Embed Size (px)
Citation preview

INJTRODUCTION

INTRODUCTION
The healthy human body is equipped with powerful set of tools to provide protection
from the diverse onslaught of microbes, foods and other ingested products
(Atkins, 2010). Unfortunately, this set ofmechanisms, known as the immune system,
sometimes goes awry and attacks the body itself. Anti-self responses are usually
generated in the process of mounting an immune response to foreign antigens, but
autoimmune disease results only if autoimmunity IS poorly regulated
(Schwartz, 2004). These breakdowns of immunological tolerance are referred to as
autoimmunity, which can be demonstrated by the presence of autoantibodies or T
lymphocytes reactive with host antigens (Abbas, 2004). Autoimmunity is present in
everyone to some extent. Autoimmune diseases are thus, defined when the
progression from benign autoimmunity to pathogenic autoimmunity occurs.
A combination of genetic predisposition and enviromnental factors contribute to the
development of autoimmune disease (Maniati, 2008) (Figure 1 ). Autoimmune disease
occurs when the autoimmune response to self constituents has damaging effects of a
structural or functional character. The concept of autoimmunity as the actual cause of
human illness (rather than a consequence or harmless accompaniment) can be used to
establish criteria that define a disease as an autoimmune disease (Alarcon-Segovia D,
2006).
Autoimmune disease is a clinical syndrome caused by the activation of autoreactive
T cells and B cells, or both, in the absence of an ongoing infection or other discernible
cause (Davidson, 2001). Activation-induced T cell death is cell cycle dependent
(Fotedar, 1995; Zhang, 2004). However, an accumulation of activated T cells resistant
to proliferation and apoptosis was also found in lupus conditions (Wither, J.E, 2000).
Autoimmune disease may arise either from defective elimination of autoreactive T or
B cells, resulting in tissue destruction, or from defective clearance of apoptotic cells
displaying autoantigens on their cell surface (Lauber, 2004). The self reactive T cell
expresses high levels of cyclin-dependent kinases inhibitors which induces a state of
"replicative senescence" and transcribes genes encoding the proinflammatory
cytokines in autoimmunity (Lawson BR, 2004).

f) \)
Immune regulation
Introduction
Figure 1. The influence of environmental, pathogens, genetic factors and
immunological factors can trigger autoimmunity in genetically predisposed individuals
under conditions of immune dysregulation (Fathman, 2005).
The cell cycle and apoptosis are opposing biological phenomena, however tolerance
play an important role in the development of autoimmunity by affecting apoptosis
(Mueller, 201 0). Mechanisms of self-tolerance, defined as a state of non
responsiveness to self, can be divided into central and peripheral tolerance. In central
tolerance, immature lymphocytes in the bone marrow (B cells) and thymus (T cells)
that recognize self-antigens with high affinity die by apoptosis or programmed cell
death (Gregory, 2004). In peripheral tolerance, mature self-reactive lymphocytes are
inactivated, killed or turned off by regulatory mechanisms including functional
anergy, Ignorance and suppression by regulatory T cells (Schwartz, 2004). The
lymphocytes escaping the tolerance and defects in tolerance have a likelihood of
developing autoimmune diseases. Accumulation of activated T and B cells with
defective tolerance and resistant to proliferation and apoptosis is found in lupus
conditions (Wither, J.E, 2000).
Impaired apoptosis is also considered one of the key mechanisms in the pathogenesis
of autoimmune disease (Mount, 1994). Studies have elucidated several important
mechanisms underlying the maintenance of immune tolerance and defective apoptotic
pathways in autoimmune diseases (Maniati, 2008). An impaired apoptosis of PBMCs
2

Introduction
were seen in autoimmune patients suggesting a defective clearance and deregulated
expression of regulatory proteins in PBMCs (Harris, 2000; Peng, 2009). The changes
in the apoptotic cell death process, resulting in inappropriate cell death or survival or
disturbances in clearing apoptotic cells, are thought to be involved in the pathogenesis
of a number of autoimmune diseases such as rheumatoid arthritis, lupus and
Hashimoto's thyroiditis (Peng, 2005; Lleo, 2008). Evidence has been provided for
defective clearance of apoptotic cells in SLE patients (Ren, 2003 ), and persistently
circulating apoptotic debris was suggested to serve as immunogen for the induction of
autoreactive lymphocytes in these individuals (Maniati, 2008).
Subthreshold • levels of .t•' ...
novel structure
~ Normal clearance of apoptotic material
NORMAL
lN Drug
~ g ;usA CTL
V-. Supra threshold
~ levelsof novel structure
Impaired clearance of apoptolic material e.g. C1 q deficiency
AUTOIMMUNE
Figure 2. The influence of environmental, pathogens, physiological factors and
immunological factors influence on apoptotic cells, which is responsible prerequisite
for triggering an autoimmune response. Clustering of autoantigens in apoptotic
surface structures (Rosen et al, 1999)
The combined action of apoptosis and anergy are results in a state of peripheral
tolerance are altered in autoimmune progression (Mueller, 201 0). Autoimmune
disease may occur only when defective clearance is linked to a modified (aberrant)
response of the macrophage to the unengulfed debris. In contrast, ingestion and
presentation of self-antigen from apoptotic cell corpses under steady-state conditions
may serve to induce immune tolerance (Gregory, 2004). The most common feature of
all autoimmune diseases is the presence of autoantibodies and inflammation,
including mononuclear phagocytes, autoreactive T lymphocytes and plasma cells
3

