Embed Size (px)
Citation preview

Enrico Fiaccadori
Acute Renal Failure Unit
Parma University Medical School
Indicazioni alle tecnichedialitiche in urgenza
Agenda
What the ED doctor should absolutely know on emergencydialysis
• When it is necessary to call the nephrologist (the indications to urgent/emergency renal replacement therapy)
• What is the minimum time needed to start a dialysis session in the urgent/emergency setting
• What RRT is able to do, and in how many time: the case of potassium
Conventional indications for starting RRT
• Severe hyperkalemia refractory to medical treatment and/or with severe EKG alterations (> 6.5 mEq/L)
• Metabolic acidosis refractory to medical therapy (pH < 7.10, HCO3- < 10 mEq/L)
• Volume overload unresponsive to diuretic therapy, especially when severe acute
respiratory failure and oliguria coexist
• Concomitant intoxication with dialyzable drug or toxin
• Oligoanuria
• Uremia (encephalopathy, pericarditis, etc.,)
• Progressive azotemia (serum creat > 8-10 mg/dL, BUN more than 100 mg/dL)
Conventional indications for starting RRT
• Severe hyperkalemia refractory to medical treatment and/or with severe EKG alterations (> 6.5 mEq/L)
• Metabolic acidosis refractory to medical therapy (pH < 7.10, HCO3- < 10 mEq/L)
• Volume overload unresponsive to diuretic therapy, especially when severe acute
respiratory failure and oliguria coexist
• Concomitant intoxication with dialyzable drug or toxin
• Oligoanuria
• Uremia (encephalopathy, pericarditis, etc.,)
• Progressive azotemia (serum creat > 8-10 mg/dL, BUN more than 100 mg/dL)
•A 76-year-old man, discharged 3 days earlier after “uncomplicated” surgery for inguinal hernia, presented to ED with vomiting, diarrhea, abdominal pain, hypotension, and a large lower abdomen and thigh hematoma
• Type 2 diabetes, arterial hypertension, severe dilated cardiomyopathy (EF 20-25%), and CKD (usual sCr 1.8 mg/dL, eGFR 36 mL/min/1.73m2)
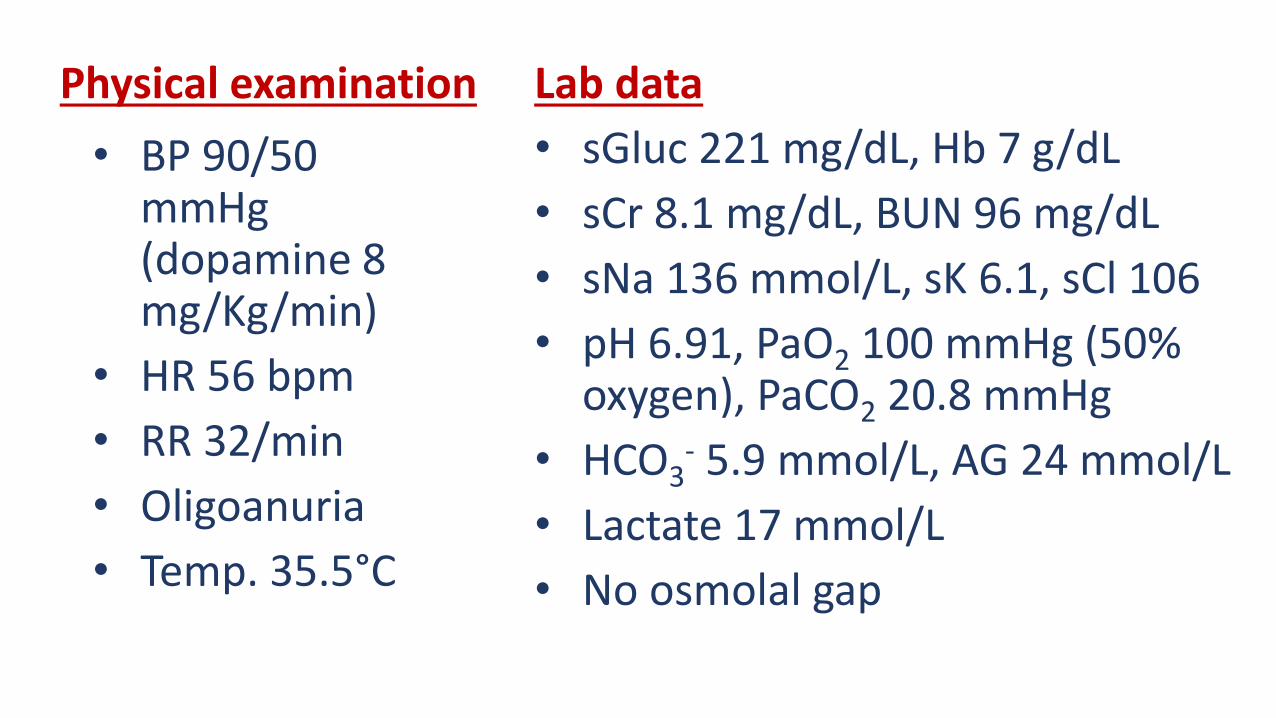
Lab data
• sGluc 221 mg/dL, Hb 7 g/dL
• sCr 8.1 mg/dL, BUN 96 mg/dL
• sNa 136 mmol/L, sK 6.1, sCl 106
• pH 6.91, PaO2 100 mmHg (50% oxygen), PaCO2 20.8 mmHg
• HCO3- 5.9 mmol/L, AG 24 mmol/L
• Lactate 17 mmol/L
• No osmolal gap
Physical examination
• BP 90/50 mmHg (dopamine 8 mg/Kg/min)
