Embed Size (px)
Citation preview

Initiation of Repetitive Ventricular Depolarizations
By Relatively Late Premature Complexes in Patients
With Acute Myocardial Infarction
ROBERT ROBERTS, MD, FACC H. DIETER AMBOS CHRlSTOFMER W. LOH, MD BURTON E. SOBEL, MD, FACC
St. Louis, Missouri
From the Cardiovascular Division, Washington University School of Medicine, 660 South EMId Avenue, St. Louis. Missouri. Work from the au- thors’ laboratory was supported in part by Grant M 17646, SCAR in Ischemic Heart Disease and Grant HL 16608 from tha National Institutes of Health, Bethesda, h4atyland. Manuscript received August 9, 1977; revised manuscrlpt received October 19.1977, accepted October 26, 1977.
Address for reprints: Burton E. SoM. MD. Cardiovascular Division, Washington University School of Msdicine, 660 South EuclM Avenue, St. Louis, Missouri 83110.
To determine whether repetitive ventricular depolarizations are more commonty preclpltated by earty compared with late premature ventrkular complexes, we analyzed continuous electrocardlographlc recordings obtalned durlng the first 10 hours In 38 patients with myocardlal Infarction without shock with the Argus/H computer system with edttor verlfkatlon of all premature ventricular complexes. Eplsodes of repetltlve ventricular depolarization were deflned as two or more consecutive complexes at a rate of 120 beats/mln or greater. Premature ventricular complexes occurring with coupling intervals from the prm noimal complex equal to or less than the Q-T Interval of the normal complex were defined as early, and those with longer coupling Intervals as late. Among all pre- mature ventricular complexes, early premature ventricular complexes accounted for 38 percent. The average coupling Interval of premature ventricular complexes from a preceding notmal complex dld not correlate with heart rate, blood pressure, Infarct sire estimated enzymatlcally, the electrocardlographlc locus of Infarction or history of previous Infarctlon. Twenty-nlne patients had a total of 337 episodes of repetltlve ventrkular depolarizations. Somewhat surprlslngly, 78 percent of these eplsodes, and all eptsodes In 22 patients, were lnltlated by late premature ventrkular complexes. Thus, repetltlve ventricular depolarizations In patients with acute myocardlal lnfarctkn Bee often preclpltated by late rather than early premature ventricular complexes.
Continuous electrocardiographic monitoring of patients in coronary care units has established the importance of premature ventricular complexes in the initiation of ventricular tachycardia and ventricular fibrillation. Early premature ventricular complexes have appeared to be particularly malignant,‘s apparently because they occur at a time when repolari- zation is incomplete and the ventricle is therefore particularly vulnerable to malignant arrhythmia. lg2 It is clear that in experimental animals subjected to myocardial ischemia, repetitive ventricle depolarizations can be induced readily by stimulation of the heart during the vulnerable period. The most widely accepted clinical criteria characterizing haz- ardous premature ventricular complexes in patients include electro- cardiographic proximity of the premature complex to the T wave of the preceding beat. ss7 On the other hand, under some circumstances ven- tricular tachycardia may be initiated by late premature ventricular complexes, and perhaps even more striking, ventricular fibrillation may occur without any warning arrhythmia and without a discrete initiating premature ventricular complex. These distinctions may be far from trivial, for they may reflect fundamentally different electrophysiologic mechanisms responsible for sudden death in ambulatory patients with ischemic heart disease as well as for malignant arrhythmia in patients hospitalized with acute myocardial infarction.
676 April 1978 lha Afnerlcn Joumsl of CARDioLoGY vohane 41

LATE PREMATURE VENTRICULAR COMPLEXES AND INFARCTION-ROBERTS ET AL
This study was performed to characterize the relative frequency with which early compared with late pre- mature ventricular complexes initiate repetitive ven- tricular depolarizations in patients hospitalized with acute myocardial infarction. Accordingly, continuous electrocardiographic recordings from 38 patients with acute myocardial infarction during the first 10 hours after admission to the coronary care unit were analyzed by computer to quantify ventricular arrhythmia. The frequency of premature ventricular complexes and coupling intervals from normal supraventricular beats to each premature ventricular complex preceded by a normal complex were analyzed in relation to the inci- dence, severity and initiation of repetitive ventricular depolarizations. Results were assessed also in relation to blood pressure, heart rate, site of infarction, history of previous infarction and enzymatically estimated in- farct size based on analysis of serial changes in plasma creatine kinase (CK) activity.
