Embed Size (px)
Citation preview

Edith Cowan UniversityResearch Online
Theses : Honours Theses
2015
Indirect approaches: A systematic review ofpaediatric dysphagia interventionsBianca PianoEdith Cowan University
This Thesis is posted at Research Online.https://ro.ecu.edu.au/theses_hons/1486
Recommended CitationPiano, B. (2015). Indirect approaches: A systematic review of paediatric dysphagia interventions. Retrieved from https://ro.ecu.edu.au/theses_hons/1486

Edith Cowan University
Copyright Warning
You may print or download ONE copy of this document for the purpose of your own research or study.
The University does not authorise you to copy, communicate or otherwise make available electronically to any other person any copyright material contained on this site.
You are reminded of the following:
• Copyright owners are entitled to take legal action against persons who infringe their copyright.
• A reproduction of material that is protected by copyright may be a copyright infringement.
• A court may impose penalties and award damages in relation to offences and infringements relating to copyright material. Higher penalties may apply, and higher damages may be awarded, for offences and infringements involving the conversion of material into digital or electronic form.

Use of Thesis
This copy is the property of Edith Cowan University. However the literary
rights of the author must also be respected. If any passage from this thesis
is quoted or closely paraphrased in a paper or written work prepared by the
user, the source of the passage must be acknowledged in the work. If the
user desires to publish a paper or written work containing passages copied
or closely paraphrased from this thesis, which passages would in total
constitute and infringing copy for the purpose of the Copyright Act, he or she
must first obtain the written permission of the author to do so.

Indirect Interventions i
Indirect Approaches: A Systematic Review of Paediatric Dysphagia Interventions
Bianca Piano
A report submitted in Partial Fulfilment of the Requirements for the Award of Bachelor
of Speech Pathology with Honours, Faculty of Computing, Health and Science,
Edith Cowan University.
Submitted (November, 2015)
I declare that this written assignment is
my own work and does not include:
(i) material from published
sources used without proper
acknowledgement; or
(ii) (ii) material copied from the
work of other students.
Signature: _____________________
Date: 16th November 2015

Indirect Interventions ii
Abstract
Background and purpose: Dysphagia can be described as difficulty within the oral,
pharyngeal and/or oesophageal phases of deglutition and occurs in approximately 80% of
children with developmental disabilities, according to the American Speech and Hearing
Association (2015). It occurs when there is impairment to the motor and/or sensory
aspects of swallowing, due to a range of disorders affecting the voluntary and reflexive
components of deglutition. The ability to swallow safely is essential in preventing
medical complications, sustaining life and maintaining social participation. Paediatric
interventions can be categorized into three broad approaches; direct, indirect and mixed.
At present, two systematic reviews have examined the efficacy of direct interventions.
Despite a large body of evidence supporting the efficacy and safety of indirect paediatric
dysphagia interventions, no studies have systematically grouped and compared the
relative effectiveness of indirect interventions, across all paediatric ages and conditions.
Methods and procedure: Following a comprehensive search of 19 databases by two
independent searches and using an identical search strategy, a systematic review
appraised 13 randomized and non-randomized control studies relating to indirect
paediatric dysphagia interventions. Based on retrieved results, indirect interventions
included modified equipment, environmental changes and altered rate of food and liquid
presentation. Articles included in the analysis were rated for quality on two separate
appraisal scales; The Cochrane Risk of Bias Tool and the Pedro Scale. Additionally,
effect size calculations and forest plots were derived to standardize and compare the
effects of individual intervention types.
Outcomes and results: The review demonstrated that whilst a lack of high quality
evidence exists in the field of paediatric dysphagia, the available RCTs are of high
methodological quality. Overall, effect size calculations demonstrate a positive trend

Indirect Interventions iii
towards improved feeding, anthropometric measures and length of hospital stay outcomes
for interventions involving modified equipment, environmental changes and altered rate
of presentation.
Conclusions: The available RCT evidence involving indirect interventions are of high
methodological quality. As effects of these interventions demonstrate positive outcomes,
Speech Pathologists should continue to implement these interventions within everyday
practice. To further validate the effects of indirect management approaches, additional
high quality research is required.
Key words: paediatric dysphagia, indirect management, intervention,
systematic review
Author: Bianca Piano
Supervisors: Dr. Charn Nang and Ms. Abigail
Lewis

Indirect Interventions iv
COPYRIGHT AND ACCESS DECLARATION
I certify that this thesis does not, to the best of my knowledge and belief;
(i) Incorporate without acknowledgement any material previously submitted for
degree or diploma in any institution of higher education;
(ii) Contain any material previously published or written by another person except
where due reference is made in the text;
(iii) Contain any defamatory material.
Signed: _________________________
Date: 16th November 2012

Indirect Interventions v
Acknowledgements
I would like to thank my Principle Supervisor Dr. Charn Nang for her guidance and
creativity throughout this project. A big thank-you to my Secondary supervisor Abigail
Lewis who has been so open to learning the methodology behind systematic reviews. You
have both been incredibly generous with your time and knowledge, and I am
exceptionally grateful for the direction you have provided.
A special thanks to Maria Woodhouse and Karen Lycett for their hard work devising the
search strategy and taking on the role of a search team. I would also like to mention
Jacqui Coombes for her statistical expertise. A big congratulations to my fellow Honors
students Ildi Bruz, Stacey Osborne and Theresa Huth, thank you for everything.
I would like to mention Timothy Chaney for supporting my studies and always listening.
Lastly, I would like to thank my Mum, Colleen Piano, to whom I dedicate this project.
You have always encouraged me to read, learn and keep going.

Indirect Interventions vi
Table of Contents
Introduction………………………………………………………………………..1
Significance of Paediatric Dysphagia.……………..………………………..1
Contribution to Evidence Based Practice….………………………………4
Management: Who and Where…….………………………………………4
Description of Interventions……….………………………………………5
Why it is Important to Conduct this Review….…………………………...9
Research Aims……………………………………………………………10
Method……………………………………………………………………………11
Research Design…………………………………………………………..11
Criteria for Considering Reviews for Inclusion...………………………...11
Search Methods for Identification of Reviews……………………………12
Data Collection and Analysis……………………………………………..14
Assessment of Methodological Quality for Included Studies…………….14
Data Synthesis…………………………………………………………….15
Results.....................................................................................................................16
Included Studies…………………………………………………………..18
Outcome Measures………………………………………………………..26
Quality Appraisal…………………………………………………………29
Reported Effects of Intervention and Data Synthesis…………………….38
Discussion………………………………………………………………………...42
Quality of Evidence……………………………………………………….42
Effects of Interventions……………………………………………………45
Potential Bias in the Review Process……………………………………...47
Implications for Research............................................................................49
Implications for Practice…………………………………………………..50
Conclusion………………………………………………………………...51
References................................................................................................................53
Appendix A..............................................................................................................64
Appendix B..............................................................................................................65
Appendix C……….… …………………………………………………………….66
Appendix D..............................................................................................................67
Appendix E …….……...…………………………………………………………..68
Appendix F….……………………………………………………………………..69
Appendix G….…………………………………………………………………….70
Appendix H….…………………………………………………………………….74
Appendix I…….…………………………………………………………………...76

Indirect Interventions 1
Indirect Approaches: A Systematic Review of Paediatric Dysphagia Interventions
Dysphagia refers to an inability or difficulty with either the motor or sensory
aspects of swallowing (Lamm, Felicia, & Cargo, 2005), and occurs as a result of
impairment to the structures involved in the oral, pharyngeal and/or oesophageal phases
of deglutition (Arvedson & Brodsky, 1993). The American Speech and Hearing
Association (ASHA, 2015) distinguishes swallowing and feeding disorders, categorizing
feeding disorders as a group of eating behaviours which may or may not be accompanied
by difficulty swallowing food and liquid. In children, disordered behaviors may include
difficulty accepting age-appropriate liquids or foods, not using appropriate feeding
devices, being unable to feed independently, food refusal and accepting a restricted
variety or quantity of food and liquid (ASHA, 2015).
Both dysphagia and feeding disorders are symptoms of various conditions
(Cichero & Murdoch, 2006) and are common in children with chromosomal, neurological
or anatomic abnormalities (Al-Sayed, Schrank, & Thach, 1994).
Few rigorous epidemiological reports of dysphagia prevalence are available for
populations of children, however one study estimates the incidence of feeding and
swallowing disorders to be 25–45% of typically developing children and up to 80% of
children with developmental disabilities (Linscheid, 2006).
Significance of paediatric dysphagia
Paediatric dysphagia is caused by impairment to the body structures and functions
associated with swallowing and feeding (Snider, Majnemer, & Darsaklis, 2011), and has
subsequent effects on everyday activity and participation (World Health Organisation’s
International Classification of Disability, Functioning and Health: ICF, 2001).

Indirect Interventions 2
Body structure and function. Following damage to cortical areas controlling
swallowing processes, the major health consequences of dysphagia include malnutrition,
dehydration (Kovar, 1997), failure to thrive (Hawdon, Beauregard, & Kennedy, 2000),
poor growth, delayed development and respiratory damage (Barbosa, Gomes, & Fischer,
2014).
In the oral phase of swallowing, impairment of cranial nerves V (trigeminal), VII
(facial) and XII (hypoglossal) (Cichero & Murdoch, 2006) may result in poor lip closure,
tongue mobility, sucking, chewing and oral transition of the bolus (Morgan, Dodrill &
Ward, 2012).
During the pharyngeal phase, cranial nerves IX (Glossopharyngeal) and X
(Vagus) (Cichero & Murdoch, 2006) may fail to invigorate causing inadequate
pharyngeal peristalsis, laryngeal elevation and excessive pooling of food or fluid in the
valleculae or pyriform sinuses (Cichero & Murdoch, 2006). This may result in aspiration,
where the supporting structures fail and there is inadequate epiglottal seal to protect the
airway, ineffective closure of the true and false vocal folds (Glass & Wolf, 1999) and/or
incoordination of swallowing and respiration (Cichero & Murdoch, 2006). Food may be
misdirected into the lungs (Lau & Smith, 2012), where respiratory rate, oxygen saturation
and overall lung development can become compromised (De Rosa Barbosa, Gomes, &
Gilberto, 2014).
In the esophageal phase, impairment of cranial nerve X (Vagus) may affect bolus
movement through the oesophagus into the stomach via peristalsis (Cichero & Murdoch,
2006).
Dysphagia may also be associated with health and nutritional compromise (Kovar,
1997). Additionally, secondary effects include increased irritability, decreased motivation
and reduced energy available for developmental activities such as play and rehabilitation

Indirect Interventions 3
(Sullivan et al., 2000). As such, Clawson, Kuchinski and Bach (2007) argue paediatric
dysphagia can be associated with a decrease in cerebral function and the exacerbation of
existing neurological impairments.
Activity and participation. According to the ICF (WHO, 2001), activities and
participation refer to an individual’s functional status. Children with dysphagia may be
limited in their ability to participate appropriately in mealtime activities (e.g., sitting at a
dinner table or adhering to socially normed mealtime behaviours) (Threats, 2007).
Additionally, as the act of eating and drinking is an important aspect of socialisation,
children may miss out on the ability to engage in food related opportunities (e.g., birthday
parties, culturally determined meals and meal time engagement). As such, children with
dysphagia may be restricted in their ability to participate in life situations (WHO, 2001)
and their ability to build relationships with family and friends can be compromised
(Snider et al., 2011). This is highlighted in a case study of a 15 year old girl who returned
to school following persistent dysphagia one year after a traumatic brain injury; the
adolescent was left socially isolated from peers during lunch because she needed to
receive non-oral feeds from the school nurse (Morgan, Ward, & Murdoch, 2004).
Research suggests the effects of dysphagia can affect an individual’s personal and
contextual modalities. For example, Anand & Scalzo (2000) argue negative, early feeding
experiences are associated with anxiety and stress. Additionally, a qualitative analysis
which sought the experiences of parents caring for children with dysphagia found that the
emotional, financial and physical burdens of caring to significantly impact the emotional
and physical well-being of parents (Cowpe-Jebson, Hanson, & Smith, 2014).

Indirect Interventions 4
Contribution to evidence based practice (EBP)
As paediatric dysphagia can impact each aspect of individual functioning, it is
important to understand effective management approaches. EBP has a role in developing
effective treatment approaches to health conditions. It is defined as the “conscientious,
explicit, and judicious use of current best evidence in making decisions about the care of
individual patients by integrating individual clinical expertise with the best available
external clinical evidence from systematic research” (Sackett, Rosenburg, Gray, Haynes
& Richardson, 1996, p.71). According to the evidence base hierarchy, various
methodologies contribute to EBP, but systematic reviews and meta-analysis comprise best
evidence (Sackett et al.).
Effective dysphagia management can target and improve individual functioning
across all aspects of the ICF. As such, the aim of management is to enhance individual
body structures and function, activity, and participation by advancing nutritional status,
physical, cognitive and psychological growth, as well as the interactions between child
and family (Arvedson, 2008). Moreover, obtaining evidence from studies designed to
answer questions about clinical practice improves management by setting new, verifiable
standards about what constitutes suitable intervention (Lass & Pannbacker, 2008).
Making well-informed decisions based on clinically relevant and systematic research is
important for minimizing harm to clients and potentially shaping health policy (Sackett et
al., 1996).
Management: who and where
As swallowing is a complex developmental process, the need for intervention is
highlighted in research (e.g., Lau & Hurst, 1999). It is important that qualified
professionals manage children with dysphagia appropriately. Speech Pathologists are
recognized by ASHA (2015) as the primary professionals involved, and “should lead both

Indirect Interventions 5
the assessment and planning” of intervention (New Zealand Guideline Group, 2006,
p.83).
Additionally, current research advocates multidisciplinary management amongst
Speech Pathologists, Nurses, Occupational Therapists, Dieticians and Paediatricians
(Arvedson, 2008; Cowpe-Jebson et al. 2014; Miller, 2001; Siktberg & Bantz, 1999).
Typically, children present with multiple medical, developmental and nutritional
concerns; therefore, collaboration from different disciplines allows for coordinated care,
which focuses on the whole child (Arvedson, 2008).
Due to the variability in age and severity of feeding and swallowing dysfunction,
children are seen in various settings (Arvedson, Clark, Lazarus, Schooling & Frymark,
2010a). For example, children may receive early intervention in acute and rehabilitation
settings. Once children reach school age, they may receive care from specialist Nurses
and Speech Pathologists (Angell, Bailey, & Stoner, 2008).
Description of interventions
A range of intervention strategies have been developed to improve the efficiency
and safety of paediatric dysphagia management (Arvedson, 2008). These interventions
can be broadly categorized into three approaches: direct, indirect and mixed.
Direct. Direct management techniques target physiological impairments (WHO,
2001) across the oral and pharyngeal phases of swallowing, and refer to stimulation,
which enhances neuromuscular control and strength (Logemann, 2000). Oral-motor
exercises, exploration, stimulation and swallowing manoeuvres (Logemann, 2000) are
used to facilitate lip closure, tongue lateralization and oral strength, whilst decreasing
tactile hypersensitivity (Ganz, 1987; Helfrich-Miller, Rector & Straka, 1986). The
underlying principle of oral-motor exercises is that by stimulating the oral structures for

