Embed Size (px)
Citation preview

813Neurology India | Nov-Dec 2009 | Vol 57 | Issue 6
Letters to Editor
T1 relaxation time sufficient to produce pallidal T1 hyperintensity in hepatolenticular degeneration. [4] Manganese is also used as MR contrast due to the above properties but surprisingly SWI failed to show any blooming. Interestingly, calcification containing diamagnetic calcium is visualized in SWI and hence is used in the seizure MR imaging protocol.[5] The magnetic susceptibility of paramagnetic manganese is much higher than diamagnetic calcium.[6] The association of manganese deposition and T1 hyperintensity is well known but the causation is not well established.
In view of normal SWI many questions remain unanswered. Are there local tissue factors affecting the paramagnetic properties of accumulated manganese in basal ganglia? Is manganese accumulation just an inciting event and the observed T1 hyperintensity due to some other cause? In cases with hepatolenticular degeneration, microscopic examination of the pallidum shows Alzheimer type II astrocytes without any calcification, melanin deposition or hemorrhage to account for the T1 hyperintensity.[1] Primate and human studies have shown that astrocytic accumulation of manganese increases glutamate/glutamine with simultaneous decrease in myo-inositol, inducing selective neuronal loss in the basal ganglia structures and reactive gliosis (Alzheimer type II astrocytes).[2,3] The T1 hyperintensity may be due to the intracellular macromolecule accumulation due to energy failure or could result from the protein hydration layer inside the cytoplasm of astrocytes.[2,7] Further studies delving into these issues are needed to understand the pathological mechanisms underlying T1 hyperintensity in acquired hepatolenticular degeneration.
Neeraj N. Baheti, Haseeb Hassan, Chaturbhuj Rathore, Syam Krishnan,
Chandrasekharan Kesavadas1
Departments of Neurology and 1Imaging Sciences and Interventional Radiology, Sree Chitra Tirunal Institute for Medical Sciences and
Technology, Thiruvananthapuram - 695 011, India. E-mail: [email protected]
PMID: *** DOI: 10.4103/0028-3886.59489
References
1. Klos KJ, Ahlskog JE, Kumar N, Cambern S, Butz J, Burritt M, et al. Brain metal concentrations in chronic liver failure patients with pallidal T1 MRI hyperintensity. Neurology 2006;67;1984-9.
2. Rovira A, Alonso J, Cordoba J. MR imaging findings in hepatic encephalopathy. Am J Neuroradiol 2008;29:1612-21.
3. Newland MC, Ceckler TL, Kordower JH, Weiss B. Visualizing manganese in the primate basal ganglia with magnetic resonance imaging. Exp Neurol 1989;106:251-8.
4. Uchino A, Noguchi T, Nomiyama K, Takase Y, Nakazono T, Nojiri J, et al. Manganese accumulation in brain: MR imaging. Neuroradiology 2007,49:715-20.
5. Saini J, Kesavadas C, Thomas B, Kapilamoorthy TR, Gupta AK, Radhakrishnan A, et al. Susceptibility weighted imaging in the diagnostic evaluation of patients with intractable epilepsy. Epilepsia 2009;50:1462-73.
6. Foese G, Gorter CJ, Smits LJ. Constantes Selectionnees Diamagnetisme, Paramagnetisme, Relaxation Paramagnetique. Masson, Paris: 1957.
7. Abe K, Hasegawa H, Kobayashi Y, Fujimura H, Yorifuji S, Bitoh S. A gemistocytic astrocytoma demonstrated high intensity on MR images: Protein hydration layer. Neuroradiology 1990;32:166-7.
Accepted on 23-10-2009
Incontinentia pigmenti with sensorimotor polyneuropathy: A novel associationSir,We report a patient with Incontinentia Pigmenti (IP) and peripheral neuropathy, an association not reported earlier.
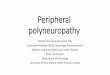
A 16-year-old girl presented with 3½ years history of dragging of left foot and inability to grip slippers, and 2½ years history of weakness of hands followed by proximal weakness of lower limbs and numbness of hands and feet. She had pigmentation of left half of body since birth, global developmental delay and a congenital dermoid cyst of the scalp removed at 1½ years of age. On examination, there was left hemiatrophy and hyperpigmentation along the lines of Blaschko over the left upper limb, trunk and lower limb, some showing a Chinese check-board pattern consistent with the diagnosis of IP[1] [Figure 1]. She had mild mental retardation and pigmentary retinopathy. There was bilateral pes cavus, hammer toes, flexion contractures of fingers at proximal interphalangeal joint, wasting of small muscles of hands, spasticity of lower limbs and moderate distal weakness of upper and lower limbs. There was a 25% reduction of pain and touch sensations in the upper limbs distal to mid-forearm, and lower limbs distal to the knees, impaired position sense in all limbs and vibration over toes, areflexia and flexor plantars bilaterally. Her stance was wide-based with high steppage, ataxic gait. Systemic examination was normal.
Nerve conduction studies showed unrecordable median, ulnar and sural sensory nerve action potentials, with prolonged latencies and reduced amplitudes of the common peroneal and posterior tibial compound motor action potentials. Magnetic resonance imaging (MRI) of brain showed a parenchymal cyst in the left hippocampus. Histopathological evaluation

