Embed Size (px)
Citation preview

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis CompanyCopyright © 2010 F.A. Davis Company
Autoimmunity
Chapter Fourteen

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Autoimmune diseases are conditions in
which damage to organs or tissues results
from the presence of autoantibody or
autoreactive cells.
This is thought to be caused by the loss or
breakdown of self-tolerance; believed to be
brought about by several mechanisms,
including clonal deletion of relevant effector
cells and active regulation by T reg cells.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Thus, in the secondary lymphoid organs,
peripheral tolerance is maintained by a delicate
balance between the T helper cell type 1 (Th1)
and T helper cell type 2 (Th2) populations.
Recent findings indicate that regulatory T cells
(Tregs) play a central role in maintaining this
balance and eliminating harmful autoimmune
responses. Also recall the roles of IL-10 and TGF-
beta.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Major histocompatibility complex (MHC)
products also seem to influence antigen
recognition or nonrecognition by determining
the type of peptides that can be presented to
the T cells.
The expression of class II molecules on cells
where they are not normally found may result
in the presentation of self-antigens for which
no tolerance has been established.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity The strongest link found to date between
certain HLA molecules and specific diseases is
between HLA-B27 and ankylosing spondylitis.
Several other mechanisms are thought be
contribute to autoimmunity: release of
sequestered antigens, molecular mimicry, and
polyclonal B-cell activation due to abnormal
expression or function of cytokines and/or
receptors

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Autoimmune diseases can be classified as
systemic or organ specific.
Organ specific disorders for thyroid,adrenal
cortex, pancreas, nervous tissue

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Systemic lupus erythematosus (SLE) is a
chronic systemic inflammatory disease
marked by alternating exacerbations and
remissions.
The immune response is directed against a
broad range of target antigens, as the typical
patient has an average of three circulating
autoantibodies.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE It appears that there is an interplay between
genetic susceptibility and environmental
factors in the development of the disease.
In whites, there is a strong association with
human leukocyte antigens (HLA) DR and DQ.
Lupus has been associated with inherited
deficiencies of complement components C1q,
C2, and C4.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE Abnormalities of Fc γ receptors on B cells,
macrophages, dendritic cells, and neutrophils that
bind IgG and prevent excessive immune
reactions have also been found.
Environmental factors include exposure to
ultraviolet light, certain medications, and
infectious agents.
Hormones, especially estrogen. These disorders
occur 10 times more often in women; onset in the
30-40s.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE The clinical signs of SLE are extremely
diverse, and nonspecific symptoms such as
fatigue, weight loss, malaise, fever, and
anorexia are often the first to appear.
Joint involvement seems to be the most
frequently reported manifestation, presenting
as a symmetric arthritis that involves the small
joints of the hands, wrists, and knees.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE After joint involvement, the next most
common signs are skin manifestations.
A classic butterfly rash across the nose and
cheeks may develop.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE One-half to two-thirds of all patients exhibit
evidence of renal involvement, with diffuse
proliferative glomerulonephritis (DPGN),
deposition of immune complexes in the
subendothelial tissues and thickening of the
basement membranes.
All of these can lead to renal failure, the most
frequent cause of death in patients with SLE.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE For a clinical diagnosis of lupus to be made, 4
of 11 specific criteria must be present: malar
rash, discoid rash, photosensitivity, oral ulcers,
arthritis, serositis, renal disorder, neurological
disorder, hematologic disorder, immunologic
disorder, and presence of antinuclear
antibodies.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE SLE is associated with more than 25
autoantibodies.
Some of the more common autoantibodies are
listed in Table 14-2.
The large number of possible autoantibodies
reflects a generalized dysregulation of the
immune system in SLE.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE The constant presence of antigenic material
triggers polyclonal activation of B cells.
There is an accompanying alteration in the
function of both Th1 and Th2 helper cells,
resulting in enhanced production of certain
cytokines that contribute to up-regulation of
antibody production by B cells (eg. IL-4 and
IL-6).