Indirect Interventions 6
function, greater opportunities to practice feeding skills occur (Ganz, 1987), abnormal
reflexes diminish and oral-pharyngeal timing and coordination improves (Snider et al.,
2011).
Impairment-level interventions are supported by a growing body of current
evidence. For example, two systematic reviews (Arvedson et al., 2010a; Arvedson, Clark,
Lazarus, Schooling & Frymark, 2010b) reported promising findings following the
appraisal of direct interventions. Additionally a number of randomized control trials
report positive effects; both Arvedson and colleagues (2010a) and Pinelli and Symington
(2005) observed positive effects following a nonnutritive sucking program, including
improved oral feeding, swallowing physiology and decreased transition time to total oral
feeding following a non-nutritive sucking program. Similarly, Fucile, McFarland, Gisel,
and Lau (2012) found sensorimotor intervention enhanced nutritive sucking and swallow–
respiration coordination in pre-terms infants. This is supported by Kamhawy and
colleagues’ (2014) study of preterm infants who saw significantly higher oxygen
saturation, accelerated transition to nipple feeding, greater weight gain and earlier
discharge following a sensorimotor intervention. Finally, Bache, Pizon, Jacobs, Vaillant
and Lecomte’s (2014) RCT of preterm infants found a pre-feeding oral stimulation
program improved breastfeeding at discharge.
Indirect. Indirect techniques refer to interventions that do not directly stimulate
the oral mechanisms for swallowing (Arvedson & Brodsky, 1993) but enhance
swallowing through compensatory strategies which improve activity and participation
limitations or modify environmental factors (WHO, 2001). Examples of indirect
interventions are listed below:
Adapted feeding equipment that is used to control liquid flow and bolus size. One
RCT found bottle type to impact rate of milk transfer and oral feeding duration in

Indirect Interventions 7
very-low-birth-weight infants (Fucile, Gisel, Schanler & Lau, 2009). Additionally,
in a second RCT of 522 infants, Yilmaz, Caylan, Karacan, Bodur and Gokcay
(2014) found cup feeding to significantly increase the likelihood of preterm
infants being exclusively breastfed at discharge, without increasing length of
hospital stay.
Diet modifications are used to support swallow physiology by enhancing the
timing, coordination and sensory input of food and liquid by altering viscosity,
texture, temperature, or taste. Evidence indicates that for children with cerebral
palsy "softer food consistencies enhance feeding safety and efficiency" (Snider et
al. 2011, p.72).
Altering rate of presentation includes pacing and cue based strategies, which
control the rate of food presentation and intake. One RCT showed a semi-demand
method promoted faster attainment of oral feeding without compromising weight
gain amongst 89 infants (McCain, Gartside, Greenburg & Lott, 2001).
Prostheses refer to specifically molded feeding plates which are inserted into the
oral cavity to minimize defects and prevent regurgitation of food into the nasal
cavity (Ravichandra, Vijayaprasad & Suzan, 2010). Although there are a large
number of single case studies documenting the successful use of prostheses in
children with cleft and lip palate (Agarwal, Rana, & Shafi, 2010; Bansar et al.
2012; Chandna, Adlakha, & Singh, 2011; Erkan, Karacay, Atay, & Gunay, 2013)
one RCT investigating the effect of orthopaedics observed no improvement in
feeding efficiency or general body growth (Masarei, Wade, Mars, Sommerlad &
Sell, 2007).
For children who cannot achieve safe swallowing or adequate nutrition and
hydration, alternative avenues of intake may occur (e.g., nasogastric tube,

Indirect Interventions 8
transpyloric tube or gastrostomy) (ASHA, 2015). Current evidence suggests that
for children with neuromuscular weakness, gastrostomy feeding can improve and
maintain adequate nutrition (Hull et al., 2012). However, Wilken (2012) argues
tube feeding is associated with trauma, decreased normalcy and aversive parent-
child relationships.
Postural modifications improve oropharyngeal musculature, protect the airway
and offer safe transit of food and liquid by adjusting the child’s position during
feeding. A systematic review conducted by Snider et al. (2011) identified that for
children with cerebral palsy, "positioning has a positive effect on feeding safety
and efficiency by decreasing the risk of aspiration and diminishing meal time" (p.
71).
To promote a relaxed infant feeding experience, environmental changes promote
feeding by altering the temperature, light or noise in the child’s immediate feeding
environment (Morgan et al., 2012). Evidence from White-Traut et al. (2002) saw
increased alertness, milk intake and earlier discharge following an auditory,
tactile, visual, and vestibular intervention used on 12 preterm infants.
Behavioral approaches are based on principles of behavioral modification and
focus on the presentation of contingencies, shaping, prompting, modeling,
stimulus fading, and antecedent manipulation. Current evidence indicates that
behavioral interventions are associated with significant improvements in feeding
behavior (Sharp, Jaquess, Morton, & Herzinger, 2010).
Mixed. A mixed approach to dysphagia combines a direct and indirect
intervention (Siktberg & Bantz,1999). Mixed approaches are supported by Wilkins,
Piazza, Groff, and Vaz (2011), who found chin prompting plus representation of food
stimuli reduced rates of expulsion in all participating children. Furthermore, Yildiz and

Indirect Interventions 9
Arikan (2012) saw positive effects on oral feeding, sucking success and vital signs (peak
heart rate and oxygen saturation) when offering pacifiers to premature infants whilst
playing lullabies during their transition to oral feeding.
Why it is important to conduct this review
Traditionally, the focus of dysphagia literature has been on adult management.
However, anatomical and functional differences to do with swallowing between adults
and children mean adult interventions may not always be appropriately applied to
paediatric populations (Lefton-Greif & Arvedson, 2007). As can be seen in the examples
of the management types presented in the previous section, current methodology
appraising all indirect interventions varies between single cases, cohort studies, quasi
randomized control trials and randomized control trials.
The current literature demonstrates that there are a large number of peadiatric,
indirect intervention studies across all levels of the evidence base hierarchy, including
some systematic reviews and meta analyses. However, the systematic reviews conducted
have either examined a specific population or condition (e.g., preterm infants [Daley &
Kennedy, 2000] or cerebral palsy [Snider et al. 2011]), or have summarized a single
intervention type only (e.g., thickened fluids [Gosa, Schooling & Coleman, 2011],
alternative avenues of intake [Watson & Mcguire, 2013] and pacing [McCormick, Tosh,
& McGuire, 2010]). Although some aspects of indirect interventions have been
systematically reviewed and there is evidence supporting the use of individual strategies
in paediatric settings across case and cohort studies, randomised control trials and some
systematic reviews, to the author’s knowledge, research is yet to group, appraise and
compare the treatment evidence and effects of all indirect approaches within a single
systematic review. In addition to providing a convenient tool for clinicians, collapsing

Indirect Interventions 10
evidence from various conditions and interventions in a single study offers a valuable
contribution to the literature by ensuring consistent methodology is used when drawing
comparisons about treatment effects.
In order to determine if a specific intervention type is effective and to make
comparisons among the effectiveness of different intervention types, a systematic review
will strengthen the availability of current evidence by appraising evidence quality and
examining the effects of pediatic dysphagia intervention. According to the evidence
hierarchy, systematic reviews and meta-analyses form the highest level of evidence based
practice, therefore, investigations using this methodology are needed to further determine
how children with dysphagia are best managed.
Research aims
This project aims to:
conduct a systematic review of indirect approaches for the management of
paediatric dysphagia;
establish the quality of the evidence for indirect paediatric dysphagia approaches;
and,
calculate effect sizes to determine the effects of indirect approaches and draw
comparisons between different types of indirect interventions.
This project aims to answer the following research questions:
(i) What is the current quality of evidence for indirect management of paediatric
dysphagia?
(ii) What is the treatment effect of indirect approaches?

Indirect Interventions 11
Method
Research Design
To answer the research questions posed, a systematic review was used to map the
current literature and “identify, appraise and synthesize” (Petticrew & Roberts, 2006, p.9)
the quality of all relevant studies. The current review followed the Cochrane method,
which is recognised as the highest standard in delivering systematic reviews related to
evidence-based health care (Higgins, Green, & Cochrane Collaboration, 2008).
Criteria for considering reviews for inclusion
Types of studies. In order that methodological quality could be rated using the
Cochrane Risk of Bias Tool (CROBT) (Appendix A) and the Pedro scale (PS) (Appendix
B), between groups, randomised controlled trials (RCTs) and quasi-randomised trials
(e.g., where participants were allocated according to order) were considered for review.
Studies were required to have a control group or comparison intervention to be included
for rating on the CROBT and PS.
Types of participants. Participants for inclusion were children aged from birth to
18 years with a developmental delay, disability, or condition that affects swallowing and/
or feeding.
Types of interventions. Articles involving indirect interventions for the
management of swallowing and feeding were considered for review.
Outcome measures. To be considered for review, articles had to contain at least
one outcome measure involving a feeding or swallowing behavior relating to body
structure and function, activity, participation or environmental change (Appendix C).
Search methods for identification of reviews
To determine a comprehensive and sensitive search strategy, two specialist

Indirect Interventions 12
Librarians were consulted prior to commencing the review. Based on a previous literature
search conducted by the author, a list of terms was generated relevant to the proposed
research aims. Following consultation with the Librarians, the following search strategy
was developed according to the PICO (Population Intervention Comparison Outcomes
Study) method. Two independent search teams used the search strategy below (Table 1.)
between May and July 2015. To retrieve a wide range of results during the search phase,
the search was not limited by publication date or language.
Table 1. Search Strategy
PICO Search
order Key words
P: paediatric S1 child* OR pediatric* OR paediatric* OR infan*
P: dysphagia S2 dysphagia OR swallowing OR deglutition OR feeding OR
feeding disorder*
P: feeding S3 feeding OR feeding disorder*
I: speech pathology S4 speech path* OR speech language path* OR speech therap*
OR intervention* OR therap*
C: speech
pathology
S5 intervention* OR therap*
O: study S6 trial OR study OR RCT OR randomized control trial OR
clinical OR evidence based
PICO S7 S1+S2+S3+S4+S5+S6
Electronic searches. Published and unpublished literature was searched across 19
electronic databases (see below). Each database was searched using the same search
strategy (Table 1.)
EBSCO
EBSCO: Medline
EBSCO: PsychINFO
EBSCO: ERIC

Indirect Interventions 13
EBSCO: Education Source
Web of Science
Scopus
SpeechBite
The Joanna Briggs Institute
ProQuest Central
TRIP
Current Controlled Trials
ClinicalTrials.gov
WHO ICTRP
NDLTD
TROVE
DART
ProQuest Dissertations and Theses Global: Health and Medicine
Handsearching. To identify additional studies not picked up in the electronic
search, handsearches of the reference lists of included studies and relevant papers was
conducted at a later date.
Data collection and analysis
Selection of studies and data extraction. The inclusion criteria (discussed above)
were used as a checklist by a primary and one of the two secondary authors (secondary
authors reviewed half of the articles each) to independently determine the appropriateness
of articles. Both raters used a preliminary data extraction form (Appendix D) to collect
information about the inclusion criteria each study met, based on titles. In the first round
of evaluation, there was disagreement over whether 21 titles met the inclusion criteria;

Indirect Interventions 14
however, this reflected rater inexperience regarding the search confines, and raters were
able to form a consensus by discussing the search strategy and re-evaluating
methodological quality in light of the search parameters. For articles that met preliminary
inclusion criteria, raters used the same preliminary data extraction form (Appendix D) to
evaluate the abstracts and full texts of these preliminary citations in more detail. No
further discrepancies were encountered in the second round of evaluation.
Assessment of methodological quality for included studies
Risk of bias was assessed by rating intervention articles on the CROBT and PS.
For included articles (discussed in the Results section), the primary author rated all
articles and two secondary raters rated half each. The CROBT was used to rate articles as
having a low, high or unclear risk of bias across the following domains: sequence
generation, allocation concealment, blinding, incomplete data, selective outcome
reporting and other sources of bias (Higgins, 2011). Similarly, the PS examined bias by
requiring raters to answer yes or no on the following criterions: specified eligibility
criteria, random allocation of subjects to groups, groups are at similar baselines regarding
the most important prognostic indicators, blinding of subjects, blinding of administering
therapists, blinding of assessors, measure of at least one key outcome were obtained from
more than 85% of subjects initially allocated to groups, all subjects received the treatment
or control condition as allocated, results of between group statistical comparisons are
reported for at least one key outcome and both point and variability measures are
provided for at least one key outcome. For both tools, the quality of included studies were
presented in data extraction tables (Appendix E and F), where a risk judgement was made
in accordance with the decision making guidelines provided by each tool (Higgins, 2011;
Physiotherapy Evidence Database, 1999).

Indirect Interventions 15
Whilst both tools aim to evaluate methodological quality and assess similar points
of bias, each have limitations (for example, the CROBT fails to account for important
markers of bias including eligibility criteria of participants, participant baselines at the
commencement of trials, between group statistical comparisons and the inclusion of
variability measures, whilst the PS neglects selective reporting and does not offer raters
the opportunity to record “other biases” which may be evident within studies). Therefore,
it was decided that both tools would be used to provide an additional measure of
reliability. The PS was chosen due to its in depth, 11 point bias examination, whilst the
CROBT was used due its option of an “unclear” rating which provides raters with an
alternative to “low” or “high risk” when an article fails to provide details about a
criterion. For ratings that did not attain full agreement from all raters, discrepancies were
discussed until agreement was achieved. Throughout rating, four discrepancies between
raters were encountered on the CRBT (relating to adequate sequence generation,
allocation concealment, selective outcome reporting and other bias). There was one
discrepancy on the PS (relating to agreement on whether there was blinding of all
therapists who administered the therapy).
Data synthesis
Once PS and CROBT quality ratings were complete, frequency data for
each item was collated to represent the overall quality of evidence across all
interventions, specific interventions and populations. The Cochrane GRADE (Grades of
Recommendation, Assessment, Development and Evaluation Working Group) approach
(Higgins, Green, & Cochrane Collaboration, 2008) is based on factors that are considered
to decrease research quality and includes (i) limitations in design and implementation; (ii)
indirectness of evidence; (iii) unexplained heterogeneity; (iv) imprecision of results; (v)

Indirect Interventions 16
high probability of publication bias; and was used to provide an overall indication of
research quality by standardising various types of bias. Graphs created in Microsoft Excel
were used to represent frequency data.
Additionally, a statistician was consulted to standardise treatment outcomes by
calculating effect sizes for each reported outcome within each included intervention
article. Effect size calculations were based on descriptive measures (means and standard
deviations) across treatment and control conditions, as reported within intervention
articles (Borenstein, Hedges, Higgins, & Rothstein, 2009). Effect size was represented by
Hedges g (g), and was derived from algorithms and interpretation instructions reported in
Borenstein and colleagues (2009). Forest plots were used to visually represent effect size
and were developed using a free forest plot tool created by Bailey (2009). Due to the large
variation in study outcomes, studies were not deemed comparable (Borenstein et al.,
2009) and therefore a meta-analysis was not possible.
Results
The search retrieved a total of 1398 articles (derived across both search teams).
After 83 duplicates were removed, 1315 articles were excluded based on title. 91 articles
met the preliminary inclusion criteria. The abstracts and full texts of these preliminary
articles were evaluated in more detail against the inclusion criteria and 9 articles met all
of the criteria. Four additional articles were included following a hand search of all
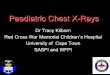
initially included articles. A flow diagram of the study selection process is presented in
Figure 1.