• HR 56 bpm
• RR 32/min
• Oligoanuria
• Temp. 35.5°C
Renal consult
•Abdomen CT scan with contrast
•Pharmacologic history

Therapy at home:Metformin 1 g x 3
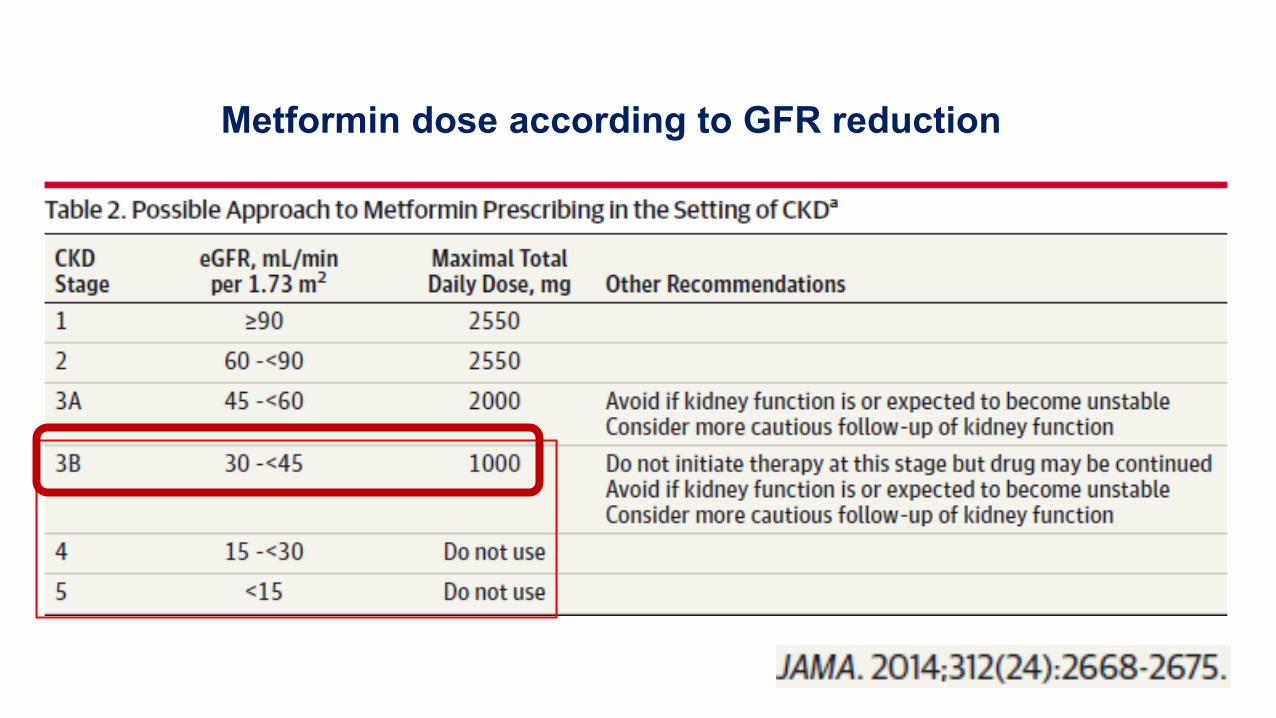
Metformin dose according to GFR reduction
The indications to emergency renal
replacement terapy in metformin intoxication are based on clinical suspicion,
not on drug levels

The indications to emergency renal
replacement terapy in metformin intoxication
are based on clinicalsuspicion, not on drug
levels
Calello DP at al. Crit Care Med 2015; 43:1716-30
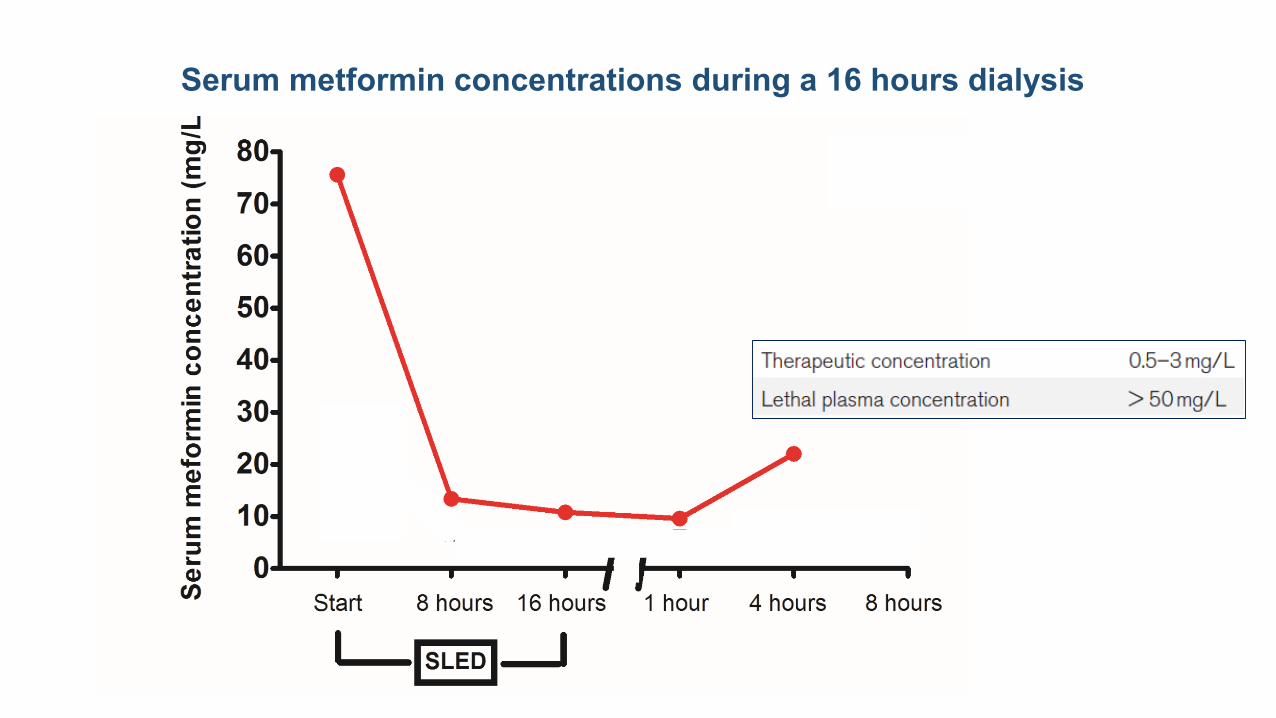
Serum metformin concentrations during a 16 hours dialysis

Physicochemical data and pharmacokinetics of metformin
Regolisti G, Fiaccadori E. Am J Kidney Dis 2017, in press
The four PK characteristics making a molecule(toxin or drug) easily removable by dialysis
• Low molecular weight (< 500-1000 daltons)
• Hydrophylic
• Low protein bound (< 70%)
• Low distribution volume (Vd < 1 L/Kg)
What is the time lagbetween the nephrologyconsult request and renal
replacement therapy (RRT) start in emergency
conditions?
