Embed Size (px)
Citation preview

Br HeartJ 1995;74:348-353
Rescue thrombolysis: alteplase as adjuvanttreatment after streptokinase in acute myocardialinfarction
J P Mounsey, J S Skinner, T Hawkins, A F N MacDermott, S S Furniss, P C Adams,P J L Kesteven, D S Reid
AbstractBackground-In acute myocardial infarc-tion patients who do not reperfuse theirinfarct arteries shortly after thrombolytictreatment have a high morbidity andmortality. Management of this high riskgroup remains problematic, especially incentres without access to interventionalcardiology. Additional thrombolytictreatment may result in reperfusion andimproved left ventricular function.Methods-Failure of reperfusion wasassessed non-invasively as less than 25%reduction of ST elevation in the electro-cardiographic lead with maximum STshift on a pretreatment electrocardio-gram. 37 patients with acute myocardialinfarction who showed electrocardio-graphic evidence of failed reperfusion 30minutes after 1.5 MU streptokinase over60 minutes were randomly allocated toreceive either alteplase (tissue type plas-minogen activator (rt-PA) 100 mg overthree hours) (19 patients) or placebo (18patients). 43 patients with electrocardio-graphic evidence of reperfusion afterstreptokinase acted as controls. Outcomewas assessed from the Selvester Q wavescore of a predischarge electrocardio-gram and a nuclear gated scan for leftventricular ejection fraction 4-6 weeksafter discharge.Results-Among patients in whom STsegment elevation was not reduced afterstreptokinase, alteplase treatment resultedin a significantly smaller electrocardio-graphic infarct size (14% (8%) v 20% (90%),P = 0.03) and improved left ventricularejection fraction (44 (10%) v 34% (16%),P = 0-04) compared with placebo. Thisbenefit was confined to patients who failedfibrinogenolysis after streptokinase (fib-rinogen > 1 gIl). In patients in whom STsegment elevation was reduced after strep-tokinase, infarct size and left ventricularejection fraction were not significantly dif-ferent from those in patients treated withadditional alteplase.Conclusion-Patients without electrocar-diographic evidence of reperfusion afterstreptokinase may benefit from furtherthrombolysis with alteplase.
(Br Heart 7 1995;74:348-353)
Keywords: alteplase; rescue thrombolysis; streptoki-nase; acute myocardial infarction
Patients with acute myocardial infarction inwhom coronary reperfusion does not occursoon after thrombolysis have a high incidenceof impaired left ventricular function and highmortality.' 2 Mechanical revascularisation maybe attempted in these patients (rescue percuta-neous transluminal coronary angioplasty),3 butas most myocardial infarctions are treated incentres without immediate access to interven-tional facilities, other therapeutic approachesare needed. One possibility is to administeradditional lytic treatment. This approachhas been successful in patients with earlyreocclusion after initially successful reper-fusion.4 Initial treatment with more than onelytic agent has also been used in an attempt toimprove reperfusion rate and to maintainpatency.5 6 However, sequential lytic treatmenthas not been tested in patients in whom reper-fusion does not occur after a single agent. Thisapproach is attractive because only patients athighest risk are exposed to the potential hazardof a second lytic agent.
Coronary reperfusion after thrombolysiscan be assessed confidently only by acutecoronary angiography. However, non-invasivemarkers of probable reperfusion have beendeveloped which may allow therapeutic deci-sions to be made in centres without access toinvasive facilities. Multiple algorithms havebeen developed to assess reperfusion non-invasively, but in this trial we focused on fail-ure of rapid reduction of ST segmentelevation.7-9 This has been shown to be a reli-able sign of persistent coronary occlusion afterthrombolytic treatment,7 which is readily avail-able and interpretable without special equip-ment or skills.We hypothesised that in patients who do
not show reperfusion on electrocardiographiccriteria after streptokinase treatment, addi-tional lytic therapy with tissue type plasmino-gen activator (rt-PA, alteplase) may result inreperfusion and improved left ventricularfunction. One possible reason for failure ofreperfusion may be failed fibrinogenolysis.'0Accordingly, a secondary hypothesis was thatadjuvant alteplase treatment would be mostbeneficial in patients who did not show fib-rinogenolysis after streptokinase. We reportthe results of a prospective randomised trial ofalteplase in patients who on electrocardio-graphic criteria failed to show reperfusion afterstreptokinase.
