Doppler to be gated toa specific depth allows determination of blood flowvelocity in the MCA just distal to the takeoff of theanterior cerebral artery. This PW Doppler interro-gation yields a velocity spectrum in the MCA foreach cardiac cycle. Integration of the area underthe velocity spectrum yields the time-velocity inte-gral (TVI) in units of cm/cardiac cycle. The productof vessel TVI and vessel cross-sectional area (unitsof cm2) is flow (units of cm3/cardiac cycle). If itis assumed that MCA cross-sectional area remainsconstant than there is a linear relationship betweenTVI and MCA blood flow. Normal TCD velocity val-ues in various patient subgroups (cyanotic versus

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 191 — #25
Congenital Heart Disease 191
noncyanotic, age, following DHCA), and undervarious CPB conditions (hematocrit, flow, pressure,acid-base status, temperature) have yet to be deter-mined. TCD determination of cerebral blood mayprove useful as a continuous surveillance moni-tor for detection of inadequate flow or obstructedcerebral venous drainage during CPB.Cerebral microemboli produce transient increases
in reflected Doppler energy as compared to thebackground Doppler spectra. These high inten-sity transient signals (HITS) can be counted bythe TCD microprocessor and displayed as micro-embolic events per hour. Due to their higherreflective capacity gaseous emboli can be detectedover a greater distance than particulate emboli andas a result have a higher sample velocity length(the product of emboli duration and velocity).At present, cerebral emboli detection with TCDrequires the constant attention of a skilled observerbecause TCD technology alone lacks sufficient sensi-tivity and specificity to distinguish between gaseousbrain emboli, particulate brain emboli and artifacts.TCD emboli detection is being investigated as tool torefine post-CPB de-airing routines and to reducethe number of cannulation and perfusion relatedinatrogenic embolic events.
Transesophageal echocardiography (TEE)7.5MHz multiplane probes are available for intra-operative use in neonates and infants. These probespossess two-dimensional continuouswave Doppler,PWDoppler, color Doppler, andM-mode capability.Although intraoperative TEE can be performedsafely in the smallest patients (2.5–3.5 kg) cautionmust be exercised as the presence of the probe in theesophagus may cause tracheal and bronchial com-pression with compromise of ventilation, inadver-tent tracheal extubation, right main stem bronchialintubation, esophageal perforation, aortic arch com-pression with loss of distal perfusion, and compres-sion of the LA resulting in left atrial hypertensionor compromise of ventricular filling. In particular,ante- or retroflexion of the probemust be performedwith caution in small patients.Intraoperative TEE has a major impact on
post-CPB decision making (such as return toCPB to repair residual lesions) in approximately
15% of cases when it is used nonselectively.Some institutions use intraoperative TEE selec-tively (approximately 30–40% of CPB cases) incases involving repair of a semilunar or AV valve,complex ventricular outflow tract reconstructions,and for delineation of complicated anatomy thatcannot be completely delineated with transthoracicechocardiography preoperatively. In the subset ofpatients undergoing valve repair and outflow tractreconstruction TEE provides the best immediateassessment of the adequacy of the operative proce-dure and if necessary directs its revision. TEE is nothelpful in assessment of residual arch obstructionfollowing stage 1 repairs as this area is poorly visu-alized. While detection of retained intracardiac airis certainly facilitated by use of intraoperative TEE itremains to be determined what role the technologywill play in improving cardiac de-airing algorithmsparticularly in neonates and infants.The role of TEE in the detection of residual VSDs
following repair of both simple and complex defectsdeserves some discussion. Residual defects <3mmare detectable by TEE but generally do not requireimmediate reoperation as they are hemodynam-ically insignificant. The majority (75%) of thesesmall defects are not present at the time of hospitaldischarge as determined by transthoracic echocar-diography. Residual defects>3mm detected by TEErequire immediate reoperation only if they are asso-ciated with intraoperative hemodynamic (elevatedLAP and/or PAP in the presence of good ventricu-lar function) and oximetric (QP:QS > 1.5:1 or RAto PA oxygen saturation step-up with FiO2 ≤ 0.5)evidence that they are significant.
Airway managementFundamental to the anesthetic care of every patientwith CHD is good airwaymanagement. As discussedpreviously, PVR is altered by changes in ventilatorypattern, PaO2, PaCO2, and pH. Changes in PVRmay dramatically affect shunt magnitude and direc-tion as well as cardiovascular function and stability.Therefore, prompt control of the airway and of ven-tilation will allow optimal pulmonary blood flow ineach patient.Children with high pulmonary blood flow partic-
ularly thosewith interstitial pulmonary edema have

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 192 — #26
192 Chapter 6
surprisingly poor lung compliance necessitatinghigher than expected airway pressures. Care mustbe taken not to insufflate the stomach duringmask ventilation. The relatively large occiput ofinfants and small children will cause the head toflex forward; placement of a small roll under theneck or shoulders will allow the head to remainin the neutral position. Placement of an oral air-way in neonates and infants will greatly facilitatemask ventilation by pulling the large tongue awayfrom the pharyngeal wall. In children<10–12 yearsold nasal endotracheal tubes are generally uti-lized as they provide better stability intra- andpostoperatively. This is particularly important inpatients undergoing intraoperative TEE examina-tions. Denitrogenation of the lungs is recommendedprior to induction in all patients including those inwhom high inspired oxygen concentrations mighttemporarily reduce PVR and compromise systemicperfusion.In patients with high venous pressure and
cyanosis, such as those with a bidirectional Glennshunt or Fontan, nasal endotracheal tubes mustbe passed cautiously as substantial nasal bleedingcan be initiated. Uncuffed endotracheal tubes with aleak at or near 25–30 cm H2O are generally used inchildren <6–8 years of age. Consideration is givento use of a cuffed endotracheal tube in patientswhere poor pulmonary compliance secondary tolung water, chest wall edema, or abdominal disten-tion are anticipated to compromise minute venti-lation. In these patients temporary inflation of thecuff will allow higher airway pressures to be utilizedas needed.
Anesthesia induction andmaintenance
Induction of anesthesiaA variety of induction techniques provide hemo-dynamic stability and improved arterial oxygensaturation in patients with cyanotic heart dis-ease. Sevoflurane, halothane, isoflurane, and fen-tanyl/midazolam do not change QP:QS in childrenwith ASDs and VSDs when cautiously administeredwith 100% oxygen. Sevoflurane (1 MAC) andfentanyl/midazolam have no significant effect on
myocardial function in patients with a single ven-tricle. Halothane (1 and 1.5MAC) depresses cardiacindex and contractilitymore than comparable levelsof sevoflurane, isoflurane, and fentanyl/midazolamanesthesia. In addition, halothane anesthesia mayresult in more severe hypotension and emergentdrug use than sevoflurane anesthesia in childrenwith CHD.No one anesthetic induction technique is suit-
able for all patients with CHD. The patient’s age,cardiopulmonary function, degree of cyanosis, andemotional state all play a role in the selectionof an anesthetic technique. IV administration ofinduction agents clearly affords the greatest flex-ibility in terms of drug selection and drug titra-tion and allows prompt control of the airway. IVinduction is the preferred technique in patientswith severely impaired ventricular systolic functionand in patients with systemic or suprasystemic PApressures.
Mask inductionMask induction of anesthesia can be accomplishedsafely in the subset of children without severecardio-respiratory compromise. However, reducedpulmonary blood flow in cyanotic patients willprolong the length of induction and the intervalduring which the airway is only partially controlled.In addition, in these patients even short intervals ofairway obstruction or hypoventilation may resultin hypoxemia. Sevoflurane and halothane are theinhalation induction agents of choice. Sevofluranecauses less myocardial depression, hypotension andbradycardia than halothane. Isoflurane and particu-larly desflurane are unsuitable agents as their pun-gency causes copious secretions, airway irritation,and laryngospasm.
IV inductionHigh-dose synthetic narcotics in combination withpancuronium (0.1mg/kg) is commonly used for IVinduction in neonates and infants. The vagolytic andsympathomimetic effects of pancuronium coun-teract the vagotonic effect of synthetic opioids.In patients with a low aortic diastolic bloodpressure and a high baseline heart rate vecuronium(0.1mg/kg) or cisatracurium (0.2mg/kg) may be

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 193 — #27
Congenital Heart Disease 193
used without affecting heart rate. In older childrenwith mild to moderately depressed systolic functionlower doses of a synthetic opioid can be used inconjunction with etomidate (0.1–0.3mg/kg).Ketamine (1–2mg/kg) is a useful induction agent.
For patients with both normal and elevated base-line PVR, ketamine causes minimal increases in PApressure as long as the airway and ventilation aresupported. The tachycardia and increase in SVRinduced by ketamine makes it unfavorable for usein patients with systemic outflow tract obstructivelesions.The myocardial depressive and vasodilatory
effects of propofol and thiopental make themunsuitable as induction agents except in patientswith simple shunt lesions in whom cardiovascularfunction is preserved.An alternative to IV induction in patients
with difficult peripheral IV access is IM induc-tion with ketamine (3–5mg/kg), succinylcholine(2–5mg/kg), and glycopyrrolate (8–10µg/kg).Glycopyrrolate is recommended to reduce the air-way secretions associated with ketamine adminis-tration and to prevent the bradycardia that mayaccompany succinylcholine administration. Thedose of succinylcholine per kg body weight ishighest in infants. This technique provides promptinduction and immediate control of the airway withtracheal intubation. It is useful in circumstanceswhere it is anticipated that initial IV access willhave to be obtained via the internal or externaljugular vein or the femoral vein. This techniqueis hampered by the fact that the short dura-tion of action of succinylcholine limits the periodof patient immobility. An alternative techniquecombines IM ketamine (3–5mg/kg), glycopyrrolate(8–10µg/kg), and rocuronium (1.0mg/kg). Thistechnique is hampered by the slightly longer timeinterval until attainment of adequate intubatingconditions with rocuronium.
Maintenance of anesthesiaAnesthesia is generally maintained using a syn-thetic opioid (fentanyl or sufentanil) based tech-nique. These opioids may be used in highdoses (25–100µg/kg fentanyl or 2.5–10.0µg/kgsufentanil) or in low to moderate doses (5–25µg/kg
fentanyl or 0.5–2.5µg/kg sufentanil). In eitherinstance these opioids are used in combination withan inhalation agent (generally isoflurane 0.5–1.0%or sevoflurane 1.0–2.0%) or a benzodiazepine(generally midazolam 0.05–0.10mg/kg). Cautionmust be exercised because the combination of nar-cotics and benzodiazepines is synergistic in reduc-ing SVR. The high-dose technique is particularlyuseful in neonates and infants. Patients in this agegroup presenting for surgery often have signifi-cant ventricular pressure and/or volume overload.In addition, many of these patients have tenuoussubendocardial and systemic perfusion secondaryto runoff into the pulmonary circulation and theassociated low aortic diastolic blood pressure. Giventhe limited contractile reserve available in theimmature myocardium, it is not surprising thatthe myocardial depressive and systemic vasodila-tory effects of inhalation agents and the synergisticvasodilatory effects of benzodiazepines and opioidsmay be poorly tolerated in this patien group.There are unique considerations for maintenance
of anesthesia during CPB. Light anesthesia, par-ticularly during cooling and rewarming, may leadto elevated SVR requiring a reduction in pumpflow rate which compromises both somatic per-fusion and the efficiency of CPB cooling andrewarming. Subclinical shivering due to inade-quate neuromuscular blockade and light anes-thesia are avoidable causes of increased systemicoxygen consumption. Increased systemic oxygenconsumption during CPB will manifest as a lowerthan acceptable venous saturation (<65%) at whatshould be an adequate CPB flow rate for the patient.Furthermore, for amembrane oxygenator at or nearits maximum flow capacity, a low venous satura-tion may result in a lower than acceptable arterialsaturation on CPB.Lower doses of opioid in conjunction with an
inhalation agent or benzodiazepine are suitable forolder patients with better cardiovascular reserve.In fact, carefully selected patients (>1 year old,no pulmonary hypertension, benign past medicalhistory) undergoing simple ASD or VSD closureare candidates for immediate tracheal extubationin the operating room or in the ICU within2–3hours.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 194 — #28
194 Chapter 6
Specific lesions
This section discusses specific lesions and theanesthetic considerations applicable to theirmanagement.
Ventricular septal defects
AnatomyAn opening in the ventricular septum that permitscommunication between the RV and LV is a Ven-tricular septal defects (VSD). Such communicationsmay exist in one or more locations in the ventric-ular septum. As illustrated in Fig. 6.10, VSD can beclassified by their location in the septum.
Subpulmonary or supracristal defectsThese are located in the infundibular septumjust below the aortic valve. Subpulmonary lesionsmay be associated with aortic insufficiency due toa lack of support for the right coronary cusp of theaortic valve and prolapse of this leaflet.
Membranous or perimembranous defectsThese defects comprise approximately 80% of allVSDs and are located in the subaortic region of
Subpulmonary
Membranous
Muscular
AV canaltype
Fig. 6.10 Location of ventricular septal defects.AV, atrioventricular.
the membranous septum. These defects are locatednear or under the septal leaflet of the TV, andcommunicate with the LV just below the aorticvalve. These defects are commonly partially closedby a collection of tricuspid valve and membranousseptal tissue giving an aneurysmal appearance to theseptum.
Conoventricular defectsThese defects involve the same area as peri-membranous defects but have extension anteriorlyand superiorly in the septum.
Inlet or canal-type defectsThese defects involve the posterior septum near theAV valves.
Muscular defectsThese defects are located in the lower trabecularseptum and may appear deceptively small oninspection from the right ventricular aspect ofthe septum due to heavy trabeculation. Thesedefects may be apical, midmuscular, anterior, orposterior.
PhysiologyA VSD is an example of a simple shunt. Thesize of the defect is the critical determinant ofthe magnitude of shunting. If the defect is small(restrictive shunt), flow through the defect will belimited and there will be a large pressure gradientacross the defect. However, as the orifice becomeslarger (approximating the size of the aortic valveorifice) and the pressure gradient across the orificedecreases, the magnitude and direction of shuntingbecomesmore dependent on the relative resistancesof the systemic and pulmonary vascular beds.Because the ratio of PVR to SVR is normally
1:10–1:20, VSDs generally result in production ofa L–R shunt. In some instances, however, the ratioof PVR to SVR may be higher, resulting in near-normal pulmonary blood flow or, in extreme cases,production of a R–L shunt.The infant with a large VSD may have near-
normal pulmonary blood flow as a result of highPVR present at birth. By the second week oflife, PVR begins to fall to near-normal levelsand pulmonary blood flow increases dramatically.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 195 — #29
Congenital Heart Disease 195
Continued decreases in PVR after birth may bedelayed by the elevated LAP that accompaniesincreased pulmonary blood flow.Large VSDs predispose the development of PVOD
during the first few years of life due to expo-sure of the pulmonary vasculature to high flowsand systemic blood pressures. The increases in PVRthat accompany PVODwill ultimately produce bidi-rectional and R–L shunts. Patients with advancedPVOD and markedly increased PVR (Eisenmenger’scomplex) generally are not candidates for VSDclosure, because closure will result in an enormousincrease in RV afterload and RV afterload mis-match. For this reason, large VSDs (Qp:Qs > 2:1) arecorrected early in childhood.An increase in LA volume and pressure parallels
the increase in pulmonary blood flow seen with alarge VSD. The resultant pulmonary venous con-gestion increases the work of breathing, decreasespulmonary compliance, and increases airway resis-tance. All of these factors predispose recurrent pul-monary infections. LV end-diastolic volumes areincreased in parallel with the increase in pulmonaryblood flow. RV end-diastolic volumes are often notincreased because shunting from the LV across theVSD into the RV occurs in systole.In VSDs with a large L–R shunt, systemic blood
flow is maintained at the expense of a large volumeload on both the RV and LV. This limits the capac-ity of the patient to meet increased cardiac outputdemands andmay result in pulmonary and systemicvenous congestion at rest. The timing of surgeryoften is dictated by failure of medical therapy tocontrol this congestion.
Surgical therapyVSDs generally are closed with a patch via a vari-ety of approaches, depending on their location. Toavoid postoperative compromise of a small ventri-cle, with its poor compliance and limited capac-ity for tension development, a ventriculotomy toapproach and correct VSDs should be avoided.Many defects are approachable through the RA andtricuspid valve, aorta, or PA. However, in someinstances, a right ventriculotomy may be the nec-essary approach. Less commonly, assessment andclosure of some muscular defects will require a leftventriculotomy. Because a left ventriculotomy may
seriously compromise myocardial function in theinfant, palliationwith PA bandingmay be preferableto a left ventriculotomy for small infants. Nonoper-ative device closure of muscular VSDs remote fromAV or semilunar valves is possible in the cardiaccatheterization laboratory.
Anesthetic managementThe anesthetic management goals are summarizedin Table 6.8.
Induction and maintenanceAs discussed previously, control of ventilation isthe most reliable way to manipulate PVR. Forinfants and children without congestive heartfailure (CHF), an inhalational induction is welltolerated. For neonates and patients with CHF, anIV induction with fentanyl or sufentanil will pro-vide better hemodynamic stability. In particular,for patients with reactive pulmonary vasculature,high doses of fentanyl and sufentanil will be usefulin blunting increases in PVR associated with sur-gical stimulation. In the absence of IV access, IMketamine and atropine may be used for induction,followed by placement of an IV catheter.
Table 6.8 Anesthetic management goals in patientswith atrial septal defect (ASD), ventricular septal defect(VSD), atrioventricular canal defect (AVC), and patentductus arteriosus (PDA).
1 Maintain heart rate, contractility, and preload tomaintain cardiac output. A reduction in cardiac outputwill compromise systemic perfusion, despite a relativelyhigh pulmonary blood flow2 Avoid decreases in the PVR:SVR ratio. The increase inpulmonary blood flow that accompanies a reducedPVR:SVR ratio necessitates an increase in cardiac output tomaintain systemic blood flow3 Avoid large increases in the PVR:SVR ratio. An increasemay result in production of a right-to-left shunt4 In instances in which a right-to-left shunt exists,ventilatory measures to decrease PVR should be used. Inaddition, SVR must be maintained or increased. Thesemeasures will reduce the magnitude of the right-to-leftshunt
PVR, pulmonary vascular resistance; SVR, systemic vascularresistance.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 196 — #30
196 Chapter 6
Post-CPB managementThe post-CPB management goals are summarizedin Table 6.9.Closure of the VSD will prevent further expo-
sure of the pulmonary vasculature to high flows andpressures. This usually will result in some imme-diate decrease in PA pressures. For patients withsmall defects and patients with large VSDs in whomPVOD has not yet developed, near-normal PA pres-suresmay result. In these patients, inotropic supportpost-CPB is rarely necessary. In fact, reduction inthe large volume load on the LV usually resultsin post-CPB hypertension. Direct vasodilators suchas sodium nitroprusside (0.5–1.0µg/kg/min) orinodilators such as milrinone (0.5–1.0µg/kg/min)may be necessary.Pulmonary artery pressures and PVR will remain
elevated in patients with underlying PVOD. In addi-tion, the pulmonary vasculature of these patientswill remain hyper-responsive to vasoconstricting
Table 6.9 Post-cardiopulmonary bypass (CPB)management goals in patients with atrial septal defect(ASD), ventricular septal defect (VSD), andatrioventricular canal defect (AVC).
1 Maintain heart rate (preferably sinus rhythm) at an
age-appropriate rate. Cardiac output is likely to be more
heart rate dependent in the post-CPB period
2 Reduce PVR through ventilatory interventions. This is
particularly important if PVOD is present
3 Inotropic support of the right ventricle may be
necessary, particularly if PVR is high. In VSD and AVC
patients the left ventricle will no longer contribute to
ejection of blood via the pulmonary artery and the right
ventricle will face a high afterload. Dobutamine
(5–10µg/kg/min) or dopamine (5–10µg/kg/min) is useful
in this instance because both agents provide inotropic
support without increasing PVR. Milrinone
(0.5–1.0µg/kg/min following a loading dose of 50µg/kg)
may also be considered. Milrinone has more direct PVR
reducing effects in addition to inotropic, lusitrophic, and
SVR reducing effects
AVC, atrioventricular canal defect; PVOD, pulmonary
vascular occlusive disease; PVR, pulmonary vascular resis-
tance; SVR, systemic vascular resistance; VSD, ventricular
septal defect.
stimuli due tomedial hypertrophy that accompaniesPVOD. Therapy to reduce PVR in the post-CPBperiod may be necessary for these patients to avoidRV afterload mismatch.Separation from CPB may be complicated by a
variety of surgical problems. Inadequate closure ofthe VSD or the presence of an unrecognized VSDmay prevent separation from CPB. Assessment ofthe presence and location of such defects in theoperating room can be accomplished with TEE. Inaddition, tricuspid valve damage due to a difficulttransatrial approach may produce tricuspid regur-gitation (TR). Patch closure of the VSD may createsubaortic or subpulmonic obstruction. Because theAV node and His bundle are often near the areawhere the surgeon is working, transient heart blockmay occur. Temporary epicardial A–V sequentialpacing may be necessary to terminate CPB.
Atrial septal defect
AnatomyStrictly speaking an atrial septal defect (ASD) is acommunication between the LA and RA due to adefect in the intra-atrial septum (IAS). The IAS con-sists of a central membranous portion and a thickerinferior and superior fatty limbus. The central mem-branous portion is formed by tissue of the septumprimum ultimately forming the fossa ovalis. Thismembrane lies posterior to the superior aspect ofthe fatty limbus.ASDs, like VSDs, are classified by their location.
Figure 6.11 illustrates the anatomy of ASDs. Thereare four morphological types of ASDs: (i) ostiumsecundum defects; (ii) ostium primum defects;(iii) inferior and superior sinus venosus defects; and(iv) coronary sinus (CS) defects. Although they areclassified as ASDs, sinus venosus and CS defects arenot truly defects in the IAS.
Ostium secundum ASDThese defects comprise 80% of ASDs. While a PFOresults from incomplete fusion of an intact fossaovalis membrane with the superior aspect of thefatty limbus, an ostium secundum ASD is the resultof actual deficiencies in the membrane (septumprimum) of the fossa ovalis.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 197 — #31
Congenital Heart Disease 197
Sinusvenosusdefect
ASD 1°
ASD 2°
Fig. 6.11 Location of atrial septal defects (ASDs).ASD 1 = primum ASD; ASD 2 = secundum ASD.Superior and inferior sinus venous defects are shown.
Ostium primum ASDIsolated ostium primum ASDs, also know as par-tial AV canal defects develop when partial fusionof the endocardial cushions separates the two AVvalves and closes the ventricular septal communi-cation, but fails to close the ostium primum. Thisdefect occurs outside the confines of the fossa ovalisinferiorly at the level of the AV valves. The isolatedostium primum defect extends from the inferior IASfatty limbus, to the crest of the IVS. A characteristicfinding of this lesion is insertion of the septal por-tions of both AV valves on the IVS at the same level.Normally insertion of the TV to the IVS is inferior tothe mitral valve (MV), producing the ventriculoa-trial septum (VAS) that separates the RA from theLV. Isolated ostium primum defects are commonlyassociated with a cleft anteriorMV leaflet andmitralregurgitation (MR) resulting from partial fusion ofthe leftward portions of the antero-superior andinfero-posterior bridging leaflets that normally fuseto form the anterior MV leaflet.
Sinus venous defectsThese defects are located either superiorly at thejunction of the RA and the SVC, or inferiorly at
the junction of the RA and the IVC. Both defects arelocated posterior to the fossa ovalis. Superior defectscomprise the majority and inferior defects are rare.These defects are believed to result from a deficiencyin the common wall that normally separates theright upper pulmonary vein/LA junction from theRA/SVC junction and the right lower pulmonaryvein/LA junction from the RA/IVC junction, ratherthan a defect in the IAS or a change in the positionof the pulmonary veins per se. Unroofing of the pul-monary vein (located posteriorly) permits drainageof the LA directly in the SVC or IVC (located ante-riorly). Intra-atrial communication occurs at thelevel of the pulmonary vein/LA junction rather thanthrough an IAS defect.Both types are associated with partially anoma-
lous pulmonary venous return (PAPVR). In the caseof the superior defect, anomalous drainage of theright upper pulmonary vein into the SVC/RA junc-tion is the most common finding. In the case ofthe inferior defect Scimitar syndrome (anomalousdrainage of the right upper and lower pulmonaryveins to the IVC/RA junction, aortopulmonary col-laterals to the right lower lobe, and hypoplasia ofthe right lung) can be seen.
CS defectUnroofing of the CS (posterior) allows direct com-munication with the LA (anterior). At its entryin the RA, the CS orifice becomes the connectionbetween the LA and RA. CS defects are commonlyassociated with a persistent left superior vena cava(LSVC) draining to a large dilated CS.
PhysiologyAn ASD is a simple shunt. A small, restrictivedefect will allow minimal shunt flow. A large defect(at least 1mm in diameter), is unrestrictive and theatria act like a single chamberwith shuntmagnitudeand direction dependent on the relative resistancesof the pulmonary and systemic vascular beds. Afterthe high PVR present after birth declines, a L–Rshunt occurs because:• PVR is 1/10–1/20 that of SVR.• Increased pulmonary blood flow increasesLAP. This favors flow of blood from the LA intothe RA.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 198 — #32
198 Chapter 6
• RV compliance is greater than LV compliance.This also favors flow of blood from the left tothe RA.A large defect will greatly increase pulmonary
blood flow however, unlike a VSD, systemic pres-sures are not transmitted to the pulmonary vascu-lature. In fact, PAP may remain normal for manyyears due to the distensibility of the pulmonaryarteries. In contrast to a patient with VSD, the onsetof PVOD may not occur until the third or fourthdecade of life for a patient with ASD. Finally, a largeASD imposes a large volume load on the LA, RA,and RV. RV volume overload (RVVO) is typicallyreported on echocardiograms in patients with ASD.
Surgical therapySome small ostium secundum ASDs can be pri-marily closed; whereas larger defects are patched,usually with pericardium. An alternative is non-operative device closure of secundum ASDs in thecardiac catheterization laboratory. Primum ASDsgenerally require patch closure and suture closureof the anterior leaflet mitral cleft. Sinus venousdefects without PAPVR can be closed primarily witha patch.An alternative procedure is performed when the
pulmonary vein(s) anomalously enter the SVC. TheSVC is transected above the origin of the anoma-lous vein(s). The proximal end of the SVC is oversewn, and the SVC orifice is directed across thedefect into the LAwith a pericardial patch. The distalend of the SVC is then anastomosed end-to-end tothe roof of the RA appendage recreating SVC to RAcontinuity.CS defects are treated as follows:• In the absence of a persistent LSVC draining to theCS, a CS defect is treated by oversewing the orificeof the CS and allowing CS blood to drain to the LA(a very small physiologic right-to left shunt).• In the presence of a persistent LSVC draining tothe CS in which the LSVC is connected to the rightSVC by the innominate vein the LSVC can be ligatedbelow the innominate vein and the CS over sewn.• In the presence of a persistent LSVC draining tothe CS in which the LSVC is not connected to theright SVC by the innominate vein the CS defectmust be closed with a patch from the LA. Thisisolates the LA from the LSVC blood and directs
LSVC blood thru through the orifice of the CS intothe RA.
Anesthetic managementThe anesthetic management goals are summarizedin Table 6.8.
Induction and maintenanceMost children with ASDs have excellent cardiacreserve and will tolerate an inhalation induc-tion without problems. Good airway manage-ment is necessary to allow manipulation of PVRand prevent reversal of L–R shunting. The pres-ence of an enlarged atrium may predispose atrialdysrhythmias; these usually are well tolerated.For children with an isolated ASD and no
PVOD early extubation in the ICU or extuba-tion in the operating room after repair is possible.An inhalational induction with sevoflurane fol-lowed by placement of an IV and administration ofpancuronium 0.1mg/kg and fentanyl 10–15µg/kgcan be used. An alternative following IV place-ment is thiopental, propofol, or etomidate in con-junction with pancuronium and a remifentanilinfusion (0.3–1.0µg/kg/min). In either case, anes-thesia is maintained with isoflurane (0.5–1.0%) orsevoflurane (1.0–2.0%) supplementation. Caudalmorphine (70µg/kg in 5–10mL of preservative-free saline) can be administered after induc-tion. A vaporizer on the CPB circuit can provideanesthesia during CPB.
Post-CPB managementThe post-CPB management goals are summarizedin Table 6.9.Separation from CPB usually is not problematic.
In primum defects, there is the possibility of heartblock, as the patch must be sutured to the crestof the IVS. In addition, the possibility of residualmitral regurgitation exists. If partial anomalous pul-monary venous drainage is unrecognized duringsinus venous defect closure, a residual L–R shuntmay exist after repair. Intraoperative TEE can beused to detect this defect. In the rare patient withPVOD, the pulmonary vasculature is likely to behyper-reactive in the post-CPB period. Therefore,it is necessary to use ventilatory measures to reducepost-CPB PVR. These manipulations will prevent

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 199 — #33
Congenital Heart Disease 199
right ventricular dysfunction secondary to increasedafterload.
Atrioventricular canal defects
AnatomyEmbryologically, there are four endocardial cush-ions that contribute to the development of the lowerostium primum portion of the atrial septum and theupper, posterior inlet portion of the IVS where theAV valves insert. The cushions also contribute tothe tissue that forms the septal leaflets of the mitraland tricuspid valves. Therefore, cushion defects, oratrioventricular canal (AVC) defects, include abnor-malities in all these structures. The terminology ofthese lesions can be confusing and is summarized(Figs 6.12 and 6.13a–c) as follows:• Partial AVC. This is an ostium primum ASD inassociation with a cleft mitral valve. There are twoseparate AV valve (mitral and tricuspid) annuli.No inlet VSD is present.• Transitional AVC. This is an ostium primum ASD,commonAV valve orifice, common antero-superiorand postero-inferior bridging leaflets with densechordal attachments to the crest of the IVS creatingfunctionally separate mitral and tricuspid valves.There is a very small or absent inlet VSD.
Atrial septum
Atrial partof CAVC
Rt vent
Parts ofcommonAV valve
Ventricularpart of CAVC
IVC
SVC
Fig. 6.12 Right ventricle opened to reveal componentsof a common atrioventricular canal defect. AV,atrioventricular; CAVC, common atrioventricular canal;IVC, inferior vena cava; Rt vent, right ventricle; SVC,superior vena cava.
• Complete AVC (CAVC). This is an ostium primumASD, common AV valve orifice, common anterio-superior and posterio-inferior bridging leaflets withvarying chordal attachments to the crest of theIVS. There is a moderate to large inlet VSD. Thetype of chordal attachments are summarized asfollows:• Rastelli A. The anterio-superior bridging leafletis effectively divided into left (mitral) and right(tricuspid) anterio-superior leaflets by choralattachments to the crest of IVS. There is usuallyattachment of the postero-inferior leaflets to thecrest of the IVS aswell. Themajority (70%) of CAVCare of this type.• Rastelli B. There are chordal attachments from theright side of the IVS (RV septal papillary muscle)to left side of the anterio-superior bridging leaflet.
RLL(a) (b) (c)
LLL
LILLSL
RSL RIL
RLL
LLL
LILLSL
RSL RIL
RLL
LLL
LIL
SL
RIL
Fig. 6.13 Types of complete atrioventricular canal seenfrom above. (a) Rastelli type A – the most frequent formof common atrioventricular canal (CAVC). The superior(anterior) bridging leaflet is effectively divided into mitral(LSL) and tricuspid (RSL) portions, both of which areattached to the crest of the ventricular septum. Thetricuspid portion represents the true anterior tricuspidvalve leaflet. (b) Rastelli type B – the least frequent formof CAVC. The superior (anterior) bridging leaflet iseffectively undivided but there are choral attachmentsfrom a right ventricle (RV) septal papillary muscle to theleft side of the leaflet. (c) Rastelli type C – the form ofCAVC most commonly associated with other majorcardiac anomalies (such as tetraology of Fallot). Thesuperior (anterior) bridging leaflet is clearly undividedwith no chordal attachments to the ventricular septum.LIL and RIL, left and right inferior (posterior) leaflets;LLL and RLL, left and right lateral leaflets; LSL and RSL,left and right superior (anterior) leaflets; SL, superior(anterior) bridging leaflet. (From Jacobs JP, et al.Congenital heart surgery nomenclature and databaseproject; atrioventricular canal defect. Ann Thorac Surg2000;69:S37, with permission.)

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 200 — #34
200 Chapter 6
There are no choral attachments to the crest ofthe IVS.• Rastelli C. There are no chordal attachments ofthe anterio-superior bridging leaflet to any portionof the IVS; there is usually an attachment to a RVfreewall papillarymuscle. This createswhat appearsto be a free-floating common AV valve. This typeis seen most commonly in conjunction with otherlesion such as TOF.
PhysiologyThese defects can result in communication betweenall four heart chambers as well as in abnormalities ofthe mitral and tricuspid valves. Because the orificebetween the four chambers is large, these lesionstend to produce dependent simple shunts. As withlarge VSDs, this results in: (i) production of a largeL–R shunt; (ii) increased pulmonary blood flow;(iii) transmission of systemic pressures to theRV andpulmonary arteries; and (iv) volume overloading ofthe RV and LV.As with large VSDs, CAVC defects predispose the
early development of PVOD. Advanced PVOD mayincrease the PVR:SVR ratio such that a bidirectionalor R–L shunt develops. This is a particular concernfor patients with trisomy 21. CAVC defects are com-mon in these patients, who are particularly prone toearly development of PVOD. In some CAVC defects,the presence of severe mitral insufficiency resultsin regurgitation of left ventricular blood directlyinto the RA (LV–RA shunt). This increases the L–Rshunt. In addition,mitral regurgitation increases thevolume work of the LV.
Surgical therapyRepair of these defects involves:• Septation of the common AV valve tissue intotwo separate competent, nonstenotic tricuspid andmitral valves.• Closure of the ostium primum ASD.• Closure of the inlet VSD.This can usually be accomplished using a one-
patch technique wherein a single patch is used toclose both the VSD and ASD and the reconstructedAV valves are re-suspended by sutures to the patch.When the VSD is large and extends to other areasof the septum (as in TOF) two patches (atrial and
ventricular) may be necessary. When the inlet VSDcomponent is small the AV valve tissue can besutured down to the crest of the ventricular septumessentially closing the VSD. A patch is then suturedto the crest of the ventricular septum and is used toclose the ASD.
Anesthetic managementThe anesthetic management goals are summarizedin Table 6.8.
Induction and maintenanceAnesthetic management is similar to that for largeVSDs. However, the child with CAVC also mayhave severe mitral regurgitation and a highly reac-tive pulmonary vasculature. Because control ofventilation is the most reliable way to manipu-late PVR, prompt and reliable control of the air-way at induction is important. The goal shouldbe to use a reduced FiO2 and to maintain PaCO2at 35–40mmHg. Inhalational induction should bereserved for infants and children with small defects,no mitral regurgitation, and no PVOD. Cardiacreserve often is limited or exhausted in patientswithlarge shunts and high pulmonary blood flow.More-over, the additional volume load imposed on theLV by mitral regurgitation will further limit cardiacreserve.An IV induction and maintenance with fentanyl
or sufentanil will provide better hemodynamic sta-bility. In particular, for patients with reactive pul-monary vasculature, high doses of fentanyl andsufentanil will be useful in blunting increases inPVR associated with surgical stimulation. In addi-tion, high doses of fentanyl or sufentanil will bluntstimulation-induced increases in SVR, which willincrease the mitral regurgitant fraction.
Post-CPB managementThe post-CPB management goals are summarizedin Table 6.9.Closure of the defects will prevent further expo-
sure of the pulmonary vasculature to high bloodflows and pressures. This usually will result in someimmediate decrease in PA pressures. In patientswith small defects and patients with large defects inwhom PVOD has not yet developed, near-normal

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 201 — #35
Congenital Heart Disease 201
PA pressures may result. However, PA pressuresand PVR will remain elevated in patients withunderlying PVOD. In addition, the pulmonary vas-culature of these patients (especially patients withtrisomy 21) will remain hyper-responsive to vaso-constricting stimuli due to medial hypertrophy thataccompanies PVOD. Therapy to reduce PVR in thepost-CPB periodmay be necessary for these patientsto avoid RV afterload mismatch.Separation from CPB may be complicated by a
variety of surgical problems. Inadequate closure ofthe defects or persistent mitral regurgitation mayprevent separation from CPB. Assessment of thepresence and location of such defects in the ORcan be accomplishedwith TEE. The presence of largeV waves on the pressure trace obtained from a leftatrial cathetermay be helpful in assessing the degreeof mitral regurgitation, whereas TEE will providedefinite information. Occasionally, patch placementreduces the left ventricular chamber size and limitsstroke volume. Because the AV node is near thearea of patch placement, heart block may occur.Temporary epicardial AV sequential pacing may benecessary to terminate CPB.
Patent ductus arteriosus
AnatomyA patent ductus arteriosus (PDA) connects themainpulmonary trunk near the origin of the left PAwith the proximal descending aorta just distal to theorigin of the left subclavian artery (Fig. 6.14).
PhysiologyA PDA is a simple shunt. When the PDA is large,there is little or no pressure gradient across the ductand shunting becomes dependent on the ratio ofPVR to SVR. Initially, the high PVR present afterbirth tends to limit the shunt magnitude of eventhe largest PDAs until PVR begins to decrease. AsPVR decreases a L–R shunt with increased pul-monary blood flow develops. In order for systemicblood flow to be maintained left ventricular outputmust increase and a volume load must be imposedon the LV. The increased pulmonary blood flowincreases pulmonary venous return and LAP. Thesefactors may, in turn, increase PVR and the work of
Asc Ao
Pulmonaryartery
Patent ductusarteriosus
Desc Ao
Fig. 6.14 Patent ductus arteriosus. Asc Ao, ascendingaorta; Desc Ao, descending aorta.
breathing. Finally, runoff of blood from the prox-imal aorta into the PA tends to compromise distalorgan perfusion and decreases aortic diastolic bloodpressure reducing CPP.
Surgical therapyClosure of the PDA was the first “cardiac” oper-ation, successfully performed by Robert Gross atChildren’s Hospital Boston in 1938. The usual sur-gical approach is via a left thoracotomy or viavideo-assisted thoracoscopic surgery (VATS). CPB isnot used. The ductus is either ligated or ligated andtransected. The left PA, left main stem bronchus, ordescending aorta is at risk to be inadvertently ligatedif the PDA is misidentified. Injury to the recurrentlaryngeal nerve is also possible.Closure of a PDA currently is being accomplished
in some cardiac catheterization laboratories usingocclusion devices. An anesthetic often is necessaryfor this procedure, because catheter insertion ispainful and placement of the device is impossible ina moving child. Dislodgement of the device down-stream into the PA or aorta may occur and requiresurgical intervention.
Anesthetic managementThe anesthetic management goals are summarizedin Table 6.8. There are a few additional consid-erations. Surgical retraction of the left lung may

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 202 — #36
202 Chapter 6
necessitate high inspired oxygen concentrationsto prevent hypoxemia. Blood pressure should bemonitored in an upper and lower extremity. Theright arm is preferable to the left arm because thesurgeon may have to place a clamp on the aorta ifcontrol of the aortic end of the PDA is lost during dis-section or ligation. In patientswith a large L–R shuntthere will be an increase in aortic diastolic bloodpressure following ligation due to cessation of runoffof blood into the pulmonary circulation. An upperand lower extremity blood pressure should be com-pared following ligation to assure that a coarctationhas not been created.
Induction and maintenanceMost patients presenting for PDA ligation are pre-mature infants with respiratory distress syndrome.Age and the likelihood that CHF exists make thesepatients poor candidates for inhalational anesthesia.A technique using high-dose fentanyl or sufen-tanil in combination with a benzodiazepine or lowinspired concentration of inhalation agent is welltolerated.For older children with an isolated PDA and no
PVOD, early extubation or extubation in the oper-ating room after ligation is possible. In this agegroup thoracotomy can be avoided using VATS. Aninhalational induction with halothane or sevoflu-rane followed by placement of an IV and admin-istration of pancuronium 0.1mg/kg and fentanyl10–15µg/kg. Alternatively a remifentanil infusion(0.5–1.0 g/kg/min) can be utilized. Anesthesiais supplemented with isoflurane (0.5–1.0%) orsevoflurane (1.0–2.0%) supplementation. Caudalmorphine (70µg/kg in 5–10mL of preservative-free saline) can be administered after induction forpostoperative analgesia if a thoractomy is used.
Coarctation of the aorta
AnatomyCoarctation of the aorta is a focal narrowing of theaorta and represents 6–8% of all congenital cardiacdefects. Coarctation of the aorta is more commonlyfound in males and is the most common lesionin patients with Turner syndrome. Almost half ofall cases have associated cardiac and noncardiac
anomalies. The anatomic pathology is remarkablyconsistent with a discrete posterior shelf or invagi-nation in the aortic wall just opposite of the inser-tion of the DA (juxta-ductal) and distal to theleft subclavian artery. In some instances this shelfmay be circumferential. Longer segment coarcta-tion and coarctation of the abdominal aorta arealso seen.It has been postulated that coarctation develops
as the result of fetal blood flow patterns whichreduce antegrade aortic blood flow with a propor-tionate increase in PA and DA blood flow. It isnot surprising then that coarctation is associatedwith aortic valve stenosis (most commonly bicus-pid aortic valve), with hypoplasia of other left heartstructures such as the mitral valve and LV, and withhypoplasia of the aortic arch. Hypoplasia of the aor-tic isthmus (the region of the aortic arch from theleft subclavian to the DA) is the isolated aortic archlesion most commonly associated with coarctation.VSDs, particularly posterior malalignment VSDsthat cause left ventricular outflow tract (LVOT)obstruction and divert flow from the ascendingaorta into the PA, are also associated with coarc-tation. In contrast, coarctation is virtually neverfound in association with obstructive right heartlesions.
PhysiologyDespite remarkably consistent anatomic pathology,the pathophysiology of coarctation is varied anddepends on the severity of the coarctation and thelocation of associated lesions (Fig. 6.15a,b). Thesevariations in pathophysiology have led to the useof confusing terms such as infantile and adultcoarctation or pre- and post-ductal coarctation,which are of little practical significance. Coarcta-tion of the aorta produces LV pressure overload anda reduction in lower body perfusion. The physio-logic consequences of a coarctation will depend onseveral factors:• The severity of the coarctation.• The extent of bypass afforded by the patent orpartially PDA.• The extent of collateralization to the distalaorta.• The type and severity of associated heart lesions.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 203 — #37
Congenital Heart Disease 203
(a) (b)
Fig. 6.15 Typical appearances of coarctation of theaorta. (a) Coarctation associated with hypoplasia of theaortic isthmus and ductal dependent perfusion of thedescending aorta present at birth. Closure of the ductusarteriosus will likely result in left ventricle (LV) afterloadmismatch with compromise of perfusion and oxygendelivery, and presentation in infancy. (b) Coarctation ofthe aorta in a patient who has tolerated ductal closureand developed extensive collateralization. Extensivefibrosis in the juxta-ductal region in association withgrowth of the native aorta has produced a discretehourglass constriction. Presentation will be as a child oryoung adult.
The DA plays a critical role in pathophysiology.Closure of the DA after birth initially occurs atthe pulmonary end with constriction of the aor-tic orifice normally delayed for several weeks ormonths. Closure of the aortic end of the DA mayabruptly impede flow of blood around the aorticshelf lesion and increase the severity of the lesion(Fig. 6.16a–c). Ductal closuremay also be associatedwith constriction of the aorta at the level of the DApresumably due to the presence of ductal tissue inthis area. When coarctation is severe, distal aorticperfusion will, in part, be supplied with blood fromthe PA via a PDA (Fig. 6.17a–c). This will result indifferential cyanosiswith a higher arterial saturationproximal to the coarctation as compared to distalto the coarctation. When the development of aorticobstruction is gradual, collateral flow to the distalaorta will be established via the intercostal, internalthoracic, subclavian, and scapular arteries.Presentation will be in infancy for all patients
except those capable of tolerating ductal clo-sure without overt hemodynamic compromise.In general, presentation beyond infancy is lim-ited to patients with an isolated coarctation ofmild to moderate severity or to those with rapid
compensatory collateral formation. In these patientsthere is a secondary phase of fibrosis that occursin the first 2–3months of life. As the child grows,the ligamentum arteriosum develops a thick fibrousshelf within the lumen of the aorta.In the presence of severe coarctation, particu-
larly in association with left heart and aortic archhypoplasia, patency of the DA is necessary to pro-vide blood flow to the aorta distal to the coarctation(R–L physiologic shunt). In this ductal dependentphysiology, RV pressures are systemic and femoralpulses are present.Ductal closure in patients with a severe coarc-
tation will result in near loss of distal perfusion.LV dilation from the acute afterload increase, leftatrial hypertension, and pulmonary edema mayensue. The reduction in LV output may be so severethat proximal hypertension will not be present.The infant may present in a profound low cardiacoutput state or following cardiopulmonary arrest. Inthe case of a less severe coarctation, ductal closurewill result in a diminution of distal perfusion andevidence of left atrial hypertension.If an anatomic intracardiac shunt lesion (such
as ASD or VSD) is also present the increasedimpedance to aortic ejection induced by the coarc-tation will enhance physiologic L–R shunting.Reductions in PVR will increase pulmonary bloodflow thereby diverting flow from the distal aorta.Left atrial hypertension will be exacerbated by theincrease in pulmonary blood flow.In all these instances institution of PGE1
(0.05–0.1µg/kg/min) to re-establish ductal andaortic patency can be lifesaving.Mechanical ventila-tory support, inotropic support, and diuretic therapyare usually necessary to stabilize the sickest infantsfollowing administration of PGE1. These patientsoften present with a profound metabolic acidosisand suffer transient renal and hepatic dysfunctionfollowing initial resuscitation.Patients presenting in childhood with coarcta-
tion will not be ductus dependent and will havewell developed collaterals. In addition, they willhave developed the concentric LV hypertrophythat accompanies chronic LV pressure overloadlesions. These patients will have proximal aortichypertension.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 204 — #38
204 Chapter 6
Pulmonaryaorta
Descendingaorta
Phrenic nerve
Vagus nerve
Phrenic nerve
Vagusnerve
(a)
(b)
(c)
Fig. 6.16 Anatomy of coarctation of the aorta involving a small patent ductus arteriosus (PDA). Closure of this PDAwill create a shelf-like invagination of the posterior aortic wall and increase the severity of the coarctation. The repairshown here (a–c) is resection of the coarcted segment, ligation of the PDA, and primary end-to-end reanastomosis ofthe aorta. Clamp placement has compromised flow to the left subclavian artery.
Surgical therapyThree basic types of repair are used for correctionof coarctation of the aorta: reverse subclavian patchangioplasty, synthetic patch angioplasty, and end-to-end anastomosis of the aorta after resection ofthe coarcted segment (see Figs 6.16 and 6.17). Theseprocedures are performed via a left thoracotomy.It is necessary to cross-clamp the aorta to performthese procedures. For older children, partial CPB ora shunt from proximal to distal aorta may be usedif the adequacy of the collateral circulation is inquestion.Presentation as an infant generally leads to
medical stabilization followed by surgical interven-tion. Complete excision of the area of coarcta-tion and surrounding ductal tissue with end-to-endanastomosis is indicated. In the case of coarcta-tion associated with a hypoplastic aortic isthmus
complete excision in conjunction with an extendedend-to-end or end-to-side anastomosis is recom-mended. The descending aorta is anastomosed tothe underside of the aortic arch in an end-to-end orend-to-side fashion.Dacron patch aortoplasty following resection of
the posterior coarctation ridge is associated withlate development of hypertension and aneurysmformation as compared to end-to-end anastomo-sis. Reverse subclavian patch angioplasty is rarelyutilized, as the rate of re-coarctation is high. Inadult patients placement of an interposition graftis usually necessary as there is insufficient mobil-ity of the aorta to allow resection and end-to-endanastomosis.Endovascular stent placement may prove to be
an alternative therapy for treatment of coarctationin older children and adults with results superior

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 205 — #39
Congenital Heart Disease 205
(a)
(b)
(c)
Patent ductusarteriosus
Phrenic nerve
Vagus nerve
Descending aorta
Phrenic nerve
Patent ductsarteriosus
Descending aorta
Vagus nerve
Descending aorta-to-sideaorta anastomosis
Incision, inferiorsurface of arch
Fig. 6.17 Anatomy of coarctation of the aorta involvinga large patent ductus arteriosus (PDA) and severe tubularhypoplasia of the aortic isthmus (arch). A good portion ofthe flow to the distal aorta is supplied from right-to-left(R–L) shunting through the PDA. The repair shown here
(a–c) is resection of ductal tissue and mobilization of thedescending aorta and aortic arch to perform a primaryreanastomosis. This increases the caliber of the aorticarch. Clamp placement has compromised flow to the leftcarotid artery.
to balloon dilation alone. This technique allows forsubsequent percutaneous stent dilations over timeas necessary.The most devastating complication associated
with coarctation repair is the development of para-plegia secondary to spinal cord ischemia. The inci-dence of paraplegia is quite low (0.14–0.40%).Several factors are associated with an increased riskof developing paraplegia: hyperthermia, prolongedaortic cross-clamp time, elevated cerebral spinalfluid (CSF) pressures, low proximal and distal aorticblood pressures, and poorly developed collaterals tothe descending aorta.
Anesthetic management
Goals1 Maintain heart rate, contractility, and preloadto maintain cardiac output. The high afterload
faced by the LV makes it particularly vulnerable toreductions in contractility.2 For neonates and infants with coarctation, con-tinuation of PGE1 (0.01–0.05µg/kg/min) to main-tain ductal patency may be necessary to preventcardiovascular collapse.3 If there is an associated ASD or VSD, reduction inthe PVR:SVR ratio should be avoided. Such reduc-tions will increase pulmonary blood flow and willnecessitate an increase in cardiac output tomaintainsystemic blood flow.4 Avoid increases in SVR. Increased SVR willworsen LV pressure overload, which may causelarge reductions in LV output.5 Cross-clamping of the aortamay produce impres-sive proximal hypertension or LV dysfunction. Thisis less likely in the presence of well-developedcollaterals.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 206 — #40
206 Chapter 6
The arterial line should be in the right arm.No blood pressure will be obtainable in the lowerextremities during cross-clamping. The left arm isan unreliable blood pressure source during clamp-ing because the proximal clamp may occlude orcompromise the origin of the left subclavian artery.This is particularly true if the left subclavian patchtechnique is utilized.
Induction and maintenanceNeonates and infants presenting for coarctationrepair generally are PGE1 dependent with compro-mised distal perfusion and pulmonary congestion.They are not candidates for inhalational anesthesia.Ketamine may worsen hemodynamics by increas-ing SVR and probably should be avoided. A tech-nique using high-dose fentanyl or sufentanil incombination with a benzodiazepine or low inspiredconcentration of an inhalation agent is well tol-erated by these patients. In older children withonly proximal systemic hypertension, IV or inhala-tional techniques are well tolerated. Regardless ofthe technique chosen, it should be appreciated thatproximal blood pressure response to stimulationwill be exaggerated.
Management after cross-clamp removalCross-clamping of the thoracic aorta has beenshown to produce increases in both proximal aor-tic blood pressure and CSF pressure and decreasesin distal aortic blood pressure. Use of sodium nitro-prusside to normalize proximal aortic blood pres-sure results in further increases in CSF pressure andfurther decreases in distal aortic blood pressure. Thiscombination of increased CSF pressure and reducedaortic blood pressure reduces spinal cord bloodperfusion pressure and may place the spinal cordat greater risk for ischemia. Therefore, vasodila-tors should be used cautiously to control extremeproximal hypertension and LV dysfunction.TEE is useful during cross-clamping, particularly
for infants with coexisting cardiac lesions. LV func-tion and the extent of intracardiac shunting can bemonitored. In some instances of severe coarctationin infants, particularly those with proximal tubu-lar hypoplasia, vasodilator therapy may be insuffi-cient to prevent LV dilatation and inotropic supportmay be necessary. Inotropic therapy for patients
with intracardiac shunts may only serve to increaseL–R shunting. Ventilatory control of PVR will becomplicated by the fact that the left lung mustbe retracted for exposure. It is important to knowwhich arch vessels are clamped during the surgicalprocedure. At least one of the carotid arteries mustbe patent for cerebral perfusion (see Figs 6.16 and6.17). The use of NIRS may be helpful in assessingthe adequacy of cerebral blood flow.Removal of the cross-clamp will result in reac-
tive hyperemia in distal tissues with subsequentvasodilation and transient hypotension. Release oflactic acid will increase PaCO2. Volume expansionand hyperventilation just before clamp removaldiminishes these effects. Cross-clamp times forthese repairs are relatively short (<15minutes),which reduces the hemodynamic consequences ofclamp removal.Postoperatively, reboundhypertensionmayoccur
and persist for up to 1 week. Initially this is likelydue an altered baroreceptor response resulting invery high circulating levels of catecholamines play arole. Later, there may be involvement of the renin–angiotensin–aldosterone system. Beta-blockers andvasodilators are used to control this hypertension.Older children without coexisting diseases are
candidates for early extubation using the techniquedescribed for PDA ligation.
Tetralogy of Fallot (TOF)
AnatomyTOF (Figs 6.18 and 6.19a,b) is actually more accu-rately described as TOF with pulmonary stenosis(TOF/PS) to distinguish it fromTOFwith pulmonaryatresia (TOF/PA) and TOF with absent pulmonaryvalve (TOF/APV). TOF is characterized by a VSD,overriding of the aorta, right ventricular hyper-trophy, and pulmonic stenosis (infundibular orsubvalvular, valvular, supravalvular, or a combina-tion). The key malformation is underdevelopmentof the right ventricular infundibulum and displace-ment of the infundibular septum resulting in rightventricular outflow tract stenosis. Patients withTOF have displacement of the infundibular sep-tum in an anterior, superior, and leftward direction.The posterior wall of the right ventricular outflowtract is formed by the infundibular septum and this

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 207 — #41
Congenital Heart Disease 207
Right aorticarch
Subpulmonarystenosis
VSD
AoPA
RA
RVLV
LA
Fig. 6.18 Anatomy in tetralogy of Fallot (TOF). Thefollowing features are notable: malalignment ventricularseptal defect (VSD), overriding aorta (Ao), infundibularpulmonic stenosis, and small pulmonary arteries. Thereis a right aortic arch with mirror image arch vesselbranching as occurs in 25% of patients with TOF. LA, leftatrium; LV, left ventricle; PA, pulmonary artery; RA,right atrium; RV, right ventricle.
RV
(a) (b)
LVMV RV
MPA
MV
LV
Fig. 6.19 (a) Long-axis view of heart illustrating thenormal relationship of the infundibular septum(stippled) and the trabecular septum (striped). (b) Longaxis view of heart in tetralogy of Fallot. Lack ofconnection between infundibular and trabecular septumresults in malalignment ventricular septal defect. Rightventricular outflow tract is narrowed by upward, anteriortilt of infundibular septum. LV, left ventricle; MPA, mainpulmonary artery; MV, mitral valve; RV, right ventricle.
abnormal displacement results in narrowing of theright ventricular outflow tract. In addition, thisdisplacement of the infundibular septum createsa large malalignment VSD with the aorta overrid-ing the intraventricular septum. Abnormalities inthe septal and parietal attachments of the outflowtract further exacerbate the infundibular stenosis(Fig. 6.20a–c). Seventy-five percent of TOF patientswill have both infundibular and valvular stenosis.A small proportion of patients will have multiplemuscular VSDs.The pulmonary valve is almost always bileaflet.
At one end of the spectrum of TOF the pulmonaryvalve may be mildly hypoplastic (reduced annu-lus size) with minimal fusion of the pulmonaryvalve leaflets. At the other end of the spectrumthe pulmonary annulus may be very small withnear fusion of the valve leaflets. In addition, thereare varying degrees of main PA and branch PAhypoplasia.The most common associated lesion, present in
25% of patients is a right aortic arch with mirrorimage arch vessel branching (innominate arterygives rise to left carotid and left subclavian, rightcarotid and right subclavian arise separately).
PhysiologyTOF is a complex shunt in which a communica-tion (VSD) and a partial obstruction to RV outfloware present. In most patients with TOF, there isa fixed and a dynamic component to RV out-flow obstruction. The fixed component is producedby the infundibular, valvular, and supra valvularpulmonary stenoses (SVAS). The dynamic compo-nent (subvalvular PS) is produced by variations inthe caliber of the RV infundibulum.In patients with TOF, the arterial saturation
is a direct reflection of pulmonary blood flow.The typical TOF patient has fixed and variablecomponents that create severe right ventricularoutflow obstruction. This produces a right-to leftshunt and cyanosis. A small subset of TOF patients(“pink tet”) haveminimal obstruction to pulmonaryblood flow at the right ventricular outflow andPA level and may have normal oxygen saturation.Some of these patients have a L–R shunt withincreased pulmonary blood flow and symptomsof CHF.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 208 — #42
208 Chapter 6
Pulmonic valve
Cristasupraventricularis
Tricuspidorifice
Viewed from septum Frontal view
PB
SB
PBPBSBSB PB
SB
RV
VSD
Infundibular chamber
PBSB
RV
Infundibular chamber
VSD
RV
PB SB
RV
PB
SB
(a) (b)
(c)
PBSB
Fig. 6.20 Spectrum of infundibular stenosis producedby abnormalities in septal and parietal bands of cristasupraventricularis. (a) Normal anatomy of cristasupraventricularis. (b) Moderate infundibular stenosisand creation of an infundibular chamber secondary tohypertrophy and anterior, superior displacement of
parietal band. (c) Severe infundibular stenosis withcreation of infundibular chamber secondary tohypertrophy and anterior, superior displacement ofboth septal and parietal bands. PB, parietal band;RV, right ventricle; SB, septal band; VSD, ventricularseptal defect.
Hypoxic or hypercyanotic episodes(“Tet spells”)The occurrence of hypoxic episodes in TOF patientsmay be life-threatening and should be anticipatedin every patient, even those who are not normallycyanotic. Spells occur more frequently in cyanoticpatients with the peak frequency of spells between2 and 3months of age. The onset of spells usuallyprompts urgent surgical intervention, so it is notunusual for the anesthesiologist to care for an infantwho is at great risk for spells during the preoperativeperiod.The etiology of spells is not completely under-
stood, but infundibular spasm or constriction mayplay a role. Crying, defecation, feeding, fever,and awakening all can be precipitating events.
Paroxysmal hyperpnea is the initial finding. There isan increase in rate and depth of respiration, leadingto increasing cyanosis and potential syncope, con-vulsions, or death. During a spell, the infant willappear pale and limp secondary to poor cardiac out-put. Hyperpnea has several deleterious effects inmaintaining and worsening a hypoxic spell. Hyper-pnea increases oxygen consumption through theincreased work of breathing. Hypoxia induces adecrease in SVR, which further increases the R–Lshunt. Hyperpnea also lowers intrathoracic pres-sure and leads to an increase in systemic venousreturn. In the face of infundibular obstruction, thisresults in an increased RV preload and an increasein the R–L shunt. Thus, episodes seem to be asso-ciated with events that increase oxygen demand

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 209 — #43
Congenital Heart Disease 209
while simultaneous decreases in Pao2 and pH andan increase in Paco2 are occurring. Treatment of a“Tet spell” includes the following:• Administration of 100% oxygen.• Compression of the femoral arteries or placingthe patient in a knee–chest position transientlyincreases SVR and reduces the R–L shunt. Manualcompression of the abdominal aorta is particularlyeffective for the anesthetized patient. After the chestis open, the surgeon can manually compress theascending aorta to increase impedance to ejectionthrough the LV.• Administration of morphine sulfate(0.05–0.10mg/kg), which sedates the patient andmay have a depressant effect on respiratory driveand hyperpnea.• Administration of 15–30mL/kg of a crystalloidsolution. Enhancing preloadwill increase heart size,which may increase the diameter of the RV outflowtract.• Administration of sodium bicarbonate to treat thesevere metabolic acidosis that occur during a spell.Correction of the metabolic acidosis will normalizeSVR and reduce hyperpnea. Bicarbonate adminis-tration (1–2mEq/kg) in the absence of a blood gasdetermination is warranted during a spell.• Phenylephrine in relatively large doses(5–10µg/kg IV as a bolus or 2–5µg/kg/min as aninfusion) increases SVR and reduces R–L shunt-ing. In the presence of severe RV outflow obstruc-tion, phenylephrine-induced increases of PVR willhave little or no effect in increasing RV outflowresistance. It is important to point out that treat-ment with α-adrenergic agents to increase SVR doesnothing to treat the underlying cause of the spellalthough the decrease in unstressed venous volumeinduced by these agents may augment preload.• Beta-adrenergic agonists are absolutely con-traindicated. Increasing contractility will furthernarrow the stenotic infundibulum.• Administration of propranolol (0.1mg/kg) oresmolol (0.5mg/kg followed by an infusion of50–300µg/kg/min)may reduce infundibular spasmby depressing contractility. In addition, slowing ofheart rate may allow for improved diastolic filling(increased preload), increased heart size, and anincrease in the diameter of the RV outflow tract.
• Extracorporeal membrane oxygenation (ECMO)resuscitation in refractory episodeswhen immediateoperative intervention is not possible.
Surgical therapy
Palliative shuntsPalliative shunt procedures to increase pulmonaryblood flow can be used for patients with TOFin whom complicated surgical anatomy precludesdefinitive repair at the time of presentation. Inaddition, some institutions delay elective completerepair until 12–18months of age with placement ofa palliative shunt if cyanosis occurs prior to that timeinterval. The disadvantages of a palliative shunt inTOF patients can be summarized as follows:• The volume load imposed on the LV by theseshunts parallels the increases in pulmonary flowproduced. There will be progressive hypertrophy ofthe body and infundibulum of the RV during theinterval from shunt placement to definitive repair asright ventricular outflow tract (RVOT) obstructionwill not be relieved.• Shunt placement may distort PA anatomy andimpair subsequent growth making definitive repairmore difficult.• A large shunt with high pulmonary blood flowputs the patient at risk for development of PVOD.
The palliative shunt procedures involve creationof a systemic-to-pulmonary arterial shunt, essen-tially a surgically created PDA. Ideally, these sur-gical shunts should be mildly restrictive simpleshunts. In the presence of a proximal obstructionto pulmonary blood flow, these shunts produce aL–R shunt and an increase in pulmonary bloodflow. The shunts can be summarized as follows(Fig. 6.21a–d):• Waterston and Potts shunts. The Waterson shunt isa side-to-side anastomosis between the ascendingaorta and the right PA. This procedure is performedvia a right thoracotomy without CPB. The Pottsshunt results is a side-to-side anastomosis betweenthe descending aorta and the left PA. This procedureis performed via a left thoracotomy without CPB.Waterston and Potts shunts are of historic interestonly. It is difficult to size the orifice of these shuntscorrectly. Too small an orifice will limit pulmonary

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 210 — #44
210 Chapter 6
RSCA
RPA
Ao PA
RSCA
TG
RPA
Ao PA
RSCA
Ao
RPA
PA PATG
RPA
RSCA
Ao
(a) (b)
(c) (d)
Fig. 6.21 Surgically created systemicto pulmonary artery shunts.(a) Blalock–Taussig shunt. (b) ModifiedBlalock–Taussig shunt. (c) Waterstonshunt. (d) Central shunt. Ao, aorta;PA, pulmonary artery; RPA, rightpulmonary artery; RSCA, rightsubclavian artery; TG, tube graft.
blood flow, whereas too large an orifice will createpulmonary overperfusion and congestion and pre-dispose to development of unilateral PVOD. Theseshunts may produce distortion of the PA, makingsubsequent definitive repair difficult. In addition,they are difficult to take down at the time of thedefinitive procedure.• Central shunt. This shunt places a synthetic tubegraft between the ascending aorta and the mainor branch PA. It often is used when prior shuntprocedures have failed.• Blalock–Taussig shunt (BTS). As originallydescribed, this involves creation of an end to-side anastomosis of the right or left subclavianartery to the ipsilateral branch PA. Currently,a modification of this procedure known as themodified Blalock–Taussig shunt (MBTS) is used.It involves interposing a length of Gore-Tex tubegraft (3.5–4.0mm in infants) between the sub-clavian or innominate artery and the branch PA.These shunts are performed on the side oppo-site the aortic arch. This shunt can be performed
with or without CPB via a thoracotomy or mediansternotomy (see Fig. 6.18).
Definitive repairCurrently, most patients with TOF have an electivefull correction between the ages of 2–10months ofage. In some centers surgery is delayed as long aspossible within this time interval with the precisetiming of repair dictated by the onset of cyanoticepisodes. Definitive repair for TOF is being accom-plished in neonates in some centers if favorableanatomy is present. Surgery is aimed at relieving theoutflow obstruction by resection of hypertrophied,obstructing muscle bundles and augmentation andenlargement of the outflow tract with a pericardialpatch. Unless the pulmonic annulus is near nor-mal size, and the pulmonary valve is only mildlystenotic, enlargement of the outflow tract involvesextension of the patch across the pulmonary valveannulus and into the main PA. Because a transan-nular patch creates pulmonic insufficiency it is bestavoided when possible. If stenosis of the PA extends

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 211 — #45
Congenital Heart Disease 211
to the bifurcation, the pericardial patch can beextended beyond the bifurcation of the pulmonaryarteries. Finally, the VSD is closed. In neonates thisis usually done through the right ventriculotomycreated for resection of RVOT obstruction and place-ment of the transannular patch. In infants and olderchildren the VSD can be closed via a trans-tricuspidvalve approach.An important surgical consideration for patients
with TOF/PS is the occurrence of coronary arteryabnormalities. Approximately 8% of patients haveeither the left main coronary artery or the leftanterior descending artery as a branch of the rightcoronary artery. In these cases, a right ventriculo-tomy to enlarge the right ventricular outflow tractwill endanger the left coronary artery. In such cases,an extracardiac conduit (RV to main PA) may benecessary to bypass the outflow tract obstructionand avoid injury to the coronary artery.
Anesthetic management
Goals1 Maintain heart rate, contractility, and preload tomaintain cardiac output. Euvolemia is important toprevent exacerbation of dynamic RVOT obstructionfrom hypovolemia and reflex increases in heart rateand contractility.2 Avoid increases in the PVR:SVR ratio. The lesssevere the RV outflow obstructive lesions, the moreimportant this becomes. Increases in PVR relativeto SVR, and decreases in SVR relative to PVR, willincrease R–L shunting, reduce pulmonary bloodflow, and produce or worsen cyanosis.3 Use ventilatory measures to reduce PVR. Caremust be taken to minimize mean airway pressureso as to avoid mechanical obstruction of pulmonaryblood flow.4 Maintain or increase SVR. This is particularlyimportant when RV outflow obstruction is severeand changes in PVR will have little or no effect onshunt magnitude and direction.5 Aggressively treat episodes of hypercyanosis.6 Maintain contractility. Depression of contractil-ity, particularly in the face of severe RV outflowobstruction, may produce RV afterload mismatch(see Chapter 2) and drastically reduce pulmonary
blood flow. The exception to this is patient in whomthe dynamic component of infundibular obstructionis active. Reducing contractility in these patientsmay reduce RV outflow obstruction via relaxationof the infundibulum.Creation of surgical shunts to increase pul-
monary blood flow presents the anesthesiologistwith several additional management problems:1 When a thoracotomy approach is used, unilaterallung retraction will be required for surgical expo-sure. The resulting atelectasis may severely com-promise oxygenation and carbon dioxide removal.Intermittent reinflation of the lung may be neces-sary during the operative procedure. These rein-flations should be coordinated with the surgeon.For all the shunts described, the main or branchPA will have to be partially occluded by a clampto allow creation of the distal anastomosis. Theresulting increase in physiological dead spacemay compromise oxygenation and carbon diox-ide removal and will increase the arterial–ETCO2gradient.2 Efforts to increase pulmonary blood flow byreducing PVR with ventilatory interventions and byincreasing L–R shunting should be initiated beforePA occlusion.3 Partial occlusion of the aorta with a clamp will benecessary during creation of Waterston, Potts, andcentral shunts. The resulting increase in LV afterloadmay compromise systolic function.4 All of the palliative shunts impose a volume loadon the LV. Inotropic support may be necessary toensure systemic and shunt perfusion after shuntcreation.5 Palliative shunts are mildly restrictive simpleshunts. It is important to maintain SVR and reducePVR to maintain pulmonary blood flow in patientswith surgical shunts.6 Be prepared to treat an episode of hypercyanosis.
Induction and maintenanceRegardless of the mode of induction, aggressivevolume expansion with 10–15mL/kg of 5% albu-men or normal saline should be initiated onceIV access is obtained. This is particularly true inpatients who have been NPO for a long intervalprior to induction. This is themost effective first line

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 212 — #46
212 Chapter 6
therapy in preventing and treating dynamic RVOTobstruction.An IV induction is desirable but most infants
and children will tolerate a mask induction witheither sevoflurane or halothane as there is a paralleldecrease in PVR and SVR. Halothane may be betterat attenuating the dynamic component of RVOTobstruction than sevoflurane given halothane’smore potent negative inotropic effect. Systemichypotension should be avoided or treated promptly.Systemic hypotension is particularly likely to causeor increase R–L shunting when RV outflow obstruc-tion is severe as anesthesia-induced decreases inPVR have little effect on decreasing RV outflowresistance. Reduced SVR can be normalized withphenylephrine (0.5–1.0µg/kg).Ketamine is a useful induction agent in patients
with TOF. Ketamine has been shown to cause nosignificant alteration in QP:QS in these patients.Fentanyl or sufentanil will provide very stableinduction and maintenance hemodynamics andwill blunt stimulation induced increases in PVR.Maintenance of anesthesia with fentanyl or sufen-tanil, a muscle relaxant, and a benzodiazepine orinhalation agent is appropriate.
Post-CPB management
Goals1 Maintain heart rate (preferably sinus rhythm)at an age-appropriate rate. Cardiac output is likelyto be more heart-rate-dependent during the post-CPB period. Atrial pacing may be necessary in thepresence of junctional ectopic tachycardia (JET).2 Reduce PVR through ventilatory interventions.3 Inotropic support of the RV may be neces-sary. Dobutamine (5–10µg/kg/min) or dopamine(5–10µg/kg/min) is useful in this instance becausethey provide potent inotropic support withoutincreasing PVR. Milrinone (0.5–1.0µg/kg/min fol-lowing a loading dose of 50µg/kg) should beconsidered for its inotropic and lusitrophic effectsand its effect on PVR.4 In patients with RV systolic or diastolic functionand an atrial fenestration a PaO2 of 40–50mmHgis acceptable in the presence of adequate cardiacoutput.
After definite repair for TOF, several factors maycontribute to impaired RV systolic and diastolicfunction:• Creation of a right ventriculotomy and placementof the RV outflow patch produces a segment ofdyskinetic RV free wall.• Protection of the RV from ischemia duringaortic cross-clamping is difficult in patients witha hypertrophied RV as occurs in TOF.• Enlargement of the RV outflow tract with atransannular patch will create pulmonary regur-gitation, which imposes a volume load onthe RV.• Stenosis or hypoplasia of the distal pulmonaryarteries or residual RV outflow obstruction willimpose a pressure load on the RV.• A residual VSD will impose a volume load onthe RV.A residual VSD is likely to very poorly toler-
ated in the patient with TOF with the most likelymanifestation being low cardiac output syndromeassociated with elevated CVP, LAP, and PAP. RVOTobstruction will be completely or nearly completelyeliminated post-repair. PVR is likely to be low andthe pulmonary vasculature very compliant. As aresult, there will be potential for a large L–R intrac-ardiac shunt with a residual VSD. This will placea large volume load on the LV and RV. An acutevolume load will not be well tolerated by the RVthat is likely to be concentrically hypertrophiedand poorly compliant in response to the chronicpressure overload that existed preoperatively. Thepresence of pulmonary insufficiency will furtherexacerbate RV dysfunction by imposing an addi-tional volume load. Any distal PA stenoses, highmean airway pressures, and elevated PVR will allincrease the regurgitant volume and subsequent RVvolume load.Following complete repair of TOF with no resid-
ual lesions and minimal intrapulmonary shunt theSaO2 should be 100%. In infants and small children,particularly those left with pulmonary insufficiencyas the result of a transannular patch and thoseexpected to have restrictive RV diastolic functionas a result of a ventriculotomy and/or extensiveRV hypertrophy the surgeon may choose to leavea “pop-off” valve by leaving the PFO open or by

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 213 — #47
Congenital Heart Disease 213
creating a small (3–4mm) atrial level fenestration.This will allow physiologic intracardiac R–L shunt-ing with the ability to augment systemic cardiacoutput at the expense of systemic oxygen saturationin the setting of RV dysfunction. There will be directdelivery of some desaturated venous blood to theLA. In these patients, a PaO2 of 40–50mmHg anda SaO2 of 70–80% is acceptable until RV functionimproves over the course of days.TEE is invaluable in assessing for residual lesions,
ventricular function and the direction of shunt-ing across the atrial fenestration. As described inChapter 2, hemodynamic and saturation data can beused to identify and quantify residual intracardiacshunts.Postoperative JET is a transient tachyarrhyth-
mia that occurs immediately following congeni-tal heart surgery. The incidence of JET followingTOF repair may be as high as 20%. JET is likelysecondary to surgical trauma in the area of theAV node secondary to the retraction necessary toexpose the VSD and RVOT from across the tricuspidvalve.JET typically manifests with a junctional rate
only slightly faster than the sinus node rate and isthe only narrow complex tachycardia in which theatrial rate is less than the ventricular rate (A:V ratio<1:1). Much less commonly (10%), there may beretrograde activation of the atrium with invertedpwaves noted and anA:V ratio of 1:1. In either case,there is loss of AV synchrony (loss of atrial kick).At a heart rate <160–170 b/min this arrhythmiamay be well tolerated. It is unlikely to be toleratedin the presence of restrictive diastolic function atany rate. JET with heart rate >170 b/min is asso-ciated with hemodynamic instability and increasedpostoperative mortality.Neither cardioversion nor adenosine is effec-
tive. Treatment of JET is atrial pacing at a rateslightly faster than the junctional rate reinitiatingA–V synchrony. This therapy is effective unlessthe junctional rate is very fast (>160–170 b/min)at which point atrial pacing at a faster rate isunlikely to improve hemodynamics because thereinitiation of A–V synchrony is offset by the reduc-tion in diastolic filling time present at theserates.
Transposition of the great arteries
AnatomyIn transposition of the great arteries (TGA) thereis concordance of the atrioventicular connectionsassociated with discordance of the ventriculoarte-rial connections. The most common manifestationof this anatomy occurs in patients with [S, D, D] seg-mental anatomy (Fig. 6.22). That is, there is atrialsitus solitus, D-loop ventricles, and D-loop greatarteries. A right-sided RA connects via a right-sidedtricuspid valve and RV to a right sided and ante-rior aorta. A left sided LA connects via a left sidedmitral valve and LV to a left sided and posterior PA.As a result, there is fibrous continuity between themitral and pulmonic valves with a lack of fibrouscontinuity between the tricuspid and aortic valves(conus). This anatomy is most commonly referredto as D-TGA.The coronary arteries in D-TGA arise from the
aortic sinuses that face the PA. In normally relatedvessels, these sinuses are located on the anteriorportion of the aorta while in D-TGA they are locatedposteriorly. In the majority of D-TGA patients(70%), the right sinus is the origin of the right coro-nary artery, whereas the left sinus is the origin of theleft main coronary artery. In the remainder of cases,there is considerable variability (Fig. 6.23).
AoPA
LA
LV
RA
RV
Fig. 6.22 Anatomy of dextro-transposition of the greatarteries (D-TGA). Ao, aorta; LV, left ventricle; PA,pulmonary artery; RA, right atrium; RV, right ventricle.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 214 — #48
214 Chapter 6
LAD LAD
LCx
LCxSingle RCA Single LCA
RCA
Usual Circumflex from RCA
RCA
RCA
RCA
LAD
LAD
LCx
LCx
LCx
Inverted coronaries Inverted circumflexand RCA
LCx
LCx
RCA RCA
LAD
LADLAD
RCA
Intramural LCA Intramural LAD
RCA
LAD
LCx
A
P
LR
A
P
LR
A
P
LR
A
P
LR
Fig. 6.23 Most common coronary artery patterns intransposition of the great arteries (TGA). The aorta isanterior and rightward of the pulmonary artery. LAD, leftanterior descending; LSA, left coronary artery; LCx, leftcircumflex; RCA, right coronary artery. (From Mayer JE,et al. Coronary artery pattern and outcome of arterialswitch operation for transposition of the great arteries.Circulation 1990;82 (suppl IV):144, with permission.)
In patients with D-TGA, the most commonlyassociated cardiac anomalies are a VSD, and subpul-monic stenosis. In D-TGA subpulmonic stenosis isleft ventricular outflow tract obstruction (LVOTO).Approximately 50% of patients with D-TGA will
present with a PDA. The FO is almost always patent,but a true secundum ASD exists in only about 5%of patients. Although angiographically detectableVSDs may occur in 30–40% of patients, only aboutone third of these defects are hemodynamicallysignificant. Thus, for practical purposes, 75% ofpatients have an intact ventricular septum (IVS).LVOTO is present in about 30% of patients withVSD and is most often due to an extensive subpul-monary fibromuscular ring or posterior malpositionof the outlet portion of the ventricular septum. Only5% of patients with IVS have significant LVOTO. Inthese patients, there is a dynamic obstruction of theLVOT during systole due to the leftward bulging ofthe ventricular septum and the anterior movementof the anterior mitral valve leaflet. The septal shiftnecessary to produce this obstruction is uncommonin neonates due to the presence of elevated PVR.Valvular PS is rare in patients with TGA. Otherless commonly seen lesions are tricuspid or mitralregurgitation (4% of each) and a coarctation of theaorta (5%).Bronchopulmonary collateral vessels (aorta to
PA proximal to the pulmonary capillaries) arevisible angiographically in 30% of patients withD-TGA. The larger and more extensive collateralsgenerally involve the right lung. These collateralsprovide a site for intercirculatory mixing and havebeen implicated in the accelerated developmentof PVOD.
PhysiologyD-TGA produces two parallel circulations withrecirculation of systemic and pulmonary venousblood. Survival depends on one or more com-munications between the two circuits to allowintercirculatory mixing (see Fig. 6.4). The sitesavailable for intercirculatory mixing in D-TGAcan be intracardiac (PFO, ASD, VSD) or extracar-diac (PDA, bronchopulmonary collaterals). Severalfactors affect the amount of intercirculatory mixing.The number, size, and position of anatomic commu-nications are important. One large, nonrestrictivecommunication will provide better mixing thantwo or three restrictive communications. Reducedventricular compliance and elevated systemic andPVR tend to reduce intercirculatory mixing by

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 215 — #49
Congenital Heart Disease 215
impeding flow across the anatomic communica-tions. The position of the communication is alsoimportant. Poor mixing occurs even with largeanterior muscular VSDs due to their unfavorableposition.Patients with PS will have low pulmonary blood
flow and may be hypoxemic despite a relativelylarge intercirculatory communication. Patients withhigh pulmonary blood flow, particularly those witha VSD in whom systemic pressures are transmit-ted to the pulmonary vasculature, are at risk ofdeveloping PVOD. In the presence of a good-sizedintercirculatory communication, these patients willinitially not be hypoxemic. However, the progres-sive development of PVOD will eventually reducepulmonary blood flow and produce hypoxemia.Finally, all patients with TGA and increased pul-monary blood flow will have a large volume loadimposed on the LA and LV.In TGA with VSD some intercirculatory mixing
occurs at the ventricular level but there is predomi-nantly anatomic R–L shunting (effective pulmonaryblood flow) at the VSD (RV to LV to PA) and PDA(RV to AO to PA) and anatomic L–R shunting (effec-tive systemic blood flow) at the PFO or ASD (LA toRA to RV to AO). Obviously, the more severe theLVOTO the more dependent effective pulmonaryblood flow will be on the presence of a PDA.In TGA with IVS the anatomic mixing sites are
usually a PDA and a PFO. The dynamics of intercir-culatory mixing in TGA/IVS are complex. Anatomicshunting at the atrial level is ultimately determinedby the size of the atrial communication and thecyclical pressure variations between the left andright atria. The volume and compliance of the atria,ventricles, and vascular beds in each circuit, as wellas heart rate and phase of respiration all influencethis relationship. Shunting is from the RA to the LAduring diastole as the result of the reduced ventric-ular and vascular compliance of the systemic circuit.In systole, shunt is from the LA to the RA primarilybecause of the large volume of blood returning tothe LA as a result of the high volume of recirculatedpulmonary blood flow.The direction of shunting across the PDA largely
depends on the PVR and the size of the intra-atrial communication.When the PVR is low and the
intra-atrial communication is nonrestrictive, shunt-ing is predominantly from the aorta to the PAvia the PDA (effective pulmonary blood flow) andpredominantly from the L–R atrium across the atrialseptum (effective systemic blood flow). When PVRis elevated, shunting across the PDA is likely to bebidirectional, which would in turn encourage bidi-rectional shunting across the atrial septum. WhenPVR is high and PA pressure exceeds aortic pressure,shunting at the PDAwill be predominantly from thePA to the aorta. This will create reverse differentialcyanosis. In this physiology the preductal arterialsaturation is lower than the postductal arterial satu-ration. This is usually the result of a restrictive atrialcommunication producing left atrial hypertensionand is associated with low effective blood flows(poor mixing) and hypoxemia. A balloon atrial sep-tostomy (BAS) can be lifesaving in this setting.Decompression of the LA promotes mixing at theatrial level and also reduces PVR and PA pressurepromoting mixing at the PDA.Themajority of neonateswithD-TGAand IVSwill
be hypoxemic (arterial saturation≤60%)within thefirst day of life. A proportion of these patients willhave severely reduced effective pulmonary and sys-temic blood flow resulting in a PaO2 < 20mmHg,hypercarbia, and an evolvingmetabolic acidosis sec-ondary to the poor tissue oxygen delivery. PGE1(maintenance 0.01–0.05µg/kg/min) is adminis-tered to dilate and maintain the patency of theDA. This will be effective in increasing effectivepulmonary and systemic blood flow, and in improv-ing PaO2 and tissue oxygen delivery if PVR < SVRand there is a nonrestrictive or minimally restric-tive atrial septal communication. In some cen-ters, all neonates stabilized on PGE1 alone havea BAS to enlarge the atrial septal communicationso that PGE1can be stopped and surgery sched-uled on a semi-elective basis. PGE1 infusion isassociated with apnea, pyrexia, fluid retention,and platelet dysfunction. Recent investigations link-ing BAS to subsequent embolic neurologic injurymust be considered in the risk-benefit analysis ofnonemergent BAS.If PGE1 does not improve tissue oxygen delivery
then an emergent BAS is performed in the catheteri-zation laboratory utilizing angiography or in the ICU

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 216 — #50
216 Chapter 6
utilizing echocardiography. These patients requiretracheal intubation and mechanical ventilation.This allows reduction of PVRvia induction of a respi-ratory alkalosis and elimination of pulmonary V /Qmismatch. Sedation and muscle relaxation reduceoxygen consumption thereby increasing mixedvenous oxygen saturation. For a given amount ofintercirculatory mixing and total systemic bloodflow, an increase in systemic venous or pulmonaryvenous saturation will result in an increase inarterial saturation.In rare instances the combination of PGE1, a BAS,
and mechanical ventilation with sedation and mus-cle relaxation may be ineffective. In this circum-stance, ECMO (either veno–arterial or veno–veno)support to improve tissue oxygenation and toreverse end-organ insult and lactic acidosis prior tosurgery is indicated.
Surgical therapy
Intra-atrial physiologic repair: Mustard andSenning proceduresBoth the Mustard and the Senning procedures areatrial switch procedures that surgically create dis-cordant atrioventricular (AV) connections in thepresence of the preexisting discordant ventriculoar-terial connections. Therefore, after repair, systemicvenous blood is routed to the LV, which is in con-tinuity with the PA. Likewise, pulmonary venousblood is routed to theRV,which is in continuitywiththe aorta. This arrangement results in physiologicbut not anatomic correction of D-TGA. Followingthese procedures the RV remains the systemic ven-tricle and the tricuspid valve remains the systemicAV valve.The Mustard procedure redirects pulmonary and
systemic venous return via an intra-atrial baffleafter excision of the interatrial septum. The baf-fle is made from pericardium or synthetic materialto preserve atrial contractility and optimize atrialgrowth potential. In the Senning procedure, autol-ogous tissue from the right atrial wall and IAS isused in place of pericardium or synthetic materialto preserve atrial contractility and optimize atrialgrowth potential. Following both procedures, pul-monary venous blood is directed over the top of
Ao
PA
Atrial baffle
RV
LV
Fig. 6.24 Schematic of completed Mustard operation.There has been creation of an atriotomy, enlargement ofatrial septal defect, and creation of an intra-atrial baffle.Orifices of superior and inferior vena cavae are encircledby distal ends of the baffle such that systemic venousblood is directed under the baffle, across the enlargedatrial septal defect into mitral valve, left ventricle, andpulmonary artery. Pulmonary venous blood remainsabove the baffle to be directed across the tricuspid valveinto the right ventricle and aorta. Ao, aorta; LV, leftventricle; PA, pulmonary artery; RV, right ventricle.
the baffle to cross the tricuspid valve while systemicvenous blood is directed beneath the baffle to crossthe mitral valve (Fig. 6.24).Long-term exposure of the RV and tricuspid valve
to systemic pressure results in progressive right ven-tricular dysfunction. Both systemic and pulmonaryvenous obstruction may occur as the result of bothprocedures. The incidence of dysrhythmias afterthese procedures is high: 64% of patients have dys-rhythmias, 28% of which are serious (bradycardia,sick-sinus syndrome, atrial flutter).
Anatomic repair or the arterial (Jatene)switch procedureThe arterial switch operation (ASO) anatomicallycorrects the discordant ventriculoarterial connec-tions. After repair, the RV is connected to the PAand the LV is connected to the aorta. Clinical suc-cess with the ASO, summarized in Fig. 6.25(a–f),was achieved in 1975. In brief, the PA and theaorta are transected distal to their respective valves.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 217 — #51
Congenital Heart Disease 217
(a) (b)
(c)
(d)
(e) (f)
Fig. 6.25 Arterial switch operation (ASO). (a) Aorta iscross-clamped and the aorta and pulmonary artery aretransected. (b) Left and right main coronary arteries areexcised from the anterior aorta using a segment of aorticwall extending from rim of aorta. (c) Equivalentsegments of pulmonary arterial wall are excised andcoronary arteries are translocated posteriorly to thepulmonary artery (neoaorta). (d) Distal pulmonaryartery is brought anterior to ascending aorta (Lecomptemaneuver), and proximal pulmonary artery (neoaorta) isanastomosed to distal aorta. (e) Sites of coronaryexplantation are repaired using pericardium. (f) Proximalaorta is sutured to distal pulmonary artery.
The coronary arteries are initially explanted fromthe ascending aorta with 3–4mm of surround-ing tissue. The explant sites are repaired eitherwith pericardium or synthetic material. The coro-nary arteries are reimplanted into the proximal PA(neoaorta). The great arteries are then switchedwith the distal PA brought anterior (LeComptemaneuver) to be reanastomosed to the old proximal
aorta (right ventricular outflow) and the distal aortareanastomosed to the old proximal PA (LV outflow).Most patients with D-TGA have coronary
anatomy that is suitable for coronary reimplan-tation. Patients with certain types of coronaryanatomy (inverted coronaries, single right coro-nary artery) are at risk for postoperative myocardialischemia and death because reimplantation canresult in distortion of the coronary ostia or nar-rowing of the artery itself. The emergence of twoparallel coronary arteries above but in contact withthe posterior valve commissure or the intramuralorigin of the coronaries also presents a technicalchallenge. These patients may require resuspensionof the neopulmonary valve after the coronaries anda surrounding tissue cuff have been excised.In order for the ASO to be successful, the origi-
nal pulmonary ventricle (LV) must have sufficientmass to be capable of becoming the systemic ventri-cle. Patient selection and the timing of the surgicalprocedure are important variables in determiningthe success of this procedure. Two-dimensionalechocardiography is used to noninvasively assessthe LV:RV pressure ratio and to determine theextent to which LV mass has regressed.The ASO was originally described in patients
with D-TGA and a large VSD or a large PDA.In these patients, the pulmonary ventricle (LV)remains exposed to systemic pressures and the LVmass remains sufficient to support the systemiccirculation. For such patients, the ASO must beperformed within the first 2–3months of life toprevent intractable CHF or irreversible PVOD. Inthese patients, the ASO is generally performedwithin the first fewweeks of life. Closure of the VSDis preferentially performed transatrially through thetricuspid valve. It is desirable to avoid approachinga VSD through the RV because an incision in theRVmay contribute substantially to postoperative RVdysfunction.In patients with D-TGA and IVS, there is pro-
gressive reduction in LV mass as the physio-logic pulmonary hypertension present at birthresolves progressively over the first days after birth.Adequate LV mass to support the systemic circu-lation exists in these patients for only the first2–3months after birth. In patients with D-TGA and

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 218 — #52
218 Chapter 6
IVS, the ASO can be performed primarily or as thesecond phase of a staged procedure. A primary ASOis generally suitable for D-TGA and IVS patientswithin the first 2months of life and is usuallyperformed within the first week of life.The two-stage repair for D-TGA with IVS is used
for neonates in whom there has been significantregression of LV mass. These are generally neonatesin whom surgery cannot be performed during thefirst several weeks of life secondary to prematurity,sepsis, low birth weight (<1.5 kg), or late referral.The LV is prepared to accept the systemic workloadby placement of a PA band. In addition, an aortopul-monary shunt with entry to the PA distal to theband is necessary to prevent hypoxemia. The bandmust be tight enough to increase pressure in the pul-monary ventricle (LV) to approximately one-halfto two-thirds that in the systemic ventricle (RV).This will increase afterload sufficiently to preventregression of LV mass. However, if the band is tootight, there may be LV decompensation secondaryto afterload mismatch.Generally a rapid two-stage repair is performed.
The ASO is performed as early as 1week afterpreparatory PA banding, often during the same hos-pitalization. This approach is based on the fact that adoubling of LVmass is seen after 1week of PA band-ing. The staged procedure is complicated by the factthat placement of the PA band to the proper tight-ness is not an easy task and that the PA band andsystemic to PA shunt may result in distortion of thePA, making the definite ASO difficult.The ASO is generally not performed on patients in
whom mechanical LVOTO (subpulmonic stenosis)exists. Correction of the LVOTO is difficult, andwithout complete correction of the LVOTO, thesepatients will be left with aortic or subaortic stenosis.On the other hand, patients with dynamic LVOTOhave been shown to have no gradient across the LVoutflow tract after the ASO.
Rastelli procedureFor patients with D-TGA, VSD, and severe LVOTO(subpulmonary stenosis), a Rastelli procedure isperformed. Closure of the VSD is performedthrough a right ventriculotomy. The VSD is closedso that LV blood is directed through the aorta.
(a) (b)
Ao
PA
RV LV
Fig. 6.26 Schematic of Rastelli procedure for repair oftransposition of the great vessels associated withpulmonic stenosis and ventricular septal defect (VSD).(a) VSD is closed with patch such that left ventricularoutput is directed across the aortic valve. (b) Proximalmain pulmonary artery is ligated and valved conduit isplaced from right ventricle to main pulmonary artery.Ao, aorta; LV, left ventricle; PA, pulmonary artery; RV,right ventricle.
The proximal PA is ligated and a valved conduitis placed from the right ventriculotomy to thePA, thereby bypassing the subpulmonic stenosis(Fig. 6.26a,b). Subaortic stenosis may result fromplacement of the VSD patch. Replacement of thevalved conduit may be necessary in later yearssecondary to calcification.
Anesthetic management
Goals1 Maintain heart rate, contractility, and preloadto maintain cardiac output. Decreases in cardiacoutput decrease systemic venous saturation with aresultant decrease in arterial saturation.2 Maintain ductal patency with PGE1(0.01–0.05µg/kg/min) in ductal-dependentpatients.3 Avoid increases in PVR relative to SVR. Increasesin PVR will decrease pulmonary blood flow andreduce intercirculatory mixing. For patients withPVOD, ventilatory interventions should be usedto reduce PVR. For patients with LVOTO that isnot severe, ventilatory interventions to reduce PVRincrease pulmonary blood flow and intercirculatorymixing.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 219 — #53
Congenital Heart Disease 219
4 Reductions in SVR relative to PVR should beavoided. Decreased SVR increases recirculationof systemic venous blood and decreases arterialsaturation.
Induction and maintenanceIn prostaglandin dependent neonates the PGE1infusion should be continued until CPB to assurean adequate intercirculatory mixing. The increasedpulmonary blood flow will limit the cardiac reserveof these patients and the immature myocardiumwill be sensitive to anesthetic-induced myocardialdepression. Anesthesia is generally induced andmaintained using a synthetic opioid (fentanyl orsufentanil) based technique. A high-dose fentanylor sufentanil technique will provide hemodynamicstability without adversely affecting intercirculatorymixing.In infants older than 6–8months, premedita-
tion may be necessary to facilitate the separationfrom the parents. In the absence of IV access oralmidazolam (0.5–1.0mg/kg) is useful. Older, better-compensated children, such as those presentingfor a Rastelli repair with a functioning systemicto PA shunt, may require a more substantial oralpremedication.In patients with reduced pulmonary blood flowor
poor intercirculatory mixing, efforts to reduce PVRshould be made to increase pulmonary blood flowand intercirculatory mixing. In patients with PVOD,ventilatory measures to reduce PVR are useful ifPVR is not fixed. An inhalational induction or anIM ketamine induction followed by placement of anIV and conversion to a high-dose fentanyl or sufen-tanil technique may be suitable for these patients.A similar approach may be taken for older childrenwith subpulmonic stenosis. A high-dose fentanyl orsufentanil technique is useful in blunting the stress-induced increases in PVR that are so detrimental tothese patients.Hypercarbia, acidosis, and hypoxemia further
increase PVR and should be avoided because of thelimited myocardial reserve of neonates and infants.This is particularly true in neonates with TGV andIVS, where systemic oxygen delivery is tenuous,and in infants with TGV and VSD, in whom leftventricular volume overload is present. In addition,
reactive increases in PVR are commonly seen in theimmature pulmonary vasculature andmay severelycompromise pulmonary blood flow.
Post-CPB management
Goals1 Maintain heart rate (preferably sinus rhythm) atan age-appropriate rate. Cardiac output is likely tobe more heart-rate-dependent during the post-CPBperiod. For patients having undergone atrial baffleprocedures, anti-dysrhythmic therapy or pacingmay be necessary.2 Myocardial ischemia after coronary reimplan-tation should be treated aggressively and promptimmediate re-evaluation of the anastomoses andthe possibility of external compression.3 Reductions in aortic and PA pressures may benecessary to help prevent suture line bleeding afterthe ASO.4 Systemic ventricular (RV after atrial baffleprocedures and LV after arterial switch proce-dures) dysfunction may necessitate inotropic andvasodilator therapy to terminate CPB. Dobutamine(5–10µg/kg/min) or dopamine (5–10µg/kg/min) isuseful. Milrinone (0.5–1.0µg/kg/min following aloading dose of 50µg/kg) may be a better choiceif SVR is high. Milrinone has direct SVR reducingeffects in addition to inotropic, lusitrophic, and PVRreducing effects.After atrial baffle repairs, there may be pul-
monary and systemic venous obstruction. Systemicvenous obstruction will produce systemic venouscongestion and a low RA pressure. Pulmonaryvenous obstruction may result in pulmonaryvenous and pulmonary arterial hypertension, pul-monary edema, and hypoxemia. Efforts to reduceSVR will reduce the RV afterload and help preventtricuspid regurgitation. Therapy for atrial dysrhyth-mias also may be necessary. TEEwill prove useful inruling out pulmonary and systemic venous obstruc-tion. In addition, large baffle leaks that may requiresurgical revision will be detected.After the arterial switch procedure, there may be
extensive bleeding from the aortic and pulmonarysuture lines. Myocardial ischemia following reim-plantation of the coronary arteries is a potential

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 220 — #54
220 Chapter 6
problem following the ASO. In some circumstances,the ischemia is transient secondary to coronary airemboli. Transesophageal echocardiography is veryuseful to assure adequate removal of air from theLA and ventricle prior to the termination of CPB.It is also useful in assessing the potency of thereimplanted coronary arteries. Maintenance of highperfusion pressures on CPB after aortic cross-clampremoval will facilitate the distal migration of airemboli. In other instances, kinking of the reim-planted artery or compromise of the implantedcoronary ostia may require immediate surgicalintervention. External compression of the coronar-ies by clot or surgical hemostatic packing materialshould also be considered. Pharmacologic inter-vention with traditional therapies to improve thebalance of myocardial oxygen demand and deliverysuch as nitroglycerin and beta-blockade are never along-term alternative to prompt surgical revision ofthe appropriate anastomosis.Despite comprehensive preoperative evaluation,
the LV of patients undergoing an ASO may bemarginal in its ability to support the systemic cir-culation in the post CPB period. This may occuras the result of myocardial ischemia, inadequateLV mass, poor protection of the LV during aorticcross-clamping, or a combination of these vari-ables. Transesophageal echocardiography is usefulin identifying and continuously evaluating bothglobal and regional LV systolic dysfunction. It alsodetects mitral regurgitation, which may occur sec-ondary to papillary muscle dysfunction or to dila-tion of the mitral valve annulus. Inotropic supportof the LV and afterload reduction may be nec-essary to terminate CPB. Initial inotropic supportis accomplished with dopamine (3–10µg/kg/min).In rare instances where LV failure is severe,epinephrine (0.05–0.50µg/kg/min) may have to beadded in combination with nitroprusside (startingat 0.15–0.50µg/kg/min).Milrinone (0.5–1.0µg/kg/min following a
50µg/kg loading dose) is a useful agent in thesepatients as it is an inodilator. These patients areat particular risk for LV dysfunction in the imme-diate postoperative period secondary to afterloadmismatch (insufficient contractility for the degreeof systemic afterload). While the vasodilation that
accompanies milrinone administration in infants issubstantially less than that seen in adult patients itis nonetheless advisable to administer the loadingdose of milrinone over 10–15minutes.A unique cycle of LV dilation initiating and
exacerbating myocardial ischemia exists in patientshaving undergone the arterial switch. Myocardialischemia, afterload mismatch, or overzealous vol-ume infusion can result in LV distension and LAhypertension. This will be particularly likely if thereis mitral insufficiency from either papillary muscledysfunction or dilation of the mitral valve annulus.LV distension may result in tension on and kinkingof the coronary re-anastomosis sites. LA hyper-tension produces elevations in PA pressure anddistension of the PA. Since the LeCompte maneu-ver (see Fig. 6.25) brings the distal PA anterior tothe ascending aorta distension of the PA may actu-ally compress or place tension on the coronary ostia.The resulting myocardial ischemia produces furtherLV dilation, progressive elevations in LA and PApressures, and continuing compromise of coronaryblood flow.TEE usually allows visualization of the reim-
planted coronary arteries and allows patency tobe assessed. In addition, TEE will provide onlineassessment of LV function, which may allow earlydetection of a kinked or compromised coronaryanastomosis. Inotropic support of the LV also can beguided by the use of TEE.
Total anomalous pulmonary venousreturn
AnatomyTotal anomalous pulmonary venous return (TAPVR)is characterized by drainage of all of the pulmonaryveins into the systemic venous system rather thandirectly into the left atrium. In this lesion there isusually a single common pulmonary venous con-fluence with no direct connection to the LA. Thepulmonary vein confluence then drains into thesystemic venous circulation via one of four of thefollowing drainage patterns (Fig. 6.27a–d):• Supracardiac (type 1). In 46% of patients, drainageof the pulmonary vein confluence is into a suprac-ardiac structure. Most commonly drainage is to the

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 221 — #55
Congenital Heart Disease 221
SVC
LARA
RA
LA
Portalvein
IVC
LA
RA
LA
RA
Coronarysinus
Commonpulmonary vein
(a) (b)
(c) (d)
Fig. 6.27 Types of totally anomalous pulmonary venousreturn (TAPVR). (a) Supracardiac. A vertical veinconnects the confluence of pulmonary veins to theinnominate vein. (b) Infracardiac. A vertical vein, whichtransverses the diaphragm, connects the confluence ofpulmonary veins to the portal vein which here has astenotic connection to the IVC. Pulmonary venous returnwill be obstructed. (c) Cardiac. The confluence ofpulmonary veins drains directly into the coronary sinus.(d) Mixed. The left pulmonary veins drain via a verticalvein into the innominate vein while the right pulmonaryveins drain directly into the right atrium.
SVC via a vertical vein that connects the pulmonaryvein confluence with the innominate vein, whichthen empties into the SVC.• Intracardiac (type 2). In 24% of patients, drainageof the pulmonary vein confluence is directly intothe RA via the CS.• Infracardiac (type 3). In 22% of patients, drainageis into an infracardiac structure such as the IVC,portal vein, or hepatic vein. A vertical pulmonaryvein passes through the esophageal hiatus ofthe diaphragm to connect the pulmonary veinconfluence to one of these infracardiac vessels.
• Mixed (type 4). In 8% of patients, pulmonaryvenous drainage is some combination of types 1,2, and 3.In general, the greater the distance the vertical veintravels the greater the likelihood that this pathwaywill be stenotic or compressed and that there willbe pulmonary venous obstruction. For this reasoninfracardiac drainage is most commonly associatedwith pulmonary venous obstruction. Some patientswith supracardiac TAPVR have compression ofthe vertical vein between the left main stembronchus and left PA. As PA pressure rises dueto obstruction of pulmonary venous return theconnecting vein may become further compressedbetween the left main stem bronchus and leftPA leading to near complete compression of theconnecting vein.
PhysiologyThe delivery of all pulmonary venous blood to theRA results in a large physiologic L–R shunt. Thereis complete mixing of systemic and pulmonaryvenous blood in the RA. There must be an anatomicR–L shunt and delivery of effective systemic bloodflow if there is to be filling of the left heart andsurvival outside the uterus. Normally, an ASD orpatent FO exists as the communication with theleft heart. The magnitude and direction of shunt-ing across the ASD or FO is determined by theprinciples of simple shunting. Normally a non ormildly restrictive atrial level communication existsin these patients. Delivery of blood across the atrialseptum can be impeded by the poor complianceof the LA and LV, as these structures tend to besmall due to reduced blood flow to the left side ofthe heart in utero. As a result, in the absence ofobstruction neonates will have a QP:QS close to 1:1.As PVR falls following birth there will preferen-tial delivery of the mixed systemic and pulmonaryvenous blood to the pulmonary circuit. Pulmonaryartery pressures will be near systemic becausealthough PVR is near normal the QP:QS will be high(>2–3:1).Compression or stenoses along the vertical vein
pathway will produce obstructed TAPVR leadingto pulmonary venous hypertension, elevated PVR,and systemic or suprasystemic RV and PA pressures.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 222 — #56
222 Chapter 6
Some of these patients may develop PVOD in uteroas well. In addition, pulmonary venous obstructionwill produce pulmonary edema further elevatingPVR, much as it does with mitral stenosis. Thesepatients have a small heart and congested lung fieldson chest radiograph.Cardiac output can be severely compromised in
these patients. Systemic or suprasystemic RV pres-sures will result in a leftward septal shift that“pancakes” the LV thereby further reducing thecompliance of the small LV. This will impededelivery of blood across the atrial septum. There islikely to be RV afterload mismatch with RV disten-sion and TR. Systemic cardiac output will be largelydependant on a physiologic R–L shunt across theDA supplied by a failing RV.These patients will be hypoxemic because all the
determinates of SaO2 with complete mixing will bereduced:• Pulmonary edema will induce intrapulmonaryshunt and V /Q mismatch leading to low SpvO2.• QP:QS will be reduced by the presence ofhigh PVR.• Low cardiac output will reduce SvO2.Efforts to increase pulmonary blood flow in
these patients will only worsen the pulmonaryedema and NO (as well as other inhaled pulmonaryvasodilators) is clearly contraindicated. In patientswith severe pulmonary venous obstruction lead-ing to suprasystemic RV and PA pressures and R–Lshunting across the DA ductal patency is neces-sary to maintain cardiac output. In patients withless severe obstruction and subsystemic RV and PApressures ductal flow will be bidirectional or L–R.In these patients ductal patency may exacerbatepulmonary edema. Patients with obstructed TAPVRpresent at birth with hypoxemia and poor systemicperfusion. In many there is an ongoing metabolicacidosis and evidence of end-organ (hepatic andrenal) dysfunction. Obstructed TAPVR is a surgicalemergency, one of the few remaining in the era ofPGE1 therapy.
Surgical therapyDefinitive repair involves anastomosis of the pul-monary venous confluence to the posterior LA,ligation of the vertical vein, and closure of the ASD.
Anesthetic management
Goals1 Maintain heart rate, contractility, and preloadto maintain cardiac output. Decreases in cardiacoutput will reduce systemic venous saturation. Ina complete mixing lesion, this will reduce arterialsaturation.2 For patients with TAPVR and pulmonaryvenous obstruction, emergency surgery is neces-sary. Efforts to increase pulmonary blood flowthrough ventilatory interventions and pulmonaryvasodilators will worsen pulmonary edema.3 For patients with increased pulmonary bloodflow, decreases in the PVR:SVR ratio should beavoided. The increase in pulmonary blood flowthat accompanies a reduced PVR:SVR ratio neces-sitates an increase in cardiac output to maintainsystemic blood flow.4 For patients with increased pulmonary bloodflow and right ventricular volume overload, ven-tilatory interventions should be used to increasePVR, reduce pulmonary blood flow, and decreasethe volume load on the RV.
Induction and maintenanceNeonates with pulmonary venous obstruction gen-erally arrive in the operating room intubated,ventilated, and on inotropic support. These patientsare best anesthetizedwith a high-dose narcotic tech-nique using fentanyl or sufentanil. Older patientswithout obstruction and compensated RV volumeoverload may be candidates for an inhalationalinduction. Patients with TAPVR, particularly thosewith venous obstruction, have a highly reactive pul-monary vasculature. High doses of fentanyl andsufentanil will be useful for blunting increases inPVR associated with surgical stimulation.
Post-CPB management
Goals1 Maintain heart rate (preferably sinus rhythm)at an age-appropriate rate. Cardiac output is likelyto be more heart-rate-dependent in the post-CPBperiod.2 In the presence of postoperative pulmonaryvenous obstruction, efforts to increase pulmonary

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 223 — #57
Congenital Heart Disease 223
blood flowmay worsen pulmonary edema. Surgicalrevision may be necessary.3 For patients with PVOD and reactive pulmonaryvasculature, blunting of stress-induced increases inPVR with narcotics is warranted.4 For patients with PVOD and reactive pulmonaryvasculature ventilatory interventions to reduce PVRand use of selective pulmonary vasodilators such asNO are warranted.5 Inotropic support of the RV may be necessary,even in the face of aggressive therapy to reducePVR. Dobutamine (5–10µg/kg/min) or dopamine(5–10µg/kg/min) is useful in this instance becauseboth agents provide potent inotropic supportwithout increasing PVR. In the absence of sys-temic hypotension milrinone (0.5–1.0µg/kg/minfollowing a 50µg/kg loading dose) can beconsidered.RV and PA hypertension are the most common
problems encountered post-CPB. This may be theresult of one or more of the following:• Residual pulmonary venous obstruction mayexist due the technical difficulty of constructing anonrestrictive surgical anastomosis.• In the presence of a nonrestrictive surgicalanastomosis an appropriate cardiac outputmay pro-duce LAhypertension due to the presence of a small,noncompliant LA and LV or LV dysfunction.• Reactive pulmonary vasoconstriction (capillaryand pre-capillary) may cause labile increasesin PVR.• Pre-existing PVOD.The use of TEE and of surgically placed PA and
LA lines is helpful in sorting out these etiologies. Thepresence of high PA pressures, an elevated LAP, anda PA diastolic pressure < 5mmHg above the LAPsuggests that LA hypertension is the cause of PAhypertension. The presence of high PA pressures,a low or normal LAP, and a PA diastolic pres-sure > 15–20mmHg above the LAP suggests thatreactive pulmonary vasoconstriction, PVOD, or pul-monary venous obstruction exists. In the presenceof reactive pulmonary vasoconstriction or PVODthe PAOP (wedge pressure) should not exceed theLAP by >3–5mmHg. A PAOP that exceeds theLAP by more than 5–10mmHg suggests that pul-monary venous obstruction exists. TEE is valuable
in assessing the patency of the pulmonary venousto LA anastomosis and in assessing ventricularfunction.
Obstruction to LV filling
AnatomySeveral congenital causes of obstruction to LV fillingexist:• Valvular mitral stenosis. Isolated congenital mitralstenosis is very rare and usually is caused by short,fused chordae tendineae.• Parachute mitral valve. In this lesion, two mitralvalve leaflets are attached to shortened chordae thatinsert on the same papillary muscle.• Supravalvular mitral stenosis. In this lesion, anobstructive ring of thickened endocardium is foundabove the mitral valve downstream from the atrialappendage.• Cor triatriatum. In this lesion, an obstructivemembrane is located upstream of the atrialappendage.
PhysiologyAll of these lesions have the same physiologic con-sequences as valvular mitral stenosis: obstruction toLV diastolic filling and pulmonary venous conges-tion. The physiology of mitral stenosis is discussedin detail in Chapter 5.
Surgical therapyResection of a supravalvular ring or of the mem-brane in cor triatriatum normally suffices. Repairof the mitral valve is a superior alternative tomitral valve replacement in infants and chil-dren. If a valve replacement is done a low-profile valve must be used to prevent LV out-flow tract obstruction. A mechanical valve gener-ally is chosen over a porcine or homograft valvebecause of the short in situ half-life of these valves.Mechanical valves require long-term anticoagula-tion, which may be problematic for growing, activechildren.The anesthetic and post-CPB management of
patients with mitral stenosis is discussed in detailin Chapter 5.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 224 — #58
224 Chapter 6
Left ventricle outflow tract obstruction
AnatomySeveral categories of congenital LV outflow tractobstruction exist:• Valvular aortic stenosis. This is most commonlycaused by a bicuspid aortic valve. Most of thesepatients will remain asymptomatic until the fourthor fifth decade of life. In infants presentingwith valvular aortic stenosis, the LV may besmall. These patients may represent a milder formof HLHS.• Subaortic stenosis. This may occur secondary to adiscretemembranous ring located 1–2 cm below theaortic valve or to a fibromuscular overgrowth ofthe LV outflow tract that produces a tunnel-likestenosis.• Congenital SVAS. This is most commonly causedby Williams–Beurin syndrome as the result of amicrodeletion in the q11.23 region of chromo-some 7. This deletion involves several genes, includ-ing the elastin gene. As a result there develops acharacteristic hourglass narrowing of the aorta atthe sinotubular junction; in a smaller percentage ofcases (approximately 30%) there is diffuse tubularnarrowing of the ascending aorta often extending tothe arch and the origin of the brachiocephalic ves-sels. In approximately 40% of SVAS patients severepulmonary stenoses and right ventricular pressureoverload exist in conjunction with SVAS.
PhysiologyInfants with aortic stenosis tend to have a smallLV and varying degrees of endocardial fibroelasto-sis secondary to prolonged subendocardial ischemia.When aortic stenosis is severe in the neonatalperiod, systemic blood flow and survival may bedependent on R–L shunting across a PDA. Thiswill result in perfusion of the periphery with sys-temic venous blood producing cyanosis. When thestenosis is severe and there is little antegrade aorticblood flow, the coronary arteries will be perfusedretrograde down the aortic arch with desaturatedblood. This, combined with the high left ventric-ular end-distolic pressure (LVEDP) that accom-panies aortic stenosis, will exacerbate myocardialischemia.
In Williams–Beurin syndrome, adhesion of theright or left aortic leaflet edge to the narrowedsinotubular junction can restrict coronary bloodflow into the sinus of Valsalva. The thickenedaortic wall may narrow the coronary artery ori-fice itself. Coronary artery dilation and tortuos-ity due to exposure of the coronary arteries tohigh pre-stenotic pressures and coronary arterystructural changes consistent with elastin arteri-opathy may further directly compromise coronaryflow. Finally, the SVAS impairs coronary diastolicflow, as the pressure in the pre-stenotic regionis lower than in the post-stenotic region duringdiastole.
Surgical therapyThese lesions usually are approached by tran-secting or opening the ascending aorta. Subaorticlesions are then approached across the aortic valve.Resection of discrete subvalvular or supravalvularmembranes is relatively straightforward. Treatmentof fibromuscular tunnel-like stenosis is difficult.Resection of the fibromuscular tissue is limited bypotential damage to surrounding structures such asthe conduction system,mitral valve and the septum.In some instances, repair of a tunnel-like stenosismay require widening of the LV outflow tract witha patch and an aortic valve replacement. SVAS isbest repaired by symmetrical reconstruction of theaortic root using two or three patches to widen theaortic sinuses. In instances where diffuse tubularhypoplasia of the aorta and arch exists, symmetricalreconstruction of the ascending aorta with exten-sion of the patch to the underside of the aortic archis necessary. In some circumstances surgical relief ofcoronary ostial stenosis may be necessary.Post-repair TEE can be used to detect residual gra-
dients and to rule out damage to the mitral valveand ventricular septum. In particular, the presenceof a small VSD should be ruled out.The anesthetic and post-CPB management of
patients with aortic stenosis is discussed in detail inChapter 5.
Single ventricle lesionsAs previously discussed, some single ventriclelesions are amenable to a two-ventricle repair