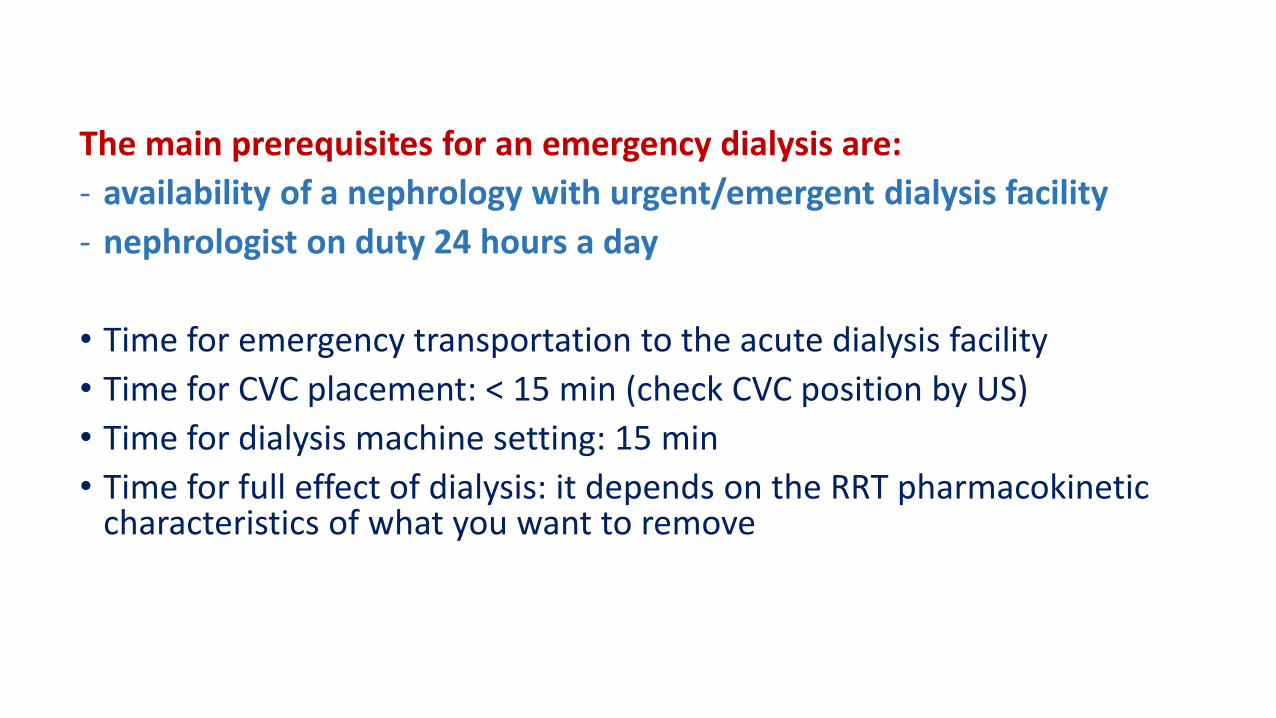
The main prerequisites for an emergency dialysis are:
- availability of a nephrology with urgent/emergent dialysis facility
- nephrologist on duty 24 hours a day
• Time for emergency transportation to the acute dialysis facility
• Time for CVC placement: < 15 min (check CVC position by US)
• Time for dialysis machine setting: 15 min
• Time for full effect of dialysis: it depends on the RRT pharmacokineticcharacteristics of what you want to remove
What dialysis isable to do and in how many time:
the case of potassium

K 8.1 mEq/L, Ca 8.5 mg/dL
K 8.2 mEq/L, Ca 10.2 mg/dL