Indirect Interventions 17
Figure 1. Flow diagram outlining search process.
Included studies
Thirteen articles were included in the final analysis. Table 2 shows the
characteristics of included studies.
Study designs. All included articles were between groups, randomised or quasi-
randomised control trials. Eleven articles comprised one intervention and one-control
group. Two studies were comprised of two intervention groups and one control group
(Collins et al., 2004; Standley et al., 2010).
Identification of evidence gap, search strategy and inclusion/ exclusion criteria
Two search teams review 19 electronic data bases
Title screen of results from search teams (1398
articles) Exclusion of 83 duplicates
Exclusion of 1307 results (irrelevant/ did not meet
inclusion criteria)
Review of 91 preliminarily included abstracts
and full text articles
82 articles further excluded for one or more of the
following: children did not serve as main participants,
no direct speech pathology application, single/ case
study or between measures design, children did not
have a swallowing disorder
Quality appraisal (13 articles rated on the
Cochrane Risk of Bias Tool and Pedro Scale)
13 citations included in the final review
9 included articles hand searched. 4 additional
articles included for appraisal

Indirect Interventions 18
Country and setting of the studies included. Details of geographic and
environmental settings are outlined below;
nine studies were based in America (Davidson et al., 2013; Fucile et al., 2008;
Hake-Brooks and Arvedson, 2008; Kirt et al., 2007; Law-Morstatt et al., 2003;
Standley, 2003; Standley et al., 2010; Simpson et al., 2002; White-Traut et al.,
2002), with eight of these American studies set in the Neonatal Intensive Care
Unit (NICU);
one study was based in Australia (Collins et al., 2004) and set in a tertiary referral
hospital;
one study (Puckett et al., 2008) was conducted in Canada and set in an NICU;
one study (Shaw et al., 1999) was based in England within hospital and home care
environments; and
one study (Yilmaz et al., 2014) was conducted in Turkey and set in an NICU.

Indirect Interventions 19
Table 2.
Characteristics of Included Studies (ordered by intervention type)
Year Author Title Study
design
Population Number of
participants
(interventio
n, control)
Interventio
n
Control Key outcomes
2004 Collins
et al.
Effect of bottles, cups, and
dummies on breast feeding
in preterm infants: a
randomized controlled trial
RCT Preterm 89- 72, 73 Equipment No
dummy
Full breastfeeding
Any breastfeeding on
discharge home
1999 Shaw et
al.
Assisted feeding is more
reliable for infants with
clefts
RCT Cleft 52, 49 Equipment SC
(ridged
bottle)
Weight
Length
Head circumference
Full tube feeding
2008 Fucile et
al.
A Controlled-flow
Vacuum-free Bottle
System Enhances Preterm
Infants’ Nutritive Sucking
Skills
RCT Preterm 15,15 Equipment SC
(standard
bottle)
Overall transfer
Rate of milk transfer
Suction amplitude
Frequency of suction
Overall transfer
Sucking breast duration
2013 Yilmaz
et al.
Effect of Cup Feeding and
Bottle Feeding on
Breastfeeding in Late
Preterm Infants: A
Randomized Controlled
Study
RCT Preterm 254, 268 Equipment SC (bottle
feeding)
Weight gain
Feeding time
Hospital stay
Infant gestational age
at discharge
Any breastfeeding
Exclusive
breastfeeding
2002 Simpson,
Schanler,
and Lau
Early introduction of oral
feeding in preterm infants
RCT Preterm 28, 23 AROP SC
(initiation
of oral
Full tube feeding
Transition from tube to
total oral feeding

Indirect Interventions 20
feeding >
48 hours
full tube
feeding)
First successful oral
feeding
4 successful oral
feedings
All oral feedings
Introduction of oral
feeding to first
successful oral feedings
First successful oral
feeding to all oral
feeding
Hospital discharge
2007 Kirk,
Alder
and King
Cue-based oral feeding
clinical pathway results in
earlier attainment of full
oral feeding in premature
infants
RCT Preterm 28, 23 AROP SC
(feeding
based on
physician
order)
PMA at full oral
feeding
PMA at full oral
feeding
Rate of weight gain
during oral feeding
phase
2003 Law-
Morstatt,
Judd,
Snyder,
Baier
and
Dhanired
dy
Pacing as a treatment
technique for transitional
sucking
RCT Preterm 18,18 AROP SC
(traditiona
l bottle
feed)
Chronological age at
NICU discharge date
PCA at NICU
discharge date
Bradycardias
Weekly weight gain
Discharge weight
2013 Davidso
n,
Hinton,
Ryan-
Wenge
Quality improvement
study of effectiveness of
Cue‐Based feeding in
infants with
Bronchopulmonary
RCT Bronchop
ulmonary
Dysplasia
55, 60 AROP SC
(traditiona
l feeding
pathway)
PMA at first oral
feeding (weeks)
Days from first to full
oral feeding
Overall weight gain (g)

Indirect Interventions 21
and
Jadcherla
dysplasia in the neonatal
intensive care unit
Average weight
velocity (g.kg/day)
2008 Puckett,
Grover,
Holt and
Sankaran
Cue-Based Feeding for
Preterm Infants: A
Prospective Trial
RCT Preterm 39, 40 AROP Demand
feed
Cues per feed
Feedings per day
Bottle feeder intake
Length of stay
Weight gain
Exit weight
PCA at exit
Adverse events
Nasal prong with
oxygen at exit
2003 Standley The Effect of Music-
Reinforced Nonnutritive
Sucking On Feeding Rate
of Premature Infants
RCT Preterm 16, 16 Environme
ntal
AM feeding rate
PM feeding rate
2010 Standley
et al.
The Effect of Music
Reinforcement for Non-
Nutritive Sucking on
Nipple Feeding Of
Premature Infants
RCT Preterm 8-8,8 Environme
ntal
SC (no
PAL)
Gavage days
Days to discharge
Discharge weight
Weight gain
2002 White-
Traut et
al.
Effect of auditory, tactile,
visual, and vestibular
intervention on length of
stay, alertness, and feeding
progression in preterm
infants
RCT Preterm 21, 16 Environme
ntal
SC Length of hospital stay
Feeding progression
Alert state
2008 Hake-
Brooks
and
Anderso
n
Kangaroo care and
breastfeeding of mother-
preterm infant dyads 0–18
months: A randomized,
controlled trial
RCT Preterm 36, 30 Environme
ntal
SC (no
KC)
Mean IBS score
Time reached exclusive
breast feed

Indirect Interventions 22
Note. AROP = Altering rate of presentation; SC = Standard care; PAL = Pacifier activated lullaby system; KC = Kangaroo care; PMA =
Postmenstrual age; PCA = Post conceptual age; IBS = Index of breastfeeding status; NICU = Neonatal intensive care unit.

Indirect Interventions 23
Participants. Articles included the following populations:
eleven articles examined populations of Preterm infants (Collins et al., 2004;
Fucile et al., 2008; Hake-Brooks & Anderson, 2008; Kirk et al., 2007; Law-
Morstatt et al., 2003; Simpson et al., 2002; Puckett et al., 2008; Standley. 2003;
Standley et al., 2010; White-Traut et al., 2002; Yilmaz et al., 2013);
one study examined infants with Cleft Palate (Shaw et al., 1999); and
one study examined infants with Bronchopulmonary Dysplasia (Davidson et al.,
2013) (Figure 2).
Figure 2. Population breakdown.
The number of participants within each intervention group ranged between eight
(Shaw et al., 1999) to 268 infants (Yilmaz et al., 2015) (across all populations and
interventions). The age of participants varied between 23 weeks (gestational age) and one
year of age. Although parents were involved in administering some interventions, no
studies directly assessed effects of intervention on parental outcomes.
84%
8%
8%
Populations
Preterm
Cleft Palate
Bronchopulmonary
Dysplasia

Indirect Interventions 24
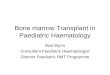
Interventions. Indirect interventions were used in all articles. However, different
approaches to indirect management were taken. Of the reviewed studies,
four involved the use of equipment (Collins et al., 2004; Fucile et al., 2008; Shaw
et al., 1999; Yilmaz et al., 2014);
five altered the rate of presentation (Davidson et al., 2013; Kirt et al., 2007; Law-
Morstatt et al., 2003; Puckett et al., 2008; Simpson et al., 2002); and
four involved environmental changes (Hake-Brooks & Anderson, 2008; Standley.
2003; Standley et al., 2010; White-Traut et al., 2002) (see Figure 3).
Figure 3. Intervention breakdown.
Interventions were administered by Nurses, (Collins et al., 2004; Davidson et al.,
2013; Fucile et al., 2008; Hake-Brookes & Anderson, 2008; Kirk et al., 2007; Law-
Morstatt et al., 2003; Pucket et al., 2008; Shaw et al., 1999; White-Traut et al., 2002;
Yilmaz et al., 2015;), attending Physicians (Kirk et al., 2007; Simpson et al., 2002),
Neonatologists (Collins et al., 2004), Physical Therapists (Law-Morstatt et al., 2003)
Occupational Therapists (Kirk et al., 2007), Lactation Consultants (Hake-Brookes &
Anderson, 2008), Music Therapists (Standley et al., 2010), Midwives (Collins et al.,
2004) and parents (Pucket et al., 2008; Shaw et al., 1999; Yilmaz et al., 2015).
31%
38%
31%
Interventions
Equipment
Altering rate of
presentation

Indirect Interventions 25
Four articles commenced intervention according to department protocols
regarding infant readiness cues (e.g., tolerance of full enteral feedings, tolerance of skin to
skin contact, ability to sustain non-nutritive suck, transition to alert state) (Davidson et al.,
2013; Kirk et al., 2007; Pucket et al., 2008; Yilmaz et al., 2015). Three articles
commenced intervention according to arbitrary time stipulations (e.g., at 34 weeks, 48
hours post full enteral feeding or 24 hours following referral to service) (Shaw et al.,
1999; Simpson et al., 2002; Standley et al., 2010). One article commenced treatment as
soon as possible post birth (Hake-Brookes & Anderson, 2008). One article commenced
trials when the participant’s mother was unable to breastfeed (Collins et al., 2004). Four
articles provided no details about commencement of intervention (Fucile et al., 2008;
Law-Morstatt et al., 2003; Standley, 2003; White-Traut et al., 2002).
Treatment intensity varied across articles and ranged between one (Fucile et al.,
2008) and eight sessions per day (Standley, 2003).
Equipment. In Collins and colleagues (2004) artificial teats (bottles and
dummies) were offered to infants of mothers who were unable to breastfeed. Fucile and
colleagues (2008) compared a controlled flow vacuum free bottle to a standard bottle.
Yilmaz and fellow researchers (2014) examined the effects of cup and bottle-feeding.
Shaw’s group (1999) compared the effectiveness of squeezable bottles to standard, ridged
feeding bottles.
Altering rate of presentation. Davidson and colleagues (2013) altered rate of
presentation of feeding by implementing a cue-based feeding strategy based on infant
driven readiness cues. Similarly, Kirt and colleagues (2007) implemented a cue-based
pathway based on feeding readiness and hunger signs. Additionally, Puckett and fellow
researchers (2008) implemented a cue-based model where infants transitioned between

Indirect Interventions 26
gavage and bottle-feeding to feeding based on demand. Law-Morstatt and colleagues
(2003) applied a paced feeding protocol where feeders regulate the number of sucks per
burst and duration of burst by systematically removing the teat to impose breathing
pauses. Simpson’s group (2002) shortened transition time to oral feeding by introducing
early oral feeding 48 hours after achieving full tube feeding.
Environmental changes. Standley (2003) used music to reinforce nonnutritive
sucking and feeding rate. Similarly, Standley and colleagues (2010) used music to
reinforce nonnutritive sucking on nipple feeding infants. White-Traut’s group (2002)
implemented an auditory, tactile, visual and vestibular intervention. Hake-Brooks and
colleagues (2008) used kangaroo care to calm the infant by raising the infant’s
temperature via swaddling and facilitating skin to skin contact between mother and child
during breastfeeding.
Outcome Measures
Outcomes were measured at baseline and immediately post treatment across all
included articles. Some articles examined performance at different schedules post-
treatment. For example, at one (White-Traut et al., 2002; Yilmaz et al., 2014), two
(White-Traut et al., 2002; Yilmaz et al., 2014), three (White-Traut et al., 2002), six (Shaw
et al., 1999; Hake-Brooks & Anderson, 2008), 13 (Shaw et al., 1999), 26 (Shaw et al.,
1999) and 34 weeks post-treatment (Standley et al., 2010).
Several articles conducted additional outcome assessments at three (Hake-Brooks
& Anderson, 2008; Yilmaz et al., 2014), six (Hake-Brooks & Anderson, 2008; Yilmaz et
al., 2014;), eight (Standley et al., 2010), nine (Standley et al., 2010), 12 (Hake-Brooks &
Anderson, 2008; Shaw et al., 1999) and 18 months (Hake-Brooks & Anderson, 2008).
Articles did not provide any additional, post treatment follow up outcomes.

