Embed Size (px)
Citation preview

8 EMN n March 2014
InFocus Potentially Fatal Side Effect of ACE Inhibitors: Angioedema
By James R. Roberts, MD
Angiotensin-converting enzyme in-hibitors (ACEIs) are one of the
most prescribed medications world-wide for hypertension. Many patients with congestive heart failure, renal dysfunction, and diabetes are also tak-ing these medications, and angioedema is a well-recognized and occasionally fatal side effect of all members of this class of medications.
ACEI angioedema occurs in up to almost one percent of treated patients. The edema is a class effect, not an overdose, and symptoms can occur any time after the first dose to up to many years, even after a patient has been well maintained on the medica-tion without this complication. The majority of patients has actually been taking the drug for extended periods, and do not recognize the culprit when the symptoms develop. The pathophys-iology is a bit cloudy, but it is thought to be caused by a decreased degrada-tion of bradykinin and up to a 10-fold increase of this potent vasodilator that increases vascular permeability. Oddly, some cases of angioedema recur for weeks and even months after the ACEI has been stopped.
Most emergency physicians are all too familiar with this nefarious com-plication. Trying to get an airway in advanced cases is a hellish endeavor and not always successful. General empiric treatment guidelines have evolved, but the value of any specific currently used reversal medication is unproven and likely minimal at best.
Emergency Department Management of Patients with ACE Inhibitor AngioedemaWinters M, Rosenbaum S, et alJ Emerg Med2013;45(5):775
These authors attempted to establish the appropriate ED management of patients with ACEI angioedema. A Medline search yielded 27 appropriate articles that were rigorously reviewed to spawn the recommendations. Un-fortunately, attempts to develop a specific treatment protocol based on a high level of evidence were not possible because of limited scientific studies.
Angioedema from ACE inhibitors is characterized by the abrupt onset of nonpitting, nonpruritic swelling in-
volving nondependent areas, usually in an asymmetric distribution. The edema is isolated to the head and neck regions and not accompanied by urticaria. The signs and symptoms in-clude shortness of breath, stridor, hoarseness, drooling, and swelling of the lips, tongue, floor of the mouth, neck and pharyngeal areas, and eye-lids. The abdominal viscera can be involved in rare cases, causing inter-mittent abdominal pain, nausea, and vomiting. These authors recommend that ACEI angioedema be considered
in any patient presenting with isolated asymmetric swelling of the areas mentioned.
A variety of anti-allergy medica-tions are generally administered. ACEI edema appears to be an allergic reaction, but it is not mediated by mast cell degranulation; therefore, the efficacy of usually effective anti- allergy drugs such as epinephrine, antihistamines, and corticosteroids is unlikely and remains unproven. No randomized controlled blinded stud-ies have compared these medications,
probably because most physicians quickly give all three. The edema gen-erally lasts 24-72 hours and spontane-ously subsides if the ACEI is halted. Standard anti-allergy medications have not been noted to be harmful, but no current evidence recommends for or against using any of them to treat ACEI angioedema.
Angioedema of the upper airway and larynx can be life-threatening. It is an ominous finding indicative of a se-vere process, and often requires ICU admission. The authors suggest the early use of fiber optic examination to determine the presence and extent of laryngeal involvement, and note that no patient with a normal larynx on fiber optic evaluation has progressed to require emergent intubation.
But intubation and cricothyrotomy may be necessary to maintain airway patency. Those presenting with respir-atory distress, stridor, drooling, and edema of the floor of the mouth are most likely to require intubation. The literature is varied on the need for ad-mission for patients with minimal and non-progressive edema. Most clini-cians consider at least observation for 12-24 hours in any patient with tongue edema. Patients who have edema lim-ited to the face and lips may be ob-served in the ED or in an observation area, but no recommendations exist for the optimal observation period.