Patients and methodsPatients were eligible for inclusion in thisstudy if they presented within six hours of the
Northern RegionalCardiothoracicCentre, FreemanHospital, Newcastleupon TyneJ P MounseyT HawkinsA F N MacDermottS S FumissD S ReidDepartment ofCardiology, RoyalVictoria Infirmary,Newcastle upon TyneJ S SkinnerP C AdamsDepartnent ofHaematology,Freeman Hospital,Newcastle upon TyneP J L KestevenCorrespondence to: Dr J PMounsey, Department ofCardiovascular Medicine,Queen Elizabeth Hospital,Edgbaston, BirminghamB15 2TH.Accepted for publication3 April 1995
348
on Novem
ber 20, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.74.4.348 on 1 O
ctober 1995. Dow
nloaded from

Alteplase as adjuvant treatment after streptokinase in acute myocardial infarction
onset of a first acute myocardial infarction.This was defined as chest pain ofmore than 30minutes' duration unresponsive to glyceryltrinitrate; electrocardiographic ST segmentelevation, either > 2 mm in at least two con-tiguous leads V1-V6 or > 1 mm in at leasttwo contiguous limb leads; or ST depressionof at least 2 mm with tall R waves in leadsV1-V3 suggesting true posterior infarction.
Specific exclusion criteria were previousQ wave myocardial infarction, previouscoronary surgery, pre-existing right or leftbundle branch block or fascicular block, andleft ventricular hypertrophy. Patients were alsoexcluded if they had any of the general con-traindications to thrombolysis. These includedactive gastrointestinal bleeding during the pre-ceding three months, cerebrovascular accidentwithin the preceding six months, any history ofcerebral haemorrhage or cerebral aneurysm,major surgery or trauma in the preceding 10days (including prolonged cardiopulmonaryresuscitation), sustained hypotension (systolicblood pressure less than 90 mm Hg) unre-sponsive to volume expansion, uncontrolledhypertension (systolic pressure persistentlygreater than 200 mm Hg on repeated mea-surement), proliferative diabetic retinopathy,or any history of bleeding diathesis. There wasno upper age limit.The study was approved by the Northern
Health Authority Ethics Committee. Allpatients gave informed consent.
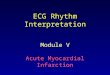
THROMBOLYTIC PROTOCOLAll patients received streptokinase (1 5 MUintravenously over 60 minutes) followed byheparin for at least 24 hours (fig 1). Aspirinwas given unless contraindicated and othertreatment was at the discretion of the responsi-ble physician. Reperfusion was assessed non-invasively from an electrocardiogram recorded90 minutes after the start of the streptokinase
The trial protocol
infusion. Probable reperfusion was defined asa reduction of ST segment elevation by 25%or more in the lead with the maximum STshift on the admission electrocardiogram.Patients with electrocardiographic evidence ofprobable reperfusion received conventionaltreatment alone. Patients with persistent STsegment elevation (presumed failed reperfu-sion) received either alteplase (Boehringer) oran identical placebo in a double blind prospec-tive trial. Assignment to treatment groups wasmade using a minimisation programme(Minim, supplied by Dr SJW Evans, depart-ment of Clinical Epidemiology, LondonHospital Medical College) to ensure roughconsistency between treatment groups for age,sex, and infarct site. Alteplase was adminis-tered in the standard dosing regimen of 100mg over three hours (10 mg as a slow bolusinjection followed by 50 mg over one hour andthen an infusion of 20 mg/h over the nexttwo hours).
COAGULATION STATEBlood samples were taken in all patientsbefore and after streptokinase to assess plasmafibrinogen concentration." The results of thisassay were not available at the time of ran-domisation. Fibrinogenolysis was defined as afibrinogen concentration of < 1 0 g/l at theend of the streptokinase infusion.
OUTCOME MEASUREMENTSElectrocardiographic infarct sizeInfarct size was estimated from electrocardio-grams recorded on admission and at hospitaldischarge. Predicted infarct size was estimatedfrom the admission electrocardiogram accord-ing to the method of Clemmensen et al."2 Inthis method, empirical formulas are used topredict the proportion of the left ventricle atrisk of myocardial infarction from a pretreat-ment electrocardiogram. For anterior myocar-dial infarctions, defined as those withmaximum ST segment elevation in leads Vl-V3, the formula is:
Predicted % anterior infarct size = 3 (1-5 (Noof leads with ST elevation) - 0 4).
