Embed Size (px)
Citation preview

InsIde The Global ReGulaToRy dIaloGue™InsIde The Global ReGulaToRy dIaloGue™
A GLOBALLY COORDINATED RESPONSE TO THE DRUG SUPPLY CHAIN PROBLEMS is being called for, as the realization takes hold among the various stakeholders that the only effective and affordable option is a unified effort. The call for collab-orative action to better assure pharmaceutical ingredient qual-ity and supply chain integrity has been forcefully sounded at recent regulator/industry conferences, and momentum for an international consortium is rapidly building. In the wake of the emerging health threats, standard-setting, pharmaceutical and supplier organizations are joining regulatory agencies in the global outreach effort and new cooperative alliances are being forged. Concerned regulators are evaluating more closely how well drug manufacturer quality systems cover the ingredient supply chain, while companies are analyzing where the QA gaps lie and taking action to fill them. USP initiatives on heavy metals and residual solvents highlight the challenges of devel-oping and implementing global standards.
A deeper understanding of the true cost of quality is among the factors driving industry to combine resources with regu-lators and other stakeholders in the search for better control over a global pharmaceutical supply chain.
As in the international financial context, the scope of the supply chain problems is heightening the recognition among the various stakeholders that the only effective and afford-able option is a unified effort.
New unforeseen alliances are being forged to develop, implement and enforce harmonized standards and solu-tions. Governmental health. customs, law enforcement and commerce agencies, international health organizations and standard setting bodies, pharmaceutical and supplier asso-ciations, individual companies and their various subsidiar-ies and departments, are all looking for new cooperative mechanisms to rationalize their efforts and maximize their resources.
Contents
2 A Call To Action
5 ICH’s Role, Q7B On Excipient GMPs Debated
6 Supply Chain Problem Clearinghouse?
9 Be Realistic About Cost Of Quality
10 Heparin Situation Prompts Amgen CAPA
14 Shift Happens In The Supply Chain
15 Registration/Pedigree Systems Improving
16 Audit Suppliers But Respect Relationship
18 IPEC, FDA Adding to Excipient Guidance
18 DMF Fees, Approval System Proposed
19 Stakeholders Extend Global Reach
24 India And China Draw Regulator Attention
26 Inspection-Sharing Pilots Launched
32 Global Harmonization Vision Needed
35 USP’s Horizon Is Expanding
37 Heavy Metals Present Hard Issues
39 Implementation Of Concern For Solvents
VoICes FRoM tHe DIALoGUe: • CDER compliance staffer Friedman on supply chain vulnerabilities (pp. 7–8) • Amgen’s CAPA response to heparin situation (pp. 11–13) • FDA official Bernstein on U.S. & WHO anti-counterfeiting efforts (pp. 21–23) • Parexel consultant Smith comparing FDA and EMEA inspections (pp. 30–32) • CDER’s Woodcock on industry/regulator roles and global harmonization (pp. 33–35)
BILL PAULSON, EDITOR-IN-CHIEf
NOvEMBER/DECEMBER 2008 | vOl. 2, NO. 6 |
InTeRnaTIonalPhaRmaceuTIcal
QualITy™
WWW.IPQPUBS.COM

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
In turn, the lesson has hit home that preventing crises is less costly than reacting to them and that quality cost modeling needs to reflect this truth.
The new regulatory emphasis on the responsibility of execu-tive management for a company’s quality system is among the pressures prompting more management attention to the cost implications of upfront quality assurance. An increasing commitment to a preventative, unified approach to manag-ing the supply chain risks is likely to follow.
The transition to a more quality-by-design based regulatory paradigm, with its potential for clearing the path to prod-uct approval and post-approval manufacturing flexibility and efficiency, is also intensifying the concern with assuring the quality of pharmaceutical ingredients through their raw material sourcing, manufacturing and distribution phases.
A Call to Action
The call to cooperative action was a keynote struck by both industry and regulators at the Pharmaceutical Ingredient Supply Chain Conference cosponsored by FDA and the Parenteral Drug Association (PDA) in September in Washington, D.C.
The call was echoed at a follow-up workshop the next week sponsored by the International Pharmaceutical Excipients Council (IPEC), which focused more specifically on the excip-ient component of the supply chain control challenge.
The PDA/FDA conference included representatives from U.S. and international regulatory bodies, industry, active pharma-ceutical ingredient (API) and excipient manufacturers and distributors, and pharmaceutical trade associations. Under discussion were: • the challenges of ensuring supply chain integrity • relevant regulations and guidances on good man-ufacturing and distribution practices (GMPs/GDPs) • the role of quality systems in supply chain operations • industry practices in the various sectors involved, and • opportunities for global cooperation and harmonization.
In the wake of the traction gained at the Washington confer-ence, the PDA/FDA planning committee made the decision to hold additional meetings to help drive forward the global supply chain effort. A follow-up conference, which included a similar cross-section of speakers and issues, was held in San Diego, California Dec. 3–5. A conference is also planned for Europe in March, and for June in China in conjunction with the Shanghai FDA.
IPEC followed up on its September conference with a European meeting on excipient GMPs held in Munich Germany on December 1–2.
FDA Center for Drug Evaluation and Research (CDER) Compliance Office staffer Edwin Rivera, who co-chaired the September PDA/FDA conference, was among those calling for the launching of a coordinated effort on a global scale.
The Division of Manufacturing and Product Quality (DMPQ) Manufacturing Assessment and Pre-approval Compliance Branch Chief played a key role in the development of ICH’s API GMP guideline Q7A and heads up FDA’s Pharmaceutical Ingredient Safety Task Force (IPQ Jan./Feb. 2008).
Rivera highlighted the “bold vision” of the planners to hold a conference that would “set the stage for the development of global initiatives to ensure the integrity of the pharmaceuti-cal ingredient supply chain.” He drew an analogy to the piv-otal meeting held in Canberra, Australia in 1996 that placed regulators and industry on a path to a globally harmonized approach to GMPs for APIs.
“For the past two and half days,” Rivera stated in his sum-mary remarks, “each of you has had the opportunity to reflect on the past to see where we have been and how we got here. You have learned about the numerous tragic events in past years implicating the pharmaceutical ingredient supply chain that have resulted in hundreds of unnecessary deaths. You have seen the impact of continuing globalization of the pharmaceutical industry and how this has contributed to an increase in counterfeit and substandard medicines. You have learned that many of these events have been attributed to substandard GMP practices or intentional adulteration of ingredients for economic gain. And of course, we have repeat-edly emphasized the need for cooperation and coordination among all stakeholders, including U.S. Customs, FDA, law enforcement agencies, and industry, to effect meaningful and lasting solutions.”
The question before us now, the FDA compliance offi-cial told the departing meeting participants, is “where will we choose to go in the future?”
At the 1996 Canberra meeting, he stressed, “more than 150 officials from world regulatory bodies and the pharmaceu-tical industry put aside their individual opinions, refrained from continuing to make excuses for their inaction, and came together for an important common cause that eventually led to the development of ICH Q7A. Are we prepared and willing to do the same today to address and resolve current problems
2 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
with the pharmaceutical ingredient supply chain? Or will we continue to ignore the risks in the supply chain, or conclude that counterfeiting or intentional substitution of active phar-maceutical ingredients or excipients cannot happen in our organizations? Will we continue to blame others for the prob-lems in the supply chain and not collaborate with federal and state authorities to address and resolve these problems?”
To counter the current threat facing us today, he concluded, “we too must come together and collectively develop a plan to stop unscrupulous or criminal elements from achieving their goals before they cause additional deaths and threaten the very core and integrity of the pharmaceutical industry.”
He urged the conference participants to take this call to action back to their respective organizations: “When asked about the problems with the pharmaceutical ingredient supply chain and what should be done about it, I hope your response will be: ‘It is time to act! Let’s roll!’”
Rivera’s co-chair for the PDA/FDA supply chain con-ference, Janeen Skutnik in her closing remarks cited the intensity at the conference as evidence that a threshold has been crossed where a coordinated global effort is now possible. Skutnik is quality and regula-tory policy director for Pfizer and is the chair-elect for IPEC-Americas.
“I don’t think I have ever been part of a pharmaceutical meet-ing that has drawn on so much emotion. And what I want to ask each of you is to take that back with you today,” Skutnik said. “The time is now. We can’t think about this any longer. We absolutely need a holistic integrative global approach to this challenge.”
Noting that “we have a tremendous opportunity to turn the image of this industry around with this issue,” she asserted that the response to the supply chain challenges needs to involve all stakeholders. In order to address these challenges, “we need to engage not just regulators, not just ourselves as pharmaceutical manufacturers, excipient manufacturers, dis-tributors. We need to engage patients. We need to engage nursing organizations, physician organizations. We need to go across departments, countries and governments.”
Clearly emerging from the conference discussions was “the need for increased transparency, trust and collaboration across all of this,” Skutnik stated. Citing the initiatives under-way in Congress and Health and Human Services (HHS) (IPQ May/June 2008), she stressed that “we have the oppor-tunity presented to us now to develop industry-based con-sensus standards…. If we don’t take it, we are going to end up in a far worse situation than we are today, and potentially with things that actually aren’t going to meet our ultimate goal of protecting patients.”
The Pfizer official emphasized the timeliness of her carpe diem plea. “Many of us were thinking about and trying to drive change five, ten years ago on some of these topics, but people weren’t ready to listen. People are ready to listen now, so we need to take action.”
She maintained further that action is really the path of least resistance. “It is a whole lot harder to justify what you did wrong,” she advised, adding that the pharmaceutical indus-try will also be held responsible for what it does not do.
“Let’s use the strength, size, and global reach of our entire industry to the benefit of patients,” the Pfizer official urged. Resources are being leveraged within companies, but “we need to be far more creative and innovative” in leveraging resources across the industry.
Skutnik cited the example of third-party auditing. “We have heard countless times in the last few months about the use of third-party auditing, third-party certification. It is in vari-ous bill proposals. It is something we need to do to protect patients. We need to get beyond ‘only I can do it best.’”
Industry should also be encouraging HHS and FDA to influ-ence other governments to adopt risk-based approaches and to use resources better, she said.
The conference co-chair further pointed to the need for learn-ing from other industries, where solutions may have already been developed and tested. Finally, she urged, “take advan-tage of the advances in technology, and spread the message and action globally.”
In introductory remarks at the IPEC conference the next week, which she also cochaired, Skutnik repeated her clarion call, proposing that a global summit be held, “preferably in 2009,” to foster a coordinated and har-monized excipient regulatory approach.
The summit would bring together organizations and gov-ernments worldwide “to talk about global GMPs, distribu-tion practices, supplier qualification, auditing, inspections, third-party certification, supply chain integrity, and qual-ity systems.” The “holistic approach” should include those involved in corporate security, sales and marketing and pro-curement, she said.
The summit would not mirror or compete with the formal tripartite ICH process, she explained, but would need to include countries from other regions in the world, such as
NOVEMBER/DECEMBER 2008 3