Methods
Patients studied: Thirty-eight patients with acute myo- cardial infarction were selected for study. They were selected on the basis of the following criteria: (1) admission to the coronary care unit within 4 hours of the onset of symptoms, and (2) the presence of at least 10 premature ventricular complexes during the 10 hour recording interval. None ex- hibited profound hemodynamic decompensation (blood pressure 95/70 mm Hg or greater, heart rate 140 beats/min or less, urinary output 20 ml/hour or greater and arterial partial pressure of oxygen 60 mm Hg or greater). In each case, myo- cardial infarction was documented by serial electrocardio- graphic changes, elevated plasma enzymes including the MB isoenzyme of CK and positive technetium-99m pyrophosphate scintigrams. The group comprised 22 men and 16 women with a mean age of 58 years (range 36 to 81). Fifteen patients had had a previous remote myocardial infarction (documented electrocardiographically and on the basis of plasma enzyme changes more than 3 months before the new episode), and the remainder had no apparent previous infarction. The site of
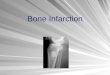
FIGURE 1. Histogram of coupling intervals from one patient during the 10 hour recording interval. Coupling intervals are measured from the onset of a preceding normal complex to the onset of an isolated premature ventricular complex, (PVC) or of the initial premature ventricular complex of a repetitive arrhyth- mia.
TABLE I
Patients Categorized According to Infarct Size
Infarct Size Index’ <
(no. q512) 25-50 >
(no. = 13) (no. 2’13)
Heart rate (beats/min)t 68 f 9 83 f 6 85f 11 Infarct size indext 14f2 31 f 2.4 58 f 4.6 Total number of PVCst 123 f 41 186 f 80 279 f 62 Lidocaine dose (mg)t 590 f 82 675 f 79 710 f 94 Patients with previous 6 4 5
myocardial infarction (no.)
l In CK-gram-equivalents/m2 body surface area. 7 Expressed as mean f standard error of the mean. $ Cumulative amount administered during the 10 hour recording in-
terval PVCs = premature ventricular complexes.
infarction was judged anterior in 22 patients, inferior in 14 and lateral in 2, on the basis of electrocardiographic and scinti- graphic criteria. All patients survived for at least 72 hours and were transferred from the coronary care unit within 5 days after admission.
Protocol: Continuous 10 hour electrocardiographic re- cordings were initiated within 2 hours of admission of each patient to the unit. Patients with 10 or more premature ven- tricular complexes per minute or two or more consecutive premature ventricular complexes were treated with bolus injections of lidocaine (1 mg/kg intravenously). If severe ar- rhythmia persisted, defined by the same criteria after two bolus injections within 20 minutes of each other, lidocaine was administered by continuous infusion and a diary was kept to record the total amount of lidocaine given. The mean total amount of lidocaine administered to patients in each group classified on the basis of infarct size is shown in Table I.
Serial blood samples for analysis of plasma CK and MB CK8 were obtained hourly through an indwelling heparin lock for the first. 10 hours and at 4 hour intervals for a total of 72 hours. The extent of infarction was estimated enzymatically based on cumulated CK released into plasma.g To avoid potential
0 200 400 600 800 1000
NORMAL-TO-PVC COUPLING INTERVAL l msec )
April 1978 The American Journal of CARDIOLOGY Volume 41 879

LATE PREMATURE VENTRICULAR COMPLEXES AND INFARCTION-ROBERTS ET AL.
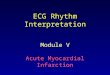
0 TOTAL PATIENTS
&j PATIENTS WITH EARLY 61 LATE PVCs
m PATIENTS WlTH ONLY LATE PVCs
tervals equal to or less than the Q-T interval of the preceding normal camp ex. Late premature ventricular complexes were defined as those with coupling intervals greater than the Q-T interval of the preceding normal complex.
