Embed Size (px)
Citation preview
Surveillance of Infection and Data Collection Page 1 of 16 Version 2.0 January 2019
Why we have a procedure?
Adherence to this procedure will ensure the Trust meets its statutory obligation to report alert organisms, and other HCAI, to the regulatory bodies. It will also provide evidence of local surveillance and the use of comparative data in the monitoring of infection rates. Timely reporting of this data to clinical areas should assist in the reduction of any healthcare associated infection. It will also ensure compliance with the Health and Social Care Act 2008: Code of Practice for the NHS for the Prevention and Control of Healthcare Associated Infections (revised January 2015). This document has been developed to provide a framework to:
Monitor the incidence of infection.
Provide early warning and investigation of problems and subsequent planning and intervention to control infection.
Monitor trends, including the detection of outbreaks.
Examine the impact of interventions.
Ensure compliance with mandatory surveillance systems.
Assist the IPCT and the Infection Prevention and Control Committee to identify risks of infection and reinforce the need for good practice.
What overarching policy the procedure links to?
This procedure is supported by the Infection Prevention and Control Assurance Policy
Which services of the trust does this apply to? Where is it in operation?
Group Inpatients Community Locations
Mental Health Services all
Learning Disabilities Services all
Children and Young People Services all
Who does the procedure apply to?
1. The Director of Infection Prevention and Control (DIPC) is responsible for providing reports on the surveillance of infection directly to the Chief Executive and the Trust Board. The CEO is required to sign off infection data collected via the HCAI DCS on the 15th of each month (this is usually undertaken in acute trust organisations).
Infection Prevention and Control Assurance - Standard Operating Procedure 3 (IPC SOP 3)
Surveillance of Infection and Data Collection
Surveillance of Infection and Data Collection Page 2 of 16 Version 2.0 January 2019
2. The Infection Prevention and Control Committee is responsible for approving this procedure and monitoring compliance.
3. The Group/Divisional Management Teams are responsible for reviewing data relating to their Division and ensuring appropriate actions are being taken e.g. investigations into cases of C.difficile infection are undertaken using principles of root cause analysis, action plans formulated and learning shared monitoring any action plans through the Group/Divisional Governance Group.
4. Line Managers are responsible for the implementation of and compliance with this procedure within their own clinical area and reporting incidents of infection/ outbreaks etc. to the IPCT
5. Ward/Unit Managers are responsible for ensuring weekly in-patient infection surveillance data form is submitted weekly (every Monday by 10am) to the IPCT using the on-line data collection form: http://luna.smhsct.local/documents/trust-forms/1757-weekly-infection-surveillance-data-returns
6. The Medical Microbiologist is responsible to ensure that appropriate tests are available to support surveillance activities and test results are reported promptly to the relevant Clinicians responsible for the care of the patient/staff member. In addition via an enhanced surveillance system, information is collected via a web-based surveillance system (Healthcare Associated Infection Data Capture System (HCAI DCS)) which is reported nationally).This system collects mandatory reporting data on the following HCAIs: - MRSA bacteraemia - MSSA bacteraemia - E.coli bacteraemia - Pseudomonas aeruginosa bacteraemia - Klebsiella spp. bacteraemia - Clostridium difficile infection This enhanced data provides a platform to identify potential interventional targets and provides robust local and national data with the potential for benchmarking and comparison within organisations and regions over time.
7. The Infection Prevention and Control Team (IPCT) is responsible for:
a) Co-ordinating surveillance activities.
b) Collating the data and feeding back surveillance data to wards/departments and advising on specific infection prevention and control procedures to minimise risk of transmission and monitor trends.
c) Ensuring that data required as part of the mandatory surveillance programme are reported on the PHE web based HCAI data capture system and is ‘signed off’ by the 15th of each month (with the Acute Trust entering the data as/ when necessary).
d) Producing surveillance reports to relevant committees and groups.
e) Co-ordinating post infection reviews following incidents of bacteraemia or C. difficile.
f) Supporting the investigation of, and learning from other types of health care associated infection as relevant.
g) Investigating suspected incidents of cross infection and outbreaks.
Surveillance of Infection and Data Collection Page 3 of 16 Version 2.0 January 2019
8. Clinicians – the Clinician in charge of the patient has a statutory duty to report notifiable communicable diseases to the Consultant in Communicable Disease Control at Public Health England, Midlands and East Regional Office.
9. Individual staffs have a responsibility to actively participate in systems of surveillance as required by the IPCT and know how/when to contact the IPCT to notify them of any HCAIs, alert conditions, potential outbreaks or areas for concern.
All staffs have a responsibility for ensuring that the principles outlined within this document are universally applied.
When should the procedure be applied?