K 7.9 mEq/L, Ca 11.0 mg/dL
K 6.1 mEq/L, Ca 10.0 mg/dL
i.v. Ca gluc 1 amp
i.v. Ca gluc 1 amp
Time +10’ (HD start)
Time + 24’ (HD 14’)
Time + 70’ (HD 60’)
Acute kidney injury, oliguria, usual EKG normal
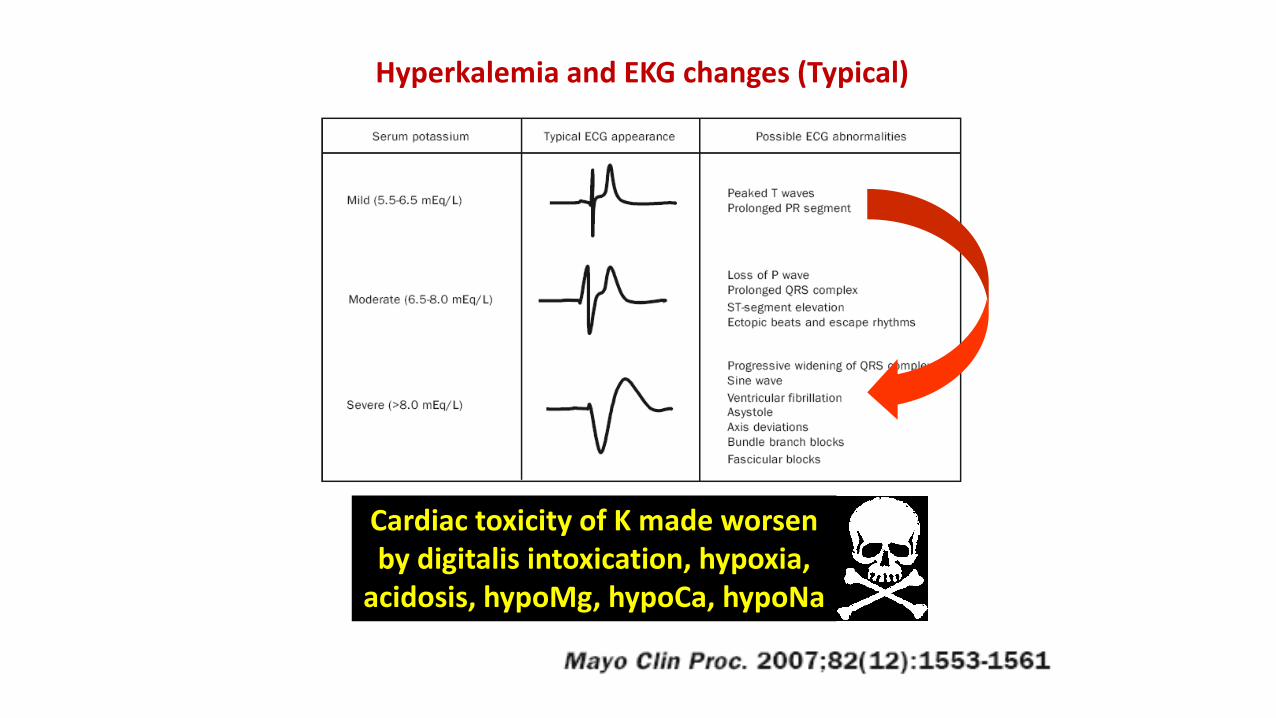
Hyperkalemia and EKG changes (Typical)
Cardiac toxicity of K made worsenby digitalis intoxication, hypoxia,
acidosis, hypoMg, hypoCa, hypoNa
Who do I call: the nephrologist or the
cardiologist?Confucius in the ED
Two types of problems withpacemakers in severe hyperK
Time to Pace-maker
positioning
Pace-maker functioning
in severe hyperkalemia
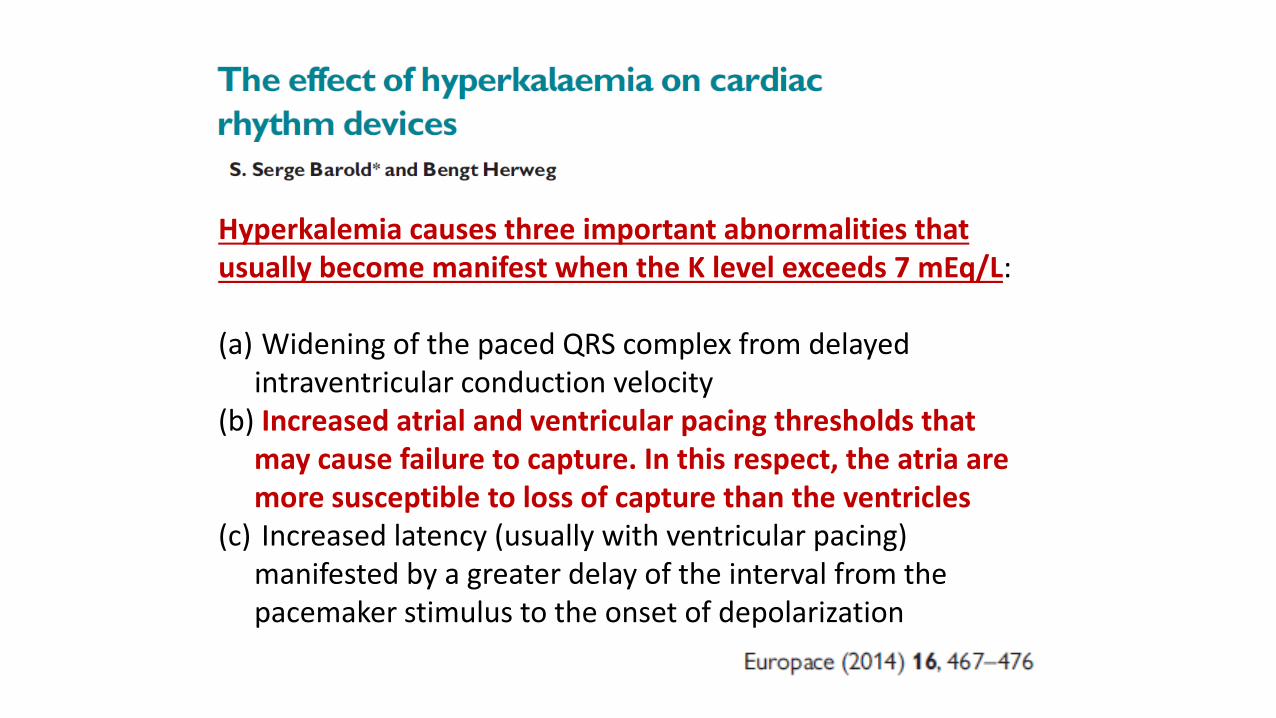
Hyperkalemia causes three important abnormalities that usually become manifest when the K level exceeds 7 mEq/L:
(a) Widening of the paced QRS complex from delayed intraventricular conduction velocity
(b) Increased atrial and ventricular pacing thresholds that may cause failure to capture. In this respect, the atria are more susceptible to loss of capture than the ventricles
(c) Increased latency (usually with ventricular pacing) manifested by a greater delay of the interval from the pacemaker stimulus to the onset of depolarization
How many hours of RRT to getK values < 6.5 mEq/L starting from 8 mEq/L?
