Embed Size (px)
Citation preview
Combined Subcision, Autologous Fat Grafting and Microskin Grafting for an Unsightly Facial Scar in Fitzpatrick Skin Type V: A Case Report
Souvik Adhikari, Tibar Bandyopadhyay, Jayanta Kr. Saha
Case Report
Department of Plastic andReconstructive Surgery Institute of Post Graduate Medical Education and ResearchKolkata, India
Received: February 06, 2012 Accepted: February 11, 2012 Arch Clin Exp Surg 2013;2: 59-62DOI:10.5455/aces.20120211102101
Corresponding author:Souvik Adhikari Department of Plastic andReconstructive Surgery Institute of Post Graduate Medical Education and Research 244 A. J. C. Bose Road Kolkata – 700020, WB, [email protected]
IntroductionUnsightly scars over the face can be an
especially difficult problem to treat and the problem is even more complicated when it becomes depressed. The scar adheres to the deeper structures and surgical revi-sion of the scar might lead to recurrence. It can also have a catastrophic outcome in patients with darker skin because of the propensity of these patients to develop hy-pertrophic scars and keloids in the area of
surgery. A variety of treatment modalities are advocated for the treatment of these unsightly scars, which might be additional-ly depressed with variable benefits. Autolo-gous fat transfer has been advocated as an effective measure for treating scars when combined with subcision when these be-come depressed. Here, we describe a pa-tient with Fitzpatrick skin type V having a linear unsightly scar over the face, who was managed with autologous fat transfer after
1Bauru Dental SchoolUniversity of São PauloBauru–SP, Brazil
2Araraquara Dental SchoolSão Paulo State UniversityAraraquara-SP, Brazil
Received: February 05, 2012 Accepted: February 29, 2012 Arch Clin Exp Surg 2012;X: X-XDOI: 10.5455/aces.20120229052919
Corresponding authorÉrica Dorigatti de AvilaDepartamento de Estomatologia da Faculdade de Odontologia de BauruUniversidade de São Paulo (USP)Avenida Alameda Octávio Pinheiro Brizola, 9-75, 17012-901 Bauru–SP, [email protected]
Original Article
Increased of Langerhans Cells in Smokeless Tobacco-Associated Oral Mucosal Lesions
Érica Dorigatti de Ávila1, Rafael Scaf de Molon2, Melaine de Almeida Lawall1, Renata Bianco Consolaro1, Alberto Consolaro1
Abstract
Objective: To evaluate the changes in the number of Langerhans Cells (LC) observed in the epithelium of smokeless tobacco (SLT-induced) lesions. Methods: Microscopic sections from biopsies carried out in the buccal mucosa of twenty patients, who were chronic users of smokeless tobacco (SLT), were utilized. For the control group, twenty non-SLT users of SLT with normal mucosa were selected. The sections were studied with routine coloring and were immunostained for S-100, CD1a, Ki-67 and p63. These data were statistically analyzed by the Student’s t-test to investigate the differences in the expression of immune markers in normal mucosa and in SLT-induced leukoplakia lesions. Results: There was a significant difference in the immunolabeling of all markers between normal mucosa and SLT-induced lesions (p<0.001). The leukoplakia lesions in chronic SLT users demonstrated a significant increase in the number of Langerhans cells and in the absence of epithelial dysplasia. Conclusion: The increase in the number of these cells represents the initial stage of leukoplakia. Key words: Smokeless tobacco, leukoplakic lesions, cancer, langerhans cells, chewing tobacco.
Introduction
Among tobacco users, there is a false be-lief that SLT is safe because it is not burned, which leads many people to quit cigarettes and start using SLT [1]. However, SLT con-tains higher concentrations of nicotine than cigarettes and, in addition, nearly 30 carci-nogenic substances, such as tobacco-specific N-nitrosamines (TSNA), which is formed during the aging process of the tobacco, [2-4] and which presents high carcinogenic poten-tial. Moreover, because the tobacco has direct
contact with the oral mucosa and creates a more alkaline environment, its products may even be more aggressive to tissue [5]. The percentage of SLT users is lower compared to cigarette users; however, usage is increasing among young individuals and it is therefore a significant and disturbing danger [6,7].