These procedures outline the Trust’s infection prevention surveillance and reporting processes, and the methods used to ensure timely reporting of Healthcare Acquired Infections (HCAI) to Public Health England (PHE). Surveillance provides good information to patients and clinical teams and is the cornerstone of infection control (DH 2003). It consists of the routine collection of data on infections among patients or staff, its analysis and the dissemination of the resulting information to those who need to know, so that appropriate action can result. Surveillance also forms part of clinical audit and clinical governance: it assists in reducing the frequency of adverse events such as infection or injury. High quality information on infectious diseases, healthcare associated infection and antimicrobial resistant organisms is essential for monitoring progress, investigating underlying causes and applying prevention and control measures (DH, 2003). Definitions
Alert organisms Alert organisms are identified in the microbiology laboratory and include organisms of clinical interest within a health care setting that may result in infection for the patient e.g. MRSA, Glycopeptide Resistant Enterococci (GRE), Extended Spectrum Betalactamases (ESBLs) and other multi-resistant organisms, Clostridium difficile, Norovirus and may result in outbreaks (see Appendix 1)
Alert conditions Alert conditions for example infectious diseases e.g. diarrhoea/vomiting, Chickenpox/Shingles, Infestations etc. (see Appendix 1)
Bacteraemia Organisms present in the bloodstream that may cause infection.
CDI Clostridium difficile infection (CDI) detected by a positive test for Clostridium difficile. Symptoms include diarrhoea.
HCAI data capture system
Web based computer database for recording HCAI episodes of bacteraemia and Clostridium difficile. The database is managed by Public Health England (PHE).
Surveillance of Infection and Data Collection Page 4 of 16 Version 2.0 January 2019
Healthcare associated infection (HCAI)
Infection acquired by a patient as a result of contact with a healthcare provider.
Invasive devices Includes all devices that break through the skin.
Multi-resistant organism Microbiological organisms resistant to common antimicrobials.
Notifiable diseases Diseases notifiable to local authority proper officers under the Health Protection (Notification) Regulations 2010. This is a legal term denoting diseases that must by law be reported to the “proper officer” i.e. the Consultant in Communicable Disease Control (CCDC) who is based at the Regional Public Health office.(see Appendix 2 for list of diseases) It is the responsibility of the Doctor in charge of the patient to make the notification.
Root Cause Analysis (RCA)
Root Cause Analysis (RCA) is a formal investigation following an incident using a specific format ending in action plan. (See IPC SOP 18: Undertaking a post infection review).
Surveillance Surveillance is a systematic method for continuous monitoring of diseases in a population in order to be able to detect changes, analyse the data, disseminate the results and put into practice effective prevention and control mechanisms.
Surveillance - Laboratory The Trust will agree with the Local Microbiology Laboratory and with the advice of the Consultant Microbiologist the organisms which will be reported by the Laboratory to the IPCT e.g. alert organisms (reviewed annually).
Surveillance - Mandatory Some surveillance is mandatory MRSA bacteraemia and Clostridium difficile positive data are used by the DH and the CQC as infection control performance indicators. The Trust must comply with all requests for Mandatory Surveillance of Healthcare associated Infection in accordance with the requests made by the Department of Health.
Surveillance - Targeted Refers to the collection of data on healthcare associated infections occurring in a defined subgroup, such as those on a particular ward, those undergoing a particular procedure or those acquiring a particular infection.
Surveillance - Voluntary The IPC Committee decides on specific surveillance programmes to undertake in response to local need.
How to carry out this procedure
All surveillance systems have four key components (DH/PHLS, 1995): 1. Data collection using standard case definitions
Surveillance of Infection and Data Collection Page 5 of 16 Version 2.0 January 2019
2. Collation of data
3. Analysis and interpretation of the data
4. Timely dissemination of information to clinical teams
Alert organisms and alert conditions are those that may cause outbreaks. The IPCT will provide advice on the control measures and management of cases and will investigate clusters of cases. It is the responsibility of the clinical team to access and follow up any microbiology results for their patients in a timely manner.
Some national surveillance schemes are mandatory, others are voluntary. Surveillance Objectives and Process Objectives of Surveillance
Assessment of infection incidence over a period of time.
Timely investigation and instigation of prevention and control measures.
To assess the effectiveness of prevention and control measures and interventions.
The prevention and early detection of outbreaks.
Mandatory reporting to Department of Health where applicable. Surveillance Process
Yearly plan agreed by the IPC Committee and reported in the Infection Prevention Annual Work-plan and Annual Report.
Data collection using standard definitions by IPCT.
Analysis and interpretation of data by IPCT.
Reports produced using standard formats.
Feedback of surveillance data by IPT.
Incidence reports produced for Group/Divisions performance management information via the Governance Assurance Unit for action by Clinical Teams and the IPCT.
Reporting Mechanisms
See IPC SOP 4: Reporting Incidents of Infection to Public Health England or the Local Authority, for further details.
Appendix 3 explains the surveillance processes used within the Trust.
Additional Information/ Associated Documents
Infection Prevention and Control Assurance Policy.