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 225 — #59
Congenital Heart Disease 225
or
(a)
(d) (e)
(b) (c)
Fig. 6.28 Diagram illustrating the sequence of repairsin the surgical staging of hypoplastic left heart syndrome(HLHS) to a fenestrated lateral tunnel Fontan.(a) Hypoplastic left heart syndrome (HLHS). (b) Initialrepair involving atrial septectomy, Damus–Kaye–Stansel(DKS) anastomosis of main pulmonary artery toascending aorta, homograft augmentation of the aorticarch, and a right modified Blalock–Taussig shunt (BTS)to supply pulmonary blood flow. (c) Initial repairinvolving atrial septectomy, DKS anastomosis of mainpulmonary artery to ascending aorta, homograft
augmentation of the aortic arch, and a right ventricleto pulmonary artery conduit to supply pulmonaryblood flow. (d) Superior cavopulmonary shunt orbidirectional Glenn (BDG). The right modified BTShas been taken down and ligated. (e) The completedtotal cavopulmonary connection or Fontan procedure.A lateral tunnel Fontan with a fenestration is shown.The small arrows indicate flow from the systemicvenous baffle to the common pulmonary venousatrium causing a small right-to-left (R–L)physiologic shunt.
while other require a staged approach to a Fontanprocedure (Fig. 6.28a–e). Single ventricle lesionsamenable to two-ventricle repair include trun-cus arteriosus, severe neonatal aortic stenosis,interrupted aortic arch and TOF with PA. Othersingle ventricle lesions such as TA and HLHSrequire a staged approach to the Fontan procedure.PA/IVS is an example of a single ventricle lesionthat is occasionally amenable to a two-ventriclerepair.
There are three phases in the single ventri-cle pathway: the initial physiology, the superiorcavopulmonary shunt (generally a bidirectionalGlenn (BDG) shunt), and the completed Fontanprocedure that creates a total cavopulmonaryconnection (TCPC). During each of these phasesthree physiologic goals must be achieved:• There must be a reliable source of an appropriatequantity of pulmonary blood flow. The appropri-ate quantity is the quantity that is sufficient to

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 226 — #60
226 Chapter 6
prevent hypoxemia but not so large as to causePVOD. The presence of PVOD is a contra-indicationto completion of the Fontan procedure.• There must be unobstructed delivery ofpulmonary venous blood to the systemic ventricle.• Theremust be an unobstructed pathway from thesystemic ventricle to all segments of the aorta.
Single ventricle pathway,initial proceduresThe initial palliative procedures described here areapplicable to any patient with single ventricle phys-iology. Most patients require multiple initial pro-cedures; rarely a patient may not require anyinitial procedure before proceeding to a superiorcavopulmonary shunt.
Initial procedures to optimize pulmonaryblood flowThe following describes the initial approach to opti-mizing pulmonary blood in patients with singleventricle physiology:• Patients with ductal dependant pulmonary bloodflow will require stabilization on PGE1 followed byplacement of a surgical aortopulmonary shunt asdescribed in the section on TOF. In most cases aMBTSwill be placed and the PDA ligated. A superiorcavopulmonary shunt (BDG) cannot be used in theneonatal period as PVR is elevated to point where asupraphysiologic SVC pressure would be necessaryto provide adequate pulmonary blood flow. Morethan 70% of patients with tricuspid atresia (TA)have ductal dependant pulmonary blood flow andrequire a shunt in the newborn period (Fig. 6.29a,band Table 6.10).• Patients with unrestricted pulmonary blood floware at risk for compromise of systemic oxygen deliv-ery due to high pulmonary blood flow in the settingof fixed cardiac output and ultimately for develop-ment of PVOD. These patients need restriction ofpulmonary blood flow:a In patients with high pulmonary blood flow andsignificant intracardiac sources of pulmonary bloodflow (type 1C or 2C TA; see Fig. 6.29 and Table 6.10)the PDA can be allowed to close. In some instancesthis will appropriately limit pulmonary blood flow.More commonly itwill be necessary tomechanically
restrict pulmonary bloodflowand reduceQP:QS andthe volume load on the systemic ventricle by band-ing the PA. The main PA is constricted with a cir-cumferential band. This reduces pulmonary bloodflow and distal PA pressure by creation of a restric-tive lesion. Banding is most effective when PApressure distal to the band is reduced to one-thirdto one-half of systemic blood pressure. Pulmonaryartery bandingmay cause distortion of themain PA.In addition, distortion of branch pulmonary arter-ies may be caused by migration of the band distally.This distortion may complicate or preclude definiterepair. Pulmonary artery banding is accomplishedvia a thoracotomy or a median sternotomy with-out CPB. An excessively tight PA band will severelyreduce pulmonary blood flow and expose the ven-tricle to high afterload. Pulse oximetry has proveduseful during PA banding because arterial desatu-ration precedes hypotension and bradycardia whenbanding is excessive. TEE is valuable in assessingventricular function during PA banding. Ventricu-lar distension may require loosening of the bandor initiation of inotropic support. TEE also allowsthe pressure gradient across the band to be deter-mined. This will help in determining the tightness ofthe band. PA banding is contraindicated in patientswhere aortic blood flow is derived from a restrictiveintracardiac pathway from the systemic ventricle orwhere this pathway is likely to become restrictiveonce the ventricular volume load is reduced by a PAband. These patients require aDamus–Kaye–Stansel(DKS) procedure (see below) to provide an unob-structed pathway to the aorta from the systemicventricle.b The treatment of patients with high pulmonaryblood flow due to major aorto-pulmonary collat-eral arteries (MAPCAs) is discussed in the sectionon TOF/PA.• Rarely the combination of a restrictive VSD andmild PS (type 2B TA; see Fig. 6.29 and Table 6.10)can result in the appropriate quantity of pulmonaryblood flow without intervention.
Initial procedures to optimize pulmonary venousblood flowIn instances where pulmonary venous blood mustcross the atrial septum to reach the systemic

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 227 — #61
Congenital Heart Disease 227
AoPDA
LA
RA
RV
LV
ΙA ΙB ΙC
ΙΙA ΙΙB ΙΙC
AoPA
Ao
PA
LA
RV
RA
Ao
PA
LA
RV
LA
RA
RV
LV LV LV
RA
RA
RV
LV
LAPAPAPA
AoAo
PALA
RA
RV
LV
(a)
(b)
Fig. 6.29 Classification of tricuspid atresia. (a) Type 1:tricuspid atresia without transposition of great vessels.Type 1A: pulmonary atresia with pulmonary blood flowvia patent ductus arteriosus or major aortopulmonarycollateral arteries (MAPCAs). Type 1B: small ventricularseptal defect and pulmonary stenosis. Type 1C: largeventricular septal defect and no pulmonary stenosis.
(b) Type 2: tricuspid atresia with dextro-transposition ofthe great vessels. Type 2A: pulmonary atresia withpulmonary blood flow via patent ductus arteriosus orMAPCAs. Type 2B: pulmonary stenosis. Type 2C: nopulmonary stenosis. Ao, aorta; LA, left atrium; LV, leftventricle; PA, pulmonary artery; RA, right atrium; RV,right ventricle.
ventricle the atrial septum must be nonrestrictive.Creating a nonrestrictive atrial septum may occurin the cardiac catheterization laboratory using aRashkind–Miller balloon atrial septostomy. In somecases the septummay be so thick as to require place-ment of a stent. A surgical atrial septectomy to createa nonrestrictive atrial septum (common atrium) canalso be performed at the time of initial palliation inprocedures that require CPB.
Initial procedures to optimize systemic blood flowWhen the pathway to the aorta from the sys-temic ventricle is obstructed (type 2C or 3B TA;see Fig. 6.29 and Table 6.10) or when the LV andproximal/transverse aorta are hypoplastic (as withHLHS) a DKS procedure alone or in conjunctionwith an aortic arch reconstruction (as with HLHS),can be used. The PA is transected just proximal toits bifurcation, and the proximal end of the PA is

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 228 — #62
228 Chapter 6
Table 6.10 Classification of tricuspid atresia.
Type Pulmonaryblood flow
Frequency(%)
Type 1: NRGA 70A No VSD, pulmonaryatresia
↓ 10
B Small VSD, pulmonarystenosis
↓ 50
C Large VSD, nopulmonary stenosis
↔↑ 10
Type 2: D-TGA 30A VSD, pulmonary atresia ↓ 2B VSD, pulmonary stenosis ↔↓ 8C VSD, no pulmonarystenosis
↑↑ 20
Type 3: L-TGA <1A VSD, D-loop ventricles,pulmonary orsubpulmonary stenosis
↓
B VSD, L-loop ventricles,sub-aortic stenosis
↑
D-loop ventricles, right ventricle anterior and rightward;D-TGA, dextro transposition of the great arteries; L-loopventricles, right ventricle anterior and leftward; L-TGA, levotransposition of the great arteries; NRGA, normally relatedgreat arteries; VSD, ventricular septal defect.
re-anastomosed end to side or side to side to theascending aorta. This provides systemic ventricle toaortic continuity (LV to proximal PA to aorta intype 3B TA; RV to proximal PA to aorta in HLHS).In the neonatal period, pulmonary blood flow isthen supplied to the oversewn end of the main PAby a MBTS in patients with type 3B TA or a MBTSor RV to PA conduit in patients with HLHS (seeFig. 6.28).
Management of single ventriclephysiologyThe primary goal in the management of patientswith single ventricle physiology is optimization ofsystemic oxygen delivery and perfusion pressure.This is necessary if end-organ (myocardial, renal,hepatic, splanchnic) dysfunction and failure are
0
5
10
15
20
25
30
35
40
45
50
0 2 4 6 8 10QP:QS
O2
deliv
ery
(mL/
kg/m
in)
300 mL/min/kg
450 mL/min/kg
Fig. 6.30 Graph of systemic oxygen (O2) delivery(mL/kg/min) versus QP:QS for two different systemicventricular outputs (300mL/kg/min and 450mL/kg/min)in single ventricle physiology. In this example oxygenconsumption is assumed to be 9mL/kg/min andSpvo2 = 95%. It is clear that systemic oxygen deliverypeaks just below a QP:QS of 1:1 (line across graph) anddeclines rapidly above or below this narrow peak.
to be prevented. This goal is achieved by balanc-ing the systemic and pulmonary circulations. Theterm “balanced circulation” is used because bothlaboratory and clinical investigations have demon-strated that maximal systemic oxygen delivery (theproduct of systemic oxygen content and systemicblood flow) is achieved for a given single ventri-cle output when QP:QS is at or just below 1:1. Thisrelationship is illustrated in Fig. 6.30. Increases inQP:QS in excess of 1:1 are associated with a progres-sive decrease in systemic oxygen delivery becausethe subsequent increase in systemic oxygen con-tent is more than offset by the progressive decreasein systemic blood flow. Decreases in QP:QS justbelow 1:1 are associated with a precipitous decreasein systemic oxygen delivery because the subse-quent increase in systemic blood flow is more thanoffset by the dramatic decrease in systemic oxygencontent.Since QP:QS is not readily measurable parame-
ter in a clinical setting SaO2 is commonly used assurrogate method of assessing the extent to which

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 229 — #63
Congenital Heart Disease 229
a balanced circulation exists. An arterial saturationof 75–80% is felt to be indicative of a balanced circu-lation. It is important to point out however that anarterial saturation of 75–80% is indicative of aQP:QSat or near 1:1 only if the pulmonary venous satura-tion is 95–100% and the mixed venous saturationis 50–55%. In fact, based on these assumptionsthe equation used to calculate QP:QS in patientswith univentricular physiology: (SaO2–SmvO2)/(SpvO2–SaO2) can be simplified to: 25/(95–SaO2).In this simplified equation SpvO2 is assumed to be95% and the A–V oxygen saturation difference isassumed to 25%. Use of this simplified equationrequires that the FiO2 be at or near 0.21 in orderthat the dissolved oxygen content of the pulmonaryvenous blood can be ignored and an SpvO2of95% used. Unfortunately, an arterial saturation of75–80% can exist at the extremes of QP:QS depend-ing on pulmonary and systemic venous saturation.Specifically, in the presence of a high QP:QS itis possible for there to be inadequate systemicoxygen delivery (systemic venous desaturation, awide Sa–vO2 difference, metabolic acidosis) in thepresence of what is considered to be an adequatearterial saturation of 75–80%. In addition, clini-cally unrecognized episodes of pulmonary venousdesaturation (SpvO2 < 90%) further confoundassessment of QP:QS based on SaO2.Mathematic modeling of univentricular phys-
iology reveals that systemic oxygen delivery(CaO2 × QP) is a complex function of cardiac output(CO), pulmonary venous oxygen content (CpvO2),systemic oxygen consumption (CVO2), and QP:QSdescribed by the equation:
CaO2 × QS = CO× CpvO21+ (QP/QS)
− CVO2QP/QS
Given the complex relationships of the multiplevariables that determine QP:QS and oxygen deliv-ery in patients with univentricular physiology, it isnot surprising that neither SaO2 nor the equation25/(95–SaO2) reliably predicts QP:QS.In fact, SaO2 correlates poorly with QP:QS and
the measurement of SpvO2 and SsvCO2 substan-tially improves estimation of QP:QS. Regressionanalysis demonstrates that SaO2 accounts for 8%of the error in estimating QP:QS while SsvCO2
0
10
20
30
40
50
60
70
0 2 4 6 8 10
QP:QS
SvO
2
300 mL/min/kg
450 mL/min/kg
Fig. 6.31 Graph of systemic Svo2 versus QP:QS for twodifferent systemic ventricular outputs (300mL/kg/minand 450mL/kg/min) in single ventricle physiology. Inthis example oxygen (O2) consumption is assumed to be9mL/kg/min and Spvo2 = 95%. It is clear that Svo2peaks at a QP:QS of 1:1 and declines rapidly above orbelow this narrow peak. Svo2 < 30 is not compatiblewith mitochondrial oxygen delivery making the clinicallyrelevant range even narrower.
and SpvO2 contribute 48% and 44% respectively.Figures 6.30 and 6.31 illustrate the effect of cardiacoutput (450 vs. 300mL/min/kg) on oxygen deliveryand SvO2 as QP:QS varies with SpvO2 = 95% andoxygen consumption = 9mL/min/kg. Figure 6.32illustrates the relationship between systemic oxygendelivery and SaO2. It is clear that while SaO2remains satisfactory over a wide range of QP:QS,SvO2 decreases precipitously outside a narrow rangeof QP:QS near 1.0. Furthermore, Sa–vO2 increasesdramatically once QP:QS > 1.0. It is also clear thata higher cardiac output allows maintenance of sat-isfactory oxygen delivery and SsvCO2 over a widerrange of QP:QS.Any combination of variables which produces a
SsvCO2 < 30% is likely to result in the developmentof anaerobic metabolism. A modification of theoxygen delivery equation can be used to take thisinto accountwhere a threshold level of capillary sat-uration (SatThresh) is defined. Any contributions tooxygen delivery by saturations below this thresholdare ignored, as they do not provide physiologicallyuseful oxygen delivery. As a result a new term

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 230 — #64
230 Chapter 6
0
5
10
15
20
25
30
35
40
45
50
0 20 40 60 80 100SaO2
O2
deliv
ery
(mL/
kg/m
in)
300 mL /min/kg
450 mL /min/kg
Fig. 6.32 Graph of systemic oxygen (O2) deliveryversus SaO2 for two different systemic ventricularoutputs (300mL/kg/min and 450mL/kg/min) in singleventricle physiology. In this example oxygenconsumption is assumed to be 9mL/kg/min andSpvo2 = 95%. Solid line on curve is QP:QS of 1:1. It isclear that systemic oxygen delivery is maximal at or neara Sao2 of 75–80%. However systemic oxygen deliveryfalls off precipitously as Sao2 increases by imperceptibleincrements above this level as QP:QS increases. It is clearthat Sao2 alone can never serve as a surrogate measure ofsystemic oxygen delivery. Figure 6.5 illustrates theminiscule increases in Sao2 that occur as QP:QS exceeds1:1 in single ventricle physiology.
“useful oxygen delivery to the body” defined asD(u)O2 = [(CaO2)(1 – SatThresh)](QS) is utilizedrather than the tradition oxygen delivery DO2 =(CaO2)(QS). A realistic SatThresh would be 30–35%.The oxygen excess factor (Ω) is calculated as
SaO2/(Sa–vO2); it is the inverse of the oxygenextraction ratio. A direct linear relationshipbetween Ω and oxygen delivery exists. This directlinear relationship is independent of SpvO2 andcardiac output; however the slope of this relation-ship increases as oxygen consumption increases.Nonetheless, interventions to improve systemicoxygen delivery will be associated with an increasein measured Ω. This is a clinically useful parameteras it can be obtainedwith a systemic saturation froman arterial blood gas or a pulse oximeter and an SVCsaturation obtained from a venous blood gas drawnfrom a central venous catheter positioned just at orabove the SVC/RA junction.These patients are at risk for subendocar-
dial ischemia because volume overload increases
ventricular end diastolic volume and pressure andbecause run-off of blood into the lower resistancepulmonary circuit reduces aortic diastolic bloodpressure. Under these conditions a small increasein heart rate may reduce subendocardial perfu-sion enough to induce ischemia and ventricularfibrillation.
Anesthetic management,pre-initial repair
Goals1 A continuous infusion of PGE1 is used to main-tain ductal patency in patients with ductal depen-dent blood flow (either systemic or pulmonary).PGE1 can be discontinued in any patient determinedby echocardiogram to have a reliable nonduc-tal source of systemic or pulmonary blood flow.Ductal patency generally produces unrestrictivepulmonary blood flow.2 A target PaO2 of 40–45mmHg and a SaO2 of70–80% is reasonable and is likely to be associatedwith adequate systemic oxygen delivery.3 In single ventricle (SV) patients with unrestrictedpulmonary blood flow control and manipulationof PVR and subsequently of QP:QS is accomplishedmost reliably through ventilatory interventions.Clinically, both hypercarbia in combination with a21% FiO2 to achieve a pH of 7.30–7.35 and normo-carbia in combination with a 17% FiO2 (inspiredN2) can be utilized to increase PVR and reduceQP:QS. Both strategies reduceQP:QS to a comparabledegree versus baseline (21% FiO2 and normocarbia)but hypercarbia results in better systemic oxygendelivery (as determined by a narrower A–V oxygensaturation difference and a higher SaO2/(Sa–vO2)),a higher mean arterial pressure, and a higher cere-bral oxygen saturation (as determined by NIRS).4 Hypercarbia (PaCO2 of 45–55mmHg) can bereliably obtained via alveolar hypoventilation orvia increased inspired carbon dioxide (3% FiCO2).Hypercarbia can be obtained utilizing hypoventila-tion without use of inspired carbon dioxide. Careis taken to assure adequate tidal volumeswithmain-tenance of FRC and avoidance of atelectasis so asnot to induce intrapulmonary shunting and V /Qmismatch resulting in inadvertent hypoxemia. Anappropriate degree of hypercarbia can be obtained

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 231 — #65
Congenital Heart Disease 231
with a tidal volume of 8–12mL/kg, PEEP of 3–5 cmH2O and a respiratory rate of 4–8 breaths/min.Additional PEEP and larger tidal volumes can beused to mechanically limit excessive pulmonaryblood flow. The lower rates are required as theinfant cools and metabolic rate decreases.5 Avoid a high FiO2 unless the PaO2<35–40mmHgand intrapulmonary V /Q mismatch is suspected.6 Because ventilatory interventions are incapableof reducingQP:QS much below 2:1 increased cardiacoutput is often necessary to ensure adequate sys-temic oxygen delivery and CPP in the these patients.The ability to recruit stroke volume with preloadaugmentation in very limited in these patientswith volume overloaded ventricles. Increasing heartrate >140–150 b/min has the potential of initiatingmyocardial ischemia in patients with aortic diastolicblood pressures in the 20–30mmHg range. This isa particular risk in patients with HLHS. Inotropicsupport may be necessary; dopamine in doses of3–5µg/kg/min is usually sufficient to accomplishthese goals.7 Once the chest is open the surgeon can mechani-cally limit pulmonary blood flow and reduce QP:QSby placing a vessel loop around a PA (usually theright). This will often dramatically improve hemo-dynamics. ETCO2 will fall as the ETCO2–PaCO2 gra-dient increases. It is not appropriate to decreaseminute ventilation at this time; in fact it may needto be increased slightly because of the increase inalveolar deadspace. A small increase in FiO2 mayalso be necessary.8 Infants with single ventricle physiology whoarrive in the operating room un-intubated fromthe ICU require special attention. These patientsmay clinically have a balanced circulation butthis occurs in the setting of several factors thatincrease PVR including low lung volumes, increasedinterstitial lung water, and hypoxia pulmonaryvasoconstriction. Following induction, intubationand mechanical lung expansion these patients mayhave a precipitous drop in PVR and immedi-ate compromise of systemic circulation. Despitethis, denitrogenation with 100% oxygen is recom-mended prior to laryngoscopy and tracheal intu-bation so as to prevent hypoxemia during thisinterval. Once the airway is secured the FiO2 can bereduced.
Induction and maintenanceThese patients have tenuous cardiovascular sta-tus with limited cardiovascular reserve. Ventricularfibrillation can be seen in association with lightanesthesia or during routine maneuvers, such asopening the pericardium. Many of them arrive inthe operating room intubated receiving inotropicsupport and PGE1. In the absence of an accu-rate prenatal diagnosis many undergo one or moredays of medical stabilization following an episode ofshock or cardiopulmonary arrest.An IV induction using a high-dose synthetic nar-
cotic technique in combination with amuscle relax-ant is recommended. A benzodiazepine (usuallymidazolam) can be added as tolerated. Inhalationagents are generally poorly tolerated. Pancuroniumis normally utilized. However, in patients with a lowaortic diastolic blood pressure and a high baselineheart rate consideration should be given to use ofone of the muscle relaxants that do not affect heartrate such as vecuronium or cisatracurium so as toavoid iatrogenic subendocardial ischemia.
Post-CPB management,post-initial repair
GoalsAfter the initial repair single ventricle physiol-ogy persists and the same principles described forpre-CPB management hold true with a few notableexceptions:1 After CPB, it is not uncommon for a high PVRto result in reduced pulmonary blood flow andhypoxemia.2 The MBTS or RV to PA conduit may betoo large or too small for prevailing physiologicconditions.3 Ventricular dysfunction may exist due to thelong CPB and DHCA or regional low flow perfu-sion intervals that are necessary to complete thesecomplicated repairs.4 Myocardial and tissue edema may be significantprecluding chest closure.5 Bleeding from long arterial suture lines may besignificant.6 Inhaled pulmonary vasodilators such as NOmay be necessary to improve SaO2 or reduce thetranspulmonary gradient in this patient population.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 232 — #66
232 Chapter 6
This is particularly true in the subgroup of patientswho have repair of partially obstructed pul-monary venous drainage at the time of their initialrepair.Management of the four clinical scenarios present
after initial repair and the appropriate interventionsnecessary are summarized in Table 6.11.
Single ventricle pathway; superiorcavopulmonary shunt, or bidirectionalGlenn (BDG)The BDG (Figs 6.28, 6.33a,b–6.35) directs systemicvenous blood from the SVC directly to the pul-monary circulation. The BDG is normally under-taken at 3–6 months of age at which point the PVRhas decreased to point where pulmonary blood flowcan be provided with systemic venous pressure asthe driving pressure. Patients who have outgrowntheir PA band, RV to PA conduit, or MBTS and havea low SaO2 and patients who are not tolerating theadditional volume on their ventricle with a loose PAband or large MBTS will be staged to a BDG earlierin this interval.The original Glenn shunt involved an end-to-side
anastomosis of the cranial end of the transected SVCto the distal end of the transected right pulmonaryartery (RPA). Both the proximal SVC and RPAwereover sewn. This procedurewas performed through aright thoracotomy without CPB. Currently the bidi-rectional Glenn is used in which the cranial endof the transected SVC is anatomosed end-to-sideto the RPA (which is in continuity with the mainand left PAs) and the cardiac end of the SVC isover sewn. This creates SVC continuity with boththe left and right pulmonary arteries and bidirec-tional pulmonary blood flow. The main PA is oversewn if it is not atretic. Unless the IVC is interruptedwith azygous continuation the azygous vein is lig-ated so that the SVC does not decompress retrogradeto the IVC thereby reducing the quantity of blooddelivered to the PAs. This procedure is performedon CPB through a median sternotomy. The previ-ous aortopulmonary shunt is ligated or the PA bandtaken down.Normally all upper extremity and cerebral venous
drainage reaches the SVC. In some patients withCHD (particularly those with heterotaxy syndrome)
there may be bilateral SVCs that are not in conti-nuity via a connecting vein. In this case a bilateralBDG must be done with one SVC anatomosed end-to-side to the RPA and the other SVC anatomosedend-to-side to the LPA. LPA to RPA continuity ismaintained.The differences between an aortopulmonary
shunt and a BDG are summarized in Fig. 6.33. Themost obvious difference between the two is that fora given cardiac output, SaO2, SpvO2, and SvO2 thevolume load on the systemic ventricle will be twiceas large with an aortopulmonary shunt as it is witha BDG. Effective pulmonary blood flow in the aor-topulmonary shunt and BDG circulations are equal.However, in the aortopulmonary shunt circulationthere is recirculated pulmonary blood (physiologicL–R shunt) while in the BDG circulation there is norecirculated pulmonary blood flow. As a result, achild with a BDG will have the same SaO2 as a childwith an aortopulmonary shunt but with a signifi-cant reduction in the volume load on the systemicventricle.Modifications of the BDG have been devised to
potentially simplify the conversion to a Fontan. Thehemi-Fontan refers specifically to a procedure inwhich atriopulmonary anastomosis is constructedbetween the dome of the RA at the RA/SVC junc-tion and the inferior surface of the RPA. A Gore-Texbaffle or dam is used to supplement the centralPA area and to isolate the cavopulmonary connec-tion from the RA. Anothermodification (incorrectlycalled a hemi-Fontan) involves creation of a doublecavopulmonary anastomosis. The cranial end of thedivided SVC is anastomosed to the superior surfaceof the RPA. The cardiac end of the divided SVC isanastomosed to the inferior surface of the RPA. Theinternal orifice of the SVC is closed with a Gore-Texpatch (see Fig. 6.35).
Anesthetic management, pre-superiorcavopulmonary shunt
GoalsThe principles outlined in section on managementof single ventricle physiology before and after theinitial repair apply here (see Table 6.11). By the ageof 3–6months when these infants present for their

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 233 — #67
Congenital Heart Disease 233
Table 6.11 Management of single ventricle physiology.
Clinical presentation Physiology Management
SaO2 75–80%Sa-vO2 25–30%BP > 60/30
Balanced flowQP:QS = 0.7–1.5:1
No intervention
SaO2 > 85–90%Sa-vO2 35–40%BP < 60/30Diastolic BP < 15–25 withMBTS; likely higher withRV–PA conduit
OvercirculatedQP:QS > 2–3:1Causes:Low PVRLarge MBTS or RV–PA conduitResidual arch obstruction
Raise PVR:Controlled hypoventilationMild acidosisLow FiO2 (0.17–0.19)
Increase systemic O2 delivery:Afterload reductionInotropic supportHematocrit >40%
Surgical intervention:Clip MBTS or RV–PA conduitRevise arch
SaO2 < 65–75%Sa–vO2 25–30%; but SvO2 likelyless than critical value of 30%BP > 70/40Diastolic BP > 40
UndercirculatedQP:QS < 0.7:1Causes:High PVRSmall MBTS or RV–PA conduitPulmonary venousdesaturation withunderestimation of actualQP:QS
Lower PVR:Controlled hyperventilationAlkalosisSedation/paralysisAggressively treat atelectasis(pulmonary venousdesaturation)
Consider NO
Increase systemic O2 delivery:Inotropic support
Surgical intervention:Revise MBTS or RV–PA conduit
SaO2 < 70–75%Sa-vO2 35–40% and SvO2 likelyless than critical value of 30%BP < 60/30
Low cardiac outputCauses:Ventricular dysfunction• Myocardial ischemia• Depressed contractility• Afterload mismatch(residual arch obstruction)• AV valve regurgitation
Minimize O2 consumption:Sedation/paralysis
Inotropic support/afterloadreduction
Surgical intervention:Repair AV valveRevise arch
Consider mechanical support:• Post-cardiotomy support• Bridge-to-transplantation
AV, atrioventriculat; BP, blood pressure; MBTS, modified Blalock–Taussig shunt; PVR, pulmonaryvascular resistance; RV–PA, right ventricle–pulmonary artery.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 234 — #68
234 Chapter 6
Flow(L /min/m2)
Flow(L /min/m2)
Pulmonary veins Vena cavae98
2 2
4
80
80
LA RA
65
65
RVRVRV
8080
= Saturation (%)
PA
22Ao–PAShunt
LV
Flow(L /min / m2)
Flow(L /min / m2)
Pulmonary veins IVC98
1 1
2
80
80
LA RA
65
65
RVRV
SVC65
80
= Saturation (%)
PA1
2
LV
AoAo
RV
(a) (b)
Fig. 6.33 (a) Depiction of saturations and blood flowsin tricuspid atresia with a nonrestrictive atrial septaldefect (ASD), a hypoplastic right ventricle (RV), andpulmonary atresia palliated with an aortopulmonaryshunt. Complete mixing occurs at the atrial level. The leftventricle (LV) is volume overloaded in this parallelcirculation to provide pulmonary blood flow. QS and QPare 2 L/min/m2 and the arterial saturation is 80%(QP:QS = 1:1.) (b) Depiction of saturations and bloodflows in tricuspid atresia with a nonrestrictive ASD,a hypoplastic RV, and pulmonary atresia palliated with abidirectional superior cavopulmonary shunt. Completemixing occurs at the atrial level. The LV is not volumeoverloaded in this series circulation. QS is 2 L/min/m2,
and QP is 1 L/min/m2; QP:QS = 0.5:1.0. Nonetheless,cardiac output and arterial saturation are identical to thepatient palliated with the aortopulmonary shunt. This isbecause arterial saturation in complete mixing isdetermined by the relative volumes and saturations ofsystemic and pulmonary venous blood. In this instance,QS and the volume of systemic venous blood reachingthe right atrium (RA) are not equal because half of QShas been diverted to become pulmonary venous blood.As a result, QP:QS is deceptive here. Ao, aorta; IVC,inferior vena cava; LA, left atrium; LV, left ventricle;PA, pulmonary artery; RA, right atrium; RV, rightventricle; SVC, superior vena cava.
cavopulmonary shunt they have generally grownand gained weight such that their QP:QS is likely tobe 1.0–1.5:1. As a result these patients aremuch lessprone to compromise of systemic oxygen deliveryby an excess of pulmonary blood flow.
Induction and maintenanceAn IV induction is preferred in these patients.Vascular access may be difficult, as many of thesepatients have prolonged ICU stays after their initialrepair. In addition, many of these patients are toler-ant to opioids and benzodiazepines following theirICU stay. This should be considered if premedicationis planned prior to IV placement.
Post-CPB management, post-superiorcavopulmonary shunt
Goals1 Maintain heart rate, contractility, and preloadto maintain cardiac output. Decreases in cardiacoutput will reduce IVC saturation. In BDG physi-ology where there is mixing of IVC and pulmonaryvenous blood in a common atrium this will reducearterial saturation.2 Low PpvO2 saturation will produce a low SaO2.Maneuvers to reduce V /Q mismatch and intra-pulmonary shunt should be undertaken. A highFiO2 may be necessary in the presence of significantV /Q mismatch.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 235 — #69
Congenital Heart Disease 235
Fig. 6.34 The anatomy of a completed bidirectionalsuperior cavopulmonary shunt. The cephalad portion ofthe superior vena cava (SVC) is anastomosed end-to-sideto the right pulmonary artery. The right pulmonaryartery is in continuity with the left pulmonary artery.A previously modified Blalock–Taussig shunt (rightsubclavian to right pulmonary artery with interposedGore-Tex graft) is ligated and the subclavian artery isbeing retracted. The azygous vein is also ligated. Thecardiac portion of the SVC is over sewn.
3 Normocarbia should be maintained. Mean air-way pressure should be kept at theminimal compat-ible with delivery of an adequate tidal volume andlung expansion. High mean airway pressure willmechanically limit the nonpulsatile pulmonaryblood flow. This can usually be accomplished witha relatively large tidal volume (10–12mL/kg), slowrespiratory rates (10–15 breaths/min), and shortinspiratory times (I:E of 1:3–1:4). PEEP should beused with caution.4 A central line placed in the internal jugular (IJ)will measure SVC pressure, which equals meanpulmonary artery pressure (mPAP) following aBDG. A surgically placed atrial line will mea-sure common atrial pressure. The transpulmonarypressure gradient (TPG) (mPAP – common atrialpressure) is usually <10mmHg with appropriateventilation. AmPAP of 12–18mmHg is usually seenin presence of good systemic ventricular function.
Azygos vein
Patch
Fig. 6.35 The anatomy of a double cavopulmonaryanastomosis with internal patch closure of the cardiacanastomosis. Both the cardiac and cephalic portions ofthe superior vena cava (SVC) are in continuity with theright pulmonary artery. The right pulmonary artery is incontinuity with the left pulmonary artery, and the mainpulmonary artery is divided and over sewn. Inferiorvena cava (IVC) blood is prevented from reaching thepulmonary arteries due to a patch occluding the rightatrium (RA)–SVC junction. The physiology is identicalto that in Figs 6.31 and 6.32.
5 Inotropic support of the systemic ventriclemay be necessary due to ventricular dysfunctioninduced by chronic volume overload and CPB.Dopamine (3–5µg/kg/min) is useful. Milrinone(0.5–1.0µg/kg/min) is useful for those patients whohave high SVR and hypertension.6 Inhaled pulmonary vasodilators such as NOgenerally do not improve SaO2 or reduce thetranspulmonary gradient in this patient popula-tion. The exception to this may be the subgroupof patients who have repair of partially obstructedpulmonary venous drainage at the time oftheir BDG.7 The most likely cause of a low SaO2 follow-ing a BDG is low cardiac output with a low

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 236 — #70
236 Chapter 6
IVC saturation. TEE will help delineate the cause(ventricular dysfunction, hypovolemia, AV valvedysfunction). If a lowSaO2 persists despite optimiza-tion of ventricular function, consideration should begiven to causes of reduced pulmonary blood flowsuch as a stenotic anastomosis or the presence ofdecompressing venous collaterals from the SVC tothe IVC.These patients will have a SaO2 of 75–80%,
similar to that prior to their BDG. The QP:QS rangesfrom 0.5–0.7:1 and as a result there will be the acutereduction in volume load on the systemic ventricleas shown in Fig. 6.33. There is an acute increase inSVC pressure and presumably in intracranial pres-sure (ICP). The volume load reduction and elevatedSVC pressure are believed to contribute to the initialsystemic hypertension and postoperative irritabil-ity that is commonly seen in these patients. Themajority of pulmonary blood flow will be suppliedvia venous blood from the brain; the largest con-tributor to venous drainage from the upper body.Hyperventilation and hypocarbia, while beneficialin reducing PVRwill also reduce cerebral blood flowand cerebral venous drainage. Maintaining normo-carbia following BDG has been demonstrated toprovide maximal QP:QS and SaO2. These patientstend to have a large ETCO2–PaCO2 gradient due toincreased physiologic dead space. An increased por-tion of the lung in these patients is ventilated butnot perfused due to the low PA driving pressure(SVC pressure).Attention is focused on the TPG that, in normal
patients, is defined as the mPAP–LAP. In BDGpatients, themPAP= SVC pressure. In BDG patientsthe equivalent of a LAP or pulmonary venous atrialpressure is the common atrial pressure. A commonatrium exists in these patients because the atrialseptectomy creates a nonrestrictive communicationbetween the LA and RA.
Definitive repair: the Fontanprocedure or total cavopulmonaryconnection (TCPC)
Fontan physiologyThe Fontan procedure is generally performedin staged patients at 2–3 years of age. Fontan
physiology is a series (“normal”) circulation thatcan be described as follows:• There is one ventricle with sufficient diastolic,systolic, and AV valve function to support systemiccirculation. This ventricle must in turn:a Be in unobstructed continuity with theaorta.b Be in unobstructed continuity with pulmonaryvenous blood.• There is unobstructed delivery of systemicvenous blood to the pulmonary circulation (totalcavopulmonary continuity).In the absence of any residual physiologic
intracardiac or intrapulmonary R–L shunting thesepatients should have a normal SaO2. It is oftenstated that pulmonary blood flow is passive andgradient driven (systemic venous pressure > meanPA pressure > pulmonary venous atrial pressure).In fact, the systemic ventricle generates the energynecessary to provide flow through the pulmonarycapillary bed because the systemic vascular bed andpulmonary vascular bed are in continuity withoutan intervening atria and ventricle to provide reser-voir and pumping capacity. As a result, the singleventricle in a series Fontan circulation is faced withhigher afterload then the systemic ventricle in atwo-ventricle series circulation.The Fontan procedure was first performed in
1968 and was applied to patients with TA. Theoriginal operation included a Glenn shunt, whichdrained the SVC directly into the distal right PA.The proximal end of the RPAwas joined to the rightatrial appendage via an aortic valve homograft anda pulmonary valve homograft valve was placed atthe IVC–RA junction. The main PA was ligated andthe ASD was closed. Subsequently, creation of theGlenn shunt and placement of homograft valves atthe RA–PA and IVC–RA junctions were eliminatedresulting in creation of a direct atriopulmonaryconnection.Since then, many modifications have been
described. Despite the modifications, the goal of theprocedure remains the same: to provide deliveryof all systemic venous blood directly to the pul-monary arteries without the benefit of the reservoiror pumping capability of a ventricle. This requirestotal cavopulmonary continuity either directly or

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 237 — #71
Congenital Heart Disease 237
Fig. 6.36 Total cavopulmonary connection using anintra-atrial lateral tunnel or baffle. The tunnel isprosthetic graft material such as Gore-Tex. A fenestrationhas been placed in this prosthetic material allowing aphysiologic right-to-left (R–L) shunt to exist whenbaffle pressure exceeds common (pulmonary venous)atrial pressure.
via the system venous atrium. Currently, the mostcommonly performed procedures are the lateraltunnel and extracardiac Fontan (Figs 6.28, 6.36and 6.37). The lateral tunnel procedure avoidsincorporating any substantial volume of atrium inthe cavopulmonary pathway while the extracar-diac procedure does not incorporate any atrium.These procedures are referred to as TCPCs. Overtime in atriopulmonary connections elevated sys-temic venous pressure leads to atrial dilatation. Theatrium often expands to a volume as large as 300–500mL. This is a source of stasis and a nidus for atrialarrhythmias. In theory, the extracardiac proceduremay offer additional protection from developmentof atrial arrhythmias due to a lack of suture lines inatrium.Contraindications to the Fontan procedure
include: early infancy, PVR > 4Woodunits/m2,severe PA hypoplasia, an ejection fraction (EF) <
25–30%, and a ventricular diastolic pressure >
25mmHg. The majority of lesions felt in the pastto be relative contraindications to the Fontan pro-cedure such as AV valve regurgitation/stenosis or
Fig. 6.37 Total cavopulmonary connection using anextracardiac conduit or baffle. The conduit is prostheticgraft material such as Gore-Tex. A small side-to-sideanastomosis between a fenestration in the conduit anda fenestration in the atrial wall can be placed allowinga physiologic right-to-left (R–L) shunt to exist whenbaffle pressure exceeds common (pulmonary venous)atrial pressure.
focally narrowed or distorted pulmonary arteriescan now be corrected at the time of the Fontanprocedure.Use of the staged single ventricle pathway
results in reduced morbidity and mortality as com-pared to the acute transition from single ventri-cle to Fontan physiology. As previously described,the staged pathway makes use of a bidirectionalcavopulmonary shunt procedure before the Fontanprocedure. Use of the cavopulmonary shunt at3–6months of age allows early reduction in thevolume overload that accompanies univentricularphysiology. This allows systemic ventricular volumeload to be reduced to normal and allows remodelingof the ventricle at lower end-diastolic volume.Acute reduction of systemic ventricular volume
in the univentricular heart results in impaired ven-tricular compliance because wall thickness doesnot regress as quickly as ventricular volume. Theresult is impaired ventricular diastolic function andelevated end-diastolic pressure. This will impedepulmonary venous return, which is a liability in theFontan procedure, because this will subsequently

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 238 — #72
238 Chapter 6
reduce pulmonary blood flow. A low cardiac outputstate will result because systemic ventricular outputcan only equal the quantity of blood that transversesthe pulmonary vascular bed. The impaired ventric-ular diastolic function that accompanies acute ven-tricular volume reduction is better tolerated in BDGor hemi-Fontan physiology than in Fontan phys-iology. When there is impairment of pulmonaryvenous return after the BDG or hemi-Fontan,blood from the IVC will continue to provide sys-temic ventricular filling and cardiac output at alower pressure than that required to traverse thepulmonary bed.A risk of the staged procedures is the development
of pulmonary arteriovenous malformations. Theseare the result of diversion of hepatic venous bloodflow (IVC) blood to a systemic capillary bed beforedelivery to the pulmonary capillary bed as occursin the bidirectional cavopulmonary shunts. This isgenerally not a problemwhen the BDG is eventuallyconverted to a Fontan.
Fenestrated FontanWith Fontan physiology, increased impedance tosystemic venous blood flow across the pulmonarycapillary bed will result in decreased delivery ofblood to the pulmonary venous atrium, systemicventricle, and aorta producing a low cardiac out-put state with a normal or near normal SaO2. Thisincreased impedance is not uncommon in the initialdays and weeks following Fontan surgery. Attemptsto increase cardiac output by increasing systemicvenous pressure may result in development ofrefractory pleural effusions and ascites. In manyinstitutions a 4mm hole or fenestration is inten-tionally left in cavopulmonary pathway or baffle.This allows systemic venous blood to “pop-off”into the pulmonary venous atrium and ultimatelyinto the systemic ventricle and aorta. This physi-ologic R–L shunt allows maintenance of systemiccardiac output at the expense of SaO2. This fenestra-tion can be easily closed in the cardiac catheteriza-tion laboratorywith an occlusion device at later datefollowing demonstration of adequate hemodynam-ics, gas exchange, and cardiac output with balloonocclusion of the fenestration.
Anesthetic management, pre-Fontan
GoalsThe principles outlined in the section on manage-ment of BDG physiology after CPB generally applyhere. At 2–3 years of age patients with a supe-rior cavopulmonary shunt (BDG) generally have astable cardiovascular systemwith a SaO2 of 75–80%unless there are significant decompressing venouscollateral vessels from the SVC to either the IVCor pulmonary venous system. These are usuallyaddressed by coil occlusion in the cardiac catheter-ization laboratory prior to the Fontan. While thesepatients will tolerate an inhalation induction froma cardiovascular standpoint it should be recognizedthat several factors might make a pure inhalationinduction difficult:• Venous congestion of the head and tongue due toa relatively high SVC pressure.• Coughing, breath holding, or any other cause ofhigh intrathoracic pressure will cause almost com-plete cessation of pulmonary blood flow. Almostimmediate arterial hypoxemia will occur.• With a QP:QS of 0.5–0.7:1.0 the speed of aninhalation induction will be slow.
Induction and maintenanceAn IV induction is preferred. Consideration shouldbe given to premedication as these patients andtheir families generally have had multiple hospitalexposures for check-ups and procedures. In addi-tion, many of these patients are tolerant to opioidsand benzodiazepines following neonatal and sub-sequent exposure. This should be considered ifpremedication is planned prior to IV placement.
Post-CPB management,post-Fontan procedure
Goals1 Maintain heart rate, contractility, and preload tomaintain cardiac output. In Fontan patients witha fenestration or intrapulmonary shunt decreasesin cardiac output will reduce SvO2 and SaO2. SvO2can be easily determined using a sample drawn froma central venous catheter.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 239 — #73
Congenital Heart Disease 239
2 Low pulmonary venous saturation will producea low SaO2. Maneuvers to reduce V /Q mismatchand intrapulmonary shunt should be undertaken.A high FiO2 may be necessary in the presence ofsignificant V /Q mismatch.3 Ventilation and acid-base management shouldbe optimized to keep PVR low. Mean airway pres-sure should be kept at the minimal compatiblewith delivery of an adequate minute ventilationand lung expansion. High mean airway pressurewill mechanically limit the nonpulsatile pulmonaryblood flow. This can usually be accomplished witha relatively large tidal volume (10–12mL/kg), slowrespiratory rates (10–15 breaths/min), and shortinspiratory times (I:E of 1:3–1:4). PEEP should beused with caution.4 A central line placed in the IJ will measure caval(baffle) pressure which equals mPAP following aFontan. A surgically placed atrial line will measurecommon atrial pressure. The TPG (mPAP – commonatrial pressure) is usually<10mmHgwith appropri-ate ventilation. A mPAP of 15–18mmHg is usuallyseen in the presence of good systemic ventricularfunction.5 Inotropic support of the systemic ventriclemay be necessary due to ventricular dysfunctioninduced by chronic volume overload and CPB.Dopamine (3–5µg/kg/min) is useful. Milrinone(0.5–1.0µg/kg/min) is useful for those patientswho have high SVR and afterload/contractilitymismatch.6 Inhaled pulmonary vasodilators such as NOgenerally do not improve SaO2 or reduce thetranspulmonary gradient in this patient popula-tion. The exception to this may be the subgroupof patients who have repair of partially obstructedpulmonary venous drainage at the time of theirFontan.Themanagement goals following the Fontan pro-
cedure are summarized in Table 6.12. Aswith a BDGpatient, attention is focused on the transpulmonarygradient (TPG). In Fontan patients themPAP=CVP.A CVP in a Fontan patient will measure pres-sure in the caval portion of the cavopulmonaryconnection and is commonly called a baffle pres-sure. As with a BDG patient in Fontan patients
the equivalent of a LAP is the common atrialpressure. In Fontan patients the pressure in thecavopulmonary connection can be obtained via apercutaneously placed central venous catheter or asurgically placed transthoracic baffle catheter. Thecommon atrial pressure is obtained via a surgicallyplaced transthoracic catheter. Thus in patients witha Fontan, the TPG= CVP – common atrial pressure.Low pulmonary blood flow produces low car-
diac output in this series circulation. The systemicventricle can only pump the volume of bloodthat is delivered to it across the pulmonary vascu-lar bed. This differs from the situation after superiorcavopulmonary shunts because, in these patients,there is a source of blood supply (IVC blood) tothe systemic ventricle that does not cross the pul-monary bed. It should be emphasized that in aFontan patient, low cardiac output will not resultin a low SaO2 unless there are significant sources ofintrapulmonary or intracardiac (fenestration, baffleleak) physiologic R–L shunting. When low cardiacoutput is due to ventricular dysfunction, common(pulmonary venous) atrial hypertension will leadto development of pulmonary edema and physio-logic R–L intrapulmonary shunting. This situationis analogous to a normal patient with series circula-tion and no intracardiac lesions. Low cardiac outputin a normal patient will result in a low SaO2 only ifa significant quantity of intrapulmonary R–L shuntexists and low cardiac output produces a low SvO2.The presence of a fenestration or baffle leak willexacerbate this SaO2 decrease in the Fontan patient.It is commonly stated that early tracheal extu-
bation and spontaneous ventilation enhance pul-monary gas exchange and hemodynamics in Fontanpatients. It must be emphasized that low lung vol-umes, hypercarbia, and hypoxemia will negate anyadvantage obtained by spontaneous ventilation.
Tricuspid atresia
AnatomyIn Tricuspid atresia (TA), there is agenesis of thetricuspid valve and no communication betweenthe RA and the hypoplastic RV (the tricuspidvalve is embryologically part of the RV). Anatomic

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 240 — #74
240 Chapter 6
Table 6.12 Management of Fontan physiology.
Physiology Clinical presentation Management
Low pulmonary blood flow andinadequate preload delivery tosystemic (common) atriumTPG 10mmHg
Causes:Baffle obstructionPulmonary artery obstructionPulmonary vein obstructionPremature baffle fenestration closure
No fenestration or prematurefenestration closureSaO2 95–100%Sa-vO2 > 35–40%Baffle pressure > 20mmHgCommon atrialpressure < 10mmHg
HypotensionTachycardiaPoor distal perfusionMetabolic acidosis
Fenestration patent or baffleleak presentSaO2 75–80%Sa-vO2 > 35–40%Baffle pressure > 20mmHgCommon atrialpressure < 10mmHg
HypotensionTachycardiaPoor distal perfusionMetabolic acidosis
Volume replacement to keep bafflepressure stableReduce PVRCorrect acidosisInotropic supportAfterload reductionConsider catheterization intervention toopen or create baffle fenestration
Systemic ventricular dysfunctionTPG = 5–10mmHg
Causes:Systolic dysfunctionDiastolic dysfunctionAV valve regurgitation/stenosisLoss of AV synchronyAfterload/contractility mismatch
No fenestration or prematurefenestration closureSaO2 85–90%Sa-vO2 > 35–40%Baffle pressure > 20mmHgCommon atrialpressure > 15mmHg
Pulmonary edemaHypotensionTachycardiaPoor distal perfusionMetabolic acidosis
Fenestration patent or baffleleak presentSaO2 70–75%Sa-vO2 > 35–40%Baffle pressure > 20mmHgCommon atrialpresure > 15mmHgPulmonary edemaHypotensionTachycardiaPoor distal perfusionMetabolic acidosis
Volume replacement to keep bafflepressure stableCorrect acidosisPEEP may be necessary for pulmonaryedemaInotropic supportAfterload reductionProvide AV synchrony(antiarrhythmics/pacing)Mechanical support (post-cardiotomysupport or bridge to transplantation)Surgical intervention (takedown to BDG)
AV, atrioventricular; BDG, bidirectional Glenn procedure; PVR, pulmonary vascular resistance; TPG, transpulmonarypressure gradient.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 241 — #75
Congenital Heart Disease 241
classification is based on the presence or absence ofTGA, the extent of PS or atresia, and the size of theVSD. This classification and the frequency of the dif-ferent lesion types are summarized in Fig. 6.29 andTable 6.10. Approximately 70% of patients with TAare type 1 and 30% are type 2. Type 3 lesions arevery rare. Fifty percent of all TA patients are type 1B.
PhysiologyTA is single ventricle physiology lesion. Thesepatients are staged to a Fontan procedure. TA isa complex shunt with complete obstruction to RVinflow and variable obstruction to RV outflow.There is a communication (ASD or patent FO)which results in an obligatory R–L shunt at theatrial level with complete mixing of systemic andpulmonary venous blood in the LA. When theASD or FO is restrictive, there will be a largeright atrial to LAP gradient. This will result in poordecompression of the RA and systemic venous con-gestion. Pulmonary blood flow can be providedby a downstream shunt from one or both of thefollowing sources:• Intracardiac. The pathways are described inTable 6.1. This downstream shunt may be simple(VSD without PS), complex (VSD with PS), or com-plex with complete obstruction (pulmonary atresiawith or without a VSD).• Extracardiac. This is generally a PDA but in olderpatients MAPCAs may have developed. When pul-monary atresia exists (types 1A and 2A) thesesimple shunts are the sole source of pulmonaryblood flow.The quantity of pulmonary blood flow associated
with each type of TA is summarized in Table 6.10.In single ventricle lesions the degree of cyanosis
will be determined largely by QP:QS. Therefore,patients with a QP:QS < 1 due to stenotic or atreticpulmonary outflow tracts, restrictive VSDs, or bothwill be more cyanotic than their counterparts withnormal or increased pulmonary blood flow. TAimposes a volume load on the LV, and increased pul-monary blood flow produces an even larger LV vol-ume load. Therefore, patientswith TA and increasedpulmonary blood flow are likely to presentwith CHF. Furthermore, patients with increasedpulmonary blood flow are at risk to develop PVOD.
Surgical therapyMore than 70% of neonates with TA have ductaldependant pulmonary blood flow and require aMBTS in association with PDA ligation. This canoften be done off-CPB through a median ster-notomy. Following initial repair, TA patients pro-ceed to a superior cavopulmonary connection orBDG at age 3–6months and then on to theFontan procedure at 1–2 years of age as previouslydescribed.
Anesthetic management
GoalsThese patients are initially managed accordingto the principles described in the section onManagement of single ventricle physiology, pre-initial repair (see Table 6.11). Subsequent man-agement for the superior cavopulmonary shuntand Fontan procedure is described in later portionsof the section on Management of single ventriclephysiology.
Post-CPB managementThese patients are managed according to the prin-ciples described in the section on Management ofsingle ventricle physiology, post-CPB management(see Table 6.11). Subsequent management for thesuperior cavopulmonary shunt and Fontan proce-dure is described in later portions of the section onManagement of single ventricle physiology.
Hypoplastic left heart syndrome
AnatomyPatients with hypoplastic left heart syndrome(HLHS) have hypoplasia of all left heart structures.In the most severe form, mitral and aortic atresiawith hypoplasia of the LA, LV, ascending aorta, andaortic arch (including coarctation) are present. Dis-tal aortic blood flow occurs via the PDA. Proximalaortic blood flow and coronary blood flow occurby retrograde filling of a tiny ascending aorta viathe PDA (Figs 6.28 and 6.38). This unique varia-tion of single ventricle physiology in HLHS patientsputs them at increased risk for development ofmyocardial ischemia.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 242 — #76
242 Chapter 6
Ao
LA
LVRA
RV
Fig. 6.38 Anatomy of hypoplastic left heart syndrome(HLHS). There is severe mitral stenosis/atresia, leftventricular hypoplasia, aortic valve atresia, andhypoplasia of the ascending aorta and transverseaortic arch. Pulmonary and systemic blood flows areboth delivered via the right ventricle. Aortic blood flowis provided via a large ductus arteriosus. There isantegrade flow from the patent ductus arteriosus (PDA)to the descending aortic and retrograde flow to theproximal aortic arch and cerebral circulation. Thecoronary arteries are perfused retrograde via the tinyascending aorta. The left ventricle (LV) is diminutive. Aoaorta; LA, left atrium; LV, left ventricle; RA, right atrium;RV, right ventricle.
PhysiologyThe HLHS is a ductal dependant single ventri-cle physiology lesion. These patients are stagedto a Fontan procedure. HLHS is a complex shuntwith complete obstruction to outflow. There is acommunication (ASD or patent FO) and a com-plete or near complete obstruction to LA outflow(mitral atresia or severe mitral stenosis) and LV out-flow (aortic atresia or severe aortic stenosis). Thisresults in an obligatory L–R shunt at the atrial levelwith complete mixing of systemic and pulmonaryvenous blood in the RA and ventricle. When theASD or FO is restrictive, there will be a large leftatrial to right atrial pressure gradient. This willresult in poor decompression of the LA, pulmonaryvenous congestion and pulmonary hypertension.These patients need emergency decompression ofthe LA (pulmonary venous chamber) and medical
stabilization prior to surgery. This requires trans-atrial stent placement in the cardiac catheterizationlaboratory.Systemic blood flow is provided by a simple
downstream shunt (PDA). The shunt at the level ofthe PDA is a dependent shunt with net systemic andpulmonary blood flow determined by the ratio ofsystemic to PVR. Low PVR relative to SVRwill allowrun-off of blood into the pulmonary circuit compro-mising systemic perfusion. Flow to the ascendingaorta, coronary arteries, and arch vessels are sup-plied entirely (aortic atresia) or almost entirely(severe mitral and aortic stenosis) retrograde fromthe PDA. Flow to the descending aorta is antegradefrom the PDA. Closure of the PDA in infants withHLHS terminates coronary and systemic blood flowand results in immediate cardiovascular collapse.PGE1 therapy is lifesaving for these patients.
Surgical therapyPatients with HLHS are staged along the single ven-tricle pathway to a Fontan procedure (see Fig. 6.28).The initial procedure utilizing a MBTS is com-monly referred to as a Norwood stage 1. The initialprocedure utilizing an RV to PA conduit is com-monly referred to as a modified Norwood stage 1or a Sano procedure. As discussed previously itmust incorporate procedures to meet the objec-tive necessary at each stage in the single ventriclepathway:• A DKS anastomosis in conjunction with anaortic arch reconstruction/coarctation repair utiliz-ing homograft or pericardial tissue is necessary toprovide an unobstructed systemic ventricle (RV) toaortic connection.• An atrial septectomy is performed to allow unob-structed delivery of pulmonary venous blood fromthe LA to the systemic RV via the RA.• A MBTS (usually 3.5mm Gore-Tex conduit) orRV to PA conduit (usually a 5 or 6mm valvelessGore-Tex conduit) is created to provide pulmonaryblood flow.The physiology of the MBTS and of the RV to PA
conduit as a source of pulmonary blood flow differin some important aspects:• With a MBTS blood is distributed to the pul-monary circulation after it has entered the systemic

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 243 — #77
Congenital Heart Disease 243
arterial tree (from the innominate artery to the PA)while with a Sano conduit blood is distributed tothe pulmonary circulation before it has enteredthe systemic arterial tree (from the RV to the PA;much like a double outlet RV). As a result, for agiven cardiac output and QP:QS, the pulse pres-sure is wider and the aortic diastolic blood pressurelower in patients with a MBTS. The higher diastolicblood pressure obtained with the Sano shunt mayprovide better cerebral, coronary and splanchnicperfusion.• The Sano shunt requires creation of a small rightventriculotomy. The RV is the systemic ventricleand the long-term functional consequences of thisventriculotomy are unknown.• The Sano conduit is valveless a resulting in somepulmonary insufficiency. The volume load on theRV induced by this is small and probably off-set by the fact that Sano shunt patients have aslightly lower QP:QS and volume load than MBTSpatients.Following stage 1 repair, HLHS patients pro-
ceed to what is often called stage 2 – a superiorcavopulmonary connection (BDG or hemi-Fontan)at age 3–6months – and then on to the Fontanprocedure at 1–2 years of age. Patients with an RV toPA conduit generally have their superior cavopul-monary connection at an earlier age than childrenwith a MBTS as they have a lower QP:QS and tendto “outgrow” their shunt sooner.
Anesthetic management
GoalsThese patients are managed according to theprinciples described in the section on Managementof single ventricle physiology, pre-initial repair(see Table 6.11). These patients have ductal depen-dant systemic blood flow. Patients with HLHSare particularly vulnerable to myocardial ischemiabecause the coronary arteries are supplied retro-grade from the PDA down a segment of hypoplasticascending aorta (often 1–2mm in diameter). Subse-quentmanagement for the superior cavopulmonaryshunt and Fontan procedure is described in laterportions of the section on Management of singleventricle physiology.
Post-CPB managementThese patients are managed according to the prin-ciples described in the section on Management ofsingle ventricle physiology, post-CPB management(see Table 6.11). Subsequent management for thesuperior cavopulmonary shunt and Fontan proce-dure is described in later portions of the section onManagement of single ventricle physiology.There are a few subtle differences inmanagement
of patients with a MBTS as opposed to a Sano RV toPA conduit in the initial postoperative period:• In patients with a MBTS, high SVR tendsto increase QP:QS, increase aortic diastolic run-off, and promote pulmonary overcirculation withcompromise of systemic oxygen delivery. After-load reduction with phenoxybenzamine is used insome institutions while in others a less aggressiveapproach utilizing milrinone is undertaken.• High SVR is less disadvantageous to a patientwith a Sano RV to PA conduit because pulmonaryblood flow is derived from the RV prior to distribu-tion to the arterial circulation and because of theinherent high resistance through the long RV to PAconduit. In these patients afterload reduction andreduced RV pressure may result in a low QP:QS andhypoxemia.
Tetralogy of Fallot with pulmonaryatresia
AnatomyTetralogy of Fallotwith pulmonary atresia (TOF/PA)involves the features of TOF and infundibular andpulmonary valvular atresia in conjunction withvarying degrees of pulmonary arterial atresia. Fourgroups are said to exist. Group 1 patients have iso-lated infundibular and pulmonary valve atresiawithamain PA and distal pulmonary arteries of near nor-mal size and architecture. In some of these patients,the main PA may extend to the atretic infundibu-lum. In others, there is short segment atresia of themain PA (Fig. 6.39a,b). Patients in this group havepulmonary blood flow supplied from a PDA. Group2 patients have absence of the main PA but the PAsare in continuity and supplied by a PDA. Group 3patients have severely hypoplastic native PAs; theleft and right PA may not be in continuity. There

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 244 — #78
244 Chapter 6
(a) (b)
Fig. 6.39 (a) Anatomy of tetraology ofFallot/pulmonary artery (TOF/PA)group 1 with short segment pulmonaryatresia, good-sized PAs in continuitysupplied by a right sided patent ductusarteriosus (PDA) and one large majoraortopulmonary collateral artery(MAPCA) from the left subclavianartery. There is a right aortic arch withmirror image arch vessel branching.(b) Illustration of TOF/PA group 3 withno main PA, small branch PAs incontinuity supplied by MAPCAs. Somelung segments are supplied by thenative PAs while others are supplieddirectly by MAPCAs. There is a rightaortic arch with mirror image archvessel branching.
aremajor aortopulmonary collateral vessels (vesselsfrom the aorta to the PA) known as MAPCAs. APDAmay be present as well. Some segments of lungmay be supplied only by blood fromMAPCAs, someonly by the native PAs, and others by both sources(see Fig. 6.39). Group 4 patients have no nativePAs and all pulmonary blood flow is derived fromMAPCAs.The anatomy of MAPCAs in TOF/PA can almost
never be clearly delineated by two-dimensionalechocardiography alone. Cardiac catheterizationand/or MRI/MRA are necessary to delineatecollateral anatomy and to determine QP:QS.
PhysiologyTOF/PA is single ventricle physiology lesion. Thislesion is generally amenable to a two-ventriclerepair. TOF/PA is a complex shunt in which acommunication (VSD) and total obstruction to RVoutflow (PA) are present. This results in oblig-atory R–L shunting across the VSD with com-plete mixing of systemic and pulmonary venousblood in the LV. Pulmonary blood flow is pro-vided by a downstream simple shunt (PDA orMAPCAs). For infants, in whom the PDA providesmost of the pulmonary blood flow, PGE1 infusion(0.01–0.05µg/kg/min) will be necessary to ensureductal patency.
Surgical therapySurgery in group 1 and 2 TOF/PA patients is aimedat establishing a reliable source of pulmonary bloodflow in the neonatal period, as these patients aredependent on PGE1 to maintain a PDA and pul-monary blood flow. These patients may undergoa palliative shunt procedure (usually a MBTS asdescribed above) or a definite procedure. The def-inite procedure would be creation of continuitybetween the RV and the main PA via placementof a RV to PA conduit with VSD closure generallyperformed via the ventriculotomyused for the prox-imal end of the conduit. In cases where short seg-ment atresia exists, itmay be possible to obtain RV toPA continuity with a direct anastomosis augmentedwith homograft material or pericardium.Patients in groups 3 and 4 present difficult man-
agement problems. As a rule these patients presentwith univentricular physiology with a tendencyfor pulmonary blood flow to become excessive(QP:QS > 2–3:1) as the PVR drops following birth.In group 3 patients neonatal repair with place-ment of a RV to PA conduit is undertaken toplace the PAs in continuity with the RV in aneffort to promote native PA growth. In this cir-cumstance the VSD is left open as a source of R–Lshunting and delivery of desaturated blood to thesystemic circulation as it would be impossible for

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 245 — #79
Congenital Heart Disease 245
the RV to deliver an adequate cardiac output tothe LA across the hypoplastic pulmonary vascularbed. These infants then undergo multiple cardiaccatheterization procedures in order to:• Dilate and stent the hypoplastic native pulmonaryarteries.• Coil embolize MAPCAs which provide pul-monary blood flowwhich is competitive with bloodflow supplied by native PAs. MAPCAs that pro-vide pulmonary blood flow to segments of lung notsupplied by native PAs must be unifocalized to theproximal pulmonary circulation.Unifocalization involves removal of the collateral
vessel from the aorta with subsequent reanasto-mosis to the RV to PA conduit or a proximal PAbranch. Although the traditional approach has beenthrough a thoracotomy more recently most groupshave favored a central approach working through amedian sternotomy. It is only when 80–90% of thepulmonary vascular bed is direct continuitywith theRV that closure or fenestrated closure of the VSDcan be considered. Usually this will mean that atleast 10–12 bronchopulmonary segments are nowin direct continuity with the RV.In group 4 patients it may be necessary to uni-
focalize several large collaterals to the distal endof conduit from the RV as the initial intervention.Alternatively several large collaterals could beunifocalized to an MBTS or central shunt. Theseprocedures serve to promote pulmonary vasculargrowth, prevent the development of PVOD, andcontrol the QP:QS.
Anesthetic managementThese patients are managed according to the prin-ciples described in the section on Management ofsingle ventricle physiology, pre-initial repair (seeTable 6.11).
Post-CPB managementThe management issues in patients with types 1and 2 TOF/PA having undergone definitive repairwith RV to PA conduit and VSD closure are similarto those encountered in care of the patient hav-ing undergone repair for TOF/PS. A few differencesmerit discussion. These TOF/PA patients will nothave pulmonary insufficiency due to the presence
of a competent valve in the conduit. The place-ment of a conduit will however require a larger rightventriculotomy and potential for significant RV freewall hypo- and dyskinesis.The management issues in patients with types 3
and 4 TOF/PA having undergone palliativeaortopulmonary shunt placement or RV to PAconduit placement without VSD closure will be sim-ilar to those described for patients with a large, non-restrictive VSD and/or PDA. This will be particularlytrue for patients with a large number of residualMAPCAs. In these patients postoperative emboliza-tion of some MAPCAs in the cardiac catheterizationlaboratory may be necessary to control pulmonaryblood flow.
Pulmonary atresia with intactventricular septum
AnatomyThere is complete obstruction to RV outflow inpulmonary atresia with intact ventricular septum(PA/IVS) (Fig. 6.40). The complete outflow obstruc-tion is at the level of the pulmonary valve dueto fusion of the valve cusps. The main PA trunkand PA branches are generally of normal or nearnormal size. The normal RV is tripartite with aninflow region (tricuspid valve), a body (the trabec-ulated apical component), and an outflow region(infundibulum). In PA/IVS, the RV tends to behypoplastic and tricuspid valve size generally paral-lels RV cavity size. In mild-to-moderate hypoplasia,the apical trabeculated component of the RV ispoorly developed or even absent. With more severedegrees of hypoplasia the infundibulum may beabsent as well. Occasionally the RV is miniscule.Approximately 25% of patients have mild hypopla-sia, 40% have moderate hypoplasia, and 35% havesevere hypoplasia. Finally, there is an ASD or patentFO and a PDA.
PhysiologyPA/IVS is a single ventricle physiology lesion thatmay be amenable to a two-ventricle repair but inmany instances patients are staged down the sin-gle ventricle pathway. PA/IVS is a complex shuntwith complete obstruction to outflow. There is a

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 246 — #80
246 Chapter 6
Normal
Atreticpulmonary
valve
Small(hypoplastic)right ventricle
Patent (open)ductus
arteriosus
Pulmonary valveatresia with
intact ventricularseptum
Fig. 6.40 Anatomy of pulmonaryatresia with intact ventricular septum(PA/IVS). The right ventricle (RV) ishypoplastic with complete obstructionto outflow due to fusion of thepulmonary valve leaflets. Pulmonaryblood flow is supplied by the patentductus arteriosus (PDA). There istricuspid regurgitation and right-to-left(R–L) shunting at the atrial level.
communication (ASD or patent FO) and a completeobstruction to RV outflow (PA). RV pressuresmay be 2–3 times systemic and RA pressure iselevated. RV filling volume in diastole is essen-tially equal to the volume of blood that is regur-gitated back across the tricuspid valve in systole.Consequently, there is an obligatory physiologicR–L shunt at the atrial level, with complete mix-ing of systemic and pulmonary venous blood in theLA. When the ASD or FO is restrictive, there will bea large right atrial to LAP gradient. This will result inpoor decompression of the RA and systemic venouscongestion. Pulmonary blood flow is provided bya downstream shunt (PDA).Persistently high RV pressures in the prenatal
and neonatal period may result in enlargementof the Thesbesian veins leading to the develop-ment of anomalous fistulous connections betweenthe RV and the epicardial coronary arteries. Retro-grade coronary blood flow through these ventricu-locoronary connections predisposes the coronarycirculation to development of proximal obstruc-tive lesions from fibrous myointimal hyperplasia.As a result of these changes, myocardium distalto any proximal coronary occlusion will be depen-dent on a high RV pressure to provide retrogradeperfusion via ventriculocoronary connections. This
physiology is described as right-ventricle dependentcoronary circulation (RVDCC).
Surgical therapyCoronary angiography is performed in all patientsPA/IVS to assess RV and tricuspid valve functionand to assess for the presence of RVDCC. Surgicaltherapy has two objectives: provision of enoughpulmonary blood flow to replace the PDA, and ifpossible, relief of RV outflow obstruction such thatforward flow through the tricuspid valve, RV, andPA is established. Decompression of the RV is con-traindicated in the presence of RVDCC. Myocardialischemia or infarction distal to coronary lesionsmay occur when perfusion pressure via ventricu-locoronary connections is reduced by RV decom-pression. Fistulous connections between the RVand the epicardial coronary arteries in the absenceof proximal coronary obstructive lesions are not acontraindication to RV decompression.Forward flow through the RV may promote
continued growth of the RV. If the RV is largeand only pulmonary valvular atresia exists, a pul-monary valvulotomy or a RV outflow transannu-lar patch may be all that is necessary. In somecases, balloon dilation of the pulmonary valve inthe cardiac catheterization laboratory is sufficient.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 247 — #81
Congenital Heart Disease 247
Because decompression of the RA and RVwill occuras long as the ASD or FO is open, the ASD orFO cannot be closed unless the RV is capable ofproviding all of the pulmonary blood flow with-out failing. If the RV is hypoplastic and the valveis severely atretic, a MBTS in combination with aRV outflow tract transannular patch may be nec-essary to provide adequate pulmonary blood flow.Because the infundibulum may be very hypertro-phied and the infundibular muscle usually is quitefibrotic the incision for the transannular patch iscarried well down into the body of the RV. The PDAis almost always ligated at the time of the initialprocedure.Following neonatal intervention one of the
following options exist depending on the presenceor absence of RVDCC and the size of the RV andtricuspid valve. In all of the repairs described theMBTS, if present is ligated.• Fontan procedure (TCPC). Staging to the fenes-trated Fontan via a superior cavopulmonary shuntis reserved for patients with RVDCC or for patientswith severely hypoplastic RVs.• One-and-a-quarter ventricle repair. In patientswith non-RVDCC and some RV mass this repairwhich consists of a BDG and an atriopulmonaryconnection between the roof of the RA andthe undersurface of the right PA opposite the BDGanastomosis in conjunction with an RV outflowpatch and a fenestrated ASD (R–L “pop-off”) or ASDclosure can be considered. This repair allows a smallamount of SVC and IVC blood to cross the tricuspidvalve and be ejected by the RV antegrade into thepulmonary bed.• One-and-a-half ventricle repair. In patients withnon-RVDCC and mild to moderate RV hypoplasiathis repair, which consists of a BDG in conjunctionwith an RV outflow patch and a fenestrated ASD(R–L “pop-off”) or ASD closure, can be considered.This repair allows IVC blood to cross the tricuspidvalve and be ejected by the RV antegrade into thepulmonary bed.• Two-ventricle repair. In patients with non-RVDCCand mild RV hypoplasia this repair, which consistsof a RV outflow patch and a fenestrated ASD (R–L“pop-off”) or ASD closure, can be considered. Thisrepair allows all or nearly all systemic venous blood
to cross the tricuspid valve and be ejected by the RVantegrade into the pulmonary bed.In all of these repairs the fenestrated ASD can be
closed at a later date in the cardiac catheterizationlaboratory if there is minimal R–L shunting andRAhypertension is not present following temporaryballoon occlusion.
Anesthetic management
GoalsThese patients are managed according to the prin-ciples described in the section on Management ofsingle ventricle physiology, pre-initial repair (seeTable 6.11). Subsequent management for the supe-rior cavopulmonary shunt and Fontan procedureis described in later portions of the section onManagement of single ventricle physiology.These patients have ductal dependant pulmonary
blood flow. Patients with PA/IVS are particularlyvulnerable to myocardial ischemia because even inthe absence of RVDCC the coronary arteries aresupplied in part retrograde from the body of theRV. Myocardial depression is poorly tolerated bothbecause it may reduce pulmonary blood flow acrossa restrictive PDA and because coronary blood flowmay be compromised if aortic pressure and RVpressure falls.
Post-CPB managementMost of these patients are managed according to theprinciples described in the section on Managementof single ventricle physiology, post-CPB manage-ment (see Table 6.11). Subsequent management forthe superior cavopulmonary shunt and Fontan pro-cedure if necessary is described in later portionsof the section on Management of single ventriclephysiology.Only those patients with an RV large enough to
require only a transannular patch will not exhibitsingle ventricle physiology. For a given cardiacoutput and QP:QS patients with a transannularpatch and a MBTS will have less of a volumeload on the LV. Following decompression of theRV PA/IVS patients are vulnerable to myocardialischemia because even in the absence of RVDCC

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 248 — #82
248 Chapter 6
the coronary arteries are supplied in part retrogradefrom the body of the RV.
Truncus arteriosus
AnatomyA single great vessel arising from the base of theheart and giving rise to the pulmonary, coronary,and systemic arteries characterizes truncus arte-riosus. There is a single semilunar valve, whichis usually abnormal, and invariably a large (non-restrictive) conoventricular septal VSD is present.The truncus straddles this large VSD (Fig. 6.41).Truncus arteriosus is classified based on the originof the pulmonary arteries. In type 1, a short pul-monary trunk originates from the truncus and givesrise to both pulmonary arteries. In type 2, bothpulmonary arteries arise from a common orificeof the truncus, whereas in type 3, the right andleft pulmonary arteries arise separately from thelateral aspect of the truncus. The VSD usually isof the infundibular or perimembranous infundibu-lar type. The truncal valve is tricuspid in mostpatients, but multiple cusps (4–7) are common and
Ao
PA
LA
VSDRA
RVLV
Fig. 6.41 Anatomy of truncus arteriosus. Type 1truncus arteriosus is illustrated here with a shortpulmonary trunk arising from the truncus. There is alarge conoventricular septal ventricular septal defect(VSD) with truncal override. Ao, aorta; LA, left atrium;LV, left ventricle; PA, pulmonary artery; RA, rightatrium; RV, right ventricle.
the valve itself may be regurgitant or stenotic.Extracardiac anomalies are seen in approximately30% of patients.
PhysiologyTruncus arteriosus is a single ventricle physiol-ogy lesion amenable to a two-ventricle repair. Thelarge (nonrestrictive) VSD allows equalization ofpressures in the RV and LV. As a result, there isbidirectional shunting and complete mixing of sys-temic and pulmonary venous blood in a functionallycommon ventricular chamber. This blood is thenejected into the truncal root, which gives rise to thepulmonary, systemic, and coronary circulations. Aswith all simple shunts, QP:QS is determined by theratio of PVR to SVR. However, in truncus arteriosus,the pulmonary and systemic circulations are sup-plied in parallel from a single vessel, and for a givenventricular output increases in flow to one circula-tory system will produce reductions in flow to theother.As with all single ventricle lesions, a low QP:QS
will reduce arterial saturation,whereas a highQP:QSwill produce ventricular volume overload withouta substantial increase in arterial saturation. Shortlyafter birth the balance of PVR and SVR is such thatpulmonary blood flow is high and the patient withtruncus arteriosus has symptoms of CHF with mildcyanosis. After cardiac reserve has been exhausted,further decreases in PVR will increase pulmonaryblood flow at the expense of systemic and coronaryperfusion. This will produce a progressive metabolicacidosis. If truncal valve insufficiency is present, thiswill obviously impose an additional volume load onthe ventricles. Given the high pulmonary bloodflowand the transmission of systemic arterial pressuresto the pulmonary vasculature present in this lesiondevelopment of PVOD is rapid. With developmentof PVOD there will be a progressive decrease in pul-monary blood flow relative to systemic blood flowand progressive hypoxemia.
Surgical therapyBecause of the risk of early development of PVOD,surgical intervention within the first months of lifeis undertaken. Definitive repair of truncus arterio-sus requires patch closure of the VSD, detachment

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 249 — #83
Congenital Heart Disease 249
of the pulmonary arteries from the truncus, andestablishment of right ventricular to PA continu-ity with a valved homograft. The RV to PA conduitrequires placement of the proximal end of theconduit over a ventriculotomy in the RV free wall.The truncal valves must be assessed at the time ofsurgery. In some instances, valve repair or replace-ment is necessary to address valvular insufficiencyor stenosis. Valvuloplasty is preferred over valvereplacement. Valve replacement in a child neces-sitates subsequent replacements as the child grows.Management of the systemic anticoagulation nec-essary with a mechanical valve is also difficult ingrowing children. The RV to PA valved conduit willeventually require replacement as the child grows.
Anesthetic management
GoalsThese patients are managed according to the prin-ciples described in the section on Management ofsingle ventricle physiology, pre-initial repair (seeTable 6.11). This is a nonductal dependant lesion.
Post-CPB management
Goals1 Maintain heart rate (preferably sinus rhythm)at an age-appropriate rate. Cardiac output is likelyto be more heart-rate-dependent in the post-CPBperiod.2 Reduce PVR when necessary through ventilatoryinterventions.3 Inotropic support of the left and RV may benecessary for the reasons addressed previously.Dobutamine (5–10µg/kg/min) or dopamine(5–10µg/kg/min) is useful in this instance becausethey provide potent inotropic support withoutincreasing PVR. Milrinone (0.5–1.0µg/kg/min fol-lowing a loading dose of 50µg/kg) should be consid-ered for its inotropic and lusitrophic effects as wellas its ability to reduce PVR.Some degree of RV dysfunction is likely to exist
due to the presence of a ventriculotomy and a largeVSD patch. This will be particularly problematic inpatients with high PVR or early PVOD. Left ven-tricular volume overload may occur secondary totruncal valve insufficiency.
Interrupted aortic arch
AnatomyThree types of Interrupted aortic arch (IAA) exist:• Type A. The arch is interrupted distal to the leftsubclavian artery at the level of the aortic isth-mus (similar to very severe coarctation). This typecomprises 15% of IAA.• Type B. The arch is interrupted between the leftcommon carotid and left subclavian arteries. Theorigin of the right subclavian artery is commonlyaberrant arising from the descending aorta distal tothe interruption. This is the most common man-ifestation of IAA and comprises 80% of all IAA(Fig. 6.42).• Type C. The arch is interrupted between theinnominate and the left common carotid and arter-ies. This is the least common manifestation of IAAand comprises 5% of all IAA.In all cases the aorta distal to the interrup-
tion is supplied by the DA. There is invariably
1
2
3
Fig. 6.42 Anatomy of interrupted aortic arch (IAA) withassociated ventricular septal defect (VSD). Type B IAA isillustrated here with the interruption between the leftcarotid and left subclavian arteries (1). There is a largeconoventricular septal defect (3) without significantposterior malalignment of the conal septum. The distalaorta (2) and left subclavian artery are supplied by thepatent ductus arteriosus (PDA). As a result there will bedifferential cyanosis with a lower SaO2 in the lower bodyand left arm than in the right arm and cerebralcirculation.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 250 — #84
250 Chapter 6
a large conoventricular septal defect with posteriormalalignment of the conal septum. The posteriormalalignment can produce subaortic LV outflowtract obstruction. The aortic valve is commonlybicuspid with commissural fusion.
PhysiologyIAA is single ventricle physiology lesion with duc-tal dependent systemic blood flow amenable to atwo-ventricle repair. IAA is a complex shunt withcomplete obstruction to aortic outflow at the levelof the interruption. A simple downstream shunt(PDA) provides aortic flowdistal to the interruption.Flow to the aorta proximal to the obstruction is sup-plied by the LV. In addition there is a simple shunt(VSD) and there may be fixed obstruction to LVoutflow (subaortic stenosis). There is a physiologicL–R shunt at the level of the VSD. In the presenceof significant LVOTO there may be compromise ofproximal aortic perfusion due to a large L–R shunt.There is predominantly a physiologic R–L shunt atthe level of the PDA. As a result there will be differ-ential cyanosis with a lower SaO2 in the lower bodyand arch vessels distal to the interruption than inthe arch vessels proximal to the interruption.The shunt at the level of the PDA is a depen-
dent shunt with net systemic and pulmonary bloodflow determined by the ratio of systemic to PVR.Low PVR relative to SVR will allow run-off of bloodinto the pulmonary circuit (increased physiologicL–R shunting at the PDA) compromising distal aor-tic perfusion. Closure of the PDA in infants withIAA terminates distal aortic flow severely compro-mising splanchnic perfusion and usually results inimmediate cardiovascular collapse. PGE1 therapy islifesaving for these patients.
Surgical therapyDefinitive surgical therapy for IAA involves primaryre-anastomosis of the proximal and distal aorta,PDA ligation, VSD closure, and resection of subaor-tic stenosis if present. Arterial cannulation for CPBrequires the use of two arterial cannula. Cannula-tion is obtained directly in the ascending aorta andin the descending aorta via the PDA. In order toreduce tension on the arch anastomosis it may benecessary to divide and ligate the left subclavian
artery during repair of type B IAA. In addition, itmay be necessary to divide and ligate an aberrantright subclavian artery if present to reduce tensionon the descending aortic portion of the anastomosis.
Anesthetic management
GoalsThese patients are managed according to the prin-ciples described in the section on Management ofsingle ventricle physiology, pre-initial repair (seeTable 6.11). These patients have ductal dependantdistal aortic blood flow. The diastolic blood pressurewill be lower and the pulse pressure wider in thedistal as compared to proximal aorta. Arterial mon-itoring sites must be chosen carefully. Right radialartery pressure will reflect distal aortic pressure inthe presence of an aberrant right subclavian artery.If the left subclavian artery is divided and ligatedduring repair, a left radial arterial line will be of littleuse post-repair.
Post-CPB management
Goals1 Maintain heart rate (preferably sinus rhythm)at an age-appropriate rate. Cardiac output is likelyto be more heart-rate-dependent in the post-CPBperiod.2 Reduce PVR when necessary through ventilatoryinterventions.3 Inotropic support of the left and RV may benecessary for the reasons addressed previously.Dobutamine (5–10µg/kg/min) or dopamine(5–10µg/kg/min) is useful in this instance becausethey provide potent inotropic support with-out increasing PVR. Milrinone (0.5–1.0µg/kg/minshould be considered for its lusitrophic effects andit effect on PVR.Determining whether there is a residual arch
obstruction is a priority following termination ofCPB. This requires accurate simultaneous measure-ments of both upper and lower aortic blood pressureobtained with either percutaneously or surgicallyplaced catheters. A significant gradient may neces-sitate surgical revision. Bleeding from the archsuture lines may be significant. Residual LVOTOmay produce LV contractility/afterload mismatch.

Alice Nelson Dinardo: “ch06” — 2007/7/16 — 12:39 — page 251 — #85
Congenital Heart Disease 251
Elevated PVR due to LA hypertension and reactivepulmonary vasoreactivity due to high QP:QS pre-operatively may result in RV contractility/afterloadmismatch as well. In addition, the long CPB anddeep hypothermic circulatory arrest (DHCA) timesnecessary to complete this procedure may fur-ther compromise LV and RV function and producemyocardial edema.
Suggested reading
Barnea O, Santamore WP, Rossi A et al. Estimation of
oxygen delivery in newborns with a univentricular
circulation. Circulation 1998;98:1407–13.Bellinger DC, Wypij D, duPlessis AJ et al. Neuro-
developmental status at 8 years in children with
dextro-transposition of the great arteries: the Boston
Circulatory Arrest Trial. J Thorac Cardiovasc Surg
2003;126:1385–96.
Hoskote A, Li J, Hickey C et al. The effects of carbon
dioxide on oxygenation and systemic, cerebral, and pul-
monary vascular hemodynamics after the bidirectional
superior cavopulmonary anastomosis. J Am Coll Cardiol
2004;44:1501–9.Ikemba CM, Su JT, Stayer SA et al. Myocardial
performance index with sevoflurane–pancuronium
versus fentanyl–midazolam–pancuronium in infants
with a functional single ventricle. Anesthesiology
2004;101:1298–305.Laird TH, Stayer SA, Rivenes SM et al. Pulmonary-to-
systemic blood flow ratio effects of sevoflurane, isoflu-
rane, halothane, and fentanyl/midazolam with 100%
oxygen in childrenwith congenital heart disease. Anesth
Analg 2002;95:1200–6.Ramamoorthy C, Tabbutt S, Kurth CD et al. Effects
of inspired hypoxic and hypercapnic gas mixtures
on cerebral oxygen saturation in neonates with
univentricular heart defects. Anesthesiology 2002;96:283–8.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 252 — #1
CHAPTER 7
Anesthesia for Heart, Heart-Lung,and Lung Transplantation
Heart transplantation
Cardiac transplantation is now common amongpatients with end-stage cardiac dysfunction that isunresponsive to maximal medical therapy andfor which no other surgical options exist. Mostadult patients are New York Heart Association(NYHA) functional class IV (symptoms at rest).These patients have an expected 1-year survivalof approximately 50–60% with optimal medi-cal therapy. A subgroup of ambulatory NYHAfunctional class III patients (symptoms with lim-ited exertion) with an impairment of exercisetolerance (VO2max < 14 mL/kg/min) predictive ofreduced 1-year survival also can be considered fortransplantation.
For infants and children, the natural historyof end-stage cardiac dysfunction is not as welldelineated in large part because of the hetero-geneity of the various congenital lesions. In addi-tion, end-stage cardiac dysfunction is more difficultto define. Growth failure secondary to severecardiac dysfunction is useful in identifying end-stage disease. Progressive pulmonary hypertension,which could preclude transplantation at a laterdate, also is considered an important indication fortransplantation.
Ninety percent of adult patients presenting forcardiac transplantation have a dilated cardiomy-opathy (DCM) secondary to ischemic heart disease.Less commonly, patients with end-stage valvular
heart disease or with intractable, life-threateningarrhythmias not amenable to medical therapy orinsertion of an implanted cardioverter defibrillator(ICD) are transplanted. Cardiac transplantation alsohas been used for unresectable cardiac tumors,sarcoidosis, amyloidosis, active myocarditis, hyper-trophic cardiomyopathies, and refractory anginanot amenable to angioplasty or surgical revascu-larization. Heart transplantation for patients withamyloidosis and sarcoidosis is tempered by evidencethat systemic progression of these diseases may limitthe long-term effectiveness of heart transplantation.In patients with acute myocarditis there is evidenceof higher mortality and rejection rates.
DCM and complex congenital heart disease repre-sent the two major indications for heart transplanta-tion for pediatric patients. In patients younger than1 year of age, 65% of transplants are for congenitalheart disease, primarily hypoplastic left heart syn-drome (HLHS). In patients between 1 and 10 yearsof age, the indications for heart transplantation aredivided equally between congenital heart diseaseand DCM. Most children requiring transplantationfor congenital lesions in this age group have hadat least one previous cardiac surgical procedure. Inpatients between 11 and 17 years of age, the primaryindication (60%) for heart transplantation is DCM.
Contraindications to heart transplantation areoutlined in Table 7.1. Severe osteoporosis, activepeptic ulcer, diverticular disease, active infection,and morbid obesity all are conditions that are
252

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 253 — #2
Heart, Heart-Lung, and Lung Transplantation 253
Table 7.1 Recipient selection for heart and heart-lungtransplantation.
Absolute contraindications1 History of emotional instability, medicalnoncompliance, or active substance abuse2 Fixed pulmonary hypertension (for cardiactransplantation, not for lung or heart-lungtransplantation)3 Significant cerebral vascular disease4 Active malignancy or life-limiting co-existent disease
Relative contraindications1 Physiological age older than 60 years2 Significant peripheral vascular disease3 Active peptic ulcer or diverticular disease4 Severe bronchitis or chronic obstructive pulmonary
disease (for cardiac transplantation, not for lung orheart-lung transplantation)5 Disease likely to recur in allograft (cardiac amyloidosis
or sarcoidosis)6 Irreversible hepatic or renal disease (may be
considered for combined cardiac and renal or hepatictransplantation)7 Immunological sensitization to donor antigens8 Severe osteoporosis9 Morbid obesity10 Active infection11 Diabetes mellitus with end-organ dysfunction
likely to be worsened by the necessity of a lifelongimmunosuppressive regiment including steroids.Corticosteroids also complicate the glucose man-agement in diabetes. Nonetheless, carefully selectedpatients with diabetes without end-organ dysfunc-tion have been shown to have 2- to 4-year survivalsimilar to nondiabetics. Chronic lung disease iden-tified as a forced expiratory volume (FEV) < 50%predicted, a forced expiratory volume in 1 second(FEV1) < 1 L, and a forced expiratory volume in1 second to forced vital capacity (FEV1:FVC) ratio<1 is believed to predispose postoperative res-piratory failure, reduced survival from lung dis-ease alone, and an increased risk of infectionon immunosuppression. Survival is favorable forelderly patients, but careful selection is necessary,particularly for patients older than 65 years of age,because they are at increased risk for infectious andsteroid complications.
Pathophysiology and adaptationof DCMThe etiologies of DCM can be summarized asfollows:• Idiopathic. Idiopathic cardiomyopathy is an irre-versible form of DCM for which no clear etio-logical factors have been identified. Familial andgenetic factors, viral and other cyotoxic insults,immune abnormalities, and metabolic, energetic,and contraction abnormalities all have been impli-cated in the pathogenesis of idiopathic DCM. It islikely that several factors interact to cause diseasein susceptible patients.• Secondary. A variety of etiological factors, bothacquired and hereditary cause or at least pre-dispose to development of a DCM. The majorityof secondary DCMs are irreversible and are dueto ischemic heart disease, hypertension, valvu-lar heart disease, or congenital heart disease.Some secondary DCMs are potentially reversible.Toxins (including alcohol and cocaine), pregnancy,infectious agents (including cytomegalovirus andtoxoplasmosis), and metabolic abnormalities(including thiamine deficiency and hypo- andhyperthyroidism) are all potentially reversibleforms of secondary DCM.
Regardless of the initiating cause, the alterationsin ventricular function in DCM are remarkablyconsistent (Fig. 7.1). Biventricular dysfunction iscommon in idiopathic and secondary DCM. Inischemic cardiomyopathy, dysfunction may be lim-ited to the left ventricle (LV). Loss of myocar-dial tissue, as occurs with infarction or fromdirect myocardial damage, results in overload andsubsequent hypertrophy of the remaining activemyocardium. For the postinfarction patient, thisprocess is known as ventricular remodeling. Hyper-trophy of active myocardium serves to reducewall stress and energy consumption. However, theprocess of hypertrophy results in changes thatadversely affect myocardial energy balance andultimately produces progressive myocardial dys-function. Increases in capillary density do notkeep pace with replication of sarcomeres. The dis-tance between capillaries increases resulting in poorsubstrate delivery to hypertrophied myocardium.In addition, the process of hypertrophy increases

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 254 — #3
254 Chapter 7
Normalheart
End-stageDCM
250
200
150
LV p
ress
ure
(mm
Hg)
100
50
050 100 150 200 250
LV volume (cc)
300 350 400 450
Fig. 7.1 Pressure–volume (PV) loops froma normal heart and a dilatedcardiomyopathic (DCM) heart. The DCMheart is dilated, has depressed systolicfunction, has reduced stroke volume at rest,and is prone to afterload mismatch. Strokevolume at rest for each heart is representedby the solid PV loop. Stroke volume after anincrease in afterload with preload andcontractility held constant is represented bythe dotted PV loop. Note the markeddecrease in stroke volume in the DCM ascompared with the normal heart withcomparable increases in afterload.
the cellular ratio of myofibrils to mitochondria,creating the potential for oxygen imbalance atthe cellular level. Eventually, myocardial necrosisresults in replacement of myocardium with con-nective tissue. This produces progressive impair-ment of contractility, which in turn, stimulatesfurther hypertrophy and progression of myocardialnecrosis. Ventricular dilatation occurs as the resultof this progressive replacement of myocardiumwith connective tissue. Eccentric hypertrophy inthe surviving myocardium further accelerates thedevelopment of ventricular dilatation.
Metabolic down-regulation and uncoupling ofcardiac β-receptors is a common feature in DCM.There is also depletion of myocardial norepine-phrine (NE) stores. As a result, NE secretion isenhanced in patients with low-output cardiac fail-ure with the degree of elevation paralleling theseverity of the failure. Serum NE levels may betwo-to-three times normal due to enhanced releaseand reduced reuptake of NE by adrenergic termi-nals. The consequence of prolonged elevation ofserum NE is gradual down-regulation (reduction inreceptor density) of cardiac βl-receptors and partialuncoupling of cardiac βl-receptors from adenylatecyclase. Interestingly, there is a greater decrease inthe density of βl-adrenergic receptors in patientswith idiopathic cardiomyopathy as compared withischemic cardiomyopathy. This may be due tolong-term adrenergic over-stimulation or anti-β-receptor antibodies in idiopathic cardiomyopathy.Uncoupling of βl-adrenoreceptors from the effectorenzyme adenylate cyclase involves phosphorylation
of the receptors by β-adrenergic receptor kinase.Progressive cardiac dysfunction also produces anincrease in the ratio of the inhibitory guaninenucleotide regulatory protein (Gi) to the stimula-tory guanine nucleotide regulatory protein (Gs).Gi inhibits and Gs stimulates adenylate cyclase.Uncoupling of βl-adrenoreceptors and an increasedratio of Gi:Gs both result in reduced levels of cyclicadenosine monophosphate (cAMP) and reducedmovement of calcium into myocytes. The conse-quence of down regulation of βl-receptors, uncou-pling of βl-receptors, and an increased Gi:Gs
ratio is an impaired ability of DCM hearts toproduce cAMP. Therefore, the contractile responseof the DCM heart to β-adrenergic receptor ago-nists (epinephrine, dopamine, dobutamine, isopro-terenol, and NE) and phosphodiesterase inhibitors(amrinone, milrinone) is markedly impaired. Thecontractile response to raising intracellular calciumand to cardiac glycosides (digoxin) is retained. Inaddition, although the depletion of myocardial NEstores does not affect the intrinsic contractile func-tion of the myocardium, it does result in an impairedcontractile response to indirect-acting β-adrenergicagonists such as ephedrine.
There is persistent inappropriate activation ofthe renin-angiotensin-aldosterone system despiteabsence of salt deprivation and intravascularvolume depletion. This induces expansion ofintravascular and extravascular volume and pro-motes fibrotic changes in the heart and kidneys.Counterbalancing this system is the atrial natriureticpeptide (ANP) and brain natriuretic peptide (BNP)

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 255 — #4
Heart, Heart-Lung, and Lung Transplantation 255
system. ANP and BNP are released from secretorygranules in the atria and ventricles respectively inresponse to cardiac chamber distention. Both pep-tides increase salt and water excretion, suppress therenin-angiotensin-aldosterone system, and inducearterial and venous vasodilation. In compensatedheart failure release of ANP and BNP is sufficientto counteract the effects of the renin–angiotensin–aldosterone release induced by mild to moderatereductions in renal perfusion. In decompensatedheart failure ANP and BNP release is insufficientto counteract the effects of the renin–angiotensin–aldosterone release induced by moderate to severereductions in renal perfusion. Elevated plasmalevels of BNP are diagnostic for heart failure andthe extent of elevation is a predictor of survival.
Therapy for patients with DCM is directed towardtreatment of neurohormonal abnormalities andinhibiting or reversing remodeling. Diuretics incombination with angiotensin-converting enzyme(ACE) inhibitors (captopril, enalapril) and beta-blockers (carvedilol, metoprolol) are first-line ther-apy. Beta-blockers and ACE inhibitors alone andin combination improve symptoms and reducemortality. Aldosterone inhibiting drugs (spiro-lactone, eplerenone) may be useful in patientswith aldosterone escape in whom ACE inhibitiononly partially suppresses aldosterone production.Angiotensin-receptor blockers (ARB) such as lor-sartan, candesartan, and valsartan are generallyreserved for patients who do not tolerate ACEinhibitors. Nesiritide, a BNP analog available inintravenous form, shows some promise in improv-ing symptoms and reducing hospital stay. Short-term use however is associated with an increasedrisk of renal dysfunction and post-dischargemortality.
Chronic therapy for DCM is problematic. Digoxinhas been shown to improve ejection fraction (EF),exercise capacity, and symptoms of heart failurein DCM. It does not substantially improve sur-vival however. Acute, intermittent, and long-termadministration of intravenous inotropic agents hasnot proved as promising. Dobutamine, dopamineand milrinone administration have not beenshown to consistently improve exercise capacity orsymptoms. In addition, short-term administration
of these agents is associated with increased post-discharge mortality particularly in the subset ofpatients with ischemic heart disease. Administra-tion of these agents is recommended only in thesetting of acute hemodynamic compromise in DCMpatients unresponsive to conventional therapy.
An alternative to these cAMP mediated inotropicagents is calcium-sensitizing agents. Levosimendanis the only such agent currently clinically avail-able. It increases inotropy in a cAMP-independentfashion by inducing a conformational change introponin C that increases the sensitivity of tro-ponin C to intracellular ionized calcium. This resultsin a concentration–response relationship betweenintracellular calcium and inotropy at lower intra-cellular ionized calcium levels than seen withcAMP-mediated agents. This agent shows somepromise in the chronic treatment of patientswith DCM.
Ventricular diastolic function andthe atrial transport mechanismDiastolic dysfunction in the form of impairedventricular relaxation and reduced ventricular com-pliance is seen in DCM. There is rapid equili-bration of left atrial and ventricular end-diastolicpressures producing a restrictive mitral inflow pat-tern with abrupt premature closure of the mitralvalve. Progressive ventricular dilatation producesatrial enlargement due to the longstanding increasein atrial afterload produced by an elevated ven-tricular end-diastolic pressure. In many instances,the atria will be dilated, hypokinetic, and filledwith spontaneous contrast on echocardiographicexamination. In these patients, the contribution ofatrial systole to ventricular filling will be minimal.As a consequence of these changes, patients withDCM require high mean atrial pressures to ensureadequate ventricular filling.
Myocardial oxygen balanceOxygen balance is impaired in patients with anischemic cardiomyopathy. Myocardial blood flowabnormalities also are present in patients withDCM despite the presence of angiography normalcoronary arteries. It has been proposed that func-tional small-vessel abnormalities due to either

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 256 — #5
256 Chapter 7
increased vascular tone or endothelial abnormal-ities account for decreased global baseline myo-cardial blood flow and impaired coronary reservein DCM. Regional perfusion defects also areseen in 45% of DCM hearts without demon-strable coronary lesions. Furthermore, myocardialischemia has been detected in patients with DCMwho are subjected to pacing-induced tachycardiaand to coronary vasodilation from dipyridamoleinfusion.
Left ventricular systolic functionWhen a patient presents for transplantation, anEF of 10–20% is likely. Compensation for theprogressive reduction in contractility occurs byuse of preload reserve. As contractility decreases,end-systolic volume (ESV) increases for a givenafterload. Increases in preload initially can be usedto normalize stroke volume (SV) under these con-ditions. Preload reserve is exhausted when thesarcomeres are stretched to their maximum dias-tolic length. When this occurs, there will be nofurther augmentation of the velocity of shorten-ing by increasing diastolic fiber length, and theventricle behaves as if preload were fixed. For agiven level of contractility, after preload reservehas been exhausted, additional increases in after-load will be accompanied by parallel decreases inSV. This is defined as a state of afterload mismatch.Patients with end-stage DCM will have exhaustedpreload reserve and will exhibit afterload mismatch(see Fig. 7.1). In addition, patients with DCM havea fixed SV due to exhaustion of preload reserveand an inability to decrease ESV by increasingcontractility.
The result of this compensation process is pro-gressive ventricular dilatation. Dilatation of theventricle has several important consequences.Ventricular dilatation can produce mitral insuffi-ciency secondary to dilation and deformation ofthe valve annulus. This type of functional mitralinsufficiency is common in DCM. Dilatation ofthe ventricle also results in elevated wall stress(wall stress = [P × r]/2h) at the conclusion ofisovolumic contraction for a given left-ventricularend-systolic pressure (LVESP). Because wall stressis synonymous with afterload, ventricular dilatationfurther compromises systolic function by producing
increased afterload at a given systolic bloodpressure.
Right ventricular function andthe pulmonary vasculatureIn instances in which DCM produces biventricu-lar dysfunction, the right ventricle (RV) will exhibitthe same alterations in systolic function, afterloadsensitivity, and diastolic dysfunction described forthe LV. The prolonged elevations of left atrial pres-sure (LAP) seen in progressive DCM have profoundeffects on the pulmonary vasculature and right ven-tricular function. Early in the disease, elevated LAPis transmitted to the pulmonary venous systemand there is reversible passive elevation of the pul-monary artery pressures while pulmonary vascularresistance (PVR) remains normal (see Fig. 5.13).Right ventricular function remains unchanged. Asthe disease progresses, reactive changes occur inthe pulmonary vasculature. Prolonged perivascu-lar edema results in arterial intimal fibroelastosisand nonreversible elevations in PVR due to obliter-ative changes in the distal pulmonary vasculatureknown as pulmonary vascular occlusive disease(PVOD). Progression of this process presents a largeincrease in right ventricular afterload similar tothat seen in severe mitral stenosis (see Fig. 5.13).Similar changes occur in infants and children withcongenital heart disease.
The RV is poorly adapted to generate pressuresthat approach systemic. As a result, afterload mis-match occurs, the RV fails, and RV output falls.Peripheral edema and hepatic congestion ensue.RV failure and dilation may lead to functional tricus-pid regurgitation and worsening symptoms of rightheart failure. In the steady state, RV output and LVoutput must be equal. Therefore, LV output is alsolimited by RV failure. In cases of severe RV dys-function or in the presence of systemic pulmonaryartery pressures, there is leftward shift of the intra-ventricular septum further compromising LV fillingand function.
When the postischemic donor RV is acutelyexposed to the elevated PVR of the recipient,severe right heart failure develops secondary toafterload mismatch. Data from the Registry of theInternational Society for Heart and Lung Transplan-tation has consistently demonstrated a continuous

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 257 — #6
Heart, Heart-Lung, and Lung Transplantation 257
relationship between preoperative PVR and postop-erative mortality. In addition pre-transplant PVR inexcess of 5 Wood units and a transpulmonary gra-dient in excess of 15 mmHg both have been clearlyassociated with increased postoperative mortality inadults. As a result, increased irreversible PVR eleva-tions remains an absolute contraindication to hearttransplantation (see Table 7.1).
Most centers perform provocative testing in theirpatients with elevated PVR using oxygen, nitricoxide (NO), sodium nitroprusside, prostaglandinE1 or a combination of these drugs in patientswith a PVR > 4 Wood units or a pulmonary vas-cular resistance index (PVRI) > 6 Wood units/m2.It has been demonstrated that adults in whomPVR can be reduced using sodium nitroprus-side or prostaglandin E1 to <2.5 Wood units whilemaintaining a systolic blood pressure >85 mmHghave a postoperative mortality similar to patientswith a resting PVR < 2.5 Wood units. Mortality inpatients with a pre-transplant PVR > 5 Wood unitsand TPG > 15 mmHg who demonstrate a reversiblecomponent to their pulmonary hypertensiondo not have increased mortality. Typically aPVR < 5 Wood units after drug therapy presents anacceptable risk. Because aggressive postoperativeuse of inodilators and selective inhaled pulmonaryvasodilators (NO, prostacyclins) is now routine andbecause PVR naturally tends to drop in the periodfollowing transplantation outcome in patients withelevated PVR has improved.
In children, a PVRI in excess of 6–7 Wood units/m2
and a transpulmonary gradient >15 mmHg havebeen associated with increased postoperative mor-tality. Most centers will consider transplantationif a PVRI < 4–6 Wood units/m2 and a transpul-monary gradient <15 mmHg can be obtainedwith some combination of inotropes, oxygen, NO,sodium nitroprusside, or prostaglandin E1 prior totransplantation.
Effect of heart-rate alterations onhemodynamicsPatients with DCM have a fixed SV and, as aresult, are dependent on maintenance of their heartrate to maintain cardiac output. With exhaustedpreload reserve, reductions in heart rate will notbe accompanied by increases in SV as seen in the
normal heart. Therefore, reductions in heart ratewill be accompanied by cardiac output decreases.Heart-rate increases will reduce diastolic filling timeand will reduce end-diastolic volume (EDV) andSV. Heart rate increases generally will result in nochange in cardiac output because the reductionin SV will be offset by the increase in heart rate.Elevations in right and LAPs by volume infusionto compensate for reduced diastolic filling time arenot practical because they will increase systemic andpulmonary venous congestion. For patients with anischemic DCM, heart-rate increases may exacerbatemyocardial ischemia.
Effect of afterload alterations onhemodynamicsReduced contractility is represented by a linear leftventricular pressure–volume relationship that hasa less positive slope and is shifted rightward. Asthe result of impaired contractile function, patientswith DCM have enhanced sensitivity to afterload(see Fig. 7.1). Small increases in afterload resultin comparatively large increases in ESV. For agiven EDV; this results in a large reduction inSV. Conversely, afterload reduction with mainte-nance of EDV will produce concomitant increasesin SV. This partly explains the unequivocal suc-cess of vasodilator therapy such as ACE inhibitorsin improving NYHA functional class and reduc-ing mortality in patients with end-stage DCM.Aggressive perioperative afterload reduction is dif-ficult considering the low systolic blood pressure ofmost patients with DCM.
The donor
The following guidelines are used to select donorsafter the diagnosis of irreversible brain deathhas been made. Echocardiographic assessment ofdonor ventricular and valvular function is routine.The final decision as whether to accept a donorheart is made by the harvesting surgeon follow-ing visual inspection of the heart and overallassessment of donor suitability and hemodynamicstability.• Age less than 55 years. Most centers have becomemore lenient given the shortage of suitable donors.For a patient who has had a long waiting list interval

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 258 — #7
258 Chapter 7
and who has been difficult to cross-match the riskof taking a heart from an older donor who is a goodcross-match may be preferable to the risk of dyingon the waiting list.• Absence of significant cardiac disease or trauma.Severe myocardial contusion usually is identi-fied by a history of blunt chest trauma, CPK-MBand troponin elevations, and echocardiographicevidence of severe ventricular dysfunction. Patientswho have suffered cardiac arrest are not necessar-ily excluded from consideration but require sub-sequent evaluation of function both clinically andechocardiographically. Generally, a desirable donorheart is maintained with less than 10 µg/kg/min ofdopamine.• Low probability of coronary artery disease.Coronary angiography is not commonly employedin evaluation of younger donors. Many centersevaluate male donors older than 45 years of ageand female donors older than 55 years of age withcoronary angiograms.• No active infection or malignancy with thepossibility of metastases.• Negative serologies for human immunodefi-ciency virus/acquired immunodeficiency syndrome(HIV/AIDS) or hepatitis B and C. Donors are alsotested for toxoplasmosis and cytomegalovirus (CMV).• ABO compatibility and human lymphocyteantigen (HLA) screen. The donor and recipient mustbe ABO blood type compatible. HLA typing forcardiac transplantation is not routine. The recip-ient’s blood is tested against a standard panel ofblood cells containing a diverse human lymphocytesample. This screen is called the panel reactive
antibody (PRA) screen. If the PRA has 5–15%reactivity, most centers will proceed with transplan-tation based on ABO compatibility. If the PRA isgreater than 15%, then a lymphocyte cross-matchbetween donor and recipient blood can be per-formed. This is a time-consuming process, as donorblood must be transported to the transplant center.Pre- and post-transplant therapy with intravenousIgG or plasmapheresis may be indicated. Recently,some success with ABO incompatible transplantshas been achieved in infants due to the imma-turity of infant ABO isohemagglutinins. Table 7.2outlines the transfusion strategy that must accom-pany ABO incompatible transplantation to preventimmunization.• Recipient donor size match. For adult patients,the donor’s body weight should be within 60–150%of the recipient’s weight. For infants and childrenthe donor’s weight should be between 80 and 160%of the recipient’s body weight. Hearts transplantedinto infants and children demonstrate normal car-diac chamber dimensional growth. Most centersprefer donors at the upper limits of size for theiradult and pediatric patients with pulmonary hyper-tension, although data to support this practice arelacking.
Aggressive hormone replacement therapy (HRT)is currently utilized by many centers in the sub-set of heart donors with depressed LV function (leftventricular ejection fraction (LVEF) < 45%) with orwithout hypotension. HRT can be summarized asfollows:• Triiodothyronine (T3) supplementation: 4.0 µgbolus followed by an infusion of 3.0 µg/h.
ABO of heartrecipient
ABO of transfused blood products
ABO ofdonor heart
Plasma Red cells Platelets
O AB AB O ABO B AB or B O AB or BO A AB or A O AB or AB AB AB O or B ABB A AB O or B ABA AB AB O or A ABA B AB O or A AB
Table 7.2 Transfusion strategy for ABOincompatable heart transplantation.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 259 — #8
Heart, Heart-Lung, and Lung Transplantation 259
• Vasopressin supplementation: 1.0 unit bolusfollowed by 0.5–4.0 units/h infusion to treat dia-betes insipidus and normalize systemic vascularresistance (SVR) (800–1200 dynes/s/cm5).• Steroid supplementation: methylprednisolone15 mg/kg bolus.• Insulin supplementation: 1.0 units/h minimum,increase to keep blood sugar 120–180 mg/dL.
Anesthetic management ofthe recipient
Goals1 Avoid increases in afterload; afterload reductioncan be attempted with caution, but EDV must bemaintained.2 Maintain preload.3 Maintain or enhance contractility.4 Maintain heart rate.5 Avoid hypercarbia, hypoxemia, and acidosis thattend to cause pulmonary hypertension and mayresult in acute RV decompensation.
Preoperative evaluationCardiac transplant patients typical1y undergoextensive medical evaluation. A summary of thisevaluation is readily available to the anesthesiol-ogist through the transplant coordinator. Severalunique management problems are common inpatients DCM. Use of an antifibrinolytic shouldbe considered for patients at risk for postoperativebleeding.
Ventricular arrhythmiasMore than 70% of DCM patients have asymp-tomatic, nonsustained ventricular tachycardia seenon ambulatory monitoring. Antiarrhythmic ther-apy is problematic for these patients consideringthe negative inotropic and arrhythmogenic effectsof many of the agents, the altered drug pharmaco-kinetics in heart failure, and the low efficacy of theseagents for patients with severe LV dysfunction. Inaddition, although therapy can reduce ventriculararrhythmias and improve exercise tolerance andventricular function, reduction in the incidence ofsudden death is unproven. An ICD may be nec-essary for patients with symptomatic ventricular
arrhythmias if medical therapy is not effective orcannot be tolerated.
Thromboembolic phenomenaPatients with an EF less than 30% and patientswith atrial fibrillation are particularly at risk for theformation of atrial and ventricular mural thrombiand subsequent systemic or pulmonary emboliza-tion. In addition, patients with left ventricularaneurysms as the result of extensive prior infarctionare also at higher risk for mural thrombus forma-tion. Long-term oral anticoagulation, primarily withcoumadin, is common for patients with DCM. Thiswill complicate the management of hemostasis aftertermination of cardiopulmonary bypass (CPB).
Preoperative mechanical ventricularsupport and the total artificial heartAt present, the limiting factor in the number ofpatients who can be offered a heart transplant is theavailability of donor hearts. In the United States, itis estimated that although 40 000 patients per yearcould benefit from a heart transplant, only approx-imately 2200 heart transplants are performedper year. Furthermore, 20% of suitable transplantcandidates die before a donor heart can be found.As a result, mechanical assist devices and the totalartificial heart are used as a bridge to cardiac trans-plantation until suitable donor hearts arc found.
Previous cardiac surgical proceduresAll patients who have undergone previous car-diac surgical procedures arc likely to have pro-longed dissection times and are at risk for bleed-ing. Adequate intravenous access is a necessity. Allblood products must be CMV compatible and trans-fused through leukocyte filters. Many patients withischemic DCM will have undergone prior coronaryartery bypass surgery. Nicking or cutting of theexisting extracardiac conduits (internal mammaryarteries and reverse saphenous veins) can severelycompromise myocardial perfusion. Likewise, sur-gical manipulation of these conduits may resultin embolization of atherosclerotic plaques into thedistal coronary vascular bed with subsequent trans-mural myocardial ischemia. A determination ofhow much myocardium is supplied by the conduits