These authors suggest that patients with respiratory distress, edema of the floor of the mouth, stridor, and drool-ing should be considered for immedi-ate intubation. Those not intubated with the potential for airway compro-mise should be admitted to the ICU. Patients with angioedema limited to the lips and face may be observed in the ED. Provided there is no progres-sion in four to six hours, discharge home with a discontinuation of the ACE inhibitor can be supported.
These authors conclude that the lit-erature does not support any specific treatment protocol with a high level of evidence. Certain medications may be of minimal benefit, but none has been proven effective. Fiber optic examina-tion of the larynx to determine disposi-tion of patients presenting with this relatively common medical condition is suggested.
Comment: I have personally seen hundreds of cases of ACEI angioedema. (Am J Cardiol 2012;109[5]:774.) It is much more common in African-American
ACEI angioedema is always treated with antihistamines, corticosteroids, and epinephrine, but none of these medications has been proven to be of clinical value. This is likely the case because the pathophysiology is not an IgE/mast-cell-mediated allergic reaction, which often responds dramatically to such interventions. The primary pathophysiology of ACEI angioedema is a buildup of bradykinin with resultant edema of the face and neck area. A synthetic bradykinin blocker, icatibant, may be the key to successful amelioration of the pathologic process. One dose costs more than $8000!
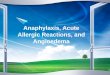
A severe example of ACE inhibitor-induced angioedema to the tongue.
LWW-EMN_March 2014_Layout.indd 8 07/02/14 12:34 AM

March 2014 n EMN 9
women in my experience, and this predi-lection is supported in studies. The edema is rather characteristic, usually first involving the lips and then the tongue or floor of the mouth. It is cer-tainly true that patients may have been on these medications for many years with no dose increase and then suddenly develop angioedema. The etiology is generally thought to be caused by an ac-cumulation of bradykinin, but the patho-physiology is still somewhat obscure. This looks like an allergy, but it is not.
Because the angioedema appears like an allergy, almost all physicians reflexively treat with epinephrine, anti-histamines, and corticosteroids. Epi-nephrine does not seem to be harmful with regard to hypertension, and the Physicians’ Desk Reference specifi-cally suggests using epinephrine as well as securing the airway in patients with significant symptoms.
Most patients who have anything more than lip or facial swelling should be admitted to the hospital for further observation. That means admitting them to a floor where they will actually be observed because decompensation can be rapid. Fiber optic intubation is
probably the best technique, but I have also used nasotracheal intubation.
Patients with ACEI angioedema usually get intubated either too early or too late. It is tempting to wait this out with careful observation, but se-curing the airway while the tongue is still passable with your laryngoscope is probably the best tactic. Many pa-tients will be intubated unnecessarily with an aggressive empiric approach. Once they are intubated, however, the emergency is over. Most physicians will give standard allergy medications, but they are of no proven value. It’s still difficult to eschew their use. The following articles will offer some po-tential life-saving interventions for this unusual process.
Fresh Frozen Plasma in the Treatment of Resistant Angiotensin-Converting Enzyme Inhibitor AngioedemaWarrier M, Copilevita CA, et alAnn Allergy Asthma Immunol2004;92(5):573
This 10-year-old article was one of the first to suggest fresh frozen
plasma (Icatibant) for treating ACEI angioedema. Another article before this letter was published similarly espoused the use of FFP. (J Allergy Clin Immunol 2002;109[2]:370.) The authors note that the inhibition of angiotensin-converting enzyme by ACE inhibitors results in diminished production of angiotensin II. This is the effect on the blood pressure and kidney function that is sought by treatment. Unfortunately, this mecha-nism also inhibits the degradation of bradykinin, and this accumulation is largely responsible for the adverse effects.
The patient in this report was tak-ing ramipril for hypertension. She had an initial episode of angioedema of the lips and fingers that resolved with anti-histamines, corticosteroids, and epi-nephrine, and the dose of ramipril was lowered. She did well for four months and then developed severe edema of the tongue and lips that was recalci-trant to any conventional therapy, including multiple doses of subcutane-ous epinephrine. She received antileu-kotrienes, cyclosporine, and intrave-nous immune globulin without benefits. Her complement level was normal, as was her total C1 inhibitor level. After four days of failure to re-solve, she had a complete resolution of symptoms within two to four hours of the infusion of two units of FFP. It was postulated that administration of FFP
leads to the breakdown of accumu-lated bradykinin with subsequent reso-lution of the angioedema.
