Embed Size (px)
Citation preview
Healthy Environment for Children
World Health Organization
WHO/SDE/PHE/02.06
Initiating
an Alliance
for Action
Initiating an Alliance for Action
© World Health Organization 2002
All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination,
World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: 41 22 791 2476; fax: 41 22 791 4857;
email: bookorders who.int). Requests for permission to reproduce or translate WHO publications – whether for sale
or for noncommercial distribution – should be addressed to Publications, at the above address (fax: 41 22 791
4806; email:–permissions who.int).
The designations employed and the presentation of the material in this publication do not imply the expression of
any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country,
territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on
maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or
recommended by the World Health Organization in preference to others of a similar nature that are not mentioned.
Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication is complete and
correct and shall not be liable for any damages incurred as a result of its use.

Healthy Environment for Children
SUMMARY
Children are exposed to serious health risksfrom environmental hazards. Over 40%of the global burden of disease attributed
to environmental risk factors fall on children below5 years of age, who account for only about 10%of the world’s population. Environmental riskfactors often act in concert, and their effects areexacerbated by adverse social and economicconditions, particularly poverty. Children areparticularly vulnerable, and action needs to betaken to allow them to grow up and develop ingood health, and to contribute to economic andsocial development. The aims for action are setby the Millennium Development Goals, whosetargets are reduced child mortality andenvironmentally sustainable development.
The Healthy Environments for Children initiativeis designed to protect children from the physicalhazards in their environment, within the contextof social, economic and behavioural determinants.This initiative should build upon the active andcommitted involvement of various stakeholders,such as decision-makers, community leaders,teachers, health professionals, nongovernmentalorganizations (NGOs), the private sector, and thefamilies. The outcome is expected to be thecreation of a concerted, popular, participatory andinclusive movement, supported by a global allianceof key institutions and organizations at the
international level, and by alliances at the nationaland local level.
This initiative is seen as an umbrella,encompassing all efforts that support action basedon scientific evidence. This should ensure thatinvestments are made to address real prioritiesthrough the most cost-effective measures. Keyelements for implementation include taking stockof ongoing efforts; creating a popular movementby mobilizing all potential players that can makea difference; consolidating and disseminatingscientific knowledge on risk factors and cost-effective interventions; initiating and promotingresearch to complement existing knowledge andsupport efficient action, and efforts to makehealthy environments for children a majorcomponent of policy-making; promoting thehealthy settings approach; and fosteringintersectoral, integrated collaboration.
Priorities will be set at the local, national orregional level by the initiative, and a number ofpriority risk factors have been identified as majorglobal issues, requiring concerted internationalaction. These are: household water security,hygiene and sanitation, air pollution, diseasevectors, chemical hazards, and injuries andaccidents. Approaches to scale up actions areproposed for each risk factor.
The present document has been prepared by the WHO Secretariat in support of discussions to beheld during the World Summit on Sustainable Development (WSSD) in Johannesburg, SouthAfrica, in August/September 2002. Information is presented to stimulate the creation of an alliancefor action, as broad-based as possible, for the initiation of a worldwide movement on HealthyEnvironments for Children during the months immediately following the WSSD.
◆ iii

Initiating an Alliance for Action

Healthy Environment for Children
TABLE OF CONTENTS
1. THE NEED FOR ACTION ............................................................................................... 1
2. ENVIRONMENTAL RISK FACTORS FOR CHILD HEALTH ....................................... 3
3. PRIORITY ENVIRONMENTAL HEALTH ISSUES......................................................... 7
3.1 Household water security ..................................................................................... 7
3.2 Hygiene and sanitation......................................................................................... 9
3.3 Air pollution ...................................................................................................... 11
3.4 Disease vectors ................................................................................................... 13
3.5 Chemical hazards ............................................................................................... 15
3.6. Injuries and accidents ......................................................................................... 17
4. CREATING HEALTHY SETTINGS ............................................................................... 18
5. MECHANISMS FOR IMPLEMENTATION .................................................................. 21
6. MONITORING CHILDREN’S ENVIRONMENTAL HEALTH ................................... 23
7. BUILDING A GLOBAL ALLIANCE ............................................................................... 24
ANNEX – THE BANGKOK STATEMENT .......................................................................... 27
◆ v

Initiating an Alliance for Action

Healthy Environment for Children
1. THE NEED FOR ACTION
Children today live in an environmentthat is vastly different from that of afew generations ago. New challenges
include increasing industrialization andglobalization, rapid urban population growth,non-sustainable consumption of naturalresources, and increases in the trade and useof chemicals. While economic developmentand improved hygiene and health care haveled to a significant decrease of childhoodmorbidity and mortality in many parts of theworld, new “modern” risks to children’s healthmust now be added to the “basic”environmental risks such as unsafe drinking-water, lack of adequate sanitation, and indoorair pollution, which are closely linked withand aggravated by persistent poverty andsocial inequity. Exposure to environmentalrisk factors during childhood may not onlyimpact on a child’s health, but ill-healthoutcomes may persist through into adult lifeor may appear during adulthood. Unsafe andunhealthy environments are thus violatingchildren’s rights to health, and represent aserious threat to the potential for sustainabledevelopment.
While the environmental burden of ill healthaffects all children, it is greatest among thepoor, whether in the poor regions of theworld, in poor countries, in poorcommunities or in poor households withincities. Inequities in child health constitutesystematic and relevant differences betweenpopulation groups that are both avoidable andunfair. These inequities not only relate to asocioeconomic gradient (e.g. income,education), but often exist in relation togender, family structure (e.g. orphans, single-parent households), geographic differences(e.g. rural versus urban), ethnicity and otherfactors.
Poor children:
■ are more likely to die in the first monthof life, in the first year of life, or beforethey reach the age of five;
■ are sick more often and more seriously;
■ are less well-nourished and are more likelyto lag behind in growth and psychosocialdevelopment;
■ are more likely to have difficulties atschool and on the job
… than better-off children.
Social, economic and behavioural factorslargely impact on the health outcomes due tounhealthy environments. Malnutritionassociated with poverty often results in anincreased susceptibility to infections and tothe effect of chemical pollutants, and so dounhealthy behaviours, such as inadequatepersonal hygiene, and the lack of a care-givingsocial environment. This requires acomprehensive approach addressing not onlythe physical environment, but also thepsychosocial and economic determinants thatimpact on health outcomes.
Healthy Environments for Children – Thefoundation of sustainable development
Sustainable development has three main
components: economic development, social
justice, and environmental protection. Healthy
environments for children are at the same time
a condition depending on all of these
elements.
Poverty is the single biggest threat to children’s
health and affects children often through
environmental factors such as sanitation and
clean air. Economic development and social
justice are prerequisites to overcome poverty.
◆ 1

Initiating an Alliance for Action
The bare survival of millions of children is at
stake and needs to be addressed now. In
addition, many environmental exposures of
children cannot be corrected during their adult
life. Healthy environments are a condition to
safeguard children’s intellectual, social and
economic potential, and the future of our
societies.
While the environmental burden of disease is
by far highest among poor children, the
environment also impacts on those children
living in medium and high income societies.
Goal and objectives
Children are more susceptible than adults tothe effects of environmental health hazards,and therefore require special protection. Theaim of the current initiative is to launch amovement to ensure appropriate action topromote healthy environments for children.This movement will be supported by analliance and involve partners from varioussectors, and at various levels of responsibility.The overall goal of the movement is to preventdisease and disability in children associatedwith biological, chemical and physicalenvironmental hazards, with due recognitionof the importance of behavioural, social andeconomic factors. This goal is in line with theMillennium Development Goals i.e. toreduce child mortality (Goal 4), and to ensureenvironmental sustainability (Goal 7). Thus,the movement should be instrumental inachieving the target to “reduce by two-thirdsbetween 1990 and 2015 the under-fivemortality rate”.
The main objectives of the movement willbe:
■ to provide the knowledge base to enableinformed policy action;
■ to raise the awareness of decision-makersand ensure their political commitmentto take action;
■ to help countries and communities createand maintain healthier environments,enabling children to grow and developto their full potential as citizens in theirown right and contribute to sustainabledevelopment; and
■ to promote safe and healthy homes andcommunities for children, as well ashealthy behaviours.
For action to be successful, credible andconcrete targets will have to be set at the locallevel, taking into consideration the priorityenvironmental threats to be addressed, theappropriate settings in which children areexposed to given risk factors, and the needsof the different age groups involved. Actionwill centre on environments where children,boys and girls of all age groups fromconception to adolescence, spend their timein their homes and surroundings, schools andrecreation areas, and community places inboth urban and rural areas, especially (but notexclusively) in the developing countries.
One major aim of the movement will be: “the
home as a safe place” for every family,
irrespective of the level of their income. There
is a need for basic protection of each child
given a space with access to clean drinking-
water and food, adequate sanitation, a space
free from risk of injury, such as unprotected
fires, or unprotected machinery and tools, a
space protected from as much indoor
pollution as possible, and with as much
daylight as possible. The child needs a
stimulating environment, including toys,
colours and enough space for play, tailored
to the different needs of infants, children and
adolescents.
It should be recalled that malnutrition isresponsible for by far the largest global burdenof disease through its effects on the immunesystem. The achievement of food security is akey prerequisite to achieve health andenvironment objectives. Therefore, themovement could not achieve its goals and
2 ◆
Healthy Environment for Children
targets without concurrent progress beingmade in combating malnutrition of childrenat all age levels.
Growing international concern calls foraction
The Convention on the Rights of the Child(1989) lays down the fundamental right ofevery child to “the enjoyment of the highestattainable standard of health”. Several recentinternational declarations and policystatements demonstrate a growingcommitment to a healthier and saferenvironment for children. Three of these areof particular relevance:
■ Declaration of the Environment Leadersof the Eight (G8) on Children’sEnvironmental Health (1997), asconfirmed by the Banff MinisterialStatement on the World Summit onSustainable Development (2002).
■ The United Nations General AssemblySpecial Session on Children (UNGASS)(2002).
■ The Bangkok Statement – A Pledge toPromote the Protection of Children’sEnvironmental Health (2002): seeAnnex.
Several other recent recommendations addressspecific issues related to healthy environmentsfor children, such as the ILO Convention 182on the Worst Forms of Child Labour (1999).
2. ENVIRONMENTAL RISK FACTORSFOR CHILD HEALTH
Throughout the world, children facesignificant threats to health from awide range of environmental hazards.
Preliminary estimates suggest that up to onethird of the global burden of disease can beattributed to environmental risk factors. Over40% of this burden fall on children under 5years of age who make up only about 10% ofthe world’s population. Inadequate drinking-water and sanitation, indoor air pollution,injuries and other risk factors are the rootcause for more than 4.7 million deathssuffered annually by children under five fromillnesses aggravated by unhealthyenvironments.
The health and environment linkagesaffecting children are numerous and complex.In most cases, exposure to a particular
environmental risk is associated with manydifferent health outcomes, and a range ofenvironmental exposures may influence aparticular disease condition. This is based onthe contribution of environmental risk factorsto global child mortality and morbidity,thereby highlighting the biggestenvironmental threats to children’s health, andillustrates the potential for disease preventionthrough the association of specific risk factorswith distinct settings. In addition, there arenon-environmental risk factors which tend toaggravate the health impacts emanating fromthe child’s environment. Nutrition is one suchkey factor, either in the form of malnutritionor the lack of micronutrients or in the formof obesity due to sedentary lifestyle orunhealthy eating habits.
◆ 3

