Embed Size (px)
Citation preview

INNOVATION
COMMERCE -YOUR BLUEPRINTFOR SUCCESS
ENABLING BETTER HEALTH
FROM IDEA TO REVENUE
ENABLING BETTER HEALTH FROM IDEA
TO REVENUE
INNOVATION
COMMERCE -YOUR BLUEPRINT
FOR SUCCESS
www.qmed-consulting.com

©2013 Qmed Consulting
Part 1:
Introduction to medical device EU funding and reimbursement -What is reimbursement?
Part 2:
Review of Germany, France, UK and Spain´s healthcare systems by Stephan Heumann
©2013 Qmed Consulting
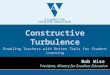
The Fourth Hurdle
Reimbursementor
Funding
Market Authorisation (CE Mark) Fourth Hurdle forMarket Access
Safety EfficacyQuality
The fourth hurdle
Regulatory StrategyDesign Phase
©2013 Qmed Consulting
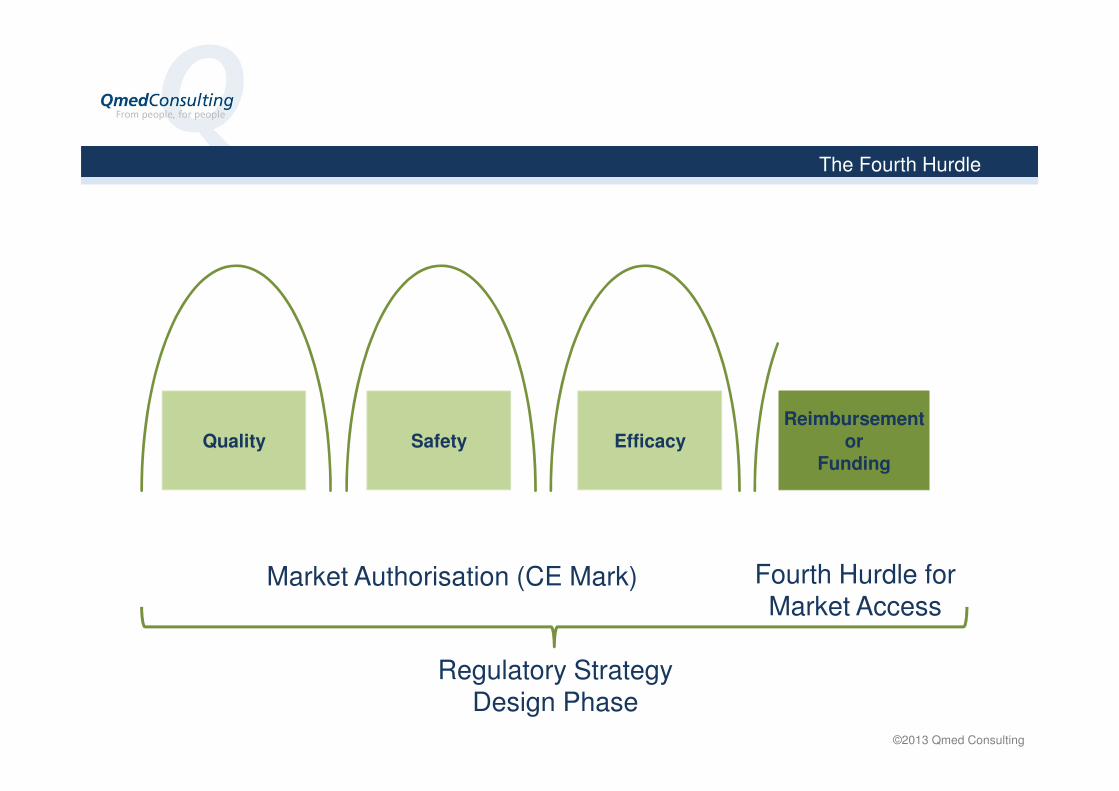
Major Global Themes
Major markets are struggling with rising health care costs
↓
Politicians say “STOP, we want more economic treatment”
↓
Health systems are looking closely at new (and sometimes old) technologies before they’ll decide to reimburse
↓
The demands for evidence (clinical and cost effectiveness) are increasing
- The most significant issues arise with new technologies
©2013 Qmed Consulting
Demand for Evidence
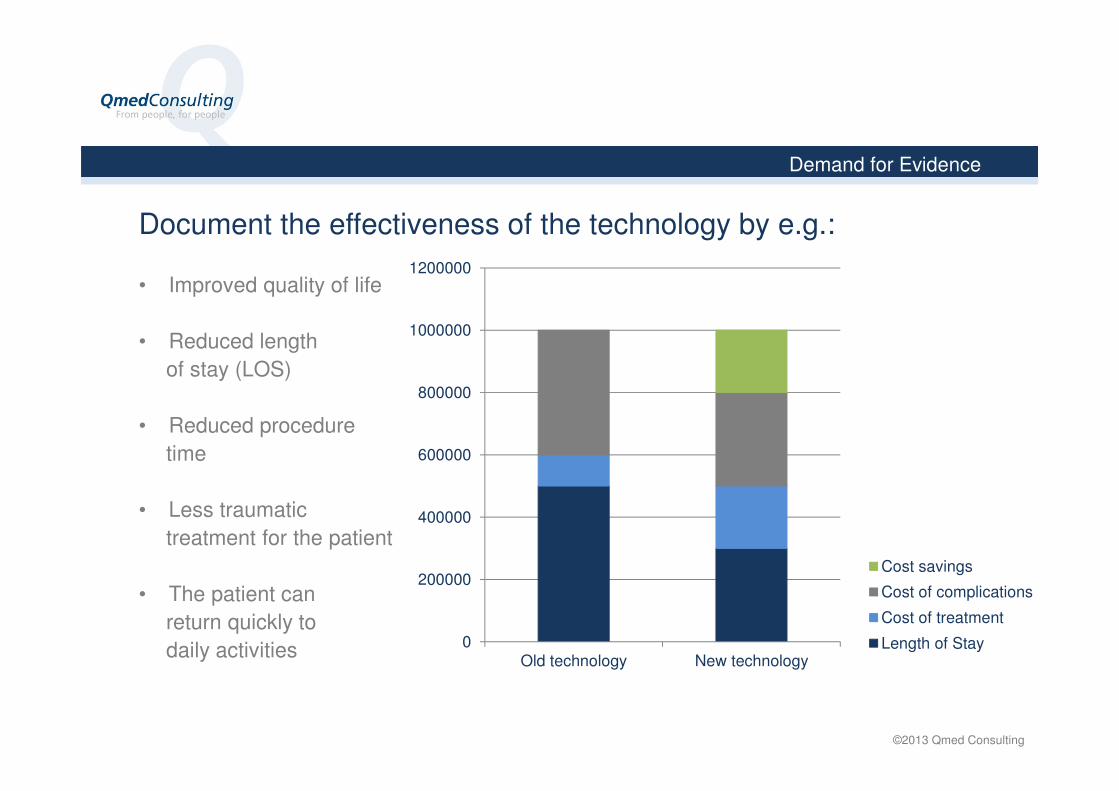
Document the effectiveness of the technology by e.g.:
• Improved quality of life
• Reduced length
of stay (LOS)
• Reduced procedure
time
• Less traumatic
treatment for the patient
• The patient can
return quickly to
daily activities 0
200000
400000
600000
800000
1000000
1200000
Old technology New technology
Cost savings
Cost of complications
Cost of treatment
Length of Stay
©2013 Qmed Consulting
What is Reimbursement?
”Reimbursement” ≠ ”Funding”
”Reimbursement” is about how healthcare providers are paidfor the services they provide:
No Reimbursement = No Payment To Provider
”Reimbursement” varies from country to country and someplaces from healthcare plan to healthcare plan
Hvad er reimbursement?
©2013 Qmed Consulting
What is Reimbursement?
Hvad er reimbursement?
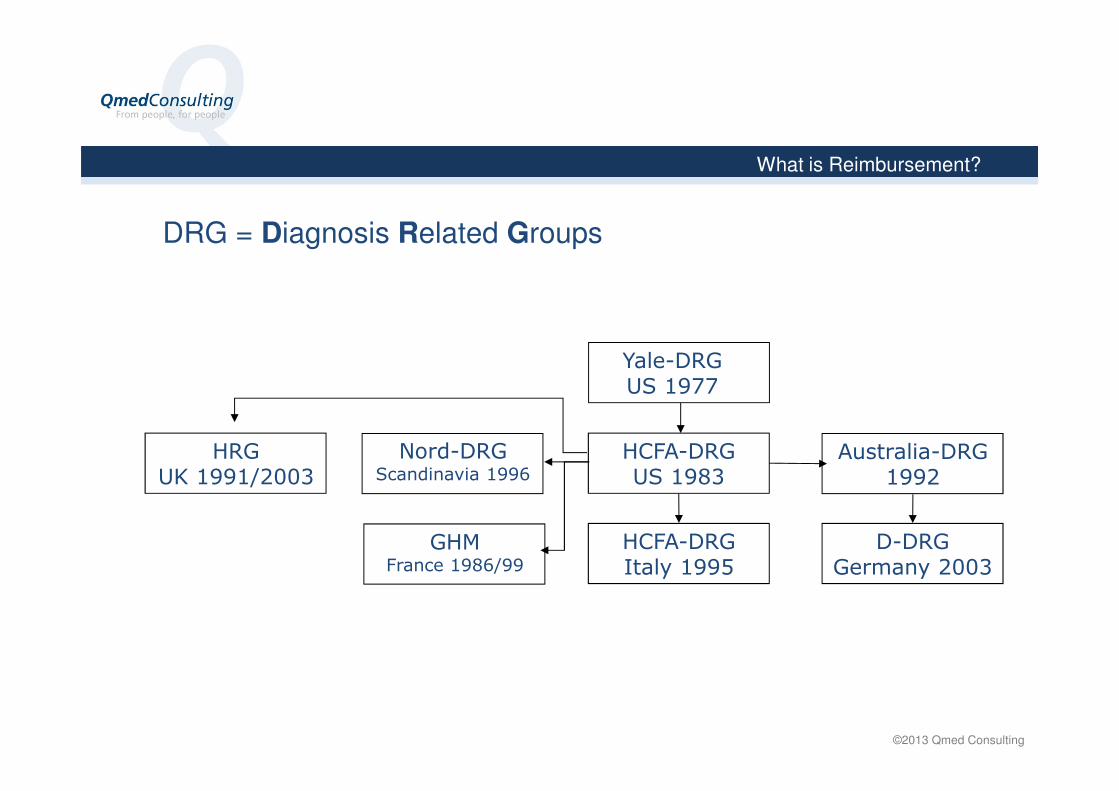
DRG = Diagnosis Related Groups
HCFA-DRGUS 1983
Yale-DRGUS 1977
HCFA-DRGItaly 1995
Australia-DRG1992
D-DRGGermany 2003
Nord-DRGScandinavia 1996
GHMFrance 1986/99
HRGUK 1991/2003