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 260 — #9
260 Chapter 7
that are patent can be made from the most recentcatheterization report.
Many children with congenital heart disease willhave undergone prior procedures. Physical exam-ination should include an evaluation of the lim-itations to vascular access and monitoring sitesimposed by previous surgery and catheterizations.A child who has undergone a palliative shuntprocedure may have a diminished pulse or anunobtainable blood pressure in the arm in whichthe subclavian artery has been incorporated intothe shunt. Children who have undergone multi-ple palliative procedures may have poor periph-eral venous access and previous surgical cut-downsites may exist. Children having multiple cardiaccatheterizations may have absent or compromisedfemoral arterial and venous access. Such find-ings have obvious implications regarding arterialand venous catheter placement, sphyingomono-metric blood pressure monitoring, the use of pulseoximetry, and the mode of induction.
PremedicationMost patients will have been called into the hospi-tal on short notice and many will have eaten solidfood in the previous 6–8 hours. In addition, patientswill have taken their initial doses of oral immuno-suppressive drugs, usually cyclosporine and aza-thioprine or mycophenolate moftil. Cyclosporineusually is administered with 10–20 mL of liquid. Toreduce the risk of aspiration in adults and olderchildren, a nonparticulate antacid such as bicitra(30 mL) should be given in addition to intravenousmetaclopromide 10 mg and an H2-receptor blockersuch as ranitidine 50 mg. For infants and smallerchildren, a period of 2–3 hours of NPO (nothingby mouth) status is sufficient and usually tran-spires before induction. Premedication with mida-zolam 0.03–0.05 mg/kg in divided doses works wellto reduce anxiety. In older children with previ-ous multiple opioid and benzodiazepine exposures,intravenous ketamine in doses of 0.5–1.0 mg/kgmay be necessary as well. In children without intra-venous access, oral premedication as will proba-bly be necessary. Supplemental oxygen should beadministered, because hypoxemia will exacerbateexisting pulmonary hypertension.
PreinductionSome transplant patients will be receiving intra-venous inotropic and vasodilator therapy whenthey arrive for surgery. These agents should be con-tinued via a reliable intravenous route. Sterility is ofthe utmost importance because the patients will beimmunosuppressed. All patients should have twolarge-bore peripheral intravenous lines. Electrocar-diogram (ECG) monitoring should allow assessmentof V5, I, II, III, aVR, aVL, and aVF. Normally twoleads (II and V5) are monitored simultaneouslyintraoperatively. A radial artery catheter is placedwith local anesthesia before induction of anesthesia.It is placed after induction in infants and chil-dren. Patient size or the presence of complex intra-cardiac anatomy generally precludes placement ofa pulmonary artery catheter in infants and chil-dren. Pulmonary artery pressures are monitoredpost-CPB with a surgically placed transthoracicPA catheter. Some centers do not place a pul-monary artery catheter in adult patients for hearttransplantation. The advantages of a pulmonaryartery catheter are discussed in Chapter 3. Thedisadvantages as they apply to cardiac transplantpatients are:• Technical difficulty in advancing the catheter inpatients with a dilated RV and low cardiac output.• An increased risk of atrial and ventricular ectopyleading to hemodynamic compromise.• An increased risk of infection.• The catheter must be withdrawn into the sterilesheath during excision of the recipient’s heart.• The catheter must be re-advanced across newsuture lines into the donor heart as CPB isterminated.
Nonetheless, central venous access is necessaryfor pressure monitoring and drug infusion in bothpediatric and adult patients. Some centers pre-fer that the right internal jugular vein not beused perioperatively because it is the preferredroute to obtain the endomyocardial biopsies usedto monitor rejection postoperatively. Placement ofa central large-bore venous sheath for use as areliable site of rapid fluid administration is war-ranted if peripheral access is poor. Multiplanetransesophageal echocardiography (TEE) is utilizedto manage pediatric and adult patients pre- and

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 261 — #10
Heart, Heart-Lung, and Lung Transplantation 261
post-CPB. After transplantation TEE is used toassess left and right ventricular function, mea-sure pulmonary artery pressures (using a tricuspidregurgitation jet), and guide management of pul-monary artery hypertension and RV dysfunction ifnecessary.
Induction and maintenanceThe choice of specific induction agents is less impor-tant than the realization that patients with DCMhave limited contractile reserve; dependence onpreload, and limited ability to respond to acuteincreases or decreases in afterload. In addition, thecirculation time will be slow given the low cardiacoutput state. These patients require an inductionthat will blunt the hemodynamic response to laryn-goscopy and tracheal intubation without unduemyocardial depression, vasodilation, and hypoten-sion. Careful titration of etomidate (0.1–0.3 mg/kg)in combination with 5–10 µg/kg of fentanyl or1–2 µg/kg of sufentanil is useful for induction. A full0.3 mg/kg dose of etomidate is often not neces-sary to induce hypnosis and loss of consciousnessin these patients. This drug combination has min-imal direct effect on heart rate, myocardial con-tractility, peripheral vascular resistance, or venouscapacitance. An overall diminution in central sym-pathetic tone will also contribute to circulatorydepression. Thiopental and propofol are less welltolerated. A nondepolarizing muscle relaxant in adose 2×ED95 such as vecuronium or pancuronium0.02 mg/kg or cisatracurium 0.04 mg/kg is used toassure prompt control of the airway. Pancuroniumis generally reserved for those patients in who alow baseline heart rate. In infants and children thevagolytic and sympathometic effects of pancuro-nium can be used to counteract the vagotonic effectsof fentanyl or sufentanil. Alternatively, rocuro-nium (1.0 mg/kg) or succinylcholine (1–2 mg/kg)can be used to perform a modified rapid sequenceinduction (cricoid pressure during positive pressureventilation) in the patient with questionable NPOstatus.
Anesthesia can be maintained with additionaldoses of opioid in conjunction with a benzo-diazepine (usually midazolam in increments of0.01–0.03 mg/kg) or a low inhaled concentration
(0.5–0.75 MAC) of isoflurane or sevoflurane.Nitrous oxide (N2O) is not a good choice as anadjuvant agent; it has a weak myocardial depres-sant effect that normally is counteracted by thesympathetic outflow it produces. In patients withDCM where elevated catecholamine levels, down-regulated β-receptors, and reduced myocardial NEstores are present, the myocardial depressant effectswill predominate.
In the instance of a child without intravenousaccess a careful inhalation induction with 100%oxygen and sevoflurane following oral medication(ketamine and midazolam) can be considered. Onceintravenous access is obtained anesthesia can bemaintained as described above. An alternative forinduction and maintenance in infants and childrenwith intravenous access is a high-dose narcotic tech-nique (50–75 µg/kg of fentanyl or 5.0–7.5 µg/kg ofsufentanil) in conjunction with a benzodiazepine(usually midazolam) or a low inhaled concentrationof isoflurane or sevoflurane and pancuronium.Caution must be used when benzodiazepines areused in conjunction with synthetic opioids, asthey are synergistic in their effects on venous capac-itance and SVR. This technique is a good choicein infants and children as postoperative intubationventilation for at least 24 hours is usually necessary.
Regardless of the choice of induction and main-tenance agent, episodes of hemodynamic com-promise must be treated promptly. Bradycardiaassociated with hemodynamic compromise can beeffectively treated with a small dose of pancuronium(0.015–0.05 mg/kg) if vecuronium or cisatracuriumhas been used. Atropine should be used cautiously.Atropine administration may initiate tachycardia,and atropine, unlike βl-adrenergic agents, increasesheart rate without any reduction in the dura-tion of systole. Therefore, for equal increases inheart rate, atropine will cause a greater reductionin the duration of diastole and will compromisesubendocardial perfusion to a greater degree thana βl-adrenergic agent. Ephedrine (a direct- andindirect-acting β- and α-agonist) 0.03–0.07 mg/kg isa reliable agent to increase heart rate without com-promising diastole. In addition, the augmentation indiastolic blood pressure obtained is beneficial whenhypotension accompanies bradycardia.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 262 — #11
262 Chapter 7
Tachycardia is detrimental for patients withischemic DCM and should be treated to avoidsubendocardial ischemia and hemodynamic com-promise. The first strategy should be to terminatenoxious stimuli and then increase the depth ofanesthesia as necessary. The use of short- or long-acting beta-blockers is not recommended consid-ering the presence of severely depressed systolicfunction. If hypotension due to reduced SVR occurs,small doses of phenylephrine (0.5–1.5 µg/kg) andvolume infusion (5 mL/kg) to increase preload topreinduction levels usually will correct the problem.Phenylephrine reliably increases SVR. Caution mustbe exercised when α-adrenergic agonists are admin-istered to patients with severe systolic dysfunction.The goal should be to normalize SVR. Overzealoususe of phenylephrine will increase afterload, induceafterload mismatch, and severely reduce SV. If thepatient fails to respond with a prompt increase inaortic blood pressure, an inotropic agent shouldbe started to avoid a downward spiral of ventric-ular dilatation, increased wall stress, reduced SVand further hypotension. Dobutamine or dopamine3–5 µg/kg/min are reasonable choices; dopamineincreases SVR more than dobutamine. Using nox-ious stimulation such as laryngoscopy and intuba-tion to treat hypotension in the lightly anesthetizedpatient with DCM must be avoided. These stim-uli will produce a sudden, dramatic increase inafterload. The subsequent afterload mismatch willproduce ventricular dilatation and may produce anadditional reduction in blood pressure.
When surgical stimulation (skin incision, ster-notomy, sternal spreading, and aortic manipula-tion) produces hypertension, additional doses ofsufentanil (0.5–2.5 µg/kg) or fentanyl (5–25 µg/kg)are indicated. On occasion control of hypertensionrequires the use of vasodilator agents or adjuvantanesthetic agents. Judicious use of low inspired con-centrations of isoflurane or sevoflurane is usuallyeffective. Sodium nitroprusside is a ready titratable,potent arteriolar dilator and can be used effectivelyto treat hypertension. An infusion can be startedat 0.25 µg/kg/min and titrated upward. However,because sodium nitroprusside is a potent arterio-lar dilator, it has the potential to induce a coronarysteal in the presence of the appropriate anatomy.
This may be of concern in patients with DCM ofischemic origin. Nitroglycerin dilates large coronaryvessels and does not dilate arterioles; therefore, it isnot implicated in the steal phenomena. Nitroglyc-erin has it greatest dilating capacity on the venousbeds and arterial dilation occurs only at higherdoses. Despite this, when used in appropriate doses,nitroglycerin and nitroprusside have been shownto be equally effective in treatment of hyperten-sion. For treatment of hypertension, nitroglycerinis started at 0.5 µg/kg/min and may be increasedup to 5 µg/kg/min.
Operative procedure
Three surgical techniques exist for orthotopicheart transplantation: the biatrial technique(Figs 7.2–7.4), the bicaval technique, and thetotal technique. These procedures are performedthrough a median sternotomy with hypother-mic CPB, bicaval cannulation, and aortic cross-clamping. After commencement of CPB using thebiatrial technique the recipient’s heart is excisedto just above the atrioventricular groove, leaving:a large cuff of left atrium containing all four pul-monary veins, a large cuff of right atrium containingthe superior vena cava (SVC) and inferior vena cava(IVC), the ascending aorta just distal to the aorticvalve, and the main pulmonary artery just distal tothe pulmonic valve.
The donor left and right atria are anastomosedto the cuffs of the recipient left and right atriawhile the donor and recipient aorta and pulmonaryartery are anastomosed. This technique creates largeatrial cavities with abnormal geometry. This resultsin a less than optimal contribution of atrial sys-tole to ventricular filling. In addition, the distortedanatomy contributes to the development of func-tional mitral and tricuspid regurgitation. It also isassociated with the development of atrial septalaneurysms, atrial thrombus, and sinus node injury.
These problems have led to application of themore anatomical bicaval and total techniques.Currently, the bicaval technique is the most com-mon technique used. These techniques result in bet-ter atrial function, a lower incidence of early and lateatrial arrhythmias, and less tricuspid regurgitation.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 263 — #12
Heart, Heart-Lung, and Lung Transplantation 263
(a)
(b)
Fig. 7.2 Operative technique for biatrial orthotopicheart transplantation. (a) The recipient heart has beenexcised leaving a cuff of right atrium containing thesuperior vena cava (SVC) and inferior vena cava (IVC)and a cuff of left atrium containing all four pulmonaryveins. The beginning of the left atrial anastomosis isdepicted. The sinoatrial (SA) node of the donor heartis depicted by the dashed oval in the right atrium. Thedonor SVC is ligated. (b) Details of the anastomosisbetween the recipient and donor left atria.
Whether they will result in long-term freedom frompacemaker implantation and better cardiac functionremains to be determined.
In the bicaval technique, the recipient’s atria arecompletely excised, leaving the SVC, the IVC, anda small cuff of left atrium containing all four pul-monary veins. In the total technique, the recipient’satria are completely excised, leaving the SVC, theIVC, and two small cuffs of left atrium: one contain-ing the two right pulmonary veins and the other
(a)
(b)
Fig. 7.3 (a) The left atrial anastomosis is completeand the new intra-atrial septum is being completed.(b) The right atrial anastomosis is being completed usinga portion of the donor IVC.
the two left pulmonary veins. In the bicavaltechnique, there are five anastomoses: the donorSVC, IVC, and posterior left atrium are anastomosedto the recipient SVC, IVC, and one pulmonary veincuff while the donor and recipient aorta and pul-monary artery are anastomosed. In the total tech-nique there six anastomoses: the donor SVC, IVC,and posterior left atrium are anastomosed to therecipient SVC, IVC, and two pulmonary vein cuffswhile the donor and recipient aorta and pulmonaryartery are anastomosed.
For children with congenital heart lesions, thetechnical aspects of the surgical procedure are morechallenging. For example, for patients with HLHS,the aorta must be reconstructed. For children hav-ing undergone a Fontan or bidirectional Glennprocedure, a caval reconstruction may be necessary.Pulmonary artery (PA) reconstruction may be

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 264 — #13
264 Chapter 7
Fig. 7.4 Details of the completed aortic and pulmonaryartery anastomoses. The aortic cannula and cross-clampare depicted. In an effort to reduce the ischemic interval,the surgeon may release the aortic cross-clamp aftercompletion of the atrial and aortic suture lines andcomplete the pulmonary artery anastomosis while theheart is being re-perfused.
necessary for patients with pulmonic atresia or RVto PA conduits.
Post-CPB management
Goals1 Maintain sinus rhythm at 100–120 b/min inadults and older children and at 130–150 b/min inneonates and infants. Atrial or atrioventricular (AV)sequential pacing may be required.2 Avoid pulmonary artery hypertension by treatinghypercarbia, hypoxemia, and acidosis.3 Aggressively treat pulmonary artery hyperten-sion with vasodilator therapy to avoid RV failure.If RV failure does occur, inotropic support of the RVand pulmonary vasodilation may be necessary.4 Maintain right atrial pressure (RAP) and LAP tooptimize SV in the setting of increased ventricularstiffness.5 Inotropic support of the LV may be necessary ifthe ischemic interval is long.
Preparation for termination of CPBThe following issues need to be considered whenformulating a plan for termination of CPB in apatient with a newly transplanted heart.
Impaired systolic functionSystolic dysfunction in the donor heart may occurfor a variety of reasons.• Ischemia-reperfusion injury. This is the mostcommon cause of allograft systolic dysfunctionpost-CPB. Preservation of the donor heart involvesapplication of the aortic cross-clamp and deliveryof cold cardioplegia to induce arrest in diastole,followed by cold storage at 4C. The ischemic inter-val, the time from when the aortic cross-clampis applied in the donor until the aortic cross-clamp is removed after implantation of the heartin the recipient is extremely important. The longerthis ischemic interval, the more likely there is tobe biventricular systolic dysfunction secondary tomyocardial fibrosis. Because there is an incremen-tal increase in mortality with ischemic times greaterthan 3.5 hours, it is desirable to keep the interval atless than 4 hours. In an effort to reduce the ischemicinterval, the surgeon may release the aortic cross-clamp after completion of the atrial and aortic suturelines and complete the pulmonary artery anastomo-sis while the heart is being reperfused. Prolongedand excessive inotropic support of the donor heartbefore cross-clamping also is undesirable because itcontributes to post-transplant ischemic dysfunction.• Brain death. Abrupt increases in intracranialpressure as the source of brain death result ingreater degree of myocardial ischemia and necro-sis (particularly of the RV) than gradual increases inintracranial pressure. There is evidence that earlysurvival following heart transplantation is reducedin patients receiving hearts from donors dying ofgunshot wounds to the head and from donorsdying from spontaneous intracranial hemorrhage.Donors who experience brain death as the result of asudden rise in intracranial pressure exhibit a hyper-dynamic cardiovascular response, massive increasesin plasma epinephrine, and histological evidence ofsevere myocardial ischemia and necrosis.• Hyperacute rejection. This rare event is caused byABO blood group incompatibility or cytotoxic recip-ient antibodies directed against donor lymphocytes.It presents as cyanosis and mottling of the allo-graft in conjunction with profoundly impaired sys-tolic function. It is impossible to separate thesepatients from CPB for any extended period of time.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 265 — #14
Heart, Heart-Lung, and Lung Transplantation 265
The only therapy available is excision of the allo-graft with placement of a total artificial heart. Thistype of rejection is preventable by careful donor andrecipient ABO typing and PRA screening.• Myocardial contusion. Patients with severe myocar-dial contusions are excluded as donors. Patientswith lesser degrees of dysfunction from blunttrauma may exhibit impaired systolic function inthe post-CPB period.• Myocardial infarction. As a result of the carefulscreening of donors this is a very rare cause of imme-diate allograft dysfunction. With an increase in theacceptable age for donors, this is likely to become amore common problem.
RV afterload mismatchImpaired right ventricular performance is a partic-ular risk in the presence of recipient pulmonaryhypertension. RV afterload mismatch may occur asthe result of severely depressed RV systolic func-tion and normal pulmonary artery pressure (PAP)and PVR or, more commonly, as the result of lessseverely depressed RV systolic function and elevatedPAP and PVR. This may result in acute allograftRV dysfunction severe enough to prevent termi-nation of CPB. Therapy in this setting will need tobe directed toward inotropic support of the RV andselective reduction of PVR.
Sinus and AV node dysfunctionIschemic injury to the sinus and AV node may pro-duce bradycardia, nodal rhythm, or heart block.Sinoatrial (SA) node dysfunction is much morecommon and approximately 10–20% of patientsneed permanent atrial pacing. In some instances, anappropriate sinus rate can be obtained with isopro-terenol. In other instances, atrial or AV sequentialpacing is necessary.
Impaired diastolic functionThe post-ischemic state of the transplanted heartis characterized by increased ventricular stiffnessand limited preload reserve resulting in a fixedSV. Increases in heart rate obtained with pacingwill reduce diastolic filling time (see Fig 5.8). This,in turn, will produce reductions in EDV and SV for agiven ESV. The net result will be little or no change
in cardiac output. Atrial or AV sequential pacing islikely to be superior to ventricular pacing due tothe presence of an appropriately timed atrial sys-tole. For a given right or left atrial pressure, atrialpacing or AV sequential pacing will provide a higherventricular EDV than ventricular pacing.
Inotropic support is useful for patients withlimited preload reserve in both sinus and pacedrhythms because SV can be augmented at a givenafterload by reducing ESV. Inotropic agents allowSV to be maintained as heart rate increases, therebyproducing increases in cardiac output. This occursbecause the reductions in EDV produced by reduceddiastolic filling time are offset by the reductions inESV produced by enhanced contractility. Optimalheart rate is 100–110 b/min for adults and olderchildren, whereas 130–150 b/min is optimal forneonates and infants. Higher heart rates resultin progressive reductions in SV such that cardiacoutput remains constant or falls.
Termination of CPBTerminating of CPB is discussed in detail inChapter 10. Particular attention must be paid todeairing the heart. Severe ventricular dysfunctionmay follow ejection of air down the coronaryarteries. The RV is particularly at risk because of theanterior location of the right coronary ostia. TEE isvaluable in guiding the deairing process.
A dose of methylprednisolone (usually 10 mg/kgin children and 500 mg in adults) will be given afteraortic cross-clamp removal. In some institutions, thedose will be given after termination of CPB.
Historically, isoproterenol, which is a potentchronotrope, dromotrope, inotrope, and vasodila-tor, has been used to enhance cardiac output dur-ing the immediate post-CPB period. Isoproterenolworks well for patients in whom minimal inotropicsupport of the RV and LV is necessary. This ismost likely when the donor heart requires min-imal inotropic support before cross-clamping, theischemic interval is short, and recipient pulmonaryartery pressure is low or mildly elevated. Generally,isoproteronol is infused at 0.01–0.05 µg/kg/min(adults) or 0.05–0.25 µg/kg/min (children). Atthese doses, heart rate is maintained in an age-appropriate range, inotropic support of the RV and

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 266 — #15
266 Chapter 7
LV is provided, and PVR and SVR are reduced.Higher doses of isoproterenol increase the incidenceof hemodynamic changes that are unfavorableto the myocardial energetics of the post-ischemicheart. Isoproterenol increases myocardial oxygenconsumption (MVo2), reduces aortic diastolic bloodpressure, is arrhythmogenic, and increases heartrate. All of these variables tend to exacerbatemyocardial ischemia. Furthermore, as the doseof isoproterenol increases, it may be difficult tomaintain systemic blood pressure due to pro-hibitive decreases in SVR. Due to these side effects,doses in excess of 0.01–0.05 µg/kg/min (adults) or0.05–0.25 µg/kg/min (children) are rarely useful asa means of providing additional inotropic supportor as a method of increasing heart rate. For thisreason many centers have moved away from iso-proterenol as first line therapy in cardiac transplantpatients using other inotropic agents and pacing asnecessary.
When isoproterenol is ineffective in producingthe desired heart rate, atrial or AV sequentialpacing should be initiated. This combination willallow maintenance of SV as heart rate is increased.When isoproterenol is ineffective in producing thedesired inotropic effect, alternative inotropic agentsshould be promptly initiated. The need for addi-tional inotropic support can be determined witheither TEE or a pulmonary artery catheter. TEE willreveal ventricular dilatation and global hypokinesis.Regional wall motion abnormalities are also possi-ble, but the ischemic insult usually is diffuse. Atrialenlargement and dilation of the mitral or tricuspidvalve annulus with subsequent mitral or tricuspidregurgitation also is possible. Pressure monitor-ing will reveal an elevated central venous pres-sure (CVP) (>15 mmHg), elevated pulmonary arteryocclusion pressure (PAOP) (>20 mmHg), or both.Cardiac output will be reduced (<2.0 L/min/m2).The advantage of the pulmonary artery catheteris that it allows measurement of PAP and calcula-tion of PVR and SVR. PAP can be estimated withTEE using a tricuspid regurgitation jet and the CVPmeasurement.
The properties of the various inotropic agentsare reviewed in detail in Chapter 4. The choiceof agent should be tailored to the clinical
picture. Epinephrine 0.01–0.10 µg/kg/min (adults),0.05–0.50 µg/kg/min (children), or dopamine5–10 µg/kg/min is a better choice than dobu-tamine or milrinone when SVR and systemic bloodpressure are low. Dobutamine 5–10 µg/kg/min ormilrinone 0.50–0.75 µg/kg/min after a 50 µg/kgloading dose are better choices when PAP and PVRare elevated. Milrinone is a fairly potent inodila-tor with salutatory effects on PVR. Its use inadults often requires a simultaneous infusion of NE(0.01–0.10 µg/kg/min) to maintain SVR and bloodpressure. This is generally not necessary in infantsand children.
When RV afterload mismatch exists with pre-served LV systolic function, there will be lowcardiac output, low systemic blood pressure, ele-vated CVP, elevated PAP, and low PAOP. TEEwill reveal a dilated right atrium and ventriclewith an under filled, hyperkinetic LV. Tricuspidregurgitation will be likely.
Therapy for RV failure involves inotropic sup-port and pulmonary vasodilatation. Pulmonaryvasodilatation with intravenous agents is prob-lematic because simultaneous reduction of SVRoccurs. Simultaneous reduction of a normal SVRmay compromise RV and systemic organ perfu-sion. Isoproterenol has historically been used dur-ing the post-cardiac transplant setting. Althoughisoproterenol is a potent inotrope and a pul-monary vasodilator, it is not a selective pul-monary vasodilator. Its β2 effects cause parallelreductions in PVR and SVR. Other intravenouspulmonary vasodilators have been evaluated inheart transplant patients. Prostaglandin El (PGE1),prostacyclin (PGI2), sodium nitroprusside (SNP),and nitroglycerin (NTG) are pulmonary vasodila-tors. Unfortunately, they are not selective pul-monary vasodilators because they cause reductionsin SVR as well. In theory, PGE1 should be a selec-tive pulmonary vasodilator because it undergoegs apronounced first-pass elimination in the lungs whilePGI2, SNP, and TNG are metabolized in one circu-lation time. In reality, all four drugs reduce PVRwhile causing a decrease in SVR such that the ratioof PVR:SVR is unchanged or, in the case of PGI2,slightly increased. Efforts to reduce PVR with PGE1,PGI2, SNP, and TNG may require simultaneous

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 267 — #16
Heart, Heart-Lung, and Lung Transplantation 267
use of inotropes and vasoconstrictors to maintainsystemic blood pressure. The simultaneous use ofinotropic support is of benefit to the afterload mis-matched RV as well. Use of PGI2 to reduce PVRseems to result in better maintenance of SV and car-diac output than PGE1, TNG, and SNP due to less ofa venodilating effect.
The use of the inhaled selective pulmonaryvasodilator NO has revolutionized treatment ofpulmonary hypertension and associated RV after-load mismatch. Aerosolized, inhaled PGI2 has a sim-ilar profile to inhaled NO. These agents are selectivefor the pulmonary circulation as no substantial con-centrations are delivered to the systemic circulationfollowing inhalation. NO delivered at 20 ppm selec-tively reduces PVR in all heart transplant recipients.Evidence suggests that the peak effect in reduc-ing PVR with NO occurs at 20–40 ppm. Continuousaerosolized PGI2 is delivered at 5–50 ng/kg/min.These agents are discussed in more detail inChapter 6.
In addition to pharmacologic methods, effortsto reduce PVR with ventilatory interventions areessential. This topic is reviewed in detail inChapter 6. A combination of a high fraction ofinspired oxygen (FiO2), an arterial partial pressureof oxygen (PaO2) > 60 mmHg, an arterial partialpressure of carbon dioxide (PaCO2) of 25–32 mmHg,a pH of 7.50–7.60, and low inspiratory pres-sures without high levels of positive end-expiratorypressure (PEEP) will produce reliable reductionsin PVR.
It is important to rule out a mechanical cause ofincreased impedance to RV ejection when RV dys-function exists in the presence of low pulmonaryartery pressures. Kinking of the pulmonary arteryanastomosis has been observed to cause mechani-cal obstruction of the RV. Kinking may be observeddirectly by the surgeon. Alternatively, it may bedetected by TEE. It also is diagnosed readily by directmeasurement of a pressure gradient between the RVand PA.
When univentricular or biventricular failure issevere and refractory to inotropic and vasodila-tor agents, a ventricular assist or circulatory assistdevice may be necessary to support circulation untilthe ventricles can recover.
Noncardiac surgery in thepost-cardiac transplant patient
The success of heart transplantation makes it likelythat anesthesiologists will encounter patients withtransplanted hearts for a variety of noncardiacsurgical procedures. Currently, the steepest drop insurvival following adult heart transplant occurs inthe first 6 months (to approximately 90% survival).For patients surviving beyond 1 year the conditionalhalf-life (time to 50% survival) is 12 years. There is asteady linear decrease in survival beyond 6 monthsof approximately 3.4% per year. Similar results existin children with the conditional half-life 17.5 yearsin the 1–10 year age group and 13.7 years in the11–17 year age group. Infant conditional survivalappears to be similar to that in the 1–10 year agegroup.
Some of the surgical procedures are purely elec-tive, whereas others are likely to be urgent oremergent. Most surgical procedures are the directresult of complications of immunosuppressive ther-apy. These complications are listed in Table 7.3. Themost commonly used immunosuppressive agentsare summarized in Table 7.4. The incidence ofcomplications requiring general surgical consulta-tion in heart transplant patients is 35–40%. Manyof these complications require operative interven-tion. Progression of atherosclerotic vascular diseasealso results in surgical intervention for aortic andperipheral vascular surgery. Finally, heart trans-plant patients undergo all types of elective surgery,including cosmetic surgery.
Table 7.3 Complications of immunosuppressionthat may require operative intervention.
Gingival hyperplasia – cyclosporine
Pancreatitis – azathioprine, corticosteroids
Cholelithiasis and cholecystitis – cyclosporine
Malignancies
Complications of corticosteroid use: cataracts, retinaldetachment, aseptic bone necrosis, perforated viscus,and gastrointestinal hemorrhage
Complications of infection

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 268 — #17
268 Chapter 7
Table 7.4 Immunosuppressive agents.
Agent Classification Mechanism of action Clinical use
Prednisonemethylprednisolone
Corticosteroid Nonspecific blockade of T-cellcytokine and cytokinereceptor production
Maintenance therapyTreatment of rejection
Cyclosporine Calcineurine inhibitor NFAT (nuclear factor)mediated inhibition of IL-2promoter gene
Maintenance therapy
Tacrolimus (FK506) Calcineurine inhibitor NFAT (nuclear factor)mediated inhibition of IL-2promoter gene
Maintenance therapy
Azathioprine Antimetabolite,6-mercatopurine derivative
Inhibitor of T-cell proliferation Adjuvant therapy
Mycophenolatemofentil (MMF)
Inhibitor of de novo purinesynthesis
Inhibitor of T-cell proliferation Adjuvant therapy in lieu ofazathioprine
Sirolimus Anti-proliferative agent(rapamycin inhibitor)
Blocks G1 to S phase of thecell cycle, inhibitor of T-cellproliferation
Adjuvant therapy in lieu ofazathioprine or MMF
Everolimus Anti-proliferative agent(rapamycin inhibitor)
Blocks G1 to S phase of the cellcycle, inhibitor of T-cellproliferation
Adjuvant therapy in lieu ofazathioprine or MMF
OKT3 Monoclonal antibody Antibody to T-cell receptorcomplex (native andactivated T cells)
Induction therapy
Basiliximab Monoclonal antibody Antibody to IL-2 receptor(activated T cells)
Induction therapy
Daclizumab Monoclonal antibody Antibody to IL-2 receptor(activated T cells)
Induction therapy
Rabbit antithymocyteγ-globulin (RATG)
Polyclonal antibody Antibody to T cells (native andactivated T cells)
Induction therapy
IL, interleukin.
Physiology of the transplanted heart
Autonomic nervous systemRegardless of the surgical technique used, the ortho-topically transplanted heart is devoid of sympatheticand parasympathetic innervation. The most impor-tant consequence of this is an altered barorecep-tor response. Normally, vagal afferent fibers fromthe atria and ventricles produce tonic inhibitionof central sympathetic outflow. When atrial andventricular volumes are reduced, vagal afferent
outflow is reduced and central sympathetic outflowincreases. In addition, activation of carotid and aor-tic baroreceptors by hypotension increases centralsympathetic outflow. The result is direct sympa-thetic stimulation of the heart and generation ofcirculating catecholamines.
In the transplanted heart, no direct sympatheticstimulation of the heart is possible. Response toactivation of baroreceptors in the patient witha transplanted heart is dependent on generationof circulating catecholamines for inotropic and

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 269 — #18
Heart, Heart-Lung, and Lung Transplantation 269
chronotropic response. It normally takes severalminutes to generate appropriate levels of circulatingcatecholamines. Although systemic catecholaminegeneration in response to arterial hypotension isenhanced, reflex systemic catecholamine releasein response to reduced atrial and ventricular vol-umes is impaired due to atrial and ventricularvagal deafferentation. As a result, abrupt decreasesin blood pressure will not be compensated forquickly.
The response of baroreceptors to endogenousand exogenous vasopressors in heart transplantpatients is normal, but feedback to the donor heartis absent. Therefore, increases in blood pressurewill be accompanied by a reflex decrease in recip-ient atrial rate but not in donor atrial rate. As aresult, there will be no reflex decrease in the trans-planted heart rate in response to phenylephrineor NE-induced hypertension. Likewise, Valsalva orother vagal maneuvers will not elicit a heart rateresponse.
Early in exercise, increases in cardiac output areacquired by increases in SV, with EDV increas-ing and ESV remaining unchanged. As exerciseprogresses, cardiac output increases as the resultof systemic catecholamine-induced increases inheart rate with maintenance of SV. Cardiac den-ervation produces presynaptic super-sensitivity dueto denervation-associated loss of neuronal cate-cholamine uptake. As a result, there is increasedsensitivity to catecholamines that are taken up byadrenergic nerve terminals (epinephrine, NE) withno increase in sensitivity to catecholamines that arenot taken up (isoproteronol).
Some degree of reinnervation of the LV withefferent sympathetic fibers is present in 80% oftransplant patients 3 years after transplantation.Reinnervation seems to be progressive but is likelynot complete until 15 years after transplantation.Patients with reinnervation have improved heartrate and contractile response to exercise and bet-ter exercise tolerance than patients without rein-nervation. The ability of some transplant patientsto experience angina is consistent with reinnerva-tion with sympathetic afferents. Reinnervation ofcardiac vagal afferents is unlikely however. Thereis some evidence that over time the recipient
(old) AV node may affect the donor (new) AVnode via conduction over the suture line. In sum-mary, sympathetic efferent and afferent reinnerva-tion may occur in some patients during the yearsafter cardiac transplantation. When reinnervationoccurs, it has physiologic importance.
Heart rateThe resting atrial rate of the transplanted humanheart is approximately 90–110 b/min. This is sig-nificantly greater than the resting atrial rate ofthe innervated human heart and demonstrates thatthe predominant effect on sinus rate in man isa slowing effect of the parasympathetic system.Heart rate increases with exercise in heart trans-plant patients are achieved through stimulation ofcardiac β2-receptors by circulating catecholamines.The increases in heart rate do not occur until afterseveral minutes of exercise and they parallel theincrease in serum catecholamines. Despite this, theheart-rate response with exercise in transplantedhearts is attenuated relative to that seen in nor-mal hearts due to the lack of efferent innervationof the SA node.
LV systolic functionThe LV of the transplanted heart exhibits normalcontractile function. Left ventricular end-diastolicvolume (LVEDV) and left ventricular end-systolicvolume (LVESV) are reduced, whereas SV andEF remain normal or low normal due to theparallel reductions in EDV and ESV. LV massis increased due to concentric hypertrophy asthe result of the arterial hypertension, whichaccompanies cyclosporine immunosuppression.
RV systolic functionThe RV exhibits normal systolic function. Right ven-tricular end-diastolic volume (RVEDV) and rightventricular end-systolic volume (RVESV) are largerthan normal, and RV wall thickness is increased.This is probably secondary to the persistent tri-cuspid regurgitation present in most patients. Inpatients with preoperative pulmonary hyperten-sion, persistence of RV dilatation and tricuspidregurgitation is the result of remodeling of the donorRV in response to recipient pulmonary circulation.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 270 — #19
270 Chapter 7
The dilation and tricuspid regurgitation may persistdespite resolution of pulmonary hypertension.
Atrial functionFollowing the biatrial technique, both right and leftatrial areas are larger than normal. These patientshave reduced right and left atrial emptying com-pared with normal subjects; the portion of totalatrial emptying contributed by the recipient atriumis much less than that contributed by the donoratrium. In addition, the asynchronous contrac-tion of donor and recipient atrium results in widevariations in diastolic flow. Following the bicavaltechnique, patients have right atrial emptying com-parable to normal subjects. Left atrial emptying,although reduced compared with normal subjects,is superior to that seen in biatrial technique patients.In addition, the left and right atrial dimensionsare smaller in patients with the bicaval or totaltechnique as compared with the biatrial technique.
Diastolic functionLV diastolic dysfunction occurs immediately afterorthotopic cardiac replacement and is related to thepost ischemic state. This dysfunction is character-ized by a restrictive ventricular filling pattern thatimproves during the first several months after trans-plantation. This restrictive pattern may manifestclinically as reduced preload reserve in response toexercise and afterload increases. The etiology of thiscontinued dysfunction is unclear. It may be inher-ent to the small allograft LVEDV. Whether patientswho receive hearts from donors smaller than them-selves may be at particular risk for reduced preloadreserve is debatable. Rejection episodes are knownto impair diastolic function, but it is unclear whetherrecurring rejection episodes produce progressiveLV and RV diastolic dysfunction in the form of arestrictive/constrictive pattern.
There also is deficient acceleration of LV relax-ation during exercise, which along with restrictiveinflow, contributes to the elevations in left ven-tricular end-diastolic pressure (LVEDP) and LAPseen during exercise. This impairment of relaxationmay be due to loss of adrenergic tone due to den-ervation, ischemic injury at the time of harvest, orimmunosuppression-induced arterial hypertension.
Issues unique to heart transplantpatientsCardiac transplant patients have a unique set ofmanagement issues, in addition to those associ-ated with the denervated heart. They are outlinedbelow.
Cardiac allograft vasculopathyThis is currently the late survival-limiting factorafter heart transplantation. In adults it accounts forone-third of the late deaths after transplantation asthe result of myocardial infarction, congestive heartfailure, and sudden death. In children it accounts for40% of the deaths between 3 and 5 years after trans-plantation. The incidence of cardiac allograft vascu-lopathy (CAV) in both adult and pediatric cardiactransplant patients is approximately 10% per yearpost-transplant with an incidence of approximately50% at 5 years.
The pathogenesis of CAV is complex, multifac-torial, and incompletely understood. It is believedthat immunologic mechanisms (number of HLAmismatches and the number and duration of rejec-tion episodes) in conjunction with nonimmunologicrisk factors (CMV seropositivity, hyperlipidemia,hypertension, older age at transplantation, diabetes)produce endothelial injury with subsequent myoin-timal hyperplasia. Unlike atherosclerotic coronaryartery disease (CAD), CAV is associated with con-centric, diffuse lesions that do not disrupt the elasticlamina and that progress rapidly. Focal, traditionalatherosclerotic plaques also are seen in cardiacallografts.
Surveillance for CAV is difficult. Patients withheart transplants may not experience angina ortypical ECG changes with myocardial ischemia andinfarction due to afferent sympathetic denerva-tion. Noninvasive testing has poor sensitivity andspecificity. Intravascular ultrasound (IVUS) is thegold standard for detection of CAV but it is tech-nically demanding, expensive, and limited by thesize of the catheter to investigation of vessels of1 mm in diameter or more. Considering these lim-itations, transplant centers currently use yearlycoronary angiography as a screen for CAV. Morefrequent angiograms may be indicated to monitorprogression in individual patients.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 271 — #20
Heart, Heart-Lung, and Lung Transplantation 271
Therapeutic options are limited. More invasiveapproaches involve angioplasty and coronary stentplacement. With this approach, short-term morbid-ity and success is similar to that seen in atheroscle-rotic disease, but the restenosis rate is high andlong-term prognosis remains poor. Drug elutingstents may prove to be more effective in the long-term. Finally, in the most severe cases, coronaryartery bypass surgery and retransplantation havebeen used. The diffuse nature of the coronarylesions makes bypass surgery an option only inselected cases. The survival rates for retransplanta-tion are significantly less than for initial transplan-tation and the incidence of malignancy is twice thatof first transplants.
HypertensionArterial hypertension is present in 75% of trans-plant patients at long-term follow-up. This is notrelated to the conventional risk factors associ-ated with hypertension but to immunosuppressionmediated increases in SVR and to denervation ofcardiac volume receptors. Immunosuppression withcalcineurin inhibitors (particularly cyclosporineversus tacrolimus), and corticosteroids is implicated.Therapy is necessary to prevent severe LV hyper-trophy and impaired ventricular function. Thisusually requires treatment with multiple classesof antihypertensive agents. Calcium entry blockersand ACE inhibitors often are used as first-linetherapeutic agents.
Atrial and ventricular arrhythmiasThe incidence of atrial and ventricular arrhythmiasduring initial hospitalization after transplantationis 55% and 79%, respectively. At late follow-up,the incidence of atrial and ventricular arrhythmiasis 40%. In general, atrial arrhythmias during theinitial hospitalization are benign, except for atrialfibrillation. Development of atrial fibrillation is asso-ciated with a threefold increase in the risk of death.The risk of death is particularly high in patients whodevelop atrial fibrillation more than 2 weeks aftertransplantation.
Permanent atrial pacing is required in approx-imately 10–20% of both pediatric and adultrecipients with symptomatic and asymptomatic
bradycardia. Development of bradycardia seems tobe related to a longer ischemic interval for the donorheart.
Subacute bacterial endocarditis (SBE)prophylaxisBacterial endocarditis is a rare complication inheart transplant patients. Nonetheless, because ofthe extent of the suture lines and the immuno-suppressed status of the patient, SBE prophylaxisis recommended the American Heart Association(AHA).
RejectionMost patients have at least one acute rejec-tion episode despite adequate immunosuppres-sion. These episodes usually occur within thefirst 3 months after transplantation with decreasingincidence thereafter. Surveillance during the firstyear is accomplished with endomyocardial biopsiesof the RV via the right internal jugular vein everyweek for the first 4–8 weeks. Some centers do notperform biopsies in children younger than 6 monthsold or less than 5 kg in weight unless it is to con-firm suspected rejection. Biopsies are graded from0 to 3 based on histologic criteria. No rejection is 0R,mild rejection is 1R, moderate rejection is 2R, andsevere rejection is 3R. After the first year, an annualbiopsy is performed in most institutions in conjunc-tion with coronary angiography to evaluate CAV. Ifclinical evidence of rejection exists, more frequentbiopsies may be indicated to document rejectionand to assess regression of histologic changes withtreatment.
Mild rejection frequently resolves spontaneouslyand is not treated. Mild rejection by biopsy usuallyis not associated with clinical evidence of allo-graft dysfunction such as hypotension, elevatedjugular venous pressure, rales, sinus rate >110,atrial fibrillation, bradycardia, or systolic dysfunc-tion by echo. Moderate or more severe rejectionis accompanied by evidence of allograft dysfunc-tion and is treated. Although normal allografts havemaintained coronary vasodilator reserve, moder-ate allograft rejection is associated with impairedreserve. Normal reserve returns after treatmentof rejection. Rejection also is accompanied by

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 272 — #21
272 Chapter 7
an attenuated coronary vasodilatory response tonitroglycerin.
First-line therapy for moderate rejection is oral orintravenous pulsed steroids. In the approximately10% of cases in which mild rejection by biopsy isassociated with allograft dysfunction, pulsed steroidtherapy is necessary. Severe rejection usually istreated with steroids and, in some institutions,a lympholytic agent such as polyclonal antithymo-cyte globulin (ATG) or murine monoclonal antibody(OKT3) is added.
Response to drugsThe response to various drugs is altered in hearttransplant patients secondary to the denervatedstate of the allograft:• Digoxin. Digoxin prolongs AV node conductionin a biphasic manner. The initial effect is mediatedvagally and is absent in the transplanted heart. Thechronic effect is mediated directly and is present inthe transplanted heart. The inotropic properties alsoare directly mediated and present.• Muscarinic antagonists. Atropine, glycopyrrolate,and scopolamine produce competitive inhibition ofacetylcholine at the muscarinic receptors of post-gangionic cholinergic nerves such as the vagus. As aresult, these drugs will not increase heart rate in thedenervated transplanted heart. The effects of thesedrugs on other organs with muscarinic cholinergicinnervation will remain.• Acetylcholinesterase inhibitors. The contention thatagents such as neostigmine and edrophoniumhave no cardiac effects while they continue tohave systemic muscarinic effects has been chal-lenged recently. Bradycardia after administrationof neostigmine, which was reversed with atropine,has been demonstrated in a heart transplantpatient. In addition, sinus arrest after administra-tion of neostigmine and glycopyrrolate for rever-sal of neuromuscular blockade reversal has beenreported in heart transplant patients. Neostig-mine produces direct stimulation of cholinergicreceptors on cardiac ganglion cells with subse-quent release of acetylcholine. In addition, thereis allograft denervation hypersensitivity of boththe postganglionic neurons and the muscarinicmyocardial receptors. These factors, combined with
intrinsic allograft SA node dysfunction may pro-duce severe SA node dysfunction or sinus arrestafter acetylcholinesterase inhibitor administrationin heart transplant patients.• Beta-adrenergic agonists. There is increased sensitiv-ity to catecholamines that are taken up by adren-ergic nerve terminals (epinephrine, NE) with noincrease in sensitivity to catecholamines that are nottaken up (isoproterenol), Improvements in systolicfunction with β-adrenergic agents are obtainableduring acute rejection episodes.• Beta-adrenergic antagonists. These agents retaintheir usual activity. The sinus rate of both the donorand recipient slow equally, demonstrating that thepredominant effect is caused by blockade of circu-lating catecholamines. There also will be a normalincrease in the refractoriness of the AV node.• Calcium entry blockers. These agents directly sup-press the sinus and AV nodes and, thus, shouldhave normal activity. Nonetheless, the negativechronotropic and dromotropic effects of verapamilhave been demonstrated to be more pronouncedin the transplanted heart. There will be no reflextachycardia from agents with strong vasodilatorproperties such as nifedipine.• Vagolytic and vagotonic agents. Drugs with vagolyticactivity (pancuronium, demerol) will not increaseheart rate, whereas drugs with vagotonic activity(fentanyl, sufentanil) will not decrease heart rate.• Adenosine. The magnitude and duration ofadenosine’s negative chronotropic and dromotropiceffects is 3–5 times greater in the transplanted heart.• Ephedrine. Cardiac drugs that are both direct andindirect acting will have a diminished effect becauseonly the direct effect will be present.
Anesthetic considerations fornoncardiac surgery in patientspost heart transplantationA variety of regional and general anesthetic tech-niques have been used safely and successfully inthe anesthetic management of patients with hearttransplants. In patients without evidence of allograftdysfunction, the following principles are useful:1 Aseptic technique is essential.2 Appreciate that compensation for acute alter-ations in preload, afterload, and contractility

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 273 — #22
Heart, Heart-Lung, and Lung Transplantation 273
are incomplete and delayed; postural effects aremagnified.3 Heart rate and blood pressure increases dueto inadequate anesthesia will be delayed untilcirculating catecholamine levels increase.4 Bradycardia will compromise cardiac output.Baseline SV is reduced and any reflex increase in SVin response to bradycardia is delayed. Atropine willnot increase heart rate. Isoproterenol and ephedrinewill increase heart rate.5 Acetylcholinesterase inhibitors (neostigmine,edrophonium) for reversal of neuromuscular block-ade may have cardiac effects. Anticholingeric agents(atropine, glycopyrrolate) must be given to blockthe peripheral muscarinic effects.6 CVP monitoring, when indicated, may have tobe obtained via a route other than the right internaljugular vein.7 Reflex bradycardia will not accompany admin-istration of vasopressor agents (phenylephrine),nor will directly induced bradycardia accompanyadministration of agents with vagotonic activity.8 Reflex tachycardia will not accompany adminis-tration of vasodilator agents (sodium nitroprusside,nifedipine, hydralazine), nor will directly inducedtachycardia accompany administration of agentswith vagolytic activity.9 Stress-dose steroid coverage should be adminis-tered to patients receiving steroids as part of theirimmunosuppression.
Heart-lung transplantation
Heart-lung transplantation can be considered forpatients with end-stage cardiopulmonary diseaseunresponsive to maximal medical therapy for whichno surgical options exist except combined heart-lung replacement. Increasingly, in an effort to makemaximum use of donated organs, double lung trans-plantation (DLT) and single lung transplantation(SLT) are being used for patients with pulmonarydisease without secondary severe cardiac dysfunc-tion. The number of heart-lung transplants peakedin 1989 (at approximately 250) and has continuedto decline (74 in 2003) as the result of the increasedof the use of DLT and SLT. In the USA approximatelythree pediatric HLTs are performed each year.
For adults, the primary indications for HLT,based on 2005 Registry data, are Eisenmengersyndrome secondary to congenital heart disease(32%), idiopathic pulmonary arterial hypertension(25%), and septic lung disease such as cystic fibrosisand bronchiectasis (15%). Other indications includeemphysema, α1-antitrypsin deficiency, and intersti-tial pulmonary fibrosis. For children, the primaryindications are congenital heart disease (40%),primary pulmonary hypertension (24%), and cysticfibrosis (16%).
Single lung transplantation
SLT can be considered for patients with end-stagelung disease without significant cardiac dysfunc-tion. Generally, patients with an LVEF > 35% anda right ventricular ejection fraction (RVEF) > 25%are considered candidates. The 2005 Registry dataindicate that, for adults, SLT is used primarilyfor patients with obstructive lung disease fromemphysema (53%), idiopathic pulmonary fibro-sis (24%), and α1-antitrypsin deficiency (8%).Increasingly, SLT is being used sparingly (1.5%) forpatients with pulmonary hypertension from idio-pathic pulmonary arterial hypertension and fromEisenmenger syndrome in whom there is not coex-istent severe cardiac dysfunction. For patients withobstructive lung disease the BODE index (B, bodymass index; O, airflow obstruction as measuredby FEV1; D, dyspnea as measured by the dysp-nea scale; E, exercise capacity as measured by the6-minute walk test) is useful in selecting candidatesfor transplantation.
For children, most lung transplantations are per-formed in the 11–17-year-old age group. SLT isused much less frequently than in adults and isused for patients with Eisenmenger syndrome inconjunction with repair of intracardiac lesions.
Double lung transplantation
DLT is also considered for patients with end-stagepulmonary disease without significant cardiacdysfunction. Two approaches to double lung trans-plantation exist: bilateral sequential single lungtransplantation (BSSLT) and en-bloc DLT. Patients

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 274 — #23
274 Chapter 7
with an LVEF > 35% and a RVEF > 25% are suit-able candidates. The trend has been to reserve DLTfor patients in whom SLT is not an option. Basedon 2005 Registry data the primary indications forDLT in adults are cystic fibrosis (32%), emphy-sema (23%), idiopathic pulmonary fibrosis (10%),α1-antitrypsin deficiency (9%), and idiopathic pul-monary arterial hypertension (7%). In addition,DLT has been used in conjunction with cardiacrepair in adults with Eisenmenger syndrome.
In children, the primary indications are cysticfibrosis (38%), idiopathic pulmonary arterialhypertension (19%), and Eisenmenger syndromein conjunction with a repair of intracardiaclesions (10%).
Living donor lobar lungtransplant (LDLLT)
In the subset of patients deemed too ill to survivelong enough to receive a cadaveric SLT or BSSLT thissomewhat controversial procedure can be consid-ered. It requires two donors, one donates the rightlower lobe the other the left lower lobe. The recipi-ent’s native lungs are excised. The majority of thesetransplants (85%) are in patients with cystic fibrosis.In these patients their small stature allows two lobesfrom ordinary size donors to provide adequate lungtissue.
Contraindications to HLT, SLT, DLT, and LDLLTare similar to those for heart transplantationand are outlined in Table 7.1. In addition, thefollowing absolute contraindications exist: severescoliosis or thoracic cage deformity, irreversible,significant respiratory muscle dysfunction, numer-ous transpleural systemic to pulmonary arterycollateral vessels, severe tracheomegly or tracheo-malacia, and Burkholderia cepacia genomovar IIIlower respiratory tract infection in cystic fibrouspatients.
Specific disease states
Obstructive lung diseaseThe most common indication for lung transplan-tation is obstructive lung disease secondary toemphysema or α1-antitrypsin deficiency. Patients
considered for transplantation generally havean FEV1 < 1 L, a requirement for supplementaloxygen at rest, and carbon dioxide retention.Pulmonary hypertension is uncommon in thesepatients. Concomitant CAD must be ruled outbecause many of these patients have long historiesof smoking.
Both SLT and BSSLT have been used for thesepatients. SLT is relatively contraindicated in twosubsets of emphysema patients: those with severebullous disease and those with bronchiectasis.Severe bullous disease may result in preferentialventilation of the nontransplanted lung. Bronchie-ctasis introduces the risk of leaving an infected lungin communication with the transplanted lung inan immunocompromised patient. These subsets ofpatients usually are considered for BSSLT.
In other patients, both SLT and BSSLT providegood early functional results. BSSLT provides betterlong-term functional results but is associated with ahigher operative mortality. Therefore, some centersconsider BSSLT in younger emphysema patients.
Pulmonary fibrosisThese patients have restrictive pulmonary physi-ology. Patients considered for transplantation gen-erally have a FVC < 1.5 L and a FEV 1 < 1.2 L,a requirement for supplemental oxygen at rest,and carbon dioxide retention. Moderate to severepulmonary hypertension is common in thesepatients.
SLT provides good function results in thesepatients as the transplant lung is preferentiallyventilated and perfused. Preferential ventilation ofthe transplant lung occurs because it is more com-pliant than the native lung. Preferential perfusionof the transplant lung occurs because PVR is higherin the native lung.
Idiopathic pulmonary arterialhypertension (IPAH)Patients in whom the cause of pulmonary hyper-tension is unexplained are said to have IPAH.This disease entity was formerly known as pri-mary pulmonary hypertension (PPH). For the diag-nosis of IPAH to be made, the secondary causesof pulmonary hypertension must be ruled out.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 275 — #24
Heart, Heart-Lung, and Lung Transplantation 275
Common causes of secondary pulmonary hyper-tension include mitral stenosis, congenital heartdisease, pulmonary embolism, and pulmonaryvenous obstruction. Seventy-three percent of IPAHpatients are female; the mean age at presenta-tion is 34 years, and the 5-year survival rate is20%. Survival is enhanced by coumadin anti-coagulation therapy, presumably because the pres-ence of low cardiac output and pulmonary vascularendothelial injury places these patients at risk forpulmonary thrombosis and worsening pulmonaryhypertension. High-dose calcium channel block-ers also improve survival, but only in the sub-group of patients who experience a greater than25% decrease in PVR and pulmonary artery pres-sure. Continuous PGI2 (epoprostenol, Flolan®)infusion improves survival and functional status.However, it usually is reserved for patients withNYHA functional class III–IV. Newer therapiesinclude bostensin (an endothelin-1 inhibitor), silde-nafil (a phosphodiesteraste-5 inhibitor), and tre-prostinil (a PGI2 analog which can be infusedsubcutaneously).
All patients with IPAH have RV dysfunction. IPAHproduces RV afterload mismatch and subsequentRV hypertrophy. Chronic exposure to the load-ing conditions that produce hypertrophy results inprogressive ventricular dysfunction as the result ofprogressive fibrosis and cell death. RV dilatationwith dilation of the tricuspid valve annulus and TRare common. Opinion regarding the best procedurefor patients with IPAH continues to evolve. HLTis the procedure of choice in IPAH patients withsevere end stage RV dysfunction or severe biven-tricular dysfunction. At present, the trend is to offerall other IPAH patients SLT or BSSLT. This strategyhas evolved because: (i) except in cases of end-stageRV systolic dysfunction, substantial recovery of theRV is possible with the normalization of pulmonaryartery pressures, which occurs after SLT and DLT;and (ii) use of SLT and BSSLT makes better use ofthe limited organ supply. Currently, 85% of lungtransplants done in patients with IPAH are BSSLT.
Eisenmenger syndromeThis syndrome occurs in patients with congenitalheart disease and pulmonary hypertension severe
enough to cause reversal of left-to-right shunts.Eisenmenger syndrome evolves in patients withintracardiac or great vessel left-to-right shunts.Initially, the left-to-right shunt produces increasedpulmonary blood flow and eccentric hypertrophyof the cardiac chambers involved. With a ventric-ular septal defect (VSD), there will be eccentrichypertrophy of the LV and RV; with an atrial septaldefect (ASD), there will be enlargement of theright atrium, left atrium, and RV. Prolonged expo-sure of the pulmonary vasculature to increasedpulmonary blood flow and pressure leads to devel-opment of pulmonary hypertension and pulmonaryvascular occlusive disease (PVOD). PVOD producesright ventricular concentric hypertrophy. As PVODadvances and PVR approaches and then exceedsSVR, intracardiac shunting becomes bidirectionaland then right to left. In the short term, theprocesses of eccentric and concentric hypertrophyprovide appropriate adaptation. However, chronicexposure to the loading conditions that producehypertrophy results in progressive ventricular dys-function as the result of fibrosis and cell death. Asa result, these patients usually have severe biven-tricular dysfunction and generally are not candi-dates for SLT and BSSLT. When LV function ispreserved, repair of the congenital cardiac defectcan be performed in conjunction with SLT andBSSLT procedures. As with IPAH, there is debateas to whether SLT is the appropriate operation forpatients with pulmonary hypertension secondary toEisenmenger syndrome.
Cystic fibrosisCystic fibrosis is a multisystem disease and isthe most common fatal inherited disease amongCaucasians. Pulmonary involvement is inevitable,and 95% of affected adults die of respiratory com-plications. Airway obstruction secondary to viscoussecretions, edema, and reactive airways leads toair trapping and an increase in functional reservecapacity (FRC), residual volume (RV), and total lungcapacity (TLC). FEV1 and FVC are reduced. In addi-tion, lung damage occurs as the result of bacterialinfections. Most patients with cystic fibrosis even-tually are colonized by Pseudomonas aeruginosa. Thispathogen is responsible for producing extensive

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 276 — #25
276 Chapter 7
tissue damage both directly and by antigenicstimulation of the immune system. Recurrentinfections and remissions are the norm. Aerosoladministration of recombinant human DNase(rhDNase) reduces the risk of infectious exacerba-tions requiring parenteral antibiotics and improvespulmonary function. rhDNase reduces the visco-elasticity, reduces the adhesiveness, and improvesthe mucociliary transportability of cystic fibrosissputum.
Chronic hypoxemia, acidosis, and physical lossof pulmonary vessels and lung tissue produce pul-monary hypertension and cor pulmonale. Rightventricular hypertrophy and dilatation develop.Chronic exposure to the loading conditions thatproduce hypertrophy results in progressive ventric-ular dysfunction as the result of progressive fibrosisand cell death.
In cases in which severe right ventricular dys-function exists, HLT is the procedure of choice. Incases in which right ventricular function is normalor slightly impaired, BSSLT is used by some centersin place of HLT. SLT is not an option for patientswith cystic fibrosis because the transplanted lungwill quickly become contaminated and infected bysecretions from the remaining lung. SLT with con-tralateral pneumonectomy has been used but hasnot been widely accepted.
Additional management problems are presentedby the presence of pancreatic insufficiency. Eighty-five percent of patients with cystic fibrosis havepancreatic insufficiency severe enough to causesteatorrhoea and malabsorption. Insufficient caloricabsorption and the anorexia of chronic disease com-bined with the increased caloric demands of chronicinfection may result in malnutrition. Enteral andparenteral feeding may be necessary. Vitamin Kdeficiency may result in prolongation of the pro-thrombin time. Glucose intolerance is common(40% of adults) and diabetes mellitus occurs in25% of adult patients.
Subclinical liver disease and hepatomegly sec-ondary to fatty infiltration are common. Only rarelyis liver dysfunction severe enough to cause hep-atocellular dysfunction and hypersplenism. As aresult, thrombocytopenia and coagulation factordeficiencies are rare.
The donor
Only 5–20% of all solid organ donors are suitablelung donors. Potential lungs are rejected because ofblunt thoracic trauma, the potential of aspirationduring resuscitation, overaggressive fluid resuscita-tion, and neurogenic pulmonary edema. The guide-lines used to select donors for lung transplantationare summarized below:1 Age younger than 65 years.2 Adequate gas exchange. The donor should havea PaO2 > 250 mmHg on FiO2 = 1.0 and PEEP= 5 cmH2O or PaO2 > 100 mmHg on FiO2= 0.4 and PEEP=5 cm H2O. Pulmonary compliance should be normalwith static pressure <20 mmHg and peak pressure<30 mmHg at a tidal volume of 15 mL/kg.3 Normal bronchoscopic examination.4 Normal serial chest radiographs.5 No history of pulmonary disease. A smokinghistory is acceptable in some centers.6 Donor recipient size match. Some programscompare donor and recipient lung size using chestradiograph measurements. A growing practice iscomparison of donor and recipient total lung capac-ity from nomograms based on age, height, andsex. In patients with obstructive lung disease, anallograft with 15–20% greater volume than thatpredicted for the recipient can be used as thesepatients have huge pleural cavities.7 No active severe infection or malignancy with thepossibility of metastases.8 Negative serologies for HIV or hepatitis B or C.9 ABO compatibility and HLA screen.
The guidelines used to select donors for HLT arethe combination of those for heart transplantationand those for lung transplantation.
Harvest of the lungs usually is accomplished inconjunction with harvest of the heart. The venacavae are transected, an incision is made in the leftatrial appendage, and the aorta is cross-clamped andcold cardioplegia is given. At this point, the pul-monary artery is injected directly with 500 µg ofPGE1 followed by infusion of 3–4 L of iced preser-vative solution which is vented out an incision inthe left atrial appendage. The lungs are partiallyinflated (60%) with FiO2 of 0.4 and the tracheaor bronchi is stapled and divided. The heart-lung

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 277 — #26
Heart, Heart-Lung, and Lung Transplantation 277
block is then removed. When the heart and lungsare to be used for separate recipients, adequate por-tions of pulmonary artery and left atrial-pulmonaryvein cuff must be allocated to each recipient. Thelungs are immersed in a cold crystalloid solutionat 4C and transported. Although the maximumischemic time is 6–8 hours, the optimal ischemictime should not exceed 5–6 hours because short-and intermediate-term patient survival may beeffected.
Operative procedure and patientpositioning
HLT is performed through a median sternotomywith hypothermic CPB, bicaval cannulation, andaortic cross-clamping. The recipient undergoesresection of the heart-lung block, leaving only aright atrial cuff in continuity with the IVC and SVC,the cut end of the distal trachea, and the cut end ofthe proximal ascending aorta. The donor heart-lungblock is implanted with anastomoses of the rightatrium, distal trachea, and ascending aorta.
SLT is performed through a standard thoracotomywith the patient in the lateral thoracotomy posi-tion. The donor lung block contains a cuff of leftatrium with two pulmonary veins, the bronchus,and the branch pulmonary artery. The other donorlung and the donor heart can be used for two otherrecipients. One lung ventilation (OLV) is establishedand a pneumonectomy is performed, followed byimplantation of the donor lung with anastomosesat the left atrium, bronchus, and branch pulmonaryartery. This procedure often can be performedwithout CPB.
Two very different surgical procedures are usedfor DLT. The en-bloc procedure is performed on CPBwith hypothermia, bicaval cannulation, aortic cross-clamping, and cardioplegic arrest of the recipientheart. A median sternotomy is used. The donordouble lung block consists of the two lungs, thedistal trachea, the main pulmonary artery, and alarge left atrial cuff with all four pulmonary veins.The donor heart can be used for another recipi-ent. The block is implanted with anastomoses at thetrachea, posterior left atrium, and main pulmonaryartery after bilateral recipient pneumonectomies.
This procedure is associated with poor healing ofthe tracheal anastomosis and reduced long-termsurvival compared with BSSLT and has been largelyabandoned.
BSSLT is the other approach to DLT. This proce-dure often can be performed without CPB, which isconsiderably more challenging for the anesthesiol-ogist. This procedure is performed with the patientsupine through a sternal bithoractomy. Properpositioning is necessary to provide adequate expo-sure for the thoracotomy portion of the incision.One approach is to position the patient’s arms sus-pended over the head. This is cumbersome andconsumptive of the small amount of space avail-able at the head of the table. In addition, it exposesthe patient to an increased risk of brachial plexusinjuries. With proper positioning of two rolls, oneon either side of the patient’s spine extending fromthe cervical to the lumbar region, the arms canremained tucked at the patient’s side. Each donorlung block contains a cuff of left atrium with twopulmonary veins, the bronchus, and the branchpulmonary artery. The donor heart can be usedfor another recipient. OLV is established and apneumonectomy is performed, followed by implan-tation of the donor lung with anastomoses atthe left atrium, bronchus, and branch pulmonaryartery. The procedure is then repeated for the nextdonor lung.
Use of CPBThe indications for use of CPB are summarized inTable 7.3.
HLT and en-bloc DLTHLT and en-bloc DLT both require hypothermic CPBwith aortic cross-clamping as described previously.
SLT and BSSLTElective CPB is used for SLT and BSSLT for thefollowing subsets of patients:• Infants and small children.• Patients with pulmonary hypertension.• Patients undergoing lung transplantation andsimultaneous repair of intracardiac defects.
For all other patients with SLT and BSSLT, CPB isinitiated only when hemodynamic, gas exchange, or

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 278 — #27
278 Chapter 7
Type of transplant CPB OLV
HLT Full hypothermic, aorticcross-clamp
No
En-bloc double-lung transplant Full hypothermic, aorticcross-clamp, cardioplegic arrest
No
SLT, BSSLTInfants, small children Full normothermic NoIntracardiac defect repair Full hypothermic, aortic
cross-clamp, cardioplegic arrestNo
Pulmonary hypertension Partial normothermic YesAll others Partial normothermic if necessary Yes
BSSLT, bilateral sequential single lung transplantation; CPB, cardiopulmonarybypass; HLT, heart-lung transplantation; OLV, one-lung ventilation; SLT,single-lung transplantation.
Table 7.5 Indications forcardiopulmonary bypass (CPB) andone-lung ventilation (OLV) in lungtransplantation.
technical difficulties are encountered in the courseof the procedure. Most SLT and BSSLT patientswithout pulmonary hypertension can be managedwithout CPB. There is a higher incidence of need forCPB in patients with restrictive lung disease. Intra-operative criteria that predict the need for use ofCPB in patients with restrictive lung disease includean arterial oxygen saturation (SaO2) < 90% with anFiO2 of 1.0, baseline mean PA pressure > 40 mmHg,mean PA pressure > 50 mmHg with the pulmonaryartery clamped, severe systemic hypotension, anda cardiac index < 2.0 L/min/m2. Avoiding CPBwhen possible is important because use of CPBcontributes to postoperative graft dysfunction inthe form of an increased arterial:alveolar oxygenratio, increased severity of radiographic pulmonaryinjury, and prolonged postoperative intubation. Itdoes not appear that use of CPB effects long-termoutcome.
Full CPB is used for infants and small childrenand for all patients undergoing simultaneous repairof an intracardiac lesion. Aortic cross-clamping andcardioplegic arrest are only necessary when intra-cardiac defects are repaired. Normothermic par-tial CPB is used for all other cases of SLT andBSSLT. Cannulation of the ascending aorta and theright atrium is used for bilateral SLT and right SLT.For patients undergoing left SLT, descending aortaand pulmonary artery cannulations have been used.
Alternatively, femoral vein and artery cannulationcan be used.
Anesthetic management
Goals1 Patients with obstructive lung disease mayexhibit auto-PEEP, stacking of breaths, and hemo-dynamic compromise with positive pressureventilation. Ventilatory interventions will benecessary.2 Pre-existing LV or RV dysfunction requires thatcontractility be maintained or enhanced.3 Avoid hypercarbia, hypoxemia, and acidosis thatwill exacerbate pulmonary hypertension and mayresult in acute RV decompensation.4 Avoid increase in the PVR:SVR ratio in patientswith Eisenmenger syndrome. This will increaseright-to-left shunting and worsen hypoxemia.
Preoperative evaluationLung transplant patients typically undergo exten-sive medical evaluation. A summary of this eval-uation is readily available to the anesthesiologistthrough the transplant coordinator.
PremedicationMost patients are called into the hospital on shortnotice and many will have eaten solid food in

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 279 — #28
Heart, Heart-Lung, and Lung Transplantation 279
the previous 6–8 hours. In addition, patients willhave taken their initial doses of oral immuno-suppressive drugs, usually cyclosporine and aza-thioprine or mycophenolate moftil. Cyclosporineusually is administered with 10–20 mL of liquid. Itis important to verify that these medications havebeen taken. To reduce the risk of aspiration in adultsand older children, a nonparticulate antacid suchas bicitra 30 mL can be given in addition to intra-venous metaclopromide 10 mg and an intravenousH2 receptor blocker such as ranitidine 50 mg. Forinfants and smaller children a period of 2–3 hours ofNPO status is sufficient and usually transpires beforeinduction.
Premedication for adults and children is mostsafely and effectively titrated by the anesthesiol-ogist before induction and while lines are placedand the history and physical examination arecompleted. Midazolam 0.03–0.05 mg/kg in divideddoses works well to reduce anxiety. Supplementaloxygen should be administered because hypoxemiawill exacerbate existing pulmonary hypertension.
PreinductionSome transplant patients will be receiving intra-venous inotropic and vasodilator therapy whenthey arrive for surgery. These agents should be con-tinued via a reliable intravenous route. Sterility isof the utmost importance because the patients willbe immunosuppressed. Patients with bronchospas-tic disease should receive bronchodilator therapybefore induction. Likewise, patients with cysticfibrosis should receive nebulized acetylcysteine orrhDNase to help break up tenacious secretions.
AdultsAll patients should have two large-bore periph-eral intravenous lines (14-gauge). If the patient’sarms are suspended over the head, venous accessin or below the antecubital fossa is not practicalbecause flow will be impaired. Placement of oneor more introducer sheaths in the internal jugularvein for use as reliable sites of rapid fluid admin-istration is warranted if peripheral access is pooror the arms are to be suspended over the head.ECG monitoring should allow assessment of V5,I, II, III, aVR, aVL, and aVF. Baseline recording
of all seven leads should be obtained for compar-ative purposes. Normally, two leads (II and V5)are monitored simultaneously intraoperatively. Ifa left thoractomy incision is used, V5 is not anoption because the lead will be in the operative field.A radial or femoral artery catheter is placed withlocal anesthesia before induction of anesthesia.When a femoral artery catheter is used, it shouldbe placed in femoral artery contralateral to the onethat will be cannulated if CPB is used.
Most centers place a pulmonary artery catheterin adults for SLT and BSSLT. The catheter can beplaced after induction in patients who are unableto lie flat or to cooperate. Some centers use PAcatheters that allow continuous cardiac output andmixed venous oxygen saturation (SvO2) moni-toring. The PA catheter is an important tool inmanaging the patient during pneumonectomy andclamping of the pulmonary artery. In addition,information obtained from the PA catheter is usedto determine whether completion of the proce-dure without CPB is feasible. It is not necessaryto direct the pulmonary artery catheter into thecontralateral pulmonary artery in patients under-going SLT. The catheter can be pulled back into themain pulmonary artery before pulmonary arteryclamping and then advanced into the contralateralpulmonary artery.
For HLT some centers do not place a PA catheterfor the same reasons outlined for heart transplantpatients. As with heart transplantation, some cen-ters prefer that the right internal jugular vein not beused as an access site in HLT patients in order thatit can be used later for obtaining endomyocardialbiopsies.
Multiplane TEE is used to help manage the patientpre- and post-CPE. After transplantation, TEE isused to assess left and right ventricular function,measure pulmonary artery pressures (using a tri-cuspid regurgitation jet), and guide managementof pulmonary artery hypertension and RV dys-function if necessary. In addition, TEE is usedto assess the pulmonary arterial and pulmonaryvenous anastomoses after lung transplantation. TEEalso has proved useful in detection and treat-ment of dynamic, infundibular RV outflow tractobstruction after lung transplantation. Patients with

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 280 — #29
280 Chapter 7
RV hypertrophy may have apposition of the wallsof the infundibulum in systole, when RV afterloadis reduced after donor lung implantation. Hypo-volemia and inotrope use tend to exacerbate thisproblem.
A thoracic or lumbar epidural can be used bothintraoperatively and for postoperative pain man-agement in SLT and BSSLT patients. The cathetercan be placed preoperatively in those patients whoare unlikely to require CPB. For patients requiringCPB, the epidural catheter is placed postoperativelyafter reversal of heparinization and correction ofcoagulation deficiencies. Some centers prefer toplace all epidural catheters postoperatively as it isoften impossible to predict whether a patient willrequire CPB. In thoracic catheters, 0.0625–0.125%bupivacaine and fentanyl 10 µg/mL at 4–8 mL/hcan be infused. In lumbar catheters preservative-free morphine 0.05 mg/mL at 5–10 mL/h canbe used.
ChildrenPlacement of an intravenous catheter before induc-tion is optimal with induction proceeding asdescribed for adult patients. Patients with preservedventricular function, an appropriate NPO interval,and cardiopulmonary stability will likely toleratean inhalation induction. ECG monitoring shouldallow assessment of V5, I, II, III, aVR, aVL, and aVF.Baseline recording of all seven leads should beobtained for comparative purposes. Normally, twoleads (II and V5) are monitored simultaneouslyintraoperatively. If a left thoractomy incision isused, V5 is not an option because the lead will bein the operative field. A radial or femoral arterycatheter is placed after induction of anesthesia. CVPmonitoring is placed after induction. For older chil-dren undergoing SLT or BSSLT with or withoutCPB, a PA catheter is placed. For all other children,an appropriately sized double-lumen central venousline is placed. The right internal jugular vein is thepreferred site. A pediatric multiplane TEE probecan be used for children weighing less than 15–20 kgand the adult multiplane TEE probe for childrenweighing more than 20–30 kg to help manage thepatient pre- and post-CPB as described previouslyfor adult patients.
For older children undergoing SLT and BSSLT,a lumbar or thoracic epidural catheter can be placedfor postoperative pain management.
Management of OLVThe indications for use of OLV are summarized inTable 7.3. In procedures performed with full CPB,lung isolation and OLV are not necessary. Theseprocedures can be managed with a standard single-lumen endotracheal tube. The anesthetic plan forSLT and BSSLT in adults and older children mustinclude a method of lung isolation and OLV becausethese procedures are being performed increasinglywithout CPB or with partial CPB. When partial CPBis used, OLV to the perfused, nonoperative lung isnecessary. Four methods of lung isolation and OLVare available.
Endobronchial intubationA standard endotracheal tube (ETT) is used andthen a bronchoscope is used to direct the ETT downthe main stem bronchus of the lung that is to beventilated.
Advantages• Applicable to any size patient with use of anappropriate-sized ETT.• Placement is easy with the appropriate-sizedfiberoptic bronchoscope. When the right mainstem bronchus is intubated, visualization of theright upper lobe (RUL) bronchus is possiblewith the bronchoscope. This helps prevent occlu-sion of the RUL bronchus by the balloon ofthe ETT.• Suctioning of secretions via the ETT before endo-bronchial intubation is easy because a large suctioncatheter or fiberoptic bronchoscope can be used.• When the procedure is completed, the ETT doesnot have to be replaced.
Disadvantages• Some deflation of the nonventilated lung willoccur passively, but most will occur by absorptionof gas. For patients with emphysema, this will resultin slow, poor lung deflation and poor operatingconditions.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 281 — #30
Heart, Heart-Lung, and Lung Transplantation 281
• Suctioning of the nonventilated lung and applica-tion of continuous positive airway pressure (CPAP)to the nonventilated lung is impossible.• In taller patients, a standard ETT may not be longenough to extend far enough into the main stembronchus to provide isolation.
Single-lumen endotracheal tube plusa bronchial blockerThis technique involves use of a Fogarty catheter orArndt blocker and a standard ETT. Laryngoscopy isperformed and the blocker is placed in the trachea,followed by placement of the endotracheal tube.Alternatively the blocker can be placed within thelumen of the ETT. In either case, a fiberoptic bron-choscope is used to guide the bronchial blockingcatheter down the appropriate bronchus.
Advantages• Applicable to any size patient with use ofan appropriate-sized ETT and bronchial blocker.Fogarty catheters with balloon sizes from 0.5–3.0 mLare available. Arndt blockers are available in 5-, 7-and 9-French catheters with high-volume low-pressure balloons. Placement is easy with theappropriate-sized fiberoptic bronchoscope.• Suctioning of secretions via the ETT before place-ment of the blocker is easy because a large suctioncatheter or fiberoptic bronchoscope can be used.• When the procedure is completed, the ETT doesnot have to be replaced and the Fogarty cathetercan be removed.
Disadvantages• Deflation of the blocked lung must occur byabsorption of gas. For patients with emphysema,this will result in slow, poor lung deflation and pooroperating conditions.• Suctioning of the nonventilated lung and appli-cation of CPAP to the nonventilated lung isimpossible.• Maintaining the position of the blocker in themain stem bronchus during surgical manipulationmay be difficult or impossible. In patients with cysticfibrosis undergoing BSSLT, this introduces the riskof contamination of the first lung transplanted withsecretions from the remaining diseased lung.
• Visualization of the RUL bronchus with a fiber-optic bronchoscope is impossible with the blockerin the right main stem bronchus. As a result,occlusion of the RUL bronchus by the balloon ofthe blocker may occur due to the high takeoff ofthe RUL bronchus. This makes surgical excisionof the right lung and the subsequent transplantbronchial anastomosis technically difficult.• The Fogerty catheter balloon is a high-pressurelow-volume balloon that may compromisebronchial mucosal blood flow.
Univent tubeThis is a standard endotracheal tube with a 3-mmouter diameter bronchial blocker, which passesthrough a 4-mm channel incorporated within thelumen of the endotracheal tube. The bronchialblocker has a 2-mm internal diameter lumen.These tubes are available with internal diametersfrom 6.0 to 9.0 mm in 0.5 mm increments andin a 3.5 mm uncuffed and 4.5 mm cuffed version.Because of the presence of the enclosed bronchialblocker, the external diameter of these tubes is con-siderably larger. The external diameter of the 8 mmUnivent tube is 13 mm which is the same as theexternal diameter of a 39-French double-lumenendotracheal tube (DLT). The external diameterof the 3.5 mm Univent tube is same as a 6 mmETT or a 26-French DLT. Optimal placement ofthe bronchial blocker requires use of a fiberopticbronchoscope.
Advantages• The arrangement of the blocker as an integral partof the ETT provides better stability of the blockerwithin the main stem bronchus during surgicalmanipulation.• It is easier to place in a patient with a difficultairway than a DLT.• The internal lumen of the blocker will allow somedecompression of the nonventilated lung and willallow the application of CPAP.• When the procedure is completed, the Univenttube does not have to be replaced with a standardETT. The bronchial blocker can be withdrawn intothe internal channel and the Univent tube can beleft in place.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 282 — #31
282 Chapter 7
Disadvantages• Due to the large external diameter, these tubesare useful only for adult patients and older children.• The internal lumen of the blocker is too small toallow adequate suctioning of secretions.• As with a standard bronchial blocker, occlusionof the RUL bronchus by the balloon of the blockermay occur.• The bronchial blocker balloon is a high-pressure low-volume balloon that may compromisebronchial mucosal blood flow.
Double-lumen endotrachealtube (DLT)DLTs are available in sizes from 26-, 28-, 32-, 35-,37-, 39-, 41-, and 43-French. The outer diameterof a 26-French DLT is equivalent to a 6.0 mm ETTand thus is appropriate size for a patient weight-ing approximately 30 kg or 8–10 years of age. Bothright- and left-sided tubes are available. Right-sidedtubes have a side lumen in the bronchial tubethat must be positioned over the RUL bronchusso that the balloon of the bronchial lumen does notocclude the RUL bronchus. Fiberoptic bronchoscopyis necessary to ensure proper positioning of bothright- and left-sided DLTs.
Advantages• Deflation and suctioning of the nonventilatedlung is easily accomplished.• Application of CPAP to the nonventilated lungis easy.• The endobronchial tube is not dislodged easilywith surgical manipulation.• Visualization of the RUL bronchus with the DLTin place is accomplished easily with a fiberopticbronchoscope.
Disadvantages• Alignment of the RUL lumen of a right-sided DLTwith the patient’s RUL can be difficult, particularlyin the presence of thick secretions.• The smallest available DLT is appropriate forchildren aged 7–8 years.• Suctioning tenacious secretions through the smalllumens of the DL tube is more difficult than throughthe lumen of a standard ETT.
• When the procedure is completed, the DLT mustbe exchanged for a standard ETT.
A left-sided DLT is the method of choice for lungisolation in adult and pediatric patients undergoingSLT and BSSLT. The left DLT provides greater versa-tility and ease of placement. A left-sided DLT, whenproperly placed, with use of a fiberoptic broncho-scope does not compromise surgical exposure forthe left pneumonectomy and the subsequent trans-plant bronchial anastomosis. Consideration shouldbe given to use of a bronchial blocker or Univenttube in patients with a difficult airway. When aleft-sided DLT is needed, placement is accomplishedas follows:1 The trachea is intubated such that the trachealcuff is just below the vocal cords and the tubeis rotated 90 to the left. The trachea cuff isinflated and the patient is ventilated. The bronchiallumen will be located just above the carina in mostnormal-sized patients.2 An appropriate-sized fiberoptic bronchoscope isintroduced down the bronchial lumen and the rightand left main stem bronchi are identified. In someinstances, it may be necessary to pull the DLT backslightly if the tip of the bronchial lumen is past thecarina. For patients with cystic fibrosis or bronchiec-tasis, thick secretions may make identification dif-ficult. A suction catheter and saline irrigation mayhave to be introduced down the bronchial lumen toclear secretions. Suctioning through the broncho-scope is difficult considering the small caliber scopesthat can fit down the DLT. Alternatively, aggres-sive cleanout with an SLT and a large bronchoscopecan be accomplished before placement of the DLT.3 The bronchoscope is advanced down the leftmain stem bronchus and the left upper lobebronchus is identified.4 While the operator keeps the tip of the broncho-scope above the left upper lobe bronchus orifice, thetracheal balloon is deflated and the DLT is advancedinto the left main stem bronchus over the bron-choscope. The tip of the bronchial lumen should beconfirmed to be above the left upper lobe bronchus.The tracheal balloon is re-inflated and ventilationcontinues.5 The bronchoscope is now placed down the tra-cheal lumen. Ideally, the tracheal lumen should be

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 283 — #32
Heart, Heart-Lung, and Lung Transplantation 283
positioned just above the right main stem bronchuswith the bronchial balloon below the rim of theorifice of the left main stem bronchus. If the DLThas been advanced too far down the left main stembronchus, the tracheal lumen may lie within theleft main stem bronchus. This is unlikely if the tipof the bronchial lumen lies above the left upper lobebronchus.6 If the tracheal lumen is within the left main stembronchus, the tracheal balloon is deflated and theDLT is pulled back until the tracheal lumen pro-vides unobstructed access to the right main stembronchus. The bronchial balloon should remain ator below the rim of the left main stem bronchusorifice. The tracheal balloon is re-inflated.7 After proper positioning is confirmed, thebronchial balloon is inflated while the bronchoscoperemains in the tracheal lumen. The bronchial bal-loon should not herniate out the left main stembronchus when the balloon is inflated. If the bal-loon herniates out of the left main stem bronchus,the DLT must be advanced slightly into the left mainstem bronchus.8 Positioning of the DLT should be rechecked withthe bronchoscope after the patient has been movedinto final position. DLT placement may change aftermovement of the patient into the lateral decubitusposition.
Induction and maintenanceAnesthetic techniques should allow for early post-operative extubation. Many patients with end-stagepulmonary disease will be unable to lie flat dueto severe dyspnea. These patients are induced inthe sitting position and, as they lose conscious-ness, they are slowly placed supine. For patientsin whom there is a risk of aspiration, induction isperformed with the patient in a slightly head upposition and cricoid pressure is applied until thetrachea is intubated.
Narcotic-induced rigidity with subsequent diffi-culty ventilating can have disastrous consequencesfor these patients. Careful titration of etomidate(0.1–0.3 mg/kg) in combination with 5–10 µg/kg offentanyl or 1–2 µg/kg of sufentanil is useful forinduction. A full 0.3 mg/kg dose of etomidate isoften not necessary to induce hypnosis and loss
of consciousness in these patients. This drug com-bination has minimal direct effect on heart rate,myocardial contractility, peripheral vascular resis-tance, or venous capacitance. An overall diminutionin central sympathetic tone will also contributeto circulatory depression. A nondepolarizing mus-cle relaxant in a dose 2 × ED95 such as vecuro-nium or pancuronium 0.02 mg/kg or cisatracurium0.04 mg/kg is used to assure prompt control ofthe airway. Pancuronium is generally reserved forthose patients in who a low baseline heart rate. Ininfants and children the vagolytic and sympathome-tic effects of pancuronium can be used to counteractthe vagotonic effects of fentanyl or sufentanil. Thesedrugs in combination with rocuronium (1.0 mg/kg)or succinylcholine (1–2 mg/kg) can be used to per-form a modified rapid sequence induction (cricoidpressure during positive pressure ventilation) in thepatient with questionable NPO status. Thiopentaland propofol are less well tolerated. Thiopental inparticular may exacerbate bronchospasm.
Anesthesia can be maintained with additionaldoses of opioid in conjunction with a benzo-diazepine (usually midazolam in increments of0.01–0.03 mg/kg) or a low inhaled concentration(0.5–0.75 MAC) of isoflurane or sevoflurane. N2Ois not a good choice as an adjuvant agent; ithas a weak myocardial depressant effect that nor-mally is counteracted by the sympathetic outflow itproduces.
For patients with obstructive lung disease(emphysema, α1-antitrypsin deficiency, cystic fibro-sis) induction and positive pressure ventilationmay produce profound hypotension. The possibil-ity that a pneunothorax is present must alwaysbe considered. This cardiovascular compromiseis secondary to air trapping or auto-PEEP. Thisauto-PEEP reduces SV and cardiac output throughthe following:• Reductions in venous return to the RV resultingin a decrease in RVEDV.• Increased impedance to RV ejection by mechan-ical compression of the pulmonary arterial systemresulting in an increase in RVESV.• Shift of the interventricular septum into theLV, which increases LV stiffness and reducesLVEDV.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 284 — #33
284 Chapter 7
This combination is particularly detrimental forpatients with compromised RV systolic function andRV afterload mismatch. Treatment requires vol-ume administration to (10–15 mL/kg of a balancedsalt solution) to normalize RVEDV and inotropicsupport to improve RV systolic function and nor-malize RVESV. Either dopamine 5–10 µg/kg/minor epinephrine 0.01–0.10 µg/kg/min (adults) or0.05–0.50 µg/kg/min (children) are effective. Inaddition, ventilation with a rapid initial inflationfollowed by an inspiratory hold or pause and along expiration time is necessary (low inspiratoryto expiratory time (I:E) ratio). This may requirehand ventilation, although pressure-control venti-lation with an intensive care unit (ICU) ventilatorworks well. PEEP should not be used.
TEE is extremely valuable in assessing ventric-ular filling and contractile function in this set-ting because filling pressures will not provide anaccurate measure of ventricular volumes.
In the most severe instances, intermittent periodsof apnea may be necessary. This apneic oxygenationmay exacerbate pre-existing pulmonary hyperten-sion via carbon dioxide retention and hypoxemia.Evaluation of pulmonary artery pressures and car-diac output with a PA catheter, RV and LV func-tion with TEE, and arterial saturation with pulseoximetry are necessary to determine the extentof hypoventilation that can be tolerated. Markedacidosis (pH of 6.94) and hypercarbia (PaCO2 of150 mmHg) can be tolerated during lung trans-plantation as long as systemic blood pressure andoxygen delivery are maintained. In some instancesinitiation of CPB may be necessary.
Blood loss may be impressive during dissec-tion for pneumonectomy in HLT, SLT, and DLTpatients with dense adhesions from previous tho-racic surgery or for patients with cystic fibrosis orbronchiectasis. A rapid transfusion device may benecessary in some cases. Some centers use antifib-rinolytics or aprotinin in both children and adultswhen CPB is used or when there are dense adhe-sions regardless of whether CPB is used. In additionto red cells, component therapy with fresh frozenplasma (FFP) and platelets often is necessary, partic-ularly when CPB is used. Manipulation of the lungsin patients with cystic fibrosis or bronchiectasis
may result in release of endotoxins with subse-quent decrease in SVR, hyperpyrexia, and increasedmetabolic rate. Management of the recipient with-out use of CPB under these conditions is extremelydifficult.
After one or both of the lungs have beenimplanted and perfused, most centers administermethylprednisolone (usually 10 mg/kg for childrenand 500 mg for adults). After lung implantationhas been completed, 5–10 cm H2O PEEP is appliedand the FiO2 selected is the lowest necessary toobtain a PaO2 of 90–100 mmHg. This is done becausethe post-ischemic lung is vulnerable to oxygen-freeradial toxicity. At the termination of the procedure,patients with DLTs have the DLT replaced with alarge single-lumen ETT. A large tube size should beused to allow easy access for postoperative fiberopticbronchoscopy.
Special considerations for SLT and BSSLTManagement of OLV and pulmonary artery clamp-ing for recipient pneumonectomy and allograftimplantation in SLT and BSSLT patients with-out CPB is a challenge. The task is made easierfor patients undergoing SLT if the lung with thepoorest ventilation and perfusion is removed andreplaced. For patients undergoing BSSLT, the lungwith the poorest ventilation and perfusion shouldbe removed first and replaced.
Maintenance of body temperature is difficultwhen CPB is not used. A warming blanket underthe patient, an actively humidified breathing circuit,a fluid/blood warmer, and a forced warm air blanketover the patient all are necessary.
One lung ventilation (OLV)Collapse of the operative lung and OLV is likelyto exacerbate air trapping and the subsequenthemodynamic compromise and carbon dioxideretention. Treatment with volume administration,inotropes, and ventilatory interventions is war-ranted as described previously. Marked hypercarbiawith acidosis is likely and generally is well toler-ated. Aggressive suctioning may be necessary tofacilitate collapse of the operative lung. PaO2 also islikely to decrease, due to intrapulmonary shunting,until the ipsilateral pulmonary artery is clamped.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 285 — #34
Heart, Heart-Lung, and Lung Transplantation 285
Administration of CPAP to the nonventilated lung,insufflation of oxygen to the nonventilated lung,or high-frequency jet ventilation (HFJV) of thenonventilated lung may improve oxygenation.
Clamping of the PARecipient pneumonectomy requires clamping ofthe ipsilateral pulmonary artery. Before clampingof the pulmonary artery, the pulmonary arterycatheter is withdrawn into the main pulmonaryartery. Palpation by the surgeon will confirm itsposition proximal to the proposed cross-clamp site.After the ipsilateral pulmonary artery has beenclamped, the catheter is advanced into the contralat-eral pulmonary artery. Clamping of the pulmonaryartery may compromise RV function due to after-load mismatch. This is most likely in patients withmild to moderate pre-existing pulmonary hyperten-sion and in those with impaired RV function. Thisis the primary reason why patients with severe pul-monary hypertension require elective CPB. If thereis any doubt regarding the ability of the patientto tolerate pulmonary artery clamping, a trial ofclamping is recommended. TEE is used to assessRV function. In addition, increased PAP and CVP,falling cardiac index, and SvO2 may occur.
Allograft implantationImmediately after allograft implantation andwashout of the preservative solution and prosta-glandin, there may be profound, transient systemichypotension. Treatment requires fluid administra-tion and α-adrenergic support. After implantationof the donor lung, there usually is an immedi-ate reduction in PA pressures and an improve-ment in pulmonary compliance and gas exchange.This period may be followed by allograft dysfunc-tion characterized by deteriorating gas exchange,decreasing pulmonary compliance, and elevatedPA pressures. This is the result of noncardiogenic,reperfusion pulmonary edema. Two factors predis-pose this process: pre-existing pulmonary hyperten-sion, which results in over-perfusion of the donorlung and a long ischemic interval, which enhancescapillary permeability.
PEEP (5–15 cm H2O) usually is necessary tomaintain adequate gas exchange when allograft
dysfunction occurs. Increased capillary permeabil-ity and the lack of pulmonary lymphatic drainagein the allograft require judicious crystalloid admin-istration. Excessively large tidal volumes shouldbe avoided because over inflation of the allo-graft will contribute to elevated PA pressuresthrough mechanical compression of the pulmonaryvasculature.
If allograft dysfunction is severe, implantation ofthe second lung in BSSLT patients may require CPB.If CPB is not used, implantation of the second lungis managed as described for the first lung.
Indications for CPBThe decision to use CPB is individualized for eachpatient. The use of CPB may become necessaryat any time during the procedure. The combina-tion of a cardiac index < 2 L/min/m2, SvO2 < 60%,mean arterial pressure (MAP) < 50–60 mmHg,SaO2 < 85–90%, and pH < 7.00 despite aggres-sive ventilatory and pharmacologic intervention isan indication for use of CPB. CPB is not nec-essary for increased pulmonary artery pressuresunless there is evidence of deteriorating RV func-tion. TEE assessment of RV function is supple-mented by use of CVP determinations. IncreasingCVP, RV distension, worsening global hypokine-sis, and new or worsening tricuspid regurgitation(TR) despite inotropic support with epinephrine,NE, or dopamine in combination with inhaled(NO 20–40 ppm) or intravenous pulmonary vasodi-lation (milrinone 0.5–1.0 µg/kg/min, nitroglycerin0.5–5.0 µg/kg/min, PGE1 0.05–0.20 µg/kg/min, orPGI2 5–20 ng/kg/min) are indications for use ofCPB. NE (0.01–0.10 µg/kg/min) is the most effec-tive agent for maintaining coronary perfusion pres-sure in patients with RV hypertension but its usemust be tempered with the knowledge that it mayincrease PVR as well.
TEE assessment of LV function is supplementedby use of pulmonary artery occlusion pressure(PAOP) determinations. Hypoxemia, hypercarbia,and reduced systemic blood pressure can allcontribute to LV dysfunction. Progressive dete-rioration in LV function (new wall motionabnormalities, LV distension, new or worsen-ing mitral regurgitation (MR)) despite aggressive

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 286 — #35
286 Chapter 7
pharmacologic and ventilatory interventions is anindication for CPB.
A metabolic acidosis is difficult to treat becausesodium bicarbonate administration will producecarbon dioxide, which must be eliminated byincreased alveolar ventilation. Obviously, increas-ing alveolar ventilation often is not possible in thesepatients.
Post-CPB management
Preparations for terminating CPB are discussed indetail in Chapter 10. Particular attention must bepaid to de airing the heart. Severe ventricular dys-function may follow ejection of air through thecoronary arteries. The RV is particularly at risk dueto the anterior location of the right coronary ostia.TEE is valuable in guiding the de-airing process.
Patients undergoing HLT have a denervated heartand are managed in the post-CPB period in thesame manner as that described for heart transplantpatients.
RV function usually improves dramatically afterlung implantation due to the immediate reduc-tion in pulmonary artery pressures. Despite this,patients with en-bloc DLT, BSSLT, or SLT mayrequire inotropic support. Patients requiring aorticcross-clamping and cardioplegic arrest are at par-ticular risk for post-CPB right and left ventriculardysfunction. In addition, the presence of lung allo-graft dysfunction may contribute to post-CPB RVdysfunction as the result of elevated PA pressures.
Postoperative care
In rare instances, extracorporeal membrane oxy-genation and independent lung ventilation may benecessary after SLT in patients with pulmonaryhypertension secondary to reperfusion pulmonaryedema. Postoperative independent lung ventilationwith a DLT has been used for patients with SLTto minimize preferential ventilation and air trap-ping in the native lung in patients with obstructivelung disease. For these patients, the native lunghas high compliance and air trapping can result inhyperinflation with subsequent displacement of themediastinum and compression of the donor lung.
Differential ventilation with hypoventilation of thenative lung has been used successfully to avoid thisproblem. Preferential perfusion of the donor lungoccurs after SLT, especially for patients with pul-monary hypertension. In cases of severe V /Q mis-match, selective hypoventilation of the native lungcombined with positioning the patient in the lateralposition with the donor lung in the nondepen-dent position may be necessary in the postoperativeperiod. This will minimize over ventilation of thenative lung and over-perfusion of the donor lung.In patients with SLT with a fibrotic native lung, posi-tioning the patient with the donor lung dependentmay help equalize ventilation to the both lungs.
Noncardiac surgery inlung transplant patients
As with heart transplant patients, lung transplant,and HLT patients may require surgical procedures.Some are purely elective, whereas others are likelyto be urgent or emergent. Most surgical proceduresare the direct result of complications of immuno-suppressive therapy. These complications are listedTable 7.2. The incidence of complications requir-ing general surgical consultation and interventionin lung transplant patients is 16%. In addition,lung transplant patients suffer airway and vascu-lar anastomotic complications that require operativeintervention. The incidence of airway complicationsin SLT and BSSLT is 12–17% per anastomosis withan associated mortality rate of 2–3%. Nine percentof nonlethal airway complications require opera-tive intervention. Similar statistics exist in pediatricpatients. The most common intervention requiredis for treatment of bronchial stenosis. This usuallyinvolves flexible and rigid bronchoscopy for laserexcision of granulation tissue, stent placement, orballoon dilatation.
Lung transplant and HLT patients present aunique set of management issues.1 Loss of cough reflex due to transection of vagal fibers.This makes the patient with a transplanted lungprone to retention of secretions and at risk for pul-monary infections. The risk of aspiration shouldnot be significantly increased, as the innervation ofthe larynx, epiglottis, and proximal trachea remain

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 287 — #36
Heart, Heart-Lung, and Lung Transplantation 287
normal. However, laryngeal nerve injury duringdissection can result in loss of protective airwayreflexes.2 Reduction in lung volumes. Mild proportionalreductions in all lung volumes are seen long termin patients after HLT, DLT, and SLT. These reduc-tions are not due to reduced elastic properties ofthe transplanted lung but are secondary to the vol-ume constraints of the recipient chest cavity andto the strength and efficiency of the thoracic mus-culature. In fact, the improvement in elastic recoiland the reduced chest wall distention that followSLT for emphysema substantially reduce the workof breathing and dyspnea.3 Ventilatory response to carbon dioxide. HLT andDLT patients have total vagal denervation, whereasSLT patients retain vagal innervation to the nativelung. HLT, BSSLT, and SLT patients all increaseminute ventilation in response to carbon diox-ide rebreathing-induced hypercapnia. However,while SLT patients increase both tidal volume andrespiratory rate, HLT and BSSLT patients exhibit anincrease in tidal volume with little or no respiratoryrate response.4 Ventilatory response to hypoxia. Lung transplantpatients have an increase in tidal volume and res-piratory rate comparable to normal patients inresponse to hypoxia.5 Rejection. Acute rejection of the transplantedlungs can be diagnosed both clinically and withtransbronchial biopsies via a flexible bronchoscope.In the absence of clinical evidence of rejection(dyspnea, fever, diffuse perihilar infiltrate on chestradiograph) biopsies are performed at regular inter-vals postoperatively, Obviously, if clinical evidenceof rejection exists, more frequent biopsies may beindicated to document rejection and to assessregression of histologic changes with treatment.Biopsies are graded from 0 to 4 based on histologiccriteria.
Acute rejection of the lungs is very common;approximately 50% of patients experience an acuterejection episode in the first 3–6 months post-transplantation. Rejection of the heart in HLTpatients, on the other hand, is uncommon. Becauserejection of the heart and lungs is not synchronous,heart biopsies are performed in HLT patients
only if there is clinical evidence of heart rejec-tion. Rejection is treated with oral or intravenouspulsed steroids. Persistent rejection unresponsive tosteroids usually is treated with a lympholytic agentsuch as polyclonal antithymocyte globulin (ATG) ormurine monoclonal antibody (OKT3).1 Bronchiolitis obliterans syndrome (BOS) and bron-chiolitis obliterans (BO). BOS is a clinical entitycharacterized by declining FEV1, FEF25–75, andFEF50/FVC. BOS is graded based on the reductionin FEV1 compared with the best baseline value(0: FEV 1 > 90% and FEF25–75 > 75%; 1: FEV1
66–80%; 2: FEV1 51–65%; 3: FEV 1 < 50%). BO isa pathologic diagnosis based on histologic evidenceof fibrous scarring of membraneous and respiratorybronchioles with partial or complete obliterationof the lumen. BOS and BO are the main sourcesof morbidity and mortality after lung transplanta-tion. The prevalence of BOS and BO for HLT, SLT,and BSSLT patients is at 25% at 1 year, 50–60% at3 years, 60% at 5 years, and 80% at 10 years in largeseries. The survival rate for lung transplant patientsis 76% at 1 year, 60% at 3 years, 49% at 5 years, and24% at 10 years.
Once established, BOS and BO follow a progres-sively worsening course. Patients with BOS and BOultimately develop severe obstructive pulmonarydisease and progressive hypoxemia. Augmentedimmunosuppression may attenuate this downhillcourse and improve survival. In severe progres-sive cases, retransplantation is the only option.However, the results are not encouraging, with a5-year survival of 45%, as BOS and BO usuallyreoccur within a short time.
The etiology is multifactorial with rejection andCMV infection both implicated. It is believed thatan alloimmune injury occurs with subsequentrelease of immunologic mediators and productionof growth factors that lead to luminal obliterationand scarring of the small airway. Monitoring forBO is accomplished with transbronchial biopsiesor open lung biopsy when transbronchial biopsiesspecimens are equivocal.2 Response to drugs. HLT patients have a den-ervated heart and have drug responses iden-tical to those described for heart transplantpatients.

Alice Nelson Dinardo: “ch07” — 2007/7/17 — 20:31 — page 288 — #37
288 Chapter 7
3 HLT patients. These patients will have all ofthe cardiac problems outlined previously for hearttransplant patients.
Anesthetic considerations fornoncardiac surgery in patientspost lung transplantation1 Sterile technique is essential.2 Patients with stenotic airways and patientswith BOS and BO may exhibit air trapping andauto-PEEP.3 Diminished cough reflex makes clearing of secre-tions difficult. Laryngeal damage will predispose toaspiration.4 Lymphatic interruption necessitates careful fluidadministration to avoid interstitial pulmonary fluidaccumulation.5 Placement of an ETT must take into account theposition of the tracheal or bronchial anastomoses.6 Patients with preoperative carbon dioxide reten-tion may exhibit carbon dioxide retention for2–3 weeks postoperatively as the centralchemoreceptors reset.7 HLT patients will present the same cardiacchallenges as heart transplant patients.8 Stress-dose steroid coverage should be admin-istered to patients receiving steroids as part ofimmunosuppression.
Suggested reading
Bengel FM, Ueberfuhr P, Schiepel N et al. Effect of sympa-
thetic reinnervation on cardiac performance after heart
transplantation. N Engl J Med 2001;345:731–8.
Boucek MM, Edwards LB, Keck BM et al. Registry of the
International Society for Heart and Lung Transplanta-
tion: eighth official pediatric report – 2005. J Heart Lung
Transplant 2005;24:968–82.
Cimato TR, Jessup M. Recipient selection in cardiac
transplantation: contraindications and risk factors for
mortality. J Heart Lung Transplant 2002;21:1161–73.
Orens JB, Estenne M, Arcasoy S et al. International guide-
lines for the selection of lung transplant candidates:
2006 update – a consensus report from the Pulmonary
Scientific Council of the International Society for Heart
and Lung Transplantation. J Heart Lung Transplant
2006;25:745–55.
Taylor DO, Edwards LB, Boucek MM et al. Registry
of the International Society for Heart and Lung
Transplantation: twenty-second official adult heart
transplant report – 2005. J Heart Lung Transplant
2005;24:945–55.
Trulock EP, Edwards LB, Taylor DO et al. Registry of the
International Society for Heart and Lung Transplan-
tation: twenty-second official adult lung and heart-
lung transplant report – 2005. J Heart Lung Transplant
2005;24:956–67.
Valantine H. Cardiac allograft vasculopathy after heart
transplantation: risk factors and management. J Heart
Lung Transplant 2004;23:S187–93.

