Embed Size (px)
Citation preview

Inflammatory Bowel Disease (IBD): Evolution of Surgical Methods
Charles A. Ternent, MDAssociate Clinical Professor of Surgery and
Director Colorectal Surgery Research, Creighton University School of Medicine, Omaha Nebraska

IBD: Surgical Treatment
• Indications for Surgery– Elective• Intractability• Risk of malignant change• Growth retardation• Local anorectal complications (fissures, abscesses and
fistulas)• Remote or systemic complications (arthritis, skin
lesions – pyoderma and erythema nodosum, eye lesions (uveitis, iritis)

IBD: Surgical Treatment
• Indications for Surgery– Urgent / Emergent • Deterioration patient’s condition (Fulminant colitis)• Local abdominal signs suggestive of perforation• Acute colonic dilatation (Toxic megacolon)
– Surgical approach variable over the decades• Ileostomy/cecostomy alone 50% mortality (Crile and
Thomas 1951)• Colectomy and ileostomy (Gardner and Miller 1951)
– Subtotal colectomy and ileostomy recommended

Ulcerative Colitis: Early Surgical Treatment
– Operations on the Nervous System (Historical perspective only)
• Schlitt 1951: operative division of the pelvic autonomic nerves (permanent sexual and bladder dysfunction)
• Levy 1956: prefrontal lobotomy report in 5 patients– “Some” improved

Ulcerative Colitis: Early Surgical Treatment
• Appendicostomy (Keetly 1895)– Simple procedure intended for very ill colitis
patients– Appendix brought up through abdominal wall
and catheter passed into cecum and used to irrigate colon
– Lockhart-Mummery 1934 reported on 79 cases• 12 deaths, rest “very satisfactory “results but ? cyclical
disease factors• Use abandoned circa 1940 in favor of ileostomy

Ulcerative Colitis: Early Surgical Treatment
• Diverting Ileostomy or Cecostomy with Subsequent Excision of the Large Intestine (Brown 1913)– Adopted in US 1920s-1940s (Strauss 1924, Cattell
1935, Lahey 1941). UK 1940s (Ogilvie 1940)– Rationale: Resting colon to allow quiescence and
possible reversal of stoma– Cattell 1948 reported ileostomy invariably
permanent and colectomy required due to failure of recovery or because of cancer risk

Ulcerative Colitis: Early Surgical Treatment
• Diverting Ileostomy with Excision of the Large Intestine (Proctocolectomy) in Stages– Gabriel 1952 reported three-stage procedure in
3-month intervals• Ileostomy (initially affected bowel left in place)• Subtotal colectomy with exteriorization sigmoid colon• Abdominoperineal resection rectosigmoid colon
– Additive morbidity and mortality from serial operations (not an efficient approach with present day anesthesia)

Ulcerative Colitis: Early Surgical Treatment
• Ileostomy with Immediate Subtotal Colectomy or Proctocolectomy (Miller 1949 and Crile and Thompson 1951)– Rationale: Minimize toxicity of septic colon left in
place especially in more toxic cases– Concern: Increased mortality in toxic patients and
increased morbidity from proctectomy in patients on high dose steroids and biologic agents• Toxic/compromised physiology – subtotal colectomy with
ileostomy• Elective refractory – proctocolectomy with ileostomy

Ulcerative Colitis Early Surgical Treatment: Colectomy with Ileostomy
Early Studies of Urgent/Emergent Colectomy for UC
Mortality Urgent / Emergent
Mortality Elective
N Urgent / Emergent
Lennard-Jones 1960 31% 4.4% 32
Brooke and Sampson 1964
16% 6% 62
Goligher 1970 14% 3% 184

Ulcerative Colitis: Early Surgical Treatment
• Techniques of Ileostomy • Initially ileostomy brought out 5 cm or so
straight and allowed serosal surface to granulate (no eversion)
• Commonly resulted in fibrosis, stenosis and partial obstruction or ileostomy dysfunction (Counsell and Goligher 1952)• Dragsted 1941 skin grafted serosal surface ileostomy
above skin level – contraction and stenosis still a problem

Ulcerative Colitis: Early Surgical Treatment
• Techniques of Stoma Creation– Patey 1951 advocated immediate suture of stoma
bowel to skin (flat stoma a problem with ileostomy)– Brooke 1952 adopted immediate mucocutaneous
suture in constructing ileostomies with evertion of the last 1-2 cm of ileal wall to create projection (standard of care today)
– Turnball 1953 would strip the terminal ileal portion of serosa and muscularis before eversion (technically difficult and without significant advantage)