Infection Prevention and Control Assurance - Standard Operating Procedure 5 IPC SOP 5: Recognition and Management of Outbreaks
Infection Prevention and Control Assurance - Standard Operating Procedure 4 IPC SOP 4: Reporting incidents of infection to PHE or the Local Authority
National enhanced mandatory surveillance of Gram-Negative Bacteraemia https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/725648/HCAIDCS_Gram_Negative_2017_Submission_Form.pdf (accessed January 2019)
Surveillance of Infection and Data Collection Page 6 of 16 Version 2.0 January 2019
Update on the reporting and monitoring arrangements and post-infection review process for MRSA bloodstream infections (March 2018) (accessed January 2019)
https://improvement.nhs.uk/documents/2512/MRSA_post_infection_review_2018_changes.pdf
Mandatory Healthcare Associated Infection Surveillance: Data Quality Statement (June 2018) https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/713604/Mandatory_Healthcare_Associated_Infection_Surveillance_Data_Quality_Statement.pdf (accessed January 2019)
Hospital Norovirus Outbreak Reporting Tool http://bioinformatics.phe.org.uk/noroOBK/
(accessed January 2019)
Clostridium difficile infection objectives for NHS organisations in 2018/19, guidance on sanction implementation and notification of changes to case attribution definitions from 2019 (March 2018) https://improvement.nhs.uk/documents/808/CDI_objectives_18_19_FINAL_Oct2018.pdf (accessed January 2019)
Department of Health (2015) The Health and Social Care Act 2008: code of practice on the prevention and control of infections and related guidance. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/449049/Code_of_practice_280715_acc.pdf (accessed January 2019)
Department of Health (2003) Winning ways. Working together to reduce Healthcare Associated Infection in England. Report from the Chief Medical officer. London. DH. Available at: http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/publicationsandstatistics/publications/publicationspolicyandguidance/dh_4064682 (accessed
January 2019)
Where do I go for further advice or information?
Infection Prevention and Control Team
Your Service Manager, Matron, General Manager, Head of Nursing, Group Director
Your Group Governance Staff Training Staff may receive training in relation to this procedure, where it is identified in their appraisal as part of the specific development needs for their role and responsibilities. Please refer to the Trust’s Mandatory and Risk Management Training Needs Analysis for further details on training requirements, target audiences and update frequencies. Monitoring / Review of this Procedure In the event of planned change in the process(es) described within this document or an incident involving the described process(es) within the review cycle, this SOP will be reviewed and revised as necessary to maintain its accuracy and effectiveness.
Equality Impact Assessment Please refer to overarching policy
Data Protection Act and Freedom of Information Act Please refer to overarching policy
Surveillance of Infection and Data Collection Page 7 of 16 Version 2.0 January 2019
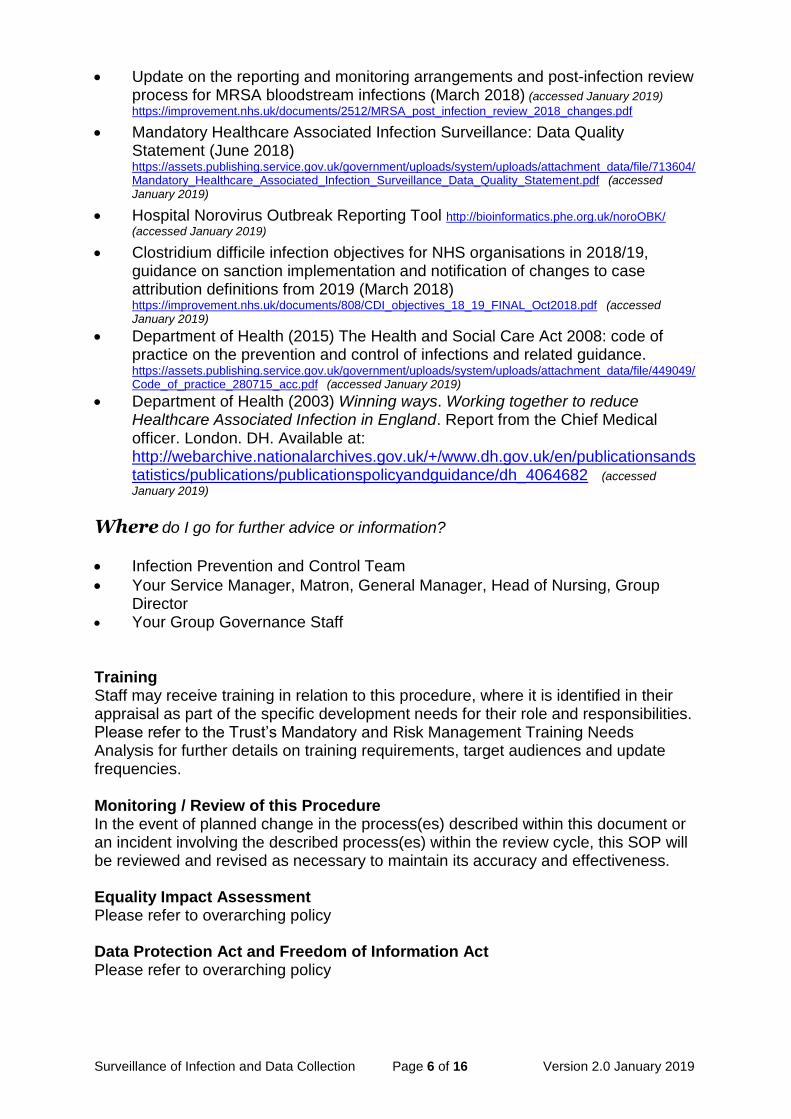
Appendix 1
Alert Organisms and Alert Conditions NB This list is not exhaustive and all incidents of infection, infestation, suspected outbreak etc. must be reported to the Infection Prevention and Control Team.