Introduction
(autoantibody producing B cells) (Fairweather, 2008). The inference that a systemic
disease is autoimmune is based on the presence of autoantibodies and their
localization in diseased tissue of antibody, complement, and T-lyrnphocytes (Rosen,
1999; Fadeel, 2005) (Figure 2).
History and dimensions of autoimmunity
This concept of autoimmunity as the cause of human illness is relatively new, and it
was not accepted into the mainstream of medical thinking until the 1950s and 1960s.
Ehrlich and Morgenroth (1898) proposed that the consequences of the formation of
self-antibodies were so severe "horror autotoxicus" that the immune system
stringently prohibited its occurrence. Although investigators observed a clear
evidence of anti-self-agglutinins, it was not until the 1950s that the general
acceptance of the concept that autoantibodies could cause immune injury (Silverstein,
2001). Autoimmune diseases affect approximately 8% of population out of which
75-78% are women population (Jacobson DL, 1997). Women are known to respond to
infection, vaccination, and trauma with increased antibody production and a more T
helper (Th) 2-predominant immune response, whereas a Th1 response and
inflammation are usually more severe in men (Fairweather, 2008). Autoimmune
diseases that are more prevalent in males usually manifest clinically before age 50 and
are characterized by acute inflammation, the appearance of autoantibodies, and a
proinflammatory Thl immune response. In contrast, female-predominant autoimmune
diseases that manifest during the acute phase, such as Graves' disease and systemic
lupus erythematosus, are diseases with a known antibody-mediated pathology
(Fairweather, 2008).
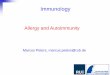
Autoimmune diseases are among the ten leading causes of death among women in all
age groups up to 65. The bar graph shows the prevalence of the top 10 autoimmune
diseases in the United States in 1996 (Jacobson DL, 1997) (Figure 3)
4

GIOYBS disease
Rheumat>ld crthlltls
Hashfnot>' 5 thl~CidlfS Vrtiligo
Type I dk:l b«es Pemido.ls anemia
Muliple scfelosls Gomerulalephtitls
S~k: Lupus E
Sjoglen Sldnd!ome
Introduction
Figure 3. The rate of particular autoimmune disorders with progression among the
population of developed countries, in which female were much affected as compared
to male population. (Showing the prevalance of top 10 autoimmune disorder in US, 1996,
(Adapted from Jacobson DL, Clin lmmunollmmunopathol, 1997)
Classification and types of human systemic autoimmune disorders
Autoimmune diseases can be classified as organ-specific or non-organ specific
depending on whether the autoimmune response is directed against a particular tissue
like the thyroid in Hashimoto's thyroiditis, or against widespread antigens such as cell
nuclear antigens in lupus (Peng, 2005; Fairweather, 2007). Systemic autoimmune
diseases include SLE, Sjogren's syndrome, scleroderma, rheumatoid arthritis, and
dermatomyositis conditions which tends to be associated with generation of
autoantibodies to antigens which are not tissue specific (Takehara, 2005).
A feature of autoimmune disease is usually referred to as "overlap syndrome". The
concept of "overlap syndromes" arises when autoimmunity comprises various forms
of disease and the development of two or more autoimmune rheumatic diseases in one
patient, the so-called overlap syndromes (Rodriguez-Reyna, 2005). The genetic and
environmental factors that led to these phenomena interact in a complex fashion and
influence the distinct phenotypic characteristics of each patient (Alarc6n-Segovia D,
2006) and some patients have an autoimmune disease sometimes termed "mixed
connective tissue disease," which has features of SLE, scleroderma, and polymyositis
(Maddison, 2000).
5