Initiating an Alliance for Action
Health-and-hygiene-environment linkages for children
Community
Setting School
Home
Risks factor
Diseaseoutcomes
Diarrhoeal diseases
Acute respiratory Infections
Tuberculosis
Perinatal effects
Nutritional diseases
Malaria & other vector diseases
Child cluster diseases
Chronic respiratory diseases
Cancer
Injuries & accidents
Drowning
Poisonings
Cognitive effects
Hous
ing
cond
ition
s
Indo
or a
ir
Food
saf
ety
and
supp
ly
Wat
er,
sani
tatio
n an
d
Outd
oor a
ir
Lead
Pest
icid
es a
ndot
her c
hem
ical
s
UV ra
diat
ion
Dise
ase
vect
ors
Occu
patio
nal
Envi
ronm
ents
Tran
spor
tatio
n
Recr
eatio
nal
activ
ities
Emer
genc
ysi
tuat
ions
While a global analysis of the burden ofdisease in children associated withenvironmental risk factors helps identifypriorities for global action, additional riskfactors may result in a high disease burden atthe regional or local level. Developing a cause-effect matrix for a particular geographicalregion based on a differentiated analysis ofthe burden of disease will help identifypriorities for regional initiatives orprogrammes to create healthy environmentsfor children.
An unequal disease burden: the risktransition
A differentiated analysis of the global burdenof disease (GBD) reveals that mostenvironmental threats to children’s health are
associated with persistent poverty and socialinequity. The two major problems are:communicable diseases due to lack of safewater and sanitation, and acute respiratoryinfections due to high levels of indoor airpollution in combination with unhealthyhousing. The virtual disappearance of thesetwo leading causes of child mortality, withthe transition towards an industrializedsociety, demonstrates the dominant influenceof socioeconomic factors on the nature andmagnitude of children’s health problems.
However, communicable diseases do notoccur exclusively in developing countries andtoxic chemicals are not exclusively associatedwith industrialized countries. There arepockets of poverty in rich countries wherecertain population groups experiencedeprivations with their associated health
4 ◆

Healthy Environment for Children
problems, which are similar to those indeveloping countries. Also, toxic chemicalsare increasingly being used in developingcountries, often with fewer controls andregulations than in industrialized countries.
There is a clear shift in the pattern of leadingenvironmental health problems in children.This differential is not only measurablebetween rich and poor countries but alsobetween population groups within a givencountry and within any urban agglomeration,ranging from periurban slums with sub-standard housing to affluent modern suburbs.Typical “modern” risks include chronicrespiratory illnesses, asthma, immunologicaldisorders, neurological, neurodevelopmentaland behavioural effects, as well as childhoodcancers. In addition, there are emerging riskssuch as environmental allergens, UV
radiation, endocrine disruptors, autoimmuneeffects, and other diseases not directly relatedto the quality of the child’s environment. Anypotential health-and-environment linkagesrequire further research and a search for othercausative factors or combinations of factors.
Environmental risks to children tend to begreater among rural populations comparedwith urban populations, and an unequaldisease burden on the rural poor may befurther aggravated by lack of access to healthcare. However, the health status of childrenliving in urban poverty is equallypreoccupying. Consequently, population-based risk assessment is the prerequisite of acost-effective strategy, with tailoredinterventions to reduce the environmentaldisease burden in children.
Transition of children’s environmental health risks with economic status
Basic risks :Unhealthy housingUnsafe water supplyLack of sanitationIndoor air pollutionLead in gasoline
Modern risks :Respiratory factors (asthma)Transport accidents (injuries)Recreational activitiesToxic chemicals
Emerging issues :UV radiationEnvironmental allergiesEndocrine disruptors
Importance ofenvironmentalrisks
Low Middle High Income
Populationsin poverty
Populationsin transition
Industrializedsocieties
Socio-economicdevelopment
Basic risks
Modernrisks
Emergingrisks
◆ 5

Initiating an Alliance for Action
Focus on action
The above overview of health andenvironment linkages demonstrates that thedesign and implementation of programmesto promote healthy environments for childrenmust, in addition to addressing global risks,tackle problems at the regional and local level.Only the selection of key risk factors locallycan guarantee that one sees the prevailinghealth risks in combination, and can detecttheir synergistic or aggravating effectsdetected.
For example, the Strategy for Children’sEnvironmental Health in Latin America andthe Caribbean has identified the following aspriorities for action: (i) water resources, waterquality and basic sanitation, (ii) indoor andoutdoor air quality, (iii) heavy metals, (iv)pesticides, and (v) climate variability andchange.
The Third European Ministerial Conferenceon Environment and Health, held in Londonin 1999, recognized (i) injuries, (ii) smokingand environmental tobacco smoke, and (iii)asthma and other related respiratory diseasesas the main environmental threats tochildren’s health in Europe. In addition, theapparent increase in childhood cancers andneurodevelopmental disorders, and the riskof water and food-related diseases are alsosubjects of major concern.
Specific issues may be of relevance togeographically defined areas of the world. Forexample, Australia has the highest rate of skincancer in the world, which is attributable topeople’s exposure to high levels of UVradiation. Frequent sun exposure and sunburnin childhood set the stage for high rates ofskin cancer later in life, and may cause oraccelerate cataract development and limit theeffectiveness of the immune system. Similarly,arsenic contamination of drinking-waterdrawn from groundwater is a priority issuein some countries of South-east Asia.
Identifying priorities and building aprogramme should take into account and seeksynergies with existing activities such as single-issue campaigns for water or food security;risk-focused programmes to eradicate theworst forms of child labour, to prevent injuriesand accidents, or to create a tobacco-freeenvironment; and disease-specificprogrammes such as Roll Back Malaria.Activities to create healthy environments forchildren should complement these effortsrather than re-create existing programmes.
As a first step, and to make the best use ofscarce resources, global action should focuson improving the health and wellbeing ofthose children who are most at risk, asdescribed in detail in the following section.
6 ◆