Results
88% 31 n (PATIENTS)
7941 9472 n (PVCSI
FIGURE 2. The distribution of patients with early and late premature ventricular complexes (PVC@. The center bar shows the percent of patients who exhibited both early (3,256) and late (4,685) premature ventricular complexes. The bar on the right shows the percent of pa- tients who exhibited only late premature ventricular complexes. None had only early premature complexes. n = number.
Heart rate averaged 79 beats/min (range 54 to 118) during the 10 hour recording interval. All patients ex- hibited premature ventricular complexes; the average frequency during the 10 hour interval was 234 f 54 (mean f standard error of the mean) (Fig. 2). Thirty- one patients (82 percent) exhibited both early and late premature ventricular complexes (total 7,941 com- plexes, of which 3,256 [41 percent] were early). The re- maining seven patients (18 percent) exhibited only late premature ventricular complexes (total 942 complexes or 11 percent of all abnormal complexes). No patient exhibited only early premature ventricular complexes. Thus, 38 percent of all isolated premature ventricular complexes plus premature ventricular complexes ini- tiating couplets or runs occurred early.
influences of cardiac catheterization on ventricular arrhyth- mia, hemodynamic changes were not monitored invasively until the completion of the 10 hour recording interval.
Analysis of electrocardiographic recordings: Contin- uous electrocardiographic recordings on magnetic tape were analyzed with the use of the Argus/H computer system, per- mitting automated detection and quantification of premature ventricular complexes at 60 times real time with human editor verification of all abnormal electrocardiographic complexes.lo Analysis incorporated three steps including (1) digitization of the electrocardiographic recording at a sampling frequency of 250/set, (2) automated detection and quantification of premature ventricular complexes by the computer system based on analysis of the digitized signal as previously de- scribed,ll and (3) definitive assignment of all potentially ab- normal complexes detected by the computer to the appro- priate category (supraventricular, ventricular or borderline).12 The Argus/H computer system provides a sensitivity rate for detection of premature ventricular complexes of approxi- mately 90 percent, reproducibility rate after digitization of f0.1 percent and essentially no false positive resultslo Data from automated analysis include the following: the frequency distribution of premature ventricular complexes, heart rate, couplets and runs of three or more premature ventricular complexes; coupling intervals from the preceding normal beat to each premature ventricular complex initiating repetitive depolarizations; and coupling intervals of all isolated pre- mature ventricular complexes measured from the onset of the preceding normal beat to the onset of the premature ven- tricular complex. An example of the output describing cou- pling intervals is shown in Figure 1.
Early versus late premature ventricular com- plexes: Relation to repetitive ventricular depo- larizations: Twenty-nine patients (76 percent) mani- fested repetitive ventricular depolarizations (total 337 episodes) (Fig. 3). Seventy-eight percent of these epi- sodes were initiated by a late premature ventricular complex. Because 38 percent of all isolated premature ventricular complexes were early, the initiation of re- petitive ventricular depolarizations by late premature ventricular complexes was significant at the P <O.Ol level. Only 22 percent (52 episodes) of repetitive ven- tricular depolarizations were initiated by early prema- ture ventricular complexes.
Repetitive ventricular depolarizations were catego- rized as couplets (two consecutive premature ventricular complexes) or runs of ventricular tachycardia (three or more consecutive premature ventricular complexes). Twenty-nine patients exhibited at least one couplet or run during the 10 hour recording interval. Among the total of 245 couplets, 84 percent were initiated by a late premature ventricular complex (Fig. 4). Similarly, among the 92 episodes of runs of ventricular tachycar- dia, 86 percent were initiated by a late premature ven- tricular complex. Only two episodes of ventricular fi- brillation occurred during the recording interval; both were initiated by late premature ventricular com- plexes.
Repetitive ventricular depolarizations were defined as two or more premature ventricular complexes occurring consec- utively at a rate of 120/min or greater. Early premature ven- tricular complexes were defined as those with coupling in-
Relation to coupling interval: Although the prev- alence of repetitive ventricular depolarizations corre- lated with the frequency of isolated premature ven- tricular complexes (Table I) (r = 0.8), it was not related to the average coupling interval expressed in absolute terms or as a fraction of the average Q-T interval of normal beats. In addition, the coupling interval of iso- lated premature ventricular complexes or of premature ventricular complexes initiating couplets or runs failed to correlate with the number of complexes and runs exhibited by the same patient, enzymatically estimated infarct size, heart rate, the site of infarction or the presence or absence of previous infarction.
680 April 1978 The American Journal ot CARDtOLOGY Volume 41

LATE PREMATURE VENTRICULAR COMPLEXES AND INFARCTION-ROBERTS ET AL.
IOOr
’ 60 w i=
2 t
k 40
t l-
= 20 v FIGURE 3. Initiation of repetitive depolarizations by early E and late premature ventricular complexes (PVCs). a
Twenty-nine patients had 337 episodes of repetitive 0 t ventricular depolarizations, of which 285 were initiated by late premature ventricular complexes. n = number.
Discussion
Ventricular premature complexes are the most common manifestation of electrophysiologic derange- ments accompanying myocardial infarction.44J3 Their occurrence during the vulnerable period of the cardiac cycle, during which electrical stimulation is prone to result in ventricular tachycardia or fibrillation, is viewed with particular alarm on the basis of many experimental and clinical observations. For example, after ligation of the left coronary artery in dogs, exogenous electrical stimulation with low energy produces ventricular tachycardia that frequently deteriorates into ventricular fibrillation. In addition, ventricular fibrillation after occlusion of the circumflex branch of the left coronary artery in anesthetized dogs is frequently associated with premature ventricular complexes occurring in close proximity to the apex of the T wave.
Significance of late ventricular premature complexes: One certainly cannot deny that exogenous
FIGURE 4. Initiation of both couplets and runs of ven- tricular complexes by early and late premature ventricular complexes (PVC+ Episodes of couplets (two consecu- tive premature ventricular complexes) are shown on the left, and runs (three or more consecutive premature ventricular complexes) on the right. Late premature ventricular complexes initiated 206 of 245 couplets and 79 of 92 runs. n = number.
cl ALL PATIENTS
PATIENTS WlTH ALL EPISODES INITIATED BY LATE PVCs
•j PATIENTS WITH AT LEAST ONE EPISODE INITIATED BY AN EARLY PVC
I 29 22 7 n(PATIENTS)
337 285 52 n (EPISODESI
or endogenous electrical stimulation of the ischemic heart during a patient’s vulnerable period can give rise to analogous phenomena. On the other hand, the rela- tive importance of late premature ventricular complexes (those that occur after the inscription of the T wave) may have been underestimated. For example, among 52 patients with acute myocardial infarction, de Soyza et a1.14 observed that the mean coupling interval of isolated premature ventricular complexes in patients with ventricular tachycardia was virtually identical to that in patients without this complication. Bleifer et a1.15 found no association between the “R on T phe- nomenon” and ventricular tachycardia in 21 ambulatory patients unless couplets or frequent premature ven- tricular complexes (12/min or more) were present con- comitantly; and Williams16 and Scherlagi7 and their co-workers noted initiation of ventricular fibrillation by late premature ventricular complexes in 7 of 17 pa- tients with acute myocardial infarction and the absence of ventricular fibrillation despite the presence of the “R
COUPLETS
:+:.:.: ::::::::: . . . :.:.:.:.: . . ...‘.‘. ‘.....‘i :.:.>:.:
. . ...‘.‘.
‘........ . . . . . . . . . :.:.>:.:
. . ...‘.‘.
j:::::::
.:.:.:.:.
:::::;:::
::::::: j
~
:.:.>:.:
::j:::::
:::::::::
:::::y:
:::::::::
.:.:.>:.
:j::::::
y::::::
:j::::j
_$g \ - ii!