Alert Organisms Alert Conditions
Acinetobacter Adenovirus Campylobacter Carbapenamase producing
enterbacteraciae (CPE) Clostridium difficile Coronavirus Creutzfeldt Jakob Disease (CJD) Cryptosporidium Escherichia coli 0157 Escherichia coli bacteraemia Extended spectrum beta lactamase
producers (ESBLs) Gardia Glycopeptide resistant enterococci
(GRE) Haemophilus influenza (Type B) Influenza virus Legionalla spp. Meticillin-resistant Staphylococcus
aureus (MRSA) as colonization or infection
Meticillin Sensitive Staphylococcus aureus (MSSA) bacteraemia
Middle Eastern Respiratory Syndrome (MERS)
Multi-resistant Gram negative bacilli Neisseria Norovirus Parvovirus Penicillin resistant Streptococcus
pneumoniae Respiratory syncytial virus Rotavirus Salmonella or Shigella spp Streptococcus pyogenes (Beta
Haemolytic Group A) Streptococcus agalactiae (Strep
group B) Varicella zoster Any unusual bacteria
Acute rash illness Cellulitis Chickenpox Diarrhoea and/or vomiting Diarrhoea with blood (dysentery) Diphtheria Food poisoning Hepatitis B Hepatitis C Infestations e.g. Scabies/head lice Influenza Measles Meningitis Meningococcal septicaemia Mumps Ophthalmia neonatorum Poliomyelitis Pyrexia of unknown origin with history of
foreign travel Rubella Scarlet fever Shingles Soft tissue infections including
nectrotising fasciitis Suspected legionellosis Suspected outbreaks Tuberculosis (chronic productive cough) Typhoid and paratyphoid fevers Viral hepatitis Viral haemorrhagic fever Whooping cough