Ileostomy Appliances
• Incontinent stomas require constant wearing of an appliance (early on a bag or box)
• Koenig 1944 patient of Strauss in Chicago developed the adherent ileostomy bag along with Rutzen– Water tight and leak resistant arrangement
• Turnbull 1975 introduced karaya gum powder to minimize leakage– Paste or wafer has soothing and efficient adhesive
• Stomahesive paste further enhanced stoma care

Ulcerative Colitis: Early Surgical Treatment
• Continent – Reservoir Ileostomy (Koch 1969 Goteburg, Sweden)
• Internal pouch created out of 45-50 cm of ileum immediately above stoma
• Continent valve requires intubation through abdominal wall to evacuate
• No stoma appliance required. Cover with gauze• Valve can slip and leak and complication and
revision rates high

Ulcerative Colitis: Early Surgical Treatment
• Diverting Transverse or Left Sided Colostomyafter distal proctocolectomy– Possible in very distal disease– High incidence of extending disease to involve
proximal colon– Staghlgren and Ferguson 1959 reported on 18
patients with this procedure. 11 required completion colectomy and ileostomy

Ulcerative Colitis: Early Surgical Treatment
• Colectomy with Ileosigmoid (Lilienthal 1903, Devine 1943,1948)– Extraperitoneal technique– Gabriel 1952 reported that 4/5 required
separation of anastomosis and ileostomy• Ileorectal Anastomosis (Aylett 1953-1963)– End to end ileorectal anastomosis with protecting
loop ileostomy for 3 weeks• FU 1963 N=123, 5% mortality, 13% conversion to
ileostomy

Ulcerative Colitis Early Surgical Treatment Ileorectal Anastomosis
• Jagelman 1953 Postal inquiry of 200 of Aylett’s patients• 25% had 6 or more stools per day• 90% considered surgery successful
• Literature 1954-1977 (Goligher, Wangensteen…)– 20-50% failure rate requiring ileostomy– 7/350 patients followed 10-15 years developed carcinoma– Goligher: reserve for patients with lesser degrees of rectal
involvement who are not interested in rectal excision or stoma
– Currently mainly considered in mild rectal disease, indeterminate colitis, high risk or older patients not good candidates for IPAA

Ulcerative Colitis: Early Surgical Treatment
• Colectomy and Partial Rectal Excision with Ileoanal Pull-Through (Ravitch 1948)– Anal mucosectomy and straight ileoanal
anastomosis– Others found great frequency of defecation and
incontinence (Goligher 1951, Wangenstein 1948)– 7-8+ BMs per day– Goligher 1980: More promising proposition
would be an ileoanal reservoir…

Ulcerative Colitis: Modern Surgical Treatment
• Proctocolectomy with Ileoanal Pouch Anal Anastomosis (IPAA)– IPAA and protecting ileostomy • Ferrari and Fonkalsrud 1978 report of successful
operation• Parks and Nichols 1978 report of 5 patients with colitis
treated with IPAA with encouraging results

Ulcerative Colitis: Modern Surgical Treatment
• Quality of life / functional issues: Proctocolectomy with permanent ileostomy vs IPAA– IPAA was associated with a significantly better perception of
body image than a permanent stoma– Quality of life in general was similar in both groups– Patients with a pouch had more long-term complications
than patients with an ileostomy within the same period of time (52.6% vs. 26.3%)
– The median number of stages for pouch construction was two, compared to a median of one stage for an ileostomy (P<0.0001).
– Counsel thoroughly preoperativelyJ Clin Gastroenterol. 2006 Sep;40(8):669-77.Quality of life after proctocolectomy with ileoanal anastomosis for patients with ulcerative colitis.Lichtenstein GR1, Cohen R, Yamashita B, Diamond RH

Ulcerative Colitis: Modern Surgical Treatment
• Restorative Proctocolectomy and IPAA• One, two or three stages? – High dose steroids / biologics, urgent/emergent
surgery increase risk of infection (3 stage)– No high risk of infection (2 stage)– No steroids or biologics and elective (possible 1
stage in some centers but potential drawbacks/risks)

Ulcerative Colitis: Modern Surgical Treatment
• Laparoscopic approaches to Proctocolectomy with permanent ileostomy and IPAA
• Is there a benefit to minimally invasive techniques?– Less blood loss– Diminished postop pain– Reduced narcotic requirement– Shorter hospital stays

Ulcerative Colitis: Modern Postoperative Issues
• Pouchitis after IPAA for UC– Most common long-term complication (25%)– Usually responds to PO antibiotics (Cipro/Flagyl)– 60% second episode– 20% chronic pouchitis (chronic maintenance
therapy – combination therapy and Rifaximin)– Budesonide and Biologics (Infliximab), VSL-3
(probiotic)– May need pouch revision or excision