Initial studies on the effects of SLT on the oral mucosa demonstrated the formation of white lesions induced by chronic exposure to tobacco, characterized by epithelial thicken-ing, increased vascularization, collagen altera-
Archives of ClinicalExperimental Surgery
Abstract
Unsightly scars pose a challenge to the plastic surgeon because apart from their appearance, they might be adhered to the underlying structures. This situation is complicated when the scar becomes hypopigmented and is found in individuals with Fitzpatrick Type V skin types. Autologous fat trans-fer following subcision has been depicted as an important modality in the management of unsightly scars that are additionally depressed. Microskin grafting can alter hypopigmented areas if applied judiciously. Taken in combination, these methods of scar revision can be important tools in the arma-mentarium of the plastic surgeon. We hereby portray a case of an unsightly facial scar adherent to the underlying structures in a woman with Fitzpatrick skin type V, who was successfully managed with a combination of subcision, autologous fat transfer and microskin grafting.
Key words: Fat transfer, microskin grafting, unsightly scar
subcision, followed by microskin grafting in the same sitting to counter the pigmentation changes.
Case ReportA 39-year-old female patient came to our clinic with
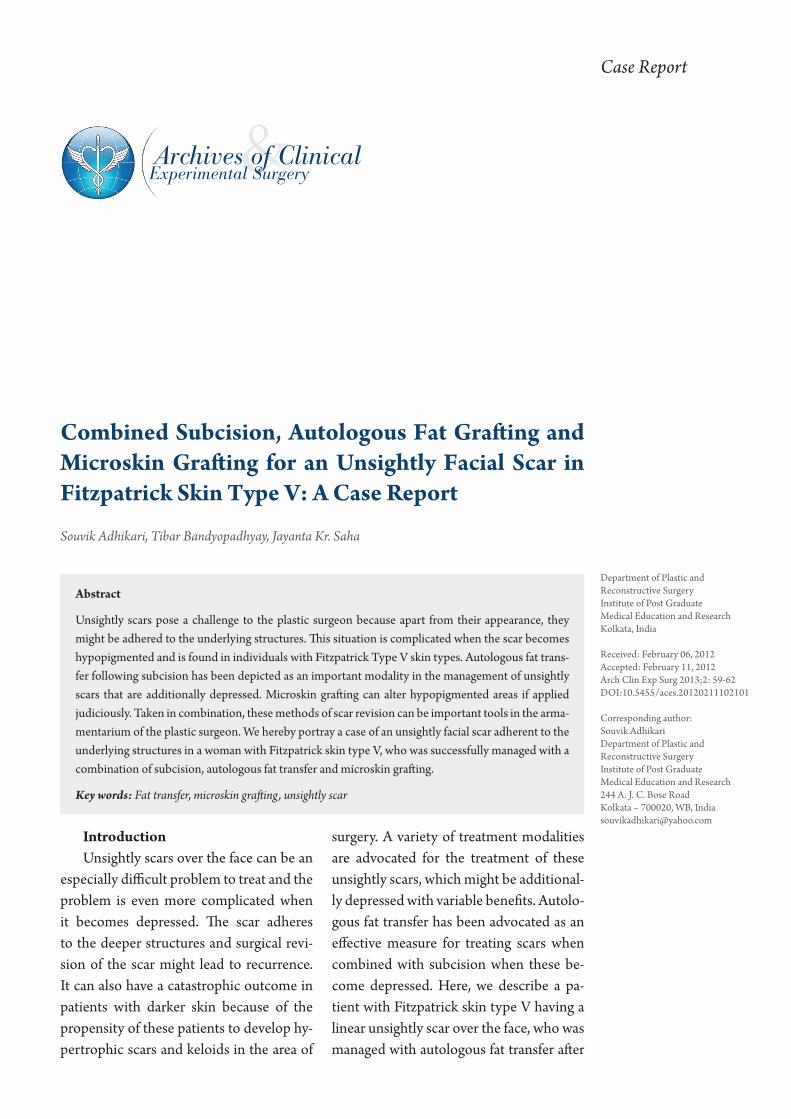
the complaint of an unsightly scar over the left half of her face, which had developed following injury to the same region by a sword about 1 year back (Figure 1). The injured area was sutured, which led to the develop-ment of a linear scar depressed at places. To complicate
Figure 1. Scar with irregular contour over the left side of the face prior to steroid injections.