Healthy Environment for Children
3. PRIORITY ENVIRONMENTAL HEALTH ISSUES
Throughout the developing world,traditional environmental healthhazards remain the primary source of
ill-health today e.g. biologically contaminatedwater, poor sanitation, indoor smoke,rampant disease vectors such as mosquitoes,an inadequate food supply, and unsafe wastedisposal which are all usually associated withpoverty and social exclusion. In addition, thevery same populations are often also exposedto toxic chemicals with little or no protection.Children’s health problems resulting fromthese hazards rank among the highestenvironmental burden of disease worldwide.
Significant progress in reducing theenvironmental burden of disease on a globalscale can only be achieved through focusingon the key risk factors. Comprehensivecomparative risk assessment suggestsconcentration on a cluster of sixenvironmental issues, as follows:
■ Household water security
■ Hygiene and sanitation
■ Air pollution
■ Disease vectors
■ Chemical hazards
■ Injuries and accidents.
The combined effects of these environmentalrisks are, in one way or another, “diseases ofpoverty” and constitute the bulk of childmortality and morbidity on a global scale. Theproposed action programme for healthyenvironments for children is designed to focuson interventions to prevent or reduce childexposure to these risk factors, and to supporthealth services at all levels in managing relateddisease outcomes. Thus it should make acrucial, if not decisive, contribution towardsachieving the Millennium Development Goal
of reducing by two thirds the under-fivemortality rate.
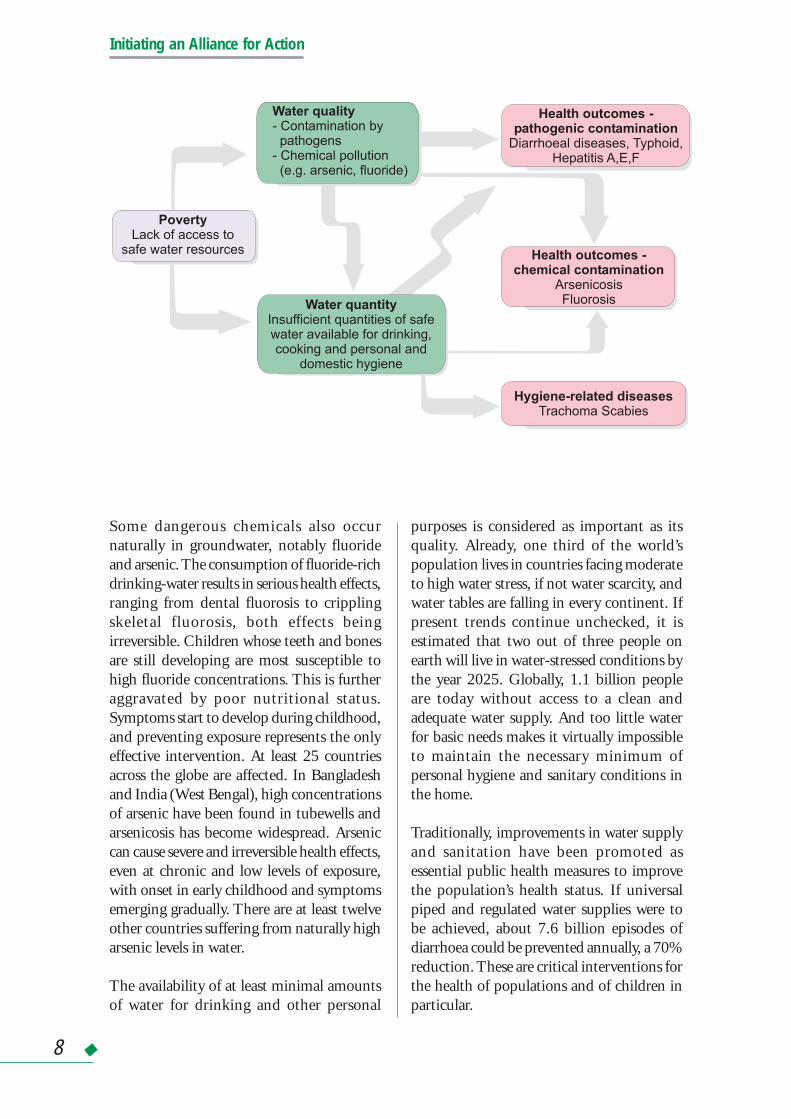
3.1 Household water security
A child’s wellbeing is highly dependent onboth the quality and the availability of water,and on how well this precious resource ismanaged. Around the world, both biologicaldisease agents and chemical pollutants arecompromising drinking-water quality.Contaminated water causes a range of diseaseswhich are often life-threatening. Of the water-borne diseases affecting children, the mostdeadly are diarrhoeal infections. Diarrhoea isestimated to cause 1.3 million child deathsper year, constituting about 15% of total childdeaths under five in developing countries. Themost dramatic event in recent history has beenthe cholera epidemic in South America, whichstarted in Peru in 1991 and then swept acrossthe continent.
The public health importance of diarrhoeaamong children lies partly in the highmortality rates as well as in the interactionsbetween malnutrition, recurrent diarrhoeaand impaired child development. Contraryto breastfed infants, bottle-fed infants arehighly exposed to the effects of unsafedrinking-water. It cannot be overemphasizedthat the transmission routes for infectiousagents are complex and thus contribute to thecomplexity of prevention. Interventions inwater supply, sanitation and hygiene areestimated to reduce diarrhoeal incidence, onaverage, by a quarter (25%) and childmortality by 65%. However, selectedinterventions have been shown to be muchmore efficient in certain settings.
◆ 7
Initiating an Alliance for Action
Some dangerous chemicals also occurnaturally in groundwater, notably fluorideand arsenic. The consumption of fluoride-richdrinking-water results in serious health effects,ranging from dental fluorosis to cripplingskeletal fluorosis, both effects beingirreversible. Children whose teeth and bonesare still developing are most susceptible tohigh fluoride concentrations. This is furtheraggravated by poor nutritional status.Symptoms start to develop during childhood,and preventing exposure represents the onlyeffective intervention. At least 25 countriesacross the globe are affected. In Bangladeshand India (West Bengal), high concentrationsof arsenic have been found in tubewells andarsenicosis has become widespread. Arseniccan cause severe and irreversible health effects,even at chronic and low levels of exposure,with onset in early childhood and symptomsemerging gradually. There are at least twelveother countries suffering from naturally higharsenic levels in water.
The availability of at least minimal amountsof water for drinking and other personal
purposes is considered as important as itsquality. Already, one third of the world’spopulation lives in countries facing moderateto high water stress, if not water scarcity, andwater tables are falling in every continent. Ifpresent trends continue unchecked, it isestimated that two out of three people onearth will live in water-stressed conditions bythe year 2025. Globally, 1.1 billion peopleare today without access to a clean andadequate water supply. And too little waterfor basic needs makes it virtually impossibleto maintain the necessary minimum ofpersonal hygiene and sanitary conditions inthe home.
Traditionally, improvements in water supplyand sanitation have been promoted asessential public health measures to improvethe population’s health status. If universalpiped and regulated water supplies were tobe achieved, about 7.6 billion episodes ofdiarrhoea could be prevented annually, a 70%reduction. These are critical interventions forthe health of populations and of children inparticular.
Water quality- Contamination bypathogens
- Chemical pollution(e.g. arsenic, fluoride)
Water quantityInsufficient quantities of safewater available for drinking,cooking and personal and
domestic hygiene
Health outcomes -pathogenic contamination
Diarrhoeal diseases, Typhoid,Hepatitis A,E,F
Health outcomes -chemical contamination
ArsenicosisFluorosis
Hygiene-related diseasesTrachoma Scabies
PovertyLack of access to
safe water resources
8 ◆

Healthy Environment for Children
Scaling-up of actions
Further strengthening of the evidence base,with better geographical coverage andspecificity for children in different age groupsis required in the area of water accessibilityand safety, and this should underpin policy-making and advocacy for cost-effectiveinterventions.
Improved water supply and sanitation haslong been targeted as a priority for health anddevelopment. It was central to theInternational Drinking Water Supply andSanitation Decade, and more recently isreflected in the Millennium DevelopmentGoals set by world leaders at the UNMillennium Summit in September 2000. Thetarget is to “halve, by 2015, the proportionof people without sustainable access to safedrinking water” through the promotion ofaffordable and environmentally soundtechnologies.
Action has also to be accelerated to fulfil thecommitment made at the UN MillenniumSummit to halt the unsustainable exploitationof water resources by developing watermanagement strategies at the regional,national and local levels, which will secureboth equitable access and adequate watersupplies.
Capacity-building efforts should be gearedtowards strengthening the enforcement ofexisting environmental regulations on waterquality and resource protection. This requiresalso close monitoring of drinking-waterquality at the local service level throughpractical and cost-effective methods.
3.2 Hygiene and sanitation
Lack of adequate sanitary facilities and poorhygienic practices are common throughoutthe developing countries; the lowest levels of
service coverage are to be found in Asia andAfrica where more than half of the ruralpopulations are excluded from anymeasurable progress in this area. Globally, 2.4billion people, most of them in developingcountries, do not have access to improvedsanitation facilities. Data collected over tenyears show that little progress has been madein reducing this number.
Unhygienic conditions and practices at thehousehold level create a dangerousenvironment with immediate health risks tochildren. Also, lack of sanitation facilities inschools helps transmit diseases. Waste dumpssited on the outskirts of almost all major citiesprovide hazardous environmental conditionsto those living nearby, and even more so tothose living as scavengers on such wastes.Sanitation interventions, technical andmanagerial, are badly needed in all areas inhouses, schools, and within the communityat large. These must be accompanied by thenecessary behavioural changes in the child andadult populations, which pose a formidablehygiene education challenge to the healthsector.
Trachoma is one of the infectious diseaseswhich are linked to environmental conditions,and is thus amenable to effectiveenvironmental interventions. Worldwidethere are around 6 million people irreversiblyblinded by trachoma and about 500 millionpeople are at risk of the disease. Improvedsanitation and hygiene behaviour contributesignificantly to the control of trachoma.Through the provision of adequate quantitiesof water alone, about one quarter of theburden of this disease could be prevented orreduced.
Intestinal worms severely affect about 10%of the population of the developing world.Children, due to their direct exposure to soiland other helminth-carrying material areespecially at risk, and they are generally moreworm-infested than adults. Intestinal parasitic
◆ 9

Initiating an Alliance for Action
infections in children can lead tomalnutrition, anaemia and retarded growth,depending upon the severity of the infection,in addition to their adverse effects on theimmune system. Exposure to helminths andhookworms can be effectively controlledthrough improved sanitation, hygiene andwater supply.
Scaling-up of actions
Further work on the evidence base, specificallytargeting children, is required across thespectrum of sanitation, hygiene andbehavioural interventions to reduce infectiousdiseases with an environmental etiology. Thisentails child-specific research efforts on theimpact of alternative sanitation methods onchild disease outcome, supported by pilot-scale and expanded implementation of high-yield health interventions, using feedbackfrom experience to guide future activities.
The setting of most significance in the child’senvironment is the home and this should begiven prime attention. This implies improved
household sanitation facilities throughaffordable interventions, including thedevelopment of a sense of responsibleownership and use following the commonrules of hygiene. All potential pathways ofdisease transmission have to be addressed,including drinking-water, safe handling offood, excreta disposal, and personal hygiene.
Improved hygiene practices, including bothhand and face washing, and safe handling anddisposal of children’s faeces should bepromoted through educational campaigns inthe community and in kindergartens andschools.
Several UN and other organizations in 2000launched FRESH (Focusing Resources forEffective School Health) to achieve morechild-friendly schools. This includes a simpleset of core interventions, health-related schoolpolicies, provision of safe water and sanitationin all schools, skills-based health and hygieneeducation, and school-based health andnutrition services.
P ontaminationof the environment and
of drinking waterresources
athogenic c
Poor hygienein a contaminated
environment leads toperson-to-person
transmission of disease andcontamination of food
Health outcomesDiarrhoeal diseasesTrachoma ScabiesHelminthic infections- Ascariasis- Trichuriasis- Hookworm
PovertyLack of access to
basic sanitation infrastructure
EducationLack on information on
health consequences of poorhygiene
10 ◆