Comment: The use of FFP is sup-ported by a variety of case reports, and most people believe it is beneficial, but it’s rarely used. Recently, Hassen et al reported on seven patients refractory to current interventions who demonstrated a temporal resolution of ACEI angio-edema. (J Emerg Med 2013;44[4]:764.) The rationale for FFP is that it provides ACE, also known as kininase II, and this catalyzes the degradation of excessive bradykinin.
One problem is that it takes a while to obtain FFP, and by that time pa-tients are either getting better or have been intubated. Once they are intu-bated, there seems little benefit in exposing them to blood products. No studies or reports support using epi-nephrine, antihistamines, or cortico-steroids, though a number of case reports support using FFP, and I be-lieve it reasonable to administer FFP as soon as possible in patients who have more than minimal swelling. Cer-tainly those who are borderline and likely will require intubation, should receive FFP if it can be given before intubation is performed. Given the lack of rapidity of obtaining FFP and the little known use for this indica-tion, it is likely that FFP will be infre-quently administered. Some patients
Continued on next page
This patient presents an intervention quandary. The isolated lip edema is not se-vere enough to cause airway problems yet. Such patients are often intubated too early or too late. Deterioration can be sudden and unexpected, but if lip edema is stable and does not progress during six hours observation, the patient is likely out of harm’s way. Some clinicians would admit this patient; others would ob-serve and send home if no there is no progression.
An example of ACE inhibitor-induced angioedema on the floor of the mouth.
An example of ACE inhibitor-induced angioedema to the tongue.
InFocus
LWW-EMN_March 2014_Layout.indd 9 07/02/14 12:34 AM

10 EMN n March 2014
InFocus
are also resistant to receiving blood products.
Therapeutic Efficacy of Icatibant in Angioedema Induced by Angiotensin-Converting Enzyme Inhibitors: A Case SeriesBas M, Greve J, et alAnn Emerg Med2010;56(3):278
This article from Germany includes a case series of eight patients with acute ACEI angioedema who were treated with a single subcutaneous injection of icatibant. ACEI angioedema re-sembles the pathophysiology behind hereditary angioedema, specifically
mediated by bradykinin-induced activation of vascular bradykinin B II receptors. Icatibant is a syn-thetic bradykinin II receptor an-tagonist used to treat hereditary angioedema, and these authors speculated that icatibant would be effective therapy for ACEI angioedema. Icatibant is stable and not degraded by bradykinin-cleaving enzymes such as ACE inhibitors.
These investigators treated eight patients with acute ACEI an-
gioedema with a single 30 mg dose of subcutaneous icatibant. All patients had angioedema for fewer than 10 hours, and were taking an ACE inhibi-tor. Following the injection of icati-bant, patients had hourly fiber optic transnasal laryngoscopy to assess reso-lution. Four patients had angioedema of the tongue and four of the laryngeal area. The most common offending drugs were enalapril and ramipril. Fol-lowing icatibant, the first symptom im-provement was noted after 50 minutes, and the mean time for complete resolu-tion was 4.4 hours. No patient required intubation or retreatment, and no addi-tional medications were used. All pa-tients did develop local reactions at the injection site. Compared with previous patients treated with corticosteroids, the results of this intervention were markedly better, particularly that no patient required intubation.
AngioedemA
Continued from previous page
Reader Feedback: readers are invited to ask specific questions and offer personal experiences, comments, or observations on inFocus topics. literature references are appreciated. Pertinent responses will be published in a future issue. Please send comments to [email protected].