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
China, India and Brazil, which are producing excipients and/or involved in developing regulatory approaches. WHO, with its global reach, should be actively involved, Skutnik maintained.
She stressed IPEC’s role in helping to assure global science- and risk-based approaches to excipient issues that “add value and at the end of the day protect patients.” Region-specific approaches, she cautioned, “are extremely problematic, not just for excipient manufacturers, but for excipient users—it can be almost impossible to comply with multiple regula-tions in various regions.”
In his opening remarks at the IPEC conference, IPEC’s current chairman David Schoneker (Colorcon Global Regulatory Affairs Director) echoed Skutnik in view-ing the intensity of the PDA/FDA supply chain confer-ence as an indicator that “industry is ready for a change.”
“I don’t think I have ever been at a conference like the last three days in Washington,” Schoneker said, pointing to a “tremendous amount of excitement in the room, emotion in the room.” Industry, he affirmed, “has finally woken up and realized that the only way forward is to work together and stop working independently as individual companies…and find a way to stop some of the problems that are out there. That realization really came to bear at the end of the meeting on Friday [and] truly, I think there is a new horizon for all of us when it comes to control of supply situations.”
Adding to the emotion at the PDA/FDA conference was the breaking news of findings in Chinese infant formula and other milk products of melamine adulteration. The latest in the series of health threats arising from contamination in Chinese manufactured products underscored the immediacy of the issues before the conference. Melamine was the culprit in China-sourced dog food adulteration that killed numerous pets in the U.S. last year.
The infant formula adulteration has resulted in tens of thou-sands of serious adverse reactions among babies in China, including 13,000 hospitalizations and a handful of confirmed deaths. FDA launched domestic investigations and sampling efforts in cooperation with other U.S. agencies out of concern that unapproved baby formula and other powdered milk-based products contaminated with melamine would find their way into local Asian markets in the U.S.
The call to arms was sounded repeatedly during the concluding panel session at the PDA/FDA conference, which addressed future pathways the global supply chain effort could take. Summary remarks by the pan-
elists were followed by a discussion of the key con-cerns and proposals emerging from the conference presentations.
Setting the stage at the panel session was a presentation by Amgen Quality VP Martin Van Trieste, which encapsulated the conference themes. The other members of the panel were: Hospira Strategic Sourcing Director Kim Cauchy; FDA officials Richard Friedman (director of DMPQ) and Michael Levy (director of CDER’s New Drugs and Labeling Compliance Division); Generic Pharmaceutical Association (GPhA) Regulatory Sciences VP Gordon Johnston; and IPEC Chairman Schoneker.
Van Trieste defined the broad goal as creating “a global qual-ity and regulatory system that assures patient safety by guar-anteeing product quality and authenticity throughout the supply chain.”
The focus should be “how can we do that on a global basis,” he said. Citing pedigree standards as an example, he maintained that “the last thing I want is to try to have to follow” for the same product is “50 state regulations on E-pedigree, and a European RFID, and a Japanese requirement…. I just can’t do it. So we have to work really hard with the regulatory bodies around the world and try to make this a global system.”
Neil Wilkinson, who served as global quality senior direc-tor at AstraZeneca prior to joining the consulting firm David Begg Associates in mid-2008, urged the need to respond to the immediacy of the problem through a coordinated effort that transcends the various interested organizations. Wilkinson has been actively involved through the European Federation of Pharmaceutical Industry Associations (EFPIA) on ICH and other European and global harmonization efforts, and repre-sented EFPIA on the Q10 expert working group.
Citing the number of individual member and trade associa-tions at the table, including PDA, ISPE, PhRMA, EFPIA, IPEC and APIC, Wilkinson maintained that in the past, “whenever a new initiative has come along, we have all gone off in our own different ways” duplicating activities around these dif-ferent organizations. “So my challenge to you on the panel, who represent a large number of the organizations I have mentioned, is how can we bring this together under one rec-ognized work stream that actually takes this forward” and develop a strategy “to engage all these different organiza-tions in an effective task force?”
Van Trieste called for the launching of a consortium that would bring these organizations together to respond to the “very serious crisis.”
4 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
Momentum for the consortium has been building since the PDA/FDA September conference, and an ini-tial launch is being targeted in February. van Trieste, who is helping spearhead the effort, is asking inter-ested parties to contact him at: [email protected].
Friedman commented that the agency called a public hearing on the section 314.70 manufacturing change regulations last year that could serve as a reference point.
ICH’s Role, Q7B on excipient GMPs Debated
The debate on the merits of using ICH as the forum for har-monizing supply chain quality regulatory standards, and excipient GMPs in particular, continued at the PDA/FDA and IPEC conferences. The success of ICH Q7A in setting a de facto global standard for API GMPs makes a compelling argument for adding a Q7B guideline on excipient GMPs to the ICH portfolio (IPQ Jan./Feb. 2008).
It was noted at the September conferences that with its regula-tor imprimatur, an ICH excipient GMP guideline would pre-empt the mushrooming of different approaches that would then require more effort to harmonize later.
On the other hand, participants pointed out that formal involvement in the ICH process has been limited to the regula-tors and innovator associations in the U.S., Europe and Japan, and that the supply chain oversight effort to be effective must reach into the developing world from where pharmaceuticals and their ingredients are increasingly being sourced.
At the PDA/FDA panel session, IPEC chairman Schoneker espoused the benefit of an ICH approach to developing harmonized excipient GMPs in light of the success of the API Q7A effort in providing a world-wide “base standard for APIs.” He pointed out that the timing may now be right for the project.
The idea when it was originally proposed, “went by the way-side” in the view that excipients were not worth “spend-ing the time on.” That view, however, he said, has changed with the impact of the supply chain problems as well as the increasing emphasis on ingredient understanding and con-trol in the evolving quality-by-design paradigm. Schoneker maintained that with the IPEC documents that have already been harmonized around the world as a basis, Q7B could be developed without “an awful lot of work being done.” Evolving the IPEC excipient GMP guide and the USP chapter incorporating it (<1078>) into an ICH document
would prompt governments and stakeholders around the world to start using it as the accepted excipient standard, as has been the case for Q7A, he maintained.
Conference co-chair Rivera commented that the current situ-ation for excipients, for which official regulations and guid-ance have not yet been established, is similar to that when the Q7A project was launched – an easier situation to deal with than harmonization ex post-facto.
Friedman recognized that ICH could be an appropriate venue in the excipient GMP context if the working group had the appropriate composition and practical orientation. However, he asserted that supply chain issues like supplier qualification would be better addressed through the more broad-based, intergovernmental Pharmaceutical Inspection Cooperation Scheme (PIC/S).
Rivera pointed to the issue as “something that the agency will have to take back and discuss internally in the center and with top agency management and decide as an agency in general what would be the best forum to move forward on many of these recommendations.”
While established as a three-region harmonization vehicle, ICH has been expanding its efforts to draw other regions and other industry sectors into the ICH harmonization process to increase its global relevancy and reach.
In turn, the interest of non-ICH countries in implementing ICH guidelines and the common technical document as a standard submission format has been growing.
In addition to the active participation in the process of groups with formal “observer” status including the World Health Organization (WHO), Canada and the European Free Trade Association (EFTA), ICH has a “Global Cooperation Group” (GCG) that provides an interface with other regional harmo-nization initiatives around the world on adopting the ICH documents.
At the ICH meeting in Portland in June, a “Regulators Forum” was established to complement the activities of the Global Cooperation Group. The forum brings the ICH regulatory authorities together with other regulators worldwide to pro-mote discussion and best practices relating to implementing the ICH guidelines and their impact on regulatory systems. Unlike the GCG, industry is not included in the forum.
NOVEMBER/DECEMBER 2008 5

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
At an October 21 “ICH regional public meeting” hosted by FDA and PhRMA in Rockville, MD, CDER International Programs Associate Director Justina Molzon highlighted ICH’s increasing global impact.
The regional public meetings are being held prior to ICH meetings to provide a forum for communication with and input from interested parties outside the ICH structure. The October Rockville meeting preceded the ICH meeting in Brussels on November 10–13.
Molzon, who has been involved with the ICH process since 1993, sees a significant “shifting of gravity” in the ICH pro-cess toward the global dimension, spurred by the acceptance of the common technical document as a regulatory lingua franca.
She explained at the October meeting that “initially, all the efforts of ICH were focused on the development of consis-tent, harmonized guidelines. Those building blocks were then assembled in a common submission format and we had a common technical document. We are now really focused on how to use the CTD in our review process.”
The move to an electronic CTD spurred the development of standard reviewer templates and the refining of good review practices. “Our focus on implementation is why so many regulators from other countries are coming to us and asking us how we do good review practices,” Molzon said. The CTD has become a “common regulatory language across all countries,” allowing for better “understanding of how one another’s process works” and spurring interaction between regulatory authorities.
More broadly, ICH is being impacted by the rapid change in “the geographical face of international drug development and trade,” Molzon stressed. “Before 1990, the U.S., Europe and Japan were where most of the R&D is taking place. That is not necessarily the case today. Interest and use of ICH guidelines by these countries reflects this change.”
ICH, the FDA representative stressed, “is committed to responding to the needs of regions and countries interested in implementing ICH guidelines. That is why you have seen so many new mechanisms developed to include non-ICH countries.”
Progress on the quality guideline series continued at the November ICH meeting in Brussels.
The annex to the ICH Q8 pharmaceutical development guideline reached final form (Step 4) for release in the three
regions. “Q8R” builds on the key concepts in the core guide-line, exploring further the evolving concepts of quality by design and their regulatory import and use.
The ICH Q8-10 Implementation Working Group (IWG), which was launched at ICH’s Portland meeting in June (IPQ July/Aug. 2008), continued working on a Q&A document to answer questions arising from the new Q8-10 guidelines. The Q11 Expert Working Group (EWG) focusing on the develop-ment and manufacture of drug substances also had its second get together at the Brussels meeting.
The ICH Q4B EWG addressing the interchangeability of pharmacopeial texts also pushed forward several initia-tives. Clearing Step 4 were three Q4B annexes addressing non-sterile microbiological testing. These “general chapters” address “Microbial Enumeration Tests” (Annex 4A), “Tests for Specified Microorganisms” (Annex 4B), and “Acceptance Criteria for Pharmaceutical Preparations and Substances for Pharmaceutical Use” (Annex 4C), respectively.
supply Chain Problem Clearinghouse?
The PDA/FDA conference panel session addressed dimen-sions of supply chain control other than excipient GMPs where harmonized standards and a unified approach would be beneficial.
Referencing a product tampering incident in which he was involved, one participant suggested that a task force be set up “to look at this whole matter of tamper-evident seals as it is applied both to APIs and excipients.” The two product types have different issues involved, he noted, “but I think there is a major gap in what we do and I think we can improve upon it.”
A clearinghouse where problems in the supply chain uncov-ered by particular companies would be available for general benefit was another focus of attention during the panel dia-logue. The clearinghouse idea has received attention at other industry/regulator forums as companies realize their limita-tions in trying to find and address the problems on an indi-vidual basis (IPQ Jan./Feb. 2008).
It was pointed out that setting specifications is not necessarily going to address criminal activity. “We can keep working on the regulations and we can keep working on the right com-mittees,” but a process for sharing each other’s knowledge on a suspect supplier or product gained through NMR or other means would be very beneficial, a participant affirmed.
6 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
CDER’s Friedman commented that one of the prob-lems that purchasers may not be aware of is the use of “show factories” and “shadow factories” in developing countries such as China.
“The show factories are nice and shiny” with the latest equip-ment, trained employees and good management, “and you walk in and that is the one you audit.” However, the facility may be subcontracting out all or part of the actual production to a very different type of shop in a rural area, where costs are much less due to the lesser standards in place.
With the knowledge that such subcontracting arrangements “are happening,” he cautioned that “if you are entering in any contracts, make sure that you require them to tell you if they are going to subcontract any part of the operation out… so that you have the option to go in and audit them if you would like.”
The previous commentor responded that this concern speaks to the need for an information-sharing mechanism so that firms don’t have to rediscover the same problem. “If we are really trying to think globally together, how can we help each other discover that shack vs. the upfront facility? I know there are legal issues. But again, if we are at a crisis, let’s think a bit differently here.”
Amgen’s Van Trieste agreed, suggesting that the legisla-tion being developed by Congressman John Dingell (IPQ
May/June 2008) could help address the legal hurdles by including a requirement to report such supply chain problems to a clearinghouse for wider dissemination. He urged participants to contact their legislative affairs departments so that the legislation can be steered in the most effective direction.
CDeR CoMPLIAnCe oFFICIAL FRIeDMAn on InDUstRY sUPPLY CHAIn VULneRABILItIes
At the PDA/FDA supply chain conference, CDER Compliance Office Division of Manufacturing and Product Quality Director Richard Friedman identified the following as vulnerabilities in the traditional quality system regarding sourcing. Friedman did not enumerate on the lack of traceability since the issue and FDA efforts to respond to it were discussed by other FDA officials at the conference (see box on pp. 21–23).
• Lackoftraceability
• Highcomplexityduetoincreasedbrokerageandtradeactivity:As your supply chain gets more complex, there are more players that you have to monitor and more business partners that you have to be sure are ethical and are going to do what needs to be done in terms of caretaking of a drug. A lot of these are redundant or unnecessary parts of the supply chain that don’t serve a social good and don’t serve a business good either. Often GMP is GBP – good business practice.
Understand that of course a company may not want to do its distribution, because they may not have a sales staff, etc. But if they use a distributor, there doesn’t need to be three or four or five shippers and distributors after that, does there? You are paying for every shipment – every truck that goes on the road, ship on the sea – that goes on after that. If you think about the future, the future actu-ally could be savings from a business point of view and certainly from a quality point of view. Your pedigrees would be a lot shorter, and with more of a direct-line kind of concept, obviously you will save money. So what is the business incentive for these middle men that don’t add any value perhaps? To protect their enterprise, the COA is often altered to remove the true identity of the manufacturer, and that is unacceptable.
• Theingredientmayberepackagedorrelabeledmultipletimes:In the process of repackaging, there could be contamination. Or it might be susceptible to moisture degradation, and now [the container] has been opened for a while and you have more moisture in the product because it is hygroscopic. And then that new risk gets transferred to the dosage form manufacturer who has to deal with it and didn’t know that certain drums were left open for a lot longer than others. And [the product] may be relabeled multiple times. If the original manufacturer’s label isn’t on there any more, there is a problem there. You must know who the maker of your ingredient is. That gets clearer and clearer as the years go on. It is an old quality concept. You have to know your raw material supplier—garbage in, garbage out.
NOVEMBER/DECEMBER 2008 7