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE Drug-induced lupus differs from the more
chronic form of the disease in that symptoms
usually disappear once the drug is
discontinued.
Typically, this is a milder form of the disease,
usually manifested as fever, arthritis, or
rashes; the kidneys are rarely involved.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE When SLE is suspected, the first test
typically done is a screening test for
antinuclear antibodies (ANA).
Fluorescent antinuclear antibody (FANA)
testing is the most widely used and accepted
test, because it detects a wide range of
antibodies and is positive in about 95 percent
of patients with SLE.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE This is an extremely sensitive test and relatively
easy to perform, but it has low diagnostic
specificity, because many of the antibodies are
associated with other autoimmune diseases.
Approximately 2 percent of healthy individuals
and up to 75 percent of older individuals yield
false-pos. results.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE Conversely, up to 5 percent of SLE patients
yield false-negative results.
It is now common practice to screen with a
1:80 dilution (or 1:160 if the patient is over 65)
to avoid low positive titers in the normal
population.
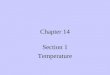
A diagram of the possible fluorescent patterns
is shown in Figure 14-2 (see also Color Plate
10 in the text).

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE Double-stranded DNA (ds-DNA) antibodies
are the most specific for SLE, because they
are mainly seen only in patients with lupus,
and levels correlate with disease activity.
The presence of these antibodies is
considered diagnostic for SLE, especially
when they are found in combination with low
levels of complement C3.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE Antibodies to ds-DNA typically produce a
peripheral or a homogeneous staining
pattern on FANA testing.
Other assays that can be used to detect
antibodies to ds-DNA include immunodiffusion,
particle agglutination and enzyme
immunoassay (EIA).

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE A second major antibody found in lupus
patients is antihistone antibody.
Histone is a nucleoprotein that is a major
constituent of chromatin.
Presence of antihistone antibody alone or
combined with antibody to ss-DNA supports
the diagnosis of drug-induced lupus.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE Antihistone and anti-DNP antibodies are also
found in lupus but are not diagnostic as they
may be seen in rheumatoid arthritis (RA) and
primary biliary cirrhosis, but the levels are
usually lower.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE On FANA, either a homogeneous pattern is
seen, representing fluorescence of the entire
nucleus, or staining of the periphery of the
nucleus occurs.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE Figure 14-2

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE Antibody to a preparation of extractable
nuclear antigen (small nuclear proteins that
associated with uridine-rich RNA) was first
described in a patient named Smith, hence the
name anti-Sm antibody.
The anti-Sm antibody is specific for SLE,
because it is not found in other autoimmune
diseases.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – SLE This and other antibodies produce a coarsely
speckled pattern of nuclear fluorescence on
FANA.
Other ANA patterns include
nucleolar, seen in systemic sclerosis and RA
centromere,seen in CREST syndrome
mitochondrial