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 289 — #1
CHAPTER 8
Pericardial Disease
Effective perioperative care for patients withpericardial disease depends on a thorough under-standing of the physiologic alterations the diseasedpericardium imposes on the heart. This chapterreviews the normal physiology of the pericardium,followed by a discussion of the physiologic derange-ments caused by a pericardial effusion or a constrict-ing pericardium. Diseases that can cause pericardialdysfunction will be discussed, including aspects ofillnesses that affect anestheticmanagement. Finally,the anesthetic management of generic patients withpericardial tamponade and constrictive pericarditiswill be reviewed.The normal pericardium is a dual envelope that
surrounds the heart and separates the chambersfrom the bordering chest wall, pleura, and great ves-sels. There is a visceral layer that is composed ofmesothelial cells adherent to the epicardial surfaceof the heart, and a thicker, fibrous parietal layer thatseparates the heart from other thoracic structures.The pericardium contains approximately 25mL ofan ultrafiltrate of plasma. The oblique sinus liesbehind the posterior wall of the left atrium (LA),where the pericardium is adherent to the vena cavaand pulmonary veins. This defines an area of thepericardial space in which an effusion does notcollect unless it is very large or under pressure.The transverse sinus is just inferior to the aorticarch and is often visualized with transesophagealechocardiography (TEE). The low compliance of thenormal parietal pericardium is responsible for thepathophysiologic mechanisms seen in pericardial
tamponade and accounts for the difference in pre-sentation in patients with either an acute or chroniceffusion.The normal pericardium is richly enervated
and inflammation can result in severe pain orvagally mediated reflexes. The pericardium is anactive structure providing myocardial stability, apotential barrier to infection and prostaglandinsecretion modulating cardiac reflexes and coro-nary tone. Afferents from the pericardium travelvia the phrenic nerve, entering the spinal cord atC4–C6. Pericardial pain often is symptomaticallyindistinguishable from a diaphragmatic source. Thephrenic nerves travel along the lateral aspects of thepericardium, where they are subject to mechani-cal or cold induced injury during cardiac surgery.The presenting symptoms of pericardial diseases arerelated to the innervation of the pericardium andthe location of adjacent structures. For example,a large pericardial effusion may present as dys-pnea, dysphagia, cough, hiccups, or hoarsenessdue to compression of adjacent lung, esophagus,diaphragm, or recurrent laryngeal nerve.There are two principle physiologic expressions of
pericardial disease: effusion, with or without tam-ponade, and constriction. It is essential to realizethat both pericardial tamponade and constrictivepericarditis produce ventricular diastolic dysfunc-tion. An understanding of the physiology of thesediastolic limitations will provide the anesthesiolo-gist with the knowledge to safely anesthetize thesepatients.
289

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 290 — #2
290 Chapter 8
ECG
PCG
JVP
S4
ac
v
x y
d
isTime
S1 S2 S3
25 cm/s
20JVF
10
5
0
−5a
Fig. 8.1 Atrial wave forms, electrocardiogram (ECG)and phonocardiogram (PCG) drawing demonstrating thenormal jugular venous pressure (JVP) waveforms andjugular venous flow (JVF). (Reprinted fromKalmanson D, Veyrat C, Chiche P. Atrial versusventricular contribution in determining systolic venousreturn. A new approach to an old riddle. Cardiovasc Res1971;5:293–302, with permission.)
Normally, venous return to the right side of theheart is accelerated during ventricular systole. Thisis due, in part, to a reduction in total intraperi-cardial volume (cardiac structures plus pericardialcontents), which generates a pressure gradient fromthe vena cava to the right atrium. This increasedrate of venous flow is represented in the rightatrial (RA) waveform by the X descent (Fig. 8.1).The second surge in venous return occurs dur-ing the latter phase of atrial systole, when thetricuspid valve opens. This is visualized as theY descent in the RA waveform (see Fig. 8.1). Anal-ysis of the RA (or central venous) pressure wave-form, right ventricular (RV) pressure tracing, andthe pulmonary capillary wedge pressure can dif-ferentiate pericardial tamponade from constrictivepericarditis.
Pericardial effusion
The clinical manifestations and hemodynamicconsequences of blood or other fluid in the
Pre
ssur
e
Rapid effusion Slow effusion
Limit of pericardial stretch
Volume over time
Criticaltamponade
Criticaltamponade
Fig. 8.2 Total intrapericardial pressure as a function ofchanging intrapericardial volume. Until a critical volumeis reached, there is little rise in pressure. Once the criticalcompliance/pressure relationship is reached, however,small additional increments in volume result in largechanges in intrapericardial pressure. (From Spodick DH.Acute cardiac tamponade. N Engl J Med2003;349:684–90, with permission.)
pericardial space are determined primarily by thevolume and rate of accumulation of the effu-sion. A slowly accumulating effusion allows timefor the parietal pericardium to stretch resulting insometimes very large, asymptomatic effusions. Con-versely, acute pericardial effusions without pari-etal pericardial stretch can lead to tamponade withresultant cardiogenic shock and death. The com-pliance curve of the normal pericardium is seenin Fig. 8.2. In either acute or chronic pericardialeffusion, when the volume exceeds the limits ofpericardial stretch, there is a sharp elevation inintrapericardial pressure. There is a reduction inventricular filling and stroke volume.In the operating room environment, the patho-
physiology of pericardial tamponade is oftenobserved in acute, hemorrhagic pericardial effu-sions. This can occur in patients with traumaticcardiac injury, iatrogenic injury (catheterizationand pericardiocentesis mishaps), aortic dissection,and post-cardiac surgery bleeding. There is associ-ated hypotension, elevated venous pressure, and asmall “quiet” heart (Beck’s triad). Hypotension isdue to a markedly reduced stroke volume causedby the compression of cardiac chambers by theeffusion, especially on the right side. An elevation

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 291 — #3
Pericardial Disease 291
in the central venous pressure (CVP) also reflectsthe restriction to cardiac filling imposed by the tensepericardium. The CVP waveform will demonstratea prominent X descent, reflecting the acceleratedvenous return associated with ventricular systoleand with the elevation of CVP. Ventricular systolereduces total intrapericardial volume by a quan-tity equal to the stroke volume, thereby allowingenhanced atrial filling. In addition, the RA wave-form will demonstrate the absence of the Y descent,reflecting the increased ventricular end-diastolicpressure due to reduced distensibility induced bythe pericardial effusion (Fig. 8.3a,b).Pericardial tamponade can occur even in the
absence of an elevated CVP if the patient is hypo-volemic (low-pressure tamponade). This can occurwhen there is concurrent trauma with exsanguina-tion, excessive diuresis in heart failure patients orin patients with effusion undergoing hemodialysis.Cardiac echocardiography is the definitive diag-
nostic technique for documenting the presenceand magnitude of a pericardial effusion. Trans-thoracic echocardiography can be performed rapidlyat the bedside with no morbidity. TEE may pro-vide superior image quality, but there is associatedrisk with insertion of the probe and patient seda-tion. In the operating room, TEE is indicated inpatients undergoing pericardiocentesis and peri-cardiectomy. Other important imaging techniquesinclude a chest X-ray (widened mediastinum andcardiac silhouette), computerized tomography, andmagnetic resonance imaging.The echocardiographic magnitude of a pericardial
effusion is graded as large, moderate, or small. Inthe supine patient, effusions layer initially along thedependent surfaces of the heart. As the volume ofthe effusion increases, it appears apically, laterally,and then anteriorly. The typical echocardiographicfeatures suggesting tamponade physiology result-ing from an effusion are: RA collapse, which occursjust before ventricular systole; RV collapse in earlydiastole; and a reduction in RV dimensions duringend-diastole (Fig. 8.4a–c). The interventricular sep-tum is displaced posteriorly during early diastole as aconsequence of the increase in RV size. The echocar-diographic demonstration of RA and RV collapse inthe presence of an effusion can be highly predictive
ECG
(a)
(b)
40
20
0
100
50
FA
pre
ssur
e (m
mH
g)
0RA
/per
icar
dial
pre
ssur
e (m
mH
g)
FA RA Pericardium
ECG40
20
0
100
50
FA
pre
ssur
e (m
mH
g)
0
RA
/per
icar
dial
pre
ssur
e (m
mH
g)
FA RA Pericardium
x y
x
Inspiration
1 s
1 s
Fig. 8.3 (a) Simultaneous femoral arterial (FA), rightatrial (RA), and intrapericardial pressure waveformsfrom a patient with pericardial tamponade. Note theexaggerated X descent, absent Y descent, equilibration ofright atrial and intrapericardial pressures and systemichypotension. (b) Right atrial pressure (RA) waveformwith simultaneous electrocardiogram and femoralarterial pressure waveform (FA). RA tracingdemonstrates timing of X and Y descents relative tocardiac cycle. Recordings were taken from a patient withpericardial tamponade after pericardiocentesis. Note thereturn of the Y descent. Also shown are simultaneousintrapericardial pressure (pericardium) and respiratorycycle (inspiration). ECG, electrocardiogram. (FromLeWinter MM, Kabbani S. Pericardial diseases. In:Zipes DP, Libby P, Bonow RO, Braunwald E (eds).Braunwald’s Heart Disease: A Textbook of CardiovascularMedicine, 7th edn. Philadelphia: Elsevier (Saunders),2005:1757–80, with permission.)
of tamponade physiology, except in situations inwhich RV compliance is already low, as in pre-existing pulmonary hypertension or a RV infarction.When wall stiffness does not allow intrapericardialpressure to exceed intracavitary pressure, chambercollapse will not be seen.In the postoperative setting, this presentation
may be difficult to discern. The formation of

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 292 — #4
292 Chapter 8
(a)
(b)
(c)
Fig. 8.4 Transesophageal (TEE) images of a patient witha larger pericardial effusion and right atrial collapse.(a) TEE image of the transgastric short-axis viewdemonstrating a large pericardial effusion along theposterior, lateral, and anterior aspects of the heart (whitearrows). (b) TEE mid-esophageal view demonstrating theeffusion along the border of the right atrium duringventricular systole (white arrow). (c) The same viewshowing right atrial collapse during ventricular diastole(white arrow).
pericardial clot alters the distribution of an effu-sion, as does the presence of adhesions between theheart, pericardium, and anterior mediastinum. Inaddition, in the setting of a reduced intravascularvolume (i.e. hypovolemia from bleeding), patientswill manifest a low CVP despite hemodynamicallysignificant pericardial tamponade.Tamponade physiology can be determined by
cardiac catheterization. In patients with straight-forward tamponade, RA catheterization reveals anaccentuated X descent, absent Y descent, and anelevated CVP (see Fig. 8.3a,b). There will be equal-ization of RA, RV end-diastolic, and pulmonary cap-illary wedge pressures. These pressures will equalintrapericardial pressure, when measured duringpericardiocentesis. These findings apply only topatients who do not have an underlying condi-tion that alters right or left ventricular compliance,such as prior infarction, pulmonary hypertension,ongoing ischemia, or left ventricular hypertrophy.Pulsus paradoxus, an exaggeration of the nor-
mal 5mmHg decrease in systolic blood pressurewith inspiration, is often seen in pericardial tam-ponade. A pulsus paradoxus is present when thisdifference exceeds 10mmHg. Although a numberof mechanisms for pulsus paradoxus have been pos-tulated, echocardiographic studies have provided acoherent explanation. During inspiration, the neg-ative pressure gradient between the periphery andthe intrathoracic veins is increased. This increasein negative intrathoracic pressure is transmitted tothe intrapericardial structures, accelerating the rateof venous return to the right-sided chambers ofthe heart. The resultant increase in RV dimensionscauses a shift of the interventricular septum to theleft, diminishing left ventricular diastolic filling andreducing left ventricular stroke volume and sub-sequent systolic arterial pressure (Fig. 8.5). Thismechanism has been confirmed by pulsed waveDoppler echocardiography. Normally, there is asmall increase (<25%) in early tricuspid blood flowvelocity and a concomitant small decrease (<10%)in early mitral blood flow velocity with inspira-tion as compared with expiration. This pattern isexaggerated in the presence of tamponade withearly tricuspid flow velocity increasing by as muchas 130%, and early mitral flow velocity decreasing

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 293 — #5
Pericardial Disease 293
Fig. 8.5 In some patients with pulsusparadoxus there is a septal shift duringinspiration limiting left ventricular fillingand reducing stroke volume. This mayaccount for the exaggerated reductionin arterial pressure observed duringinspiration. (From Goldstein JA. Cardiactamponade, constrictive pericarditis, andrestrictive cardiomyopathy. Curr ProblCardiol 2004;29:503–67, withpermission.)
PA Ao
RA
RV
LA
LV
Tense pericardial effusion
Increased PA flow
Increasedreturnmaintainspressure
Decreased Ao flowand pressure
Pressurefalls
Decreasedfilling
Expiration Inspiration
Increasedfilling
by as much as 50% with inspiration as comparedwith expiration.Pulsus paradoxus can be observed in patientswith
disorders unrelated to pericardial tamponade. Theseinclude severe chronic obstructive pulmonary dis-ease, asthma, and pulmonary embolism. Further,pulsus paradoxus may be absent in patients withpericardial tamponade who have coexistent cardiacpathology. Any condition that allows equalizationof venous return between the right and left sides ofthe heart, such as an atrial septal defect, will preventexpression of a pulsus paradoxus. In addition, pul-sus paradoxus will not be demonstrable wheneverthe interventricular shift that accompanies inspi-ration is prevented by conditions that reduce leftventricular compliance and distensibility such asleft ventricular hypertrophy, left ventricular failure,infarction, ischemia, or aortic valve incompetence.Finally, pulsus paradoxus may not be demonstrablein patients with elevated RV end-diastolic pressuredue to pulmonary hypertension or pulmonary out-flow obstruction. The hemodynamic characteristicsof cardiac tamponade are summarized in Table 8.1.The therapy for hemodynamically significant
pericardial tamponade is drainage. The recom-mended approach for removal of the effusionwill depend on the acuity and severity of hemo-dynamic compromise. Percutaneous pericardio-centesis under ultrasound guidance and localanesthesia can be performed at the bedside andmay be life-saving. Blind pericardiocentesis is
Table 8.1 The hemodynamic characteristics of cardiactamponade.
• Diastolic dysfunction with impaired right heart filling• Elevated right atrial pressure• Prominent X descent on central venous pressurewaveform• Blunted or absent Y descent on central venous pressurewaveform• Equalization of diastolic pressures• Diminished intracardiac chamber volumes• Diastolic collapse of right atrium and ventricle• Right ventricular septal shift during late diastole withinspiration• Decreased blood pressure, cardiac output, and strokevolume• Increased systemic vascular resistance• Increased heart rate• Pulsus paradoxus• Exaggerated transvalvular flow with respiration
associated with a high rate of complications includ-ing pneumothorax, coronary artery or internalmammary artery laceration, and ventricular cham-ber perforation. These complications are even morelikely if there are pericardial adhesions betweenthe pericardium and anterior mediastinum, as inpostoperative cardiac surgical patients, patients whohave received chest irradiation, or when there isassociated pericarditis. The success of pericardio-centesis is partly a function of the etiology of theeffusion. Pericardiocentesis under fluoroscopic or

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 294 — #6
294 Chapter 8
echocardiographic control is very successful forlarge malignant or uremic effusions, whereas peri-cardiocentesis for a postoperative effusion, evenunder fluoroscopic or echocardiographic guidance,has limited success.
Surgery for pericardial effusion andtamponadeThe indications and timing of surgery for a pericar-dial effusion depend on the etiology of the effusion,its rate of accumulation, and the severity of thehemodynamic compromise.There are three surgical options for permanent
drainage of recurrent pericardial effusions: a peri-cardial window, a partial pericardiectomy, or afull pericardiectomy. A pericardial window createscontinuity between the pericardium and pleura orthe pericardium and peritoneum. It can be per-formed under local anesthesia, with the patientin the semi-sitting position. Its advantages includeobtaining a pericardial specimen for pathologicexamination and minimal physiologic trespass. Forthese reasons, it is the approach taken most oftenfor patients with malignant pericardial effusions,whose life expectancy from their underlying dis-ease is measured in weeks to months, or for patientswith hemodynamically significant uremic pericar-dial effusions who are awaiting initiation or inten-sification of hemodialysis. The operative mortalityis very low and is primarily a function of thepatient’s underlying disease. The drawbacks to apericardial window include a significant incidenceof re-accumulation of the effusion, as well as thepotential development of constrictive pericarditis.Pericardioscopy allows visualization of much of
the epicardial surface, as well as examination ofthe intrapericardial structures. It is useful in direct-ing intraoperative biopsy for diagnostic purposes.Because of the possibility of mechanically-induceddysrhythmias during periocardioscopy, prepara-tions for emergent electrical cardioversion or defib-rillation must be made before the induction ofanesthesia.In as many as 75% of patients undergoing full or
partial pericardiectomy the indication for the proce-dure is refractory pericardial effusion. Of these, themost common etiologies are neoplastic disease and
uremia. The incidence of pericardial tamponade inthe period immediately after cardiac surgery maybe as high as 1–5%. In these patients, mediasti-nal exploration for bleeding with clot removal isrequired when signs and symptoms of tamponadeare present.
Anesthetic technique for pericardialeffusion and tamponadePatients undergoing a pericardiectomy fortamponade or recurrent effusion present a uniqueconstellation of problems for the anesthesiologist.The anesthetic considerations in these patientsare outlined in Table 8.2. It is essential that thecardiac anesthesiologist obtain a preoperativeassessment of the effusion’s magnitude, and moreimportantly, its hemodynamic effect. Except whenthe patient’s condition does not allow time forpreoperative echocardiography and/or catheteri-zation, this information should be available andreviewed.Ventricular filling in diastole is limited to a vary-
ing degree by the effusion. This can range fromtrivial compromise to cardiovascular collapse. Anymaneuver that reduces venous return has thepotential of further diminishing diastolic filling tothe point at which stroke volume becomes inade-quate to sustain life. Such maneuvers potentiallyinclude positive-pressure ventilation, hypovolemia,and systemic venodilatation.
Initial management of patients withan effusionThe degree of RA and RV collapse is assessed eas-ily with echocardiography, and this informationusually is available before induction. Patients withtamponade will require volume infusion to raiseCVP and improve RV filling. It may be necessaryto increase the CVP to 20 or 30mmHg in somepatients. Most patients with tamponade will havecomplete emptying of the RV and left ventricle (LV)in systole as a compensatory measure. If echocar-diographic examination or previous history suggestssystolic impairment, inotrope infusion is warrantedto optimize stroke volume. An agent that is notassociated with vasodilation (e.g. epinephrine) isindicated. Vasodilationmust be avoided as it reduces

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 295 — #7
Pericardial Disease 295
Table 8.2 Anesthetic considerations in pericardial effusion and tamponade.
• Administer preoperative sedation or analgesia with caution. These patients are often on the verge of cardiovascularcollapse• In cases of severe tamponade (i.e. patient in extremis or cardiovascular collapse), consider relieving the restriction todiastolic filling before the induction of anesthesia• Administer positive pressure ventilation with caution until tamponade physiology has been relieved• Maintain filling pressures high enough to overcome diastolic filling restrictions. The central venous pressure orpulmonary capillary wedge pressure may need to be 20–30 mmHg• Avoid vasodilation – the resulting hypotension will worsen the diastolic filling dysfunction• Avoid bradycardia – an elevated heart rate is a normal compensatory mechanism in cardiogenic shock• Consider inotropic support in the interval before the tamponade is relieved (epinephrine)• Prepare for a rebound in hemodynamics once the pericardial space is drained in acute tamponade. The sudden rise inblood pressure in patients with normal left ventricular function can be dramatic• Carefully evaluate the necessity for invasive monitoring. Intra-arterial pressure monitoring is very helpful and can usuallybe accomplished pre-induction without delay. Central venous access is usually not indicated and may lead to unnecessarydelays and increased morbidity in some patients. Intraoperative TEE is helpful in documenting and guiding the pericardialfluid drainage. In addition, TEE can monitor heart function during this interval of unstable and changing hemodynamics
TEE, transesophageal echocardiography.
RV filling and systemic blood pressure in patientswho have a fixed stroke volume. Alpha-adrenergicsupport may be necessary to maintain perfusionpressure. Since the stroke volume is fixed, heartrate must remain normal to high to maintain anadequate cardiac output.Patients in extremis should undergo pericar-
diocentesis with local anesthesia, preferably withechocardiographic or fluoroscopic guidance, beforethe induction of general anesthesia and initiation ofpositive-pressure ventilation. Although blind peri-cardiocentesis using an ECG lead on the exploringneedle to detect injury current has been used in thepast, echocardiographic guidance is now standard.Reference to the pericardial compliance curve (seeFig. 8.2) indicates that the entire effusion need notbe drained before induction of general anesthesia. Itis necessary to remove only a small volume of fluidto place the patient below the bend of the pericar-dial pressure–volume curve and effect a dramaticimprovement in hemodynamics.
PremedicationDrainage of pericardial fluid is often an urgent oremergent procedure for patients with some degreeof hemodynamic compromise. Extreme caution
with premedication is warranted. Midazolam inincrements 0.5–1.0mg is a reasonable approach.
Pre-inductionAs for other cardiac surgical procedures, ECG leadsfor I, II, III, aVR, aVL, aVF, and V5 should be inplace before induction. Adequate intravenous (IV)access with at least one large-bore (14- or 16-gauge)catheter should be obtained. Ideally, a radial arterycatheter is placed before induction. Central venousaccess is usually not indicated in most patients.
Induction and maintenanceFor the patient with a small, hemodynamicallyinsignificant effusion the anesthetic managementwill be dictated primarily by the patient’s under-lying medical condition and the general principlesoutlined in anesthetic care. For patients with tam-ponade, great care must be employed if the decisionis made to proceed without first relieving some ofthe effusion percutaneously.The patient should be prepped and draped before
induction in case emergent surgical decompres-sion is needed after induction. Induction withagents with minimal cardiovascular effects is war-ranted. Etomidate 0.3mg/kg in combination withfentanyl 1–3µg/kg or sufentanil 0.2–0.3µg/kg is

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 296 — #8
296 Chapter 8
appropriate. Ketamine 1–2mg/kg IV may be usedbecause it maintains heart rate, contractility, andsystemic vascular resistance (SVR). Caution mustbe exercised for patients who have high existingsympathetic tone because the negative inotropiceffects of ketamine will predominate. Muscle relax-ants should be chosen to offset any vagotonic effectsof the narcotics. Amnesia can be maintained withbenzodiapines or low doses of inhalational agents.After the effusion has been relieved, the choice ofanesthetic agents should be guided by the patient’sunderlying disease state and consideration ofpostoperative ventilatory requirements.A TEE probe can be inserted after induction and
tracheal intubation. This allows online assessmentof ventricular filling and contractility. In addition,the completeness of fluid evacuation can be easilyassessed.Drainage of a large effusion and relief of tampon-
ade generally produces a marked improvement inhemodynamics. In some patients, this rapid alter-ation in fluid statusmay produce pulmonary venouscongestion or pulmonary edema. This is due to thesudden increase in pulmonary venous return to theLA and LV. This is particularly likely if there isreduced LV systolic function or lesions that predis-pose an elevation of left atrial pressure (i.e. mitralregurgitation, mitral stenosis or poor LV compli-ance). Treatment will require vasodilation with IVnitroglycerin or a similar agent.
Constrictive pericarditis
Constrictive pericardial disease, like pericardial tam-ponade, causes a restriction to diastolic filling.In contrast to tamponade, however, all chambersare affected equally and the pattern of restric-tion to filling is distinctly different. The clinicalmanifestations of constrictive pericarditis may bequite subtle and easily mistaken for a restrictivecardiomyopathy.Constrictive pericarditis is an inflammatory pro-
cess caused by a myriad of processes. The morecommon causes are idiopathic, infectious (viral >
bacterial), neoplastic, autoimmune, uremic, post-irradiation or surgery, post-traumatic, and post-myocardial infarction. Tuberculosis was the most
common cause; however, this is no longer true indeveloped countries.The underlying pathologic process in constric-
tive pericarditis is a thickened, fibrotic, scarred, anddensely adherent pericardium,with the visceral andparietal layers often fused and occasionally calcified.The antecedent illness may be subclinical pericardi-tis, with fibrin deposition and subclinical effusionformation; a pericardial effusion with incompleteresorption or drainage; or an infiltrative or reactiveprocess.Constrictive pericarditis equally impairs late dias-
tolic filling of all heart chambers. Over time, thisresults in symptoms of biventricular failure. Earlyin the course of the patient’s illness, fluid retentionpartially compensates for the restriction in diastolicfilling by maintaining an elevated central venousvolume. This results in a clinical picture similarto right-sided congestive heart failure with ascites,pleural effusions, and peripheral edema. There isa reflex tachycardia serving to maintain strokevolume and cardiac output. Although myocar-dial systolic function usually is intact, epicardialcompression of coronary arteries with resultantischemia can occur. As stroke volume becomeslimited due to inadequate preload, symptoms ofchronic low cardiac output prevail, includingweightloss, fatigue, muscle wasting, and cachexia.The physical examination demonstrates an
elevation in jugular venous pressure. Cardiac exam-ination reveals a heart with a fixed point of max-imal impulse (heart adhered to pericardium) anda pericardial knock. The pericardial knock is heardbest in early diastole (the time of maximal fillingin pericarditis) along the left sternal border. Theknock occurs when the heart rapidly fills and thereis abrupt cessation of flow when the pericardialrestriction is encountered. The ECG in pericarditischanges as the disease progresses. In the acute phasethere is diffuse ST segment elevation and PR seg-ment depression. In later stages, T-wave inversionis present.An additional finding in constrictive pericarditis
is Kussmaul’s sign, the apparently paradoxical risein CVP with inspiration. In pericardial tamponade,the increase in negative intrathoracic pressure asso-ciated with inspiration is transmitted to the heart,

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 297 — #9
Pericardial Disease 297
ECG
40
20
RA X Y
LVLVLVmm
Hg
Fig. 8.6 Right atrial (RA) and left ventricular (LV)pressure waveforms obtained from patient withconstrictive pericarditis. Prominent X and Y descents givecharacteristic “M” and “W” appearance to the right atrialpressure waveform. Note also that right and left heartpressures are elevated and equal throughout diastole.(Reprinted from Lorell BH, Grossman W. Profiles inconstrictive pericarditis, restrictive cardiomyopathy, andcardiac tamponade. In: Grossman W (ed). CardiacCatheterization and Angiography, 3rd edn. Philadelphia:Lea & Febiger, 1986, with permission.)
resulting in a transient decrease in CVP, strokevolume, and systolic pressure (pulsus paradoxus).In contrast, the thickened unyielding pericardiumin constrictive pericarditis prevents the changesin intrathoracic pressure associated with ventilationfrom being transmitted to the heart. This restrictionresults in either no change or an increase in CVP atthe time of inspiration. This difference in the effectof ventilation has important clinical implications forthe anesthetic management of these two groups ofpatients.Hemodynamicmonitoring is important in patients
with constrictive pericarditis and reveals charac-teristic findings. The CVP waveforms demonstrateprominent X and Y descents, imparting a character-istic “M” or “W” shape to the atrial pressure wave-form (Fig. 8.6). There is early diastolic equilibrationof pressure within all four chambers, revealed bythe equalization of pressures in diastole betweenthe atrium and ventricle. Ventricular filling is ini-tially rapid, due to the increased venous pressure,which is seen as a sharp dip in intraventricular pres-sure. After the limit to filling imposed by the stiff,unyielding pericardium has been reached, furtherdiastolic filling is halted abruptly. This appears onhemodynamic recordings as a “square root sign”or “dip and plateau,” characteristic of constrictivepericarditis (Fig. 8.7a,b).
40
20
20
10
0RV LV
(a)
40
20
20
10
0RA
x y
LV
(b)
Fig. 8.7 (a) Right (RV) and left ventricular (LV)pressure tracings from a patient with constrictivepericarditis, demonstrating the rapid early diastolicfilling, followed by the abrupt cessation of filling once thelimit imposed by the pericardium has been reached. Thishas been described as a “dip and plateau” or “squareroot” sign. (b) Simultaneous tracing of LV and right atrial(RA) waveforms. Note also the equilibration throughoutdiastole of right and left ventricular pressures. (Reprintedfrom Vaitkus PT, Cooper KA, Shuman WP, Hardin NJ.Images in cardiovascular medicine: constrictivepericarditis. Circulation 1996;93:834, with permission.)
Table 8.3 summarizes the hemodynamic findingsin constrictive pericarditis.
Etiology of pericardial disease
The hemodynamic alterations seen in pericardialdisease will have a great impact on the anestheticmanagement of these patients. It is important toremember that the underlying illness causing thepericardial disease may have equal or even greaterweight in the considerations necessary for a safe

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 298 — #10
298 Chapter 8
Table 8.3 Hemodynamic characteristics in pericarditis.
• Diastolic dysfunction with abrupt diastolic fillingresistance• Elevation and equalization of diastolic pressures• Prominent X and Y descent (“M” or “W” sign)• Ventricular dip and plateau (square root sign)• Decreased cardiac output, stroke volume• Kussmaul’s sign• Pulsus paradoxus uncommon (approximately 33%)• Pericardial knock present
anesthetic. This section will review the anestheticimplications of those disease states.
UremiaPericardial effusions may be seen in as many as20% of patients with hemodialysis-dependant renalfailure. Initiation or intensification of hemodialysiswill resolve a hemodynamically significant effu-sion in two-thirds of patients. Operative drainagefor uremic pericardial effusions should be reservedfor patients who have not responded to augmen-tation for their dialysis regimen. The effusion maybe hemorrhagic, and if left untreated, may evolveinto constrictive pericarditis. Asymptomatic effu-sions are common in patients with chronic renalfailure.Renal failure alters the anesthetic management
of patients with a pericardial effusion or constric-tive pericarditis in a number of ways. The pre-operative evaluation must include close scrutinyof the patient’s coagulation capability due to theimpairment of platelet function associatedwith ure-mia. Efforts to correct a coagulopathy should beundertaken before surgical intervention for con-strictive pericarditis, because surgical hemostasis ofraw, bleeding surfaces will be difficult to achievein the presence of a bleeding disorder. Admin-istration of desmopressin (DDAVP), 0.3–0.4µg/kgmay improve platelet function and coagulopathy inuremic patients.Renal failure alters the kinetics of many anes-
thetic agents, especially nondepolarizing musclerelaxants. Cisatracurium is preferred in renal fail-ure patients because of its independence fromrenal function for metabolic clearance. Although
patients with chronic renal failure are adaptedto a higher than normal baseline plasma potas-sium concentration, succinylcholine must be usedwith caution to avoid the possibility of furtherhyperkalemia.
Infectious pericarditisTuberculosis accounts for approximately 4% ofacute pericarditis cases. Initial symptoms are vari-able with most patients presenting with a fever,weight loss, night sweats, pericardial friction rub,and pleural and pericardial effusions, with 40%demonstrating tamponade physiology. In mostpatients, tuberculosis pericarditis is self-limiting andclinically seems to be idiopathic in origin untilother evidence of tuberculosis is discovered. Manypatients with pericardial effusions will require peri-cardiectomy to treat a reaccumulation of fluid,in spite of initial pericardiocentesis. Up to one-half of patients with acute tuberculous pericarditiscan develop constrictive pericarditis requiring peri-cardiectomy 2–4months after presentation. Spu-tum culture is the most frequent positive diagnostictest in those patients who present with acute peri-carditis. Acid-fast staining of pericardial fluid isinfrequently positive, unlike culture results. Patho-logic examination of pericardial biopsy specimensis occasionally positive. Untreated tuberculous peri-carditis has a highmortality in the range of 30–40%.Some authors recommend early surgery for apericardial window, to prevent effusion reaccumu-lation and possibly the development of late constric-tion, and early full pericardiectomy if a thickenedpericardium is found at that time.Viral pericarditis can be due to a variety of
agents, including coxsackie B, echoviruses, vari-cella, mumps, hepatitis B, or cytomegalovirus. Viralpericarditis is more common in immunosuppressedpatients. Bacterial agents usually are staphylococ-cus, pneumococcus, or meningococcus. Infectionspreads from adjacent sites and occurs in associationwith hematogenously seeded bacterial endocarditisor from extension of a subdiaphragmatic abscess.Although acute bacterial pericarditis is unusualin the antibiotic era, purulent pericarditis occursmost often in immunosuppressed patients or inthe setting of a preexisting effusion (such as with

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 299 — #11
Pericardial Disease 299
uremia). Constriction may be a late consequenceof incomplete drainage of a purulent effusion.Histoplasmosis is the most common fungal etiol-ogy. As with other infectious agents, pericardialinvolvement is most likely in those patients whoare immunosuppressed. If the patient has receivedamphotericin B, consideration must be given tothe possibility of impaired renal function and, lessfrequently, hemolysis or hypokalemia.
Idiopathic pericarditisThis is the most common cause of acute pericarditisin many series, and certainly includes many cases ofviral pericarditis in which the virus is not identified.
Post-myocardial infarction pericarditisPericarditis within a few days to a week aftermyocardial infarction occurs in 5–10% of patients.The typical presentation is new chest pain, asso-ciated with an evanescent pericardial friction rub.New chest pain after a myocardial infarction mustbe differentiated from other, more serious com-plications of an infarction. The new chest pain ofpost-infarction pericarditis must be distinguishedfrom that of unstable angina, an extension of theoriginal infarction, or an additional infarction. His-tory, serial ECGs, echocardiograms, and cardiac-specific isoenzyme concentrations will help makethe diagnosis. New chest pain associatedwith amur-mur may herald a post-infarction ventricular septaldefect (VSD) or post-infarction mitral regurgitation,due to papillary muscle rupture or ischemia. Thelatter conditions usually are associated with hemo-dynamic compromise, whereas pericarditis after anacute infarction is not. If there is serious question ofdifferentiating themore benign pericarditis from theother two conditions, echocardiographywill resolvethe issue quickly. If a patient with post-infarctionpericarditis requires surgical intervention, appro-priate anesthetic management will be determinedprimarily by the presence and severity of underlyingmyocardial ischemia, as well as residual myocardialsystolic and diastolic function.
Connective tissue disordersThe systemic manifestations of systemic lupus ery-thematosus are protean. Pericarditis is the mostfrequent cardiac manifestation, with tamponade
occurring infrequently, and constrictive pericardi-tis occurring rarely. Myocardial involvement maylead to conduction abnormalities or, infrequently,contractile dysfunction with direct impairment ofsystolic function. There may be direct involve-ment of cardiac valves in 20% of patients withlupus. In some, valvular dysfunction may be severeenough to be clinically significant. Rarely, an arteri-tis can result in clinically significant coronaryartery disease. In addition, accelerated atheroscle-rosis in patients with lupus, in part a consequenceof prolonged corticosteroid use, increases the riskof myocardial ischemia and infarction. Patientswith lupus severe enough to necessitate operativeintervention for effusive, pericardial, or valvulardisease usually are receiving systemic steroid ther-apy and will need prophylactic corticosteroid ther-apy to protect them from a chronically suppressedpituitary–adrenal axis.Nonsteroidal anti-inflammatory agentsmay inter-
fere with platelet thromboxanes, resulting in acoagulation defect. However, fewer than 10%of patients with lupus will have a significantthrombocytopenia. Lupus patients may have acirculating anticoagulant, which presents as anotherwise unexplained prolonged partial thrombo-plastin time (aPTT). The lupus anticoagulant is atest-tube anticoagulant only interfering with thephospholipid tissue thromboplastins used for thelaboratory determination of the partial thrombo-plastin time and is not associated with a bleedingtendency in vivo. In fact, patients with a lupusanticoagulant are at risk for thrombotic events.Therefore, long-term anticoagulation should beconsidered for patients with a lupus anticoagulantwho are undergoing valve replacement.Pulmonary involvement may result in restrictive
lung disease, with a resulting diffusion defect andarterial hypoxemia. Chronic renal failure may bea late result of lupus, with well recognized impli-cations for anesthetic management. Active lupuscerebritis may make conduct of a procedure such aspericardiocentesis difficult or impossible under localanesthesia.Chronic constrictive pericarditis can occur as
a complication of rheumatoid arthritis. Approx-imately one-third of patients with rheumatoid

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 300 — #12
300 Chapter 8
arthritis will have pericardial thickening or effu-sion seen by echocardiography. Pericarditis usuallyis seen only in those patients with otherwise severemanifestations of their disease. In these patients,constrictive pericarditis usually improves after peri-cardiectomy. Conduction system abnormalitiesmaybe due to myocardial rheumatoid nodules or frominflammatory changes. Severe rheumatoid arthritisis associated with cervical spine disease includingatlantoaxial subluxation and the potential for spinalcord or vertebral artery compression. There is pos-sible involvement of the temporomandibular andcricoarytenoid joints further complicating airwaymanagement. Most rheumatic pleural effusions willspontaneously resolve, but some will require per-cutaneous or surgical drainage or decortication forrecurrent pleuritis.
MalignanciesMalignant pericardial disease is associated mostcommonly with cancers of the breast and lung,Hodgkin disease, and other lymphomas. The spec-trum of pericardial disease associated with malig-nancies ranges from acute hemorrhagic pericardialtamponade, to compression syndromes from tumormasses (Fig. 8.8), to constrictive physiology from anoncompliant pericardium encasedwith infiltrating
Fig. 8.8 This pregnant patient has marked ventricularcompression from her liver (white arrow A), and herHodgkin lymphoma tumor mass (white arrow B). Thispatient exhibited classic symptoms of a constrictivepericardial disease due to her pregnancy and extrinsicneoplastic pathology.
tumor. Unlike patients with radiation-induced con-strictive pericarditis, patients with pericardial dis-ease secondary to a malignancy may present withsigns and symptoms of pericardial tamponade,constrictive disease, or a combination of both.Large mediastinal masses, which can be seen
in patients with Hodgkin lymphoma, pose signifi-cant risk of intrathoracic airway compression duringthe institution of positive pressure ventilation inde-pendent of endotracheal intubation. The physicalpresence of such masses should be sought bycomputerized tomography or magnetic resonanceimaging before surgical intervention for pericar-dial disease. The functional significance of ante-rior mediastinal masses can be evaluated byflow–volume spirometry. If functional intrathoracicairway compression is present, there often will bea flattening of the expiratory phase of the flow–volume loop in the supine but not sitting posi-tions. Furthermore, many such patients will reportsymptoms of air hunger or a sensation of chestcompression in the supine but not in the lateralor sitting positions. When such signs or symptomsare present, serious consideration must be givento performing the surgical procedure under localanesthesia or after an effective course of radiationor chemotherapy to reduce the size of the medi-astinal mass. Fiberoptic intubation with the patientappropriately sedated, but breathing spontaneously,also may reveal the presence of functional airwayobstruction thatmight not be appreciated by routinechest X-ray or computerized tomography.Current chemotherapy for Hodgkin lymphoma
includes several agents with anesthetic impli-cation including bleomycin (pulmonary fibro-sis, respiratory failure possibly associated withhigh inspired concentrations of oxygen), doxoru-bicin (myocardial dysfunction), and prednisone(suppression of the pituitary–adrenal axis).Chronic effusions or pericarditis can present
months to years after radiation therapy, especiallyafter mantle irradiation for Hodgkin disease, lym-phoma, or other thoracic neoplasms. Typically,patients have received 4500 rads or more. The like-lihood of pericardial injury varies with total doseof radiation administered, as well as the amount ofheart included in the radiation portal. If the primary

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 301 — #13
Pericardial Disease 301
radiation-induced lesion is symptomatic pericar-dial constriction, then pericardiectomy should beconsidered. At surgery, the pericardium and adja-cent tissue will be very friable and denselyadherent; bleeding will be a major intraoperativeconsideration.
Prior cardiac surgeryUnlike tamponade frommost other causes, inwhichechocardiography demonstrates the effusion to behomogenous, the collection of blood around theheart may usually be loculated (areas of clottedand unclotted blood). Echocardiographic findingstypical of effusive tamponade such as RA and RVcollapse, Doppler flow variation across the mitraland tricuspid valves with respiration and swingingof the heart within the effusion are not commonlyseen in the postoperative period. Localized compres-sion of each of the cardiac chambers, as well as ofthe pulmonary outflow tract has been reported. Pul-sus paradoxus may not be seen due to the presenceof hypovolemia. The presence of hemodynamiccompromise (hypotension, low urine output, lowcardiac output) in combination with the echocar-diographic finding of a pericardial separation widthof >10mm has been shown to have 100%sensitivity for detection of postoperative cardiactamponade.Postoperative constrictive pericarditis is the most
common cause of constrictive pericarditis requir-ing pericardiectomy, with an overall incidence of0.2–0.3%of all patients undergoing cardiac surgery.Constrictive physiologymay present in the immedi-ate postoperative period or, more typically, monthsto years later. Povidone-iodine irrigation around theheart may be one etiologic factor in postoperativeconstrictive pericarditis.Pericardial closure at the time of the original
procedure decreases the incidence of periopera-tive cardiac tamponade from blood pooling, as wellas subsequent constrictive pericarditis that resultsfrom organized hematoma around the posterioraspect of the heart. Closure of the pericardiumgreatly facilitates re-exploration during subsequentcardiac surgery by preventing the right ventricleand anteriorly placed grafts from becoming denselyadherent to the anterior chest wall. This not only
reduces the amount of bleeding during subsequentsurgery but also makes catastrophic entry into car-diac chambers in re-exploration much less likelyto occur. However, the pericardium is not closedroutinely at the end of cardiac surgery by all sur-geons for a number of reasons. For patients withdilated ventricles or those who have developedmyocardial edema while supported by cardiopul-monary bypass (CPB), closure of the pericardiummay restrict ventricular diastolic filling enough tobe hemodynamically significant, especially if pre-existing left ventricular compliance is low (as withaortic stenosis). Furthermore, some surgeons areconcerned that pericardial closure may kink or oth-erwise mechanically distort anterior or lateral coro-nary grafts, compromising both short-termflow andlong-term patency.
Surgery for constrictive pericarditisPatients with constrictive pericarditis do not presentemergently for pericardiectomy. A thorough reviewof the cardiac catheterization data, echocardio-graphic examination and other data by the anes-thesiologist before the induction of anesthesia ismandatory. Patients undergoing pericardiectomyfor constrictive disease present a spectrum ofanesthetic challenges different from the patientwith pericardial tamponade. Unlike anesthetizing apatient with a pericardial effusion, duringwhich themost difficult aspects of the anesthetic occur beforeinduction and during the early part of an other-wise brief procedure, pericardiectomy for constric-tive disease requires ongoing vigilance and oftenendurance during a long and difficult surgery.Pericardiectomy for constrictive disease usually
involves extensive dissection of tissue which isadherent to thin-walled cardiac chambers, the greatvessels, coronary arteries, or aortocoronary saphe-nous vein grafts. Perioperative mortality can beas high as 10%, with hemorrhage being a signif-icant or primary cause of death. Massive hemor-rhage can occur from inadvertent entry into cardiacchambers, or the patient can bleed more slowly,but continuously, from raw dissected surfaces. Itis imperative that venous access be adequate toguarantee timely volume, blood, and coagulationfactor replacement, as needed. Usually, patients

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 302 — #14
302 Chapter 8
undergoing pericardiectomy for constrictive diseaseare explored through a median sternotomy. Manywill have undergone prior cardiac surgery, andalthough pump oxygenator standby is common,CPB is required in only 10% of such patients. Theprimary reason for avoiding CPB for constrictivepericardiectomy is the need for systemic anticoag-ulation and excessive. In patients with constrictionsecondary to prior cardiac surgery, dense adhesionsaround the heart may incorporate epicardial saphe-nous vein or internal mammary coronary grafts,and damage during pericardiectomy, with eitherbleeding or myocardial ischemia, can result.Although some surgeons will approach the heart
through a left lateral thoracotomy and removepericardium from the LV only, most will use amedian sternotomy and resect as much pericardiumas is possible. Pericardial resection usually willextend over the entire anterior surface, exclu-sive of pericardium that overlies coronary arterygrafts, laterally to the phrenic nerves, and inferi-orly to the diaphragmatic surface. When CPB isnot used, the anesthesiologist must expect frequentmechanically-induced dysrhythmias, and thereforehave the capability of electrical cardioversion anddefibrillation. In addition, frequent manipulationand displacement of the heart during the dissectionwill cause wide swings in stroke volume and bloodpressure. If the extent of the dissection or the poten-tial complications of reentering the chest of a patientwho has undergone prior cardiac surgery requiresthe institution of CPB, then the anesthesiologistmust be prepared to deal with ongoing hemor-rhage, with surgical hemostasis difficult to achieve.Adequate reserves of red cells, as well as plateletsand other blood products, must be immediatelyavailable.
Anesthetic technique for constrictivepericarditisTable 8.4 outlines the goals for anestheticmanagement in constrictive pericarditis.
PremedicationThe principle determinant of preoperative sedationwill be the patient’s underlying medical condition.For example, a young, otherwise healthy patient
Table 8.4 Anesthetic goals in constrictive pericarditis.
• Maintain adequate central venous volume• Avoid bradycardia. Diastolic filling is limited by theconstricting pericardium, and slow heart rates will resultin low cardiac output• Establish generous venous access. Prolonged, continuousbleeding is common and a major cause of mortality• Aggressively treat platelet, red cell, and clotting factordepletion• Positive-pressure ventilation is not detrimental; changesin intrathoracic compliance are poorly transmittedthrough a stiff, adherent pericardium• Be prepared for a long, tedious surgery• Transesophageal echocardiography (TEE) is indicated asthere is expected hemodynamic instability and volumeswings
with constrictive pericarditis secondary to mantleirradiation for Hodgkin disease years earlier can bepremedicated as for any other major operation. Thepremedication of a patient with severe rheuma-toid arthritis undergoing pericardiectomy for con-strictive disease who also has an unstable cervicalspine will be determined primarily by the needfor sedation and topical anesthesia for an awakeintubation. If the patient is undergoing pericardiec-tomy secondary to prior cardiac surgery, premedi-cationwill be determined primarily by the adequacyof myocardial revascularization and the presenceof residual angina or ischemia. If the patient hasresidual myocardial ischemia, then premedicationconsiderations are similar to those for primaryrevascularization.Except when myocardial ischemia is likely, rel-
ative tachycardia need not be avoided. Increasedheart rate maintains cardiac output compensatingfor the restriction in diastolic filling.
PreinductionPatients are prepared as for coronary artery bypassgraft (CABG) or valve surgery. Adequate IVaccess, including central venous access, is essential.A pulmonary artery catheter with thermodilutioncapability may be indicated, independent of theetiology of the constrictive disease. The ability to

Alice Nelson Dinardo: “ch08” — 2007/7/16 — 12:40 — page 303 — #15
Pericardial Disease 303
measure cardiac output, as well as right- and left-sided filling pressures, is often useful, even thoughmyocardial contractility will be normal in manypatients with constrictive pericarditis.
Induction and maintenanceMyocardial performance is abnormal in constric-tive pericarditis. There is diastolic dysfunction withabnormal filling resulting in either compensatedor uncompensated heart failure. Anesthetic agentsmay further compromise these patients. The induc-tion of anesthesia depends on the etiology of thepatient’s constrictive pericarditis and the anticipatedduration of surgery. Inductionmay be similar to thatused for coronary artery bypass surgery, if the dura-tion of surgery is expected to be lengthy and signif-icant residual ventricular dysfunction is anticipatedin the immediate postoperative period. This wouldinclude a combination of fentanyl 10–25µg/kgor sufentanil 1–3µg/kg, together with a benzodi-azepine and inhalational agent. If the etiology ofconstrictive pericarditis is secondary to prior coro-nary revascularization, then a significant potentialfor perioperative myocardial ischemia exists, andongoing vigilance for myocardial ischemia must bemaintained throughout the anesthetic. Sternotomy,dissection, and removal of the pericardium caninjure entrapped coronary bypass grafts as well asa grafted internal mammary artery.Unlike the patient with a pericardial effusion,
changes in intrathoracic pressure are not transmit-ted to the heart through the thickened pericardiumin constrictive disease. This eliminates the need
to avoid positive pressure ventilation and makesinduction and maintenance quite similar to that forcoronary revascularization. The primary differencebetween surgery for revascularization and constric-tive pericarditis is that the latter is of shorter dura-tion,with a greater risk of severe hemorrhage.Manyof these patients will require inotropic support dur-ing surgery and for a period of time after surgery.The patient with constrictive pericarditis may takeas long as a month to regain normal hemodynamicsand ventricular function.
Suggested reading
Asher CR, Klein AL. Diastolic heart failure: restrictive
cardiomyopathy, constrictive pericarditis, and cardiac
tamponade: clinical and echocardiographic evaluation.
Cardiol Rev 2002;10:218–29.Demangone D. ECG manifestations: noncoronary heart
disease. Emerg Med Clin North Am 2006;24:113–31.Goldstein JA. Cardiac tamponade, constrictive pericardi-
tis, and restrictive cardiomyopathy. Curr Probl Cardiol
2004;29:503–67.Maisch B, Seferovic PM, Ristic AD et al. Task Force on the
Diagnosis and Management of Pericardial Diseases of
the European Society of Cardiology. Guidelines on the
diagnosis and management of pericardial diseases exec-
utive summary; the Task Force on the Diagnosis and
Management of Pericardial Diseases of the European
Society of Cardiology. Eur Heart J 2004;25:587–610.Spodick DH. Acute cardiac tamponade. N Engl J Med
2003;349:684–90.Troughton RW, Asher CR, Klein AL. Pericarditis. Lancet
2004;363:717–27.

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 304 — #1
CHAPTER 9
Anesthesia for Surgery ofthe Thoracic Aorta
Thoracic aorta lesions are among the most clinicallychallenging and acutely life-threatening lesionsencountered by the cardiac anesthesiologist. Theperioperative mortality ranges from 10 to 35%.Morbidity, including myocardial infarction (12%),respiratory failure (25%), stroke (3%), and renalfailure (9%), remains significant despite aggres-sive intensive care interventions. The majority ofthese patients are older and approximately 30%have coexisting pulmonary, vascular, renal, andcoronary artery disease placing them at the veryhighest risk. Despite these significant risks, in manypatients operative care remains the best optionfor long-term survival. For example, the 2-yearsurvival in patients with untreated thoracic orthoracoabdominal aortic aneurysm is 25%,whereasthe expected 2-year survival after surgery isapproximately 70%.Aortic disease may present at any age, including
the newborn. In younger patients, aortic diseaseusually presents secondary to congenital defects,Marfan disease (aneurysms), bicuspid aortic valvedisease with aneurysm formation, and aortic trans-action after blunt chest trauma. In older patients,the disease is associated with atheroscleroticperipheral vascular disease, hypertension, diabetesmellitus, and tobacco abuse.All patients presenting for aortic surgery require
an extensive evaluation by the anesthesiologist. Insome cases, the surgery is urgent in nature (aortictransection and aortic dissection) and the evaluationis necessarily limited. Nevertheless, a brief reviewof all available laboratories, cardiac studies, and
radiographic studies is crucial. This information willallow the anesthesia team to quickly assess riskand plan for the operative procedure. Managementof preoperative medications, institution of beta-blocker therapy (if indicated), placement of invasivemonitoring devices, and surgical strategies can all bedetermined in the preoperative period. Assemblingan appropriate operative team, including perfusion-ists, nursing staff, and blood bank personnel, isrequired before any aortic procedure. The operativeteam must communicate closely before the surgerybegins because line placement, drug selection, andblood banking preparation all depend on the extentof the proposed surgery. In any aortic procedure,the anesthesiology teammust prepare for blood sal-vage techniques and be ready for potential massivetransfusion of blood and blood products.There are multiple approaches to the repair
of aortic lesions that will affect the conduct ofanesthesia. For example, the repair of a type Aaortic dissection may require deep hypothermic cir-culatory arrest (DHCA) with retrograde cerebralcardioplegia. A descending aortic aneurysm repairmay employ left heart bypass with monitoring anddrainage of lumbar cerebral spinal fluid. This inter-play between surgery and anesthesia places aorticsurgery among the most challenging in cardiacanesthesiologist’s domain.
Classification of aortic lesions
Aortic lesions may be classified into three patho-physiologic subtypes: aortic dissection, aortic
304

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 305 — #2
Anesthesia for Surgery of the Thoracic Aorta 305
aneurysm, and aortic transection. Aortic tran-section and acute aortic dissections are surgicalemergencies requiring immediate intervention.Aortic aneurysms and chronic aortic dissectionsoften are repaired electively.
Aortic dissectionAcute aortic syndromes include aortic dissection,intramural hematoma, and symptomatic aorticulcer. Aortic dissection is defined as a separationof the layers of the aortic wall with variable prox-imal and distal extension. In 90% of the cases, anintimal tear is identified, whereas in the remain-der, no intimal tear is observed (Fig. 9.1a,b). In theabsence of an intimal tear, it is thought that there is
(a)
(b)
Fig. 9.1 (a) Transverse section of the descending aortashowing the dissection flap and a point of connectionbetween the true and false lumen (by color flow). (b) Thisis the same patient demonstrating a transesophagealechocardiography (TEE) long-axis view of the descendingaorta. The dissection flap is clearly seen as the point ofcommunication between the true and false lumen.
a rupture of the vasa vasorumwith bleeding into thearterial media creating an intramural hematoma.The incidence of aortic dissection ranges from 5–30cases per million people per year. Pain is the mostcommon presenting symptom; however, there maybe a wide range of presentations secondary to dis-tal organ system involvement. The dissection flapmay propagate antegrade and/or retrograde involv-ing any side branch of the aorta. There may resultmalperfusion syndromes, tamponade, and aorticvalve regurgitation.A high clinical index of suspicion is required in
order to make a timely diagnosis. Prompt evalu-ations with computed tomography (CT) scanning,magnetic resonance imaging (MRI), and/or trans-esophageal echocardiography (TEE) are all highlysensitive and specific modalities to diagnose aor-tic dissection. Risk factors for aortic dissectioninclude hypertension, aortic medial disease, Marfansyndrome, congenital bicuspid aortic valve, aorticatherosclerosis, and blunt chest trauma. Approxi-mately 70% of patients with aortic dissections havea history of hypertension. Cocaine abuse may be acausative factor in some otherwise healthy individ-uals. Frequently, the acute event precipitating thedissection is never determined. Iatrogenic injuriesfrom surgical manipulation of the aorta and place-ment of diagnostic or therapeutic devices into theaorta may result in acute dissection. The ratio ofmales to females with aortic dissection is approxi-mately 3:1, and the peak incidence is in the 5–7thdecades of life. A dissection less than 14-days-old isdefined as acute, and a dissection older than 2weeksis defined as chronic. Approximately 33% of allthoracic aneurysms will present as an acute dissec-tion. Anatomically, 60% of dissections involve theascending aorta, 20% involve the transverse arch,and 20% involve the descending aorta.Aortic dissections are described according to
either the DeBakey or Stanford classification(Fig. 9.2). DeBakey classified dissections on theinitial site of injury and the location of aortic exten-sion. In type I and II dissections, the inciting lesionoccurs in the ascending aorta. Type I lesions extendinto the descending aorta, whereas type II lesionsare limited to the ascending aorta. Both of thesedissectionsmay render the aortic valve incompetent

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 306 — #3
306 Chapter 9
DeBakeyType I Originates in the ascending aorta, propagates at least to the aortic arch and often beyond it distallyType II Originates in and is confined to the ascending aortaType III Originates in the descending aorta and extends distally down the aorta or, rarely, retrograde into the aortic arch and ascending aortaStanfordType A All dissections involving the ascending aorta, regardless of the site of originType B All dissections not involving the ascending aorta
Stanford
DeBakey Type I Type II Type III
Type A Type B
Fig. 9.2 The DeBakey and Stanford classificationsystems for aortic dissections. (From Nienaber CA,Eagle KA. Aortic dissection: new frontiers in diagnosisand management. Part 1: From etiology to diagnosticstrategies. Circulation 2003;108:628–35, with permission.)
due to retrograde involvement and deformation ofthe aortic valve annulus. In a type III dissection,the intimal tear is in the descending aorta. Type IIIlesions are further subdivided into subtype A, whichhas a retrograde extension into the proximal aorticarch, and subtype B, which has antegrade extensioninto the descending aorta. In the Stanford classifica-tion, type A dissections are those with any involve-ment of the ascending aorta, and type B dissectionsinvolve only the descending aorta distal to the leftsubclavian artery. Younger patientswith underlyingconnective tissue abnormalities are prone to type Adissections; older patients will commonly presentwith a type B dissection.Management of these patients depends on the
location of the lesion and extent of the dissection.Medical management involves controlling bloodpressure andmyocardial contractility. This often is atemporizing measure until the patient can undergosurgical repair. Patients with a Stanford A lesionwho undergo surgical repair have a significantly
lower hospital mortality rate than patients who aremanaged medically. In comparison, patients witha Stanford B lesion do not have a significant dif-ference in mortality with either medical or surgicalmanagement (Fig. 9.3). The overall in-hospitalmor-tality is approximately 30% for proximal dissectionsand 10% for patients with distal dissections. Thepredictors of in-hospital mortality include proxi-mal dissection, age >65 years, shock, pulse, andneurologic deficits.
Aortic transectionRupture of the aorta often results from nonpene-trating chest injuries sustained in trauma. Althoughprompt diagnosis and treatment are crucial for sur-vival, this lesion may remain clinically silent andthus untreated. Anatomically, the heart and distalaorta are mobile components, whereas the aorticarch is fixed by the great vessels. During the deceler-ation phase of an acceleration–deceleration injury,the arch motion slows with the body while theremaining heart and aortic components continue inmotion. This energy creates a shearing force on theaorta leading to injury. Up to 95% of aortic injurieswill occur at the isthmus where the aorta is teth-ered by the ligamentum arteriosum. Additional sitesof injury include the aortic hiatus in the diagram,mid-thoracic descending aorta, and origin of theleft subclavian artery. Multiple sites of aortic injuryoccur in up to 20% of patients (Fig. 9.4a–d).An estimated 10–15% of fatal automobile acci-
dent victims suffer aortic rupture. Eighty-to-ninetypercent of these patients die at the scene. Amongthe 10–20% surviving 1hour after the injury, anadditional 30% die within 6hours, 49% within24hours, and 72% within 8 days. Should thepatient make it to surgery, the mortality rate forrepair of this lesion is approximately 20%.
Aortic aneurysmAneurysms are classified by their etiology, loca-tion, and shape. Aortic pathology predisposinganeurysm includes atherosclerosis, cystic medialnecrosis, syphilitic aortitis, trauma, postoperativefalse aneurysms, connective tissue disorders and

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 307 — #4
Anesthesia for Surgery of the Thoracic Aorta 307
Fig. 9.3 Fourteen-day mortality in 645patients from the The InternationalRegistry of Acute Aortic Dissection(IRAD) stratified by medical (Med) orsurgical (Surg) management for eithertype A or B dissection. (Modified fromHagan PG, Nienaber CA, Isselbacher EM,et al. The International Registry of AcuteAortic Dissection (IRAD) – new insightsinto old disease. JAMA2000;283:897–903, with permission.)
60
50
40
30
Cum
ulat
ive
mor
talit
y, (
%)
20
10
0<24hours
1 2 3 4 5
Days following presentation
6 7 8 9 10 11 12 13 14
All patients (n = 645)A/Med (n = 98)A/Surg (n = 320)B/Med (n =188)B/Surg (n = 41)
(a) (b)
(c) (d)
Fig. 9.4 Angiographic studies from four patients with aortic transection following motor vehicle accidents. The defectcan have a number of anatomic locations and presentations. (a) Transection in the descending aorta. (b) Transection inthe innominate artery. (c) Fusiform transection of the descending aorta. (d) Transection at the ligamentum arteriosum.

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 308 — #5
308 Chapter 9
(a) (b)
Fig. 9.5 Types of thoracic aortic aneurysms.(a) Fusiform. (b) Saccular. (From Magilligan DJ Jr,Ullyot DJ. The heart. I. Acquired diseases. In:Way LW (ed). Current Surgical Diagnosis and Treatment.Norwalk, CT: Appleton & Lange, 1991:359, withpermission.)
congenital aortic anomalies. Aneurysms with con-current dissection are more common to the ascend-ing aorta, whereas atherosclerotic aneurysms areprimarily localized to the descending aorta. TheDeBakey and Stanford classifications, which werediscussed under aortic dissections, are commonlyused to describe the location and extent of thislesion. Aneurysms are described morphologicallyas fusiform or saccular (Fig. 9.5a,b). Fusiformaneurysms have a higher operative mortality thansaccular aneurysms. The male to female ratio isapproximately 2:1, although women have a higherincidence of aneurysm rupture. This disorder tendsto affect older patients with the mean age fordiagnosis is in the sixth decade of life. A psue-doaneurysm occurs when there is a well-definedcollection of blood and thrombus outside of thevessel wall. Exsanguination in a psuedoaneurysmis prevented by the surrounding connective tissue.This defect is sometimes referred to as a containedrupture or false aneurysm.Larger aortic aneurysms, expanding aneurysms,
and symptomatic aneurysms require surgical inter-vention. Patients with an aortic diameter >55mmand without surgical intervention have a 2-yearsurvival rate of <25%. The operative mortality forrepair is 20–34% for acute dissections and 8–22%for chronic dissections. These patients have a highincidence of coexisting pulmonary, cardiac, and
vascular disease complicating their intraoperativeand postoperative care.
Diagnosis of aortic lesions
Aortic lesions often present with a constellationof symptoms suggesting the ongoing events. Thesesymptoms are a result of expansion, dissection, orrupture of the aorta (Table 9.1). Severe anteriorchest or back pain is the most common present-ing symptom. Pain may occur directly from aorticexpansion or from involvement of nearby struc-tures. Pain may extend into the neck, shoulders, orabdomen. The intensity of pain may not correlatewith the size of the lesion. Up to a half of patientswith aortic lesions will be asymptomatic. Possibleexplanations for the lack of symptomsmight includedistracting injuries in the patient with trauma, achronic disease process or other masking coexistingdisease processes (i.e. cardiac ischemia). Any patientwith a suspected aortic lesion requires immediateevaluation and diagnosis.Chest radiography is a rapid and easily accessi-
ble method for diagnosing aortic lesions (Fig. 9.6).Table 9.2 lists eight classic radiographic signs con-sistent with aortic injury. Loss of the aortic knobcontour is the most consistent finding on chestradiograph for patients with aortic injury. However,radiograph under penetration or venous mediasti-nal bleeding may cause false-positive studies. Thenext most common finding is superior mediastinalwidening. Radiographs are assessed for the ratio ofmediastinal to chest width (M/C). An M/C ratio of>0.25 is consistent with an aortic injury.More sophisticated imaging techniques such as
angiography, CT, MRI, aortography, transthoracicechocardiography (TTE), and TEE provide supe-rior specificity and sensitivity of diagnosis overchest radiographs. Historically, aortography hasbeen considered the “gold standard” in assessinglesions of the aorta. However, this modality iscostly, invasive, and time consuming. Addition-ally, aortography subjects patients to potentiallynephrotoxic contrast agents. Although aortographyremains the superior diagnostic modality for coro-nary artery anatomy evaluation and branch vesselinvolvement, numerous studies have evaluated

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 309 — #6
Anesthesia for Surgery of the Thoracic Aorta 309
Table 9.1 Presenting signs and potential etiologies for patients with thoracic aortic lesions. The frequency of thesefindings, as calculated from previous studies is indicated when obtainable.
Symptoms/clinicalfinding
Possible etiology Frequency(%)
Chest or back pain Active aortic dissection >50
No clinical findings Distracting injuries, chronic dissection 5–50
Angina Aortic dissection into coronary arteries 5.8
Acute myocardial infarction Aortic dissection into coronary arteries/thrombus
Aortic regurgitation Aortic valve injury/ascending arch injury 10–50
Assymetric upper extremity pulseamplitude
Arch interruption 9–45
Hypertension of the upperextremities
Distal aortic occlusion/rupture 37
Distant heart sounds Pericardial tamponade/pericardial effusion
Hypotension Hypovolemia/aortic dissection
Pulmonary edema Lung contusion/myocardial contusion/acute aorticinsufficiency
Hemothorax Traumatic injury/descending thoracic injury 3
Respiratory difficulty Bronchial or tracheal compression/atelectasis/pneumonitis/acute aortic insufficiency withpulmonary edema rib fractures
8
Pneumothorax
Confusion Hypotension/acute head injury
Horner syndrome
Paraplegia Spinal cord ischemia/trauma 2.3–2.6
Hemoptysis Erosion of bronchus/pulmonary contusion trauma
External chest wall abnormalities 35
Jaw pain Referred secondary dissection 8.8
Hoarseness Stretching/compression of laryngeal nerve 8.6
Dysphasia Esophageal compression or erosion 5
Hematemasis Esophageal compression of erosion 5
Melena Direct intestinal injury/intestinal infarction
Anuria or hematuria Renal injury/renal infarction/hypovolemia 2–3
diagnostic alternatives with promising results(Table 9.3). Several series have shown MRI to be100% sensitive and specific in diagnosing aorticlesions. Furthermore, MRI or CT in combinationwith TTE has equivalent sensitivity and specificity toaortography for evaluating such lesions. The limited
ability of CT and MRI to evaluate the aortic valve iswell supplemented by adding echocardiography.TEE provides excellent resolution of intrathoracic
structures in a rapid, relatively noninvasive fash-ion. For patients with a suspected thoracic aorticlesion, intraoperative TEE can make or confirm

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 310 — #7
310 Chapter 9
Fig. 9.6 Posteroanterior roentgenogram of a patientpresenting with a chronic transverse arch aorticaneurysm. Note the aneurysm at the aortic knob, thedeviation of the trachea and elevation of the lefthemidiaphragm. At surgery, the left phrenic nerve wasstretched and splayed by the aneurysm. (FromCommarata BJ. Anesthesia for surgery of the thoracicaorta. In: DiNardo JA (ed). Anesthesia for Cardiac Surgery,2nd edn. Stamford, CT: Appleton & Lange, 1998:259–76,with permission.)
Table 9.2 Chest radiograph findings in thoracic aorticlesions.
Loss of aortic contourMediastinal wideningDisplacement of the right paraspinous interfaceDeviation of the trachea to the rightDisplacement of the nasogastric tube to the rightLeft hemothoraxDepression of the left mainstem bronchus below 40 fromhorizontalLeft apical cap
the diagnosis, locate dissection sites, identify thetrue and false lumen, evaluate the surgical repair,and assess the adequacy of perfusion during car-diopulmonary bypass (CPB) (Fig. 9.7a,b). In com-parison with aortography, TEE provides a highersensitivity,
Table 9.3 Sensitivities, specificities, and predictivevalues of imaging techniques for the diagnosis of thoracicaortic dissection.
Technique Sensitivity(%)
Specificity(%)
PPV(%)
NPV(%)
Angiography 77–88 94–100 95–100 71–84CT 80–83 88–100 83–100 71–88MRI 100 100 100 100TEE 97–99 98–100 98–100 96–99
CT, computed tomography; MRI, magnetic resonance imag-ing; NPV, negative predictive value; PPV, positive predictivevalue; TEE, transesophageal echocardiography.
(a)
(b)
FL
TL
Fig. 9.7 (a) M-mode transesophageal echocardiography(TEE) of a dissection. The true and false lumen areclearly demonstrated. The true lumen will expandduring systole. FL, false lumen; TL, true lumen.(b) Pseudoaneurysm of the aortic root. The defect alongthe noncoronary cusp is clearly seen with color Doppler.
significantly shorter examination time and thrombusidentification. TEE is indicated intraoperatively toassess myocardial performance, signs of ischemia,heart valve status, and post-repair aortic integrity.For patientswith trauma, TEE is highly sensitive andspecific for evaluation of aortic injuries.

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 311 — #8
Anesthesia for Surgery of the Thoracic Aorta 311
TEE has several limitations. Lesions of the dis-tal ascending aorta are difficult or impossible tovisualize with TEE secondary to interference of thetrachea and left main stem bronchus. Examina-tion of the subdiaphragmatic descending aorta islimited. Ultrasonic artifacts sometimes are confusedwith intimal tears and lead to an incorrect diagnosis.Despite these limitations, TEE is a widely used peri-operative and intraoperative diagnostic modality forevaluating patients with aortic injuries.
Airway compression fromaortic lesions
The aortic arch saddles the left main-stem bronchusas the vessel makes the transition from ascending totransverse to descending aorta (Fig. 9.8). Ultimately,the descending aorta assumes its location along theposterior wall of the bronchus. A thoracic aortic
Right commoncarotid artery
Rightsubclavian
artery
TracheaLeft commoncarotid artery
Esophagus
Brachiocephalictrunk
Rightprimary
bronchus
Right upperlobe bronchus
Left subclavianartery
Aortic arch
Ligamentumarteriosum
Trachealbifurcation
Left primarybronchus
Thoracic aorta
Esophagus,thoracic part
Fig. 9.8 The anatomic relationship of the esophagus,great vessels and the trachea. (Adapted fromClemente CD. Anatomy: A Regional Atlas of the HumanBody, 2nd edn. Baltimore/Munich: Urban &Schwarzenberg, 1981:181, with permission.)
lesion can impinge upon and damage the tracheaor main-stem bronchus, leading to tracheomala-cia and respiratory distress (Fig. 9.9a,b) Thoracicaortic lesions usually cause compression or devia-tion of the left main-stem bronchus; however, theright main-stem bronchus and trachea also may becompromised.Symptoms of airway compression may be exac-
erbated by changes in body position. A preoper-ative history and examination revealing stridor,wheezing, cough, or tracheal deviation should raisesuspicion of aortic impingement and possible tra-cheomalacia. Unilateral vocal cord paralysis, whichresults from compression of the recurrent laryn-geal nerve between the aorta and trachea, maypresent clinically as voice hoarseness. Preopera-tive pulmonary function testing with flow–volumeloop analysis will reveal an intrathoracic obstruc-tive process in severe cases. Radiographic studiesmay be useful in delineating the extent of airwaycompromise caused by aortic lesions.
Surgical approach andmanagement
Patients with a suspected aortic dissection requireimmediate diagnosis, invasive monitoring, andtreatment. Medical management focuses on painand blood pressure control to reduce disease exten-sion. Narcotics are effective for pain control, anda wide variety of vasoactive agents includingbeta-blocking agents, sodium nitroprusside, andangiotensin-converting enzyme (ACE) inhibitorscan be used for blood pressure control. The ther-apeutic goal is to reduce the shear forces alongthe dissection flap. Patients with hemodynamicinstability or significant comorbidity (i.e. pericar-dial tamponade, acute aortic regurgitation, shock)often require emergent intubation and preparationfor surgery.
VentilationThe location of the aortic lesion will dictate the sur-gical approach necessary for repair. Ascending andtransverse aortic arch lesions are repaired througha median sternotomy without the requirement forone-lung ventilation (OLV). These patients can be

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 312 — #9
312 Chapter 9
(a) (b)
Fig. 9.9 (a) The trachea is markedly deviated secondaryto an aortic aneurysm. (b) The trachea and left mainstembronchus may be compressed from an aortic aneurysm.Left-sided double lumen endotracheal tubes may bedifficult to place in these patients. (From Hunt D,Schwab F. Chest trauma. In: Rosen P, Doris P, Barkin Ret al. (eds). Diagnostic Radiology in Emergency Medicine.
St. Louis: Mosby Year Book, 1992:77–100 andSmith MS, Grichnik KP. Anesthetic considerations forlung transplantation and thoracic aortic surgery. In:Miller RD, Reves JG (eds). Atlas of Anesthesia, Vol. VIII:Cardiothoracic Anesthesia. Philadelphia: CurrentMedicine (Churchill Livingstone), 1999:6.1–18, withpermission.)
managed with a single lumen endotracheal tube.Lesions of the distal transverse arch and descendingaorta are repaired through a left thoracotomy. Sur-gical exposure is enhanced and trauma to the leftlung is minimized by providing OLV with the leftlung collapsed. Caution is indicated as the aneurysmmay impinge on the trachea or bronchus resulting intube malposition, airway damage, or aortic rupture.
Aortic cross-clampingAortic cross-clamping at some level is required forrepair of all thoracic aortic lesions. The placementof the aortic cross-clamps for repair of various aorticlesions is summarized in Fig. 9.10(a–f). Aortic cross-clamping creates potential for end-organ ischemia.The organs at risk vary with the position of thecross-clamps.Spinal cord ischemia is a potential consequence of
aortic cross-clamping. Anatomically, the blood sup-ply to the spinal cord is derived from several sources.A single anterior spinal artery arises from the ver-tebral arteries at the level of the foramen magnumand supplies the anterior two-thirds of the spinalcord. A pair of posterior spinal arteries arises fromthe posterior inferior cerebellar arteries and supplies
the remainder of the cord. The vertebral, deep cervi-cal, intercostal, and lumbar arteries also contributeto spinal cord perfusion as the anterior and posteriorradicular arteries (Fig. 9.11). The largest radicularartery is the arteria radicularis magna or artery ofAdamkiewicz, which supplies the majority of bloodto the lower two-thirds of the spinal cord. The originof this vessel is localized to T9–T12 in over 60% ofpatients. Therefore, in contrast to the upper spinalcord, the lower cord has a relatively limited bloodsupply with fewer collateral vessels and is at risk forischemia during aortic cross-clamping or hypoten-sive periods. Ligation of intercostals arteries at thetime of surgery is controversial. Ligation of lowerintercostal arteries is associated with a greater therisk of neurologic deficit (Fig. 9.12).Spinal cord perfusion pressure (SCPP) is the dif-
ference between mean arterial pressure (MAP) andthe cerebrospinal fluid (CSF) pressure. Efforts toimprove perfusion necessitate either an increase inMAP or a reduction in CSF pressure. Lumbar drainsreduce CSF volume and pressure thereby augment-ing SCPP (Fig. 9.13a,b). The literature is contradic-tory on the benefit of CSF fluid drainage in patients;however, many institutions routinely employ this

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 313 — #10
Anesthesia for Surgery of the Thoracic Aorta 313
Descending aorta Descending aorta
Left thoracotomy Left thoracotomy
GOTT shunt
Coronary circulation
Perfused by heartO2 by lung
Descending aorta
Left thoracotomy
Perfused by heartO2 by lung
Ascending aorta
Cardioplegia Cardioplegia
RA Femoral vein RA Femoral vein
Median sternotomy
Aortic
Median sternotomyDHCA ± retrograde
cerebral perfusion ordirect vessel cannulation
Perfused by circuitO2 by circuit
Descending aorta
Left thoracotomy
Perfused by heartO2 by lungs
Perfused by heartO2 by lung
Coronary circulationPerfusion and O2by collaterals
Coronary circulation Coronary circulation
LA LV LA PA Femoral vein
Centrifugalpump
Reservoir,oxygenator, pump
Reservoir,oxygenator, pump
Perfused by pumpO2 by lungs
Perfused by shuntO2 by lungs
Perfused by circuitO2 by circuit
Perfused by circuitO2 by circuit
(a) (b)
(c) (d)
(e) (f)
Reservoir,oxygenator, pump
Fig. 9.10 Location of aortic cross clamp (—), surgical approach, and circulatory adjuncts for repair of aortic lesions.(a–d) Descending aorta. (e) Ascending aorta. (f) Aortic arch. (From Commarata BJ. Anesthesia for surgery of thethoracic aorta. In: DiNardo JA (ed). Anesthesia for Cardiac Surgery, 2nd edn. Stamford, CT: Appleton & Lange,1998:259–76, with permission.)

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 314 — #11
314 Chapter 9
Vertebral artery
AscendingcerviclearterySubclavian
artery
Basilar artery
Anterior spinal artery
Radicular arteries,C3–C4Radicular arteries,C5–C6
Radicular arteries,C7–C8
Radicular arteries,T3–T4
Posterior spinalartery
Radicular artery ofAdamkiewicz,T11–T12
Lumbar-sacralradicular arteries
Fig. 9.11 Blood supply of the spinal cord. (FromSmith MS, Grichnik KP. Anesthetic considerations forlung transplantation and thoracic aortic surgery. In:Miller RD, Reves JG (eds). Atlas of Anesthesia, Vol. VIII:Cardiothoracic Anesthesia. Philadelphia: Current Medicine(Churchill Livingstone), 1999:6.1–18, with permission.)
modality with good result. There are numerous casereports of patients with new onset paraplegia aftersurgery with resolution of symptoms after CSF fluiddrainage.Some centers employ selective cooling of the
spinal cord via lavage of the subarachnoid space.Corticosteroids, thiopental, N-methyl-D-aspartatereceptor antagonists, papaverine, and magnesiumalso have undergone studies evaluating their pro-tective effects on the spinal cord. Although manyagents have shown success in the laboratory, clinicalefficacy is difficult to establish. The single best inter-vention to reduce spinal cord injury is limiting theaortic cross-clamp time to an absolute minimum.Among the most common perioperative injuries
associated with repair of thoracic aorta lesions is
100
80
60
Per
cent
40
20
0
LigatedOccludedReattached
7 8 9Intercostal artery
10 11 12
Fig. 9.12 Percentage of patients with neurologic deficitby intercostal artery and artery status. The lower toposition of the artery on the spine, the higher the risk ofdeficit with ligation. (From Safi HJ, Miller CC III, Carr Cet al. Importance of intercostal artery reattachmentduring thoracoabdominal aortic aneurysm repair. J VascSurg 1998;27:58–68, with permission.)
postoperative paraplegia. The incidence of para-plegia after thoracic aortic repair ranges from2–40%, depending on the site of the lesion andthe degree of aortic involvement and aortic dis-section. Patients with dissection have at least atwofold greater incidence of postoperative para-plegia when compared with those without dissec-tion. Despite numerous animal and human studies,the precise mechanism of spinal cord injury dur-ing aortic cross-clamping remains uncertain. Con-tributing factors include aortic cross-clamp time,extent of aneurysm, presence of hypotension orshock, urgency of operation, aneurysm with con-current dissection, diabetes, and advanced patientage. The spinal cord will tolerate a limited period ofischemia before irreversible cellular injury occurs(Fig. 9.14). A cross-clamp time of <30minutes isusually safe and carries a minimal risk for post-operative paraplegia. Thirty to sixty minutes ofcross-clamp time leaves patients more vulnerableto injury, whereas times >60minutes approach a90% incidence of paraplegia. Therefore, for repairsexceeding 30minutes, patients may benefit fromextracorporeal circulatory techniques to augmentend-organ perfusion.Somatosensory-evoked potentials (SSEPs) and
motor-evoked potentials (MEPs) can be used to

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 315 — #12
Anesthesia for Surgery of the Thoracic Aorta 315
40
30
20
Mea
n pr
essu
re (
mm
Hg)
10
0
−10−10 0 10
AXCon
AXCoff
Time (min)
20 30 40 50 60 70
40
30
20
Mea
n pr
essu
re (
mm
Hg)
10
0
−10−10 0 10
AXCon
AXCoff
Time (min)
SCPP = 30 mmHg
20 30 40 50 60 70
SCPP = 22 mmHg
(a)
(b)
Fig. 9.13 Spinal cord perfusion pressure (SCPP) (distalaortic pressure, upper line; cerebral spinal fluid pressure,lower line) was lower in the control group of dogs (a)than in the cerebrospinal fluid (CSF) drainage group ofdogs (b). AXC, aortic cross-clamp. (From McCullough JL,Hollier LH, Nugent M. Paraplegia after thoracic aorticocclusion: influence of cerebrospinal fluid drainage.Experimental and early clinical results. J Vasc Surg1988;7:153–60, with permission.)
detect intraoperative spinal cord ischemia. Bothevaluate amplitude and latency of signal transduc-tion as a marker of neuronal integrity (Fig. 9.15).SSEP involves stimulation of upper or lowerextremity peripheral nerves with signal observa-tion at the cervical spine and scalp. The electricalsignal, which is carried by the dorsal columns,assesses the integrity of afferent long tracts withinthe spinal cord. SSEP monitoring also may be help-ful in assessing the adequacy of distal perfusionvia extracorporeal circulation. This type monitor-ing is not routinely employed at all centers. Somedata find no reduction in postoperative neurologicaldeficits associated with the use of SSEP monitoring.
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
Pro
babi
lity
of s
pina
l cor
d in
jury
(par
aple
gia
or p
ares
is)
0.2
0.1
0
Safe Vulnerable Certain
30 60 90Aortic cross-clamp time (min)
Fig. 9.14 Relative risk of ischemic spinal cord injuryrelative to aortic cross-clamp time. (From Svensson LG,Loop FD. Prevention of spinal cord ischemia in surgery.In: Bergan JJ, Yao JST (eds). Arterial Surgery: NewDiagnostic and Operative Techniques. New York: Grune &Stratton, 1988:273–85, with permission.)
Also, the predominantly efferent anterior horn areaseems to be most sensitive to ischemia. SSEP mon-itoring directly assesses the dorsal column but canonly indirectly monitor these motor areas withinthe cord. SSEP monitoring cannot differentiatebetween peripheral and central ischemia causingobserved changes. Motor-evoked potential moni-toring detects the area of interest in the spinal cord,but it is technically difficult outcome data regardingits use is contradictory.Renal insufficiency is common after procedures
of the thoracic aorta with an incidence of approx-imately 10%. Reported risk factors for postopera-tive renal failure include reduced left ventricular(LV) function, need for reoperation, renal ischemictime exceeding 30minutes, postoperative respira-tory insufficiency, preexisting renal dysfunction,urgent or emergency procedures, and large vol-umes of blood loss during the procedure. Ade-quate hydration and renal perfusion pressure areimportant for renal protection. Several therapeuticinterventions to avoid this complication are advo-cated; however, clinical efficacy is uncertain. Mostclinicians agree that intraoperative urine output of0.5–1.0mL/kg/h is considered a measure of ade-quate renal perfusion and function; however, thisassumption may be invalid. Common pharmaco-logic interventions include “renal dose” dopamine

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 316 — #13
316 Chapter 9
P1
Amplitude Amplitude
Latency Latency
N1
Fig. 9.15 Somatosensory evokepotentials (SSEPs) and motor evokedpotentials (MEPs) latency and amplitudedeterminations during aortic surgery.(From Meylaerts SA, Jacobs MJ, vanIterson V et al. Comparison of transcranialmotor evoked potentials andsomatosensory evoked potentials duringthoracoabdominal aortic aneurysm repair.Ann Surg 1999;230:742–9, withpermission.)
(2–4µg/kg/min), fenoldopam, and mannitol. Man-nitol induces an osmotic diuresis and acts as anoxygen-free radical scavenger. There are little datasupporting the use of dopaminergic agonists forrenal protection in this clinical scenario. The anes-thesia team should focus on appropriate hydrationprior to aortic cross-clamping and maintenance ofdistal perfusion pressure. Extracorporeal circulatorytechniques may be beneficial in providing bloodsupply to an otherwise ischemic kidney duringaortic cross-clamping.
Distal aortic arch and descendingthoracic aortic lesionsThese lesions are repaired through a left thoraco-tomywith the aid of OLV. A number of options existin the management of these lesions.
Simple aortic cross-clampingConceptually, the simplest method for repairingdistal aortic arch and descending thoracic aorticlesions involves cross-clamping the aorta and pro-ceeding with the surgical procedure. As shown inFig. 9.10a, the aorta is clamped proximally and dis-tally to the lesion. Coronary and cerebral perfusionare uninterrupted by this arrangement and distalaortic perfusion is either temporarily interrupted oroccurs via collateral vessels. Pulmonary blood flowcontinues normally. This method produces proxi-mal aortic hypertension, which may produce LVafterload mismatch, LV distension, mitral regurgi-tation (MR), and myocardial ischemia. Pharmaco-logic management of LV function during this periodis challenging. Aortic cross-clamp time ideally islimited to <30minutes.
To provide flow to the areas below the distalclamp, several techniques have been developed. Theconcept behind all of them is diversion of bloodfrom the heart for distribution to the distal aorta.This serves two purposes: it provides blood flowto the areas distal to the aortic cross-clamp, and itoffers a nonpharmacologic method to control prox-imal aortic hypertension and LV distension duringthe cross-clamp period. The available methods aredescribed below.
Passive shuntingThe work of Gott and colleagues developed the tri-dodecymethyl ammonium chloride–heparin shuntconsisting of sized, nonthrombogenic plastic tub-ing. The segment of tubing is placed into the aortabetween the proximal clamp and the aortic valve,and the other end of the tubing is placed into theaorta beyond the distal clamp (Fig. 9.10b). Thismethod has several advantages and disadvantages.
Advantages• The shunt provides a method for distal perfusionwithout the need for systemic heparinization.• The shunt is quickly and easily placed.
Disadvantages• Precise control of shunted blood is impossible toregulate.• Other problems include bleeding from the inser-tion sites, accidental dislodgement during the pro-cedure, migration of the proximal end of theshunt across the innominate or left carotid artery,blockage of the surgeon’s field of view, kinking ofthe shunt, embolic stroke, and death.

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 317 — #14
Anesthesia for Surgery of the Thoracic Aorta 317
Left heart bypassLeft heart bypass removes a fraction of oxygenatedblood from either the left atrium or the left ven-tricle for delivery to the distal aorta or femoralartery (Fig. 9.10c). A centrifugal pump is used inthis arrangement. No oxygenator is needed becauseoxygenated blood from the left heart is used.
Advantages• The amount of blood diverted from the leftatrium to distal aorta can be precisely controlled.Communication with the perfusionist is essential.• The system is relatively easy to insert.• Minimal heparinization is needed (activatedclotting time (ACT) = 150 seconds).• Patients undergoing left heart bypass havesmaller differences between the upper and lowerextremity mean arterial pressure, higher intraoper-ative urine output, lower incidence of postoperativeazotemia, and less blood loss in comparison withpatients with a passive shunt.
Disadvantages• No blood or fluid can be added to the bypasssystem because there is no reservoir. Large-boreperipheral or central venous access is a necessity.• The absence of a heat exchanger does not allowthe patient to be actively warmed or cooled.A 4% incidence of postoperative renal failure is
associated with left heart bypass, as compared with9% and 11% for simple cross-clamping and CPB,respectively. However, left heart bypass has noteliminated complications from aortic surgery. A 3%early mortality rate, 1.5% reversible renal failurerate, and 2.3% incidence of permanent spinal cordinjury have been reported despite using left heartbypass for patients undergoing repair of descendingthoracic aortic lesions.
Partial cardiopulmonary bypassPartial cardiopulmonary bypass (CPB) exists whenonly a portion of the systemic venous drainage tothe heart is captured and returned to the CPB cir-cuit (Fig. 9.10d). During partial CPB, the remainingportion of systemic venous return is to the rightatrium. This blood makes its way to the pulmonarybed, where gas exchange occurs. The blood then
returns to the left atrium and left ventricle, whereit is ejected into the systemic circulation. For par-tial CPB to be effective the heart must be beatingwith ejection and the lungs must be ventilated. Inthe absence of ventilation, systemic venous bloodthat enters the right atrium ultimately will reachthe systemic circulation without gas exchange hav-ing occurred. This will result in hypercarbia andhypoxemia.The source of venous blood for this technique
can be the femoral vein, left atrium, or pulmonaryartery. The right atrium is poorly accessible froma left thoracotomy. Arterial outflow from the CPBcircuit is delivered to a distal aortic site or to thefemoral artery. The CPB circuit contains a venousreservoir, a heat exchanger, and an oxygenator.The oxygenator portion of the circuit is redundantwhen the left atrium is used as the source of venousblood.
Advantages• The patient can be actively warmed. This isa major advantage if hypothermia becomes aproblem.• Blood and fluid can be added easily to the systemvia the venous reservoir.• All shed blood can be scavenged by the car-diotomy suction and returned to the venousreservoir without the need for a cell-saver system.• Precise control of the amount of blood divertedfrom the heart to the distal aorta is possible. The per-fusionist partially occludes the venous drainage linewith a clamp and controls arterial outflow with thepump head to determine the balance between prox-imal and distal blood flow. Close communicationwith the surgeon and perfusionist is essential.
Disadvantages• Full systemic anticoagulation with heparin isnecessary.• Left heart bypass with partial CPB requires inten-sive vigilance to hemodynamics by both the anes-thesiologist and the perfusionist. There is a sharedcirculation in place. It is possible for the perfusion-ist to divert too much blood from the heart therebydepriving the heart, head, and upper extremitiesadequate blood supply. The use of an upper and

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 318 — #15
318 Chapter 9
lower arterial line as well as intraoperative TEEassist the team in assessing upper body and lowerbody blood flow.
Ascending aorta and aortic arch lesionsAscending aortic and aortic arch lesions requirefull CPB. They are repaired through a median ster-notomy. The clamps interrupt coronary circulationnecessitating cardiac arrest and cardioplegia. Allof the systemic venous drainage to the heart iscaptured and returned to the CPB circuit and sub-sequently to the patient. In lesions of the ascendingaorta (Fig. 9.10e), arterial cannulation for return ofoxygenated blood to the patient can be obtained inthe distal ascending aorta, aortic arch, or femoralartery. This arrangement allows cerebral perfusionto be maintained. Venous cannulation usually isobtained via the right atrium.If the aortic arch is involved, the great vessels to
the head and upper extremities must be excluded(Fig. 9.10f). In this arrangement, there is no sourceof cerebral blood flow. As a result, some modifi-cations must exist to provide either cerebral bloodflow or to minimize the effects of cerebral ischemiaduring the cross-clamp period. In the absence ofcerebral perfusion, mitigation of the effects of cere-bral ischemia can be accomplished through the useof DHCA. Combining DHCA with continuous ret-rograde cerebral perfusion (CRCP) may extend thesafe arrest limit to between 65 and 90minutes andreduce the risk of neurologic injury during thesurgical procedure. Continuous retrograde cerebralperfusion is accomplished by low pressure delivery(20–30mmHg) of hypothermic (20C), oxygenatedblood from the CPB circuit to the superior venacava with venting of the effluent via the aorticarch. This approach has many advantages, includ-ing its technical ease, ability to easily visualize bloodreturning from the great vessels, and the removal ofparticulate material from arterial sites.
Anesthetic technique for aorticsurgery
Goals1 Obtain a thorough understanding of the type andlocation of the lesion. Review the operative plan and
prepare for use of OLV and adjuvant methods toprovide distal perfusion when indicated.2 Prepare for potential blood loss, includingpharmacologic measures to reduce bleeding.3 Determine necessary invasive and noninvasivemonitoring.4 Minimize hemodynamic perturbations duringinduction and maintenance of general anesthesia.
EvaluationReview of the patient’s medical history and priorradiographic, echocardiographic, and angiographicstudies is critical for the anesthesiologist’s under-standing of preexisting conditions and current sta-tus. Information regarding the patient’s prior lungstatus may provide insight into his ability to tol-erate OLV for long periods. Evaluation of existingradiological studies will help determine the surgi-cal approach, which will dictate monitoring and theneed for OLV.Control of both blood pressure and ejection veloc-
ity are the mainstays of hemodynamic optimizationof the patient with an aortic lesion. Increased bloodpressure and ejection velocity are capable of extend-ing an existing dissection or causing aneurysmrupture. Aggressive control of blood pressure withvasodilators is likely to cause a reflex tachycar-dia and an increase in left ventricular change inpressure over change in time LV (dp/dt), therebyincreasing ejection velocity and the sheer forces onthe aortic lesion. This scenario is particularly likelyin otherwise healthy patient with trauma who mayalready have a hyperdynamic LV secondary to bloodloss and high catecholamine levels. Simultaneouscontrol of both blood pressure and ejection velocityis best obtained with a combination of beta-blockersand vasodilators.
PremedicationPatients who present for elective repair of lesionsoften are hemodynamically optimized beforesurgery. Oral antihypertensive agents may includebeta-blockers, calcium channel blockers, diuretics,and ACE inhibitors. Calcium channel and beta-blocking agents may be advantageous in providingsimultaneous blood pressure and heart rate control.It is essential to continue all preoperative vasoactive

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 319 — #16
Anesthesia for Surgery of the Thoracic Aorta 319
medications. Rebound tachycardia or hypertensionfrom medication withdrawal may be disastrous.Treatment with anxiolytic agents assist in control-ling hypertension and tachycardia and, therefore,minimize aortic wall tension.In contrast, patients presenting emergently for
repair of an aortic lesion are often poorlycontrolled. In the absence of hypotension orshock, beta-blocking agents along with vasodila-tors are indicated. Esmolol, metoprolol, or otherbeta-blockers are commonly used intravenousβ-receptor-blocking agents in this setting. Theadvantages of esmolol include its high specificityfor the β1-receptor and its short duration of action.Options for vasodilator therapy include nitroprus-side, nitroglycerin, trimethaphan, and halogenatedinhalational anesthetic agents. Nitroprusside is apotent arterial vasodilator andmay induce coronarysteal and subsequent myocardial ischemia. Addi-tionally, distal organ and spinal cord perfusion maybe further compromised in patients receiving nitro-prusside during aortic cross-clamping. Nitroglycerinis primarily a venodilator. This medication gen-erally is easier to titrate and provides dilation ofthe large coronary arteries. However, nitroglycerinmay not provide adequate arterial relaxation andblood pressure reduction. Both drugs may compro-mise oxygenation during OLV by blunting hypoxicpulmonary vasoconstriction. The clinical use oftrimethaphan is limited by its side effect profile andtachyphylaxis.
PreinductionPreparation for massive blood loss is critical.Bilateral upper-extremity 14-guage or 16-gaugeintravenous catheters should be placed. Large-borecentral venous access is required. The location forarterial line placement will depend on the locationof the lesion.Distal aortic lesions (Stanford type B) will neces-
sitate placement of a right upper extremity (radial)arterial line. In repairing this lesion, the proximalaortic cross-clamp will probably be placed distal tothe innominate artery. Therefore, the patency of theright subclavian arterywill be preserved throughoutthe procedure.
Proximal aortic lesions (Stanford type A) willnecessitate placement of a left upper extremityarterial line. The left subclavian artery probably willbe distal to the aortic clamp site and should be used.Femoral artery cannulation is used in conjunc-
tion with right radial artery cannulation in patientsundergoing repair of aortic arch or descendingthoracic aortic lesions with distal perfusion. Thefemoral artery cannula is necessary to monitorthe adequacy of distal perfusion. Communicationwith the surgeon is necessary to determine whichfemoral artery can be used for monitoring pressurewhen a femoral artery also is going to be used forperfusion.All necessary vasopressor and vasodilatory agents
and six units of typed and cross-matched bloodshould be available in the operating room beforeinduction. Antifibrinolytics are often used to reducebleeding. Epidural catheters often are used innonanticoagulated patients undergoing electiveprocedures. Caution must be exercised as inadver-tent vascular placement of the catheter may delaythe procedure. A test dose with 3–5mL of 1.5%lidocaine with 1:200 000 epinephrine is importantto confirm correct placement of the catheter. Con-firming normal coagulation status before epiduralcatheter removal is essential.
InductionThere is no one anesthetic technique recom-mended for aortic surgery. The overriding factorin choosing any agent is hemodynamic control.For elective procedures, a narcotic induction withfentanyl (15–25µg/kg) or sufentanil (1–3µg/kg)will minimize hemodynamic disturbances. Anintermediate-acting, nondepolarizing neuromuscu-lar blocker such as vecuronium (0.1mg/kg), rocuro-nium (0.6mg/kg), or cisatracurium (0.2mg/kg)will provide adequate muscle relaxation. Providingsmall doses of muscle relaxant during the nar-cotic infusion will minimize opioid-induced chestwall rigidity. Amnesia must be accomplished withbenzodiazepines and/or inhalational agents.Patients undergoing emergent procedures often
require a rapid sequence induction. A sedativehypnotic such as sodium thiopental (3–5mg/kg),

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 320 — #17
320 Chapter 9
propofol (2.0–2.5mg/kg), or etomidate(0.2–0.3mg/kg) in combination with a smallernarcotic dose (fentanyl 10µg/kg or sufentanil1.0µg/kg) will blunt the hemodynamic effects oflaryngoscopy and will provide rapid induction ofgeneral anesthesia. Succinylcholine 1–2mg/kg isused for rapid muscle relaxation, although largedoses of nondepolarizing agents are an alternative.Protection of the airway and the potential for aspi-ration must be weighed against the undesirablehemodynamic response to direct laryngoscopy. Theaddition of beta-blockade and vasodilator therapybefore laryngoscopy will help attenuate this unde-sirable response. After the airway is secured, deep-ening the anesthetic with a supplemental narcoticdose will improve hemodynamic stability.Lesions of the ascending and aortic arch are
managed with a single-lumen endotracheal tubeof appropriate size. As discussed previously, aor-tic lesions may cause both tracheal and bronchialcompression and caution should be exercised intube placement. Repair of lesions of the distal aorticarch and descending thoracic aorta are facilitatedby OLV. The options available for providing OLVare discussed in detail elsewhere. Many prefer aleft-sided double-lumen endotracheal tube (DLT)unless collapse of the left main-stem bronchus hasoccurred. In these instances, a right-sided DLT isused. Achieving and maintaining proper position-ing of the right upper lobe bronchus lumen canbe problematic. This is particularly true when sur-gical manipulation of the tracheal-bronchial treeis necessary to mobilize the aorta. The left-sidedDLT is placed using fiberoptic bronchoscopy. Thisapproach virtually guarantees proper tube position.This approach, although very useful for all patientsrequiring DLT placement, is particularly importantfor patients with thoracic aortic lesions in whomunsuspected compression of the left main stembronchus may exist. Blind advancement of the left-sided DLT under these circumstances may result inbronchial or aortic disruption. If unsuspected leftmain-stem bronchus compression is diagnosed withfiberoptic visualization, a right-sided DLT may bechosen.A rapid-sequence induction with cricoid pres-
sure may be necessary for the usual indications.
Placement of a DLT under these circumstances maybe difficult because of the DLT’s large size andthe propensity of the tracheal cuff to catch andtear on the patient’s teeth as the tip of the tubeis maneuvered to align with the larynx. When apotentially difficult DLT placement is anticipatedin a patient requiring a rapid sequence induction,placement of a Univent tube (a single lumen tubewith bronchial blocker in place) may be considered.The bronchial blocker can be directed into eithermain-stem bronchus. In addition to being easier toplace in the trachea than a DLT, this tube elimi-nates the need for exchanging a DLT to a singlelumen endotracheal tube at the end of the surgicalprocedure for patients who require postoperativeventilation. Disadvantages of this device includehigh bronchial cuff occlusion pressures and com-promised ability to actively deflate, apply continu-ous positive airway pressure (CPAP) or suction thenondependent lung.
Intraoperative managementAfter induction of general anesthesia, additionalvenous access and monitoring lines are placed.Monitoring includes a 5-lead electrocardiogram(aV5 lead is not possible in left thoracotomy patientsand a modified V5R can be employed), as well asarterial and pulmonary artery catheters. Intraopera-tive TEE should be employed if not contraindicated.If a DLT is used, the tube position should be checkedwith the fiberoptic bronchoscope after the patienthas been positioned laterally to ensure that the tuberemains optimally positioned.Preparation for massive transfusion and red cell
salvage before incision is recommended. Six units ofcompatible blood should be present throughout theprocedure. Immediate availability of platelets andfresh frozen plasma also is crucial. A rapid transfu-sion device can be indispensable, particularly whenfull or partial CPB is not used.
Ascending aortic and aortic arch repairsThese lesions require full CPB and may requireDHCA. There may be associated acute aorticinsufficiency with an aortic dissection or a dilatedaortic root. Theremay be pericardial tamponade and

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 321 — #18
Anesthesia for Surgery of the Thoracic Aorta 321
myocardial ischemia if the dissection involves thecoronary ostia.
Distal aortic arch and descendingthoracic aortic lesionsIf the approach is cross-clamp without distal cir-culatory support, vigorous afterload control withan intravenous or inhalational agent will be nec-essary. Reduction of MAP to approximately 20%below baseline with nitroglycerin or nitroprussidebefore aortic cross-clamping will minimize walltension in the proximal aortic segment after theclamp is placed. Isoflurane also has been advo-cated as a vasodilatory agent in this setting. Patientshave received up to 2.5 ± 0.3% isoflurane forhemodynamic control during aortic cross-clampingwithout negative consequence. Blood pressure
manipulation must always consider the potentialdetrimental effects on end-organ perfusion.After cross-clamp application, blood pressure is
maintained. Placement of the cross-clamp causesan acute increase in LV afterload and reductionin cardiac output. However, the pulmonary arteryocclusion pressure and central venous pressure usu-ally will remain unchanged. Diastolic dysfunction iscommon after cross-clamp placement. If pulmonarycapillary wedge pressure (PCWP) increases withcross-clamp application, three etiologies must beentertained:1 LV afterload mismatch with LV failure anddilation. LV dilation may be accompanied by devel-opment of a new V wave on the PCWP trace,suggesting functional MR. TEE is valuable in assess-ing LV size and function during this period. Left
Table 9.4 Clinical scenarios andtherapeutic interventions during leftheart bypass.
PP DP PCWP TEE Intervention
↑ ↓ ↑ ↑ LVEDA Increase pump flow
↑ ↓ ↓ ↓LVEDA Increase pump flow, volume infusion
↑ ↑ → →LVEDA Vasodilation in conjunction with← ← LVEDA volume infusion
↑ ↑ ↑ ↑ LVEDA Vasodilator, maintain pump flow,allow venous drainage to temporarilyexceed arterial outflow when usingpartial CPB circuit
↓ ↓ ↓ ↓ LVEDA Volume infusion, temporaryvasopressor support
↓ ↓ ↑ ↑ LVEDA Increase pump flow, inotropicsupport if resolution of LV distentiondoes not improve LV performanceand proximal pressure
↓ ↑ ↑ ↑ LVEDA Institution of inotropic supportfollowed by incremental decrease ofpump flow to avoid further LVdistention
↓ ↑ ↓ ↓ LVEDA Decrease pump flow, if proximalpressure is low after desired distalpressure is reached then volumeinfusion
CPB, cardiopulmonary bypass; DP, distal pressure; LV, left ventricle; LVEDA,left ventricular end-diastolic area; PCWP, pulmonary capillary wedge pressure;PP, proximal pressure; TEE, transesophageal echocardiography.

Alice Nelson Dinardo: “ch09” — 2007/7/17 — 20:32 — page 322 — #19
322 Chapter 9
ventricle dilatation with or without functional MRis an indication for immediate intervention withvasodilators. If LV dilation persists despite after-load reduction, initiation of inotropic support iswarranted.2 Myocardial ischemia may be accompanied byST segment changes, but monitoring of ischemiais hampered by the lack of a V5 lead. TEE candiagnose new regional wall motion abnormali-ties. Aggressive treatment of myocardial ischemia isindicated.3 Impaired LV diastolic function due to impairedrelaxation. Determination of impaired relaxationrequires TEE to obtain Doppler spectra of the mitralvalve inflow, pulmonary venous flow and tissueDoppler. Afterload reduction may improve diastolicfunction.Acidosis may be treated with aggressive venti-
lation and bolus administration of sodium bicar-bonate. A continuous infusion of bicarbonate(0.05mEq/kg/min) during cross-clamping may bemore efficacious. Large doses of sodium bicarbon-ate administered immediately before cross-clamprelease will cause a transient iatrogenic hypercarbia,which when combined with a metabolic acidosis,can result in profound acidemia.The physiologic changes associated with cross-
clamp removal include hypotension, pulmonaryhypertension, and metabolic acidosis. Prepara-tion for cross-clamp removal will help mini-mize or attenuate these undesirable consequences.Several minutes before cross-clamp removal, thepatient should be volume loaded to a PCWP of10–20mmHg. TEE can adequately assist with LVvolume assessment. All vasodilating agents are dis-continued and the cross-clamp is removed overa several-minute period. Hyperventilation beforecross-clamp removal will help minimize the acido-sis and the pulmonary hypertension associated withclamp removal. Despite these measures, patientsmay require variable periods of vasopressor supportafter removal of the aortic cross-clamp. Intractable
hypotension after cross-clamp removal is anindication for reapplication of the cross-clamp.If a shunt or assisted circulatory method is used,
attention to the proximal and distal perfusion pres-sures is critical. In the case of passive shunts, atten-tion is focused on adequacy of flow and patencyof the shunt. Little control of proximal and dis-tal pressure is possible. Proximal hypertension withthe shunt patent requires pharmacologic interven-tions as described for simple cross-clamping. Distalhypotension with a patent shunt is problematic.Interventions to elevate proximal blood pressurewith vasopressors and volume infusion may elevatedistal pressure; however, such interventions mayproduce unacceptably high proximal pressures.Left heart bypass and partial CPB provide bet-
ter proximal hemodynamic control and more pre-dictable distal perfusion than a passive shunt. Withleft heart bypass and partial CPB, the easiest initialapproach is to decide, in conjunction with the per-fusionist, the amount of flow that will be divertedto the distal aorta after cross-clamp application. Thisdepends on the size of the patient and the desireddistal perfusion pressure. Usually, distal perfusionpressure is maintained at 40–60mmHg. Remem-ber, it is essential to ensure adequate LV volumefor heart and great vessel perfusion.After this has been established, the balance of
proximal and distal pressure is fine-tuned andman-aged as shown in Table 9.4 using proximal pressure,distal pressure, PCWP, and TEE.
Suggested reading
Campos JH. An update on bronchial blockers during
lung separation techniques in adults. Anesth Analg
2003;97:1266–74.Hagan PG, Nienaber CA, Isselbacher EM et al. The Interna-
tional Registry of Acute Aortic Dissection (IRAD): new
insights into an old disease. JAMA 2000;283:897–903.Khan IA, Nair CK. Clinical, diagnostic, and management
perspectives of aortic dissection. Chest 2002;122:311–28.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 323 — #1
CHAPTER 10
Management ofCardiopulmonary Bypass
The cardiac anesthesiologist is integrally involvedwith commencing, maintaining, and terminatingcardiopulmonary bypass (CPB). It is essential for theanesthesiologist to have a working knowledge of theCPB circuit to aid the surgeon and perfusionist indiagnosing and treating the problems that may beassociated with extracorporeal circulation.
The CPB circuit
The CPB circuit is intended to isolate the cardiopul-monary system so that optimal surgical exposurecan be obtained for operations on the heart andgreat vessels. For this isolation to be effective, theCPB circuit must be able to perform the functions ofthe intact cardiopulmonary system. At a minimum,the circuit must be capable of adding oxygen andremoving carbon dioxide from blood and of provid-ing adequate perfusion of all organs with this blood.In addition, the circuit must be able to fulfill theserequirements without doing permanent damage tothe cardiopulmonary system, the blood, or any ofthe patient’s end organs. Substantial differencesexist between adult and pediatric CPB and theseare summarized in Table 10.1 and are addressedthrough this chapter. The components of a typicalCPB circuit are illustrated in Fig. 10.1. The compo-nents of the circuit are described in the followingsections.
Venous drainageFor the cardiopulmonary system to be isolated,all venous return to the heart must be made
Table 10.1 Comparison of adult and pediatriccardiopulmonary bypass.
Parameter Adult Pediatric
Minimum CPB Rarely Frequentlytemperature <25–32C 15–25C
Use of DHCA or RLFP Rarely Frequently
Pump primeDilution of blood 25–33% 100–200%volumeWB or PRBC added Rarely Usually
Perfusion pressure 50–80mmHg 20–50mmHg
pH-stat management Rarely Usually, attemperaturebelow 28–30C
Glucose managementHyperglycemia Frequently, Occasionally
requiresinsulin
Hypoglycemia Rarely Occasionally
CPB, cardiopulmonary bypass; DHCA, deep hypothermiccirculatory arrest; PRBC, packed red blood cells; RLFP,regional low flow perfusion; WB, whole blood.
available to the CPB circuit. Blood is collected fromthe venous circulation and then drains by a siphoninto a reservoir that lies on or near the floor wellbelow the patient. The pressure gradient for venousdrainage (cm H2O) is the height difference betweenthe RA and the venous reservoir. The flow rateof venous blood (venous return) is determined
323

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 324 — #2
324 Chapter 10
Venouscannula
ArterialArterialcannulacannula
Arterial line
Arterialline filterArterial line
pressurePump suckersArterialpump
Oxygenator
Venous line
Venous reservoirGas source
Filter
Arterialcannula
Fig. 10.1 A typical cardiopulmonarybypass (CPB) circuit.
by this pressure difference and by the resistancein the venous drainage system (cannula and tub-ing). For a given mean systemic venous pressureand venous resistance, maximum venous return isreached when the right atrial (RA) pressure fallsto zero. When the RA pressure is less than zerothe superior vena cava (SVC) and inferior venacava (IVC) collapse and the heart acts as a Starlingresistor.
Total (also complete or full) CPBTotal CPB exists when all of the systemic venousdrainage to the heart is diverted to the CPB circuit.Total CPB is best accomplished with either directcannulation of both the SVC and IVC or with use oftwo-stage single venous cannula in the RA.• Direct cannulation of the SVC and IVC. This tech-nique is necessary for all procedures that requireopening of the RA or right ventricle (RV). It is alsocommonly used in procedures where retraction of acompletely empty RA may facilitate surgical expo-sure (mitral valve exposure via the left atrium (LA)).Normally all systemic venous return can be cap-tured via cannulation of both the SVC and IVC.In children with congenital heart disease, capturingall sources of systemic venous return may be prob-lematic. Other sources of systemic venous returnmay exist such as a persistent left SVC draining
to the coronary sinus. In children with hetrotaxysyndrome there may be an interruption of the infra-hepatic IVC with the hepatic veins draining directlyto the floor of the right-sided atrium and azygousor hemi-azygous continuation of the IVC drainingto a right- or left-sided SVC. For total CPB, oncethe cavae (and other sources of systemic venousreturn) are cannulated, surgical tourniquets or tapesare passed around the external circumference ofthe vessels. When these tourniquets are tightenedaround the cannulas the right heart can be iso-lated completely and subsequently opened withoutentrainment of air into the venous circuit or obscu-ration of the surgical field by venous blood. Duringdelivery of antegrade cardioplegia, it is essential thatat least one tourniquet be left un-tightened to allowegress of cardioplegia solution from the coronarysinus without distention of the right atrium. A largercannula is used in the IVC as compared with theSVC, because a larger portion of systemic venousreturn (two-thirds) is from the IVC.• Two-stage venous cannula in the RA. The single-cannula system is satisfactory for procedures thatdo not require opening the RA or RV, such as coro-nary artery bypass grafting or aortic valve replace-ment. Venous drainage is accomplished with onelarger bore cannula with two orifices inserted viaan incision in the RA appendage. One orifice

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 325 — #3
Management of Cardiopulmonary Bypass 325
(32–36-French outer diameter) lies directly in theIVC and the other (40–51-French outer diameter)lies in the RA proximal to the SVC–RA junction.Coronary sinus and persistent left SVC return iscollected continuously via the orifice that lies at theSVC–RA junction.
The vast majority of operative procedures in chil-dren require the use of either total CPB or deephypothermic circulatory arrest (DHCA). Venouscannulation for DHCA is usually accomplished witha single large venous cannula in the right atrium.Once cooling is complete and circulatory arrestcommences the cannula can be removed to allowmaximum exposure.
Partial CPBPartial CPB exists when only a portion of the sys-temic venous drainage to the heart is diverted to theCPB circuit. During partial CPB, the remaining por-tion of systemic venous return is to the RA. Ideally,this blood makes its way to the RV and pulmonarybed, where gas exchange occurs. The blood thenreturns to the LA and left ventricle (LV), where itis ejected into the systemic circulation. For partialCPB to be effective, two things must be true:1 The heart must be beating and ejecting. If ejec-tion is ineffective or nonexistent, distention of theheart will occur and systemic blood flow will beinadequate.2 The lungs must be ventilated. In the absence of ven-tilation, systemic venous blood that enters the RAwill ultimately reach the systemic circulation with-out gas exchange. This will result in hypercarbia andhypoxemia.
During partial CPB, the patient’s systemic bloodflow is provided in part by the CPB circuit and in partby the patient’s heart. The patient’s arterial pH, par-tial pressure of oxygen (PO2), and partial pressure ofcarbon dioxide (PCO2) are a reflection of the quan-tity and effectiveness of these two sources of blood.Therefore, during partial CPB, blood for blood gasanalysis must be drawn from the patient and notfrom the CPB circuit.
Partial CPB can be accomplished with the cannu-lation techniques described for total CPB simply bypartially impeding venous return to the CPB circuitwith a clamp on the venous drainage line. More
commonly, partial CPB is the result of cannulationof the right atrium directly with a small cannulaor indirectly via the femoral venous system. A can-nula is inserted retrograde up a femoral vein towardthe heart into the IVC or RA. This system is muchless effective than caval cannulation via the rightatrium because the femoral vein limits the size ofthe cannula that can be inserted. This inhibits opti-mal systemic venous drainage because of the largepressure drop across the long, narrow cannula. This,in turn, elevates RA pressure, which for a givenmean arterial pressure (MAP) and systemic venousresistance, further compromises venous return. Forthese reasons, with femoral venous cannulation, itis often impossible to divert all venous return to theCPB circuit. The major advantage of femoral venouscannulation is that it can be provided emergentlyand quickly without a sternotomy. Partial CPB isused under the following circumstances:• During repair of thoracic aortic lesions.• As temporary support for cardiogenic shockafter interventional cardiac catheterization orelectrophysiologic procedures.• In patients undergoing reoperative procedures toprovide elective or semi-emergent decompressionof the heart or great vessels when they are adherentto the underside of the sternum.
Even with appropriate cannulation techniques,there may be compromise of venous return to theCPB circuit. An air lock may occur when large bub-bles of air become lodged in the venous drainagelines. This air usually is entrained into the venousdrainage lines from around loose cannulation sites.This can occur even when the right heart is notdirectly open to air. An air lock acutely disruptsthe siphon effect. This causes RA pressure to riseabove zero and venous return to the venous reser-voir to fall. Malposition of the venous cannula is aconstant risk particularly in infants and neonates.Even partial obstruction of IVC return can result inrenal, hepatic, and gastrointestinal hypoperfusionand the development of ascites. Poor SVC drainagecan result in engorgement and cyanosis of the headand neck. SVC obstruction can easily lead to cerebralischemia particularly given the low cerebral perfu-sion pressure (CPP) that results from the low MAP

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 326 — #4
326 Chapter 10
utilized during pediatric CPB. If poor SVC drainageis suspected, the surgeon should be alerted so thatthe cannula can be repositioned. Transducing thecentral venous pressure (CVP) catheter will allowmeasurement of the pressure in the SVC and isuseful in detecting poor SVC drainage.
Venous reservoirs are either of the soft shell, col-lapsible type or the hard shell, noncollapsible type.Hard shell reservoirs are constructed of rigid plasticvented to atmosphere with the venous and car-diotomy reservoirs integrated in one unit. Thesereservoirs allow better visualization of the reser-voir volume and easier removal of venous cannulaair than soft shell reservoirs. Soft shell reservoirsalso require a separate cardiotomy reservoir. Thesereservoirs generally have a smaller priming volumethan their hard shell counterparts but can presenta significant obstruction to venous return if theybecome distended.
Assisted venous drainage is a technique usedin adult cardiac surgical patients to augmentvenous return while utilizing small venous can-nulas primarily during minimally invasive proce-dures. Assisted venous drainage may be via a kineticor vacuum assisted system. In the kinetic system,a centrifugal pump is interposed in the venousdrainage system between the patient and thevenous reservoir. Vacuum assisted venous drainage(VAVD) involves application of a vacuum (−40 cmH2O) to a closed hard shell venous reservoir. Bothmethods serve to augment the pressure gradientfor venous drainage. Both techniques have beenapplied to neonates and infants to allow use ofsmaller venous cannula and to reduce CPB primevolume. With use of 3/16-inch venous and arte-rial tubing, no arterial line filter, no prime in thevenous line, and use of VAVD, the prime volumefor a neonatal circuit can be as low 200 mL. Unfor-tunately, these techniques are not without risk.Using VAVD, arterial line emboli distal to the arte-rial filter is increased eight-to tenfold over that seenwith conventional gravity venous drainage due toentrainment of air into the venous system. Arte-rial air embolism may also occur as the result ofinadvertent positive pressurization of the venouscircuit resulting in a paradoxic air embolus acrossan intracardiac communication.
Arterial inflowNormally, arterial inflow is obtained via a cannulaplaced in the lesser curve of the ascending aortaproximal to the innominate artery. This arrange-ment allows perfusion of all vessels of the arch anddistal aorta, as well as perfusion of the coronaryostia. Adult cannulas range from 19- to 24-Frenchin outer diameter (6.3–8.0 mm). Pediatric cannulasrange from 8.0- to 17.0-French in outer diame-ter (2.7–5.7 mm). Because the distal end of thearterial cannula is significantly smaller than thearterial inflow line, a large pressure drop existsacross the arterial cannula. At normal bypass flowsof 2.0 L/min/m2, a gradient in excess of 120 mmHgmay exist across an appropriate diameter cannula.This pressure drop is the result of a high velocity jetout the distal end of the cannula. It is essential thatthis jet be directed into the center of the aorta andnot up into the innominate artery so that a cerebraloverperfusion injury does not occur.
As with venous cannulation, arterial cannula-tion particularly in infants and neonates can betechnically challenging. In circumstances where theascending aorta and aortic arch are hypoplastic andsystemic blood flow is ductual dependant (as inhypoplastic left heart syndrome) it may be neces-sary to obtain systemic perfusion through the duc-tus arterious by cannulating the pulmonary artery(PA). When the aortic arch is interrupted, cannu-lation of the aorta both proximal and distal to theinterruption is necessary. Because the arterial can-nula is relatively large as compared to the aorta ininfants and neonates, complete or partial obstruc-tion of the aorta by the cannula itself is possible.If dampening of the arterial trace, distension of thesystemic ventricle, or an increase in CPB line pres-sure occurs with placement or manipulation of thearterial cannula, the surgeon should immediatelybe made aware of the situation so the cannula canbe repositioned. Some centers utilize near infra-red spectroscopy (NIRS) and transcranial Doppler(TCD) technology as adjunctive methods to assesscerebral blood flow during CPB.
In patients undergoing re-operative proceduresit may be necessary to obtain arterial inflow viaa femoral artery when the heart or great ves-sels are adherent to the underside of the sternum.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 327 — #5
Management of Cardiopulmonary Bypass 327
Placement of the cannula in the femoral artery pro-vides retrograde perfusion to the proximal aorta andcoronary ostia. This route has several limitations.The smaller caliber of the femoral vessel limits thesize of the arterial cannula that can be used withoutrisk of damage to the artery. The smaller the can-nula, the larger will be the pressure drop across it. Ifthe pressure drop is severe, flow will be limited afterthe safe maximum arterial perfusion line pressure(about 300 mmHg) has been reached. Perfusion tothe leg in which the cannula is placed is limited bythe fact that the cannula occupies the entire lumenof the femoral artery and is directed proximally.This may result in an ischemic leg and a persistentmetabolic acidosis. When the cannula is removed,there is often a washout of lactic acid resulting in ametabolic acidosis that may require treatment withsodium bicarbonate and alveolar hyperventilation.
PumpsThere currently are two types of pumps usedon modern CPB machines to provide nonpul-satile flow: the double-headed nonocclusive rollerpump (Fig. 10.2) and the centrifugal blood pump(Fig. 10.3).
Double-headed roller pumpThe double-headed roller pump is the most com-monly used. The double-headed roller pump is apositive volume displacement pump. At least one
Fig. 10.2 A typical double headed nonocclusive rollerpump. One head of the pump will be in contact with thepump boot at all times as is shown here.
head is in contact with the pump boot at all timesto push blood forward and ensure continuous for-ward flow. The pump boot is the piece of tubing incontact with the pump heads. It generally is thickerand more durable than the other sections of tub-ing in the CPB circuit. Roller pumps are driven bya load-independent electric motor. After the pumpspeed has been set, the pump will continue the for-ward displacement of the same volume of blood,even if the resistance to flow is increased by kink-ing or clamping the arterial line. This will resultin a large pressure increase in the arterial inflowline, which can result in the rupture of connectionsbetween sections of tubing. To avoid this type ofdisaster pressure gauges are placed on the arterialinflow line. If arterial line pressure rises to danger-ous levels (300 mmHg) pump flow can be reducedto allow line pressure to fall until the problem isidentified and corrected.
Centrifugal pumpThe centrifugal pump is a kinetic pump. It operateson the constrained vortex principle. Blood is driventhrough the pump by centrifugal forces generatedby a vortex in the pump. It has been suggestedthat this causes less trauma to blood componentsthan the roller pump. Although the pump is drivenby a load-independent electric motor, this pumpdoes not behave like the roller pump. When line
Fig. 10.3 A typical centrifugal pump. Entrained air willbe drawn to the apex of the pump away from the outletat the base of the pump.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 328 — #6
328 Chapter 10
resistance is increased, blood flow falls as the shearforces between the layers of blood are increasedand less forward displacement of blood occurs. Thisresistance dependence prevents increases in arterialline pressure when clamping or kinking occurs. Thepump is said to be inflow responsive as well. If alarge quantity of air is introduced into this pump,cohesive forces will no longer exist between layersof blood and pumping will cease. In addition, therisk of micro air embolization is reduced becausesmall, low-density air bubbles become trapped inthe center of the vortex.
OxygenatorsOxygenators perform the gas exchange functionsof the lung in the CPB circuit. Despite the factthat oxygenators are incorporated in a system inwhich blood is pumped under pressure, all gasexchange occurs at atmospheric pressure becausethe oxygenators are vented to the atmosphere.There currently are two types of oxygenators avail-able: bubble oxygenators and membrane oxygena-tors. Membrane oxygenators are the primary typeof oxygenator currently used.
Bubble oxygenatorsBubble oxygenators provide oxygen delivery to andcarbon dioxide removal from blood via a gas bubble-blood interface (Fig. 10.4). The venous blood fromthe venous drainage line and the blood from thecardiotomy lines drain passively to the bottom por-tion of a bubble column. The bottom portion ofthe bubble column is separated from the gas entrychamber by a dispersion or diffusor plate. The dis-persion plate breaks up the bulk gas (100% oxygenor an oxygen/carbon dioxide mixture) into bub-bles of appropriate size for gas exchange. This gasis bubbled through blood and gas exchange occursas the bubble-blood mixture rises upward to the topof the bubble chamber. Heat exchange also occursas the gas mixture rises. At the top of the bubblechamber the bubble-blood mixture passes througha debubbler/defoamer chamber. This chamber hasa large surface area of polyurethane mesh spongethat is coated with a silicone antifoaming agent andcovered with polyester mesh fabric. The antifoam-ing agent causes bubbles to collapse by reducing
Down comer
CO2 vents
Oxygenatingtubes
Metal heatexchanger
Defoamer
Water outlet
Arterialreservoir pool
Arterial outlet
Blood/gas mixing chamberDiffusor plate
Oxygenating gas
Venous inlet
Water inlet
Hydrostaticbarrier
Fig. 10.4 Cutaway view of a typical bubble oxygenator.Water inlet and outlet for heat exchange coils are locatedat the bottom of the oxygenator. Oxygen inflow is alsolocated at the bottom. Venous blood passively enters thebottom of the oxygenator via venous cannulas andvenous drainage line. Oxygen (O2), carbon dioxide(CO2), and heat exchange all occur as bubble-bloodmixture is carried to the top of the oxygenator.Bubble-blood mixture then passes into a debubbler/defoamer chamber before spilling over into the arterialreservoir. From the arterial reservoir, blood is pumped tothe patient via arterial inflow line and arterial cannula.
surface tension and the other components mechan-ically disrupt the bubbles. This arrangement servesto eliminate the majority of gaseous microemboli.From here, the blood spills over into an arterialreservoir. The reservoir provides an area for fur-ther elimination of microbubbles by allowing themto rise to the top of the blood. Blood in the arterialreservoir is then pumped to the patient. The volume