Indirect Interventions 27
All articles included outcome measures, which could be dived into three
categories; anthropometric (comparative, morphological traits) (Ulijaszek & Kerr, 1999),
feeding and length of stay measures. Outcomes according to article are outlined in Table
3.
Table 3.
Outcome Measures for Included Articles (ordered according to outcome)
Outcome
category
Study Outcome
Feeding Fucile et al. (2008) Overall transfer
Rate of milk transfer
Suction amplitude
Frequency of suction
Overall transfer
Sucking breast duration
Yilmaz et al. (2014) Feeding time
Any breastfeeding
Exclusive breastfeeding
Standley et al. (2010) Gavage days
Davidson et al. (2013) Days from first to full oral feeding
Standley (2003) AM feeding rate
PM feeding rate
Puckett et al. (2008) Feeding
Feedings per day
Bottle feeder intake
Collins et al. (2004) Full breast feeding
Any breastfeeding at discharge home
White-Traut et al. (2002) Feeding progression
Alert state
Hake-Brooks and
Anderson (2008)
Feeding
Time reached exclusive breast feed
Simpson et al. (2002) Full tube feeding

Indirect Interventions 28
Transition from tube to all oral feeding
Introduction from oral feeding to first
successful oral feed
Anthropometric Kirk et al. (2007) Rate of weight gain during oral feeding phase
PMA at full oral feeding
Yilmaz et al. (2014) Weight gain
Infant gestational age at discharge
Shaw et al. (1999) Weight
Length
Head circumference
Full tube feeding
Law-Morstatt et al. (2003) Chronological age at NICU discharge date
PCA at NICU discharge date
Bradycardias
Weekly weight gain
Discharge weight
Standley et al. (2010) Discharge weight
Weight gain
Davidson et al. (2013) PMA at first oral feeding
Overall weight gain
Average weight velocity
Puckett et al. (2008) Weight gain
Exit weight
PCA at exit
Adverse events
Nasal prong with oxygen at exit
Length of stay Yilmaz et al. (2014) Hospital stay
Law-Morstatt et al. (2003) Weeks in study
Standley et al. (2010) Days to discharge
Puckett et al. (2008) Length of stay
White-Traut et al. (2002) Length of stay
Simpson et al. (2002) Hospital discharge
Note. PMA = Postmenstrual age; PCA = Post conceptual age; IBS = Index of
breastfeeding status.

Indirect Interventions 29
Quality appraisal
Articles were appraised for quality across a number of groups (all included articles
and individual intervention type). Final ratings for all intervention articles on both scales
can be seen in Table 4 and 5. Despite biases relating to the implementation of
interventions (around the allocation concealment and blinding of participants, therapists
implementing intervention), the Cochrane GRADE approach (Higgins et al., 2008)
suggests intervention articles were of high methodological quality with transparent
outcome reporting and specified eligibility criteria of participants.
Combined quality ratings for all included articles. On the CROBT high scoring
(low risk of bias) items included selective reporting bias (93%), complete outcome data
(77%) and other bias (77%). Low scoring (high risk of bias) items related to allocation
concealment (70%) and blinding of participants, personnel and outcome assessors (70%).
Combined quality ratings for the CROBT can be seen in Figure 5.
Figure 5. Combined ratings- CROBT

Indirect Interventions 30
Table 4.
Risk of Bias Summary (PS): Agreed Rater Judgements for Each Risk of Bias Criterion for Each Included Study
Criterion
Study
Eli
gib
ilit
y c
rite
ria
wer
e sp
ecif
ied
Subje
cts
wer
e ra
ndom
ly a
lloca
ted t
o g
roups
(in
a c
ross
over
stu
dy, su
bje
cts
wer
e
random
ly a
lloca
ted a
n o
rder
in w
hic
h
trea
tmen
ts w
ere
rece
ived
)
All
oca
tion w
as c
once
aled
The
gro
ups
wer
e si
mil
ar a
t bas
elin
e
regar
din
g t
he
most
im
port
ant
pro
gnost
ic
indic
ators
Ther
e w
as b
lindin
g o
f al
l su
bje
cts
Ther
e w
as b
lindin
g o
f al
l th
erap
ists
who
adm
inis
tere
d t
he
ther
apy
Ther
e w
as b
lindin
g o
f al
l as
sess
ors
who
mea
sure
d a
t le
ast
one
key
outc
om
e
Mea
sure
s o
f at
lea
st o
ne
key
outc
om
e w
ere
obta
ined
fro
m m
ore
than
85%
of
the
subje
cts
init
iall
y a
lloca
ted t
o g
roups
All
su
bje
cts
for
whom
ou
tcom
e m
easu
res
wer
e av
aila
ble
rec
eived
the
trea
tmen
t or
contr
ol
condit
ion a
s al
loca
ted o
r, w
her
e th
is
was
not
the
case
, dat
a fo
r at
lea
st o
ne
key
outc
om
e w
as a
nal
yze
d b
y “
inte
nti
on t
o
trea
t”
The
resu
lts
of
bet
wee
n-g
roup s
tati
stic
al
com
par
isons
are
repo
rted
for
at l
east
one
key
outc
om
e
The
study
pro
vid
es b
oth
poin
t m
easu
res
and
mea
sure
s of
var
iabil
ity f
or
at l
east
one
key
outc
om
e
Collins et
al. (2004)
Yes Yes Yes No No No No Yes Yes Yes Yes
Shaw et al.
(1999)
Yes Yes Yes Yes No No No Yes Yes Yes Yes
Simpson et
al. (2002)
Yes Yes No Yes No No No Yes No Yes Yes
Standley
(2003)
Yes Yes No Yes Yes Yes No Yes Yes Yes Yes
White-
Traut et al.
Yes Yes No Yes Yes No Yes No No Yes No

Indirect Interventions 31
(2002)
Kirk et al.
(2007)
Yes No No Yes No No No Yes No Yes Yes
Fucile et al.
(2008)
Yes No No Yes No No No Yes No Yes Yes
Law-
Morstatt et
al. (2003)
Yes No No Yes No No No Yes No Yes Yes
Davidson et
al. (2013)
No No No No No No No Yes No Yes Yes
Standley et
al. (2010)
Yes Yes No Yes Yes No No Yes No Yes Yes
Yilmaz et
al.
Yes Yes Yes Yes No No Yes Yes Yes Yes Yes
Puckett et
al. (2008)
Yes Yes No Yes No No No Yes Yes Yes Yes
Hake-
Brooks and
Anderson
(2008)
Yes
Yes
No No No No No Yes No Yes Yes
Note. Red = No; Green = Yes.

Indirect Interventions 32
Table 5.
Risk of Bias Summary (CROBT): Agreed Rater Judgements for Each Risk of Bias Criterion for Each Included Study
Criterion
Article
Adeq
uat
e
sequen
ce
gen
erat
ion
All
oca
tion
conce
alm
ent
Bli
ndin
g o
f
par
tici
pan
ts,
per
sonnel
and o
utc
om
e
asse
ssors
Inco
mple
te
outc
om
e dat
a
addre
ssed
Fre
e of
sele
ctiv
e
outc
om
e
report
ing
Oth
er b
ias
Collins et al. (2004) Low Low High Low Low High
Shaw et al. (1999) Low Low High Low High Low
Simpson et al. (2002) High High High Unclear Low Low
Standley (2003) High High Low High Low Low
Kirk et al. (2007) High High High Low Low Low
Fucile et al. (2008) High High High Low Low Low
Law-Morstatt et al. (2003) High High High Low Low Low
Davidson et al. (2013) High High High Low Low High
Standley et al. (2010) High High Low Low Low Low
Yilmaz et al. 2014 Low Low Low Low Low Low
White-Traut et al. (2002) Unclear Unclear Low High Low Low
Puckett et al. (2008) Low High High Low Low High

Indirect Interventions 33
Note. Red = No; Green = Yes; Yellow = Unclear.
Hake-Brooks and Anderson
(2008)
Low High High Low Low Low

Indirect Interventions 34
On the PS, highest scoring (low risk of bias) items included reported results of
between-group statistical comparisons for at least one key outcome (100%), point
measures and measures of variability for at least one key outcome (92%) and
specification of eligibility criteria (92%). Low scoring (high risk of bias) items included
blinding of all therapists who administered the therapy (93%), blinding of all assessors
who measured at least one key outcome (84%) and concealment of treatment allocation
(76%). Combined quality ratings for the PS can be seen in Figure 6.
Figure 6. Combined ratings- PS
Quality appraisal based on intervention type
Equipment. On the CROBT, all articles relating to the use of equipment had a
low risk of other bias. 75% of articles had a high risk of bias relating to participant
allocation concealment. Combined quality ratings for use of equipment can be seen in
Figure 7.

Indirect Interventions 35
Figure 7. Combined quality ratings for interventions involving equipment- CROBT.
On the PS, all articles examining the use of equipment reported results of
between-group statistical comparisons for at least one key outcome, specified eligibility
criteria, obtained measures of at least one key outcome from more than 85% of the
subjects initially allocated to groups and provided both point measures and measures of
variability for at least one key outcome. No articles blinded subjects or therapy assistants.
Combined quality ratings for use of equipment can be seen in Figure 8.
Figure 8. Combined quality ratings for interventions involving equipment- PS.

Indirect Interventions 36
Rate of presentation. All CROBT appraisals for interventions that altered the rate
of presentation had a low risk of bias relating to blinding of participants, personnel and
outcome assessors, allocation concealment and were free of selective outcome reporting.
40% of articles had a high risk of other bias. Combined quality ratings for interventions
altering rate of presentation can be seen in Figure 9.
Figure 9. Combined quality ratings for interventions altering rate of presentation-
CROBT.
On the PS, all articles altering the rate of presentation blinded all subjects,
therapists who administered the therapy and assessors who measured at least one key
outcome. Additionally, all articles included measures of at least one key outcome from
more than 85% of the subjects initially allocated to groups, reported results of between-
group statistical comparisons for at least one key outcome and provided both point
measures and measures of variability for at least one key outcome. 100% of studies
articles failed to conceal allocation. Combined quality ratings for interventions altering
rate of presentation can be seen in Figure 10.

Indirect Interventions 37
Figure 10. Combined quality ratings for interventions altering rate of presentation- PS
Environmental change. On the CROBT, all articles examining interventions
involving an environmental change had a low risk of other bias. 75% of articles had a
high risk of bias in relation to blinding of participants, personnel and outcome assessors.
Combined quality ratings for interventions involving an environmental change can be
seen in Figure 11.
Figure 11. Combined quality ratings for interventions involving an environmental
change- CRBT.

Indirect Interventions 38
On the PS, all environmental interventions specified eligibility criteria, randomly
allocated subjects to groups and reported between-group statistical comparisons for at
least one key outcome. All articles failed to blind therapists administering therapy and
75% of studies did not conceal allocation. Combined quality ratings for interventions
involving an environmental change can be seen in Figure 12.
Figure 12. Combined quality ratings for interventions involving an environmental change
- PS.
Reported effects of intervention and data synthesis
Data synthesis was performed on nine articles (Davidson et al., 2013; Fucile et al.,
2008; Kirk et al., 2007; Law-Morstatt et al., 2003; Puckett et al., 2008; Shaw et al., 1999;
Simpson et al., 2002; Standley et al., 2010; Yilmaz et al., 2014). Four articles (Collins et
al., 2004; Hake-Brooks & Anderson, 2008; Standley, 2003; White-Traut et al., 2007) did
not provide descriptive measures and were therefore not included in data synthesis.
Equipment. Three out of four articles examining use of equipment reported
positive effects on feeding. Two studies (Collins et al., 2004; Yilmaz et al., 2014) found
infants randomized to cup feeding were more likely to be exclusively breastfed on

Indirect Interventions 39
discharge, with Yilmaz and colleagues reporting increased rates of breastfeeding at three
and six months post discharge, when compared to bottle fed controls. In Fucile and
colleagues (2008), infants using a controlled vacuum free bottle demonstrated greater
overall milk transfer, rate of transfer and more mature sucking signs, however differences
in sucking amplitude were observed between intervention and standard care infants.
Yilmaz and colleagues reported no significant reduction in time spent feeding and
frequency of feeding problems. One study reported weak anthropometric effects; Shaw and
colleagues (1999) observed no significant change in crown-heel length. However, Shaw’s
group saw the use of a squeezable bottle lead to statistically significant differences in
weight gain and head circumference. The use of equipment was observed to have positive
effects on length of stay; Collins and colleagues found infants using equipment remained in
hospital for shorter periods of time, whilst Yilmaz and colleagues observed a significant
difference between groups for length of hospital stay.
Data synthesis revealed a positive effect of equipment on eight feeding outcomes;
sucking breast duration at six to eight feedings per day (n = 30, g = 0.27, 95% CI: -0.42,
0.97) and sucking duration were observed in Fucile and colleagues (2008). Yilmaz’ team
(2014) reported positive effects for any breastfeeding at three months (n = 522, g = 0.02,
95% CI = -0.14, 0.19) and feeding time (n = 522, g = 0.06, 95% CI = -0.11,0.23).
Additionally, the use of equipment had a statistically significant effect on any
breastfeeding at six months (n = 522, g = 0.28, 95% CI: 0.10, 0.45), any breastfeeding at
discharge (n = 255, g = 0.08, 95% CI: -0.08, 0.25) and exclusive breastfeeding at
discharge (n = 255, g = 1.01, 95% CI: 0.83, 1.19) in Yilmaz’ group. One positive effect
was observed for anthropometric measures in Shaw and colleagues (length at week 6 [n =
100, g = 0.00, 95% CI: -0.39, 0.19]). One positive effect was observed for length of stay
measures in Yilmaz and colleagues (hospital stay duration [n = 254, g = 0.09, 95% CI -

Indirect Interventions 40
0.26, 0.08]). See Appendix G for effect sizes and corresponding forest plots for
interventions involving modified equipment use.
Altering rate of presentation. Four studies reported positive effects on feeding
when interventions altered the rate of presentation, with three studies reporting shorter
time to oral feeding; Simpson and colleagues (2002) found infants who were introduced
to early oral feeding attained total oral feeding significantly earlier than controls who
were tube fed for longer than 48 hours, (however, no difference was observed in overall
transfer and rate of milk transfer). Kirk and colleagues (2007) found infants following a
cue based pathway reached full oral feeding earlier than standard care controls, whilst
Davidson’ team (2013) saw infants in the cue based feeding group reach full oral feeding
in significantly less time. Additionally, Law-Morstatt’s group (2003) observed more
efficient sucking patterns at discharge. Two studies reported positive effects on
anthropometric measures; Law-Morstatt and colleagues and Puckett and colleagues
(2008) saw increases in clinical stability with decreased adverse events. Weight gain of
study infants varied; Davidson’s team saw greater average weight velocity in the cue
based group, however, two studies (Law-Morstatt et al.,; Puckett et al.,) did not report
statistically significant weight gain. Length of stay was reported to be significantly shorter
in one study (Puckett et al.) however these effects were not replicated (Law-Morstatt et
al.).
Data synthesis revealed a positive but non-significant effect of altering rate of
presentation on three anthropometric outcomes: average weight velocity (n = 155, g =
0.18, 95% CI: -0.17, 0.55); PMA at first oral feed (n = 115, g = 0.08%, 95% CI: -0.27,
0.45 (both Davidson et al., 2013); and rate of weight gain (n = 51, g = 0.41, 95% CI: -
0.13, 0.96) (Kirk et al., 2007). Altering rate of presentation had a statistically significant
effect (n = 51, g = 0.94, 95% CI: 0.19, 1.69) on one feeding outcome (introduction of oral

Indirect Interventions 41
feeding to first full oral feed) (Simpson et al., 2002). Additionally, positive effects (n =
29, g = 0.24, 95% CI: -0.46, 0.95) were observed for a second feeding outcome (first
successful oral feed) (Simpson et al.). Four significant effects were observed for length of
stay measures: length of stay after entry adjusted for gestation age (n= 39, g = 0.58, CI: [-
1.03,-0.14] (Pucket et al., 2008); non adjusted length of stay n= 39, g = 0.58, CI: [-1.03,-
0.14] (Pucket et al.); hospital discharge (days n= 13, g= 0.56, CI: [-1.29, 0.15]; and weeks
n = 13, g = 0.55, [-1.27, 0.17]) (Simpson et al., 2002). See Appendix H for effect sizes
and corresponding forest plots for interventions altering rate of presentation.
Environmental changes. All studies involving environmental change reported
positive effects relating to feeding: Standley and colleagues (2010) and Standley (2003)
found music reinforced non-nutritive sucking to significantly shorten time required for
gavage feeding, with increased overall feeding rates. Hake-Brooks and Anderson (2008)
found Kangaroo Care infants to breastfeed significantly longer, than standard care,
control infants, with Kangaroo Care infants more likely to be exclusively breast fed at
discharge. White-Traut and colleagues (2002) reported increased alertness leading to a
more rapid transition to breast-feeding following an auditory, tactile, visual, and
vestibular intervention. Positive effects on length of stay were also observed in Standley
and colleagues and White-Traut and colleagues who reported decreased length of
hospitalisation.
Data synthesis revealed a positive effect of interventions involving an
environmental change on two feeding outcomes reported in Standley and colleagues
(2010); number of gavage days at weeks 34 (n = 16, g = 0.93, 95% CI: -0.04, 1.91) and
36 (n = 15, g = 0.05, 95% CI: -0.90, 1.00). Standley’s group also reported positive effects
for two anthropometric outcomes: weight gain at week 36 weeks (n = 15, g = 0.68, 95%
CI: -1.42, 0.58) and discharge weight at week 34 (n = 15, g = 0.32, 95% CI: -0.63, 1.28).