©2013 Qmed Consulting
What is DRG?
DRG = Diagnosis Related Groups,
Categorization of patients
Requirements:- Clinically meaningful
Discharges (or visits) that are clinically somehow alike – both diagnosis and
treatment
- Resource homogeneousThe discharges (visits) have to cost fairly the same
- Not too many groups (average), normally 500-1.000 groups/country, applied in different ways
Only a few discharges give high uncertainty when average costs are
calculated

©2013 Qmed Consulting
What is Reimbursement? – Markers in the DRG System
Hvad er reimbursement?
DRG
Diagnosis (ICD)
Procedure
Complications
Gender, <18 y. and co-morbidities
Status at Discharge
Length of stay

©2013 Qmed Consulting
Summary
”Reimbursement” is about how the ”provider” is paid by the ”payer” for the services they deliver
”Reimbursement” varies from country to country
DRG ⇒ Payment of a predetermined lump sum paid to “provider" by the "payer"
DRG = diagnosis code + procedure code + othersDiagnosis code = ICD-kode, International Classification of Diseases, publicated by WHO
Procedure code, varies from country to country
Others, e.g. LOS, complications, co-morbidities

©2013 Qmed Consulting
Summary
The payment covers the full consumption of resources during hospitalization (ward, personnel, devices, medicine, radiology, operating room, etc.)
Some healthcare systems have ”pass-through” systemer ⇒additional payment for some medical devices.

©2013 Qmed Consulting
Stephan Heumann
- Qmed Commercial Healthcare Expert
- Responsible for Qmed’ reimbursement projects
- Experience from international hospital systems
- Commercial experience, medical devices
Review of Germany, France, UK and Spain´s healthcare systems by Stephan Heumann

©2013 Qmed Consulting
Qmed Consulting ApS
Ørnevej 2 • 4600 Køge
TEL.: +45 65 64 10 10Mail: [email protected]
www.qmed-consulting.com
1 ©2013 Solve2Access, All rights reserved 1 ©2013 Solve2Access, All rights reserved
Go-home-meeting:
Medical device reimbursement systems in the EU Medicoindustrien and Medico Innovation
Wednesday, November 27, 2013, Lyngby, Denmark
Presented by: Stephan Heumann, Founder of solve2access and Commercial Healthcare Expert at QmedConsulting

2 ©2013 Solve2Access, All rights reserved 2
Solve2Access Holding B.V – Member of the Global Alliance Team
Sung koo Tompot Stephan Heumann
“”We help medical companies to demonstrate the value of their products, develop market access and increase sales””
Making a difference with a long history in the healthcare sector. We have extensive knowledge & experience in reimbursement, clinical and economic evidence and HTA strategies. Helping companies to implement the right strategy to access the market with their product is our goal.
We are Commercial Healthcare Experts at QmedConsulting
3 ©2013 Solve2Access, All rights reserved 3 3 ©2013 Solve2Access, All rights reserved 3
The healthcare market is evolving
Ageing population demanding solutions
High rate of innovation
and product launches
Pressure of Health Care
budget constraints Economic trend
Social trend
Innovation trend
4 ©2013 Solve2Access, All rights reserved 4 ©2013 Solve2Access, All rights reserved
Barriers for medical innovation
EVIDENCE
VALUE
REIMBURSEMENT
MARKET
Revenues from
customers
Medical products

5 ©2013 Solve2Access, All rights reserved 5 ©2013 Solve2Access, All rights reserved
Become opportunities for companies

6 6
Different markets require specific actions
Germany England
France Italy Spain
7 ©2013 Solve2Access, All rights reserved 7
Reimbursement as a part of the Market Access Strategy
Market Access = CE Mark or AHRQ approval + HTA process + Reimbursement
Market Access is the process in which a company brings a medical product to market which becomes available for patients. Access is defined as a patient's ability to obtain medical care. There is a process to get the allowance to use a product on a market (CE Mark, AHRQ, etc.)
Because of the limited budgets in each country, HTA bodies approve on a national level if the
treatment, device or drug should be covered for reimbursement
If the product has the permission to be used, someone has to pay for it
Reimbursement is necessary, but not for all products

8 ©2013 Solve2Access, All rights reserved 8
Why does it make sense to think about the different reimbursement requirements?
Different countries requires different market access keys
General EU or country specific laws and regulations for medical devices EC Directive 93/42, 98/79, 90/385 EEC etc. Medizinproduktegesetz (MPG; Germany), Dänemark?
Country specific HTA (Health Technology Assessment) HAS France, GBA Germany, NICE England, AHRQ USA, mini HTA Denmark (no national HTA anymore) etc.
Country specific reimbursement G-DRG and EBM Germany HRG and Drug Tariff list England Swiss DRG DK-DRG
9 ©2013 Solve2Access, All rights reserved 9
Why does it make sense to think about the different reimbursement requirements?
The huge one US market vs.
The different EU markets
All markets have
different requirements for accessing the market
10 ©2013 Solve2Access, All rights reserved 10 ©2013 Solve2Access, All rights reserved
What is Reimbursement?
• For Medical Device- and Pharma companies there is no automatisms to get reimbursement after CE-market
• New products can fit into existing or it is necessary to apply for new reimbursement or there will be no reimbursement
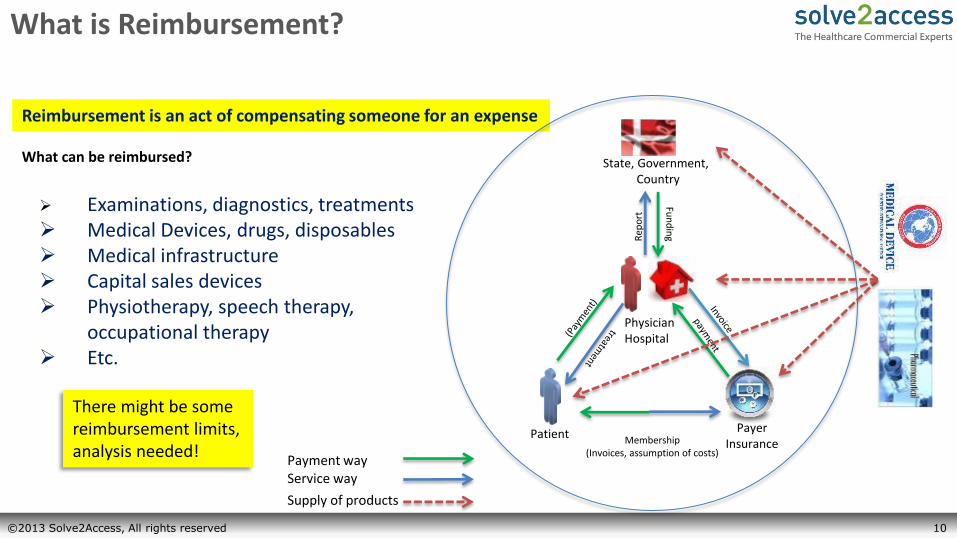
Reimbursement is an act of compensating someone for an expense
Examinations, diagnostics, treatments Medical Devices, drugs, disposables Medical infrastructure Capital sales devices Physiotherapy, speech therapy,
occupational therapy Etc.
Patient
Physician Hospital
Payer Insurance
State, Government, Country
Membership (Invoices, assumption of costs)
Fun
din
g Rep
ort
Payment way Service way
Supply of products
What can be reimbursed?
There might be some reimbursement limits, analysis needed!

