Embed Size (px)
Citation preview

Inhibition of Ninjurin 1 restores erectile functionthrough dual angiogenic and neurotrophic effects inthe diabetic mouseGuo Nan Yina,b, Min Ji Choia,b, Woo Jean Kima,b, Mi-Hye Kwona,b, Kang-Moon Songa,b, Jin-Mi Parka,b, Nando Dulal Dasa,b,Ki-Dong Kwona,b, Dulguun Batbolda,b, Goo Taeg Ohc, Gou Young Kohd,e, Kyu-Won Kimf,g, Ji-Kan Ryua,b,1,and Jun-Kyu Suha,b,1
aNational Research Center for Sexual Medicine and bDepartment of Urology, Inha University School of Medicine, Incheon 400-711, Korea; cDivision of Lifeand Pharmaceutical Sciences, Ewha Womans University, Seoul 120-750, Korea; dNational Research Laboratory of Vascular Biology and Stem Cells andeGraduate School of Medical Science and Engineering, Korea Advanced Institute of Science and Technology, Daejeon 305-701, Korea; and fNeurovascularCoordination Research Center, College of Pharmacy and gResearch Institute of Pharmaceutical Sciences, Seoul National University, Seoul 151-742, Korea
Edited by David W. Russell, University of Texas Southwestern Medical Center, Dallas, TX, and approved May 20, 2014 (received for review February 24, 2014)
Penile erection is a neurovascular phenomenon, and erectile dys-function (ED) is caused mainly by vascular risk factors or diseases,neurologic abnormalities, and hormonal disturbances. Men withdiabetic ED often have severe endothelial dysfunction and pe-ripheral nerve damage, which result in poor response to oralphosphodiesterase-5 inhibitors. Nerve injury-induced protein 1(Ninjurin 1, Ninj1) is known to be involved in neuroinflammatoryprocesses and to be related to vascular regression during the em-bryonic period. Here, we demonstrate in streptozotocin-induceddiabetic mice that inhibition of the Ninj1 pathway by administeringNinj1-neutralizing antibody (Ninj1-Ab) or by using Ninj1-knockoutmice successfully restored erectile function through enhanced penileangiogenesis and neural regeneration. Angiopoietin-1 (Ang1) ex-pression was down-regulated and angiopoietin-2 expression wasup-regulated in the diabetic penis compared with that in controls,and these changes were reversed by treatment with Ninj1-Ab.Ninj1 blockade-mediated penile angiogenesis and neural regenera-tion as well as recovery of erectile function were abolished byinhibition of Ang1–Tie2 (tyrosine kinase with Ig and epidermalgrowth factor homology domain-2) signaling with soluble Tie2antibody or Ang1 siRNA. The present results suggest that inhi-bition of the Ninj1 pathway will be a novel therapeutic strategyfor treating ED.
diabetes mellitus | male sexual dysfunction | peripheral neuropathy
Erectile dysfunction (ED), which is defined as an inability toattain or maintain penile erection sufficient for satisfactory
sexual intercourse (1), is caused by a variety of pathologic con-ditions including vascular risk factors or diseases, neurologicabnormalities, and hormonal disturbances (2, 3). Diabetes mel-litus is one of the most common causes of ED, and about 50–75% of male diabetic patients have ED (4, 5). Multiple patho-genetic factors, such as endothelial dysfunction, atherosclerosis,autonomic neuropathy, inflammation, fibrosis, and hypogonad-ism, are involved in diabetic ED (4–6). The multiple factorscausing diabetic ED contribute to reduced responsiveness tocurrently available oral phosphodiesterase-5 (PDE5) inhibitors,which enhance the nitric oxide (NO)–cGMP pathway by inhib-iting the breakdown of cGMP (7). The severity of endothelialdysfunction and peripheral neuropathy are mainly responsiblefor the poor responsiveness of diabetic patients to PDE5 inhib-itors (8, 9). Because the effects of PDE5 inhibitors depend onendogenous NO formation, PDE5 inhibitors fail to increase thecGMP level above the threshold required for penile erection ifbioavailable NO is insufficient as the result of severe endothelialdysfunction or peripheral neuropathy (9). Therefore, a new treat-ment strategy that corrects both endothelial dysfunction and pe-ripheral neuropathy is required for men with diabetic ED.
A variety of strategies targeting therapeutic angiogenesis andneural regeneration have been introduced to restore erectilefunction at the preclinical level. Angiopoietins, the ligands fortyrosine kinase with Ig and epidermal growth factor homologydomain-2 (Tie2, also called Tek), are a family of angiogenicgrowth factors that play a crucial role in blood vessel remodeling,maturation, and stabilization (10–12). We recently reported inmouse models of type I and type II diabetic ED that local de-livery of synthetic angiopoietin-1 (Ang1) or angiopoietin-4 pro-tein into the penis restores erectile function by enhancingendothelial cell regeneration (13–15). Bennett et al. (16) dem-onstrated in a rat model of type I diabetic ED that replication-defective herpes simplex virus vector encoding neurotrophin-3(NT3) gene induces partial recovery of erectile function by re-storing penile neuronal nitric oxide synthase-positive (nNOS+)neurons (16). However, a treatment strategy targeting both en-dothelial and neural regeneration in diabetic ED has not yetbeen explored.Nerve injury-induced protein 1, or Ninjurin-1 (Ninj1), is a cell-
surface protein and an adhesion molecule. Ninj1 was discoveredduring the identification of molecules related to nerve injuryand is known to be up-regulated in neuronal and Schwann cellsafter sciatic nerve injury (17). It also was reported that Ninj1 is
Significance
Curative treatment modalities for erectile dysfunction (ED) arenot available. Penile erection is a neurovascular phenomenon,and ED is caused mainly by vascular and neurologic disturbances.Here we demonstrate that inhibition of nerve injury-inducedprotein 1 promotes penile angiogenesis and neural regenerationthrough angiopoietin-1–Tie2 signaling and rescues erectile func-tion in diabetic mice. Our preclinical work shed light on the ap-plication of therapeutic angiogenesis and neural regeneration forthe treatment of human ED.
Author contributions: G.N.Y., G.Y.K., K.-W.K., J.-K.R., and J.-K.S. designed research; G.N.Y.,M.J.C., W.J.K., M.-H.K., K.-M.S., J.-M.P., N.D.D., K.-D.K., and D.B. performed research;G.N.Y. and G.T.O. contributed new reagents/analytic tools; G.N.Y., M.J.C., W.J.K., M.-H.K.,K.-M.S., J.-M.P., N.D.D., K.-D.K., and D.B. analyzed data; G.N.Y., J.-K.R., and J.-K.S. wrotethe paper; G.T.O. generated Ninj1-KO mice; K.-W.K. contributed Ninj1 antibody; J.-K.R.and J.-K.S. organized the project; and G.Y.K., K.-W.K., J.-K.R., and J.-K.S. supervisedthe project.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission.
Data deposition: cDNA microarray data have been deposited in the Gene ExpressionOmnibus database, www.ncbi.nlm.nih.gov/geo (accession no. GSE57525).1To whom correspondence may be addressed. E-mail: [email protected] or [email protected].
This article contains supporting information online at www.pnas.org/lookup/suppl/doi:10.1073/pnas.1403471111/-/DCSupplemental.
www.pnas.org/cgi/doi/10.1073/pnas.1403471111 PNAS | Published online June 16, 2014 | E2731–E2740
MED
ICALSC
IENCE
SPN
ASPL
US
Dow
nloa
ded
by g
uest
on
June
7, 2
020

responsible for the progression of multiple sclerosis, an autoim-mune inflammatory disease of the CNS characterized by de-myelination and axonal damage (18). The expression of Ninj1 issignificantly increased in CNS lesions of patients with multiplesclerosis, and Ninj1-neutralizing antibody suppresses neuro-inflammatory responses in an experimental model of allergicencephalomyelitis that mimics multiple sclerosis (18). Moreover,Ninj1 is known to induce the regression of hyaloid blood vessels,a transiently existing vascular system involved in maturation ofthe lens during the embryonic period, and inhibition of Ninj1with neutralizing antibody delays regression of the hyaloid bloodvessels (19). These findings suggest that Ninj1 has a functionalrole in the regulation of nervous and vascular systems. There-fore, inhibition of the Ninj1 pathway might be efficacious for thetreatment of diabetic ED, which is characterized by both endo-thelial dysfunction and peripheral neuropathy.Here, we studied the effectiveness of Ninj1-neutralizing anti-
body in promoting regeneration of penile endothelial and neu-ronal cells and restoration of erectile function in a mouse modelof diabetic ED. Our results show that a single injection of Ninj1-neutralizing antibody into the penis induced significant recoveryof erectile function in diabetic mice; this recovery was accom-panied by enhanced cavernous endothelial cell proliferation andsuccessive phosphorylation of Akt protein kinase B and endo-thelial nitric oxide synthase (eNOS), decreased production ofreactive oxygen species (ROS), decreased endothelial cell apo-ptosis, and restoration of penile nNOS+ through the secretion ofneurotrophic factors. The Ang1 expression was down-regulated,and the expression of angiopoietin-2 (Ang2), an endogenous an-tagonist of Ang1, was up-regulated in the diabetic penis comparedwith their expression in controls; this effect was reversed by treat-ment with Ninj1-neutralizing antibody. The endothelial and neuralregeneration as well as the recovery of erectile function mediatedby Ninj1 blockade were abolished by inhibition of Ang1–Tie2signaling with soluble Tie2 antibody (sTie2-Fc) or siRNA for Ang1.Ninj1-KO mice were resistant to diabetes-induced cavernousendothelial and neuronal cell damage, and erectile function wasrescued in these mice.