Healthy Environment for Children
3.3 Air pollution
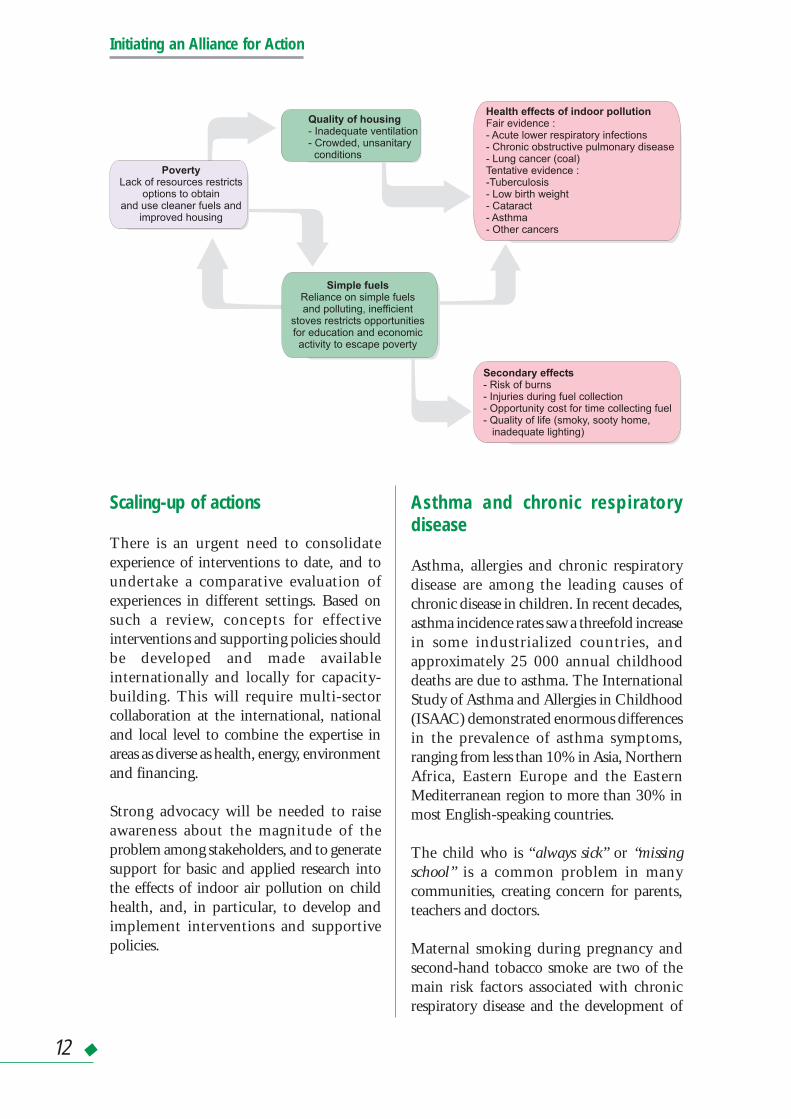
Air pollution is a major environment-relatedhealth threat to children and a risk factor forboth acute and chronic respiratory disease.Outdoor air pollution, primarily aconsequence of traffic and industrialprocesses, remains a serious problem in citiesthroughout the world, particularly in themegacities of developing countries. It isestimated that a quarter of the worldpopulation is exposed to unhealthyconcentrations of air pollutants. In recentyears, indoor air pollution has received moreand more attention: a pollutant releasedindoors is a thousand times more likely toreach the lungs than a pollutant releasedoutdoors. Indoor air pollution is strikinglydifferent in industrialized and developingcountries, and also varies between urban andrural settings. While the main concern indeveloping countries is the exposure tocombustion products from biomass fuel andcoal, poor indoor environments in theindustrialized world are characterized byreduced ventilation, the presence of biologicalagents such as moulds, and a myriad ofchemicals in furnishing and constructionmaterials.
Acute respiratory infections
More than half of the 2.1 million annualdeaths in children under five caused by acutelower respiratory infections may be associatedwith indoor air pollution, lack of adequateheating, or other precarious living conditions.Indoor air pollution from the combustion ofbiomass and coal is a serious and widespreadproblem in developing countries. Some 3billion people worldwide rely on biomass fuelsand coal for cooking and heating needs. Ofthese, approximately 800 million depend onagricultural residues and animal dung assources of fuel because of severe fuel woodshortage. Traditional low-efficiency cookingstoves produce heavy smoke with fine
particles, carbon monoxide, and carcinogeniccompounds.
Infants are most at risk due to the immaturityof their respiratory organ systems and theirhigh exposure when carried on their mother’sback or placed near the cooking stove. Theassessment of the burden of diseaseattributable to indoor air pollution, which iscurrently under way, will further strengthenthe evidence that indoor air pollution presentsa substantial risk to children’s health anddemands concerted global action.
While second-hand tobacco smoke andcertain outdoor air pollutants are known riskfactors for acute respiratory infections, indoorair pollution from biomass fuel smoke is byfar the biggest single contributor to the globalburden of disease. In principle, severaldifferent types of interventions are capable ofproducing a reduction in exposure to indoorair pollution. These include (i) interventionsrelating to the source of pollution, e.g.changing to cleaner fuels or improved stoves,(ii) interventions in the living environment,e.g. better ventilation, and (iii) changes in userbehaviour, e.g. keeping children away fromthe smoke or eliminating tobacco smokingin the home. Beyond their effectiveness inreducing the level of indoor air pollution,these interventions should also meet severalother criteria such as local participation, inparticular of women, to ensure a culturallyappropriate and sustainable approach.
Initial work on assessing the economic costsand benefits of interventions in householdenergy is encouraging. For example, the cost-effectiveness of an improved stove appears tocompare favourably with other importanthealth interventions. However, asinterventions to reduce indoor air pollutionhave a wide range of implications for healthand quality of life, an appropriate assessmentof their cost-effectiveness may require novelapproaches.
◆ 11
Initiating an Alliance for Action
Scaling-up of actions
There is an urgent need to consolidateexperience of interventions to date, and toundertake a comparative evaluation ofexperiences in different settings. Based onsuch a review, concepts for effectiveinterventions and supporting policies shouldbe developed and made availableinternationally and locally for capacity-building. This will require multi-sectorcollaboration at the international, nationaland local level to combine the expertise inareas as diverse as health, energy, environmentand financing.
Strong advocacy will be needed to raiseawareness about the magnitude of theproblem among stakeholders, and to generatesupport for basic and applied research intothe effects of indoor air pollution on childhealth, and, in particular, to develop andimplement interventions and supportivepolicies.
Asthma and chronic respiratorydisease
Asthma, allergies and chronic respiratorydisease are among the leading causes ofchronic disease in children. In recent decades,asthma incidence rates saw a threefold increasein some industrialized countries, andapproximately 25 000 annual childhooddeaths are due to asthma. The InternationalStudy of Asthma and Allergies in Childhood(ISAAC) demonstrated enormous differencesin the prevalence of asthma symptoms,ranging from less than 10% in Asia, NorthernAfrica, Eastern Europe and the EasternMediterranean region to more than 30% inmost English-speaking countries.
The child who is “always sick” or “missingschool” is a common problem in manycommunities, creating concern for parents,teachers and doctors.
Maternal smoking during pregnancy andsecond-hand tobacco smoke are two of themain risk factors associated with chronicrespiratory disease and the development of
Quality of housing- Inadequate ventilation- Crowded, unsanitaryconditions
Simple fuelsReliance on simple fuelsand polluting, inefficient
stoves restricts opportunitiesfor education and economicactivity to escape poverty
Secondary effects- Risk of burns- Injuries during fuel collection- Opportunity cost for time collecting fuel- Quality of life (smoky, sooty home,
inadequate lighting)
PovertyLack of resources restricts
options to obtainand use cleaner fuels and
improved housing
Health effects of indoor pollutionFair evidence :- Acute lower respiratory infections- Chronic obstructive pulmonary disease- Lung cancer (coal)Tentative evidence :-Tuberculosis- Low birth weight- Cataract- Asthma- Other cancers
12 ◆

Healthy Environment for Children
asthma, particularly if the exposure to smokeoccurs during periods of lung growth anddevelopment. While the lack ofimmunological challenge by infections inearly life appears to favour the developmentof allergies later in life, the relationshipbetween early infections and asthma is lessclear. Early-life exposure to allergens maysensitize children, thereby increasing the riskof the so-called atopic diseases such as hayfever, eczema, dermatitis and asthma. It is yetunclear whether air pollution contributes tothe development of asthma. However,exposure to biomass fuels is strongly associatedwith chronic obstructive pulmonary disease(COPD), and exposure to coal smoke withlung cancer.
Indoor and outdoor air pollutants canenhance the severity of chronic respiratorydisease, and increase both the frequency andseverity of asthma attacks. Important indoorair triggers include smoke (from cooking,smoking and heating), moulds, dust mites,cockroach allergens and other biologicalagents, while known outdoor air triggersinclude ozone and particulate matter.Additional non-environmental triggers ofasthma include pharmaceuticals, rigorousexercise, temperature changes and emotionalfactors.
Asthma and allergic disorders particularlyaffect urban children. Poor households andschools are more likely to be reservoirs for dustmites, cockroach allergens, moulds and otherindoor triggers of asthma. Poor children aremore likely to be hospitalized for asthma, andmore likely to suffer chronic health effects andsocial dysfunction. Poor children are also leastlikely to benefit from the best care practices:they tend to receive treatment in emergencyrooms without follow-up by chronic careproviders, are less likely to receive themaintenance medication required, and haveno access to environmental and socialcounselling.
Scaling-up of actions
Stronger advocacy is required to raise theawareness of decision-makers and the generalpublic about the burden that chronicrespiratory disease in children imposes on thefamily, the community, and the health systemabout the associated economic costs andpreventive and curative solutions available.Policy-makers, healthcare workers, andcommunities – in particular families andschools - have specific roles to play in theprevention and treatment of chronicrespiratory diseases that start in childhood.Healthcare workers are in a position toidentify children at particular risk of chronicrespiratory disease, and to suggest appropriateactions that families and communities cantake to protect them.
Policy measures to eliminate smoking are tobe strengthened in all countries, especially inthose settings where children spend most oftheir time. Furthermore, measures to controloutdoor air pollution are key elements in theprevention of chronic respiratory disease inchildren. Research into the causes of asthma,and the effectiveness and cost-effectiveness ofpreventive measures should be strengthened.
3.4 Disease vectors
Major global demographic, environmentaland societal changes occurring in the lastdecade contribute to the re-emergence ofvector-borne and other diseases, many ofwhich have an important impact on children’shealth and development. A considerableproportion of the disease burden for four keyvector-borne diseases malaria,schistosomiasis, Japanese encephalitis anddengue haemorrhagic fever falls on childrenunder five years of age.
Malaria is rampant in Sub-Saharan Africa andmany countries in Asia and Latin America,
◆ 13