11 ©2013 Solve2Access, All rights reserved 11 ©2013 Solve2Access, All rights reserved
Different elements of Reimbursement
• Reimbursement via HTA ( Health Technology Assessment)
• Reimbursement via DRG (Diagnostic Related Groups)
12 ©2013 Solve2Access, All rights reserved 12 ©2013 Solve2Access, All rights reserved
Economic + Clinical Evidence = Reimbursement
• Decisions on the use of technology are made at all levels in the health care system. They often include a unification of complicated medical, patient-related, organizational and economic information in a context where there may also be ethical problems. …
• Decisions must be made on an evidence-based foundation where all relevant circumstances and consequences are systematically illustrated by means of scientific methods.

13 ©2013 Solve2Access, All rights reserved 13 ©2013 Solve2Access, All rights reserved
HTA Process in Germany - What is the GBA?
• The Federal Joint Committee (G-BA) is the highest decision-making body of the joint self-government of physicians, dentists, hospitals and health insurance funds in Germany.
• It issues directives for the benefit catalogue of the statutory health insurance funds (GKV) for more than 70 million insured persons and thus specifies which services in medical care are reimbursed by the GKV. In addition, the G-BA specifies measures for quality assurance in inpatient and outpatient areas of the health care system.
14 ©2013 Solve2Access, All rights reserved 14 ©2013 Solve2Access, All rights reserved
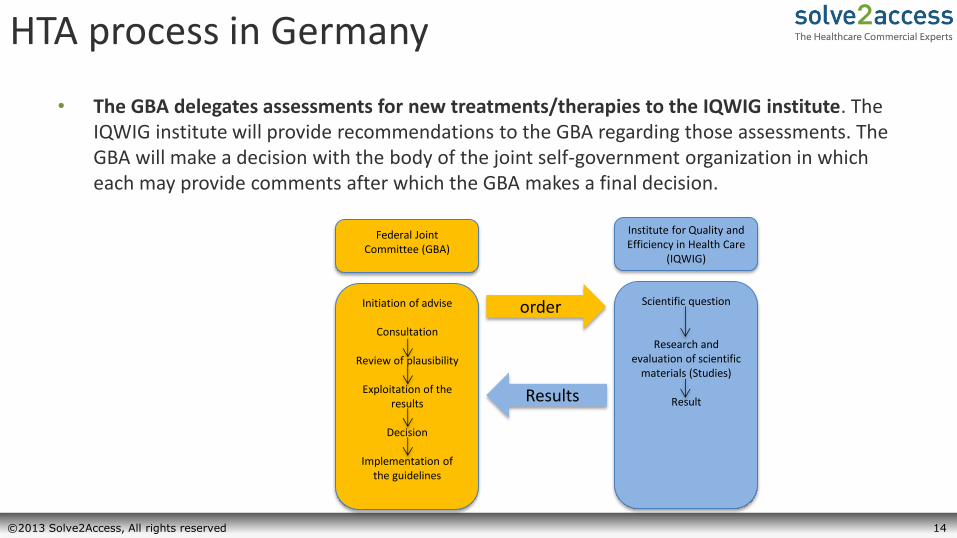
HTA process in Germany
• The GBA delegates assessments for new treatments/therapies to the IQWIG institute. The IQWIG institute will provide recommendations to the GBA regarding those assessments. The GBA will make a decision with the body of the joint self-government organization in which each may provide comments after which the GBA makes a final decision.
Federal Joint Committee (GBA)
Initiation of advise
Consultation
Review of plausibility
Exploitation of the results
Decision
Implementation of
the guidelines
Scientific question
Research and evaluation of scientific
materials (Studies)
Result
order
Institute for Quality and Efficiency in Health Care
(IQWIG)
Results
15 ©2013 Solve2Access, All rights reserved
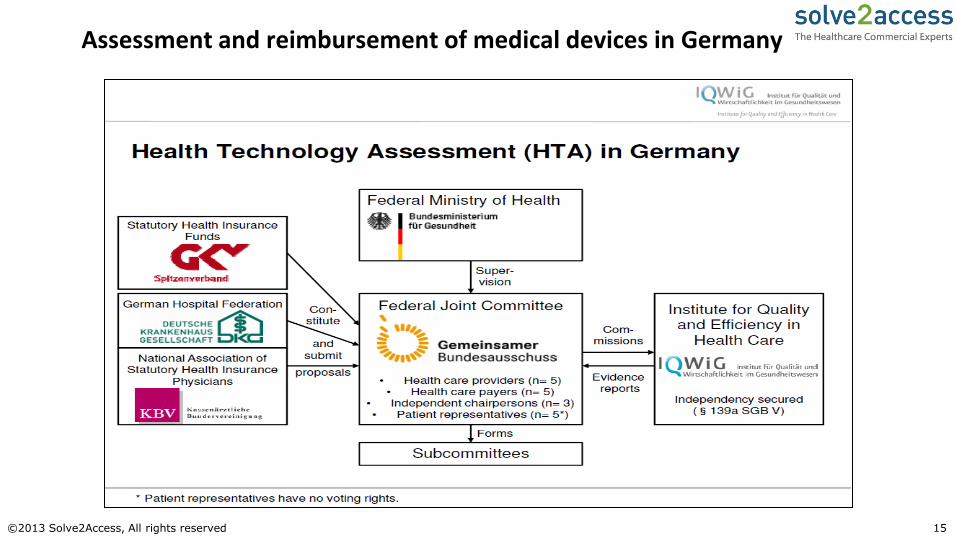
Assessment and reimbursement of medical devices in Germany

16 ©2013 Solve2Access, All rights reserved

17 ©2013 Solve2Access, All rights reserved 17 ©2013 Solve2Access, All rights reserved
What should not happen in a publication?
What kind of costs? - Doctor time - Nurse time - Treatment time - Operation time - Intensive care unit time - Materials - … - Compare to what other
treatment method
It is important to demonstrate the value of your product to get it reimbursed in the entire treatment process / clinical pathway
The cost of pressure ulcers in the UK, GERRY BENNETT, CAROL DEALEY, JOHN POSNETT, Age and Ageing 2004; 33: 230–235, DOI: 10.1093/ageing/afh086, Age and Ageing Vol. 33 No. 3 British Geriatrics Society 2004; all rights reserved
18 ©2013 Solve2Access, All rights reserved 18 ©2013 Solve2Access, All rights reserved
Is the evidence to obtain CE mark sufficient to achieve market access or reimbursement?
Functionality Safety Risk assessment
Medical necessity Therapeutic benefit Economic benefits
19 ©2013 Solve2Access, All rights reserved 19 ©2013 Solve2Access, All rights reserved
Different elements of Reimbursement
• Reimbursement via HTA ( Health Technology Assessment)
• Reimbursement via DRG (Diagnostic Related Groups)

20 ©2013 Solve2Access, All rights reserved 20 ©2013 Solve2Access, All rights reserved
DRG’s in general!
Side diagnosis
Side diagnosis
Side diagnosis
Side diagnosis
Age
Gender
Ventilation hrs.
Birth weight*
Main diagnosis
Procedure
Procedure
Patient exit reason (normal, died, transferred)
The combination of these components lead into hundred sometimes more then thousand different DRGs. Your product can be classified into an ICD or Procedure code and may lead into a higher reimbursement/DRG.