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 329 — #7
Management of Cardiopulmonary Bypass 329
in the reservoir provides a volume buffer thatallows the perfusionist to react to changes in venousreturn without pumping the reservoir dry and thenpumping air into the patient.
Oxygen is relatively less soluble and diffusible inblood than carbon dioxide (ratio of 1:25). There-fore, oxygen delivery is enhanced by the presenceof small bubbles where the surface area availablefor gas exchange is large. Carbon dioxide removal,on the other hand, is enhanced by the presence oflarge bubbles where the volume of the gas bubblesis large. In reality, the bubble size is somewherebetween these two extremes (3–7 µm). For a givenbubble size, an increase in the flow of bubblesthrough blood results in enhanced carbon dioxideremoval. Therefore, arterial partial pressure of car-bon dioxide (PaCO2) is controlled by the gas to bloodflow ratio (GBFR). Some additional control of PaCO2
can be obtained by using an oxygen/carbon dioxidemixture instead of 100% oxygen as the bulk gas.Independent control of arterial partial pressure ofoxygen (PaO2) is difficult as the fraction of inspiredoxygen (FiO2) is fixed (100% oxygen) or very nearlyfixed (oxygen/carbon dioxide). Removal of nitrogenbubbles is difficult and, therefore, oxygen/nitrogenmixtures are not used.
The bubble-blood interface is not physiologic dueto the constantly changing blood-gas interface. Thisresults in traumatization of the blood. Increasinggas flow to enhance gas exchange results in furthertraumatization of the blood. In addition, increas-ing gas flow increases the number and decreasesthe size of the bubbles generated. This increases therisk that gaseous microemboli will reach the arterialcirculation.
Membrane oxygenatorsMembrane oxygenators allow oxygen delivery toand carbon dioxide removal from blood across a thinmembrane, eliminating any direct blood gas con-tact. The high resistance inherent in the membraneoxygenators does not allow gravity flow of venousblood through the membrane into an arterial reser-voir. As a result, the venous drainage and car-diotomy lines empty into a venous reservoir and arepumped through the membrane and then out to thepatient via the arterial line. As would be expected,
the pressure drop across the membrane increaseslinearly with increasing flow.
Membrane oxygenators generally are of twotypes: microporous membranes and solidmembranes.• Microporous membranes. Microporous membranesare made of polypropylene with small, hydrophobicpores (0.03–0.07 µm in diameter) impermeable toblood and gas. These pores cover at least 50% of themembrane surface. Upon exposure to blood, thesepores become covered with a thin proteinacouslayer through which gas exchange occurs withoutblood and gas coming in direct contact. These micro-porous membranes offer little or no limitation to thediffusion of carbon dioxide or oxygen. Eventually,over the course of several hours the gas exchangecapacity of these membranes deteriorates as serumevaporates and plugs the micropores.
There are two types of microporous membranes:hollow fiber and parallel plate or pleated sheet.Hollow fiber membranes are composed of a largebundle of polypropylene microporous capillarytubes 200–300 µm in diameter knitted together ina mesh, wrapped around a solid core and insertedinto a cylindrical shell. Gas flows on the insideof the fibers and blood flows on the outside ofthe fibers; a design known as extra luminal flow(ELF). This allows air in the blood path to be rec-ognized during priming. In addition, in the eventof fiber rupture, blood will contaminate only thefibers affected with little effect on the gas exchangecapacity of the membrane. Counter-current flow ofgas and blood is induced by introducing gas into thefibers at one end of the cylinder and introducingblood around the fibers at the other end. In addition,the path of blood around the knitted mesh of fibersinduces crosscurrent flow with blood flowing per-pendicular to the fibers. A hollow fiber membraneoxygenation system is illustrated in Figs 10.5–10.7.The performance characteristics of this membraneare summarized in Fig. 10.8.
In the pleated sheet design a continuous micro-porous sheet is folded and compressed like a col-lapsible fan. Gas flows on one side of the sheetand blood flows on the other side with flow dis-tribution promoted by polypropylene screens. Thepleated design induces counter-current flow of

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 330 — #8
330 Chapter 10
1. Venous reservoir 2. Cardiotomy reservoir 3. Connection key 4. Venous retrurn connector: 3/16-1/4″ I.D. 5. Turrets 6. Arterial blood outlet: 3/16-1/4″ I.D. 7. Venous reservoir outlet: 3/16/1/4″ I.D. 8. Venous blood inlet: 3/16-1/4 I.D. 9. Scavenging connector10. Sampling connector11. Arterial temperature probe site12. Venous temperature probe site13. Recirculation line clamp14. Gas inlet15. Gas escape16. Sample port luer17. Drug port luer18. Cardiotomy bypass port
9 518
3
2
1
13
16
10
178
12
15
11
6
7
14
4
Fig. 10.5 Cutaway view of a DidecoLilliput 1 hollow fiber microporousmembrane oxygenator. The venousreservoir (1) is located at the top of thedevice and incorporates a cardiotomyreservoir (2), whereas the membraneoxygenator is located at the bottom.Cardiotomy suction blood enters at 9.Venous return blood passively entersthe venous reservoir at 4. Venousreturn and filtered cardiotomy bloodexit at 7. From there blood is deliveredto a pump (roller or centrifugal) and ispumped into the membraneoxygenator at 8. After undergoing gasand heat exchange within theoxygenator blood exits at 6 and isdelivered to the arterial cannula by thesame pump which pumped blood intothe membrane oxygenator. Fresh gas(sweep gas) enters the membraneoxygenator at 14 and exits at 15. If aninhalation agent were added to thesweep gas it would be scavenged at 15.
blood and gas. These types of membranes provideless gas exchange surface area per unit volume ofblood than hollow fiber membranes. As a resultthey require a larger blood priming volume thanhollow fiber membranes to provide comparablegas exchange. Both hollow fiber and pleated sheetarrangements of microporous material allow a largesurface area (up to 4.5 m2) for gas exchange tobe contained in a relatively small space. However,neonate and infant membrane oxygenators are ofthe hollow fiber type to minimize prime volume.• Solid (nonporous) membranes. These membranesare constructed of methyl silicon rubber that isthin enough (<25 µm) to permit diffusion of gas.These membranes do offer some limitation to thediffusion of carbon dioxide and oxygen with car-bon dioxide diffusing five times as easily as oxygen.As a result, these membranes require a greater gasexchange surface area and thus a greater primingvolume than microporous membranes to providecomparable gas exchange. These membranes have
greater longevity (days verses hours) than micro-porous membranes and are reserved for use inextracorporeal membrane oxygenation (ECMO)circuits.
Although modern membranes themselves offerlittle impedance to the diffusion of gas, there areother characteristics of membrane oxygenators thatlimit gas exchange. The primary determinants ofoxygen and carbon dioxide exchange across a mem-brane are the solubility and diffusibility of oxygenand carbon dioxide in blood and their partial pres-sure gradient across the membrane. Because oxygenis relatively less soluble and diffusible in blood thancarbon dioxide, oxygen exchange is dependent onthe thickness of the blood film and the pressure gra-dient for oxygen across the membrane. The vastmajority (90%) of the resistance to oxygen diffu-sion in a membrane oxygenator system is diffusionof oxygen into blood and not diffusion across themembrane. The pressure gradient for oxygen canbe increased by increasing the oxygen content of

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 331 — #9
Management of Cardiopulmonary Bypass 331
Fig. 10.6 Photo of the heat exchange unit of the DidecoLilliput 1 with the rest of the system removed. Wateroutlet (upper) and inlet (lower) ports are clearly seen atthe lower right.
Fig. 10.7 Photo of an assembled Dideco Lilliput 1 systemmounted on the heat exchanger. The heat exchange unitis inserted into the core of the membrane oxygenator.Water inlet and outlet ports are seen as in Fig. 10.5.
1.000.900.800.700.600.500.400.300.200.100.00
80706050403020100
O2
tran
sfer
red
(cc/
min
)/(L
/min
)C
O2
tran
sfer
red
(cc/
min
)/(L
/min
)d
P (
mm
Hg)
0 0.2
HE performance
=T
b(ou
t)−T
b(in
)/T
w(in
)−T
b(in
)
0.4 0.6Blood flow Qb (L /min)
Blood flow (L /min)
0.8 1.0 1.2
0 0.2 0.4 0.6 0.8 1.0 1.2
80706050403020100
140.0120.0100.080.060.040.020.00.0
Blood flow (L/min)
Blood flow (L/min)
0 0.2
0.0 0.4 0.8 1.2
0.4 0.6 0.8 1.0 1.2
O2 transfer
CO2 transfer
d P blood
Fig. 10.8 Performance characteristics of the DidecoLilliput 1 oxygenator and heat exchanger over a typicalrange of blood flows through the membrane. As theupper limits of blood flow are reached gas (oxygen (O2)and carbon dioxide (CO2)) transfer diminishes as doesthe performance factor (η) of the heat exchange unit.The pressure drop across the membrane also increases asblood flow increases. HE, heat exchange; dP, pressurechange.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 332 — #10
332 Chapter 10
Oxygenator Patientweight(kg)
Oxygenatorprime (mL)
Total circuitprimeincludingoxygenator(mL)
Manufacturerreference flowrate (mL/min)
Dideco Liliput 1 <8 60 Neonate 300 800Infant 320
Dideco Liliput 2 <20 105 Infant 425 2300Toddler 575
Cobe Optimin <40 170 Toddler 790 5000Small adult 1110
Cobe Optima >40 260 Adult 1300 8000
Table 10.2 Comparison of membraneoxygenators.
the fresh gas flow. However, because of the lowdiffusibility of oxygen in blood, a thick blood filmor boundary layer will result in poor oxygen deliv-ery to the cells most distant from the membrane,even when the pressure gradient for oxygen is high.Modern membranes have design features to induceeddy currents or static mixing which serves to dis-rupt the boundary layer and enhance diffusion ofoxygen into blood.
Because carbon dioxide is relatively more solublethan oxygen, carbon dioxide exchange is dependentonly on the pressure gradient for carbon dioxideacross the membrane. Normally, fresh gas flowto the membrane oxygenator contains no carbondioxide, and thus the gradient for carbon dioxideremoval will not be improved by lowering the car-bon dioxide content of the fresh gas. The rate ofcarbon dioxide removal can be increased by increas-ing the rate of fresh gas flow or sweep rate to theoxygenator; this is analogous to increasing alveolarventilation.
An important measure of oxygenator perfor-mance is reference flow rates as defined by the man-ufacturer and the Association for the Advancementof Medical Instrumentation (AAMI). Carbon diox-ide reference flow is defined as the maximum flowof blood with a hemoglobin of 12 g/dL, zero basedeficit, and an oxygen saturation of 65% at a tem-perature of 37C that can enter an oxygenator andsubsequently leave the oxygenator with the car-bon dioxide content decreased by 38 mL/L. Oxygenreference flow is defined as the maximum flow
Table 10.3 Comparison of membrane oxygenator heatexchange capacity.
Oxygenator Membranesurface area(m2)
Heat exchangesurface area(m2)
Dideco Liliput 1 0.34 0.02Dideco Liliput 2 0.64 0.02Cobe Optimin 1.0 13.74Cobe Optima 1.9 13.74
of blood with a hemoglobin of 12 g/dL, zero basedeficit, and an oxygen saturation of 65% at a tem-perature of 37C that can enter an oxygenator andsubsequently leave the oxygenator with the oxygencontent increased by 45 mL/L. The recommendedreference flow rate is the lesser of these two val-ues. The performance characteristics of a range ofmembrane oxygenation systems typically utilizedare summarized in Tables 10.2 and 10.3.
Heat exchangersHeat exchangers are necessary to produce theactive cooling and rewarming of the patient’s bloodrequired for systemic hypothermia on CPB. Heatexchange is accomplished by a countercurrent flowof water and the patient’s blood. Water of a pre-determined temperature is pumped into a spiralstainless steel coil as blood flows in the oppositedirection over the coil. The countercurrent flowarrangement provides the most efficient method of

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 333 — #11
Management of Cardiopulmonary Bypass 333
heat exchange. Water input temperature is deter-mined by mixing various proportions of hot andcold water before its introduction into the coil.A device capable of accurately producing water ofthe appropriate temperature and pumping it to theheat exchange coils is a necessary component of theCPB circuit.
Heat exchange coils are inserted into the coreof the membrane oxygenator in some systems (seeFig. 10.6) or are located prior to blood entry into themembrane in others. They are generally not locatedin the CPB circuit after the oxygenator in orderto minimize the risk of systemic gaseous micro-emboli that may be produced during rewarmingas the solubility of gases in blood is reduced. Asthe temperature gradient between the venous bloodinput and water input decreases, heat exchangeslows exponentially. Nonetheless, the temperaturegradient between venous blood input and waterinput is kept between 8C and 10C to avoidlarge changes in gas solubility. During warming,the heated water input temperature never exceeds40C to avoid heat damage to blood and tissue.
Heat exchangers are rated according to the per-formance factor (PF). The PF is the amount of heatactually transmitted to blood divided by the max-imal amount of heat that could theoretically betransferred. The PF of heat exchangers varies from0 to 1 with a PF of 1 (100% efficiency) being unob-tainable. The performance characteristics of a typicalinfant and neonatal heat exchanger are illustratedin Fig. 10.8. The heating and cooling efficacy of theDideco Lilliput 2 system would be expected to beinferior to that of the Lilliput 1 given that the twosystems have the same heat exchange surface areaand the Lilliput 2 is utilized for larger patients atalmost three-times the reference flow rate of theLilliput 1 (see Table 10.3).
Cardiotomy suctionCardiotomy or pump suction is incorporated intomost CPB circuits, where it serves as an impor-tant source of blood conservation. Most systemsuse a roller pump to provide the necessary suc-tion. The collected blood goes either to a filteredcardiotomy reservoir and then to the venous reser-voir or directly to a venous reservoir that contains
a filter. Often, the cardiotomy suction is used beforeinitiation of CPB during cannula placement. It isessential that adequate heparinization be obtainedbefore use of cardiotomy suction so that clot is notintroduced into the cardiotomy or venous reservoir.
Blood from the pericardial collected by car-diotomy suction and returned to the venous reser-voir is know to activate the extrinsic coagulationpathway during CPB. In fact it has been demon-strated that aspirated pericardial blood returned tothe venous reservoir is the most important activatorof the coagulation system during CPB. In additionto bone and fat fragments, pericardial aspirate is richin tissue factor (TF) and procoagulant cellular (pri-marily platelet) derived microparticles. It has alsobeen demonstrated that elimination of pericardialcardiotomy suction return to the venous reservoiror washing of pericardial cardiotomy blood prior toreturn reduces inflammatory mediator generationand thrombin, neutrophil, and platelet activation.
Cardiotomy suction is also the major source ofblood trauma and hemolysis during CPB due to thesimultaneous aspiration of air and blood. For thisreason, it is important that the pump head on thecardiotomy suction turns only fast enough to allowaspiration of blood. If a sucking sound is heard fromthe cardiotomy, sucker aspiration of air is occurringand the pump head rotation should be slowed.
Vent lineVenting is intended to prevent blood from collectingin the ventricles during CPB. When blood collectsin the ventricles, distension of the ventricles andwarming of the heart may occur. Distension causesmechanical damage to the heart from subendo-cardial compression and also compromises surgicalexposure. The risk of distension is greatest whenthe blood return to the right or left heart is highand when the ventricles are no longer effectivelyejecting blood. As CPB commences, bradycardia,ventricular fibrillation, or asystole may occur andprevent effective ventricular ejection. Myocardialhypothermia during cardioplegic arrest will be com-promised by warm blood collecting in the ventriclesduring aortic cross-clamping in the unvented heart.
Figure 10.9 illustrates the most common causesof continued blood return to the right and left

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 334 — #12
334 Chapter 10
Bronchial
Leftatrium
Leftventricle
Aorta
Coronary
Thebe
sian
Pul
mon
ary
arte
ry
Rightventricle
Rightatrium
Fig. 10.9 Potential sources of continued blood flow toright and left heart during cardiopulmonary bypass(CPB). Bronchial flow is derived from aorta and returnsto left atrium. Coronary blood flow returns to the rightatrium via coronary sinus but variable proportions mayreturn to the left atrium and ventricle via thebesian veins.Shunt is seen between the aorta and pulmonary artery.This shunt may be anatomical (patent ductus arterious)or surgical (Blalock–Taussig, Potts, Waterston). Finally,aortic regurgitation may be responsible for blood flowinto left ventricle on CPB before aortic cross-clamping.
ventricles after institution of CPB with all IVC andSVC return diverted to the circuit. Blood flow to theright heart during CPB usually is the result of coro-nary blood flow. Most coronary blood flow comesfrom coronary arteries and their collaterals. A smallportion comes from noncoronary collaterals, usu-ally of pericardial and mediastinal origin. Coronaryvenous blood returns to the coronary sinus, whichis located near the junction of the IVC and the RA.Coronary sinus return can be captured by a prop-erly positioned single cannula or with separate IVCand SVC cannulas with the tourniquets loosened.For procedures in which the right heart is opened,coronary sinus blood can be captured with the car-diotomy suction. Coronary sinus blood flow (except
that contributed by noncoronary collaterals) willcease when the aortic cross-clamp is applied andcoronary arterial blood flow ceases.
Blood flow to the left heart during CPB arisesfrom several sources. The Thebesian veins drain avery small portion of the coronary circulation intothe LA and ventricle. This flow will cease when theaortic cross-clamp terminates coronary blood flow.The bronchial veins drain into the pulmonary veinsand subsequently into the LA and ventricle. Thebronchial circulation may be very large in patientswith cyanotic heart disease. In patients with con-genital heart disease, a large portion of pulmonaryblood flow may be supplied by anatomic (patentductus arteriosus, aortopulmonary collaterals) orsurgical (Blalock–Taussig, Waterston, Potts, centralshunts) systemic-to-pulmonary artery communi-cations. If these communications are not ligatedor controlled before institution of CPB, the bloodreturn to the PA, and subsequently to the LA andLV, may be very large. In this circumstance ventingwill relieve left heart distention. However, unlessCPB flow rate is increased by an amount equal tothe vented blood systemic oxygen delivery to thepatient will be compromised. Flow return to the LValso may result from an incompetent aortic valve. Inthis instance, retrograde filling of the LV with bloodfrom the aortic cannula will occur until the aorticcross-clamp is applied.
Normally, right ventricular venting is unneces-sary because coronary sinus flow is captured bythe venous drainage system. Several sites are avail-able for left ventricular venting. The right superiorpulmonary vein provides relatively easy retrogradeaccess to the LA and the ventricle via the mitralvalve. The insertion site subsequently can be usedfor placement of a transthoracic LA pressure line.Direct venting of the left ventricular apex is possible,but this route requires careful repair and may resultin damage to the LV. Direct venting via the LA is alsopossible. The PA can be used to vent both the rightheart and the left heart. A competent mitral valvewill limit effective venting of the LV via this route.
The vent line returns blood either to the filteredcardiotomy reservoir and then to the venous reser-voir or directly to a venous reservoir that containsa filter. The vent line may be either active or passive.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 335 — #13
Management of Cardiopulmonary Bypass 335
The risk of active venting is that after the ventriclehas been emptied of blood, continued active ventingmay result in entrainment of air into the ventricu-lar cavity. In procedures in which the heart is notopened (such as coronary artery bypass grafting),this entrainment of air will require the additionalstep of evacuating air from the heart before ter-mination of bypass. Close communication betweensurgeon and perfusionist are necessary to avoid thiscomplication.
Micropore filtersMost CPB circuits are equipped with both car-diotomy and arterial microporous filters. These fil-ters remove particulate contaminants such as bone,tissue, and fat fragments from blood and preventmicro- and macro- air emboli. Screen filters aremade of a woven polyester mesh. These filters havea 30–40 µm pore size and a large working sur-face area. This pore size makes these filters usefulfor trapping both air and particulate microemboliwithout high resistance to flow or damage to cel-lular blood elements. Depth filters are composedof packed fibers of Dacron and filter by impactionof particles on their wetted surface. These filterstend to lose their air-filtering capabilities over time,cause more hemolysis, and are more damaging toplatelets.
Screen filters commonly are used on the arterialside of the circuit. The vent at the top of the filterallows air to be vented directly back to the venousreservoir so that it is not trapped in the filter. This isimportant in cases of massive air emboli, in whichthe presence of trapped air will greatly reduce thefilter surface area and allow the pressure in the filterto become high enough to translocate air across thefilter and into the arterial circulation of the patient.The arterial filter also has a bypass line so that it canbe excluded from the circuit if it becomes cloggedwith debris. A combination of depth and screenfilters is used in most cardiotomy reservoirs.
UltrafiltratorsUltrafiltrators are devices commonly added to theCPB circuit to remove excess fluid and producehemoconcentration. When used in conjunctionwith CPB, these devices produce an ultrafiltrate that
occurs as the result of a hydrostatic pressure gradi-ent across a semipermeable membrane. These arethe same devices that can be used for hemodialysiswhen they are used in conjunction with a dialysate.When used during CPB, they are commonly calledhemoconcentrators as they produce an increase inhematocrit by removing excess fluid.
These devices consist of a core of microporoushollow fibers made of polysulfone, polyamide, orpolyacrylonitrile material arranged in a bundle. Thepore size generally is 0.30–0.40 µm. Due to the pres-sure drop across the device, blood inflow must beobtained from the arterial side of the CPB circuitwhile blood outflow is diverted to the cardiotomyreservoir or venous reservoir. The ultrafiltrate iscollected in a container connected to a vacuumsource.
The ultrafiltrate is discarded and has the com-position of glomerular filtrate. The rate at whichultrafiltrate is produced is dependent on the trans-membrane pressure gradient (TMP). TMP is deter-mined by the arterial inlet pressure (Pa), the venousoutlet pressure (Pv), the absolute value of appliedsuction at the outlet (Pn), the oncotic pressure at theinlet (Pi), and the oncotic pressure at the outlet (Po):
TMP = Pa + Pv
2+ Pn − Pi + Po
2
is increased by using the regulated vacuum sourceconnected to the outlet of the device. TMP shouldnot exceed 500 mmHg.
A number of different ultrafiltration techniquesexist.
Continuous ultrafiltrationContinuous ultrafiltration (CUF) refers to ultrafil-tration occurring throughout CPB or during thoseintervals when venous reservoir volume is suffi-cient to allow it. This system would be expected toproduce hemoconcentration (Fig. 10.10).
Modified ultrafiltrationModified ultrafiltration (MUF) allows ultrafiltrationto continue after weaning from CPB. MUF allowsthe CPB circuit to remain primed while both thepatient’s blood volume and the CPB circuit contentsare hemoconcentrated. MUF may be performed

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 336 — #14
336 Chapter 10
Hemoconcentrator
Regulatedvacuumsource
Cardiotomyreservoir
Venousreservoir
From patient
Arterial filter
To patientArterialpump
Arterial filter
To patient
Hemoconcentrator
Regulatedvacuumsource
Cardiotomyreservoir
Venousreservoir
From patient
Arterialpump
Ultrafiltratecollectioncontainer
Recir.line
Membraneoxygenator
Ultrafiltratecollectioncontainer
Membraneoxygenator
Fig. 10.10 Two arrangements that allow continuous ultrafiltration (CUF), dilutional ultrafiltration (DUF), andzero-balance ultrafiltration (ZBUF) to be performed during cardiopulmonary bypass (CPB).
utilizing either an arteriovenous or veno-venoussystem. In the arteriovenous system inflow to theultrafiltrator during MUF is directly from the aor-tic cannula. Outflow from the ultrafiltrator is tothe right atrium. Blood volume is kept constant asultrafiltrate is lost by replacing it with blood fromthe CPB circuit, which passes through the ultra-filtrator before being delivered to the right atrium(Fig. 10.11). In the veno-venous system, the IVCcannula provides inflow to the ultrafiltrator withthe aid of a roller pump while outflow from theultrafiltrator is returned to the SVC cannula. Bloodvolume is kept constant as ultrafiltrate is lost byreplacing it with blood from the CPB circuit, whichpasses through the ultrafiltrator before being deliv-ered to the SVC. The end point for terminationof MUF following CPB varies from institution toinstitution and may depend on either a set timeinterval (15–20 minutes), a set hematocrit (40%)or a set volume removed (750 mL/m2). Heparinanticoagulation must be maintained during MUFwith protamine reversal of heparin initiated aftertermination of MUF.
The major advantage of MUF over CUF is thatit allows hemoconcentration to continue once CPBhas been terminated. As a result MUF normallyallows a greater degree of hemoconcentration thancan be obtained with CUF alone particularly insmall children. Some institutions utilize both CUF
and MUF, as the techniques are not mutuallyexclusive.
Use of MUF is not without potential problems.MUF use has been associated with air cavitating intothe circuit potentially increasing the risk of iatro-genic air embolism. MUF has been demonstratedto increase plasma heparin concentrations that mayrequire reevaluation of the protamine dose. MUFhas also been demonstrated to cause reductionsin plasma aprotinin, opioid, and benzodiazepinelevels. While the reductions in anesthetic agentsare generally clinically insignificant, the clinical sig-nificance of plasma aprotinin level reductions isunknown. Patient hypothermia is a potential com-plication of MUF if the system is not modified toallow warming of re-infused filtrate.
Dilutional ultrafiltration and zero-balanceultrafiltrationDilutional ultrafiltration (DUF) and zero-balanceultrafiltration (ZBUF) utilize the same system asCUF but involve high-volume ultrafiltration duringCPB in which crystalloid solution is continuouslyused to replace the ultrafiltrate in order to main-tain reservoir volume. ZBUF utilities ultrafiltrationrates of 200 mL/kg/min while DUF utilizes ratesof 40–80 mL/kg/min. These methods do not resultin hemoconcentration but may be beneficial inremoving inflammatory mediators. MUF is usually

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 337 — #15
Management of Cardiopulmonary Bypass 337
Venous reservoir
Arterial line filterclamped out and bypass
opened
Cardioplegia pump used as MUF pump(crystalloid raceway tubing removed)
MUFhemoconcentrator
Ultrafiltratecollection
Blood cardioplegia systemwarmed to 37°C
Vacuum
Monitor MUF line pressure
Rightatrium
Aorta
Oxygenator
Monitor line pressure
Arterialpump
Fig. 10.11 A typical arteriovenous modified ultrafiltration (MUF) circuit. Input to the ultrafiltrator is via the aorticcannula with warmed, hemoconcentrated blood returned to the patient via the venous cannula. Blood from the venousreservoir can also be hemoconcentrated and returned to the patient.
used in conjunction with these techniques to obtainhemoconcentration.
Circuit primeBasic prime solutions in adults are usually iso-tonic crystalloid solutions (lactated Ringer’s lactateor Plasmalyte). Some institutions add albumin tothe CPB prime to increase the oncotic pressureof a crystalloid prime and to precoat the mem-brane oxygenator so as to delay absorption of fib-rinogen with subsequent platelet activation. It hasbeen consistently demonstrated that albumin andcrystalloid primes reduce the CPB positive fluidbalance, postoperative weight gain, and providebetter preservation of platelet counts as comparedto pure crystalloid primes. No clear clinical out-come advantage associated with these differenceshas been demonstrated. Enthusiasm for increas-ing the oncotic pressure of the CPB prime withhydroxyethyl starch is tempered by the fact that itsuse compromises post-CPB hemostasis.
The volume and composition of the CPB circuitprime for pediatric patients has more importantphysiologic consequences than in adult patients.
In order to keep prime volumes, exposure of thepatient’s blood to artificial surfaces, and hemodilu-tion to a minimum, the appropriate size circuit isessential in the pediatric population. The smallestmembrane oxygenator with a reference flow ratecapable of meeting the anticipated CPB flow rates isselected. In addition, the smallest diameter venousand arterial tubing that will not impede anticipatedflow due to high resistance is selected. The tubingis kept as short as possible by positioning the CPBclose to the OR table. The volumes of various tubingdiameters per 1 foot of length are: 3/16 inch – 5 mL;1/4 inch – 9.7 mL; 3/8 inch – 21.7 mL; and 1/2 inch –38.6 mL. For infants and neonates 3/16 inch arterialand 1/4 inch venous tubing is used. With currentlyavailable technology, the smallest CPB prime vol-ume for neonatal use is approximately 300 mL.Given that the blood volume of a 4.0 kg neonateis approximately 340 mL, 100% dilution of thepatient’s blood volume is expected upon initiationof CPB (Table 10.4).
Both Ringer’s lactate solution and Plasmalytecontribute to the development of a metabolic acido-sis with initiation of CPB. Ringer’s lactate solution

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 338 — #16
338 Chapter 10
Table 10.4 Estimated blood volume (EBV) comparison.
Patient weight(kg)
Estimated bloodvolume (mL/kg)
<10 8510–20 8020–30 7530–40 70
>40 65
does this via hyperchloremia and Plasmalyte viaan increase in unmeasured anions, most proba-bly acetate and gluconate. Hemofiltration of thecircuit prime prior to initiation of CPB is aneffective method to normalize electrolyte balance(particularly potassium and pH) and reduce inflam-matory mediator concentrations. Additional com-ponents commonly added to the CPB prime aresodium bicarbonate, mannitol, calcium chloride,and magnesium.
The circuit prime volume to patient blood vol-ume ratio would be expected to decrease plasmaunfractionated heparin (UFH) levels with initiationof CPB unless an appropriate quantity of heparinis added to the CPB prime. Most institutions addUFH to the CPB prime (3–4 unit/mL of prime) toreach a CPB target UFH concentration similar to thepatient’s plasma UFH concentration.
Blood is often added to the prime to reacha target CPB hematocrit. Whole blood can beused to prevent dilution of coagulation factorsin pediatric patients. The target CPB hematocritand the degree of coagulation factor dilution thatis tolerated vary from institution to institution.Hemodilution during hypothermic CPB may beadvantageous because it offsets the increase inblood viscosity induced by hypothermia and pro-motes microvascular flow. In addition, systemichypothermia reduces whole-body and cerebraloxygen consumption 5% for each 1C decreasein body temperature allowing the reduction inoxygen delivery which accompanies reduction ofred cell mass and oxygen-carrying capacity tobe tolerated. The hematocrit (Hct) on CPB canbe accurately predicted in the following manner
when the pump is primed with an asanguineoussolution:• Estimated blood volume (EBV) is calculated usingthe patient’s weight and Table 10.4.• Patient red cell mass (RCMP)=patient hematocrit(Hct)× EBV.• Hct on CPB = RCMP/(EBV+ prime volume).
In a 4.0 kg neonate with a hematocrit of 45%,the expected CPB hematocrit would be 24% usinga 300 mL asanguineous circuit prime.
The CPB red cell mass (RCMCPB) necessaryto obtain a target hematocrit on CPB can bedetermined as follows:
RCMCPB = [(desired Hct on CPB)
× (EBVP + prime volume)] − RCMP
The volume of blood prime necessary to obtain thedesired RCMCPB will depend on whether wholeblood or packed cells are used in the prime. TheRCM of a blood product is determined by multi-plying the hematocrit of the blood product by itsvolume. Therefore, the RCM of a unit of packed cellsmight be (0.7×350 mL) or 245 mL, whereas that ofwhole blood will be (0.4× 350 mL) or 140 mL. The4.0 kg neonate described would have to the havethe CPB circuit primed with 98 mL of whole bloodto reach a target CPB hematocrit of 30%.
An ancillary method of limiting the hemodilu-tion induced by the CPB prime is the techniqueof retrograde autologous priming (RAP). This tech-nique is initiated in the 5–10 minutes just priorto commencing CPB. A 1000 mL blood collectionbag is connected to the CPB circuit and is sus-pended at a level 20 cm higher than the patient’sright atrium. The technique involves three steps.First, blood from the patient’s aorta is permitted toflow retrograde through the arterial filter displacingapproximately 300 mL of semi-sanguineous pumpprime into the collection bag. It is often necessaryto use phenylephrine to maintain a systemic sys-tolic blood pressure >100 mmHg during this phase.Next, volume in the venous reservoir is pumped for-ward through the membrane oxygenator into thecollection bag until the reservoir volume is reducedto 200 mL. At this point, additional blood from thearterial cannula is allowed to fill the venous reser-voir retrograde via the arterial filter purge line.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 339 — #17
Management of Cardiopulmonary Bypass 339
The added venous reservoir volume is then pumpedforward into the collection bag until sanguineousfluid leaves the oxygenator. This displaces approxi-mately 300 mL of semi-sanguineous prime. Finally,the collection bag in lowered and as CPB com-mences the prime solution from the venous lineis drained into the collection bag yielding an addi-tional 300 mL of prime solution. In a typical adultpatient approximately 800–1000 mL of a 1500 mLasanguineous CPB prime can be removed with thismethod. The semi-sanguineous solution in the col-lection bag can be processed via a cell-saver systemand re-infused.
Circuit coatingRecent attempts to attenuate the deleteriouseffects of blood contact with nonphysiologicsurfaces have focused on modification of CPB tub-ing and membrane surfaces. A number of CPBcoating substances are currently under investiga-tion. These include a phosphorylcholine coating,a poly 2-methoxyethylacrylate coating, a siloxane/caprolactone oligomer coating and covalent hep-arin binding via the terminal amine. To datethere is conflicting evidence as to whetherthese surface modifications reliably reduce throm-bin formation and the associated consumptionof platelets, fibrinogen, and antithrombin, allowreduced doses of heparin to be utilized, or attenu-ate complement activation and initiation of systemicinflammation.
Preparation for CPB
The anesthesiologist has several important respon-sibilities in ensuring safe preparation for CPB. Theseare described in the following sections.
Assess anticoagulationBefore use of cardiotomy suction, cannulation, andcommencing bypass, it is essential that adequateanticoagulation be obtained. Inadequate anticoag-ulation will result in thrombus formation on thecannulas during cannulation and on the oxygenatoronce CPB commences. UFH currently is the primaryanticoagulant used for CPB. UFH is an animal tissue(bovine lung, porcine intestinal mucosa) derived
mucopolysaccharide (glycosaminoglycan) that hasan antithrombin (AT)-III dependant anticoagulantmechanism of action. AT-III is responsible for bind-ing to and inactivating the serine proteases throm-bin (factor IIa), factor Xa, factor IXa, factor XIa, andfactor XIIa. AT-III is 10–20 times more efficient ininactivating thrombin and factor Xa than it is ininactivating factors IXa, and XIa, and XIIa. Bindingof AT-III to a specific pentasaccharide induces aconformation change in AT-III that enhances bind-ing to and subsequent inhibition of these serineproteases by a factor of 1000–10 000. This pen-tasaccharide is present in about a third of the10–90 mucopolysaccharide chains that compriseUFH. In combination with AT-III, any mucopolysac-charide chain containing the specific pentasaccha-ride (UFH, low molecular weight heparin (LMWH),fondaparinux) can inhibit factor Xa while onlymucopolysaccharides with the specific pentasaccha-ride and a chain length ≥18 can inhibit factor IIa.This is due to the fact that a chain lengthof at least 18 monosaccharides is necessary tolink factor IIa (thrombin) to AT-III. As a result,the anti-factor Xa/anti-factor IIa ratio of thesemucopolysaccharides is solely dependent on theirchain lengths. Essentially all the mucopolysaccha-ride chains in UFH contain >18 monosaccharideunits.
It generally is acknowledged that an activatedclotting time (ACT) in excess of 480 seconds is nec-essary to ensure adequate anticoagulation for thesafe conduct of CPB. An UFH dose does not reliablyresult in a predictable plasma UFH concentrationand that the plasma UFH concentration does notnecessarily correlate with the anticoagulant effect ofUFH. For this reason, a test such as the ACT, whichquantitates the functional anticoagulant effect ofUFH in a dose responsive fashion, must be usedprior to CPB. Hypothermia, hemodilution, plateletdysfunction, and low coagulation factor levels alsoprolong the ACT. When any of these conditions arepresent the ACT will overestimate the anti-factor IIaand anti-factor Xa effects of heparin. These condi-tions are commonly present during CPB in infantsand children.
Automated ACT determination is used in mostinstitutions. Kaolin or celite, both potent activators

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 340 — #18
340 Chapter 10
of the contact phase of coagulation, is used to initi-ate clot formation in whole blood. The two mostcommon devices automated ACT devices are theHemochron® (International Technidyne Corp.) andthe Hemotec® (Medtronic).• The Hemochron device requires placement of2 mL of whole blood into a test tube containingeither kaolin or celite and a small iron cylinder.A timer is started and the test tube is placed in thedevice where it is rotated in a nearly horizontal posi-tion within a magnetic field and heat block. The ironcylinder rolls along the bottom side of the tube untilenough clot forms to entrain it. Once the cylinderis entrained and is longer detected by the magneticfield the timer stops signaling the clotting time.• The Hemotec device requires placement of 0.4 mLof blood into each of two chambers that containkaolin or celite. Each chamber contains a flag likeplunger that can be raised vertically and allowed tofall passively. The chambers are placed in the devicecontaining a heating block. A timer is started andthe device raises the plungers in each chamber andallows them to fall. As clot forms the passive descentof the plunger is progressively inhibited. A photo-optical sensor detects descent of the plunger. Whenthe velocity of the decent of the plunger falls to apredetermined value the timer stops signaling theclotting time. The ACT is the average of the twoseparate determinations.• The Hemochron® and Hemotec® ACT determi-nations are not interchangeable. The Hemochron®
determinations are typically longer than theHemotec® determinations for a given heparin level.This difference is particularly pronounced in infantsand children.
UFH is dosed in USP units not milligramsbecause UFH preparations vary in the number ofUSP units per milligram. Generally speaking UFHis prepared as 100 USP unit/mg and packaged as1000 USP unit/mL. UFH can be dosed in two waysas follows:• Empirically. Many institutions use an age orweight based empiric protocol to determine theinitial pre-CPB dose of heparin. A typical adultdose of UFH would be 300–400 unit/kg. The largecircuit prime volume to blood volume ratio (partic-ularly in infants and children) would be expected
to decrease plasma heparin levels with initiationof CPB unless an appropriate quantity of heparinis added to the CPB prime. Most institutions addheparin to the CPB prime in a quantity sufficient(3–4 unit/mL) to give the prime volume an UFHconcentration similar to that of the patient. As aresult, 5000–10 000units are added to a 1500 mLadult prime. A typical UFH dose in children isas follows: patients <30 kg − 200 unit/kg; patients>30 kg−300 unit/kg. UFH is added to the CPB primeas follows: patients <30 kg − 2.5 unit/mL of CPBprime; patients >30 kg−3.0 unit/mL of CPB prime.• Individualized heparin dose response. Some insti-tutions make use of technology that allows thepatient UFH dose response to be determined andthe individualized UFH dose to achieve a targetACT to be administered. The two most commonlyused commercially available tests are the heparinresponse test (HRT, Hemochron®) and the heparindose-response test (HDR, Medtronic Hemotec®).These monitors will allow detection of patientswith an altered UFH dose response (those requir-ing a larger or smaller dose of UFH per kilogram toachieve a target ACT than the “average” empiricallydosed patient).
If a baseline ACT is drawn, the following factorsmust be taken into consideration:• An ACT drawn after incision will be shorter thanone drawn before incision presumably due to theprocoagulant state induced by surgical stress.• Patients on preoperative UFH infusions and thosewith factor deficiencies that impair the intrin-sic and common coagulation pathways will haveprolonged ACT.
UFH should always be given into a central line ordirectly into the heart (usually the right atrium) bythe surgeon. This is necessary to ensure that the UFHdose has reached the central circulation. The CVPport of a PA catheter or a central venous catheterworks well in this regard. The ACT should be mea-sured after UFH administration. The clinical onsetof UFH is rapid with peak arterial ACT prolongationoccurring within 30 seconds and peak venous ACTprolongation occurring within 60 seconds.
Heparin resistance, more properly called alteredheparin dose responsiveness may occur in somepatients. It is generally defined as an ACT <480

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 341 — #19
Management of Cardiopulmonary Bypass 341
seconds following administration of 500 unit/kgof UFH. Generally, a 400 unit/kg dose of UFHis effective in prolonging the ACT to more than400 seconds. Approximately 50% of patients whohave been receiving preoperative intravenous (IV)UFH therapy will have an ACT of less than400 seconds after a 400 unit/kg dose of UFH.The etiology of this resistance is unknown, anddoses of UFH as high as 1000 unit/kg may beneeded for these patients. UFH resistance hasbeen observed in elderly patients due to decreasedAT-III levels and in patients with thrombocyto-sis. Platelet factor 4 (which neutralizes heparin)may be released in excess in patients with throm-bocytosis after UFH administration. Other causesof UFH resistance include AT-III deficiency; infec-tive endocarditis, intracardiac thrombus, shock, andlow-grade disseminated intravascular coagulation.Fresh frozen plasma (FFP) (a source of AT-III) andrecombinant AT-III administration have been usedas a method of improving UFH response in patientswith documented AT-III deficiency. They have alsohas been used to reduce the UFH requirement incases in which the source of UFH resistance isunknown.
Administration of UFH for CPB may result inhypotension due to calcium binding and can betreated with calcium administration (1–2 mg/kg).If UFH is administered over 1–2 minutes and ade-quate intravascular volume is maintained, calciumadministration usually is unnecessary.
If the ACT is more than 480 seconds, no addi-tional UFH is necessary. The ACT should be checkedevery 20 minutes until CPB commences. AdditionalUFH may be necessary if an extended period of timeelapses. If the ACT is less than 480 seconds after theinitial UFH dose, additional UFH will be necessary.By constructing a UFH dose–response curve, therequired UFH dose can be determined. Most centersno longer use this cumbersome method; instead,an additional 100 unit/kg of UFH is administeredand the ACT is checked 5 minutes later. This processshould be repeated until an ACT level greater than480 seconds is reached or until the total UFH doseequals 600 unit/kg. Before reaching the 600 unit/kgdose it may be prudent to make certain that the UFHis reaching the central circulation, that the UFH is
really UFH and is not outdated, and to try a differentlot of UFH.
When the UFH dose reaches 600 unit/kg with-out an ACT of more than 480 seconds one ofthe following interventions should be undertakento increase plasma AT-III levels and improveheparin dose responsiveness: 0.015–0.03 unit/kgof FFP (1–2 units in an adult) should be admin-istered and the ACT should be rechecked, or75 unit/kg of recombinant AT-III should be admin-istered. In either case the possibility that enhancedheparin dose responsiveness will exacerbate hep-arin rebound (described later) and contribute topost-CPB bleeding must be kept in mind.
If the ACT is still less than 480 seconds,additional UFH in 100 unit/kg increments shouldbe administered. In patients deemed to be athigh risk for UFH resistance, it is best to begin theheparinization process as early as possible so thatthe commencement of CPB will not be undulydelayed.
Arterial cannulationArterial cannulation generally occurs before venouscannulation. Prior placement of the arterial can-nula allows prompt commencement of CPB if severehemodynamic compromise occurs with venouscannulation. The arterial cannula usually is placedin the ascending aorta via an aortotomy encir-cled by two purse-string sutures after adequateheparinization has been obtained. Transesophagealechocardiography (TEE) may be useful in guid-ing cannula placement. Arterial blood pressure andaortic wall tension must be carefully controlled toavoid a hematoma or intimal dissection at the can-nulation site. Generally, a systolic blood pressureless than 100 mmHg or a mean blood pressure lessthan 60–70 mmHg is satisfactory. It may be neces-sary to use vasodilator therapy to accomplish this.The anesthesiologist should aid the surgeon in visu-ally examining the arterial cannula and arterialinflow line for air bubbles after they are connectedand before bypass commences. These bubbles mustbe eliminated before bypass starts by disconnect-ing the cannula and the inflow line, holding themupright, and tapping them with clamps. This allowsthe bubbles to float upward, where they can be

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 342 — #20
342 Chapter 10
flushed out before the inflow line and cannula arereconnected.
Obstruction of the lumen of the aorta may occurif the cannula is introduced too far into the aorta.Because the arterial cannula is relatively largeas compared to the aorta in infants and neonates,complete or partial obstruction of the aorta by thecannula itself is possible. Constant vigilance is nec-essary to avoid this problem. If dampening of thearterial trace, distension of the systemic ventricle, oran increase in CPB line pressure occurs with place-ment or manipulation of the arterial cannula, thesurgeon should immediately be made aware of thesituation so the cannula can be repositioned.
Venous cannulationPlacement of the venous cannula requires that thesurgeon manipulate the right atrium and potentiallythe IVC and SVC. This manipulation may result incompromise of venous return to the heart as well asa variety of atrial dysrhythmias such as atrial prema-ture beats, atrial fibrillation, or atrial flutter. Theseperturbations may result in hemodynamic compro-mise. For this reason, it is essential that the internalcardioversion paddles be on the surgical field, readyto be synchronized before atrial cannulation com-mences. Placement of the venous cannula also mayresult in rapid blood loss. This blood can be collectedwith the cardiotomy suction and rapid transfu-sion of prime solution can occur via the arterialcannula.
TemperatureVarious sites are available for monitoring body tem-perature. The core is considered to be the well-perfused organs; the shell is an intermediate areathat consists mainly of less well-perfused muscleand fat. Shell temperature will lag behind coretemperature during cooling and rewarming. Homo-genous cooling and rewarming should result in aminimal temperature gradient between core andshell temperature.
Tympanic membraneThis is a core temperature site. These probes pro-vide close correlation to the temperature at the baseof the brain during cooling and rewarming and to
actual brain temperature during stable hypother-mia. These probes are associated with minimal riskof tympanic membrane damage.
EsophagusThis is a core temperature site. During rapid cool-ing and rewarming and during CPB, temperaturemeasurements in the esophagus must be interpretedwith caution. Because of their proximity to themediastinum, probes in the esophagus will reflectchanges in the CPB perfusate temperature and thetemperature of blood or fluid in the pericardialspace not detected in other core sites. Esophagealtemperatures will fall quickly during cooling andrise rapidly during rewarming and may not accu-rately reflect the patient’s temperature in othercore sites. The blood temperature, as measured bythe PA catheter, closely approximates esophagealtemperature. The reliability of PA catheter tem-perature monitoring on CPB is limited becausethere is little or no pulmonary blood flow atthis time.
NasopharyngealThese probes, like tympanic membrane probes, pro-vide close correlation to the temperature at thebase of the brain during cooling and rewarm-ing and to actual brain temperature during stablehypothermia. There is little risk associated withplacement of these probes and, as a result, thissite is preferred by many institutions to the tym-panic membrane. This site is not influenced by acutechanges in mediastinal temperature changes andwill more closely reflect actual core temperaturechanges.
Rectum and urinary bladderRectal temperature is not a core temperature but ameasure of shell temperature. Bladder temperatureand rectal temperature correlate closely. High urineoutput creates closer correlation between bladdertemperature and core temperature. Temperaturechanges in the rectum and bladder will lag behindtemperature changes in the core sites. These probesare therefore very useful in determining whetherthe core and shell temperatures have equilibratedafter cooling and rewarming.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 343 — #21
Management of Cardiopulmonary Bypass 343
Temperature monitoring in association with CPBand particularly DHCA is of paramount impor-tance given that hypothermia prior to and duringCPB and DHCA and the avoidance of hyperthermiaafter CPB and DHCA are the mainstays of cere-bral protection. It has been demonstrated clinicallyin association with DHCA that core temperaturemonitoring sites (esophagus, tympanic membrane,nasopharyngeal, and PA) track brain temperature.However, temperature at these sites differs fromtrue brain temperature by several degrees, some-times overestimating and sometimes underestimat-ing true brain temperature. None of these sitesconsistently and accurately measures brain tem-perature. Shell sites, such as rectum and bladder,may be useful in assuring homogenous somaticrewarming but perform poorly as measures of braintemperature. It is prudent then to use temperaturereadings from multiple sites (both core and shell)during cooling and rewarming.
Baseline assessment of the pupilsThe pupils should be checked for symmetry, and anyasymmetry due to iridectomies or the like should benoted.
Commencing CPB
The anesthesiologist must work in concert with theperfusionist and the surgeon to ensure that CPBcommences smoothly. The anesthesiologist mustremain alert to help solve problems.
Assess venous drainageWhen the clamps are taken off the venous line,there should be continuous flow of venous bloodfrom the venous cannula(s) into the pump reser-voir. If this does not occur, the venous line must beexamined for air lock, residual clamps, or mechan-ical obstruction of the cannula due to malposition.The surgeon and perfusionist must be alerted if theyare not aware of the situation. The head and neckshould be assessed for adequate venous drainage,and the pupils should be rechecked for symmetry.Poor SVC drainage will result in engorgement andcyanosis of the head and neck. If poor SVC drainageis suspected, the surgeon should be alerted so that
the cannula can be repositioned. Measurement ofthe pressure in the SVC (not the RA) is useful indetecting poor SVC drainage. The monitoring sitemust be cephalad to the SVC lumen of a two-stage venous cannula or cephalad to the tourniquetaround the SVC cannula when the SVC is cannu-lated separately. This can be accomplished by trans-ducing the side port of the PA catheter introducer ora catheter in the SVC. PA catheters migrate furtherout into the pulmonary arterial system during CPBand ventricular apical retraction. The PA cathetershould be pulled back 5 cm as CPB commences toprevent it from lodging in the wedge position.
Assess arterial inflowWhen the pump head begins to turn, there shouldbe continuous flow of the crystalloid prime followedby oxygenated blood into the aorta. The arterialwaveform will take on a nearly nonpulsatile flat lineform punctuated by intermittent small pulsations asthe LV ejects its small residual volume. When anextremely low (<30 mmHg) or nonexistent pres-sure is observed as CPB commences, dissection atthe site of aortic cannulation must be excludedimmediately. It is heralded by dilation and bluishdiscoloration of the cannulated vessel, a reductionin arterial pressure, and an increase in the pumpline pressure. An aortic dissection requires immedi-ate attention. The dissection site must be repairedand an alternate cannulation site must be found.
Misdirection of the aortic cannula into one ofthe arch vessels should be assessed as CPB com-mences. A high arterial perfusion line pressureis likely to result but is not uniformly observed.If the subclavian or innominate artery is cannu-lated, the blood pressure measured in the ipsilateralradial artery will be abnormally high with wider-than-normal pulsations, whereas that measuredin the contralateral radial artery will be abnor-mally low (below 30 mmHg). Cannulation of eithercarotid artery will result in an abnormally low pres-sure, regardless of which radial artery pressure isbeing monitored. Unilateral otorrhea, rhinorrhea,conjunctival edema, facial edema, and facial cold-ness are later signs of arch vessel cannulation andare the result of cerebral overperfusion. Misdirec-tion has been reported into the innominate artery;

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 344 — #22
344 Chapter 10
left subclavian artery, and left carotid artery. If mis-direction is suspected, immediate action to correctthe placement is necessary.
The risk of misdirection of the arterial cannulainto one of the arch vessels is higher in reopera-tive procedures because the surgeon may need tocannulate the aorta higher to avoid the previouscannulation site. TEE is not reliable in visualizingthe ascending aortic cannulation site due to theblind spot created by the trachea and bronchus.However, longitudinal plane imaging reliably allowsvisualization of the left subclavian and left carotidarteries. In conjunction with color flow Dopplerimaging, it is possible to detect preferential direc-tion of the jet of blood out of the cannula into oneof these arteries. Some centers utilize NIRS and TCDtechnology as adjunctive methods to assess cerebralblood flow during CPB.
Assess oxygenator functionAfter CPB has commenced the oxygenator func-tion must be rapidly assessed. There should beimmediate visual assessment of bright red bloodleaving the oxygenator. Infrared oxygen satura-tion monitors on the venous and arterial lines willverify that the blood leaving the oxygenator is satu-rated with oxygen. Optical fluorescence technologyallows on-line monitoring of both venous and arte-rial PO2, PCO2, and pH. Blood gas analysis is rou-tine and will provide information on oxygenation,carbon dioxide elimination, and acid-base status. Ifarterialized blood does not leave the oxygenator, itmust be assessed immediately for malfunction. Themost likely cause of failure is an inadequate supplyof fresh gas to the oxygenator from a flow metermalfunction, gas line switch or gas line leak.
Inadequate arterial oxygenation also may occurif the maximum flow capacity of the oxygenatoris exceeded. Inadequate arterial oxygenation mayoccur at flow rates less than the maximal flow capac-ity if a very low mixed venous saturation existsas bypass commences. The most common causesof a low mixed venous oxygen saturation as CPBcommences are as follows:• Low pre-bypass cardiac output.• Oxygen consumption that is abnormally high dueto shivering, light anesthesia, or hyperthermia.
• The surface area of the oxygenator is toosmall to meet the metabolic demands of a largepatient.
Discontinue ventilationVentilation should be discontinued after bypasshas commenced unless partial CPB is initiated anda significant volume of blood continues to flowthrough the pulmonary arteries. Complete collapseof the lungs provides optimal surgical exposure,whereas continuous positive airway pressure poten-tially inhibits exposure and has no proven benefit inthe post-CPB period.
Assess need for ventingThe anesthesiologist can aid the surgeon in the deci-sion to vent by observing the right and left heart fordilation with TEE and by examining the RA and pul-monary artery pressure traces on CPB. An elevationof the RA pressure suggests continued blood returnand dilation of the right heart. An elevation of thePA pressure suggests left ventricular distension withmitral valve incompetence and retrograde flow ofblood into the PA.
Supplement neuromuscular blockadeIt is important to administer a muscle relaxantas CPB commences to prevent the large increasesin systemic oxygen consumption that accompanyshivering and to prevent the diaphragmatic move-ment that compromises surgical exposure duringthe operative procedure. The effect of hypothermicCPB on nondepolarizing neuromuscular blockadeis complex. Hypothermic CPB in the absence ofneuromuscular blockade enhances electrochemicalneuromuscular transmission, assessed by electro-myogram (EMG) but attenuates mechanical func-tion, assessed by twitch tension development.Clinically, the goal is attenuation of the mechani-cal response with neuromuscular blocking agents.Vecuronium neuromuscular blockade as assessedby twitch tension is enhanced and prolonged byhypothermic CPB, whereas pancuronium neuro-muscular blockade as assessed by twitch tension isunaltered.
From a practical point of view, any of thenondepolarizing muscle relaxants can be utilized

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 345 — #23
Management of Cardiopulmonary Bypass 345
to ensure muscle relaxation during CPB. It hasbeen demonstrated that pancuronium require-ments are increased at the initiation of CPB andduring rewarming. Presumably, hemodilution atthe onset of CPB reduces the plasma concentra-tion of neuromuscular blocking agents, whereasrewarming reverses hypothermia-induced depres-sion of twitch tension development. Pancuronium0.05 mg/kg at the start of CPB, followed by pan-curonium 0.01 mg/kg/h while on CPB, is sufficient.When DHCA is used, a large enough dose of relaxantto last the entire arrest period must be administeredat the outset.
Conduct of CPB
After CPB has commenced, the perfusionist assumesprimary responsibility for its safe conduct with thecooperation of the surgeon and anesthesiologist.It is necessary to be familiar with the effects ofCPB on various organ systems to make rationalmanagement decisions.
TemperatureCPB is most commonly conducted in conjunctionwith systemic hypothermia. Systemic hypother-mia reduces systemic oxygen consumption andreduces cerebral oxygen consumption. Q10 definesthe ratio of oxygen consumption at a definedtemperature to the oxygen consumption at tem-perature 10C lower. Systemic Q10 is approxi-mately 2.5, whereas cerebral Q10 is approximately2.1–3.5. Reductions in oxygen consumption per-mit reductions in oxygen supply to be tolerated.Levels of hypothermia have been defined as fol-lows: mild (32–35C), moderate (26–31C), deep(20–25C), and profound (<20C). Unfortunately,not all authors adhere to this classification and caremust be taken when comparing data from studies.For instance, it is not uncommon for temperatures<20C used in conjunction with pediatric cardiacsurgery to be called “deep hypothermia”.
Normothermic CPB for CABG surgery is utilizedin some institutions. When normothermic CPB isconducted so as to avoid inadvertent cerebral hyper-thermia there is no difference in cognitive outcomeas compared to hypothermic CPB in CABG patients.
Systemic blood flowSystemic blood flow on CPB can be varied instan-taneously and is determined by the rate of arterialpump head rotation. In the steady state, systemicblood flow and venous return must be equal, just asthey are in the intact circulatory system. If venousreturn is compromised for any reason, then systemicblood flow may transiently exceed venous returnand the volume of blood in the venous reservoirwill diminish. As the volume of blood in the venousreservoir falls, the perfusionist must decrease sys-temic blood flow by decreasing the speed of pumprotation. Simultaneously, volume is added to thevenous reservoir while the source of compromisedvenous return is aggressively pursued and cor-rected. If the venous reservoir is inadvertentlyemptied, massive arterial air embolization mayoccur. This disastrous complication is preventable inseveral ways:• Vigilance on the part of the perfusionist andanesthesiologist.• Level sensors on the venous reservoir that soundand/or shut down the arterial pump head when apredetermined reservoir volume is reached.• Bubble sensors on the arterial perfusion line thatshut down the arterial pump head before massivetransfusion of air occurs.
Optimal flow rates for CPB have yet to bedefined clearly, although the goal is to maintainsystemic and cerebral oxygen delivery. Flows of2.0–2.4 L/min/m2 are used for infants, children, andadults during mild to moderate systemic hypother-mia. Due to age-related differences in the relation-ship of surface area to weight, these flow ratesexpressed in milliliters per kilograms per minutewill be substantially higher in the neonate thanin the adult. The recommended full flow ratesfor CPB are summarized in Table 10.5. Low flowCPB in neonates and infants conducted in con-junction with temperatures of 18–25C is gener-ally defined as 50–70 mL/kg/min or approximately1.0–1.5 L/min/m2. Flows as low as 1.2 L/min/m2
will not compromise whole-body oxygen deliverywhen moderate systemic hypothermia is employed.At such low flow rates, with higher temperature,systemic oxygen delivery is maintained by increasedperipheral extraction of oxygen. Because low mixed

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 346 — #24
346 Chapter 10
Table 10.5 Full cardiopulmonary bypass (CPB) flowrates.
Patientweight(kg)
Full CPBflow rates(mL/kg/min)
<3 150–2003–10 125–17510–15 120–15015–30 100–12030–50 75–100>50 50–75
venous oxygen saturations result, oxygen deliveryreserve is compromised.
To improve surgical exposure during complexintracardiac repairs and arch reconstructions inneonates and children and during aortic archrepairs in adults, DHCA may be used. DHCA allowscessation of blood flow, cannula removal, andexsanguination of the patient into the venous reser-voir. DHCA has been studied most extensively inpediatric patients.
Systemic blood pressureMean arterial pressure (MAP) on CPB is deter-mined by the relationship between pump flow andsystemic vascular resistance (SVR):
SVR = [(MAP− CVP)× 80]/pump flow rate
Recall that the CVP on CPB with adequate venousdrainage will be zero and that 80 is a conversionfactor (Wood units to dynes s/cm5). For a givenSVR, the MAP can be instantaneously increased ordecreased by increasing or decreasing pump flow.Likewise, the perfusionist is able to maintain MAPwhen acute increases or decreases in SVR occurby decreasing or increasing pump flow. It is notuncommon for MAP to decrease to 30–50 mmHgas CPB commences despite pump flow rates of2.0–2.4 L/min/m2 or approximately 4 L/min in a70-kg patient.
This is due, in part, to the enormous decrease inviscosity that occurs when the patient’s blood vol-ume and the asanguineous prime first mix. Viscos-ity, as discussed previously, is a major determinant
of SVR. Several other factors have been identifiedwhich influence SVR on CPB:• Temperature. The incidence of low SVR is signifi-cantly higher during normothermic compared withhypothermic CPB. This may be caused by vaso-constriction induced by hypothermia or release ofvasodilator substances during normothermia. Longperiods of rewarming during reperfusion also seemto contribute to low SVR.• Age and peripheral vascular disease. Older patientsand patients with peripheral vascular disease are lesslikely to exhibit low SVR during CPB secondary toa less compliant arterial system.• Diabetes mellitus. Diabetics are less likely toexhibit low SVR during CPB secondary to coexist-ing vascular disease, sympathetic neuropathy withnear maximum vasodilation at rest, and reducedbaroreceptor sensitivity.• Left ventricular function. Patients with LV ejectionfraction (EF) < 40% are less likely to exhibit lowSVR during CPB. These patients tend to be receivingvasodilator therapy to improve systolic function andmay have near-maximal vasodilation at rest.
Cerebral blood flowThe control of cerebral blood flow on CPB is depen-dent on several factors, as described in the followingsections.
Cerebral autoregulationCerebral blood flow autoregulation is altered byhypothermic nonpulsatile CPB. Cerebral blood flowis autoregulated between MAP values of 30 and110 mmHg during CPB in patients without cere-brovascular disease or preexisting hypertension.In contrast, in the intact circulation of normal,nonhypertensive patients, cerebral blood flow isautoregulated between MAP values of 50 and150 mmHg. Unfortunately, there are no data on thelower limit of cerebral autoregulation on CPB inpatients with coexisting cerebrovascular disease. Itmay be prudent to maintain a slightly higher MAP(higher than 50 mmHg) on CPB in patients withknown cerebrovascular disease although there is noevidence to support or refute this recommendation.
Aging has not been shown to have an effecton cerebral autoregulation during CPB. Diabetics

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 347 — #25
Management of Cardiopulmonary Bypass 347
appear to have impaired cerebral autoregulationduring CPB. Cerebral autoregulation is lost andcerebral vascular responses to PaCO2 are attenuatedunder conditions of deep (18–20C) hypothermiaCPB in infants and children. This is felt to be due tocold induced vasoparesis.
Acid-base managementElectrochemical neutrality is important in preserva-tion of cellular protein and enzyme structure andmaintenance of the constant transcellular hydro-gen (H+) ion gradient necessary for many cellu-lar processes. In addition, optimal functioning ofthe imidazole buffering system is dependent onmaintenance of cellular electrochemical neutrality.The imidazole group of the amino acid histidineis present on many blood and cellular proteinsand is an important buffer. Electrochemical neu-trality occurs when there are equal concentrationsof hydroxyl (OH−) and hydrogen (H+) ions. Astemperature decreases, the dissociation constant(pK) of aqueous systems such as those found incells increases. This process results in a reduc-tion in the concentrations of OH− and H+ ionsas temperature decreases. If there are equal con-centrations of OH− and H+, then electrochemicalneutrality will be maintained. Recall that pH is theinverse log of the H+ ion concentrations; as theH+ ion concentration decreases, pH increases. Thus,for electrochemical neutrality to be maintained,pH must increase as temperature decreases. In anelectrochemically neutral cell at 37C, the measured
pH will be 7.40, whereas in an electrochemi-cally neutral cell at 20C, the measured pH willbe 7.80.
Changes in cellular pH during hypothermia aremediated through PaCO2 homeostasis. As temper-ature decreases, the solubility of carbon dioxide inblood increases. If the total carbon dioxide contentof blood is held constant, this increase in carbondioxide solubility will result in a reduction in PaCO2.For example, if the total carbon dioxide content isheld constant and the measured PaCO2 at 37C is40 mmHg, then the measured PaCO2 at 20C willbe 16 mmHg. This situation causes pH to increaseas temperature decreases and electrochemicalneutrality to be maintained.
pH-Stat and α-stat regulation are acid-base man-agement methods that directly influence blood flowto the brain and other organs. Although pH-stat andα-stat acid-base management commonly are men-tioned in association with temperature-correctedand temperature–uncorrected blood gases, it mustbe emphasized that these are entirely differentconcepts. The method of blood gas interpreta-tion (corrected or uncorrected) does not dictatethe method of acid-base management (pH-stat orα-stat). In fact with the use of Table 10.6, α-stator pH-stat management is possible with use ofboth temperature-corrected and uncorrected bloodgases. In addition, is important to point out that ata patient temperature of 37C there is no differ-ence between pH-stat and α-stat management. Thedifference between these two strategies becomes
Table 10.6 Alpha-stat versus pH-stat acid-base management.
Patienttemp.(C)
Temperature uncorrected Temperature corrected(reported at 37C) (reported at patient temperature)
α-statpH
pH-statpH
α-statPCO2
pH-statPCO2
α-statpH
pH-statpH
α-statPCO2
pH-statPCO2
37 7.40 7.40 40 40 7.40 7.40 40 4033 7.40 7.34 40 47 7.44 7.40 35 4030 7.40 7.30 40 54 7.50 7.40 29 4027 7.40 7.26 40 62 7.55 7.40 26 4023 7.40 7.21 40 74 7.60 7.40 22 4020 7.40 7.18 40 84 7.65 7.40 19 4017 7.40 7.14 40 96 7.69 7.40 17 40

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 348 — #26
348 Chapter 10
more marked as patient temperature progressivelydecreases below 37C and is not clinically relevantuntil patient temperature <30C (see Table 10.6).
When a blood gas sample is drawn from a patientat 25C and sent to the blood gas laboratory, thesample is warmed to 37C before measurement. Thevalues obtained at 37C are called the temperature-uncorrected values. These values are converted totemperature-corrected values using a nomogram.The nomogram accounts for temperature-inducedchanges in pH, oxygen solubility, and carbon diox-ide solubility in a closed-blood system. When pHand PaCO2 are measured at 37C and then correctedto a lower temperature, the electrochemically neu-tral pH will be higher and the corrected PaCO2 willbe lower than the normal values at 37C. Therefore,electrochemical neutrality is maintained by keepingpH alkalotic in temperature-corrected blood gasesand normal in temperature-uncorrected gases. Thisis known as α-stat regulation. For practical pur-poses, it is easier to use uncorrected gases and keeppH and PaCO2 in the range considered normal at37C. Cerebral blood flow and oxygen consumptionare appropriately coupled when α-stat regulation isused. Deep hypothermia in the presence of α-statregulation produces loss of cerebral autoregulationsuch that cerebral blood flow varies directly witharterial pressure.
pH-Stat regulation refers to maintaining pHand PaCO2 at normal values for 37C whentemperature-corrected gases are used and at acidoticvalues when temperature-uncorrected gases areused. pH stat is maintained by adding carbon diox-ide to the ventilating gas during hypothermic CPBto increase PaCO2 and decrease the pH. In contrast toα-stat regulation, in which total carbon dioxide con-tent is kept constant, pH stat regulation results in anincrease in total carbon dioxide content. The cere-bral vasculature maintains vasomotor responsesto varying PaCO2 during hypothermic CPB. Thisresponse is maintained during moderate hypother-mia and is attenuated during deep hypothermiadespite the fact that deep hypothermia inducesloss of cerebral blood flow autoregulation. WhenpH-stat regulation is used with moderate hypother-mic CPB, there is uncoupling of cerebral blood flowand metabolism and loss of cerebral autoregulation.
As a result, cerebral blood flow varies linearly witharterial blood pressure and cerebral hyperperfu-sion exists with cerebral blood flow far in excessof that dictated by cerebral metabolic rate. Thishyperperfusion state is the result of reduced cerebraloxygen consumption induced by hypothermia andcerebral vasodilation resulting from a dispropor-tionately high PaCO2 for the degree of hypothermiapresent. The potential danger of the hyper-perfusedstate is increased delivery of microemboli into thecerebral circulation.
Clinical trials in adults suggest that use of α-statmanagement during normothermic or hypothermicCPB results in improved cognitive outcome follow-ing cardiac surgical procedures. The question as towhether pH-stat or α-stat management should beutilized during DHCA in adults is a source of debate.In infants and children, pH-stat management isgenerally initiated once the perfusate temperature<28–30C.
Pump flow ratesCerebral blood flow and oxygen delivery are main-tained with flow rates as low as 1.0 L/min/m2 andperhaps as low as 0.5 L/min/m2 when moderatelyhypothermic CPB (26–29C) and α-stat regulationare used. There is preferential distribution of bloodflow to the brain when low pump flows are used.Despite this, cerebral oxygen delivery at these flowsis maintained at the expense of increased cerebralextraction of oxygen and decreased jugular venousoxygen saturation. In addition, despite the fact thatsomatosensory neural transmission remains intactwhen moderate systemic hypothermia is used andpump flow is reduced to 0.5 L/min/m2, signifi-cant cerebral lactate accumulation develops after15 minutes.
Low flow rates are used most commonly in con-junction with pediatric open-heart procedures toimprove surgical exposure. In neonates, infants,and children, cerebral blood flow and cere-bral metabolism are unaffected by reductions inconventional pump flow rates less than 45%.When conventional flow rates (150 mL/kg/min forneonates and 100 mL/kg/min for infants and chil-dren) are reduced 45–70% at moderate hypother-mia (26–29C) with α-stat acid-base management,

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 349 — #27
Management of Cardiopulmonary Bypass 349
cerebral blood flow and metabolic rate decreasewith a compensatory increase in oxygen extrac-tion. Similar reductions during deep hypothermia(18–22C) do not produce increased oxygen extrac-tion. Minimal acceptable low flows on CPB forpediatric patients are not yet clearly defined, butcellular oxygen debt occurs at 5–30 mL/kg/min at18C and at 30–35 mL/kg/min at 28C. In neonatescooled to 18C, cerebral blood is detectable in themiddle cerebral artery by TCD as long as CPB flowrate is at least 30 mL/kg/min.
Myocardial blood flowOn CPB, the coronary ostia are provided withhemodiluted, nonpulsatile blood flow until the aor-tic cross clamp is applied. Aortic cross-clamping forcardiac surgery involves placing a completely occlu-sive clamp across the ascending aorta between theaortic cannula and the aortic valve, such that thecoronary circulation is excluded from the CPBcirculation. Aortic cross-clamping has evolved asthe method of choice for providing an immobile,bloodless field for the cardiac surgeon. Depend-ing on the operative procedure and technique,variable periods of time may pass from theonset of CPB until placement of the aortic cross-clamp. It is therefore necessary to be famil-iar with the effects of CPB, hemodilution, andhypothermia on myocardial oxygen delivery anddemand.
Myocardial oxygen deliveryMyocardial oxygen delivery is the product of coro-nary blood flow and the oxygen-carrying capac-ity of the blood. Coronary blood flow in turn isdependent on the pressure gradient between theaorta and the myocardial tissue. For the subendo-cardium, the tissue most likely to be hypoperfused,this gradient is equal to the MAP minus the rightor left ventricular intracavitary pressure. The fac-tors described in the following sections play a majorrole in determining oxygen and substrate delivery tothe myocardium, particularly the subendocardium,during CPB.• Coronary stenoses. Due to the pressure dropacross stenoses, perfusion to the area suppliedby the stenosed artery will be compromised if
MAP is reduced. Therefore, whereas cerebral bloodflow can be maintained with perfusion pressuresas low as 30 mmHg, myocardium supplied bystenosed arteries is poorly perfused at this pressure.Such low perfusion pressures should not be toler-ated for more than a few minutes in patients withcritical stenoses. Subendocardial ischemia in the dis-tribution of a critical coronary stenosis is avoidedif MAP is maintained at 80 mmHg in the beat-ing empty heart. However, subendocardial ischemiais inevitable in the distribution of a critical coro-nary stenosis when ventricular fibrillation existsdespite maintenance of MAP. This ischemia is seento develop after as little as 15 minutes of ven-tricular fibrillation with MAP values as high as80 mmHg.• Ventricular distension. Ventricular distentionmarkedly elevates intracavitary pressure and com-promises subendocardial perfusion for a given MAP.The causes of ventricular distension have been dis-cussed previously. If ventricular distension is likelyto persist, then ventricular venting is necessary.Ventricular distension can be terminated promptlywhen aortic insufficiency exists by placing the aorticcross-clamp.• Ventricular fibrillation. As systemic cooling onCPB progresses, the heart becomes progressivelymore bradycardic. When the temperature of theheart reaches approximately 28C, coarse ventric-ular fibrillation ensues and myocardial wall tensionincreases. As the temperature of the heart contin-ues to drop, the ventricular fibrillation becomesfiner, myocardial oxygen consumption decreases,and ventricular wall tension diminishes. Ven-tricular fibrillation, particularly in hypertrophiedmyocardium, results in poor perfusion of the sub-endocardium due to increased myocardial walltension and a reduced perfusion gradient. Whenthe MAP is less than 50–60 mmHg, subendocardialperfusion will be compromised when ventricularfibrillation exists.• Hemodilution. In the presence of adequate perfu-sion pressures, myocardial oxygen delivery is poten-tially compromised by the reduced oxygen-carryingcapacity of the hemodiluted systemic perfusatedespite the fact that the decreased temperatureallows more oxygen to be carried in solution.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 350 — #28
350 Chapter 10
Oxygen delivery to the nonhypertrophied ejectingmyocardium is unlikely to be compromised unlessthe Hct is less than 15%. In the presence of coro-nary stenoses or concentric hypertrophy, Hct valuesin the 20–30% range may be needed to preventischemia during normothermic CPB.• Hypothermia. Hypothermia reduces coronaryvasodilator reserve capacity and potentially lim-its myocardial oxygen delivery. Therefore, despitethe fact that hypothermia reduces myocardialoxygen consumption (described later), subendocar-dial ischemia develops in the beating, empty heartwhen MAP is lower than 50 mmHg at 28C due toattenuated coronary vasodilator reserve.
Myocardial oxygen demandCPB provides a state of hypothermic, hemodiluted,nonpulsatile flow during which the heart is calledupon to do little or no mechanical work in the formof generating pulsatile flow. The two major deter-minants of myocardial oxygen consumption on CPBare temperature and the functional status of themyocardium.• Temperature. As Fig. 10.12 illustrates, the lowerthe temperature of the heart, the less oxygen it
6.0
4.0
2.0
cc/1
00 g
/min
0
37°C 32°C 28°C
Beating nonworkingFibrillatingArrest
22°C
Fig. 10.12 Left ventricular oxygen consumptionduring three functional states (beating empty, fibrillating,and arrested) and at four temperatures. Hypothermiaclearly reduces myocardial oxygen consumption for anyfunctional state. Below 37C, the beating empty heartconsumes the most oxygen, followed in decreasingorder by the fibrillating and arrested heart. (FromBuckberg GO, et al. Studies on the effects ofhypothermia on regional myocardial blood flow andmetabolism during cardiopulmonary bypass I. Theadequately perfused beating, fibrillating, and arrestedheart. J Thorac Cardiovasc Surg 1977;73:89, withpermission.)
consumes per minute for a given functional state.For the beating empty heart, oxygen consump-tion per beat increases as temperature decreasesdue to the positive inotropic effect of hypother-mia on the myocardium. However, this increase inoxygen consumption per beat is overshadowed bythe larger relative decrease in heart rate inducedby cold, such that oxygen consumption per minutefalls.• Functional status. The functional status of themyocardium whether beating and empty, fibril-lating, or arrested plays an important role indetermining myocardial oxygen consumption (seeFig. 10.12). Below 37C, the heart consumes lessoxygen fibrillating than it does beating and empty.Recall, however, that subendocardial perfusionis compromised by fibrillation due to increasedwall tension. Subendocardial perfusion will be fur-ther compromised in the un-vented fibrillating,heart.
Renal functionNormally, renal blood flow is autoregulatedbetween renal artery pressures of 80 and 180 mmHg.Despite this, systemic flows as low as1.6–1.8 L/m2/min and sustained MAP as low as50 mmHg during hypothermic, hemodiluted, non-pulsatile CPB do not result in a deterioration ofpost-CPB renal function. In addition, pH manage-ment, pulsatile versus nonpulsatile flow, and CPBtemperature do not influence renal function dur-ing or after CPB. The quantity of urine output onCPB is not a reliable predictor of post-CPB renaldysfunction. The presence of preexisting renal dys-function, post-CPB ventricular dysfunction and lowcardiac output, use of intra-aortic balloon pump(IABP), emergency operative procedures, DHCA,prolonged CPB time, valve surgery, diabetes mel-litus, and advanced age have all been identified asindependent predictors of post-CPB renal dysfunc-tion and acute renal failure. In fact, the presence ofpost-CPB ventricular dysfunction and low cardiacoutput is a major risk factor in the development ofpost-CPB renal dysfunction and failure.
Generally, a urine output of 1 mL/kg/h is con-sidered adequate while on CPB. Although urineoutput on CPB has not consistently been correlated

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 351 — #29
Management of Cardiopulmonary Bypass 351
with post-CPB renal function, oliguria (urine output<0.5 mL/kg/h) must be considered a harbinger ofrenal hypoperfusion and ischemia.
Recommendations forconduct of CPB
Lower limits of MAPThe safe lower limits of MAP on CPB must bedetermined with all organ systems in mind. If theaortic cross-clamp is applied within 1–2 minutesafter the start of CPB, a MAP greater than 30 mmHgwith a pump flow of 2.0–2.4 L/min/m2 is accept-able for patients without cerebrovascular disease.For patients with known cerebrovascular disease,a MAP in excess of 50 mmHg may be more pru-dent. If there is a delay in placing the aortic cross-clamp, then attention should be directed towardoptimal perfusion of the myocardium. A MAP ofat least 50 mmHg should be maintained for per-fusion of the beating, empty heart. If ventricularfibrillation develops and is likely to persist for morethan a few minutes, then MAP must be elevatedto at least 60–80 mmHg to ensure subendocar-dial perfusion. Likewise, if ventricular fibrillationis likely to persist, myocardial temperature shouldbe decreased to reduce oxygen consumption andimprove perfusion by lowering wall tension. A ventmust be placed if left ventricular distension occurs.If coronary stenosis or ventricular hypertrophy alsoexists, MAP must be elevated to 80–100 mmHgand the cross-clamp should be applied as soon aspossible.
If high pump flows are needed to maintain thedesired MAP, the maximal flow capacity of the oxy-genator may be exceeded. If this is likely, then SVRcan be increased and pump flow can be decreasedto maintain MAP. SVR can be increased by transfu-sion of blood into the venous reservoir to increaseviscosity. Generally, this strategy is reserved forthose instances in which the Hct is less than 20%.SVR can also be increased by increasing arterio-lar tone. The simplest way to accomplish this is byinfusing an α-agonist such as phenylephrine intothe pump. As a rule, as CPB progresses, arteriolartone will increase and the phenylephrine can bestopped.
Upper limits of MAPGenerally, a mean arterial blood pressure less than70 mmHg is maintained to remain within the limitsof cerebral autoregulation and to reduce noncoro-nary collateral blood flow after the aortic cross-clamp has been applied. Because the noncoronarycollaterals originate from the mediastinum and peri-cardium, the blood they deliver to the heart will beat the same temperature as the patient (25–30C).While the aortic cross-clamp is in place and theheart is arrested with cardioplegia, optimal myocar-dial temperature is usually between 8C and 15C.Excessive noncoronary collateral flow will causethe heart to rewarm and compromise myocardialpreservation. Excessive noncoronary collateral flowalso will compromise surgical exposure by causingbleeding from the incised coronary artery. There areseveral strategies available to reduce MAP and eachhas its own advantages and disadvantages:• Reduction of pump flow is useful as a temporizingmaneuver, but a prolonged reduction may result insystemic and cerebral hypoperfusion.• Sodium nitroprusside is a very effective arterio-lar dilator and thus very useful in reducing SVR.It is easily titratable, has no negative inotropicproperties, and has a short half-life. It has, how-ever, been implicated in causing reversible plateletdysfunction. Nitroglycerin does not cause plateletdysfunction, is easily titratable, and has a short half-life and no negative inotropic properties but is muchless effective than nitroprusside. This decreasedeffectiveness is because nitroglycerin is primarilya venodilator and actively adheres to the plasticcomponents of the CPB circuit.• Volatile anesthetic agents such as sevoflurane,desflurane, and isoflurane are very effective, easilytitratable arteriolar dilators. The vaporizer must bespliced into the fresh gas flow line of the oxygena-tor. Caution must be exercised when CPB vaporizersare filled with inhalation agent because the plas-tic components of the oxygenator may crack ifagent is accidentally spilled on them. During CPBwith a membrane oxygenator, inhalational anes-thetic agents are completely eliminated from thecirculation 10–15 minutes after they are discontin-ued. Nonetheless, it is prudent to discontinue theseagents before removal of the aortic cross-clamp to

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 352 — #30
352 Chapter 10
allow adequate time for their elimination beforecoronary blood flow resumes if there is a concern.
Urine outputA urine output of at least 1.0 mL/kg/min is desir-able on CPB. Urine output should be assessedevery 15 minutes while on CPB. If urine out-put falls below 0.1 mL/kg/15 min (0.5 mL/kg/h),action is necessary. Aortic perfusion pressure shouldbe increased to at least 50 mmHg. If this fails toincrease urine output or if aortic perfusion pressureis already optimized consideration should be givento improving hematocrit to at least 25%. Induc-tion of diuresis with furosemide 0.5–1.0 mg/kg ormannitol 0.5–1.0 g/kg is of no proven utility butcan be considered in circumstances where exten-sive use of cardiotomy suction leads to hemolysisand hemoglobinuria. In this circumstance alkaliza-tion of the urine with sodium bicarbonate shouldalso be considered. Prophylactic administration ofdopamine or fenoldopam during CPB is of noproven benefit in improving renal function duringor after CPB.
Monitoring of anticoagulationMaintenance of anticoagulation must continue onCPB. The anticoagulant effect of UFH is prolongedby the presence of hemodilution, the anticoagulanteffect of hypothermia, and the prolonged half-lifeof UFH associated with hypothermia. Nonetheless,the anticoagulation status of the patient should bemonitored at least every 30 minutes with an ACT.More frequent ACT assessment is necessary dur-ing periods of cooling and rewarming. Care mustbe taken to ensure adequate anticoagulation duringrewarming.
Preparation for terminationof CPB
It is essential that an organized approach be takento preparing for the termination of CPB so that asmooth transition is ensured. The anesthesiologisthas a number of responsibilities as outlined below.
Ensure rewarmingAfter induced systemic hypothermia, it is neces-sary to ensure that adequate core rewarming has
occurred before termination of CPB. The perfu-sionist will assume responsibility for using the heatexchanger to rewarm the patient when instructedto do so by the surgeon. Generally, rewarmingwill take place for 30–60 minutes before termi-nation of CPB, depending on the degree of thehypothermic state and its length. As with cooling,the site of temperature measurement is impor-tant in assessing homogeneous core rewarming.Equilibration of the bladder or rectal temperatureand the nasopharyngeal temperature at 36–37C isdesired.
The rate of rewarming is important, as increasedcerebral oxygen extraction has been noted in adultsduring rapid rewarming. In the setting of constantcerebral oxygen delivery this increase in oxygenextraction results in a wider cerebral AVO2 satu-ration difference (a lower jugular venous oxygensaturation). This increase in cerebral oxygen extrac-tion during rewarming is associated with sub-sequent cognitive defects, particularly in elderlypatients. Better cognitive outcome is achieved fol-lowing coronary artery bypass surgery in adultswhen slow rewarming (2C difference betweennasopharyngeal and CPB perfusate temperature) iscompared to more standard rewarming (4–6C dif-ference between nasopharyngeal and CPB perfusatetemperature).
Enthusiasm for homogenous somatic rewarmingshould also be tempered by the fact that brain tem-perature continues to increase for at least 6 hoursfollowing CPB procedures. Postoperatively, actualbrain temperature is underestimated by esophageal,tympanic and rectal temperatures and may rise tolevels that exacerbate neuronal injury. The maxi-mum postoperative temperature as measured by aPA catheter in the first 24 hours is weakly associatedwith a greater amount of cognitive dysfunction aftercardiac surgery in adults.
Despite homogeneous core rewarming, it is notuncommon for the patient’s core temperature todrop 2–3C in the hour after termination of CPB.This is due to reperfusion of the cold extrem-ities, which results in a re-equilibration of thepatient’s temperature at a lower core temperature.The greater the difference between the nasopharyn-geal and the rectal or urinary bladder temperature

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 353 — #31
Management of Cardiopulmonary Bypass 353
when CPB is terminated, the greater will be theexpected temperature afterdrop. This temperatureafterdrop may result in arterial vasoconstriction andshivering, which will increase myocardial oxygenconsumption. Infusing sodium nitroprusside or pro-viding vasodilatation with an inhalational anes-thetic while maintaining MAP greater than or equalto 50–70 mmHg by increasing pump flow has beenadvocated as a method of decreasing afterdrop. Thismethod allows the poorly perfused cold extremitiesto be perfused with warmed blood before termina-tion of CPB. Therefore, the caloric load of peripheralrewarming is in large part assumed by the heatexchanger and not the patient. Warmed, humidifiedairway gases have not been found to be beneficialin decreasing afterdrop in adults because humidi-fiers contribute relatively little heat to the large heatdeficit that exists at the termination of CPB. The useof heat exchange systems utilizing circulating waterin pads in direct contact with the have been foundto be beneficial in preventing afterdrop in adults,infants, and children. In infants and children, con-vection systems utilizing forced warm air are usefulas well due to the larger surface-area-to-volumeratio in these patients.
Ensure adequate anesthesia andmuscle relaxationAwareness is unlikely to exist during systemichypothermia but may occur during rewarming.Unfortunately, this has not been well studied.Appropriate care dictates that some provisionfor amnesia be made as rewarming occurs.Volatile anesthetic agents may be continued dur-ing this interval to assure amnesia. A benzo-diazepine such as midazolam 0.05–0.15 mg/kg,or lorazepam 0.025–0.05 mg/kg, administered asrewarming commences, can be used. Alternatively,a propofol infusion can be initiated. A muscle relax-ant should be titrated to ensure adequate relax-ation as the hypothermic attenuation of mechanicalmuscle function is reversed.
Perform an air drillAfter procedures in which the heart chambers areopened, or in closed procedures in which air mayhave entered a heart chamber, it is necessary to
evacuate all intracardiac air before termination ofCPB to avoid systemic air embolism. In some cen-ters, the surgeon floods the field with carbon dioxideduring open procedures to reduce entrainment ofair. It is felt that the higher solubility of carbondioxide in blood and tissue (25 times > air) mayreduce the risk of air embolic mediated neurologicevents.
TEE is invaluable during deairing as it allows theeffectiveness of the previously described proceduresto be monitored on line. Air is particularly likelyto be retained in the LV apex, LA, right coronarysinus, and the pulmonary veins. The right upperpulmonary veins in particular tend to entrain airgiven their more vertical entry into the LA. Removalof retained air requires flow through the pulmonarycirculation and the heart. TEE surveillance, com-bined with the joint efforts of the surgeon, anesthe-siologist, and perfusionist, are necessary to preventsystemic air emboli during evacuation procedures.Ejected air will tend to track along the anterioraspect of the aorta (air rises). The first manifes-tation of small amounts of ejected air may be STsegments elevations in the territory of the anteriorright coronary artery (leads II, II, aVF). In the casesof anteriorly placed coronary artery bypass grafts thedistribution will tend to be more global.
To remove detected air, the following steps areuseful:• The patient is placed in the head-down position.• The lungs are ventilated and the table is rolledfrom side to side to help remove sequestered airfrom the pulmonary veins.• With the open atrium under a pool of blood,the venous line is partially clamped and the lungsare ventilated so that the ventricle becomes filledwith blood. The ventricle is then freed of air eitherby aspiration on a vent line or by apical needleaspiration while the heart is elevated and massaged.• The atriotomy or vent insertion site is closedunder a pool of blood or fluid.• The proximal aorta is evacuated of air eitherthrough the cardioplegia cannula or through aneedle placed in the aorta.• The aortic cross-clamp is not removed until theheart and aorta are free of air so that no air is ejectedsystemically.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 354 — #32
354 Chapter 10
• The LV may be vented directly through the apexwith an 18-gauge needle by the surgeon. Afterventing, the puncture site is sutured closed.
Determine factors that may maketermination of CPB difficultCommunication with the surgeon is essential here.It is best to know about the possibility of residualdefects or incomplete revascularization before ter-mination of CPB. Such information will affect themanagement of the patient if termination of CPBis difficult or impossible. Factors that increase thelikelihood of a need for inotropic support to termi-nate CPB include: poor preoperative systolic func-tion, a history of congestive heart failure, pre- orintraoperative inotropic support, poor myocardialpreservation, a long cross-clamp time, incompleterevascularization, advanced age, female gender allincrease the likelihood that post-CPB inotropicsupport will be needed.
DefibrillationAfter rewarming and removal of the aortic cross-clamp, it may be necessary to defibrillate the heart.Several factors have been shown to be importantin determining the ease of defibrillation after aorticcross-clamp removal:• A serum potassium level of approximately5 mEq/L decreases the defibrillation thresholdcompared with levels approximately 0.5 mEq/Llower. In many institutions where potassiumcardioplegia solution is used, serum potassiumlevels are in the 5 mEq/L range at the timeof aortic cross-clamp removal. If defibrillation isunsuccessful in the presence of a low serumpotassium, infusion of potassium should beconsidered.• Aortic perfusion pressure and the duration ofreperfusion after aortic cross-clamp removal areimportant. Recall that subendocardial perfusion iscompromised during ventricular fibrillation on CPB.A longer reperfusion period after aortic cross-clampremoval allows for washout of the products ofanaerobic metabolism and for replenishment ofenergy stores. For these reasons, a mean aorticblood pressure of at least 50 mmHg for greater
than 5 minutes is likely to increase the success ofdefibrillation.• Myocardial temperature at the time of defibril-lation should be greater than 30C. Recall thatspontaneous fibrillation occurs at a myocardialtemperature of 28C.• Patients with valvular heart disease are morelikely to need multiple defibrillation attempts com-pared with patients without valvular disease. Thisdoes not appear to be due to the increased heartweight and size often associated with valvular heartdisease.• Lidocaine reduces the number and the energydose of DC shocks required for ventricular defibril-lation. Lidocaine 1 mg/kg is given 5 minutes beforeaortic cross-clamp removal. Prophylactic lidocaineinfusions are unnecessary. Lidocaine infusions ini-tiated after CPB in coronary artery bypass patientshave been shown to slightly decrease the incidenceof nonsustained ventricular tachycardia with noapparent clinical benefit. Infusions of lidocaine arewarranted for treatment of high grade ventricularectopy.• Hypomagnesemia occurs in up to 70% of patientsafter CPB and may predispose ventricular andsupraventricular tachyarrhythmias. As a result,some centers supplement magnesium (2.0–4.0 g or100 mg/kg in children) before or immediately aftertermination of CPB.
After optimization of conditions as describedabove, ventricular defibrillation is accomplished bythe use of internal paddles. Much lower energy lev-els are required than for transthoracic defibrillation;2.5–20.0 J or watt-seconds using internal paddles issufficient to defibrillate most hearts. Defibrillationenergy is started at 2.5 J and increased in 2.5–5.0-Jincrements. Inability to defibrillate a heart of apatient in whom conditions have been optimizedsuggests ongoing myocardial ischemia from poorrevascularization or from coronary air or particu-late emboli. Coronary air embolus is particularlycommon in procedures in which the left hearthas been opened. When coronary air embolus issuspected, efforts should be made to increase per-fusion pressure to break up bubbles and movethem through to the venous side of the circula-tion. Increasing MAP on CPB will increase coronary

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 355 — #33
Management of Cardiopulmonary Bypass 355
perfusion pressure. This in combination with nitro-glycerine administration to dilate the epicardialcoronary arteries and phenylephrine administra-tion to further elevate MAP may be helpful in thissituation.
Potassium and acid-base balanceHypokalemia will compromise defibrillation andhas been discussed. Hyperkalemia presents otherproblems. As the serum potassium level climbsgreater than 5 mEq/L, the PR and QT intervalsshorten and the T waves become peaked. A serumpotassium level greater than 6 mEq/L will increasethe incidence of dysrhythmias and conductionabnormalities due to a reduction in the threshold formembrane depolarization. This may predispose thepatient to pacemaker-induced dysrhythmias. Pac-ing may not be possible as the serum potassiumapproaches 7 mEq/L. As levels reach 9–10 mEq/Lidioventricular rhythm progresses to ventricularasystole and fibrillation.
Immediate treatment of elevated serum potas-sium with electrocardiogram (ECG) changes isindicated. IV calcium chloride 10 mg/kg or cal-cium gluconate 50 mg/kg, sodium bicarbonate0.5–1.0 mEq/kg, or 1 mL/kg of 50% dextrose and0.1 unit/kg of regular insulin all work immediatelyto reduce serum potassium by shifting it intracel-lularly. Where severe hyperkalemia exists, diuretictherapy will be necessary to increase the excretionof potassium as well. Alpha-stat pH managementshould continue as the patient is warmed. Total car-bon dioxide, PaCO2, and pH should be correctedif necessary before termination of CPB. It may benecessary to give sodium bicarbonate to treat ametabolic acidosis or to adjust oxygenator gas flowto correct PaCO2.
In patients with compromised renal function,efforts must be made to avoid hyperkalemia result-ing from use of potassium cardioplegia. It is possibleto scavenge the cardioplegic solution from the coro-nary sinus so that it does not end up in the pump andelevate the serum potassium. In addition, it also ispossible to use cold crystalloid cardioplegia withoutpotassium in these patients. ZBUF may also be usedto reduce serum potassium prior to termination ofCPB in these patients.
Obtain pacingAfter the aortic cross-clamp has been removed, theheart has been defibrillated, and potassium andacid-base status has been corrected, it may be neces-sary to obtain pacing. Although many patients willbe in sinus rhythm, slow rates may compromisecardiac output, and therefore pacing is beneficial.In other patients, sinus rhythm is not immediatelypresent at CPB termination. Pacing is initiated withuse of epicardial pacing wires. Epicardial pacing canbe bipolar (two wires on the heart) or unipolar(one wire on the heart, one through the skin ofthe epigastric area). Atrial, ventricular, or atrial andventricular wires may be placed. Atrial wires usuallyare placed at or near the RA appendage. Ventricularwires are placed on the free wall of the RV. The wiresare brought out through the skin in the epigastricarea and can be removed easily postoperatively. Byconvention, the atrial wires are brought out on theright side of the epigastric area and the ventricularwires are brought out on the left side. The combi-nation of atrial and ventricular wires allows atrial,ventricular, or atrial ventricular sequential pacingwhen used in combination with a dual output (atrialand ventricular) sequential external pacemaker.
An additional set of leads placed on the LVallows biventricular pacing. Pacing of the RV aloneproduces septal wall dyskinesis and asynchronousdelayed activation of the LV. Biventricular pacingimproves septal wall motion and produces simul-taneous activation of the right and left ventri-cles. Biventricular pacing improves global systolicfunction in patients with low ejection fraction.
Because electrocautery is used extensively inthe post-CPB period, the sensing threshold (milli-volts) of the pacemaker may have to be increasedtoward the nonsensing or asynchronous mode toprevent inhibition of the pacemaker by electro-cautery radiofrequency current. In general asyn-chronous (nonsensing) pacing is used post-CPB toavoid electromagnetic interference (EMI) from elec-trocautery. If the SA node rate is slow and AV nodeconduction is intact atrial pacing (AOO) should beprovided as activation of ventricular contractionvia the native conduction system provides opti-mal ventricular synchrony. When both SA and AVnode dysfunction exist AV sequential pacing (DOO)

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 356 — #34
356 Chapter 10
will be necessary and the optimal AV interval toprovide AV synchrony will need to be determined.Generally, an interval of 150 ms is chosen to startin adults and then varied within the 120–200-msrange as needed to optimize ventricular filling andcardiac output. Infants will need a shorter PR inter-val. At pacing rates of 150–170 b/min this intervalwill likely be 100–120 ms in duration.
An alternative to DOO pacing when AV nodalblock or a very prolonged AV interval exists in thepresence of normal SA node function is DDD pac-ing. This mode will allow tracking (sensing) of theatrial rate with subsequent ventricular sensing andpacing to a set maximum rate at which point thepacemaker will produce Wenchebach type block.The disadvantage of this mode of pacing is that itis susceptible to EMI interference.
The current output (milliamperes) of the pace-maker is increased slowly until the desired cardiacchamber is captured. Each pacemaker spike mustresult in appropriate atrial and/or ventricular cap-ture and contraction. There also must be appropriatesequential contraction of the atria and ventricleswhen atrial ventricular sequential pacing is desired.It is necessary to look at both the ECG trace and theheart to ensure capture. After the minimum currentoutput necessary for capture has been determined(usually 5–10 mA), the current output is increasedby 5 more milliamperes to ensure continued cap-ture. In patients having undergone previous cardiacsurgery (redos), atrial and ventricular scarring maynecessitate higher current outputs than normal toobtain capture. In some instances, capture may notbe possible until the epicardial pacer wire is movedto a site with less scarring.
Arterial pressure and pump flowAfter the aortic cross-clamp has been removed, theMAP should be maintained in the 60–80 mmHgrange to allow adequate reperfusion of the heartto replenish adenosine 5-triphosphate (ATP) storesand remove anaerobic metabolites. In preparationfor termination of CPB, it is best to accomplish thisby maintaining a calculated SVR in the range of1000–1500 dynes s/cm5 and adjusting pump flowsaccordingly. SVR can be varied with the use of eitherphenylephrine or nitroprusside as needed.
HematocritGenerally, a hematocrit greater than 25% is soughtas CPB terminates. Advance planning is needed toachieve this goal. Reduction of the prime volumemay be needed for some patients, as described pre-viously. Vigorous diuresis during CPB may result inhemoconcentration; likewise, the use of an ultra-filtration device during CPB will achieve the sameend. Transfusion of red blood cells may be neces-sary if these methods fail or are not appropriatedue to low venous reservoir levels on CPB. Lowhematocrit levels (<22%) as CPB terminates at37C may result in low SVR due to decreasedviscosity.
Resume ventilationBefore terminating CPB, it is necessary to be cer-tain that the lungs are easily reinflated, that if thepleural cavity is not opened that no pneumothoraxexists, and that all fluid is removed from open chestcavities. Caution should be exercised when reinflat-ing the lungs of patients with internal mammaryartery (IMA) grafts to avoid stretching or avulsingthe grafts. It also is necessary to resume ventilationat minute ventilation that will prevent hypercarbiaafter CPB terminates. Large increases in pulmonaryvascular resistance (PVR) are seen with small eleva-tions in arterial carbon dioxide after cardiac surgery.Such elevations in PVR may cause RV failure inpatients with compromised RV systolic function. Itshould be remembered that carbon dioxide pro-duction is likely to be higher at the termination ofCPB than it was before initiation of CPB due to thedifferences in body temperature.
For infants and children, it may be desirable tomaintain mild hypercarbia in certain instances. Inpatients undergoing systemic to PA shunt proce-dures, pulmonary overperfusion (recirculation ofpulmonary venous blood into the pulmonary cir-culation) may occur if the shunt is large and PVRis low. Hypercarbia may provide protection fromoverperfusion by increasing PVR. Conversely, highpulmonary vascular resistance and high airwaypressures will compromise pulmonary blood flow inchildren having undergone the Fontan procedure(total cavopulmonary connection) due to the lowdriving pressure for pulmonary blood flow.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 357 — #35
Management of Cardiopulmonary Bypass 357
Termination of CPB
Termination of CPB is accomplished after the hearthas been de-aired, ventilation has been resumed,electrolyte (particularly calcium and potassium)homeostasis has been achieved, and adequatemyocardial contractility, rate and rhythm have beenestablished. A coordinated effort between surgeon,perfusionist, and anesthesiologist is then directedtoward allowing the heart to fill and eject as venousdrainage into the CPB reservoir is reduced andfinally terminated.
Volume infusion following termination of CPBis guided by both direct and TEE visualization ofheart size and by analysis of intracardiac pressuresand systemic blood pressure. Because volume caninitially be delivered intravenously or via the arte-rial cannula, communication between the surgeon,anesthesiologist, and perfusionist is necessary. Therange of filling pressures expected to provide opti-mal preload for a particular patient should be dis-cussed before termination of CPB. Visual inspectionof the heart will provide information on distensionand wall motion but it must be remembered thatit is primarily the free wall of the RV that is visi-ble through a median sternotomy. The functionalstatus of the RV is not necessarily the same as thatof the LV. TEE allows visualization of the LV.
The endpoint of volume infusion is optimiza-tion of preload recruitable stroke work. If preloadrecruitable stroke work exists then volume infusionshould induce an increase in blood pressure withlittle or no elevation in ventricular end-diastolicpressure as measured by atrial pressures. If furtherinfusion of volume results in an increase in heartsize and elevation of pulmonary artery occlusionpressure (PAOP) or left atrial pressure (LAP) and/orright atrial pressure (RAP) with no increase in bloodpressure than it can be assumed that preload isoptimized. Further volume infusion at this pointwill not improve arterial blood pressure and willlikely distend the heart, elevate ventricular end-diastolic pressure and wall stress, and compromisesubendocardial perfusion leading to a decrease inarterial blood pressure.
If inotropic support is anticipated to be neces-sary for termination of CPB, it should be started
5 minutes before termination of CPB. Starting theinfusion of inotropic agents too soon increasesmyocardial oxygen consumption while the heartis being reperfused on CPB. This compromises thereplenishment of energy stores and serves no usefulpurpose.
CPB should be terminated at a pump flow andSVR that are reasonable for the patient. If the perfu-sionist is pumping 5 L/min with a MAP of 50 mmHg,then the patient will have to have a cardiac out-put greater than 5 L/min to maintain a MAP of70 mmHg after CPB has been terminated. If such anoutput is an unreasonable expectation, then effortsmust be made to increase SVR to a normal rangebefore termination of CPB. This will allow termina-tion of CPB at the desired MAP with a cardiac outputthat the patient can realistically produce. Recall thaton CPB, SVR = (MAP × 80)/pump flow, with thenormal range 1000–1500 dynes s/cm5.
CPB is terminated by gradually clamping thevenous line so that venous return to the reservoiris impeded. Simultaneously, the perfusionist slowsthe rate of the arterial pump head. This results ingradual transfusion of blood to the patient via thearterial cannula. The volume of blood in the venousreservoir will slowly drop as the process continues.When adequate preload is obtained as assessed byPAOP, RAP, visual inspection of the heart, and TEEthe transfusion is terminated.
As the heart fills with blood, ejection is noted.The simplest way to assess this is by observingthe arterial waveform. Elevation of filling pres-sures with evidence of poor ejection is indicativeof contractility/afterload mismatch. There is eitherpoor systolic function or a level of afterload thatis excessive for the inotropic state of the heart.If SVR has been normalized before termination ofCPB, efforts can be directed toward increasing thecontractile state of the heart with inotropes.
Administration of calcium salts at this time iscontroversial. In some institutions, calcium chlo-ride 5–10 mg/kg or calcium gluconate 25–50 mg/kgis used as the first intervention in this setting.Calcium chloride increases the inotropic state ofthe myocardium and induces an increase in SVRthat outlasts the inotropic effects. Often, thisintervention is all that is required to complete

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 358 — #36
358 Chapter 10
termination of CPB. There is evidence, however,that calcium chloride administration is contraindi-cated at this time because of the compromisedcalcium homeostasis that accompanies the insultof aortic cross-clamping. Administration of calciummay exacerbate ischemic damage by causing accu-mulation of intracellular calcium. Beta-adrenergicagents, on the other hand, increase intracellularcalcium but also promote its reuptake into the sarco-plasmic reticulum and may be more appropriate inthis setting.
Before therapy for low arterial pressure is ini-tiated, the possibility that a discrepancy existsbetween the intra-arterial radial arterial pressureand the central aortic or femoral artery pressureshould be investigated. This can be determined bysimultaneous observation of the central aortic andradial artery pressures and will prevent unnecessarytherapeutic interventions. Central aortic pressurecan be monitored easily by having the surgeon placea small needle in the ascending aorta or aortic can-nula attached to a length of pressure tubing that ispassed over the drapes to a transducer. After CPB,intra-arterial radial arterial systolic pressure mayunderestimate central aortic, brachial, or femoralartery systolic pressure by as much as 40–50 mmHgin a significant number of both children and adults.This effect is most pronounced following periodsof DHCA. It has been demonstrated that the gra-dient develops upon initiation of CPB and is notaffected by vasodilators or vasopressors. Becausethis discrepancy may persist for up to 90 minutesafter the termination of CPB, it may be necessaryto place a femoral arterial line for continued mon-itoring. The etiology of this discrepancy appears tobe a reduction in pulse wave velocity implying anacute reduction in radial arterial elastance leading toreduced pulsatility in the peripheral arteries. Botharterial-to-venous shunting in forearm blood ves-sels and peripheral vasospasm have been implicatedas well.
If the patient separates from CPB with highfilling pressures, ventricular distension, low car-diac index (below 2 L/min/m2), and low MAP(under 40 mmHg), prolonged efforts to correct thehemodynamics of CPB should not be made. Rein-stitution of CPB will prevent the downward spiral
induced by subendocardial ischemia and elevatedwall tension. In addition, it will allow reperfusionof the heart during a low energy consumption state.After CPB has been reinstituted several questionsmust be addressed:• Was the ventricular failure biventricular or wasonly one ventricle involved?• Was there PA hypertension and RV failure?• Was there RV or LV ischemia?• Is the prosthetic valve working properly?• Is all of the monitoring equipment functioningproperly and giving accurate information?• Are there other unsuspected lesions such as pre-viously clinically insignificant mitral regurgitation(MR)?• Is the repair of the congenital lesion complete andsuccessful? Is there a residual defect that requiresrepair?• Is the heart rate and rhythm optimized?• Is the appropriate type of pacing being per-formed and is the pacemaker capturing the desiredchambers?Having addressed these questions, therapy directedtoward specific problems can be instituted, andanother attempt can be made to terminate CPB.
Post-CPB management
After termination of CPB, it is necessary to stabilizethe patient and to reverse heparinization to allowdecannulation and chest closure.
Protamine administrationProtamine is a polyvalent cation derived fromsalmon sperm that is currently used to neutral-ize systemic UFH. Protamine is given after stablehemodynamics are maintained after termination ofCPB. It should not be administered until the likeli-hood that having to reinstitute CPB is small. Afterprotamine neutralization of UFH begins, the car-diotomy suction should not be used and removalof the arterial and venous cannulas should proceed.This prevents contamination of the heparinized CPBcircuit with protamine should prompt reinstitu-tion of CPB be necessary and prevents thrombusformation on the cannulas.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 359 — #37
Management of Cardiopulmonary Bypass 359
There are several approaches to the neutralizationof UFH with protamine:• Reverse extrapolation. Some centers use 1.0 mg ofprotamine for each 100 USP units of UFH deter-mined to exist at the termination of CPB. This ratiois based on the in vitro protamine to UFH neutral-ization ratio of 1:1. Some institutions believe thisratio to be more like 1.3:1.0. An ACT is obtainedwhen CPB terminates and reverse extrapolation ofthe patient’s UFH dose response curve is used tocorrelate the ACT with the amount of UFH present.This method has been criticized because the ACTobtained at the termination of CPB is prolongedby factors other than UFH, such as CPB-inducedplatelet dysfunction and hemodilution. This mayresult in an overestimation of the UFH present atthe termination of CPB and a larger than necessaryprotamine dose.• Empiric dosing. Some centers simply administera fixed dose. This method does not rely on anypost-CPB assessment of residual UFH effect such asACT to determine the protamine dose. Nonethe-less, these methods have been shown to result inadequate UFH reversal. In the case of the fixeddose regimen, UFH reversal is obtained at muchlower protamine doses than predicted by the reverseextrapolation method. The dose of protamine isbased on either the patient’s weight (3–4 mg/kg)regardless of the UFH dose, or 1.0 mg of protaminefor each 100 USP units of UFH administered at theonset of CPB.• Anti-factor Xa assay. This UFH assay is used to cal-culate the protamine dose based on the patient’sblood volume and a neutralization ratio of 1:1.Despite the fact that not all UFH present in bloodexerts an anticoagulant effect and need be neu-tralized, this method has been shown to provideadequate UFH reversal with low doses of protamine.• In vitro protamine titration. This method requiresACT tubes (celite or kaolin) containing protamine.Assuming a protamine to heparin neutralizationratio of 1:1 this method allows determination ofthe whole blood heparin level. Typically the resultsof this test are used in combination with anestimate of the patient’s blood volume to deter-mine the appropriate protamine dose to neutralizecirculating UFH.
Both the protamine response test (PRT,Hemochron®) and the heparin/protamine titrationtest (HPT, Medtronic Hemotec®) provide in vitroprotamine titration. The HPT method measures clot-ting times enhanced by addition of thromboplastinin several channels that contain varying quantitiesof protamine. The first channel to clot is the chan-nel in which the protamine to heparin ratio is closestto neutralization. The absolute clotting time is notimportant; only the determination of the channelwith the appropriate ratio. Therefore, the determi-nation should be independent of non-UFH factorsthat prolong the ACT. This method results in ade-quate UFH reversal at lower doses of protamine thanpredicted by the reverse extrapolation using only apost-CPB ACT.
The PRT uses two channels. One channel is thenative ACT (post-CPB) the other channel is an ACT(post-CPB) with either 20 or 40 µg of added pro-tamine. The results of the clotting times in thesetwo tubes are used to construct a linear protaminedose–response relationship extrapolated back to abaseline (pre-CPB) ACT. In combination with anestimate of the patient’s blood volume the neutral-izing dose of protamine can be determined withreverse extrapolation. This determination will notbe independent of non-UFH factors that prolongthe ACT.
The ACT should be checked after administra-tion of the selected protamine dose. The goal is toreturn the ACT to a normal value. Excess pro-tamine is clearly detrimental to platelet functionby nature of its inhibitory effects on the plateletreceptor GPIb/IX/V interaction with vWF that is acritical component of platelet adhesion and aggre-gation. Administration of additional protamine isnot benign and tends to delay detection and treat-ment of thrombocytopenia, platelet dysfunction,and coagulation factor deficiencies.
There are several potential adverse reactions asso-ciated with protamine administration. These pro-tamine reactions occur in both children and adults.The incidence of protamine reactions in childrenfollowing cardiac surgery is lower than in adults(approximately 10%); on the order of 1.76–2.88%depending on the stringency of criteria linking theepisode to protamine administration. Risk factors