Initiating an Alliance for Action
where children under five suffer highmortality and morbidity. In older children,malaria remains an important cause ofmortality and morbidity and significantlycontributes to low educational achievement.Malaria exists in 100 countries and accountsfor more than 800 000 deaths annually,mostly in children under five. About 90% ofthe disease burden resides in Africa.
Schistosomiasis is a water-borne disease thataffects children and adolescents mainlybecause of their specific behaviours: lack ofhygiene and swimming in contaminatedwater. It is endemic in 74 developingcountries, with more than 80% of infectedpeople living in Sub-Saharan Africa. Highinfection rates and individual worm loads setthe scene for a debilitating infection whichmay cause severe damage to the liver orbladder over many years, and can result inpremature death.
Japanese encephalitis occurs only in Southand South-east Asia, where it is linked withirrigated rice production ecosystems.Outbreaks occur in cycles. The annualnumber of clinical cases is estimated at about40 000. Some 90% of these cases are childrenin rural areas, with a 20% case-fatality rate.
Dengue affects mainly urban populations (theAedes species that transmit dengue are adaptedto the man-made environment), and inchildren the infection can develop intodengue haemorrhagic fever or dengue shocksyndrome with high levels of mortality.Annually, mortality due to dengue fever isestimated at around 13 000; more than 80%of these deaths occur in children.
A combination of five interventions indifferent settings is proposed for themosquito-borne diseases: use of insecticide-impregnated mosquito nets; the fitting ofscreens to windows, doors and eaves of houses;the application of zooprophylaxis in placeswhere mosquitoes are distinctly zoophilic; theuse of insect repellents; and improved watermanagement.
For the control of schistosomiasis, casedetection and drug treatment proved to bemost cost-effective in the short term, but asprevalence levels drop it becomes increasinglyexpensive to keep them low. Enhancedenvironmental management, provision ofbasic sanitation and community healtheducation should be put into place to makethe achievement of drug treatmentsustainable.
Scaling-up of actions
Sound and sustainable approaches tocontrolling disease vectors, and integratedprevention strategies should be put in place.This requires increased research into thedevelopment of safe alternative pesticides, andon alternative approaches such as biologicalcontrol and integrated vector management.The use of such approaches should bepromoted at community level. Decision-making criteria and procedures forcommunity-based interventions should bedeveloped, with the aim of reducing thetransmission risk in specific agriculturalecosystems.
Efforts should build on existing programmesfor vector-borne disease control. In the caseof malaria, collaboration with the Roll BackMalaria (RBM) programme on rapidassessment of the malaria situation, onpromoting the use of bednets andchemoprophylaxis, and on developingzooprophylaxis for malaria control in riceirrigation schemes offers opportunities in thisrespect.
Given the importance of personal behavioursfor prevention of vector-borne diseases,education on hygiene practices andbehaviours among parents, child care-giversand children should be provided. Safedomestic water management should bepromoted with the aim of reducing denguerisk.
14 ◆
Healthy Environment for Children
3.5 Chemical hazards
The use of chemicals has increaseddramatically due to the economicdevelopment in various sectors includingindustry, agriculture and transport. As aconsequence, children are exposed to a largenumber of chemicals of both natural andman-made origin. Exposure occurs throughthe air they breathe, the water they drink orbathe in, the food they eat, and the soil theytouch (or ingest as toddlers). They are exposedvirtually wherever they are: at home, in theschool, on the playground, and duringtransport.
Chemicals may have immediate, acute effects,as well as chronic effects, often resulting fromlong-term exposures. About 47 000 personsdie every year as a result of such poisoning.Many of these occur in children andadolescents, are unintentional (“accidental”),and can be prevented if chemicals wereappropriately stored and handled. Chronicexposures to various chemicals may result ina number of adverse outcomes, includingdamage to the nervous and immune systems,impairment of reproductive function anddevelopment, cancer, and organ-specificdamage. Sound management of chemicals,
particularly heavy metals, pesticides andpersistent organic pollutants, is a prerequisitefor the protection of children’s health. Dueto the magnitude of their health impact onchildren, the initial focus for action will beon lead and pesticides, but this by no meansimplies that other chemicals should beignored.
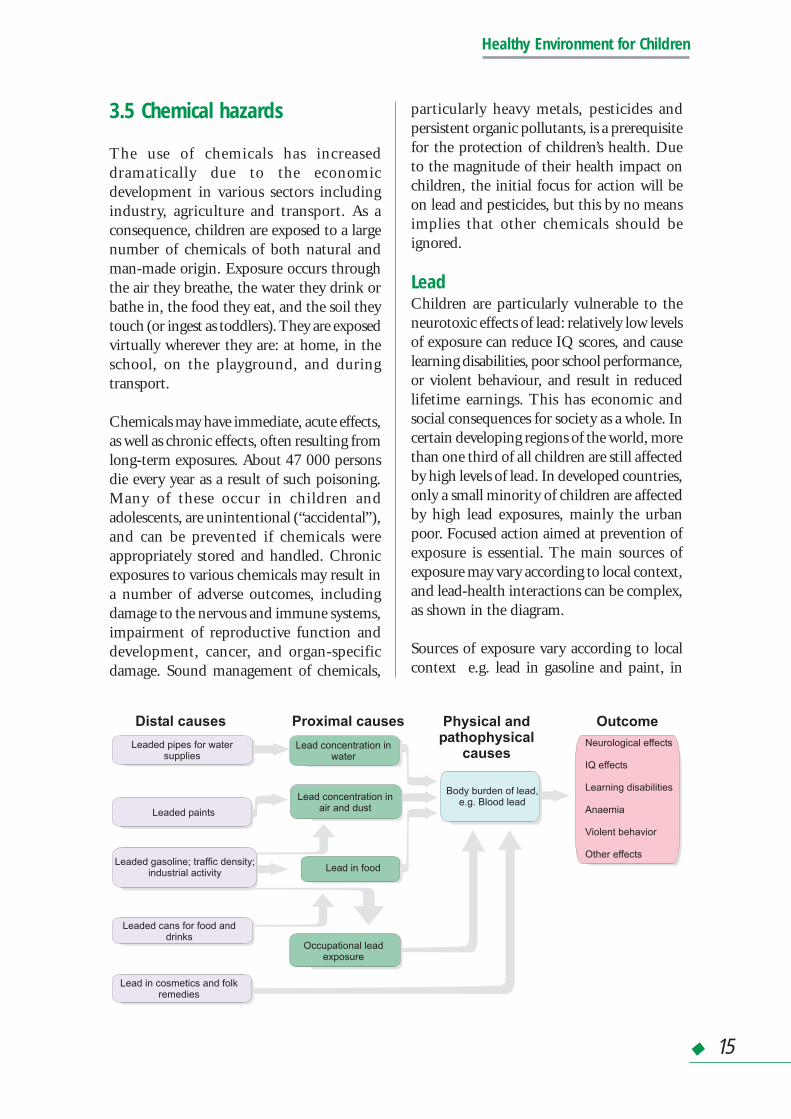
LeadChildren are particularly vulnerable to theneurotoxic effects of lead: relatively low levelsof exposure can reduce IQ scores, and causelearning disabilities, poor school performance,or violent behaviour, and result in reducedlifetime earnings. This has economic andsocial consequences for society as a whole. Incertain developing regions of the world, morethan one third of all children are still affectedby high levels of lead. In developed countries,only a small minority of children are affectedby high lead exposures, mainly the urbanpoor. Focused action aimed at prevention ofexposure is essential. The main sources ofexposure may vary according to local context,and lead-health interactions can be complex,as shown in the diagram.
Sources of exposure vary according to localcontext e.g. lead in gasoline and paint, in
Lead concentration inwater
Lead concentration inair and dust
Neurological effects
IQ effects
Learning disabilities
Anaemia
Violent behavior
Other effects
Leaded pipes for watersupplies
Leaded paints
Leaded gasoline; traffic density;industrial activity
Leaded cans for food anddrinks
Lead in cosmetics and folkremedies
Lead in food
Occupational leadexposure
Body burden of lead,e.g. Blood lead
Proximal causesDistal causes Physical andpathophysical
causes
Outcome
◆ 15

Initiating an Alliance for Action
glazed ceramics, in emissions from smelters,in battery recycling industries, use of leadpipes for water supply, or a contaminant infood or an ingredient in traditional medicines.
A number of activities are being undertaken,including awareness-raising, preparation ofstudy protocols and documents on leadexposure, estimation of the global burden ofdisease (GBD), and provision of technicaladvice to countries on a case-by-case basis.Focused action aimed at prevention ofexposure is essential and efforts to reduce leadexposure have to be intensified in the light ofthe large percentage of children in the worldwho are affected.
Pesticides
Pesticides are used in agriculture and in publichealth programmes as important elements inan integrated approach to vector control.However, they may pose a serious healthproblem to the whole population. The risksare higher for infants, children andadolescents, as they may be exposed duringperiods of special vulnerability.
Unsafe use, storage and disposal of pesticidesare the main causes of acute poisoning.Pesticides such as insecticides, herbicides androdenticides are accessible to children in ruralareas, but may also be found by toddlersexploring their home, garden sheds or garages.A study in Canada showed that almost 60%of poisoning cases registered at a paediatrichospital were due to pesticides and that theeffects of most pesticides were acute andsevere. In developing countries, the realincidence of pesticide poisoning is difficultto assess, but is assumed to be high. A largenumber of child and adolescent workers areexposed to pesticides through agriculturalwork, as they are commonly involvedinformally in the preparation and applicationof pesticides. Children are also exposed asbystanders during spraying for agriculturalpest control.
Chronic, low-level exposure to pesticides islinked with neurological, developmental,reproductive and other effects in children.Persistent pesticides that are present in thediets of small children (including breast milk)raise particular concern. They accumulate infatty tissue, and remain stored in the fattytissue of the body over long periods.
Scaling-up of actions
More child-specific research, as well asactivities to strengthen surveillancemechanisms and promote regulatorymeasures and risk-reduction interventions, arerequired in addition to the ongoing provisionof information and technical advice tocountries, collection of case data on children’sexposure and poisoning, classification ofpesticides by hazard, and recommendationson the public health use of pesticides.
Policy actions and regulatory measures shouldbe put in place to reduce or eliminate exposureto priority chemical pollutants affecting childhealth and development, such as persistentorganic pollutants and heavy metals. As a firststep in reducing children’s exposure to lead,governments should be urged to phase outthe use of leaded gasoline. Mechanisms shouldbe put in place to provide logistical, financialand technical support for such efforts.Regulatory measures should be encouragedto promote safe use of chemicals andsubstitution by safer alternatives. Integratedagricultural practices should be promoted toreduce reliance on the use of toxic pesticides.
At the local level, action should be taken topromote the safe use of chemicals throughthe provision of evidence-based informationon health risks from exposure to chemicalsand on cost-effective interventions todecision-makers. Aspects of chemical safetyand health should be incorporated into schoolcurricula, and health personnel should betrained to recognize and prevent toxicexposures. The commitment and active
16 ◆