Indirect Interventions 42
Significant effects were observed for length of stay measures reported in Stadley and
colleagues (2010; days to discharge at week 32 (n= 8, g = 0.27, CI: [-1.2, 0.66]), days to
discharge at week 34 (n = 8, g = 0.11, CI: [-1.07, 0.84]) and days to discharge at week (36 n =
8, g = 0.43, CI: [-1.43, 0.57]). See Appendix I for effect sizes for interventions and
corresponding forest plots involving an environmental change.
Discussion
A systematic review was conducted in order to establish the quality of the
evidence for indirect paediatric dysphagia interventions, and to draw comparisons
between the effects of various indirect approaches. In turn, 13 randomised and quasi-
randomised control articles were examined to answer the following research questions:
(i) What is the current quality of evidence for indirect management of paediatric
dysphagia?
(ii) What is the treatment effect of indirect approaches?
Quality of evidence
Quality of all included evidence. The literature search demonstrated that there
are a large number of studies advocating the efficacy of indirect interventions for children
with paediatric dysphagia. However, despite the quantity, the availability of high quality
of studies is sparse. This was demonstrated throughout the search process, where a large
proportion of retrieved results were excluded on the basis of not being randomised
intervention trials. Nonetheless, for the 13 RCTs supplied in this review, articles were
deemed to be of high quality according to the Cochrane GRADE approach (Higgins et al.,
2002).
For articles included in this review, bias predominately reflected limitations
related to the implementation of intervention, which resulted in attrition bias (Searle,
1999). Ratings on both the CROBT and PS were consistent in revealing a high risk of bias

Indirect Interventions 43
relating to the allocation concealment and blinding of participants, therapists
implementing intervention and outcome assessors. According to Karanicolas, Farrokhyar,
and Bhandari, (2010), failure to conceal treatment allocation by blinding can be
problematic. In their account, blinding is described as a means of minimizing the risk of
differential assessment of outcomes, as it prevents biased treatment effects, where the
expectation of a response is provided or scored, rather than the response itself
(Karanicolas, Farrokhyar, & Bhandari, 2010).
Unfortunately, the nature of the studies included in this review, as well as speech
pathology literature more generally, mean interventions are reliant on a behavioural
modification which results in a degree of inherent bias (Karanicolas, Bhandari, Walter
(2009). For example, it may not always be possible to blind treatment conditions from
assessors (e.g., it is difficult to blind an administering therapist from viewing bottle type
as they need to see what they are doing). Other times, it may not be necessary to blind
participants (e.g., when working with infants, their young age may mean it is not
necessary to conceal treatment allocation). These factors make it increasingly difficult to
blind trials within speech pathology, when compared to other areas of healthcare, such as
medicine, which can achieve blinding with placebos (Karanicolas, Farrokhyar, &
Bhandari, 2010).
Even so, Karanicolas and colleagues (2010) argue creative or novel techniques
can make blinding achievable. For example, one article (White-Traut et al., 2002)
included in the current review was able to achieve a low of bias pertaining to blinding by
assigning separate individuals for intervention and outcome assessment. In this study the
assessor was positioned behind a screen and required to wear soundproof headphones
before entering the room to assess the outcome (participant behavioral state). This

Indirect Interventions 44
blinding attempt was commendable as it successfully concealed the group allocation
without impairing the ability to accurately assess outcomes (Karanicolas et al., 2009).
Karanicolas and colleagues (2010) suggest that if blinding is not possible, induced
bias can be counterbalanced by accurate reporting. Across the CROBT and PS, included
articles were not selective in their reporting; all articles included results of between-group
statistical comparisons, with most studies providing measures of variability and
addressing incomplete outcome data. The inclusion of outcomes prevented within-study
publication bias, where systematic differences between reported and unreported findings
exist, and statistically significant outcomes are reported in favor of non-significant effects
(Higgins, 2011).
Finally, most articles specified eligibility criteria. Whilst providing the
characteristics of study participants enables replication for future studies, it also allows
results to be more easily generalized back to a broader population of individuals with the
same features (Morgan et al., 2011).
Articles examining equipment use. According to the GRADE approach (Higgins
et al., 2008), interventions involving adapted equipment were of moderate quality.
Moderate ratings reflected a number of high-risk judgements relating to the absence
blinding for participants, therapists and assessors. As discussed previously, blinding an
equipment change is challenging and it is realistic assume some degree of inherent bias
(Karanicolas et al., 2009). However, a large proportion of the interventions modifying
equipment also failed to address incomplete outcome data, which resulted selective
reporting and the possibility of publication bias (Higgins et al., 2008).
Quality of articles involving an environmental change. According to the
GRADE approach, articles involving an environmental change were deemed to be of high
quality (Higgins et al., 2008). Articles consistently reported participant eligibility criteria

Indirect Interventions 45
on the CROBT and PS. Both scales revealed a high risk of bias relating to the blinding of
participants, assistants and outcome assessors. Similar to articles involving an equipment
change, blinding a temperature, noise or lighting change is improbable due to the reasons
previously discussed.
Quality of articles altering rate of presentation. Ratings for interventions
altering schedule of intake indicate low or no risk of bias on most criterions and were
deemed to be of high quality according to the GRADE approach. Unlike the
aforementioned interventions, authors consistently blinded participants, therapists and
assessors. However, study design limitations resulted in a moderate risk of other bias. For
example, Kirk and colleagues (2007) examined a retrospective group of infants, rather
than randomised controls. Whilst study infants were randomised, the use of historic
controls meant control group infants were not matched for gestational age, birth or
weight, and this may have led to bias as study and control groups may not have been at
similar baselines. Additionally, feeding pathway compliance was not measured in this
study and there may have been subsequent variations in treatment intensity may have
impacted treatment efficacy (Searle, 1999).
Effects of interventions
Equipment. Reported outcomes of articles examining equipment use, as well as
the effect size calculations conducted in this review indicate the use of modified
equipment has a positive effect on feeding. Whilst most of the included articles reported
positive outcomes in relation to feeding and anthropometric measures, data synthesis
revealed positive effects on feeding and length of stay measures. Notably, of the feeding
outcomes, cup feeding resulted in both positive and some statistically significant
increases in breastfeeding prior to and post discharge (Yilmaz et al., 2014). The idea that
modified equipment leads to improved feeding is consistent with current evidence.

Indirect Interventions 46
Yilmaz and colleagues argue the positive effects of cup feeding relate to the idea that
modified equipment can provide an alternative to enteral nutrition, and instead promote
positive parent-infant interactions through the development of eye contact and body
language. Additionally, unlike enteral nutrition, cup feeding is argued to encourage self-
regulation as the infant is provided with the opportunity to learn to how to increase or
restrict their intake.
Reported outcomes and effect size calculations suggest modified equipment has a
small effect on hospital stay duration (Yilmaz et al., 2014). It is likely that these effects
can be supported by the explanation above, and it can be further inferred that an
alternative to enteral nutrition reduces reliance on hospital bound equipment (e.g.
nasogastric tube), whilst promoting self regulation and feeding independence.
Although data synthesis revealed a positive effect for one anthropometric measure
(length at week 6) following the use of a squeezable bottle in Shaw and colleagues
(1999), it is likely this effect was counterbalanced by no change in two effects (weight
and crown-heel length) reported in the same study.
Altering rate of presentation. All articles altering rate of presentation reported
positive outcomes across length of stay, anthropometric and feeding outcomes. Effect
analysis performed in this review suggest that altering the rate of presentation intake does
lead to improved feeding, anthropometric and length of stay outcomes.
In terms of feeding outcomes, effect calculations computed in this review support
the early introduction of oral feeding, as this significantly shortened the time to the first
full oral feed (Simpson et al., 2002). Additionally, early oral feeding was supported by a
second positive effect (first successful oral feed). Pridham, Brown, Sondel, Green, Wedel,
and Lai (1998) argue positive feeding outcomes resulting from cue-based methods reflect

Indirect Interventions 47
an individualised approach to feeding, where feeding decisions are based on the infant’s
unique physical and developmental markers.
Additional research suggests these effects offer support to the idea that preterm
infants who appear clinically ready, and are given the opportunity to feed orally, may
improve the development of their suck-swallow-breathe coordination with early practice
(Simpson et al., 2002). This notion is supported by a range of impairment based
intervention literature, which advocates the use of oral-motor exercises and exploration to
improve paediatric dysphagia. On the contrary, some evidence suggests that infants who
are introduced to oral feeding too early may learn to feed with immature and disordered
sucking patterns (Simpson et al.).
Significant effects were observed for three length of stay measures; length of stay
after entry adjusted for gestation age (Pucket et al., 2008); non adjusted length of stay
(Pucket et al.); and hospital discharge (days and weeks) (Simpson et al., 2002). Overall, it
appears altering rate of presentation results in reduced time in hospital.
According to effect analysis, altering the rate of presentation revealed a generated
a positive trend towards improved anthropometric outcomes (average weight velocity,
PMA at first oral feed and rate of weight gain), however, these effects were non-
significant.
Environmental. Articles involving an environmental change reported positive
effects for feeding and length of stay measures.
Data synthesis revealed environmental changes resulted in two improved feeding
outcomes (number of gavage days at weeks 34 and 36 [Standley et al., 2010]), however,
these outcomes were deemed to be non-significant. Similarly, this study reported non-
significant, positive effects for two anthropometric outcomes (weight gain at week 36
weeks and discharge weight at week 34). Environmental interventions resulted in

Indirect Interventions 48
significant effects on length of stay and suggest environmental changes result in reduced
duration of hospital stay.
Potential bias in the review process
Whilst this review was conducted in accordance with the Cochrane guidelines for
systematic reviews (Higgins et al., 2008) and steps were taken to strengthen reliability
and validity, there are a number of methodological limitations, which are outlined below;
The first relates to time; the time to search and review articles was limited to three
months. This may have impacted results as older data released outside the time, or
newly published data was not considered.
Effect size calculations may be skewed in their ability to validate the effects of
intervention (Borstein et al. 2009), as analysis was based on the reported
measurements of only nine studies. Due to time restrictions, no further
calculations or attempts to contact authors for missing data were made for the four
studies which failed to provide the required descriptive measures.
Whilst some articles measured outcomes at similar intervals, articles varied in
treatment intensity. Due to the principles of experience dependent neuroplasticity
(Kleim, 2008), positive effect outcomes may reflect the use of high intensity
intervention schedules, rather treatment effects alone.
Finally, the author acknowledges that articles deemed to be of high quality
according to GRADE quality ratings may be influenced by the inclusion criteria
which stipulated that only RCTs would be included for review. However, this is
beyond the authors control as the implementation of a stringent inclusion criterion
reflects the limitations of the CROBT and PS, which can only rate RCTs (Higgins
et al. 2009; Physiotherapy Evidence Database, 1999).
Implications for research

Indirect Interventions 49
The review process demonstrates a lack of high quality evidence exists. This is
demonstrated by the search, which aimed to capture and appraise a broad range of high
quality, indirect intervention evidence across a range of paediatric conditions. As the
development of effective dysphagia management has been recognised to be paramount in
reducing related health care costs (Siktberg & Bantz, 1999), additional research is
required. There are a number of further areas, which should be considered in order for
future studies to advance the current evidence base. These are outlined below.
Due to a lack of RCTs, only three intervention approaches could be summarised.
Additional between groups RCTs should be conducted in the area of diet
modifications, use of prosthesis, alternative avenues of intake, postural
modifications and behavioural approaches.
As no studies included in this review involved measures relating to parental
outcomes and study infants are reliant on their caregivers for intervention, parental
outcomes (e.g., opinions of intervention change, stress, enjoyment of their child)
should be included within treatment data. Future studies should consider broader
outcome measures, which relate to quality of life changes for participating
families.
To determine if change has been maintained post intervention, future RCTs should
provide information regarding long term follow up of feeding and swallowing.
The majority of studies in the present review were conducted in NICU settings
with limited transferability to real world settings. To determine the
appropriateness of interventions, ongoing studies should involve a broader range
of settings (e.g., home and school).
Future studies should include wider range of participant populations. 13 of the 15
studies included in this review were based on populations of preterm infants.