ResultsMetabolic Variables. The fasting and postprandial blood glucoseconcentrations were significantly higher in the diabetic mice thanin control mice. Also, body weight was significantly lower in thediabetic mice than in the controls. The body weight and bloodglucose levels of the diabetic mice did not differ significantlyregardless of the treatment given (SI Appendix, Tables S1–S4).
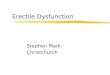
Increase in Ninj1 Expression in the Penis of Diabetic Mice and inMouse Cavernous Endothelial Cells Exposed to the High-GlucoseCondition. Immunofluorescent staining revealed that the expres-sion of Ninj1 protein was significantly higher in cavernous en-dothelial cells and in the dorsal nerve bundle of the diabetic miceby approximately three- or fourfold, respectively, than in controlmice (Fig. 1 A–D). The contents of endothelial cells and neu-rofilament were significantly lower in the penis of diabetic micethan in controls (Fig. 1 A–D). Western blot analysis also revealedincreased Ninj1 expression in the penis of diabetic mice both invivo and in primary cultured mouse cavernous endothelial cells(MCECs) exposed to the high-glucose condition in vitro (Fig. 1E–H). These findings gave us a rationale to use Ninj1 blockadefor the treatment of diabetic ED.
In Vivo Detection of Ninj1-Neutralizing Antibody in the Penis ofDiabetic Mice. To determine the distribution of exogenouslyinjected Ninj1-neutralizing antibody in the penis and to distin-guish it from endogenous Ninj1 expression, immunofluorescentstaining was done with TRITC-conjugated rabbit secondary an-tibody (Zymed Laboratories) at 1, 3, and 6 h after intracavernous
injection of rabbit polyclonal antibody against Ninj1 (2.5 μg/20 μL;provided by K.-W.K.) into the diabetic mice. Ninj1 antibody wasdetected in both the corpus cavernosum tissue and in the dorsalnerve bundle of the diabetic mice (SI Appendix, Fig. S1).
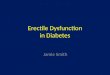
Ninj1-Neutralizing Antibody Restores Erectile Function in DiabeticMice. To determine the physiological relevance of intracavernousinjection of Ninj1-neutralizing antibody, we evaluated erectilefunction during electrical stimulation of the cavernous nerve invivo. A representative intracavernous tracing after stimulation ofthe cavernous nerve (5 V, 12 Hz, 1 ms) for 1 min in age-matchedcontrol and diabetic mice 2 and 4 wk after treatment is shownin Fig. 2 A and B. During electrical stimulation of the cavernousnerve, the ratios of maximal intracavernous pressure (ICP) andtotal ICP to mean systolic blood pressure (MSBP) were signifi-cantly lower in untreated and IgG-treated diabetic mice thanin age-matched controls. At 2 wk after treatment, a single intra-cavernous injection of high-dose Ninj1-neutralizing antibody(2.5 μg/20 μL) induced recovery of erection parameters, whichreached up to 90% (maximal ICP) or 96% (total ICP) ofcontrol values, whereas low-dose Ninj1-neutralizing antibody(1.0 μg/20 μL) partially restored erectile function (Fig. 2 C and D).At 4 wk after administration of high-dose Ninj1-neutralizingantibody (2.5 μg/20 μL), erectile function recovery was notas great as observed at 2 wk after treatment but still wassignificantly higher than in the untreated or IgG-treated di-abetic groups (Fig. 2 E and F). No detectable differences in
PECAM-1/ Ninj1A
Con
trol
DMNinj1β-actin
E
Peni
s
GNG HG
MC
EC
s
Ninj1β-actin
CNeurofilament/ Ninj1
DM
B*
0.00.51.01.52.02.53.03.5
Nin
j1(+
) are
a/C
aver
nosu
m
C DM
*0.00.20.40.60.81.01.2
End
othe
lial a
rea/
Cav
erno
sum
C DM
D
Nin
j1(+
)are
a/D
NB
012345 *
C DM0.00.20.40.60.81.01.2
*
NF
(+) a
rea/
DN
B
C DM
Rel
ativ
e ra
tio
(Nin
j1 / β-
actin
)F*
0.00.51.01.52.02.5
C DM
H*
NG HG
Rel
ativ
e ra
tio
(Nin
j1 / β-
actin
)
0.00.51.01.52.02.5
C
Fig. 1. Increase in Ninj1 expression in the diabetic condition. (A) PECAM-1(green) and Ninj1 (red) immunostaining in penis tissue from age-matchedcontrol (C) and diabetic (DM) mice. (Scale bar: 100 μm.) (B) The Ninj1-immunopositive area or endothelial cell content in cavernous tissue wasquantified by ImageJ (n = 6). *P < 0.001 vs. control group. (C) Neurofilament(green) and Ninj1 (red) immunostaining in each group. Nuclei were labeledwith DAPI (blue). (Scale bar: 25 μm.) (D) The Ninj1-immunopositive area orneurofilament content in the dorsal nerve bundle was quantified by ImageJ(n = 6). *P < 0.001 vs. control group. (E) Representative Western blots forNinj1 in mouse penis. (F) Normalized band intensity values (n = 4). *P < 0.001vs. control group. (G) Representative Western blot for Ninj1 in MCECs afterexposure to the normal-glucose (NG) or high-glucose (HG) condition for 48 h.(H) Normalized band intensity values (n = 4). *P < 0.001 vs. NG group (Mann–Whitney u test). Data are mean ± SE. The relative ratio of control or NGgroup was arbitrarily set equivalent to 1. DNB, dorsal nerve bundle; MCECs,mouse cavernous endothelial cells; NF, neurofilament.
E2732 | www.pnas.org/cgi/doi/10.1073/pnas.1403471111 Yin et al.
Dow
nloa
ded
by g
uest
on
June
7, 2
020

MSBP were found among the experimental groups (SI Appendix,Tables S1 and S2).
Ninj1-Neutralizing Antibody Induces Proliferation of CavernousEndothelial Cells in Diabetic Mice. Immunofluorescent staining ofcavernous tissue with an antibody to platelet/endothelial adhe-sion molecule 1 (PECAM-1) was performed in age-matchedcontrol and diabetic mice 2 wk after treatment. We found sig-nificantly lower cavernous endothelial cell contents in the un-treated and IgG-treated diabetic mice than in the control mice.Intracavernous injection of high-dose Ninj1-neutralizing anti-body (2.5 μg/20 μL) completely restored cavernous endothelialcell content (Fig. 3 A and B). To test whether the increase incavernous endothelial cell content was the result of endothelialcell proliferation, we assessed the number of endothelial cellsstaining positive for phosphohistone H3 (a nuclear protein in-dicative of cell proliferation). We noted significant increases inphosphohistone H3+ endothelial cells in diabetic mice 2 wk afterinjection of high-dose Ninj1-neutralizing antibody (2.5 μg/20 μL)(Fig. 3 A and C). Intracavernous injection of low-dose Ninj1-neutralizing antibody (1.0 μg/20 μL) also induced recovery ofendothelial content through endothelial cell proliferation but notat the level of the control group (Fig. 3 A–C).
Ninj1-Neutralizing Antibody Decreases Cavernous Endothelial CellApoptosis in Diabetic Mice. Double labeling of cavernous tissuewith antibodies to PECAM-1 and cleaved caspase-3 showed thatthe number of apoptotic cells in cavernous endothelial cells wassignificantly greater in the untreated and IgG-treated diabeticgroups than in the control group. Intracavernous injections of
both low-dose (1.0 μg/20 μL) and high-dose (2.5 μg/20 μL) Ninj1-neutralizing antibody decreased apoptosis in the cavernous en-dothelial cells of the diabetic mice significantly, to a level com-parable to that found in the age-matched controls (Fig. 3 Aand D).
Ninj1-Neutralizing Antibody Induces Cavernous Akt and eNOSPhosphorylation in Diabetic Mice. Western blot analysis showedthat the expression of cavernous phospho-Akt (Ser473) andphospho-eNOS (Ser1177) was significantly lower in the IgG-treated diabetic mice than in the age-matched controls. High-dose Ninj1-neutralizing antibody (2.5 μg/20 μL) significantly in-duced phosphorylation of Akt and eNOS in the diabetic mice ascompared with IgG-treated diabetic mice, but no significantdifference in total Akt and total eNOS expression was notedamong the four experimental groups (Fig. 3 E–G).