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 360 — #38
360 Chapter 10
for these reactions (NPH insulin use, previous drugreaction, or an allergy to protamine or fish) mayexist in up to 40% of cardiac surgical patients.
Reactions to protamine (defined as arterialhypotension, pulmonary hypertension, or both) areassociated with increased mortality following coro-nary artery bypass surgery. It is unclear whetherintervention to treat these events reduces mortalityor whether there is a cause and effect relationshipbetween the hemodynamic events and mortality.It is possible that the hemodynamic events are asurrogate marker for the ultimate cause such as anenhanced pro-inflammatory response.
The reactions associated with protamineadministration are described in the sections thatfollow.
Systemic hypotensionThis is the most common reaction to pro-tamine administration and it is more commonin patients with poor ventricular function. Thedecrease in systemic blood pressure is multifactorial.A decrease in SVR mediated via a nitric oxide/cyclicguanosine monophosphate (NO/cGMP) depen-dent and endothelial-mediated mechanism hasbeen implicated, as has pulmonary histaminerelease. Protamine-induced platelet aggregationand release of vasoactive substances also mayproduce systemic hypotension, particularly whenplatelet concentrates are infused in associationwith protamine. Protamine induced reduction inmyocardial contractility has also been implicated.
The incidence of this reaction appears to berelated to the speed of infusion. Regardless ofthe infusion site (right atrium, LA, aorta, periph-eral vein) this reaction can be avoided or at leastdecreased in severity when a slow infusion (overmore than 3 minutes) of protamine is used. Somecenters advocate prophylactic administration of cal-cium chloride/gluconate or H1 and H2 blockers toattenuate this reaction. These interventions are ofunproven benefit.
Pulmonary hypertensionPulmonary hypertension after protamine may beso profound as to result in RV failure and circu-latory collapse. This reaction is idiosyncratic and
is associated with high levels of thromboxanesand C5a anaphylatoxins, which result in broncho-constriction and pulmonary vasoconstriction in sus-ceptible patients after protamine administration.Heparin-protamine complexes are the likely ini-tiating mechanism. This reaction seems to occurin susceptible patients regardless of whether theprotamine is infused into the right or LA, admin-istered as a bolus, or given as a slow infusion.Patients with pre-existing pulmonary hyperten-sion are not at greater risk for this reaction.Fortunately, this reaction is rare, occurring in lessthan 3% of cases. Pulmonary hypertensive episodesin children following protamine administration arevery rare.
True allergic (anaphylactic andanaphylactoid) reactionsTrue allergic reactions require the presence ofimmunoglobulin E (IgE) or immunoglobulin G(IgG) antibodies to the substance in question. Typ-ical manifestations of this type of reaction includehypotension, flushing, urticaria, bronchospasm,and pulmonary edema secondary to capillary leak.IgE-mediated reactions are the result of IgE-antigencomplex causing mast cells degranulation. IgGmediated reactions are the result of activation of thecomplement cascade by the IgG-antigen complex.
Formation of these antibodies is enhanced inpatients who have been exposed previously to theallergen or to a substance that is similar to the aller-gen. An increased incidence of protamine reactionshas been reported to occur in:• Patients taking NPH insulin. These patients are pre-sumed to be pre-sensitized to protamine from theinsulin preparation. An incidence of reactions ashigh as 27% has been reported, but prospectivestudies suggest an incidence of approximately 0.6%.• Patients with fish (not shellfish) allergies. Thesepatients are believed to be at higher risk due to sev-eral case reports but prospective analysis does notsupport this contention.• Vasectomized men. IgG (antisperm) antibodies toprotamine are found in 29% of vasectomized menbut they are present in low titers and prospectiveanalysis does not support the contention that thesepatients are at higher risk.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 361 — #39
Management of Cardiopulmonary Bypass 361
• Previous protamine reaction. These are thehighest risk patients.
The risk of an adverse response to protamineis 25 times higher in patients with protamine-specific IgG antibody and 95 times higher in patientswith protamine-specific IgE antibody. However, thepercentage of patients exposed to protamine orprotamine-like substances that go on to developIgG or IgE antibodies is low. Furthermore, notall patients with IgG antibodies to protaminedevelop reactions to protamine. Therefore, theoverall risk of true allergic reactions in patientswho were previously sensitized to protamine seemsto be low.
Efforts have been made to identify patients sus-pected to be at risk for protamine may be testedfor IgE and IgG antibodies. Skin testing commonlyis used to test for IgE-mediated hypersensitiv-ity. Enzyme-linked immunosorbent assays (ELISAs)and radioallergosorbent tests (RASTs) are used todetect minute quantities of circulating IgG and IgEto an allergen. Both skin testing and ELISA inpatients at risk for protamine reactions have beenshown to have a high false-positive rate and poorspecificity. In other words, many patients with apositive test for protamine antibodies do not go onto develop a reaction. This severely limits the valueof this type of testing.
Noncardiogenic pulmonary edemaThis reaction has been reported to occur as bothan immediate and a delayed reaction (more than20 minutes after administration) to protamine in asmall number of case reports. It is not entirely clearthat protamine alone is responsible for this reaction,as concomitant blood product administration alsohas been implicated.
Heparin reboundHeparin rebound may occur after protamineadministration. This phenomenon is defined as are-prolongation of the ACT occurring 1–8 hoursafter adequate UFH neutralization. The elevatedACT renormalizes with additional protamine. Sev-eral etiologies have been suggested. A large quantityof UFH remains bound to plasma proteins for up to6 hours after clinically adequate neutralization of
UFH with protamine. As protamine is cleared, theprotein-bound UFH dissociates slowly and bindsto AT-III to produce an anticoagulant effect. It isnot surprising, then, that the incidence of heparinrebound is reduced when a heparinization proto-col that uses lower UFH doses is compared withone that uses higher doses. Concurrent protaminemetabolism also may be a factor. Heparin reboundalso may be due to enhancement of residual UFHby infusion of blood components such as FFP thatelevate AT-III levels.
Recommendations for protamineadministration• Slow administration (25–50 mg/min) of the cho-sen protamine dose into the right atrium via acentral venous catheter. The central venous routeis chosen over peripheral venous administration toensure that the drug reaches the central circulationjust as with UFH administration.• If systemic hypotension due to a decrease inSVR occurs, the protamine infusion should bestopped. The SVR should be elevated with anα-agonist (phenylephrine, norepinephrine) andpreload should be optimized with volume infusion.The protamine infusion can then be restarted slowlywhile SVR and preload are maintained.• If pulmonary hypertension occurs, immediateaction is necessary. The protamine should bestopped in an effort to reduce pulmonary vascu-lar resistance while the circulation is supported.Infusion of epinephrine may be necessary to pro-vide inotropic support of the RV. If pulmonaryhypertension persists, infusion of nitroglycerin, orprostaglandin E1 (started at 0.01–0.05 µg/kg/min)into the right atrium will help reduce PVR andimprove RV function. Inhaled NO may be a bet-ter alternative, as it will not exacerbate systemichypotension. In either case, simultaneous infusionof norepinephrine into a left atrial catheter pro-vides treatment for both elevated PVR and reducedSVR. Protamine infusion may have to continuewith continued vasopressor vasodilator therapy. Insevere cases, reinstitution of CPB may be neces-sary to provide cardiopulmonary support. Follow-ing subsequent discontinuation of CPB protamineadministration may have to be avoided.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 362 — #40
362 Chapter 10
• If an anaphylactic or anaphylactoid reactionoccurs in association with protamine administra-tion, therapy with epinephrine, steroids, H2 blockers,and bronchodilators is warranted.• An ACT should be repeated after protamine infu-sion. If the ACT remains elevated above normal(120 ± 40), an additional 0.25–0.50 mg/kg of pro-tamine can be administered and the ACT rechecked(essentially in vivo protamine titration). No changein the ACT will essentially eliminate excessprotamine as the source of ACT elevation.
Alternatively, a heparinase ACT test can beperformed. Two-chamber cartridges are available(Medtronic Hemotec®). Both chambers containkaolin and calcium chloride. One chamber con-tains highly purified heparinase capable of rapidlyneutralizing 6 USP unit/mL of UFH. A >10–15%elevation of the native ACT relative to the hepari-nase ACT is indicative of the need for additionalprotamine regardless of the absolute ACT values asfollows:a If the heparinase ACT is normal and the nonhep-arinase ACT is within 10–15% of this value, thenthe UFH has been neutralized and no additionalprotamine is necessary.b If the heparinase ACT is normal and the nonhep-arinase ACT is elevated, then UFH is present andmore protamine is warranted.c If both the heparinase ACT and the nonhepari-nase ACT are elevated above normal and are within10–15% of each other, the patient should be evalu-ated for other causes of an elevated ACT besides UFHsuch as factor deficiencies (intrinsic and commonpathway). No further protamine is necessary.d If both the heparinase ACT and the nonhep-arinase ACT are elevated above normal and thenonheparinase ACT is elevated more than 10–15%above the value of the heparinase ACT, the patienthas both UFH and other factors as a cause.Additional protamine and evaluation for factordeficiencies both are warranted.
In vitro protamine dose assay (PDAO,Hemochron®) can be done as well. This test usesa two-channel system in which one channel isthe native ACT and the other has 10 µg pro-tamine added. Reverse extrapolation of the tworesults back to a baseline ACT in combination with
the patient’s blood volume yields the supplementalprotamine dose. Administration of additional pro-tamine is not benign and tends to delay detectionand treatment of thrombocytopenia, platelet dys-function, and coagulation factor deficiencies by thesurgical team.• If heparin rebound is suspected, the ACT shouldbe rechecked and use of the one of the methodsto detect residual UFH described above considered.Additional protamine 0.25–0.50 mg/kg should thenbe administered. This usually is adequate to treatheparin rebound.
Causes of impaired hemostasisfollowing protamine administrationHemostasis following termination of CPB andprotamine administration can be problematic fora number of reasons.
Surgical bleedingThe surgical field must be assessed carefully forbleeding sites. This inspection must include the cutsternal edges, the harvest site of the mammaryartery, and the back of the heart. Many of the sur-gical procedures involve long suture lines in vesselswith systemic pressures. In addition portions of thesuture line such as the posterior aortic wall maybe concealed making detection and control of thebleeding site challenging.
Platelet function defectsIn adults, this is the most common cause of bleed-ing after CPB once heparin has been reversed andsurgical bleeding has been controlled. Platelet dys-function may be secondary to CPB, particularly ifthe CPB time >2 hours or to preoperative anti-platelet therapy with aspirin, nonselective non-steroidal anti-inflammatory drugs (NSAID), plateletGPIIb/IIIa-receptor antagonists, or ATP recep-tor (P2Y12) blockers (thienopyridines). Plateletfunctional defects tend to compound hemostasisproblems from all other causes.
Transient defects in platelet plug formation andaggregation are seen in all patients after CPB. Gen-erally, platelet function returns to near normalstatus 2–4 hours after CPB. This transient dysfunc-tion is caused by platelet surface glycoprotein (GP)

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 363 — #41
Management of Cardiopulmonary Bypass 363
receptors that are redistributed internally intoplatelets during CPB. The presence of plasmin isresponsible for this inactivation or redistributionof GP receptors. These GP receptors are essentialfor platelet adhesion and aggregation. Tethering,translocation and stable arrest of platelets lead-ing to platelet adhesion and aggregation in arte-rioles requires at least four platelet GP receptors(GPVI, GPIb/IX/V, GPIa/IIa, GPIIb/IIIa) and threeligands (von Willebrand factor (vWF), collagen,fibrinogen).
Platelet GPIIb/IIIa receptors are the final commonpathway in platelet aggregation. They bind withhigh affinity to fibrinogen and mediate platelet-to-platelet aggregation via a fibrinogen bridge.The GPIIb/IIIa antagonists abciximab (Reopro®),eptifibatide (Integrilin®) and tirofiban (Aggrastat®)inhibit this aggregation irrespective of the platelet-activating stimulus. These agents are commonlyused in patients who present for surgery followingpercutaneous interventional coronary arterial pro-cedures such as angioplasty and stent placement.Both eptifibatide and tirofiban bind competitivelyand have short (2 hours) half-lives. As a result theygenerally do not cause bleeding problems. Abcix-imab is a large monoclonal antibody that bindsirreversibly and sterically blocks the receptor for thelife of the platelet. Patients presenting for surgeryfollowing administration of this agent within a1–2 week time frame usually require aggressivereplacement of platelets following CPB.
Aspirin (acetylsalicylic acid) ingestion irreversiblyinhibits platelet cyclo-oxygenase 1 (COX-1) for the10–15 day life span of the platelet. This resultsin inhibition of platelet thromboxane A2 produc-tion. Thromboxane A2 is potent vasoconstrictorand stimulant for platelet activation and aggre-gation. Preoperative aspirin ingestion has beenshown to increase blood loss after CPB by exac-erbating CPB-induced platelet dysfunction. Addi-tionally, 15–20% of patients who ingest aspirinare hyper-responders, which further contributes toplatelet dysfunction. Nonselective NSAID have sim-ilar effects to aspirin lastly only as long as significantblood levels are maintained.
Thienopyridines (clopidogrel, ticlopidine) areagents that selectively and irreversibly block platelet
adenosine diphosphate (ADP) receptors P2Y1 andP2Y12. These receptors are responsible for ADP-induced platelet activation and aggregation. Bothreceptor pathways must be intact for normal plateletresponses to occur. P2Y1 linked to the Gq path-way is responsible for platelet shape change andtransient aggregation triggered via an increase inintracellular calcium. P2Y12 linked to the Gi path-way is responsible for completion and amplificationof the aggregation response via inhibition of adeny-lyl cyclase. Clopidogrel is used almost exclusively asticlopidine use is associated with an unacceptableincidence of neutropenia.
The anti-platelet effects of aspirin and clopido-grel are synergistic. Ideally, aspirin and clopidogrelwould have to be discontinued for 10–15 days priorto surgery for termination of their clinical effect.There may reluctance to discontinue these med-ications prior to surgery, as discontinuation hasbeen associated with acute coronary syndrome andcoronary stent thrombosis.
Desmopressin acetate (DDAVP) in a dose of0.3 µg/kg increases levels of factor VIII and vWF.Von Willebrand’s factor is known to mediateplatelet aggregation and adherence on thrombo-genic surfaces. The increased levels of vWF thatresult from DDAVP infusion may be responsiblefor improving platelet function post-CPB. Despitethis, DDAVP is not consistently effective in reducingblood loss or homologous transfusion requirementsin pediatric and adult cardiac surgical patients whengiven after CPB and protamine administration. Ofparticular importance DDAVP is not consistentlybeen effective in the subset of adult CABG patientstaking preoperative aspirin.
Thromboelastography may be useful in identi-fying patients who will benefit from DDAVP afterCPB and protamine reversal of UFH. Patients withan maximal amplitude (MA) < 50 mm indicativeof reduced platelet function demonstrate less bloodloss and a reduction in homologous transfusionrequirements after CABG surgery with DDAVPcompared with placebo.
DDAVP relaxes vascular smooth muscle andshould be administered slowly (over 20–30 minutes)to avoid reductions in SVR with subsequenthypotension.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 364 — #42
364 Chapter 10
ThrombocytopeniaPlatelet counts decrease during CPB, but generallythey do not fall below 100 000 in adults. In gen-eral, the fall in platelet counts on CPB is slightlygreater than what would be expected with hemod-ilution, with the difference being due to plateletadherence to synthetic surfaces, platelet destruc-tion, platelet sequestration in the lungs, and plateletconsumption in wounds. Because platelet func-tion defects are so prevalent, thrombocytopenia,when it does exist, is an important cause of alteredhemostasis.
In infants and children, platelet functional defectsinduced by CPB are overshadowed by the presenceof CPB-induced dilutional thrombocytopenia. Dilu-tional thrombocytopenia is a problem in neonatesand infants given the relatively large CPB pumpprime volumes and the absence of platelets in allprime solutions except fresh, unrefrigerated wholeblood. Whole blood stored for more than 48 hoursusing ACD or CPD at 4C is devoid of platelets.
In centers where refrigerated whole blood(<1 week old) is used to prime a 300 mL CPB cir-cuit for infants and neonates (2–5 kg) there is a50–80% immediate post-CPB reduction in preop-erative platelet count. The largest reductions areseen in the smallest patients undergoing the longestprocedures.
Prophylactic platelet transfusion after CPB is notwarranted; however, when there is post-CPB bleed-ing unrelated to residual heparin or surgical bleed-ing, platelets should always be administered as afirst-line treatment. A unit of platelets contains5.5× 1010 platelets; 0.1 unit/kg generally will raisethe platelet count by 50 000–80 000. In most cases,this will control the bleeding. For cases in whichother deficiencies exist, platelet therapy will preventplatelet defects from compounding the problem.
Platelet transfusions of 0.5–1.0 unit/kg may benecessary to normalize the post CPB platelet count(250–600 K/µL) in neonates and infants. Thrombo-cytopenia just prior to termination of CPB orfollowing protamine administration consistentlycorrelates with excessive postoperative blood lossin children. Since platelets are suspended in FFP,platelet transfusions in these patients also provide asubstantial FFP transfusion. The minimum volume
of FFP suspension for 1 unit of platelets is 20 mL(concentrated platelets) while the usual volumeis 40 mL. Therefore, a 2-unit platelet transfusionwould provide a 4-kg patient with a 10–20 mL/kgFFP transfusion.
Dilution of clotting factorsThe extent to which dilution of coagulation factors ispresent depends on the size of the patient, the extentof pre-existing factor deficiencies, and the volumeand composition of the CPB pump prime.
In adults, factor levels rarely fall below the 30%level, leaving the coagulation system intact. Like-wise, the fibrinogen level is reduced by dilutionduring and after CPB but rarely falls below thecritical 100 mg/dL level. It is not surprising, then,that the prophylactic administration of FFP has notbeen shown to reduce bleeding after routine CPBprocedures in adult patients without preexistingcoagulopathies.
Dilution of coagulation factors in neonates andinfants is less likely if the CPB pump prime con-sists of whole blood or reconstituted whole blood(packed red blood cells and FFP). Dilution of coagu-lation factors is particularly likely to occur when thepatient is polycythemic (reduced plasma volume).Significant dilution of coagulation factors is likelyif an asangeous colloid or crystalloid prime is used.Dilution of coagulation factors and red cells can bemitigated by use of conventional or MUF. Childrenwhose transfusion requirements in the immedi-ate post-CPB period are met with whole bloodthat is less than 48 hours old have total transfu-sion requirements 85% less than those treated withcomponent therapy.
Cryoprecipitate may be indicated in some cir-cumstances. Both hypofibrinogenemia and reducedfactor XIII are correlated with postoperativeblood loss. Cryoprecipitate contains fibrinogen,factor VIII/vWF, and factor XIII. One unit of cryo-precipitate (20–30 mL) contains 150 mg of fibrino-gen and 80–120 units of factor VIII/vWF. Thisquantity of fibrinogen is comparable to whatwould be found in 75 mL of FFP. This quantity offactor VIII/vWF is comparable to what would befound in 80–120 mL of FFP. In small patients, wherevolume constraints limit transfusion, cryoprecipitate

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 365 — #43
Management of Cardiopulmonary Bypass 365
is a much more efficient source of fibrinogen,factor XIII and factor VIII/vWF. In childrencryoprecipitate 0.5–1.0 unit/kg is transfused forbleeding that persists following normalization ofplatelet count. In adults, cryoprecipitate is usuallytransfused at 0.25–0.50 unit/kg.
FibrinolysisThe continued generation of thrombin during CPBdespite heparinization is largely responsible forinduction of ongoing fibrinolysis. Adjuvant therapyto improve hemostasis post-CPB is directed towarduse of anti-fibrinolytic agents. Sequential cleavageof fibrin by the serine protease plasmin is responsi-ble for fibrinolysis. Plasmin is the activated form ofplasminogen. Plasminogen contains 5-lysine bind-ing domains or kringles that allow it to bind tothe lysine residues on partially lysed fibrin. Fibrinbound plasminogen is subsequently cleaved to plas-min by tissue plasminogen activator (t-PA). t-PAalso contains lysine binding domains that allowsbinding to fibrin. Free t-PA is capable of convert-ing fibrin bound plasminogen to plasmin but t-PAbound to fibrin lysine residues stimulates activa-tion of plasminogen to plasmin by two orders ofmagnitude.
Antifibrinolytic agentsThree antifibrinolytic agents currently are in use.Each improves hemostasis after CPB. Ideally, theseagents are administered before CPB and beforestimulation of the coagulation and fibrinolytic pro-cesses. The three agents epsilon (ε)-aminocaproicacid (EACA), tranexamic acid (TXA), and aprotininare summarized below.
Lysine analogsThe lysine analogs TXA and EACA inhibit fibrinoly-sis by: (i) binding to plasminogen thus renderingit incapable of binding to the lysine residues onfibrin; and (ii) inhibiting the proteolytic action ofplasmin. The reduction in plasmin generation isalso beneficial in that plasmin is a potent plateletactivator. Subsequent to plasmin induced plateletactivation the platelet adhesion molecule GPIb/IX/Vundergoes proteolysis or translocation away fromthe platelet surface. TXA is 6–10 times more potentthan EACA.
AprotininAprotinin is naturally occurring (bovine lung)59-amino-acid polypeptide that is a serine proteaseinhibitor. Aprotinin is a potent inhibitor of fibri-nolysis and prevents plasmin activation of plateletseven at low doses. Plasma concentrations of apro-tinin inhibit the action of plasmin and kallikreinby reversible binding to the active serine sites ofthese enzymes. Because aprotinin binds 30 timesmore avidly to plasmin than kallikrein, a higherplasma concentration of aprotinin is needed toinhibit kallikrein as compared with plasmin. Con-centrations of aprotinin high enough to inhibitkallikrein are not maintained throughout CPB,even when high doses are used. Therefore, inhi-bition of the contact activation system probablyis not as important to the action of aprotinin asinhibition of plasmin induced fibrinolysis. Admin-istration of aprotinin to patients undergoing CPBresults in reduced formation of fibrin degradationproducts, increased α-antiplasmin (an inhibitor ofplasmin) and plasminogen activator inhibitor activ-ities, and decreased tissue plasminogen activatorrelease.
In addition to its effects on plasmin, aprotininhas direct effects on platelets that serve to reduceplatelet activation. Thrombin, a serine protease,is the main effector protease of the coagulationcascade and arguably the most important phys-iologic platelet agonist. It has now been estab-lished that thrombin activation of platelets occursvia G-protein coupled protease activated receptors(PAR). Human platelets express PAR-1 and PAR-4.PARs are essentially receptors that carry their owntethered ligand. Thrombin recognizes and binds tothe NH2-terminal extracellular domain of PAR-1and PAR-4. Subsequent proteolysis by thrombinresults in exposure of a new NH2-terminus thatbinds intramolecularly to the body of the recep-tor producing transmembrane signaling. This PAR-1ligand-receptor coupling mediates platelet activa-tion at physiologic thrombin concentrations. Apro-tinin blocks thrombin proteolysis of PAR-1 andas a result prevents thrombin induced plateletactivation. Aprotinin does not however inhibitplatelet activation via epinephrine, ADP, orcollagen.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 366 — #44
366 Chapter 10
Aprotinin is also capable of inhibiting monocyteexpression of TF induced by CPB. TF productionduring CPB results in thrombin generation via theTF-factor VIIa pathway. Aprotinin also counteractsheparin-induced reduction of platelet contractileforce similar to that seen with protamine reversalof heparin. Aprotinin also blunts the inflamma-tory response induced by CPB and heart and lungreperfusion in a manner similar to that of methyl-prednisolone by inhibiting release of interleukinsand tumor necrosis factor.
Dosage and administration ofantifibrinolytic agentsProphylactic administration of these agents(before commencement of CPB) is superior toadministration following commencement of CPB.
ε-aminocaproic acidThis drug is typically given as 100–150 mg/kg IVafter induction and 10–15 mg/kg/h, usually for5–6 hours. Higher doses (as much as 40 g) have beenused, but no dose-response data exist to supportthem. A smaller loading dose with a higher infu-sion rate may provide more stable plasma levels.In adults an ε-aminocaproic acid (EACA) loadinginfusion of 50 mg/kg given over 20 minutes and amaintenance infusion of 25 mg/kg/h maintains aconstant therapeutic plasma concentration of EACA(>130 µg/mL). In children ranging in age from5 months to 4 years, and in weight from 7.2 to18.9 kg, with CPB prime volumes of 650–850 mL,a bolus of 75 mg/kg over 10 minutes, 75 mg/kgin the CPB prime, and a continuous infusionof 75 mg/kg/h following the bolus maintains thesame therapeutic plasma concentration. The drugis renally concentrated and the infusion rate shouldprobably be decreased in accordance with creatinineclearance.
Tranexamic acidThis drug can be given as a single bolus of50–100 mg/kg IV following induction. More typ-ically it is given as 10–20 mg/kg IV after induc-tion and 1–2 mg/kg/h, usually for 5–6 hours.A smaller loading dose with a higher infusion ratemay provide more stable plasma levels. In adults,
tranexamic acid (TXA) administered as a bolus doseof 12.5 mg/kg over 30 minutes, 1 mg/kg in the CPBprime, and a continuous infusion of 6.5 mg/kg/hresults in a constant therapeutic plasma concentra-tion of 53 µg/mL. Similarly, TXA administered as abolus dose of 30 mg/kg over 30 minutes, 2 mg/kgin the CPB prime, and a continuous infusion of16 mg/kg/h should result in a constant therapeu-tic plasma concentration of 126 µg/mL. In chil-dren undergoing re-operative procedures, TXA ina dose of 100 mg/kg as a bolus over 30 minutes,100 mg/kg in the CPB prime, and as a continuousintra-operative infusion of 10 mg/kg/h is superiorto placebo in reducing blood loss, total transfusionrequirements and total donor unit exposure. Thedrug is renally concentrated and the infusion rateshould be decreased in accordance with creatinineclearance.
AprotininAprotinin is dosed in kallikrein inhibition units(KIU). A KIU is defined as the quantity of aprotininthat produces 50% inhibition of 2 kallikrein units.Aprotinin is packaged to contain 10 000 KIU/mLthat is equivalent to 1.4 mg/mL. Aprotinin is admin-istered to adults on a fixed dose protocol. The highdose or Hammersmith regimen consists of:• 2 million KIU (280 mg) as an IV loading dose over30 minutes after induction.• 500 000 KIU/h (70 mg/h) as an intraoperativeinfusion.• 2 million KIU (280 mg) in the pump prime.
Recent evidence suggests that dosing on a perkilogram basis provides more consistent plasmaaprotinin levels than a fixed dose regimen. Ininfants and children dosing on a per kilogram basisis more common. Given the discrepancy betweenweight and body surface area (BSA) in infants andneonates and small children it has been suggestedthat dosing on a per meter squared basis in thispatient population will produce more consistentaprotinin concentrations and less likelihood of sub-and supra-therapeutic aprotinin levels than dosingon a per kilogram basis. In addition, more consistentplasma levels are achieved if the CPB prime dose isnot based on patient weight or BSA but on the actualvolume of the CPB circuit relative to either of these

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 367 — #45
Management of Cardiopulmonary Bypass 367
two variables. Nonetheless, two commonly usedaprotinin dosing regimens for infants and childrenare as follows:• 30 000 KIU/kg as bolus to the patient and added tothe CPB prime in addition to a continuous infusionof 10 000 KIU/kg/kg.• 1.7 × 106 KIU/m2 (240 mg/m2) as a bolus tothe patient and added to the CPB prime in addi-tion to a continuous infusion of 4 × 105 KIU/m2/h(56 mg/m2/h).
The incidence of both mild and severe allergicreactions to aprotinin following initial exposureis similar in children and adults and is approxi-mately 0.5–1.0%. The incidence of both mild andsevere allergic reactions on re-exposure in adultsand children is similar and is approximately 2.8%.Up to 9% of the re-exposure reactions may befatal. The likelihood of a reaction on re-exposure isincreased if the re-exposure occurs within 6 monthsof the initial exposure with 95% of all reportedre-exposure events occurring within 6 months ofinitial exposure. Patients who are likely to haveprevious exposure are those who have undergoneprior cardiac surgical procedures including chil-dren undergoing staged procedures. In particular,bridge to cardiac transplant patients are likely tohave prior exposure. A second exposure is likely atthe time of device explantation and cardiac trans-plantation. Aprotinin use also has been extendedto noncardiac surgical procedures (orthopedics, ear,nose and throat (ENT)) and previously was used fortreatment of pancreatitis.
Neither skin testing, nor antiaprotinin IgG nor IgEantibody testing is specific enough to be clinicallyuseful for prediction of anaphylaxis on re-exposure.Very high levels of antiaprotinin IgG antibodies mayhelp identify patients at risk. It is recommended thata test dose of aprotinin 0.5 or 1.0 mL be adminis-tered before both initial and subsequent adminis-trations keeping in mind that test doses have beenreported to trigger acute reactions. If there is noreaction after 10 minutes, the bolus dose can begiven. Pre-treatment with H1, H2 antagonists andcorticosteroids prior to re-exposure has been rec-ommended but this practice has not been criticallyevaluated. In a patient with a history of prior expo-sure is probably prudent to delaying injection of the
test dose until the surgeon is ready to commenceCPB so that circulatory support can be initiatedimmediately in case of a reaction. In all patients,aprotinin should not be added to the CPB pumpprime until it is certain that the patient has notreacted to the test dose or bolus dose.
Efficacy of antifibrinolytics agentsThere are many studies examining the efficacyof EACA, TXA, and aprotinin in reducing bloodloss and allogeneric transfusion requirements.Most studies compare these agents to placebo,but some head-to-head comparison studies exist.Comparisons are complicated by the fact that notall groups use comparable dosages of these agents.In children, such determinations are more compli-cated given the large variability in patient size, typeof operative procedure, age-related distribution andelimination kinetics, CPB prime volume and theuse of ultrafiltration. There are anecdotal reports ofadverse thrombotic events such as shunt thrombosisand premature fenestration closure associated withuse of lysine analogs and aprotinin in children. Todate, there exists little objective evidence to accu-rately quantify the risk of such events with use ofthese agents.
Aprotinin• Meta-analysis of trials of aprotinin compared to aplacebo control group in adults demonstrates thathigh-dose aprotinin in effective in reducing thenumber of patients who require transfusion fol-lowing CABG, redo-CABG, CABG/valve, and valvesurgery. High-dose aprotinin also reduces the inci-dence of postoperative re-exploration for bleedingfollowing surgery.• High-dose aprotinin has been demonstrated toreduce blood loss and transfusion requirementsin patients undergoing heart, heart-hung, andlung transplantation. In addition, aprotinin reducesblood loss and transfusion requirements in patientsreceiving mechanical circulatory assist devices.• High-dose aprotinin has been demonstratedto reduce blood loss and transfusion require-ments in patients taking perioperative aspirin.Similar efficacy of high-dose aprotinin has beendemonstrated in patients taking perioperativeclopidogrel discontinued <5 days prior to surgery.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 368 — #46
368 Chapter 10
• High-dose aprotinin has been demonstrated toreduce blood loss and transfusion requirementsin patients undergoing off-pump coronary arterybypass (OBCAB).• In children with congenital heart disease under-going cardiac surgery, meta-analysis of appropriatetrials indicates that while aprotinin use reducesthe proportion of children of children receivingallogeneric transfusions it does not reduce chesttube drainage or the total volume of blood trans-fused. This analysis is plagued by the limitationthat both intra-study and inter-study variabilityin a number of parameters involving the patient(age, weight, cyanotic versus noncyanotic, proce-dure type, redo versus primary surgery), the CPBcircuit (prime volume and composition, ultrafiltra-tion use), the aprotinin dose (fixed, per kg, per m2),and the outcome variables (blood loss, transfu-sion requirement, cost analysis) make comparisonsbetween studies difficult.
Lysine analogs• At comparable doses, TXA and EACA havecomparable efficacy.• EACA and TXA are better than placebo in limitingthe number of patients transfused after CABG.• TXA and EACA are comparable to high-doseaprotinin in limiting the number of patientstransfused following CABG.• High-dose aprotinin may be superior to TXA orEACA in limiting transfusion following CABG/valvesurgery or redos. A recent propensity score analysissuggests that TXA and aprotinin have comparableefficacy in this high-risk group.• In pediatric patients undergoing primary andrepeat surgery, TXA and EACA, as compared toplacebo, reduce the number of patients being trans-fused, total blood product exposure and blood lossacross a wide age range. A well-controlled trial com-paring aprotinin to lysine analogs in children hasnot been conducted.
Special considerations regardinguse of aprotinin
Activated clotting timeKaolin ACT are used to measure Activated clottingtime (ACT) in conjunction with aprotinin use. Celite
ACT are prolonged in the presence of aprotinin dueto aprotinin inhibition of contact activation as wellas the ability of aprotinin to preferentially inhibitcelite mediated activation in vitro. Concern existsas to whether this aprotinin induced in vitro pro-longation is correlated with in vivo anticoagulation.Kaolin ACT is unaffected by aprotinin except at veryhigh plasma levels (400 KIU/mL) because kaolin isa more potent contact activating agent than celiteand kaolin binds aprotinin. While adequate hep-arinization for CPB has been demonstrated usingcelite ACT in conjunction with a lower heparindose than would be used with a kaolin ACT, themajority of centers use the kaolin ACT in conjunc-tion with aprotinin. Therapeutic plasma levels ofaprotinin also prolong both the activated partialthromboplastin time (aPTT) and the R of the throm-boelastograph (TEG) but not the prothrombin time(PT) as a result of aprotinin’s effect on contact acti-vation. This makes use of these parameters difficultin post-CPB bleeding treatment algorithms.
Renal functionAprotinin is filtered; rapidly bound to the brushborder of the proximal convoluted tubules and sub-sequently enters the cytoplasm of these tubulesby pinocytosis. Ninety percent of the administereddose appears in the cytoplasm in a few hours andremains there for 12–14 hours until metabolized.Aprotinin compromises deep cortical and medullaryperfusion and autoregulation via its tubule basedeffects on kallikrein–kinin pathways and via renalafferent arteriolar vasoconstriction. These effects areexacerbated by hypothermia.
High-dose aprotinin administration in adultsis associated with tubular proteinuria and tran-sient (1–7 days) mild plasma creatinine eleva-tions (0.5 mg/dL). Similar creatinine elevationsare seen with low-dose aprotinin (30 000 KIU/kgin the pump prime) in pediatric cardiac surgi-cal patients. The vast majority of data to dateindicates that aprotinin administration has min-imal adverse clinical effect on renal function.However, recent investigations have associatedaprotinin use with an increased risk of renal dys-function (creatinine increase) and renal failurerequiring dialysis. In addition, preoperative use ofangiotensin-converting enzyme (ACE) inhibitors in

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 369 — #47
Management of Cardiopulmonary Bypass 369
combination with intraoperative aprotinin use isassociated with a higher incidence of acute renalfailure. With these issues in mind, aprotinin shouldbe used at a reduced dosage in patients with pre-existing renal dysfunction and should not be admin-istered to patients taking ACE inhibitors at the timeof surgery.
Coronary artery bypass graft patencyConcerns that aprotinin use may contribute toearly graft occlusion or postoperative myocardialinfarction have not been substantiated.
Deep hypothermic circulatory arrestConcern has been raised regarding the use of apro-tinin in association with Deep hypothermic circu-latory arrest (DHCA) due to reports of increasedmortality, renal failure, myocardial infarction, dis-seminated intravascular coagulation, and death.Others report significant reductions in homologousblood requirements and a trend toward improvedoutcome with aprotinin despite significant, tran-sient renal dysfunction. It is unlikely that aprotininalone can be implicated in the development of renalfailure following DHCA. Previously it was thoughtthat aprotinin use was associated with thrombosisin association with DHCA, however, this thrombo-sis was due to a failure to appreciate the aprotinineffect on celite ACT resulting in sub-therapeuticheparinization. More recent reports of thrombosishave occurred in the setting of adequate hepariniza-tion emphasizing that use of aprotinin during DHCArequires further elucidation.
Post-CPB bleeding and point ofcare testing
Transfusion algorithms utilizing Post-CPB bleed-ing and point of care testing (POCT) can reducetransfusions following cardiac surgery in adults byappropriately directing the use of nonerythrocyteblood products to deal with specific coagulationabnormalities. Two such protocols utilizing POCTincluding TEG are provided in Fig. 10.13.
It should be emphasized that use of these algo-rithms are complicated by the use of aprotinin,which prolongs the aPTT, the celite ACT (and to
a lesser extent the kaolin ACT), and the R ofthe TEG.
Decannulation
Generally, the venous cannula is removed first.With the arterial cannula in place, urgent reinsti-tution of CPB can be accomplished quickly. Hemo-dynamic compromise due to atrial dysrhythmiasand volume loss may accompany removal of theatrial cannula. As long as only a small portion ofthe protamine has been infused, volume infusionvia the arterial cannula can be undertaken safely.
To avoid undue stress on the aortotomy andto allow its easy closure, the aortic systolic bloodpressure should be 100–120 mmHg in adults.Vasodilator therapy may be necessary to achievethis goal.
Pericardial and chest closure
The pericardium is not routinely closed after allcardiac surgical procedures. When a normal peri-cardium, small ventricular volumes, and low fill-ing pressures exist, pericardial closure does notaffect left ventricular diastolic or systolic function.For patients with distended ventricles, myocar-dial edema, and poor systolic function after CPB,pericardial closure may further compromise hemo-dynamics secondary to extrinsic reduction in dias-tolic filling. Chest closure may produce the sameeffects. In patients with severe post-CPB ventriculardysfunction, this compromise may prohibit peri-cardial and/or chest closure despite initiation oracceleration of inotropic and vasodilator therapy.In these patients, the chest is left open and coveredwith a piece of nonlatex rubber or an adhesive plas-tic drape, with closure accomplished 2–3 days afterthe procedure.
On occasion, one or both of the epicardial pacerwires may short out and become nonfunctionalwhen the chest is closed. Therefore, atrial and ven-tricular epicardial pacing should be checked afterthe sternal edges are allowed to fall together butbefore chest closure. If the wires become nonfunc-tional, it may be necessary for the surgeon to movethem to alternate sites on the atrium and ventriclebefore chest closure.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 370 — #48
370 Chapter 10
Microvascular bleedingby observation of
surgical field
Coagulation testsperformed
Allnormal
Surgicalre-exploration
of chest
Fibrinogen<144 mg/dL
Point-of-care
aPTT > 57 s
Point-of-care
PT >16.6 s
Thromb MA< 48 mm
PLT<102 K/mm3
and/orand/or
Platelet transfusion orDDAVP administration
Fresh frozen plasmatransfusion
Cryoprecipitatetransfusion
Microvascular bleeding
Fibrinogen
Fibrinogen <100 mg/dLTEG LY30 < 7.5%hTEG R > 20 mmTEG R > 2X hTEG R
1.Protamine Platelets FFP EACA Cryoprecipitate
2. 3. 4.
Platelet count < 100 Kand MA < 45 mm
Platelet countCelite TEG
with/without heparinase
Fig. 10.13 Two adult transfusion algorithms usingpoint-of-care testing to determine nonerythrocytetransfusion requirements. aPTT, activated partialthromboplastin time; EACA, ε-aminocaproic acid; FFP,fresh frozen plasma; hTEG, heparinasethromboelastograph; MA, TEG maximal amplitude;LY30, TEG % lysis at 30 minutes; PT, prothrombin time;R, TEG reaction time; TEG, thromboelastograph.
(From Shore-Lesserson L, Manspeizer HE, DePerio Met al. Thromboelastography-guided transfusion algorithmreduces transfusions in complex cardiac surgery. AnesthAnalg 1999;88:314 and Nuttall GA, Oliver WC,Santrach PJ et al. Efficacy of a simple intraoperativetransfusion algorithm for non-erythrocyte componentutilization after cardiopulmonary bypass. Anesthesiology2001;94:775, with permission.)
Management of unusualproblems on CPB
For patients requiring CPB, there are severalconditions that present difficult managementproblems.
Cold-reactive proteinsCold-reactive proteins are proteins that, whencooled below a specific temperature (their thermal
amplitude or critical temperature) precipitate orcause red cell agglutination. The subsequentmicrovascular occlusion can lead to cerebral andmyocardial ischemia and infarction as well ashepatic and renal dysfunction. Subsequent hemo-lysis also can complicate the picture. Patients withthese proteins present difficult management prob-lems for procedures in which systemic hypother-mia and cold cardioplegic solutions are normallyused. Cold reactive proteins can be classified

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 371 — #49
Management of Cardiopulmonary Bypass 371
as follows:• Cold agglutinins (CA). These are monoclonal orpolyclonal immunoglobulin M (IgM) antibodiesdirected against the I or i antigen of the redcell membrane. These antibodies react most effi-ciently with red cells at low temperatures. Theresult is agglutination of red cells, complement fixa-tion with subsequent microvascular occlusion, andischemia. Antibody binding occurs best at low tem-peratures, whereas complement fixation occurs bestat high temperatures. Hemolysis occurs in the ther-mal range of 10–30C because this is the optimalrange of overlap between antibody binding andcomplement fixation.
CA are more common in patients with infec-tious or lymphoproliferative diseases as well as inhuman immunodeficiency virus/acquired immun-odeficiency syndrome (HIV/AIDS) patients. Anidiopathic form of CA disease also exists. The idio-pathic form is more common in older patients andwomen, and usually involves monoclonal IgM anti-bodies to the I antigen of the red cell membrane. Theinfectious forms such as Myoplasma pneumoniatend to involve polyclonal IgM antibodies while thelymphoproliferative disorders involve monoclonalIgM antibodies. Normal persons have low titersof anti-I antibodies that react at low temperatures<20C) and are not clinically significant.
Most cases involving cold-reactive proteins andCPB are in patients with CA.• Cryoglobulins. These are serum proteins orprotein complexes that undergo reversible precip-itation at low temperatures. The result is multi-organ ischemia and dysfunction from microvas-cular occlusion. Type I cryoglobulins consist ofmonoclonal IgG (multiple myeloma) or IgM(Waldenstrom’s macroglobulinemia). Type II cryo-globulins consists of monoclonal IgM directedagainst polyclonal IgG and usually are associatedwith autoimmune, infectious, and lymphoprolif-erative disorders. Type III cryoglobulins consist ofpolyclonal IgM directed against polyclonal IgG andare associated with infections and autoimmunediseases.
There is limited experience (three reportedcases) in patients with cryoglobulins undergoingprocedures requiring CPB.
• Paroxysmal cold hemoglobinuria. These IgG anti-bodies are associated with syphilis, have a crit-ical temperature below 20C, and are potenthemolysins. There are no case reports of CPB inpatients with this disorder.
Recommendations for patients with CA1 Detection of CA over clinically relevant temper-atures can be accomplished at the time of cross-matching by direct Coombs’ tests done at 4C, 25C,and 37C. If this is positive, titers at the varioustemperatures can be performed. This will give anaccurate but not precise determination of thermalamplitude and titers preoperatively.2 Systemic temperatures are kept above the ther-mal amplitude of the CA. If DHCA is planned,the thermal amplitude of the CA must be knownto determine whether temperatures <20C arefeasible.3 Myocardial preservation can be accomplished asfollows:a Cardioplegia can be avoided entirely and warmischemic arrest can be used. This method is unac-ceptable when long cross-clamp times are expectedor when preoperative myocardial dysfunctionexists.b Warm crystalloid or blood cardioplegia can beused, but the advantages of hypothermia in reduc-ing myocardial oxygen consumption are lost. Inaddition, frequent instillations of cardioplegia willbe needed to keep the heart arrested.c Cold crystalloid cardioplegia can be used as innormal circumstances. However, the temperatureof the cardioplegia (4–8C) generally is below thecritical temperature and will initiate autoaggluti-nation. This may result in micovascular thrombusformation and infarction, nonhomogenous deliveryof cardioplegia, and hemolysis.d Delivery of warm cardioplegia followed by deliv-ery of cold cardioplegia. The right heart is com-pletely isolated with the use of bicaval cannulationand tourniquets. The right atrium is then openedto allow visualization of the coronary sinus. Warmcrystalloid cardioplegia is infused until all of theblood is washed out of the coronaries. Cold crys-talloid cardioplegia is then delivered. The pres-ence of noncoronary collaterals may add blood

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 372 — #50
372 Chapter 10
to the coronary circulation despite aortic cross-clamping. Therefore, efforts must be made to reducenoncoronary collateral flow by keeping perfusionpressures on CPB low as discussed previously.e For patients who have CA detected preopera-tively and in whom the thermal amplitude and titersare high, plasmapheresis may be used to decreasethe cold agglutinin titer and increase the marginof safety for use of hypothermia. Plasmapheresiscarries the risk of large volume shifts in patientswith limited cardiac reserve. Further, it is expen-sive, carries an infectious risk, and is of uncertainefficacy.f Efforts should be made to warm all IV fluids.g Efforts to avoid nonautologous transfusionsshould be made because donor red cells will not becoated with C3d. C3d is a component of the com-plement system, which coats some of the patient’sred cells after an episode of agglutination and affordssome protection from subsequent agglutination andlysis.h Steroids may help prevent or mitigate theagglutination and lysis process.
Sickle cell diseaseSickle cell disease (SCD) and sickle cell trait (SCT)are heredity hemoglobinopathies resulting from amutant form of the β-globin gene on chromo-some 11. This gene normally codes for the produc-tion of the β-globin chains of hemoglobin A (Hb A).The mutant gene codes for production of Hb S.SCD is present in patients who are homozygous forhemoglobin S (Hb SS). SCT is present in patientswho are heterozygous for hemoglobin S (Hb AS).Two other hemoglobinopathies exist which includehemoglobin S: Hb SC and Hb S/β-thalassemia.Some patients with these two hemoglobinopathieshave disease manifestations as severe as Hb SSpatients.
Concern in these patients centers largely on theuse of hypothermic CPB. Hypothermia without thebenefit of hemodilution can potentially increaseblood viscosity, reduce capillary perfusion, pro-mote stasis, and thus increase the risk of sickling.Furthermore, hypoxia and acidosis promote sick-ling because sickling occurs when the red cell isin the deoxygenated state. Preoperative therapy
focuses on:• reducing Hb S (the substrate for sickling);• increasing normal Hb A (the substrate foroxygen-carrying capacity).
Experience suggests that a target of Hb S < 30%and Hct > 30% is reasonable in high-risk (Hb SS,Hb SC and Hb S/thalassemia) patients prior to ini-tiation of hypothermic CPB. Transfusion alone isusually sufficient to reach a target Hct of 30%and exchange transfusions are generally required toreach both targets. Hb AS patients have been treatedwith exchange transfusions prior to CPB proce-dures, but recent experience with these patientsindicates that hypothermic CPB can be used with-out prior exchange transfusions if hemodilution isused and hypoxia and acidosis are avoided.
Heparin induced thrombocytopenia (HIT)Heparin administration normally causes an immedi-ate, transient, reversible reduction in platelet countfollowing due to induction of platelet aggrega-tion. This is commonly referred to as Type I HIT.HIT Type II (unfortunately, also commonly justcalled HIT) is an immunological process involvingthe development of anti-heparin platelet factor 4(PF4) antibodies. Heparin binds with high affin-ity to PF4 and induces a conformational changein PF4 exposing two or three epitopes capable ofbinding primarily IgG but also IgA and IgM anti-bodies. The IgG-heparin-PF4 complex then binds toplatelets via their FcγRIIa receptors. Cross-linkingof the receptors leads to platelet activation andrelease of PF4 from α-granules. Platelet bound PF4on activated platelets complexes with heparin andIgG binds to this complex via its Fab domain leav-ing its Fc domain free to bind to and activatean adjacent platelet via its FcγRIIa receptor. Thisamplification process leads to intense platelet acti-vation and aggregation with subsequent productionof procoagulant microparticles.
HIT is a clinicopathologic syndrome generallydefined as a ≥50% reduction in platelet countand a positive assay for anti-heparin/PF4 antibodiesoccurring between 5 and 10 days following expo-sure to UFH. Heparin-induced thrombocytopeniawith thrombosis or skin lesions (HITT) is a severeform of HIT with high morbidity and mortality.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 373 — #51
Management of Cardiopulmonary Bypass 373
Two types of assays (antigenic and functional/biologic) are currently used for detection of anti-heparin PF4 antibodies. ELISA capable of detectingIgG, IgA, and IgM antibodies to PF4 are com-mercially available. The most commonly utilizedfunctional assay is the 14C-serotonin release assay(SRA). Washed donor platelets previously incu-bated with 14C-serotonin are mixed with subjectplasma suspected to contain to anti-heparin PF4antibodies. In vitro platelet activation is quanti-tated by measurement of released 14C-serotonin.As such this assay is capable of detecting onlytiters of anti-heparin PF4 antibodies high enoughto induce platelet aggregation. This assay is techni-cally demanding to perform and requires speciallydesigned equipment.
The incidence of anti-heparin PF4 antibody for-mation in cardiac surgical patients prior to surgeryis approximately 13–19%, while the incidence fol-lowing cardiac surgery is approximately 50% by
ELISA and 20% by SRA. In the absence of continuedexposure to UFH there should be clearance of anti-heparin PF4 antibodies within 2–6 weeks. ClinicalHIT occurs in approximately 2% of patients follow-ing cardiac surgery with about half of those patientsexperiencing associated thrombosis.
In a patient suspected of having HIT prior to car-diac surgery or in a patient with a previous historyof HIT scheduled for cardiac surgery the algorithmpresented in Fig. 10.14 is useful.
The best available strategies for anticoagulationfor CPB in patients with anti-heparin PF4 antibodiescan be summarized as follows:• Direct thrombin inhibitors (DTI) without UFH. Theactive-site pocket of thrombin catalyzes most of thefunctions of thrombin while the fibrinogen-bindingsite (exosite 1) mediates binding of thrombin tofibrinogen. Exosite 2 is the heparin-binding site.Hirudin is the most potent DTI known, isolatedfrom the salivary glands of the medicinal leech. It is
Positive Negative
YesNo
Avoid UFH before and after surgeryand
CPB anticoagulation with UFH
Alternative CPB anticoagulation(see text)
Wait until anti-heparin PF4antibody test is negative
(2–6 weeks)
Urgent surgery
Suspected HITOR
Previous history of HIT
Anti-heparin PF4 antibody testing
Fig. 10.14 Algorithm outlining care of patients with heparin-induced thrombocytopenia (HIT) or suspected HIT.CPB, cardiopulmonary bypass; UFH, unfractionated heparin; PF4, platelet factor 4.

Alice Nelson Dinardo: “ch10” — 2007/7/16 — 12:40 — page 374 — #52
374 Chapter 10
a bivalent thrombin inhibitor as it binds to both pre-viously described active sites. It binds to both solubleand fibrin bound thrombin. The clinically availabledirect thrombin inhibitors used in place of UFH forCPB are:a Lepirudin (recombinant hirudin) is an irreversiblybinding bivalent thrombin inhibitor.b Bivalirudin is a synthetic peptide analog ofhirudin and is a bivalent thrombin inhibitor. Unlikelepirudin it reversibly binds to thrombin.c Argatroban is a monovalent synthetic thrombininhibitor with reversible activity at the active-sitepocket of thrombin. Argatroban does not bind toexosite 1.There is no antidote available for the reversal ofthe anticoagulant effect of DTI in the sense thatUFH is reversible with protamine. Termination ofDTI effect is dependent on metabolism, redistri-bution, and elimination of the drug. In the caseof bivalirudin and argatroban disassociation of thedrug from thrombin also plays a role.
The ecarin clotting time (ECT) is used to monitorthe anticoagulant effect of lepirudin and bivalirudin.The ECT is a modification of the ACT that uses ecarinas an activator. Ecarin activates prothrombin tothe intermediate thrombin product meizothrombin.Meizothrombin has limited procoagulant activityas compared to thrombin. However, like throm-bin it binds to lepirudin and bivalirudin with 1:1stoichiometry. The ECT will thus be prolongedby DTI with the ECT determined by the relativeconcentrations of meizothrombin and lepirudin orbivalirudin. There is good correlation between ECTand plasma levels of lepirudin and bivalirudin.Unfortunately, the ECT is not commercially avail-able for point of care testing and must be run in ahospital-based laboratory.• Platelet inhibition in association with standard UFHuse. Heparin dependant platelet activation in thepresence of HIT antibodies can be achieved with acontinuous IV infusion of prostaglandin I2 (prosta-cyclin). Iloprost and Flolan (epoprostenol) are stable
forms of prostacyclin that have been used success-fully in conjunction with standard UFH doses forCPB. Success has also been reported with use of con-tinuous IV infusion of prostaglandin E2 but this hasnot been as rigorously investigated. Other plateletinhibiting drugs such as dipyridamole and aspirinhave been used in conjunction with these agentsas well. Recently, success with use of a continuousIV infusion of tirofiban (a short acting GP IIb/IIIainhibitor) in conjunction with standard UFH hasbeen reported.
Suggested reading
Arnold DM, Fergusson DA, Chan AK et al. Avoiding trans-
fusions in children undergoing cardiac surgery: a meta-
analysis of randomized trials of aprotinin. Anesth Analg
2006;102:731–7.
Barak M, Katz Y. Microbubbles: pathophysiology and
clinical implications. Chest 2005;128:2918–32.
Despotis GJ, Gravlee G, Filos K, Levy J. Anticoagulation
monitoring during cardiac surgery: a review of cur-
rent and emerging techniques. Anesthesiology 1999;91:1122–51.
Kanazawa M, Fukuyama H, Kinefuchi Y, Takiguchi M,
Suzuki T. Relationship between aortic-to-radial arte-
rial pressure gradient after cardiopulmonary bypass and
changes in arterial elasticity. Anesthesiology 2003;99:48–53.
Kimmel SE, Sekeres MA, Berlin JA et al. Risk factors
for clinically important adverse events after protamine
administration following cardiopulmonary bypass. J Am
Coll Cardiol 1998;32:1916–22.
McKinlay KH, Schinderle DB, Swaminathan M et al.
Predictors of inotrope use during separation from
cardiopulmonary bypass. J Cardiothorac Vasc Anesth
2004;18:404–8.
Viaro F, Dalio MB, Evora PR. Catastrophic cardiovascular
adverse reactions to protamine are nitric oxide/cyclic
guanosine monophosphate dependent and endothe-
lium mediated: should methylene blue be the treatment
of choice? Chest 2002;122:1061–6.
Warkentin TE, Greinacher A. Heparin-induced throm-
bocytopenia and cardiac surgery. Ann Thorac Surg
2003;76:2121–31.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 375 — #1
CHAPTER 11
Mechanical Circulatory Support
This chapter focuses on mechanical circulatorysupport devices currently available for clinical usein the United States. The intra-aortic balloon pump(IABP), centrifugal pumps, axial flow pumps, ven-tricular assist devices (VAD), and the total artificialheart (TAH) will be covered. These devices aresummarized in Tables 11.1–11.3.
Indications for mechanicalcirculatory support
The indications for mechanical circulatory supportare the presence of left ventricular (LV) failure,right ventricular (RV) failure, or both in the set-ting of maximal intravenous (IV) inotropic supportfollowing correction of acid-base and electrolyteabnormalities and hypovolemia. Maximal inotropicsupport is defined as use of two or more of thefollowing:• Dobutamine >10µg/kg/min.• Dopamine >10µg/kg/min.• Epinephrine >0.2µg/kg/min.• Milrinone >0.75µg/kg/min, after a loading doseof 50µg/kg/min.Ventricular failure is defined as one or both of thefollowing:• LV dysfunction:a cardiac index < 1.8–2.0 L/min/m2;b systolic blood pressure < 90mmHg or meanarterial pressure (MAP) < 70mmHg;c left atrial (LA) pressure > 18–25mmHg;
• RV dysfunction:a cardiac index < 1.8–2.0 L/min/m2;b systolic blood pressure < 90mmHg or MAP <
70mmHg;c right atrial (RA) pressure > 18–20mmHg.
Device selection
The type of mechanical circulatory device selecteddepends, in large part, on the setting in which thedevice is to be used. The goal of mechanical sup-port is to initiate support prior to development ofend-organ dysfunction and to prevent end-organdysfunction from developing. Mechanical circula-tory assist devices are currently used in three majorcapacities.
Bridge to recoveryTemporary circulatory support is used in the subsetof patients with cardiogenic shock in whom recov-ery of significant myocardial function is expected.Patients in this category receive short-term to inter-mediate (days to weeks) mechanical circulatorysupport during a critical interval while ventricularfunction recovers. The assist device is then weanedand explanted. The most common indications forthis type of circulatory support are:• Postcardiotomy cardiogenic shock. This is esti-mated to occur in 2–6% of all patients undergoingsurgery for coronary revascularization or valverepair or replacement. One percent of all these
375

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 376 — #2
376 Chapter 11
Table 11.1 Extracorporeal devices.
Device Mechanism Support Indications
IABP Pneumatic counterpulsation LVAD Short term• postcardiotomy
ECMO Centrifugal or Partial or total CPB Short term (adults)nonocclusive roller head • postcardiotomy
Nonpulsatile • post-cardiac arrest
Short to intermediate term(infants/children)• postcardiotomy• post-cardiac arrest• bridge-to-transplant
BioMedicus Centrifugal LVAD and/or RVAD Short termNonpulsatile In parallel • postcardiotomy
TandemHeart Centrifugal LVAD Short termNonpulsatile In parallel • postcardiotomy
• post-catheter intervention
Abiomed Pneumatic membrane LVAD and/or RVAD Short termBVS 5000 Pulsatile In parallel • postcardiotomy
Thoratec Pneumatic membrane LVAD and/or RVAD Short to intermediate termPulsatile In series or in parallel • postcardiotomy
• bridge-to-transplant
Abiomed Pneumatic membrane LVAD and/or RVAD Short to intermediate termAB5000 Pulsatile In series or in parallel • postcardiotomy
• bridge-to-transplant
Berlin Heart Pneumatic membrane LVAD and/or RVAD Short to intermediate termPulsatile In series or in parallel • postcardiotomy
• bridge-to-transplant• pediatric sizes
Medos VAD Pneumatic membrane LVAD and/or RVAD Short to intermediate termPulsatile In series or in parallel • postcardiotomy
• bridge-to-transplant• pediatric sizes
ECMO, extracorporeal membrane oxygenation; LVAD, left ventricular assist device; RVAD, right ventricular assist device;VAD, ventricular assist device.
postcardiotomy patients require mechanical circu-latory support. This is probably the largest patientsubset requiring bridge to recovery support. The useof centrifugal pumps and VAD as temporary circula-tory support in patients with cardiogenic shock aftercardiac surgical procedures has been less success-ful than the bridge to transplantation experience.Although small individual series have survival rates
as high as 40%, the Combined Registry for theClinical Use ofMechanical Ventricular Assist Pumpsand Artificial Hearts reports that the overall hospi-tal discharge rate is 25%. This low survival rate issimilar for patients supported with both VAD andcentrifugal pumps. Factors that have been asso-ciated with poor outcome include renal failure,perioperative myocardial infarction, and infection.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 377 — #3
Mechanical Circulatory Support 377
Table 11.2 Intracorporeal devices.
Device Mechanism Support Indications
HeartMate IP Pneumatic pusher plate LVAD Intermediate to long termPulsatile In series • bridge-to-transplant
• destination therapy
HeartMate XVE Electric pusher plate LVAD Intermediate to long termPulsatile In series • bridge-to-transplant
• destination therapy
Novacor Electric pusher plate LVAD Intermediate to long termPulsatile In series • bridge-to-transplant
• destination therapy
Jarvik 2000 Electric axial flow LVAD Intermediate to long termNonpulsatile In series • bridge-to-transplant
• destination therapy
MicroMed VAD Electric axial flow LVAD Intermediate to long termNonpulsatile In series • bridge-to-transplant
• destination therapy• pediatric version
HeartMate II Electric axial flow LVAD Intermediate to long termNonpulsatile In series • bridge-to-transplant
• destination therapy
LVAD, left ventricular assist device; VAD, ventricular assist device.
Table 11.3 Orthotopic prosthetic ventricles.
Device Mechanism Support Indications
CardioWest Pneumatic membrane Total artificial heart Intermediate to long termPulsatile • bridge-to-transplant
Abiocor Electrohydralic membrane Total artificial heart Intermediate to long termPulsatile • bridge-to-transplant
• destination therapy
Most patients who do survive are New York HeartAssociation (NYHA) functional class I or II.• Post acute-myocardial infarction (MI) cardiogenicshock.• Myocarditis-induced cardiogenic shock.• Support during medical or ablative therapy forintractable dysrhythmias.• Support during or following complicatedinterventional cardiac catheterization procedures.
Bridge to cardiac transplantationIn the case of a bridge to transplantation, a mechan-ical assist device is implanted with the intentionof providing intermediate to long-term (weeks tomonths) support until a suitable donor heart isfound or until the patient dies from irreversibledamage to other organ systems. Devices used for abridge to transplantation must allow patient mobi-lization and discharge from an intensive care unit

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 378 — #4
378 Chapter 11
Table 11.4 Criteria for left ventricular assist device(LVAD) placement as a bridge to cardiac transplantation.
Inclusion criteria1 Patient is a transplant candidate2 Hemodynamic data:
Cardiac index < 2.0 L/min/m2
Systolic BP < 80 mmHgPAOP > 20 mmHg
Exclusion criteria1 Technical issues:
BSA < 1.5 m2
Aortic valve insufficiency (if valve not repaired orreplaced with a bioprosthesis)
Right-to-left intracardiac shunt (if left unrepaired)Severe aortic atherosclerotic diseaseAbdominal aortic aneurysmMechanical cardiac valvesLV thrombus
2 Fixed PVR with PVR > 8 Wood units3 Factors deemed to increase perioperative risk:
Mechanical ventilationUrine output < 30 mL/hPyrexiaElevated WBC countRAP > 16 mmHgPT > 16 secondsRe-operation
BP, blood pressure; BSA, body surface area; LV, left ventricle;PAOP, pulmonary artery occlusion pressure; PT, prothrom-bin time; PVR, pulmonary vascular resistance; RAP, rightatrial pressure; WBC, white blood cell.
(ICU) setting because the wait for a donor heartmay be long. The criteria for use of a left ventricularassist device (LVAD) as a bridge to transplantationare shown in Table 11.4.At present, the limiting factor in the number of
patients who can be offered a heart transplant isthe availability of donor hearts. It is estimated thatwhile 5–10% of the total population suffers fromend-stage, refractory heart failure that could ben-efit from a heart transplant, only approximately2500 donor hearts are available per year. Further-more, 25–30% of suitable transplant candidates diebefore a donor heart can be found. In the subsetof heart failure patients eligible for mechanical sup-port up to 70%will die without mechanical support
while awaiting transplant. As a result, mechanicalassist devices and the TAH are being used withgreater frequency as a bridge to cardiac trans-plantation. For transplant candidates at immediaterisk of end-organ dysfunction, these devices pro-vide mechanical circulatory support until a suitabledonor heart is found.The outcome after bridge to transplantation
is very good. Currently, approximately 70% ofpatients who receive an assist device as a bridgesurvive to transplant and 70% of those patientsgo on to hospital discharge. After hospital dis-charge, LVAD patients without pre-existing organdysfunction have 1- and 2-year actuarial survivalrates similar to patients receiving orthotopic hearttransplantation without mechanical circulatorysupport.The HeartMate (IP, XVE, and II), Novacor,
MicroMed, and Jarvik 2000 devices are all intra-corporeal (implantable) devices used exclusivelyfor bridge to transplantation in patients requiringonly LV support. The Thoratec VAD and AbiomedAB5000 also can be used in this capacity. Bridge totransplantation patients who require biventricularassist device (BiVAD) support are candidates for aTAH, the Thoratec VAD, or the Abiomed AB5000.In infants and small children the Berlin Heart orMedos VAD could serve this purpose.
Destination therapyIn this setting permanently implanted LVAD serveas an alternative to chronic medical therapy inpatients who are not cardiac transplant candidates.In general, patients selected for destination ther-apy are older (age >65 years) with end-organ dys-function from diabetes or other chronic medicalproblems and with other significant physical and/orpsychiatric co-morbidities. The REMATCH trial,which made use of the HeartMate XVE devicedemonstrated improved survival and quality of lifeover a 2-year period in patients with an implantedVADas compared to patients receiving chronicmed-ical therapy. Currently, the HeartMate XVE device isFood and Drug Administration (FDA) approved forthis purpose and the Novacor device is undergoingtrials for this use in the RELIANT Trial. As shown

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 379 — #5
Mechanical Circulatory Support 379
in Table 11.2, other devices are likely to be used inthis capacity in the future.
Complications
Thromboembolism, perioperative hemorrhage, andinfection are the three major complications associ-ated with use of circulatory assist devices and theTAH, particularly when used long term for a bridgeto transplantation or destination therapy.
Classification of devices
Several classifications of mechanical circulatorysupport devices exist, and there is considerableoverlap between classifications.
Orthotopic and heterotopic prostheticventriclesHeterotopic prosthetic ventricles provide mechan-ical support in parallel or in series with the intactnative ventricles. These devices are commonlycalled ventricular assist devices (VAD). Some VADare designed only for LV support, whereas othersmay be used for left ventricular (LVAD), right ven-tricular (RVAD), or biventricular support (BiVAD).Table 11.1 summarizes the uses of the clinicallyavailable devices.Orthotopic devices providemechanical support in
place of the excised native ventricles. The nativeatria are surgically placed in continuity with theprosthetic ventricles. Orthotopic prosthetic ventri-cles are described more commonly as total artificialhearts (TAH).
Series versus parallel circulatorysupportA circulatory support device may be used in paral-lel or in series with the native ventricular system,depending on how cannulation for the device isachieved. When inflow to the device is achievedvia cannulation of the native atrium and outflowis via cannulation of the corresponding great vessel,the device is said to be “in parallel” with the nativeventricular system. When inflow to the device isachieved via cannulation of the apex of the native
Ao LA PA RA
LRL
Ao Apex
(a) (b)
Fig. 11.1 (a) Schematic of a Thoratec ventricularassist device (VAD) in parallel with the left heart.(b) Schematic of a Thoratec VAD in parallel with theright heart and in series with the left heart. Ao, aorta;LA, left atrium; PA, pulmonary artery; RA, right atrium.
ventricle and outflow is via cannulation of the cor-responding great vessel, the device is said to be“in series” with the native ventricle. Some devicesalways are used in series with the native ventri-cle, some are always used in parallel, and some canbe used in either a series or parallel arrangement.Figure 11.1a,b illustrates parallel and series arrange-ment. Tables 11.1 and 11.2 describe which devicesare used in series and in parallel.In general, the series arrangement provides better
filling and a higher device output for two rea-sons. First, the device does not compete with thenative ventricle for atrial blood the way it must ina parallel arrangement. Second, native ventricularsystole serves to fill the prosthetic ventricle. Theseries arrangement also provides the native ven-tricle with a low-impedance outflow tract into theprosthetic ventricle, which greatly reduces nativeventricular diameter and systolic wall stress. Themajor disadvantage of a series arrangement is thatthe ventricular apex may become akinetic or dys-kinetic after removal of the ventricular cannula. Forpatients who are to be transplanted, this is not animportant issue. However, it is a very importantissue for patients who are ultimately to be weanedoff mechanical support.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 380 — #6
380 Chapter 11
Pulsatile versus nonpulsatile flowBoth orthotopic and heterotopic prosthetic ventri-cles provide pulsatile flow, whereas centrifugal andaxial pumps provide nonpulsatile flow. Two types ofpulsatile prosthetic ventricles are currently in use:pneumatic and electromechanical. Pulsatile pneu-matic pumps use pressurized air to eject bloodfrom the prosthetic ventricular chamber. Pulsatileelectromechanical pumps convert electrical energyto the mechanical energy necessary to eject bloodfrom the prosthetic ventricular chamber.
Extracorporeal versus intracorporeal(implantable) devicesSome devices are extracorporeal, whereas othersare intracorporeal. With extracorporeal devices, thepumping device is located outside the body, withboth the inflow and outflow conduits enteringthe patient’s thoracic cavity. Implantable devicesare implanted in the patient’s pericardial cavityor pre-peritoneally. Anatomical constraints gen-erally make it difficult to implant intracorporealdevices into patients with a body surface area(BSA) < 1.5m2.
Triggering modes and percentage ofsystolePulsatile pumps have a number of different waysin which ejection can be triggered. In the case ofTAH, the ejection rate is set by the operator and isanalogous to the heart rate. Because VAD are usedin conjunction with the native ventricular system,more options are available to trigger a VAD ejectioncycle.
ManualThis mode, also known as the single stroke mode, isused for de-airing of the device after implantation.It allows a single ejectionwith the touch of a button.
AsynchronousIn the asynchronous mode, the VAD ejects at a ratedecided upon by the operator. This produces a fixedrate, variable stroke volume mode of operation. Athigher device rates, the time available for diastolicfilling will be reduced. This can in part be offset byincreasing preload to the device. In this mode there
will be beats in which the device and the ventricleeject at the same time.
Fill-to-emptyIn this mode, also known as the volume mode, thedevice is programmed to trigger ejection only whenthe VAD is filled with blood in diastole. This pro-duces a fixed stroke volume variable rate mode ofoperation. In this triggering mode, the VAD ejec-tion rate will vary with preload. When preload tothe VAD is high, the VAD ejection rate will be high;likewise, when preload to the VAD is poor, the VADejection rate will be low.Device and ventricular ejection rates will dif-
fer and will vary phasically. In the case of seriesLVAD, aortic valve opening is rarely seen at restin this mode but may be present during exercise.In a series device, when device filling coincideswith LV diastole, filling is said to be synchronous.In this setting, LV volume at the commencementof LV contraction is small and ejection is insuffi-cient to open the aortic valve. In a series device,when device filling coincides with LV systole, fillingis said to be counter-synchronous. In this setting,there is no ejection out of the aortic valve as thelow-impedance pathway during native ventricularsystole is into the device.
SynchronousIn the synchronous mode, an external electrical sig-nal, usually the R wave of the electrocardiogram(ECG) is used to trigger VAD ejection. Using a pro-grammable delay, the operator can use this modeto reduce ventricular afterload by preventing thedevice from ejecting into the aorta or pulmonaryartery at the same time as the native ventricle.In addition to having various triggering modes,
some devices allow the operator to program the per-centage of systole. This allows the operator to decidewhat percentage of each prosthetic ventricular cycleis devoted to ejection. Obviously, as the prostheticventricular ejection rate increases, the time betweencycles diminishes. The advantage of reducing thepercentage of systole is that it allows a greater pro-portion of each cycle to be devoted to prostheticventricular filling. However, for a given ejectionrate, reducing the percentage of systole increases

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 381 — #7
Mechanical Circulatory Support 381
the rapidity of the ejection phase. The more rapidthe ejection phase, the more likely are turbulentflow and damage to formed blood elements withresultant hemolysis.
Device description
Intra-aortic balloon pumpThe Intra-aortic balloon pump (IABP), first intro-duced into clinical use in 1968, has become animportant method of providing circulatory supportin a wide variety of patients.The IABP consists of a catheter-mounted balloon,
a pump, a gas source, and a microprocessor console.The balloon is thin-walled, measures 2×20 cm, andcontains 30–40mL of volume when inflated. Thecatheter has a hollow central lumen, which allowspercutaneous placement over a guide wire, as wellas the recording of central aortic pressure. The pumpinflates and deflates the balloon at precisely timedintervals, with either carbon dioxide or helium asthe inflating or shuttle gas. Carbon dioxide car-ries less of an embolic risk if the balloon rupturesbecause it is absorbed quickly. Helium has a lowerdensity, allowing faster inflation and deflation, andcurrently is the preferred gas. The console displaysthe ECG, the arterial waveform, and the balloonpressure trace. The console controls exactly whenthe pump inflates and deflates the balloon.Proper functioning of the IABP depends on
the precise timing of balloon inflation anddeflation relative to the cardiac cycle. Ballooninflation (Fig. 11.2) optimally occurs immediatelyafter the closure of the aortic valve as representedby the dicrotic notch on the central arterial pres-sure tracing. The resultant increase in aortic volumeincreases diastolic arterial pressure (diastolic aug-mentation) and improves systemic and coronaryartery perfusion pressure. The increase in aorticdiastolic pressure depends on a number of vari-ables: the nonaugmented aortic diastolic pressure,the compliance of the aorta, the size of the balloon,and the volume of gas in the balloon (fromminimalto full volume). Balloon inflation in the noncompli-ant aorta of an elderly patient will produce a higheraugmented diastolic pressure than the same balloonin a compliant aorta.
Inflation
Fig. 11.2 A properly positioned intra-aortic balloonpump (IABP) inflating in the proximal descending aorta.
In the absence of coronary stenoses, augmen-tation of aortic diastolic blood pressure increasescoronary blood flow in both the proximal and distalcoronary arteries. In the presence of critical coro-nary stenoses, the IABP does not improve coronaryblood flow distal to the stenoses. It is conceivablethat coronary beds distal to a stenosis could haveimproved coronary perfusion with IABP counter-pulsation if collaterals from a nonstenosed coronaryartery supply the beds.Deflation of the balloon (Fig. 11.3) is adjusted to
occur immediately before LV ejection, at the onsetof the upstroke of the central arterial waveform.Optimal balloon deflation is established when thearterial diastolic pressure is maximally reduced(unloading). The duration of isovolumic contractionof the left ventricle is determined by the pres-sure gradient between the left ventricle and theproximal aorta. Balloon deflation quickly lowersproximal aortic pressure, thereby reducing afterloadby decreasing the impedance to ejection out the leftventricle. This shortens the duration of isovolumiccontraction, which in turn reduces myocardial oxy-gen consumption. Reduction of myocardial oxygenconsumption, rather than augmentation of coro-nary blood flow, is the primary method by whichthe IABP ameliorates myocardial ischemia.In addition to reducing myocardial oxygen con-
sumption, properly timed IABP deflation improves

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 382 — #8
382 Chapter 11
Deflation
Fig. 11.3 A properly positioned intra-aortic balloonpump (IABP) deflating in the proximal descendingaorta.
LV systolic function on a beat-to-beat basis bydecreasing systolic wall stress. Increases in ejectionphase indices of systolic function, such as ejectionfraction, are directly proportional to IABP-induceddecreases in systolic wall stress.
Indications and contraindicationsThe indications for IABP use are summarizedbelow:1 Patients with refractory myocardial ischemia.2 Patients with cardiogenic shock:a myocardial infarction;b myocarditis;c cardiomyopathy;d pharmacologic depression.3 Stabilization of patients before cardiac surgery:a myocardial infarction;b postinfarction ventricular septal defect (VSD);c mitral regurgitation;d bridge to cardiac transplantation.4 Support of patients after cardiac surgery:a reversible LV dysfunction;b intraoperative myocardial infarction;c allograft dysfunction after heart transplantation.5 Support of non cardiac surgical patients:a support during percutaneous coronaryangioplasty;
b to maintain coronary artery patency after throm-bolytic therapy or angioplasty in the setting of acutemyocardial infarction;c support during noncardiac surgical procedures.There are few absolute contraindications to the useof the IABP. Aortic valve incompetence is a con-traindication because balloon inflation in diastolewill increase the regurgitant fraction. Aortic dis-section and aortic aneurysm are contraindicationsbecause balloon inflation could promote frank aor-tic rupture. Severe peripheral vascular disease maymake placement of the IABP via the femoral arteryimpossible.
InsertionMost IABP catheters are inserted percutaneouslyusing the Seldinger technique via the femoral arteryretrograde into the descending aorta. Surgical cutdown to expose the femoral artery, followed bycannulation of the artery under direct vision usingthe modified Seldinger technique, is reserved forsituations in which location of the femoral arterypercutaneously may be difficult, such as withhypotension, lack of pulsatile flow on cardiopul-monary bypass (CPB), obesity, and peripheral vas-cular disease. The IABP usually is placed throughan arterial sheath, but newer models allow place-ment of the IABP catheter directly into the femoralartery without a sheath. This is a useful alterna-tive for patients with small femoral arteries or withperipheral vascular disease.The balloon should be placed so that the prox-
imal tip is distal to the left subclavian artery andthe distal end is proximal to the renal arter-ies. The length of IABP catheter required is esti-mated by the distance from the femoral artery tothe sternomanubrial junction. Final position canbe verified with a chest radiograph, fluoroscopy,transesophageal echocardiography (TEE), or directpalpation of the descending aorta by thesurgeon.When severe peripheral vascular disease pre-
cludes retrograde insertion via the femoral artery,the balloon catheter can be placed antegrade inthe descending thoracic aorta via the right subcla-vian artery, the axillary artery, or the ascendingaorta. Placement via the ascending aorta requires

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 383 — #9
Mechanical Circulatory Support 383
a sternotomy. The technique is used only forpostcardiotomy patients who cannot otherwise beweaned from CPB and necessitates subsequentremoval under anesthesia in the operating room.
ComplicationsThe incidence of complications from intra-aorticballoon counterpulsation that are severe enoughto require balloon removal or surgical interventionranges from 17 to 35%. The most common com-plication is lower limb ischemia. However, thereare reports of every major branch of the aortabeing occluded by thrombus, embolus, or balloon-induced dissection. Other complications includethrombocytopenia and balloon or console failure.
Management of the IABPOptimal performance of the IABP depends onproper triggering and timing. The microprocessor iscapable of using a number of signal modalities totrigger IABP inflation and deflation.• ECG. This is the signal most commonly used totrigger the IABP. The R wave is used as the cen-tral timing event that directs balloon inflation tooccur during the T wave (diastole) and balloondeflation immediately before the subsequent QRScomplex (onset of systole). Due to the time neces-sary for Rwave detection, and for the timenecessaryto shuttle helium out of the balloon, triggeringIABP deflation from the immediately precedingR wave generally results in less than optimal tim-ing and unloading. As a result, consoles detect theR wave and inflate in diastole after a preset inter-val that allows completion of mechanical systole.After another preset interval, the balloon deflatesin anticipation of the next mechanical systole.The ECG signal to the IABP console can be
the ECG transmitted by a cable from the oper-ating room monitor or the ECG derived from aseparate set of patient leads directly to the IABPconsole. The former is preferable if the skin leadshave not been placed before surgical prepping anddraping. Radiofrequency current from the electro-cautery used in the operating room can interferewith the ECG trigger. The IABP leads have a specialbuilt in radiofrequency filter that helps alleviate thisproblem. Alternatively, using the operating room
monitor in the more heavily filtered nondiagnos-tic mode will help filter out some of the noise.Other maneuvers that diminish the effect of radio-frequency current include placing all ECG leads ina single frontal plane, which reduces the potentialdifference between any of the leads, and usingthe lowest electrocautery current setting possible,in short bursts. In the ECG triggering mode pacerspikes are rejected as a triggering stimulus by themicroprocessor.• Arterial waveform. The upstroke of the arterialwaveform can be used by the microprocessor in amanner similar to the R wave of the ECG. A pres-sure trigger threshold (systolic pulse height frombaseline) between 7 and 30mmHg can be set.• Internal. This mode is used during a systole, CPBor ventricular fibrillation. A fixed rate of 80 b/minor a variable rate of 40–120 b/min in increments offive can be set. Some models allow fixed internalrates of 40, 60, 80 or 120 b/min.• Pacer spikes. Atrial, ventricular, and atrioventricu-lar (AV) sequential pacer spikes can complicate bal-loon triggering. IABP consoles can be programmedto use the atrial and/or ventricular pacer spikes as atrigger or to ignore (“reject”) the pacer spikes. Withsome consoles, when the balloon is in the ECG trig-ger mode, pacer spike rejection is automatic. If themicroprocessor has difficulty ignoring a pacer spike,the use of bipolar pacing or ECG leads thatminimizethe pacer spikes may be necessary. Pacer spikes areused as triggers only when an ECG trigger is noteffective.Although the ECG is normally used to trigger
balloon inflation and deflation, proper counter-pulsation timing can only be confirmed by exam-ination of an arterial pressure waveform. Whenthe radial artery is transduced, there is a 60msdelay in waveform transmission from the centralaorta. When the femoral artery is used, there is a120ms delay in waveform transmission from thecentral aorta. Inflation using these arterial pressure-monitoring sites must be adjusted accordingly. Ide-ally, balloon inflation occurs at the dicrotic notch inthe central aorta. When the radial artery pressureis monitored, inflation should be adjusted to occur60ms before the radial artery dicrotic notch. Whenthe femoral artery pressure is monitored, balloon

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 384 — #10
384 Chapter 11
140
120
mm
Hg
100
Assistedsystole
Diastolicaugmentation
Assisted aorticend diastolic
pressure
Assistedsystole
80
Fig. 11.4 Arterial pressure trace froma patient receiving 1:1 intra-aorticballoon pump (IABP) support withproper timing.
140Unassisted systole
Unassisted aorticend diastolic
pressureAssisted aorticend diastolic
pressure
120
100
80
Assistedsystole
Diastolicaugmentation
mm
Hg
Fig. 11.5 Arterial pressure trace froma patient receiving 1:2 intra-aorticballoon pump (IABP) support withproper timing.
inflation should be adjusted to occur 120ms beforethe femoral artery dicrotic notch.The details of proper timing are illustrated in
Figs 11.4–11.7. Proper timing requires that theIABP be triggered every second or third R wave(1:2 or 1:3). This allows observation of assisted andunassisted systole and of assisted and unassistedaortic end-diastolic pressure. Some IABP consolescontain a “verify” option that highlights the periodof balloon inflation in real time on the arterialwaveform (Fig. 11.8). This feature is a useful aidin obtaining proper timing. Timing may be accom-plished in the automatic ormanualmode. The auto-matic mode uses the R wave and an algorithm thattriggers balloon inflation after an interval based onheart rate, which allows completion of mechanicalsystole. Balloon deflation is triggered after anotherpreset interval based on heart rate. Fine-tuning oftiming is obtained by use of the inflation and defla-tion controls on the console (Fig. 11.9). Inflation is
made to occur later in the cardiac cycle by using therightward facing “Later” arrow or by moving theinflation slide “out” or to the right on older mod-els. Inflation is made to occur earlier in the cardiaccycle by using the leftward facing “Earlier” arrow orby moving the inflation slide “in” or to the left onolder models. A similar control slide is used to finetune deflation. In the manual mode, the inflationand deflation slides are much more responsive andcause greater changes in timing than they do in theautomatic mode. In the manual mode, changes inheart rate >10 b/min require retiming. In the auto-matic mode, changes in heart rate are adjusted forautomatically.Observation of the balloon pressure waveform
also yields useful information about IABP function(Figs 11.10–11.12).Timing will be complicated by the presence of
arrhythmias and large variations in heart rate.Recall that the timing of balloon deflation in systole

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 385 — #11
Mechanical Circulatory Support 385
Inflation of the IAB prior to aortic valve closure
Waveform characteristics:
• Inflation of IAB prior to dicrotic notch • Diastolic augmentation encroaches onto systole (may be unable to distinguish)
Physiologic effects: • Potential premature closure of aortic valve • Potential increase in LVEDV and LVEDP or PCWP • Increased left ventricular wall stress or afterload • Aortic regurgitation • Increased MVO2 demand
Inflation of the IAB markedly after closure of the aortic valve
Waveform characteristics: • Inflation of the IAB after the dicrotic notch • Absense of sharp V • Sub-optimal diastolic augmentation
Physiologic effects: • Sub-optimal coronary artery perfusion
Unassistedsystole
Diastolicaugmentation
Assistedsystole
Assisted aorticend diastolic
pressure
Unassistedsystole
Diastolicaugmentation
Assisted systole
Dicroticnotch
Assisted aorticend diastolic
pressure
(a) Early inflation
(b) Late inflation
Fig. 11.6 Arterial waveforms resulting from (a) early balloon inflation and (b) from late balloon inflation. Thephysiologic consequences of these timing errors are summarized. IAB, intra-aortic balloon; LVEDP, left ventricularend-diastolic pressure; LVEDV, left ventricular end-diastolic volume; PCWP, pulmonary capillary wedge pressure.
is determined by a preset interval from the previousQRS. As a result, premature beats or acute increasesor decreases in heart rate may result in poor timing.Newer software allows better adjustment of timingto these events. Random rate changes as seen withatrial fibrillation are problematic as timing cannotbe easily defined by the microprocessor. As a result,software has been developed that allows timing tobe changed from predictive to R-wave triggereddeflation. The trade off is less accurate balloon defla-tion timing in favor of preventing balloon inflationin systole.At very high heart rates (>130–140 b/min), the
IABP may be incapable of inflation and deflationrapid enough to provide proper timing. In this set-ting, using the balloon pump at a 1:2 ratio usuallyis necessary. At slow heart rates, premature balloondeflationwill occur in pumps that have a preset limiton the duration of inflation.
AnticoagulationAnticoagulation is necessary both to prevent throm-bus formation on the balloon or catheter and inthe cannulated peripheral vessel. An unfraction-ated heparin (UFH) infusion is used to maintainan activated clotting time (ACT) between 150 and200 seconds or a partial thromboplastin time (PTT)between 60 and 80 seconds (1.5–2.0 times con-trol). In the postoperative setting, initiation of hep-arin infusion may be delayed for 12–24hours oruntil chest tube drainage is minimal. Alternativeapproaches include aspirin or low-molecularweightdextran in place of or in addition to UFH.
CardioWest TAHThe CardioWest TAH is the direct descendent of theSymbion (Jarvik) J7-70 TAH. Because implantationof the TAH requires excision of the native ventri-cles, this device is used only as a bridge to cardiac

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 386 — #12
386 Chapter 11
Premature deflation of the IAB
during the diastolic phase
Waveform characteristics:
• Deflation of IAB is seen as a sharp drop following diastolic augmentation • Suboptimal diastolic augmentation • Assisted aortic end diastolic pressure may be equal to or less than the unassisted aortic end diastolic pressure • Assisted systolic pressure may rise
Physiologic effects: • Sub-optimal coronary perfusion • Potential for retrograde coronary and cartoid blood flow • Angina may occur as a result of retrograde coronary blood flow • Sub-optimal afterload reduction • Increased MVO2 demand
Waveform characteristics: • Assisted aortic end-diastolic pressure may be equal to the unassisted aortic end diastolic pressure • Rate of rise of assisted systole is prolonged • Diastolic augmentation may appear widened
Physiologic effects: • Afterload reduction is essentially absent • Increased MVO2 consumption due to the left ventricle ejecting against a greater resistance and a prolonged isovolumetric contraction phase • IAB may impede left ventricular ejection and increase the afterload
Unassistedaortic
end-diastolicpressure
Diastolicaugmentation
Assistedsystole
Assisted aorticend-diastolic
pressure
Diastolicaugmentation
Prolonged rateof rise of
assisted systole
Unassistedsystole
Widenedappearance
Assisted aorticend-diastolic
pressure
(a) Early deflation
(b) Late deflation
Fig. 11.7 Arterial waveforms resulting from (a) early balloon deflation and (b) from late balloon deflation. Thephysiologic consequences of these timing errors are summarized. IAB, intra-aortic balloon.
transplantation. Patientswho are not suitable candi-dates for cardiac transplantation are not candidatesfor the TAH.The CardioWest has a 70-mL stroke volume and
can deliver cardiac outputs of 9.5 L/min. It is apneumatically driven device and each ventricle hasa pneumatic driveline. The drivelines are attached toa drive console on wheels. The drive console is largebecause it contains four air compressors, a primaryand a backup for each ventricle (Fig. 11.13).The prosthetic ventricles are rigid polyurethane,
Dacron mesh shells divided into a blood and
a pneumatic chamber by a four-layer polyurethanediaphragm. The diaphragm is flexible but non-compliant and each layer is separated by a smallamount of graphite for lubrication. UnidirectionalMedtronic-Hall tilting disc valves are located in theblood chamber. The ventricles are identical, exceptthat the spacing between the inflow and outflowvalves in the right ventricle is larger to allow foraortic outflow when the ventricles are attachedtogether with a Velcro patch (Fig. 11.14).The pneumatic chamber communicates with
the pneumatic drive system via the pneumatic

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 387 — #13
Mechanical Circulatory Support 387
Fig. 11.8 Use of the “verify” feature highlights theperiod of balloon inflation in real time on the arterialwaveform. A balloon pressure waveform is displayed onthe third channel.
driveline. As pressurized air is introduced into thepneumatic chamber, the diaphragm moves suchthat the blood chamber becomes pressurized aswell.When the pressure in the blood chamber exceedsthe device filling pressure, the inflow valve willclose. When pressure in the blood chamber exceedsaortic or pulmonary artery pressure, the outflowvalve opens and ejection commences. These pro-cesses constitute the isovolumic and ejection phasesof systole in the prosthetic ventricle (Fig. 11.15a,b).At the end of systole, air is vented passively from
the pneumatic chamber to the atmosphere and thepressure in the blood chamber falls. This constitutesisovolumic relaxation. When the pressure in theright atrium and left atrium exceeds the pressure inthe blood chamber of the corresponding prostheticventricle, the inflow valve opens. The diaphragmis free to move in such a manner that virtually
Fig. 11.9 Intra-aortic balloon pump (IABP) control console showing the inflation and deflation “Earlier” and “Later”buttons to fine balloon timing. Earlier models had actual slides. IAB, intra-aortic balloon.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 388 — #14
388 Chapter 11
Peak inflation(positive overshoot)
Plateau (full inflation of IAB)
IABdeflation
IABinflation
Return to zero baseline
Peak deflation(negative
overshoot)
Zero baseline
Fig. 11.10 A normal balloon pressure waveform. IAB,intra-aortic balloon.
Catheter kink
Rounded balloonpressure waveform.Loss of plateau resultingfrom kink or obstructionOf shuttle gas. This maybe caused by a kink in cathetertubing, improper IAB catheterposition, the sheath not pulledback to allow inflation of IAB,IAB too large for aorta, IAB isnot fully unwrapped, or H2O condensation in external tubing.
Fig. 11.11 A balloon pressure waveform from a kinkedballoon catheter. IAB, IAB, intra-aortic balloon.
Gas loss
Leak in the closedsystem causing theballoon pressurewaveform to fall belowzero baseline.This may be due to aloose connection, leak in IABcatheter, H2O condensation in externaltubing, or a patient who is tachycardic and febrile which causes increasegas diffusion through the IAB membrane.
Fig. 11.12 A balloon pressure waveform from a balloonwith a gas leak. IAB, intra-aortic balloon.
the entire volume of the prosthetic ventricle canfill with blood as all the air leaves the pneumaticchamber. This constitutes diastole in the prostheticventricle (see Fig. 11.15).
InsertionPlacement of the TAH requires CPB with aorticcross-clamping and bicaval cannulation. The device
Fig. 11.13 Schematic of the CardioWest total artificialheart (TAH) showing the pneumatic drivelines, driveconsole, and cardiac output monitor and device unit(COMDU).
34976
RIGHT
3493
8
LEFT
Fig. 11.14 Close-up of the CardioWest total artificialheart (TAH) prosthetic ventricles joined by a Velcropatch. The atrial inflow cuffs are shown in thebackground. The Dacron outflow grafts are shown in theforeground. The pneumatic drivelines are at the bottomof the picture.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 389 — #15
Mechanical Circulatory Support 389
Fig. 11.15 Schematic of theCardioWest total artificial heart (TAH)in (a) end-diastole and (b) end-systole.
Blood flow
(a) (b)
Blood
Air Air
AirAir exhausted
Arterial graft
Housing
Diaphragm
Base
Blood flow
Atrial cuff
Strokevolume
is placed in the patient’s pericardial cavity with theRV and LV pneumatic drivelines exiting throughthe skin. The patient’s native ventricles are excised,leaving a large cuff of right and left atrium. Theinflow cuff of each ventricle is anastomosed tothe appropriate atrium. End-to-end anastomosesare created between the outflow graft of the pros-thetic ventricle and the appropriate great vessel.The TAH has been placed in patients weighing aslittle as 50 kg, but the best fit is in patients withweights in the 80-kg range (BSA>1.7m2)with largehearts. Closure of the chest after device implan-tation in patients who are too small can producepulmonary and systemic venous obstruction. Theinferior vena cava (IVC) and the left upper andleft lower pulmonary veins are at particular riskof obstruction. Venous obstruction limits deviceoutput and is ultimately fatal.
Management of the TAHThe TAH is monitored with the cardiac output mon-itor and diagnostic unit (COMDU). COMDU allowsanalysis of air exhaust flow during diastole throughtransduction of a pneumotach. The flow is displayedas a curve with respect to time (Figs 11.16 & 11.17).Integration of this curve yields the volume of airdisplaced from the pneumatic chamber during dias-tole. When averaged over several beats, this is equalto cardiac output. The system allows computationof cardiac output for each ventricle. In addition,transduction of the driveline pressure allows devicefilling and emptying to be monitored over time, asillustrated in Figs 11.18 and 11.19.The heart rate and percentage of systole are set
by the operator and complete ejection is sought on
1 2
Air
Driver
3-wayvalve
Start ofintegration
Fill volume
1 2
Diastole
Inflow valveopens
SystoleF
low
(L
/min
)
Flowtransducer
Air
3-way valve openedto vacuum or
room air
Fig. 11.16 Schematic of the CardioWest total artificialheart (TAH) pneumotach and the resulting fill-rate curvederived from air flow out of the device in diastole.
each cycle. The drive pressures are set just highenough to completely empty the ventricle. Theoccurrence of a full eject pattern is then seen on theair-pressure waveform. The device is not allowed tofill completely on each beat. This allows automaticadjustment for the difference in volumes pumpedby the two ventricles; the LV pumps more than theRV because of the existence of bronchial flow. Italso provides for preload reserve. As venous returnincreases (such as with patient position changes orexercise), stroke volume can increase up to the limitof the 70mL.The maximum end-diastolic volume of the pros-
thetic ventricle may be difficult to achieve whendiastole is short (slow ejection rate, high percentageof systole) and filling pressure is low. The pneu-matic drive system of the CardioWest TAH allowsvacuum to be applied to the pneumatic chamber

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 390 — #16
390 Chapter 11
50
40
30
20
Fill
ing
rate
(L
/min
)
10
0.1 0.2Seconds
80 b/min
0.3
Completefilling
of rightventricle
LFV= 77RFV=75
LCO=6.2RCO=6.0
Fig. 11.17 Actual fill rate curve from a CardioWest totalartificial heart (TAH) patient. There is complete filling ofthe right ventricle. Left fill volume (LFV) and right fillvolume (RFV) are obtained by integrating the area underthe left and right fill rate curves. The product of LFV anddevice rate (80 b/min) yields the left cardiac output(LCO). The product of RFV and device rate (80 b/min)yields the right cardiac output (RCO).
1
Air
AirAirAir
2
21 3
DiastoleSystole
Outflowvalveopens
3-way valveopened toair supply
Fullejection
3
Pressuretransducer
Driver
3-wayvalve
Pre
ssur
e (m
mH
g)
Air
Fig. 11.18 Schematic of the CardioWest total artificialheart (TAH) pressure transducer and the resultingpressure waveform in systole and diastole.
during isovolumic relaxation and diastole to has-ten the fall in blood chamber pressure and enhancediastolic filling. To reduce the likelihood of entrain-ing air around anastomotic sites and introducing therisk of air embolism, vacuumgenerally is not applieduntil the patient’s chest is closed. Normally, −25 to−50mmHg of vacuum is applied.
AnticoagulationAnticoagulation generally is started after pro-tamine reversal of intraoperative UFH and chest
Ejectionphase
Incompleteejection
Completeejection
point
Completeejectionplateau
Dia
stol
e
Sys
tole Complete
fillingdeflection
Fig. 11.19 Actual pressure waveform from a CardioWesttotal artificial heart (TAH) patient. The second waveformfrom the left indicates incomplete emptying of theprosthetic ventricle. This can be rectified either byafterload reduction or by increasing driveline pressure.The third waveform from the left indicates drivelinepressure just high enough to ensure complete emptyingof the prosthetic ventricle. The fourth waveform from theleft also indicates complete emptying of the prostheticventricle. An excessive plateau is indicative of a drivelinepressure that is higher than necessary. Complete filling ofthe prosthetic ventricle is indicated by the negativedeflection in the pressure waveform during diastole. Thisis produced by the compliant diaphragm reboundingover the air exhaust port in the base of the prostheticventricle. In the instance illustrated here, complete fillingof the prosthetic ventricle occurs at end-diastolefollowing the second waveform.
tube drainage less than 100mL/h for 3 con-secutive hours. Low-molecular-weight dextran(dextran 40) infused at 25mL/h and oral or naso-gastric dipyridamole (75–100mg 3–4 times/day) arestarted. When chest tube drainage is minimal andserous, the dextran is stopped and a continu-ous UFH infusion is initiated; the goal is to keepthe PTT 1.5–2.0 times control. At 1–2weeks post-operatively, the UFH is discontinued and coumadinis started; the goal is an international normalizedratio (INR) of 1.5–2.0. Some centers add aspirin(325–975mg/day) as well.
Thoratec VAD systemThe Thoratec VAD or Pierce–Donachy VAD(Figs 11.19 & 11.20) is an extracorporeal, pulsatileVAD that can be used in parallel with the RV andin parallel or in series with the LV. The device has

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 391 — #17
Mechanical Circulatory Support 391
Fig. 11.20 Thoratec ventricular assist device (VAD). Theinflow to the device is on the right and the outflow is onthe left. The pneumatic drive and incorporated electriccable are at the bottom of the device.
an effective stroke volume of 65mL and can delivera cardiac output of 6.5 L/min. It is a pneumaticallydriven device and has a pneumatic driveline. Thedriveline is attached to a drive console on wheels.The drive console is large because it contains four aircompressors, two for each driver, a primary and abackup. A Hall sensor built into the rigid case mon-itors movement of the pump diaphragm. A smallmagnet mounted on the diaphragm triggers the Hallsensor when the two come in contact. This informa-tion is transmitted to the console via an electricalcable and allows the control console to know whenthe blood chamber is full. In addition, transductionof the driveline pressure allows device filling andemptying to be monitored over time as describedfor the CardioWest TAH.The prosthetic ventricle is a rigid polysulfone
case divided into a blood and a pneumatic cham-ber by a flexible, noncompliant polyurethanediaphragm. Unidirectional Bjork–Shiley monostrutDerlin inflow and outflow valves are located in the
blood chamber. The pneumatic chamber commu-nicates with the pneumatic drive system via thepneumatic driveline. The same principles for sys-tole and diastole as described for the CardioWestTAH apply.
InsertionThe device rests on the anterior abdominal wall.The device is extracorporeal thereby limiting patientmobility. The inflow and outflow conduits are tun-neled into the thoracic cavity. For use as an RVAD,the inflow cannula is inserted in the right atriumand the Dacron outflow conduit is anastomosedend-to-side to the pulmonary artery. For use as aparallel LVAD, the inflow cannula is inserted in theleft atrium and the Dacron outflow conduit is anas-tomosed end-to-side to the aorta. For use as a seriesLVAD, the inflow conduit is inserted in the LV apexand the Dacron outflow conduit is anastomosedend-to-side to the aorta.Insertion requires a median sternotomy. In the
postcardiotomy setting, CPB already is in usebecause failure to wean from CPB is the indicationfor placement of the device. Postcardiotomy supportis generally accomplished with atrial cannulationrather than cannulation of the LV apex. This facili-tates subsequent weaning of the device. For patientswith a bridge to transplantation, CPB is necessaryfor LV apical cannulation.
Management of the Thoratec VADFour triggering modes are available: manual, asyn-chronous, fill-to-empty, and synchronous. In theasynchronous mode, the operator chooses thepumping rate and percentage of systole. In the fill-to-empty mode, the Hall sensor detects a full bloodchamber and triggers ejection. The device typically isused in the fill-to-empty mode. In this mode, deviceoutput is calculated by the console as the productof stroke volume (65mL) and device rate. Deviceoutput, as determined by the console, is accurateonly when complete filling occurs.The drive pressures are set approximately
100mmHg higher than systolic pressure (230–250mmHg for the LVAD and 140–160mmHg forthe RVAD). The percentage of systole is set to

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 392 — #18
392 Chapter 11
equal one-half the device rate (percentage of sys-tole at 60 b/min = 30%; percentage of systole at80 b/min = 40%). These measures produce com-plete emptying with an ejection time of 300ms. Theoccurrence of a full eject pattern is then seen onthe air pressure waveform (see Fig. 11.19). Com-plete device filling also can be seen on the pressurewaveform (see Fig. 11.19).The maximum end-diastolic volume of the pros-
thetic ventricle may be difficult to achieve whendiastole is short (slow ejection rate, high percent-age of systole) and filling pressure is low. Vacuumcan be applied to the pneumatic chamber duringdiastole as described for the CardioWest TAH.
AnticoagulationAnticoagulation is as described for theCardioWest TAH.
Abiomed AB5000, Medos VAD, andBerlin HeartThese devices are very similar to the Thoratec VAD.They are extracorporeal, pulsatile VAD that can beused in parallel with the RV and in parallel or inseries with the LV. The prosthetic ventricle is a rigidcase divided into a blood and a pneumatic chamberby a flexible, noncompliant diaphragm. Unidirec-tional inflow and outflow valves are located in theblood chamber. The pneumatic chamber commu-nicates with the pneumatic drive system via thepneumatic driveline. Vacuum can be applied to thepneumatic chamber during diastole. The indicationsfor use and anticoagulation management of thesedevices are the same as the Thoratec VAD. The fol-lowing important differences exist between thesedevices and the Thoratec VAD:• Neither the Medos VAD nor Berlin Hearthas a Hall sensor and therefore cannot oper-ate autonomously in a fill-to-empty mode (fixedstroke volume, variable rate). They operate asyn-chronously in a fixed rate (set by the operator)variable stroke volume mode. They all allow con-trol of percent systole, device rate, and right and leftdrive pressures. The Medos VAD and Berlin Heartare applicable to the pediatric population as theyhave pumps of variable blood chamber volume.
The Medos system has four sizes:a Infant. RVAD 9mL, LVAD 10mL;b Pediatric. RVAD 22.5mL, LVAD 25mL;c Adult. RVAD 54mL, LVAD 60mL;d Adult. RVAD 72mL, LVAD 80mL.The Berlin Heart has six sizes; 10, 25, 30, 50, 60,and 80 mL for either RVAD or LVAD use.• The Abiomed AB5000 has a 120mL blood cham-ber with a 95mL stroke volume and a 25mL resid-ual end-systolic volume. This device has a sensorthat triggers ejection when full filling (cessation ofdiastolic gas flow) is detected. Because ejection pres-sure is fixed (420mmHg for LVAD, 300mmHg forRVAD) the ejection time for complete emptyingincreases as afterload increases. The device operatesautonomously in a fill-to-empty mode (fixed strokevolume, variable rate). Increases in afterload anddecreases in preload will decrease pump output asa result of decreased pump rate with a fixed strokevolume.
HeartMate IP and XVE left ventricularassist systemThe HeartMate VAD (Figs 11.21–11.23a,b) is animplantable, pulsatile LVAD used in series withthe native heart. The device has a stroke volumeof 83mL and is capable of providing 11 L/min ofcardiac output. It is available in pneumatically (IP)and electromechanically (XVE) driven versions. Thepneumatic version has an external driveline. Thedriveline is connected to the pneumatic drive sys-tem and system controller, which are on wheels.The pneumatic drive system and system controllerare small because there are no air compressors.An electric motor is used to drive a diaphragm airpump. The electromechanically driven, vented elec-tric version has a percutaneous electric and air ventline that attaches to a portable system controllerand battery pack that can be worn by the patient.The sealed electric (SE) version under developmentis totally implantable and has power transductionoccurring through transcutaneous induction coilswith no percutaneous lines.The outer shell of the device is titanium; the inner
blood-contacting surface of the shell is lined withsintered titaniummicrospheres. A rigid pusher platecovered by a flexible, biocompatible, polyurethane

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 393 — #19
Mechanical Circulatory Support 393
Aorta
HeartDiaphragm
Heartmateblood pump Connection to
external airpower supply
Fig. 11.21 Schematic of an implanted pneumaticHeartMate IP left ventricular assist system (LVAS).Cannulation of the left ventricle (LV) apex and theend-to-side anastomosis to the aorta are depicted.The percutaneous driveline is depicted exiting theabdominal wall.
Fig. 11.22 Photograph of the HeartMate IP leftventricular assist system (LVAS). Device inflow is onthe left and outflow to the Dacron graft is on the left.The pneumatic driveline is being held.
diaphragm divides the prosthetic ventricle in two.On one side of the pusher plate is the blood cham-ber; on the other side is the pneumatic or electro-mechanical pumping mechanism. 25mm porcineunidirectional inflow and outflow valves are placed
Outlet Full pump
Empty pump
Air
Inlet
Flexible diaphragmRigid pusher-plate
Stroke limiter
Stroke sensorStroke magnet
(a)
(b)
Fig. 11.23 Schematic cross-section of the pneumaticHeartMate IP LVAS. Both diastole (a) and systole (b) aredepicted.
in the blood chamber. The textured surfaces areintended to promote formation of a pseudointimallining after contact with blood.In the pneumatic version, a preset volume of air
is delivered to the blood pump during each beat.Each stroke of the console air pump corresponds toone beat of the blood pump delivered via a pistonthat drives the pusher plate into the blood chamber.In the electromechanical version, the rotary motionof a low-speed torque motor is converted to thelinear action of the pusher plate via helical cams.Energy is transferred to a copper coil, creating anintra-LVAD electromagnetic field to actuate rotorassembly rotation. One revolution of the motor isrequired for complete excursion of the pusher plate.In both instances, the excursion of the pusher platereduces the volume of and pressurizes the bloodchamber.When the pressure in the blood chamber exceeds
native LV pressure, the inflow valve closes. Whenthe pressure in the blood chamber exceeds aor-tic pressure, the outflow valve opens and pumpingcommences. This represents the isovolumic andejection phases of device systole.When the pneumatic piston or the motor is
switched off, air is vented to the atmosphere from

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 394 — #20
394 Chapter 11
the pumping chamber and the pusher plate is freeto move. When the pressure in the native left ven-tricle (the chamber filling the prosthetic ventricle)exceeds the pressure in the blood chamber, theinflow valve opens and diastolic filling commences.A Hall sensor in the pneumatic pump detects a fullblood chamber and triggers ejection. This allowsbeat-to-beat stroke volume and device output datato be derived and displayed. In addition, a six-beatmoving average of LVAD output also is displayed.
InsertionThe device can be implanted intraperitoneally or ina preperitoneal pocket in the left upper quandrant.The inflow and outflow conduits are tunneled intothe thoracic cavity. The inflow conduit is insertedinto the LV cavity via the LV apex and the Dacronoutflow conduit is anastomosed end-to-side to theascending aorta. Insertion requires a median ster-notomy and use of CPB. A single cable containingthe necessary electrical and pneumatic conduits topower, control and vent air from the device istunneled through the abdominal wall.
Management of the HeartMate devicesThe pneumatic device can function in the asyn-chronous, fill-to-empty, or synchronous modes.The device usually is operated in the fill-to-emptymode with pump ejection triggered by the trans-ducer when the pump is full. LVAD ejection dura-tion can be set by the operator from 200 to 450msto achieve complete emptying of the device with-out compromising device filling. Because minimalLVAD filling time is 50% of the selected LVAD ejec-tion duration LVAD rate varies inversely with ejec-tion duration. The LVAD rate varies from 89b/minat an ejection duration of 450ms to 140 b/min atan ejection duration of 200ms. The control con-sole monitors device output as the product of devicestroke volume and rate on a beat-to-beat basis.The vented electric version does not use a
Hall sensor to measure diaphragm displacement.Ejection duration is constant and LVAD ratevaries by automatic changes in LVAD fillingtime as determined by the pump controller.This is feasible because the device is rela-tively afterload-insensitive. As preload increases,
the pump controller detects a shorter intervalbetween diaphragm and rotor interaction andsubsequently shortens LVAD filling time.
AnticoagulationFormation of the pseudointimalmembrane obviatesthe need for full anticoagulation with heparin orcoumadin. Aspirin (81mg/day) and dipyridamole(75mg three times/day) have been used as the solelong-term anticoagulants. Coumadin may be addedfor patientswith pre-existing thrombus in the nativeheart.
Novacor LVADThe Novacor LVAD (Figs 11.24–11.26a–c) is animplantable pulsatile LVAD used in series with thenative heart. The device has a stroke volume of70mL and is capable of providing 10 L/min of car-diac output. It is the prototypical pulsatile electro-mechanical pump, configured to convert electricalenergy to the mechanical energy necessary to ejectblood from the prosthetic ventricular chamber. Thenewest version of the Novacor has a percutaneouselectric conduit and air vent line, which attaches
Fig. 11.24 Schematic of an implantedelectromechanically driven Novacor left ventricular assistsystem (LVAS) device. Cannulation of the left ventricle(LV) apex and the end-to-side anastomosis to the aortaare depicted. The percutaneous driveline is depictedexiting the abdominal wall.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 395 — #21
Mechanical Circulatory Support 395
Fig. 11.25 Photograph of the Novacor left ventricularassist system (LVAS) device. Device inflow with the leftventricle (LV) apex cannula in place is on the right anddevice outflow to the Dacron graft is on the left. Thedriveline with enclosed electrical cables is seen loopedunder the pump.
to a portable microprocessor/system controller andbattery pack that can be worn by the patient.This prosthetic ventricle consists of a bio-
compatible sac bonded to symmetrically opposedpusher plates housed in a lightweight shell. 21mmCarpentier–Edwards porcine unidirectional inflowand outflow valves are placed in the blood chamber.A solenoid energy converter is used to transfer elec-trical energy to mechanical energy via preloadedbeam springs, which then drive the pusher plates.When the solenoid is open, energy is stored in thebeam springs, the pusher plates and blood sac arefree to expand, and diastolic filling of the pros-thetic ventricle via the left ventricle takes place.When the solenoid is closed, the energy stored in thebeam springs is released. The resulting compressionof the blood sac between the pusher plates cre-ates the pressure necessary for the isovolumic andejection phases of systole. Displacement transduc-ers within the solenoid energy converter monitorpusher-plate position. This allows beat-to-beat fillvolume, residual volume, and stroke volume to bedetermined. This information, in combination withdevice rate, allows device output data to be derivedand displayed.
InsertionDevice insertion is as described for the HeartMate IPand XVE left ventricular assist system (LVAS).
Management of the NovacorThe systemwas originally designed to operate in thefill rate trigger mode. In the fill rate trigger mode,the rate at which the pump fills is used to triggerejection. At the start of device filling, the pump fillrate is high. Toward the end of device filling, thepump fill rate falls. By adjusting the end of fill thresh-old setting, the percentage bywhich the fill ratemustfall to trigger device ejection can be set. In actualclinical practice, filling of the Novacor occurs duringLV diastole in some beats and during LV systole inother beats while in the fill rate trigger mode. Thisoccurs as the result of changes in preload and heartrate with changes in patient activity level. Despitethis, the aortic valve rarely opens. Patientswhohavebeen discharged from the hospital with the Novacordevice have the end of fill threshold set to 100%. Thisallows the device to function as if in a fill-to-emptymode. This allows reliable pump function with nooperator intervention. The control console displaysbeat-to-beat LVAD output as the product of LVADstroke volume and rate. Beat-to-beat visualizationof the fill-rate curve also is available.
AnticoagulationAnticoagulation is as described for the TAH.
Abiomed BVS 5000The Abiomed BVS 5000 (Fig. 11.27) is an extracor-poreal pulsatile VAD used in parallel with the nativeventricles. The device has an effective stroke vol-ume of 80mL and a cardiac output of 5 L/min. Itis a pneumatically driven system and has a pneu-matic driveline attached to a computerized controlconsole on wheels.The device consists of atrial and ventricular cham-
bers arranged vertically in a rigid polycarbonatehousing (Fig. 11.28). The atrial and ventricularchambers are polyurethane bladders. The ventric-ular chamber contains polyurethane unidirectionaltri-leaflet inflow and outflow valves.The atrial bladder fills continuously by gravity
from the patient’s native atrium. The ventricular