For inferior infarcts, defined as those witheither maximum ST segment elevation inleads II, III, and a VF, or ST segment depres-sion in leads V1-V3, the corresponding for-mula is:
Predicted % inferior infarct size = 3 (0-6(ESTsegments in leads II, III, and aVF) + 2) + 3(1 5(No of non-inferior leads with ST eleva-tion) - 0 4).
Resultant QRS estimated infarct size wasestimated from the pre-discharge electrocar-diogram by the Selvester QRS score.'3 Thissystem contains 54 criteria and awards a maxi-mum of 32 points. Each of these points repre-sents about 3% of the left ventricle so, forcomparison with the predicted infarct size, theSelvester score was multiplied by three toyield a measure of the proportion of infarctedleft ventricle. The QRS score is of limitedvalue in assessing infarct size.'4 We measured
349
on Novem
ber 20, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.74.4.348 on 1 O
ctober 1995. Dow
nloaded from

Mounsey, Skinner, Hawkins, MacDermott, Furniss, Adams, et al
it solely for comparison with potential infarctsize (as assessed from the admission electro-cardiogram), to assess non-invasively whethermyocardial salvage had occurred. Inter-estingly, in our population Q wave score wassignificantly correlated with ejection fraction(r = 0-63, P < 0-001) in contrast to the data ofChristian et al.'4
All electrocardiographs were scored by twoexperienced cardiologists, each of whom wereunaware of treatment assignment or outcome.ST elevation was measured to the nearest 0 5mm in all leads except aVR.
Left ventricular ejection fractionLeft ventricular ejection fraction was assessedby nuclear gated blood pool imaging four tosix weeks after hospital discharge. Global ejec-tion fraction was estimated from the left ante-rior oblique projection with a standardcomputer software package. The left anterioroblique angulation was selected for eachpatient to achieve optimal separation of theright and left ventricles.
DATA ANALYSISStudent's t test and the X2 test with Yates'scorrection when appropriate were used forstatistical analysis. Significance was assumedto be P < 0-05. Continuous variables arequoted as means (SD). Statistical analysiswere performed using spss/pc. The samplesize (> 32 randomly allocated patients) wascalculated to detect an improvement in leftventricular ejection fraction of 10 percentagepoints, assuming a to be 10%, a to be 0 05,and ,B to be 02.1'
Table 1 Baseline patient characteristics. Values are means (SD) unless stated otherwise
Streptokinase Streptokinase Streptokinaseonly + rtPA + placebo(n = 43) (n =19) (n = 18) Pvalue
Age (years) 63 (9) 63 (10) 63 (10) 0 9No (%) of men 30 (70) 11 (58) 13 (72) 0 4No (%) with infarct site:
Anterior 14 (32) 10 (53) 10 (56)Inferior 28 (65) 8 (42) 6 (33)Other 1 (2) 1 (5) 2 (11) 0 7
Time to streptokinase (h) 3 3 (1 9) 3-4 (1 9) 4-3 (2-1) 0-2Time to rt-PA (h) - 5-6 (1 9) 6-5 (2 2) 0-3
*For difference between rt-PA and placebo assessed by t or x2 test.
Table 2 Main outcome measures
Streptokinase Streptokinase Streptokinaseonly + rtPA + placebo(n = 43) (n = 19) (n = 18) Pvalue
Mean (SD) infarct size (%):Predicted 21 (8) 26 (13) 25 (8) 0 9Resultant 10 (9) 14 (8) 20 (9) 0-03
Ejection fraction (%) 49 (13) 44 (10) 34 (16) 0-04
*For difference between alteplase and placebo assessed by t or x2 test.