Ninj1 Regulates Expression of Ang1 and Ang2 in Diabetic Mice in Vivoand in MCECs in Vitro. Cavernous Ang1 protein expression wassignificantly lower and Ang2 protein expression was significantlyhigher in the IgG-treated diabetic mice than in the age-matchedcontrols. The expression of both Ang1 and Ang2 proteins returned
E
4 w
eeks
M
ax IC
P/M
SB
P
C NT
IgG2.5
**#
DM
0.0
0.40.2
0.60.81.0
2 w
eeks
M
ax IC
P/M
SB
P
C NT
IgG1.02.5
**#
N-AbDM
0.0
0.40.2
0.60.81.0
C
No treatment IgG 1.0 μgNinj1 Ab
STZ-induced diabetic mice
Control 2.5 μg120100
50
0
A
0 2 4 0 2 4 0 2 4 0 2 4 0 2 4(Minutes)
2 w
eeks
ICP
(c
m H
2O)
No treatment IgG Ninj1 Ab 2.5 μgSTZ-induced diabetic mice
ControlB
0 2 4 0 2 40 2 4 0 2 4
130
100
50
0(Minutes)
4 w
eeks
ICP
(c
m H
2O)
**#
0
2010
304050
D
2 w
eeks
Tot
al
ICP/
MS
BP(
AU
C) F
**#
0
2010
30405060
4 w
eeks
Tot
al
ICP
/MS
BP
(AU
C)
C NT
IgG1.02.5
N-AbDM
C NT
IgG2.5
DM
Fig. 2. Ninj1-neutralizing antibody restores erectile function. (A and B)Representative ICP responses for the age-matched control (C), untreateddiabetic mice, or diabetic mice stimulated at 2 wk (A) or 4 wk (B) aftera single intracavernous injection of IgG (2.5 μg) or Ninj1-neutralizing anti-body (Ninj1 Ab, 1.0 μg or 2.5 μg). The cavernous nerve was stimulated at 5 V.The stimulus interval is indicated by a solid bar. (C and D) Ratios of meanmaximal ICP and total ICP (area under the curve) to MSBP at 2 wk aftertreatment (n = 8). *P < 0.01 vs. control and Ninj1 antibody (2.5 μg) groups;#P < 0.01 vs. NT and IgG groups. (E and F) Ratios of mean maximal ICP and totalICP (area under the curve) to MSBP at 4 wk after treatment (n = 6). *P < 0.01vs. control and Ninj1 antibody (2.5 μg) groups; #P < 0.01 vs. NT and IgGgroups. P values were determined by one-way ANOVA. Data are mean ± SE.AUC, area under curve; DM, diabetes mellitus; N-Ab, Ninj1 Ab; NT, notreatment; STZ, streptozotocin.
PE
CA
M-1
Mer
ged
Cle
aved
casp
ase-
3A
PH
3M
erge
dP
EC
AM
-1
Control NT IgG 2.5 μg
STZ-induced diabetic mice
1.0 μg
PE
CA
M-1
Ep-AKT
AKT
p-eNOSeNOS
β-actin
C IgG 1.0 2.5Ninj1 AbDM
05
10152025
B
End
othe
lial a
rea/
Cav
erno
sum
(%)
**#
#†
Rel
ativ
e ra
tio
(p-A
kt/ A
kt)
*##
C IgG1.02.5
N-AbDM
0.00.20.40.60.81.01.2F
No.
PH
3(+
)EC
s/H
PF
02468
10121416
**
# #
C
C NT
IgG1.02.5
N-AbDM
No.
C-c
aspa
se-3
(+)E
Cs/
HP
F **# #
05
1015202530
D
C NT
IgG1.02.5
N-AbDM
*
#†
Rel
ativ
e ra
tio
(p-e
NO
S/ e
NO
S) G
0.00.20.40.60.81.01.2
Ninj1 Ab
C IgG1.02.5
N-AbDM
C NT
IgG1.02.5
N-AbDM
Fig. 3. Ninj1-neutralizing antibody restores cavernous endothelial content.(A) PECAM-1 (green) and phosphohistone H3 (PH3; red) or PECAM-1 (red)and cleaved caspase-3 (green) immunostaining in penis tissue from age-matched control (C), untreated diabetic mice (NT), or diabetic mice 2 wkafter receiving a single intracavernous injection of IgG (2.5 μg) or Ninj1-neutralizing antibody (Ninj1 Ab, 1.0 μg or 2.5 μg). Nuclei were labeled withDAPI (blue). (Scale bars: Top Row, 100 μm; Middle Row, 25 μm; Bottom Row,50 μm) (B) Quantification of cavernous endothelial cell content by ImageJ(n = 6). (C) Number of PH3-immunopositive endothelial cells per high-powerfield (n = 6). (D) Number of apoptotic cells in endothelium per high-powerfield (n = 6). In B–D, *P < 0.001 vs. C, Ninj1 antibody (1.0 μg), and Ninj1antibody (2.5 μg) groups; #P < 0.001 vs. N and IgG groups; †P < 0.05 vs. Ninj1antibody (1.0 μg) group. (E) Representative Western blots for phospho-Akt(p-Akt)/Akt and phospho-eNOS (p-eNOS)/eNOS at 2 wk after treatment.(F and G) Normalized band intensity values for p-Akt/Akt (n = 4) (F) andp-eNOS/eNOS (G). *P < 0.001 vs. C, Ninj1 antibody (1.0 μg), and Ninj1 anti-body (2.5 μg) groups; #P < 0.001 vs. IgG group; †P < 0.001 vs. Ninj1 antibody(1.0 μg) group. The P values were determined by one-way ANOVA. Data aremean ± SE. C-caspase-3, cleaved caspase-3; DM, diabetes mellitus; ECs, en-dothelial cells; N-Ab, Ninj1 Ab; STZ, streptozotocin.
Yin et al. PNAS | Published online June 16, 2014 | E2733
MED
ICALSC
IENCE
SPN
ASPL
US
Dow
nloa
ded
by g
uest
on
June
7, 2
020

to control values after treatment with Ninj1-neutralizing antibody(Fig. 4 A and B). To confirm further that Ninj1 is involved in theregulation of Ang1 and Ang2, the MCECs were treated with Ninj1siRNA or plasmid encoding the Ninj1 gene. Knockdown of theNinj1 gene with siRNA increased Ang1 mRNA expression anddecreased Ang2 mRNA expression, whereas overexpression ofthe Ninj1 gene decreased Ang1 mRNA and increased Ang2mRNA expression (Fig. 4 C and D).