Healthy Environment for Children
involvement of communities in such effortsshould be solicited.
3.6 Injuries and accidents
Each year unintentional injuries account formore than 400 000 deaths globally, themajority in children and adolescents. Mostof these occur in low- and middle-incomecountries. Many of those who survive theseinjuries suffer life-long disabling healthconsequences. In the European region, 3 to 4deaths out of 10 that occur in childrenbetween the ages of 0 and 4 years are aconsequence of injury.
Injuries are commonly classified based on“intentionality”. Most road traffic injuries,poisoning, falls, fire and burn injuries, anddrowning are unintentional. Intentionalinjuries include interpersonal violence(homicide, sexual assault, neglect andabandonment, and other maltreatment),suicide, and collective violence (war).Evidence suggests that some children andadolescents are more vulnerable to certaintypes of injuries. For example, poisoning,drowning, burns, and maltreatment bycaregivers affect primarily small children,while road traffic accidents, interpersonalviolence and sports injuries tend to affect olderchildren and adolescents. In addition, injuriestend to be more prevalent in boys.
Unfortunately, poor children commonly livein unsafe environments and are, therefore,exposed to risks that increase their likelihoodof being injured. These children areparticularly vulnerable as they have less chanceof overcoming these risks, and have feweradvantages such as access to educationalopportunities and health services.
The injury rates and patterns differ fromcountry to country, even within the sameregion, and from urban to rural areas. Forexample, in the rural areas injuries are related
mainly to farming activities, pesticidepoisoning, and drowning. In the urban areas,most injuries are traffic related, or linked togadgets and electrical appliances, falls orpoisonings resulting from householdchemicals and pharmaceuticals ingested bysmall children. The environmental factorsleading to injury may also be associated withsocial factors, such as family stress and criticallife events (e.g. hospitalization or chronicdisease of a parent, or change of residence).
The environmental factors leading to injuriesare often associated with other environmentalhealth risks. For example, home and schoolconstruction and furnishing materials can leadto unintentional injuries, and poisoning mayresult from exposure to chemicals unsafelyused or stored. Intentional injuries resultingfrom child maltreatment are associated withphysical and cognitive deficits in the abusedinfants, poor parenting skills, marital conflict,and lack of social support systems for families.Urban transport, land use patterns, andrecreation areas are linked to road trafficinjuries, as well as to exposure to air pollutionand noise. Workplaces pose specific physicaland chemical risks to adolescent workers,whose vulnerability is increased by unsafebehaviours.
There is a need to identify how these multipleenvironmental health risks cluster in certainsettings in order to plan preventive strategiesthat can lead to cost-effective health gainsamong children and adolescents. The keysettings to consider include, for example, thehome, the school and the route to the school,playgrounds, leisure and sports areas, therural-agricultural environment, and urbantransport.
Community-based interventions usingrelevant information on local patterns ofinjury and their causes have reduced the ratesof injuries in many countries (especially theindustrialized ones). The prevention ofinjuries is achieved through environmental
◆ 17

Initiating an Alliance for Action
modifications, changing the designs orstructures (engineering), applying and/orreinforcing regulatory measures, and, overall,changing unsafe behaviours througheducation.
Scaling-up of actions
Further work is required on reviews of theexisting evidence on the links betweenenvironmental factors and injuries occurringin specific settings. The preparation anddissemination of reports on the magnitudeof those risks, their common determinants,and on the most susceptible groups wouldhelp communities to plan interventions.
Strategies for action should be defined andproposed for each of the settings considered
(home, school, playground, other), basedupon the priority issues identified and theexperience with preventive interventions andtheir effectiveness. Pilot projects to addresschildhood environmental and injury risksthrough integrated preventive strategies andtheir evaluation especially in developingcountries will stimulate the policy processand ensure that interventions are based onevidence.
Regulatory measures, environmental changes,and education play a crucial role in theprevention of injuries and accidents inchildren’s environments. However, the mostsuccessful interventions are those where thesethree approaches are combined.
4. CREATING HEALTHY SETTINGS
Children are often exposed not just toone physical risk factor at a time, butto several of them simultaneously.
Their effects are mostly modulated bybehavioural, social and economic conditions,resulting in an exacerbation of ill-healthoutcomes. Sound approaches to create healthyenvironments for children, therefore, need toaddress a whole plethora of factors acting inconcert. Bearing this in mind, it is evidentthat the child itself should be placed in thecentre of action, and not individual riskfactors. This necessitates taking a holisticapproach, with a view to improving thesettings or places where children spend theirlives.
The focus is on places where children live andgrow: the home, the school and the
community. Health hazards and theirdeterminants in children’s everydayenvironment have to be identified andprotective measures that can be adopted byparents, families, neighbours, teachers, healthand community workers, the localpopulation, and the children themselves haveto be devised, promoted and facilitated.
Many of the determinants of risk in children’smicroenvironments lie beyond the control ofthe local community. Policies and strategieswill be advocated and promoted to addressthe larger socioeconomic and political factorscontributing to contamination anddeterioration of the environment andimpeding progress towards a resolution ofthese problems.
18 ◆

Healthy Environment for Children
Health hazards in the home and thecommunity
Indoor air pollution from cooking andheating (notably using wood, coal andcharcoal) and inadequate ventilation are themajor hazards in the family home in ruralareas of developing countries. Tobacco smokeis a significant indoor contaminant in manyplaces. Lack of clean water is another majorhazard and the further the source of waterfrom the home, the greater the risk to health.Contamination of food and poisoning fromhousehold products is difficult to avoid incramped and ill-equipped homes or shelters.Overcrowding exacerbates sources ofinfection. Houses may provide inadequateshelter; they may be too cold, too hot,inadequately lit and damp. Dangeroussubstances in building materials, such as leador asbestos, pose additional problems, as dovarious building standards, for example unsafeelectrical wiring.
Settings in the community include the school,the street, the playground, the workplace(farming, commerce, industry, the informalsector, “cottage industries”), industrial sites,waste dumps, and the interior of vehiclesduring transport and in rural areas, the homeand the surrounding fields.
The school environment shares some of thesame problems as the home. The physicalschool environment includes the schoolbuilding and all its contents (includingphysical structures, infrastructure, furniture,and the use and presence of chemicals andbiological agents), the site on which a schoolis located, and the surrounding environmentincluding air, water, nearby land uses,roadways and other hazards, as well asmaterials that children may come into contactwith. Provision of safe water, sanitation andshelter are basic necessities for a healthyphysical learning environment. Equallyimportant is protection from biological,
physical (e.g. noise) and chemical risks thatcan threaten children’s health. Hazardsincluding infectious diseases transmittedthrough water, and physical risks associatedwith poor construction and maintenancepractices are examples of risks children faceat school throughout the world.
The safety of outdoor air in the communitydepends on proximity to the pollutingindustry, power plants, and areas of hightraffic load. Inside cars and buses, and in thestreet, especially in urban areas, children areexposed to high levels of the classiccontaminants associated with motor vehicleexhaust. Millions of street children in theworld live, work, sleep and breathe in thestreet 24 hours a day, and are particularlyvulnerable to multiple potentially fatal hazardsincluding abuse, unintentional injury andviolence.
In the workplace, children’s exposure may notbe very different from adults but children areless experienced, less aware and less able toask for or comply with safety regulations.They are also more vulnerable to adversehealth effects, such as musculo-skeletal traumaand stress, as well as to exposures to toxicchemicals. In rural areas, children work in thefields without any protection even whenpesticide spraying is going on all around andabove them.
Children often play near dumps, landfills, andillegal discharges and may be exposed todangerous levels of toxic substances. Theground itself (including the floor of houses)is also a source of chemical and biologicalcontaminants such as pesticide residues andlead if near heavy traffic.
◆ 19