Table 3 Lytic state
Streptokinase only Randomised group(n = 43) (n = 37) Pvalue
Mean (SD) fibrinogen (g/l):Initially 3-6 (1-4) 3-8 (1-3) 0 560 minutes after streptokinase 1-0 (1-1) 1-3 (1-0) 0-2
No (%) of patients without fibrinogenolysis60 minutes after streptokinase 17 (40) 24 (65) 0-01
ResultsA total of 129 patients fulfilled the entryrequirements and were screened for inclusionin the trial. Forty three patients (33 3%) didnot show a reduction in ST segment elevation(presumed failed reperfusion); of these, 37were randomly allocated to receive alteplase(19 patients) or placebo (18 patients); the sixremaining patients did not give their consent.Eighty six patients (66-6%) showed a reduc-tion in ST segment elevation of >i25%, 90minutes after the initiation of streptokinase(presumed reperfusion); 43 of them wererecruited into the control (streptokinase only)group. Table 1 shows the baseline characteris-tics of the patient cohort. Overall mean agewas 63 1 (9) years and 54 (68%) patients weremen. Randomised patients were well matchedfor baseline infarct site, but there was a signifi-cant excess of inferior infarcts among patientswith presumed reperfusion (65% (28) com-pared with 38% (20) in the randomised group,P = 0-043). Mean time from the onset ofsymptoms to initiation of thrombolysis was 3-6(1 9) hours (range 0-6-10 25) overall; in ran-domised patients the time from the onset ofsymptoms to initiation of rt-PA or placebo was6-0 (2-1) hours (range 2-1-10-8). There wereno systematic differences in time to treatmentbetween the treatment groups.
EFFECTS ON INFARCT SIZE AND EJECTIONFRACTIONTable 2 shows the effects of the three throm-bolytic regimens on infarct size and ejectionfraction. Predicted infarct size, as estimatedfrom the admission electrocardiogram wassimilar in all three groups. However, resultantinfarct size, estimated from the predischargeelectrocardiogram, was significantly smaller inpatients randomly allocated to alteplase com-pared with those allocated placebo. Similarly,patients randomly allocated to alteplase hadsignificantly higher ejection fractions at four tosix weeks than patients who received placebo.Patients with presumed reperfusion afterstreptokinase alone were not significantly dif-ferent from patients without presumed reper-fusion who received alteplase. One patientfrom each of the three treatment arms died inhospital and therefore did not have a gatedblood pool scanning (see below). Two furtherpatients refused to have gated scanning. Bothreceived active alteplase and neither had car-diac failure on routine follow up. Their pre-dicted pretreatment infarct sizes were 38%and 26%; their predischarge QRS infarct sizeswere respectively 12% and 9%-thus bothshowed electrocardiographic evidence ofmyocardial salvage.
INFLUENCE OF FIBRINOGENOLYSISTable 3 shows fibrinogen concentrations incontrol (streptokinase only) and randomisedpatients. There were no significant differencesin mean concentrations initially or 60 minutesafter streptokinase. Overall 41 out of 80 (51 %)patients did not show fibrinogenolysis at 60minutes. These included 24 out of 37 (65%)patients who were later randomised and 17
350
on Novem
ber 20, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.74.4.348 on 1 O
ctober 1995. Dow
nloaded from

Alteplase as adjuvant treatment after streptokinase in acute myocardial infarction
Table 4 Influence offibrinogenolysis. Values are means (SD) unless stated otherwise
Streptokinase Streptokinase Streptokinaseonly + alteplase + placebo P value *
Fibrinogen < 1 gil 60 minutes after streptokinaseNo of patients 26 7 6Infarct size (%):
Predicted 21 (7) 29 (19) 25 (8) 0-6Resultant 11(8) 15 (7) 17 (6) 0-6
Ejection fraction (%) 49 (13) 46 (12) 41 (13) 0-6Fibrinogen >1 gll 60 minutes after streptokinase
No of patients 17 12 12Infarct size (%):
Predicted 22 (10) 23 (9) 25 (9) 0-6Resultant 9 (11) 13 (8) 21 (10) 0-04
Ejection fraction (%) 47 (16) 44 (10) 30 (17) 0-04
*For difference between alteplase and placebo assessed by t test.
out of 43 (40%) control (streptokinase only)patients. The proportion of patients who didnot show fibrinogenolysis was significantlyhigher among those later randomised-that is,those who presumably failed to reperfuse-than among controls-that is those whopresumably reperfused (65% compared with40%, P = 0 01). Among randomised patients,seven of the 19 (37%) who received alteplaseand six of the 18 (33%) who received placeboshowed fibrinogenolysis after streptokinase(P = 0 9).