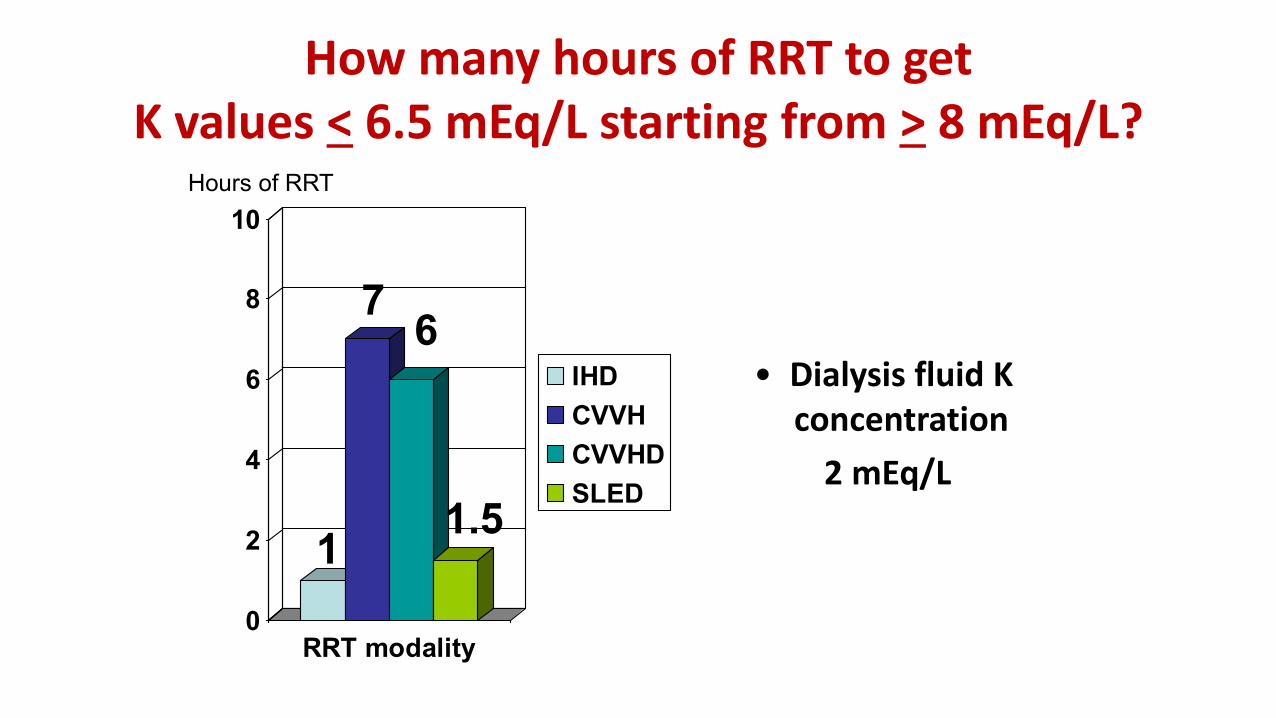
How many hours of RRT to getK values < 6.5 mEq/L starting from > 8 mEq/L?