Introduction
However, systemic lupus erythematosus is an autoimmune connective-tissue disorder
with a wide range of clinical features, which predominantly affects women
(D'Cruz, 2007). A number of environmental triggers and a number of genetic
susceptibilities roles in causing autoimmunity (Fathman, 2005). SLE is polygenic
where multiple genes appear to influence a person's chance of developing lupus when
triggered by environmental factors. HLA region on chromosome 6 mutations may
occur randomly or may be inherited. HLA class I, class II, and class III are associated
with SLE, but only class I and class II contribute independently to increased risk of
SLE (Martens, 2009).
Antibodies to DNA (anti-DNA) are the serological hallmark of systemic lupus
erythematosus (SLE) and unique markers of the immunological disturbances critical
to disease pathogenesis (Pisetsky, 2009). SLE is best known for its array of
antinuclear antibodies, antibodies to many other self-components are well described.
In the case of IgG and clotting factors, it is possible that the true autoantibody target is
cell bound in the form of immune complexes or of activated clotting factors
(Kavai, 2008). In the form of immune complexes, anti-DNA autoantibodies can
deposit in the tissue to incite inflammation and damage; in addition, these complexes
can induce cytokine production, most prominently, type 1 interferon (Pisetsky, 2009).
The lymphoproliferative and autoimmune disorder occurs in a primary form, not
associated with a rheumatic disease, and as a complication of rheumatoid arthritis,
SLE, or scleroderma. Patients develop infiltration of exocrine glands, mostly salivary
and lachrymal glands, with activated polyclonal CD4 + T cells, together with
hypergammaglobulinemia, autoantibodies, and sometimes vasculitis (Price EJ, 1995).
Multiple sclerosis (MS) is an autoimmune disorder characterized by multifocallesions
of the CNS myelin and accumulating clinical signs due to axonal damage
(Keegan, 2002). Myelin is damaged due to an immune attack consisted of several
pathways and molecules, leading to impaired nerve function (Grigoriadis, 2006).
Autoantibodies and autoreactive T cells activated against myelin antigens myelin
basic protein (MBP), proteolipid protein (PLP), and myelin oligodendrocyte
glycoprotein (MOG), have been detected in MS patients (Garren, 1998). It is
considered that MS as a CD4+T-helper 1 (Thl)-mediated inflammatory demyelinating
disease (Hafler, 2004).
6

Introduction
Primary Sjogren's syndrome (SS) is an autoimmune disorder associated with
lymphocytic infiltration of salivary and lachrymal glands and systemic production of
autoantibodies (Tucci, 2005). The presented autoantigens are mainly SSA/Ro,
SSB/La, a.-fodrin and ~-fodrin, or cholinergic muscarinic receptors. Help from
CD4 cells leads to production of specific autoantibodies. Anti-SSA/Ro antibodies
may be detected alone, whereas anti-SSB/La antibodies are always found in
conjunction with anti-SSA/Ro, suggesting a spreading of the autoantibody response
(Gottenberg, 2003).
Rheumatoid arthritis (RA) is a common chronic inflammatory polyarthritis of
worldwide distribution, with a female predominance of 3:1 and a peak onset in the
fourth decade of life. Intense inflammation occurs in synovial joints, so that the
normally delicate synovial "membrane" becomes infiltrated with mononuclear
phagocytes, lymphocytes, and neutrophils. An essential feature of the rheumatoid
nodule, as with the joint lesion, is tissue destruction (Highton, 2007). Autoimmune
diseases of joints are marked by inflammation, followed by generation of increased
amounts of collagen in skin and viscera, accompanied by certain antinuclear
antibodies (Clements PJ, 2000). In rheumatic disease, probing the transcriptome of
circulating immune cells has shed light on mechanisms underlying the pathogenesis
of complex diseases, such as systemic lupus erythematosus (Bauer JW, 2009).
Analysis of relevant signaling pathways at the protein level is an important step
towards understanding the functional consequences of aberrant gene expression.
Scleroderma is characterized by marked vascular abnormalities, the most dramatic of
which is the episodic reduction in peripheral arterial perfusion (often provoked by
cold temperatures) known as Raynaud's phenomenon which causes an impairment of
circulation which can lead to pain, infections, and frequent ischemic amputation of the
distal fmgertips (Anderson, 2007).
Apoptosis
Apoptosis is a highly regulated process that faci litates deletion of unwanted or
damaged cells in various circumstances of stress and plays a fundamental role in the
maintenance of tissue homeostasis (Fadeel, 2005). Apoptosis elicits specific cell
surface changes, such as the exposure of phosphatidylserine, present on the
7

Introduction
intracellular aspect of the cell membrane, resulting in the swift uptake and degradation
of apoptotic cells either by local resident cells or infiltrating phagocytes
(Stuart, 2002). This process is very rapid such that apoptotic cells are conspicuously
absent in normal tissues. Furthermore, cell deletion by apoptosis leading to clearance
by professional phagocytes such as macrophages is not associated with
proinflammatory mediator release but rather causes release of anti-inflammatory
agents (Green DR. 2000). The mechanisms whereby macrophages and semi
professional phagocytes (including mesangial cells) recognize and ingest apoptotic
cells are complicated and may involve numerous molecules including the vitronectin
receptor (rr.Jh integrin), CD36, thrombospondin, the phosphatidylserine receptor, the
first component of complement Clq, jJ2 thrombomodulin, class A scavenger
receptors, etc (Savill, 2002 ; Platt N, 2000).
Phases of apoptotic death
Apoptotic cell death can be divided into a triggering phase (ligation of "dedicated
death receptor" such as Fas, or withdrawal of growth/survival factors), a signaling
phase (protein kinase cascades that include MAPK family, JNK and p38), an
execution phase (activation of caspases and nucleases), and a burial phase
(phagocytosis of dying cells by neighboring cells) (Utz PJ, 1998).
Apoptotic impairment in autoimmunity
Autoimmune disease arise either from defective elimination of autoreactive T or B
cells, resulting in tissue destruction, or from defective clearance of apoptotic cells
displaying autoantigens on their cell surface (Lauber, 2004) . However, the immune
homeostasis and immune tolerance are dependent on apoptosis induction and the
rapid clearance of cell corpses, in peripheral and central lymphoid organs
(Siegel, 2000). The removal of apoptotic cells in organism by macrophages and
nonprofessional phagocytes receptors promote phagocytosis by enhancing binding to
the apoptotic cell. Phagocytic defects have also been linked to autoimmune
conditions; macrophages from patients with systemic lupus erythematosus (SLE)
show defects in clearance of apoptotic cells (Tas, 2006; Maniati, 2008).
A major direction in apoptosis research related to autoimmunity concerns aberrations
in the disposition, clearance of apoptotic debris (Gaipl US, 2005). A large numbers of
8