Initiating an Alliance for Action
Components of healthy environments for children
Provision of basic necessities ■ Shelter■ Warmth■ Water■ Food■ Light■ Ventilation■ Sanitary facilities■ Emergency medical care
Protection from biological threats ■ Moulds■ Water-borne pathogens■ Food-borne pathogens■ Vector-borne diseases■ Venomous animals■ Rodents & hazardous insects
Protection from physical threats ■ Traffic and noise■ Violence and crime■ Injuries and accidents■ Radiation■ Heat and dust
Protection from chemical threats ■ Air pollution■ Water pollution■ Pesticides and other chemicals■ Hazardous waste■ Hazardous materials and finishes■ Cleaning agents■ Second-hand tobacco smoke
Who can do what in the community?
Many health hazards are common to allsettings and appropriate interventions willtake this into account. However, problems ineach setting may best be tackled by a specificset of actors. There is a need to identify andsupport solutions, which build on the capacityof community members, local resources andvested interests.
Typical patterns of risk and the most frequent,by resulting health hazards, can be identifiedso that efforts can be devoted most efficientlyto priority problems. Teachers, parents, healthand social workers, local organizations and,
in some cases, older children can all contributeto an initial assessment which is thecommunity’s first task.
Core messages, key targets, and priority actioncan then be decided by local committees ofteachers, health workers and local communityleaders (such as religious leaders, villagecouncils, and civilian groups). Simplemeasures requiring materials and equipment,which can be made locally, can be undertakenthrough collective community effort, withfinancial and technical support from localmunicipal or national authorities whenrequired. Such an initiative could be thecreation of smoke-free public spaces and
20 ◆
Healthy Environment for Children
schools. Next comes the identification andadaptation of appropriate technologies andfacilitatory mechanisms to support action(financially and technically), which is locallycontrolled and implemented.
A key protective factor in the home is parental(usually maternal) presence. Given theirmultiple responsibilities, poor women areunlikely to be able to devote much time towatching their children. Fuel and watersources close to the home to reduce the hoursspent in these survival activities are essential.Basic education in simple and cheap hygieneand nutrition (handwashing, breastfeeding)and prevention of unintentional injuries cansignificantly reduce risks. Simple appropriatetechnologies such as fuel-efficient, closedstoves are urgently needed.
Teachers play a major role in education onprevention and protection; older children andyoung people who are particularly effectivein conveying essential messages and providingexamples to young children can assist themin this task. Community groups, coordinatedby local health workers, can also provideinformation and simple training to groups ofadults. This requires finding or designingclear, simple educational materials and basicprotection messages to be integrated intoschool curricula. Targeted mass mediaprogrammes, such as radio and TVcampaigns, could effectively support thisprocess.
5. MECHANISMS FOR IMPLEMENTATION
The key to implementing a programmeon Healthy Environments forChildren will be the creation of a
concerted, popular, participatory andinclusive “movement”, which addresses theissue in an integrated manner, centring on thechildren rather than on individualenvironmental hazards. The basic principleon which the movement builds is that thestakeholders at every level can make adifference e.g. decision-makers atinternational, regional, national andcommunity levels, community leaders,teachers, NGOs, the private sector andfamilies. Besides the health sector, themovement must involve various other sectors,including environment, energy, transport,housing, agriculture and education. Actionneeds to be based on scientific evidence toensure that the major environmentaldeterminants of adverse health outcomes inchildren are adequately addressed, and thatthe most appropriate interventions are
considered. It needs to be driven by a strongcommitment to act primarily at the local andnational level.
While working towards achieving theMillennium Development Goals and theirspecific targets, the movement needs to gofurther than only reducing child mortality byaiming at combating morbidity andimproving the quality of life of children. Indeveloping strategies for action, the principleof subsidiarity should prevail i.e. actionsshould be taken at the lowest appropriatelevel, and as near as possible to the respectivetarget group. Decisions and actions that canmost effectively be taken at the local levelshould not be taken at the national level orhigher. As a first step, specific, ambitious butachievable targets for action with clearlyidentified responsibilities, and traceablemilestones must be established at the local,national, and international level. Mechanismsneed to be put in place to ensure the provision
◆ 21

Initiating an Alliance for Action
of technical, financial and other supportrequired in countries to implement nationalinitiatives through integrated, intersectoralmechanisms and building nationalpartnerships for action.
The major elements of the implementationstrategy are envisaged to be:
■ Taking stock of ongoing efforts. A majorpreliminary step is to evaluate workcurrently underway. This requires thecollection of information on ongoingefforts that are targeting children in thefield of health and environment at alllevels, with an emphasis on internationaland major national efforts, and thepreparation of an inventory highlightingthe need for action and the potential forcooperation and synergies.
■ Creating a popular movement. Healthyenvironments for children will onlybecome a reality if all the potential playersfeel that they can make a difference fromtheir respective angle. Takingresponsibility for action with theknowledge that everyone can make adifference will ensure the success of theinitiative. The movement needs toencompass all children, rich and poor,living in rural and urban communities,both in developing and in industrializedcountries.
■ Consolidating and disseminatingscientific knowledge. Action to be takenmust be evidence-based. The collection,evaluation and dissemination ofinformation on children’s health,environmental determinants, and theirlinkages, as well as on cost-effectiveinterventions and their efficacy constitutea first line of action. Use of generallyagreed, scientifically validated indicatorsis essential to measure progress. Finally,simple and easily accessible systems todisseminate this information need to beestablished.
■ Research and development. Evidence-based actions require an investment inresearch to supplement existingknowledge, in particular leading to animproved knowledge base on children’senvironmental health risk factors andtheir linkages, and to the developmentand evaluation of operationalinterventions and their cost-effectiveness.However, this investment into researchshould not delay immediate action onissues where adequate knowledge isalready available.
■ Influencing policies. Healthyenvironments for children should beplaced high on the public health agenda,and should be an integral part ofdevelopment policies. Children’s healthand the environment should be a drivingforce for multisectoral policies. Onesuccess story is that of lead removal oflead from gasoline, a transport policymeasure, was based on evidence of theadverse cognitive effects in exposedchildren, and resulted in improvedenvironmental conditions and childhealth. Efforts should be made to increaseawareness among high-level decision-makers of the importance of providingsafe and clean environments for children,and of promoting healthy behaviours inorder to ensure children’s growth,development and good health.
■ The healthy settings approach. Integratedapproaches are the key to creating healthyenvironments for children. The conceptof healthy schools, healthy homes, andhealthy communities provides anappropriate mechanism to implementsuch approaches. It covers thedissemination of information about, andthe promotion of, cost-effective,economically sustainable and culturallyappropriate interventions for improvingthe quality of the children’s homes andschools, and community environments.This includes education and awareness-
22 ◆

Healthy Environment for Children
building, provision of basic necessities inthe respective setting, and ensuringprotection from biological, physical andchemical risk factors. In the case ofcommunities, the healthy settingsapproach allows the mobilization ofcommunity leaders to champion thenecessary actions, and the creation ofmechanisms for participatory action byvarious community groups.
■ Support to the health sector. Raising theawareness of health professionals aboutenvironmental risk factors in children andtheir linkage to adverse health outcomes,whether they occur during childhood orlater in life, is key. It requires thedevelopment of appropriate training andguidance materials for physicians, nurses,midwives, and other health professionals,and the inclusion of such material incurricula. Expanding monitoring,surveillance and response systems should
allow the detection and management ofpaediatric disease outbreaks ofenvironmental etiology. Specific healthsector interventions need to be developedand evaluated, building on existingservices and networks, and making betteruse of available interventions and tools.
■ Intersectoral cooperation. Multi-sectoral,integrated approaches are required.Interventions through appropriatesectors, other than the health sector, canin many instances better ensure thatpreventive actions are taken through cost-effective interventions. Sectors to beinvolved include environment, transport,agriculture, housing, energy, and others.Sound agricultural policies, for example,could result in a reduction of children’sexposure to pesticides. The educationsector is key here, since knowledge is oneof the most effective tools to avoidunhealthy environments and behaviours.
6. MONITORING CHILDREN’SENVIRONMENTAL HEALTH
Children’s health and wellbeing arestrongly affected by environmentalproblems, but too little is known
about how much of the burden of diseasecaused by environmental problems falls onchildren. A programme of independentauditing and monitoring of progress inimproving the health status of children inrelation to their environment has to beestablished at the national and internationallevel. Several recent international declarations,including the G8 Ministerial Statement onthe World Summit on SustainableDevelopment (2002), highlighted the needfor more information and called for action todevelop children’s environmental healthindicators.
These indicators will not only guide policiesand action, and help governments to assessthe success of their programmes, but will alsospeak more forcefully for children than wordsalone. A project to launch an international,collaborative effort to develop, pilot-test andmonitor indicators will be initiated at theWorld Summit on Sustainable Developmentby the US Environmental Protection Agency,in cooperation with a variety of national andinternational partners. The initiative buildson ongoing efforts, such as the framework forchildren’s environmental health indicatorsdeveloped by WHO and the activities ofregional institutions in Europe and theAmericas.
◆ 23

Initiating an Alliance for Action
Home
Community
Ambientenvironment
Exposure-side indicators Health-side indicators
Preventiveactions
Remedialactions
Morbidity
Mortality
A s i m p l e m o d e l o fe n v i r o n m e n t a lh e a l t h i n d i c a t o r s
This recognizes three sets ofenvironment health indicators :those that represent exposuresto environmental hazards(`exposure-side´indicators),t h o s e t h a t r e p r e s e n thealth effects arising fromthese exposures (`health-side´indicators),and those thatrepresent the responses tothese risks (`action´indicators).
Action indicators
The Joint Monitoring Programme for WaterSupply and Sanitation (JMP), whichcombines WHO’s and UNICEF’s experienceand resources, may serve as a model systemfor monitoring children’s environmentalhealth. Since 1991, the JMP has regularlyreported on the status of the water supply andsanitation sector, and supports countries intheir monitoring efforts.
The estimation of the environmental burdenof disease at the national and local level willalso contribute directly to the monitoring ofchildren’s environmental health. Guidance forthis assessment is currently being prepared forten environmental risk factors. Futureassessments will directly reflect the diseaseburden borne by children and therebymonitor progress in reducing differentenvironmental health problems over time.
7. BUILDING A GLOBAL ALLIANCE
Why a Global Alliance?
The diversity of challenges and playersinvolved in addressing children’senvironmental health indicates that no singleentity – be it a government or WHO – cantackle the problems alone. Rather, a broad-based alliance is needed that draws on theunique and complementary strengths ofseveral government departments and sectors(at local and national level), consumer groupsand NGOs, the private sector, the UN familyas well as Foundations, and research andacademic groups. By working together, theywill more effectively address the gaps incapacity and the needs that exist in many
countries to develop and implement effectiveprogrammes and policies. Moreover, byworking together they will be able toaccomplish the tasks and objectives thatwould otherwise be unattainable or delayed.
An alliance can draw upon new andcompelling evidence of the effectiveness ofinterventions to tackle the various dimensionsof children’s environmental health, link thatknowledge to community action, andmobilize additional resources forimplementation. Further, a strong and multi-institutional alliance could advocate globallyfor increased resources to promote healthyenvironments for children, as well as for the
24 ◆