0
2
4
6
8
10
RRT modality
IHD
CVVH
CVVHD
SLED
• Dialysis fluid K concentration
2 mEq/L
Hours of RRT
1
76
1.5
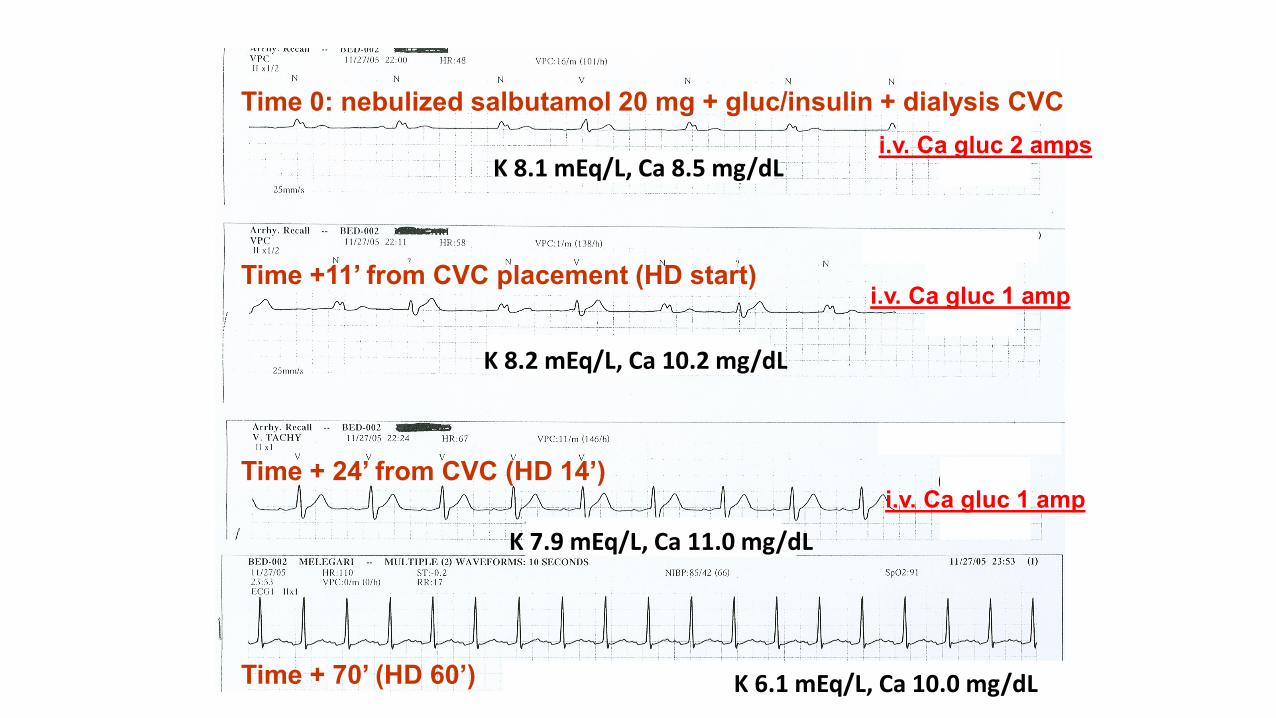
K 8.1 mEq/L, Ca 8.5 mg/dL
K 8.2 mEq/L, Ca 10.2 mg/dL
K 7.9 mEq/L, Ca 11.0 mg/dL
K 6.1 mEq/L, Ca 10.0 mg/dL
i.v. Ca gluc 2 amps
i.v. Ca gluc 1 amp
i.v. Ca gluc 1 amp
Time 0: nebulized salbutamol 20 mg + gluc/insulin + dialysis CVC
Time +11’ from CVC placement (HD start)
Time + 24’ from CVC (HD 14’)
Time + 70’ (HD 60’)
Take home messages
- Know the indications to emergency dialysis
- Know the time-lag (logistics) for nephrologist(and other specialists) activation
- Know the pharmacokinetic bases of the effects of emergency dialysis (what isremovable and what is not removable)
- Know the pathophysiological bases and the time–lag of emergency dialysis effects (notalways the most efficient treatment is the most rapid)





