Introduction
apoptotic cells are generated continuously which are efficiently engulfed by
macrophages that recognize them via a battery of receptors. These receptors includes
CD14, PS, PS-R, together with the integrin ocv133, CD36/vitronectin, a receptor for
phosphatidylserine, class A scavenger receptor SR-A, the ATP-binding cassette
transporter, ABC-1 , MER and the oc-2-macroglobulin receptor, CD91. Additional
intermediate factors including thrombospondin, C 1 q, C-reactive protein which may
opsonise apoptotic cells or function in bridging macrophage and apoptotic-cell
surfaces (Savill, 2002; Devitt, 2003). (Figure 4)
Mer
ICAM3
c RecoenHIOn of non-dNctqlll
N~ Rmew. ftmmunolog;
Figure 4. Receptors that are expressed by the apoptotic cells and the phagocytes for
the purpose of clearance mechanisms.
A. Innate recognition of non-self involves phagocyte CD14, i3 2-integrins (which bind the
opsonic complement fragment inactivated C3b, iC3b) and the CD91-calreticulin complex
(which can bind the first component of complement, C1q, and mannose-binding lectin,
MBL, which recognizes pathogen-like apoptotic-cell-associated molecular patterns)
B. Recognition of altered-self involves an array of scavenger receptors, including the class
A scavenger receptor (SRA), CD68, LOX1 (oxidised low-density lipoprotein receptor 1)
and C036, which recognize oxidised sites on apoptotic cells that mimic oxidised low
density lipoprotein (oxLDL).
9

Introduction
C. Recognition of non-detaching self involves disabling the detachment signals that are
conferred by apoptotic-cell CD31 and, possibly, similar alterations in another
immunoglobulin-superfamily member, intercellular adhesion molecule 3 (ICAM3). Disabled
apoptotic-cell CD31 binds tightly to phagocyte CD31 , which may promote binding of the
bridging protein thrombospondin-1 (TSP1) by phagocyte integrins. (Savill, 2002)
Defects in clearance lead to exposure of autoantigens, which subsequently results in
autoimmune diseases, however the engulfment process is a potential therapeutic
target. The process of corpse removal occurs via a series of recognizable steps.
Initially, a phagocyte binds to the apoptotic cell, leading to specific recognition of the
target, phagocytic cup formation and sustained signaling that induces actin
rearrangement and phagocytosis. Ultimately, the apoptotic cell is completely
internalized, and its corpse is processed for degradation (Kinchen, 2007).
Immunization of normal mice with large amounts of apoptotic cells leads to mild and
short-lived autoimmunity, indicating the potential immunogenicity of apoptotic debris
(Mohan, 2001 ). Complement is important in the clearance of apoptotic debris
(Navratil, 2000). The absence ofCR2 converts the mildly autoimmune B6/lpr strain to
a strain with severe lupus-like disease, probably reflecting impaired handling of
apoptotic debris as do B6/lpr mice lacking C4 (Einav, 2002). Humans with Clq
deficiency develop SLE almost uniformly, as do mice in which the Clq gene is
deleted (Botto M., 2001 ). The well-known association between SLE and complement
deficiency may reflect the role of the classical pathway in disposing of apoptotic
corpses (Waldport MJ, 2001). A number of signals distinguish apoptotic cells from
normal cells and a significant number of phagocyte receptors have been identified to
be involved in sensing the presence and the uptake of apoptotic cells (Savill, 2002;
Henson PM, 2006)
Apoptotic impaired cells express potential autoantigens on their cell
surface
Apoptosis acts to preserve peripheral T cell homeostasis, participating m the
elimination of both immature thymocytes during thymic development and mature
peripheral T cells following antigen stimulation (Janssen, 2000; Zandman-Goddard,
2002). The combined action of apoptosis and anergy are results in a state of peripheral
tolerance but this balance is altered in autoimmune progression (Abbas, 2004).
10