Table 4 summarises the effect of fib-rinogenolysis after streptokinase on infarct sizeand ejection fraction. In patients who showedneither reperfusion nor fibrinogenolysis afterstreptokinase, infarct size was significantlysmaller and ejection fraction better preservedamong those who received active alteplasethan among those who received placebo;patients who received alteplase were not sig-nificantly different from those with presumedreperfusion after streptokinase alone. By con-
trast, in the group who did not show reperfu-sion but showed fibrinogenolysis afterstreptokinase there was no significant differ-ence in either resultant infarct size or ejectionfraction between alteplase and placebo groups.Likewise, among these patients, neither groupwas significantly different from patients withpresumed reperfusion and fibrinogenolysisafter streptokinase alone. In patients with pre-sumed reperfusion after streptokinase aloneoutcome was similar regardless of fibrinogenconcentration; fibrinogenolysis was not pre-dictive of outcome.
MORTALITY AND COMPLICATIONSMortality at six weeks was 3-75%. Threepatients died, one from each of the three treat-ment arms. There were five episodes of bleed-ing, only one of which, a gastrointestinalhaemorrhage, required transfusion. Thisoccurred in a patient randomly allocatedplacebo. Minor bleeds included two haemop-tyses, one epistaxis, and one rectal bleed.There were no cerebral haemorrhages.
DiscussionIn this prospective study we found thatpatients with acute myocardial infarctionwhose ST segment elevation did not reduce by25% or more 90 minutes after initiation of
streptokinase and who received additional lytictreatment with alteplase had improved leftventricular function and smaller Q wave scoresthan patients who received placebo. A pre-specified subgroup analysis suggested that theimprovement in outcome was confined topatients who also did not show fibrino-genolysis-that is, fibrinogen concentrationwas > 1 0 g/l after streptokinase. In the smallgroup of patients without reduction in ST seg-ment elevation 90 minutes after streptokinaseand fibrinogen concentrations < 1 0 g/l, adju-vant alteplase conferred no extra benefit.We chose a reduction in ST segment eleva-
tion of 25% or more as the non-invasiveindicator of probable reperfusion. We pre-viously found that this sign is highly sensitive(> 95%) but non-specific (43%) for coronaryreperfusion when assessed angiographically90 minutes after treatment with anisoylatedstreptokinase plasminogen activator complex.7Hogg et al reported a high sensitivity (93%) fora fall in ST segment elevation of 50%, buttheir post thrombolytic electrograms wererecorded much later than in our study (at 302(141) minutes).'6 When the criterion of Hogget al was applied to a population with angio-graphically proved reperfusion at 90 minutes,sensitivity for reperfusion fell to only 68%.7
Frequent (every 5-10 minutes) measure-ment of ST segment height is a more sensitiveindicator of reperfusion than sampling at twofixed points. Shah et al showed that compari-son of a single pretreatment electrocardiogramwith one taken at 90 minutes failed to detectimpending reperfusion in more than 10% ofpatients.'7 If we had sampled ST segmentsmore frequently, fewer patients may havereceived adjuvant thrombolysis. However, wewanted to identify failed reperfusion and tomaximise the potential impact of alteplase inthe patients who needed it-and this arguedfor treatment to be given as early as possible.Inevitably an arbitrary time limit must beapplied in this situation and we chose 90 min-utes after the initiation of streptokinase. Asecondary consideration in the use of electro-cardiographic assessment at fixed time pointswas a desire to test the efficacy of a manage-ment strategy which could be widely applied.Continuous ST segment monitoring requiresmore nursing time than is usually available in abusy coronary care unit. Relief of chest painwas not used in the current study because,although it is a sensitive sign of timing ofreperfusion when followed sequentially,'7 itsassessment at a fixed time point is difficult,especially if it is not concordant with the elec-trocardiographic results.
