Embed Size (px)
Citation preview

© Clinical Chemistry
Infectious Lymphadenopathies
Teresa Scordino MD
University of Oklahoma Health Sciences Center
DOI: 10.15428/CCTC.2018.288654

2
Patterns of lymphoid hyperplasia
• Follicular pattern- Follicular hyperplasia
- Syphilis
- HIV lymphadenopathy
- Castleman disease
- Progressive transformation of
germinal centers
• Sinus pattern- Sinus histiocytosis
- Rosai Dorfman disease
- Hemophagocytic syndrome
• Diffuse pattern- Some cases of HSV, EBV
• Paracortical / mixed pattern- EBV lymphadenitis
- HSV lymphadenitis
- Granulomatous lymphadenitis
- Dermatopathic lymphadenopathy
- Drug reaction
- Toxoplasmosis
• Necrosis- HSV
- Cat scratch disease
- Kikuchi Fujimoto disease
- Lupus lymphadenitis

3
• Acute phase
o Neutrophilic infiltrate
o Microabscesses → may coalesce into larger abscesses
• Later stages
o Chronic inflammation
o Histiocytes
Bacterial lymphadenitis - general

4
• Numerous causeso Infection
– Tuberculosis and other mycobacteria
– Leishmania
– Fungal infection
– Cat scratch disease
– Lymphogranuloma venereum
o Noninfectious syndromes (sarcoidosis)
o Foreign material
o Malignancy
– Classical Hodgkin lymphoma, T cell lymphomas, and other malignancies
Granulomatous lymphadenitis

5
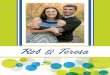
• Histoplasma capsulatum
o Granulomatous inflammation, often necrotizing
o 2-4 m, narrow-based budding yeast
• Cryptococcus neoformans
o Granulomatous inflammation
o Clear spaces may be visible around organisms
• Coccidioides immitis
o Granulomatous inflammation
o Large spherules containing small endospores
Fungal lymphadenitis
Histoplasma, GMS stain
Coccidioides immitisPhoto courtesy of Kristian Schafernak

6
Mycobacterium tuberculosis lymphadenitis
• Lymph nodes are the second most commonly involved site
• Necrotizing granulomas
M. tuberculosisPhoto courtesy of Kristian Schafernak

7
Atypical Mycobacterial lymphadenitis
• Atypical mycobacteria• M. avium, M. marinum,
M. kansasii
• Necrotizing and non-necrotizing granulomas
• Foamy macrophages
M. avium, AFB stain

8
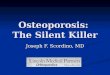
• Cat scratch disease
• Lymphadenopathy 1-3 weeks after exposure
• Early: small abscesses, follicular hyperplasia
• Late: large stellate necrotizing granulomas -abscesses surrounded by palisading histiocytes
• Warthin-Starry, IHC may reveal organisms
• PCR, serology
Bartonella henselae lymphadenitis
Palisading
histiocytes
Neutrophils

9
• Chlamydia trachomatis serovars L1-L3
• May be preceded by genital ulcer
• Unilateral tender enlargement of regional
nodes
• Morphologically similar to cat scratch
lymphadenitis
Lymphogranuloma venereum lymphadenitis

10
• Immunosuppressed patients
• Bartonella infection with associated vascular proliferation
• Skin lesions often present
• Nodular proliferation of small vessels
• Mild endothelial atypia
• Extravasated RBCs
• Granular material visible on H&E (arrow)
Bacillary angiomatosis

11
• Primary infection: typically involves nodes near site of primary infection (inguinal > cervical)
• Secondary infection: generalized lymphadenopathy
• Follicular hyperplasia
• Paracortical expansion with small lymphocytes, plasma cells, immunoblasts
• Thickening of capsule
• Perivascular lymphoplasmacytic infiltrate
Syphilitic lymphadenitis
Plasma cells

12
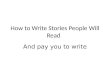
Toxoplasma lymphadenitis
Reactive germinal center
Monocytoid B cells
Epithelioid histiocytes
Epithelioid histiocytes
encroaching on GC