RUNS 0 A// Couplets 8 Runs
245 206 39 92
m lnitioted by Lafe PVCs
m lnitioted by Early PVCs
- 79 n (EPISODES)
April 1978 The American Journal of CARDIOLOGY Volume 41 691

LATE PREMATURE VENTRICULAR COMPLEXES AND INFARCTION-ROBERTS ET AL
on T phenomenon” in 49 percent of patients studied. Even in the canine model, spontaneous ventricular tachycardia has been associated with long coupling in- tervals and initiation of repetitive depolarizations by late premature ventricular complexes.16
In this study, 84 percent of all couplets, 86 percent of all episodes of ventricular tachycardia and the two ep- isodes of ventricular fibrillation were initiated by late premature ventricular complexes. The possibility that treatment with lidocaine may have contributed to the apparent propensity of late premature ventricular complexes to initiate these repetitive ventricular de- polarizations must be considered because the drug may have selectively affected one class of premature ven- tricular complexes or its sequelae. Lown and Vassaux,l* MogensenlQ and others demonstrated that lidocaine diminishes repetitive ventricular depolarizations. However, in our study the amount of lidocaine admin- istered and the temporal relation between its adminis- tration and the occurrence of repetitive ventricular depolarizations were similar in patients with repetitive depolarizations initiated by early and late premature ventricular complexes. Among patients categorized in three groups according to enzymatically estimated in- farct size, the cumulative lidocaine dose did not vary markedly, although a somewhat smaller dose was re- quired in patients with the smallest infarcts.
Electrophysiologic mechanisms: Our observations indicate that premature ventricular complexes occur- ring with relatively long coupling intervals in patients hospitalized with acute myocardial infarction frequently initiate repetitive ventricular depolarizations. It appears likely that several different electrophysiologic mecha- nisms may contribute to ventricular arrhythmia in pa- tients with acute myocardial infarction.17J0J1 In our study the majority of both early and late premature ventricular complexes exhibited considerable variation in the coupling intervals (Fig. 1). Schamroth2* suggested that early premature complexes with rigidly fixed coupling intervals may reflect reentry. Premature ventricular complexes with no fixed coupling interval
are more compatible with parasystole, and late diastolic extrasystoles with ventricular tachycardia due to in- creased automaticity with high degrees of exit block. According to these interpretations, the ventricular ar- rhythmia occurring in our patients was probably due to automaticity rather than reentry. Early after the onset of ischemic injury, reentry within the myocardium ap- pears to be a prominent factor. Somewhat later, en- hanced automaticity may be more important. Later, in patients convalescing from myocardial infarction, ma- lignant ventricular arryhthmia may be due to enhanced automaticity of surviving Purkinje fibers near the region of previous infarction.
Implications: It is not clear whether the electro- physiologic mechanisms underlying the relatively late premature ventricular complexes seen in our study in patients hospitalized with acute myocardial infarction differ from those giving rise to early premature ven- tricular complexes at the same time in the same pa- tients. It is also not yet clear whether disparate funda- mental mechanisms such as fast primary inward current in contrast to slow secondary inward current give rise to repetitive ventricular depolarizations and, if so, whether each is associated with a particular class of premature complexes. We cannot exclude the possibility that in some patients early or late premature ventricular complexes, or both, may be manifestations of an underlying electrophysiologic instability of the heart that gives rise to repetitive ventricular depolarization independently. However, the frequent initiation of re- petitive ventricular depolarizations by late premature ventricular complexes attests to their potential im- portance as warning arrhythmias on the one hand, and as precipitants of malignant arrhythmias that may re- quire pharmacologic suppression on the other.
Acknowledgment
We appreciate Kenneth W. Clark’s assistance with com- puter programming and Carolyn Lohman’s preparation of the manuscript.
References
1. Wiggers CJ, WBgria R: Ventricular fibrillation due to single, lo- calized induction and condenser shocks applied during the vul- nerable phase of ventricular systole. Am J Physiol 128500-505, 1940 Smirk FH, Palmer DG: A myocardial syndrome. With particular reference to the occurrence of sudden death and of premature systoles interrupting antecedent T waves. Am J Cardiol6:620-629, 1960 Wolff GA, Veith F, Lown 6:’ A vulnerable period for ventricular tachycardia following myocardial infarction. Carcliovasc Res 2: 111-121, 1968
8.