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
• Certificatesofanalysis–theoriginalmanufacturer’sCOAisnotalwaysobtained;alsooverrelianceontheCOAsandfre-
quentlynon-specificIDtestsonthecompositesample:The square root of N plus 1 – these kind of approaches can work. I am not
saying they are not statistically valid in many cases. But I hear the EU talking about testing every drum, and there is a reason behind
that. Part of the thought is, are the suppliers supplying your company really operating under GMP in the first place?
And the question I have been asking for years: Is the laboratory operating under good manufacturing practice? You are going to look
at the COA and trust that COA. I have seen some really interesting things at chemical manufacturers through the years with respect to
lab controls and the qualifications of the lab personnel. But it is up for grabs whether you can trust the data on a COA, whether we can
accept the COA each time and just do an ID test and trust everything else. I think a more risk-based approach that I have been hearing
is called for. To default to the minimum: I am sure none of you would tell your kids that or anybody you are mentoring at work – do the
least possible. Those people are not going to be in good stead for the future. It is the same way when it comes to this type of issue.
• Suppliermanagementqualificationprograms,qualityagreements,lifecyclemonitoring–allofthisisoftendeficient:Again
we have seen a lot of good programs and we hear great things from the industry about the direction they are going. Q10 people were
singing from the same song book. So it really does seem like people are ready to shift the paradigm. And that is great news for every-
one. I heard some good things about lifecycle monitoring yesterday. Certainly three lots and then not worrying about it again is not the
way to do it.
• Distantmanufacturingsitescanincludespecialrisks:I am still in the middle of reading the 700-page book The World is Flat, by
Thomas Friedman….He talks about goods and services [going overseas]. And producers of goods and services are different things.
You probably could do a paper audit for a producer of services. But a producer of goods – you have to be there and see if they actually
can make those goods, and you have to check periodically in person to see if they are still doing it, and even have a person-in-the-
plant strategy in some cases….There are certain cases where there needs to be hand holding for suppliers that don’t have a quality
culture yet. If the risk is going to be taken to go with that supplier, then there has to be significant hand holding and presence in the
region most likely.
Distant manufacturing sites because of geographical proximity are not audited by the drug product manufacturers in many cases,
especially excipients, which third parties can help accomplish. FDA inspections may be infrequent, and the regional authority might
not either inspect or they may not be at the mature state yet that other regulatory authorities are.
• Counterfeitingandsubstitutionofcheaperingredientsinwholeorinparttomakeaquickbuckis not uncommon. If you were
at the PDA conference, you heard Alison Sabin, acting director of the Office of Enforcement, talking about the fact that we have a lot
of prosecutions and a lot of fines every year. And those are cases that keep going forward and that can come to fruition, but it takes
many years and there are a lot of other ones in the works. There will always be the .1% that ruins it for the rest of us and makes our
jobs tougher each day. But they are always going to be out there. It is our job to make it as tough as possible so they look in another
direction, find another industry to prey on.
There are some good definitions out there for counterfeits. The WHO definition is “deliberately and fraudulently mislabeling with
respect to its identify or source.” You know the story on substitution of cheaper ingredients for commodities. Examples include
melamine which killed hundreds of pets, diethylene glycol for glycerin, over-sulfated chondroitin for heparin – all of those substitu-
tions caused deaths, and they are all fairly recent.
8 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
Be Realistic about Cost of Quality
In his presentation at the closing panel session, Van Trieste highlighted other key concerns emerging from the earlier conference presentations and discussions and offered addi-tional insights on how to address them.
He stressed the need for realism about the cost of qual-ity when purchasing or outsourcing from developing countries where regulatory oversight may be lax.
Risk management principles may dictate the need for analyt-ical testing of every batch and every container, which in turn may impact purchasing decisions. “The total cost of quality is going to be a lot higher if you put those safeguards in place, and I think you need to do that when you are going to the developing world.”
Addressing the criminal dimension of the supply chain control challenge, Van Trieste stressed that the pharmaceu-tical quality system is “not designed to find criminals. It is designed to keep the honest people honest.”
“We have to think differently and be smarter,” he asserted, including doing “a better job of auditing.” He cited the exam-ple of one big pharma company that, depending on risk, may send someone from its corporate security office to look at the situation from the criminal vantage point. Not doing skip-lot testing of material coming from regions where there is high criminal activity is also an appropriate practice.
Auditing is another place where cost cutting may be counterproductive, van Trieste said.
He pointed out that the limitations of paper audits were noted by regulators as well as industry during the conference. While paper audits may be of use before the auditing is con-ducted, “you have to have feet on the ground. You have to see what is going on.” Van Trieste has “never seen a paper audit or a survey come back that had bad news in it.” You won’t hear, for example, he quipped, that there is paint peeling on the ceiling above an open reactor, as Colorcon’s Schoneker reported at the conference he had found during an audit.
Also, Van Trieste noted, visiting the vendors is key in build-ing relationships, and “if you don’t have a relationship with someone, it is a lot easier for them to” take unfair advantage.
On third-party auditing, he stressed that U.S. and EU regulators have all affirmed publicly that shared audits in principle are an acceptable approach. Industry needs to “get over” its long-standing “irrational fear” accordingly.
Citing the same point made earlier at the conference by Lilly Global Quality Systems Director Barbara Allen, Van Trieste pointed to the amount of variability in auditing skills within companies themselves. “We accept that. Why shouldn’t we accept the variability of a third party doing that for us?” Using the third party approach, he said, would allow for “longer, more thorough audits, and more of them,” with increased patient protection the result.
Noting that there are recognized bodies such as USP, IPEC and APIC offering third-party programs and that the approach is used in the electronics and auto industry, Van Trieste suggested that pharma needs to change its perspec-tive on them. “We will get there faster if we do this and we will allow our suppliers to focus on continuous improve-ment.” Key suppliers now may be hosting five audits a week, he noted. Instead of concentrating on making their product better, “they are running around entertaining people. We have to stop this. We have to think differently.”
Van Trieste commented on suppliers that are reluctant to host pharma visits. Where possible, establish the provision for auditing before contracts are signed, he advised. When single source suppliers won’t allow auditing, “you are going to have to put in place stringent risk management principles. Every container has to be sampled and tested…. You are going to have to develop analytical methods that can detect adultera-tion. You are going to have to do those harder things. That is the cost when you get into these situations.”
The Amgen official went on to emphasize that develop-ing a good cost-of-quality model, “which is really the cost of poor quality,” is important in gaining executive man-agement support.
“We do a bad job educating our CEOs, our executive man-agement,” he said. “We have to talk to them in terms they use, so they can understand this is just as important as every-thing else they are dealing with.”
Van Trieste touted “a very simplified model” that is “very easy to implement,” put in place by Johnson & Johnson and described in an article published in Pharmaceutical Engineering in 2006. When Amgen implemented a similar system and executive management saw the cost implications, action fol-lowed quickly, he reported.
“There is already a cost of quality model out there that works for our industry,” he stressed. “We don’t need to reinvent things.” Relying on the formative work done by experts like Juran and Deming and companies like Toyota, the drug quality official noted that he has never had to “invent a quality system.”
NOVEMBER/DECEMBER 2008 9

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
The dialogue on the cost of quality with executive manage-ment will be spurred by discussing “the story of heparin” and the cost dimension of the recalls, stock devaluation and lawsuits such events incur, Van Trieste advised. In this con-text, a prevention argument becomes compelling.
The purchasing departments also need to be educated by the quality organization about the total cost of ownership. For example, they should be informed that, “if you are going to go to China and you are going to buy a raw material from a supplier we have no history on, we are going to open up every container upon receipt, we are going to do full ana-lytical on every container, we are going to do near magnetic resonance (NMR) testing to see if there is adulteration.” Purchasing would then understand that that is not the lowest cost provider.
Quality should not let purchasing do its job, Van Trieste asserted. “Get some fortitude. Be tough, or FDA will come in and be tough for you.”
Likewise, he emphasized that the cost of material control from vendors who can not assure that the purchaser’s speci-fications are met needs to be factored into the cost equation.
The Amgen official explored other elements in the supply chain equation where the application of a formal risk management approach is called for.
Like other pharmaceutical companies, Amgen has instituted a risk-tiered supplier evaluation and management system that provides for different auditing and monitoring approaches based on usage, supply chain knowledge and process robust-ness. Amgen’s goal for lower-tiered suppliers, Van Trieste commented, is “to move them up or move them out.”
He stressed the advantage of providing a preferred supplier list to R&D departments and encouraging their selection from it, “so quality doesn’t have to spend a lot of time and money in R&D saying I have to go audit all the suppliers. You already have a supplier database.” If that approach is taken, he asserted, “five years from now you will be wondering where all the work went, because you will be preventing those problems.”
Heparin situation Prompts Amgen CAPA
Outlining Amgen’s “supplier life cycle management pro-gram” at the conference, the biotech company’s Director of Supplier Quality Eric Berg highlighted Amgen’s response to the heparin situation as an example of its risk-based supply management program in action.
Amgen does not make heparin, Berg explained. But with the view that “industry news is our news,” the company acted quickly to understand more deeply its foreign-sourced mate-rials and the risks involved. The initiative was given top pri-ority, he stressed. In turn, Amgen is using the learnings to inform and improve its supplier management program.
Applying its corrective and preventive action (CAPA) pro-cedures, Amgen conducted surveys of its suppliers to gain a better understanding of the suppliers’ supply chain. It also held executive level supplier meetings to review controls and reinforce supply chain security, and put in place controls to identify at-risk materials moving through procurement.
The company also focused on its analytical capabilities. Experiments were performed to determine methods that would detect adulterants, and short-term near magnetic reso-nance (NMR) screen testing was applied to at-risk materials.
Amgen is now developing a global adulteration test-ing strategy based on the learnings, and sourcing teams are evaluating and reporting alternative options to executive management. long term enhancements to minimize risk will involve a combination of more dis-cerning QC methods, focused sourcing and relational supplier management.
Berg emphasized that “science is driving” Amgen’s assess-ment process. Factors in the material risk evaluation include usage, supply chain knowledge, and process robustness.
Key questions in the Amgen analysis were: • Would adulter-ation impact patient or process? • Is the supply chain trans-parent? Are there distributors and repackers? • Is sufficient material testing performed each time it changes custody? • How is the manufacturer audited? and • Are there produc-tion steps in the supply chain that can be proven to remove or identify impurities?
Amgen’s analysis showed that compendial testing was not adequate to detect adulteration, but that NMR “can unam-biguously” detect adulterants and identify their structure. Amgen is also pursuing NMR for use in quality control, both at the purchaser and the supplier level.
For complex media, Amgen found that no single technique has emerged as sufficient, and that process-relevant specifica-tions are needed for these materials. For some raw materials, chromatography and spectroscopy methods were found to provide some detection capability.
10 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
AMGen’s CAPA ResPonse to HePARIn sItUAton
The following is a discussion by Amgen Supplier Quality Director Eric Berg at the PDA/FDA September conference of the actions Amgen took in response to the heparin situation to better understand and control the company’s ingredient supply chain.
For us, industry news became our news. We acted quickly. And even though Amgen does not have heparin as a product, we put in place
a mechanism and a CAPA to drive action within our organization.
We [considered] materials originating from many countries, [acknowledging] that bad guys can be everywhere – you can get bad mate-
rials from anywhere. We focused our lens, though, on the China piece to better understand China sourcing, because frankly we didn’t
understand it. We made this initiative a top priority. We have applied our learnings and are taking them back to our supplier lifecycle
management program.
I have been at Amgen in the supplier quality job for three and a half years. If you asked me a year ago – and people did, my partners in
strategic sourcing – ‘Eric, what materials do we get from China? We are getting inquiried.’ I would have said, ‘zero materials come from
China. A couple of plastic parts come from Taiwan, but no chemicals come from China.’ As a result of this approach and what we have
done to go deeper to understand our supply chains, I now understand that I didn’t know what I didn’t know. I understand that we have
at Amgen five chemicals that come from China and 89 that are ingredients to make chemicals that come from China. My understanding
of my supply chain all of a sudden puts me right in the middle of the story.
Now we have gone through our whole process and learned about these in more depth, and understand that none of our drug products
at Amgen contains ingredients manufactured in China. So we can answer that question with high confidence now. But I went through a
process to learn that, and I am going to describe that to you.
So we put in place a CAPA. We conducted surveys of our suppliers. The surveys were directed letters from the desk of Martin Van Trieste
to the names of the people at all of our suppliers, with the list of all of the materials that they gave us and directed questions to say: ‘Is
this material China sourced? If so, what controls are in place? Are there ingredients used to make this material that were China sourced?
If so, what were the controls in place?’ And that gave us an understanding and the ability to do a positive check and to better worry
about our supply chain.
Through that process we ended up having executive meetings to review it. I was very pleased to see top companies really felt the sever-
ity of the issue and really responded to it. And even though it was maybe difficult for them to be transparent because of that vulnerability,
because of that threat that we might go direct, they still understood and partnered with us. I can tell you for sure, we have had others
where we didn’t have that transparency, because we didn’t have a relationship, because we weren’t really a big enough customer for
them. And the complexities that were illustrated earlier [at the conference] I think are very real.
We put ERP [Enterprise Resource Planning] controls in place. What I mean by that is, as we went through a process to understand the
risks of these materials, we were able to focus our lens and say, ‘of these seven or eight, these ones that come from China and these
other ones that have ingredients that come from China, we are going to micro-manage and put a little block in our SAP system, so that
when it comes to us we can understand it coming through.’
We have tried to perform adulteration experiments to understand if our analytical technologies and capabilities are going to detect adul-
teration if it is there – thinking of adulteration not as parts per million, but as a macrocontaminant.
NOVEMBER/DECEMBER 2008 11