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Antiphospholipid antibodies are a
heterogeneous group of antibodies that bind to
phospholipid alone or lipoprotein.
They can affect every organ in the body, but
they are especially associated with deep-vein
and arterial thrombosis and with morbidity in
pregnancy.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity The lupus anticoagulant, one of the several
types of antiphospholipid antibodies, was so
named because it produces prolonged
activated partial thromboplastin time (aPTT)
and prothrombin time (PT).
The lupus anticoagulant may also cause false-
positive results for the VDRL test for syphilis.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Patients with this antibody have an increased
risk of clotting and spontaneous abortion.
Platelet function may also be affected.
There are several EIA methods for
antiphospholipid antibodies that are sensitive
and relatively simple to perform.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Rheumatoid arthritis (RA) is another
example of a systemic autoimmune
disorder.
RA can be characterized as a chronic,
symmetric, and erosive arthritis of the
peripheral joints that can also affect multiple
organs such as the heart and the lungs.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA In addition to a decline in functional ability,
there is a reduced life expectancy.
As in SLE, there appears to be an association
of RA with certain MHC class II genes.
The strongest association appears with certain
DR4 alleles.
This “shared epitope” on the HLA class II β
chain may act to facilitate antigen presentation
to Th cells and to B cells.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA Key symptoms: morning stiffness around the
joints lasting at least 1 hour; swelling of the
soft tissue around three or more joints;
swelling of the proximal interphalangeal,
metacarpophalangeal, or wrist joints;
symmetric arthritis; subcutaneous nodules; a
positive test for rheumatoid factor (RF); and
radiographic evidence of erosions in the joints
of the hands, the wrists, or both.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA Other systemic symptoms of RA may include
anemia, pericarditis, lymphadenopathy,
splenomegaly, interstitial lung disease, or
vasculitis.
For many years, there has been a search for
an infectious agent or agents that may be
involved in the cause of RA, but a causal
relationship has not been established.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA The earliest lesions in rheumatoid joints
show an increase in cells lining the synovium
and an infiltration of mononuclear cells, CD4+
and CD8+ T lymphocytes, B cells, plasma
cells, macrophages, and neutrophils.
The balance between proinflammatory and
anti-inflammatory cytokines appears to be
tipped toward continual inflammation.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA Proinflammatory cytokines found in synovial
fluid include interleukins, and tumor necrosis
factor-alpha (TNF-α).
Collagenase and other tissue-degrading
enzymes are also released from cells that line
the joint cavity.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA The end result is destruction of connective
tissue, cartilage, and bone.
Approximately 75 percent of patients with RA
have the rheumatoid factor antibody (RF).
It is most often of the IgM class and is directed
against the FC portion of IgG.
However, this antibody is not specific for RA,
as it is found in 5 percent of healthy individuals
and in 10–20 percent of those over 65.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA In RA, IgM antibodies combine with IgG, and
these immune complexes become deposited
in the joints, resulting in a type III (or immune
complex) hypersensitivity reaction.
The complement protein C1 binds to the
immune complexes, activating the classical
complement cascade.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA C3a and C5a are generated, which act as
chemotactic factors for neutrophils and
macrophages.
Other autoantibodies found include antikeratin
antibody, antiperinuclear antibody, antifilaggrin
(nucleolar staining in FANA), and anti-Sa
antibody.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA All of these antibodies are directed against
citrullinated proteins.This family of antibodies
is detected using cyclic citrullinated peptides
(CCP); hence, the antibodies are called anti-
CCP.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – RA Anti-CCP is now the lead marker for
detection of RA, because it is much more
specific than RF. EIA shows 74% sensitivity
and specificity of 96%; precedes symptoms by
several years
In addition, low titers of antinuclear antibodies
are present in about 40 percent of patients.
The pattern most identified is the speckled
pattern directed against ribonucleoprotein.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis CompanyCopyright © 2010 F.A. Davis Company
Autoimmunity - RAOther nonspecific indicators of
inflammation:
ESR, CRP, and complement components
Treatment: NSAIDs, injectable cortisone,
anti-TNF and anti-TNF receptor, and anti-
CD20 on B cells

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Autoimmune thyroid diseases (AITDs),
including Hashimoto’s thyroiditis and Graves’
disease, are examples of organ-specific
autoimmune diseases.
Although these conditions have distinctly
different symptoms, they do share some
antibodies in common, and both interfere with
thyroid function.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD Follicles within the thyroid are filled with
material called colloid.
The primary constituent of colloid is
thyroglobulin, a large iodinated glycoprotein,
which is the storage form of the thyroid
hormones triiodothyronine (T3) and thyroxine
(T4).

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD Under normal conditions, thyrotropin-releasing
hormone (TRH) is secreted by the
hypothalamus to initiate the process that
eventually causes release of hormones from
the thyroid.
TRH acts on the pituitary to induce release of
thyroid-stimulating hormone (TSH).

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD TSH, in turn, binds to receptors on the cell
membrane of the thyroid gland, causing
thyroglobulin to be broken down into
secretable T3 and T4.
Production of autoantibodies interferes with
this process and causes under- or overactivity
of the thyroid.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD Hashimoto’s thyroiditis, also known as
chronic autoimmune thyroiditis, is most
often seen in middle-aged women, although it
may occur anywhere from childhood up to
about 70 years of age.
Patients develop a combination of goiter (or
enlarged thyroid), hypothyroidism, and thyroid
autoantibodies.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD Symptoms of hypothyroidism include dry
skin, decreased sweating, puffy face with
edematous eyelids, weight gain, and dry and
brittle hair.
The thyroid shows hyperplasia with an
increased number of lymphocytes, altering the
cellular architecture of the thyroid.
Antibodies to thyroglobulin predominate,
progressively destroying thyroglobulin.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD Graves’ disease is characterized by
hyperthyroidism and is the most prevalent
aotimmune disease in the US.
The disease is manifested as thyrotoxicosis, with
an enlarged goiter, accompanied by nervousness,
insomnia, depression, weight loss, heat
intolerance, sweating, rapid heartbeat,
palpitations, breathlessness, fatigue, cardiac
dysrhythmias, and restlessness.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunityn – AITD
The major antibodies found in Graves’
disease include thyroid-stimulating hormone
receptor antibody (TSHRab) and antibodies to
thyroid peroxidase.
Strong association with DR3