Cavernous Angiogenesis and Recovery of Erectile Function by Ninj1-Neutralizing Antibody Are Dependent on the Ang1–Tie2 SignalingPathway. We determined whether the Ang1–Tie2 signaling path-way participated in the cavernous angiogenesis induced byNinj1-neutralizing antibody and subsequent restoration of the
erectile responses in diabetic mice treated with sTie2-Fc (4 μg/20 μL).Immunofluorescent staining of cavernous tissue with an anti-body to PECAM-1 was performed in age-matched controland diabetic mice 2 wk after treatment. Enhancement of cav-ernous angiogenesis by Ninj1-neutralizing antibody was pro-foundly diminished in diabetic mice treated with sTie2-Fc (Fig. 4E and F). A BrdU incorporation assay and cleaved caspase-3analysis revealed that the increase in endothelial cell pro-liferation and decrease in endothelial cell apoptosis mediatedby Ninj1-neutralizing antibody also was significantly attenuatedin diabetic mice treated with sTie2-Fc (SI Appendix, Fig. S2).Moreover, physiologic erection studies revealed that erectilefunction was not recovered after administration of Ninj1-neu-tralizing antibody in diabetic mice treated with sTie2-Fc (Fig. 4
Ang2
Ninj1Ang1
GAPDH
RT-PC
R
SC siC Mo MyA
C IgG 1.0 2.5Ninj1 AbDM
WB
β-actin
Ang1Ang2
PEC
AM-1
EControl IgG Fc
Ninj1 AbsTie-2 (+)
STZ-induced diabetic mice
sTie-2 (-)
L
PH3
/ DAP
IM
agni
ficat
ion
J Normal glucose ScrambledsiNinj1
siAng1 (+)
High glucose
siAng1 (-)
0.00.20.40.60.81.0
* *#
Max
IC
P/M
SBP
†HE
ndot
heliu
m/
Cav
erno
sum
(%)F
05
10152025 #
†
**
I
Tota
l IC
P(A
UC
)
01020304050
* *#
†
IgGFc sTie-2(-)sTie-2(+)
C
Num
ber o
f tu
bes/
Fiel
d
K
01020304050
*
#†
Perc
ento
f PH
3(+
)EC
s/H
PF
M
0.00.20.40.60.81.0
*
#
†
HGsiNinj1
NG SC siAng1(+)
siAng1(-)
0 2 40
50
100120
2 w
eeks
ICP
(cm
H2O
)
G
0 2 4 0 2 4 0 2 4 0 2 4(Minutes)
BR
elat
ive
ratio
(Ang
1/ β
-act
in)
0.00.20.40.60.81.01.2
*#
#
DM
C IgG1.02.5
N-AbR
elat
ive
ratio
(Ang
2/ β
-act
in)
0.00.51.01.52.02.53.0 *
##
DM
C IgG1.02.5
N-Ab
Rel
ativ
e ra
tio D
SCsi M
oM
y
Ang1 Ang2
** *
*
0.00.51.01.52.02.53.0
SCsi M
oM
y
N-AbDM
Fig. 4. Ninj1-neutralizing antibody–induced cavernous angiogenesis and recovery of erectile function are dependent on the Ang1–Tie2 pathway. (A)Representative Western blots for Ang1 and Ang2 in penis tissue from age-matched control mice (C) or diabetic mice (DM) 2 wk after receiving a singleintracavernous injection of IgG (2.5 μg) or Ninj1-neutralizing antibody (Ninj1 Ab, 1.0 μg or 2.5 μg). (B) Normalized band intensity values (n = 4). *P < 0.05 vs. C,Ninj1 Ab (2.5 μg) groups; #P < 0.05 vs. IgG group (Kruskal–Wallis test). (C) Representative RT-PCR for Ninj1, Ang1, and Ang2 in MCECs transfected with Ninj1siRNA (si) or plasmid encoding Ninj1 gene (My). (D) Normalized band intensity values (n = 4). *P < 0.05 vs. scrambled siRNA (SC) and myc-tagged mock-treated(Mo) (Mann–Whitney u test). (E–I) PECAM-1 immunostaining (E) and quantification (F) and representative ICP responses (G–I) in each group at 2 wk aftertreatment (n = 6). (Scale bar: 50 μm.) Fc, dimeric-Fc (4 μg); sTie2-Fc, soluble Tie2 antibody (4 μg). *P < 0.001 vs. C and Ninj1 antibody (2.5 μg) + sTie2 (−) groups;#P < 0.001 vs. IgG and Fc groups; †P < 0.001 vs. Ninj1 antibody (2.5 μg) + sTie2 (−) group. DM, diabetes mellitus; STZ, streptozotocin. (J–M) Tube formationassay (J), quantification (number of tubes per field; screen magnification, 40×; n = 4) (K), phosphohistone H3 (PH3; red) staining (L) and (quantification(percent of PH3-immunopositive endothelial cells per high-power field; n = 4) (M) in MCECs exposed to the normal-glucose (NG) or high glucose (HG)condition, which were transfected with scrambled (SC), Ninj1, or Ang1 siRNA. Nuclei were labeled with DAPI (blue). (Scale bars: J, 500 μm; L, Upper, 50 μm; L,Lower, 25 μm.) In K and M, *P < 0.001 vs. NG and Ninj1 siRNA + Ang1 siRNA (−) groups; #P < 0.001 vs. SC group; †P < 0.001 vs. Ninj1 siRNA + Ang1 siRNA (−)group. P values in F, H, I, K, and M were determined by one-way ANOVA. Data are mean ± SE. AUC, area under curve; N-Ab, Ninj1 Ab; STZ, streptozotocin;WB, Western blot.
E2734 | www.pnas.org/cgi/doi/10.1073/pnas.1403471111 Yin et al.
Dow
nloa
ded
by g
uest
on
June
7, 2
020

G–I). No detectable differences in MSBP were found among thefive experimental groups (SI Appendix, Table S3).We further examined the role of the Ang1–Tie2 pathway in
Ninj1 siRNA-mediated angiogenesis in MCECs. An in vitroMatrigel assay revealed impairments in tube formation inMCECs exposed to high-glucose conditions, and these impair-ments were completely restored by treatment with Ninj1 siRNA.Cotransfection of MCECs with Ang1 siRNA diminished Ninj1siRNA-mediated enhancement of tube formation (Fig. 4 J andK). Moreover, Ninj1 siRNA-mediated endothelial cell prolifer-ation also was abolished by Ang1 siRNA in MCECs exposed tothe high-glucose condition (Fig. 4 L and M).
Ninj1-Neutralizing Antibody Decreases Cavernous ROS Production inDiabetic Mice. We performed Western blots to evaluate the cav-ernous tissue expression of p47phox (an active catalytic subunit ofNADPH oxidase) and inducible NOS (iNOS) in age-matchedcontrol and diabetic mice 2 wk after treatment. Cavernousp47phox and iNOS protein expression was significantly higherin the IgG-treated diabetic mice than in the age-matched con-trols. Intracavernous injection of Ninj1-neutralizing antibody(2.5 μg/20 μL) significantly decreased cavernous p47phox and iNOSexpression in the diabetic mice (Fig. 5 A–C).The generation of superoxide anion and peroxynitrite (which
is derived from NO and superoxide anion) was determinedby hydroethidine staining and immunohistochemical staining ofnitrotyrosine, respectively. The fluorescent products of oxidizedhydroethidine and nitrotyrosine expression in cavernous en-dothelial cells of the corpus cavernosum were higher in theIgG- and Fc-treated diabetic groups than in the control group.Intracavernous administration of Ninj1-neutralizing antibody(2.5 μg/20 μL) significantly decreased the generation of superoxideanion and peroxynitrite. Furthermore, the decrease in cavernousROS production mediated by Ninj1-neutralizing antibody wasblocked completely in the presence of sTie2-Fc (Fig. 5 D–F).We further examined whether macrophages participated in
the decrease in ROS production mediated by Ninj1 blockade.Immunofluorescent staining and hydroethidine staining revealedincreased infiltration of Ninj1+ macrophages as well as an in-crease in oxidized hydroethidine and nitrotyrosine expressionin the macrophages of diabetic mice, whereas the infiltrationof macrophages and the generation of ROS in macrophageswere profoundly decreased in Ninj1-KO mice that receivedstreptozotocin (STZ) (SI Appendix, Fig. S3 A–C). Ninj1 proteinexpression also was significantly higher in RAW 264.7 mac-rophages exposed to the high-glucose condition than in thecells exposed to the normal-glucose condition (SI Appendix,Fig. S3 D and E). Western blot analysis revealed an increase inthe expression of p47phox, iNOS, and nitrotyrosine in RAW264.7 cells exposed to the high-glucose condition. These levelsreturned to baseline after treatment with Ninj1 siRNA (SI Ap-pendix, Fig. S3 D and F–H). Similar to the results seen withMCECs, Ang2 protein expression was significantly higher inRAW 264.7 cells exposed to the high-glucose condition than inthe cells exposed to the normal-glucose condition, and this ele-vated expression of Ang 2 protein returned to baseline level aftertreatment with Ninj1 siRNA (SI Appendix, Fig. S3 D and I).Almost no Ang1 protein expression was observed in RAW 264.7cells (SI Appendix, Fig. S3D).
Ninj1-Neutralizing Antibody Restores Penile Nerve Content byPromoting the Secretion of Neurotrophic Factors in Diabetic Mice.The expression of nNOS and neurofilament in both the corpuscavernosum tissue and the dorsal nerve bundle was significantlylower in the IgG- and Fc-treated diabetic mice than in age-matchedcontrols. Intracavernous administration of Ninj1-neutralizing anti-body (2.5 μg/20 μL) completely restored penile nNOS-containingnerve fiber and axonal contents (neurofilament) in diabetic mice
(Fig. 6 A–C). To test whether the effects of Ninj1-neutralizingantibody were mediated by the production of neurotrophic fac-tors, we performed Western blot analysis for BDNF, NGF, andNT3. The cavernous expression of neurotrophic factors wassignificantly higher in diabetic mice receiving Ninj1-neutraliz-ing antibody (2.5 μg/20 μL) than in IgG- or Fc-treated diabeticmice, which was comparable to the levels found in age-matchedcontrols (Fig. 6 D and E). However, the Ninj1-neutralizingantibody-mediated increase in the expression of neurotrophicfactors and subsequent restoration of penile nerve contentwas remarkably diminished by pretreatment with sTie2-Fc(Fig. 6 A–E).
Conditioned Medium Derived from MCECs Regulates the Productionof Neurotrophic Factors in Neuro2A Cells. Because the results of ourin vivo study indicated that the Ang1–Tie2 pathway is crucial forNinj1-neutralizing antibody–mediated secretion of neurotrophicfactors and subsequent neural regeneration (Fig. 6 A–E), wefurther investigated whether conditioned medium derived fromMCECs cultured under the high-glucose condition with or with-out treatment with siRNA for Ninj1 and Ang1 affected theexpression of neurotrophic factors in neuro2A cells. Similar to
p47phoxC IgG 1.0 2.5
Ninj1 AbDM
β-actiniNOS
A
C IgG1.02.5
N-AbDM
*#
Rel
ativ
e ra
tio
(p47
phox
/ β-a
ctin
)B
0.00.51.01.52.02.53.0
HE
Mer
ged
PE
CA
M-1
Control IgG FcNinj1 Ab
sTie-2 (+)
STZ-induced diabetic mice
sTie-2 (-)
Nitr
o-T
Mer
ged
PE
CA
M-1
D E
No.