Adjuvant thrombolysis was administeredwhen the patency of the infarcted artery wouldbe expected to be 50-60% (thrombolysisin myocardial infarction (TIMI) grade II orIII).' Patencies after streptokinase treatmentimprove to about 75% at three hours,' so ifprobable reperfusion status had been assessedat this stage the proportion of patients requiringadditional lytic treatment would have beenreduced. In the event, although the anticipatedpersistent occlusion rate was 40-50% at the
351
on Novem
ber 20, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.74.4.348 on 1 O
ctober 1995. Dow
nloaded from

Mounsey, Skinner, Hawkins, MacDermott, Furniss, Adams, et al
time of assessment, only 33% of our patientsmet the electrocardiographic criteria for per-sistent occlusion.A fall in ST segment elevation of 25% or
more is of limited value in predicting coronarypatency-that is, the specificity is low-but,after single agent thrombolysis, patients whohave such a fall but no angiographic evidenceof reperfusion have well preserved left ventric-ular function.7 The converse electrocardio-graphic sign-persistent ST segment elevationafter thrombolysis-is highly predictive of per-sistent coronary occlusion and impaired leftventricular function.7 In our previous studyejection fraction was as low as 28% in thisgroup, compared with 47% in patients withreduced ST segment elevation of 25% ormore.The thrombolytic action of streptokinase is
associated with a systemic lytic state; failure toachieve fibrinogenolysis 90 minutes after initia-tion of lytic treatment is associated with persis-tent coronary occlusion.'0 We found that whenfibrinogen concentrations were measured at60 minutes patients with presumed reperfu-sion-that is, those with reduced ST segmentelevation-had an overall good outcomeregardless of whether they showed fib-rinogenolysis. Among the 40% of these whodid not show fibrinogenolysis the favourableoutcome may possibly be attributed to late fib-rinogenolysis with subsequent clot lysis or tothe presence of a preformed collateral circula-tion. In patients with presumed failed reperfu-sion-that is, persistent ST segmentelevation-alteplase improved outcome onlyin the 65% with failed fibrinogenolysis-thatis, fibrinogen concentration > 1 gIl. In thosewith fibrinogenolysis, outcome was good andnot improved by rt-PA. A possible explanationof this is that, although streptokinase did notcause reperfusion it reduced plasma viscosityand so improved peri-infarct microcirculationsufficiently to limit infarct size.'8 19 The strep-tokinase induced reduction in plasma viscosityclosely parallels fibrinogen concentrations andso will not occur in patients who do not showdefibrination. Alternatively, these patients mayhave been destined to show reperfusion latewith streptokinase alone, alteplase thus beingof no further benefit.
Combination thrombolysis using streptoki-nase and rt-PA results in a superior patencyrate (TIMI grade II or III) at 90 minutes whencompared with either rt-PA or streptokinasegiven as monotherapy in conventional regi-mens.56 In the GUSTO (global utilisation ofstreptokinase and alteplase for occluded coro-nary arteries) trial this improvement inpatency did not translate to an improve-ment in either left ventricular function or mor-tality6-only accelerated alteplase was superiorto the other regimens in this respect.' Also inthe GUSTO trial-and presumably also in thegeneral population of patients with infarc-tion-flow of TIMI grade III at 90 minutesachieved by whatever regimen was the bestpredictor of outcome. Left ventricular func-tion was identical in the groups with flow ofTIMI grades 0, I, and II at 90 minutes. Our
data are not strictly comparable with eitherthose of the GUSTO6 or KAMIT (Kentuckyacute myocardial infarction)5 trials. We stud-ied patients treated initially with streptokinase,presumably with flow of TIMI grade 0 or Iflow at 90 minutes and found an improvedoutcome after additional, delayed rt-PA treat-ment. A high risk population was selected forintervention and, by the surrogate end point ofleft ventricular function, an improvement wasobserved. This improvement was similar inmagnitude to that observed in the ISAM(intravenous streptokinase in acute myocardialinfarction) trial of streptokinase and placebo,20but it was much larger than that observed earlyafter infarction in the TAMI (thrombolysisand angioplasty in myocardial infarction) andTIMI (thrombolysis in acute myocardialinfarction) trials.2' 22 The value of left ventricu-lar function as a surrogate end point in trials oflytic treatment has been questioned.2324 In thegeneral population of patients with infarctionejection fraction is about 50% in both throm-bolytic and placebo groups.24 We observed agreater ejection fraction in the treatmentgroup probably because the study populationwas confined to high risk patients with persis-tently occluded arteries. These patients hadmost left ventricle to gain, or lose. A largertrial would be needed to determine whetherthe improvement in left ventricular functionwe observed would translate into a mortalitybenefit.
Rescue angioplasty has been advocated forpatients with persistent coronary occlusion orearly recurrent ischaemia after thrombolysis.25Repeat thrombolysis is beneficial in patientswith early recurrent ischaemia after myocar-dial infarction.4 Our data suggest that addi-tional lytic treatment may also be beneficial inpatients with evidence of persistent coronaryocclusion after thrombolysis. Most cardiaccentres do not have access to immediateangioplasty; our data suggest that additionalthrombolysis may be substituted with benefitto the patient.
Combination thrombolysis results in a sig-nificant excess of haemorrhagic strokes oversingle agent thrombolysis in all regimens so fartested. In GUSTO the haemorrhagic strokerate for combination treatment was 0.94%,6which is almost double the rate for streptoki-nase alone, 0 49-0 54%. We did not set upour study to test formally the safety profile ofcombination thrombolytic treatment in persis-tent coronary occlusion, but the absence oftreatment related complications suggests thatserious haemorrhage rates greatly in excess ofthose seen in GUSTO are unlikely.
In conclusion, among patients with acutemyocardial infarction in whom streptokinasedoes not reduce ST segment elevation by 25%or more after 90 minutes, further thrombolysiswith rt-PA resulted in significantly better leftventricular function and a smaller resultantelectrocardiographic infarct size when com-pared with placebo. This improvement ininfarct size and left ventricular functionwas confined to patients who did not showfibrinogenolysis (fibrinogen concentration
352
on Novem
ber 20, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.74.4.348 on 1 O
ctober 1995. Dow
nloaded from

Alteplase as adjuvant treatment after streptokinase in acute myocardial infarction
> 1 g/l) after streptokinase. These findingsneed to be confirmed in a larger, preferablymulticentre, trial. Our data suggest, however,that in acute myocardial infarction treatmentwith an additional thrombolytic agent shouldbe considered if ST segment elevation fails toresolve and if plasma fibrinogen concentrationremains above 1-0 g/l.
We acknowledge the expert help of Dr D Appleton, depart-ment of medical statistics, University of Newcastle upon Tyne,in both the planning and the analysis of this trial. We acknowl-edge the gift of alteplase and identical placebo from BoehringerIngelheim.
1 GUSTO Angiographic Investigators. The effects of tissueplasminogen activator, streptokinase, or both, on coro-nary artery patency, ventricular function and survivalafter acute myocardial infarction. N Engl J Med 1993;329:1615-22.
2 Vogt A, von Essen R, Tebbe U, Feuerer W, Appel KF,Neuhaus KL. Impact of early perfusion status of theinfarct related artery on short term mortality after throm-bolysis for acute myocardial infarction: retrospectiveanalysis of four German multi-center studies. J Am CollCardiol 1993;21:1391-5.
3 Fung AY, Lai P, Topol EJ, Bates ER, Buordillon PDV,Walton JA, et al. Value of percutaneous transluminalangioplasty after unsuccessful intravenous streptokinasetherapy in acute myocardial infarction. Am J Cardiol1986;58:686-91.
4 Barbash GI, Hod H, Roth A, Faibel HE, Mandel Y, MillerHI, et al. Repeat infusions of tissue type plasminogenactivator in patients with acute myocardial infarction andearly recurrent ischaemia. J Am Coll Cardiol 1990;16:779-83.
5 Grines CL, Nissen SE, Booth DC, Gurley JC, Chelliah N,Wolf R, et al. A prospective, randomized trial comparingcombination half dose tissue type plasminogen activatorand streptokinase with full dose tissue type plasminogenactivator. Circulation 1991;84:540-9.
6 GUSTO Investigators. An international randomized trialcomparing four thrombolytic strategies for acute myocar-dial infarction. NEnglJMed 1993;329:673-82.
7 Saran RK, Been M, Furniss SS, Hawkins T, Reid DS.Reduction in ST segment elevation after thrombolysispredicts either coronary reperfusion or preservation ofleft ventricular function. Br Heart3t 1990;64: 113-7.
8 Barbash GI, Roth A, Hod H, Miller HI, Rath S, Har-ZahavY, et al. Rapid resolution of ST segment elevation andprediction of clinical outcome in patients undergoingthrombolysis with alteplase (recombinant tissue plas-minogen activator): results of the Israeli study of earlyintervention in myocardial infarction. Br Heart 7 1990;64:241-7.