Introduction
Apoptosis contributes to autoimmune phenomena via the failure to terminate immune
responses and to control autoreactive lymphocytes (Fadeel, 2005). A significant number
of investigations have linked the failure to achieve programmed cell death or to clear
apoptotic cells induces autoimmunity (Fadeel, 2005; Maniati, 2008). Although defects
in apoptosis propagate autoimmunity and disease susceptibility, however a breakdown
of multiple immunoregulatory mechanisms is required for full disease penetrance. The
disease phenotype generated by targeted deletion of the Clq gene and impaired
clearance played an important role in apoptotic cell clearance (Figure 5).
•· NllriiWII conditions
b. Autoimmunity/Mer chfldenqt
Low flux
High flux
Mor
SR-A
CDl6
• Robvit production of antl·
.............. lnfl•-•tory
......,.. cytollnH
•Tcall•lcall toleranu
• LowerptVduction ofantl· lnfl<tmmotory cytotlnes
• T call I I cell tolerance
• Pro-Immune .,_..,tatioft of self· antigen
• Autoimmunity
Figure 5. Impaired clearance of apoptotic cells cause autoantigens to initiate systemic
autoimmunity. (Rosen eta/., 2001, Nature Med Reviews)
In autoimmunity, a buildup of non-phagocytosed apoptotic cells was occurs and
consequently undergoes modification of antigen structure. Thus a pro-immune
presentation of the self-antigen induces an autoimmune response (Rosen, 2001,
Mitchell DA, 2002).
11

Introduction
The ongm of the autoantibodies typically present in the sera of patients with
autoimmune conditions such as SLE (often directed towards intracellular antigens
such as DNA, ribonucleoproteins and nucleosomes) has been perplexing as these
autoantigens are normally invisible to the immune system because of their localization
within the cell (Stuart, 2002). Cells undergoing apoptosis exposes potential
autoantigens upon their cell surface which make them available for interaction with
immunologically competent cells (Maniati, 2008). The autoantigens expressed by
apoptotic cells are immunogenic and altered self motifs developed by undergoing
various post-translational modifications (Eggleton, 2008). Cleavage by granzyme B
(GrB) is predictive for autoantigenicity of self-proteins, thereby further implicating
CTL-induced death in the initiation and propagation of autoimmunity (Darrah, 2010).
However, unique modification of potential intracellular autoantigens raises the
possibility that cytotoxic lymphocyte-mediated death of target cells may play a
specific role in the development of autoimmunity (Niland B, 20 I 0).
A number of protein autoantigens have been shown to have undergone
post-translational modification (Doyle, 2001 ). Rheumatoid arthritis patients frequently
have antibodies to citrullinated proteins, which can be demonstrated in inflamed
synovium (Baeten, 2001). Many SLE-associated autoantigens undergo cleavage
during apoptosis, and it has been argued that this process and also phosphorylation
render these proteins immunogenic (Utz, 2000). Autoimmunity may reflect epitope
spreading, that is, the recruitment ofT cells reactive to additional epitopes on the
autoantigen (Anderton, 2002).
Tolerance usually does not extend to all epitopes, however a mechanism capable of
enlisting progressively more autoreactive T cells might amplify any initial breakage
of tolerance (Ho, 2006). B cells expressing antibody cross-reactive with self
determinants could then selectively take up autoantigens, process them, and express
autoantigenic peptides, including cryptic epitopes (Farris, 2000).
12

Introduction
Figure 6. The sequestration of various autoantigens from the apoptotic cells which
have the potential to induce an inflammatory response due to dysfunctional clearance
mechanisms. A cell that is undergoing apoptosis releases debris containing molecules that
have localized in surface blebs. Abundant evidence indicates that these molecules travel to
where they can stimulate the formation of autoantibodies. Other evidence shows that certain
structural features of these molecules, such as coiled-coils, contribute to the probability that
they will induce an immune response (Plotz, 2003).
Defective clearance of apoptotic cells induces autoimmunity
Defects of apoptotic pathways in T cells promote the survival of potentially
autoreactive, proinflammatory cells (Pamaik R, 2000). Failure to eliminate activated
cells can result in prolonged effector functions, such as CD40 ligand for B cells,
inappropriate survival of primed autoantibody-producing B cells, or cytokine release
by macrophages (Maniati E, 2008).
A common feature of autoimmune diseases is the breakdown of tolerance of self
antigens, a consequence of which is the production of autoantibodies reactive with
multiple self proteins. Apoptosis acts as a source of immunogens (Nagata 2010,
Maniati E, 2008). It has been speculated that highly accelerated rates and/or abnormal
sites or abnormal processing of apoptotic cells could lead to autoantibody production.
The elucidation of the biochemical pathways and specific proteins that regulate
apoptosis provide a remarkable opportunity to manipulate the fate of the cell
(Stuart L et a!., 2002).
13