Indirect Interventions 50
Although 40% of infants who experience oral feeding difficulties are born
prematurely (Pridham et al., 1998), and it is likely that current research reflects
this epidemiological pattern, examining a diverse range of populations would
broaden the depth of evidence and increase the representativeness of results for
full term infants with dysphagia.
To avoid placebo effects and high risk of bias assessments, RCTs should take
steps to ensure participants, administering assistants and outcome assessors
involved in trials are appropriately blinded to treatment conditions.
As meta-analysis could not be completed in this review, future high quality RCTS
should be used in meta-analysis. As meta-analysis is considered the highest level
of evidence (Sacket et al. 1996), meta-analysis would provide evidence-based way
of making direct comparisons between various indirect intervention types in order
to determine the most effective treatment option (Borstein et al. 2009).
Interestingly, Speech Pathologists were not involved in the development or
implementation of any of the reviewed interventions. As swallowing is a range of
Speech Pathology practice, and ASHA (2015) regards Speech Pathologists as key
members of swallowing intervention teams, future studies should input from
Speech Pathologists in order to share information regarding intervention design
and implementation.
Implications for practice
According to effect calculations, it appears that interventions involving the use of
environmental changes, modified equipment and altered rate of presentation lead to
improved feeding, subsequent advances in anthropometric outcomes and reduced time
spent in hospital. Although the reviewed intervention evidence did not directly include
speech pathology involvement, environmental changes, equipment modifications and

Indirect Interventions 51
altering rate of presentation are well reported as management approaches in speech
pathology literature (ASHA, 2005; Arvedson, 2008; Arvedson & Brodsky, 1993; Cichero
& Murdoch, 2006; Kovar, 1997; Siktberg & Bantz, 1999). Additionally, as these
interventions contain a behavioural component, they can be readily applied to speech
pathology practice. As such, use of these interventions should be continued to advance the
outcomes of children with dysphagia. Improving these measures will likely lead to
benefits in the activity and participation of children with feeding and swallowing
disorders (WHO, 2001), as research suggests improvements in swallow function can
positively influence development (Sullivan et al., 2000), socialisation (Morgan et al.,
2004) and psychological function (Anand & Scalzo, 2000).
The current review highlights the continued need for multidisciplinary
management between many different health care professionals. Interventions were
implemented by seven different healthcare professions, with each article involving a
number of professions to achieve positive swallowing outcomes. As dysphagia is a
complex, multifaceted disorder, multidisciplinary management is required to achieve
holistic, person centred care (Wilken, 2012).
Conclusion
Whilst the review process demonstrates that more high quality research is needed,
the available RCTs are of high methodological quality, and the current review contributes
to the current evidence by synthesising and appraising indirect intervention evidence for
paediatric dysphagia. Additionally, this research supports previous research by suggesting
the use of modified equipment, environmental changes and altering rates of presentation
have positive effects on feeding, anthropometric and length of stay outcomes. Future
studies are needed to further validate the effects of intervention.

Indirect Interventions 52
References
Agarwal, A., Rana, V., & Shafi, S. (2010). A feeding appliance for a newborn baby with
cleft lip and palate. National Journal of Maxillofacial Surgery, 1(1), 91-93.
doi:10.4103/0975-5950.69149.
Al-Sayed, L. E., Schrank, W.I., & Thach, B. T. (1994). Ventilatory sparing strategies and
swallowing pattern during bottle-feeding in human infants. Journal of Applied
Physiology, 77(1), 78-83.
Amaizu, N., Schanler, R. J., Shulman, R. J., & Lau, C. (2008). Maturation of oral feeding
skills in preterm infants. Acta Pædiatrica, (97)1, 61-67.
American Speech and Hearing Association (2015). Paediatric Dysphagia. Retrieved from
http://www.asha.org/Practice-Portal/Clinical-Topics/Pediatric-Dysphagia/
Anand, K. J., & Scalzo, F. M. (2000). Can adverse neonatal experiences alter brain
development and subsequent behavior? Biology of the Neonate, 77(2), 69–82.
doi:10.1159/000014197.
Angell, M. E., Bailey, R. L., & Stoner, J. B. (2008). Family perceptions of facilitators and
inhibitors of effective school-based dysphagia management. Language, Speech,
and Hearing Services in Schools, 39(2), 214-226. doi:10.1044/0161-
1461(2008/021).
Arvedson, J. C. (2008). Assessment of paediatric dysphagia and feeding disorders-
clinical and instrumental approaches. Developmental Disabilities Research
Reviews, 14(2), 118-127. doi-10.1002/ddrr.17.
Arvedson, J. C., & Brodsky, L. (1993). Paediatric swallowing and feeding:
Assessment and management. San Diego, Calif: Singular Pub. Group.

Indirect Interventions 53
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010a). The effects of
oral-motor exercises on swallowing in children: an evidence-based systematic
review. Developmental Medicine and Child Neurology, 52(11), 1000-1013.
Arvedson, J., Clark, H., Lazarus, C., Schooling, T., & Frymark, T. (2010b). Evidence-
based systematic review: Effects of oral motor interventions on feeding and
swallowing in preterm infants. American Journal of Speech-Language Pathology,
19(4), 321-40. doi:10.1044/1058-0360(2010/09-0067.
Bache, M., Pizon, E., Jacobs, J., Vaillant, M., & Lecomte, A. (2014). Effects of pre-
feeding oral stimulation on oral feeding in preterm infants: A randomized clinical
trial. Early Human Development, 90(3), 125.
Bailey, T.M. (2009). Forest Plot Tool (Version 504) [MS Excel workbook].
Downloadable from URL http://www.cardiff.ac.uk/psych/home2/mat/
Bansal, R., Kumar Pathak, A., Bhatia, B., Gupta, S., & Gautam, K. (2012). Rehabilitation
of a one-day-old neonate with cleft lip and palate using palatal obturator: A case
report. International Journal of Clinical Paediatric Dentistry, 5(2), 145-147.
doi:10.5005/10005-1154.
Barbosa, L. D. R., Gomes, E., & Fischer, G. B. (2014). Clinical signs of dysphagia in
infants with acute viral bronchiolitis. Revista Paulista De Pediatria, 32(3), 157-
163.
Boddy, J., Skuse, D., & Andrews, B. (2000). The Developmental Sequelae of Nonorganic
Failure to Thrive. Journal of Child Psychology and Psychiatry, 41(8), 1003-1014.
doi:10.1017/S002196309900637X
Borenstein, M., Hedges, L.V., Higgins, J.P.T., & Rothstein, H. R. (2009). Introduction to
meta-analysis. Chichester, U.K: John Wiley & Sons.

Indirect Interventions 54
Browne, J. V., & Ross, E. S. (2011). Eating as a neurodevelopmental process for high-
risk newborns. Clinics in Perinatology, 38(5), 731– 743.
doi:10.1016/2011.08.004.
Chandna, P., Adlakha, V. K., & Singh, N. (2011). Feeding obturator appliance for an
infant with cleft lip and palate. Journal of the Indian Society of Pedodontics and
Preventive Dentistry, 29(1), 71. doi:10.4103/0970-4388.79950.
Clawson, E. P., Kuchinski, K. S., & Bach, R. (2007). Use of behavioral interventions and
parent education to address feeding difficulties in young children with spastic
diplegic cerebral palsy. Neurorehabilitation, 22(5), 397-406.
Cichero, J. A. Y., & Murdoch, B. E. (2006). Dysphagia: Foundation, theory and practice.
Chichester, England: Wiley.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.).
Mahwah, New Jersey: Erlbaum.
Collins, C. T., Ryan, P., Crowther, C. A., McPhee, A. J., Paterson, S., & Hiller, J. E.
(2004). Effect of bottles, cups, and dummies on breast feeding in preterm infants:
Randomised controlled trial. BMJ: British Medical Journal, 329 (7459), 193.
Comrie, J. D., & Helm,J. M. (1997). Common feeding problems in the intensive care
nursery: Maturation, organization, evaluation, and management strategies.
Seminars in Speech and Language, 18(3), 239-260.
Cowpe-Jebson, E., Hanson, B., & Smith, C. H. (2014). What do parents of children with
dysphagia think about their MDT? A qualitative study. British Medical Journal,
4(10). doi:10.1136/bmjopen-2014-005934.

Indirect Interventions 55
Daley, H. K., & Kennedy, C. M. (2000). Meta analysis: effects of interventions on
premature infants feeding. The Journal of Perinatal & Neonatal Nursing, 14(3),
62-77.
Erkan, M., Karacay, S., Atay, A., & Gunay, Y. (2013). A modified feeding plate for a
newborn with cleft palate. Cleft Palate-Craniofacial Journal, 50(1), 109-112.
Fucile, S., Gisel, E., Schanler, R. J., & Lau, C. (2008). A controlled-flow vacuum-free
bottle system enhances preterm infants’ nutritive sucking skills. Dysphagia, 24(2),
145-151. doi:10.1007/s00455-008-9182-z.
Ganz, S. F. (1987). Decreasing tongue thrusting and tonic bite reflex through neuromotor
and sensory facilitation techniques. Physical & Occupational Therapy in
Pediatrics, 7(4), 57–75.
Gosa, M., Schooling, T., & Coleman, J. (2011). Thickened Liquids as a Treatment for
Children With Dysphagia and Associated Adverse Effects: A Systematic Review.
Infant, Child, & Adolescent Nutrition, 3(6), 344-350.
doi:10.1177/1941406411407664.
Hawdon, J. M., Beauregard, N., Slattery, J., & Kennedy, G. (2000). Identification of
neonates at risk of developing feeding problems in infancy. Developmental
Medicine and Child Neurology, 42(4), 235-239. doi:10.1111/j.1469-
8749.2000.tb00078.x.
Helfrich-Miller, K. R., Rector, K. L., & Straka, J. A. (1986). Dysphagia: Its treatment in
the profoundly retarded patient with cerebral palsy. Archives of Medical
Rehabilitation, 67(8), 520–525.

Indirect Interventions 56
Higgins, J. P. T., Green, S., & Cochrane Collaboration. (2008). Cochrane handbook for
systematic reviews of interventions. Chichester, England: Wiley-Blackwell.
Howe, T., & Wang, T. (2013). Systematic review of interventions used in or relevant to
occupational therapy for children with feeding difficulties ages birth-5 years. The
American Journal of Occupational Therapy, 67(4), 405-415.
doi:10.5014/ajot.2013.00456.
Hull, J., Aniapravan, R., Chan, E., Chatwin, M., Forton, J., Gallagher, J., Gibson, N., ...
Simonds, A. (2012). British Thoracic Society guideline for respiratory
management of children with neuromuscular weakness. Thorax, 67(5), 1-40.
Kamhawy, H., Holditch‐Davis, D., Alsharkawy, S., Alrafay, S., & Corazzini, K.
(2014).Non‐nutritive sucking for preterm infants in Egypt. Journal of Obstetric,
Gynecologic, & Neonatal Nursing, 43(3), 330-340. doi:10.1111/1552-6909.12310
Karanicolas, P. J., Bhandari, M., Walter, S.D. (2009). Radiographs of hip fractures were
digitally altered to mask surgeons to the type of implant without compromising the
reliability of quality ratings or making the rating process more difficult. Journal of
Clinical Epidemiology, 62(3), 214–23.
Karanicolas, P. J., Farrokhyar, Forough, K., & Bhandari, M. (2010). Blinding: Who,
what, when, why, how? Canadian Medical Association: Vancouver.
Kirk, A. T., Alder, S. C., & King, J. D. (2007). Cue-based oral feeding clinical pathway
results in earlier attainment of full oral feeding in premature infants. Journal of
Perinatology: Official Journal of the California Perinatal Association, 27(9), 572-
8.
Kovar, A, J. (1997). Nutrition Assessment and Management in Paediatric Dysphagia.

Indirect Interventions 57
Seminars in Speech and Language Pathology, 18(1), 39-49.
Lamm, N., Felica, A., & Cargan, A. (2005). Effect of Tactile Stimulation on Lingual
Motor Function in Paediatric Lingual Dysphagia. Dysphagia, 20(4), 311-324.
doi:10.1007/s00455-005-0060-7.
Lass, N. J., & Pannbacker, M. (2008). The application of evidence-based practice to
nonspeech oral motor treatments. Language, Speech, and Hearing Services in
Schools, 39(3), 408-421. doi:10.1044/0161-1461(2008/038).
Lau, C., & Smith, E. (2012). Interventions to improve the oral feeding performance of
preterm infants. Acta Paediatrica, 101(7), 269-274. doi:10.1111/j.1651-
2227.2012.02662.x.
Law-Morstatt, L., Judd, D. M., Snyder, P., Baier, R. J., & Dhanireddy, R. (2003). Pacing
as a treatment technique for transitional sucking patterns. Journal of Perinatology:
Official Journal of the California Perinatal Association, 23(6), 483-8.
Lefton-Greif, M.A., & Arvedson, J.A. (2007). Paediatric feeding and swallowing
disorders: State of health, population trends, and application of the international
classification of functioning, disability, and health. Seminars in Speech and
Language, 17(3), 161-165. doi:10.1055/s-2007-984722.
Linscheid, T. R. (2006). Behavioral Treatments for Paediatric Feeding Disorders.
Behavior Modification, 30(1), 6-23.
Logemann, J. A. (2000). Therapy for children with swallowing disorders in the
educational setting. Language, Speech, and Hearing Services in the Schools,
31(2), 50-55.

Indirect Interventions 58
Masarei, A. G., Wade, A., Mars, M., Sommerlad, B. C., & Sell, D. (2007). A randomized
control trial investigating the effect of presurgical orthopedics on feeding in
infants with cleft lip and/or palate. The Cleft Palate-Craniofacial Journal, 44(2),
182-193. doi:10.1597/05-184.1.
McCain, G. C., Gartside, P. S., Greenberg, J. M., & Lott, J. W. (2001). A feeding protocol
for healthy preterm infants that shortens time to oral feeding. The Journal of
Pediatrics, 139(3), 374-379. doi:10.1067/mpd.2001.117077.
McCormick, F. M., Tosh, K., & McGuire, W. (2010). Ad libitum or demand/semi-
demand feeding versus scheduled interval feeding for preterm infants. The
Cochrane Database of Systematic Reviews, 2010(2), CD005255.
Miller, C. (2011). Aspiration and Swallowing Dysfunction in Paediatric Patients. Ican-
Infant, Child, & Adolescent Nutrition, 3(6), 336-343.
doi:10.1177/1941406411423967.
Moja, L. P., Telaro, E., D'Amico, R., Moschetti, I., Coe, L., & Liberati, A. (2005).
Assessment of methodological quality of primary studies by systematic reviews:
Results of the metaquality cross sectional study. British Medical Journal,
330(7499), 1053-1053. doi:10.1136/bmj.38414.515938.8F.
Morgan, A. T., Dodrill, P., & Ward, E. C. (2012). Interventions for oropharyngeal
dysphagia in children with neurological impairment. The Cochrane Database of
Systematic Reviews, 2012(10), 1-41 doi:10.1002/14651858.CD009456.pub2.
Morgan, A., Ward, E., & Murdoch, B. (2004). A case study of the resolution of paediatric
dysphagia following brainstem injury: clinical and instrumental assessment.
Journal of Clinical Neuroscience, 11(2), 182-190.