9 Krucoff MW, Croll MA, Pope JA, Granger CB, O'ConnerCM, Sigmon KN, et al. Continuous 12-lead ST segmentrecovery analysis in the TAMI 7 study. Circulation1993;88:437-47.
10 Brugeman J, van der Meer J, Takens BH, Hillege H, LieKI. A systemic non-lytic state and local thrombolytic fail-ure of anistreplase in acute myocardial infarction. BrHeartJ7 1990;64:355-8.
11 Clauss A. Rapid physiological coagulation method in deter-mination of fibrinogen. Acta Haematol 1957;17:237-40.
12 Clemmensen P, Grande P, Saunamaki K, Pederson F,Svendsen JH, Wagner NB, et al. Effect of intravenousstreptokinase on the relation between initial ST predictedsize and final QRS estimated size of acute myocardialinfarcts. JAm Coil Cardiol 1990;16:1252-7.
13 Wagner GS, Freye CJ, Palmeri ST, Roark SF, Stack NC,Ideker RE, et al. Evaluation of a QRS scoring system forestimating myocardial infarct size. I. Specificity andobserver agreement. Circulation 1982;65:342-7.
14 Christian TF, Clements IP, Behrenbeck T, Huber KC,Chesebro JH, Gersh BJ, et al. Limitations of the electro-cardiogram in estimating infarct size after acute reperfu-sion therapy for myocardial infarction. Ann Intern Med1991;114:264-70.
15 Gore SM, Altman DG. Statistics in practice. London: BritishMedical Association, 1982:6-8.
16 Hogg KJ, Hornung RS, Howie CA, Hockings N, DunnFG, Hlllis WS. Electrocardiographic prediction of coro-nary artery patency after thrombolytic treatment in acutemyocardial infarction: use of the ST segment as a non-invasive marker. BrHeartJ 1988;60:275-80.
17 Shah PK, Cercek B, Lew AS, Ganz W. Angiographic vali-dation of bedside markers of reperfusion. J Am CollCardiol 1993;21:55-61.
18 Moriaty AJ, Hughes R, Nelson SD, Balnave K.Streptokinase and reduced plasma viscosity: a secondbenefit. EurJHaematol 1988;41:25-36.
19 Arntz HR, Perchalla G, Roll D, Heitz J, Schafer JH,Schroder R. Blood rheology in acute myocardial infarc-tion: effects of high dose i/v streptokinase compared toplacebo. EurHeartJ7 1992;13:275-80.
20 Voth E, Tebbe U, Schicha HS, Neuhaus KL, Schroder Rfor the ISAM study group. Intravenous streptokinase inacute myocardial infarction (ISAM) trial: serial evalua-tion of left ventricular function up to 3 years after infarc-tion estimated by radionuclide ventriculography. Y AmColl Cardiol 1991;18:1610-6.
21 Harrison JK, Califf RM, Woodlief LH, Kereiakes D,George BS, Stack RS, et al. Systolic left ventricular func-tion after reperfusion therapy for acute myocardial infarc-tion. Circulation 1993;87:1531-41.
22 Cheesbro JH, Knatteraud G, Roberts R, Borer J, CohenLS, Dalen J. Thrombolysis in myocardial infarction(TIMI) trial phase I: a comparison between intravenoustissue plasminogen activator and intravenous streptoki-nase. Clinical findings through hospital discharge.Circulation 1987;76:142-54.
23 CaliffRM, Harrelson-Woodlief L, Topol EJ. Left ventricu-lar ejection fraction may not be useful as an endpoint ofthrombolytic therapy comparative trials. Circulation1990;82:1847.
24 Van de Werf F. Discrepancies between the effects of coro-nary reperfusion on survival and left ventricular function.Lancet 1989;i:1367-89.
25 Califf RM, Topol EJ, Stack RS, Ellis SG, George BS,Kereiakes DJ, et al. Evaluation of combination throm-bolytic therapy and timing of cardiac catheterization inacute myocardial infarction. Results of thrombolysis andangioplasty in myocardial infarction-phase 5 random-ized trial. Circulation 1991;83:1543-56.
353
on Novem
ber 20, 2021 by guest. Protected by copyright.
http://heart.bmj.com
/B
r Heart J: first published as 10.1136/hrt.74.4.348 on 1 O
ctober 1995. Dow
nloaded from