things, the scar started to hypertrophy for which she was given 4 doses of locally administered Inj. Triamci-nolone spaced at monthly intervals. The ultimate result was aesthetically very poor, resulting in a linear de-pressed atrophic scar with hypopigmentation from the steroid injections. The Manchester Scar Scale Score at the beginning of treatment was 14, which came down to 13 at the end of steroid injection treatment.
On examination, the patient was healthy and was of normal build and stature. She was classified as having Fitzpatrick Type V skin with average sebum produc-tion. There was a linear scar of about 10 cm over the left half of her face, extending downwards from the zy-gomatic region to end just above the mandibular rim on the left side. The scar was 3 mm in breadth in the upper aspect, gradually increasing to about 5 mm in the lowermost portion. The scar itself was atrophic and hy-popigmented, compared to the surrounding skin, and was depressed at places, being tightly adherent to the
underlying structures. The zone of skin surrounding the scar also had a lesser degree of hypopigmentation. Apart from this linear scar, there were a few acne scars in both her right and left cheeks, but there was no ac-tive acne.
Upon examining the patient, we chalked out a plan of initial subcision of the scar followed by autologous fat transfer and microskin grafting for the hypopigmen-tation, all to be done in the same sitting. Informed con-sent was obtained.
The patient was put under general anesthesia and fat was harvested from the medial aspect of her right thigh, using the standard liposuction 14G cannula on a 60 cc syringe after infiltrating with Klein’s solution. Around 25 cc of fat was harvested. The harvested fat was allowed to separate in layers by sedimentation only for a period of 20 min and centrifugation was avoided. The lower layer, comprising of tumescent fluid admixed with blood, was discarded after separation and the pro-cessed fat was transferred to multiple 2 cc syringes fit-ted with 18 G blunt tip cannulae.