Indirect Interventions 59
New Zealand Guideline Group. (2006). Traumatic brain injury: Diagnosis, acute
management, and rehabilitation. Wellington, New Zealand: Author.
Petticrew, M., & Roberts, H. (2006). Systematic reviews in the social sciences: A
practical guide. Malden, MA: Blackwell Pub.
Physiotherapy Evidence Database. (1999). The Pedro Scale. Sydney, Australia: Centre
for Evidence-based Physiotherapy.
Pinelli, J., Symington, A., & Ciliska, D. (2002). Nonnutritive sucking in High‐Risk
infants- Benign intervention or legitimate therapy? Journal of Obstetric,
Gynecologic, & Neonatal Nursing, 31(5), 582-591. doi-10.1111/j.1552-
6909.2002.tb00084.x.
Pridham, K., Brown, R., Sondel, S., Green, C., Wedel, N. Y., & Lai, H. C. (1998).
Transition time to full nipple feeding for premature infants with a history of lung
disease. Journal of Obstetric, Gynaecologic, and Neonatal Nursing, 27(5), 572-
578.
Puckett, B., Grover, V., Holt, T., & Sankaran, K. (2008). Cue-Based Feeding for Preterm
Infants: A Prospective Trial. American Journal of Perinatology, 25(10), 623-628.
Ravichandra, K. S., Vijayaprasad, K. E., Vasa, A. A. K., & Suzan, S. (2010). A new
technique of impression making for an obturator in cleft lip and palate patient.
Journal of the Indian Society of Pedodontics and Preventive Dentistry, 28(4), 311-
314. doi:10.4103/0970-4388.76165.
Searle, A. (1999). Introducing research and data in psychology: A guide to methods
and analysis. London: Routledge.
Sackett, D. L., Rosenberg, W. M. C., Gray, J. A. M., Haynes, R. B., & Richardson, W. S.

Indirect Interventions 60
(1996). Evidence based medicine: What it is and what it isn't: It's about integrating
individual clinical expertise and the best external evidence. British Medical
Journal, 312(7023), 71-72.
Shaker, C. S. (2013). Cue-based feeding in the NICU: Using the infant's communication
as a guide. Neonatal Network, 32(6), 404-408.
Sharp, W. G., Jaquess, D. L., Morton, J. F., & Herzinger, C. V. (2010). Paediatric Feeding
Disorders: A Quantitative Synthesis of Treatment Outcomes. Clinical Child and
Family Psychology Review, 13(4), 348-365. doi:10.1007/s10567-010-0079-7.
Shaw, W. C., Bannister, R. P., & Roberts, C. T. (1999). Assisted Feeding is More
Reliable for Infants with Clefts: A Randomized Trial. The Cleft Palate-
Craniofacial Journal, 36(3), 262-268.
Siktberg, L. L., & Bantz, D. L. (1999). Management of children with swallowing
disorders. Journal of Paediatric Health Care, 13(5), 223-229. doi:10.1016/S0891-
5245(99)90003-2.
Simpson, C., Schanler, R. J., & Lau, C. (2002). Early introduction of oral feeding in
preterm infants. Pediatrics, 110(3), 517-22.
Snider, L., Majnemer, A., & Darsaklis, V. (2011). Feeding Interventions for Children
With Cerebral Palsy- A Review of the Evidence. Physical & Occupational
Therapy in Pediatrics, 31(1), 58-77. doi:10.3109/01942638.2010.523397.
Standley, J. M. (2003). The effect of music-reinforced nonnutritive sucking on feeding
rate of premature infants. Journal of Paediatric Nursing, 18(3), 169-73.

Indirect Interventions 61
Standley, J. M., Cassidy, J., Grant, R., Cevasco, A., Szuch, C., Nguyen, J., Walworth, D.,
Adams, K. (2010). The effect of music reinforcement for non-nutritive sucking on
nipple feeding of premature infants. Paediatric Nursing, 36(3).
Sullivan, P. B., Lambert, B., Rose, M., Ford-Adams, M., Johnson, A., & Griffiths, P.
(2000). Prevalence and severity of feeding and nutritional problems in children
with neurological impairment: Oxford feeding study. Developmental Medicine
and Child Neurology, 42(10), 674-680. doi:10.1111/j.1469-8749.2000.tb00678.x.
Taylor-Goh, S. (2005). Royal College of Speech and Language Therapists clinical
guidelines: Disorders of feeding, eating, drinking & swallowing. Bicester, UK:
Speechmark Publishing Ltd.
Threats, T. (2007). Use of the ICF in dysphagia management. Seminars in Speech and
Language, 17(4), 323-333. doi:10.1055/s-2007-986529.
Ulijaszek, S. J., & Kerr, D. A. (1999). Anthropometric measurement error and the
assessment of nutritional status. The British Journal of Nutrition, 82(3), 165-77.
Watson, J., & McGuire, W. (2013). Nasal versus oral route for placing feeding tubes in
preterm or low birth weight infants. The Cochrane Database of Systematic
Reviews, (2013)2, 1-23.
White-Traut, R. C., Nelson, M. N., Silvestri, J. M., Vasan, U., Littau, S., Meleedy-Rey,
P., Patel, M. (2002). Effect of auditory, tactile, visual, and vestibular intervention
on length of stay, alertness, and feeding progression in preterm infants.
Developmental Medicine and Child Neurology, 44(2), 91-97.
doi:10.1017/S0012162201001736.

Indirect Interventions 62
Wilken, M. (2012). The impact of child tube feeding on maternal emotional state and
identity: a qualitative meta-analysis. Journal of Paediatric Nursing, 27(3), 248-55.
doi:10.1016/j.pedn.2011.01.032.
Wilkins. W., Piazza, C. C., Groff, R. A., & Vaz, P. C. (2011). Chin prompt plus re-
presentation as treatment for expulsion in children with feeding disorders. Journal
of Applied Behavior Analysis, 44(3), 513-522. doi:10.1901/jaba.2011.44-513.
Williams, S., Witherspoon, K., Kavsak, P., Patterson, C., & McBlain, J. (2006). Paediatric
feeding and swallowing problems: An interdisciplinary team approach. Canadian
Journal of Dietetic Practice and Research, 67(4), 185-190.
doi:10.3148/67.4.2006.185.
World Health Organization. (2001). International classification of functioning, disability
and health: ICF. Geneva: World Health Organization.
Yildiz, A., & Arikan, D. (2012). The effects of giving pacifiers to premature infants and
making them listen to lullabies on their transition period for total oral feeding and
sucking success. Journal of Clinical Nursing, 21(4), 5-6.
Yilmaz, G., Caylan, N., Karacan, C. D., Bodur, I., & Gokcay, G. (2014). Effect of Cup
Feeding and Bottle Feeding on Breastfeeding in Late Preterm Infants: A
Randomized Controlled Study. Journal of Human Lactation, 30(2), 174-179.
doi:10.1177/0890334413517940.

Indirect Interventions 63
Appendix A
CROBT (Higgins et al. 2008)
Domain Description Review authors’
judgment
Sequence generation
Describe the method used to generate the
allocation sequence in sufficient detail to
allow an assessment of whether it should
produce comparable groups.
Was the allocation
sequence
adequately
generated?
Allocation concealment
Describe the method used to conceal the
allocation sequence in sufficient detail to
determine whether intervention allocations
could have been foreseen in advance of, or
during, enrolment.
Was allocation
adequately
concealed?
Blinding of
participants, personnel
and outcome assessors
Assessments should be
made for each main
outcome (or class of
outcomes)
Describe all measures used, if any, to blind
study participants and personnel from
knowledge of which intervention a participant
received. Provide any information relating to
whether the intended blinding was effective.
Was knowledge of
the allocated
intervention
adequately
prevented during
the study?
Incomplete outcome
data
Assessments should be
made for each main
outcome (or class of
outcomes)
Describe the completeness of outcome data
for each main outcome, including attrition and
exclusions from the analysis. State whether
attrition and exclusions were reported, the
numbers in each intervention group
(compared with total randomized
participants), reasons for attrition/exclusions
where reported, and any re-inclusions in
analyses performed by the review authors.
Were incomplete
outcome data
adequately
addressed?
Selective outcome
reporting
State how the possibility of selective outcome
reporting was examined by the review
authors, and what was found.
Are reports of the
study free of
suggestion of
selective outcome
reporting?
Other sources of bias
State any important concerns about bias not
addressed in the other domains in the tool. If
particular questions/entries were pre-specified
in the review’s protocol, responses should be
provided for each question/entry.
Was the study
apparently free of
other problems
that could put it at
a high risk of bias?

Indirect Interventions 64
Appendix B
PS (Physiotherapy Evidence Database, 1999)

Indirect Interventions 65
Appendix C
Outcome measures for the inclusion of intervention articles (adapted from the WHO ICF
[2001]
Body structure
and function
Activity Participation Environmental
factors
(personal and
contextual)
Outco
me
measur
es
Aspiration
Pain
Failure to thrive
Malnutrition
Dehydration
Death
Growth
Physiologic function
(i.e. tongue mobility
and strength, jaw
mobility and
strength, coordination
of suck-swallow-
respiration, pooling
of food or fluid,
hyolaryngeal
excursion).
Swallow initiation
Oral feeding
(breast or
bottle)
Consistency of
diet
Broader diet
Independent
feeding
Tube feeding
Mealtime behavior
Quality of life
Mealtime
participation
Inclusion/
socialization
School/ vocational
attendance
Carer burden
Familial stress
Client opinion

Indirect Interventions 66
Appendix D
Preliminary data extraction form
Criteria for inclusion
Article
Birth-18
Indirect
intervention
Group
treatment
Outcomes
English
language

Indirect Interventions 67
Appendix E
Data extraction form- CROBT (Higgins et al. 2008)
Article
title:
Adequate
sequence
generatio
n
Allocation
concealmen
t
Blinding of
participant
s,
personnel
and
outcome
assessors
Incomplete
outcome
data
addressed
Free of
selective
outcome
reportin
g
Other
bias
Rating
Notes

Indirect Interventions 68
Appendix F
Data extraction form- PS (Physiotherapy Evidence Database, 1999)
Criteria Where/ rating
Eligibility criteria were specified
Subjects were randomly allocated to
groups (in a crossover study, subjects
were randomly allocated an order in
which treatments were received)
Allocation was concealed
The groups were similar at baseline
regarding the most important
prognostic indicators
There was blinding of all subjects
There was blinding of all therapists who
administered the therapy
There was blinding of all assessors who
measured at least one key outcome
Measures of at least one key outcome
were obtained from more than 85% of
the subjects initially allocated to groups
All subjects for whom outcome
measures were available received the
treatment or control condition as
allocated or, where this was not the
case, data for at least one key outcome
was analyzed by “intention to treat”
The results of between-group statistical
comparisons are reported for at least
one key outcome
The study provides both point measures
and measures of variability for at least
one key outcome

Indirect Interventions 69
Appendix G
Data synthesis for articles using modified equipment
Intervention Control
N Mean (SD) N Mean(SD) Effect
size CI95%
Fucile et al. (2008) rate of milk transfer at 1-2
feedings/day 15 14.1(3.5) 15 17.7(4.7) -0.84 [-1.57, -0.11]
Fucile et al. (2008) rate of milk transfer at 6-8
feedings/day 15 12.3(4.7) 15 18.9(3.4) -1.56 [-2.36, -0.76]
Fucile et al. (2008) sucking breast duration at
1-2 feedings/day 15 12.8(7.6) 15 16.2(16.2) -0.26 [-0.96, 0.43]
Fucile et al. (2008) sucking breast duration at
6-8 feedings/day 15 16.1(11.3) 15 13.4(7.6) *0.27 [-0.42, 0.97]
Fucile et al. (2008) suction amplitude at 1-2
feedings/day 15 -35.8(21.2) 15 -26.2(19.8) -0.45 [-1.16, 0.25]
Fucile et al. (2008) suction amplitude at 6-8
feedings/day 15 -52.0(47.3) 15 -35.7(25.7) -0.41 [-1.12, 0.28]
Shaw et al. (1999) head circumference at week
6 52 38.1(1.5) 48 38.5(1.5) -0.26 [-0.65, 0.12]
Shaw et al. (1999) head circumference at week
13 51 40.4(1.3) 49 41(1.3) -0.43 [-0.83, -0.04]
Shaw et al. (1999) head circumference at week
26 50 43.5(1.2) 49 44(1.3) -0.38 [-0.78, 0.11]
Shaw et al. (1999) head circumference at week
52 50 46.1(1.4) 49 47.1(1.4) -0.68 [-1.08, 0.02]
Shaw et al. (1999) length at week 6 52 55.3(2.0) 47 55.3(2.2) *0.00 [-0.39, 0.19]
Shaw et al. (1999) length at week 13 51 60.2(2.2) 48 60.3(1.9) -0.04 [-0.43, 0.45]

Indirect Interventions 70
Shaw et al. (1999) length at week 26 50 66.7(2.5) 49 66.8(2.1) -0.04 [-0.43, 0.25]
Shaw et al. (1999) length at week 52 50 74.8(3.0) 49 75.1(2.3) -0.10 [-0.50, 0.27]
Shaw et al. (1999) weight at week 6 52 4.3(0.5) 49 4.4(0.5) -0.10 [-0.49, 0.83]
Shaw et al. (1999) weight at week 26 52 7.0(1.5) 49 7.3(0.7) -0.27 [-0.66, 0.11]
Shaw et al. (1999) weight at week 52 50 9.2(1.2) 49 9.6(1.0) -0.36 [-0.76, 0.02]
Yilmaz et al. (2014) any breastfeeding at 3m 254 223.0(88.0) 268 221.0(82.0) *0.02 [-0.14, 0.19]
Yilmaz et al. (2014) any breastfeeding at 6m 254 176.0(69.0) 268 158.0(59.0) *0.28 [0.10, 0.45]
Yilmaz et al. (2014) any breastfeeding at
discharge 254 252.0(99.0) 268 244.0(91.0) *0.08 [-0.08, 0.25]
Yilmaz et al. (2014) exclusive breastfeeding at
3m 254 196.0(77.0) 268 126(47) *1.10 [0.91, 1.28]
Yilmaz et al. (2014) exclusive breastfeeding at
6m 254 146.0(57.0) 268 113(42) *0.66 [0.48, 0.83]
Yilmaz et al. (2014) exclusive breastfeeding at
discharge 254 184.0(72.0) 268 123(46) *1.01 [0.83, 1.19]
Yilmaz et al. (2014) feeding time 254 13.7(1.7) 268 13.6(1.6) *0.06 [-0.11,0.23]
Yilmaz et al. (2014) hospital stay 254 25.7(2.2) 268 25.9(2.2) *0.09 [-0.26, 0.08]
Yilmaz et al. (2014) infant gestational age at
discharge 254 36.4(2.6) 268 36.5(2.5) -0.03 [-0.21, 0.13]
Yilmaz et al. (2014) weight gain in the first 7
days of study 254 16.7(1.5) 268 16.8(1.5) -0.06 [-0.23, 1.00]
Note. * = Positive effect of treatment (where 0.0-0.3 has a small effect, 0.3-0.5 has a moderate effect and 0.5-1 has a large effect). To demonstrate
positive effects of reduced length of stay, outcomes relating to length of stay measures have been inverted from negative to positive.