Introduction
Diminished clearance of apoptotic
' cells e.g. C1 q Autoantigen deficiency presentation by dendritic cells
' t Autoimmune
/ Disease
Facilitation of autoimmune
Diminished
/' responses apoptosis of autoreactive lymphocytes e.g. Fas mutation
Stuart L et a/ , 2002
Figure 7. The mechanisms responsible for autoimmune disorder (Stuart eta/., 2002)
Figure 8. This figure shows the possibility that the encounter leads also to the entry of
the tRNA synthetase into the immature DC and the maturation of the immature DC into
a mature APC, probably with the help of other local cytokine signals. The synthesis of
autoantibodies, shown on the right, might follow conventional T-cell-dependent or -
independent pathways. APRIL, a proliferation-inducing ligand; BAFF, B-cell-activating
factor of the tumour-necrosis factor family; BAFFR, BAFF receptor; PRR, pattern
recognition receptor; TLR, Toll-like receptor (Plotz, 2003).
14

Introduction
The molecules that elicit an autoantibody response are likely to do so in the same
manner as does foreign antigen. Presumably, this involves interaction with the surface
of an immature dendritic cell (DC) or other antigen-presenting cell (APC).
Autoantigens have shown chemoattractive for immature DCs are histidyl-transfer
RNA synthetase (His-RS), through interaction with CC-chemokine receptor 5
(CCR5); and asparaginyl-tRNA synthetase (Asn-RS), through interaction with CCR3
(Plotz, 2003).
The failure to achieve programmed cell death or to clear apoptotic cells causes the
autoimmune phenomena via two ways. The failure to terminate immune responses
and to control autoreactive lymphocytes and other is the exposure of self-antigens
in an inflammatory context that can initiate immune responses against
them (Fadeel, 2005). Although, defects in apoptosis propagate autoimmunity
and significantly contribute to disease susceptibility, a breakdown of
multiple immunoregulatory mechanisms is required for full disease penetrance
(Maniati, 2008). Apoptotic cells have been proposed as a possible source of nuclear
SLE autoantigens (Plotz PH, 2003). A defect in the clearance machinery and a
subsequent overload of apoptotic cells is a potential mechanism for the breakdown of
self-tolerance in SLE (Potter PK, 2003). The generation of the autoimmune response
is that non-ingested apoptotic cells undergo secondary necrosis, favoring responses
against self-antigens (Fadeel, 2005).
Tumour suppressor protein "p53"
In order to elucidate the mechanism responsible for apoptotic impairment, p53 gene
was studied, as p53 is the apoptosis inducing gene and p53 triggers the apoptotic
phenomenon. A significant number of p53 inducible genes are under expressed and a
number of p53 repressible genes are over expressed in autoimmune PBMCs
(Aune et al., 2004). The p53 tumor suppressor gene, a nuclear transcription factor,
plays an important role in the control of cell proliferation and apoptosis. The pivotal
· role of p53 in maintaining genomic integrity has earned it the nickname "guardian of
the genome" (Vogelstein, 2000). The consensus DNA-binding sequence for p53
consists of two repeats of the 10 bp motif 50-PuPuPuC(A/T)(A/T)GPyPyPy-30
separated by 0-13 bp ( elDiery, 1992 ). Activation of p53 by cellular stresses such as
DNA damage, hypoxia and oncogene activation leads to the induction of cell cycle
15

Introduction
arrest or apoptosis. Transactivation of the p53 target genes p21, GADD45 and 14-3-3
is involved in mediating cell cycle arrest by p53 ( elDeiry, 1995; Kastan 1992;
Hermeking, 1997; Chan 2000). Transcriptional repression by p53 has been shown be
important for the promotion of apoptosis (Ho, 2003). Targets of p53 mediated
repression include cyclin B1, b-tubulin, Map4, survivin, AFP and POLD1 genes
(Innocente, 2005; Li, 2001).
Mutational inactivation of p53
Once p53 dependent mechanisms are broken, conditions for the rapid accumulation of
genetic changes are established. The most common changes to the p53 gene are
missense point mutations within the coding regions. Over 80% of point mutations are
localized within the specific DNA binding domain of the p53 protein (Blagosklonny,
2000). A large number of p53 point mutations are have a dominant negative effect,
that transform the cells by acting as inhibitory proteins competing with and blocking
the activity of endogenous wild type p53 protein. Dominant negative p53 mutants
possesses an incorrect protein conformations and produce inactive mixed tetramers
with wild type p53 (Chan et al., 2004). Inactivation of wild-type p53 by mutant p53 is
generally thought to inhibit p53 binding to DNA (Nicholls et al., 2002; Willis et al.,
2004). Besides losing p53 function, some mutant p53 proteins acquire a novel
function that contributes to transformation and oncogenic potential by mode of "gain
of function" mutants (Dittmer et al., 1993; Blagosklonny, 2000).
Non-mutational inactivation of p53
Whenever wild type p53 does not retains its active pathways and any mutation if not
found, then there is always a possibility of its inactivation either by non-mutational
pathways. A range of various posttranslational modifications like phosphorylation,
acetylation, ubiquitination etc also decides the functionality as well as inactivation of
p53 protein (Coutts, 2009). Some of the normal cellular functions of p53 can be
modulated and sometimes inhibited by interaction with viral oncoproteins like SV 40
large T antigen, adenovirus ElB, HPV E6 protein or with the cellular protein E3
ligase Mdm2. Inactivation of p53 also includes ARF through gene deletion, promoter
methylation and aberrant subcellular localization of p53 (Puisieux et al., 2006).
16

