Embed Size (px)
Citation preview
Infantile Infantile HypertrophicHypertrophic Pyloric Pyloric StenosisStenosis
TresaraTresara C. Bell, MDC. Bell, MDKings County Medical CenterKings County Medical Center
22 October, 200422 October, 2004
Pyloric Pyloric StenosisStenosis
Infantile Infantile hypertrophichypertrophic pyloric pyloric stenosisstenosis (IHPS) is a (IHPS) is a condition that effects young infants.condition that effects young infants.The pylorus becomes abnormally thickened and The pylorus becomes abnormally thickened and manifests as obstruction to gastric emptying.manifests as obstruction to gastric emptying.Infants with IHPS are clinically normal at birth, and Infants with IHPS are clinically normal at birth, and subsequently develop subsequently develop nonbiliousnonbilious forceful forceful ((““projectileprojectile””) vomiting during the first few weeks of ) vomiting during the first few weeks of postnatal life.postnatal life.Gastric outlet obstruction leads to emaciation and, Gastric outlet obstruction leads to emaciation and, if left untreated, may result in deathif left untreated, may result in death
Historical PerspectiveHistorical PerspectiveDespite its frequency, it was virtually unknown Despite its frequency, it was virtually unknown prior to 1627, when a clinical description with prior to 1627, when a clinical description with survival was described by survival was described by FabriciousFabricious HildanusHildanus..Over the next 2 centuries, only 7 additional cases Over the next 2 centuries, only 7 additional cases were described, some without pathologic proof were described, some without pathologic proof and of doubtful origin.and of doubtful origin.HaraldHarald HirschsprungHirschsprung presented 2 infant girls with presented 2 infant girls with pathologically proved IHPS at the German pathologically proved IHPS at the German Pediatric Congress in 1887.Pediatric Congress in 1887.A profusion of scientific interest was triggered, and A profusion of scientific interest was triggered, and by 1910, 598 cases had been recognized. Even as by 1910, 598 cases had been recognized. Even as late as 1905, its existence was still occasionally late as 1905, its existence was still occasionally doubted.doubted.
EpidemiologyEpidemiologyThe incidence of IHPS is approximately 2 to 5 per The incidence of IHPS is approximately 2 to 5 per 1,000 births per year in most white populations.1,000 births per year in most white populations.Less common in India, and among black and Less common in India, and among black and Asian populations, with a frequency that is oneAsian populations, with a frequency that is one--third to onethird to one--fifth that in the white population.fifth that in the white population.The maleThe male--toto--female ratio is approximately 4:1.female ratio is approximately 4:1.There is a There is a famlilialfamlilial link, but a hereditary link, but a hereditary propensity to the development of IHPS is likely propensity to the development of IHPS is likely polygenic with no single locus accounting for the polygenic with no single locus accounting for the fivefold increase in the risk of firstfivefold increase in the risk of first--degree degree relatives.relatives.
EpidemiologyEpidemiology
Male and female children of affected fathers carry Male and female children of affected fathers carry a risk of 5% and 2% respectively, of developing a risk of 5% and 2% respectively, of developing IHPS.IHPS.
Male and female children of affected mothers Male and female children of affected mothers carry a risk of 20% and 7%, respectively of carry a risk of 20% and 7%, respectively of developing IHPS.developing IHPS.
Concordance in monozygotic twins is 0.25Concordance in monozygotic twins is 0.25--0.44, 0.44, and that in and that in dizygoticdizygotic twins is 0.05twins is 0.05--0.10.0.10.

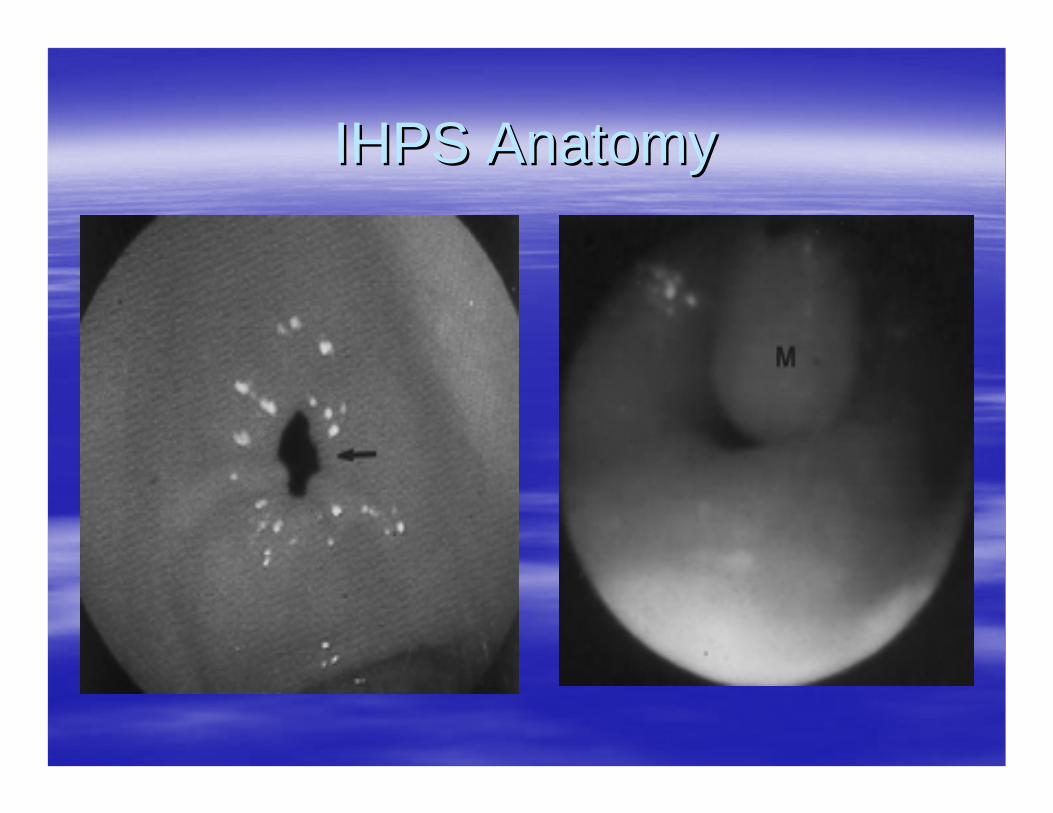
IHPS AnatomyIHPS AnatomyIn IHPS the pyloric ring is no longer In IHPS the pyloric ring is no longer a clearly defined separation a clearly defined separation between the pyloric canal and between the pyloric canal and duodenum.duodenum.Instead the muscle of the pyloric Instead the muscle of the pyloric antrumantrum is is hypertrophichypertrophic (3 or more (3 or more mm), which separates the normal mm), which separates the normal antrumantrum (1mm thickness) from the (1mm thickness) from the duodenum.duodenum.The lumen is filled with compressed The lumen is filled with compressed and redundant mucosa, which and redundant mucosa, which obstructs the passage of gastric obstructs the passage of gastric contents.contents.
IHPS AnatomyIHPS Anatomy

Clinical PresentationClinical Presentation
Varies with length of symptoms.Varies with length of symptoms.Recent onset of forceful Recent onset of forceful nonbiliousnonbilious vomiting, vomiting, typically described as typically described as ““projectile.projectile.””Frequency of vomiting is initially intermittent, but Frequency of vomiting is initially intermittent, but will progress to follow all feedings.will progress to follow all feedings.Emesis may become blood tinged with protracted Emesis may become blood tinged with protracted vomiting, likely related to gastritis.vomiting, likely related to gastritis.Since the child is unable to achieve adequate Since the child is unable to achieve adequate nutrition, he or she exhibits a voracious appetite.nutrition, he or she exhibits a voracious appetite.

Clinical PresentationClinical PresentationStarvation can exacerbate diminished hepatic Starvation can exacerbate diminished hepatic glucoronylglucoronyl transferasetransferase activity, and indirect activity, and indirect hyperbilirubinemiahyperbilirubinemia may be seen in 1may be seen in 1--2% of 2% of affected infants. affected infants. Prolonged vomiting leads to the loss of large Prolonged vomiting leads to the loss of large quantities of gastric secretions rich in Hquantities of gastric secretions rich in H+ + and and ClCl-- ..As a result of dehydration, the kidney attempts to As a result of dehydration, the kidney attempts to
conserve Naconserve Na+ + to maintain volume, by exchanging to maintain volume, by exchanging them for Kthem for K+ + and Hand H+ + (paradoxical (paradoxical aciduriaaciduria). ). The net result is a loss of HThe net result is a loss of H+ + and Kand K++, which results , which results in in hypokalemichypokalemic, , hypochloremichypochloremic metabolic acidosis.metabolic acidosis.
EtiologyEtiology
It has been found that, when compared to It has been found that, when compared to controls, in IHPS specimens, the muscle layer is controls, in IHPS specimens, the muscle layer is deficient in:deficient in:–– the quantity of nerve terminalsthe quantity of nerve terminals–– markers for nervemarkers for nerve--supporting cellssupporting cells–– peptidepeptide--containing nerve fiberscontaining nerve fibers–– nitric oxide nitric oxide synthasesynthase activityactivity–– mRNA production for nitric oxide mRNA production for nitric oxide synthasesynthase–– Interstitial cells of Interstitial cells of CajalCajal
OhshiroOhshiro and and PuriPuri. Pathogenesis of infantile . Pathogenesis of infantile hypertrophichypertrophic pyloric pyloric stenosisstenosis: recent progress. : recent progress. PediatrPediatr SurgSurg IntInt (1998)13:243(1998)13:243--252.252.
EtiologyEtiologyIHPS specimens contain increases in:IHPS specimens contain increases in:–– InsulinInsulin--like growth factorlike growth factor–– plateletplatelet--derived growth factorderived growth factor
It is postulated that this abnormal innervation of It is postulated that this abnormal innervation of the muscular layer leads to failure of relaxation of the muscular layer leads to failure of relaxation of the pyloric muscle, increased synthesis of growth the pyloric muscle, increased synthesis of growth factors, and subsequent hypertrophy, hyperplasia, factors, and subsequent hypertrophy, hyperplasia, and obstruction.and obstruction.There is an increased incidence of IHPS in infants There is an increased incidence of IHPS in infants receiving erythromycin. The reason is unclear, receiving erythromycin. The reason is unclear, although a although a prokineticprokinetic effect on gastric muscle effect on gastric muscle contraction is postulated.contraction is postulated.
EtiologyEtiology
The The hypergastrinemiahypergastrinemia hypothesis proposes hypothesis proposes that an inherited increase in the number of that an inherited increase in the number of parietal cells initiates a cycle of increased parietal cells initiates a cycle of increased acid production, repeated pyloric acid production, repeated pyloric contraction, and delayed gastric emptying.contraction, and delayed gastric emptying.–– Development of IHPS after initiation of feedings, Development of IHPS after initiation of feedings,
increased postprandial increased postprandial gastringastrin levels, markedly levels, markedly increased gastric acid secretion in infants with increased gastric acid secretion in infants with IHPS, and the induction of IHPS in puppies after IHPS, and the induction of IHPS in puppies after pentagastrinpentagastrin infusion support this hypothesis.infusion support this hypothesis.

DiagnosisDiagnosisInitially suggested by the typical clinical Initially suggested by the typical clinical presentation.presentation.The mass is firm, mobile, approximately 2 cm, The mass is firm, mobile, approximately 2 cm, best palpated from the left, located in the midbest palpated from the left, located in the mid--epigasrtriumepigasrtrium beneath the liver edge.beneath the liver edge.Palpation of the hard muscle mass or olive is Palpation of the hard muscle mass or olive is diagnostic in conjunction with a typical history.diagnostic in conjunction with a typical history.Diagnosis by palpation of olive only successful Diagnosis by palpation of olive only successful 49% of cases in recent years vs. 78% 30 years 49% of cases in recent years vs. 78% 30 years ago. ago. Palpation requires a calm infant with relaxed Palpation requires a calm infant with relaxed abdominal musculature, which is difficult in these abdominal musculature, which is difficult in these hungry babies.hungry babies.MacadesiMacadesi and Oates. Clinical diagnosis of pyloric and Oates. Clinical diagnosis of pyloric stenosisstenosis: a declining art. BMJ : a declining art. BMJ 1993;306:5531993;306:553--555.555.
DiagnosisDiagnosisIf the olive is not palpable in an infant who has a If the olive is not palpable in an infant who has a clinical picture suggestive of IHPS, further studies clinical picture suggestive of IHPS, further studies are warranted.are warranted.UltrasonographyUltrasonography is used to measure the thickness is used to measure the thickness of the pyloric wall and the length of the pyloric of the pyloric wall and the length of the pyloric canal.canal.–– normal wall thickness <2mm, IHPS >4 mm normal wall thickness <2mm, IHPS >4 mm –– normal length of the pyloric canal <10 mm, normal length of the pyloric canal <10 mm,
IHPS >14 mmIHPS >14 mmSensitivity and specificity as high as 100%Sensitivity and specificity as high as 100%Heller, et al. Application of new imaging modalities to the evalHeller, et al. Application of new imaging modalities to the evaluation of uation of common pediatric conditions. J common pediatric conditions. J PediatrPediatr 1999; 135(5): 6321999; 135(5): 632--639.639.
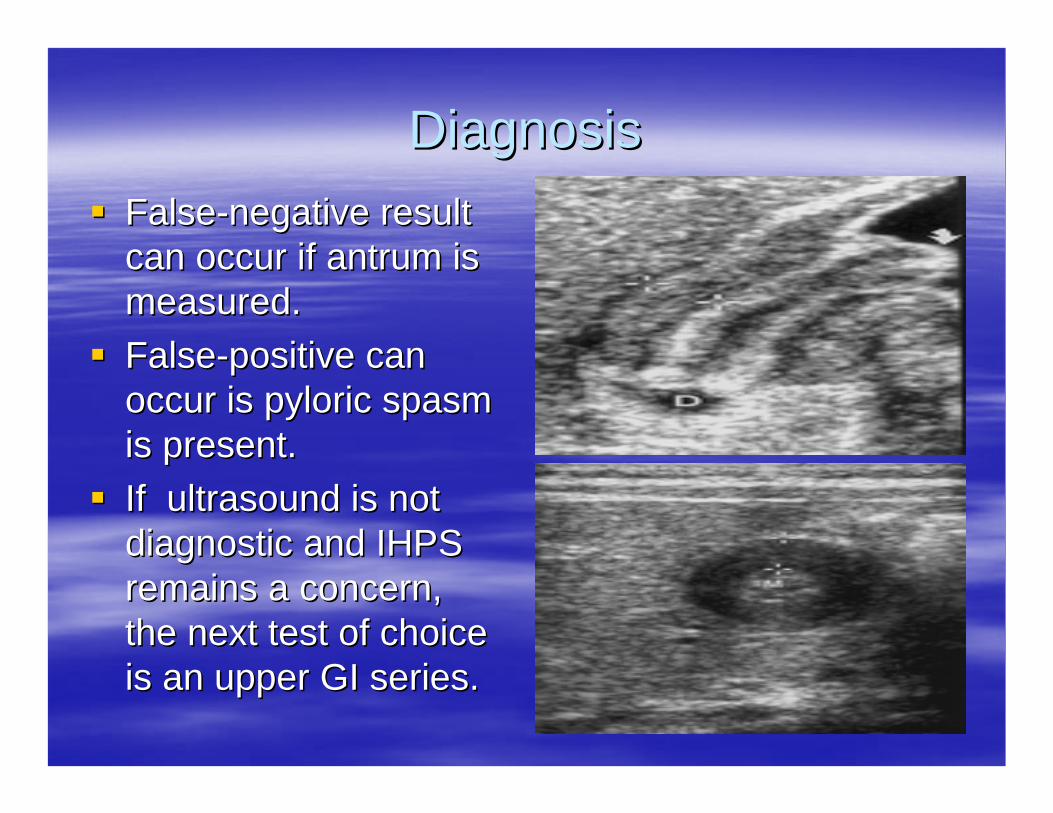
DiagnosisDiagnosisFalseFalse--negative result negative result can occur if can occur if antrumantrum is is measured.measured.FalseFalse--positive can positive can occur is pyloric spasm occur is pyloric spasm is present.is present.If ultrasound is not If ultrasound is not diagnostic and IHPS diagnostic and IHPS remains a concern, remains a concern, the next test of choice the next test of choice is an upper GI series.is an upper GI series.
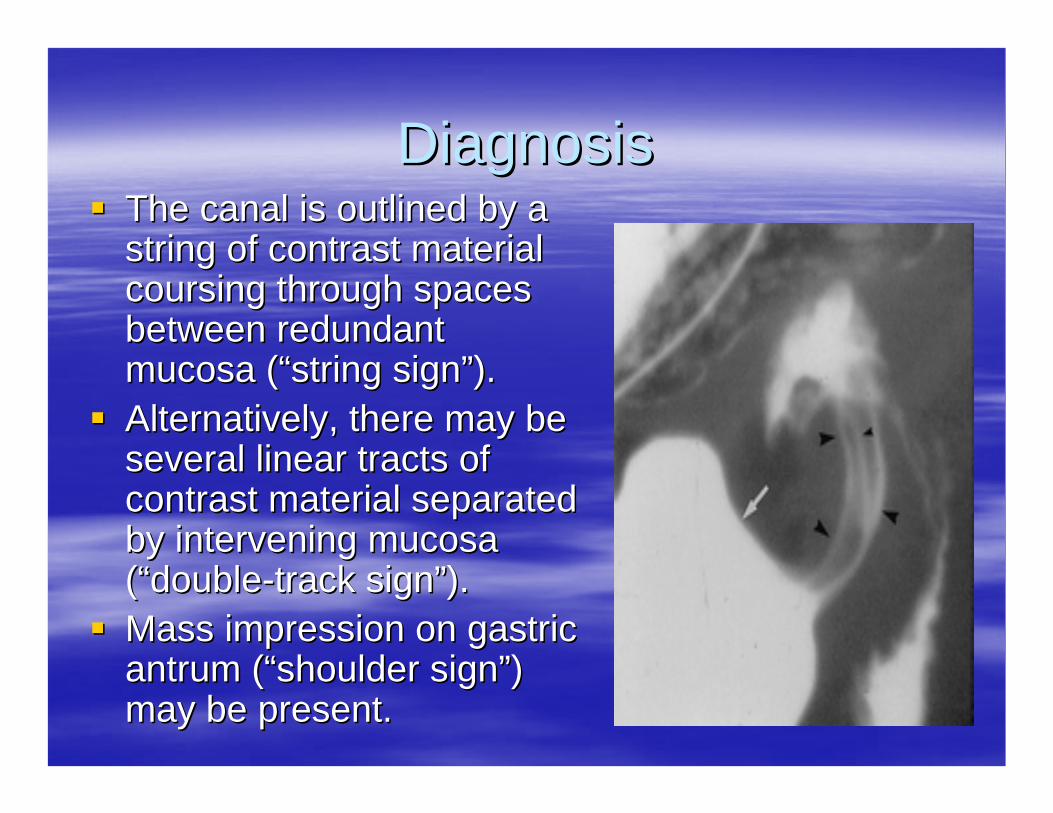
DiagnosisDiagnosisThe canal is outlined by a The canal is outlined by a string of contrast material string of contrast material coursing through spaces coursing through spaces between redundant between redundant mucosa (mucosa (““string signstring sign””).).Alternatively, there may be Alternatively, there may be several linear tracts of several linear tracts of contrast material separated contrast material separated by intervening mucosa by intervening mucosa ((““doubledouble--track signtrack sign””).).Mass impression on gastric Mass impression on gastric antrumantrum ((““shoulder signshoulder sign””) ) may be present.may be present.

DiagnosisDiagnosis
Upper Upper endoscopyendoscopy is used in rare occasions when is used in rare occasions when other imaging modalities are inconclusive.other imaging modalities are inconclusive.NasogastricNasogastric aspirates after 3aspirates after 3--4 hours of fasting.4 hours of fasting.–– IHPS was present in 92% of patients with IHPS was present in 92% of patients with
nasogastricnasogastric aspirate of 10ml or more.aspirate of 10ml or more.–– GER was diagnosed in 86% of patients with GER was diagnosed in 86% of patients with
nasogastricnasogastric aspirates of less than 10ml.aspirates of less than 10ml.
Differential DiagnosisDifferential Diagnosis
GastroesophagealGastroesophageal reflux, with or without reflux, with or without hiatalhiatalhernia. Differentiated by hernia. Differentiated by radiologicradiologic studies. Also studies. Also amount of amount of vomitusvomitus is smaller, and the infant does is smaller, and the infant does not usually lose weight.not usually lose weight.Adrenal insufficiency. Differentiated by absence of Adrenal insufficiency. Differentiated by absence of metabolic acidosis, metabolic acidosis, hyperkalemiahyperkalemia, and elevated , and elevated urinary sodium.urinary sodium.Viral gastroenteritis. Unusual in infants less than 6 Viral gastroenteritis. Unusual in infants less than 6 weeks of age. Associated with significant diarrhea weeks of age. Associated with significant diarrhea and sick contacts.and sick contacts.
TreatmentTreatmentThe preoperative treatment is directed toward The preoperative treatment is directed toward correcting the fluid, acidcorrecting the fluid, acid--base, and electrolyte base, and electrolyte losses. losses. Intravenous fluid therapy is begun with 0.45Intravenous fluid therapy is begun with 0.45––0.9% 0.9% saline, in 5saline, in 5––10% dextrose, with the addition of 10% dextrose, with the addition of potassium chloride in concentrations of 30potassium chloride in concentrations of 30––5050��mEqmEq/L. /L. Fluid therapy should be continued until the infant Fluid therapy should be continued until the infant is is rehydratedrehydrated and the serum bicarbonate and the serum bicarbonate concentration is less than 30concentration is less than 30��mEq/dLmEq/dL, which , which implies that the alkalosis has been corrected. implies that the alkalosis has been corrected.

TreatmentTreatment
Correction of the alkalosis is essential to prevent Correction of the alkalosis is essential to prevent postoperative apnea, which may be associated postoperative apnea, which may be associated with anesthesia with anesthesia Most infants can be Most infants can be rehydratedrehydrated within 24 hours. within 24 hours. Vomiting will usually stop once the stomach is Vomiting will usually stop once the stomach is empty. Occasionally an infant will require empty. Occasionally an infant will require nasogastricnasogastric suction.suction.Once resuscitated the infant can undergo the Once resuscitated the infant can undergo the FredetFredet--RamstedtRamstedt pylormyotomypylormyotomy, which is the , which is the procedure of choice.procedure of choice.
TreatmentTreatmentIf the mucosa is entered (usually on the duodenal If the mucosa is entered (usually on the duodenal side), it can be primarily side), it can be primarily repaitedrepaited and reinforced and reinforced with an with an omentalomental patch.patch.Large perforations are managed by closing the Large perforations are managed by closing the pyloromyotomypyloromyotomy, rotating the pylorus 90, rotating the pylorus 90°°, and , and repeating the repeating the myotomymyotomy..Mortality and morbidity of less that 0.5%Mortality and morbidity of less that 0.5%PostPost--operative complications:operative complications:–– Wound infectionWound infection–– ImcompleteImcomplete myotomymyotomy, treated by repeat , treated by repeat
myotomymyotomy or or endoscopicendoscopic balloon dilation.balloon dilation.
TreatmentTreatment
Diet can be resumed within 6 to 12 hours postDiet can be resumed within 6 to 12 hours post--operatively.operatively.PostPost--operative vomiting may occur in up to 50% of operative vomiting may occur in up to 50% of infants. Thought to be secondary to edema of the infants. Thought to be secondary to edema of the pylorus at the incision site.pylorus at the incision site.Most infants will tolerate full diet within 24 to 48 Most infants will tolerate full diet within 24 to 48 hours.hours.

TreatmentTreatment
Laparoscopic Laparoscopic pyloromyotomypyloromyotomy is performed is performed primarily for improved primarily for improved cosmesiscosmesis and shorter and shorter operative time, with comparable length of stay and operative time, with comparable length of stay and morbidity. morbidity. Decreased rate of duodenal perforation.Decreased rate of duodenal perforation.Increased rate of incomplete Increased rate of incomplete myotomiesmyotomies and and incisionalincisional hernias, requiring rehernias, requiring re--operationoperation..YagmurluYagmurlu, et al. Laparoscopic , et al. Laparoscopic pyloromyotomypyloromyotomy: a : a concurrent single institution series. J concurrent single institution series. J PedatrPedatr SurgSurg2004;(39)3:2922004;(39)3:292--296.296.
TreatmentTreatment
EndoscopicEndoscopic balloon dilation has been used to balloon dilation has been used to treat IHPS. The treat IHPS. The seromuscularseromuscular ring was not reliably ring was not reliably disrupted to relieve the obstruction. Most patients disrupted to relieve the obstruction. Most patients failed balloon dilation and were treated with failed balloon dilation and were treated with pyloromyotomypyloromyotomy..Ogawa, et al. Successful Ogawa, et al. Successful endoscopicendoscopic balloon dilatation for balloon dilatation for hypertrophichypertrophicpyloric pyloric stenosisstenosis. J . J PediatrPediatr SurgSurg 1996; (31)12:17121996; (31)12:1712--1714.1714.Hayashi, et a. Balloon catheter dilation for Hayashi, et a. Balloon catheter dilation for hypertrophichypertrophic pyloric pyloric stenosisstenosis. J . J PediatrPediatr SurgSurg 1990; (25)11:11191990; (25)11:1119--1121.1121.
TreatmentTreatment
Atropine sulfate has been used to treat IHPS with Atropine sulfate has been used to treat IHPS with some success, however infants may not tolerate some success, however infants may not tolerate diet for at least 5 days. diet for at least 5 days. Surgery was necessary in 30% of the patients.Surgery was necessary in 30% of the patients.YamatataYamatata, et al. , et al. PyloromyotomyPyloromyotomy vs. atropine sulfate for infantile vs. atropine sulfate for infantile hypertrophichypertrophicpyloric pyloric stenosisstenosis. J . J PediatrPediatr SurgSurg 2000; 35(2):3382000; 35(2):338--41.41.












![Pathophysiology of Hypertrophic Pyloric Stenosis Revisited ... · 2] = 0.45 × BL [cm]/creatinine [mg/dl] (creatinine [mg/dl] = µmol/l/88.4). 2.1. Limits The presented study has](https://img.pdfslide.us/doc/110x75/5f304cc9286f493b842f23d7/pathophysiology-of-hypertrophic-pyloric-stenosis-revisited-2-045-bl-cmcreatinine.jpg)
