Indirect Interventions 71
Figure 14. Forest plot demonstrating the effects of interventions using modified
equipment.
-3-2
.5-2
-1.5
-1-0
.50
0.5
11
.5
Fuci
le e
t al
. (2
008
) -
Rat
e o
f m
ilk t
ransf
er @
1-2
fee
din
gs/
day
Fuci
le e
t al
. -
Rat
e o
f m
ilk t
ransf
er @
6-8
fee
din
gs/
day
Fuci
le e
t al
. -
Suck
ing b
reas
t du
rati
on @
1-2
fee
din
gs/
day
Fuci
le e
t al
. -
Suck
ing b
reas
t du
rati
on @
6-8
fee
din
gs/
day
Fuci
le e
t al
. -
Suct
ion a
mpli
tud
e @
1-2
fee
din
gs/
day
Fuci
le e
t al
. -
Suct
ion a
mpli
tud
e @
6-8
fee
din
gs/
day
Shaw
et
al.
(19
99
) -
Hea
d c
ircu
mfe
ren
ce @
wk 6
Shaw
et
al.
- H
ead
cir
cum
fere
nce
@ w
k 1
3
Shaw
et
al.
- H
ead
cir
cum
fere
nce
@ w
k 2
6
Shaw
et
al.
- H
ead
cir
cum
fere
nce
@ w
k 5
2
Shaw
et
al.
- L
eng
th @
wk 6
Shaw
et
al.
- L
eng
th @
wk 1
3
Shaw
et
al.
- L
eng
th @
wk 2
6
Shaw
et
al.
- L
eng
th @
wk 5
2
Shaw
et
al.
- W
eigh
t at
wk
6
Shaw
et
al.
- W
eigh
t @
wk
26
Shaw
et
al.
- W
eigh
t @
wk
52
Yil
maz
et
al. (2
014
) -
Any
bre
astf
eedin
g @
3m
Yil
maz
et
al. -
Any
bre
astf
eed
ing
@ 6
m
Yil
maz
et
al. -
Any
bre
astf
eed
ing
at
dis
char
ge
Yil
maz
et
al. -
Excl
usi
ve
bre
astf
eedin
g a
t 3m
Yil
maz
et
al. -
Excl
usi
ve
bre
astf
eedin
g a
t 6m
Yil
maz
et
al. -
Excl
usi
ve
bre
astf
eedin
g a
t dis
char
ge
Yil
maz
et
al. -
Fee
din
g t
ime
Yil
maz
et
al. -
Hosp
ital
sta
y
Yil
maz
et
al. -
Infa
nt
ges
tati
onal
ag
e at
dis
char
ge
Yil
maz
et
al. -
Wei
gh
t g
ain i
n t
he
1st
7 d
ays
of
stu
dy
Eff
ect
Siz
e F
avou
rs i
nte
rven
tion
F
avou
rs c
on
trol

Indirect Interventions 72
Appendix H
Data synthesis table for articles altering rate of presentation
Intervention Control
N Mean (SD) N Mean(SD) Effect size CI95%
Davidson et al. (2013) average weight velocity 55 14.0(11.0) 60 12.0(10.0) *0.18 [-0.17, 0.55]
Davidson et al. (2013) days from first to full oral feeding 55 9.0 (6.0) 60 19.0 (13.0) -0.96 [-1.35, -0.58]
Davidson et al. (2013) overall weight gain 55 350.0 (195.0) 60 461.0(316.0) -0.41 [-0.78, -0.00]
Davidson et al. (2013) PMA at first oral feeding 55 35.2 (1.63) 60 35.0(2.7) *0.08 [-0.27, 0.45]
Kirk et al. (2007) PMA at full oral feeding 28 252.0 (10.0) 23 258.0(11.0) -0.56 [-1.11, -0.01]
Kirk et al. (2007) rate of weight gain 28 14.5 (11.4) 23 9.4(13.0) *0.41 [-0.13, 0.96]
Law-Morstatt et al. (2003) bradycardias during feedings 18 15.7 (23.8) 18 34.4(33.0) -0.65 [-0.13, 0.96]
Law-Morstatt et al. (2003) chronological age at NICU discharge 18 5.0(3.0) 18 7.0(3.0) -0.65 [-0.22, 0.47]
Law-Morstatt et al. (2003) discharge weight 18 2196.0(342.0) 18 2360.0(418.0) -0.41 [-1.06, 0.22]
Law-Morstatt et al. (2003) mean bradycardias per week 18 6.12(8.51) 18 13.55(11.87) -0.70 [-1.36, -0.04]
Law-Morstatt et al. (2003) PCA at discharge date 18 36.0(2.0) 18 37.0(2.0) -0.48 [-1.13, 0.15]
Law-Morstatt et al. (2003) weekly weight gain 18 206(73.8) 18 251.0(108.0) -0.47 [1.12, 0.71]
Law-Morstatt et al. (2003) weeks in study 18 2.2(0.9) 18 2.6(1.1) -0.38 [-1.02, 0.26]
Pucket et al. (2008) adverse events 39 3.5(3.3) 40 12.8(14.4) -0.87 [-1.33, -0.41]
Pucket et al. (2008) bottle feeder intake 39 154.4(2.0) 40 155.8(20.1) -0.09 [-0.53, 0.34]

Indirect Interventions 73
Pucket et al. (2008) exit weight 39 2304.0(234.0) 40 2379.0(227.0) -0.32 [-0.76, 0.11]
Pucket et al. (2008) LOS after entry adjusted for gestation age 39 10.0(3.4) 40 14.5(4.3) *1.14 [-1.61, -0.67]
Pucket et al. (2008) nonadjusted LOS 39 10.0(6.3) 40 14.5(8.6) *0.58 [-1.03,-0.14]
Pucket et al. (2008) PCA at exit weight gain 39 35.8(1.1) 40 36.5(1.5) -0.52 [0.97, -0.08]
Pucket et al. (2008) weight gain 39 12.6(4.1) 40 12.7(3.5) -0.02 [-0.46, 0.41]
Simpson et al. (2002) 4 successful oral feedings: PMA 13 34.1(1.7) 16 35.3(1.4) -0.75 [-1.49, -0.01]
Simpson et al. (2002) 4 successful oral feedings: PNA 13 43.6(13.7) 16 54.4(12.6) -0.80 [-1.54, -0.06]
Simpson et al. (2002) all oral feedings: PMA 13 43.5(1.6) 16 36.0(1.5) -0.94 [-1.69, -0.19]
Simpson et al. (2002) all oral feedings: PNA 13 46.4(13.9) 16 58.7(14.5) -0.83 [-1.58, -0.09]
Simpson et al. (2002) first successful total oral feed 13 13.8(8.8) 16 11.9(6.4) *0.24 [-0.46, 0.95]
Simpson et al. (2002) first successful oral feeding: PMA 13 34.4(1.) 16 34.3(0.9) -1.95 [-2.82, -1.08]
Simpson et al. (2002) first successful oral feeding: PNA 13 32.1(9.9) 16 46.9(10.9) -1.37 [-2.16, -0.57]
Simpson et al. (2002) hospital discharge (d) 13 57.0(17.7) 16 67.0(16.6) *0.56 [-1.29, 0.15]
Simpson et al. (2002) hospital discharge (w) 13 36.0(2.1) 16 37.1(1.8) *0.55 [-1.27, 0.17]
Simpson et al. (2002) introduction of oral feeding to 1st oral feed 13 9.3(7.7) 16 3.7(3.5) *0.94 [0.19, 1.69]
Simpson et al. (2002) introduction to oral feeding 13 31.1(1.3) 16 33.7(14.0) -2.15 [-3.05, -1.25]
Simpson et al. (2002) transition from tube to all oral feeding 13 26.8(12.3) 16 38.4(14.0) -0.84 [-1.59, -0.10]
Note. * = Positive effect of treatment (where 0.0-0.3 has a small effect, 0.3-0.5 has a moderate effect and 0.5-1 has a large effect); PMA =
Postmenstrual age; PCA = Post conceptual age; LOS = Length of stay; PNA = Post natal age. To demonstrate positive effects of reduced length
of stay, outcomes relating to length of stay measures have been inverted from negative to positive.

Indirect Interventions 74
Figure 15. Forest plot demonstrating the effects of interventions altering rate of
presentation.
-4-3
-2-1
01
2
Dav
idso
n e
t al
. (2
013
) -
Av
erag
e w
eig
ht
vel
oci
ty
Dav
idso
n e
t al
. -
Day
s fr
om
fir
st t
o f
ull
ora
l fe
edin
g
Dav
idso
n e
t al
. -
Over
all
wei
ght
gai
n
Dav
idso
n e
t al
. -
PM
A a
t fi
rst
ora
l fe
edin
g
Kir
k e
t. a
l. (
200
7)
- P
MA
at
full
ora
l fe
edin
g
Kir
k e
t al
. -
Rat
e o
f w
eigh
t g
ain
Law
-Mors
tatt
et
al.
(20
03
) -
Bra
dyca
rdia
s d
uri
ng f
eed
ing
s
Law
-Mors
tatt
et
al.
- C
hro
nolo
gic
al a
ge
at N
ICU
dis
char
ge
Law
-Mors
tatt
et
al.
- D
isch
arg
e w
eig
ht
Law
-Mors
tatt
et
al.
- M
ean
bra
dyca
rdia
s p
er w
eek
Law
-Mors
tatt
et
al.
- P
CA
at
dis
char
ge
dat
e
Law
-Mors
tatt
et
al.
- W
eek
ly w
eig
ht
gai
n
Law
-Mors
tatt
et
al.
- W
eek
s in
stu
dy
Puck
et e
t al
. (2
00
8)
- A
dv
erse
even
ts
Puck
et e
t al
. -
Bott
le f
eed
er i
nta
ke
Puck
et e
t al
. -
Exit
wei
gh
t
Puck
et e
t al
. -
LO
S a
fter
entr
y a
dju
sted
for
ges
tati
on
age
at b
irth
Puck
et e
t al
. -
No
nad
just
ed L
OS
Puck
et e
t al
. -
PC
A a
t ex
it
Puck
et e
t al
. -
Wei
gh
t g
ain
Sim
pso
n e
t al
. (2
002
) -
4 s
ucc
essf
ul
ora
l fe
edin
gs:
PM
A
Sim
pso
n e
t al
. -
4 s
ucc
essf
ul
ora
l fe
edin
gs:
PN
A
Sim
pso
n e
t al
. -
All
ora
l fe
edin
gs:
PM
A
Sim
pso
n e
t al
. -
All
ora
l fe
edin
gs:
PN
A
Sim
pso
n e
t al
. -
Fir
st s
ucc
essf
ul
tota
l ora
l fe
ed
Sim
pso
n e
t al
. -
Fir
st s
ucc
essf
ul
ora
l fe
edin
g:
PM
A
Sim
pso
n e
t al
. -
Fir
st s
ucc
essf
ul
ora
l fe
edin
g:
PN
A
Sim
pso
n e
t al
. -
Hosp
ital
dis
char
ge
(d)
Sim
pso
n e
t al
. -
Hosp
ital
dis
char
ge
(wk)
Sim
pso
n e
t al
. -
Intr
od
uct
ion o
f o
ral
feed
ing t
o 1
st o
ral
feed
Sim
pso
n e
t al
. -
Intr
od
uct
ion t
o o
ral
feed
ing:
PN
A
Sim
pso
n e
t al
. -
Intr
od
uct
ion t
o o
ral
feed
ing:
PW
A
Sim
pso
n e
t al
. -
Tra
nsi
tion
fro
m t
ub
e to
all
ora
l fe
edin
g
Eff
ect
Siz
e F
avou
rs i
nte
rven
tion
F
avou
rs c
on
trol

Indirect Interventions 75
Appendix I
Data synthesis for articles involving an environmental change
Intervention Control
N M (SD) N M (SD)
Effect
Size 95% CI
Standley et al. (2010) discharge weight at week 32 8 2.2(0.5) 8 2.4(0.5) -0.28 [-1.21, 0.64]
Standley et al. (2010) discharge weight at week 34 8 2.2(0.36 7 2.1(0.1) *0.32 [-0.63, 1.28]
Standley et al. (2010) discharge weight at week 36 8 2.2(0.28) 6 2.6(0.6) -0.78 [-1.83, 0.23]
Standley et al. (2010) gavage days at week 32 8 46.7(17.3) 8 48.5(15.8) -0.09 [-1.02, 0.82]
Standley et al. (2010) gavage days at week 34 8 46.7(17.3) 8 33.2(8.5) *0.93 [-0.04, 1.91]
Standley et al. (2010) gavage days at week 36 8 68.8(25.3) 7 67.7(13.3) *0.05 [-0.90, 1.00]
Standley et al. (2010) days to discharge at week 32 8 5.1(2.36) 8 6.0(3.5) *0.27 [-1.2, 0.66]
Standley et al. (2010) days to discharge at week 34 8 3.8(2.75) 7 4.1(1.8) *0.11 [-1.07, 0.84]
Standley et al. (2010) days to discharge at week 36 8 6.5(2.4) 6 7.8(3.5) *0.43 [-1.43, 0.57]
Standley et al. (2010) weight gain at week 32 8 1.0(0.5) 8 1.1(0.5) -0.28 [-1.21, 0.65]
Standley et al. (2010) weight gain at week 34 8 1.0(0.4) 7 0.7(0.3) *0.68 [-0.29, 1.67]
Standley et al. (2010) weight gain at week 36 8 1.3(0.3) 6 1.5(0.6) -0.41 [-1.42, 0.58]
Note. * = Positive effect of treatment (where 0.0-0.3 has a small effect, 0.3-0.5 has a moderate effect and 0.5-1 has a large effect). To demonstrate
positive effects of reduced length of stay, outcomes relating to length of stay measures have been inverted from negative to positive.

Indirect Interventions 76
Figure 16. Forest plot demonstrating the effects of interventions involving an environmental
change.
-2.5
-2-1
.5-1
-0.5
00
.51
1.5
22
.5
Sta
nd
ley e
t al
. (2
010
) -
Dis
char
ge
wei
ght
@ w
k 3
2
Sta
nd
ley e
t al
. -
Dis
char
ge
wei
ght
@ w
k 3
4
Sta
nd
ley e
t al
. -
Dis
chra
ge
wei
ght
@ w
k 3
6
Sta
nd
ley e
t al
. -
Gar
vag
e d
ays
@ w
k 3
2
Sta
nd
ley e
t al
. -
Gar
vag
e d
ays
@ w
k 3
4
Sta
nd
ley e
t al
. -
Gar
vag
e d
ays
@ w
k 3
2
Sta
nd
ley e
t al
. -
PO
day
s to
dis
char
ge
@ w
k 3
2
Sta
nd
ley e
t al
. -
PO
day
s to
dis
char
ge
@ w
k 3
4
Sta
nd
ley e
t al
. -
PO
day
s to
dis
char
ge
@ w
k 3
6
Sta
nd
ley e
t al
. -
Weig
ht
gai
n @
wk 3
2
Sta
nd
ley e
t al
. -
Weig
ht
gai
n @
wk 3
4
Sta
nd
ley e
t al
. -
Weig
ht
gai
n @
wk 3
6
Eff
ect
Siz
e F
avou
rs i
nte
rven
tion
F
avou
rs c
on
trol