Introduction
p53 ubiquitination
In normal cells, p53 is present at extremely low levels because the protein is very
rapidly degraded following synthesis. p53 is subject to a variety of post-translational
modifications, including phosphorylation, sumoylation, acetylation, methylation and
ubiquitination, which all impact significantly on p53 activity (J.P. Kruse, 2008). A
pictorial representation of p53 protein showing the domains and amino acids involved
with ubiquitination.
However, p53 can be modified by several E3 ubiquitin ligases, including MDM2,
CHIP, Pirh2, COPl , ARF binding protein and E6AP (Marine, 2010; Tripathi et al,
2007; Brooks, 2006; Yang, 2004).
p53
1-100 101-300 301-393
Transactivation DNA binding Neg
Ill rv
~p60 Mdm2
P300/CBP
Mdmx
Figure 9. Showing the domains of mdm2 and p53 involved with protein-protein
interactions and sites of p53 ubiquitination (Coutts, 2009).
One of the important components of the p53 degradation pathway is Mdm2. Mdm2
tightly and affects its cellular localization, stability and activity through a variety of
mechanisms (Marine, 2010). Mdm2 is an E3 ligase of p53 and itself the product of
p53 inducible gene (Honda, 2000; Fang, 2000; Yang, 2004). It binds toN-terminus of
p53 and inhibits p53 transactivation function as well as induces its degradation by
ubiquitination. Mdm2 monoubiquitinates six lysine residues (370, 372, 373, 381 , 382,
386) at C-terminal region ofp53 (Lai Z, 2001). Ubiquitination ofp53 has emerged as
a mechanism of p53 control which plays important roles in regulating its stability and
activity (Coutts, 2009).
17

Introduction
Relevance of Biomarkers in autoimmunity
The goal of studies of autoimmune disease biomarkers is to identity markers that
fluctuate with disease development and severity, and then normalize following
successful therapy (Casiano, 1998). The development of genomic and proteomic
technologies provides an unprecedented ability to identify novel biomarkers to
diagnose, classify, and guide therapeutic decision making in patients with
autoimmune disease. Peripheral blood is a convenient and rich source of potential
biomarkers, but surveying purified cell populations and target tissues can also
enhance our understanding of disease states (Olsen, 2004).
A biomarker indicates a change in expression or state of a protein that correlates with
the risk or progression of a disease, or with the susceptibility of the disease to a given
treatment. Biomarkers are characteristic biological properties that can be detected and
measured in parts of the body fluids and tissues. They may indicate either normal or
diseased processes in the body. Biomarkers can be specific cells, molecules, or genes,
gene products, enzymes, or hormones (Gibson, 2010). The structural modification
during cytotoxic granule-induced cell death is a frequent and striking feature of
autoantigens, and may be an important principle driving disease. Such autoimmune
disease-specific arrays include self-antigens, viral proteins and peptides, and bacterial
antigens with complex carbohydrates and recombinant proteins (Fathman, 2005).
The perfect marker could serve as a diagnostic tool, as well as a monitoring device for
therapeutic drug efficacy. Current biomarker discovery efforts are focused on three
groups of proteins reflective ofthe autoimmune disease process:
( 1) Degradation products arising from destruction of affected tissues,
(2) Enzymes that play a role in tissue degradation,
(3) Cytokines and other proteins associated with immune activation (Prince, 2005).
A list showing the serum biomarkers that are overexpressed during autoimmune
condition development and progression and induces an immune response against the
secreted proteins is shown below (Table 1 ).
18

Introduction
Tablet. List of serum biomarker proteins expressed in various
autoimmune disorder conditions.
Autoimmune Disease Biomarker Antigen Humoral response Reference SLE IFN-alpha Autoantibodies Kirou, 2005
Pro-inflammatory mediators
SLE Nephrities components of Autoantibodies Rovin, 2007
complement (C3 , C4), to C3 and C4,
double stranded DNA anti-double stranded DNA antibodies (ADNA).
SLE andMCTD 70 kDA, Ribonucleo Auto-antibodies Salmhofer , conditions protein 2007
Hypocomplementemic Cl q Anti-C1q Mok, 2010 urticarial vasculitis, non- autoantibodies SLE active glomerulonephritis
TP53 SLE, Rheumatoid TBP Anti-p53 Chauhan et arthritis, organ-specific autoantibodies al. , 2004 autoimmune diseases, Anti-TBP MCTD/OS autoantibodies
serum C-type Inflammation Olewicz-
Systemic Sclerosis natriuretic peptide Anti -centromere,
Gawlik , (CNP), 2010
anti-Sci 70 antibodies, anti-
Doran, 2008 RNA polymerase III, anti-fibrillarin
Willebrand factor, Endothelial cell Tinazzi, vascular endothelial damage and skin 2010 growth factor, fibrosis intracellular adhesion molecule- I, monocyte chemotactic protein-!
RNA Pol III anti-RNA polymerase III Nihtyanova, antibodies 2010
CD31 was used as a reduction in the Akhmetshina pan-endothelial cell number of , 2010
19