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
We quickly understood that NMR is a technology that can help us to understand if adulteration is present. What we have done is micro-
manage those materials when they come in. It is a very small volume, but when they come in we would take them to an analytical lab,
do NMR and use that as a screen to say, ‘should we be concerned about this? Should we be investigating this more deeply?’ If so, we
would. If not the material goes though its regular path of normal QC testing, normal release and review.
We have a global strategy we are employing. We are focused very much cross-functionally. Our sourcing teams are evaluating those
places where we believe we have a risk. I can tell you that just the exercise of more deeply understanding our supply chain tells me
where I have risks. It tells me where I have suppliers that aren’t really responding to me. I can’t have that. If I have an issue one day and
I have to do an investigation and it takes four months to get something back, it is not worth it…. Supplier quality focuses on and needs
change control. I want to prevent issues. I want to know the changes before they happen at a company. So if I have a company that won’t
even respond to me in terms of this exercise, it gives me a clear view of that risk.
So science has driven our assessment. I have described a bit about what we are doing in terms of our risk. Further, we analyzed these
questions. It is a very holistic picture of supplier management. I agree with what IPEC says. It is not about more and more testing. It is
about better understanding your supply chain – having relationships with those people, better understanding their customers, their eco-
nomics, what are the other risks that might be out there. It is about understanding the distributors, the repackagers, and looking at it and
saying, ‘is this necessary? Are there other suppliers that can give it to us in a tighter supply chain, other suppliers that maybe would tell
us when changes happen, that would respond more effectively with issues?’
We looked at our auditing program to try to understand, are we best understanding the picture on the audits that we are doing? And then
we are looking at our steps in the supply chain to see, can we remove or identify impurities?
If our supplier quality program were 100% perfect, I wouldn’t need a safety net. But I haven’t found anything yet in life that is 100% per-
fect. And as a quality professional, I have to do everything I can to make sure that life-saving products make it to the patients. So NMR,
we are seeing, is a key technology for detecting adulteration. Through the experiments that we have done, we understand that it can
unambiguously detect adulteration with absolute structural assignment. We are seeing that this technology could be deployed in the QC
space. I am advocating, and at Amgen we are pursuing projects to do this, to bring NMR to the QC space. I would advocate for chemical
manufacturers to look at, can you bring NMR in? Is there a way that we could get NMR results on C of As? Is there some way of bringing
this operationally to the industry for the purpose of detecting and preventing adulteration from getting through?
For complex media, there is no single technique that has been identified yet, so we are still pursuing that. So this is a big nut to crack….
We are also looking at, what are those other things that would even further fortify our supplier quality program – NMR being this sort of
safety net – with a real focus being on, what about our audit program to address the new risks? How are we gathering knowledge before
we go out and do an audit? How are we driving our auditors in a consistent way? Are we asking the right questions when we are doing
the audit? Are we generating the kind of questions that can help us raise a flag? That is what we are looking at.
And then physical audits: When I say physical audits back to the original manufacturers, I was doing physical audits of whom I thought
the manufacturers were, and as I learned more and more, I see there is maybe another place back in the supply chain. This opens up
the complexities and probably the costs for audits. I understand there are many places in the supply chain – my naivete is gone. I now
know more about what I didn’t know, and know that my audit program does have to go to different places.
We focus a lot on trying to get good communication with suppliers. I think it is a function of relationships. You know if you have good
communication with somebody, because they are honest with you. And you know that for a lot of people it is transactional in nature.
12 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
The biotech firm has moved to enhance its procedures to ensure ongoing awareness and control of risks in sourced material. These include: audit questionnaires and checklists to gain knowledge on raw materials and adulteration con-trols at the supplier level; reinforcing supplier change noti-fication commitments; and enhanced adulteration detection processes.
In his summary, Berg affirmed his belief that “this is a time where we transform supplier quality for industry.” He stressed the current opportunities for pharmaceutical com-panies to work collaboratively with suppliers on win/win approaches that build trust and “reduce waste on both sides.” Given the supply chain complexities and number of mate-rials involved, a risk management approach is critical, Berg stressed, as well as transparency built on the mutual commit-ment to patient safety.
Citing the need for companies to evaluate their supply chains based on the heparin experience, Van Trieste commented at the panel session that a good CAPA system is not reactive but proactive, and should encompass not just events at the facility but “events everywhere.”
He cited the worsening economy as another example of a trigger for this proactive assessment. “When the economy
gets bad, people do more criminal activity.” Also, for exam-ple, truckers may be more inclined to turn off their refrig-eration units at times to save fuel, making temperature tails more critical. Natural disasters may be another appropriate trigger for a CAPA response. Van Trieste reviewed the key provisions in the Dingell legisla-tive proposal, noting that they include “very strong enforce-ment powers for the agency and very strong protection for consumers.”
Continuing in the risk management vein, the Amgen official cautioned that companies need to consider the “unintended consequences” of this tightened regula-tory environment.
For example, “it is going to take the material longer to get through customs,” and inventories and ordering patterns will need to be adjusted accordingly.
Vendors may also drop out due to the added complexity and expense, and inventories will have to be sufficient to accom-modate the transition to new suppliers. The tightening of reg-ulatory standards and oversight in countries such as India and China has already caused many facilities to close, and the impact on the global supply chain needs to be anticipated, Van Trieste said.
What we are advocating for and driving for with our suppliers is to really have transparency with change notifications…. We have quality
agreements in place and we are really trying to make that a clear expectation. And certainly there is a whole gradient of changes. So this
is our dialogue with our suppliers – what is important that Amgen wants to know about, and what are those ones that we don’t waste
your time or our time on. But it is defining that. At this point I am erring on the side of wanting to know more.
The responses that we have received in terms of the assessment that we have just gone through really becomes a new piece of our
knowledge management of our suppliers, much like animal-derived materials did a couple of years ago – to be able to look at that and
understand if anything has changed since last we talked about this with our suppliers.
Then we are looking at how we design in quality into our programs – so working further back in our sourcing programs, putting in the
right questions, putting in the right requirements for when our sourcing guys are looking for things. I just want to declare that our audit
and supplier change notification process is comprehensive across our material base. Detection or remediation are being applied, as I
described.
We are also looking at, and kind of going though a pilot, is there a simple mechanism that we could do to look at the material packaging
as it comes in, the material documentation as it comes in, and compare it to what we know is good material packaging and good mate-
rial documentation? I think we have learned in some of the adulteration cases that have come through that something that looks funny
probably is. Is there a way of actively checking? So what we are talking about is a visual detection program. Or think about it as digital
photos that our incoming QC folks can check against key materials.
NOVEMBER/DECEMBER 2008 13

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
On the proposed registration requirement for pharmaceu-tical ingredient suppliers, he joined other participants at the conference including IPEC’s Schoneker in maintaining that repackers and excipient manufacturers should not be exempted from paying a registration fee as the draft legisla-tion provides. Otherwise, they will register to gain a market-ing position, he maintained.
Van Trieste also expressed support for the photo library approach espoused during the conference.
“It is a good idea to take pictures of the seals, the drums, the labels, the certificates of analysis, your packing invoices, etc. and check it.” And it is not difficult. “You keep it all on the computer and check it when it comes in each time.” He pointed out that FDA uses this approach to uncover prob-lems during their investigations, finding that “something looks different than the drum next to it.” So keep those pic-tures, he advised. “It is a good practice, and it is easy to do. You can do it pretty quickly. It is not something that takes 100 years to get done.”
A “key takeaway” from the conference, concluded Van Trieste, is that “the sense of urgency when you leave here today has to be high.” He encouraged everyone in the room to “get involved, be active” and to work toward forming a consortium to develop global standards. Another key take-away is “caveat emptor” – “when you are buying something from somebody, it is your responsibility to beware of what you are buying.”
shift Happens In the supply Chain
GPhA’s Johnston in his concluding remarks voiced a similar take-home message, emphasizing that “the drivers that we have in place right now are really time-critical.”
Pointing to the conference emphasis on the responsibilities of industry and regulators to move towards patient safety, Johnston asked the participants to consider “how we can col-lectively move forward, and when do we move forward to make this happen?”
In terms of the pending legislation in particular, the question is, “how can the stakeholders in this room impact the legis-lation to make it be workable and practical and benefit both industry and FDA?” Johnston maintained that “a lot of good ideas” surfaced at the conference “that can move discussion forward probably in the right way.”
Noting the presentations on the relevant initiatives under-way, for example at USP, FDA and WHO, the GPhA official asked participants to consider further “how do we lever-age all these various stakeholders to raise the bar on those producers of goods and services in the four corners of the globe.” This will be a “major job” necessitating everybody’s attention, he asserted. He pointed to the heightened concern at the conference on upstream controls. At issue is how “we make those improvements in quality and assure that quality upstream from the pharmaceutical industry.”
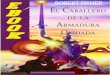
BAXteR’s InItIAL sUPPLY CHAIn RIsK ReDUCtIon PLAn
At the December PDA/FDA supply chain conference, Baxter Healthcare Supplier Quality Director Matthew Anderson presented the following chart depict-ing the initial focus of the supplier/supply chain risk reduction plan Baxter has put place in the wake of the hep-arin adulteration problem. Anderson explained that one of the first actions the company took was to identify risks and potential vulnerabilities. An action plan was then created to reduce the identified risks. The plan, Anderson noted, provides an agreed-upon structured approach that is rou-tinely reviewed by senior management.
• Reviewed existing methods • Developing enhanced screening and
testing technologies• Investigating new technologies
Ability to detect contamination
• Enhanced new supplier programControl of new suppliers
• Supply chain mapping• Expansion of master COA/picture
library • Expansion of tamper-proof measures
Tampering during transport
• Enhanced and standardized auditor training program
• Standardized audit reports Ability to detect problems during audits
• China-based• API suppliers• Ingredients
Review of high risk suppliers
14 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
Johnston also highlighted the discussion on the need to consider third-party audits and how to leverage them in the supply chain control effort.
Hospira’s Cauchy, who had spoken earlier at the conference on the generic industry viewpoint on the API and excipient supply chain issues, joined in supporting the third-party con-cept at the panel session.
Whether the audits are done by private companies or non-governmental organizations (NGOs) or involve shared regu-latory agency inspections, “we need to challenge the system,” he said. However, he cautioned on the need to address the liability concerns up front to get full industry buy in.
Cauchy also echoed “the need to make sure that the quality and procurement people are in the front seat of the car, as well as R&D, to make sure your needs are being addressed.”
The Hospira official further cautioned on the implica-tions on supplier requalification of the rapidly chang-ing marketplace and regulatory environment.
Noting that plants are closing, being sold and/or moving to Asia, Cauchy suggested that “just because they were an approved or preferred supplier when they were in Spain or Italy does not mean when they move the plant to China, they are going to continue to be at that same level.”
Hospira is also seeing a marked increase in process changes given the need to “stay competitive with all these new play-ers coming in from Asia. We have the traditional players in the U.S., Europe and elsewhere who are trying to compete, and so they are doing many, many process changes. That is something we have to keep a very close eye on.”
Cauchy further noted that the more powerful analytical equipment and methods are creating level-of-detection issues. Switching from parts per million to parts per billion raises impurity profile issues with API suppliers. “What was acceptable in the past may not be acceptable in the future.”
He echoed the point made by Van Trieste and others on the need to factor in the “total cost of ownership” and the “cost of compliance” when supplier decisions are made. He also urged the need for industry and regulators to continue to strive for “a level playing field” – a front-burner concern among pharmaceutical ingredient suppliers located in the U.S. and Europe (IPQ Nov./Dec. 2007).
Registration/Pedigree systems Improving
During the summary session, CDER regulators Friedman and Levy underscored other key points raised at the meeting.
Friedman began by highlighting the significance of the melamine contamination in Chinese baby food products that surfaced while the conference was in progress and the level of response the problem was drawing from FDA.
He also commented on FDA’s move to an electronic Drug Registration and listing System (e-DRlS) and the implications of the legislative proposal for regis-tration fees.
The new electronic registration system was rolled out in pilot form in July. The pilot will extend to July 2009, after which paper registrations will no longer be accepted. “So we are going to have instant information from manufacturers,” Friedman commented, “and that will help us with our data-bases and it will help us get a real idea of our inventory of foreign and domestic firms.” Citing the experience in the device center with registra-tion fees significantly decreasing the number of registrants, Friedman emphasized the importance of coupling the new listing requirements with fees in the drug context as well.
He underscored the problem the CDER staff has in determin-ing which firms are actually making products for the U.S. market vs. “just trying to look like they are registered at FDA and use that on a web site or in their advertisements to falsely give the impression that they have some sort of stamp of approval from FDA” through inspection or document review – which in fact “is just not true with a lot of these guys.”
In fiscal year 2008, the Center For Devices and Radiological Health (CDRH) implemented a new system encompassing electronic registration and annual fees and an active re-regis-tration process. CDRH is finding that the system has improved the data allowing the center to more accurately identify the type of establishment registered, the devices manufactured, and whether or not the establishment should be registered. The registration fees are targeted for the application review, including associated inspections (IPQ May/June 2008).
In its FY 2009 budget, FDA proposed instituting a reinspec-tion user fee, allowing the agency to charge for the cost of the inspection when it is deemed necessary to confirm that cor-rections have been made to previously cited problems.
NOVEMBER/DECEMBER 2008 15