13
• Lymph node findings vary with stage of disease
• Pattern A
o Follicular hyperplasia
o Monocytoid B cells may be present
• Pattern C
o Small, regressed follicles
o Increased interfollicular plasma cells
• Pattern B
o Intermediate between patterns A and C
HIV lymphadenitis

14
• Frequently involves cervical lymph nodes
• Follicular hyperplasia
• Paracortical expansion
o Variably-sized lymphocytes, immunoblasts,
plasma cells
o Sheets of immunoblasts, RS-like cells may be
seen
• Necrosis may be present
Epstein-Barr virus lymphadenitis

15
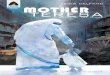
Epstein-Barr virus lymphadenitis
Immunoblasts
Necrosis
Reed-Sternberg-like cell
EBER

16
• Hyperplastic follicles may be present
• Paracortical expansion with lymphocytes, plasma cells, immunoblasts
• Diffuse areas of necrosis with karyorrhectic debris, neutrophils
• Viral cytopathic effect
• Association with CLL/SLL
Herpes simplex lymphadenitis
HSV IHC
Necrosis
Viral cytopathic
effect

17
• Infection is a common cause of
lymphadenopathy
• Familiarity with the features of infectious
lymphadenopathies is important
o Helps prevent misdiagnosis of malignancy
o Gives the clinician a specific diagnosis
o Helps direct appropriate further testing and
management
Conclusions

18
References
1. Asano S. Granulomatous lymphadenitis. J Clin Exp Hematopathol 2012;52(1):1-16.
2. Lin MH, Kuo TT. Specificity of the histopathological triad for the diagnosis of toxoplasmic lymphadenitis: polymerase chain reaction study. Pathol Int. 2001;51(8):619-23.
3. Loissant A, Ferry JA, Soupir CP, Hasserjian RP, Harris NL, Zukerberg LR. Infectious mononucleosis mimicking lymphoma: distinguishing morphological and immunophenotypicfeatures. Mod Pathol 25(8):1149-59 2012
4. Medeiros LJ, Lin P, Miranda RN. Infectious mononucleosis. In: Diagnostic Pathology: Lymph Nodes and Extranodal Lymphomas, Second Edition. Elsevier, PA 2018: 78-83.
5. Miranda RN, Khoury JD, Medeiros LJ. Cat scratch lymphadenitis. In: Atlas of Lymph Node Pathology, Atlas of Anatomic Pathology, Springer, NY, 2013: 35-36.
6. Miranda RN, Khoury JD, Medeiros LJ. Fungal lymphadenitis: Histoplasma, Cryptococcus, and Coccidioides. In: Atlas of Lymph Node Pathology, Atlas of Anatomic Pathology, Springer, NY, 2013: 53-57.
7. Miranda RN, Muzzafar T, Medeiros LJ. Human immunodeficiency virus lymphadentitis. In: Diagnostic Pathology: Lymph Nodes and Extranodal Lymphomas, Second Edition. Elsevier, PA 2018: 122-131.
8. Pittaluga, S. Viral-associated lymphoid proliferations. Semin Diagn Pathol. 2013 May ; 30(2): 130–136.
9. Salem A, Loghavi S, Khoury JD, Agbay RL, et al. Herpes simplex infection simulating Richter transformation: a series of four cases and review of the literature. Histopathology 2017;70(5):821-831
10. Zangwill KM. Cat scratch disease and other Bartonella infections. Adv Exp Med Biol2013;764:159-66

19
Disclosures/Potential Conflicts of Interest
Upon Pearl submission, the presenter completed the Clinical Chemistry
disclosure form. Disclosures and/or potential conflicts of interest:
▪ Employment or Leadership: No disclosures
▪ Consultant or Advisory Role: No disclosures
▪ Stock Ownership: No disclosures
▪ Honoraria: No disclosures
▪ Research Funding: No disclosures
▪ Expert Testimony: No disclosures
▪ Patents: No disclosures

Thank you for participating in this
Clinical Chemistry Trainee Council
Pearl of Laboratory Medicine.
Find our upcoming Pearls and other
Trainee Council information at
www.traineecouncil.org
Download the free Clinical Chemistry app
on iTunes today for additional content!
20
Follow us: