Embed Size (px)
Citation preview

Fetal, Infant, and Childhood Growth Are Predictors of Coronary Heart Disease,Diabetes, and Hypertension in Adult Men and WomenClive Osmond and David J.P. Barker
MRC Environmental Epidemiology Unit, University of Southampton, Southampton General Hospital, Southampton, United Kingdom
Many human fetuses have to adapt to a limited supply of nutrients. In doing so they permanentlychange their structure and metabolism. These programmed changes may be the origins of anumber of diseases in later life, including coronary heart disease, hypertension and noninsulin-dependent diabetes. We review epidemiologic studies in which the incidence of these diseases hasbeen related to the recorded, early growth of individuals, while considering factors in the adultlifestyle, such as obesity and socioeconomic status. We discuss possible mechanisms. Forhypertension these mechanisms include placentation, maternal blood pressure, fetal undernutrition;childhood growth, activation of the renin-angiotensin system, renal structure, programming of thehypothalamic-pituitary-adrenal axis, vascular structure, and sympathetic nervous activity. Fornoninsulin-dependent diabetes we discuss mechanisms concerning both insulin resistance andinsulin deficiency. We include a review of evidence for the programming of serum cholesterol andclotting factor concentrations. We address the timing of critical windows for coronary heart disease,reviewing studies that allow assessment of the relative importance of fetal, infant, and childhoodgrowth. We argue for a research strategy that combines clinical, animal, and epidemiologicalstudies. Key words: birth weight, childhood growth, coronary heart disease, diabetes, epidemiology,hypertension, infant growth, intrauterine growth, maternal nutrition, programming hypothesis.
Environ Health Perspect 1 08(suppl 3):545-553 (2000).http.//ehpnetl .niehs.nih.gov/docs/2000/suppl-3/545-553osmond/abstract. html
Introduction to ProgrammingIn fetal life the tissues and organs of the bodygo through what are called critical periods ofdevelopment (1). These critical periods may
coincide with periods of rapid cell division.Programming describes the process whereby a
stimulus or insult at a critical period of devel-opment has lasting or lifelong effects (2,3).The development of the sweat glands is an
interesting example of this process (4). InJapan in the early years of this century, mili-tary expansion took Japanese soldiers and set-
tlers into unfamiliar climates. There were widedifferences in people's abilities to adapt to hotclimates. Physiological studies showed this wasrelated to the number of functioning sweat
glands. People with more functioning sweat
glands cooled down faster. Rather thanattributing the differences in sweat glandnumbers to genetic effects, Japanese physiolo-gists explored the early development of theglands. They found that at birth all humanshave similar numbers of sweat glands, butnone of them function. In the first 3 years
after birth, a proportion of the glands becomefunctional, depending on the temperature to
which the child is exposed. The hotter theconditions the greater the number of sweat
glands that are programmed to function. After3 years the programming is complete and thenumber of sweat glands is fixed. The develop-ment of sweat glands encapsulates the essence
of programming-a critical period when thesystem is plastic and sensitive to the environ-
ment, followed by loss of plasticity and a fixedfunctional capacity.
Programming ofanUndernourished Fetus
Undernutrition is one of the influences thatprogram the human body and has lifelongconsequences. Rickets demonstrates thatundernutrition at a critical stage of early lifeleads to persisting changes in structure. Whatis new is the recent realization that some ofthe body's memories of early undernutritionbecome translated into pathology and therebydetermine disease in later life (5). However,this is unsurprising given animal experimentsthat show that undernutrition in utero leadsto persisting changes in blood pressure, cho-lesterol metabolism, insulin response to glu-cose, and a range of other metabolic,endocrine, and immune functions known tobe important in human disease (2,6).
The human fetus adapts to undernutri-tion by metabolic changes, redistribution ofblood flow, and changes in the production offetal and placental hormones that controlgrowth (7).
Metabolic changes. The immediate meta-bolic response of the fetus to undernutritionis catabolism: it consumes its own substratesto provide energy (8). More prolongedundernutrition leads to a slowing in growth.This enhances the ability of the fetus to sur-vive by reducing the use of substrates andlowering the metabolic rate. Slowing ofgrowth in late gestation leads to dispropor-tion in organ size, since organs and tissuesgrowing rapidly at the time are affected themost. Undernutrition in late gestation may,for example, lead to reduced growth of the
kidney, which is developing rapidly at thattime. Reduced replication of kidney cells maypermanently reduce cell numbers, becauseafter birth there seems to be no capacity forrenal cell division to catch-up (9,10).
Redistribution ofbloodflow. While slowingits rate of growth, the fetus may protect tis-sues that are important for immediate sur-vival, especially the brain. One way in whichthe brain can be protected is by redistributionof blood flow to favor it (11,12). This adapta-tion occurs in many mammals. In humans ithas exaggerated costs for tissues other thanthe brain, notably the liver and other abdomi-nal viscera, because of the large size of thehuman brain.
Endocrine changes. Nutrition has profoundeffects on fetal hormones and on the hor-monal and metabolic interactions betweenthe fetus, placenta, and mother on whosecoordination fetal growth depends (8). Fetalinsulin and the insulin-like growth factors(IGF) are thought to have a central role inthe regulation of growth and respond rapidlyto changes in fetal nutrition (13). If a motherdecreases her food intake, fetal insulin, IGF,and glucose concentrations fall, possiblythrough the effect of decreased maternalIGF. This leads to reduction in transfer ofamino acids and glucose from mother tofetus and ultimately to lower fetal growthrates (14). In late gestation and after birth,the growth hormone and IGF axis of thefetus take over a central role from insulin indriving linear growth. Whereas undernutri-tion leads to a fall in the concentrations ofhormones that control fetal growth, it leadsto a rise in cortisol, whose main effects are oncell differentiation (7).
Programming of CoronaryHeart DiseaseThe suggestion that coronary heart diseasemight originate during fetal developmentcame from showing the similarity of the geo-graphic pattern of death rates among babies
This article is based on a presentation at the Workshopto Identify Critical Windows of Exposure for Children'sHealth held 14-16 September 1999 in Richmond, Virginia.
Address correspondence to C. Osmond, MRCEnvironmental Epidemiology Unit, University ofSouthampton, Southampton General Hospital,Southampton, UK. Telephone: 44 2380 777624. Fax:44 2380 704021. E-mail: [email protected]
Received 30 December 1999; accepted 7 April2000.
Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000 545

OSMOND AND BARKER
in Britain during the early 1900s (15) and thepattern of today's death rates from coronaryheart disease. The usual certified cause ofdeath in newborn babies at that time was lowbirth weight. The suggestion that events inchildhood influence the pathogenesis of coro-nary heart disease was not new. A focus onintrauterine life, however, offered a newopportunity for research.
Early epidemiological studies that pointedto the possible importance of programmingin coronary heart disease were based on theexamination of men and women in middleand late life whose body measurements atbirth were recorded. Surviving records werefound in Hertfordshire, Preston, andSheffield in the United Kingdom. TheHertfordshire records were maintained byhealth visitors and include measurements ofgrowth in infancy as well as birth weight. InPreston and Sheffield, detailed obstetricrecords documented body proportions atbirth (16,17).
Sixteen thousand men and women bornin Hertfordshire from 1911 to 1930 havenow been traced from birth to the presentday. Death rates from coronary heart diseasefell between those at the lower and upperends of the birth weight distribution (Table
Table 1. Death rates from coronary heart diseaseamong 15,726 British men and women according to birthweight.Birth weight,lb (kg)< 5.5 (2.50)
6.5 (2.95)7.5 (3.41)8.5 (3.86)9.5 (4.31)
>9.5(4.31)All
Standardizedmortality ratio
100818074556574
No. of deaths
5713729828910357
941
Table 2. Standardized mortality ratios for coronary heartdisease in 3,302 Finnish men from 1924 to 1933.
Birth weight, Standardized mortality ratiokg (Ib) (No. of deaths)
<2.5(5.5) 84(11)3.0 (6.6) 83 (44)3.5 (7.7) 99 (124)4.0 (8.8) 76 (80)
> 4.0 (8.8) 66 (27)All 85 (286)p value for trend 0.09
Term babies onlyPonderal index Standardized mortality ratioat birth (kg/m3) (No. of deaths)< 25 116 (59)27 105 (88)29 72 (64)
> 29 56 (33)All 86 (244)p value for trend < 0.0001
1) (18). A study in Sheffield showed that itwas people who were small at birth becausethey failed to grow, rather than because theywere born early, who were at increased risk ofcoronary heart disease (17). The associationbetween low birth weight and coronary heartdisease has been confirmed in studies of menin Uppsala, Sweden (19), and Caerphilly,Wales (20), and among women in the UnitedStates. Among 80,000 women in theAmerican Nurses Study there was a fall in therelative risk of nonfatal coronary heart diseaseacross the range of birth weights (21). Anassociation between low birth weight andprevalent coronary heart disease was alsoshown in a study in South India (22). AmongIndian men and women 45 years of age andolder the prevalence of the disease fell from18% in those who weighed 5.5 lb at birth to4% in those who weighed 7 lb or more.
The Hertfordshire records and the Nursesand Caerphilly studies did not include mea-surements of body size at birth other thanweight. The weight of a newborn baby, with-out a measure of its length, is as crude a sum-mary of its physique, as is the weight of achild or adult without a measure of height.The addition of birth length allows a long,thin baby to be distinguished from a short,fat baby. With the addition of head circum-ference, the baby whose body is small in rela-tion to its head as a result of brain-sparingmay also be distinguished. These phenotypesreflect differing fetal adaptations to undernu-trition, hypoxia, and other influences andthey have different long-term consequences.
In Sheffield, death rates for coronaryheart disease were higher in men who wereshort at birth (23). The mortality ratio forcoronary heart disease in men who were 18.5in. or less in length was 138 compared with98 in the remainder. Thinness at birth, asmeasured by a low ponderal index (birthweight/length3), was also associated withcoronary heart disease. Table 2 shows thatalthough among men born in Helsinki,Finland, low birth weight was associatedwith raised death rates for coronary heart dis-ease, there was a stronger association withthinness at birth, especially in men born atterm (24). Men who were thin at birth, asmeasured by a low ponderal index, had death
rates that were twice those of men who had ahigh ponderal index.
In Finland, increased death rates fromcoronary heart disease were associated withlow placental weight. In Sheffield, however,coronary heart disease did not vary with pla-cental weight but showed a U-shaped rela-tion with the ratio of placental weight tobirth weight, with the highest mortalityratios at either end of the distribution. Thepattern of body proportions at birth that pre-dicts death from coronary heart diseasetherefore may be summarized as a small headcircumference, shortness or thinness, whichreflect retarded fetal growth, and either lowplacental weight or an altered ratio of placen-tal weight to birth weight.
These findings suggest that influenceslinked to early fetal and placental growthhave an important effect on the risk of coro-nary heart disease and stroke. It has beenargued, however, that people whose growthwas impaired in utero and during infancy maycontinue to be exposed to an adverse environ-ment in childhood and adult life, and it isthis later environment that produces theeffects attributed to programming (25-28).However, in three of the studies that havereplicated the association between birthweight and coronary heart disease, data onlifestyle factors including smoking, employ-ment, alcohol consumption, and exercisewere collected (19-21). Allowance for themhad little effect on the association betweenbirth weight and coronary heart disease.
In studies exploring the mechanismsunderlying these associations, the trends incoronary heart disease with birth weight werefound to parallel similar trends in two of itsmajor risk factors-hypertension and non-insulin-dependent diabetes mellitus (29,30).Table 3 illustrates the size of these trends,with the prevalence of noninsulin-dependentdiabetes mellitus and impaired glucose toler-ance falling 3-fold between men who weighedup to 5.5 lb at birth and those who weighedover 9.5 lb (29). These associations withsmall size at birth are again independent ofsocial class, cigarette smoking, and alcoholconsumption. Influences in adult life, how-ever, add to the effects of the intrauterineenvironment. For example, the prevalence of
Table 3. Prevalence of noninsulin-dependent diabetes and impaired glucose tolerance in men 59-70 years of age.
Odds ratio adjustedBirth weight, % with impaired glucose for body mass indexlb (kg) No. of men tolerance or diabetes (95% confidence interval)
< 5.5 (2.50) 20 40 6.6 (1.5-28)6.5 (2.95) 47 34 4.8 (1.3-17)7.5 (3.41) 104 31 4.6 (1.4-16)8.5 (3.86) 117 22 2.6 (0.8-8.9)9.5 (4.31) 54 1 3 1.4 (0.3-5.6)
>9.5 (4.31 ) 28 1 4 1.0All 370 25
Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000546

EARLY GROWTH AND HEART DISEASE, DIABETES, HYPERTENSION
impaired glucose tolerance is highest inpeople who had low birth weight but becomeobese as adults.
Programming of HypertensionAssociations between low birth weight andraised blood pressure in childhood and adultlife have been extensively demonstrated aroundthe world. Law and Shiell published a system-atic review of studies describing the associationbetween birth weight and blood pressure(31)-a review based on 34 studies of morethan 66,000 people of all ages in many coun-tries. In almost all the studies an increase inbirth weight was associated with a fall in bloodpressure, and there was no exception to this inthe studies of adults, which now total nearly8,000 men and women. The associations areless consistent in adolescence, perhaps becausethe tracking of blood pressure from childhoodthrough adult life is perturbed by the adoles-cent growth spurt. These associations were notconfounded by socioeconomic conditions atthe time of birth or in adult life (32. The dif-ference in systolic pressure associated with akilogram difference in birth weight was around3.5 mmHg. In clinical practice this would be asmall difference, but there are large differencesbetween the mean values of populations.Available data suggest that lowering the meansystolic pressure in a population by 10 mmHgwould correspond to a 30% reduction inattributable mortality (33).
The association between low birth weightand raised blood pressure depends on babieswho were small for dates, after reduced fetalgrowth, rather than on babies who were bornpreterm (16,34). Although in these studiesalcohol consumption and higher body massindex were also associated with raised bloodpressure, the associations between birth weightand blood pressure were independent of them.Nevertheless, body mass index remains animportant influence on blood pressure and, inhumans and animals, the highest pressures arefound in people who were small at birth butbecome overweight as adults.
As has already been discussed, birthweight is a crude measure of fetal growth thatdoes not distinguish shortness and thinness,differences in head size, or variations in thebalance of fetal and placental size. In contrastto the associations between birth size andcoronary heart disease, those between birthweight and blood pressure are generally asstrong as those between thinness or shortnessand blood pressure (35-38).
Possible MechanismsPlacentation. Men and women who wereborn in Sharoe Green Hospital in Preston 50years ago had systolic blood pressures that fellbetween subjects with low and high birthweight (16,35), as in other studies. In
addition, however, their blood pressuresincreased with increasing placental weight.Subjects with a mean systolic pressure of 150mm Hg or more, a level sometimes used todefine hypertension in clinical practice, com-prise a group who as babies were relativelysmall in relation to the size of their placentas.A rise in blood pressure with increasing pla-cental weight was also found in 4-year-oldchildren in Salisbury, UK, and among 8-year-old children in Adelaide, Australia (37,39).However, in studies of children and adultsthe association between placental enlargementand raised blood pressure has been inconsis-tent (40). For example, in a study of men andwomen born in Aberdeen, Scotland, afterWorld War II, at a time when food was stillrationed, raised blood pressure was associatedwith small placental size (41). Animal studiesoffer a possible explanation for this inconsis-tency. In sheep the placenta enlarges inresponse to moderate undernutrition in mid-pregnancy (42,43). This is thought to be anadaptive response to extract more nutrientsfrom the mother. It is not, however, a consis-tent response and occurs only in ewes thatwere well nourished before pregnancy.
Maternal bloodpressure. In some studiesthe blood pressures of the mothers duringand after pregnancy have been recorded(37,44,45). They correlate with the off-springs' blood pressure. However, the associa-tions between body size at birth and laterblood pressure are independent of the moth-ers' blood pressures. Recent observationsshow that if the mother's blood pressure ismeasured throughout a 24-hr period ratherthan by isolated readings at antenatal clinics,there is a continuous inverse associationbetween birth weight and maternal bloodpressure (46). It could be argued, therefore,that the association between low birth weightand raised blood pressure reflects an associa-tion, possibly genetic, between a mother'sambulatory blood pressure and the bloodpressure of her offspring. However, thedemonstration that experimental undernutri-tion during gestation programs blood pres-sure in animals (47) argues against thisinterpretation. An alternative explanation isthat raised blood pressure during pregnancyreflects failure of maternal cardiovascularadaptations to pregnancy, which includeperipheral vasodilation, with consequent fetalundernutrition, low birth weight, and raisedblood pressure in the offspring.
Fetal undernutrition. Several lines ofevidence support the thesis that it is poordelivery of nutrients that programs raisedblood pressure in humans. Maternal height,parity, and cigarette smoking, which influencefetal growth, have not been found to berelated to the offsprings' blood pressure otherthan in small preterm babies (37,48). In
Jamaica children whose mothers had thintriceps skinfolds in early pregnancy and lowweight gain during pregnancy (49) had raisedblood pressure. There were similar findings ina group of children in Birmingham, UK (50).In The Gambia, low pregnancy weight gainwas associated with higher blood pressure inchildhood (51). In Aberdeen, Scotland, theblood pressures of middle-age men andwomen were related to their mothers'intakes of carbohydrate and protein duringpregnancy (41).
Childhood growth. Studies in the UnitedStates, the United Kingdom, and Hollandhave shown that blood pressure in childhoodpredicts the likelihood of developing hyper-tension in adult life. These predictions arestrongest after adolescence. In children therise of blood pressure with age is closelyrelated to growth and is accelerated by theadolescent growth spurt. These observationshave led Lever and Harrap to propose thatessential hypertension is a disorder of growth(52). The hypothesis that hypertension is adisorder of accelerated childhood growth canbe reconciled with the association with lowbirth weight by postulating that postnatalcatch-up growth plays an important role inamplifying changes established in utero.
Renin-angiotensin system. There is evidencethat the fetal renin-angiotensin system is acti-vated during intrauterine growth retardation(53). However, in a follow-up study of menand women born in Sheffield, those who hadbeen small at birth had lower plasma concen-trations of inactive and active renin (54).Causes of raised blood pressure that are notmediated by increased rates of renin releasetend to result in low concentrations of renin,and therefore, at first sight, these findings sug-gest that the association between impaired fetalgrowth and raised blood pressure must involvemechanisms other than the renin-angiotensinsystem. However, low concentrations of reninin adult life do not exclude the possibility thatthe renin-angiotensin system has exerted anearlier but lasting influence.
Renalstture. An alternative explanationfor the low plasma renin concentrations ofpeople who were small at birth is that theyreflect a relative deficit of nephrons. Brenneret al. has suggested that retarded fetal growthleads to reduced numbers of nephrons whichin turn leads to increased pressure in theglomerular capillaries and the development ofglomerular sclerosis (55,56). This sclerosisleads to further loss of nephrons and a self-perpetuating cycle of hypertension and pro-gressive glomerular injury. The numbers ofnephrons in the normal population varieswidely, from 300,000 to 1,100,000 or more(55). Animal and human studies have shownthat low rates of intrauterine growth are asso-ciated with reduced numbers of nephrons
Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000 547

OSMOND AND BARKER
(57). Studies using fetal ultrasound haveshown that babies who are small for gesta-tional age have reduced renal growth duringthe critical period at 26-34 weeks of gesta-tion. This reduces the anteroposterior size ofthe kidney but does not diminish kidneylength (58). It has been suggested that duringnormal childhood development, kidneygrowth lags behind the increases in bodyweight, and blood pressure rises to maintainrenal homeostasis (59).
Endocrine. Animal studies have led to thehypothesis that fetal undernutrition leads tolife-long changes in the hypothalamic-pituitary-adrenal axis of the fetus, which inturn resets homeostatic mechanisms control-ling blood pressure (60,61). A recent study of9-year-old children in Salisbury, UK, showedthat those who had been small at birth hadincreased urinary adrenal androgen and glu-cocorticoid metabolite excretion (62), prelim-inary evidence that the hypothalamic-pituitary-adrenal axis is programmed inhumans. The growth hormone insulin-likegrowth factor 1 (IGF-1) axis may also be pro-grammed in utero. Children of low birthweight have raised plasma IGF-1 concentra-tions (48,63). The highest concentrations arein children who had the lowest birth weightsbut attain the largest body size in childhood.Raised IGF-1 concentrations may thereforebe linked to catch-up growth. IGF-1 isknown to be important for the growth ofblood vessels (64), and raised concentrationscould be one of the processes underlying thesuggested association between catch-upgrowth and raised blood pressure in later life.
Vascular structure. The elastic recoil ofthe aorta is important in maintaining bloodflow in the peripheral circulation and in thecoronary arteries during diastole. Reducedelasticity (compliance) in the aorta is amarker of cardiovascular disease (65). It isassociated with hypertension, and also withleft ventricular hypertrophy because the workof the left ventricle is increased (66,67). Menand women 50 years of age in Sheffield whowere small at birth had reduced compliancein the large arteries of the trunk and legs (44).Martyn and Greenwald have proposed thatimpaired synthesis of the scleroprotein elastinis one of the mechanisms underlying the asso-ciation between low birth weight and raisedblood pressure (68). The elasticity of largerarteries largely depends on elastin (69), whichis laid down in utero and during infancy andthereafter turns over slowly (69). Its half-lifein humans is approximately 40 years (70).Reduced elastin deposition leads to less com-pliant, stiffer arteries, which will lead to raisedblood pressure. The loss of elastin with agingwill amplify the increase in blood pressure.
In the growth-retarded fetus there arechanges in blood flow in several vascular
beds, including the descending aorta andcerebral vasculature (71). These are brain-sparing adaptations that lead to preferentialperfusion of the brain at the expense of thetrunk (11,12,72). If sustained they may leadto reduced growth of the abdominal visceraand stunting at birth. Because elastin deposi-tion in a blood vessel in utero is related to theflow of blood, reduced flow in the large arter-ies of the trunk and legs as a consequence ofbrain-sparing may be associated with reducedelastin deposition, less compliant arteries, andconsequent hypertension. Diversion of oxy-genated blood away from the trunk to sustainthe growth of the brain increases peripheralresistance (71,73), and echocardiography hasshown that growth-retarded fetuses havehypertrophy of both ventricles (74,75).Cardiac myocytes become terminally differ-entiated before birth and the load on theheart influences their rate of maturation.Early pressure loading leads to fewer but largermyocytes. Left ventricular enlargement isknown to be a strong predictor of morbidityand death from coronary heart disease inde-pendent of its association with raised systolicblood pressure and increased body mass (76).Among 67-year-old men in Hertfordshirethose who had had low weight at 1 year of agehad concentric enlargement of the left ventri-cle (77). This may reflect the long-termeffects of prenatal blood diversion to thebrain in a baby who is stunted at birth andwhose growth does not catch up in infancy.An association between low weight aroundthe age of 1 year and later concentric left ven-tricular hypertrophy has also been found in asample of children and adults in Lorraine,France (78).
Recent studies suggest that low birthweight is associated with persisting alterationsin vascular structure and function in additionto its associations with compliance. Amongmen in Hertfordshire, those who had had lowbirth weight had narrow bifurcation angles intheir retinal blood vessels (79). People withhypertension have similar changes in retinalvascular geometry. In a study of children inthe United Kingdom, those who had lowbirth weight had reduced flow-mediateddilatation in the brachial artery after theartery had been occluded and released. Flow-mediated dilatation depends on the endothe-lium. These findings suggest, therefore, a linkbetween low birth weight and endothelialdysfunction (80).
Nervous system. People with high bloodpressure tend to have a high resting pulse rate(81). This is associated with high cardiac out-put, hyperdynamic circulation, and features ofincreased sympathetic nervous system activity(82). Among men and women in Preston,those who had low birth weight had a higherresting pulse rate (83). This is consistent with
the hypothesis that increased sympatheticnervous activity is established throughretarded growth in utero and leads to raisedblood pressure in later life.
Programming of Noninsulin-Dependent DiabetesInsulin has a central role in fetal growth, anddisorders of glucose and insulin metabolismare therefore an obvious possible link betweenearly growth and cardiovascular disease (13).Although obesity and a sedentary lifestyle areimportant in the development of noninsulin-dependent diabetes, they seem to lead to thedisease only in predisposed individuals.Family and twin studies have suggested famil-ial predisposition, but the nature of this pre-disposition is unknown. The disease tends tobe transmitted through the maternal ratherthan paternal side of the family (84).
Size at Birth and Noninsulin-Dependent DiabetesA number of other studies have confirmed theassociation between birth weight, impairedglucose tolerance, and noninsulin-dependentdiabetes that was first reported inHertfordshire (18,29,85-88) (Table 3). In theHealth Professionals Study in the UnitedStates, the odds ratio for diabetes, after adjust-ing for current body mass, was 1.9 amongmen whose birth weights were less than 5.5 lbcompared with those who weighed 7-8.5 lb(89). Among the Pima Indians in the UnitedStates, the odds ratio for diabetes was 3.8 inmen and women who weighed less than 5.5 lb(90). In Preston it was the thin babies whodeveloped impaired glucose tolerance and dia-betes. Lithell and colleagues confirmed theassociation with thinness in Uppsala, Sweden(87) (Table 4). The prevalence of diabetes was3 times higher among men in the lowest fifthof ponderal index at birth. This was a strongerassociation than that with birth weight, withthe prevalence of diabetes only twice as highamong men in the lowest fifth of birth weight.Among the Pima Indians, in whom diabetesin pregnancy is unusually common, youngmen and women with birth weights over 9.9lb had an increased prevalence of noninsulin-dependent diabetes (90). The association
Table 4. Prevalence of noninsulin-dependent diabetesby ponderal index at birth among men 60 years of age inUppsala, Sweden.
Ponderal index Prevalence ofat birth (kg/m3) Number of men diabetes(%)<24.2 193 11.924.2 193 5.225.9 196 3.627.4 188 4.3
> 29.4 201 3.5All 971 5.7p value for trend 0.001
Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000548

EARLY GROWTH AND HEART DISEASE, DIABETES, HYPERTENSION
between birth weight and noninsulin-dependent diabetes was therefore U-shaped.The increased risk of diabetes among babieswith high birth weights was associated withmaternal diabetes in pregnancy.
Insulin ResisanceBoth deficiency in insulin production andinsulin resistance are thought to be importantin the pathogenesis of noninsulin-dependentdiabetes (91). There is evidence that bothmay be determined in fetal life. Men andwomen with low birth weight have a highprevalence of the insulin resistance syndrome(92) in which impaired glucose tolerance,hypertension, and raised serum triglycerideconcentrations occur in the same patient. Thepatients are insulin resistant and have hyper-insulinaemia. Table 5 shows results for a sam-ple of the men in Hertfordshire. Phillips et al.(93) carried out insulin tolerance tests on 103men and women in Preston. At any value ofadult body mass index, insulin resistance wasgreater in people who had a low ponderalindex at birth. In addition, at each ponderalindex, resistance was greater in those withhigh body mass index. The greatest meanresistance was therefore in those with lowponderal index at birth but high body massindex as adults.A recent study in San Antonio, Texas, con-
firmed the association between low birthweight and insulin resistance in a different eth-nic group. In 30-year-old Mexican Americansand non-Hispanic white people, those withlower birth weight had a higher prevalence ofthe insulin resistance syndrome (94). Amongmen and women in the lowest third of thebirth weight distribution and the highest thirdof current body mass index, 25% had the syn-drome. In contrast, none of the people in thehighest third of birth weight and lowest thirdof current body mass index had the syndrome.In a study of young adults in the city ofHaguenau, France, those who had hadintrauterine growth retardation had raisedplasma insulin concentrations when fastingand after a standard glucose challenge (95).They did not show any of the other abnormal-ities that occur in the insulin resistance syn-drome. An interpretation of this is that insulinresistance is a primary abnormality to which
other changes are secondary. A recent study ofmen and women who were in utero during theDutch famine provides direct evidence thatfetal undernutrition can program insulin resis-tance and noninsulin-dependent diabetes (96).Men and women exposed to famine in uterohad higher 2-hr plasma glucose concentrationsthan those born before or those conceived afterthe famine. They also had higher fasting pro-insulin and 2-hr plasma insulin concentra-tions, suggesting insulin resistance.
Law et al. reported associations betweenthinness at birth and raised 30-minute plasmaglucose concentrations in 7-year old childrenin Salisbury, UK (97). Whincup et al. studiedBritish children 10-11 years of age and foundthat those who had lower birth weight hadraised plasma insulin concentrations bothfasting and after oral glucose (98). This isconsistent with the association between lowbirth weight and insulin resistance. Amongthese children, however, the plasma glucoseconcentrations of those who had low birthweight were unaltered, which implies thatdespite being insulin resistant they were ableto maintain glucose homeostasis. In contrastYajnik and colleagues found that Indian chil-dren 4 years of age who had low birth weightshad raised plasma glucose and insulin concen-trations, suggesting that at the levels of poorfetal growth and insulin resistance that prevailin India, even young children are unable tomaintain glucose homeostasis (99). Forresterand colleagues found an association betweenshortness at birth and reduced glucose toler-ance among children in Jamaica, in whomthe serum glycated hemoglobin levels roseprogressively between those who were 52 cmor more in length at birth and those whowere 46 cm or less (100). These findings inchildren provide further support for thehypothesis that noninsulin-dependent dia-betes originates from impaired developmentin utero and that the seeds of diabetes in thenext generation have already been sown andare apparent in today's children.
MechanismsThe processes that link thinness at birth withinsulin resistance in adult life are not known.Babies born at term with a low ponderal indexhave a reduced mid-arm circumference, which
Table 5. Prevalence of the insulin resistance syndrome in men 59-70 years of age according to birth weight.Odds ratio adjusted
Birth weight, % with insulin for body mass indexlb (kg) No. of men resistance syndrome (95% confidence interval)<5.5(2.50) 20 30 18(2.6-118)
6.5(2.95) 54 19 8.4(1.5-49)7.5(3.41) 114 17 8.5(1.5-46)8.5(3.86) 123 12 4.9(0.9-27)9.5(4.31) 64 6 2.2(0.3-14)
> 9.5 (4.31) 32 6 1.0All 407 14
implies that they have a low muscle bulk aswell as less subcutaneous fat (101). It istherefore possible that thinness at birth isassociated with abnormalities in the structureand function of muscle that develop inmidgestation and persist into adult life, inter-fering with insulin's ability to promote glu-cose uptake. Magnetic resonance spectroscopystudies show that people who were thin atbirth have lower rates of glycolysis and gly-colytic adenosine triphosphate productionduring exercise (102). In response to undernu-trition a fetus may reduce its metabolic depen-dence on glucose and increase oxidation ofother substrates, including amino acids andlactate. This has led to the hypothesis that aglucose-sparing metabolism persists into adultlife, and that insulin resistance arises as a con-sequence of similar processes, possibly becauseof reduced rates of glucose oxidation ininsulin-sensitive peripheral tissues.
When the availability of nutrients to thefetus is restricted, concentrations of anabolichormones including insulin and IGF-I fall,while catabolic hormones, including gluco-corticoids rise. Persisting hormonal changescould underlie the development of insulinresistance. Bjorntorp has postulated that glu-cocorticoids, growth hormone, and sexsteroids may play a major role in the evolutionof the metabolic syndrome (103).
Recent advances in assay methodologymake it possible to specifically measureplasma concentrations of the precursor ofinsulin, 32-33-split proinsulin (104,105).Higher concentrations are found in peoplewho had low birth weight and low weight at1 year (29). The significance of raised plasmasplit proinsulin concentrations remainsunclear, but they are thought to indicate bothinsulin resistance and pancreatic P-celldysfunction.
Insulin DeficiencyInfants who are small for dates have fewer,B cells (106). There are conflicting reports onwhether the P-cell mass is reduced in subjectswith noninsulin-dependent diabetes (107). Asa working hypothesis it seems reasonable topropose that nutritional and other factorsdetermining fetal and infant growth influencethe size and function of the adult pancreaticP-cell complement. Whether and when non-insulin dependent diabetes supervenes will bedetermined by the rate of attrition of D cellswith aging, and by the development ofinsulin resistance, of which obesity is animportant determinant (108).
In a sample of 103 of the men andwomen who participated in the Prestonstudy, Phillips and colleagues (109) mea-sured insulin secretion following intravenousinfusion of glucose. The insulin responsewas not related to birth weight or other
Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000 549

OSMOND AND BARKER
measurements at birth. This argues against alink between reduced fetal growth andinsulin deficiency in adult life. Similarly, astudy of men in Stockholm found no associ-ation between birth weight and insulinresponses to infused glucose (110). Birthlength and other measures of birth size werenot available in that study. There was, how-ever, an association between short statureand a low insulin response. It is possible thatinsulin resistance in adult life changesinsulin secretion and obscures associationswith fetal growth. Studies of younger peoplemay resolve this; a study by Robinson andcolleagues (111) of men 21 years of ageshowed that those with lower birth weighthad reduced plasma insulin concentrationsat 30 min. Another study of men of similarage showed that a low insulin response toglucose was associated with a high placentalweight and a high ratio of placental weightto birth weight. This study also confirmedthe association between low insulin secretionand short stature (112). In contrast a studyof young Pima Indians showed that thosewith low birth weight had evidence ofinsulin resistance but no defect in insulinsecretion (113).
In Mysore, South India, men and womenwith noninsulin-dependent diabetes showedsigns of both insulin resistance and insulindeficiency (114). A high prevalence of insulinresistance, central obesity, and noninsulin-dependent diabetes in people from SouthIndia living in Britain has been observed(115,116). The study of men and women inMysore again showed this. Those who hadnoninsulin-dependent diabetes also had a lowinsulin increment after a standard challenge,indicating that they were insulin deficient aswell as resistant. However, whereas insulinresistance was associated with low birthweight, noninsulin-dependent diabetes wasassociated with shortness at birth in relationto birth weight (i.e., a high ponderal index)and with maternal adiposity.
These findings led to a novel explanationfor the epidemic of noninsulin-dependentdiabetes in urban and migrant Indian popula-tions (114). Widespread fetal undernutritionpredisposes the Indian population to insulinresistance. When these people move to cities,their levels of physical activity diminish.Young women, no longer required to do agri-cultural work or walk long distances to fetchwater and firewood, become fatter and moreinsulin resistant. They are therefore unable tomaintain glucose homeostasis during preg-nancy, even at relatively low levels of obesity,and become hyperglycemic, though not nec-essarily diabetic. It is known that high plasmaglucose concentrations within the normalrange influence fetal growth and lead tomacrosomia (117).
Programming of SerumCholesterol and ClottingFactor ConcentrationsStudies in Sheffield, UK, show that theneonate who has a short body and low birthweight in relation to the size of its head,although within the normal range of birthweight, has persisting disturbances of choles-terol metabolism and blood coagulation(118-120). Disproportion in body length rel-ative to head size is thought to result fromundernutrition in late gestation. The fetusdiverts oxygenated blood away from thetrunk to sustain the brain. This affects thegrowth of the liver, of which two functions,regulation of cholesterol and of blood clot-ting, seem to be permanently perturbed.Disturbance of cholesterol metabolism andblood clotting are both important features ofcoronary heart disease.
The Sheffield records included abdominalcircumference at birth as well as length, and itwas reduction specifically in this birth mea-
surement that predicted raised serum low-density lipoprotein cholesterol and plasmafibrinogen concentrations in adult life(118,119). The differences in concentrationsacross the range of abdominal circumference(Table 6) were large, statistically equivalent to
30% differences in mortality caused by coro-
nary heart disease. The findings for plasmafibrinogen concentrations, a measure of bloodcoagulability, were of similar size.
Because both cholesterol and fibrinogenmetabolism are regulated by the liver, one
interpretation of these findings is thatreduced abdominal circumference at birthreflects impaired liver growth and consequent
reprogramming of liver metabolism. Furtherunderstanding of liver programming may
come more rapidly from animal studies thanfrom human studies. Experiments with rats
have shown that undernutrition in utero can
permanently alter the balance of two liverenzymes, phosphoenol-pyruvate carboxyki-nase and glucokinase, that are involved in thesynthesis and breakdown of glucose, respec-
tively (121). A low-protein diet during gesta-tion permanently changes the balance ofenzyme activity in the offspring in favor ofsynthesis. It is thought that this reflectsenhancement of cell replication in the area
around the portal vein, which carries bloodfrom the gut to the liver, at the expense ofthe cells around the hepatic vein. Theseexperiments are of particular interest becausethey show that undernutrition after birthhas no effect and because the two enzymesare not normally synthesized until afterbirth, which suggests that their productioncan be regulated before the genes encodingthem are transcribed.
Infant and Childhood GrowthTwo studies of coronary heart disease and itsrisk factors in adult life contain data on bothbirth measurements and postnatal growth.These are the studies in Hertfordshire, UK,and Helsinki, Finland.
In Hertfordshire, health visitors recordedthe weight of infants when they reached1 year of age. In men there have been 853deaths from coronary heart disease (18). Riskwas more strongly associated with weight at1 year of age (x2, = 27.5, p < 0.0001) thanwith birth weight (x2i = 8.5, p < 0.005).Standardized mortality ratios fell progres-sively from 105 for those who weighed up to18 lb down to 42 for those who weighed27 lb or more, a relative risk of 2.5. However,in women, among whom there were only 88deaths, the closer association was with birthweight (x21 = 4.3, p = 0.04). Weight at 1 yearof age is more weakly associated with systolicblood pressure than is birth weight (122),equally as associated with glucose tolerance(29) and serum cholesterol concentrations(118), and more strongly associated withplasma clotting factor concentrations (119).
In Helsinki the maternity hospital recordshave been linked to school records, whichinclude measurements of height and weightevery 6 months between 6 and 16 years of age(123). Death from coronary heart disease wasassociated with low birth weight and morestrongly with a low ponderal index at birth(Table 2). Men who died from coronaryheart disease had an above-average body massindex at all ages from 6 to 16 years. In asimultaneous regression the hazard ratio fordeath from the disease increased by 14%(95% confidence interval 8-19%; p <0.0001) for each unit (kg/m3) decrease inponderal index at birth and by 22%(10-36%, p = 0.0001) for each unit (kg/m2)
Table 6. Mean serum cholesterol concentrations according to abdominal circumference at birth in men and women50-53 years of age.
Abdominal circumference, Total cholesterol Low-density lipoproteininches (cm) No. of people (mmol/L) cholesterol (mmol/L)
< 1 1.5 (29.2) 53 6.7 4.512.0(30.5) 43 6.9 4.612.5 (31.8) 31 6.8 4.413.0 (33.0) 45 6.2 4.0
> 13.0 (33.0) 45 6.1 4.0All 217 6.5 4.3
Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000550

EARLY GROWTH AND HEART DISEASE, DIABETES, HYPERTENSION
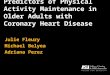
increase in body mass index at 11 years ofage. Thus, the highest death rates from coro-nary heart disease occurred in boys who werethin at birth but whose weight caught up sothat they had an average or above-averagebody mass index from 6 years of age.However, there was also some evidence of aninteraction. Figure 1 shows contours of haz-ard ratio for death from coronary heart dis-ease. Those with a high ponderal index atbirth cross few contour lines by developing ahigh body mass index in childhood. In con-trast those with a low ponderal index at birthincrease their risk more dramatically by devel-oping a high body mass index. Conversely, itis insufficient to know only the body massindex of an 11-year-old boy. His future riskof death from coronary heart disease dependson his intrauterine growth. To predict thefuture, we need to know both the present andthe past.
Catch-up growth could be associated withadverse outcomes through altered body com-position in later life. Babies who are thin atbirth lack muscle. It is possible that if theydevelop a high body mass index in childhood,they have a disproportionately high fat mass.
SummaryAssociations between low birth weight andcoronary heart disease, raised blood pressure,and noninsulin-dependent diabetes have beenrepeatedly demonstrated. Relatively fewstudies have had access to measurements ofbirth size other than weight. This is a majorlimitation because birth weight is a crudesummary index of growth, and because bloodpressure and glucose/insulin metabolism canbe programmed by nutritional influences thatdo not alter birth weight. Studies that indudebirth length suggest that thinness at birth is
20
iz-
1.6cc
o 1.0e1.4'- 16-cc
CD
14 1.2 0.4>-~~~~~~~~A0.61.0 0.810I
20 22 24 26 28 30 32
Ponderal index at birth (kg/m3)Figure 1. Hazard ratios for death from coronary heartdisease according to ponderal index at birth and bodymass index at 11 years of age. Arrows indicate averagevalues. Subjects are 3,641 men born at the HelsinkiUniversity Central Hospital from 1924 to 1933.
associated with the development of insulinresistance. Other associations, for example,those with blood pressure, are less consistent.One interpretation of this is that blood pres-sure can be programmed at various stages ofgestation, whereas insulin resistance is pro-grammed in late gestation, when dispropor-tionate fetal growth is manifest. This is,however, an uncertain inference and is notborne out by the Dutch famine study inwhich reduced glucose tolerance was associ-ated with exposure to famine at any stage ofgestation. Associations between placental sizeand later disease differ among studies. In ani-mals placental responses to undernutritiondepend on the mother's nutritional statebefore pregnancy, but we have little informa-tion about this in humans. However, placen-tal growth and function do seem to beinfluences that program the fetus, even whenthe placenta is not clinically abnormal.
The FutureIf we are to use the information outlinedhere, to prevent disease we need to progressbeyond epidemiologic associations to greaterunderstanding of the cellular and molecularprocesses that underlie them. We need toknow what factors limit the delivery of nutri-ents and oxygen to the human fetus, how thefetus adapts to a limited supply, how theseadaptations program the structure and physi-ology of the body, and by what molecularmechanisms nutrients and hormones altergene expression. Further research requires astrategy of interdependent clinical, animal,and epidemiologic studies.
As yet, we do not know the true impact ofmaternal nutrition on fetal development. Therelatively disappointing effects of nutritionalinterventions in pregnancy on fetal growth inhumans have led to the view that fetal devel-opment is little affected by changes in mater-nal nutrition except in circumstances offamine. However, it is clear that birth weightalone is an inadequate summary measure offetal growth; we need a more sophisticatedview of optimal fetal development that takesaccount of the long-term sequelae of fetaladaptations to undernutrition.
REFERENCES AND NOTES
1. Widdowson EM, McCance RA. A review: new thoughts ongrowth. Pediatr Res 9:154-156 (1975).
2. Lucas A. Programming by early nutrition in man. In: TheChildhood Environment and Adult Disease (Bock GR, Whelen J,eds). Chichester:Wiley, 1991:38-55.
3. Lucas A. Role of nutritional programming in determining adultmorbidity. Arch Dis Child 71:288-290 (1994).
4. Diamond J. Pearl Harbor and the Emperor's physiologists. NatHist 12:2-7 (1991).
5. Barker DJP. Fetal origins of coronary heart disease. Br Med J311:171-174 (1995).
6. Barker DJP. Mothers, Babies and Health in Later Life.Edinburgh:Churchill Livingstone, 1996.
7. Fowden AL. Endocrine regulation of fetal growth. Reprod FertilDev 7:351-363 (1995).
8. Harding JE, Johnston BM. Nutrition and fetal growth. ReprodFertil Dev 7:539-547 (1995).
9. Widdowson EM. Immediate and long-term consequences ofbeing large or small at birth: a comparative approach. In: Size atBirth. Ciba Symposium 27 (Elliott K, Knight J, eds). Amsterdam:Elsevier, 1974;65-82.
10. Hinchliffe SA, Lynch MRJ, Sargent PH, Howard CV, Van VeizenD. The effect of intrauterine growth retardation on the develop-ment of renal nephrons. Br J Obstet Gynaecol 99:296-301(1992).
11. Campbell AGM, Dawes GS, Fishman AP, Hyman Al. Regionalredistribution of blood flow in the mature fetal lamb. CirculationRes 21:229-235 (1967).
12. Rudolph AM. The fetal circulation and its response to stress.J Dev Physiol 6:11-19 (1984).
13. Fowden AL. The role of insulin in prenatal growth. J Dev Physiol12:173-182 (1989).
14. Oliver MH, Harding JE, Breier BH, Evans PC, Gluckman PD.Glucose but not a mixed amino acid infusion regulates plasmainsulin-like growth factor-1 concentrations in fetal sheep.Pediatr Res 34:62-65 (1993).
15. Barker DJP, Osmond C. Infant mortality, childhood nutrition andischaemic heart disease in England and Wales. Lancet1:1077-1081 (1986).
16. Barker DJP, Bull AR, Osmond C, Simmonds SJ. Fetal and pla-cental size and risk of hypertension in adult life. Br Med J301:259-262 (1990).
17. Barker DJP, Osmond C, Simmonds SJ, Wield GA. The relation ofsmall head circumference and thinness at birth to death from car-diovascular disease in adult life. Br Med J 306:422-426 (1993).
18. Osmond C, Barker DJP, Winter PD, Fall CHD, Simmonds SJ.Early growth and death from cardiovascular disease in women.Br Med J 307:1519-1524 (1993).
19. Leon DA, Lithell H, Vagero D, McKeigue P, Koupilova I.Biological and social influences on mortality in a cohort of15,000 Swedes followed from birth to old age [Abstract). JEpidemiol Community Health 51:594 (1997)
20. Frankel S, Elwood P, Sweetnam P, Yarnell J, Davey Smith G.Birthweight, body-mass index in middle age, and incident coro-nary heart disease. Lancet 348:1478-1480 (1996).
21. Rich-Edwards JW, Stampfer MJ, Manson JE, Rosner B,Hankinson SE, Colditz GA, Willett WC, Hennekens CH. Birthweight and risk of cardiovascular disease in a cohort of womenfollowed up since 1976. Br Med J 315:396-400 (1997).
22. Stein CE, Fall CHD, Kumaran K, Osmond C, Cox V, Barker DJP.Fetal growth and coronary heart disease in South India. Lancet348:1269-1273 (1996).
23. Martyn CN, Barker DJP, Osmond C. Mothers' pelvic size, fetalgrowth, and death from stroke and coronary heart disease inmen in the UK. Lancet 348:1264-1268 (1996).
24. Forsen T, Eriksson JG, Tuomilehto J, Teramo K, Osmond C,Barker DJP. Mother's weight in pregnancy and coronary heartdisease in a cohort of Finnish men: follow up study. Br Med J315:837-840 (1997).
25. Kramer MS, Joseph KS. Commentary: Enigma of fetal/infantorigins hypothesis. Lancet 348:1254-1255 (1996).
26. Paneth N, Susser M. Early origin of coronary heart disease (the"Barker hypothesis"). Br Med J 310:411-412 (1995).
27. Elford J, Whincup P, Shaper AG. Early life experience and adultcardiovascular disease: longitudinal and case-control studies.lnt J Epidemiol 20:833-844 (1991).
28. Ben-Shlomo Y, Davey Smith G. Deprivation in infancy or in adultlife: which is more important for mortality risk? Lancet337:530-534 (1991).
29. Hales CN, Barker DJP, Clark PMS, Cox LJ, Fall C, Osmond C,Winter PD. Fetal and infant growth and impaired glucose toler-ance at age 64. Br Med J 303:1019-1022 (1991).
30. Barker DJP, Osmond C, Golding J, Kuh D, Wadsworth MEJ.Growth in utero, blood pressure in childhood and adult life, andmortality from cardiovascular disease. Br Med J 298:564-567(1989).
31. Law CM, Shiell AW. Is blood pressure inversely related to birthweight? The strength of evidence from a systematic review ofthe literature. J Hypertens 14:935-941 (1996).
32. Koupilova I, Leon DA, Vagero D. Can confounding by sociode-mographic and behavioural factors explain the associationbetween size at birth and blood pressure at age 50 in Sweden?J Epidemiol Community Health 51:14-18 (1997).
33. Rose G. Sick individuals and sick populations. lnt J Epidemiol14:32-38 (1985).
34. Leon DA, Koupilova I, Lithell HO, Berglund L, Mohsen R, Vagero0, Lithell U-B, McKeigue PM. Failure to realise growvth potentialin utero and adult obesity in relation to blood pressure in 50year old Swedish men. Br Med J 312:401-406(1996).
Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000 551

OSMOND AND BARKER
35. Barker DJP, Godfrey KM, Osmond C, Bull A. The relation of fetallength, ponderal index and head circumference to blood pres-sure and the risk of hypertension in adult life. Paediatr PerinatEpidemiol 6:35-44(1992).
36. Barker DJP, Gluckman PD, Godfrey KM, Harding JE, Owens JA,Robinson JS. Fetal nutrition and cardiovascular disease in adultlife. Lancet 341:938-941 (1993).
37. law CM, Barker DJP, Bull AR, Osmond C. Maternal and fetalinfluences on blood pressure. Arch Dis Child 66:1291-1295(1991).
38. Taylor SJC, Whincup PH, Cook DG, Papacosta D, Walker M.Size at birth and blood pressure; cross sectional study in 8-11year old children. Br Med J 314:475-480(1997).
39. Moore VM, Miller AG, Boulton TJC, Cockington RA, HamiltonCraig I, Magarey AM, Robinson JS. Placental weight, birthmeasurements, and blood pressure at age 8 years. Arch DisChild 74:538-541 (1996).
40. Whincup P, Cook D, Papacosta 0, Walker M. Birth weight andblood pressure: cross sectional and longitudinal relations inchildhood. Br Med J 311:773-776 (1995).
41. Campbell DM, Hall MH, Barker DJP, Cross J, Shiell AW,Godfrey KM. Diet in pregnancy and the offspring's blood pres-sure 40 years later. Br J Obstet Gynaecol 103:273-280 (1996).
42. McCrabb GJ, Egan AR, Hosking BJ. Maternal undernutritionduring mid-pregnancy in sheep; variable effects on placentalgrowth. J Agric Sci 118:127-132 (1992).
43. McCrabb GJ, Egan AR, Hosking BJ. Maternal undernutritionduring mid-pregnancy in sheep. Placental size and its relation-ship to calcium transfer during late pregnancy. Br J Nutr65:157-168 (1991).
44. Martyn CN, Barker DJP, Jespersen S, Greenwald S, Osmond C,Berry C. Growth in utero, adult blood pressure, and arterialcompliance. Br Heart J 73(2):116-121 (1995).
45. Whincup PH, Cook DG, Shaper AG. Early influences on bloodpressure: a study of children aged 5-7 years. Br Med J299:587-591 (1989).
46. Churchill D, Perry IJ, Beevers DG. Ambulatory blood pressure inpregnancy and fetal growth. Lancet 349:7-10 (1997).
47. Langley SC, Jackson AA. Increased systolic blood pressure inadult rats induced by fetal exposure to maternal low proteindiets. Clin Sci 86:217-222 (1994).
48. Whincup P, Cook D, Papacosta 0, Walker M, Perry I. Maternalfactors and development of cardiovascular risk: evidence from astudy of blood pressure in children. J Hum Hypertens8:337-343 (1994).
49. Godfrey KM, Forrester T, Barker DJP, Jackson AA, Landman JP,Hall JSE, Cox V, Osmond C. Maternal nutritional status in preg-nancy and blood pressure in childhood. Br J Obstet Gynaecol101:398-403 (1994).
50. Clark PM, Atton C, Law CM, Shiell A, Godfrey K, Barker DJP.Weight gain in pregnancy, triceps skinfold thickness and bloodpressure in the offspring. Obstet Gynaecol 91:103-107 (1998).
51. Margetts BM, Rowland MGM, Foord FA, Cruddas AM, Cole TJ,Barker DJP. The relation of maternal weight to the blood pres-sures of Gambian children. Int J Epidemiol 20(4):938-943 (1991).
52. Lever AF, Harrap SB. Essential hypertension: a disorder of growthwith origins in childhood? J Hypertens 10:101-120 (1992).
53. Kingdom JCP, McQueen J, Connell JMC, Whittle MJ. Fetalangiotensin 11 levels and vascular (Type 1) angiotensin receptorsin pregnancies complicated by intrauterine growth retardation.Br J Obstet Gynaecol 100:476-482 (1993).
54. Martyn CN, Lever AF, Morton JJ. Plasma concentrations ofinactive renin in adult life are related to indicators of foetalgrowth. J Hypertens 14:881-886(1996).
55. Mackenzie HS, Brenner BM. Fewer nephrons at birth: a missinglink in the etiology of essential hypertension? Am J Kidney Dis26:91-98 (1995).
56. Brenner BM, Chertow GM. Congenital oligonephropathy: aninborn cause of adult hypertension and progressive renal injury?Curr Opin Nephrol Hypertens 2:691-695 (1993).
57. Merlet-benichou C, Leroy B, Gilbert T, Lelievre-Pegorier M.Retard de croissance intra-uterin et deficit en nephrons [Transl:Intrauterine growth retardation and inborn nephron deficit].Medecine/Sciences 9:777-780 (1993).
58. Konje JC, Bell SC, Morton JJ, de Chazal R, Taylor DJ. Humanfetal kidney morphometry during gestation and the relationshipbetween weight, kidney morphometry and plasma active reninconcentration at birth. Clin Sci 91:169-175 (1996).
59. Weder AB, Schork NJ. Adaptation, allometry, and hypertension.Hypertension 24:145-156 (1994).
60. Edwards CRW, Benediktsson R, Lindsay RS, Seckl JR.Dysfunction of placental glucocorticoid barrier: link betweenfetal environment and adult hypertension? Lances 1994341:355-357 (1994).
61. Seckl JR. Glucocorticoids and small babies. 0 J Med87:259-262 (1994).
62. Clark PM, Hindmarsh PC, Shiell AW, Law CM, Honour JW,Barker DJP. Size at birth and adrenocortical function in child-hood. Clin Endocrinol 45:721-726 (1996).
63. Fall CHD, Pandit AN, law CM, Yajnik CS, Clark PM, Breier B,Osmond C, Shiell AW, Gluckman PD, Barker DJP. Size at birthand plasma insulin-like growth factor-1 concentrations. ArchDis Child 73:287-293 (1995).
64. Ferns GAA, Motani AS, Anggard EE. The insulin-like growth fac-tors: their putative role in atherogenesis. Artery 18:197-225(1991).
65. Lehmann ED. Pulse wave velocity as a marker of vascular dis-ease [Reply]. Lancet 348:1587 (1996).
66. Safar ME, Levy B, Laurent S, London GM. Hypertension and thearterial system: clinical and therapeutic aspects. Hypertension8 (suppl 7):S1 13-S1 19 (1990).
67. Folkow B. Structure and function of the arteries in hypertension.Am Heart J 114:938-947 (1987).
68. Martyn CN, Greenwald SE. Impaired synthesis of elastin inwalls of aorta and large conduit arteries during early develop-ment as an initiating event in pathogenesis of systemic hyper-tension. Lancet 350:953-955 (1997).
69. Rucker RB, Tinker D. Structure and metabolism of arterialelastin. lnt Rev Exp Pathol 17:1-47 (1977).
70. Rucker RB, Dubick MA. Elastin metabolism and chemistry:potential roles in lung development and structure. EnvironHealth Perspect 55:179-191 (1984).
71. AI-Ghazali W, Chita SK, Chapman MG, Allan LD. Evidence ofredistribution of cardiac output in asymmetrical growth retarda-tion. Br J Obstet Gynaecol 96:697-704 (1989).
72. Dicke JM. Poor obstetrical outcome. In: Clinical Obstetrics(Pauerstein CJ, ed). New York:John Wiley and Sons,1987:421-439.
73. Rizzo G, Arduini D. Fetal cardiac function in intrauterine growthretardation. Am J Obstet Gynecol 165:876-882 (1991).
74. Veille JC, Hanson R, Sivakoff M, Hoen H, Ben-Ami M. Fetal car-diac size in normal, intrauterine growth retarded, and diabeticpregnancies. Am J Perinatol 10:275-279 (1993).
75. Murotsuki J, Challis JRG, Han VKM, Fraher LJ, Gagnon B.Chronic fetal placental embolization and hypoxemia causehypertension and myocardial hypertrophy in fetal sheep. Am JPhysiol 272:R201-R207 (1997).
76. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP.Prognostic implications of echocardiographically determinedleft ventricular mass in the Framingham heart study. N EngI JMed 332:1561-1566 (1990).
77. Vijayakumar M, Fall CHD, Osmond C, Barker DJP. Birth weight,weight at one year, and left ventricular mass in adult life. BrHeart J 73:363-367 (1995).
78. Zureik M, Bonithon-Kopp C, Lecomte E, Siest G, Ducimetiere P.Weights at birth and in early infancy, systolic pressure, and leftventricular structure in subjects aged 8 to 24 years.Hypertension 27[part 1]:339-345 (1996).
79. Chapman N, Mohamudally A, Cerutti A, Stanton A, Aihie SayerA, Cooper C, Barker DJP, Rauf A, Evans J, Wormald R, et al.Retinal vascular network architecture in low-birth-weight men.J Hypertens 15:1449-1453 (1997).
80. Leeson CPM, Whincup PH, Cook DG, Donald AE, Papacosta 0,Lucas A, Deanfield JE. Flow-mediated dilation in 9- to 11-yearold children. The influence of intrauterine and childhood factors.Circulation 96:2233-2238 (1997).
81. Julius S, Krause L, Schork NJ, Mejia AD, Jones KA, van de VenC, Johnson EH, Sekkarie MA, Kjeldsen SE, Petrin J.Hyperkinetic borderline hypertension in Tecumseh, Michigan. JHypertens 9:77-84 (1991).
82. Esler M, Julius S, Zweifler A. Mild high-renin essential hyper-tension: neurogenic human hypertension? N EngI J Med296:405-411 (1977).
83. Phillips DIW, Barker DJP. Association between low birthweightand high resting pulse in adult life: Is the sympathetic nervoussystem involved in programming the insulin resistance syn-drome? Diabet Med 14:673-677 (1997).
84. Mitchell BD, Valdez R, Hazuda HP, Haffner SM, Monterrosa A,Stern MP. Differences in prevalence of diabetes and impairedglucose tolerance according to maternal or paternal history ofdiabetes. Diabetes Care 16:1262-1267 (1993).
85. Fall CHD, Osmond C, Barker DJP, Clark PMS, Hales CN, StirlingY, Meade TW. Fetal and infant growth and cardiovascular riskfactors in women. Br Med J 310:428-432 (1995).
86. Phipps K, Barker DJP, Hales CN, Fall CHD, Osmond C, ClarkPMS. Fetal growth and impaired glucose tolerance in men andwomen. Diabetologia 36:225-228 (1993).
87. Lithell HO, McKeigue PM, Bergland L, Mohsen B, Lithell UB,
Leon DA. Relation of size at birth to non-insulin dependent dia-betes and insulin concentrations in men aged 50-60 years. BrMed J 312:406-410 (1996).
88. Olah KS. Low matemal birthweight - an association with impairedglucose tolerance in pregnancy. J Obstet Gynaecol 16:5-8 (1996).
89. Curhan GC, Willett WC, Rimm EB, Stampfer MJ. Birth weightand adult hypertension and diabetes mellitus in US men[Abstract]. Am J Hypertens 9:11 A (1996).
90. McCance DR, Pettitt DJ, Hanson RL, Jacobsson LTH, KnowlerWC, Bennett PH. Birth weight and non-insulin dependent dia-betes: thrifty genotype, thrifty phenotype, or surviving smallbaby genotype? Br Med J 308:942-945 (1994).
91. DeFronzo RA. The triumvirate: beta cell, muscle, liver. A collu-sion responsible for NIDDM. Diabetes 1988;37:667-687.
92. Barker DJP, Hales CN, Fall CHD, Osmond C, Phipps K, ClarkPMS. Type 2 (non-insulin-dependent) diabetes mellitus, hyper-tension and hyperlipidaemia (syndrome X): relation to reducedfetal growth. Diabetologia 36:62-67 (1993).
93. Phillips DIW, Hirst S, Clark PMS, Hales CN, Osmond C. Fetalgrowth and insulin secretion in adult life. Diabetologia37:592-596 (1994).
94. Valdez R, Athens MA, Thompson GH, Bradshaw BS, Stern MP.Birthweight and adult health outcomes in a biethnic populationin the USA. Diabetologia 37:624-631 (1994).
95. Leger J, Levy-Marchal C, Bloch J, Pinet A, Chevenne D, PorquetD, Collin D, Czernichow P. Reduced final height and indicationsfor insulin resistance in 20 year olds born small for gestationalage: regional cohort study. Br Med J 315:341-347 (1997).
96. Ravelli ACJ, van der Meulen JHP, Michels RPJ, Osmond C,Barker DJP, Hales CN, Bleker OP. Glucose tolerance in adultsafter prenatal exposure to the Dutch famine. Lancet351:173-177 (1998).
97. Law CM, Gordon GS, Shiell AW, Barker DJP, Hales CN.Thinness at birth and glucose tolerance in seven year old chil-dren. Diabet Med 12:24-29 (1995).
98. Whincup PH, Cook DG, Adshead F, Taylor SJC, Walker M,Papacosta D, Alberti KGMM. Childhood size is more stronglyrelated than size at birth to glucose and insulin levels in 10-11-year-old children. Diabetologia 40:319-326 (1997).
99. Yajnik CS, Fall CHD, Vaidya U, Pandit AN, Bavdekar A, Bhat DS,Osmond C, Hales CN, Barker DJP. Fetal growth and glucose andinsulin metabolism in four-year-old Indian children. Diabet Med12:330-336 (1995).
100. Forrester TE, Wilks RJ, Bennett Fl, Simeon D, Osmond C, AllenM, Chung AP, Scott P. Fetal growth and cardiovascular risk fac-tors in Jamaican schoolchildren. Br Med J 312:156-160 (1996).
101. Robinson SM, Wheeler T, Hayes MC, Barker DJP, Osmond C.Fetal heart rate and intrauterine growth. Br J Obstet Gynaecol98:1223-1227 (1996).
102. Taylor DJ, Thompson CH, Kemp GJ, Barnes PRJ, Sanderson AL,Radda GK, Phillips DIW. A relationship between impaired fetalgrowth and reduced muscle glycolysis revealed by 31p magneticresonance spectroscopy. Diabetologia 38:1205-1212 (1995).
103. Bjorntorp P. Insulin resistance: the consequence of a neuroen-docrine disturbance? Int J Obesity 19 (suppl 1:S6-S10 (1995).
104. Sobey WJ, Beer SF, Carrington CA, Clark PM, Frank BH, Gray IP,Luzio SD, Owens DR, Schneider AE, Siddle K. Sensitive andspecific two-site immunoradiometric assays for human insulin,proinsulin, 65-66 split and 32-33 split proinsulins. Biochem J260:535-541 (1989).
105. Temple RC, Carrington CA, Luzio SD, Owens DR, Schneider AE,Sobey WJ, Hales CN. Insulin deficiency in non-insulin-depen-dent diabetes. Lancet i:293-295 (1989).
106. Van Assche FA, Aerts L. The fetal endocrine pancreas. ContribGynecol Obstet 5:44-57 (1979).
107. Hellerstrom C, Swenne I, Andersson A. Islet cell replication anddiabetes. In: The pathology of the endocrine pancreas in dia-betes (Lefebvre PJ, Pipeleers DG, eds.) Heidelberg:Springer,1988;141-170.
108. Hales CN, Barker DJP. Type 2 (non-insulin-dependent) diabetesmellitus: the thrifty phenotype hypothesis. Diabetologia35:595-601 (1992).
109. Phillips DIW, Barker DJP, Hales CN, Hirst S, Osmond C.Thinness at birth and insulin resistance in adult life.Diabetologia 37:150-154 (1994).
110. Alvarsson M, Efendic S, Grill VE. Insulin responses to glucose inhealthy males are associated with adult height but not withbirth weight. J Intern Med 236:275-279(1994).
111. Robinson S, Walton RJ, Clark PM, Barker DJP, Hales CN,Osmond C. The relation of fetal growth to plasma glucose inyoung men. Diabetologia 35:444-446 (1992).
112. Wills J, Watson JM, Hales CN, Phillips DIW. The relation offetal growth to insulin secretion in young men. Diabet Med13:773-774 (1996).
552 Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000

EARLY GROWTH AND HEART DISEASE, DIABETES, HYPERTENSION
113. Leger J, Levy-Marchal C, Bloch J, Pinet A, Benali K, Porquet D,Collin D, Czernichow P. Evidence for insulin-resistance develop-ing in young adults with intra-uterine growth retardation[Abstract]. Diabetologia 40:A53 (1997).
114. Fall CHD, Stein CE, Kumaran K, Cox V, Osmond C, Barker DJP,Hales CN. Size at birth, maternal weight, and non-insulin depen-dent diabetes in South India. Diabet Med 15:220-227 (1998).
115. Mather HM, Keen H. The Southall diabetes survey: prevalenceof known diabetes in Asians and Europeans. Br Med J291:1081-1084 (1985).
116. McKeigue PM, Shah B, Marmot MG. Relation of central obesityand insulin resistance with high diabetes prevalence and car-diovascular risk in South Asians. Lancet 337:382-386 (1991).
117. Farmer G, Russell G, Hamilton-Nicol DR, Ogenbede HO, Ross IS,Pearson DWM, Thom H, Kerridge DF, Sutherland HW. The influ-ence of maternal glucdse metabolism on fetal growth, develop-ment and morbidity in h17 singleton pregnancies in nondiabeticwomen. Diabetologia i1:134-141 (1988).
118. Barker DJP, Martyn CN, Osmond C, Hales CN, Fall CHD. Growthin utero and serum cholesterol concentrations in adult life. BrMed J 307:1524-1527,(1993).
119. Barker DJP, Meade TW, Fall CHD, Lee A, Osmond C, Phipps K,Stirling Y. Relation of fetal and infant growth to plasma fibrino-gen and factor VIl cbncentrations in adult life. Br Med J304:148-152 (1992).
120. Barker DJP, Martyn CN, Osmond C, Wield GA. Abnormal liver
growth in utero and death from coronary heart disease. Br MedJ 310:703-704 (1995).
121. Hales CN, Desai M, Ozanne SE, Crowther NJ. Fishing in thestream of diabetes: from measuring insulin to the control offetal organogenesis. Biochem Soc Trans 24:341-350 (1996).
122. Law CM, deSwiet M, Osmond C, Fayers PM, Barker DJP,Cruddas AM, Fall CHD. Initiation of hypertension in utero andits amplification throughout life. Br Med J 306:24-27 (1993).
123. Eriksson JG, Forsen T, Tuomilehto J, Winter PD, Osmond C, BarkerDJP. Catch-up growth in childhood and death from coronary heartdisease: longitudinal study. Br Med J 318:427-431 (1999).
Environmental Health Perspectives * Vol 108, Supplement 3 * June 2000 553