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
FDA’s registration system remained a concern in the full report issued to Congress in September by the Government Accountability Office (GAO) on its study of FDA’s foreign drug inspection program.
GAO had issued a preliminary report to Congress on its research in November 2007 citing serious weaknesses in the program, and during the April round of hearings following the heparin contamination commented on FDA’s developing initiatives in the area (IPQ May/June 2008).
The full report includes updates to the earlier testimonies. GAO reemphasized the weaknesses in the information in FDA databases on foreign establishments subject to inspec-tion, adding that the recent FDA initiatives had not fully addressed them.
Generally, GAO continued to recommend that FDA strengthen its registration system and enforce a yearly update require-ment, along with conducting more foreign inspections to level the enforcement playing field, and ensuring corrections are made when deficiencies are found.
Levy gave a presentation at the PDA/FDA conference on pedigree and other tracking and labeling efforts in which FDA is involved. During the panel session, he reaffirmed that “in the post-heparin world,” the agency would “ideally” like to see a “universal and uniform” international electronic pedigree with information that goes “back all the way in the supply chain so that people can trace back to raw ingredients when prob-lems are occurring.”
The pedigree concept has “traditionally been associated with finished dosage forms” and the route they take from manu-facturer to wholesaler to chain drug house to pharmacy, Levy commented in his presentation. However, “after the heparin incident,” ideally “this e-pedigree would go back not only to the manufacturer, but we would go back a couple of more steps into active ingredients and raw materials as well.”
The U.S. Congress helped bolster FDA’s efforts in the 2007 FDA Amendments Act. FDAAA provided the agency with “new tools to facilitate electronic track and trace e-pedigrees across the drug supply chain and to develop standards and identify and validate effective technologies to secure the drug supply chain against counterfeit, diverted, subpotent, sub-standard, adulterated, misbranded or expired drugs,” Levy explained.
FDAAA requests FDA to develop the standards by March 2010, to harmonize with international standards to the extent
practical, and to consult with stakeholders on promising technologies. FDA proceeded to publish companion Federal Register announcements in March asking for comment on a series of relevant questions involving standards for a numeri-cal identifier, validation, track and trace and authentication, and for promising technologies. The docket closed in May.
Levy commented at the summary panel that, while there have been a series of high-profile health threats in drugs and baby food, the agency has to deal “almost every day” with dietary supplements coming into the U.S. from China that are adulterated with active ingredients from approved phar-maceuticals. Common are weight loss dietary supplements containing active drug ingredients and other products con-taining the erectile disfunction drug sildenafil.
Audit suppliers But Respect Relationship
In his closing remarks at the PDA/FDA conference, IPEC chairman Schoneker focused on the problems that arise in the supplier/purchaser relationship when purchasing agents focus on driving price down to the exclusion of the quality assurance component.
Over the last few days, Schoneker commented, “we heard a lot about building relationships between suppliers and users.” However, in practice there may be “a purchasing agent who comes at you every single year and says… ‘you have been a great supplier, we have no rejects or anything else. But we have an internal policy that we expect a 10% price reduction every year from you.’” Noting that such meetings with big pharma are not uncommon, the Colorcon official explained that they may include threats to cut off the supplier and/or reformulate if the price reduction is not agreed to.
The message the purchasing agent is sending is that the relationship “you worked so hard building” with the qual-ity people and the formulators doesn’t matter, Schoneker observed. And that message has repercussions. “I guarantee you when that customer asks for a favor they are not going to get any preferential treatment. They are going to get exactly what we have to give them and nothing more, as opposed to the company that develops a relationship and is fair, and it is a win/win situation that is good for the user and good for the supplier.” Similarly, Schoneker’s advice is not to “beat up” on suppliers that admit they may have problems meeting the purchaser’s specification requirements. A good supplier “is trying to sell you the best thing he can and do what he says he can do.” Big pharma needs to make an informed decision about the finan-
16 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
cial liability, rather than goading the supplier’s sales repre-sentative into promising what can’t be delivered.
SST Technical Affairs Executive Director Arthur Fabian commented that the specifications the manufacturer is trying to impose are frequently inappropriate.
As a distributor, SST has “run into this an awful lot.” The specifications were probably created outside the mindset of a quality-by-design (QbD) development program and have inappropriate limits and ranges, particularly for particle size. “When a supplier can’t meet your specs,” Fabian advised, “you really need to ask the question as a customer, ‘do we know if these specifications are in fact the specifications needed?’”
“You get what you pay for,” Schoneker reminded the phar-maceutical industry participants. “High quality suppliers, premium products,” and potentially higher prices, “is prob-ably the right way to go, and the kinds of suppliers you ought to be working with.”
Take home messages from the conference identified by Schoneker included going back and convincing “manage-ment in our own companies to set up these programs that are team based and understand the situation.”
Participants also need to take back the message, repeat-edly voiced during the conference, on the need to have “real, qualified audit information for every supplier for every material, and begin developing a workable pro-gram to get there.” And although they may not admit it, “most firms are not there.”
In line with the conference discussions, Schoneker asserted that “we have to come to that recognition first and then build the system we need. It is going to have to include some fash-ion of sharing audit information. It is the only possible way it can work.”
Referencing his earlier presentation and that by industry consultant Irwin Silverstein, who directs the IPEC affiliate third-party program International Pharmaceutical Excipients Auditing (IPEA), Schoneker affirmed that IPEC will be “working extremely hard on the excipient side to find good ways to do this. We want to work with you and hear your thoughts and try to build the standards that are needed, the guidelines that are needed, the forums that are needed, so that we can get there.”
IPEC/IPEA is moving to establish a formal program for certifying the GMP compliance of excipient manufac-
turers that will extend beyond its current one-day audit approach.
The certification will be sponsored by the excipient manu-facturer. The audit report on which the certification is based will be available at a nominal charge to the pharmaceutical customer. The certification will entail a comprehensive multi-day audit to assess the compliance of the site quality system with excip-ient GMP expectations. The supplier’s certificate will then be posted on the IPEA website for reference by the pharmaceu-tical industry.
IPEA is seeking accreditation for its excipient GMP certifica-tion program from the American National Standards Institute (ANSI). A preliminary application has been accepted.
ANSI, Silverstein explained, “requires: • that we develop an auditable standard • that we have a documented certification program • that we create the administration of the program which would be all of the documents and records to support our operation • that we establish objective expectations for conformance to the certification standard • that we establish a certification body that will evaluate the application and the audit report that forms the basis for granting certification • we will need a quality manual, just as any site that is certified by ISO 9000, because that is the roadmap ANSI will use to audit IPEA • and then we will have to host an ANSI assessment.”
In his concluding remarks, Schoneker also advocated closer cooperation with API-oriented groups like APIC, which has been developing a similar set of guidances to IPEC’s. “We need to start having some discussion with them about how to build a system that maybe has the same framework – that could be used in both areas, with appropriate expertise.”
Schoneker joined in recognizing the growing momentum witnessed at the conference. “I think we are over the hump,” he said. “We have some systems out there that were just wait-ing for the time, that were ahead of their time. I think the time is now, and the key is we have to get you involved. We have to all get involved together. And we have to join the efforts that groups like IPEC and other people are doing and make it happen.”
He stressed that “it is going to be critical that user/supplier relationships and the trust that we have improve to the point where each party has a much better understanding of the others’ process and problems. This needs to be a technical dis-cussion, not just a purchasing or supply chain discussion.”
NOVEMBER/DECEMBER 2008 17

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
IPeC, FDA Adding to excipient Guidance
IPEC has just released a new guideline on “Qualification of Excipients for Use in Pharmaceuticals,” intended to help build an effective user/supplier relationship.
At the IPEC conference, Schoneker described the new guide-line as “really a roadmap to what an excellent excipient qualification should look like, from the time the excipient manufacturer comes up with the idea that he wants to sell into this industry all the way through how users should be thinking when they are selecting their excipients and their suppliers, and then negotiating contracts at the end.”
These three “phases” – the excipient supplier’s process (“Phase 1”), the user’s process (“Phase 2”), and the negotiation process (“Phase 3”), are discussed in separate sections of the guideline.
The Phase I section, previously released as a stand alone guide by IPEC-Americas, provides background concerning excipient manufacture, regulation and controls, and provides guidance to excipient suppliers on the development of an excipient and its specifications. Phase 2 provides guidance on how users should assess the excipients for inclusion in their formulations. And Phase 3 addresses the development of an agreement between the excipient supplier and pharmaceuti-cal user to define excipient quality requirements.
The guideline references relevant guidance and standards from IPEC, ICH and the U.S., EU and Japanese agencies and pharmacopeias as well as from other standard-setting bodies and publications. Also included are a glossary and flow diagrams displaying the process pathways detailed in the document. The diagrams outline the sequential steps and appropriate decision points that should be evaluated in the excipient development and qualification process.
At the PDA/FDA supply chain conference, CDER com-pliance official Friedman pointed out that FDA does “inspect procurement indirectly” by “talking to the QA staff about how they select” the materials and who is making the decisions.
“If the QA department does not have the final decision in your companies on which vendors you are using – whether you are a raw material, intermediate, API supplier, or you are finished dosage form supplier – there is something wrong with your quality system,” Friedman advised. “Your QA unit has to make that decision. It should not be procurement driven and only price driven. Because some very bad mis-takes will be made.”
FDA management is committed to work to lower the risk of substandard ingredients by: • promoting GMP for ingredi-ent manufacturing • promoting good distribution practice and good import practice for ingredient commerce and trans-port • strengthening border protection, and • developing new rapid communication networks. However, Friedman stressed, “we are going to need a heck of a lot of help from industry in improving their daily supplier qualification and monitoring programs. Otherwise we won’t be successful.”
Friedman reported that the CDER compliance office is currently working on additional guidance on pharma-ceutical ingredient QA/QC that will consider physical attribute concerns as well as GMP/GDP issues.
While the ingredient adulteration/contamination incidents have been high profile due to their profound implications for drug safety and efficacy and involve a severity of risk that is “intolerable,” Friedman stressed that there are many more examples where lack of understanding or control of raw materials have caused drug quality problems and recalls.
A project now underway at the CDER compliance office to study the mechanistic root cause of product recalls, under the direction of industry consultant and statistician Lynn Torbeck, is pointing to raw material control as a prime cause of product failures.
Noting the preliminary findings, Friedman commented that “there are things that go on with raw materials that lead to failures that we don’t always understand…. There are mul-tivariate reasons” that may involve a complex interaction of three or four variables, which at their extremes will lead to failure. “That is not something that you will predict through DOE of raw materials or of your process,” he said.
The purpose of the recall study, Torbeck explained at the PDA/FDA regulatory conference earlier in the week, is to identify which recalls have the most potential patient impact, to identify the specific manufacturing root causes of the qual-ity defect, and to identify the trends so that preventive actions can be taken. The goal, he said, is to help FDA hone the focus of inspections in areas causing variability and improve com-pliance, build feedback loops to reviewers, and inform indus-try to promote voluntary compliance.
DMF Fees, Approval system Proposed
The implications of the current drug master file (DMF) system on supply chain control and the potential for evolving the way DMFs are used are issues that continue to receive atten-
18 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
tion and generated further discussion at the PDA/FDA and IPEC conferences.
Schoneker’s experience in advancing IPEC awareness in China has been that there is a “common misunderstand-ing” there about the U.S. DMF system. Companies including international big pharma subsidiaries located there believe wrongly “that somehow a drug master file is either needed to sell your product for use in a drug in the U.S., or that that DMF is in fact reviewed by the FDA and approved, and that means that your material is approved for use in a U.S. drug.”
He stressed that FDA does not review a DMF until a drug application is filed that references it. The large number of DMFs on file at FDA that have never been referenced and reviewed reflects the marketing advantage suppliers in China and elsewhere feel they gain in being able to tell cus-tomers in Europe and Asia that they are an FDA regulated/approved firm. Schoneker likened this DMF problem to FDA registration – a system which suppliers also have an incen-tive to abuse if fees are not levied.
Creating an approval process for API (Type II) DMFs has been proposed as a solution to the challenge of developing a generic drug regulatory system more con-ducive to API manufacturing changes. SST’s Fabian, a long-time proponent, made the case at the September conference that an approval process would help solve other of the API concerns being discussed as well.
“It is my opinion and the opinion of others that the drug master file system in the United States for a multi-customer environment is cumbersome, inadequate, and it doesn’t work.” In turn, “there are a lot of reasons that have been given over the last 15 years as to why drug master files cannot be approved.” However, Fabian maintained, approval of Type II drug master files would solve key multisourcing issues, and with 60% and rising of prescriptions now generic, “is worth talking about.”
One of the major reasons cited for not having the approval process is that many of the DMFs are not referenced. However, charging DMF registration fees would quickly result in a dra-matic decline in the filings and remove this approval pro-cess obstacle, Fabian asserted. Getting the right people to the table and doing “some out-of-the-box thinking” could result in “a workable DMF system for the generic industry,” he maintained.
A former FDA generic drugs reviewer in the audience noted that until FDAMA, the agency did have an approval process
for bulk antibiotics that “actually worked quite well, and was very efficient. I think it gave finished dosage form manufac-turers a considerable amount of certainty when they refer-enced that in their applications. So if we go forward in these discussions we do have that history to draw on.” Joining in the DMF dialogue, CDER’s Friedman commented that the fee would have to be large enough to serve as a true deterrent, noting that inspection costs are also a factor to con-sider. He suggested that, depending on the legal constraints, the system could be made more transparent by publishing a list of active (referenced) and inactive DMFs on the internet.
Schoneker suggested “having some sort of a sunset time – that if a DMF is not referenced within a certain period of time it goes into an inactive status. If you combine that with a reg-istration fee, I think now you start putting some teeth in it.”
Pointing out that “there are other controls we can put on it too,” he maintained that “most people in industry, I don’t think, want to see the DMF system go away, because there are certain benefits to that, both from the excipient and the API side. The key is how do we make it work in the best way. And I think some of these ideas need to be thrashed out a little bit more.”
stakeholders extend Global Reach
The increasingly global nature of the pharmaceutical ingredi-ent supply chain and its problems are reflected in the efforts of stakeholder organizations to become more inclusive and cooperative in pursuing their goals (IPQ Jan./Feb. 2008).
Associations like ISPE, PDA and IPEC have been expanding their relationships with Chinese and Indian regulatory authorities and helping to meet the infor-mation and training needs in these and other develop-ing areas.
For example, a memorandum of understanding (MOU) between PDA and the Shanghai FDA was announced at the PDA/FDA regulatory conference which proceeded the supply chain meeting.
IPEC, as part of the effort to expand its forum for develop-ing and harmonizing excipient guidelines beyond the U.S., Europe and Japan, formed IPEC-China in July. Schoneker explained at the September conference that mem-bers are now being sought, including multinational compa-nies interested in China. IPEC is “working very closely” with
NOVEMBER/DECEMBER 2008 19