Ulcerative Colitis: Modern Postoperative Issues
• Crohn’s disease (CD) and IPAA: Outcomes– One of most common long-term inflammatory complications– Leading cause of pouch failure (10% if CD known preop and
carefully selected / 50% if CD develops postop)– Treatment
• Topical / oral mesalamine or steroids• Antibiotics • Immunomodulators• Biologics may be considered in refractory disease of IPAA particularly if
extra-intestinal symptoms• Consider pouch excision - revision

Crohn’s Disease: Early Reports
• Non-specific enteritis descriptions– Moynahan 1907, Mayo-Robson 1908, Leeds and
Dalziel 1913– Burrill Crohn NY 1932 established the clinical and
pathologic entity of regional or granulomatous enteritis • Anywhere in GI tract • Skip lesions

Crohn’s Landmark Paper

Crohn’s Disease: Evolution of Surgical Treatment
• Diverting stoma• Bypass with or without exclusion• Resection with stoma• Resection with anastomosis +/- stoma• Stricturoplasty +/- resection• Radical vs conservative resection of bowel
and mesentery (resect to grossly not microscopically normal tissue)

Crohn’s Disease: Early Surgical Treatment
• Bypass with exclusion advocated in mid 1930s (Mount Sinai Hospital, NY)
• President Eisenhower had successful bypass without exclusion for Crohn’s (Heaton et al 1964)
• Surgical resection popularized with increasing safety of surgery (Glotzer and Siren 1971)
• Clear indication for bypass operation alone is duodenal Crohn’s (Fielding et al 1970)

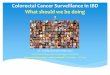
Crohn’s Disease and Fistula-in-Ano
• Fistula Definition– Abnormal communication/tract between any
two epithelium lined surfaces– Presence of a rectal or anal internal opening
• Etiology– Most common result of cryptoglandular
infections – IBD/Crohn’s, Infectious, Cancer, HIV and other
immunocompromised states

MRI Complex Anterior Fistula-in -Ano

Classification of Anal Fistulas

Anal Fistula in Ancient GreeceHippocrates (ca. 460-370 BC)
• Aware of anorectal fistulas and tried to interpret mechanism of origin (first description)• Attempted to treat them conservatively using
laxatives and purgative medications or surgically via anoscope
• Understood importance of the surgical option but lacked appropriate tools
• Numerous operations exist• Aim to decrease recurrence and incontinence rates

Louis 14th
17th Century France• Had anal fistula in 1686
at age 47 after developing an abscess in the “Foundation” from riding horses
• Recurrent abscesses made it impossible for the King to walk
• Surgery as we know it today did not exist
• Difficult for the King to adopt majestic airs

Francois Felix: A Great Barber-Surgeon and The Royal Anus
• Born in Avignon c 1635• Developed technique to perform an
operation on the monarch after practicing with peasants/prisoners at King’s request• Found that addressing the internal fistula
opening was key to the operation while preserving life and anal sphincter continence

Francois Felix: A Great Barber-Surgeon and The Royal Anus
• SETONOne or more threads or horsehairs or a strip of linen introduced beneath the skin by a knife or needle to provide drainage or to produce or prolong inflammation
?

Francois Felix: A Great Barber-Surgeon and The Royal Anus
• The King required 4 operations for healing of fistula (staged fistulotomies with setons)
• Back to riding horses by 3 months• Felix was knighted, bought a town (Tassy) and asked
that the barber trade be separated from surgery• Became the surgeon of the Sun King• Had PTSD from ordeal and apparently was not able to
touch a scalpel thereafter• Helped to establish the French Royal Academy of
Surgery in 1731 under King Louis XV

Crohn’s Disease: Anorectal Fistula Modern Surgical/Medical Treatment
• Drain abscess if present• Drain fistulas with setons to minimize
festering and abscess recurrence as immunomodulator and biologic agents started
• As fistula tracts dry up and therapy effective can remove setons (may have to replace and re-drain depending on CD activity

Crohn’s Disease: Modern Surgical Treatment
• Fissure– Pain and bleeding can be excruciating and may
be main complaints of CD– May be atypical, lateral or associated with
edematous skin tags (CD)– Maximize medical management when active
disease related fissures and symptoms usually improve
– Surgery only if not CD related and no active CD and anal sphincter hypertonic

IBD: Modern Surgical Treatment
• Timing of Surgery: Immunomodulator Biologic and Steroid Therapy– Ulcerative Colitis: high dose steroids and
biologics increase infection risk – stage colectomies
– Crohn’s Disease: literature on biologics controversial – time surgery around biologic dose to maintain optimized medical management. Steroids and biologic combinations increase risk of infection

IBD Surgery Conclusions
• Extensive progress over last 100+ years• Future: Genotype-phenotype correlations
may help guide surgery and medical therapy • Continued improved medical management
will continue to compliment evolving surgical techniques and capabilities
• The Cure…