Healthy Environment for Children
use of effective tools. Acting together, thealliance members could provide aclearinghouse for information and research,which will be a basis for community andnational action.
The structure of the alliance will be criticalfor providing the political links, direction andform which will facilitate intersectoral actionand community participation. Experience inmany other areas of public health suggests thatfor the goals and objectives of the initiativeto be optimally met, a flexible structure willwork best. It needs to reflect global diversity,be able to endorse a selected number ofstrategic directions and actions, and remainopen to future partners who may wish to joinover the months and years to come.
In each area of environmental risks describedabove, many players are already active. It iscrucial to acknowledge past and ongoingwork, and to highlight the potential value thatwill be added as alliance members are drawninto scaled-up, and more globally orientedactions. The alliance’s success, however, willnot be limited to its ability to address each ofthe issues separately, but rather by the way inwhich, through acting together, bettersolutions will be found for addressingchildren’s health issues and environmental riskfactors in a more effective and synergistic way.
The sharing of information, expertise andefforts will result in the following importantbenefits: firstly, increasing the effectiveness ofinterventions; secondly, expanding the reachof limited resources; and thirdly, stimulatinggovernments and others to act in a collective,coherent approach. The alliance is expectedto make a measurable difference to theattainment of its objectives within a 3 to 5year framework.
Local, community-based approaches areessential to support the sustainability ofinterventions. Local movements will requirenot only political backing from national
governments and the close involvement ofcommunities and civil society, but also thesupport and guidance of an internationalalliance.
Global direction, advocacy and resourcemobilization are essential. However, nationalmovements are vital for creating and ensuringsafe and healthy environments for childrenand promoting hygienic behaviours. Nationalmovements will catalyse the efforts of differentstakeholders, coordinate actions, andstrengthen networks. They will help identifythe main environmental risks and preparelocal strategies for informing theircommunities, and for promoting educationand research on environmental health issues.They will ensure that global ideas aretranslated into local reality.
Developing the Global Alliance
The first activities for developing the allianceare adequate planning and agreements on howto operate. The Alliance should aim atbecoming fully functional by early 2003. Thetasks to be accomplished are likely to include:
■ An event to mark the founding of thealliance, and to give an indication ofpriority areas for future action.
■ Initial alliance members at the global andnational levels will be identified throughwidely published “calls to action”.Identification of appropriate alliancemembers is a critical step as it determinesthe legitimacy of the initiative and theability to develop new insights, ideas andapproaches, and to establish consensus.Alliance members should beinterdependent in reaching solutions toidentified problems and issues.
■ A small interim stakeholder group willbe set up (to be broadened with time),whose first task will be to convene a series
◆ 25

Initiating an Alliance for Action
of consultative and “brainstorming”meetings to help further define the keyobjectives, functions and outcomes of thealliance, and to steer the alliance in theagreed direction.
■ A communication and advocacy strategywill be developed which will focus onmobilizing additional financial resourcesand encouraging key decision-makers tosupport the planned actions.
■ In this process, the specific contributionof each alliance member in the initiativewill be identified and agreed upon.
■ Task Forces to tackle specific issues anddevelop draft plans of action will be setup. They will, for example, identifyoperational research priorities, or selectspecific issues and work areas like water
and sanitation, indoor air pollution,chemical hazards, injuries, and diseasevectors. This will help to focus theinterests and energies of the diversegroups.
■ Continuous review of ongoing orplanned activities of the different alliancemembers will help determine emergingopportunities for future collaboration.
■ As this work progresses, the alliancefounders will announce sets of time-bound objectives attainable within thenewly created resource and political basefor the Healthy Environments forChildren initiative, and action plans forimplementation will rapidly be put inplace.
26 ◆

Healthy Environment for Children
ANNEX
THE BANGKOK STATEMENTA pledge to promote the protection of Children’s Environmental Health
We, the undersigned scientists, doctors and public health professionals, educators,environmental health engineers, community workers and representatives from a number
of international organizations, from governmental and nongovernmental organizations in South-East Asian and Western Pacific countries, have come together with colleagues from differentparts of the world from 3 to 7 March 2002 in Bangkok, Thailand, to commit ourselves to workjointly towards the promotion and protection of children’s health against environmental threats.
Worldwide, it is estimated that more than one-quarter of the global burden of disease (GBD)can be attributed to environmental risk factors. Over 40% of the environmental disease burdenfalls on children under 5 years of age, yet these constitute only 10% of the world population.The environmental burden of paediatric disease in Asia and the Pacific countries is not wellrecognized and needs to be quantified and addressed.
We recognize:
That a growing number of diseases in children have been linked to environmental exposures.These range from the traditional waterborne, foodborne and vector-borne diseases and acuterespiratory infections to asthma, cancer, injuries, arsenicosis, fluorosis, certain birth defects anddevelopmental disabilities.
That environmental exposures are increasing in many countries in the region; that new emergingrisks are being identified; and that more and more children are being exposed to unsafeenvironments where they are conceived and born, where they live, learn, play, work and grow.Unique and permanent adverse health effects can occur when the embryo, fetus, newborn,child and adolescent (collectively referred to as “children” from here onwards) are exposed toenvironmental threats during early periods of special vulnerability.
That in developing countries the main environmental health problems affecting children areexacerbated by poverty, illiteracy and malnutrition, and include: indoor and outdoor air pollution,lack of access to safe water and sanitation, exposure to hazardous chemicals, accidents andinjuries. Furthermore, as countries industrialize, children become exposed to toxicants commonlyassociated with the developed world, creating an additional environmental burden of disease.This deserves special attention from the industrialized and developing countries alike.
◆ 27

Initiating an Alliance for Action
That environmental hazards arise both from anthropogenic and natural sources (e.g. planttoxins, fluoride, arsenic, radiations), which separately and in combination can cause seriousharm to children.
That restoring and protecting the integrity of the life-sustaining systems of the earth are integralto ensuring children’s environmental health now and in the future. Therefore, addressing globalchanges such as human population growth, land and energy use patterns, habitat destruction,biodiversity loss and climate change must be part of efforts to promote children’s environmentalhealth.
That despite the rising concern of the scientific community and the education and social sectorsabout environmental threats to children’s health and development, progress has been slow andserious challenges still remain.
That the health, environment and education sectors must take concerted action at all levels(local, national, global), together with other sectors, in serious efforts to enable our countries toassess the nature and magnitude of the problem, identify the main environmental risks tochildren’s health and establish culturally appropriate monitoring, mitigation and preventionstrategies.
We affirm:
That the principle “children are not little adults” requires full recognition and a preventiveapproach. Children are uniquely vulnerable to the effects of many chemical, biological andphysical agents. All children should be protected from injury, poisoning and hazards in thedifferent environments where they are born, live, learn, play, develop and grow to become theadults of tomorrow and citizens in their own right.
That all children should have the right to safe, clean and supportive environments that ensuretheir survival, growth, development, healthy life and well-being. The recognition of this right isespecially important as the world moves towards the adoption of sustainable developmentpractices.
That it is the responsibility of community workers, local and national authorities and policy-makers, national and international organizations, and all professionals dealing with health,environment and education issues to ensure that actions are initiated, developed and sustainedin all countries to promote the recognition, assessment and mitigation of physical, chemicaland biological hazards, and also of social hazards that threaten children’s health and quality oflife.
28 ◆

Healthy Environment for Children
We commit ourselves:
To developing active and innovative national and international networks with colleagues, inpartnership with governmental, nongovernmental and international organizations for thepromotion and protection of children’s environmental health, and urge WHO to support ourefforts in all areas, especially in the following four:
PROTECTION AND PREVENTION – To strengthen existing programmes and initiatenew mechanisms to provide all children with access to clean water and air, adequate sanitation,safe food and appropriate shelter:
■ Reduce or eliminate environmental causes and triggers of respiratory diseases and asthma ,including exposure to indoor air pollution from the use of biomass fuels and environmentaltobacco smoke.
■ Reduce or eliminate exposure to toxic metals such as lead, mercury and arsenic, to fluoride,and to anthropogenic hazards such as toxic wastes, pesticides and persistent organicpollutants.
■ Reduce or eliminate exposure to known and suspected anthropogenic carcinogens,neurotoxicants, developmental and reproductive toxicants, immunotoxicants and naturallyoccurring toxins.
■ Reduce the incidence of diarrhoeal disease through increased access to safe water andsanitation and promotion of initiatives to improve food safety.
■ Reduce the incidence of accidents, injuries and poisonings, as well as exposure to noise,radiation, microbiological and other factors by improving all environments where childrenspend time, in particular at home and at school.
■ Commit to international efforts to avert or slow global environmental changes, and alsotake action to lessen the vulnerability of populations to the impact of such changes.
HEALTH CARE AND RESEARCH – To promote the recognition, assessment and study ofenvironmental factors that have an impact on the health and development of children:
■ Establish centres to address issues related to children’s environmental health.
■ Develop and implement cooperative multidisciplinary research studies in association withcentres of excellence, and promote the collection of harmonized data and their dissemination.
■ Incorporate children’s environmental health into the training for health care providers andother professionals, and promote the use of the environmental history.
■ Seek financial and institutional support for research, data collection, education, interventionand prevention programmes.
■ Develop risk assessment methods that take account of children as a special risk group.
◆ 29
Initiating an Alliance for Action
EMPOWERMENT AND EDUCATION – To promote the education of children and parentsabout the importance of their physical environment and their participation in decisions thataffect their lives, and to inform parents, teachers and caregivers and the community in generalon the need and means to provide a safe, healthy and supportive environment to all children:
■ Provide environmental health education through healthy schools and adult educationinitiatives.
■ Incorporate lessons on health and the environment into all school curricula
■ Empower children to identify potential risks and solutions.
■ Impart environmental health expertise to educators, curriculum designers and schooladministrators.
■ Create and disseminate to families and communities culturally relevant information aboutthe special vulnerability of children to environmental threats and practical steps to protectchildren.
■ Teach families and the community to identify environmental threats to their children, toadopt practices that will reduce risks of exposure and to work with local authorities and theprivate sector in developing prevention and intervention programmes.
ADVOCACY – To advocate and take action on the protection and promotion of children’senvironmental health at all levels, including political, administrative and community levels:
■ Use lessons learned to prevent environmental illness in children, for example by promotinglegislation for the removal of lead from all gasoline, paints, water pipes and ceramics, andfor the provision of smoke-free environments in all public buildings.
■ Sensitize decision-makers to the results of research studies and observations of communityworkers and primary health care providers that need to be accorded high priority to safeguardchildren’s health.
■ Promote environmental health policies that protect children.
■ Raise the awareness of decision-makers and potential donors about known environmentalthreats to children’s health and work with them and other stakeholders to allocate necessaryresources to implement interventions.
■ Work with the media to disseminate information on core children’s environmental healthissues and locally relevant environmental health problems and potential solutions.
For all those concerned about the environmental health of children, the time to translateknowledge into action is now.
Bangkok, 7 March 2002
30 ◆





