814 Neurology India | Nov-Dec 2009 | Vol 57 | Issue 6
Letters to Editor
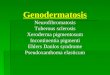
of sural nerve showed chronic uniform axonopathy (predominantly large fiber) with mild regenerative activity [Figure 2]. These features were consistent with hereditary neuropathy of axonal type. She was not exposed to toxins, not diabetic, had normal liver and renal functions, normal hemogram, ESR of 40 mm/h, negative RA factor, LE cell and ANA, and no systemic symptoms to suggest any acquired cause of neuropathy.
The neuroectodermal manifestation of IP involves the skin, hair, teeth, nails, eyes and the central nervous
system.[2,3] Early mental subnormality, spasticity, hemiatrophy, cystic lesion in hippocampus and pigmentary retinopathy were the central nervous system anomalies in our patient. Peripheral nervous system abnormalities have not been reported in IP. Peripheral nerves are derivatives of the neuroectodermal placode while the perineurium develops from the mesoderm.[4] Hence, the association of peripheral neuropathy in our patient with IP can be explained by the hypothesis of common embryological origin from the neuroectoderm. The presence of a later onset of polyneuropathy in adolescence is also unusual considering that most
Figure 1: (a-c) Hyperpigmentation along the lines of Blaschko over the left leg, hand and trunk, some showing a Chinese check-board pattern, (d) Hammer toes, early pes cavus and pigmentation of the left foot
Figure 2: Histopathology of left sural nerve shows: (a) Features of chronic uniform axonopathy with mild regenerative activity (H and E stain, 350),(b) Higher magnification reveals predominant loss of large myelinated fiber with occasional regenerating cluster (K-pal stain for myelin, 3320),
(c) Neurofilament immunostaining for axons highlights the depletion of large diameter axons. Regenerative axonal sprouting is visible as clusters of dot like brown staining of the smaller diameter axons (Neurofilament Immunohistochemistry, 3320)

815Neurology India | Nov-Dec 2009 | Vol 57 | Issue 6
Letters to Editor
symptoms manifest in early childhood. Though IP is a relatively non-progressive disorder, this late presentation may either suggest a later detection only after significant weakness has set in or a more progressive course of IP.
Sanju P. Joy, Samhita Panda, Girish B. Kulkarni, Pramod Kumar Pal, Yasha T. Chickabasaviah1,
Rajani R. Battu2
Departments of Neurology, 1Neuropathology, National Institute of Mental Health and Neurosciences, 2Vitreoretinal Services, Narayana
Netralaya, Bangalore, India.E-mail: [email protected]
PMID: *** DOI: 10.4103/0028-3886.59490
References
1. Landy SJ, Donnai D. Incontinentia pigmenti (Bloch-Sulzberger syndrome). J Med Genet 1993;30:53-9.
2. Pinheiro A, Mathew MC, Thomas M, Jacob M, Srivastava VM, Cherian R, et al. The clinical profile of children in India with pigmentary anomalies along the lines of Blaschko and central nervous system manifestations. Pediatr Dermatol 2007;24:11-7.
3. Hadj-Rabia S, Froidevaux D, Bodak N, Hamel-Teillac D, Smahi A, Touil Y, et al. Clinical study of 40 cases of incontinentia pigmenti Arch Dermatol 2003;139:1163-70.
4. Halata Z, Grim M, Christ B. Origin of spinal cord meninges, sheaths of peripheral nerves, and cutaneous receptors including Merkel cells. An experimental and ultrastructural study with avian chimeras Anat Embryol (Berl) 1990;182:529-37.
Accepted on 09-10-2009
Intracerebral hemorrhages in Vogt-Koyanagi-Harada diseaseSir,Vogt -Koyanagi -Harada (VKH) d isease i s a multisystem disorder characterized by granulomatous panuveitis with exudative retinal detachments often associated with neurologic, acoustic and cutaneous manifestations. [1] The neurological features of VKH disease include headache, meningismus, cranial nerve palsies, hemiparesis, transverse myelitis and ciliary ganglionitis. [1] Intracerebral hemorrhage has not been described earlier. We describe a male patient with VKH disease who presented with ataxia secondary to intracerebral hemorrhage.
A 26-year-old gentleman presented with acute onset headache, vomiting, imbalance while walking and incoordination of the upper limbs. There was no history of weakness, sensory impairment or any cranial nerve deficit. He gave a history of recurrent nontraumatic
uveitis involving the right eye for the last 2 years. His first evaluation 2 weeks into the illness showed reduced visual acuity (20/200) in the right eye, the left eye being normal (20/20). The anterior chamber showed flare with hazy media. Evaluation for sarcoid, tuberculosis, syphilis and vasculitis was negative. He was initiated on steroids, with total improvement over 4 weeks. He later discontinued steroids due to weight gain. One month after stopping steroids, he developed redness of the same eye with visual deterioration. Evaluation showed exudative retinal detachment. Eventually, he developed complicated cataract and prepthisical changes. He also had two episodes of low-grade fever with headache and terminal neck stiffness without altered sensorium or focal deficits and was treated symptomatically. Examination at the present admission revealed patches of vitiligo on his back. Visual acuity was 20/20 in the left eye and no perception of light in the right eye. Ophthalmic evaluation showed phthisis bulbi and complicated cataract in the right eye [Figure 1]. The left eye showed optic disc edema, tortuous veins and choroidal folds [Figure 2]. Neurological examination showed gaze-
Figure 1: Complicated cataract in the right eye
Figure 2: Fundus picture of the left eye showing optic disc edema with choroidal folds and tortuous veins