21 ©2013 Solve2Access, All rights reserved 21 ©2013 Solve2Access, All rights reserved
Nordic DRG

22 ©2013 Solve2Access, All rights reserved 22 ©2013 Solve2Access, All rights reserved
Reimbursement Analysis – example NORD DRG

23 ©2013 Solve2Access, All rights reserved 23 ©2013 Solve2Access, All rights reserved
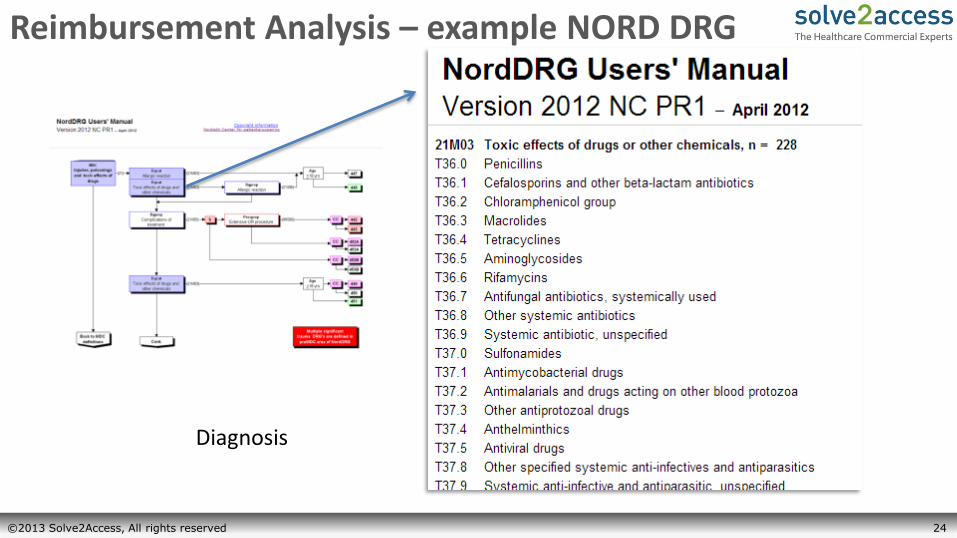
Reimbursement Analysis – example NORD DRG
With a click in the different boxes you get more information's about the procedures and diagnosis which guide into the different DRGs
24 ©2013 Solve2Access, All rights reserved 24 ©2013 Solve2Access, All rights reserved
Reimbursement Analysis – example NORD DRG
Diagnosis

25 ©2013 Solve2Access, All rights reserved 25 ©2013 Solve2Access, All rights reserved
Reimbursement Analysis – example NORD DRG
Procedures

26 ©2013 Solve2Access, All rights reserved 26 ©2013 Solve2Access, All rights reserved
Reimbursement Analysis – example NORD DRG
Clinical Pathways
27 ©2013 Solve2Access, All rights reserved 27 ©2013 Solve2Access, All rights reserved
Reimbursement Analysis – example NORD DRG
These information's / data's show us, in which North DRG medical devices, pharmaceuticals and clinical pathways are reimbursed or can be reimbursed in the future. When it is identified, where your product should be placed, it is possible to apply for reimbursement via the North DRGs. It is an complex process and you need to have:
- An understanding where your product is placed in the treatment process / Nord DRG process
- A strategy where it could be placed in the future - An understanding of the diagnosis and procedure codes
application process - An understanding of the cost calculation process - Strong evidence to apply for reimbursement - An network which will make it happen
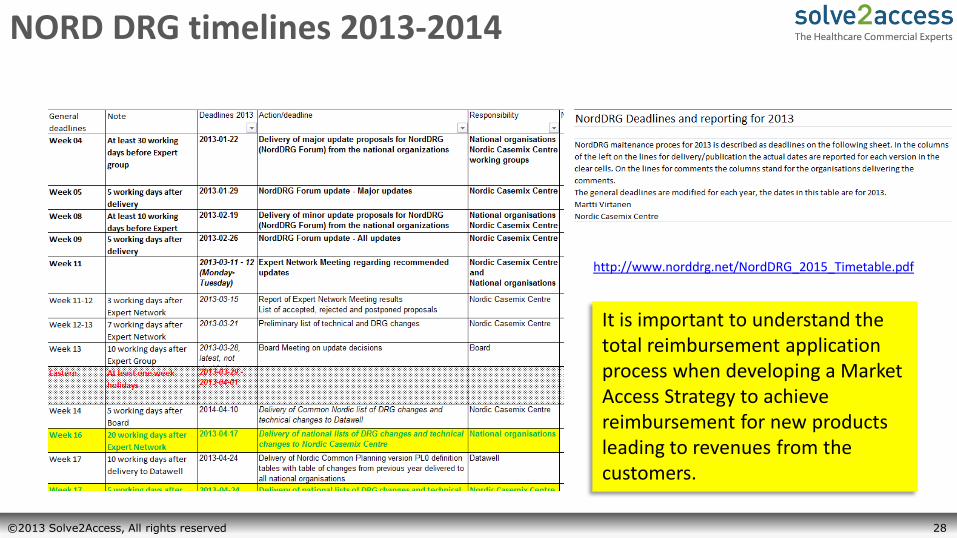
28 ©2013 Solve2Access, All rights reserved 28 ©2013 Solve2Access, All rights reserved
NORD DRG timelines 2013-2014
http://www.norddrg.net/NordDRG_2015_Timetable.pdf
It is important to understand the total reimbursement application process when developing a Market Access Strategy to achieve reimbursement for new products leading to revenues from the customers.
29 ©2013 Solve2Access, All rights reserved 29
Germany
30 ©2013 Solve2Access, All rights reserved 30 ©2013 Solve2Access, All rights reserved
Germany
• Decentralized health insurance system – A health insurance is mandatory for any German person (public or private)
– Medical devices funded via medical procedure (DRG payment), additional remuneration (Zusatzentgeld, ZE) or different post acute tariff lists (GOÄ, EBM, etc.).
31 ©2013 Solve2Access, All rights reserved 31 ©2013 Solve2Access, All rights reserved
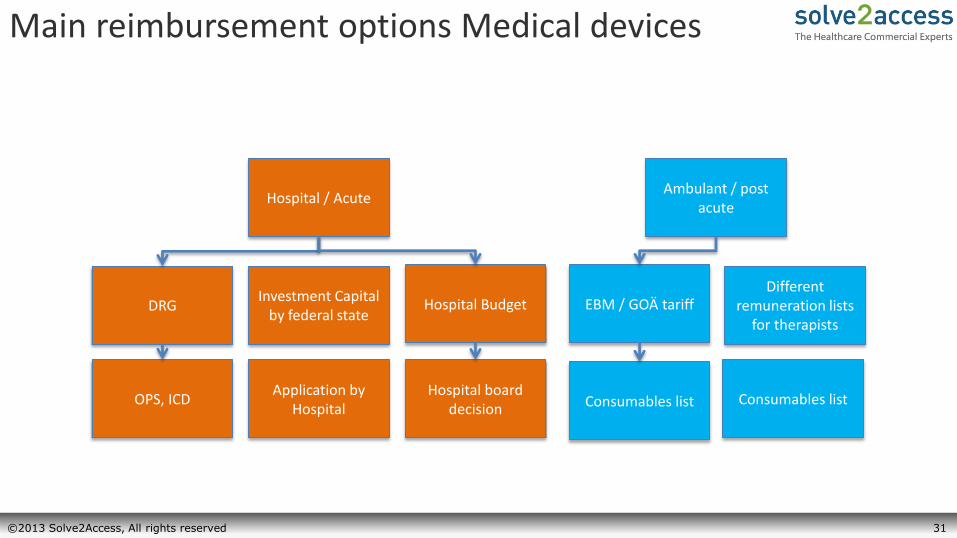
Main reimbursement options Medical devices
Hospital / Acute
DRG Investment Capital
by federal state Hospital Budget
OPS, ICD Application by
Hospital Hospital board
decision
Ambulant / post acute
EBM / GOÄ tariff
Consumables list
Different remuneration lists
for therapists
Consumables list