Subcision was next done along the whole length of the scar, using a 3-0 silk thread mounted on a straight needle. Following subcision, the bleeding was con-trolled by manual application of pressure for about 5 min.
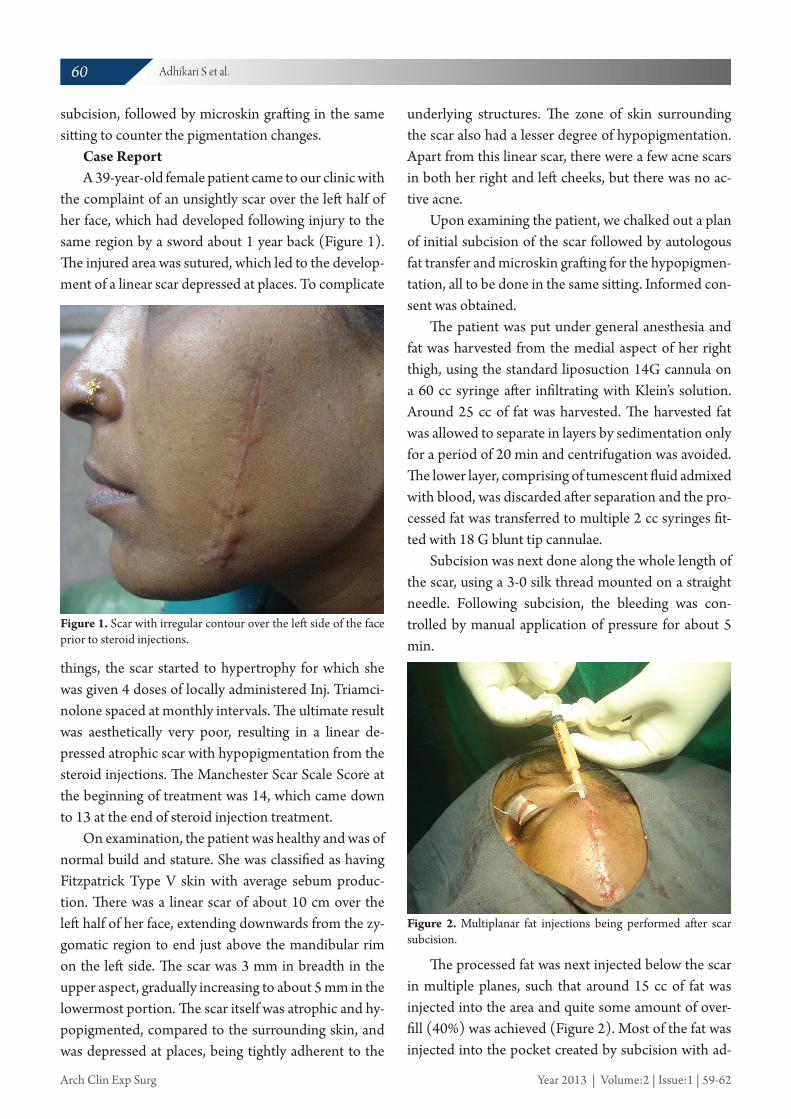
The processed fat was next injected below the scar in multiple planes, such that around 15 cc of fat was injected into the area and quite some amount of over-fill (40%) was achieved (Figure 2). Most of the fat was injected into the pocket created by subcision with ad-
Figure 2. Multiplanar fat injections being performed after scar subcision.
60 Adhikari S et al.
Arch Clin Exp Surg Year 2013 | Volume:2 | Issue:1 | 59-62
ditional fat being injected into the intramuscular and submuscular planes to compensate for the expected postoperative absorption.
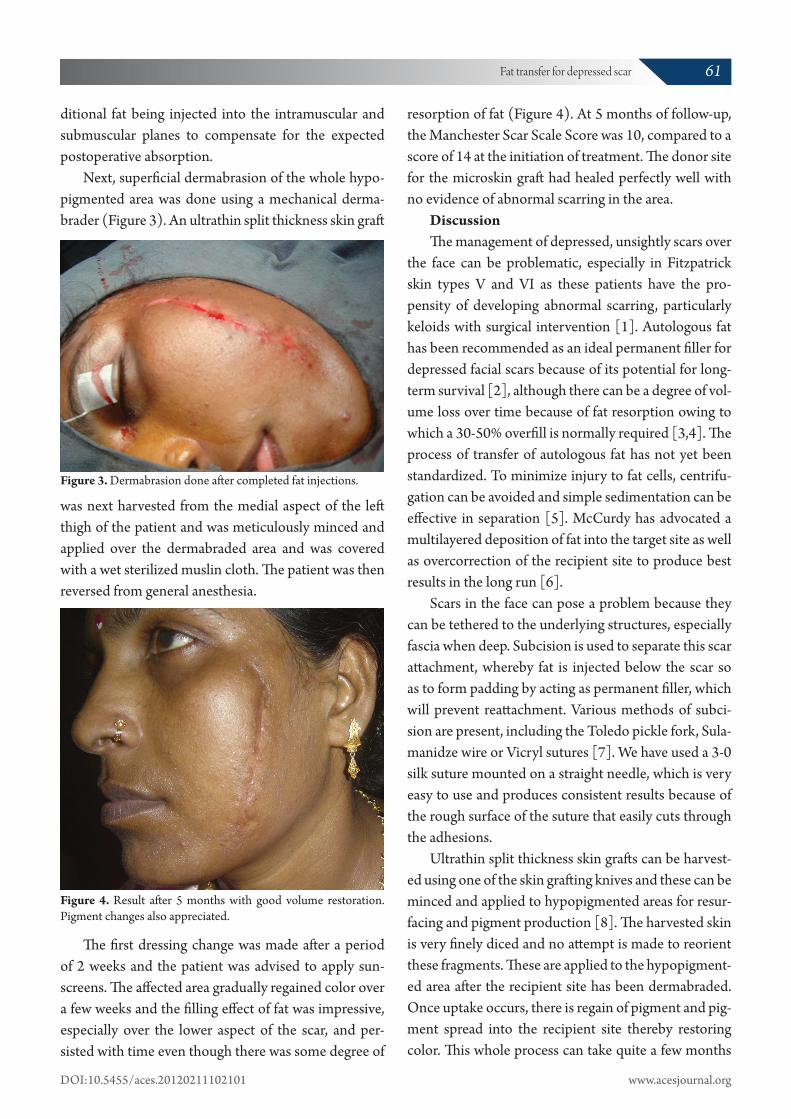
Next, superficial dermabrasion of the whole hypo-pigmented area was done using a mechanical derma-brader (Figure 3). An ultrathin split thickness skin graft
Figure 3. Dermabrasion done after completed fat injections.
was next harvested from the medial aspect of the left thigh of the patient and was meticulously minced and applied over the dermabraded area and was covered with a wet sterilized muslin cloth. The patient was then reversed from general anesthesia.
The first dressing change was made after a period of 2 weeks and the patient was advised to apply sun-screens. The affected area gradually regained color over a few weeks and the filling effect of fat was impressive, especially over the lower aspect of the scar, and per-sisted with time even though there was some degree of
Figure 4. Result after 5 months with good volume restoration. Pigment changes also appreciated.
resorption of fat (Figure 4). At 5 months of follow-up, the Manchester Scar Scale Score was 10, compared to a score of 14 at the initiation of treatment. The donor site for the microskin graft had healed perfectly well with no evidence of abnormal scarring in the area.
DiscussionThe management of depressed, unsightly scars over