Dr. Roberts: We read with great interest your column, “Think Twice Before routinely administering oxygen.” (2013;35[11]:12; http://bit.ly/1mGWoeM.) He has addressed an important issue concerning oxygen admin-istration and hyperoxia in emergency situations. We cannot agree more about the problems with extreme hyperoxia. Many studies, including the ones reviewed, have found that long-term exposure to high oxygen (>300mm Hg) leads to pulmonary toxicity and poor outcomes. (Crit Care Med 2014;42[2]:387; JAMA 2010;303[21]:2165.) calzia et al (Crit Care Med 2010;38[10 suppl]:s559) and others, however, hypothesize that hyperoxia during the acute phase could be beneficial. it is also likely that oxygen, like any other drug, may have its own therapeutic dose range, and no uniform range may apply to all ages or all clinical situations.
Traditional recommendations targets a Pao2 of 55-80 mm Hg in acutely ill pediatric patients on mechani-cal ventilation. (N Engl J Med 2000;342[18]:1301; Intensive Care Med 2008;34[1]:17.) The definitions of hyperoxia could also be different in the pediatric age group. in fact, hyperoxia (Pao2 > 300 mm Hg) as defined by the studies above were not commonly seen in children from our PicU (0.006% of a total of 3041 Pao2 records).
We have examined the association between hyperoxia and outcomes in acutely ill children in our PicU (manuscript under peer review for publication), and performed a retrospective analysis of prospectively collected data from 246 mechanically ventilated children. Partial pressure of oxygen in 1785 arterial blood gas samples during the first 72 hours of mechanical ventilation was analyzed. The mean and maximum Pao2 values were used to create receiver-operator characteristics (roc) curves for determining Pao2 cutoffs that could predict survival. (Figure 1.)
Mean Pao2 of 100 had 75% sensitivity and 60% specificity for predicting survival on roc curves and a maximum Pao2 of 150 had 72% sensitivity and 61% specificity for survival. Based on these cutoffs of mean and maximum Pao2 values, we created four groups (Group i: Pao2 55-100 mm Hg, Group ii: 101-150, Group iii: 151-200, Group iV: 201-300; Table 1). Patients
in groups ii, iii, and iV showed better survival compared with the traditional normoxemic group i.
a multivariate logistic regression analysis revealed PrisM iii score and mean Pao2 group to be independent predictors of survival after adjustment for age, sex, length of mechanical ventilation and incidence of nosocomial infections. We also compared Pao2 values from 594 children (3041 records) and found that max Pao2 range of 200-300 mm Hg appeared to be associated with a higher incidence of culture-positive nosocomial infections.
our data suggest that mild hyperoxia (Pao2 of 100-200 mm Hg) during the first 72 hours of mechanical ventilation in children may be associated with higher survival and lower culture-positive nosocomial infections. Further studies should address optimal Pao2 levels for acutely ill mechanically ventilated children. — L. G. Saptharishi, MD, & Sunit Singhi, MD, Chandigarh, India
Dr. Roberts responds: Many thanks to drs. saptharishi and singhi for their comments. Providing high levels of inspired oxygen is a universal reflex action in critically ill patients, but like any other intervention, it may have downsides. The detrimental effects of prolonged hyperoxia are not well defined, difficult to prove when multiple treatments are simultane-ously instituted, and not often addressed in the literature. The work of these physicians adds significantly to our knowledge.
Mean PaO2 Category
Children who survived (%)
Children who died (%)
Pearson Chi square p value
55 -100 (i) 50 (64.1) 28 (35.9)
< 0.001101-150 (ii) 110 (86.6) 17 (13.4)
151 -200 (iii) 37 (92.5) 3 (7.5)
201 - 300 (iV) 1 (100) 0 (0)
Max PaO2 Category
Children who survived (%)
Children who died (%)
Pearson Chi square p value
55 -100 (i) 7 (38.9) 11 (61.1)
< 0.001101-150 (ii) 49 (71.0) 20 (29.0)
151 -200 (iii) 87 (85.3) 15 (14.7)
201 - 300 (iV) 48 (96.0) 2 (4.0)
Table 1: Survival of children in different subgroups of mean and maximum PaO2.