Surveillance of Infection and Data Collection Page 8 of 16 Version 2.0 January 2019
Appendix 2
Notifiable Infectious Diseases
Diseases that are notifiable are:
Acute encephalitis
Acute infectious hepatitis
Acute meningitis
Acute poliomyelitis
Anthrax
Botulism
Brucellosis
Cholera
Diphtheria
Enteric fever (typhoid or paratyphoid fever)
Food poisoning
Haemolytic uraemic syndrome (HUS)
Infectious bloody diarrhoea
Invasive group A streptococcal disease
Legionnaires’ disease
Leprosy
Malaria
Measles
Meningococcal septicaemia
Mumps
Plague
Rabies
Rubella
Severe Acute Respiratory Syndrome (SARS)
Scarlet fever
Smallpox
Tetanus
Tuberculosis
Typhus
Viral haemorrhagic fever (VHF)
Whooping cough
Yellow fever
Report other diseases that may present significant risk to human health under the category ‘other significant disease’.
N.B. ALL the diseases listed above MUST be notified to the Infection Prevention and Control Team IMMEDIATELY in addition to the local Public Health England Area Office:
West Midlands West HPT, 2nd Floor, Kidderminster Library Market Street Kidderminster Worcestershire DY10 1AB Phone: 0344 225 3560 (option 2) (Out of hours for health professionals only: please phone 01384 679 031)
Notification Form: https://www.gov.uk/government/publications/notifiable-diseases-form-for-registered-medical-practitioners (accessed January 2019)
Surveillance of Infection and Data Collection Page 9 of 16 Version 2.0 January2019
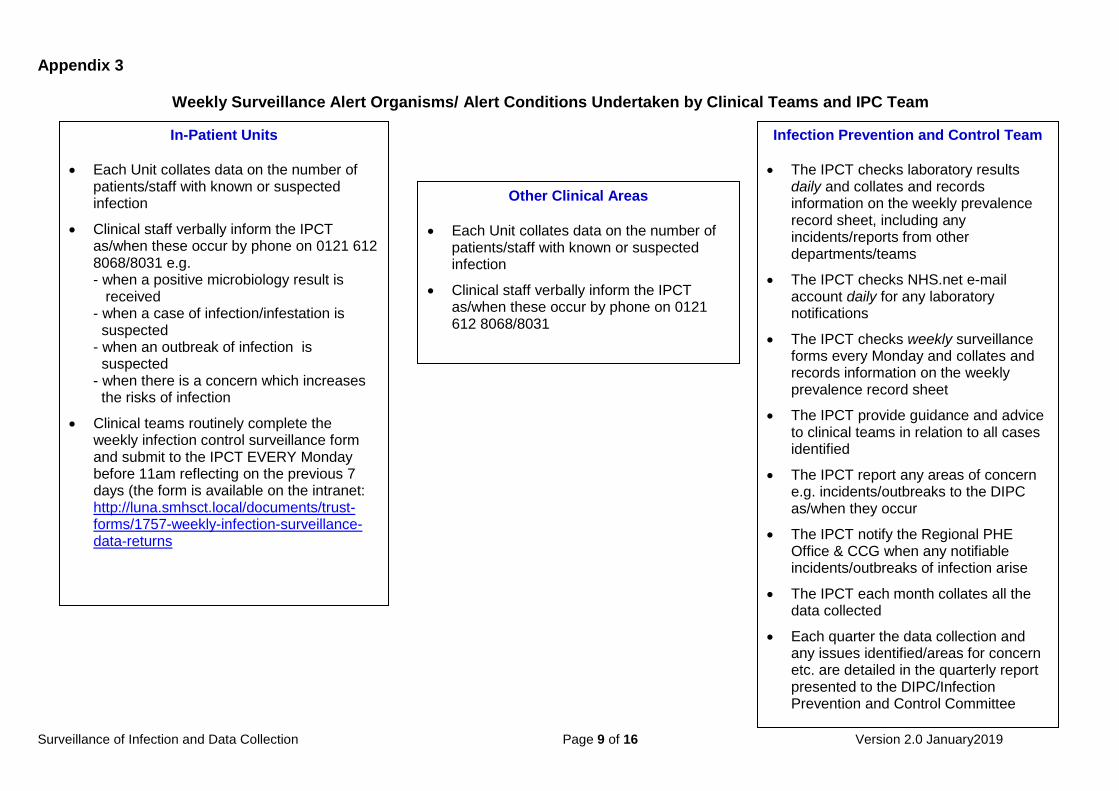
Appendix 3
Weekly Surveillance Alert Organisms/ Alert Conditions Undertaken by Clinical Teams and IPC Team