the face can be problematic, especially in Fitzpatrick skin types V and VI as these patients have the pro-pensity of developing abnormal scarring, particularly keloids with surgical intervention [1]. Autologous fat has been recommended as an ideal permanent filler for depressed facial scars because of its potential for long-term survival [2], although there can be a degree of vol-ume loss over time because of fat resorption owing to which a 30-50% overfill is normally required [3,4]. The process of transfer of autologous fat has not yet been standardized. To minimize injury to fat cells, centrifu-gation can be avoided and simple sedimentation can be effective in separation [5]. McCurdy has advocated a multilayered deposition of fat into the target site as well as overcorrection of the recipient site to produce best results in the long run [6].
Scars in the face can pose a problem because they can be tethered to the underlying structures, especially fascia when deep. Subcision is used to separate this scar attachment, whereby fat is injected below the scar so as to form padding by acting as permanent filler, which will prevent reattachment. Various methods of subci-sion are present, including the Toledo pickle fork, Sula-manidze wire or Vicryl sutures [7]. We have used a 3-0 silk suture mounted on a straight needle, which is very easy to use and produces consistent results because of the rough surface of the suture that easily cuts through the adhesions.
Ultrathin split thickness skin grafts can be harvest-ed using one of the skin grafting knives and these can be minced and applied to hypopigmented areas for resur-facing and pigment production [8]. The harvested skin is very finely diced and no attempt is made to reorient these fragments. These are applied to the hypopigment-ed area after the recipient site has been dermabraded. Once uptake occurs, there is regain of pigment and pig-ment spread into the recipient site thereby restoring color. This whole process can take quite a few months
61Fat transfer for depressed scar
DOI:10.5455/aces.20120211102101 www.acesjournal.org

in large areas. This is akin to melanocyte transfer to the depigmented areas [9-11]. This procedure has the ad-vantage that abnormal scarring in the donor site can be minimal and usually improves with time [12].