1.0
0.8
0.6
0.4
0.2
0.00.0 0.2 0.4 0.6 0.8 1.0
Sens
itivi
ty
ROC Curve
Source or theCurve
1 - Specificity
PaO2MeanPaO2MaxReferenceLine
Figure 1: Predictive abilities of mean and maximum PaO2 levels: ROC curve.
Fresh frozen plasma (FFP) has been reported to diminish ACEI in-duced angioedema markedly. FFP contains kininase II (also known as angiotensin converting enzyme/ ACE). Supplying ACE that has been inhibited by ACEI medica-tions can hasten the breakdown of accumulated bradykinin.
LWW-EMN_March 2014_Layout.indd 10 07/02/14 12:35 AM

March 2014 n EMN 11
InFocus
The authors concluded that the subcutaneous injection of the specific bradykinin B II receptor antagonist
icatibant resulted in rapid symptom improvement and prompt complete recovery from ACEI angioedema.
Most subjects were discharged within 24 hours. The scientific rationale for using bradykinin B II receptor blocker is that it blocked excessive bradykinin stimulation. The authors note that their observations should be confirmed in a prospective random-ized controlled trial, but their results were impressive.
Comment: Icatibant is currently available in the United States for about $8000 per 30 mg dose. It has been reported by other authors to be effective in ACEI angioedema. This drug was developed for treating
hereditary angioedema, but its use for ACEI angioedema is exciting. An-other drug developed for hereditary angioedema, ecallantide, decreases bradykinin production, and was thought to be potentially useful for ACEI angioedema, but it was found to be ineffective. Trials were stopped when the lack of clinical effect was demonstrated.
Click and Connect! Access the links in EMN by reading this issue on our website or in our iPad app, both available on www.EM-News.com.
Read InFocus and Earn CME!
Emergency Medicine News is again offering cMe for readers who complete a quiz about this article. You may read the article here, on our website, or in our iPad app, and then complete the quiz, answering at least 70 percent of the questions correctly to earn cMe credit.
Visit http://cMe.lWW.com for more information about this educational offering and to complete the cMe activity. This enduring material is available to physicians in all specialties, nurses, and other allied health professionals. lippincott continuing Medical education institute, inc., is accredited by the accreditation council for continuing Medical education to provide continuing medical education for physicians. lippincott continuing Medical education institute, inc., designates this enduring material for a maximum of 1 AMA PRA Category 1 Credit™. Physicians should only claim credit commensurate with the extent of their participation in the activity. This activity expires Feb. 28, 2015.
dr. roberts has disclosed that the U.s. Food and drug administration has not approved the use of icatibant and ecallantide for treating acei angioedema as discussed in this article. Please consult the products’ labeling for approved information.
Learning Objectives for This Month’s CME Activity: after participating in this cMe activity, readers should be better able to describe and assess the side effects of ace inhibitors and the benefits and limitations of various interventions for patients with angioedema.
Dr. Roberts is the chairman of emergency med-icine and the director of the division of toxi-cology at Mercy Catholic Medical Center, and a professor of emer-gency medicine and toxicology at the Drexel University College of Medicine, both in Philadelphia.
n read The Procedural Pause, EMN’s newest blog by dr. roberts and his daughter, Martha roberts, acNP, ceN, at http://bit.ly/Procedural Pause.
n read all of dr. roberts’ past columns at http://bit.ly/robertsin Focus.
n comments about this article? Write to EMN at [email protected].
FastLinks
A systematic review of the pub-lished literature on interventions to reduce ED use by a multi-institution team of researchers revealed that pa-tient education initiatives yielded de-creases in ED use ranging from 21 percent to 80 percent. (Acad Emerg Med 2013;20[10]:969.) Prehospital di-version, in comparison, only resulted in drops of three percent to seven percent. The most surprising of all, some studies showed that adding ED capacity reduced use from nine per-cent to 54 percent, but one study found increased use of 21 percent, perhaps as a result of greater supply causing higher demand.