32 ©2013 Solve2Access, All rights reserved 32 ©2013 Solve2Access, All rights reserved
Side diagnosis (ICD)
Side diagnosis (ICD)
Side diagnosis (ICD) Side diagnosis (ICD)
Age Gender
Ventilation hrs. Birth weight*
Main diagnosis (ICD)
Procedure (OPS)
Procedure (OPS)
Patient exit reason (normal, died, transferred)
- Over 1,200 different DRG’s in Germany in 2013 - The InEK institute calculates every year a new
catalogue - Solve2Access has direct contact to one of the decision
makers
Grouping Process – opportunities for Reimbursement
*only for children
- Thousands of different diagnosis (ICD) and procedures (OPS) codes
- DIMDI institute is organizing the application process for new ICD and OPS codes
- Solve2Access has two direct contacts at DIMDI
- The whole process (DIMDI) of new ICD and OPS code compared with the reimbursement (InEK) is controlled by the GBA (joint federal committee), which is responsible for the HTA (Health Technology Assessment) process in Germany. GBA will allow and forbid new treatment options, check the existing ones, and decide who should pay-
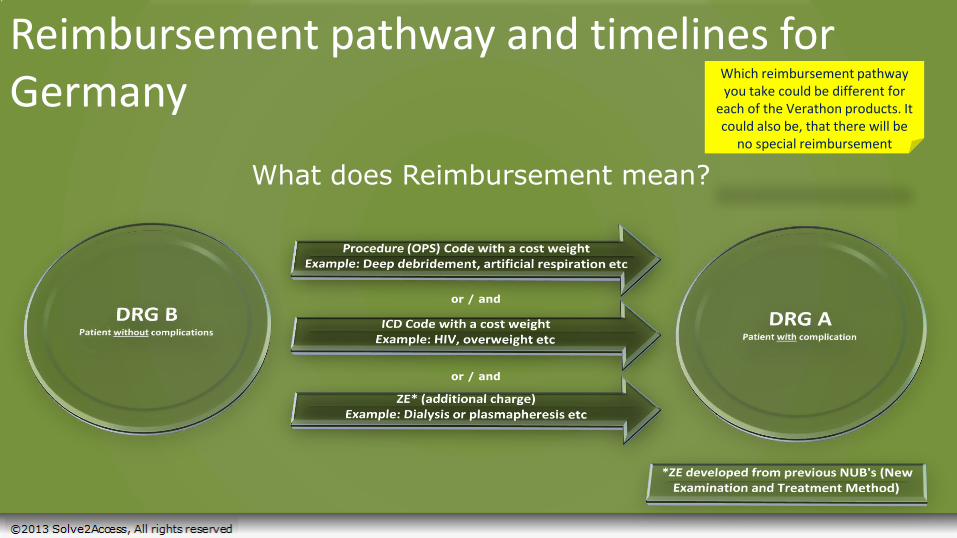
Reimbursement pathway and timelines for Germany
What does Reimbursement mean?
or / and
or / and
Which reimbursement pathway you take could be different for
each of the Verathon products. It could also be, that there will be
no special reimbursement
34 ©2013 Solve2Access, All rights reserved 34
Reimbursement example
Patient: Max Mustermann Age: 47 years Lenght of stay: 30 days
Baserate: 3.068.37 €
Reimbursement example 1.0
Diagnosen
Maindiagnosis: L03.10 Phlegmon of the upper extremity
Sidediagnosis: M72.65 Necrotizing fasciitis: pelvic region and thigh [pelvis, femur, hip, sacroiliac joint]
35
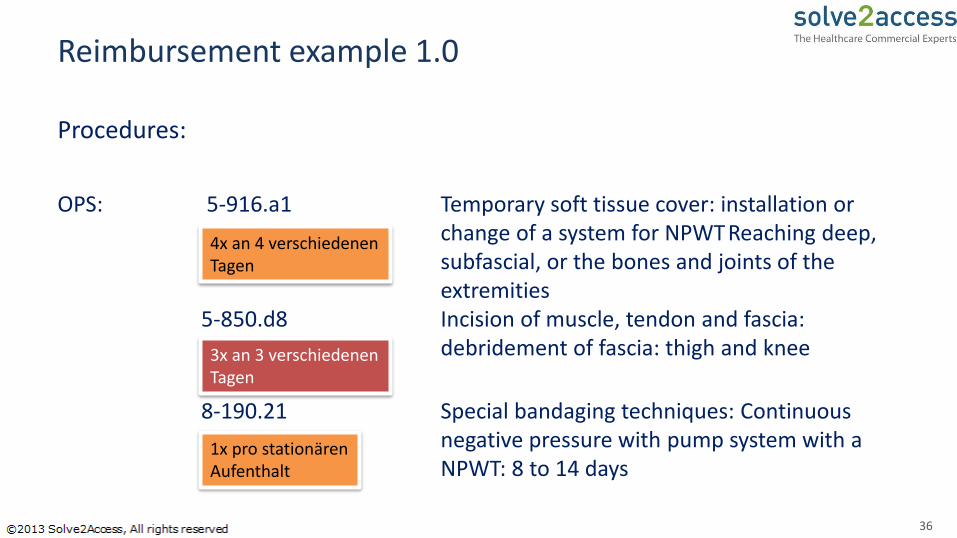
Reimbursement example 1.0
Procedures:
OPS: 5-916.a1 Temporary soft tissue cover: installation or change of a system for NPWT Reaching deep, subfascial, or the bones and joints of the extremities 5-850.d8 Incision of muscle, tendon and fascia: debridement of fascia: thigh and knee
8-190.21 Special bandaging techniques: Continuous negative pressure with pump system with a NPWT: 8 to 14 days
36
4x an 4 verschiedenen Tagen
3x an 3 verschiedenen Tagen
1x pro stationären Aufenthalt
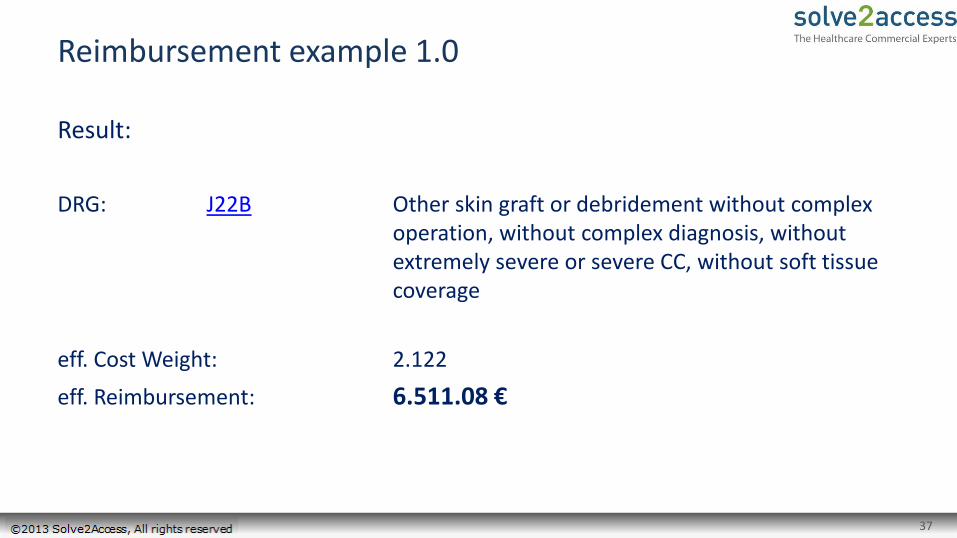
Reimbursement example 1.0
37
Result:
DRG: J22B Other skin graft or debridement without complex operation, without complex diagnosis, without extremely severe or severe CC, without soft tissue coverage
eff. Cost Weight: 2.122
eff. Reimbursement: 6.511.08 €

Reimbursement example 2.0
Diagnosen
Maindiagnosis : M72.65 Necrotizing fasciitis: pelvic region and thigh [pelvis, femur, hip, sacroiliac joint]
Sidediagnosis: L03.10 Phlegmon of the upper extremity
38
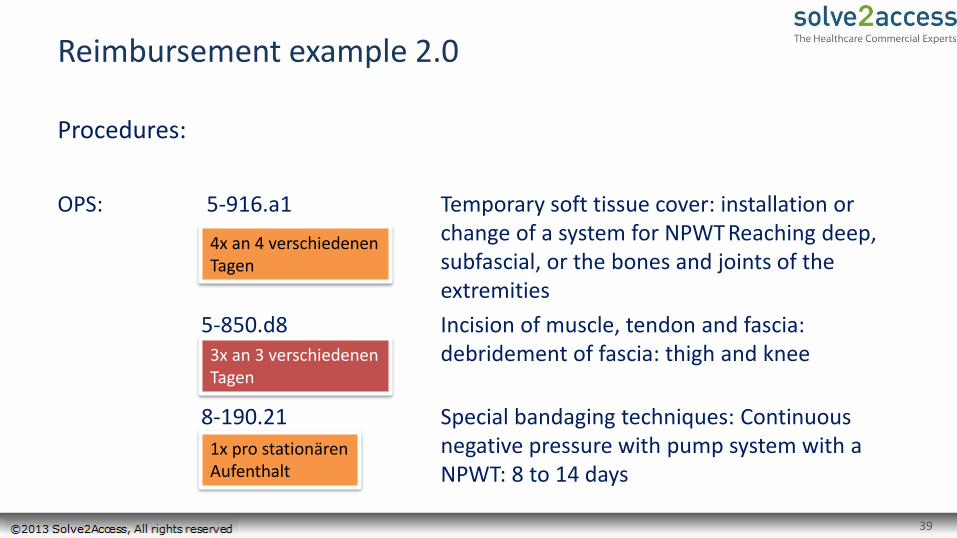
Reimbursement example 2.0
39
Procedures:
OPS: 5-916.a1 Temporary soft tissue cover: installation or change of a system for NPWT Reaching deep, subfascial, or the bones and joints of the extremities
5-850.d8 Incision of muscle, tendon and fascia: debridement of fascia: thigh and knee
8-190.21 Special bandaging techniques: Continuous negative pressure with pump system with a NPWT: 8 to 14 days
4x an 4 verschiedenen Tagen
3x an 3 verschiedenen Tagen
1x pro stationären Aufenthalt

Reimbursement example 2.0
40
Result:
DRG: I22B Tissue / skin grafting, except by the hand, with a small area or the tissue transplantation with extensive tissue transplantation without complications, without treatment at several local., without soft tissue damage, without compl. tissue transplantation, with complications
eff. Cost Weight: 2,775
eff. Reimbursement: 8.514,73 €