2.
3.
9.
10.
Lown B, Fakhro AM, Hood WB Jr, et al: The coronary care unit. 11. Clark KW, Noifa FM, Cox JR Jr, et al: High performance computer New oersoectives and directions. JAMA 199:188-198, 1967 oroarams for raoid analvsis of lona ECG records. Proc San Dieao Mel&r L$ Dunning AJ: Textbook of Coronary Care. Philadelphia, &o&d Symp i3:139-i44,1974- Charles Press, 1972, p 118, 119 12. Oliver GC, NoHe FM, Wolff GA, et al: Detection of premature Blelfeid W, Yerx W: Primare und sekundare Arrhythmien beim ventricular contractions with a clinical system for monitoring Herzinfarkt. Verh Dtsch Ges Inn Med 76:611-614, 1970 electrocardiographic rhythms. Comput Biomed Res 4523-541, El-Sherlf N, Myerburg RJ, Scha~Iag BJ, et al: Electrocardiographic 1971 antecedents of primary ventricular fibrillation. Value of the R-on-T 13. Taibot S, Dreifus LS: Characteristics of ventricular extrasystoles
682 April 1978 The American Journal of CARDKKGGY Volume 41
phenomenon in myocardial infarction. Br Heart J 38:415-422, 1976 Roberts R, Henry PD, Sobei BE: An improved basis for enzymatic estimation of infarct size. Circulation 52:743-754, 1975 Shell WE, Laveiie JF. Coveii JW, et al: Early estimation of myo- cardiil damage in conscious dogs and patients with evolving acute myocardial infarction. J Clin Invest 52:2579-2590, 1973 Noile FM, Oliver GC, Kieiger RE, et al: The Argus/H system for rapid analysis of ventricular arrhythmias. In, Computers in Cardi- ology. Long Beach, California, IEEE Computer Society, 1974, p 37

LATE PREMATURE VENTRICULAR COMPLEXES AND INFARCTION-ROBERTS ET AL.
14.
15.
16.
17.
18.
and their prognostic significance: a reappraisal of their method of classification. Chest 67:665-674, 1975 de Soyza N, Biseett JK, Kane JJ, et al: Ectopic ventricular pre- maturity and its relationship to ventricular tachycardia in acute myocardial infarction in man. Circulation 50529-533, 1974 Bleifer SB, Sheppard JJ, Karpman ML, et al: Relationship of the R-on-T phenomenon to the development of ventricular tachycardii (abstr). Circulation 44:Suppl lkll-142, 1971 Williams DO, Scherlag BJ, Hope RR, et al: The pathophysiology of malignant ventricular arrhythmias during acute myocardial ischemia. Circulation 50:1163-l 172, 1974 Scherlag BJ, Et-Sherlf N, Hope R, et al: Characterization and lo- calization of ventricular arrhythmias resulting from myocardial ischemia and infarction. Circ Res 35:372-383, 1974 Lown 6, Vassaux C: Lidocaine in acute myocardial infarction. Am
19.
20.
21.
22.
Heart J 76:586-587, 1968 Mogensen L: Ventricular tachyarrhythmias and lignocaine pro- phylaxis in acute myocardial infarction. Acta Med Stand 5 13: l-80, 1970 Myerburg RJ, Gelband H, NIlsson K, et al: Long-term electro- physiological abnormalities resulting from experimental myocardial infarction in cats. Circ Res 41:73-84, 1977 Corr PB, Sobel BE: Automated data processing. An essential de- cision-making aid in the treatment of acute myocardial infarction. In, Advances in Cardiology, Vol 20 (Vogel JHK, ed). Basel, Swit- zerland, S Karger, 1977, p 54 Schamroth L: The genesis and evolution of ectopic ventricular rhythm. In, The Disorders of Cardiac Rhythm. Oxford, Blackwell Scientific Publications, 1971, p 138
April 1978 The American Journal of CARDIOLDDY Volume 41 683