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
the Shanghai FDA, the council chairman reported. “We are going to be translating all of our guidelines into Mandarin and putting on a lot of seminars over there, and other things. So this is going to be an exciting new way forward.” The council has also been in discussions with Brazil about start-ing an IPEC branch there and is interested in developing an IPEC-India. “So IPEC is going even more global then we were before.”
The regulatory agencies, including FDA and EMEA, have also been very actively pursuing cooperative arrangements to help address the global supply chain challenges.
One facet in FDA’s outreach effort is the establishment for the first time of offices in foreign countries (IPQ May/June 2008). The agency is moving quickly to begin setting up for-eign posts in China, India, Europe and Latin America before the end of 2008.
In a mid-October update, HHS explained that the first FDA staff will be posted in Beijing this year, with additional staff to be posted there and in Shanghai and Quanzhou next year. The current plan calls for eight U.S. nationals in China.
FDA is moving to also post staff in New Delhi in 2008 and open at least one additional office in India in 2009. Plans at present are for 10 U.S. nationals to be posted in India. The U.S. government is in the process of pursuing India’s formal approval of the post.
In both nations, the mid-October release explains, “personnel would work closely with local authorities as well as indus-tries that ship food and medical products to the United States to improve safety efforts. Their activities will include provid-ing technical advice, conducting additional inspections, and working with government agencies and private sector enti-ties interested in developing certification programs.”
FDA is also in the process of opening overseas offices in Europe and Latin America, with a fifth office in the Middle East to follow by mid-2009.
HHS Secretary Mike Leavitt commented in the update that “increasing our presence overseas will provide greater pro-tections to American consumers at home and benefit our host countries as well. Opening these offices will mark a key mile-stone in the globalization of our efforts to enhance the safety of imported food and medical products.”
FDA Commissioner Andrew von Eschenbach added that “the globalization of the food supply and medical product
manufacturing has demanded that we do things differently. Through our Beyond our Borders initiative, we won’t have to send our experts to another country to work with foreign governments and regulated industry to improve our over-sight – we will have staff living there and working on the ground 365 days a year.”
The release notes that department officials are also working to conclude Memoranda of Understanding (MOUs) with a number of countries in Central America to work together on product safety. These collaborations “could include information-sharing on their respective regulatory systems and joint work-shops and training on the safety of food and medical products.”
FDA’s international collaborations include supporting the World Health Organization (WHO) in its efforts to help countries enhance their regulatory infrastructure and approaches to ensuring product safety, quality and integrity.
WHO’s International Medical Products Anti-counterfeiting Taskforce (IMPACT) is the most significant coordinated public/private partnership addressing the global counterfeit problem (see box on pp. 21–23).
WHO is also involved in overseeing GMP compliance through its Prequalification of Medicines Program.
Indicative of the organization’s GMP oversight presence was a “notice of concern” issued to Sandoz in September regard-ing deviations found at its Sparton, South Africa plant during an inspection conducted in May. As a result of the findings, WHO suspended a Sandoz turberculosis product (isoniazid plus rifampcin) manufactured at the facility from its list of prequalified medicines until a reinspection could be con-ducted to verify the firm’s corrective actions.
The notice of concern is similar in function to an FDA warn-ing letter. They are issued by WHO following adverse com-pliance findings, the organization explains, “to remind a manufacturer or research organization of their obligations to quality assurance and to inform suppliers and procurement agencies of potential risks associated with a given product, manufacturer or organization.” WHO clarifies that a notice of concern does not imply a public health threat. “If WHO iden-tifies a public health risk, appropriate additional steps will be taken to advise the public.”
WHO outlines its inspection activity and summarizes the findings on its website, and provides other supplier and product information related to its Prequalification of Medicines Program.
20 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
USP has also been actively engaged with helping other countries address the problems of counterfeit and sub-standard drugs in their supply chains.
The program, which is overseen by USP’s Drug Quality and Information Program Director Patrick Lukulay, is funded by the U.S. Agency for International Development (AID). It involves USP’s working with drug regulatory authorities in Africa, Latin America and Southeast Asia to strengthen their quality control laboratories and assessment efforts in order to gain better oversight of the drugs coming into and circulat-ing within their countries. The program also works with local
manufacturers to make them more compliant and encourage better GMP practices.
The USP/AID program helps in setting up drug quality mon-itoring sites at various strategic points within the countries. Products are randomly selected and tested and the results shared with the ministries of health so that action can be taken. Anti-malarial, TB and HIV drugs are the main targets.
USP is finding that the sophistication of the counterfeited products has gone up, and that real active ingredient is now being used but without meeting quality standards.
FDA oFFICIAL BeRnsteIn on U.s. & WHo AntI-CoUnteRFeItInG eFFoRts
At the PDA/FDA Pharmaceutical Ingredient Supply Chain Conference in September, FDA Office of the Commissioner Pharmacy Affairs Director Elisa Bernstein discussed the agency’s efforts to improve supply chain integrity. She noted that FDA’s international focus includes supporting WHO in its efforts to help countries enhance their regulatory infrastructure and approaches to ensuring product safety, quality and integrity. The following is Bernstein’s description of the ongoing work to secure the supply chain in the U.S. and the global efforts of the International Medical Products Anti-Counterfeiting Taskforce (IMPACT) on which she serves.
U.s. Domestic supply Chain security Initiatives
I want to focus a little bit on what we are doing for supply chain security domestically…. When you look at how we deal with this prob-lem of counterfeits and diversion and supply chain security, there are a whole lot of players involved, both from the private sector and the public sector…. We are working together to solve some of these problems and put solutions in place.
At FDA in 2004 we stood back and talked with all the stakeholders. We looked at some of the vulnerabilities in the U.S. supply chain, and we came up with an action plan on how to try and address [them] and try to ensure that it is more safe and secure.
Our action plan is a multi-layered approach: • First we said you need to secure the product and the packaging. Here we rely on tech-nology and talk about the use of technology, and I will go into some of these. • We talked about movement of drugs. You need to secure how drugs move through the supply chain and make sure in the business transactions between business partners in the supply chain [you are] dealing with a legitimate business partner. And I know there are ways to identify if the business partner in the supply chain is legitimate. • We also said we need to ensure that there is appropriate regulatory oversight and enforcement of laws at the state and the federal level. • Increase the penalties.• Increase the vigilance and awareness of health professionals and consumers so that they are more en guard to help in this fight. • And also international collaboration.
What is the U.S. supply chain doing with respect to drugs using anti-counterfeiting features?…. Here is what we are seeing in terms of trends across industry: Manufacturers are actually using a lot of these different types of technologies to secure the product packages, to secure the labeling and to secure the actual product itself, to make it easier for FDA and others to identify if you are dealing with a counterfeit or the genuine authentic.
A lot of supply chain partners are working on pilots using some of these technologies that authenticate the product and using some of the technologies for tracking and tracing. Those have been going on for years, and I am still hearing about new pilots that are being cre-ated, new partners across the supply chain.
NOVEMBER/DECEMBER 2008 21

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
Manufacturers are exploring mass serialization. What does that do? Mass serialization is our term for putting a number on every single
bottle. So if each bottle had its own serial number, then you can track that bottle. And that gives that individual bottle a unique character
to it, so that if a bottle goes astray, you can help find it. If you want to make sure that it was handled by the appropriate people along the
way in the supply chain, you can create what is called a pedigree that uses that number for that bottle, so you can know the chain of
custody for each particular bottle. Because without individual serialization or unique serialization, every bottle looks the same, and you
don’t know which one might have been handled by inappropriate people in the supply chain.
What companies are looking at and exploring is putting that unique number in either a bar code or on a RFID tag. We are working on
some standards development that I am going to talk about in a minute.
Other things that are going on with manufacturers is that they are being very helpful to FDA’s forensic chemistry center, which is in
Cincinnati. [The center is] developing their own reference library, so that if there is a suspect counterfeit, we can quickly analyze it
against an authentic standard. That is extremely helpful. So having manufacturers share up-to-date versions of their products has been
really useful.
So with respect to RFID, very few of the products on the market right now have RFID on them. Again there are some pilots. FDA has a
compliance policy guide, 400.210, that talks about using RFID for pilots. We extended it last year and it is meant to expire in December
of ‘08. And at some point in the near future, we will be announcing whether we are going to extend it again, revoke that or modify it in
some way.
With respect to the pedigree, knowing who has the product, where it has been, this actually has been a big issue on the state front as
well as in Congress. When you pass that pedigree, FDA has national federal laws for who has to pass a pedigree and when. The states
have their own laws, and it is becoming very confusing in the marketplace. So FDA has said we need a universal pedigree and a uni-
form pedigree so that every one passes it and you are passing the same pedigree. Ideally, we would want to see an electronic pedigree,
because you don’t want pieces of paper flying all over the place that could also be counterfeited. We have said that in order to get that,
Congress would have to change the law.
Some of the tools that we have with respect to pedigrees [are provided by] the Prescription Drug Marketing Act. Pedigrees make sense
– knowing where a product is, where it has been, where it is going, helps ensure that you have a legitimate product. But there are chal-
lenges in the current pedigree law. Not everybody has to pass a pedigree. It is not for all transactions. It is not universal. It is not uniform.
There was a lawsuit related to the Prescription Drug Marketing Act, and just last month, a federal appellate court upheld a preliminary
injunction that prohibited FDA from enforcing a very key piece of the pedigree regulations that we have in place. So this is actually very
challenging out there.
One very exciting piece though that came up in FDAAA when it was passed in September 2007 is that it gives FDA the authority to
develop standards for authentication, identification, tracking and tracing and validation of prescription drugs. This is exciting for us
because this says, ‘FDA you have a role to put in place standards in the U.S. so that everybody can be on the same page with respect to
tracking and tracing and authentication and identification. And Congress said in that law that for serialization, the standard for putting
that number on there, you have to have that number in place by March 2010. So they gave us a deadline.
There is also a big effort outside of FDA that FDA is a part of, GS1, which is a big international standards organization. These are all the
different types of standards that GS1 is working on for tracking and tracing and serialization and validation. So there is a lot of work
going on in the U.S. and globally.
22 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
Global Anti-counterfeiting efforts of WHo’s IMPACt
Two years ago WHO decided to take on efforts related specifically to counterfeit medical products – not just drugs but devices as well.
WHO created IMPACT, the International Medical Products Anti-Counterfeiting Taskforce. I am the U.S. delegate for this task force, and I
am the chair of the regulatory working group on the taskforce.
What this task force is doing is creating a toolkit – different types of tools that regulators and even the private sector can use to put
measures in place for combating counterfeit drug and medical products and preventing counterfeiting.
We are looking at the experiences from different countries. One of the working groups created model legislation, which [provides]
national principles for setting up infrastructure within a country for combating counterfeit drugs and medical devices. We are developing
training materials and different types of methodologies. So for investigators that go out either on inspections or to investigate an incident,
there is an enforcement strategy manual.
We are also looking at different types of tools to help countries identify where the problems are. In fact, we just finished developing this
tool: that if a country wants to look at where the gaps are, they would sit down for pretty much a whole day and look through their laws,
their regulations, their needs, and they would answer this long and intense questionnaire. And at the end of it, what they get are the
regulatory gaps with respect to the country’s regulation, legislation and other types of infrastructure for combating counterfeit medical
products. Actually that tool is in beta testing right now, and it will be very exciting to find out what the results will be.
So this is the largest and most coordinated international public/private partnership to address the public health issues related to coun-
terfeit medical products.
Just because I am the chair, I am going to tell you a little bit about a couple of the tools that we are developing. And of particular interest
– I know that there is a session later about good distribution practices – what our group in the IMPACT has done is we took the existing
WHO GDPs and we went through them and identified where they could be beefed up and changed to address counterfeit medical prod-
ucts and supply chain security issues. We came up with our suggestions. We gave those suggestions back to the WHO technical working
group that is in charge of it. They sent it around for comment, and in October they are going to be considering whether or not to adopt
these suggestions. There might be after October a revised WHO good distribution practices document.
We are also working on a guidance specifically for combating counterfeit medical products that are sold over the internet, which is a
huge challenge for regulators right now because the internet [eliminates] borders and makes it very difficult with the movement of drugs
and devices all over the place. This is a big challenge, but we are going to try to come up with some sort of guidance for countries for
combating and addressing the internet.
We are also looking at revising [WHO’s] Good Pharmacy Practices. We are looking at developing a sampling strategy so that coun-
tries don’t use all of their resources going out and sampling the marketplace randomly. What this is going to look at is doing a risk-
based approach to try and identify counterfeits using limited resources. Everybody has limited resources these days, so it is a waste of
resources to just go out and pick a pharmacy or a wholesaler here or there. What this is going to look at is using a risk-based approach
for sampling.
Finally, IMPACT is looking at ways that governments can respond quickly when there is a suspect counterfeit product.
NOVEMBER/DECEMBER 2008 23