In-Patient Units
Each Unit collates data on the number of patients/staff with known or suspected infection
Clinical staff verbally inform the IPCT as/when these occur by phone on 0121 612 8068/8031 e.g. - when a positive microbiology result is received - when a case of infection/infestation is suspected - when an outbreak of infection is suspected - when there is a concern which increases the risks of infection
Clinical teams routinely complete the weekly infection control surveillance form and submit to the IPCT EVERY Monday before 11am reflecting on the previous 7 days (the form is available on the intranet: http://luna.smhsct.local/documents/trust-forms/1757-weekly-infection-surveillance-data-returns
Other Clinical Areas
Each Unit collates data on the number of patients/staff with known or suspected infection
Clinical staff verbally inform the IPCT as/when these occur by phone on 0121 612 8068/8031
Infection Prevention and Control Team
The IPCT checks laboratory results daily and collates and records information on the weekly prevalence record sheet, including any incidents/reports from other departments/teams
The IPCT checks NHS.net e-mail account daily for any laboratory notifications
The IPCT checks weekly surveillance forms every Monday and collates and records information on the weekly prevalence record sheet
The IPCT provide guidance and advice to clinical teams in relation to all cases identified
The IPCT report any areas of concern e.g. incidents/outbreaks to the DIPC as/when they occur