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD When antigen–antibody combination occurs, it
mimics the normal action of TSH and results in
receptor stimulation, with the release of thyroid
hormones to produce the symptoms of
hyperthyroidism.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD The three major thyroid autoantibodies
present are antibodies to thyroglobulin,
thyroid peroxidase, and TSH receptors.
Antibodies to thyroglobulin can be detected
in 90% of patients with Hashimoto’s thyroiditis.
Healthy individuals may have a low titer of
antithyroglobulin antibody, but in patients with
Hashimoto’s thyroiditis, the titer is
considerably higher.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD Antibodies to thyroglobulin can be
demonstrated by indirect immunofluorescent
assays (IIF), passive agglutination, and EIA.
Since antithyroglobulin antibodies are not
found in all patients, a negative test result
does not necessarily rule out Hashimoto’s
disease.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD Antibodies to peroxidase are most commonly
measured by EIA, although IIF and particle
agglutination assays are also used.
These antibodies can be found in
approximately 90 percent of patients with
Hashimoto’s disease and 80 percent of
patients with Graves’ disease, so the two
cannot be distinguished on the basis of
this test.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – AITD The third major autoantibody, anti-TSHR
antibody, is typically associated with
Graves’ disease.
Elevation of the thyroid hormones and free
triiodothyronine (T3) and thyroxine (T4) is
checked first if this disease is suspected.
TSH levels are low because of antibody
stimulation of the thyroid.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis CompanyCopyright © 2010 F.A. Davis Company
Autoimmunity - AITD
Anti-TSHR found in Hashimoto's
disease binds to a different epitope,
preventing the binding of TSH,
leading to reduced T3 and T4

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Autoimmune diabetes mellitus, now termed
type IA diabetes, is a chronic autoimmune
disease that occurs in genetically susceptible
individuals as a result of environmental
factors.
Approximately 10 percent of patients with
diabetes mellitus have the immune-mediated
form of the disease.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – DM This form of diabetes mellitus is characterized
by insufficient insulin production caused by
selective destruction of the beta cells of the
pancreas, located in clusters called the islets
of Langerhans.
Family studies indicate that there is an
inherited genetic susceptibility to the disease,
probably attributable to multiple genes within
the HLA system.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – DM Environmental influences include the
possibility of viral infections and early
exposure to cow’s milk.
Antibody production could possibly be initiated
as a result of molecular mimicry, with a virus
as the stimulating antigen triggering antibody
production against a self-antigen.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – DM Progressive inflammation of the islets of
Langerhans in the pancreas leads to fibrosis
and destruction of most beta cells.
The subclinical period may last for years, and
only when 80 percent or more of the beta cells
are destroyed does hyperglycemia become
evident.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – DM The generalized inflammation that results is
responsible for the destruction of beta cells.
It is apparent that autoantibody production
precedes the development of type IA diabetes
mellitus by up to several years.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – DM Among the antibodies found are antibodies
to two tyrosine phosphatase-like
transmembrane proteins called insulinoma
antigen 2 (IA-2 or ICA 512) and IA-2βA
(phogrin); anti-insulin antibodies; antibodies to
the enzyme GAD; and antibodies to various
other islet cell proteins, called islet cell
antibodies (ICAs).

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Multiple sclerosis (MS) is an inflammatory
autoimmune disorder of the central nervous
system.
It is characterized by the formation of lesions
called plaques in the white matter of the brain
and spinal cord, resulting in the progressive
destruction of the myelin sheath of axons.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – MS As is the case for most other autoimmune
diseases, a combination of genetic and
environmental factors is responsible for
development of MS.
Once initiated, the immune response becomes
directed against self-antigens that are
indistinguishable from the original foreign
antigen.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – MS Within the plaques, T cells and macrophages
predominate, and they are believed to
orchestrate demyelination.
Antibody binds to the myelin membrane and
may initiate the immune response, stimulating
macrophages and specialized phagocytes
called microglial cells.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – MS The cascade of immunologic events results in
acute inflammation, injury to axons and glia,
structural repair with recovery of some
function, and then postinflammatory
neurodegeneration. (relapse, remission
pattern)
Activated T cells must penetrate into the
central nervous system to begin the response.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – MS The two most common tests for diagnosis
of MS are oligoclonal banding and the CSF
IgG index.
Oligoclonal bands are increased in the spinal
fluid in 75–90 percent of patients with MS,
producing several distinct bands on protein
electrophoresis that are not seen in the serum.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Myasthenia gravis (MG) is an autoimmune
disease that affects the neuromuscular
junction. It is characterized by weakness and
fatigability of skeletal muscles.
Antibody-mediated damage to the
acetylcholine (ACH) receptors in skeletal
muscle leads to this progressive muscle
weakness.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – MG Early signs are drooping of the eyelids and the
inability to retract the corners of the mouth,
often resulting in a snarling appearance.
Other symptoms may include difficulty in
speaking, chewing, and swallowing and
inability to maintain support of the trunk, the
neck, or the head.
If respiratory muscle weakness occurs, it can
be life threatening.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – MG MG is often associated with the presence of
other autoimmune diseases, such as SLE, RA,
pernicious anemia, and thyroiditis.
MG is also associated several HLA antigen
abnormalities.
Approximately 80–85 percent of patients have
antibody to ACH receptors; this appears to be
the main contributor to the pathogenesis of the
disease.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
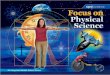
Autoimmunity – MG Normally, ACH is released from nerve endings
to generate an action potential that causes the
muscle fiber to contract.
When the antibody combines with the receptor
site, binding of ACH is blocked, and the
receptors are destroyed because of the action
of antibody and complement (see Fig. 14-5).

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – MG Figure 14-5

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity Goodpasture’s syndrome is characterized by
the presence of autoantibody to glomerular,
renal tubular, and alveolar basement
membranes.
Signs of renal involvement include gross or
microscopic hematuria, proteinuria, decreased
creatinine clearance, and increased BUN and
creatinine levels.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – GS Pulmonary symptoms include hemorrhage,
dyspnea, weakness, fatigue, and cough.
Severe necrosis of the glomerulus is triggered
by an antibody that has specificity for a
specific region of collagen.
Immune deposits accumulate, and
complement fixation causes injury because of
the release of oxygen species and proteolytic
enzymes.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – GS This syndrome differs from glomerulonephritis
as a result of the nonspecific accumulation of
circulating immune complexes found in other
autoimmune diseases.
In Goodpasture’s syndrome, specific
antibasement antibodies can be demonstrated
by the formation of a smooth, linear ribbonlike
pattern on direct immunofluorescent assay of
patient glomerular basement membrane.

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – Crohn’s disease An inflammatory GI disease appearing anywhere
between the mouth and the anus, mostly in the
large intestine; may present with bloody stools;
may be triggered by an undefined microbe
Leads to malabsorption and malnutrition
Therapy includes corticosteroids and antiTNF
Should be distinguished from celiac disease (due
to gluten) and irritable bowel syndrome (due to
gas production in the bowel; often linked to stress
and anxiety)

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity - Scleroderma Primarily in the skin but may involve multiple
organs
Breakdown of parenchymal tissue with
replacement by rapidly dividing fibroblasts.
Leads to excess collagen production and
stiffening or hardening of the tissue
Trigger for initial damage is unknown but ANA
(anti-centromere pattern) may be detected

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmunity – Sjorgren’s syndrome Clinically presents as dry eyes , dry mouth, dry
nasal passages, and vaginal dryness
50% of patients have other systemic
autoimmune disorders (SLE,RA, scleroderma)
Autoantibodies, including anti-RNP, and T cells
are involved in destruction of exocrine glands;
75% have RF.
Usually have leucopenia and elevated ESR

Clinical Immunology & SerologyA Laboratory Perspective, Third Edition
Copyright © 2010 F.A. Davis Company
Autoimmmunity – Addison’s disease Autoimmune destruction of the parenchyma of
the adrenal cortex, resulting in reduced
production of glucocorticoids and
mineralocorticoids
Often syptom-free until majority of organ is
destroyed