Reimbursement example 3.0
41
Prozeduren
OPS: 5-916.a1 Temporary soft tissue cover: installation or change of a system for NPWT Reaching deep, subfascial, or the bones and joints of the extremities 5-850.d8 Incision of muscle, tendon and fascia: debridement of fascia: thigh and knee
8-190.21 Special bandaging techniques: Continuous negative pressure with pump system with a NPWT: 8 to 14 days
4x an 4 verschiedenen Tagen
4x an 4 verschiedenen Tagen
1x pro stationären Aufenthalt
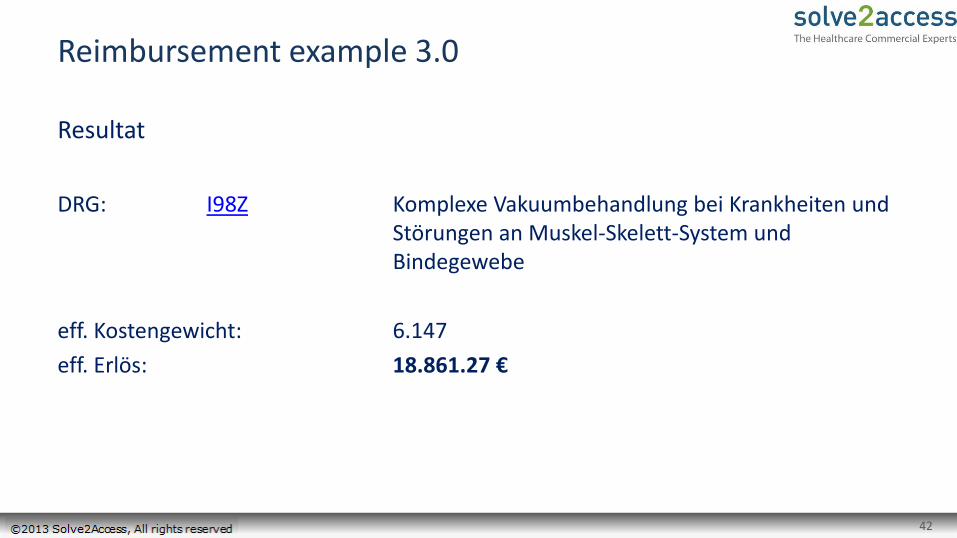
Reimbursement example 3.0
42
Resultat
DRG: I98Z Komplexe Vakuumbehandlung bei Krankheiten und Störungen an Muskel-Skelett-System und Bindegewebe
eff. Kostengewicht: 6.147
eff. Erlös: 18.861.27 €
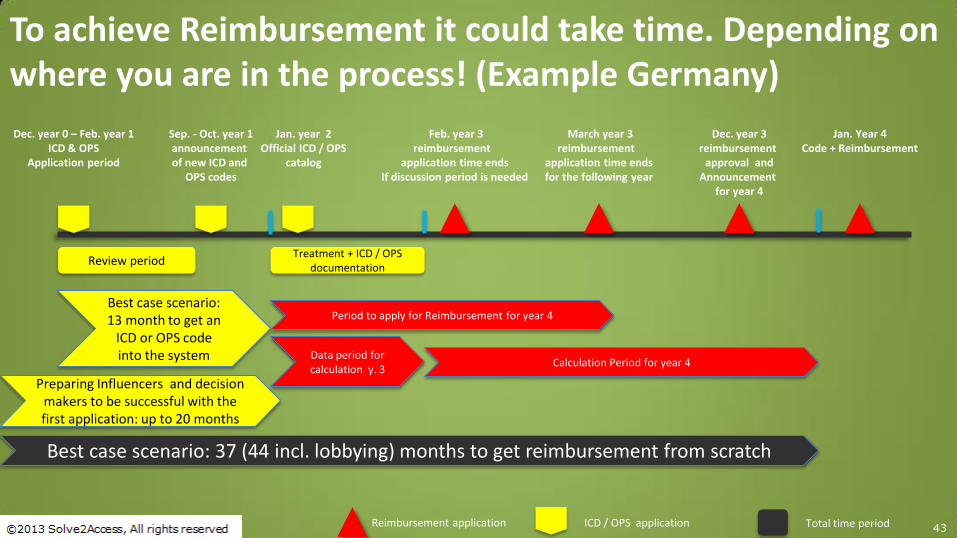
43
Review period
To achieve Reimbursement it could take time. Depending on where you are in the process! (Example Germany)
Reimbursement application ICD / OPS application
Dec. year 0 – Feb. year 1 ICD & OPS
Application period
Jan. year 2 Official ICD / OPS
catalog
March year 3 reimbursement
application time ends for the following year
Dec. year 3 reimbursement
approval and Announcement
for year 4
Jan. Year 4 Code + Reimbursement
Sep. - Oct. year 1 announcement of new ICD and
OPS codes
Total time period
Best case scenario: 13 month to get an
ICD or OPS code into the system
Preparing Influencers and decision makers to be successful with the first application: up to 20 months
Treatment + ICD / OPS documentation
Period to apply for Reimbursement for year 4
Calculation Period for year 4
Feb. year 3 reimbursement
application time ends If discussion period is needed
Data period for calculation y. 3
Best case scenario: 37 (44 incl. lobbying) months to get reimbursement from scratch

44 ©2013 Solve2Access, All rights reserved 44 ©2013 Solve2Access, All rights reserved
United Kingdom
45 ©2013 Solve2Access, All rights reserved 45 ©2013 Solve2Access, All rights reserved
United Kingdom -England
• England is the biggest country* of the United Kingdom** Centralized healthcare system for 90% funded via taxes
Care delivery coordinated by GPs who are grouped in GP practices, who are grouped into 211 clinical commissioning groups, which hold +/-80% of the total healthcare budget
*>80% of population of the United Kingdom lives in England ** England, Scotland, Northern Ireland and Wales form the United Kingdom

46 ©2013 Solve2Access, All rights reserved 46 ©2013 Solve2Access, All rights reserved
Overview of healthcare system (England)
Budget £80,000,000,000
211 Clinical Commissioning Groups
GPs GPs
Patient Patient Patient
Hospitals
Hospitals
Buy care
Buy care
Budgetholders Previous situation Situation 2013
GP practises
47 ©2013 Solve2Access, All rights reserved 47 ©2013 Solve2Access, All rights reserved
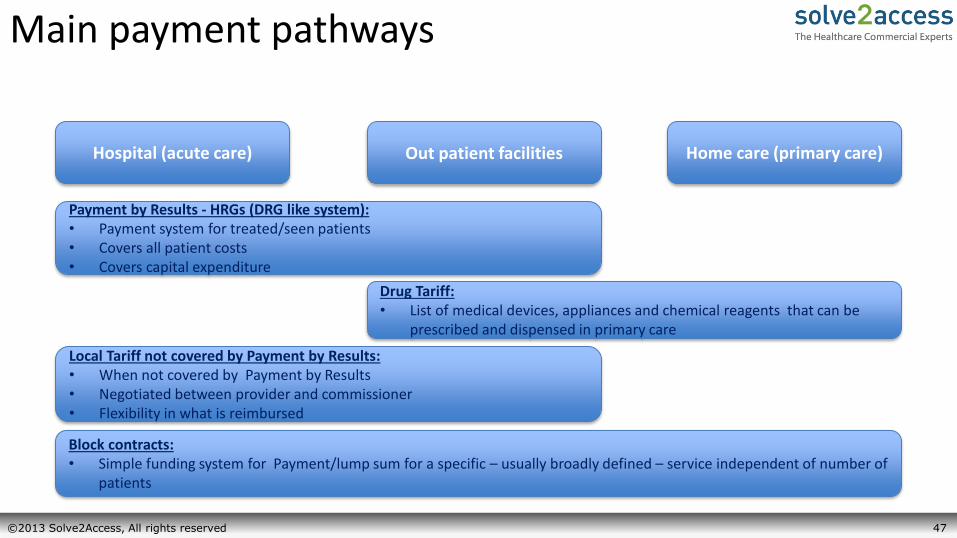
Main payment pathways
Hospital (acute care) Out patient facilities Home care (primary care)
Payment by Results - HRGs (DRG like system): • Payment system for treated/seen patients • Covers all patient costs • Covers capital expenditure
Drug Tariff: • List of medical devices, appliances and chemical reagents that can be
prescribed and dispensed in primary care
Local Tariff not covered by Payment by Results: • When not covered by Payment by Results • Negotiated between provider and commissioner • Flexibility in what is reimbursed
Block contracts: • Simple funding system for Payment/lump sum for a specific – usually broadly defined – service independent of number of
patients
HRG English DRG payment system
Payment system for hospital and out patient clinic care: • Includes capital investment costs •Coding for similar levels of NHS resource use
Are existing codes available that could be used? •Process takes 1 month to get confirmation
Process to apply for a new code: •Anybody can apply for a new code (companies, medical societies) •Application is at least 1 year until new code may be published •Another 3 years to set a tariff

Drug Tariff
Application until listing 3-6 months when: 1. Products are safe and of good quality 2. Appropriate for GP and nurse prescribing 3. They are cost effective It doesn’t mean that you make revenues when you are listed on the drug tariff list. You have to win tenders with your products.