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
India and China Draw Regulator Attention
Cooperative inspection and compliance information-sharing arrangements with foreign regulatory agencies are another important component in FDA’s outreach strategy.
The motivation for pursuing such arrangements is clear in the face of the statistics on rapid growth in for-eign drug facilities and products under FDA regulatory purview.
The agency’s database indicates that the number of drugs produced overseas for the U.S. market (including finished drugs, intermediates and APIs) and the number of foreign facilities producing those drugs more than doubled between 2001 and 2007. Foreign drug facilities registered with FDA grew from about 1,200 to 2,800 during this period, while drug products expanded from about 17,000 to 43,000.
However, FDA inspection resources have not expanded, nor have the number of foreign drug inspections the agency has been able to conduct.
“While we are going to step them up a little,” Friedman com-mented at the supply chain conference, compliance officers scheduling the inspections “are going to have to make some very difficult choices – choices none of us in this room want to make.” The data on the lines of drug imports charted against the number of U.S. import field exams and tests paints a simi-larly disturbing picture. Between 2002 and 2007, human drug import lines mushroomed from 142,000 to 312,000, while drug field exams/tests were actually fewer in 2007 (2,300) than in 2002 (3,400).
The shift overseas of manufacturing for drugs mar-keted in the U.S. – and to China and India in particular – is also writ large in the data from new and abbrevi-ated new drug applications (NDAs/ANDAs).
An “establishment evaluation request” (EER) from the FDA reviewing offices to the field organization is triggered for all facilities listed in the applications involved in production, testing and packaging, etc. The EER may result in an inspec-tion if deemed necessary to assess or confirm the facility’s GMP compliance status.
The FDA EER data from 1992 to 2007 shows a dramatic uptick in the number and percentage of foreign facilities listed, with the trend accelerating around 2000, particularly on the ANDA side (see box at right).
Salient in the EER data is the shift of API production to India for generic products. The number of Indian API plants listed in ANDAs exploded from 30 in 1999 to 450 in 2007 – account-ing for almost 40% of the total last year.
An increasing number and percentage of APIs for newly marketed NDA products are also being made in India. The number expanded from three in 1999 to 61 in 2007, making up about one in six of those listed last year. Altogether, only one out of four API manufacturers cited in NDAs in 2007 was located in the U.S.
For all types of facilities listed in innovator and generic applications, the move abroad is apparent but not as dra-matic. About half of facilities of all types referenced in both NDAs and ANDAs are in the U.S., down from about two-thirds in 1992.
LoCAtIon oF FACILItIes LIsteD In nDAs AnD AnDAs (1992–2007)
The following is a breakdown of the location of facilities listed in NDAs and ANDAs in 1992, 1999 and 2007. Included in the data are facilities for making finished dosage forms and APIs, control testing labs, sterilization, packaging/labeling, etc.
US Other foreign India China
ANDAs (all)
1992 1121 478 8 8
1999 1504 441 20 12
2007 2310 1125 867 57
ANDAs (API)
1992 84 365 8 8
1999 135 389 30 20
2007 151 497 450 56
NDAs (all)
1992 611 224 1 0
1999 900 542 3 2
2007 743 596 69 8
NDAs (API)
1992 106 224 1 0
1999 102 275 3 2
2007 88 275 61 7
24 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
At the PDA/FDA conference, U.S. Department of Commerce Office of Health and Consumer Goods Director Jeffrey Gren pointed to data indicating that by 2004 India and China together were producing about half of global API production, with Europe about one quarter. However, by 2007, India’s and China’s share had continued to grow substantially to over two thirds (68%), with Europe’s dropping to 16%.
During the 2004–2007 timeframe there was a significant decline in the API manufacturing sites globally from approxi-mately 2,000 to 1,144 – reflecting in part regulatory tightening in India and China, both of which have upgraded their GMP oversight programs.
Data from India presented at the supply chain conference by Mumbai, India-based industry consultant Ajit Dangi, indi-cates that 500 facilities have been closed down there due to GMP noncompliance since 2005 following the amendment to India’s drug and cosmetic act (“Schedule M”) making GMP mandatory. Dangi noted that a bill has been introduced into the Indian parliament to make counterfeiting a non-bailable offence and enhancing punishment up to life imprisonment.
Along with its expanding export market, India’s domestic market is also growing rapidly and is expected to triple in size over the next decade to about $20 billion.
One of India’s major pharmaceutical manufacturers and a large supplier of generic drugs to the U.S., Ranbaxy, ran into significant GMP compliance problems with FDA in 2008.
In mid-September, FDA issued a pair of warning letters and an import alert involving generic drugs produced by Ranbaxy’s Dewas and Paonta Sahib plants in India.
The import alert was being issued because of the “extent and nature of the violations,” an FDA release at the time explained. The alert provided for any API and both sterile and non-sterile finished drug products manufactured at the two plants to be detained at the U.S. border. About 30 different generic products were covered by the alert. FDA informed Ranbaxy in the warning letters that no NDAs or ANDAs for products manufactured at the two facilities would be approved until the deviations cited were corrected.
The release clarified that the action was “proactive” and did not involve removing products from the market, since “FDA has no evidence to date that Ranbaxy has shipped defective products.”
The warning letters were based on inspection findings at the two facilities in early 2008. The main problems noted during the inspections involved beta lactam cross-contamination controls, recordkeeping, failure investigations, and aseptic processing operations.
During April and May, Ranbaxy submitted lengthy responses to the findings. According to the FDA release, “the agency then evaluated its findings, Ranbaxy’s responses, and the firm’s overall inspectional history – an evaluation that required substantial time due to the complex scientific and technical nature of both the identified deficiencies [and] the firm’s responses. Ultimately, FDA concluded that the firm’s responses were not adequate and that the warning letters were the appropriate regulatory response.”
Showing the interlinking nature of the global regula-tory community, WHO issued a position paper the day following the FDA September announcement explain-ing the agency action and its impact on the organiza-tion’s Prequalification of Medicines Program.
Noting that FDA had not found marketed Ranbaxy products out of specification and had advised that Ranbaxy medications continue to be taken until they could be replaced with product from other manufacturers, WHO “strongly advised” that consumers not interrupt their drug therapy “where alternative treatments are not available” nor switch to non-prequalified products, whose quality has not been documented by WHO.
As of September, Ranbaxy had 18 products prequalified by WHO, two of which were antiretrovirals (lamivudine and zidovudine) manufactured at the Paonta Sahib plant impli-cated in the FDA action. WHO notes in its release that it had performed several inspections at the Ranbaxy Paonta Sahib site – most recently in June 2008 – and that during each of these inspections, some non-compliances with GMP were observed. However, “after each inspection the company sub-mitted corrective action plans to rectify these non-compli-ances and in general the site was considered to be operating at an acceptable level of compliance with WHO GMP.”
WHO added in the position paper that it would be “closely monitoring the case and planning a series of extraordinary actions on top of its routine monitoring activities to confirm if products prequalified by WHO from Ranbaxy continue to meet all the necessary requirements.” The WHO actions will include: eliciting clarification from Ranbaxy in the issues raised by FDA; close contact with FDA under the confidenti-ality agreement concerning the Ranbaxy products; and con-tact and liaising with other national regulatory authorities
NOVEMBER/DECEMBER 2008 25

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
and UN agencies such as UNICEF. If public health concerns arise in relation to these activities, WHO said, the affected products would be suspended from the prequalification list and stakeholders informed.
In a presentation on the evolving regulatory picture in China at the supply chain conference, industry consul-tant Wilkinson noted that steps there to beef up GMP enforcement include the use by the Shanghai FDA of a fleet of trucks with mobile testing labs to visit com-panies and test the quality of their pharmaceutical ingredients.
While the Chinese regulatory system is still “young,” Wilkinson affirmed that “Chinese regulators are listening” and want to “learn from the rest of the world on the best ways of doing things.” Blood products and parenterals are a focal point of their risk-based approach. “They do have an API certification system and are evolving their GMPs, and they are even talking about QbD. They recognize that this is something that will be necessary in the future.”
[Editor’s Note: The Nov./Dec. 2007 issue of IPQ provides an extended analysis of drug quality regulatory developments in China.]
Inspection-sharing Pilot Launched
Aware of their own resource limitations, FDA and EMEA have been very actively pursuing cooperative inspection and compliance information-sharing arrangements, both between themselves and with other outside authorities, to help address the global regulatory challenges (IPQ July/Aug. 2008).
FDA and EMEA together have recently launched three initiatives which will build on the confidentiality/infor-mation-sharing agreements that have been put in place.
One of the projects involves piloting joint inspections in the U.S. and EU for finished products. A few companies have already been approached as candidate sites. Sites to be con-sidered need to be making products of mutual concern with similar inspection deadlines in the two regions. The hope is to complete a joint inspection in the next few months.
A second pilot is focused on inspection coverage of API sites outside the two regions. FDA and EMEA will explore the exchange of inspection schedules and results. The objective is to identify sites of mutual interest, avoid duplication, ratio-nalize resources and extend inspection coverage. Joint inspec-
tions may be part of the approach. The Australian Therapeutic Goods Administration (TGA) is joining in the API pilot.
The third project involves stepping up EMEA/FDA collab-oration on a risk-based approach to the issue of dedicated production facilities for products posing high cross-contam-ination risks.
Industry concern grew following the release of a draft EU guideline, now being reviewed, that would have required dedicated facilities based on product type, which industry felt, would be unnecessarily restrictive and not risk-based. The EU anticipates publishing a revision of its guideline during the first quarter of 2009. FDA is also reviewing its existing regulations and draft guidance on the high-risk product groups penicillin and cephalosporins.
The three quality-oriented projects are among the out-comes of talks that have been taking place between the EU and the U.S. through the Transatlantic Economic Council (TEC) and its offshoot the “Transatlantic Administrative Simplification” (TAS), focused specifi-cally on the regulation of medicines. The umbrella TEC is a broad high-level trade initiative to remove unnec-essary red tape and rationalize relevant policies.
A workshop was held to initiate the TAS project in conjunc-tion with the TEC meeting in November 2007. At the TAS workshop, industry was asked to present to the regulators proposals for where the regulatory procedures and guidance for medicines could be simplified and streamlined through transatlantic cooperation and harmonization. The ground-rules were that the proposals should not require legislative changes and should maintain or increase current levels of public health protection.
The industry proposals were presented in four thematic panels addressing quality and inspections, pharmacovigi-lance, scientific collaboration and guideline formatting and electronic submission. The forum included broad-based industry participation with representatives from different industry facets and organizations. The regulatory participa-tion included the EC, the EMEA, heads of the national medi-cines agencies, and various divisions of FDA.
Addressing a session at the September PDA/FDA annual meeting on the Transatlantic Administrative Simplification project, industry consultant Wilkinson explained its significance. Wilkinson, then with AstraZeneca, represented EFPIA at the TAS 2007 forum.
26 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
For industry, the workshop invitation “felt a bit like Christmas,” Wilkinson said. Senior regulators from the U.S. and EU asked industry to “come and tell them about things that frustrate you and don’t add value to the regulatory sys-tems and ultimately the health care to the patient.” The focus was on regulatory areas that could be addressed on a transat-lantic or wider international level where there was unproduc-tive “red tape” and “blind compliance” and both regulator and industry resources could be redeployed “to things that actually mattered in terms of patient safety.”
Once the topics had been agreed to and prioritized, the goal was to have a “roadmap” in place by June 2008 for bilateral work through the EU/U.S. confidentiality agreements or through multilateral venues such as ICH.
The eclipsed schedule was met and a “Medicines Regulation: Transatlantic Administrative Simplification Action Plan” was released in June.
Among the collaborative projects agreed to by the EC/EMEA and FDA in the plan were the two inspection pilot initiatives and the dedicated facilities review. The agreement on these three initiatives had already been announced following the meeting of the Transatlantic Economic Council in May, at which a number of issues involving various regulatory agen-cies were addressed.
The TAS plan also provides for collaboration on combating counterfeit medicines. In addition to the collaborative work with the WHO IMPACT initiative, the plan calls for the EC/EMEA and FDA to exchange information on future require-ments for track-and-trace and authentication systems and on specific cases of counterfeits.
Other of the plan’s 18 action items call for collaboration on addressing biosimilar/follow-on biologics and a report on this effort to the EC/EMEA/FDA bilateral meeting by the end of 2009, and further collaborative work in areas such as biomarker development and validation, risk management, advanced therapies, herbal medicines and the ICH Common Technical Document.
Quality-oriented projects recommended by industry at the November 2007 workshop that didn’t make the immedi-ate action list were review of the EU policy on retesting of imported products, which industry maintained does not meet value and risk-based criteria, and a proposal for working toward a global pharmacopeia or, short of that, mutual accep-tance of pharmacopeial standards. Mutual acceptance would allow companies to be able register products as compliant with either the U.S., European or Japanese Pharmacopoeias
and make that acceptable in the other region’s registrations. Another proposal put forth by industry at the late-2007 workshop was for FDA and Europe to issue standardized “Certifications of Pharmaceutical Products” (CPPs) that can be used by other regulatory agencies around the world as proof that a product has been licensed/registered in the U.S. or Europe. On the EU retesting issue, Wilkinson noted that EFPIA has “gone back” to the regulators and “challenged this as an area that should be looked at again, because we don’t see it as a risk-based approach at all.” In a letter to the EC, EFPIA expressed its belief that accommodation could be made for eliminating the retesting requirement for products manufactured in facili-ties found GMP compliant without changing the EU legisla-tion. The decision to not include it as an action item reflected EU concern that a legislative change would be needed.
Wilkinson commented that the dedicated facility issue, like that of rationalizing inspection resources, “is a good one for U.S. and EU regulators to work together on, because we don’t want different guidances in this area.” He praised ISPE’s technical paper, “Risk MaPP,” as helping to address the deci-sion making around “this complex area.”
Overall, Wilkinson views TAS as a “very positive initiative,” bringing regulators, law makers and industry to the table to “focus on risk-based activities and ultimately on protection of the patient.”
“We are on this journey. We are trying to support this shift towards a more science-based way of working and science and risk-based regulatory systems.” The current economic climate, the global problems that have arisen and the concern of the politicians have helped drive forward the TAS initia-tive, he said.
Joining Wilkinson in addressing the TAS session at the PDA/FDA conference were EMEA Inspections Sector Head Emer Cooke and CDER Compliance Office Deputy Director Nicholas Buhay.
While “a lot of the work” on inspection information sharing and other of the TAS proposals for cooperation “was already underway” through the EU/U.S. confidentiality agreements, Cooke commented, the TAS process “has been very helpful in stimulating interest” and giving the initiatives “political vis-ibility and helping to move them forward.”
With reference to the inspection-related pilots, Cooke com-mented that both the U.S. and the EU are very supportive of exploring how international inspection resources can be most
NOVEMBER/DECEMBER 2008 27