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 396 — #22
396 Chapter 11
Solenoid core Main springPreload spring
Pusher plate
Frame
Pump sac
Pump housing ring
(a)
(b)
(c)
Fig. 11.26 Schematic cross-section of the Novacor left ventricular assist system (LVAS). (a) The pump is filled, thesolenoid is opened. The preload spring limits expansion of the pump sac to 70mL. (b) The solenoid is closed andmagnetically latched. This constitutes isovolumic contraction. (c) End of ejection with complete pump emptying.
bladder is pressurized by introduction of pressur-ized air into rigid air chamber around the bladder.When the pressure in the air chamber is atmo-spheric, atrial bladder pressure exceeds ventricularbladder pressure, the inflow valve opens, and theventricular bladder fills with blood. This constitutes
diastole in the device. When the ventricular blad-der is full, the air chamber is pressurized. Whenventricular bladder pressure exceeds atrial bladderpressure, the inflow valve closes. When pressurein the ventricular bladder exceeds aortic or pul-monary artery pressure, the outflow valve opens

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 397 — #23
Mechanical Circulatory Support 397
Heart
Left heartBVS pump
Right heartBVS pump
BVS drive console
BVScannulae
Fig. 11.27 Schematic of an implanted pneumatically driven Abiomed BVS5000 used as a biventricular assist device(BiVAD). Cannulation of the left atrium (LA) and the end-to-side anastomosis to the aorta are depicted, as arecannulation of the right atrium (RA) and the end-to-side anastomosis to the main pulmonary artery. The percutaneousdrivelines are depicted exiting the abdominal wall. The device is seen to be located below the level of the patient’s heart.
and ejection commences. These processes constitutethe isovolumic and ejection phases of systole in theprosthetic ventricle (Fig. 11.29a,b).
InsertionThe device is mounted on IV poles below the level ofthe patient’s heart. Polyvinyl chloride (PVC) tubingbrought through the chest wall connects the inflowand outflow cannulas to the device. For use as anRVAD, the inflow cannula is inserted in the rightatrium and the Dacron outflow conduit is anas-tomosed end-to-side to the pulmonary artery. Foruse as an LVAD, the inflow cannula is inserted inthe left atrium and the Dacron outflow conduitis anastomosed end-to-side to the aorta. Insertionrequires a median sternotomy. Although CPB is
not absolutely necessary for insertion of the device,it is commonly used. In the postcardiotomy set-ting, CPB already is in use because failure to weanfrom CPB is the indication for placement of thedevice. When intermediate- to long-term supportis needed the inflow and outflow cannula of theBVS5000 can be used with the Abiomed AB5000system so that a device “device swap” can takeplace.
Management of the Abiomed BVS 5000The pneumatic control console monitors pumpfunction by analysis of air return from the pneu-matic driveline. Pump rate and diastolic/systolicintervals are determined automatically and thepump functions in the fill-to-empty mode. Device

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 398 — #24
398 Chapter 11
Fig. 11.28 Photograph of the AbiomedBVS5000 device. Device inflow is at the top, outflow is atthe bottom. The pneumatic driveline is seen entering thebottom third of the device on the left.
output is monitored and displaced by the controlconsole. A unique feature of this device is that thesystem is operator-independent. Therefore, engi-neering and perfusion staff is not necessary duringoperation of the device.When the device is used as a BiVAD, differential
recovery of the RV and LV function requires care-ful management due to the limitation of 5 L/min ondevice output. As RV function recovers, total pul-monary output will be a combination of RVAD out-put and native RVoutput. If at the same time there isno LV recovery, systemic output will be determinedby LVADoutput. If the combined pulmonary outputexceeds themaximal output of the LVAD (5 L/min),then LV, LA, and pulmonary venous congestionwilloccur. The solution is to reduce RVAD output sothat pulmonary and systemic outputs are matched.A similar scenario can be described for LV recoveryin the absence of RV recovery.
AnticoagulationAnticoagulation ismaintainedwith anUFH infusionto keep the ACT at 150–200 seconds.
Blood inflowfrom patient
Blood inflowfrom patient
Inflowbladder
fills
Inflowvalvecloses
Outflowbladderejects
Outflowvalveopens
Airpressureapplied
Airexhaust
Vent
Inflowbladderempties
Inflowvalveopens
Outflowbladder
fills
Outflowvalvecloses
Vent
Blood outflowto patient
Arterialpressure
(a) (b)
⇐ ⇐
⇐⇐
⇐
⇐
⇐
⇐
Fig. 11.29 Schematic cross-section of the AbiomedBVS5000 device. (a) End-systole and (b) end-diastole aredepicted.
Centrifugal pumpsCentrifugal pumps are extracorporeal, nonpulsatilepumps used in parallel with the native ventricles(Fig. 11.30). The BioMedicus pump can be used asboth a RVAD and LVAD. This device is capable ofproviding outputs of 2.0–6.0 L/min. The Tandem-Heart is intended for LVAD use. It is small witha 7mL prime volume and can provide flows of3.5–4.0 L/min.Centrifugal pumps use a constrained vortex to
impart kinetic energy to fluid in a rotating head. Therotating head consists of a series of concentricallyarranged cones or fins contained within a rigid plas-tic shell (see Fig. 10.3). Rotary motion is impartedto the cones or fins by a drive console. Couplingof the drive console to the pump head is accom-plished with magnets in the base of the pump head.Rotation of the cones or fins creates a vortex that isconstrained by the rigid plastic housing. This createslower pressure at the center of the pump than at theperiphery. The pressure gradient draws blood into

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 399 — #25
Mechanical Circulatory Support 399
Fig. 11.30 Schematic of a centrifugal pump used for leftventricular support. Cannulation of the left atrium andthe aorta are depicted. The centrifugal pump driveconsole is not shown.
the center of the pump and imparts pressure to theblood as it leaves the pump at the periphery.This arrangement produces a pump that is very
afterload and preload dependent. As a result, pumpoutput at a given revolutions/min can vary greatly.At a given revolutions/min increasing outlet pres-sure or decreasing preloadwill reduce pump output.Outlet pressure is a combination of the pressuredrop across the outlet cannula and the resistance ofthe recipient vascular bed. For example, at an out-let pressure of 200mmHg, a Bio-Medicus pump cangenerate 4 L/min of flow at 200 revolutions/min.Increasing outlet pressure to 400mmHg requires3000 revolutions/min to maintain 4 L/min of flow.At the extremes, clamping the inflow or outflow
line will result in no pump output despite the factthat the pump head continues to rotate. Becausepump output decreases as afterload increases, linepressure in a centrifugal pump can never reachthe point at which connections will come apart orthe pumping mechanism will fail. This is a majoradvantage of centrifugal pumps over occlusive rollerpumps. Because pump output does not vary directlywith revolutions/min,monitoring centrifugal pumpoutput requires use of a Doppler or electromagneticflow probe on the outflow line.Another advantage of centrifugal pumps over
occlusive roller pumps is the reduced potential to
pump air into the circulation. Inadvertently intro-duced air tends to remain in the low-pressure cen-ter of the pump and is not introduced into thecirculation.
InsertionThe BioMedicus device is mounted on the driveconsole. Polyvinyl chloride (PVC) tubing broughtthrough the chest wall or sternotomy connects theinflow and outflow cannulas to the device. StandardCPB arterial and venous cannulas are used. For useas an RVAD, the inflow cannula is inserted in theright atriumand the outflow cannula is inserted intothemain pulmonary artery. For use as an LVAD, theinflow cannula is inserted in the left atrium and theoutflow cannula is inserted into the ascending aorta.Insertion is accomplished via a median sternotomy.Due to the high incidence of postoperative bleeding,impairment of venous drainage into the device andpulmonary dysfunction in the postcardiotomy set-ting the sternal edges often are left unopposed andan occlusive dressing is placed over the sternotomy.The chest is then closed after the device has beenremoved in the operating room.Although CPB is not absolutely necessary for
insertion of the device, it is commonly used. Inthe postcardiotomy setting, CPB is already in useas failure to wean from CPB is the indication forplacement of the device.The TandemHeart device and the small drive con-
sole can lie on the patient’s leg. The inflow andoutflow to the device are placed percutaneously.The femoral vein is cannulated and the inflow can-nula is directed across the atrial septum into theLA under direct vision in the operating room (OR)or with use of fluoroscopy or TEE in the catheter-ization laboratory. The femoral artery is used fordevice outflow. The device provides parallel LVADsupport.
Management of the centrifugal pumpThe centrifugal pump requires the presence ofa trained individual. Flow is adjusted to meetmetabolic demands. If flow does not increasewith increases in pump revolutions/min, reducedpreload or elevated afterload should be treated. Ele-vated MAP should be treated by reducing systemic

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 400 — #26
400 Chapter 11
vascular resistance (SVR) with a vasodilator. Ele-vated pulmonary artery pressure (PAP)may requiretreatment with a pulmonary vasodilator. A pul-monary artery catheter will allow low assessment ofboth RVADpreload (central venous pressure (CVP))and LVAD preload (pulmonary artery occlusionpressure (PAOP)).Centrifugal pumps are prone to thrombus forma-
tion in the pump head due to heat produced in thebearing housing during rotation. As a result, somemanufacturers recommend changing the pumphead every 24–48hours. In addition, pump flowslower than 2 L/min are associated with pump headand cannula thrombus formation.
AnticoagulationAUFH infusion is used tomaintain an ACT between100 and 200 seconds or a PTT between 60 and80 seconds (1.5–2.0 times control). The pump headmust be monitored for thrombus formation andmust be changed if there is evidence of thrombus.
Axial pumpsAxial pumps are intracorporeal pumps used inseries with the left ventricle. These compact pumpsemploy an impeller mechanism that is the onlymoving part. At the proximal end of the pumpstationary airfoil-shaped vanes may be used tostraighten blood flow prior to entry into an impeller.The impeller then imparts radial velocity (kineticenergy) to the blood as it draws blood into the pump.At the distal end of the pump there is a set of station-ary diffuser (stator) vanes serving to impart axialvelocity by straightening flow. This converts kineticenergy to static pressure (potential energy) as bloodleaves the pump.These pumps are small; about the size of a C
or D cell battery. They have small priming vol-umes but operate at very high rotational speeds(8000–10 000 revolutions/min) allowing them togenerate 6–8 L/min of nonpulsatile flow(Figs 11.31 & 11.32). There are three axial pumpsavailable for clinical use:
Jarvik 2000The two-blade impeller is a neodymium-iron-boronmagnet mounted on two ceramic bearings mounted
Fig. 11.31 Schematic of an implantedelectromechanically driven HeartMate II axial flow leftventricular assist system (LVAS). Cannulation of the leftventricle (LV) apex and the end-to-side anastomosis tothe aorta are depicted. The percutaneous driveline isdepicted exiting the abdominal wall.
Flow straightenerMotor stator
Stator housing
Diffuser
Inducer/impeller
Flow tube
Blood flow
Fig. 11.32 Schematic cross-section of the MicroMedDeBakey ventricular assist device (VAD) axial pump.Blood enters through the flow straightener drawn in bythe combination inducer (helical blades) and impeller.Radial flow is converted to axial flow by the stationaryblades of the diffuser prior to blood exiting the pump.The electric motor is depicted as well. The percutaneousdriveline is depicted at bottom left.
in a titanium housing. Outflow stator blades directflow into a 16mm outflow graft. A brushless DCcurrent motor within the titanium housing createsthe electromagnetic force to rotate the impeller. Themotor is driven via a percutaneous power cable con-nected to a system controller and 12-volt battery

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 401 — #27
Mechanical Circulatory Support 401
pack system that can be worn by the patient ona belt. The controller allows manual adjustmentof the impeller revolutions/min. Infant and childversions of the Jarvik 2000 are currently underdevelopment.
MicroMed (DeBakey) VADThis pump has a 25mL prime volume includingthe titanium inflow cannula. Stationary airfoil-shaped vanes are used to straighten blood flowprior to entry into the inducer/impeller (a combi-nation of helixically and axially oriented blades).The inducer/impeller has six blades with eight mag-nets sealed in each blade. Outflow diffuser (stator)blades direct flow into the outflow graft. A brushlessDC current motor within the titanium housing cre-ates the electromagnetic force necessary to rotatethe impeller. The motor is driven via a percuta-neous power cable connected to a system controllerand 12-volt battery pack system that can be wornby the patient. An ultrasonic flow probe on theoutflow cannula allows continuous measurementand display of pump output on the laptop drivenClinical Data Acquisition Unit. Changes in pumprevolutions/min are made using this unit as well.The cable for the flow probe is bundled in with thepercutaneous power cable. A pediatric version oftheMicroMed VAD; the DeBakey VAD® Child nowhas FDA humanitarian device exemption (HDE)status. This device is intended for patients with aBSA between 0.7m2 and 1.5m2 and thus suit-able for children between approximately 5–16 yearsof age.
HeartMate IIThree stationary airfoil-shaped vanes are used tostraighten blood flow prior to entry into a three-vane impeller that is suspended in the sintered tita-nium pump housing on two composite ball and cupbearings. Outflow diffuser (stator) blades direct flowinto the outflow graft. Amagnet is incorporated intothe impeller rotor and a DC current brushless elec-tric motor is used to generate the electromagneticcurrent necessary to rotate the impeller. The motoris driven via a percutaneous power cable connectedto a system controller and 12-volt battery packsystem that can be worn by the patient.
InsertionThese devices are implanted in a preperitonealpocket in the left upper quadrant. The inflowand outflow conduits are tunneled into the tho-racic cavity. Insertion requires amedian sternotomy(MicroMed and HeartMate II) or left thoracotomy(Jarvik 2000) and use of CPB. The inflow con-duit of the MicroMed and HeartMate II devices isinserted into the LV cavity via the LV apex andthe Dacron outflow conduit is anastomosed end-to-side to the ascending aorta. The Jarvik 2000device is implanted directly into the LV without aninflow conduit and the Dacron outflow conduit isanastomosed end-to-side to the proximal descend-ing aorta. The power cable of all three devices istunneled through the abdominal wall.
Management of axial pumpsThese devices are remarkably simple to operatewithpump output determined by revolutions/min andP (aortic pressure–LV pressure). Increasing pumprevolutions/min will increase pump flow until thenegative inflow pressure is low enough to causesuction and collapse of the LV around the inflowportion of the pump. In addition, for a given rev-olutions/min pump flow is inversely proportionalto P. In other words, the lower the P the higherthe pump flow at a given revolutions/min. As aresult, these pumps are highly afterload and preloadsensitive. P is most effectively reduced by low-ering aortic pressure (afterload reduction) or byincreasing LV pressure (preload augmentation, LVcontraction). In fact, in the presence of increased LVcontractility semi-pulsatile flow may occur both asthe result of aortic valve opening and as the resultof cyclic increases in pump output with the Preduction that accompanies LV contraction. Mostcenters program axial pumps at a revolutions/minthat allows the native aortic valve to open at leastseveral times per minute as a method of prevent-ing stasis and potential thrombus formation on theaortic valve.
AnticoagulationAnticoagulation is as described for the TAH.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 402 — #28
402 Chapter 11
Extracorporeal membrane oxygenationExtracorporeal membrane oxygenation (ECMO)circuits (Fig. 11.33) are a modification of the CPBcircuit described in detail in Chapter 10. Specifically,ECMO circuits differ from the typical CPB circuit inthe following aspects:• A silicone membrane oxygenator is used in placeof a microporous membrane oxygenator. Siliconemembranes remain functional for days as comparedto hours for microporous membranes.• No cardiotomy suction is used in anECMOcircuit.• A closed venous reservoir (bladder) systemis used in conjunction with a servomechanism.The servomechanism functions to control pumpflow relative to bladder pressure.• ECMO circuits can be used for venovenous (VV)or venoarterial (VA) support. VA support is simi-lar to CPB and is used for mechanical circulatorysupport. VV support is used for patients with severepulmonary dysfunction in the setting of preservedmyocardial function. Venous blood is drained froma proximal location in the central venous circulation
O2Blender
CO2
Membraneoxygenator
Pre-membranepressuremonitor
O2
Fluids
Pump Heparin
Venousreservoir
Heatexchanger
Post-membranepressure monitor
Arterialcannula
Fig. 11.33 Schematic of a venoarterial (VA)extracorporeal membrane oxygenator (ECMO) circuit.Peripheral cannulation via the right internal carotidartery and right internal jugular vein is depicted.A nonocclusive roller pump is depicted; some circuitsuse a centrifugal pump in this same location. Unlikecardiopulmonary bypass (CPB), rapid cooling andrewarming is not necessary and as a result the heatexchange unit can be located distal to the silicone gasexchange membrane. The servomechanism linking theclosed venous reservoir and the pump is not shown.Drugs and fluids in limited quantities can be added tothe circuit in the locations depicted.
(superior vena cava (SVC) or high right atrium).After gas and heat exchange take place in the ECMOcircuit this blood is returned to a more distal site inthe central venous circulation (mid right atrium) tobe pumped by the patient’s heart.VA ECMO is particularly useful in the pedi-
atric population and is commonly used for post-cardiotomy support and as a bridge to transplant.ECMO can be initiated with peripheral vascularcannulation, provides biventricular support, andcan provide adequate systemic oxygen delivery inthe presence of pulmonary hypertension and intra-cardiac right to left shunting. In addition, manypediatric patients are too small for placement ofcurrently available VAD. Rapid initiation of ECMO(rapid response ECMO) is used in both the adultand pediatric population to facilitate resuscitationfollowing acute hemodynamic decompensation orcardiac arrest. In adults and older children, an initialperiod of resuscitationwith ECMOmay provide suf-ficient cardiopulmonary stabilization and reversal ofend-organ injury to permit VAD insertion.
InsertionECMO can be initiated with either peripheral orcentral cannulation. VA ECMO in pediatric patientsis commonly initiated by surgical exposure of theright internal carotid artery and right internal jugu-lar vein. In adults and older children peripheralcannulation of the femoral artery and vein can beutilized. In the postcardiotomy setting cannulationis generally via the right atrium and aorta.
Management of ECMOVA ECMO is managed much like CPB. Whenvenous drainage is adequate the heart will be com-pletely empty, no ejection will occur, and ventila-tion will be unnecessary. More commonly ECMO isconducted in a manner similar to partial CPB. Therewill be incomplete capture of all venous drainage,some systemic ventricular ejection will occur, andsome minute ventilation will be necessary. Sincethere is a small (30mL) closed venous reservoir theamount of blood pumped to the patient can onlyexceed the amount of blood returning to the venousreservoir for a matter of seconds. When this occursthe venous bladder begins to collapse and the

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 403 — #29
Mechanical Circulatory Support 403
servomechanism slows the pump rate appropriatelyto equalize drainage and pump output. Generally,pumps flows of 100–150mL/kg/min are neededin pediatric patients in the absence of significantventricular ejection.
AnticoagulationAn UFH infusion is used to maintain an ACT of180–250 seconds.
Anesthetic considerations
The cardiac anesthesiologist is likely to encounterpatients with a circulatory assist device or a TAH inthe following circumstances:• Heart transplantation candidates who requireplacement of a VAD or a TAH as a bridge to trans-plantation to prevent deterioration in their medicalcondition.• Heart transplantation candidates with a VAD orTAH in place who present for cardiactransplantation.• Postcardiotomy shock patients who require a cir-culatory assist device or a TAH to allow separationfrom CPB.• Postcardiotomy shock patients who have hadtheir circulatory assist device weaned and whorequire operative explanation of the device.• Patients with end-stage cardiomyopathies whoundergo permanent implantation of a VAD.
Device insertionInduction and maintenance of anesthesia for inser-tion of a VAD or TAH in a patient with an end-stagecardiomyopathy should bemanaged as described forpatients undergoing heart transplantation. Implan-tation of VAD and the TAH requires a mediansternotomy or thoractomy and CPB. In addition,placement of the TAH requires bicaval venous can-nulation and aortic cross-clamping. Anastomosis ofthe outflow graft to the side of the ascending ordescending aorta can often be performed off CPBwith application of a partially occluding or side-biting aortic clamp. Application of this clamp mayincrease impedance to LV ejection and cause LVafterload mismatch with subsequent LV distention.If this technique is chosen, careful monitoring ofLV function with TEE is essential. Placement of
the inflow conduit into the apex of the LV is gen-erally performed on CPB although off-CPB tech-niques have been described. Some surgeons placethe inflow conduit during induced ventricular fib-rillation, whereas others apply an aortic cross-clampand administer cardioplegia. Centrifugal pumps areused almost exclusively for postcardiotomy support.As a result, they are placed while on CPB as well.Many of the patients presenting for placement
of a mechanical assist are anti-coagulated withcoumadin because of their dilated cardiomyopathy.These patients usually require replacement of coag-ulation factors, particularly when there is dilutionof factors on CPB as they already have reducedfactor levels. When the PT is markedly elevated,adding fresh frozen plasma to the pump prime inplace of a crystalloid solution is warranted. An addi-tional risk for blood loss is the fact that up to 50%of bridge-to-transplant patients have had previouscardiac surgeries.Limiting transfusion of homologous blood prod-
ucts helps reduce the risk of postoperative pul-monary dysfunction, which can seriously impairRV function. In addition, avoidance of homologousblood products limits patient exposure to antibodies,whichmaymake subsequent typing for heart trans-plantation difficult. Leukocyte filters should be usedwhen administering homologous blood products.Cytomegalovirus (CMV) negative blood should beused in CMV-negative patients.Use of aprotinin has been shown to reduce blood
loss and transfusion requirements for packed cellsand components in patients receiving a LVAD.Aprotinin is discussed in detail in Chapter 10. Theincidence of both mild and severe allergic reac-tions on re-exposure in adults and children issimilar and is approximately 2.8%. Nine percentof the re-exposure reactions are fatal. The likeli-hood of a reaction on re-exposure is increased ifthe re-exposure occurs within 6months of the ini-tial exposure with 95% of all reported re-exposureevents occurring within 6 months of initial expo-sure. When aprotinin is used at the time of deviceinsertion and again at transplantation, re-exposurewithin this interval is not uncommon.The existence of a patent foramen ovale (PFO) or
any site for intracardiac shunting must be excluded

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 404 — #30
404 Chapter 11
before placement of any mechanical assist devicethat is capable of reducing LA pressure below RApressure. Decompression of the LV and reduction inLA pressure below RA pressure will produce right-to-left intracardiac shunting and hypoxemia. Thisis particularly likely in the setting in which RApressure is elevated, such as when there is con-comitant RV dysfunction or elevated pulmonaryartery (PAP pressure. In addition, it introduces thepossibility of producing systemic air emboli frombubbles introduced into the RA by IV lines. All of thedevices described in this chapter except the IABP,are capable of producing such shunting. Either sur-gical examination or TEE can be used to determinewhether a PFO exists. Two-dimensional echocar-diographic views of the intra-atrial septum in con-junction with color flow imaging may be sufficientto detect a PFO. However, because most patientsreceiving mechanical assist devices have elevatedLA pressures, the presence of a PFO by TEE shouldnot be ruled out without the use of provocativemeasures to reduce left atrial pressure (LAP) belowright atrial pressure (RAP). Release of a Valsalvamaneuver (actually release of sustained positiveinspiratory pressure) will transiently reduce LAPbelow RAP. When this is used in conjunction withagitated saline contrast, TEE imaging of the RA, LA,and intra-atrial septumdetection of a PFO is reliable.TEE should be used to assess the ascending aorta
and thoracic aorta for the presence of atheroma-tous disease and calcifications that will influence thesite of aortic outflow cannula placement. Epiaor-tic scanning may be useful in guiding placement ofthe device outflow conduit on the ascending aorta.TEE should be used to assess for the presence ofintracardiac thrombi.Comprehensive assessment of all four valves by
TEE is necessary prior to VAD placement:• Aortic valve. Placement of an LVAD is contraindi-cated in the presence of a mechanical aortic valveor significant aortic insufficiency. Thrombus for-mation on the mechanical aortic valve can resultfrom the absent or minimal aortic valve openingthat occurswhen the LVAD is functioning normally.Aortic valve insufficiency will not permit effective(decompression of LA and LV) or efficient (highcardiac output) LVAD functioning because a large
portion of LVAD ejection will be regurgitated intothe native LV. The problemworsens as LVADoutputincreases. In these circumstances, the aortic valvecan either be replaced with a bioprosthesis or moreuncommonly removed and pericardial patch clo-sure of the aortic annulus performed. Aortic stenosisis not a contraindication to LVAD placement.• Pulmonary valve. RVAD placement is contraindi-cated in the setting of pulmonary valve insuffi-ciency as it will not permit effective (decompressionof RA and RV) or efficient (high cardiac output)RVAD functioning because a large portion of RVADejection will be regurgitated into the native RV.• Mitral valve. The presence of significant mitralstenosis is a contraindication to placement of anLVAD in series with the LV. Significant mitralstenosis will impede inflow into the LV and sub-sequently into the inflow cannula of the LVADand will not allow decompression of the LA.Mitral valve repair or bioprosthetic replacementwill be necessary. With parallel LVAD placement(LA and aortic cannulation) mitral stenosis is not acontraindication.• Tricuspid valve. Assessment of the tricuspid valveprior to LVAD placement. The etiology of any pre-existing tricuspid regurgitation should be carefullydelineated, as regurgitation is likely to be worsenedby LVAD placement as described below.Following device placement, meticulous deair-
ing of the native cardiac chambers and the assistdevice is necessary to prevent systemic air emboli.The patient usually is kept in steep Trendelenbergposition until deairing is completed. TEE is use-ful in detecting intracardiac air and in guiding thede-airing process.
Management of patients withdevices in placePost-device implantation management is tailoredto the patient, the specific device, and the setting.The following issues must be considered.
Function of the nonassisted ventricleProper functioning of an LVAD requires an RVthat functions well enough to match the com-bined output of the LV and the LVAD. An RVthat is capable of delivering only 3 L/min to the

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 405 — #31
Mechanical Circulatory Support 405
pulmonary circulation and LA will severely com-promise optimal functioning of an LVAD that candeliver 6 L/min. Because many patients requiringLVAD implantation have concomitant RV dysfunc-tion, there may be a need for inotropic/vasodilatorormechanical support (RVAD) of theRV after LVADimplantation.Approximately 10% of patients implanted with
an LVAD require placement of an RVAD for RVfailure. Preoperative clinical factors that are use-ful in predicting the need for mechanical supportof the RV after LVAD implantation are youngerpatients, low BSA patients, female patients, patientswith a nonischemic cardiomyopathy (more likelyto involve both ventricles than ischemic origin),and patients receiving mechanical ventilatory sup-port. In addition, patients with low preoperativePAP (systolic, mean, diastolic), significant tricus-pid regurgitation (TR), and low right ventricularstroke work index (RVSWI) are at risk. Low PAP inthese patients is not an indication of low pulmonaryvascular resistance (PVR) but rather of severelydepressed RV function and low RV output.The indications for RVAD support following
LVAD placement are as follows:• Maximal inotropic support in the setting of nitricoxide (NO) and/or prostaglandin.• Low mean and diastolic PAP, elevated CVP, anddiminished RVSWI.• Decreased LVAD flow (<2.4 L/min).• Dilated, hypokinetic RV by echocardiographicexamination.• Decreased urine output and/or a high fraction ofinspired oxygen (Fio2) requirement.The effects of LVAD implantation on RV function
are complex and are summarized:• Contractility. Complete pressure unloading of theLV with an LVAD shifts the intraventricular sep-tum to the left and reduces the LV contributionto RV contraction. Systolic ventricular interdepen-dence is such that LV contraction may account formost RV-developed pressure and volume outflow.In addition, there may be loss of RV contrac-tion in the areas adjacent to the leftward-shiftedintraventricular septum. As a result, LVAD inser-tion generally results in impairment of RV systolicfunction.
• Afterload. Insertion of an LVAD generally pro-duces a reduction in RV afterload. Insertion ofan LVAD results in reduction of LA pressures byreducing LV distention. Reduction in LA pres-sures results in reduced pulmonary venous con-gestion and a reduction in PVR and PA pressuresdespite the increase in cardiac output and pul-monary blood flow that accompanies implantation.Reduction of RV afterload improves RV functionthrough enhanced shortening of the RV free wall.Not all patients have immediate normalization ofPVR and PA pressures. Patients with longstand-ing pulmonary venous congestion may have anadditional component of pulmonary hypertensionthat may take days or weeks to resolve. In addi-tion, although PA pressures decrease routinely afterLVAD implantation, the transpulmonary gradient(mean pulmonary arterial pressure–left atrial pres-sure) routinely increases slightly post implantationbut falls by 24hours postoperatively. This is mostlikely due to the residual pulmonary edema, andthe effects of CPB and blood product administrationon the pulmonary vascular bed.• Preload. LVAD insertion increases cardiac outputthat in turn produces an increase in RV preload. Inaddition, LVAD insertion improves RV complianceand RV end-diastolic volume (EDV) increases whileRV end-diastolic pressure (EDP) decreases.• Tricuspid valve function. LVAD implantation gen-erally acutely decreases mitral regurgitation whileworsening tricuspid regurgitation both acutely andchronically. Poor apposition of the tricuspid valveleaflets after LV decompression with a LVAD occursas the result of a leftward shift of the intraventricularseptum and the increased RV volume load. There isgenerally dilation of the tricuspid annulus and left-ward deviation of the septal components of the tri-cuspid subvalvular (chordae and papillary muscles)apparatus.• Coronary perfusion. LVAD insertion may improveRV function by increasing aortic blood pressure andimproving RV coronary blood flow.On balance, LVAD insertion results in global impair-ment of RV systolic function, which is offset byincreased RV preload and reduced RV afterload suchthat RV output is maintained or increased. As men-tioned, 10% of patients receiving an LVAD will

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 406 — #32
406 Chapter 11
require placement of an RVAD for RV failure thatpersists despite aggressive pharmacologic therapy toimprove RV function. These patients usually have acomponent of pulmonary vascular resistance thatis not immediately reduced by decompression ofthe LV, and underlying RV contractile dysfunctionparticularly of the intraventricular septum. Septaldysfunction causes the intraventricular septum tomove away from the RV free wall during systole.The RV free wall cannot compensate for this move-ment, even in the setting of reduced afterload andRV stroke volume falls.Treatment of RV dysfunction and TR with
pulmonary vasodilators and inotropes will be nec-essary for patients who manifest severe RV dys-function after LVAD implantation. Severe RVdysfunctionwill produce a low LVADoutput in con-junctionwith a high CVP and TRwith RV distentionand hypokinesis seen with TEE. TEE is valuablein guiding therapy to reduce TR and improve RVfunction. In some circumstances a tricuspid annu-loplasty may be warranted at the time of LVADimplantation.
Preload to the deviceProper functioning of all assist devices excluding theIABP are dependent on delivery of adequate volumeto the device. TEE is useful in determining the etiol-ogy of poor preload to a device. The following causesshould be considered:• Hypovolemia.• Poor positioning/obstruction of the inflow can-nula. This is particularly important in RVAD andLVAD operating in parallel with the native heart ascannulas are placed in the RA or LA. TEE is usedto ensure unobstructed inflow to the device. Caremust be taken to ensure that atrial cannula do notcross theAVvalve or impinge on the intra-atrial sep-tum. For devices in series with the native heart, theventricular cannula must not impinge on the ven-tricular free wall, septum, or papillary muscles. Nosubstantial pressure gradient should exist across theinflow conduit. In addition, significant mitral steno-sis will impede inflow into the LV and subsequentlyinto the inflow cannula of the LVAD and will notallow decompression of the LA.• IVC, SVC, or pulmonary venous obstruction inTAH patients. In TAH patients, TEE is used to ensure
that there is no obstruction of the SVC, IVC, orpulmonary veins.• Impaired RV functionwith delivery of inadequatevolumes of blood across the pulmonary circulationto a LVAD.
Afterload presented to the deviceThe performance of both pulsatile and nonpul-satile assist devices is influenced by afterload. Asaddressed previously, centrifugal and axial pumpshave reduced performance as vascular resistanceincreases. At very high afterload, pulsatile pumpswill develop increasing residual volumes as theyfail to empty completely. This is analogous to anincreasing end-systolic volume in the native ven-tricle with the end result being a reduced strokevolume. By increasing driveline pressure, pneu-matic pumps can be made to empty completelyat higher afterload. The result will be elevatedMAP or PAP and the potential for more hemol-ysis. At systolic pressures in excess of 160mmHg,the Novacor device exhibits increased residual vol-ume and begins to overheat. As SVR increasesin patients with the pneumatic HeartMate theejection time necessary to completely empty thedevice increases. This, in turn, reduces maximalpump rate/min because minimal LVAD filling timeis a fixed proportion of the selected LVAD ejec-tion duration. With the Abiomed BVS 5000 andAB 5000 devices increased afterload will increasethe duration of ejection and for a given diastolicfilling period will reduce the pump rate/min. Inall of these circumstances, afterload reduction iswarranted.Another source of device malfunction related to
afterload is obstruction to outflow. TEE is used toensure that there is no significant pressure gradi-ent distal to the outflow cannulas or conduits in thegreat vessels.
ArrhythmiasAtrial and ventricular arrhythmias are not uncom-mon in the subset of patients requiring circulatoryassist devices. They often resolve as the patient’shemodynamic status improves. The presence ofatrial and ventricular arrhythmias in patients withan LVAD is often not of significant hemodynamicconsequence provided the PVR is not elevated.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 407 — #33
Mechanical Circulatory Support 407
In these patients there may be adequate passivedelivery of blood across the pulmonary vascularbed to the LVAD even during ventricular tachy-cardia (VT) and ventricular fibrillation (VF) in amanner similar to Fontan patients (total cavopul-monary connection without pulsatile RV function).In patients with elevated PVR the inability to con-trol these arrhythmias will require placement ofan RVAD.
Catecholamine resistant vasodilatoryshock (CRVS)A subset of patients will exhibit CRVS follow-ing placement of a mechanical circulatory sup-port device. This manifests as low SVR and highunstressed venous volume (high venous capaci-tance) that is resistant to high doses of potent cate-cholamine vasoconstrictors such as norepinephrine.Hypotension is common as SVR is low and preloadto the assist device is low as well. In circum-stances where preload to an LVAD or TAH ismaintained, hypotension may persist despite andoutput in excess of 6–7 L/min. CRVS is dueto a combination of factors including endoge-nous NO release, arginine vasopressin (AVP) defi-ciency, intracellular acidosis (opens KATP chan-nels), and contact phase activation-induced sys-temic inflammatory response. These patients gen-erally have a favorable response to AVP infusion(0.01–0.05units/min) in combination with lowerdoses of norepinephrine. AVP infusion repletesAVP deficiency, restores α1-receptor responsive-ness to norepinephrine by closing KATP chan-nels, and potentiates the vasoconstrictor effectsof norepinephrine by suppressing cyclic guanosinemonophosphate (cGMP) release induced by NO. Inaddition, AVP administration increases release ofcorticotropin (ACTH). Patients receiving an LVADare often treated with amiodarone, angiotensin-converting enzyme (ACE) inhibitors, andmilrinonein the perioperative period that will exacerbatehypotension.
Cardiac output determinationThe determination of cardiac output in patientswith mechanical circulatory assist devices issummarized.
• TAH. Cardiac output is displayed by the COMDUof the CardioWest TAH. A thermodilution pul-monary artery catheter is not necessary and, in fact,must be removed before device implantation.• LVAD. Device output is equal to systemic car-diac output as long as the aortic valve remainsclosed. TEE will readily determine if this is true.This situation is likely for devices in series with theLV and less likely for devices in parallel with theLV. If there is ejection from the native LV in con-junction with device output, then thermodilutioncardiac output can be used as an accurate mea-sure of the combined native ventricular and deviceoutput. Patients with LVAD require pulmonarycatheters to aid in management of concomitant RVdysfunction.• RVAD. Device output is equal to pulmonic out-put as long as the pulmonic valve remains closed.TEE will readily determine if this is true. BecauseRVAD are generally placed in series with the RV,the total pulmonic output ismore likely to be a com-bination of native RV output and RVAD output. Inthis setting, thermodilution cardiac outputs will notbe accurate because the transit times of blood andsaline through the native RV and the RVAD will bedifferent. Thiswill interferewith the thermodilutiontechnique.
Effects of ventilationPositive-pressure ventilation may adversely affectRV function by mechanically compressing the pul-monary vasculature if peak airway pressures arehigh. This can reduce native RV output and deliveryof blood to an LV assist device.The TAH ventricle functions as an extra-thoracic
chamber surrounded by atmospheric pressure indiastole and connected to an atrium and greatvessels that are surrounded by intrathoracic pres-sure. Because there is no compliant intraventricularseptum, there is no ventricular interdependence.Increases in intrathoracic pressurewill reduce fillingof the native atria from the systemic and pul-monary veins but will enhance filling of the pros-thetic ventricles. Despite this, respiratory variationof systemic blood pressurewill occur in the setting ofhypovolemia or dilation of venous capacitancevessels.

Alice Nelson Dinardo: “ch11” — 2007/7/16 — 12:40 — page 408 — #34
408 Chapter 11
Effects of induction andmaintenance agentsInduction and maintenance of anesthesia in thepatient with an assist device or TAH should takeinto account the hemodynamic effects of the chosenanesthetic agents. The effect of induction agents onmyocardial contractilitymust be taken into account.Although the effects of agents on myocardial con-tractility are not important in TAH patients, theeffects of agents on the peripheral vasculature doinfluence hemodynamics.
Device weaningDevices are weaned by gradually withdrawing sup-port while assessing ventricular function and hemo-dynamics. This usually requires the presence of a PAcatheter and arterial line. The IABP is weaned bydecreasing the pump rate from1:1 to 1:2 to 1:3. Cen-trifugal and axial pumps are weaned by decreasingthe pump flow rate. The risk of thrombus formationis enhanced when the pump flow rate is at or lessthan 2 L/min. Therefore, adequate anticoagulationshould bemaintained and the pump should bewith-drawn promptly after weaning down to this level.Weaning of pulsatile devices involves adjustment ofthe device to operate at a decreased fixed rate. TEEhas proved to be very valuable in guiding wean-ing of circulatory assist devices because it allowson-line assessment of RV and LV function duringthe weaning process.
Monitoring considerationsArterial line placement may be difficult and pulseoximetry monitoring inconsistent in patients with
nonpulsatile flow from axial and centrifugal pumps.Allowing the native ventricle to eject by temporarilyreducing pump rate may be necessary for arte-rial line placement. Insertion of central venouscatheters in patients with pulsatile RVAD imposesan increased risk of entraining air into the centralcirculation particularly when vacuum is applied tocannulas situated in the RA. Vacuum should betemporarily discontinued when this procedure isundertaken. In addition, care must be taken whena central venous line is accessed for volume or druginfusion while vacuum is applied.
Suggested reading
Cheung AT, Savino JS, Weiss SJ. Beat-to-beat aug-
mentation of left ventricular function by intraaortic
counterpulsation. Anesthesiology 1996;84:545–54.Copeland JG, Smith RG, Arabia FA et al. Cardiac replace-
ment with a total artificial heart as a bridge to
transplantation. N Engl J Med 2004;351:859–67.Horton SC, Khodaverdian R, Chatelain P et al. Left
ventricular assist device malfunction: an approach
to diagnosis by echocardiography. J Am Coll Cardiol
2005;45:1435–40.Mancini D, Burkhoff D. Mechanical device-based meth-
ods of managing and treating heart failure. Circulation
2005;112:438–48.Miller LW, Lietz K. Candidate selection for long-term left
ventricular assist device therapy for refractory heart
failure. J Heart Lung Transplant 2006;25:756–64.Ochiai Y, McCarthy PM, Smedira NG et al. Predictors
of severe right ventricular failure after implantable
left ventricular assist device insertion: analysis of
245 patients. Circulation 2002;106:I198–202.

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 409 — #1
CHAPTER 12
Myocardial Preservation duringCardiopulmonary Bypass
Myocardial preservation techniques are afundamental component of contemporary car-diac surgery. The ability to suspend metabolicdemand and preserve myocardial viability dur-ing the operative procedure allows the surgeonopportunity and time to complete complex repairs.Early efforts in cardiac surgery were hinderedby postoperative myocardial failure after tech-nically successful operative procedures due toextensive damage sustained during the opera-tive procedure. Myocardial necrosis was commonin patients dying after cardiac surgery and thisnecrosis occurred during cardiopulmonary bypass(CPB). Researchers soon found myocardial preser-vation techniques to reduce myocardial injuryafter CPB.Initially, surgeons attempted to operate on both
normothermic and hypothermic empty, beating,or fibrillating hearts. These conditions providedpoor operative exposure and resulted in myocardialnecrosis. Eventually, aortic cross-clamping evolvedas the method of choice to exclude the heart fromthe circulation thereby enhancing surgical expo-sure by providing a bloodless field. A bloodlessfield however, came at the cost of myocardialperfusion. The heart must survive this intervalof ischemia (cross-clamp interval) without injury(Fig. 12.1). Myocardial preservation techniquessoon evolved and now provide optimal protec-tion of the heart during aortic cross-clamping andin the reperfusion period following clamp release.This chapter reviews myocardial preservation
during aortic cross-clamping and in the immediatereperfusion interval.
Consequences of aortic cross-clampingMyocardial ischemia occurs as the result of severelycompromised or absent myocardial perfusion. Incontrast, hypoxia refers to a reduction in substratedelivery with maintained perfusion. Because aor-tic cross-clamping isolates the coronary circulationfrom perfusion, global myocardial ischemia resultsunless they are adjunct protective measures. Tounderstand the nature of these protective mea-sures, it is necessary to examine the consequencesof global myocardial ischemia.
Cessation of oxidative phosphorylationThis is the first metabolic derangement to occur.There is disruption of the electron transport chainand the Kreb’s cycle is inhibited. This occurs withinminutes of cross-clamping and results in termina-tion of high-energy phosphate production in theform of adenosine triphosphate (ATP) and creatinephosphate (CP).
Depletion of ATP and CP storesATP supplies energy directly to the myocardium;whereas CP acts as an intermediate energy sourceto resupply ATP. During ischemia, there is immedi-ate depletion of CP stores. Within 15 minutes, ATPstores are reduced by one-half and CP stores areessentially depleted.
409

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 410 — #2
410 Chapter 12
Cross-clampOn
Pre-bypass Cardioplegia Reperfusion
Off
(Early) (Late)
Fig. 12.1 A schematic diagram representing thechronology of a cardiac surgical procedure in whichextracorporeal circulation and intermittent cardioplegiaare used. Injury from ischemia can occur (a) beforecardiopulmonary bypass is initiated, as a result ofcoronary artery disease or other disease processes,hypotension, or ventricular fibrillation; (b) duringintermittent cardioplegia between infusions of solution,or when cardioplegia is poorly distributed because ofcoronary lesions present before revascularization orobstructions in the grafts; (c) during the reperfusionperiod, which can be divided into early and latecomponents. In reality, the potential for reperfusioninjury exists at each of these intervals when (a)resolution of pre-bypass hypotension or dysrhythmiasrestores blood flow; (b) cardioplegia solution is infused athigh delivery pressures (“perfusion” injury) or has aninappropriate composition; and (c) coronary blood flowwith unmodified systemic blood is restored after removalof the cross-clamp, especially if a terminal “reperfusion”dose of cardioplegia is not given. Systemic hypotensionand physical or embolic obstructions to coronary bloodflow can also induce injury during this period. (FromVinten-Johansen J, Ronson RS, Thourani VH,Wchsler AS. Surgical myocardial protection. In:Gravlee GP, Davis RF, Kurusz M, Utley JR (eds).Cardiopulmonary Bypass: Principles and Practice, 2nd edn.Philadelphia: Lippincott Williams & Wilkins,2000:214–64, with permission.)
Anaerobic metabolismGlucose is the only substrate available for anaer-obic metabolism in the myocardium. To providesubstrate for glycolysis, glycogenolysis must occur.Large glycogen stores may provide ample substratefor anaerobic production of ATP, but unless there isadequate washout of the hydrogen ions and lactateproduced from anaerobic glycolysis, further glycol-ysis is inhibited by sufficiently high concentrationsof these metabolites. Generally, anaerobic produc-tion of ATP ends a few minutes after it starts in theglobally ischemic myocardium.
Inhibition of free fatty acid oxidationNormally, free fatty acids are the major energysource for the myocardium in the post-absorptivestate. Ischemia interferes with free fatty acid oxi-dation, fatty acid uptake, and transfer into themyocardium.
Depletion of the adeninenucleotide poolAfter 30–40minutes of global ischemia, the progres-sive degradation of ATP to adenosine 5-diphosphate(ADP), ADP to adenosine monophosphate (AMP),and AMP to inosine and hypoxanthine depletesthe myocardium of its adenine sources. Therefore,reperfusion of energy sources to replenish ATP lev-els will be fruitless at this time unless the adenineprecursors to form ATP are provided as well.
Impairment of calcium homeostasisThe consequences of impaired calcium home-ostasis are summarized in Fig. 12.2. Homeosta-sis of intracellular calcium is dependent on twoATP-dependent processes: sequestration of calciuminto the sarcoplasmic reticulum and extrusion ofcalcium across the sarcolemma. At 30minutes ofglobal ischemia, the myocardium’s ability to reg-ulate intracellular calcium is impaired by deple-tion of ATP stores. Loss of calcium homeostasisresults in sustained myocardial contracture becausesequestration of calcium is necessary to breakthe actin–myosin cross-bridges that allow diastolicrelaxation to occur. In addition, high intracellu-lar calcium levels cause further depletion of ATPstores through activation of myosin adenosinetriphosphatase (ATPase).
Disruption of cellular architectureBy30minutes of global ischemia, there is swelling ofthemitochondria and sacroplasmic reticulumdue toincreased osmolarity generated by the metabolitesof anaerobic metabolism. After 30minutes, there isprogressive accumulation of the products of mem-brane degradation. Ischemia-induced reduction offree radical scavengers results in continued lipid per-oxidation and membrane destruction via oxygen-free radicals. After 60minutes, there is destructionof the cell membrane such that cell death occurs.

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 411 — #3
Myocardial Preservation 411
Reduced coronary flow
Reduced availability of oxygen
Reduced synthesis of ATP
Failure of Ca2+ homeostasis
Activation ofCa2+ lipasesActivation of
Ca2+ ATPases
MitochondrialCa2+ overload
Impairedmitochondrial function
Failure of ATPproduction
Increased usageof ATP
Reduced ATP
Loss of structure and function
Raised cytosolic Ca2+
Fig. 12.2 Consequences of impaired calciumhomeostasis secondary to reduced coronary blood flow.ATP, adenosine triphosphate; ATPases, adenosinetriphosphatases. (From Nayler WG. The role of calciumin the ischemic myocardium. Am J Pathol1981;102:262–70, with permission.)
CardioplegiaCardioplegia the solution used to arrest and pro-tect the heart during aortic cross-clamping. Sincethe introduction of cardioplegia in 1955, the com-position and mode of administration has evolvedgreatly. Cardioplegia solutions arrest the heartin diastole resulting in a profound reduction inmetabolic demand. In addition, cardioplegia playsa restorative role replenishing energy stores inischemic hearts. There is great variability in theadministration, timing, composition, and tempera-ture of the various cardioplegia regimens. Despitethese variations, the basic components of cardiople-gia systems are similar (Fig. 12.3), and the goals ofcardioplegia administration remain unchanged.Aortic cross-clamping drastically reduces oxygen
and substrate supplies to the myocardium.
Cardioplegia solutions, administered immediatelyupon cross-clamp application, promptly reducemyocardial oxygen consumption. In addition, car-dioplegia provides substrates to meet these reducedenergy demands so that pre-ischemic energy storesare not depleted. Cardioplegia solutions induce elec-tromechanical arrest of the heart in diastole. Arrestin diastole can be induced by depolarized arrest(elevated potassium), polarized arrest (adenosine,potassium channel openers, procaine, lidocaine), orarrest by influencing calciummechanisms (elevatedmagnesium, calcium antagonists).Because electromechanical work constitutes
95% of total myocardial oxygen consumption, thearrested heart will have very low energy require-ments. In the arrested state, only basal energyrequirements (those required to keep cellularmetabolic processes intact)must bemet. Figure 12.4illustrates the very low oxygen consumption asso-ciated with induced arrest. Aerobic and anaerobicmetabolism can provide enough energy to meetbasal energy requirements as long as there is peri-odic replenishment of substrates and washout ofmetabolites.There is considerable variability in the compo-
sition of cardioplegia solutions used in differentinstitutions. Despite this wide variety of composi-tion, there are certain properties all solutions mustshare. Cardioplegia must:• induce prompt arrest of the heart in diastole toreduce myocardial oxygen consumption.• incorporate hypothermia to further reducemyocardial oxygen consumption.• provide sufficient substrates tomeet themetabolicdemands of the arrested heart.• provide buffering to counteract the acidosis thataccompanies ischemia.• provide increased osmolarity to prevent thecellular edema that accompanies ischemia.• provide membrane stabilization with additives oravoidance of hypocalcemia.• have no adverse effects of its own.• have a composition suitable for delivery to allareas of the myocardium.Table 12.1 lists a typical cardioplegia solu-tion used in contemporary practice. To fulfillthese requirements, a typical cardioplegia solution

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 412 — #4
412 Chapter 12
Retrograde cardioplegia
Antegrade cardioplegia
Pressuremonitoring
line
Pressurerelief line
Patientdeliveryline Temperature
probe port
Heatexchanger
Roller pump
Blood crystalloidshunt
Oxygenator
HK LK
Crystalloidcardioplegia
Fig. 12.3 Components of a cardioplegia deliverysystem. A modern cardioplegia delivery system isdemonstrated. Oxygenated blood may be diverted fromthe oxygenator of the cardiopulmonary bypass (CPB)circuit and mixed with a high potassium (HK)-containingcrystalloid cardioplegia solution for induction ofelectromechanical arrest or with a low potassium(LK)-containing cardioplegia solution. The ratio of bloodto crystalloid may be varied and the solution is pumpedvia a roller pump to a heat exchanger for warming orcooling before administration. The line pressure andtemperature of the cardioplegia solution is monitored.Perfusion of the myocardium may be antegrade throughthe coronary arteries or retrograde through a catheter in
the coronary sinus. The retrograde catheter is usuallyplaced before CPB through the right atrial wall and notthe coronary sinus. Evidence of successful cannulation ofthe coronary sinus includes dark blood (secondary to thehigh oxygen extraction of the heart) returning from thecatheter, visualization of the catheter in the coronarysinus by transesophageal echocardiography (TEE), andintravascular pressure monitoring. During retrogradeperfusion, a pressure of 30–50mmHg is desirable. (FromSchell RM, Applegate RL, Reves JG. Cardiopulmonarybypass. In: Miller RD (ed). Atlas of Anesthesia.Philadelphia: Current Medicine (Churchill Livingstone),1999:9.1–30, with permission.)
contains the components described in the followingsections.
PotassiumIncreasing extracellular potassium concentration toinduce depolarized arrest is the primary method
used to induce electromechanical arrest in mostcardioplegia solutions.Extracellular hyperkalemia results in depolar-
ization of the cell membrane, inactivation ofthe voltage-dependent fast sodium channel, andsustained diastole. This effect is reversed after

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 413 — #5
Myocardial Preservation 413
6.0
4.0
2.0
0
cc/1
00 g
/min
37°C 32°C 28°C 22°C
Beating nonworkingFibrillatingArrest
Fig. 12.4 Left ventricular oxygen consumption duringthree functional states (beating empty, fibrillating, andarrested) and at four temperatures. Hypothermia reducesmyocardial oxygen consumption for any of thefunctional states. Below 37C, the beating empty heartconsumes the most oxygen, followed in decreasing orderby the fibrillating and the arrested heart. (FromBuckberg GD. Studies of the effects of hypothermia onregional myocardial blood flow and metabolism duringcardiopulmonary bypass. J Thorac Cardiovasc Surg1977;73:87–94, with permission.)
Table 12.1 Components of a typical cardioplegiasolution.
Induction cardioplegia solutionTHAM solution 2.11g 71.60mLGlutamate∗ 32.43g 44.27mLAspartate† 27.72g 44.27mLCPD 17.76mLKCl 26.6mEq 13.25mLLidocaine 49.77mg 2.53mLD5W 88.125mL
Total volume 282.500mL
Subsequent cardioplegia solutionTHAM solution 1.59g 53.3mLGlutamate 24.39g 33.3mLAspartate 20.80g 33.3mLCPD 13.3mLKCl 0.00mEq 0.00mLLidocaine 49.77mg 2.53mLD5W 66.8mL
Total volume 202.5mL
CPD, citrate phosphate dextrose; KCl, potassium chloride;THAM, Tris-hydroxylmethyl aminomethane.∗ Glutamate concentration is 7.32% in H2O.† Aspartate concentration is 6.25% in H2O.
15–20minutes by the normal metabolism and ioniccurrents present in the myocyte. The potassiumconcentration necessary to induce prompt arrestvaries from solution to solution. For example,myocardial hypothermia reduces the extracellularpotassium concentration required to induce arrest.Crystalloid cardioplegia solutions require lowerextracellular potassium concentrations to inducearrest than do blood cardioplegia solutions.Nonetheless, cardioplegia solutions generally
have a potassium concentration ranging from15–30mEq/L. This concentration produces promptelectromechanical arrest. Concentrations of potas-sium higher than 40mEq/L are detrimental becausethey increase calcium influx by increasing calciumconductance. Recall that increased intracellular cal-cium will increase wall tension and myocardialoxygen consumption. In addition, increasing cal-cium conductance while ischemia-induced loss ofcalcium homeostasis is occurring will exacerbateischemic damage.
HypothermiaHypothermia is an important component of car-dioplegia solutions because it reduces myocardialoxygen consumption even in the arrested heart,reduces the degree of extracellular hyperkalemianeeded to cause electromechanical arrest and isadditive with potassium-induced arrest in pre-venting ischemic damage. Cardioplegia is typicallyadministered in one of three temperatures: cold5–10C, tepid 27–30C , and warm 33–38C. Gen-erally, a combination of temperatures is used withinitial cold or tepid administration later followedby a “hot shot” of warm cardioplegia just beforeremoval of the aortic cross-clamp. Despite deliveryof these cold solutions into the coronary arteries, itoften is difficult to cool the myocardium to <15C.Incomplete cooling may be due to the presence ofcoronary stenoses preventing homogenous deliv-ery of the cold cardioplegia solution, noncoronarycollaterals perfusing the heart with warm blood orsystemic venous return warming the heart.
CalciumLoss of calcium homeostasis is associated withcell dysfunction and death after ischemia. For this

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 414 — #6
414 Chapter 12
reason, one might assume that the addition of cal-cium to cardioplegia solutions is detrimental. In fact,a small amount of calcium (>50mM) is necessaryto prevent the calcium paradox and to allow func-tional recovery after aortic cross-clamp removal.Calcium paradox is the massive cellular destruc-tion that occurs when the myocardium is perfusedwith a calcium-containing solution after a period ofcalcium-free perfusion. Calcium paradox is due towashout of calcium from the sarcolemma with sub-sequent inability of the sarcolemma to limit calciuminfluxwhen presentedwith a calcium load. Calciumparadox is more likely to occur if the cardioplegiasolution is alkalotic.Despite this risk, most crystalloid cardioplegia
solutions do not have calcium added to them; theycontain <1mM/L of calcium. Blood cardioplegiarequires no additional calcium. Calcium paradoxis prevented by delivery of an adequate con-centration of calcium via the systemic perfusatefrom noncoronary collaterals and by the pres-ence of hypothermia. Blood cardioplegia solutionsdeliver varying concentrations of calcium to themyocardium. The exact concentration depends onhow extensively the blood solution is diluted beforeit is used as a medium for cardioplegia. In fact,most cardioplegia solutions contain the anticoag-ulant citrate-phosphate-dextrose (CPD) to chelatecalcium thereby making calcium unavailable inthe coagulation system. The CPD solution actsto chelate calcium, buffer the blood, and providedextrose as a substrate for glycolysis.
SodiumThe optimal sodium concentration is unknown, butmost cardioplegia solutions avoid extreme hypo- orhypernatremia relative to intracellular sodium con-centration. Perfusion of the heart with a hypona-tremic solution may predispose accumulation ofintracellular calcium with subsequent increases inwall tension and myocardial oxygen consumption.Perfusion of the heart with a hypernatremic solu-tion results in accumulation of intracellular sodium.This may result in cellular edema. It also may resultin an accumulation of intracellular calcium as thesodium–calcium exchange pumpmoves sodium outand calcium into the cell. For these reasons, most
cardioplegia solutions have sodium concentrationsin the range of 100–120mEq/L.
MagnesiumHigh-dose magnesium can induce cardiac arrestin the absence of other agents. Magnesium inlower doses acts to stabilize cell membranes, blockphosphorylation of myosin (preserving high energysubstrates), and acts as a slow channel calciumblocker.
BufferingAnaerobic metabolism accompanying ischemiaresults in cellular acidosis. Acidosis results innegative inotropy, reduced glycolysis, and depres-sion of myocardial contractile proteins. The accu-mulation of acid results in inhibition of furtheranaerobic metabolism. Buffering allows anaerobicmetabolism to continue and reduces ATP deple-tion in the ischemic myocardium. As myocardialtemperature decreases, the appropriate uncorrectedpH becomes more alkalotic. Therefore, the bufferschosen must be effective at the alkalotic pH foundin the hypothermic myocardium. Tromethamine(THAM), bicarbonate, phosphate, and histidine areall used as buffers in cardioplegia solutions.Histidine is a common buffer and is superior to the
others because the pKa shifts into the alkaline rangeas temperature decreases; therefore it is an effectivebuffer over a wide variety of temperatures and pHlevels. In addition, there is greater buffering capac-ity than crystalloid cardioplegia solutions bufferedwith standard concentrations of either bicarbon-ate or THAM. Blood cardioplegia provides bettermyocardial buffering than crystalloid cardioplegiabufferedwith bicarbonate due to the presence of thehistidine buffering system in blood. Histidine addedto crystalloid cardioplegia can provide a bufferingcapacity similar to that of blood cardioplegia.
OsmolarityBecause myocardial edema accompanies ischemia,cardioplegia solutions are formulated to minimizefurther accumulation of intracellular fluid. Cardio-plegia solutions with osmolarities >400mOsm/Lexacerbate myocardial edema, probably by induc-ing increases in intracellular sodium. On the otherhand, solutions with a low osmolarity will result

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 415 — #7
Myocardial Preservation 415
in accumulation of intracellular water and fur-ther edema. The ideal osmolarity remains undeter-mined, but probably is approximately 370mOsm/L.Mannitol and albumin are the additives commonlyused to manipulate osmolarity in cardioplegiasolutions.
SubstratesEnergy production during anaerobic metabolismrequires provision of a substrate. Glucose andinsulin as components of a cardioplegia solutionallow uptake of glucose into the myocardiumfor use during anaerobic metabolism. Anaero-bic metabolism results in the production of lac-tic acid and nicotinamide adenine dinucleotide(NADH). Accumulation of these metabolites leadsto the eventual shutdown of further anaerobicmetabolism. Substrate provision is useful onlyif there is periodic washout of the metabolitesthat inhibit anaerobic metabolism. In fact, in theabsence of periodic washout of metabolites, sub-strate enhancement has been demonstrated to bedeleterious tomyocardial recovery after aortic cross-clamping. In clinical practice, this washout occursthrough noncoronary collateral flow or throughintermittent infusion of cardioplegia.The use of glucose and insulin before aortic cross-
clamping may result in improved post-cross-clampmyocardial function. Infusion of insulin and glu-cose before aortic cross-clamping results in a shiftfrom oxidative lipolysis to glycolysis. There is anincrease in glycogen stores. This pre-ischemic accu-mulation of glycogen stores and the early shift toanaerobic metabolism may have a protective effectduring ischemia.Glucose and insulin concentrations in cardio-
plegia solutions vary greatly from institution toinstitution. In fact, some institutions do not addeither entity to their solutions. Some glucose ispresent in blood cardioplegia and, therefore, littleor no glucose must be added when blood is used asa cardioplegia vehicle.
Crystalloid versus blood cardioplegiasolutionsCardioplegia solutions are delivered in either a crys-talloid or a blood medium. There are important
differences between the two formulations. Crystal-loid solutions generally are prepared by the hospitalpharmacy in containers that are delivered to theperfusionist. Blood solutions are prepared by draw-ing off oxygenated blood from the CPB circuit intoa separate reservoir and mixing it with a prepre-pared crystalloid base solution. The ratio of bloodto crystalloid base varies from institution to institu-tion (4:1 to 1:4). Potassium and other additives arethen added to the blood in the sufficient amounts toobtain the desired concentration. Both solutions canbe temperature regulated and administered cool,tepid, or warm. Cold blood cardioplegia is diluted toa hematocrit of 10–15% to reduce microcirculatorysludging.Blood cardioplegia is formulated using oxy-
genated blood from the CPB circuit. The amount ofoxygen delivered to themyocardium by a blood car-dioplegia solution is only a fraction of the solution’stotal oxygen content. The fraction of total oxygencontent available for delivery is dependent on thesolution’s temperature and the hematocrit. Thelower the temperature and the higher the hemat-ocrit, the less oxygen will be available for deliveryto the myocardium. The hypothermia-induced left-ward shift of the oxyhemoglobin dissociation curveincreases hemoglobin’s affinity for oxygen anddecreases oxygen availability to the myocardium.The delivery of oxygen carried in the dissolved stateis unaffected by changes in hemoglobin’s affinityfor oxygen. For this reason, solutions with highhematocrit, in which the quantity of oxygen carrieddissolved in plasma is reduced, will have a reducedoxygen-delivery capacity at low temperatures.Crystalloid cardioplegia is not routinely oxy-
genated. Oxygenation of crystalloid solutions isaccomplished easily by bubbling gas into the solu-tion before delivery. Aeration of a bicarbonate con-taining crystalloid cardioplegia solution with 100%oxygen drives off carbon dioxide and results insevere alkalosis. For this reason, aeration with a95–98% oxygen and 2–5% carbon dioxide mixtureis recommended. An increase in the total oxygencontent of a crystalloid solution occurswith decreas-ing temperature due to the enhanced solubility ofoxygen in crystalloid at low temperatures. Crystal-loid cardioplegia solutions are capable of delivering

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 416 — #8
416 Chapter 12
Table 12.2 Advantages of blood cardioplegia.
Improved capillary perfusion due to the presence of red cells
More homogenous delivery of blood cardioplegia in the
presence and absence of coronary stenoses
Improved buffering due to the presence of the histidine
buffering system present in red cells
Reduced myocardial edema due to the oncotic tension of
blood
Reduced risk of calcium paradox and improved functional
recovery after ischemia due to the physiologic calcium
concentration provided by blood
Presence of red cell enzyme catalase to scavenge free radicals
produced by ischemia
their entire oxygen content to the myocardiumbecause all oxygen is carried in the dissolved state.Therefore, as the temperature of a crystalloid cardio-plegia solution decreases, the quantity of oxygen itdelivers to the myocardium increases.Blood cardioplegia solutions offer several poten-
tial advantages over crystalloid solutions (Table 12.2).Whether these differences between blood and crys-talloid cardioplegia solutions offer any clear clinicaladvantage remains less clear. There is an exten-sive literature in both animals and humans onthis topic. Meta-analysis of randomized clinical tri-als for all types of cardiac surgery demonstratesthat blood cardioplegia is associated with fewerepisodes of post-bypass low cardiac output syn-dromes, but there is no difference in myocardialinfarction and death. In surgery for coronary arterybypass grafting, there is little to no evidence to sup-port the superiority of cold blood versus cold crys-talloid cardioplegia. Oxygenated blood cardioplegiasolutions provide better preservation of myocardialhigh-energy phosphate stores, myocardial architec-ture, and function than nonoxygenated crystalloidcardioplegia solutions in animals. Likewise, ani-mal work demonstrates that oxygenated crystalloidcardioplegia provides better myocardial preserva-tion than nonoxygenated crystalloid cardioplegia.When differences in calcium concentration are con-trolled, oxygenated blood cardioplegia and oxy-genated crystalloid cardioplegia provide comparabledegrees of left ventricular functional recovery andATP preservation.
Comparison of blood and crystalloid cardiople-gia solutions remains challenging. Review of theliterature demonstrates a lack of controlled, ran-domized trials, marked differences in the compo-sitions, delivery, and temperatures of the varioussolutions, and wide variation in patient populationsand end-points. Despite these obstacles, there isgeneral agreement in the surgical community thatfor patients with preserved left-ventricular func-tion undergoing coronary artery bypass surgery,intermittent delivery of oxygenated blood cardio-plegia solution is at least equal or superior tointermittent delivery of nonoxygenated crystalloidcardioplegia solution. In patients with compromisedpreoperative left-ventricular function, oxygenatedblood cardioplegia provides superior preservation ofpostoperative left-ventricular function.
Adjuvant agentsThere is almost an infinite number of adjuvantagents added to cardioplegia solutions in clinicalpractice. In addition to the essential componentsdescribed above, there are a number of adjuvantagents that can be added to cardioplegia. Many ofthe agents have been well tested in in vitro and ani-mal experiments, yet lack rigorous clinical scrutiny.These adjuvant agents are added to cardioplegia fordifferent reasons, but usually are employed to pre-servemyocardial function and diminish reperfusioninjury. Some of these agents include calcium chan-nel blockers, allopurinol, free radical scavengers,and adenine nucleotides.Loss of calcium homeostasis is a major factor
in causing ischemia-induced myocardial damage.The addition of calcium channel blockers in car-dioplegia solutions may prevent calcium influxand subsequent high-energy phosphate hydroly-sis during cardioplegic arrest by preventing calciuminflux during reperfusion. Animal studies havedemonstrated improved preservation of myocar-dial function with the addition of calcium channelblockers to crystalloid and blood cardioplegia solu-tions. The evaluation of calcium channel block-ers in cardioplegia is more difficult. There arereports of benefit; however, study differences inthe composition of cardioplegia solutions, in thedosages of calcium channel blockers added to

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 417 — #9
Myocardial Preservation 417
the cardioplegia solutions, in the operative proce-dures, and in the extent of preoperative ventricu-lar dysfunction make it difficult to draw any firmconclusions about the efficacy of calcium chan-nel blockers added to cardioplegia solutions. Theissue of whether their routine use is justified isunresolved, but the data suggest that their addi-tion will be of greatest value in patients at highestrisk for calcium-induced ischemic damage. The ben-efits of calcium channel blockers in cardioplegia arebalanced against associated negative inotropy andatrioventricular (AV) nodal dysfunction.Allopurinol is a competitive inhibitor of xanthine
oxidase; whereas, its chief metabolite, alloxanthine,is a noncompetitive inhibitor. Xanthine oxidaseis an important enzyme in the generation of thefree radicals implicated in causing myocardial dam-age upon reperfusion of the ischemic myocardium.Allopurinol added to cold blood and crystalloid car-dioplegia improves myocardial protection in theseverely ischemic animal ventricle.An alternative to inhibition of free radical pro-
duction is supplementation with agents capableof scavenging free radicals. Animal studies havedemonstrated improved myocardial protection inthe ischemic myocardium after use of crystalloidcardioplegic supplemented with the free radicalscavengers superoxide dismutase (SOD), catalase,deferoxamine, and mannitol.Myocardial ischemia promotes production of
adenosine. Adenosine added to cardioplegia mit-igates postischemic ventricular function in ani-mals. Acadesine, a purine nucleoside analog,raises adenosine levels in ischemic myocardium.Acadesine selectively augments adenosine produc-tion in ischemic myocardium without increasingproduction in nonischemic myocardium. Althoughthe mechanism of action is unclear, the action ofacadesine seems to be mediated through adeno-sine A1- and A2-receptors and may act throughactivation of the ATP-sensitive potassium chan-nel. Acadesine added to cold cardioplegia improvespostischemic ventricular function in animalmodels.
Cardioplegia and reperfusion injuryReperfusion injury is defined as the functional,metabolic, and structural alterations caused by
reperfusion after a period of temporary ischemia.Cardioplegia solutions can protect the heart duringthe ischemic insult and reduce reperfusion injury.Reperfusion injury is characterized by intracellu-lar calcium accumulation, cellular swelling, micro-circulatory dysfunction, and reduced ventricularcompliance. Reperfusion solutions are infused intothe myocardium after completion of the surgicalprocedure and before removal of the aortic cross-clamp. They are formulated to prevent or minimizethe reperfusion injury that accompanies reperfusionof the heart with systemic blood.Restorative cardioplegia to reduce reperfusion
injury improves ventricular function after aorticcross-clamping. As with cardioplegia, there arein vitro and animal data to support its use. Controlledclinical trials are more difficult to conduct. Dif-ferences in the composition, temperature, deliveryof the solutions used, and in the operative proce-dures performed, make it difficult to draw any firmconclusions regarding the efficacy of reperfusionsolutions in humans.Despite this, there is support for use of reper-
fusion solutions in patients with preexisting, poorventricular function and in those who require longcross-clamp times.Resuscitation of ischemic myocardium can be
accomplished through warm induction of cardio-plegic arrest. The goal is to resuscitate ischemic areaswhile optimizing preservation of the nonischemicareas. Warm induction of cardioplegic arrest afteraortic cross-clamping combined with rapid ventric-ular decompression on CPB improves repletion ofmyocardial energy stores and improves myocardialrecovery after an acute ischemic event in patientswith ventricular hypertrophy. Table 12.3 lists theideal qualities present in restorative cardioplegia toreduce reperfusion injury.Many of the same concerns for cardioplegia
solutions are present for reperfusion solutions.For reperfusion solutions, sufficient potassium tomaintain arrest in diastole is required. This isaccomplished clinically using 8–10mEq/L in ablood medium. For warm induction solutions,25mEq/L of potassium in a blood medium isrequired. Hypothermia delays the repair of dam-aged enzyme systems because the repair process

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 418 — #10
418 Chapter 12
Table 12.3 Restorative cardioplegia to reducereperfusion injury.
Maintain arrest of the heart in diastole to reducemyocardial oxygen consumptionInduce normothermia to optimize the rate of metabolicrecoveryInitiate aerobic metabolism with an oxygenated solutionProvide buffering to counteract acidosis and optimizeenzymatic and metabolic recoveryProvide increased osmolarity to minimize reperfusionedemaProvide sufficient substrate to allow aerobic energyproductionTemporarily reduce calcium ion availabilityProvide substrate to scavenge free radicals
is temperature-dependent. Clinically, use of a nor-mothermic (37C) reperfusion solution improvesfunctional recovery.Glutamate and aspartate are amino acids that
serve to replenish Kreb’s cycle intermediates thatare depleted during ischemia and which enhanceaerobic metabolism and reparative processes.Reperfusion and warm induction with a mono-sodium L-glutamate (MSG) and monosodiumL-aspartate (MSA) containing solution results in thereturn of oxidative metabolism, enhanced oxygenuptake, improved ATP repletion, and better preser-vation of systolic function after ischemic insult.The addition of L-arginine to cardioplegia results inreduced biomarkers of injury in patients. Themech-anism of action may be due to increased nitric oxideproduction.As previously discussed in detail, maintenance
of temperature-appropriate pH is essential toongoing cellular metabolic processes. Because aci-dosis accompanies ischemia, any reperfusion solu-tion must counteract acidosis and normalize pH.TRAM is often employed as a buffer in bloodreperfusion solutions. Additional buffering capac-ity is available in the form of histidine when ablood reperfusate is used. The glutamic acid-sodiumhydroxide buffer system has been used with clinicalsuccess in crystalloid reperfusate.Similar to cardioplegia solutions used to pre-
vent ischemia, reperfusion solutions must prevent
progression of the edema that accompaniesischemia. Maintenance of an osmolarity of360mOsm/L and avoidance of perfusion pressures>60mmHg are effective in this regard. Becauseloss of calcium homeostasis is the major determi-nant of reperfusion injury, careful control of cal-cium concentration in the reperfusate is essential.The optimal concentration of calcium in reper-fusate is unknown, but concentrations in the rangeof 0.15–0.25mmol/L are common. Clinically, thedesired calcium concentration in a blood reperfusateis obtained by using CPD to chelate excess calciumbefore its administration.Free radical damage occurs with reperfusion of
ischemic myocardium with an oxygen-containingsolution. Modification of the reperfusate withthe free radical scavengers superoxide dismutase,catalase, and mannitol is common.There are other reperfusion strategies that may
offer clinical benefit. Graded reoxygenation andreperfusion is associated with diminished injury inexperimental models. Neutrophil depletion reducesboth the clinical and biochemical indices of myocar-dial reperfusion injury after elective coronaryrevascularization with CPB. Sevoflurane reducesneutrophil activity when included in the cardiople-gia solution. N-acetylcysteine, which can increaseglutathione levels, reduces the rise in troponin-Iwhen added to cold blood cardioplegia. Esmolol iseffective when added to cold continuous retrogradeblood cardioplegia. Fructose-1,6-diphospate, anendogenous high-energy gylcolytic pathway inter-mediary, enhances ATP production and reducesthe biochemical markers of injury when added tocardioplegia. Finally, ischemic preconditioning hasbeen found to be beneficial in myocardial pro-tection during surgery on the beating heart, butoffers no additional protection when employed inconjunction with CPB and aortic cross-clamping.
Cardioplegia deliveryCardioplegia is delivered under pressure to theheart via either a pressurized bag or roller pumpsystem. The roller pump system offers severaladvantages including easy incorporation of a con-tinuous cooling system to maintain cardioplegiahypothermia, easy incorporation of the mixing

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 419 — #11
Myocardial Preservation 419
apparatus necessary for blood cardioplegia systems,and second-to-second control of cardioplegia infu-sion pressure and flow rates. The delivery systemshould have a filter to prevent particular contam-inants from reaching the coronary circulation andinducing coronary vasospasm.It is necessary to have a means of monitoring
infusion pressure because excessive infusion pres-sures can result in myocardial edema and ventricu-lar dysfunction. Infusion pressure is monitored inthe cardioplegia line itself or directly at the siteof administration. Safe delivery pressure will bedictated by the site of administration.During the period of aortic cross-clamping,
cardioplegia should be infused at least every20minutes. This strategy allows washout ofmetabolites and replacement of the cardioplegiasolution components that are either depleted orwashed out by noncoronary collateral flow. Ifelectrocardiograph (ECG) or visual evidence ofmyocardial contraction is present, infusion of car-dioplegia is necessary immediately, regardless of thetime elapsed since the previous infusion. There issome evidence to support continuous administra-tion of cold blood cardioplegia during aortic cross-clamping. One advantage to this approach includessteady-state hypothermia. A significant disadvan-tage is the impediment to the surgeon’s opera-tive field visibility during distal coronary arteryanastomoses.The optimal cardioplegia infusion volume is
unknown. In general, 10–20mL/kg/min of car-dioplegia are delivered during the initial infu-sion with the larger volumes being reservedfor hypertrophied ventricles. Subsequent infusionusually is 10–15mL/kg. With this method, theinfusion site and the safe maximal delivery pres-sure will limit the rate of infusion. Some centersare more concerned with the duration of car-dioplegia delivery than the volume infused andprefer to deliver cardioplegia by controlling infu-sion pressure and delivering cardioplegia over aspecified time interval (i.e. 1.5–3.0minutes forinitial arrest, and 1.0–1.5minutes for subsequentinfusions).After the initial arrest, the composition of
subsequent infusions is modified. After diastolic
arrest with hyperkalemic, hypothermic cardio-plegia, diastolic arrest can be maintained with ahypothermic solution containing a lower potassiumconcentration. Patients receiving cold crystalloidhigh-potassium (20 or 27mEq/L) cardioplegia inboth the initial and subsequent infusions had ahigher incidence of postoperative high-grade ven-tricular ectopy and AV nodal dissociation dysrhyth-mias than patients receiving an initial infusionof cold crystalloid high-potassium cardioplegia fol-lowed by subsequent infusions of cold crystalloidlow-potassium (5 or 7mEq/L) cardioplegia. No dif-ferences in postoperative ventricular function couldbe detected between the two groups in either ofthese studies.Optimal delivery of cardioplegia must be tailored
to the operative procedure and operative tech-nique. Several methods are available for cardiople-gia delivery. Delivery may be via the arterial system(antegrade) or via the venous system (retrograde).
Infusion into the aortic rootThis method is accomplished by placement of acannula into the aorta root between the aorticcross-clamp and the aortic valve and coronary ostia.Placement of a cannula with two lumens, one forcardioplegia delivery and the other for venting orpressure monitoring, is popular and allows mea-surement of aortic root pressure during cardioplegiadelivery (Fig. 12.5). For this method to be effective,the aortic valve must be competent. Otherwise, thecardioplegia solution will flow into the left ventriclewith resultant ventricular distension and inade-quate delivery of cardioplegia down the coronaryarteries.
Infusion into the graftsIn revascularization procedures, cardioplegia can beinfused down the free end of each saphenous veinafter completion of the distal anastomosis. This isusually performed by the surgeon with a syringeconnected to the free end of the coronary graft. Thecardioplegia is highly effective but is limited to thedistribution of the chosen coronary artery. On occa-sion, small air emboli may be injected down thecoronary graft. Typically, this is an incidental find-ing on transesophageal echocardiographic (TEE)

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 420 — #12
420 Chapter 12
Fig. 12.5 Top: Double-lumen catheter used for deliveryof cardioplegia into the aortic root. Lumen connected toa stopcock can be used for venting via aortic root or formeasurement of aortic root pressure. Catheter is placedin aortic root with use of purse-string suture andneedle-tipped stylet shown in place here. After catheterhas been placed in the aorta, the stylet is removed and
the central lumen is used for cardioplegia infusion.Bottom: Hand-held cannula used to directly cannulatecoronary ostia for delivery of cardioplegia solution.(From DiNardo JA. Myocardial preservation.In: DiNardo JA (ed). Anesthesia for Cardiac Surgery,2nd edn. Stamford, CT: Appleton & Lange, 1998:349–64,with permission.)
examination and is without clinical significance(Fig. 12.6).
Infusion directly into the coronary ostiaThis method is used for procedures in which theaortic valve is incompetent and cardioplegia can-not be delivered into the aortic root or for pro-cedures in which the aortic root must be opened(aortic valve replacement). For this method to workeffectively, the surgeon must identify the coronaryostia and cannulate them with specially designedcatheters through which cardioplegia is infused (seeFig. 12.5). The catheters come in a variety of sizesto allow proper placement without damage to theostia. Delivery of cardioplegia with this methodcan be complicated in several ways. The tip of thecatheter may extend past the bifurcation of the leftmain coronary artery such that the catheter mayonly perfuse either the left anterior descending orthe circumflex artery. This is particularly true inpatients with bicuspid aortic valves because the leftmain coronary artery is shorter than normal. In50% of patients, the conus artery to the right ven-tricle (RV) arises separately from the aortic sinusand will not be perfused by cannulation of the rightcoronary ostium. Finally, damage to the ostia withlate stenosis can occur with direct cannulation.For all three of these antegrade delivery
sites, the infusion pressure should not exceed150mmHg.
(a)
(b)
Intramyocardial air
Fig. 12.6 Intramyocardial air is observed in the apicalseptal wall before separation from cardiopulmonarybypass (a). This air may have come from inadvertentinjection of air down a coronary graft duringadministration of cardioplegia. The area was initiallydyskinetic, however, after a short washout interval, theair was absorbed and the wall motion abnormalityresolved (b).

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 421 — #13
Myocardial Preservation 421
Retrograde coronary sinus perfusionRetrograde coronary sinus perfusion (RCSP)infusions cardioplegia into the coronary sinus ret-rograde into the great and small cardiac veins. Thelarge venous network is free of atherosclerotic dis-ease allowing adequate retrograde perfusion of theentire myocardium via this route.This method requires placement of a purse-string
suture in the right atrium (RA) and creation ofa small atriotomy. A specially designed coronarysinus catheter is placed in the coronary sinus bythe surgeon via the atriotomy. TEE is useful toconfirm proper positioning of the coronary sinuscatheter (Fig. 12.7). A balloon at the tip of thecatheter helps secure the catheter and ensuresthat cardioplegia flow does not spill back into theright atrium. Delivery of cardioplegia commencesafter application of the aortic cross-clamp. Most ofthe retrograde perfusion drains via the thebesianveins, but either the aortic root or the left ventricle
(a)
(b)
Coronary sinus
Retrograde coronarysinus catheter in place
Fig. 12.7 The coronary sinus is easily visualized withtransesophageal echocardiography (TEE) (a). Theretrograde coronary sinus catheter is seen in thecoronary sinus (b).
is usually vented during cardioplegia infusion toallow egress of the solution. The coronary sinuscatheter has an additional central lumen allow-ing pressure monitoring during cardioplegia infu-sion. If infusion pressures are too high, there maybe injury to the coronary venous system. Nor-mal retrograde perfusion occurs at a pressure of30–50mmHg.Retrograde cardioplegia is popular for a num-
ber of reasons. The retrograde route of cardioplegiaadministration is particularly useful in aortic valvereplacement thereby avoiding in direct cannula-tion of the coronary ostia. Retrograde perfusion issuperior to aortic root perfusionwhen aortic incom-petence exists. RCSP results in more homogeneousdistribution of cardioplegia than antegrade deliv-ery in animals and humans with coronary stenoses.This may be secondary to the large venous net-work free of atherosclerotic disease. Troponin Irelease is reduced immediately after surgery withretrograde cardioplegia compared to antegrade car-dioplegia (Fig. 12.8). Retrograde perfusion is usefulin reoperative procedures in patients with patentinternal mammary artery (IMA) grafts. Retrogradeperfusion during IMA occlusion will provide car-dioplegia delivery to the myocardium distal to thepatent graft.
8*
*P < 0.056
cTnl
(µg
/L)
4
2
0
Preop. 24 48Time (h)
Group AGroup R
72 Discharge
Fig. 12.8 The time course of troponin I (cTnI)concentration for antegrade and retrograde cardioplegiagroups in a trial of 58 randomized patients undergoingelective coronary artery bypass grafting. *P < 0.05between groups. (From Franke U, Wahlers T, Cohnert TUet al. Retrograde versus antegrade crystalloid cardioplegiain coronary surgery: value of troponin-I measurement.Ann Thorac Surg 2001;71:249–53.)

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 422 — #14
422 Chapter 12
RCSP provides poor protection of the RV and pos-terior septum probably as a result of venovenousshunting through arteriosinusoidal and thebe-sian vessels directly into the RV. As a result,only 30–70% of delivered retrograde cardioplegiareaches myocardial tissue. Interestingly, antegradecardioplegia is also associated with diminished rightventricular protection compared to the left ventri-cle. The reasons for this are unclear; however, itmay be related to uneven distribution of cardiople-gia solution with antegrade delivery or a baselinemetabolic difference between the right and left ven-tricle. To maximize myocardial protection, manyinstitutions utilize both antegrade and retrogradecardioplegia in a single patient.
Myocardial protection agents inaddition to cardioplegiaMyocardial preservation is influenced by factorsother than the efficient delivery of cold cardioplegicsolution. The most important of these factors arediscussed in the sections that follow.
Topical hypothermiaMyocardial oxygen demands drop by 90% in nor-mothermic arrest to 1mL oxygen (O2)/100 g/min.At 22C, oxygen requirements drop to 0.3mL/100 g/min in the arrested heart. Further reductionof oxygen consumption occurs with temperatures<22C; however, the incremental gain is mini-mal. Despite this, many clinicians target 4–6Cfor optimal myocardial preservation. As discussedpreviously, it is difficult to achieve this degree ofhypothermia in clinical practice. It is possible, withthe use of cold cardioplegia solution and topicalsaline slush or ice chips, to achieve and maintaintemperatures lower than 15C. Unfortunately, theuse of saline slush and ice chips has been associatedwith problems. Myocardial damage due to freezinghas been demonstrated in hearts exposed to slush orice for more than 30minutes. Phrenic nerve pare-sis due to freezing has been reported in 60–80% ofcases inwhich slush or ice is used. For these reasons,many centers use either intermittent or continuousinfusions of saline at 4C into the pericardial well toobtain topical cooling.
Control of noncoronary andbronchial collateral blood flowExcessive bronchial collateral blood flow results inwarming of the heart by distending it with blood atthe temperature of the systemic perfusate. Exces-sive noncoronary collateral flow results not onlyin distension and warming of the heart but in thewashout of cardioplegia solutions as well. Systemichypothermia on CPB is effective in reducing warm-ing, but careful control of systemic flow and pres-sure on CPB is necessary to reduce the magnitudeof collateralized flow.
Decompression of the heartDistension of the heart has two deleterious conse-quences: it results in poor distribution of cardiople-gia solution to the subendocardium due to the highintracavitary pressures, and it results in warming ofthe heart due to distension of the heart with bloodat body temperature. For these reasons, venting ofthe heart is usually employed.
Preventing warming of the posteriorsurface of the heartBecause the posterior surface of the heart lies ontop of the mediastinum, which is at systemic tem-perature, it is at high risk of warming during aorticcross-clamping. To prevent this, many surgeonsplace a pad soaked in iced saline behind the heartin the pericardium to shield it from the mediasti-nal structures. This may help prevent mitral valvedysfunction secondary to posterior papillary mus-cle ischemia. The TEE probe emits energy and heatwhenever imaging is in progress. For this reason,imaging should be suspended during this portion ofthe surgical procedure.
Special considerations in neonates,infants, and childrenDespite advances in the surgical correction of con-genital cardiac lesions, postoperative low cardiacoutput leading to long-term ventricular dysfunc-tion or death continues to be a concern. Thishas focused attention on the effectiveness of cur-rent myocardial protection techniques in the repairof congenital heart disease. Most work to dateon myocardial preservation has involved adult

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 423 — #15
Myocardial Preservation 423
humans or adult animal preparations. Unfortu-nately, the existence of major structural, metabolic,and functional differences between infant and adulthearts makes extrapolation of these studies toneonates and infants difficult. These differences aresummarized in the following sections.
Calcium homeostasisNeonatal hearts have a poorly developed sarcoplas-mic reticulum and T-tubule system. In addition,the sarcoplasmic reticulum has reduced calciumstorage capacity and a reduced activity of sarcoplas-mic calcium ATPase, the enzyme responsible forcalcium re-uptake. These differences result in agreater reliance on extracellular calcium to provideexcitation-contraction coupling and are a factor inthe diminished tension development capabilities ofthe neonatal myocardium.
Substrate metabolismIn the adult heart 90% of ATP production is derivedfrom fatty acid oxidation. The main ATP sub-strate in neonatal hearts is glucose. As comparedto adults, the noninsulin-dependent glucose trans-porter (GLU1) is much more highly expressed thanthe insulin-dependent glucose transporter (GLU4).
ATPase activityFetal light-chain myosin has a diminished ability tohydrolyze ATP, which contributes to the diminishedtension-development capability of neonatal hearts.This light-chain myosin remains in patients withcongenital heart disease.
Capacity for anaerobic metabolismThe neonatal heart has an enhanced capacity foranaerobic metabolism compared with the adultheart secondary to its large glycogen stores. For thisreason, the neonatal heart tolerates longer periodsof hypoxia.
Tolerance for ischemiaThe neonatal heart possesses greater tolerancefor ischemia (severely reduced or absent perfu-sion) than adult hearts due to enhanced glyco-gen stores, better maintenance of ischemic cal-cium exchange, higher levels of ATP substrates,
and increased amino acid use. In the absence ofperfusion, the enhanced capacity for anaerobicmetabolism of the immature myocardium leads toa rapid accumulation of the products of anaerobicmetabolism such as lactate. Therefore, prolongedischemia results in severe acidosis and tissue dam-age and in the rapid inhibition of further produc-tion of high-energy phosphates in the neonatalmyocardium. Cyanosis further increases the vul-nerability of the neonatal heart to ischemia. Themyocardium of cyanotic children is more vulnera-ble to cardiac ischemia/reperfusion injury than themyocardium of noncyanotic children presumablydue to depletion of endogenous antioxidant reserve.
Tension developmentIn comparison to the adult heart, the neonatal heartcontains a reduced number of poorly organized con-tractile units. In the immaturemyocardium, a largerproportion of the myocyte is devoted to the proteinsynthetic processes needed for cell growth. In addi-tion to the factors already addressed, this accountsfor the reduced tension development capabilities ofthe neonatal heart. This reduced tension develop-ment capability makes the neonate very susceptibleto any depression of systolic function after cardiacsurgery.Work done both in animals and in humans sug-
gests that improved myocardial preservation can beobtained in neonates, infants, and children by tai-loringmyocardial preservation efforts to the specificneeds of the immature myocardium:• Delivery of cardioplegia to neonates, infants,and small children requires some modifications;20–30mL/kg of cardioplegia may be necessary toinduce arrest. The pressure of antegrade deliverymust be modified such that, in the neonate, infu-sion pressure is nomore than 40–50mmHg to avoidmyocardial edema.• Topical cooling is much more effective in theneonate than in the adult due to the smaller car-diac mass and greater surface area: wall thicknessratio in neonates.• Improved post-ischemic functional recoveryoccurs with use of hypothermic blood potas-sium cardioplegia with a normal serum calciumconcentration.

Alice Nelson Dinardo: “ch12” — 2007/7/16 — 12:41 — page 424 — #16
424 Chapter 12
• Infants younger than 3months of age and infantswith preoperative heart failure have an increasedsusceptibility to ultrastructural myocardial injurydespite the use of cold crystalloid cardioplegia andtopical hypothermia.• Children with ventricular hypertrophy haveincreased vulnerability to ischemia/reperfusioninjury. This is due, at least in part, to reducedmicrovascular (capillary) density and impairedglucose uptake.• There may be difficulty in obtaining adequatemyocardial protection in the presence of volumi-nous bronchial and noncoronary collateral bloodflow. Noncoronary collateral flow will wash outcardioplegia, and that bronchial return will resultin warming of the heart. This collateral bloodflow can be eliminated through the use of circu-latory arrest. In fact, improved recovery of rightventricular function, reduced need for post-CPBinotropic support, and less evidence of myocar-dial necrosis, as indicated by myocardial bandenzymes of creatinine phosphokinase-myocardial
band (CPK-MB) levels, have been demonstrated inpatients undergoing tetralogy of Fallot repair withsystemic deep hypothermic arrest in addition tocardioplegic protection.
Suggested reading
Doenst T, Schlensak C, Beyersdorf F. Cardioplegia in pedi-
atric cardiac surgery: dowe believe inmagic?Ann Thorac
Surg 2003;75:S678–84.Guru V, Omura J, Alghamdi AA, Weisel R, Fremes SE.
Is blood superior to crystalloid cardioplegia? A meta-
analysis of randomized clinical trials. Circulation
2006;114(Suppl I):I-331–8.Kevin LG, Novalija E, Stowe DF. Reactive oxygen
species as mediators of cardiac injury and protec-
tion: the relevance to anesthesia practice. Anesth Analg
2005;101:1275–87.Ovrum E, Tangen G, Tollofsrud S et al. Cold blood cardio-
plegia versus cold crystalloid cardioplegia: a prospective
randomized study of 1440 patients undergoing coro-
nary artery bypass grafting. J Thorac Cardiovasc Surg
2004;128:860–5.

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 425 — #1
CHAPTER 13
Special Considerations duringCardiac Surgery
This chapter will address topics that require specialconsideration during the conduct of cardiac surgery.
Deep hypothermic circulatoryarrest
Deep hypothermic circulatory arrest (DHCA) is atechnique employed to improve exposure of intrac-ardiac defects and to facilitate aortic arch recon-struction in infants and children. In adults, DHCAis used primarily during aortic arch reconstructions.DHCA allows cessation of cardiopulmonary bypass(CPB), venous and arterial cannula removal, andexsanguination of the patient into the venous reser-voir of the CPB circuit. There has been substantialrefinement of the technique of DHCA since its suc-cessful inception in the 1970s. Currently DHCA isused selectively and for short intervals.Determination of the safe period of DHCA
is problematic because it varies depending onthe defined primary acceptable outcome as wellas on independent variables such as patientpopulation (infant versus adult), co-morbidities(cerebrovascular, renal, genetic), and DHCA tech-nique (pH management, hematocrit management).In neonates and infants, DHCA intervals generallydo not exceed 60minutes as DHCA intervals longerthan 40minutes are associated with a nonlinearincreasing likelihood of adverse neurodevelopmen-tal outcomes including seizures. In adults, DHCAintervals of less than 30–40minutes are common.
HypothermiaHypothermia is arguably the most important com-ponent of DHCA. Hypothermia-induced reductionin cerebral metabolic rate for oxygen (CMRO2)slows the rate of depletion of high-energyphosphates and the development of intracellu-lar acidosis. This delays or prevents the neuronalenergy failure that leads to terminal membranedepolarization and subsequent neuronal injuryor death during an ischemic episode. The Q10defines the ratio of organ oxygen consumption ata defined temperature to the oxygen consump-tion at a temperature 10C lower. The cerebralQ10 is approximately 3.65 in children and 2.3in adults. The cerebral metabolic rate is approx-imately 10–15% of its normothermic baseline at15C. If it is assumed that 3–5minutes of cerebralischemia can be tolerated at 37C and the Q10 is 3.0,9–15minutes of ischemia can be tolerated at 27Cand 27–45minutes can be tolerated at 17C.In addition to reducing CMRO2, hypothermia
also serves to ameliorate some of the sequalae ofneuronal ischemia when instituted prior to theischemia insult. Specifically, hypothermiamarkedlyreduces release of the excitatory neurotransmittersglutamate, aspartate, and glycine that accompanycerebral ischemia and subsequent reperfusion. Inenergy deprived cells, glutamate is neurotoxic inpart due to the role it plays in inducing massivecalcium influx via N-methyl-D-aspartate (NMDA)receptors. Hypothermia also blunts the inhibitory
425

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 426 — #2
426 Chapter 13
effect of hypoxia on nitroxidergic (postganglionicparasympathetic nerve where nitric oxide (NO)is the neurotransmitter) induced cerebral vasodi-latation. In addition, hypothermia may attenuateneutrophil migration into ischemic tissue.
pH stat versus α-stat managementpH-stat and α-stat are described in detail inChapter 10. Experimentally pH-stat managementduring DHCA offers several advantages over α-statmanagement:
Suppression of CMRO2
There is better suppression of CMRO2 with pH-statas compared to α-stat management. pH-stat man-agement reduces CMRO2 by 40% over that seenwith α-stat management at 17C.
Brain coolingDuring the cooling phase of deep hypothermia,pH-stat management provides faster and morehomogenous brain cooling than does α-stat man-agement. This is a direct consequence of thedecreased cerebral vascular resistance and increasedcerebral blood flow (CBF) that accompanies pH-statmanagement.
Oxyhemoglobin dissociation curveHypothermia induces a leftward shift of the oxy-hemoglobin dissociation curve such that duringα-stat management at 17C the P50 of fetalhemoglobin is 5.0 as compared to 20.0 at 37C.The increased affinity of hemoglobin for oxygenreduces the ability of hemoglobin to off-load oxygento tissue. As a result, a substantial portion (56–96%)of the oxygen delivered to brain during CPB at17C is obtained from dissolved oxygen making ahigh CBF to CMRO2 ratio necessary. pH-stat man-agement is advantageous in this setting because itresults in increased CBF compared to α-stat man-agement and because the relative acidosis whichaccompanies pH-stat management induces a right-ward shift of the oxyhemoglobin dissociation curvesuch that the P50 of fetal hemoglobin increases to6.9 at 17C improving off-loading of oxgyen fromhemoglobin to the brain.
Aortopulmonary collateralsThe presence of numerous and often large collat-eral vessels from the arch vessels and thoracic aortato the pulmonary arterial system is common inneonates, infants, and children with atretic pul-monary arterial systems. The number and size ofthese vessels increase in proportion to the dura-tion of cyanosis. On CPB, with α-stat managementthe resulting alkalosis reduces pulmonary vascu-lar resistance and increases cerebral vascular resis-tance such that these vessels divert blood fromthe cerebral circulation to the pulmonary circula-tion. As a result, pH-stat management results inbetter cerebral protection than α-stat managementwhen circulatory arrest is induced in the presenceof aortopulmonary collaterals (APCs).
Cerebral oxygenationpH-stat management increases pre-DHCA corti-cal oxygen saturation (ScO2) and increases thehalf-life of arrest ScO2 as compared to α-statmanagement. pH-stat management also providesbetter preservation of intracellular pH and betterpreservation of cerebral energy stores (high-energyphosphates) and tissue oxygenation (nicotinamideadenine dinucleotide (NADH), cytochrome aa3).A strategy of pH-stat management during coolingand arrest coupled with pH-stat management dur-ing rewarming results in better recovery of cerebralenergy stores and intracellular pH than a strategy ofpH-stat management during cooling and arrest cou-pled with α-management during rewarming. Theseeffects are largely mediated through reduction ofCMRO2 during arrest and increased cerebral oxygendelivery during the cooling phase prior to arrest andduring the reperfusion and rewarming phase afterarrest.
HematocritIt has long been assumed that hemodilution is anessential component of DHCA because hemodi-lution offsets the viscosity and rheologic changesthat can compromise microcirculatory flow dur-ing low temperature CPB. Recent laboratory stud-ies demonstrate that a hematocrit of 30% doesnot impair cerebral microcirculation during orafter DHCA. Furthermore, a hematocrit of 10%

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 427 — #3
Special Considerations 427
severely compromises cerebral oxygen deliveryduring cooling prior to DHCA. In addition, a higherhematocrit (30% compared to 20% or 10%) dur-ing cooling and at the onset of DHCA extends theinterval of DHCA that can be tolerated withoutneurologic injury.
Arterial oxygen partial pressure (Pao2)management during CPB for DHCANormoxic reperfusion is superior to hyperoxicreperfusion in mitigating free radical-induced neu-ronal injury following neuronal ischemia. Hyper-oxic CPB and DHCA results in more free radicaldamage than normoxic CPB and DHCA. However,this damage is offset by the more severe hypoxicneuronal damage that accompanies normoxic CPBand DHCA. This is likely due to the fact that themajority of the brain’s oxygen requirements duringDHCA are met by dissolved oxygen. Hyperoxic CPBclearly increases the amount of dissolved oxygenavailable to the brain.
Conduct of DHCACooling for DHCA involves both surface and corecooling. Surface cooling in neonates and infantssurface is very effective and is initiated once sur-gical preparation begins. In adults, surface coolingis generally less effective given their smaller surfacearea toweight ratio. Surface cooling is accomplishedusing unwarmed intravenous fluids, unhumidifiedgases, reducing the room temperature to 10–12C,setting the heating/cooling blanket to 4–5C, andpacking the patient’s head in ice. These techniquesallow the patient to be cooled to 30–32C beforebeginning CPB and core cooling. Surface coolingrequires close observation of the progression of theoperative procedure as premature cooling can pre-dispose to dysrhythmias (bradycardia, ventricularirritability) and hypotension.The most effective method of cooling for DHCA is
core cooling on CPB. A vasodilator such as sodiumnitroprusside or phentolamine (0.2mg/kg) may beadministered into the CPB circuit as core cool-ing commences to promote vasodilation and morehomogenous cooling. A vasodilator may also beused before core rewarming. Methylprednisolone(30mg/kg in infants and neonates, 1 g in adults),
magnesium sulfate, lidocaine, and mannitol areoften added to the CPB prime. The minimumhematocrit during cooling, arrest, and rewarmingis unknown, however many believe it should be>25%. Based on clinical trial data, many centersaim for a hematocrit of 30% during these inter-vals in neomates and infanta. Anesthetic agents(synthetic opioid and benzodiazepine) and amusclerelaxant are administered prior to DHCA to min-imize oxygen consumption during cooling andarrest.Ideally, DHCA should commence when the elec-
troencephalogram (EEG) is isoelectric and CMRO2is minimal. In adults, it is necessary to obtain anasopharyngeal temperature of 12–18C or to havecooled the patient on CPB for more than 50minutesto obtain this goal. In neonates and infants this isgenerally accomplishedwith 15–20minutes of cool-ing and a tympanic membrane temperature<15C.At this point the rectal temperature is invariably<18C. Longer intervals of core cooling shouldbe used for children with extensive systemic topulmonary artery collaterals.pH-statmanagement is generally used in pediatric
patients while α-stat management is more com-monly used in adults. pH-stat management is usedonce patient tympanic membrane temperature isbelow 30C during both cooling and rewarming.Four different mixtures of oxygen/carbon dioxidefor use as the sweep gas in the membrane oxygena-tor are available: 97% oxygen/3% carbon dioxide,96% oxygen/4% carbon dioxide, 95% oxygen/5%carbon dioxide, and 94% oxygen/6% carbon diox-ide. The use of carbon dioxide in the membraneoxygenator sweep gas is summarized in Table 13.1.In smaller infants and in patients with extensive
APCs the next higher mixture of oxygen/carbondioxide than normally indicated is utilized. When
Table 13.1 The use of carbon dioxide (CO2) in themembrane oxygenator sweep gas.
Patient temperature (C) % O2/CO2
30–28 97/328–22 96/422–15 95/5

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 428 — #4
428 Chapter 13
CPB commences the perfusate is at 30C havingbeen previously recirculated with the chosenoxygen/carbon dioxide mixture.Target brain temperature at the end of rewarm-
ing on CPB is 35–36C. Slow core rewarming willallow this target temperature to be reached withoutinducing cerebral hyperthermia as it is detrimen-tal to neurological outcome following DHCA. Atno point in the rewarming process should rectal,esophageal, or tympanic membrane temperaturesexceed target brain temperature if cerebral hyper-thermia is to be avoided. Slow core rewarming alsoameliorates temperature afterdrop following termi-nation of CPB by promoting more homogenoussomatic rewarming.
Alternatives to DHCAIn an effort to prevent the potentially deleteriouseffects of DHCA on cerebral perfusion and oxygena-tion, efforts have been directed toward technicalinnovations to avoid the use of DHCA. Currentlyboth antegrade cerebral perfusion (ACP) and retro-grade cerebral perfusion (RCP) are used clinically.Whether these techniques can reliably extend theperiod of safe DHCA remains to be determined.
Antegrade cerebral perfusionArterial CPB circuit flow can be delivered selectivelyto the cerebral circulation antegrade via the circleof Willis following cannulation of the innominateartery or right carotid artery. With this technique,the arch vessels are snared and the descendingaorta is cross-clamped to provide a bloodless oper-ative field (Fig. 13.1). In neonates and infants, ACPis commonly called regional low flow perfusion(RLFP). The technique is similar to that used inadults except that a graft may be placed on theinnominate artery to provide access for the can-nula. This graft can then be used as a modifiedBlalock–Taussig shunt (innominate artery to rightpulmonary artery).The optimal flow rates, delivery pressure,
temperature, and acid-base balance (pH-stat orα-stat) of the selective cerebral perfusate haveyet to be determined. Cerebral overperfusion isa potential risk with this technique. In adults,flow rates of 200–250mL/min at a temperature
Arterial cannula
Atrial bloodscavenger
Fig. 13.1 Schematic of the operative field during theascending aorta and aortic arch reconstruction portion ofhypoplastic left heart syndrome repair utilizing antegradecerebral perfusion (regional low flow perfusion). Cerebralblood flow is supplied by an arterial cannula from thecardiopulmonary bypass (CPB) circuit placed in the distalportion of a graft anastomosed to the innominate artery.The proximal portions of the innominate artery, leftcarotid artery, and left subclavian artery are snared andthe descending aorta is cross-clamped to provide abloodless operative field. The graft will later be used tocreate a modified Blalock–Taussig shunt (innominateartery to right pulmonary artery). (From Pigula FA. Archreconstruction without circulatory arrest: Scientific basisfor continued use and application to patients with archanomalies. Semin Thorac Cardiovasc Surg Pediatr Card SurgAnnu 2002;5:105, with permission.)
of 8–12C with α-stat management are generallyutilized. In neonates and infants, flow rates of40–80mL/kg/min at a temperature of 15–22CwithpH-stat management are generally utilized.
Retrograde cerebral perfusionArterial CPB circuit flow can be delivered selectivelyto the cerebral circulation retrograde via the cere-bral venous system. The superior vena cava (SVC) iscannulated with proximal snaring of the SVC belowthe azygous vein and above the right atrium. Arte-rial output from the CPB circuit is directed to thiscannula to provide retrograde cerebral perfusion via

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 429 — #5
Special Considerations 429
the SVC and azygous venous system. The descend-ing aorta is cross-clamped but the arch vessels mustbe left open to atmosphere to provide low-pressurearterial drainage. RCP provides some cerebral per-fusion, helps tomaintain cerebral hypothermia, andwashes debris out of the arterial system. In order toprevent run-off of blood from the cerebral venouscirculation into the lower body venous circulationduring RCP it is necessary to maintain lower bodyvenous pressure. This is accomplished with partialrather than complete exsanguination of the patientvia the venous cannula following DHCA and priorto RCP.The optimal flow rates, delivery pressure, temper-
ature, and acid-base balance (pH-stat or α-stat) ofthe selective cerebral perfusate have yet to be deter-mined. Cerebral edema is a potential risk with thistechnique. In adults, flow rates of 200–300mL/minat a temperature of 8–12Cwith α-statmanagementat a pressure of 25mmHg are generally utilized.
Adjuncts to DHCAIn an effort to mitigate the neuronal damage thataccompanies the use of DHCA a number of adjuncttherapies have been investigated.
ThiopentalBarbiturates offer no protection from global anoxia,which is the primary insult induced by DHCA.Barbiturates administered in associationwithDHCA(approximately 1.0 g in adults) do offer enhancedcerebral metabolic suppression in the setting ofincomplete brain cooling and amelioration of injuryinduced by cerebral air emboli during rewarming(focal ischemic event). Barbiturates administeredduring cooling for DHCA are potentially deleteri-ous because they reduce cerebral blood (the primarymechanism of brain cooling) and prevent cooling-induced accumulation of high-energy phosphatestores and increased intracellular pH. Due to a lackof good clinical data, no clear consensus exists as tothe utility of barbiturates in ameliorating neuronalinjury associated with DHCA.
SteroidsThe role of steroids in mitigating neuronal damagefollowing DHCA is unclear. Studies to date have not
demonstrated clear benefit. However, it has beensuggested that administration several hours priorto initiation of DHCA is of more benefitial thanadministration in the CPB pump prime.
Investigational agentsSeveral agents including inhalational anesthetics(particularly desflurane), inhibitors of oxygen freeradical generation such as allopurinol and leuko-depleted blood are currently being investigated asagents to mitigate neurologic injury associated withDHCA.
Hematocrit on CPB andtransfusion of blood products
The issues surrounding transfusion of red cell andblood component therapy in adult cardiac surgi-cal patients is complex and has received a greatdeal of attention in the last several years. Both lowhematocrit on CPB and perioperative transfusion totreat low hematocrit have been implicated in thefull range of adverse outcomes following cardiacsurgery. Analysis of this relationship is hamperedby the fact that most of the data are drawn fromobservational studies rather than from controlledrandomized trials and by the relative heterogeneityof the study groups compared. Neither the mini-mal allowable hematocrit on CPB nor the relativerisk/benefit of perioperative transfusion to treat lowhematocrit are clearly defined.The risks associated with a reduced hematocrit on
CPB can be summarized as follows:• Renal dysfunction. CPB hemodilution to a thresh-old hematocrit ranging from <21% to <26% isassociated with increased likelihood of postopera-tive renal dysfunction including acute renal fail-ure and the requirement for renal replacementtherapy (dialysis). This decrease in renal func-tion is also associated with increased operativemortality and hospital stay. An oxygen delivery<272mL/min/m2 in conjunctionwith CPB hemod-ilution is associated with postoperative acute renalfailure.• Neurologic dysfunction. Nadir hematocrit on CPBis an independent predictor of perioperative strokewith each 1% decrease in hematocrit below 29%

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 430 — #6
430 Chapter 13
associated with a 10% increase in the odds ofsuffering a perioperative stroke.• Poor overall outcome. Lowest hematocrit on CPBis associated with increased mortality, intra-aorticballoon pump placement, intensive care unit (ICU)and hospital stay, return to CPB and worse 0–6 yearsurvival.The risks associated with perioperative transfu-
sion of packed red blood cells (PRBC) and otherblood products are summarized as follows:• Infectious complications. Perioperative transfusionof PRBC in patients undergoing cardiac surgeryis associated with an increased risk of septicemiaand bacteremia, superficial and deep wound infec-tions, and nosocomial pneumonia. Transfusion ofother blood products such as platelets, fresh frozenplasma, and cryoprecipitate may also increase therisk of infectious complications.• Poor overall outcome. Perioperative transfusion ofPRBC in patients undergoing cardiac surgery isassociated with an increased risk of postoperativemorbidity from all causes (cardiac, renal, neuro-logic, respiratory, and infectious). Each unit ofPRBC transfused incrementally increases the riskof an adverse outcome. In addition, periopera-tive transfusion of PRBC is associated with reduc-tions in short-term survival, long-term survival(5–10 years), and quality of life. There is conflict-ing evidence as to whether platelet transfusions areassociated with adverse clinical outcomes.It is unclear whether use of leukoreduced or
leukodepleted blood products mitigates the risk ofperioperative blood transfusion. Likewise, there isconflicting evidence as towhether the age of bankedtransfused PRBC contributes to the risk of trans-fusion. The most prudent course is to avoid a lowhematocrit on CPB and to limit perioperative trans-fusion of blood products whenever possible. Thisrequires a multi-modal approach using some or allof the techniques outlined in Table 13.2.
Neurologic outcome followingcardiac surgery
Neurologic complications following adult cardiacsurgery include stroke, encephalopathy, and cog-nitive dysfunction. Stroke occurs in approximately
Table 13.2 Interventions to limit blood producttransfusion in cardiac surgery.
Prevent and treat preoperative anemia• Limit preoperative blood drawing for testing• Appropriate interval between preoperative autologousblood donation and elective surgery• Recombinant human erythropoietin (EPO) andsupplemental iron administration more than 1week priorto surgery
Pharmacological interventions to limit perioperativeblood loss• Antifibrinolytic agents:a Aprotininb Lysine analogues (tranexamic acid, ε-aminocaproic acid)
• Desmopressin (DDAVP, 1-deamino-8-D-argininevasopressin)• Recombinant factor VIIa (rFVIIa)
Intraoperative salvage of blood• Use of cell saver during re-operative procedures• Salvage and transfusion of CPB circuit volume followingtermination of CPB
Hemoconcentration on CPB• Continuous ultrafiltration (CUF)• Modified ultrafiltration (MUF)
Reduce CPB circuit prime volume• Use of smallest possible tubing length/diameter• Use of smallest possible venous reservoir/oxygenatorsystem• Retrograde autologous priming (RAP)
Point of care testing (POCT) to identify coagulationdefects• ACT• Protamine titration• Thromboelastography (TEG)• Platelet count, fibrinogen level, PT, aPTT
ACT, activated clotting time; aPTT, activated partialthromboplastin time; CPB, cardiopulmonary bypass;PT, prothrombin time.
1–3% of patients while postoperative cognitive dys-function is far more common affecting upwardsof 30–65% of patients at 1month and 20–40% ofpatients at 6months. The etiology of these neu-rologic complications is complex and involves the

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 431 — #7
Special Considerations 431
interplay of several variables including cerebralemboli, global cerebral hypoperfusion, systemicinflammatory response, and genetic predisposition.The fact that the incidence of cognitive dysfunc-tion and stroke following off-pump coronary arterybypass graft surgery (CABG) and on-pump CABG isnot significantly different emphasizes the complex,multi-factorial nature of this problem.
Cerebral emboliBoth micro- and macroemboli are delivered tothe brain during CPB despite the use of arte-rial and venous filters. There is concern thatthe increased CBF associated with pH-stat man-agement can contribute to neurologic morbid-ity by increasing the embolic load to the brainand by inducing intra-cerebral steal of bloodflow. This contention is unproven; nonetheless,α-stat management remains the standard duringadult CPB.Particulate macroemboli are generally com-
posed of atheromatous or calcific debris from theaorta, cardiac valves, or great vessels. Microembolican be gaseous or particulate. Particulate micro-emboli arise primarily from fat, marrow, bone wax,and other material in the pericardial well that areaspirated into the CPB circuit via cardiotomy suc-tion. Gaseous microemboli arise from air that isintroduced directly into the heart during open car-diac chamber procedures or from air introducedinto the CPB circuit. Perfusionist interventions,specifically injection of drugs (and air) into thevenous reservoir, and entrainment of air aroundthe venous cannula introduce air into the venousreservoir that can transit the oxygenator and arte-rial line filter to reach the arterial circulation asmicroemboli.Cerebral emboli are associated with neurocogni-
tive deficits and stroke following cardiac surgery.The number of cerebral microemboli (microembolicload) delivered during CPB is related to the develop-ment of cognitive dysfunction occurring followingCABG surgery. However, similar degrees of cogni-tive dysfunction occur following CABG and cardiacvalve surgery despite the fact that the cerebralgaseous microembolic load is higher during valvesurgery. This suggests that the type of cerebral
microemboli may be a more important factor thanthe number of microemboli in the development ofcognitive dysfunction. Lipid microemboli, such asthose generated with use of cardiotomy suction,are particularly damaging to the cerebral microvas-cular endothelium and probably play a signifi-cant role in the genesis of microembolic cognitivedysfunction. Cerebral macroembolic load, as mea-sured by the extent of aortic atheromatous disease(atheromatous burden), is associated with strokefollowing cardiac surgery. The role of macroemboliin the genesis of cognitive dysfunction is less clear.
Methods to reduce microemboliA number of modifications to the CPB circuitry andsurgical technique have been utilized to reduce par-ticulate and gaseousmicroemboli. They are summa-rized below. Although none of these modificationshas been conclusively shown to be of benefit inreducing neurocognitive deficits, each reduces thenumber of emboli detected by echocardiography ortranscranial Doppler.• Reduce perfusionist interventions and surgicalfield venous line manipulations to a minimum. Theperfusionist should carefully remove air from allsyringes prior to drug or flush administration. Hardshell venous reservoirs allow air to rise to the toppossibly reducing the number of venous air embolithat reach the arterial circulation as compared tosoft shell venous reservoirs.• Diversion of cardiotomy suction to cell-saver ordiscarding cardiotomy suction to avoid contam-ination of the venous reservoir with particulatemicroemboli.• Use of a gas diffuser to insufflate carbon dioxideinto the surgical wound to displace air with moresoluble and more easily absorbed carbon dioxideduring open chamber procedures.
Methods to reduce macroemboliEfforts to reduce macroemboli employ strategies toreduce dislodgement of atherosclerotic debris fromthe ascending aorta. These strategies as applied toCABG are summarized:• Use of epiaortic ultrasonic scanning to identifyaortic cannulation and aorticmanipulation sites freeof atheromata.