The IPCT notify the Regional PHE Office & CCG when any notifiable incidents/outbreaks of infection arise
The IPCT each month collates all the data collected
Each quarter the data collection and any issues identified/areas for concern etc. are detailed in the quarterly report presented to the DIPC/Infection Prevention and Control Committee
Surveillance of Infection and Data Collection Page 10 of 16 Version 2.0 January 2019
Appendix 4
Surveillance of Infection and Data Collection Page 11 of 16 Version 2.0 January 2019
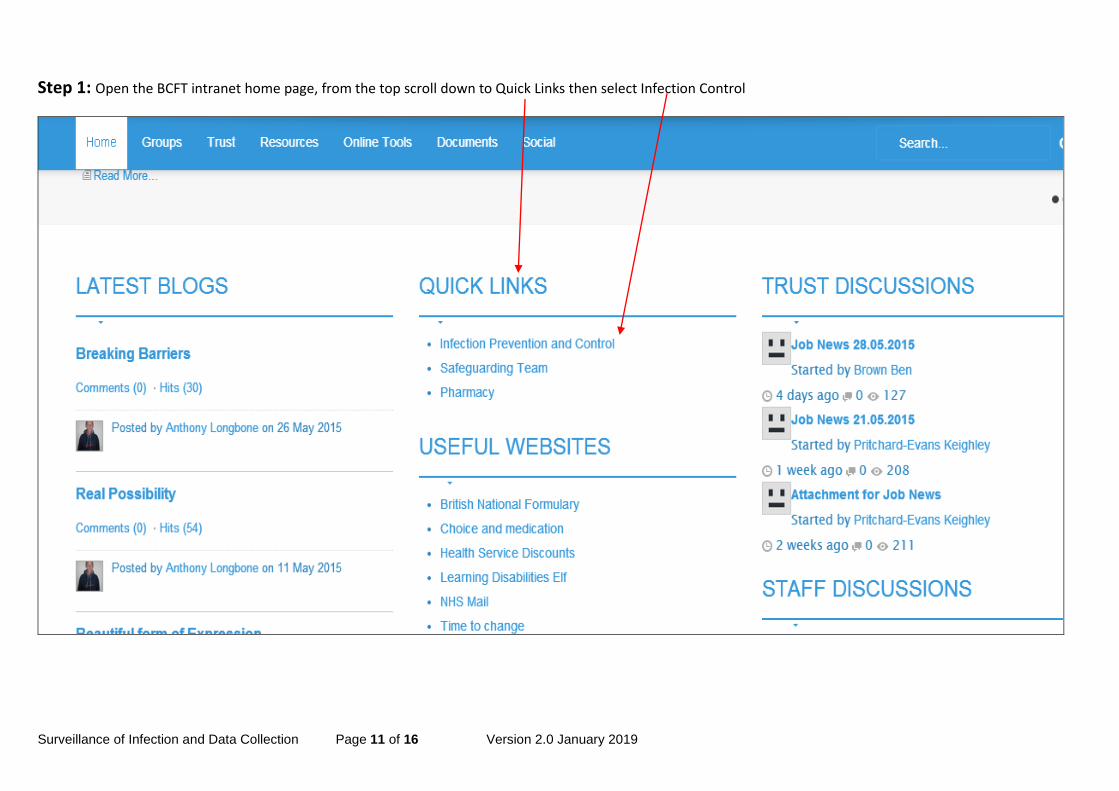
Step 1: Open the BCFT intranet home page, from the top scroll down to Quick Links then select Infection Control
Surveillance of Infection and Data Collection Page 12 of 16 Version 2.0 January 2019
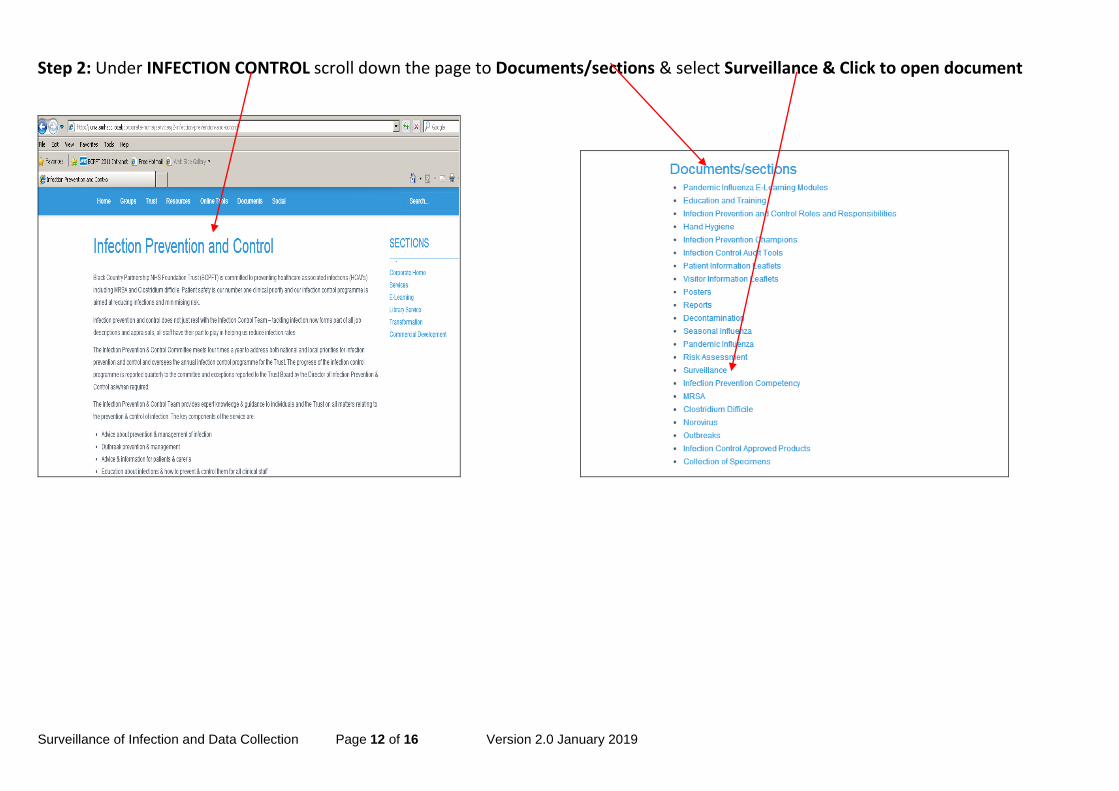
Step 2: Under INFECTION CONTROL scroll down the page to Documents/sections & select Surveillance & Click to open document
Surveillance of Infection and Data Collection Page 13 of 16 Version 2.0 January 2019
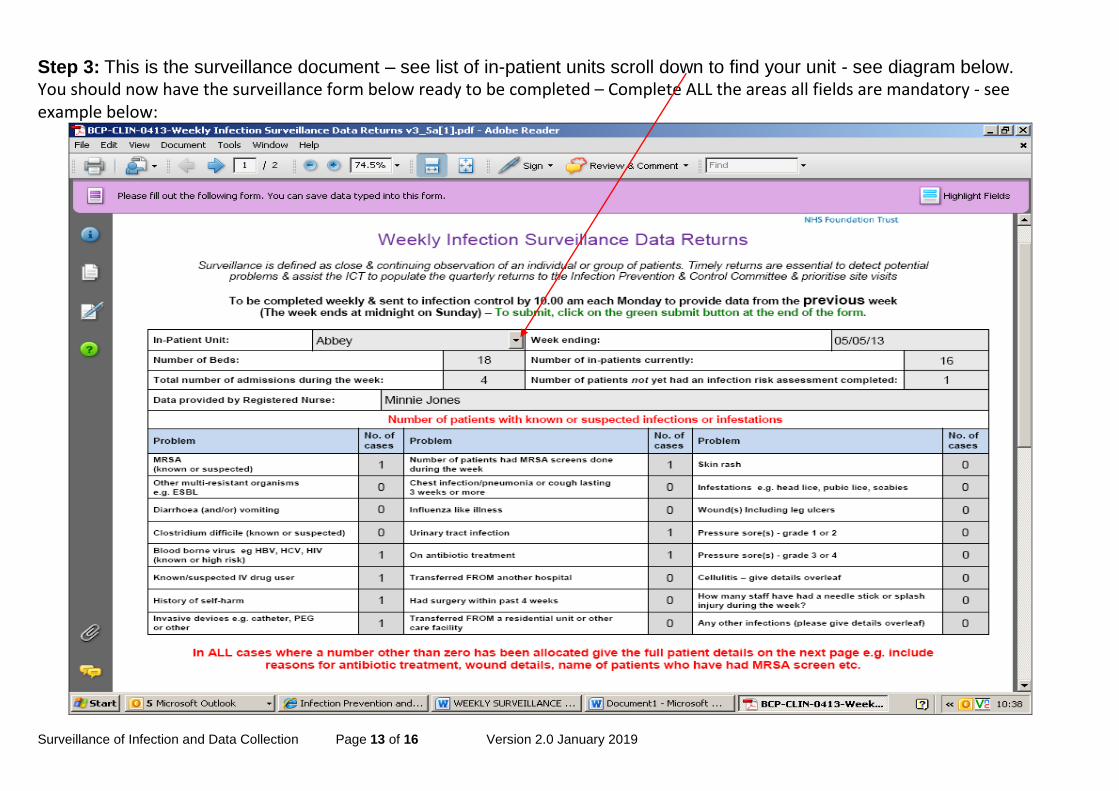
Step 3: This is the surveillance document – see list of in-patient units scroll down to find your unit - see diagram below. You should now have the surveillance form below ready to be completed – Complete ALL the areas all fields are mandatory - see example below:
Surveillance of Infection and Data Collection Page 14 of 16 Version 2.0 January 2019
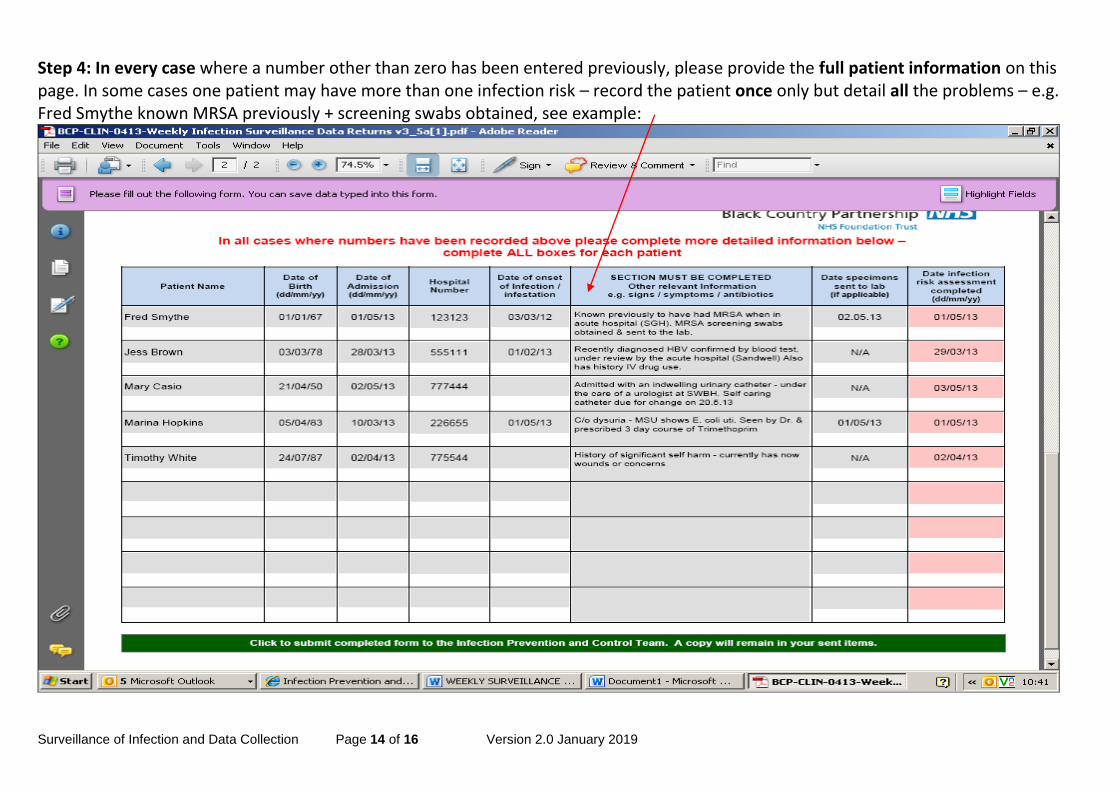