HE
(+)
EC
s/H
PF **#
†
0100200300400
IgGFc sTie-2 (-)sTie-2 (+)
C
N-AbDM
Rel
ativ
e ra
tio
( iNO
S/ β
-act
in)
*#
C
0.00.51.01.52.02.5
Nitr
o-T
(+) a
rea/
End
othe
lial a
rea
(%)
**#
†
F
0102030405060
C IgG1.02.5
N-AbDM
IgGFc sTie-2 (-)sTie-2 (+)
C
N-AbDM
Fig. 5. Ninj1-neutralizing antibody decreases cavernous ROS production ina Tie2-dependent manner. (A) Representative Western blot for p47phox andiNOS in penis tissue from age-matched control (C) or diabetic (DM) mice 2 wkafter a single intracavernous injection of IgG (2.5 μg) or Ninj1-neutralizingantibody (Ninj1 Ab; 1.0 μg or 2.5 μg). (B and C) Normalized band intensityvalues (n = 4). *P < 0.05 vs. C and Ninj1 Ab (2.5 μg) groups; #P < 0.05 vs. IgGgroup (Kruskal–Wallis test). (D) In situ detection of superoxide anion andnitrotyrosine production in each group at 2 wk after treatment. (Scale bars:100 μm.) Fc, dimeric-Fc (4 μg); sTie2-Fc, soluble Tie2 antibody (4 μg). (E and F)Number of ethidium bromide fluorescence-positive endothelial cells perhigh-power field (n = 6) (E) and the quantification of nitrotyrosine-immu-nopositive endothelial area (n = 6) (F). *P < 0.001 vs. C, Ninj1 antibody (2.5μg) + sTie2 (-) groups; #P < 0.001 vs. IgG and Fc groups; †P < 0.001 vs. Ninj1antibody (2.5 μg) + sTie2 (−) group (one-way ANOVA). Data are mean ± SE.DM, diabetes mellitus; ECs, endothelial cells; HE, hydroethidine; iNOS, in-ducible nitric oxide synthase; p47phox, an active catalytic subunit of NADPHoxidase; N-Ab, Ninj1 Ab; Nitro-T, nitrotyrosine; STZ, streptozotocin.
Yin et al. PNAS | Published online June 16, 2014 | E2735
MED
ICALSC
IENCE
SPN
ASPL
US
Dow
nloa
ded
by g
uest
on
June
7, 2
020

the results from diabetic mice in vivo, Ang1 protein expressionwas significantly lower in MCECs exposed to the high-glucosecondition than in the cells exposed to the normal-glucose con-dition, whereas Ninj1 protein expression was increased by thehigh-glucose condition. These levels returned to baseline aftertreatment with Ninj1 siRNA. However, knockdown of Ang1 withsiRNA did not affect Ninj1 expression in MCECs (Fig. 6 F andG). The protein expression of neurotrophic factors was signifi-cantly lower in neuro2A cells treated with conditioned mediumderived from MCECs exposed to the high-glucose condition thanin the cells treated with conditioned medium from MCECsexposed to the normal-glucose condition. Furthermore, the ex-pression of neurotrophic factors was significantly increased bytreatment with conditioned medium from Ninj1 siRNA-trans-fected MCECs exposed to the high-glucose condition. Condi-tioned medium from both Ninj1 siRNA and Ang1 siRNAcotransfected MCECs completely abolished the effect of theNinj1 siRNA-mediated increment in neurotrophic factor ex-pression in neuro2A cells (Fig. 6 H and I).
Ninj1-KO Mice Are Resistant to Diabetes-Induced Angiopathy andNeuropathy and Have Restored Erectile Function. To confirm fur-ther the results regarding the role of Ninj1 in the pathogenesis ofdiabetic ED resulting from angiopathy and neuropathy, we ex-amined the effect of STZ administration in Ninj1-KO mice. At8 wk after the injection of STZ and induction of diabetes, theratios of maximal ICP and total ICP to MSBP were significantlylower in WT mice that received STZ than in untreated WT mice,whereas erectile function was relatively preserved in Ninj1-KOmice that received STZ (Fig. 7 A–C). In accordance with thisfinding, targeted depletion of the Ninj1 gene rescued the di-abetes-induced decrease in cavernous endothelial and neuronalcell contents as well as the increase in endothelial cell apoptosis(Fig. 7 D–K).
Transcriptome Analysis of Ninj1 Target Genes in MCECs. To identifythe genes regulated by Ninj1 siRNA, a microarray analysis wasperformed (SI Appendix, Fig. S4 A–C). MCECs were exposed tothe normal-glucose or high-glucose condition and transfected
BDNF
-actin
C IgG Fc sTie2
(+)
DMN-Ab
sTie2
(-)
NGFNT3
Mou
se p
enis
D
-actin
Ang1Ninj1
MC
EC
s
NG SC siAng
1 (+)
HGsiNinj1
siAng
1 (-)
F
BDNF
NT3
H
NGF
CM treatment
Neu
ro2A
NG SC siAng
1 (+)
HGsiNinj1
siAng
1 (-)
-actin
Rel
ativ
e ra
tio
* *
#
** **##
†††
E BDNFNGFNT-3
0.00.20.40.60.81.01.21.4
DMIgG Fc sTie2 (-)sTie2 (+)
C
N-Ab
NG SC siAng1 (+)
HGsiNinj1
siAng1 (-)
CM treatment
*#
†*
##
††
I
0.00.5
1.01.5
2.0 BDNFNGFNT-3
*Rel
ativ
e ra
tio
G
siAng1 (+)siNinj1
Rel
ativ
era
tio
NG SC
HG
siAng1 (-)
*#
# †
*
0.00.51.01.52.02.5 Ang1
Ninj1
Control IgG Fc sTie2 (+)
STZ-induced diabetic miceNinj1 Ab
sTie2 (-)
Cav
erno
sum
nNO
S/D
API
Dor
sal n
erve
N
F/D
API
Dor
sal n
erve
nNO
S/D
API
A
#
* †*
C
0.00.20.40.60.81.01.2
DM
IgGFc sTie2 (-)sTie2 (+)
C
N-Ab
NF
(+)a
rea/
DN
BnN
OS
(+) n
erve
fibe
rs/
Cav
erno
sum
or D
NB
#
††
#
** **
B
0.00.20.40.60.81.01.2
DM
IgG Fc sTie2 (-)sTie2 (+)
C
N-Ab
CavernosumDorsal nerve
Fig. 6. Ninj1-neutralizing antibody induces neural regeneration. (A) nNOS (green) and neurofilament (red) immunostaining in penis tissue from age-matched control (C) or diabetic mice 2 wk after a single intracavernous injection of IgG (2.5 μg), dimeric-Fc (Fc, 4 μg), Ninj1-neutralizing antibody (Ninj1 Ab, 2.5μg), or Ninj1-neutralizing antibody (2.5 μg) + soluble Tie2 antibody (sTie2-Fc, 4 μg). Nuclei were labeled with DAPI (blue). (Scale bars: corpus cavernosum,50 μm; dorsal nerve bundle, 25 μm.) (B and C) Quantification of the nNOS- (B) or neurofilament (NF)-immunopositive area (C) in cavernous tissue by ImageJ (n = 6).(D) Western blot for neurotrophic factors. (E) Normalized band intensity values (n = 4). In C and E, *P < 0.001 vs. C and Ninj1 antibody (2.5 μg) + sTie2 (−)groups; #P < 0.001 vs. IgG and Fc groups; †P < 0.001 vs. Ninj1 antibody (2.5 μg) + sTie2 (−) group. BDNF, brain-derived neurotrophic factor; DM, diabetesmellitus; DNB, dorsal nerve bundle; NGF, nerve growth factor; NT3, neurotrophin-3; NF, neurofilament; N-Ab, Ninj1 Ab; STZ, streptozotocin. (F–I) Conditionedmedium (CM) of MCECs regulates the production of neurotrophic factors in neuro2A cells. (F and H) The MCECs transfected with scrambled (SC), Ninj1, orAng1 siRNA were exposed to the normal-glucose (NG) or high-glucose (HG) condition (F). Then the supernatant was transferred to Neuro2A cells (H). (G and I)Normalized Western blot band intensity values (n = 4). *P < 0.01 vs. NG and Ninj1 siRNA + Ang1 siRNA (-) groups; #P < 0.01 vs. SC group; †P < 0.01 vs. Ninj1siRNA + Ang1 siRNA (-) group. P values were determined by Kruskal−Wallis test (B, E, G, and I) or one-way ANOVA (C). Data are mean ± SE.
E2736 | www.pnas.org/cgi/doi/10.1073/pnas.1403471111 Yin et al.
Dow
nloa
ded
by g
uest
on
June
7, 2
020

with scrambled or Ninj1 siRNA. We selected genes that changedmore than 1.5-fold at the ratios calculated by both conditions,i.e., MCECs exposed to the normal-glucose condition comparedwith those exposed to the high-glucose condition + scrambledsiRNA, and MCECs exposed to the high-glucose condition +Ninj1 siRNA compared with those exposed to the high-glucosecondition + scrambled siRNA. After data filtering, 9,103 geneswere changed more than 1.5-fold (SI Appendix, Fig. S4, B and C).The functional clustering analysis on the common genes showedthat 6.5%, 6.2%, and 5.9% of these were involved in cell death,apoptosis, and cell proliferation, respectively (SI Appendix, Fig.S4, B and C). The selected genes relevant to apoptosis (47 genes)or proliferation (37 genes) are summarized in SI Appendix,Tables S5 and S6. These genes included previously known Ninj1targets, such as Angpt1 (Ang1) and Angpt2 (Ang2) (highlightedin SI Appendix, Tables S5 and S6). The expression of Ninj1
mRNA was significantly increased in MCECs exposed to thehigh-glucose condition as compared with the normal-glucosecondition; this level returned to baseline after treatment withNinj1 siRNA (SI Appendix, Fig. S4 D and E).
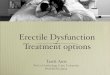
DiscussionHere, we investigated whether inhibition of the Ninj1 pathwayexerts beneficial effects in diabetic ED. In a mouse model ofdiabetic ED, a single intracavernous injection of Ninj1-neutral-izing antibody or targeted depletion of the Ninj1 gene success-fully restored erectile function through dual angiogenic andneurotrophic effects. The detailed mechanisms of action by whichinhibition of the Ninj1 pathway restores erectile function are sum-marized in Fig. 8.To investigate whether the recovery of erectile response was
related to an increase in the number of endothelial cells, we
B
Max
ICP
/MSB
P
*#†
WT Ninj1-KO
0.0
0.40.2
0.60.8
PEC
AM
-1P
H3
WT WT+STZ Ninj1-KO+STZNinj1-KOD
PEC
AM
-1M
erge
dC
leav
edca
spas
e-3
Mer
ged
Cav
erno
sum
nNO
S/ D
AP
ID
orsa
l ner
ve
NF/
DAP
ID
orsa
l ner
venN
OS
/DA
PI
WT WT+STZ Ninj1-KO+STZNinj1-KO
PEC
AM
-1N
inj1
Mer
ged
H
C
Tota
l IC
P/M
SBP
(AU
C)
*#†
0
2010
304050
05
10152025
End
othe
lial a
rea/
Cav
erno
sum
(%)
30
*†
E
WT
Ninj1-KO
J
*#†
0.00.20.40.60.81.01.2
NF
(+) a
rea
/D
NB
K
WT+STZ Ninj1-KO Ninj1-KO+STZWT130100
50
00
8 w
eeks
ICP
(cm
H2O
)
2 4 0 2 4 0 2 4 0 2 4
A
(Minutes)
No.
PH3
(+)
EC
s/H
PF
05
101520
*#†
F*
#†
No.
C-c
aspa
se-3
(+
)EC
s/H
PF
05
1015202530
G*
020406080
100
Nin
j1 (+
) are
a/E
ndot
helia
l are
a (%
)I
STZ (+)(-) (+)(-)WT Ninj1-KO
STZ (+)(-) (+)(-)
STZ (+)(-) (+)(-)
WT
Ninj1-KO
STZ (+)(-) (+)(-)
WT
Ninj1-KO
STZ (+)(-) (+)(-)
WT
Ninj1-KO
STZ (+)(-) (+)(-)
#††#
**nNO
S(+
) ne
rve
fiber
s
0.00.20.40.60.81.01.2
CavernosumDorsal nerve
WT
Ninj1-KO
STZ (+)(-) (+)(-)
WT
Ninj1-KO
STZ (+)(-) (+)(-)
Fig. 7. Ninj1-KO mice are resistant to diabetes-induced angiopathy and neuropathy and have restored erectile function. (A) Representative ICP responses forWT mice, WT mice receiving STZ, Ninj1-KO mice (Ninj1-KO), or Ninj1-KO mice receiving STZ. (B and C) Ratios of mean maximal ICP (B) and total ICP (C) (areaunder the curve) to MSBP were calculated for each group at 8 wk after the induction of diabetes (n = 6). *P < 0.001 vs. WT + STZ (−) group; #P < 0.01 vs. Ninj1-KO + STZ (−) group; †P < 0.001 vs. WT + STZ (+) group. (D) PECAM-1 (green) and phosphohistone H3 (PH3; red) or PECAM-1 (red) and cleaved caspase-3immunostaining in each group. Nuclei were labeled with DAPI (blue). (Scale bars: PECAM-1-PH3 images, 25 μm; PECAM-1–cleaved caspase-3 images, 50 μm.)(E) Endothelial cell content in cavernous tissue was quantified using ImageJ. (F) Number of PH3-immunopositive endothelial cells per high-power field. (G)Number of apoptotic cells in endothelium per high-power field. *P < 0.001 vs. WT + STZ (-) group; #P < 0.001 vs. Ninj1-KO + STZ (−) group; †P < 0.001 vs. WT +STZ (+) group. (H) PECAM-1 (green), Ninj1 (red), nNOS (green), or neurofilament (red) immunostaining in each group. Nuclei were labeled with DAPI (blue).(Scale bars: PECAM-1-Ninj1 images, 100 μm; corpus cavernosum, 50 μm; dorsal nerve bundle, 25 μm. (I–K) Quantification of Ninj1 (I), nNOS (J), and neuro-filament (K) in cavernous tissue or dorsal nerve bundle using ImageJ. Note there is no expression of endogenous Ninj1 in Ninj1-KO mice. *P < 0.05 vs. WT +STZ (−) group; #P < 0.05 vs. Ninj1-KO + STZ (−) group; †P < 0.05 vs. WT + STZ (+) group. The P values were determined by one-way ANOVA (B, C, E, F, and K),Kruskal–Wallis test (G and J), or Mann–Whitney u test (I). Data are mean ± SE. AUC, area under curve; C-caspase-3, cleaved caspase-3; DNB, dorsal nervebundle; ECs, endothelial cells; NF, neurofilament.
Yin et al. PNAS | Published online June 16, 2014 | E2737
MED
ICALSC
IENCE
SPN
ASPL
US
Dow
nloa
ded
by g
uest
on
June
7, 2
020

evaluated the expression of PECAM-1 by immunohistochemicalanalysis. In agreement with the results of previous studies inSTZ-induced diabetic rats (20–22) and mice (14), the cavernousendothelial area was significantly lower in untreated or IgG-treated diabetic mice than in control mice. Intracavernous in-jection of high-dose Ninj1-neutralizing antibody (2.5 μg/20 μL)induced complete recovery of the PECAM-1+ endothelial areain the corpus cavernosum of diabetic mice. Immunohistochem-ical examination of phosphohistone H3 expression showed thatthe increase in cavernous endothelial content by Ninj1-neutraliz-ing antibody was partly the result of the endothelial proliferation.In the present study, cavernous expression of Ang1 was down-
regulated and that of Ang2 was up-regulated by the diabeticcondition, and Ninj1-neutralizing antibody restored the expres-sion of Ang1 and Ang2 to the levels in controls. Similar to thisfinding, knockdown of the Ninj1 gene increased the Ang1/Ang2ratio in primary cultured MCECs, whereas overexpression of theNinj1 gene decreased the Ang1/Ang2 ratio. The Ang1–Tie2signaling pathway plays an important role in generating a non-leaky, stable, functional vasculature (23) and also is known to beinvolved in endothelial cell survival through the phosphatidyli-nositol 3-kinase/Akt pathway (24, 25). A previous study reportedthat Ninj1 promotes cell–cell adhesion and induces productionof Wnt7b and Ang2, which lead to apoptosis and destabilizationof endothelial cells in the hyaloid vascular system, while sup-pressing the expression of Ang1, an endothelial cell survivalfactor (19). We recently reported that in diabetic mice intra-cavernous administration of synthetic Ang1 gene or proteinrestores erectile function by enhancing endothelial cell pro-liferation and decreasing endothelial cell apoptosis (14, 15). Inthe present study, we show that inhibition of the Ang1–Tie2pathway with sTie2-Fc diminished the increase in cavernousendothelial cell proliferation and decrease in endothelial cellapoptosis mediated by Ninj1-neutralizing antibody and failed torestore erectile function in the diabetic mice in vivo. Moreover,
Ninj1 siRNA-mediated enhancement of tube formation and en-dothelial cell proliferation was abolished by cotransfection withAng1 siRNA in MCECs in vitro. Collectively, these findings sug-gest that restoration of the Ang1/Ang2 balance is crucial for Ninj1blockade-mediated cavernous angiogenesis and subsequent re-covery of erectile function. However, the exact mechanisms bywhich Ninj1 regulates the expression of Ang1 and Ang2 arelargely unknown and remain to be clarified.The generation of superoxide anion and peroxynitrite was
significantly higher in the penis of diabetic mice than in controls.Endothelial cells generate ROS, which may play a physiologic orpathologic role depending on the level of ROS. Low levels ofROS act as signaling molecules that induce endothelial cellproliferation and migration in response to a variety of stimuli,such as ischemia and angiogenic factors (26, 27). In pathologicconditions in which ROS already are generated at high levels(e.g., in the penis of diabetic mice, as shown in the present study),the high levels of ROS induce apoptosis and cell death (28).Similar to our results showing a decrease in the production ofROS in the penis of diabetic mice treated with synthetic Ang1(14), Ninj1-neutralizing antibody significantly reduced the gener-ation of superoxide anion and peroxynitrite in endothelial cells ofdiabetic mice, possibly by inhibiting the expression of cavernousp47phox and iNOS, respectively. In accordance with these results,Ninj1-neutralizing antibody significantly reduced the number ofapoptotic cells in the cavernous endothelium of diabetic mice.Pretreatment of diabetic mice with sTie2-Fc completely abolishedthe effect of Ninj1-neutralizing antibody on the generation of ROS.This finding suggests the importance of the Ang1–Tie2 pathway inthe Ninj1 blockade-mediated regulation of ROS production.Macrophages play an essential role in inflammation and in-
crease oxygen uptake, resulting in the accumulation of ROSduring inflammation (29). Similar to a previous study showingthat Ninj1 blockade decreased the infiltration of macrophages inan experimental model of allergic encephalomyelitis (18), tar-geted depletion of the Ninj1 gene significantly reduced diabetes-induced infiltration of macrophages and the generation of ROSin macrophages.The amount of intact nNOS+ neurons is crucial for proper
erectile function, because NO derived from nerve terminalsinitiates penile erection by inducing the dilatation of cavernoussinusoids, and subsequent shear stress-mediated activation ofAkt and eNOS sustains penile erection (30). In the present study,intracavernous injection of high-dose Ninj1-neutralizing anti-body (2.5 μg/20 μL) completely restored nNOS+ nerve contentin the penis of diabetic mice. We further examined the mech-anisms by which Ninj1-neutralizing antibody induces neuralregeneration. The expression of neurotrophic factors, such asBDNF, NGF, and NT3, was significantly lower in the penis ofdiabetic mice than in controls, but the expression was restoredremarkably by treatment with Ninj1-neutralizing antibody. Sim-ilar to the results in vivo, the expression of neurotrophic factorproteins was down-regulated in neuro2A cells treated with con-ditioned medium derived from MCECs exposed to the high-glucose condition. Furthermore, the expression was profoundlyrestored by Ninj1 siRNA-transfected conditioned medium. In-hibition of the Ang1–Tie2 signaling pathway with sTie2-Fc orAng1 siRNA abolished the Ninj1 blockade-mediated increase inneurotrophic factors and restoration of nNOS-positive neuronsin diabetic mice in vivo and in neuro2A cells in vitro. A recentstudy reported that Ang1 inhibits apoptosis of retinal neuronsand prevents neuronal dysfunction in a mouse model of oxygen-induced retinopathy (31). Thus, Ang1 may have a protectiveeffect on ischemia-induced neuronal loss. Further studies arenecessary to document how the Ang1–Tie2 signaling pathwayregulates the expression of neurotrophic factors.Finally, we examined the effect of targeted depletion of the
Ninj1 gene on diabetes-induced angiopathy and neuropathy.
nNOSNeurofilament
Neurotrophic factor(BDNF, NT-3, NGF)
ROS
p47phox
iNOS
Cell deathEC survival, regeneration
Akt/eNOSactivation
Penile erection
Nerve Endothelium
Ninj1Ninj1 neutralizing Ab
Ang2 Ang1
Fig. 8. Schematic diagram of a proposed mechanism showing how Ninj1blockade restores erectile function in diabetic mice. Ang1, angiopoietin1;Ang2, angiopoietin-2; BDNF, brain-derived neurotrophic factor; EC, endo-thelial cell; eNOS, endothelial nitric oxide synthase; iNOS, inducible nitricoxide synthase; NGF, nerve growth factor; Ninj1, nerve injury-induced pro-tein 1; nNOS, neuronal nitric oxide synthase; NT-3, neurotrophin-3; ROS,reactive oxygen species.
E2738 | www.pnas.org/cgi/doi/10.1073/pnas.1403471111 Yin et al.
Dow
nloa
ded
by g
uest
on
June
7, 2
020

Endothelial cell and nerve content were preserved and erectilefunction was rescued in Ninj1-KO mice receiving STZ. Theseresults suggest that therapeutic endothelial and neural regenerationmay provide a pathway for the treatment of diabetic ED.However, our study had some limitations. First, this study did
not explain how Ninj1 regulates the expression of Ang1 andAng2 or how the Ang1–Tie2 signaling pathway is involved in theregulation of neurotrophic factor expression mediated by Ninj1-neutralizing antibody or by Ninj1 siRNA. Second, the duration ofrecovery of erectile function was relatively short. Further studiesare needed to test whether repeated intracavernous injections ofNinj1-neutralizing antibody or the development of more potentNinj1-blocking peptide would induce more durable recovery oferectile function. Finally, our data demonstrating that Ninj1 in-hibition plays a positive role in neural regeneration in diabeticpenis in vivo are inconsistent with the study by Araki and Mil-brandt (17), which showed that Ninj1 facilitates neurite exten-sion in cultured dorsal root ganglion neurons in vitro. Thisdisparity may result from different experimental conditions orfrom the observation of different organ systems.In summary, our results indicate that inhibition of the Ninj1
pathway rescues erectile function in diabetic mice by inducingboth angiogenesis and neural regeneration in an Ang1-Tie2–dependent manner. The dual angiogenic and neurotrophiceffects of Ninj1 blockade, especially local therapy in the form ofneutralizing antibody or blocking peptide, opens a new avenuethrough which to treat diabetic ED.
Materials and MethodsExpanded methods are available in SI Appendix, SI Methods.
Study Design. The primary aim of the present study was to investigate themechanisms through which inhibition of the Ninj1 pathway restoresdiabetes-induced erectile function. To do so, we administered Ninj1-neutralizing antibody into the penis of diabetic mice and also used Ninj1-KO mice. Detailed mechanisms were evaluated with WT or Ninj1-KO miceand primary cultured MCECs and Neuro2A cells. All parameters of ge-netically modified mice and diabetic mice were compared with those oflittermate controls.
Animals and Treatments. The experiments were approved by the InstitutionalAnimal Care and Use Subcommittee of Inha University. Male 8-wk-old C57BL/6Jmice (Orient Bio) and Ninj1-KO mice (B6.129P2-Ninj1TM1GTO/J, provided byG.T.O.) were used in this study. Ninj1-KO mice were backcrossed with C57BL/6for at least seven generations. The primer sequences for genotyping were asfollows: WT (forward): 5′-GAG ATA GAG GGA GCA CGA CG-3′; Neo (forward):5′-ACG CGT CAC CTT AAT ATG CG-3′; reverse primer: 5′-CGG GTT GTT GAG GTCATA CTT G-3′. Diabetes was induced by i.p. injections of multiple low doses ofSTZ (50 mg/kg body weight in 0.1 M citrate buffer, pH 4.5) for 5 d consecu-tively as previously described (20). Eight weeks after diabetes was induced,the mice were anesthetized with ketamine (100 mg/kg) and xylazine (5mg/kg) i.m. and were placed supine on a thermoregulated surgical table.
To test the efficacy of Ninj1-neutralizing antibody, the mice were dis-tributed into five groups: age-matched controls, diabetic mice withouttreatment, diabetic mice receiving a single i.v. injection of mouse IgG controlantibody, diabetic mice receiving a single i.v. injection of low-dose (1.0 μg/20 μL)mouse neutralizing antibody to Ninj1 (BD Biosciences), and diabetic micereceiving a single intracavernous injection of high-dose (2.5 μg/20 μL) mouse
neutralizing antibody to Ninj1. In the pilot study, we determined the opti-mal concentration to induce maximal recovery of erectile function.
For the inhibition study with sTie2-Fc, the mice were distributed into fivegroups: age-matched controls, diabetic mice receiving a single intracavernousinjection of mouse IgG control antibody, diabetic mice receiving a singleintracavernous injection of dimeric-Fc, diabetic mice receiving a singleintracavernous injection of high-dose (2.5 μg/20 μL) mouse neutralizing anti-body to Ninj1, and diabetic mice receiving a single intracavernous injectionof high-dose (2.5 μg/20 μL) mouse neutralizing antibody to Ninj1 and s.c. in-jection of sTie2-Fc (4 μg/20 μL) (R&D Systems). sTie2-Fc was administered imme-diately before the injection of Ninj1-neutralizing antibody. We evaluated erectilefunction by cavernous nerve electrical stimulation 2 or 4 wk after treatment.The penis was harvested for histologic examination and biochemical study.