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 432 — #8
432 Chapter 13
• Use of “no-touch technique” where the proxi-mal ends of saphenous vein or radial artery graftsare “Y-ed” off an internal mammary artery graft toavoid a partial occluding (site-biting) clamp on theaorta.• Use of “single cross-clamp technique” whereproximal aortic graft anastomoses are constructedafter the aortic cross-clamp is placed without useof partial occluding (site-biting) clamp on theaorta.• Cannulation of the axillary artery, innominateartery or the distal aortic arch when atheromatousdisease of the ascending aorta is severe and dif-fuse. Alternatively, DHCA can be used to replacethe ascending aorta.• Use of an aortic cannula with a deployable intra-aortic 120-µ filter to capture particulate emboli“sandblasted” or dislodged from the aorta byturbulent flow from the aortic cannula.• Use of a longer aortic cannula to reduce turbu-lence in the aorta and potentially reduce creation ofmicroemboli.• Use of off-CPB technique in combination witha “no-touch technique”.Use of these strategies show promise in reduc-ing stroke and cognitive dysfunction. It remainsto be determined whether off-pump CABG per seresults in better neurologic outcome as comparedto on-pump CABG when appropriate measures todeal with an atheromatous aorta are utilized witheach approach.
Cerebral hypoperfusionGiven what is known about cerebral autoregula-tion in adults, a mean arterial pressure (MAP)≥50mmHg on CPB is commonly targeted. Clearevidence supporting this target MAP during CPBis lacking however. There is no consistent linkbetween a MAP < 50mmHg on CPB per se andsubsequent neurologic dysfunction. The combina-tion of reduced MAP (<50–60mmHg) on CPB anda large burden of aortic atheromata may increasethe risk of CPB related stroke. Cerebral injuryinduced bymacroemboli is presumably exacerbatedby the reduced collateral perfusion accompanyinghypotension. The neurologic sequalae of a reducedMAP during CPB in patients with cerebrovascular
disease or with impaired cerebral autoregulation(elderly patients, hypertensive patients, diabetics,patients with prior strokes) has not been system-atically investigated. Given the currently availabledata, maintenance of MAP ≥ 50mmHg on CPB isreasonable and a higher target MAP (70–90mmHg)is indicated for patients at high risk for neurologicdysfunction.
Pharmacologic interventions toimprove neurologic outcomeA wide range of pharmacologic agents has under-gone investigation as neuroprotective agents inadults undergoing cardiac surgery. To date, lido-caine, remaceamide (an NMDA antagonist), andaprotinin have shown the most promise. In retro-spective analyses, high-dose aprotinin use has beenassociated with a reduced incidence of neurocog-nitive deficits and stroke following cardiac surgery.These conclusions require verification in placebo-controlled, randomized trials. The mechanism ofaprotinin’s neuroprotective effect is unknown. Itmay be due to its anti-inflammatory properties orto an associated reduction in cerebral microem-boli as the result of the reduced use of cardiotomysuction and platelet transfusions. Lidocaine blocksvoltage-dependent fast sodium channels, reducescerebral metabolic rate, and reduces release of theexcitatory neurotransmitters. Remaceamide blocksthe effects of ischemia induced glutamate release onNMDA channels and thereby prevents the influxof calcium that exacerbates neuronal injury anddeath.
Renal function
Acute renal failure in adults following cardiacsurgery is amajor source ofmorbidity andmortality.The incidence and outcome in children is remark-ably similar to adults. Approximately 13% of adultswith a normal serum creatinine (<1.0µmol/dL)have occult renal insufficiency defined as a crea-tinine clearance <60mL/min. These patients havea risk (odds ratio of 2.8) for postoperative dial-ysis. This is similar to patients with mild renalinsufficiency defined as a serum creatinine between1.0 and 1.33µmol/dL. Creatinine clearance can be

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 433 — #9
Special Considerations 433
calculated using the Cockcroft–Gault equation:
CCR(mL/min)
= [(140 – age)×weight]/(PCR × 72) for men;CCR(mL/min)
= [(140 – age)×weight]/(PCR × 85) for women.Where CCR = creatinine clearance, PCR = serumcreatinine in milligrams/deciliters (mg/dL), age inyears, weight in kilograms (kg).The etiology of renal failure following car-
diac surgery and CPB is multi-factorial with bothischemic and direct nephrotoxic etiologies. Lowflow, nonpulsatile CPB may produce renal perfu-sion pressures below the limit of renal autoreg-ulation resulting in ischemia-reperfusion injury.This insult is exacerbated by CPB hemodilution.Although it is clear that CPB plays a role in the gen-esis of renal dysfunction following cardiac surgery,it is only one of multiple factors as evidenced by thefact that off-CPB cardiac surgical procedures do nothave a lower incidence of renal dysfunction thanon-CPB procedures. Atheromatous aortic embolihave been implicated in the genesis of renal failureas well. Mediators released as part of the systemicinflammatory response, particularly tumor necrosisfactor-α (TNF-α) and interleukin-6 (IL-6), producerenal microvascular changes that can result in tubu-lar damage. Finally, many cardiac surgical patientswill be exposed to nephrotoxic angiographic con-trast agents preoperatively. It is important to pointout that patients with pre-existing renal dysfunc-tion are at no greater risk than patients withnormal renal function for renal injury. However,patients with pre-existing renal dysfunction are atgreater risk for acute renal failure and the require-ment for renal replacement therapy following agiven renal insult than patients with normal renalfunction.A number of interventions commonly employed
to prevent renal dysfunction following cardiacsurgery and CPB particularly in high-risk patientsare summarized:• Prophylactic infusion of sodium bicarbonate(154mmol/L at 3mL/kg/h prior to angiographiccontrast administration and at 1mL/kg/h for6 hours after administration) is probably superior
∗ ∗ ∗ ∗ ∗ ∗
40
30
20
Pre
dict
ed %
∆Cr
10
010 15 20
Lowest Hct during bypass (%)25 30 35
Fig. 13.2 The influence of intraoperative bloodtransfusion on the relationship between fractionalchange in creatinine (%Cr) and lowest hematocrit(Hct) on cardiopulmonary bypass. Parallel lines representthe number on units of packed red blood cells transfusedintraoperatively: ∗ = 9units; = 6units; = 3units; = 0units. Both low hematocrit on cardiopulmonarybypass and transfusion to treat the low hematocritcontribute to the development of renal dysfunction.(From Swaminathan M, et al. The association of lowesthematocrit during cardiopulmonary bypass with acuterenal injury after coronary artery bypass surgery.Ann Thorac Surg 2003;76:789, with permission.)
to prehydration in preventing contrast medium-induced nephropathy.• Preload and cardiac output should be optimizedin both the pre- and post-CPB periods.• A hematocrit <25% on CPB should be avoided,keeping in mind that PRBC transfusion to treata low hematocrit increases the risk of developingrenal dysfunction (Fig. 13.2). Strategies to avoidCPB hemodilution and transfusion are summarizedin Table 13.2.• Maintenance of CPB flow rates≥2L/min/m2 andmean arterial pressure ≥50–70mmHg are proba-bly prudent in high-risk patients. A more importantdeterminant than pump flow may be the productof pump flow and arterial oxygen content with acritical valve of 272mL/min/m2.• No meaningful correlation between urine outputon CPB and postoperative renal function has beendemonstrated.• Prophylactic administration of “low-dose” or“renal dose” dopamine (1–3µg/kg/min) increasesurine output but has not been demonstrated toimprove or prevent perioperative renal dysfunction.

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 434 — #10
434 Chapter 13
There is concern that prophylactic dopamineadministration may not be benign given the factthat it is associated with release of markers suchas β2-microglobulin that are indicative of sub-clinical renal tubular injury. In addition, prophy-lactic dopamine administration may compromisesplanchnic mucosal perfusion and predispose todevelopment of postoperative atrial fibrillation.• Prophylactic administration of low doses ofthe selective dopamine-1 receptor (D1) agonistfenoldopam mesylate (0.01–0.03µg/kg/min) maybe renoprotective particularly in patients withpre-existing renal dysfunction. At higher dosagesfenoldopam has a vasodilator profile similar tosodium nitroprusside.• Diuretic administration (furosemide, mannitol)in conjunction with CPB increases urine output butis not renoprotective and may in fact be associatedwith an increased risk of serum creatinine elevationand acute renal failure due to part to the neuro-hormonal effects (renin–angiotensin–aldosterone)of preload reduction and hypovolemia.
Inflammatory sequalae ofcardiac surgery and CPB
Cardiac surgery and CPB are known to be apotent stimulus for initiation of both pro- and anti-inflammatory responses. The balance of the elicitedpro- and anti-inflammatory mediators deter-mines the clinical manifestations of this response.A preponderance of anti-inflammatory mediatorsproduces the compensatory anti-inflammatoryresponse syndrome (CARS) while a preponder-ance of pro-inflammatory mediators produces thesystemic inflammatory response syndrome (SIRS).SIRS is characterized by tissue and endothelialinjury leading to enhanced capillary permeability(capillary leak syndrome) and transmigration ofleukocytes into interstitial fluid with subsequentactivation of sequestered leukocytes and amplifica-tion of the inflammatory process. The spectrum ofSIRS induced responses range from tissue edemato end-organ dysfunction and failure. Immediatepostoperative fever and leukocytosis is a commonrelatively benign manifestation of SIRS. Postopera-tive sepsis and SIRS is more likely in cardiac surgery
patients who have reduced monocyte human lym-phocyte antigen DR (HLA-DR) expression. Thisreduced expression is felt to be a manifestationof the relative predominance of anti-inflammatorystimuli over pro-inflammatory stimuli resulting ina state of immunoparesis.The systemic inflammatory response associated
with cardiac surgery and CPB is initiated by a varietyof stimuli. Contact activation, heparin-protaminecomplexes, endothelial ischemia/reperfusion injury,and gut translocation of endotoxins have beenimplicated. Mechanical sheer stress, hemodilution,hypothermia, autotransfusion of unprocessed shedblood, and use of cardiotomy suction play a role.Genetic polymorphisms influence the response toinitiating stimuli. The magnitude of the inflamma-tory response is enhanced in neonates, infants andsmall children due, in part, to the high circuit sur-face area to blood volume ratio as compared toadults.Initiating stimuli induce the release of inflam-
matory mediators via a number of pathways assummarized in Fig. 13.3. The complement cascadeis activated via both the classic and alternativepathway. Exposure of blood to the CPB circuitresults in conversion of factor XII to factor XIIawith initiation of thrombin formation. In addi-tion, factor XIIa leads to conversion of prekallikreinto kallikrein with production of bradykinin andalternative pathway activation (C3) of the com-plement cascade. This process is exacerbated bythe fact that the CPB circuit lacks the endothe-lial cell surface inhibitors that normally limit C3activation. Endotoxin and ischemia/reperfusionmediators also initiate complement activation viathe alternative pathway. Activation of the comple-ment pathway via the classical pathway (C1 and C4)occurs due to the presence of heparin-protaminecomplexes.There is production and release of both pro-
and anti-inflammatory cytokines from activatedmonocytes, macrophages, lymphocytes, and vas-cular endothelium. Cytokines are inflammatorymediators that can act on the cells that pro-duced them (autocrine), on cells in the vicinity(paracrine) or systemically (endocrine). The inten-sity of the inflammatory response as measured by

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 435 — #11
Special Considerations 435
Initiating stimuli• Contact activation (CPB circuit)• Mechanical shear stress• Cardiotomy suction• Endotoxin release• Ischemia / reperfusion injury• Heparin-protamine complexes
Complement activation• Classical pathway (C1, C4)• Alternative pathway (C3)
Factor XII activation• Thrombin production• Plasmin production• Kallikrein production
Endothelial cell adhesion moleculeexpression
Cytokine releasePro-inflammatory• IL-1β• IL-6• IL-8• TNF-α
Leukocyte adhesion moleculeexpression
Leukocyte transmigration anddegranulation
SIRS
NF-B activation
Cytokine releaseAnti-inflammatory• IL-1ra• IL-10• TNFsr-1 and 2iNOS up-regulation Bradykinin release
Fig. 13.3 Schematic of the inflammatory cascadeassociated with cardiac surgery and cardiopulmonarybypass leading to systemic inflammatory responsesyndrome (SIRS). Inflammatory mediators are in boldboxes. Solid arrow and line is stimulatory. Dashed arrow
and line is inhibitory. CPB, cardiopulmonary bypass; IL,interleukin; iNOS, inducible nitric oxide synthase;NF-κB, nuclear factor-κB; ra, receptor antagonist; TNF,tumor necrosis factor; TNFsr, tumor necrosis factorsoluble receptor.

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 436 — #12
436 Chapter 13
Platelet-leukocyte
aggregation
Rollingleukocytes
Firmadherence
Transendothelialmigration and
release ofgranules
Endothelium
P selectin
E selectin
L selectin
Interstial spaceActivatedintegrin
ICAM/VCAM
Fluidleakage
Fig. 13.4 Schematic ofleukocyte–platelet–endothelial cellinteraction leading to leukocytemargination, rolling, and adhesion.Transmigration of a leukocyte across theendothelial cell layer followed by leukocytedegranulation is illustrated. ICAM,intercellular adhesion molecule; VCAM,vascular cell adhesion molecule. (FromPaparella D, et al. Cardiopulmonary bypassinduced inflammation: pathophysiologyand treatment. An update. Eur JCardiothorac Surg 2002;21:232–244, withpermission.)
pro-inflammatory cytokine levels such as TNF-α,IL-1β, IL-6, and IL-8 has been linked to the devel-opment of end organ dysfunction (myocardial,pulmonary, renal, hepatic) and sepsis in the peri-operative period. Endothelial inducible nitric oxidesynthase (iNOS) is up-regulated by the inflamma-tory process resulting in higher levels of NO. Thesehigher levels result in increased vascular perme-ability and vasodilatation. Bradykinin release resultsin vasodilation and enhanced vascular permeabilityas well.Production of these inflammatorymediators leads
to induction of nuclear factor κB (NF-κB), thetranscription factor responsible for expression ofboth endothelial and leukocyte adhesion molecules(selectins and integrins). These molecules promotethe margination, rolling, adhesion, and transmigra-tion of leukocytes through the endothelium intothe extravascular space (Fig. 13.4). Degranulationof leukocytes releases elastase andmyeloperoxidasethat lead to tissue damage. Release of cytokines bythese leukocytes further escalates the inflamma-tory response. In addition, once NF-κB is inducedit up-regulates cytokine production.A number of different approaches aimed at effec-
tive attenuation of SIRS following cardiac surgeryhave been investigated (Table 13.3) but none haveproven uniformly effective. This is not surpris-ing considering the multi-mediator nature of thesystemic inflammatory response. A multi-modalapproach will likely be needed. Nonetheless, thetwo most commonly employed drug therapies areaprotinin and glucocorticoids.
Table 13.3 Therapies to modulate the systemicinflammatory response to cardiac surgery andcardiopulmonary bypass (CPB).
Avoidance of CPB• Off-pump coronary artery bypass grafting (OPCAB)Modification of the CPB circuit• Use of biocompatible CPB circuits:a Covalent heparin binding coatingb Phosphorylcholine coatingc Poly 2-methoxyethylacrylate coatingd Siloxane/caprolactone oligomer coating• Normoxic rather than hyperoxic CPB• Avoidance of cardiotomy suction• Avoidance of unwashed autotransfusionSelective digestive decontamination• Nonabsorbable oral antibiotics (polymyxin E, tobramycin,amphotericin B)
Hemofiltration on CPB• Continuous ultrafiltration (CUF)•Modified ultrafiltration (MUF)• Dilutional ultrafiltration (DUF)• Zero-balance ultrafiltration (ZBUF)Leukocyte depletion• Use of leukodepleted blood or leukocyte filtersComplement inhibition• C5 monoclonal antibody (pexelizumab)• C1-esterase inhibitor• C4A rich plasma administration to C4A-deficient patients
Free radical scavengers – antioxidants• Allopurinol•Mannitol• Ascorbic acid (vitamin C)• α-Tocopherol (vitamin E)
Serine protease inhibitors• AprotininGlucocorticoids•Methylprednisolone• Dexamethasone
CPB, cardiopulmonary bypass.

Alice Nelson Dinardo: “ch13” — 2007/7/16 — 12:41 — page 437 — #13
Special Considerations 437
High-dose aprotinin regimens producingplasma levels ≥30µg/mL (215KIU/mL) inhibitCPB-induced kallikrein production. Kallikrein isresponsible for production of bradykinin and foractivation of the complement system both ofwhich play a prominent role in the genesis ofSIRS. Kallikrein is also responsible for produc-tion of plasmin, an additional source of com-plement activation. Aprotinin at lower plasmalevels is also capable of directly inhibiting plas-min. Aprotinin also plays an important role inattenuation of SIRS through inhibition of up-regulation of pro-inflammatory adhesionmoleculessuch as the integrin CD11b.Multi-level inhibition ofthe leukocyte-endothelial cell adhesion cascade byaprotinin inhibits leukocyte transmigration throughvascular endothelium. Aprotinin is also capable ofinhibiting cytokine-induced production of iNOS.Glucocorticoids reduce inflammation via a num-
ber of mechanisms. They inhibit NF-κB, themain transcription factor of genes for inflam-matory proteins and also increase the transcrip-tion of many anti-inflammatory proteins suchas IL-10- and IL-1-receptor antagonist. In addi-tion, glucocorticoids decrease endotoxin releaseand leukocyte adhesion molecule (CD 11b) expres-sion. The optimal timing, dosage, and formula-tion of glucocorticoid administration remain to bedetermined.
Suggested reading
Appoo JJ, Augoustides JG, Pochettino A et al. Periop-
erative outcome in adults undergoing elective deep
hypothermic circulatory arrest with retrograde cere-
bral perfusion in proximal aortic arch repair: evalua-
tion of protocol-based care. J Cardiothorac Vasc Anesth
2006;20:3–7.
Habib RH, Zacharias A, Schwann TA et al. Role of
hemodilutional anemia and transfusion during car-
diopulmonary bypass in renal injury after coronary
revascularization: implications on operative outcome.
Crit Care Med 2005;33:1749–56.Hogue CW, Jr, Palin CA, Arrowsmith JE. Cardiopul-
monary bypass management and neurologic outcomes:
an evidence-based appraisal of current practices. Anesth
Analg 2006;103:21–37.Karkouti K, BeattieWS,Wijeysundera DN et al. Hemodilu-
tion during cardiopulmonary bypass is an independent
risk factor for acute renal failure in adult cardiac surgery.
J Thorac Cardiovasc Surg 2005;129:391–400.Koch CG, Li L, Duncan AI et al. Morbidity and mortality
risk associatedwith red blood cell and blood-component
transfusion in isolated coronary artery bypass grafting.
Crit Care Med 2006;34:1608–16.Laffey JG, Boylan JF, Cheng DC. The systemic inflamma-
tory response to cardiac surgery: implications for the
anesthesiologist. Anesthesiology 2002;97:215–52.Wijeysundera DN, Karkouti K, Beattie WS, Rao V,
Ivanov J. Improving the identification of patients at
risk of postoperative renal failure after cardiac surgery.
Anesthesiology 2006;104:65–72.Zhang S, Wang S, Li Q et al. Capillary leak syndrome
in children with C4A-deficiency undergoing cardiac
surgery with cardiopulmonary bypass: a double-blind,
randomised controlled study. Lancet 2005;366:556–62.

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 439 — #1
Index
Page numbers in italics refer to figures and those in bold to tables
abciximab 363Abiocor device 377Abiomed AB5000 376, 378,
392, 406Abiomed BVS 5000 376, 395–8,
397, 398, 406ABO blood typing, heart
transplantation 258ABO incompatible heart
transplantation 258, 258acadesine 417acceleration time (A1) 65ACE inhibitors see angiotensin
converting enzymeinhibitors
acetylcholinesterase inhibitors,heart transplant recipients272, 273
acetylsalicylic acid see aspirinacid-base managementalpha-stat vs. pH-stat 347,
347–8, 426CPB 347–8, 355DHCA 426, 427
acoustic quantification (AQ) 73activated clotting time (ACT)
87–8aprotinin use 368for CPB 339–41, 352protamine dose determination
359, 362activated partial thromboplastin
time see partialthromboplastin time,activated
acute renal failure (ARF) 432–4after thoracic aorta surgery
315–16, 317preoperative assessment of risk
13, 13preventive interventions 13,
433, 433–4adenine nucleotides, depletion
410adenosinecardioplegia solutions 417congenital heart disease 186heart transplant recipients
272stress testing 5–6
afterloadaortic regurgitation 146, 147aortic stenosis 139–40dilated cardiomyopathy 257ejection fraction 30mechanical circulatory support
405, 406mismatch 25–6after mitral valve surgery161
aortic stenosis 136, 138,140
aortic surgery 321–2dilated cardiomyopathy254, 256
heart transplant recipients265, 266–7
neonates 171mitral regurgitation 159, 161mitral stenosis 151–2, 153
myocardial oxygen demand94
pressure–volume loops 24,24–6, 25, 26
air, intracardiacduring CPB 335removal 353–4role of TEE 82–3, 353transplant recipients 265,286
air embolism 431during CPB 345prevention 353–4
air locks, CPB venous drainagelines 325
airwaycomplications, lung
transplantation 286compression, aortic lesions
311, 311, 312management, congenital heart
disease 191–2aldosterone inhibiting drugs,
dilated cardiomyopathy255
Alfieri stitch 166aliasing 62, 63Allen’s test 44–5allergic reactionsaprotinin 367protamine 360–1, 362
allopurinol 417α1-antitrypsin deficiency 273,
274α-adrenergic agonists 105
see also phenylephrine
439

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 440 — #2
440 Index
α-stat acid-base managementCPB 347, 347–8DHCA 426, 427
American College ofCardiology/AmericanHeart Association(ACC/AHA)
classification of heart failure 3indications for aortic valve
replacement 164indications for CABG surgery
90, 91–2indications for mitral valve
surgery 165intraoperative TEE monitoring
130, 131American Society of
Anesthesiologists (ASA),monitoring standards42–3
American Society ofEchocardiography (ASE)
intraoperative TEE monitoring130, 131
mitral valve classification148–9
recommended TEE views 67aminophylline 6amiodarone 186anaerobic metabolism 410, 415,
423anaphylactic/anaphylactoid
reactions, protamine360–1, 362
anemia, myocardial oxygendelivery 99–100
anesthetic preconditioning(APC) 99, 115–16, 116
angina pectoris 100aortic stenosis 137classification 4exercise ECG testing 6exertional 98, 98indications for CABG 91pathogenesis 96, 97–8rest 98, 98unstable 1, 3indications for CABG 91–2pathogenesis 96–7
variant (Prinzmetal’s) 99see also myocardial ischemia
angiotensin converting enzymeinhibitors (ACE-I)
aprotinin interaction 368–9CABG 110congenital heart disease
187–8dilated cardiomyopathy 255valvular heart disease 131
angiotensin-receptor blockers(ARB), dilatedcardiomyopathy 255
antegrade cerebral perfusion(ACP) 428, 428
antiarrhythmic agents,congenital heart disease186
anticoagulationCPB 339–41, 352, 373–4ECMO 403heart transplant recipients
259IABP recipients 385mechanical assist device
insertion 403total artificial heart 390VADs 394, 398, 400valvular heart disease 131–2see also heparin
anti-factor Xa assay 359antifibrinolytic agents 365–9dosage and administration
366–7efficacy 367–8
antihypertensive agents, aorticsurgery 318–19
antiplatelet agentspost-CPB bleeding problems
363preoperative discontinuation
16–17, 110, 131see also aspirin; clopidogrel
antithrombin-III (AT-III) 339deficiency 341recombinant 341
aortaascending, surgery 313, 318,
320–1atheromatous disease 83–4,
84coarctation see coarctation of
aortadescending thoracic, surgery
313, 316–18, 321–2epiaortic ultrasound scanning
83, 84orientation and identity, TEE
85TEE evaluation 83–4, 84TEE views 69, 70, 71–2, 72
aortic aneurysms, thoracic306–8
airway compression 312diagnosis 308–11, 309, 310false 308fusiform 308, 308saccular 308, 308
aortic arch
distal, surgery 313, 316–18,321–2
interrupted see interruptedaortic arch
reconstruction, single ventriclelesions 225, 227–8
surgery 313, 318, 320–1TEE views 72, 72
aortic cannulas for CPB 326,341–2
assessment of inflow 343–4macroembolus reduction 432removal 369TEE visualization 84, 344
aortic cross-clamping 349anesthetic management 321,
321–2aortic surgery 312–16, 313coarctation repair 206myocardial consequences
409–10, 410, 411reducing embolus formation
432removal 354spinal cord ischemic time
314, 315aortic diastolic pressure,
congenital heart disease182
aortic dissection 305, 305–6aortic regurgitation with 143,
147classification 305–6, 306at CPB cannulation site 343diagnosis 308–11, 309, 310,
310mortality rates 306, 307paraplegia complicating 314surgical approach and
management 311aortic lesions, thoracicairway compression 311, 311,
312classification 304–8diagnosis 308–11
aortic perfusion pressure, CPB seeperfusion pressure, CPB
aortic regurgitation (AR) 143–8anesthetic technique 146–8cardiac catheterization 37, 38mitral regurgitation with 144,
145, 163mitral stenosis with 163pathophysiology and
adaptation 143–6, 144TEE 80–1, 81
aortic rootabnormalities 80, 143

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 441 — #3
Index 441
cardioplegia infusion 410,419
aortic stenosis (AS) 135–43anesthetic technique 140–3cardiac catheterization
35–7, 36congenital supravalvular
(SVAS) 224congenital valvular 224critical 140discovered during CABG 165grading of severity 79–80indications for valve
replacement 164mitral regurgitation with
163–4mitral stenosis with 163pathophysiology and
adaptation 135–40post-bypass management
132, 132–3, 142–3preoperative evaluation
129–30, 130severe neonatal 172, 175, 224TEE 79–80
aortic surgery 304–22anesthetic management
318–22, 321aortic cross-clamping 312–16,
313arterial pressure monitoring
45surgical approach 311–18,
313ventilation 311–12
aortic transection, traumatic306, 307
diagnosis 308–11, 309aortic valve 134–48anatomy 134, 134–5, 135area 35, 37, 79, 80indicating surgery 135
assessment, VAD insertion404
bicuspid 143, 224dimensionless index (DI) 80indications for replacement
164pulmonary autograft for
replacement 133, 164TEE evaluation 79–81TEE views 68, 69, 71
aortography 20–1, 308–9, 310aortopulmonary collateral
arteries, multiple seemultiple aortopulmonarycollateral arteries
aortopulmonary shunts, surgicalsingle ventricle lesions 225,
226TEE evaluation 86tetralogy of Fallot 209–10,
210vs. bidirectional Glenn
procedure 232, 234aprotinin 365–6, 437allergic reactions 367dosage and administration
366–7efficacy 367–8mechanical assist device
insertion 403neuroprotective effects 432
argatroban 374L-arginine 418arginine vasopressin see
vasopressinarrhythmias see dysrhythmiasarterial blood pressuremean see mean arterial blood
pressuremonitoring 44–6coarctation of aorta 45, 206congenital heart disease188
see also blood pressurearterial cannulationfor CPB 326–7, 341–2, 369for monitoring 44–6
arterial inflow, for CPB 326–7assessment 343–4
arterial switch operation (ASO)216–18, 217
post-CPB management219–20
ASD see atrial septal defectsaspirinmechanical circulatory support
390, 394preoperative use 16–17, 18,
363assisted venous drainage, CPB
326asthma, preoperative assessment
12–13atherosclerotic disease 96–8, 97coronary angiography
33–4, 34ATP, depletion 409, 410ATPase 423atria, TEE evaluation 85atrial arrhythmias, heart
transplant recipients 271atrial fibrillationaortic stenosis with 136
heart transplant recipients271
mitral regurgitation 157, 159,161
mitral stenosis 149–50, 151preoperative evaluation 2
atrial function, transplantedheart 270
atrial natriuretic peptide (ANP)130, 254–5
atrial septal defects (ASD)196–9
anatomy 196–7, 197anesthetic management 195,
198physiology 197–8post-CPB management 196,
198–9repaired, TEE evaluation 86surgical therapy 198total anomalous pulmonary
venous return 221atrial septectomyhypoplastic left heart
syndrome 242single ventricle lesions 225,
227atrial septostomy, balloon
215–16, 227atrial septum 196movement, pressure estimates
83TEE views 69, 70
atrioventricular (AV) block 4atrioventricular canal (AVC)
defects 199–201anatomy 199, 199–200anesthetic management 195,
200post-CPB management 196,
200–1atrioventricular (AV) node
dysfunction, hearttransplant recipients 265
atropine 112aortic valve surgery 141, 147heart transplantation 261,
272automated border detection
(ABD) 73autonomic innervationat birth 171transplanted heart 268–9
AVC defects see atrioventricularcanal defects
awareness during anesthesia132, 353
A waves 51, 51, 52cannon 51, 52

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 442 — #4
442 Index
axial pumps, circulatory support400, 400–1
axis, cardiac 2azathioprine 268
bacterial pericarditis 298–9balanced circulation concept,
single ventricle physiology228, 228–9
balloon atrial septostomy (BAS)215–16, 227
Barlow syndrome 155baroreceptor response, heart
transplant recipients268–9
basiliximab 268Beck’s triad 290–1beclomethasone, inhaled 12benzodiazepinesaortic valve surgery 142congenital heart disease 193coronary revascularization
109, 112–13heart transplantation 260,
261lung transplantation 283see also diazepam; lorazepam;
midazolamBerlin Heart 376, 392Bernouilli equation 64, 79–80β2-agonists, asthma control
12, 13β-adrenergic agonistsdilated cardiomyopathy 254heart transplant recipients
272see also dobutamine;
dopamine; epinephrine;isoproterenol;norepinephrine
β-adrenergic receptors, dilatedcardiomyopathy 254
beta-blockers (β-adrenergicantagonists)
aortic surgery 318–19aortic valve surgery 141CABG 110dilated cardiomyopathy 255heart transplant recipients
272tachycardia management
104–5see also individual agents
bicarbonate therapy 433aortic surgery 322“Tet spells” 209
bicitra 260, 279
bidirectional Glenn procedure(BDG) see superiorcavopulmonary shunt
BioMedicus device 376, 398,399
bioprosthetic heart valves133–4
bivalirudin 374biventricular assist devices
(BiVAD) 376, 379, 398bladder temperature monitoring
342–3Blalock–Taussig shunts 210,
210arterial pressure monitoring
45modified (mBTS) 210, 210hypoplastic left heartsyndrome 242–3
single ventricle lesions 225,226
tricuspid atresia 241bleeding/hemorrhageabnormal, preoperative
evaluation 16–19complicating pericardiectomy
301post-CPB 362–9, 370surgical 362
bleeding time 18, 88blood floweffective 172, 173rates, CPB 345–6, 346
blood gases, arterial 11blood pressure (BP)age-related variation 183,
183control, aortic surgery
318–19, 321, 322on CPB 346diastolic (DBP), myocardial
oxygen delivery 95during exercise testing 7intraoperative monitoring
44–6, 188myocardial oxygen balance
95, 104during off-pump CABG 115perioperative myocardial
ischemia 101see also arterial blood pressure;
hypertension;hypotension
blood transfusion see transfusionof blood products
blood volume, estimated (EBV)338, 338
BODE index 273
bradycardia 2aortic regurgitation 145–6,
147aortic stenosis 138–9, 139,
141coronary revascularization
112heart transplantation 261mitral regurgitation 158–9myocardial oxygen delivery
95bradykinin 436, 437braincooling 426temperature 342, 352, 428
brain death, myocardial effects264
brain natriuretic peptide (BNP)254–5
bronchiolitis obliterans (BO)287
bronchiolitis obliteranssyndrome (BOS) 287
bronchodilators 12–13Bruce treadmill protocol 6bubble oxygenators 328, 328–9buffering, cardioplegia solutions
414bupivacaine, hyperbaric 117
CABG see coronary artery bypassgraft
calciumadministrationcongenital heart disease
186during CPB 341CPB termination 124, 355,357–8
cardioplegia solutions 413–14homeostasismyocardial ischemia 410,411
neonatal myocardium 423reperfusion solutions 418serum, ECG effects 4
calcium channel blockers 106aortic surgery 318–19CABG patients 110cardioplegia solutions 416–17heart transplant recipients
272calcium paradox 414caloric requirements, pediatric
patients 187Canadian Cardiovascular Society
Classification of Angina 4cannon A waves 51, 52

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 443 — #5
Index 443
carbon dioxideend-tidal (ETco2), monitoring
189membrane oxygenator sweep
gas 427partial pressure in arterial
blood (Paco2)
CPB circuits 329hypothermic CPB 347, 348pulmonary vascularresistance 180
reference flow 332ventilatory response, lung
transplant recipients 287carboxyhemoglobin 12cardiac allograft vasculopathy
(CAV) 270–1cardiac catheterization 10interpretation of data 20–41left heart 20–1pericardial disease 291, 292,
297, 297right heart 20valvular lesions 23, 35–8
cardiac output (CO)aortic regurgitation 145–6aortic stenosis 138, 139, 139continuous (CCO), monitoring
55–6, 57determination 21–2, 55–7circulatory assist devicerecipients 407
Doppler method 64factors affecting accuracy57
Fick method 22thermodilution (TD)method 22, 55–7
Fontan physiology 239mixed venous oxygen
saturation 58neonates 170–1resistance calculations 22–3
cardiac output monitor anddiagnostic unit (COMDU)389, 389, 390
cardiac surgerychronology 410prior see prior cardiac surgery
cardiac tamponade see pericardialtamponade
cardiogenic shock, mechanicalcirculatory support375–7, 403
cardioplegia 411–22delivery 410, 418–22delivery system 412, 418–19infusion volume 419
neonates, infants and children423–4
reperfusion injury 417–18,418
solutions 411–17, 419adjuvant agents 416–17buffering 414components 411–15, 413crystalloid vs. blood415–16, 416
osmolarity 414–15cardiopulmonary bypass (CPB)
323–74aortic surgery 318, 320–1circuit 323–39, 324coating 339prime 337–9
cold-reactive proteins 370–2commencing 343–5conduct 345–51decannulation 369flow rates 345–6, 346, 433glucose and insulin
homeostasis 14–15heart-lung transplantation
(HLT) 277, 278hematocrit for 338, 350,
429–30heparin-induced
thrombocytopenia372–4, 373
hypothermic see hypothermicCPB
inflammatory sequelae 434–7lung transplantation 277,
278, 285–6myocardial preservation
during 409–24normothermic 345partial 325–6aortic surgery 317–18, 322
pediatric 323bleeding problems after364, 366–7
cerebral blood flowregulation 347, 348–9
circuit prime 337circuits 324, 326termination 353, 356
pericardial and chest closure369
pericardiectomy 302preparation for 339–43recommendations for conduct
351–2sickle cell disease 372termination 357–8coronary revascularization119–24
factors causing difficulty354
heart transplantation265–7
management after seepost-CPB management
preparation for 352–6valve surgery 132–3, 354
total (complete, full) 324–5cardiopulmonary resuscitation
(CPR), emergency CABG119
cardiotomy suction 333cardio-to-thoracic ratio 5cardiovascular evaluation 1–10history and physical
examination 1–2investigations 2–10
cardiovascular physiology,pediatric 167–71
CardioWest total artificial heart377, 385–90, 388, 389
insertion 388–9management 389, 389–90,
390catecholamine resistant
vasodilatory shock(CRVS) 407
catecholamines 121–2, 123catheters, TEE visualization
86–7cavopulmonary anastomosis,
double 232, 235cavopulmonary connection, total
see Fontan procedurecavopulmonary shunt, superior
see superiorcavopulmonary shunt
cell death, myocardial ischemia410
central shunt, tetralogy of Fallot210, 210
central venous access 46–8heart transplantation 260pediatric patients 46, 48, 189right ventricular assist device
recipients 408central venous catheters 46central venous measurements
51–9central venous pressure (CVP)constrictive pericarditis
296–7, 297on CPB 346monitoring, pediatric patients
189, 189pericardial tamponade 290–1,
291, 294

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 444 — #6
444 Index
central venous pressure (CVP)(Cont’d)
resistance calculations 22–3see also right atrial pressure
centrifugal pumpsCPB 327, 327–8mechanical circulatory support
398–400, 399cerebral blood flowautoregulation 346–7on CPB 346–9, 432transcranial Doppler 190–1
cerebral emboli 431–2transcranial Doppler 191
cerebral metabolic rate foroxygen (CMRO2)
acid-base management 426during hypothermia 425
cerebral oxygenationmonitoring 190pH-stat vs. α-stat management
426cerebral oxygen consumption,
hypothermic CPB 345cerebral oxygen extraction,
during rewarming 352cerebral perfusionantegrade 428, 428continuous retrograde 313,
318, 428–9on CPB 432
cerebrospinal fluid (CSF)drainage, aortic surgery312–14, 315
cerebrovascular disease 351,432
chamber dilatation, diastolicpressure–volume curve27
chamber stiffness, increased26–7, 27
CHARGE association 185chemistry, serum 16chemotherapeutic agents 300chest closure, after cardiac
surgery 369chest radiograph (CXR)preoperative 5, 11thoracic aortic lesions 308,
310, 310children see pediatric patientschordae tendinae, rupture 156cisatracuriumaortic surgery 319aortic valve surgery 141congenital heart disease
192–3coronary revascularization
112, 113
heart transplantation 261lung transplantation 283renal failure 298
citrate-phosphate-dextrose(CPD) solution 414
clonidine, intrathecal 116–17clopidogrelpost-CPB bleeding problems
363preoperative use 16, 18, 110,
131clotting factors, dilution by CPB
364–5coagulationmonitoring 87–9preoperative studies 16tests after CPB 88
coagulopathycongenital heart disease 19,
185CPB-associated 364–5renal failure 18–19, 298systemic lupus erythematosus
299Coanda effect 78coarctation of aorta 202–6anatomy 202anesthetic management
205–6arterial pressure monitoring
45, 206physiology 202–3, 203surgical therapy 204, 204–5,
205coating, CPB circuit 339cocaine abuse 305cognitive dysfunction,
postoperative 430–1cold agglutinins (CA) 371–2cold-reactive proteins 370–2collateralsbronchopulmonary, TGA 214coarctation of aorta 203coronary artery 34, 93,
94, 96multiple aortopulmonary see
multiple aortopulmonarycollateral arteries
myocardial protection 422,424
color-flow (CF) Doppler 63, 63compensatory anti-inflammatory
response syndrome(CARS) 434
complement activation 434,435
compliance (distensibility),ventricular
causes of poor diastolic 26–7
decreased 27–8, 28–30neonates 171
computerized tomography (CT)10
aortic lesions 309, 310conduction defects, preoperative
evaluation 4congenital heart disease (CHD)
167–251anesthesia induction and
maintenance 192–3cardiac catheterization 23,
40–1coagulopathies 19, 185heart transplantation 252,
260, 263–4myocardial protection
techniques 422–4pathophysiology 171–82preoperative evaluation
182–6preoperative preparation 186,
186–92pulmonary artery catheters
50–1pulmonary assessment 11–12surgically repaired, TEE
evaluation 86TEE 84–6, 191
connective tissue disorders,pericardial disease299–300
conotruncal anomalies 185constrictive pericarditis 289,
296–303anesthetic technique 302–3,
303diagnosis 54, 296–7, 297etiology 296, 297–301hemodynamics 297, 297, 298surgery for 301–2
continuity equation 64–5, 78,80
continuous cardiac output (CCO)monitoring 55–6, 57
continuous-wave (CW) Doppler62–3, 63
contractilityafter LVAD implantation 405myocardial oxygen demand
94neonates 171pressure–volume loops 25, 25
cooling methods, for DHCA 427Coombs’ test, direct 371coronary air embolism 354–5coronary angiography 32–5CABG patients 107–9heart transplant donors 258

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 445 — #7
Index 445
interpretation of data 34–5technique 21, 21, 22
coronary angioplasty, failed,emergency CABG117–19
coronary arteriesanatomy 32, 32–3, 33pre-CABG evaluation107–9
anomalous RV connections246
cardiac allograft vasculopathy270–1
cardioplegia infusion 420collaterals 34, 93, 94, 96congenital abnormalities 182tetralogy of Fallot 211transposition of greatarteries 213, 214
obstruction to flow seecoronary stenosis
reimplantation, TGA 217,219–20
TEE views 69, 70thrombus formation 34
coronary artery bypass graft(CABG) surgery 90–128
anesthesia induction andmaintenance 111–14
fast-track technique 113,113–14
high-dose narcotictechnique 111–13
anesthetic management106–24
aprotinin and graft patency369
cardiac allograft vasculopathy271
cardioplegia infusion 419–20,420, 421
constrictive pericarditis after302, 303
coronary blood flow dynamics90–3
emergency 117–19, 120glucose management 117,
119heart transplantation after
previous 259–60hypothyroid patients 16indications 91–2intrathecal and epidural
analgesia 116–17, 118ischemic and anesthetic
preconditioning 115–16long-term outcome 124–8,
125–6, 127myocardial ischemia 100–6
myocardial oxygenation93–100
off-pump 114, 114–15post-CPB management
119–24preinduction management
110–11premedication 109–10preoperative assessment 12,
106–9repeat, preoperative
evaluation 106, 108, 109strategies to reduce cerebral
emboli 431–2valve disease discovered
during 165–6coronary artery disease (CAD)chest radiography 5coronary angiography 33, 34coronary steal 99hematocrit levels 100hypothyroidism 16pacing-induced ischemia 27pathogenesis 96–8, 97, 98pre-CABG evaluation 107–9preoperative ECG 4pulmonary assessment 12stress testing 6–7see also atherosclerotic disease
coronary artery spasm 34, 99postoperative 120
coronary blood flow 90–3autoregulation 90–3, 93collateral 93, 94congenital aortic stenosis 224during CPB 334, 334
coronary circulation, rightventricle-dependent(RVDCC) 246, 247
coronary ostia, cardioplegiainfusion 420, 420
coronary perfusionafter LVAD implantation
405–6reduced time available for 95
coronary perfusion pressure(CPP) 90, 93
congenital heart disease181–2
reduced 95coronary revascularization
see coronary arterybypass graft (CABG)surgery
coronary sinus (CS)blood flow during CPB 334cannula, TEE evaluation 87defects 197, 198
retrograde perfusion (RCSP)421, 421–2
TEE views 69, 70coronary steal 99, 99coronary stenosis (flow
obstruction)atherosclerotic 96–8, 97, 98angiography 33–4, 34
conduct of CPB 351dynamic 98, 98, 105–6myocardial oxygen delivery
95–6, 349pre-CABG evaluation 107–9
coronary stentstemporary, off-pump CABG
114, 115vs. CABG 124–8, 127
coronary vasomotor toneatheromatous disease 98, 98variations 98–9
coronary vasospasm see coronaryartery spasm
corticosteroids (glucocorticoids)for DHCA 429heart allograft rejection 272heart transplant donors 259inhaled (ICS) 12see also methylprednisolone
cor triatriatum 223cough reflex, lung transplant
recipients 286–7coumadin 390, 394CPB see cardiopulmonary
bypasscreatine phosphate (CP),
depletion 409creatinine clearance 432–3cryoglobulins 371cryoprecipitate 17, 19, 88post-CPB period 364–5
C wave 51, 52cyanosiscoagulopathy 19induction of anesthesia 192myocardial vulnerability to
ischemia 423pathophysiologic relevance
179preoperative evaluation 183,
185tetralogy of Fallot 179, 207
cyclosporine 260, 268, 279cystic fibrosis 274, 275–6cytokines 434–6, 435
daclizumab 268Damus–Kaye–Stansel (DKS)
procedure 225, 226,227–8, 242

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 446 — #8
446 Index
DDAVP see desmopressind-dimers, fibrin 88l-deamino-8-d-arginine
vasopressin seedesmopressin
DeBakey classification, aorticdissection 305–6, 306
deceleration time (D1) 65, 65deep hypothermic circulatory
arrest (DHCA) 346,425–9
acid-base management 348,426
adjuncts to 429alternatives to 428–9aortic surgery 313, 318,
320–1aprotinin use 369conduct 427–8hematocrit 426–7hypothermia 425–6Pao2 management 426–7temperature monitoring 343venous cannulation 325
defibrillation 354–5defibrillators 49–50depth of anesthesia, myocardial
ischemia 104, 105desflurane 115, 192desmopressin (DDAVP)post-CPB bleeding problems
363uremic patients 13, 19, 298
dexmedetomidine 114dextran 390DHCA see deep hypothermic
circulatory arrestdiabetes mellitus (DM)CPB 346heart transplantation 253insulin infusion 15, 15myocardial ischemia 101preoperative evaluation
14–15dialysis, preoperative 13diastole, length, aortic stenosis
138, 138diastolic blood pressure (DBP),
myocardial oxygendelivery 95
diastolic (dys)functioncardiac catheterization 26–30constrictive pericarditis 296,
303coronary angiography 34–5dilated cardiomyopathy 255heart transplant recipients
265, 270
pre-CABG evaluation 106,107, 108
TEE assessment 74–6diastolic pressure time
index:systolic pressureindex (DPTI:SPTI) ratio103–4
diastolic pressure–volume curves27, 27, 28–30
diazepam 109, 113DiGeorge syndrome 185digitalis toxicity 4digoxin 255, 272dilated cardiomyopathy (DCM)
252, 253–7anesthetic management
261–2etiologies 253medical therapy 255pathophysiology and
adaptation 253–7, 254diltiazem 110, 186dimensionless index (DI), aortic
valve 80dip and plateau sign, constrictive
pericarditis 297, 297dipyridamolemechanical circulatory devices
390, 394stress testing 5–6
direct thrombin inhibitors 18,373–4
distensibility see compliancediuretics 255, 434DNase, recombinant human
(rhDNase) 276dobutamineafter CABG 121, 124aortic valve surgery 142, 147,
148congenital heart disease 186heart transplantation 262,
266interrupted aortic arch 250maximal inotropic support
375mitral valve surgery 153,
155, 160stress testing 5–6, 10tetralogy of Fallot 212total anomalous pulmonary
venous return 223transposition of great arteries
219truncus arteriosus 249
dopamineafter CABG 121, 124aortic valve surgery 142, 147congenital heart disease 186
heart transplantation 262,266
interrupted aortic arch 250lung transplantation 284maximal inotropic support
375mitral valve surgery 155renal protection 315–16,
433–4single ventricle lesions 231,
239tetralogy of Fallot 212total anomalous pulmonary
venous return 223transposition of great arteries
219, 220truncus arteriosus 249
Doppler principle 60Doppler ultrasoundcolor-flow (CF) 63, 63continuous-wave (CW) 62–3,
63pressure gradients 63, 64principles 60–1pulsed-wave (PW) 62, 62spectra measurements 64,
64–5transcranial (TCD) 190–1velocity–time integral 64–5,
65double cavopulmonary
anastomosis 232, 235double-headed roller pump
327, 327double inlet left ventricle (DILV)
175Down syndrome see trisomy 21ductal dependent circulation
172ductus arteriosus (DA) 168,
168, 169closure 168–70coarctation of aorta 202, 203,
203delayed closure 170patent see patent ductus
arteriosusductus venosus 167–8, 168, 169closure 170
dysrhythmiasadvanced ECG monitoring 43after Mustard and Senning
procedures 216circulatory assist device
recipients 406–7exercise ECG testing 6–7heart transplant recipients
271

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 447 — #9
Index 447
off-pump CABG 115preoperative evaluation 2
Ebstein’s anomaly 162ecarin clotting time (ECT) 374ECG see electrocardiogramechocardiography 10contrast 10, 86M-mode 61, 61pericardial effusion 291stress 7, 10transesophageal see
transesophagealechocardiography
transthoracic (TTE) 10two-dimensional (2-D) 61,
61–2ECMO see extracorporeal
membrane oxygenationEisenmenger syndrome 273,
274, 275ejection fraction (EF) 30–1aortic stenosis 135, 136, 137,
137CPB 346determination 21, 30interpretation 34mitral regurgitation 157, 158pre-CABG evaluation 106,
107, 109TEE assessment 72–3
elastance (stiffness) 26effective arterial (Ea) 24,
24–5, 30increased chamber 26–7, 27increased muscle 27ventricular (Ees) 24, 24–5, 30
elderly patients see older patientselectrocardiogram (ECG)advanced monitoring 43,
43–4congenital heart disease
surgery 188coronary revascularization
110exercise stress test 6–7IABP control 383lung transplant surgery 279,
280myocardial ischemia diagnosis
102preoperative 2–5serum potassium
abnormalities 4, 14electroencephalogram (EEG)
monitoring 130electrolyte disturbances 4,
13–14Elhers–Danlos syndrome 143
emphysema, lungtransplantation 273, 274
end-diastolic area (EDA) 72–3,76
endobronchial intubation280–1
endocarditis, infectiveaortic regurgitation 143prophylaxis, heart transplant
recipients 271valve repair surgery 134
endocrine disorders,preoperative evaluation14–16
endomyocardial biopsies 271endotracheal intubation see
tracheal intubationendotracheal tubes (ETT)double-lumen (DLT) 282–3,
320pediatric 192single lumen, one-lung
ventilation 281thoracic aortic surgery 320
end-systolic area (ESA) 72–3,76
end-tidal carbon dioxide (ETco2)
monitoring 189ephedrine 112heart transplant recipients
272heart transplant surgery 261valve surgery 141
epidural analgesia/anesthesiaaortic surgery 319coronary revascularization
117, 118lung transplantation 280valve surgery 132
epinephrineafter CABG 120, 122, 124aortic valve surgery 142, 148congenital heart disease 186ductus arteriosus closure 168heart transplantation 266lung transplantation 284maximal inotropic support
375mitral valve surgery 153,
155, 161post-CPB management 361transposition of great arteries
220epoprostenol see prostacyclinε-aminocaproic acid (EACA)
365, 367dosage and administration
366efficacy 368
eptifibatide 363erythrophoresis 19esmolol 104–5aortic surgery 319aortic valve surgery 141cardioplegia solutions 418congenital heart disease 186“Tet spells” 209
esophageal temperaturemonitoring 342–3
etomidateaortic regurgitation 147aortic surgery 320congenital heart disease 193emergency CABG 118heart transplant surgery 261lung transplant surgery 283mitral valve surgery 160pericardial disease 295–6
everolimus 268exerciseheart transplant recipients
269stress testing 6–7, 9–10
external jugular cannulation 48extracorporeal membrane
oxygenation (ECMO)376, 402–3
insertion 402lung transplant recipients 286management 402–3oxygenators 330, 402“Tet spells” 209transposition of great arteries
216venoarterial (VA) 402, 402–3venovenous (VV) 402
factor VIII 17, 364–5factor IX 17factor XI deficiency 17fast-track anesthetic technique,
coronaryrevascularization 113–14
fatty acid oxidation 410, 423femoral artery cannulation
45–6cardiac catheterization 20CPB 326–7IABP insertion 382
femoral vein cannulation 20,325
fenoldopam 186, 434fentanylaortic surgery 319, 320aortic valve surgery 140, 141,
142, 147congenital heart disease 193

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 448 — #10
448 Index
fentanyl (Cont’d)coronary revascularization
111, 112, 113emergency CABG 118heart transplantation 261,
262lung transplantation 283mitral valve surgery 154, 160pericardial disease 295–6, 303
fetal circulation 167–8, 168, 169persistence (PFC) 168
FEV1 see forced expiratoryvolume in 1 second
FEV1/FVC 12fibrin degradation 88fibrinogen 88, 364–5fibrinolysis, post-CPB 365Fick determination, cardiac
output 21–2filters, micropore 335fish allergies 360FK506 268fluid managementcongenital heart disease 187CPB termination 121, 357renal dysfunction 13tetralogy of Fallot 209,
211–12Fontan procedure 236–9, 237anesthetic management 238fenestrated 238post-CPB management
238–9, 240pulmonary atresia with intact
interventricular septum247
staged approach to 225,225–36, 237–8
foramen ovale (FO) 168closure 170patent see patent foramen
ovaleforced expiratory volume in 1
second (FEV1) 11, 12, 13lung transplantation 274
forced mid-expiratory flow(FEF 25–75%) 11
forced vital capacity (FVC) 11fractional area change (FAC)
72, 73, 76Frank–Starling mechanism 24free fatty acid oxidation 410,
423free radical scavengers 417, 418fresh frozen plasma (FFP) 17,
341, 364fructose-1,6-diphosphate 418furosemide 352, 434
Glenn procedure 232bidirectional (BDG) see
superior cavopulmonaryshunt
glucocorticoids see corticosteroidsglucosecardioplegia solutions 415homeostasis, during CPB
14–15perioperative management
15glycemic control 15CABG 117, 119, 120–1congenital heart disease 187
glycopyrrolate 112congenital heart disease 187,
188, 193heart transplant recipients
272Gorlin equation 35, 135Gott shunt 313, 316
H2-receptor blockers 260, 279halothane 192, 212heart failureACA/AHA classification 3congenital heart disease 183,
185constrictive pericarditis 296dilated cardiomyopathy 255mechanical circulatory support
375preoperative evaluation 1see also right ventricular failure
heart-lung transplantation (HLT)273
anesthetic management278–80, 283–4
contraindications 253, 274indications 273, 276noncardiac surgery after
286–8operative procedure 277, 278post-CPB management 286
HeartMate II device 377, 378,400, 401
HeartMate IP device 377, 378,392–4, 393, 406
HeartMate XVE device 377,378, 392–4, 393
heart rate (HR)abnormalities 2age-related variation 183,
183aortic regurgitation 145–6aortic stenosis 138, 138–9,
139congenital heart disease 182
dilated cardiomyopathy 257heart transplant recipients
265, 269mitral regurgitation 159mitral stenosis 150–1, 152,
153myocardial ischemia 101myocardial oxygen balance
94–5, 95, 104see also bradycardia;
tachycardiaheart transplantation 252–73anesthetic management
259–62bridge to 259, 377–8, 378,
403contraindications 252–3, 253donors 257–9noncardiac surgery after
267–73anesthetic principles 272–3physiology of transplantedheart 268–70
unique management issues270–2
operative procedure 262–4,263, 264
post-CPB management 264–7preoperative evaluation
259–60heat exchangers 331, 332,
332–3hematocrit (Hct) 16, 429–30congenital heart disease 185coronary artery disease
99–100CPB 338, 350, 429–30CPB termination 356DHCA 426–7postoperative renal
dysfunction 433, 433hematologic evaluation,
preoperative 16–19hematoma, spinal, after
intrathecal/epiduralanalgesia 117
hemi-Fontan procedure 232,238
Hemochron® 340, 359, 362hemodilution, myocardial
oxygen delivery 349–50hemodynamic parameters,
derived 58, 59hemoglobin 16hemoglobinopathies 372hemoglobinuria, paroxysmal
cold 371hemophilia 17

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 449 — #11
Index 449
hemorrhage seebleeding/hemorrhage
hemostasis, post-CPB 362–9Hemotec® 340, 359, 362heparinconcentration testing 88, 359monitoring effects 87–8,
339–41, 352rebound 361, 362resistance 340–1unfractionated (UFH)for CPB 338, 339–41, 352HIT patients 18, 374IABP recipients 385protamine neutralization358–65
total artificial heartrecipients 390
VADs 398heparinase ACT test 362heparin dose–response test
(HDR) 88, 340heparin-induced
thrombocytopenia (HIT)372–4, 373
heparin-inducedthrombocytopenia andthrombosis (HITT) 18,372
heparin/protamine titration test(HPT) 359
heparin response test (HRT) 340hepatic veinsblood flow velocity 83fetal circulation 167–8
heterotaxy syndrome 173, 324hibernating myocardium 8high-dose narcotic techniqueaortic stenosis 140–2congenital heart disease
192–3, 219coronary revascularization
111–13heart transplantation 261
high dose thrombin time (HiTT)88
hirudin 373–4histidine 414, 418histoplasmosis 299HIT see heparin-induced
thrombocytopeniaHLA-DR 434Hodgkin lymphoma 300,
300–1, 302hormone replacement therapy
(HRT), transplant donors258–9
hyperacute rejection, heart grafts264–5
hypercalcemia 4hypercarbia, single ventricle
physiology 230–1hyperglycemia, CPB-associated
15hyperkalemia 4, 13–14, 355hypertensionaortic valve surgery 142coronary revascularization
112heart transplant recipients
271heart transplant surgery 262management 105myocardial ischemia risk 104preoperative evaluation 2
hyperventilation 180hypocalcemia, in congenital
heart disease 185hypokalemia 4, 14, 355hypomagnesemia 354hypoplastic left heart syndrome
(HLHS) 241–3anatomy 241, 242anesthetic management 243heart transplantation 252myocardial ischemia 182physiology 172, 175, 242post-CPB management 243staged approach to Fontan
procedure 225, 225–36,242–3
hypotensionaortic valve surgery 141–2circulatory assist device
recipients 407coronary revascularization
112heart transplant recipients
268–9management 105myocardial oxygen balance
95, 104pericardial tamponade 290–1protamine-induced 360, 361
hypothermiacardioplegia solutions 413classification 345DHCA 425–6topical 422, 423, 427see also deep hypothermic
circulatory arresthypothermic CPB 345cerebral blood flow 346–9cold-reactive proteins 370–2myocardial oxygen balance
349, 350, 350pediatric patients 423–4pump flow rates 348–9
rewarming prior totermination 352–3
sickle cell disease 372systemic blood flow 345–6systemic blood pressure 346
hypothyroidism, preoperativeevaluation 15–16
hypoxemiatotal anomalous pulmonary
venous return 222transposition of great arteries
215hypoxia, ventilatory response,
lung transplant recipients287
IABP see intra-aortic balloonpump
immunosuppressive drugs 268complications 267, 267preoperative doses 260, 279
indomethacin 170induction of anesthesiaaortic surgery 319–20aortic valve surgery 140–2,
147circulatory assist device
recipients 408congenital heart disease
192–3constrictive pericarditis 303coronary revascularization
111–12heart transplantation 261–2lung transplantation 283–4mitral valve surgery 153–4,
160pericardial effusion 295–6rapid sequenceaortic surgery 319–20emergency CABG 118heart transplantation 261lung transplantation 283
single ventricle lesions 231,234, 238
valve surgery 132infants see neonates; pediatric
patientsinfectious complications,
transfusion of bloodproducts 430
infectious pericarditis 298–9inferior vena cava (IVC)cannulation for CPB 324, 325fetal circulation 167–8, 169
inflammatory mediators 434,435
inflammatory sequelae 434–7,435

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 450 — #12
450 Index
inhalational anesthetic agents seevolatile anesthetic agents
inotropic supportaortic valve surgery 142, 147,
148CABG post-bypass 121–4CPB termination 357dilated cardiomyopathy 254,
255heart transplantation 262,
265, 266interrupted aortic arch 250lung transplantation 285maximal 375mechanisms of action 123mitral valve surgery 153,
154, 155, 160, 161neonates 171pericardial effusion 294–5single ventricle lesions 231,
235, 239tetralogy of Fallot 212total anomalous pulmonary
venous return 223transposition of great arteries
219, 220truncus arteriosus 249
insulinadministration 15, 15CABG 117, 119, 121heart transplant donors259
cardioplegia solutions 415homeostasis, during CPB
14–15NPH, protamine allergy 360resistance 14
integrelin 16, 18intercirculatory mixing 174,
176intercostal arteries, ligation 312,
314internal jugular veincannulation 46–8, 47pulmonary artery catheter
placement 49internal mammary artery (IMA)dissection 110graft flow, vasoactive agents
affecting 120retrograde cardioplegia
infusion 421interrupted aortic arch (IAA)
249–51anatomy 249, 249–50physiology 172, 175, 250
intra-aortic balloon pump (IABP)376, 381, 381–5, 382
anticoagulation 385
complications 383indications and
contraindications 382insertion 382–3management 383–5, 384,
385, 386, 387, 388mitral regurgitation 160TEE evaluation 87weaning 408
intra-atrial septum see atrialseptum
intrathecal analgesia, coronaryrevascularization116–17, 118
intravascular ultrasound (IVUS),cardiac allograftvasculopathy 270
intraventricular dependence, inneonates 171
ischemia, myocardial seemyocardial ischemia
ischemia-reperfusion injury seereperfusion injury
ischemic preconditioning115–16, 418
isofluraneaortic surgery 321aortic valve surgery 142congenital heart disease 192,
193coronary revascularization
113–14coronary steal 99heart transplantation 261lung transplantation 283myocardial protection 115–16
isoproterenolcongenital heart disease 186heart transplant recipients
265–6mitral valve surgery 155
isovolumic contraction 23, 23isovolumic relaxation time
(IVRT) 74, 74
Jarvik 2000 device 377, 378,400–1
Jatene procedure see arterialswitch operation
Judkin’s technique 21, 22junctional ectopic tachycardia
(JET), after tetralogy ofFallot repair 213
kallikrein 365, 434, 437kallikrein inhibition units (KIU)
366ketamine
induction 193, 212, 296premedication 187, 188, 260
Kussmaul’s sign 296–7
L-arginine 418laryngoscopy 112, 141LeCompte maneuver 217, 217,
220left anterior descending (LAD)
artery 33left atrial appendage (LAA)
68–9, 70, 85left atrial enlargement (LAE) 3,
5mitral regurgitation 157, 158mitral stenosis 149
left atrial hypertrophy 149, 157left atrial pressure (LAP) 51,
51–4aortic stenosis 136A wave 51, 52C wave 51, 52elevated 40, 41interpretation 28, 30mitral regurgitation 156, 157,
158mitral stenosis 37, 149–50V wave 51, 52–3X and Y descent 51, 53–4see also pulmonary capillary
wedge pressureleft atrium (LA)blood flow during CPB 334identification using TEE 85
left circumflex artery 32, 33left heart bypass, aortic surgery
313, 317, 322left heart catheterization 20–1“left main equivalent” lesions
107–9left-to-right shunts 172, 173cardiac output determination
57pulmonary arterial
hypertension 40–1, 41quantitation 39–40
left ventricle (LV)blood flow during CPB 334TEE evaluation 85venting during CPB 334–5
left ventricular assist devices(LVAD) 376, 377, 379,391–401
anesthetic management afterinsertion 404–8
indications 378, 378–9insertion 404see also specific devices

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 451 — #13
Index 451
left ventricular diastolic(dys)function
aortic stenosis 135–6aortic surgery 322pre-CABG evaluation 106,
107, 108TEE assessment 74, 74–6, 77see also diastolic (dys)function
left ventricular end-diastolicpressure (LVEDP)
aortic regurgitation 144, 147aortic stenosis 136coronary blood flow 90, 93diastolic pressure–volume
curves 28–30measurement 51, 52, 54mitral regurgitation 159, 160mitral stenosis 153myocardial ischemia 102myocardial oxygen delivery
95pressure–volume loops 23
left ventricular end-diastolicvolume (LVEDV) 23, 30
aortic regurgitation 143–4,145, 146
aortic stenosis 136, 142–3interpretation 28–30measurement 21mitral regurgitation 156,
157–8, 160mitral stenosis 150, 150, 151,
152, 153pressure–volume loops 25
left ventricular end-diastolicvolume index (LVEDVI)28, 30
left ventricular end-systolicpressure (LVESP) 23
left ventricular end-systolicvolume (LVESV) 30
measurement 21pressure–volume loops 23, 25
left ventricular end-systolicvolume index (LVESVI)28, 30
left ventricular (LV) filling,congenital causes ofobstruction to 223
left ventricular hypertrophy(LVH) 4, 5
aortic regurgitation 143–4,144
aortic stenosis 135mitral regurgitation 156, 157,
157–8left ventricular outflow tract
(LVOT), TEE 71, 84
left ventricular outflow tractobstruction (LVOTO)
congenital 224transposition of great arteries
214, 218left ventricular stroke work
(LVSW) 31left ventricular stroke work
index (LVSWI) 59left ventricular systolic
(dys)functionafter CABG 120aortic stenosis 136, 137–8CPB 346dilated cardiomyopathy 256mitral regurgitation 157, 158TEE assessment 72–3transplanted heart 269
left ventriculography 21, 21,31–2, 32
lepirudin 374leukocyte-endothelial cell
adhesion cascade 436,436
leukotriene receptor antagonists(LTRAs) 12
levosimendanafter CABG 122–4dilated cardiomyopathy 255mechanism of action 122,
123levothyroxine 16lidocainecongenital heart disease 186hyperbaric 117neuroprotective effects 432premature ventricular
contractions 59termination of CPB 354
ligamentum arteriosum 168local anesthesia, vascular access
44, 47lorazepamaortic valve surgery 142CABG 109, 113CPB management 353valvular heart disease 130
lungs, thallium uptake 8lung transplantation 273–88anesthetic management
278–86bilateral sequential single
(BSSLT) 273–4, 277–8,278
anesthetic management284–6
contraindications 253, 274donors 276–7double (DLT) 273–4
en bloc 277, 278operative procedure 277–8
indications 274–6living donor lobar (LDLLT)
274noncardiac surgery after
286–8operative procedure 277–8patient positioning 277post-CPB management 286postoperative care 286single (SLT) 273anesthetic management284–6
operative procedure 277–8,278
postoperative care 286lung volumespulmonary vascular resistance
180transplanted lungs 287
lupus anticoagulant 299LVADs see left ventricular assist
deviceslymphoma, Hodgkin 300,
300–1, 302lysine analogs 365, 366, 368
magnesiumcardioplegia solutions 414congenital heart disease 186termination of CPB 354
magnetic resonance imaging(MRI) 10, 11
aortic lesions 309, 310maintenance of anesthesiaaortic valve surgery 140–2,
147circulatory assist device
recipients 408congenital heart disease 193constrictive pericarditis 303coronary revascularization
113heart transplantation 261–2lung transplantation 283–4mitral valve surgery 153–4,
160pericardial effusion 295–6single ventricle lesions 231,
234, 238valve surgery 132
malignant pericardial disease294, 300, 300–1
mannitol 316, 352, 434MAP see mean arterial blood
pressure

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 452 — #14
452 Index
MAPCAs see multipleaortopulmonary collateralarteries
Marfan syndrome 143mask induction of anesthesia
192maximum voluntary ventilation
(MVV) 12MBTS see Blalock–Taussig
shunts, modifiedmean arterial blood pressure
(MAP)during CPB 346, 351–2, 432,
433CPB termination 356, 357,
358myocardial blood flow 349resistance calculations 22–3
mean arterial bloodpressure–heart rate(BP–HR) quotient 104
mechanical circulatory support375–408
anesthetic considerations403–8
bridge to heart transplantation259, 377–8, 378, 403
bridge to recovery 375–7classification of devices
379–81complications 379destination therapy 378–9device insertion 403–4device selection 375–9extracorporeal devices 376,
380indications 375intracorporeal devices 377,
380post-device implantation
management 404–8triggering modes/percentage
of systole 380–1weaning 408see also specific devices
mediastinal masses, malignant300
Medos VAD 376, 392membrane oxygenators
329–32, 332ECMO 330, 402microporous 329–30, 330,
331solid 330–2
meperidine 188metabolic disorders, ECG effects
4–5metabolic equivalents (METs) 6
metabolism, myocardialduring global ischemia
409–10neonates 171, 423substrates in cardioplegia
solutions 415methylprednisolone 268DHCA management 427transplant recipients 265, 284
metoclopramide 118, 260, 279metoprolol 104MicroMed (DeBakey) VAD 377,
378, 400, 401micropore filters 335midazolamaortic valve surgery 141, 142congenital heart disease 187,
188, 193, 219coronary revascularization
109, 113CPB management 353emergency coronary
revascularization 119heart transplantation 260,
261lung transplantation 279, 283pericardial effusion 295
middle cerebral artery (MCA),transcranial Doppler190–1
milrinoneafter CABG 122, 124congenital heart disease 186,
196, 212heart transplantation 266interrupted aortic arch 250lung transplantation 285maximal inotropic support
375mitral valve surgery 153,
155, 161off-pump CABG 115single ventricle lesions 235,
239total anomalous pulmonary
venous return 223transposition of great arteries
219, 220truncus arteriosus 249
mitral annulus 148mitral inflowDoppler assessment 74, 74parameters, normal values 74
mitral regurgitation (MR)155–61, 156
after mitral valve surgery 82anesthetic technique 159–61aortic regurgitation with 144,
145, 163
aortic stenosis with 163–4cardiac catheterization 37,
37–8diastolic pressure–volume
curves 28, 156–8, 157dilated cardiomyopathy 256discovered during CABG
165–6ejection fraction 30–1grading of severity 79indications for surgery 165ischemic 156, 165–6pathophysiology and
adaptation 156–9, 157percutaneous endovascular
repair 166, 166post-bypass management
133, 160–1TEE 78–9V waves 37–8, 52, 53
mitral stenosis (MS) 149,149–55
anesthetic technique 153–4aortic regurgitation with 163aortic stenosis with 163cardiac catheterization 35–7,
36congenital supravalvular 223congenital valvular 223critical 153parachute 223pathophysiology and
adaptation 149–52, 150,151, 152
post-CPB management 154–5severity estimation 78, 78TEE 76–8
mitral valve 148–61Alfieri stitch 166anatomy 148–9assessment, VAD insertion
404indications for surgery 165TEE evaluation 76–9TEE views 70, 71
mitral valve area (MVA) 76,149
cardiac catheterization 35,36–7
Doppler measurement 65, 65,78, 78
M-mode echocardiography 61,61
monitoring 42–89advanced ECG 43–4arterial pressure 44–6ASA standards 42–3central circulation pressure
48–59

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 453 — #15
Index 453
central venous access 46–8circulatory assist device
recipients 408coagulation 87–9congenital heart disease
188–91coronary revascularization
110–11pulmonary artery catheter
48–59transesophageal
echocardiography 58–87valve surgery 130
monosodium L-aspartate (MSA)418
monosodium L-glutamate(MSG) 418
morphinepremedication 109, 130“Tet spells” 209
motor evoked potentials (MEPs)314–15, 316
multiple aortopulmonarycollateral arteries(MAPCAs)
pH stat vs. α-stat management426
tetralogy of Fallot withpulmonary atresia 244,244, 245
tricuspid atresia 227, 241muscarinic antagonists, heart
transplant recipients 272muscle relaxantsaortic surgery 319aortic valve surgery 141, 147congenital heart disease
192–3coronary revascularization
111–12, 113, 113CPB management 344–5, 353heart transplantation 261see also individual agents
muscle stiffness, increased 27Mustard operation 216, 216mycophenolate mofentil 268myocardial blood flow, on CPB
349–50myocardial contusion, donor
hearts 258, 265myocardial infarction (MI)dilated cardiomyopathy after
253emergency coronary
revascularization 119,120
indications for CABG 91–2newly transplanted heart 265pathogenesis 97
pericarditis complicating 299postoperative (PMI) 101–2preoperative ECG 4
myocardial ischemia 100–6aortic surgery 322congenital heart disease
181–2consequences of global
409–10coronary revascularization
111diagnosis 102–3ECG monitoring 43, 43–4emergency CABG 117–19exercise testing 6, 7incidence of perioperative
101mitral regurgitation 156,
165–6off-pump CABG 114outcome after 101–2pacing-induced 27postoperative 101, 120preconditioning 115–16prediction 103–4preoperative ECG 4pulmonary atresia with intact
ventricular septum247–8
symptomatic vs. asymptomatic101
TEE monitoring 73–4, 102–3thallium imaging 8tolerance in neonates 423transposition of great arteries
219–20treatment 104–6see also angina pectoris
myocardial oxygen balance93–100
aortic stenosis 137, 137dilated cardiomyopathy
255–6myocardial oxygen consumption
(MVo2)
aortic regurgitation 145, 145assessment 103causes of increased 93–5during CPB 350, 350effect of cardioplegia 411, 413mitral regurgitation 158
myocardial oxygen deliveryaortic regurgitation 145causes of reduced 95–100during CPB 349–50mitral regurgitation 158
myocardial perfusionscintigraphy 7–9
myocardial physiology 20–41
myocardial preservation409–24, 410
additional factors 422cardioplegia 411–22neonates, infants and children
422–4myocardial regional wall motion
abnormalities see regionalwall motion abnormalities
myocardial supply–demand ratio(DPTI:SPTI) 103–4
myocardial wall segments seewall segments
myocardial wall tension see walltension, myocardial
N-acetylcysteine 418narcotic agents see opioidsnasopharyngeal temperature
monitoring 342near infra-red spectroscopy
(NIRS) 190neonatescentral venous access 189circulatory changes 167–70,
169myocardial performance
170–1myocardial preservation
techniques 422–4platelet dysfunction 19pulmonary vascular changes
170see also pediatric patients
neostigmine, heart transplantrecipients 272
nesiritide 255neurological outcome 430–2hematocrit 429–30interventions to improve
431–2neuromuscular blockade,
at CPB commencement344–5
neuromuscular blocking agentssee muscle relaxants
nicotine 12nifedipine 106, 110nitric oxide (NO) 180–1, 436inhaled 181, 267, 361
nitric oxide synthase, inducible(iNOS) 436
nitroglycerin (NTG) 105–6aortic surgery 319aortic valve surgery 142congenital heart disease 186CPB management 351heart transplantation 262,
266–7

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 454 — #16
454 Index
nitroglycerin (NTG) (Cont’d)lung transplantation 285mitral valve surgery 155,
160, 161post-CPB management 361
nitroprusside, sodium (SNP)105
after CABG 124aortic surgery 319aortic valve surgery 142, 147congenital heart disease 186,
196CPB management 351, 353DHCA management 427heart transplantation 257,
262, 266–7mitral valve surgery 154,
155, 160, 161transposition of great arteries
220nitrous oxide (N2O)aortic valve surgery 142coronary revascularization
113heart transplantation 261
nodule of Arantius 134non-steroidal anti-inflammatory
drugs (NSAIDs) 18, 299,363
norepinephrine (NE)after CABG 120, 122, 124congenital heart disease 186ductus arteriosus closure 168heart transplantation 266lung transplantation 285mitral valve surgery 155secretion, dilated
cardiomyopathy 254Norwood stage 1 procedure 242modified 242
Novacor device 377, 394,394–5, 395, 396
afterload to 406indications 378
NPH insulin 360N-terminal pro-brain natriuretic
peptide (NTproBNP) 16nuclear factor κB (NF-κB) 436,
437nutritional support, congenital
heart disease 187Nyquist limit 62
obstructive lung diseaseanesthetic management
283–4lung transplantation 273, 274
off-pump coronary artery bypass(OPCAB) graft surgery114, 114–15
OKT3 268older patientsCPB 346, 352premedication 109–10
one-and-a-half ventricle repair247
one-and-a-quarter ventriclerepair 247
one-lung ventilation (OLV)lung transplantation 277anesthetic management284–5
indications 278techniques 280–3
thoracic aortic surgery311–12, 320
opioidscongenital heart disease 193high-dose technique see
high-dose narcotictechnique
intrathecal 116–17see also fentanyl; morphine;
sufentaniloral hypoglycemic agents 15osmolarity, cardioplegia
solutions 414–15oxidative phosphorylation,
cessation 409oxygenators 328, 328–32, 331,
332assessing function 344ECMO 330, 402
oxygen consumption (Vo2) 6,57–8
determination 22during hypothermia 345myocardial (MVo2) see
myocardial oxygenconsumption
oxygen contentarterial (Cao2) 57mixed venous (Cvo2) 57
oxygen delivery (Do2) 57myocardial see myocardial
oxygen deliverysingle ventricle physiology
228, 228–30, 230useful, to body 230
oxygen excess factor () 230oxygen fraction, inspired (Fio2),
single ventricle physiology230, 231
oxygen partial pressure, arterial(Pao2)
CPB 329
DHCA 427ductus arteriosus closure 168pulmonary vascular resistance
180transposition of great arteries
215oxygen reference flow 332oxygen saturationcerebral (Sco2) 190, 426mixed venous (Svo2) 39continuous monitoring 49,57–8
single ventricle physiology229, 229
pulmonary arterial (PAo2) 39pulmonary venous (Spvo2)
39single ventricle physiology175–6, 229
shunt characterization 23, 38,39, 185
superior vena cava (Ssvco2)
39, 229systemic arterial (Sao2) 39after bidirectional Glenn234, 235–6
intercirculatory mixing174, 176
monitoring 188single ventricle physiology173–6, 228–9
systemic venous 174oxyhemoglobin dissociation
curve, duringhypothermia 426
pacer spikes, IABP control 383pacingCPB termination 355–6, 369electrodes, pulmonary artery
catheters 49heart transplant recipients
265, 266-induced ischemia 27
Paco2 see carbon dioxide, partialpressure in arterial blood
pancuroniumaortic valve surgery 141, 147congenital heart disease 192coronary revascularization
111–12, 113CPB 344–5heart transplantation 261lung transplant surgery 283
panel reactive antibody (PRA)screen 258
Pao2 see oxygen partial pressure,arterial

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 455 — #17
Index 455
paraplegiacomplicating coarctation repair
205complicating thoracic aortic
surgery 314–15, 315paroxysmal cold hemoglobinuria
371partially anomalous pulmonary
venous return (PAPVR)197
partial thromboplastin time,activated (aPTT) 17, 88,368
patent ductus arteriosus (PDA)201, 201–2
anesthetic management 195,201–2
coarctation of aorta 203, 204,205
hypoplastic left heartsyndrome 242
interrupted aortic arch 250TEE 68tetralogy of Fallot with
pulmonary atresia 243,244, 244
transposition of great arteries214, 215, 218
patent foramen ovale (PFO)detection of patency 86mechanical assist device
insertion 403–4total anomalous pulmonary
venous return 221transposition of great arteries
214, 215PCWP see pulmonary capillary
wedge pressurePDA see patent ductus arteriosuspeak pressure gradients,
estimation 83pediatric patientsarterial cannulation 44, 45–6blood volumes 337, 338cardiac catheterization 20cardiovascular physiology
167–71central venous access 46, 48,
189CPB see under
cardiopulmonary bypassDHCA 346, 425, 427–8heart transplantation 252,
258, 260lung transplantation 273,
274, 280mechanical circulatory support
392, 401, 402
myocardial preservationtechniques 422–4
psychological considerations182–3
pulmonary artery catheters49, 50
TEE 65, 87, 191see also congenital heart
disease; neonatesPEEP see positive end expiratory
pressurepentobarbital 188performance factor, heat
exchangers 333perfusion pressure, CPB 323,
349defibrillation 354–5renal function 352
pericardial disease 289–303diastolic pressure–volume
curves 27, 27–8etiology 297–301
pericardial effusions 289, 290–6anesthetic technique 294–6,
295diagnosis 291, 291–2, 292malignant 294, 300–1percutaneous
pericardiocentesis 293–4surgical treatment 294uremic 294, 298
pericardial knock 296pericardial tamponade 289anesthetic technique 294–6,
295diagnosis 53, 291, 291–2hemodynamic effects 290–3,
293percutaneous
pericardiocentesis 293–4surgical treatment 294
pericardial window 294pericardiectomyconstrictive pericarditis 301–2pericardial tamponade 294
pericardiocentesis 293–4, 295pericardioscopy 294pericarditisconstrictive see constrictive
pericarditisidiopathic 299infectious 298–9post-myocardial infarction
299pericardiumaspirated blood from 333closure after cardiac surgery
301, 369compliance curve 290, 290
normal physiology 289–90,290
peripheral intravenous (IV)access, coronaryrevascularization 110
peripheral vascular disease 346,382
peripheral vascular resistance seesystemic vascularresistance
PFO see patent foramen ovalePGI2 see prostacyclinpHpulmonary vascular resistance
180regulation during CPB 347–8see also acid-base management
phentolamine 427phenylephrine 105, 106aortic valve surgery 141–2congenital heart disease 186coronary revascularization
110, 112, 120CPB management 351heart transplantation 262mitral valve surgery 153–4tetralogy of Fallot 209, 212
phosphodiesterase III (PDE III)inhibitors 122, 123
pH-stat acid-base managementCPB 347, 347–8DHCA 426, 427
Pierce–Donachy VAD seeThoratec VAD system
Plasmalyte 337–8plasmapheresis, cold agglutinins
372plasmin 365, 437plasminogen 365platelet aggregometry 89platelet counts 18, 88post-CPB period 364
platelet dysfunction 18–19after CPB 362–3assessment 18congenital heart disease 19medication-induced 18qualitative 18–19uremia-associated 13, 18–19,
298platelet factor 4 (PF4) 341, 372antibodies 372, 373
platelet glycoprotein (GP) IIb/IIIainhibitors 16, 18, 363
platelet glycoprotein (GP) IIb/IIIareceptors 363
platelet transfusions 364pleural pressure 54

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 456 — #18
456 Index
point of care testing (POCT),post-CPB bleeding 369,370
positive end expiratory pressure(PEEP) 54
congenital heart disease 180lung transplantation 284, 285
post-CPB management 358–69antifibrinolytic agents 365–9aortic regurgitation 147–8aortic stenosis 132, 132–3,
142–3ASD, VSD and AVC defects
196, 196, 198–9coagulation tests 88coronary revascularization
119–24decannulation 369Fontan procedure 238–9, 240heart transplantation 264–7hemostatic problems 362–9interrupted aortic arch 250–1lung transplantation 286mitral valve surgery 154–5,
160–1protamine administration
358–62pulmonary atresia with intact
ventricular septum247–8
single ventricle lesions 231–2,234–6
tetralogy of Fallot 212–13total anomalous pulmonary
venous return 222–3transposition of great arteries
219–20truncus arteriosus 249
posterior descending artery 32,33
postoperative analgesia, CABG116–17, 118
postoperative period, myocardialischemia 120
potassiumbalance, termination of CPB
354, 355cardioplegia solutions
412–13, 419reperfusion solutions 417–18replacement 14serum, disturbances 4, 13–14
Potts shunt 209–10prednisone 268pregnancy test 16preinduction phaseaortic surgery 319aortic valve surgery 140,
146–7
congenital heart disease186–92
constrictive pericarditis 302–3coronary revascularization
110–11heart transplantation 260–1lung transplantation 279–80mitral valve surgery 153,
159–60pericardial effusion 295
preloadafter LVAD implantation 405assessment 55, 72–3ejection fraction 30to mechanical circulatory
assist devices 406myocardial oxygen demand
94optimizationcoronary revascularization111, 121
CPB termination 357pressure–volume loops 24, 24reserve 25, 26after CABG 121aortic regurgitation 145,148
aortic stenosis 136, 136–7dilated cardiomyopathy256
mitral regurgitation 158mitral stenosis 150, 151–2,154
neonates 171preload recruitable stroke work
(PRSW) 25, 31, 357premature ventricular
contractions (PVCs) 2, 59premedicationCABG 109–10congenital heart disease
187–8, 188constrictive pericarditis 302heart transplantation 260lung transplantation 278–9mitral regurgitation 159pericardial effusion 295thoracic aortic surgery
318–19valvular heart disease 130–2
preoperative evaluation 1–19CABG patients 106–9cardiovascular 1–10congenital heart disease
182–6endocrine 14–16hematologic 16–19renal function 13–14respiratory 11–13
valvular heart disease 129–30pressure gradientscardiac catheterization
35–6, 36Doppler measurement 63, 64peak, estimation 83
pressure half-time (PHT) 65, 65aortic regurgitation 81mitral stenosis 78, 78
pressure rate quotient (PRQ)104
pressure–volume loops,ventricular 23, 23–6, 24,25, 26
aortic regurgitation 143–5,144
aortic stenosis 135–6, 136mitral regurgitation 28,
156–8, 157mitral stenosis 149, 150
prime, CPB circuit 337–9prior cardiac surgeryheart transplantation after
259–60pericardial disease 301, 302,
303procainamide, congenital heart
disease 186propofolaortic surgery 320aortic valve surgery 140congenital heart disease 193coronary revascularization
113, 114propranolol 104"Tet spells" 209
prostacyclin (PGI2, epoprostenol)aerosolized 181, 267for CPB 18, 374heart transplant recipients
266–7idiopathic pulmonary arterial
hypertension 275lung transplantation 285
prostaglandin E1 (PGE1)
aerosolized 181congenital heart disease 186ductus arteriosus maintenance
168, 170coarctation of aorta 203,205
single ventricle lesions 226,230
tetralogy of Fallot withpulmonary atresia 244
transposition of greatarteries 215, 218
heart transplantation 257,266–7

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 457 — #19
Index 457
lung transplantation 285mitral valve surgery 155post-CPB management 361
prostaglandin E2 (PGE2) 374prosthetic heart valvesmitral position 154, 154patient mismatch (VP-PM)
134special considerations 133–4TEE evaluation 82, 82
protamine 358–65adverse reactions 359–61allergic reactions 360–1, 362causes of impaired hemostasis
after 362–5dose determination methods
88, 359recommended use 361–2
protamine dose assay (PDAO)362
protamine response test (PRT)359
prothrombin time (PT) 17, 88proximal isovolemic surface area
(PISA) method 78pseudoaneurysms, aortic 308pseudonormalization, LV
diastolic function 75, 75pseudoxanthoma elasticum 143psychological considerations,
congenital heart disease182–3
pulmonary alveolar pressure(Palv) 51
pulmonary arterial hypertension(PAH)
aortic regurgitation 145aortic stenosis 138assessment 40–1, 41congenital heart disease
179–80management 180–1
idiopathic (IPAH) 273, 274–5mitral regurgitation 158mitral stenosis 150, 151, 153,
154–5total anomalous pulmonary
venous return 223pulmonary arteryclamping, lung transplantation
285orientation and identity,
TEE 85rupture 59
pulmonary artery (PA)banding
single ventricle lesions 226transposition of great arteries
218
pulmonary artery catheters(PACs) 48–59
aortic valve surgery 140components 48–9coronary revascularization
110–11efficacy and complications
58–9emergency CABG 118, 119heart transplantation 260hemodynamic profiles 58, 59lung transplantation 279measurements 51–8mitral valve surgery 153placement 49–51TEE evaluation 87
pulmonary artery diastolicpressure (PADP) 49, 50
pulmonary artery occlusionpressure (PAOP) 22–3,28
pulmonary artery pressure (PAP)40
mean (mPAP)determination 54Doppler estimation 83resistance calculations 22–3
measurement 54vs. PCWP 53
pulmonary artery systolicpressure (PASP) 49, 50,83
pulmonary artery wedgeangiogram 40
pulmonary atresiawith intact ventricular septum
(PA/IVS) 225, 245–8anatomy 245, 246anesthetic management247
physiology 172, 175, 245–6post-CPB management247–8
surgical therapy 246–7tetralogy of Fallot with
(TOF/PA) 175, 243–5,244
with tricuspid atresia 175,227, 228
pulmonary blood flow (QP) 39,172
effective (QPeff ) 39, 172, 173single ventricle physiology
172, 225–6transposition of great arteries
174, 176tricuspid atresia 228, 241
pulmonary blood flow:systemicblood flow ratio (QP :QS)
39, 174, 176after bidirectional Glenn 234,
236pulmonary arterial
hypertension 40–1single ventricle physiology
228, 228–9, 229, 230, 231total anomalous pulmonary
venous return 221, 222tricuspid atresia 241
pulmonary capillary wedgepressure (PCWP) 51
aortic regurgitation 146, 147aortic surgery 321, 321–2aortic valve surgery 140atrial septum movement
predicting 83A wave 52coronary blood flow 90, 93coronary revascularization
111mean 54measurement 49, 50mitral regurgitation 159–60mitral stenosis 153myocardial ischemia diagnosis
102vs. PAP 53see also left atrial pressure
pulmonary dysfunction 12pulmonary edemaafter lung transplantation 285after pericardial effusion
drainage 296protamine-induced 361reperfusion, lung
transplantation 286total anomalous pulmonary
venous return 222pulmonary fibrosis, idiopathic
273, 274pulmonary function,
preoperative assessment11–13
pulmonary function tests (PFTs)11, 12
pulmonary hypertensionprimary see pulmonary arterial
hypertension (PAH),idiopathic
protamine-induced 360, 361pulmonary infarction 59pulmonary regurgitation (PR)
162–3, 163peak pressure gradient
estimation 83TEE 82

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 458 — #20
458 Index
pulmonary stenosis (TS) 82,162
with restrictive VSD 226tetralogy of Fallot 207, 208transposition of great arteries
214, 215tricuspid atresia with 175,
227, 228pulmonary valve 162–3aortic valve replacement see
Ross procedureassessment, VAD insertion
404TEE evaluation 81–2tetralogy of Fallot 207
pulmonary vascular occlusivedisease (PVOD) 40, 41,275
atrioventricular canal (AVC)defects 200, 201
congenital heart lesions179–80
dilated cardiomyopathy 256mitral stenosis 150, 151post-CPB management 196total anomalous pulmonary
venous return 222, 223transposition of great arteries
215truncus arteriosus 248ventricular septal defects 195
pulmonary vascular resistance(PVR) 22–3
changes at birth 170congenital heart disease
179–80control 180–1
CPB termination 356dilated cardiomyopathy
256–7mitral stenosis 150, 151,
154–5pre-heart transplant
assessment 257pulmonary vascular
resistance:systemicvascular resistance(PVR:SVR) ratio 177–9,178, 179
tetralogy of Fallot 211total anomalous pulmonary
venous return 222transposition of great arteries
218–19pulmonary vasculatureassessment of anatomy 23cardiac catheterization
evaluation 40–1changes at birth 170
congenital heart lesions179–80
pulmonary vasodilator therapycongenital heart disease
180–1heart transplant recipients
266–7mitral valve surgery 155single ventricle lesions 231–2,
235, 239pulmonary veinsobstructioncongenital heart disease180
pulmonary arterialhypertension 40, 41
total anomalous pulmonaryvenous return 221–3
TEE views 68, 69total anomalous return see
total anomalouspulmonary venous return
pulmonary vein wedgeangiogram 40
pulmonary venous congestion,ventricular septal defects195
pulmonary venous flowDoppler assessment 74, 74–5optimizing, single ventricle
lesions 226–7velocity 83
pulmonary venous pressure(Pv) 51
pulmonary venous return(PVR) 59
pulmonic valve see pulmonaryvalve
pulsed-wave (PW) Doppler 62,62
pulse oximetry 42pulse repetition frequency (PRF)
62, 63pulsus paradoxus 292–3, 293pumps, CPB 327, 327–8pupils, assessment 343
Q10 345, 425QP see pulmonary blood flowQP :QS see pulmonary blood
flow:systemic blood flowratio
QS see systemic blood flow
rabbit antithymocyte γ-globulin(RATG) 268
radial artery cannulation 44–5,45
coronary revascularization110
radiation-induced pericardialdisease 300–1
radicular artery of Adamkiewicz312, 314
radionuclide angiography 9–10combined with perfusion
scintigraphy 9equilibrium (ERNA) 9–10first pass (FPRNA) 9–10
radionuclide ventriculography 9ranitidine 260, 279Rashkind–Miller balloon atrial
septostomy 227Rastelli procedure 218, 218rate-pressure product (RPP) 103rectal temperature monitoring
342–3red cell mass (RCM)blood products 338CPB (RCMCPB) 338patient (RCMP) 338
red cells,technetium-99m-labeled9
regional analgesia/anesthesiacoronary revascularization
116–17, 118valve surgery 132
regional low flow perfusion(RLFP) 428
regional wall motionabnormalities (RWMA)102–3
left ventriculography 21–2pre-CABG evaluation 106–7,
109stress-induced 10TEE 71, 73–4
regurgitant fraction 37rejectionheart transplants 271–2lung transplants 287
relaxation, ventricular 28pressure–volume curves 27,
28TEE 74, 75, 75
remaceamide 432renal failureacute postoperative see acute
renal failureplatelet dysfunction 13,
18–19uremic pericardial effusions
294, 298

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 459 — #21
Index 459
renal function 432–4during CPB 350–1, 352, 429effects of aprotinin 368–9preoperative assessment
13–14renal transplant recipients 13renin-angiotensin-aldosterone
system, dilatedcardiomyopathy 254,255
repeat cardiac surgery see priorcardiac surgery
reperfusion injurycardioplegia and 417–18, 418pediatric patients 424transplanted heart 264
resistances 22–3respiratory distress, aortic lesions
309, 311respiratory evaluation 11–13restrictive filling pattern, TEE
74, 75, 75–6retrograde autologous priming
(RAP) 338–9retrograde cerebral perfusion
(RCP) 313, 318, 428–9retrograde coronary sinus
perfusion (RCSP) 421,421–2
reverse redistribution 8Revised Cardiac Risk Index 1, 2rewarming 352–3, 428rheumatic heart diseaseaortic valve 135, 143mitral stenosis 76–7, 149, 149tricuspid stenosis 81–2
rheumatoid arthritis 299–300,302
right atrial appendage (RAA) 85right atrial enlargement (RAE)
4right atrial pressure (RAP) 28,
51–4atrial septum movement
predicting 83A wave 51C wave 52mean 54measurement 50, 51V wave 52–3X descent see X descentY descent see Y descent
right atrium (RA)blood flow during CPB 334cannulation, for CPB
324–5identification using TEE 85
right coronary artery 32, 33right heart catheterization 20
right-to-left shunts 172, 173quantitation 39–40
right ventricle (RV), TEEevaluation 85
right ventricle-dependentcoronary circulation(RVDCC) 246, 247
right ventricular assist devices(RVAD) 376, 379
after LVAD implantation 405,406
cardiac output determination407
central venous line insertion408
insertion 404Thoratec system 391–2
right ventricular ejection fraction(RVEF) 56
right ventricular end-diastolicpressure (RVEDP) 28, 54
right ventricular end-diastolicvolume (RVEDV) 56
right ventricular end-systolicvolume (RVESV) 56
right ventricular failureafter LVAD implantation 405,
406dilated cardiomyopathy 256heart transplant recipients
265, 266mitral regurgitation 158, 160mitral stenosis 150, 151, 153,
154–5tricuspid valvular disease 162
right ventricular functionaortic regurgitation 145aortic stenosis 138dilated cardiomyopathy
256–7heart transplant recipients
265idiopathic pulmonary arterial
hypertension 275lung transplantation 284, 286LVAD implantation and
404–6mitral regurgitation 158mitral stenosis 150, 151pre-CABG evaluation 107TEE assessment 76transplanted heart 269–70
right ventricular hypertrophy(RVH) 4
right ventricular outflow tract(RVOT)
obstruction, tetralogy of Fallot206–7, 212
TEE 71, 84
right ventricular stroke workindex (RVSWI) 59
right ventricular systolic pressure83
Ringer’s lactate solution 337–8rocuroniumaortic surgery 319congenital heart disease 193coronary revascularization
113heart transplantation 261lung transplantation 283
Rosenthal syndrome 17Ross procedure 133, 164
saline-contrast echocardiography86
Sano procedure 242, 243saphenous vein graftsagents affecting flow through
120cardioplegia infusion 419–20
saturation see oxygen saturationsaturation threshold (SatThresh)
229–30Scimitar syndrome 197scopolamine 109, 119, 272Senning procedure 21614C-serotonin release assay
(SRA) 373Sestamibi imaging 7, 8–9sevofluranecardioplegia solutions 418congenital heart disease 192,
193heart transplantation 261lung transplantation 283myocardial protection 115,
116shockcardiogenic see cardiogenic
shockcatecholamine resistant
vasodilatory (CRVS) 407shunts 171–2, 173cardiac catheterization 38–40classification 177–9complex 177–9, 178, 179dependent 177Gott 313, 316localization 38mechanical assist device
insertion 403–4palliative, tetralogy of Fallot
209–10, 210quantification 39–40restrictive and nonrestrictive
177, 177

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 460 — #22
460 Index
shunts (Cont’d)saline-contrast
echocardiography 86saturation data 23, 38, 39simple 177, 177, 178TEE 85–6see also aortopulmonary
shunts, surgical; superiorcavopulmonary shunt
sickle cell disease 372sildenafil 181single ventricle lesions 175,
224–39Fontan procedure see Fontan
procedureinitial procedures 226–31management of single
ventricle physiology228–30, 232–4, 233
staged approach to Fontanprocedure 225, 225–36
superior cavopulmonaryshunt/bidirectional Glenn232–6
two-ventricle repair 224–5single ventricle physiology
172–6, 176anatomic subtypes 175management 228–30, 232–4,
233myocardial ischemia 182shunts 179
sinoatrial (SA) node dysfunction,heart transplant recipients265
sinus venosus defects 197sirolimus 268smoking 12Society of Cardiovascular
Anesthesiologistsmitral valve classification
148–9recommended TEE views 67
sodium, cardioplegia solutions414
sodium nitroprusside seenitroprusside, sodium
somatosensory-evokedpotentials (SSEPs)314–15, 316
spinal cordblood supply 312, 314ischemiacoarctation repair 205, 206intraoperative monitoring314–15, 316
thoracic aorta surgery312–15, 315
spinal cord perfusion pressure(SCPP) 312–14, 315
spirometry 11square root sign, constrictive
pericarditis 297, 297Stanford classification, aortic
dissection 306, 306stents, endovascular, coarctation
of aorta 204–5steroids see corticosteroidsstiffness see elastancestress echocardiography 7, 10stress testing 5–7exercise 6–7methods compared 7pharmacological 5–6
stroke 430–1, 432stroke index (SI) 59stroke volume (SV) 59angiographic measurement
21aortic stenosis 135, 136, 137,
138–40, 139dilated cardiomyopathy 254,
256Doppler measurement 64pressure–volume loops 25–6,
26right ventricular ejection
fraction (RVEF) catheters56
stroke work (SW) 23, 24, 31ST segment changes 7, 43–4stunned myocardium 8subaortic stenosis 218, 224subclavian vein cannulation 46subendocardial perfusioncongenital heart disease
181–2during CPB 349, 350single ventricle physiology
230subendocardial pressure,
congenital heart disease182
succinylcholineaortic regurgitation 147aortic surgery 320congenital heart disease 193emergency CABG 118heart transplantation 261lung transplantation 283mitral valve surgery 160
suction, cardiotomy 333sufentanilaortic surgery 319, 320aortic valve surgery 140–1,
142, 147congenital heart disease 193
coronary revascularization111, 112
emergency CABG 118heart transplantation 261,
262lung transplantation 283mitral valve surgery 154, 160pericardial disease 295–6, 303
superior cavopulmonary shunt(bidirectional Glennprocedure; BDG) 225,232–6
anatomy 232, 235anesthetic management
232–4Fontan procedure after 237–8post-CPB management 234–6vs. aortopulmonary shunt
232, 234superior vena cava (SVC)cannulation for CPB 324poor drainage, CPB 325–6, 343pressure, after bidirectional
Glenn 236TEE views 68, 69
supravalvular aortic stenosis(SVAS), congenital 224
sympathetic nervous systemdevelopment at birth 171stimulation, congenital heart
disease 181transplanted heart 268–9
syphilis 371systemic blood flow (QS) 39, 172during CPB 345–6, 346effective (QSeff ) 39, 172, 173optimizing, single ventricle
lesions 227–8single ventricle physiology
172transposition of great arteries
174, 176systemic inflammatory response
syndrome (SIRS) 433,434–7, 435
interventions to modulate436, 436–7
systemic lupus erythematosus299
systemic vascular resistance(SVR) 22–3, 24, 59
on CPB 346, 351CPB termination 356, 357
systole, length, aortic stenosis138, 138
systolic function 30–2, 34impaired, newly transplanted
heart 264–5

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 461 — #23
Index 461
pre-CABG evaluation 106–7,109
TEE assessment 72–3see also left ventricular systolic
(dys)function; rightventricular function
TA see tricuspid atresiatachycardiaaortic regurgitation 146aortic stenosis 138, 138, 141,
143coronary revascularization
112heart transplantation 262myocardial oxygen balance
94–5, 95, 104preoperative 2treatment 104–5
tacrolimus 268TAH see total artificial hearttamponade, pericardial see
pericardial tamponadeTandemHeart device 376, 398,
399technetium-99m 9technetium-99m-labeled red
cells 9technetium-99m
methoxyisobutyl isonitrilesee Sestamibi
TEE see transesophagealechocardiography
temperatureafterdrop, after CPB 352–3CPB 345, 346DHCA 427monitoring 43CPB 342–3pediatric patients 189–90during rewarming 352
myocardial preservation 413,422
see also hypothermiatetralogy of Fallot (TOF) 206–13anatomy 206–7, 207, 208anesthetic management
211–12cyanotic 179, 207hypoxic or hypercyanotic
episodes ("Tet spells")208–9
physiology 179, 207post-CPB management
212–13preoperative evaluation
11–12
with pulmonary atresia(TOF/PA) 175, 243–5,244
shunting 177–9single ventricle physiology
172, 175surgical procedures 209–11
TGA see transposition of greatarteries
thallium-201 imaging 7, 8THAM 413, 414, 418theophylline 12–13thermodilution (TD) technique,
cardiac output 21–2,55–7
thiopentalaortic surgery 319–20contraindications 193, 283for DHCA 429
thoracic aorta see aortaThoratec VAD system 376,
390–2, 391indications 378insertion 391management 391–2in parallel 379
thrombin 365, 434thrombin inhibitors, direct 18,
373–4thrombin time, high dose (HiTT)
88thrombocytopenia 18, 88heparin-induced (HIT) 18,
372–4, 373post-CPB period 364
thromboelastography (TEG) 89,89, 363
thromboembolism, hearttransplant recipients 259
thrombosis 96, 97thyroid hormone replacement
16ticlopidine 363tirofiban 18, 363, 374tissue Doppler 75, 76tissue plasminogen activator
(t-PA) 365tobacco use 12total anomalous pulmonary
venous return (TAPVR)173, 220–3
anatomy 220–1, 221management 222–3
total artificial heart (TAH) 377,385–90, 388, 389
anesthetic management ofrecipients 406, 407, 408
bridge to heart transplantation259, 385–6, 403
insertion 388–9, 403–4management 389, 389–90,
390total cavopulmonary connection
(TCPC) see Fontanprocedure
total spinal anesthesia, coronaryrevascularization 117
tracheal intubationaortic valve surgery 141congenital heart disease 192coronary revascularization
112thoracic aortic surgery 320
tranexamic acid (TXA) 365, 367dosage and administration
366efficacy 368
transbronchial biopsies 287transcranial Doppler (TCD)
190–1transesophageal
echocardiography (TEE)10, 59–87
after valve surgery 82, 132,133
aortic lesions 309–11, 310,310
aortic surgery 321, 321–2atrial septum movement 83basic physics 60, 60–1complications 87congenital heart disease
84–6, 191contraindications 87CPB cannulas 87, 344Doppler spectra measurements
64–5, 65examination 72heart transplantation 260–1,
266imaging techniques 61–3intracardiac air 82–3, 353intracardiac and endovascular
catheters 86–7intracardiac pressure estimates
83lung transplantation 279–80LV diastolic function 74–6LV systolic function, ejection
fraction and preload72–3
mechanical assist devices404, 406, 408
myocardial ischemia 102–3pericardial effusion 291, 296probes 65–6, 66insertion 66

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 462 — #24
462 Index
transesophagealechocardiography (TEE)(Cont’d)
pulmonary and hepaticvenous blood flow 83
regional wall motion analysis73–4
RV function 76saline contrast 86thoracic aorta 83–4transposition of great arteries
85, 220valvular heart disease 76–82,
130, 131views 67, 67–72, 68, 69, 70,
71, 72transfusion of blood products
429–30interventions to limit 430lung transplantation 284mechanical assist device
insertion 403post-CPB bleeding 369, 370risks 430thoracic aortic surgery 319,
320transmembrane pressure
gradient (TMP) 335transposition of great arteries
(TGA) 213–20anatomy 213, 213–14, 214anesthetic management
218–19dextro- (D-TGA) 213, 213–14physiology 174, 176, 214–16post-CPB management
219–20surgical procedures 216,
216–18, 217TEE 85, 220tricuspid atresia with 227,
228transpulmonary gradient (TPG)
23single ventricle lesions 235,
236, 239tricuspid atresia (TA) 239–41anatomy 239–41classification 227, 228, 241management 241physiology 172, 175, 241staged approach to Fontan
procedure 225, 225–36tricuspid regurgitation (TR) 162after LVAD implantation 405cardiac catheterization 38cardiac output determination
57causes 162, 162
peak pressure gradientestimation 83
TEE 81, 81, 162tricuspid stenosis (TS) 81–2, 162tricuspid valve 161–2assessment, VAD insertion
404TEE 68, 81–2
triiodothyronine (T3) 258triple index (TI) 103trisomy 21 (Down syndrome)
11, 185, 200tromethamine (THAM) solution
413, 414, 418troponin I 421, 421truncus arteriosus 248–9anatomy 248, 248physiology 172, 175, 248
tuberculosis, pericardial disease296, 298
Turner syndrome 20222q11.2 chromosomal deletion
185two-dimensional (2-D)
echocardiography 61,61–2
two-ventricle repair 224–5,247, 248
tympanic membrane,temperature monitoring342
ultrafiltrationcontinuous (CUF) 335, 336dilutional (DUF) 336, 336–7modified (MUF) 335–6, 337zero-balance (ZBUF) 336,
336–7ultrafiltrators 335–7ultrasoundbasic physics 60, 60–1epiaortic scanning 83, 84guidance, internal jugular vein
cannulation 46, 47, 47intravascular (IVUS), cardiac
allograft vasculopathy270
umbilical arteryarterial pressure monitoring
46, 188cardiac catheterization via 20
umbilical vein 20, 167univentricular lesions see single
ventricle lesionsUnivent tube 281–2, 320uremiapericardial effusions 294, 298platelet dysfunction 13,
18–19, 298
urinalysis 16urine output, during CPB 350–1,
352
VACTERL association 185vacuum assisted venous drainage
(VAVD) 326VADs see ventricular assist
devicesvagolytic/vagotonic agents, heart
transplant recipients 272Valsalva maneuver 86valve areascardiac catheterization
evaluation 35, 36–7Doppler measurement 64–5
valve prosthesis-patientmismatch (VP-PM) 134
valvular heart disease 129–66alternatives to surgical repair
166, 166anesthesia induction and
maintenance 132cardiac catheterization 23,
35–8long-term prognosis 134monitoring 130, 131multiple valve lesions 163–4postoperative TEE 82, 132,
133premedication 130–2preoperative evaluation 5,
129–30, 130previously undiagnosed, found
during CABG 165–6pulmonary assessment 12special considerations 133–4TEE monitoring 76–82, 130,
131weaning from bypass and
post-bypass period132–3, 354
vasectomy, protamine allergy360
vasodilator therapy 105aortic regurgitation 146, 147aortic surgery 319during CPB 351–2, 353DHCA management 427mitral valve surgery 154, 160see also pulmonary vasodilator
therapyvasopressin 110, 259, 407VATER association 185vecuroniumaortic surgery 319aortic valve surgery 141, 147congenital heart disease
192–3

Alice Nelson Dinardo: “index” — 2007/7/16 — 12:41 — page 463 — #25
Index 463
coronary revascularization112, 113
heart transplantation 261lung transplantation 283
velocardiofacial syndrome 185velocity, red blood cell flow
60–1velocity–time integral (VTI)
64–5, 65vena contracta 79venous cannulas for CPB 324–5placement 342removal 369TEE evaluation 87
venous drainage, for CPB 323–6assessment 343assisted 326
ventilationcirculatory assist device
recipients 407congenital heart disease 186,
192discontinuation, start of CPB
344lung transplant recipients 286monitoring methods 42resumption, after CPB 356thoracic aortic lesions 311–12
ventilatory interventionscontrol of PVR 180, 181, 239,
267single ventricle physiology
230–1, 234–5venting, during CPB 333–5,
334, 344, 422ventricular arrhythmias, heart
transplant recipients 259,271
ventricular assist devices (VAD)376, 377, 379, 390–401
anesthetic management ofrecipients 404–8
insertion 403–4in parallel/in series 379, 379TEE evaluation 87triggering modes/percentage
of systole 380–1see also left ventricular assist
devices; specific devicesventricular distension, during
CPBmyocardial oxygen delivery
349venting 333–4, 344
ventricular failure 375see also heart failure
ventricular fibrillation, duringCPB 349, 350, 350, 351
ventricular remodeling, dilatedcardiomyopathy 253–4
ventricular rupture, mitral valvereplacement 155
ventricular septal defects (VSD)194–6
anatomy 194, 194anesthetic management 195,
195physiology 194–5post-CPB management 196,
196repaired, TEE evaluation 86,
191surgical therapy 195tetralogy of Fallot 207, 207,
211, 212transposition of great arteries
214, 215tricuspid atresia with 227,
228video-assisted thoracoscopic
surgery (VATS) 201, 202viral pericarditis 298vital capacity (VC) 12Vo2max 6
volatile anesthetic agentsaortic stenosis 142coronary revascularization
113CPB management 351–2, 353myocardial protection 99,
100, 115–16, 116see also individual agents
volume infusion see fluidmanagement
von Willebrand factor (vWF)363, 364–5
VSD see ventricular septal defectsV waves 51, 52–3mitral regurgitation 37–8, 52,
53
wall motion abnormalities seeregional wall motionabnormalities
wall segmentsblood supply 32, 32–3left ventriculography 21, 31,
32TEE imaging 73, 73
wall tension, myocardial 93–4neonates 423
Waterston shunt 209–10, 210Williams–Beurin syndrome 224
X descent 51, 53–4, 290, 290constrictive pericarditis 297,
297pericardial tamponade 291,
291
Y descent 51, 53–4, 290, 290constrictive pericarditis 297,
297pericardial tamponade 291,
291