In our patient, the linear depressed and hypopig-mented scar was managed appropriately, using a com-bination of microskin grafting and autologous fat trans-fer following subcision. The pigmentary change was reversed after a few months and the scar remained un-attached to deeper tissues because of the filler effect of the injected fat. The patient satisfaction was immense.
ConclusionAutologous fat transfer is an important weapon in
the armamentarium of the plastic surgeon for manag-ing depressed, unsightly scars anywhere in the body. Combined with microskin grafting, many atrophic and hypopigmented scars can be adequately managed as well. However, the patients need to be followed long term to note if the pigmentation effect or the filling ef-fect is permanent.
GrantNoneConflict of interestsNoneReferences
1. Shockman S, Paghdal KV, Cohen G. Medical and surgical management of keloids: a review. J Drugs Dermatol 2010;9:1249-1257.
2. Coleman SR. Long-term survival of fat transplants: controlled demonstrations. Aesthetic Plast Surg 1995;19:421-425.
3. Asaadi M, Haramis HT. Successful autologous fat injection at 5-year follow-up. Plast Reconstr Surg 1993;91:755-756.
4. Matsudo PK, Toledo LS. Experience of injected fat grafting. Aesthetic Plast Surg 1988;12:35-38.
5. Smith P, Adams WP Jr, Lipschitz AH, Chau B, So-rokin E, Rohrich RJ, et al. Autologous human fat grafting: effect of harvesting and preparation tech-niques on adipocyte graft survival. Plast Reconstr Surg 2006;117:1836-1844.
6. McCurdy JA, Jr. Five years of experience using fat for leg contouring (Commentary). Am J Cosmet Surg 1995;12:228.
7. Sulamanidze MA, Shiffman MA, Sulamanidze GM. Management of Facial Rhytids by Subcutane-ous Soft Tissue Dissection. Int J Cosmet Surg Aes-thetic Dermatol 2000;2:255.
8. Tsukamoto K, Osada A, Kitamura R, Ohkouchi M, Shimada S, Takayama O. Approaches to repigmen-tation of vitiligo skin: new treatment with ultrason-ic abrasion, seed-grafting and psoralen plus ultravi-olet A therapy. Pigment Cell Res 2002;15:331-334.
9. Olsson MJ, Juhlin L. Long-term follow-up of leuco-derma patients treated with transplants of autolo-gous cultured melanocytes, ultrathin epidermal sheets and basal cell layer suspension. Br J Derma-tol 2002;147:893-904.
10. Gauthier Y, Surleve-Bazeille JE. Autologous graft-ing with noncultured melanocytes: a simplified method for treatment of depigmented lesions. J Am Acad Dermatol 1992;26:191-194.
11. Kahn AM, Cohen MJ. Repigmentation in vitiligo patients. Melanocyte transfer via ultra-thin grafts. Dermatol Surg 1998;24:365-367.
12. Gupta DK. Microskin Grafting for Vitiligo. Spring-er, London, UK, 2009;122.
© GESDAVThis is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted, non-commercial use,
distribution and reproduction in any medium, provided the work is properly cited.
62 Adhikari S et al.
Arch Clin Exp Surg Year 2013 | Volume:2 | Issue:1 | 59-62

![System Specifications for Standard Boot Firmware ... size sector Smaller size sector 64 bytes 64 bytes 64 bytes Data flash User area [ max 64 KB] flash 0 [ max 64 KB] (64 bytes x 1024)](https://img.pdfslide.us/doc/110x75/5aab4f497f8b9a2e088ba56b/system-specifications-for-standard-boot-firmware-size-sector-smaller-size-sector.jpg)



