Two other less startling interven-tions also appeared to reduce ED use: managed care and patient financial in-centives such as ED copays, coinsur-ance, or high deductibles. A much larger body of literature is available on these strategies, and nine of 10 studies on patient financial incentives found decreases of three percent to 50 per-cent, while 10 of 12 managed care stud-ies had decreases ranging from one percent to 46 percent.
“The education piece was a bit of a surprise to us,” says Sofie Rahman Morgan, MD, an assistant professor of emergency medicine at Emory Univer-sity in Atlanta. “It’s a low-tech solu-tion. The studies generally just gave
patients or families a booklet on self-care, and in a couple it was comple-mented with a one-on-one session with a nurse. That’s incredibly simple, and something that would probably make people happier with the care they receive, as opposed to a copay-ment, which leaves a more negative reaction.”
But when the researchers tried to delve further into the outcomes of the interventions, beyond simply the re-duction in ED use itself, they found that the studies yielded little insight. “We wanted information on the finan-cial outcomes and the health outcomes of these interventions, and there’s very little in the literature,” said Dr. Morgan, adding that only eight of the 39 articles in their review (20.5%) included any cost data. “If the driver behind this is trying to reduce costs associated with ED care, why aren’t there studies look-ing at what cost reductions the inter-ventions achieved? This should be a primary outcome.”
The literature has many other limi-tations on this topic: almost all the studies are observational, and they are not comparing apples with apples in many cases. Some measured ED visits in total, for example, while others as-sessed ED visits per user.
“And a lot of the studies, espe-cially the patient education studies, involved pretty small sample sizes,” Dr. Morgan added. “If policymakers and insurers are going to be moving
forward to support interventions to reduce ED use, it needs to be an evi-dence-based movement. In my mind, our review is a first step, assessing what evidence is already out there and where there are gaps in the knowledge. The best approach is probably going to be some combina-tion of these, and what is right may vary by insurer, region, or organiza-tion trying to do this.”
Hospitals, insurers, policymak-ers, and researchers also need to be looking at a much broader question, said Brent Asplin, MD, the chief clinical officer at Catholic Health Partners, Ohio’s largest health sys-tem, and a former chair of emer-gency medicine at the Mayo Clinic. “What should be done to most effec-tively meet the needs of a population for acute unscheduled care? That’s not just about ED use, which is too narrow of a question. It’s about look-ing at a whole range of options: pri-mary care, virtual care, urgent care, retail care, and so on,” he said. “How do we structure systems so that we’re meeting the patients’ needs with the most efficient resource we have available at the time those needs arise?”
Dr. Asplin noted that today’s health care system has evolved to meet the needs of providers rather than the needs of patients when it comes to acute unscheduled care. “The traditional approach has been
to punish patients after the fact for choosing the wrong venue — ‘it was inappropriate to come to the ED for this, so we won’t cover it!’ — rather than making the system as seamless as we can for them,” he said. “If you think about how the rest of our lives work, that’s not the way it is. Retail, banking, and other areas of the econ-omy are all about meeting needs in real time. Why would we be sur-prised that people would start to ex-pect the same from health care?” (Read an EMN article on acute un-scheduled care solutions at http://bit.ly/1a1tQac.)
Opportunities for cost savings are there for the taking by care for low-acuity problems in alternate settings, and even greater savings lay in wait for finding safe and reli-able alternatives to hospital care and in reducing the variability by which patients get admitted to the hospital. “I’m more interested in looking at the back door to the ED — the decision process for who gets admitted — than the front,” Dr. Asplin said. “We have the opportu-nity to reduce variation and create safe and preferable alternatives there with a much greater potential for cost savings.”
Click and Connect! Access the links in EMN by reading this issue on our website or in our iPad app, both available on www.EM-News.com.
Reduce ed use
Continued from page 1
LWW-EMN_March 2014_Layout.indd 11 07/02/14 12:35 AM