Introduction
marker lymphatic capillaries and lymphatics vessels
CCR5 Delta32 Autoantibodies Martens,
Rheumatoid arthritis 2009
Impaired Tolluso, ZAP-70 ofB cells apoptosis, 2009
immune activation Prolonged Survival
citrullinated alpha- Autoantibodies Lundberg, enolase 2008
circulating TNF- Autoantibodies Corona-alpha and E-selectin and Tissues Sanchez , (sE-selectin) damages 2009
Multiple Sclerosis VLA -4 integrin neuroinflammato Brahamachar ry cascade in i, 2010 CNS
Relapsing-remitting Interferon beta Inflammatory Gandhi, 201 0 (IFNbeta) Signalling
Multiple sclerosis Prolyl oligopeptidase N erurodegenerati Tenorio-(RRMS). (POP) on and Laranga ,
Inflammatory 2010 responses
aquaporin 4 anti -aquaporin 4- Min, 2010
Sjogren's syndrome antibody
Auto-antibodies Tobon, 2010 tyrosine kinase3- mediated chronic ligand damages of
lymphoid tissues
Wegener's membrane-bound anti-neutrophil Westra, 2009 Granulomatosis PR3 (mPR3) cytoplasmic
autoantibodies (AN CAs)
Autoimmune amylase a-2A amylase a-2A JWWiley, pancreatitis (AlP) autoantibodies 2009
Biomarker protein arrays have been constructed and validated for over a number of
autoimmune diseases, including connective-tissue diseases (such as SLE, scleroderma
and myositis), primary biliary cirrhosis, experimental autoimmune encephalomyelitis
and multiple sclerosis, rheumatoid arthritis, diabetes, Crohn's disease, and sclerosing
cholangitis (Fathman, 2005).
20

~ CV) '--~ '-
I
~
Introduction
The systemic autoimmune diseases are a complex group of disorders characterized by
elaboration of high titer autoantibodies and immune-mediated damage of tissues. The
presence of a immune effector pathways drive the generation/release of autoantigens,
which in tum fuel the immune response (Rosen, 1999, 2001; Fadok, 2001). Protein
arrays have been shown to have applications in profiling the antibody repertoire in
healthy individuals and subjects with autoimmune diseases (Cahill, 2001). A humoral
immune response is generated to disease associated antigens during the development
of autoimmune diseases and rendering serum autoantibody detection suitable for
early-stage diagnosis of autoimmune diseases. Analysis of relevant signaling
pathways at the protein level is an important step towards understanding the
functional consequences of aberrant gene expression in autoimmunity.
Autoantigen
Autoantibodies
Tcell Beef!
Figure 10. Discrete components of the autoimmune process from the presentation of MHC-peptide complexes to T cells to the production of autoantibodies by plasma cells analyzed using various genomic and proteomic technologies. The numbers in the figure indicate the technologies that have demonstrated potential in the analysis of the corresponding components. (1) Peptide-MHC tetramer arrays. (2) Reverse-phase protein analysis (3) Multiparameter flow cytometry for intracellular antigens. (4) eDNA analysis and oligonucleotide microarrays. (5) Antibody profiling (6) Bead-based multiplex assays. (7) Autoantigen analysis and profiling (8) Wholeproteome analysis by 20-PAGE. Both mass spectrometry and 2D gel electrophoresis can be used to analyze complex mixtures of proteins and/or peptides (Fathman CF, 2005).
21

Introduction
In this study, the objectives were to identify novel biomarkers which are
overexpressed during autoimmunity. The delineation of such targets are important for
the understanding of mechanisms responsible for autoimmune disorder. By finding
the biomarkers of the diseases, therapy can be elucidated in order to minimize the
pathological severity and diseases spreading. We have implemented 2D-PAGE
proteomics based strategies to find the autoantigens profiles. Direct evidences have
shown defective apoptotic machinery with the development of autoimmune disorder,
however genetic evidences also had shown that defects in individual cell-death genes
can lead to autoimmune disorders. To detect the whether p53 function was impaired
in autoimmune condition, we will investigate the factors responsible for p53
inactivation. Further, to elucidate the mechanisms responsible for apoptotic
impairment in PBMCs of autoimmune patients. The role of overexpressed co
activators or transcription factors in autoimmunity and their cross-talk with p53
inactivation is of our interest. In concise biomarker protein analyses in autoimmune
disorder and their role in context to inactivation of p53 protein and apoptosis will be
described in the following thesis. We presented here experimental evidence and
mechanisms for autoimmune disorder phenomenon due to aberration of the apoptosis
and p53 inactivation. In view of this, following were the main aims and objectives of
the study undertaken:
22