50 ©2013 Solve2Access, All rights reserved
Key stakeholders for reimbursement Hospital setting (Inpatient & Outpatient)
Stakeholder Level of Influence Role
Physicians
Pharmacist
Clinical Engineer
Purchasing manager
Hospital management
Advocate for products
Advises on medical equipment and devices
Responsible for reimbursement
Influencer Decision-maker
Supervises and decides on purchases Has close relationship with manufacturers and is aware of new product launches
Decides on budget allocation
User’s opinion will be critical in the
decision to acquire a device
Nurses Input on ease of use
Advises on disposables Mostly focused on cost
Hospital management
51 ©2013 Solve2Access, All rights reserved
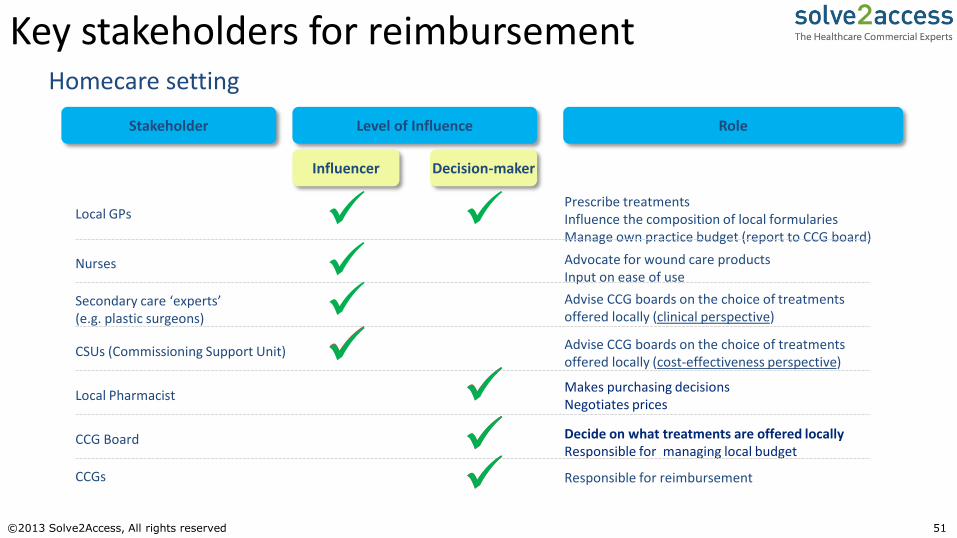
Key stakeholders for reimbursement Homecare setting
Stakeholder Level of Influence Role
Influencer Decision-maker
Local GPs
CSUs (Commissioning Support Unit)
Local Pharmacist
CCG Board
Prescribe treatments Influence the composition of local formularies Manage own practice budget (report to CCG board)
Advise CCG boards on the choice of treatments offered locally (cost-effectiveness perspective)
Responsible for reimbursement
Makes purchasing decisions Negotiates prices
Decide on what treatments are offered locally Responsible for managing local budget
Nurses Advocate for wound care products Input on ease of use
CCGs
Secondary care ‘experts’ (e.g. plastic surgeons)
Advise CCG boards on the choice of treatments offered locally (clinical perspective)
52 ©2013 Solve2Access, All rights reserved 52 ©2013 Solve2Access, All rights reserved
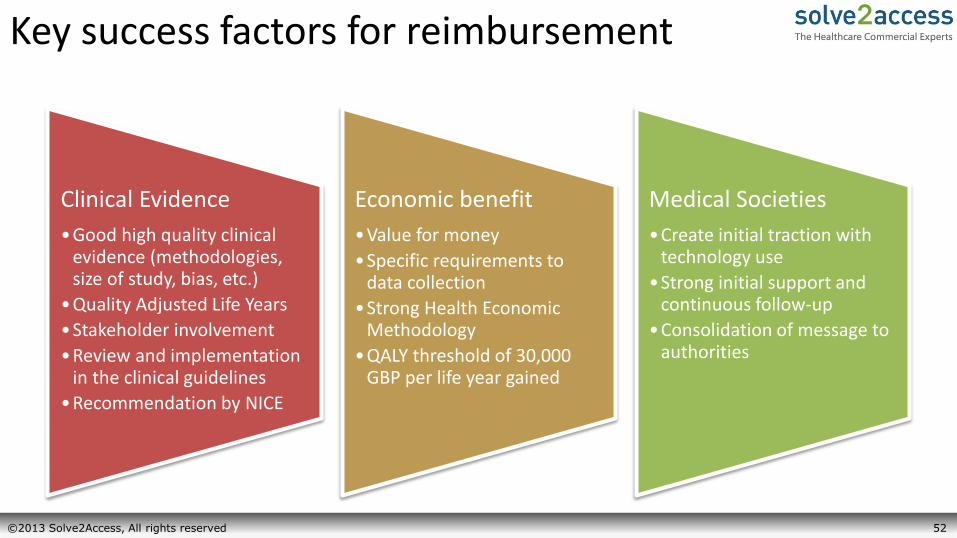
Key success factors for reimbursement
Clinical Evidence
•Good high quality clinical evidence (methodologies, size of study, bias, etc.)
•Quality Adjusted Life Years
•Stakeholder involvement
•Review and implementation in the clinical guidelines
•Recommendation by NICE
Economic benefit
•Value for money
•Specific requirements to data collection
•Strong Health Economic Methodology
•QALY threshold of 30,000 GBP per life year gained
Medical Societies
•Create initial traction with technology use
•Strong initial support and continuous follow-up
•Consolidation of message to authorities

53 ©2013 Solve2Access, All rights reserved 53 ©2013 Solve2Access, All rights reserved
France
54 ©2013 Solve2Access, All rights reserved 54 ©2013 Solve2Access, All rights reserved
France
• Centralized system, funded by the National Healthcare Insurance – Care delivery coordinated by 22 regional healthcare agencies (ARS)
– Medical devices funded by medical procedure (DRG payment) or positive list (LPPR), depending upon care setting
55 ©2013 Solve2Access, All rights reserved 55 ©2013 Solve2Access, All rights reserved
GHS: French DRG payment system
• Expenditure of product typically integrated into hospital services – Hospitals must accept that product will reduce costs
– Health Economics play important role to demonstrate benefits
• Medical Societies can apply for new procedure codes – Specific payment must be negotiated separately
– Long and complex process, taking usually 2 to 3 years
– Demands intense follow-ups with Societies and authorities
– Benefit for authorities: control of the use of technology

56 ©2013 Solve2Access, All rights reserved 56 ©2013 Solve2Access, All rights reserved
LPPR: List of reimbursable products and services
• Considers the product and the required service for proper use – Evaluation period around 1 year (published 6 months)
• Complementary nature: additional funding for product
• Inclusion by generic name: easy access, lower payment
– Type of product according to its indications and technical specifications without mentioning the brand name or company
– No formal evaluation
• Inclusion by brand name: complex access; higher payment
– Innovative and/or high-cost products
– Reimbursement dossier evaluated by the CNEDiMTS
– Authorities always intend to shift products into the generic name
57 ©2013 Solve2Access, All rights reserved 57 ©2013 Solve2Access, All rights reserved
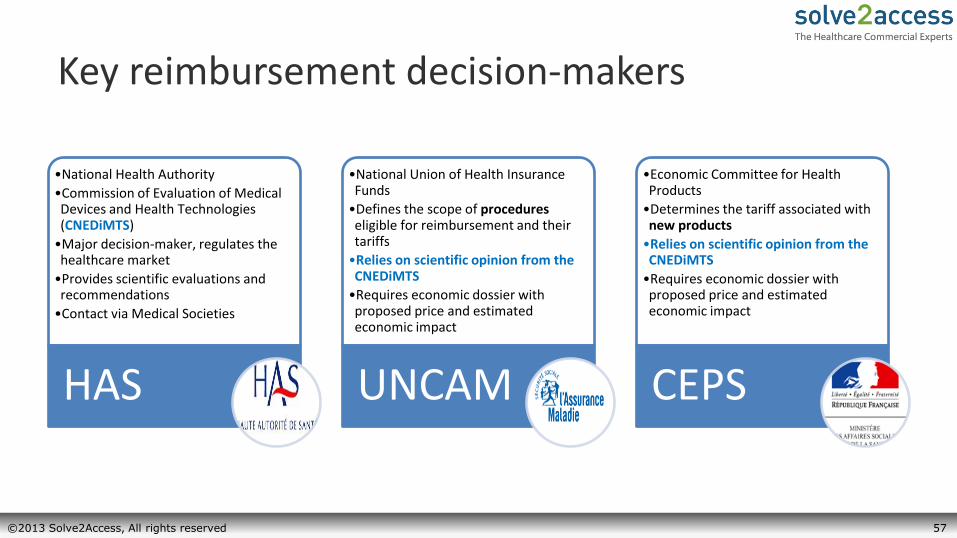
Key reimbursement decision-makers
•National Health Authority
•Commission of Evaluation of Medical Devices and Health Technologies (CNEDiMTS)
•Major decision-maker, regulates the healthcare market
•Provides scientific evaluations and recommendations
•Contact via Medical Societies
HAS
•National Union of Health Insurance Funds
•Defines the scope of procedures eligible for reimbursement and their tariffs
•Relies on scientific opinion from the CNEDiMTS
•Requires economic dossier with proposed price and estimated economic impact
UNCAM
•Economic Committee for Health Products
•Determines the tariff associated with new products
•Relies on scientific opinion from the CNEDiMTS
•Requires economic dossier with proposed price and estimated economic impact
CEPS