For the Ninj1-KO study, the mice were distributed into four groups: WTcontrols, WT mice receiving STZ (50 mg/kg body weight, for 5 d), Ninj1-KOmice, and Ninj1-KO mice receiving STZ (50 mg/kg body weight, for 5 d). At8 wk after the induction of diabetes, we measured erectile function duringelectrical stimulation of the cavernous nerve, and then the penis was har-vested for histologic examination. Fasting and postprandial blood glucoselevels were determined with an Accu-check blood glucose meter (RocheDiagnostics) before the mice were killed.
Measurement of Erectile Function, Histologic Examinations, and In Situ Detectionof Superoxide Anion. Measurement of erectile function, histologic examina-tions, and in situ detection of superoxide anion were performed as describedin SI Appendix, SI Methods.
Cell-Culture Experiments. Cell culture, transfection assay, RT-PCR, cDNA micro-array, and in vitro tube formation assay were performed as described inSI Appendix, SI Methods.
Preparation of Conditioned Medium from MCECs and Transfer to Neuro2A Cells.To examine the effect of conditioned medium derived from MCECs onNeuro2A cells, the MCECs were cultured and treated under the followingconditions: MCECs exposed to normal-glucose condition (5 mmol), MCECs ex-posed to the high-glucose condition (30 mmol) and transfected with scrambledsiRNA (200 pmol), MCECs exposed to the high-glucose condition (30 mmol)and transfected with Ninj1 siRNA (200 pmol), and MCECs exposed to the high-glucose condition (30 mmol) and transfected with both Ninj1 siRNA (200 pmol)and Ang1 siRNA (200 pmol). The MCECs were transfected with Ninj1 siRNA orAng1 siRNA for 24 h and then exposed to the high-glucose condition for an-other 48 h. The culture supernatants were collected and centrifuged for 10minat 200 × g to remove cell debris and then were transferred to Neuro2A cells.After 12 h, Neuro2A cells were harvested for Western blot analysis.
Western Blot. Western blot analysis was performed as described in SI Ap-pendix, SI Methods.
Statistical Analysis. The results are expressed as mean ± SE. For parametricdata, intergroup comparisons were made by one-way ANOVA followed byNewman–Keuls post hoc tests. We used the Mann–Whitney u test or Kruskal–Wallis test to compare nonparametric data. Probability values less than 5%were considered significant. We used SigmaStat 3.11 software (Systat Soft-ware) for statistical analyses.
ACKNOWLEDGMENTS. This work was supported by Grant A110076 fromthe Korea Healthcare Technology R&D Project, Ministry for Health, Welfareand Family Affairs, Republic of Korea (to J.-K.S. and J.-K.R.); by MedicalResearch Center Grant 2014R1A5A2009392 (to J.-K.R.); and by Grant2012RIA3A2026454 (to G.T.O.) from National Research Foundation, fundedby the Korean government (Ministry of Science, ICT and Future Planning).
1. National Institutes of Health Consensus Development Panel on Impotence (1993)
Impotence. NIH Consensus Conference. JAMA 270(1):83–90.2. Friedewald VE, et al.; American Journal of Cardiology; Journal of Periodontology (2009)
The American Journal of Cardiology and Journal of Periodontology Editors’ Consensus:
Periodontitis and atherosclerotic cardiovascular disease. Am J Cardiol 104(1):59–68.3. Lue TF (2000) Erectile dysfunction. N Engl J Med 342(24):1802–1813.4. Hakim LS, Goldstein I (1996) Diabetic sexual dysfunction. Endocrinol Metab Clin North
Am 25(2):379–400.5. Malavige LS, Levy JC (2009) Erectile dysfunction in diabetes mellitus. J Sex Med 6(5):
1232–1247.6. Vignozzi L, et al. (2007) Testosterone regulates RhoA/Rho-kinase signaling in two
distinct animal models of chemical diabetes. J Sex Med 4(3):620–630, discussion
631–632.
7. Martínez-Jabaloyas JM, et al. (2001) Prognostic factors for response to sildenafil in
patients with erectile dysfunction. Eur Urol 40(6):641–646, discussion 647.8. Musicki B, Burnett AL (2007) Endothelial dysfunction in diabetic erectile dysfunction.
Int J Impot Res 19(2):129–138.9. Angulo J, et al. (2010) Diabetes exacerbates the functional deficiency of NO/cGMP
pathway associated with erectile dysfunction in human corpus cavernosum and penile
arteries. J Sex Med 7(2 Pt 1):758–768.10. Davis S, et al. (1996) Isolation of angiopoietin-1, a ligand for the TIE2 receptor, by
secretion-trap expression cloning. Cell 87(7):1161–1169.11. Ward NL, Dumont DJ (2002) The angiopoietins and Tie2/Tek: Adding to the com-
plexity of cardiovascular development. Semin Cell Dev Biol 13(1):19–27.12. Suri C, et al. (1996) Requisite role of angiopoietin-1, a ligand for the TIE2 receptor,
during embryonic angiogenesis. Cell 87(7):1171–1180.
Yin et al. PNAS | Published online June 16, 2014 | E2739
MED
ICALSC
IENCE
SPN
ASPL
US
Dow
nloa
ded
by g
uest
on
June
7, 2
020

13. Kwon MH, et al. (2013) Effect of intracavernous administration of angiopoietin-4 on
erectile function in the streptozotocin-induced diabetic mouse. J Sex Med 10(12):2912–2927.
14. Jin HR, et al. (2011) Intracavernous delivery of a designed angiopoietin-1 variant
rescues erectile function by enhancing endothelial regeneration in the streptozotocin-induced diabetic mouse. Diabetes 60(3):969–980.
15. Jin HR, et al. (2010) Intracavernous delivery of synthetic angiopoietin-1 protein asa novel therapeutic strategy for erectile dysfunction in the type II diabetic db/db
mouse. J Sex Med 7(11):3635–3646.16. Bennett NE, et al. (2005) Improvement in erectile dysfunction after neurotrophic
factor gene therapy in diabetic rats. J Urol 173(5):1820–1824.17. Araki T, Milbrandt J (1996) Ninjurin, a novel adhesion molecule, is induced by nerve
injury and promotes axonal growth. Neuron 17(2):353–361.18. Ifergan I, et al. (2011) Role of Ninjurin-1 in the migration of myeloid cells to central
nervous system inflammatory lesions. Ann Neurol 70(5):751–763.19. Lee HJ, et al. (2009) Ninjurin1 mediates macrophage-induced programmed cell death
during early ocular development. Cell Death Differ 16(10):1395–1407.20. Jin HR, et al. (2009) Functional and morphologic characterizations of the diabetic
mouse corpus cavernosum: Comparison of a multiple low-dose and a single high-dose
streptozotocin protocols. J Sex Med 6(12):3289–3304.21. Zhang LW, et al. (2008) Role of increased penile expression of transforming growth
factor-beta1 and activation of the Smad signaling pathway in erectile dysfunction instreptozotocin-induced diabetic rats. J Sex Med 5(10):2318–2329.
22. Burchardt T, et al. (2000) Reduction of endothelial and smooth muscle density inthe corpora cavernosa of the streptozotocin induced diabetic rat. J Urol 164(5):1807–1811.
23. Augustin HG, Koh GY, Thurston G, Alitalo K (2009) Control of vascular morphogenesisand homeostasis through the angiopoietin-Tie system. Nat Rev Mol Cell Biol 10(3):165–177.
24. Kim I, et al. (2000) Angiopoietin-1 regulates endothelial cell survival through thephosphatidylinositol 3′-Kinase/Akt signal transduction pathway. Circ Res 86(1):24–29.
25. Papapetropoulos A, et al. (2000) Angiopoietin-1 inhibits endothelial cell apoptosis viathe Akt/survivin pathway. J Biol Chem 275(13):9102–9105.
26. Stone JR, Collins T (2002) The role of hydrogen peroxide in endothelial proliferativeresponses. Endothelium 9(4):231–238.
27. Łuczak K, Balcerczyk A, Soszy�nski M, Bartosz G (2004) Low concentration of oxidantand nitric oxide donors stimulate proliferation of human endothelial cells in vitro. CellBiol Int 28(6):483–486.
28. Griendling KK, Sorescu D, Ushio-Fukai M (2000) NAD(P)H oxidase: Role in cardiovas-cular biology and disease. Circ Res 86(5):494–501.
29. Brüne B, et al. (2013) Redox control of inflammation in macrophages. Antioxid RedoxSignal 19(6):595–637.
30. Hurt KJ, et al. (2002) Akt-dependent phosphorylation of endothelial nitric-oxidesynthase mediates penile erection. Proc Natl Acad Sci USA 99(6):4061–4066.
31. Lee J, et al. (2013) Angiopoietin-1 guides directional angiogenesis through integrinalphavbeta5 signaling for recovery of ischemic retinopathy. Sci Transl Med 5(203):203ra127.
E2740 | www.pnas.org/cgi/doi/10.1073/pnas.1403471111 Yin et al.
Dow
nloa
ded
by g
uest
on
June
7, 2
020