Step 4: In every case where a number other than zero has been entered previously, please provide the full patient information on this page. In some cases one patient may have more than one infection risk – record the patient once only but detail all the problems – e.g. Fred Smythe known MRSA previously + screening swabs obtained, see example:
Surveillance of Infection and Data Collection Page 15 of 16 Version 2.0 January 2019
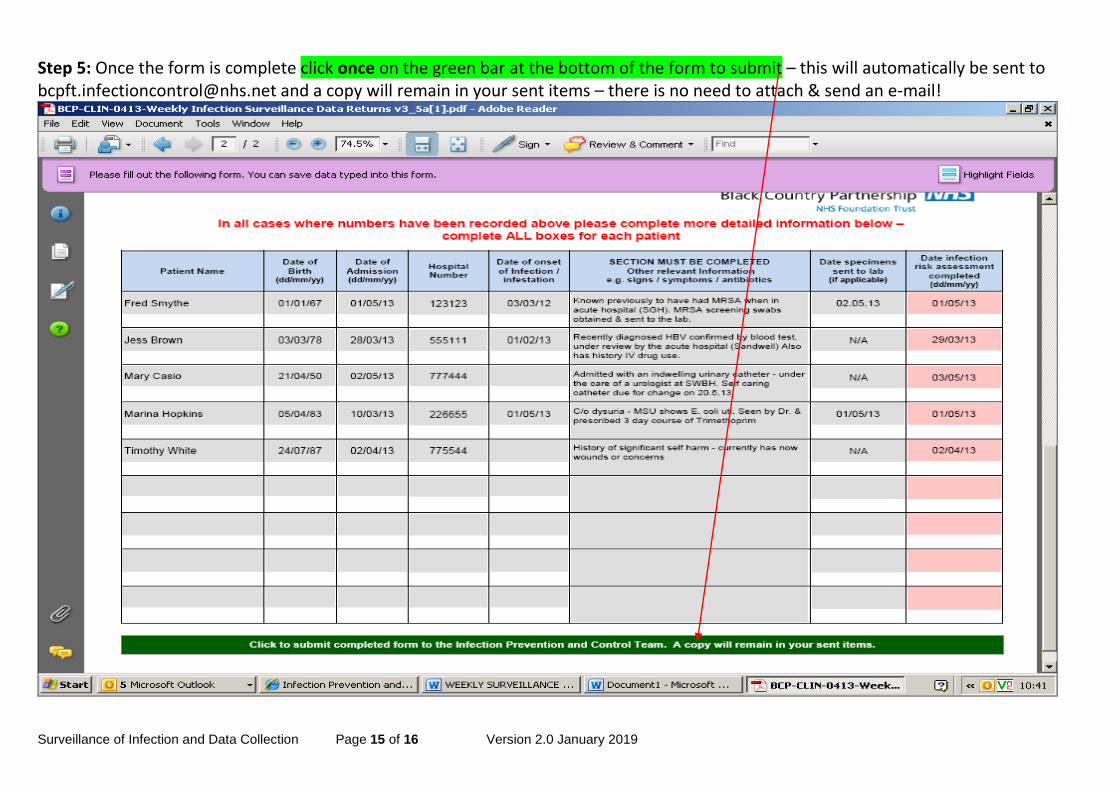
Step 5: Once the form is complete click once on the green bar at the bottom of the form to submit – this will automatically be sent to [email protected] and a copy will remain in your sent items – there is no need to attach & send an e-mail!
Surveillance of Infection and Data Collection Page 16 of 16 Version 2.0 January 2019
Standard Operating Procedure Details
Review and Amendment History
Version Date Description of Change
2.0 Jan 2019 Procedure reviewed and all internet links & contact details
updated
Appendix 4 added
1.0 Dec 2015 New Procedure established to supplement Infection Control Assurance Policy
Unique Identifier for this SOP is BCPFT-COI-POL-05-03
State if SOP is New or Revised Revised
Policy Category Control of Infection
Executive Director whose portfolio this SOP comes under
Executive Director of Nursing, AHPs and Governance
Policy Lead/Author Job titles only
Infection Prevention and Control Team
Committee/Group Responsible for Approval of this SOP
Infection Prevention and Control Committee
Month/year consultation process completed
n/a
Month/year SOP was approved January 2019
Next review due January 2022
Disclosure Status ‘B’ can be disclosed to patients and the public