58 ©2013 Solve2Access, All rights reserved
Spain
59 ©2013 Solve2Access, All rights reserved 59 ©2013 Solve2Access, All rights reserved
Spain
• Fragmented system, funded by the National Healthcare System
– Each of the 17 regions have autonomy to allocate their healthcare budget
– DRG system only used for statistical purposes; medical devices funded almost entirely from hospital/providers’ budgets
– Economic crisis has created strong pressure on regions to reduce healthcare expenditure
Spanish Health Care System
• “Sistema Nacional de Salud” covers all Spanish Citizens
– “Cartera de Servicios”: basic health care package
– Budget allocation to each Region as the Funding source
• DRG used only for statistical purposes, not payment
– National HTA Agency: ISCIII
• Regional Health Authorities have autonomy to decide how to use their budgets
– Main criteria: previous year’s expenditures
– May add extra coverage
– 6 Regional HTA agencies
• Independent Evaluations and Guidelines
– National decisions don’t affect Regions unless it is included in the basic health care package
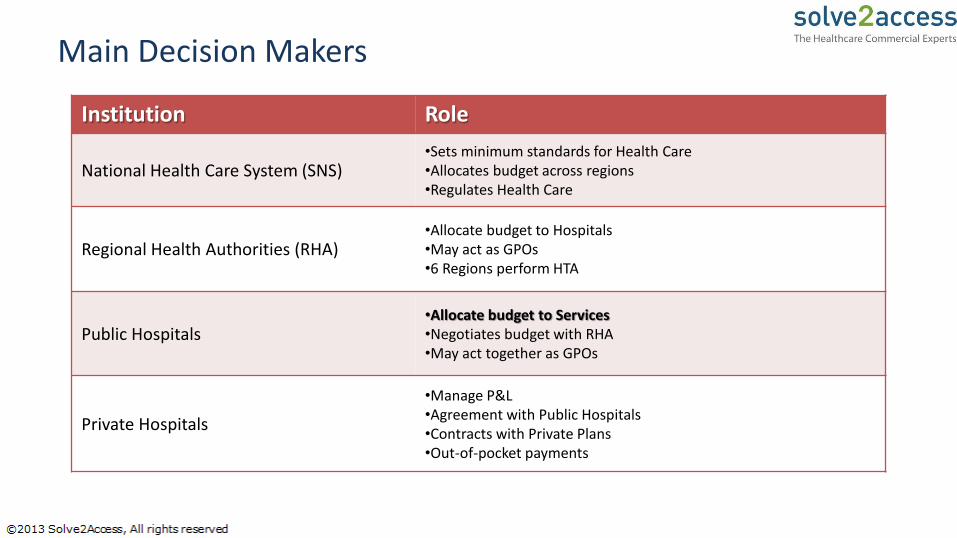
Main Decision Makers
Institution Role
National Health Care System (SNS) •Sets minimum standards for Health Care •Allocates budget across regions •Regulates Health Care
Regional Health Authorities (RHA) •Allocate budget to Hospitals •May act as GPOs •6 Regions perform HTA
Public Hospitals •Allocate budget to Services •Negotiates budget with RHA •May act together as GPOs
Private Hospitals
•Manage P&L •Agreement with Public Hospitals •Contracts with Private Plans •Out-of-pocket payments
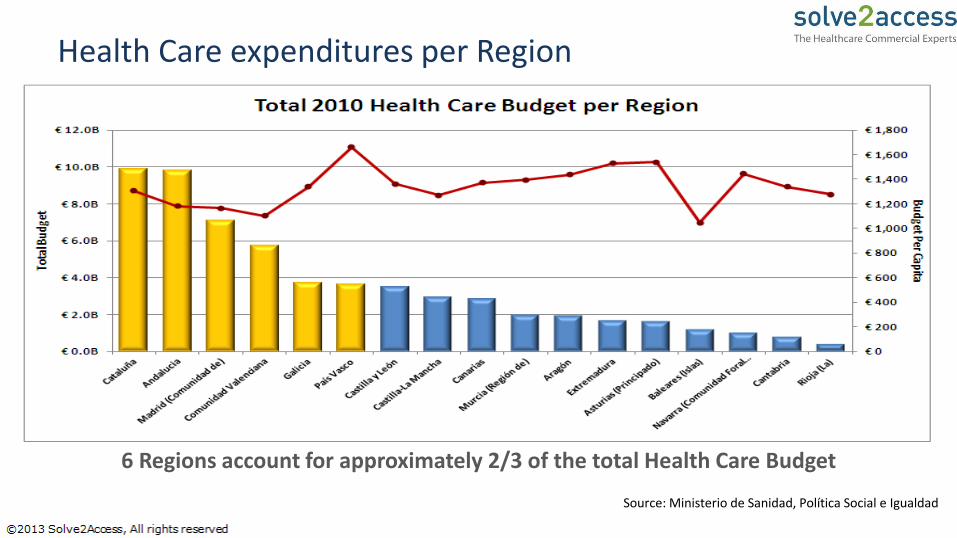
Health Care expenditures per Region
6 Regions account for approximately 2/3 of the total Health Care Budget
Source: Ministerio de Sanidad, Política Social e Igualdad

63 ©2013 Solve2Access, All rights reserved
Medical Device Pathway
Market Access Reimbursement /
Funding Pricing Purchasing
•CE Mark •HTA for National and Regional Health Services Portfolio
•Hospitals typically fund Medical Devices though Budget
•RHA and Hospitals may provide extra budget (very rare)
•Relationship is fundamental
•No National Pricing list
•Regional and Hospital negotiations with Manufacturers
•Individual and GPOs
•Hospitals purchase directly from manufacturers
•Tenders for amounts above € 18,000

Spain: Key take-aways
• Regions are independent from each other
• Fundamental to establish presence in both Primary and Specialized Care
• Tenders drive Budget allocation and, in the longer term, Reimbursement
• Addressing stakeholders before Tenders are published is key to success
65 ©2013 Solve2Access, All rights reserved
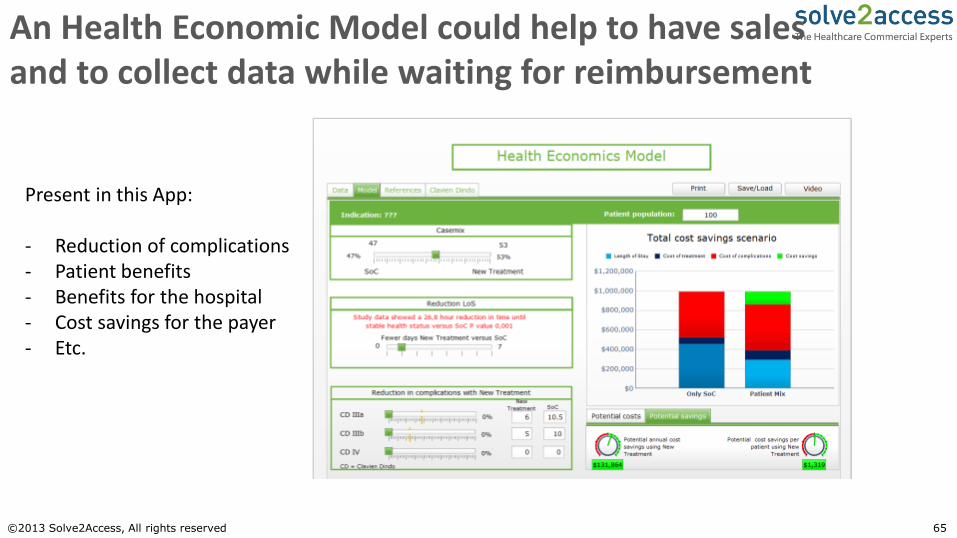
An Health Economic Model could help to have sales and to collect data while waiting for reimbursement
Present in this App: - Reduction of complications - Patient benefits - Benefits for the hospital - Cost savings for the payer - Etc.

66 ©2013 Solve2Access, All rights reserved 66 ©2013 Solve2Access, All rights reserved
When to start thinking about reimbursement?
In which part of the process are you with your new product?
You should know the realistic market size of your product
You should start to think about how to overcome Market Access hurdles. (Design Phase)
You should be in the process of assessing the Market Access for different countries
If you did not plan your Market Access strategy, it could be too late to achieve your revenue targets.
67
Summary and takeaways
Reimbursement is more then getting paid for a Medical Device (Market Access Strategy)
Reimbursement can be covered via DRG or via different Health Care Budgets
In which country to start first? Where are the early adopters?
It is necessary to start as early as possible with the Reimbursement Strategy, because it takes time to achieve reimbursement
It is absolutely necessary to assess the different market requirements to achieve reimbursement and to ensure that these needs can be addressed. (HTA process, Regulatory)
Depending on the product or method a project budget to achieve reimbursement is required
Do your reimbursement analysis as early as possible in your regulatory strategy
During the process it is necessary to answer the question: What value for money do the customers get

Thank You