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
effectively deployed. “I think both sides want to see if we can increase inspectional coverage outside the regions involved. This will allow us to coordinate or collaborate on sites of mutual interest, and hopefully in the long term help us to have a better oversight globally of sites outside our respec-tive territories.”
Noting that the “program to program” discussions are increasing, Buhay stressed that “overall, FDA considers enhanced collaboration and administration a win/win” and is “committed very much to it.”
“All of these things that are taking place – shared inspection information, third party inspections, enhanced communica-tion between the site and the regulator – all of these combined could allow us to reach the goals of administrative simplifica-tion,” he said. “We are very enthusiastic about the opportuni-ties for better regulation, more effective regulation, regulation that doesn’t seem to be honorous but rather helpful.”
At the session, Cooke outlined the envisioned process
for the API inspection information-sharing pilot and
the progress in making it operational.
“We are starting off with sharing information on the inspec-
tions that we have performed and planned, and this allows
us then to see whether there are sites of mutual interest to the
parties involved. If there are sites of mutual interest, we can
look and see whether we can rely on the inspections that have
been performed or are planned to be performed by one of the
participating authorities. If the authority in fact wasn’t plan-
ning on covering the activity of interest to another authority,
they would be asked to see whether they could do that within
the scope of their inspection. And then the third possibility is
that there would be a joint inspection of the site. But this is
not the preferred option. The preferred option is to see how
much we can rely on exchange of information.”
eU/U.s. GMP DIFFeRenCes not seen As A HURDLe to InsPeCtIon CooPeRAtIon
During the discussion period at the TAS session of the PDA/FDA annual conference in September, the three pre-senters – FDA’s Buhay, EMEA’s Cooke, and industry representative Wilkinson – were asked about the impact of differences in the EU and U.S. GMPs on inspection cooperation. The following are their comments:
BUHAY:Differences in GMP: I am always amazed at this consideration, because many times we have made line-by-line/control principle-by-control principle comparisons of the GMP regulations in the states and from the EC, and frankly we see very little difference.… There is always the possibility of differences in interpretation [on] what constitutes adequate performance to the GMP requirements... because we apply principles, not detailed descriptive statements of what needs to be done in a vastly com-plex and variable set of circumstances for producing pharmaceutical products. So I think that the procedures that we are putting in place, certainly those we have at FDA, require reconciliation of the different views on any set of findings before it is presented as a position.
COOKE:We are looking for ways to make this work and we are not trying to find all the obstacles, real or imagined, that might be there. We could go through this exercise and have a step-by-step approach as to what you would do when you meet a problem, and we would never get it started if we did that. So one of the principles is that we will use our best efforts to come to an agreement.
With respect to the GMP standards issue, I don’t see this as an issue. We see very little real differences. There might be a heading here or there that is quotable in one respect but not in the other. But when it gets to really major problems, we are expecting to have common agreement on those. With respect to coordination, I think the key there is having the cooperation of the company concerned.
WILKINSON:I fully agree with Emer and Nick that the reality is that 99.9% of the GMPs are the same essentially. We have a lot of exercises in comparing, and we shouldn’t really try and block initiatives with the ‘what if’ scenarios. One point bearing in mind is that a lot of this work will be in the area of API inspections, where there is a common global standard [ICH Q7A]. So there is only one standard that the inspectors will be working to.
28 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
When the discussions on the initiative were launched at the end of 2007, Cooke explained, a number of competent author-ities who are performing significant numbers of inspec-tions of APIs outside of their territories were approached. Coalescing for the pilot from the European side were EMEA, the EU member states France, UK, Germany, and Ireland, the European Directorate for the Quality of Medicines & Healthcare (EDQM), the Australian TGA and FDA.
The effective kickoff for the project was a teleconference in early July. “We got lots of good ideas coming out of that tele-conference, and we started to work then on templates for exchange of information and rules of engagement for partici-pating authorities covering the various options outlined in the project,” Cooke said.
A second teleconference was held in September to help move the pilot into its operational phase. “We are hoping very much that this is going to work,” Cooke commented. “If this is going to work, we see immense possibilities in extending in other areas, but we want to make sure that we get it right in the start.”
For the various transatlantic projects that are underway, Cooke sees a great deal of enthusiasm on both sides to move these forward, and a “high level of commitment from both parties.”
The EMEA views its “EudraGMP” database as an important facilitator in the international collaboration effort and is enhancing the information the database contains and its availability accordingly.
Cooke stressed that EudraGMP is “the first pan-European source of information” on European manufacturers and com-petent authority inspections and a “key tool” in facilitating exchange of information, transparency and cooperation. “It is designed to facilitiate inspection planning so that we can focus our resources better. So that instead of a number of countries going to the same site to inspect related activi-ties, we can try to ensure that only one authority can cover all the activities for the whole of the EU. We see that it will avoid duplication of inspections and will facilitate exchange of information on non-compliance.” The new system will allow information on non-compliant manufacturers to be shared in a much easier and more rapid manner, Cooke said. The EMEA will be making parts of the database public, with limited data available in early 2009 and more substantial information made available from members states by the beginning of 2011.
Cooke stressed that EMEA is currently discussing “with a number of our international partners as to how they can com-municate with the EudraGMP in the best way to help them get the benefits from this and help us get any cooperation that we might be able to get out of this…. We see this data-base as having a great potential in terms of increasing global transparency and we are looking to share this information with as many of our partners as we can.”
EMEA’s 2009/2010 workplan calls for inclusion of certificates issued by its MRA partners to the EEA. Another planned pro-vision is the sharing of rapid alert information on defective products to all those with access to the database. A further module will cover planned inspections outside the EEA.
[Editor’s Note: A discussion by Cooke of the EudraGMP and other EMEA initiatives underway to respond to the global quality regulatory challenges is included in the July/August issue of IPQ on pp. 15–19.]
At a conference on inspections sponsored by FDANews in mid-October in Bethesda, MD, Paraxel consultant Peter Smith, a former FDA compliance official with for-eign inspection responsibilities, discussed the impli-cations of performing joint EMEA/FDA inspections under the pilot projects.
Smith pointed to several questions that would need to be addressed: • Who will take the lead? • Would there be an inspection fee, and if not how would the inspections be funded? • What format would the report take? • How would differences in freedom of information (FOI) regulations be addressed? and • Where there are GMP differences, for example between FDA’s asceptic guidance and Annex 1 of the EU GMPs, which would apply?
The FOI issue is a substantial one, Smith commented, since “the Europeans have no FOI rule at all” and “Her Majesty’s Secrets Act [in the U.K.] actually prohibits release of govern-ment findings to the public,” while FDA is generally obli-gated under its FOI rules to release them.
Smith went on to compare the inspection procedures and approaches of the FDA and EMEA (see box on next page).
While there are differences, Smith noted that the inspection process inside facilities has become more similar recently, with European interest increasing in documentation and FDA’s inspectors spending more time observing operations. The influence of a more quality systems-oriented approach has helped drive that convergence (IPQ July/Aug. 2008).
NOVEMBER/DECEMBER 2008 29

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
PAReXeL ConsULtAnt sMItH CoMPARInG FDA AnD eMeA InsPeCtIons
At a conference on inspections sponsored by FDANews in mid-October in Bethesda, MD, Parexel consultant Peter Smith compared the inspection procedures and approaches of the FDA and the EMEA. Smith made the comparison in the context of discussing the initiative for increased information sharing and joint inspections that the two regulatory bodies are developing. While Smith pointed out differences in the approaches and pro-cedures, he also noted that the inspection process inside facilities in recent years has become more similar, with European interest increasing in documentation and FDA inspectors spending more time observing opera-tions. Prior to joining Parexel (then KMI), Smith had a lengthy FDA career during which he conducted foreign inspections and served as a compliance officer with responsibility for foreign inspection oversight.
FDA publicly provides a lot of detailed information about how they are going to do the inspections and what the inspectors will look for, [which] any company can use to prepare for an inspection.
[For the EMEA], the key reference is the EUDRALEX, Volume 4 – their GMP regulations along with various annexes. They have the docu-ment ‘Compilation of Community Procedures on Inspections and Exchange of Information – Conduct of Inspections of Pharmaceutical Manufacturers.’ By title, you would think it would talk a lot about how an inspection is going to be done. [However,] it primarily is admin-istrative. It really doesn’t have much information in there on actually how the inspection is going to be conducted when the inspectors arrive at the site – what they are going to be doing, what they are going to be looking for. And then there is the document, the ‘Joint Audit Programme for EEA [the European Economic Area] GMP Inspectorates.’ This is exchange of information between the inspectorates within the member states.
What I am trying to say here is that EMEA doesn’t actually put out a lot of information as FDA does in its compliance programs and so forth about how they are going to do inspections. So it is a little bit more difficult to prepare for those inspections and realize what is going to be happening than it would be for FDA.
I want to point out differences in the inspectorqualifications: For FDA, basically the inspector has a bachelor’s degree, usually within a scientific discipline – chemistry, biology, it could be engineering. In many cases, they do not have advanced degrees…. FDA does have orientation and basic training courses – evidence development and law, and then specific training in certain pharmaceutical and medical device areas. And of course FDA has developed the ‘pharmaceutical inspectorate’ cadre, where they now are actually giving them special training and have certain levels to achieve and so forth, in an effort to try and bring the inspectors to a point where they can actually inspect intelligently the very complex and high tech facilities that they need to inspect. Some do have advanced degrees, and the experience level varies in terms of the number of years that people have been in FDA and how long they have done inspections. Obviously, there is going to be an influx of new inspectors. It will take them two or three years to really become independent if they are hired now. So you are going to be seeing a new generation of FDA inspectors entering your plants soon.
On the EMEA side, many have PhDs, and they really are required to have the qualifications that would allow them to be a qualified person (QP). They generally tend to be a little more educated than FDA inspectors. The MHRA requires a minimum of five years of experience in industry as a prerequisite. Seldom in FDA do you have people that have worked in industry. They may have worked in industry for a short time, but most inspectors were not part of industry. They came to FDA right out of college. The Swedish inspectorate has an aver-age of 10 years experience.
Of course [EMEA inspectors] may come from different member states. In the teams that I have seen, there might be somebody from England and France, or Italy and Spain. Very often it is a mix of nationalities. The good thing is the inspections are conducted in English. That helps all of us very much…. But the difference is because they have industry experience, they know some problems with particular
30 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
operations and can be more understanding about some of the issues. They may say, ‘gee you have a [particular brand of] tablet press. The last time I ran that press we had a problem here or there. They can be that specific. Whereas I think FDA perhaps will not be. So in some cases, in terms of process and equipment, the Europeans can be much more diligent in looking at some of the issues that might come up. I think it is very important to understand the differences that you can see between the two inspectorates.
There are some differences in approaches and methodology between FDA and EMEA: I think the first line is most important – FDA is more enforcement oriented…. From day one when I was in FDA we were told we are a law enforcement agency. The FDC Act is a con-sumer protection law, but it is still a law…. We were told we are law enforcement agents and we carry a badge…. The difference here is FDA is trying to build a case – taking copies of the documents, maybe Xeroxed boxes of documents, because they want to present to their compliance people all of the things they found wrong. I think very seldom will the EMEA folks actually take copies. They are much more assessment oriented. They will discuss things. They are almost consultative sometimes. Because they have worked in industry, very often they are much more comfortable talking with manufacturing people and understanding some of the issues they have, whereas FDA tends to be a little bit more by the book. FDA will spend time documenting violations, whereas EMEA will make notes and report violations.
Certainly CBER is a center-directed process, and there is much communication on the CDER side with the directives, the guidelines, the compliance programs from CDER, and then the input from CDER during or after the inspections. Whereas in EMEA, it is really an inspector-directed process. The inspector really decides how he or she is going to manage the inspection. They do much of the follow-up following the inspection. There is no real central place that gets clearance, like the center’s compliance offices and the lawyers and so forth within FDA. All of those components don’t really exist in the EMEA.
Both will begin by reviewing deviations, failures and other problem indicators, and this is very common. Most auditors understand that companies really do operate in routine circumstances, day to day, pretty well. They know how to do what they are intended to do. They usually work okay to make money. But the FDA and all auditors want to see how you handle non-routine situations. That is why they ask about complaints, deviations, change control – all of those are non-routine activities, and the inspectors want to see how you handle those. So that is on both sides. That is equivalent. They may come at it from a little different direction, but eventually they are going to come to the same conclusions.
FDA tends to be more system focused and documentation focused. Whereas the EMEA may be more operations focused. They may spend more time out in the plant actually watching the operations and speaking to the people out there and so forth vs. FDA that may spend the preponderance of their time in the conference room reviewing documents.
[FDA’s] primary interest in investigations is the methodology for resolving deviations, whereas the EMEA looks at the justification for the resolution of the deviations. So there is a little difference there. Again, it is a little more assessment oriented on the EMEA side, whereas it is a little more enforcement oriented on the FDA side.
FDA will generally not look at internal audit reports, and on the EMEA side they may want to see the audit reports for the API manufac-turers or some indication that that API manufacturer has been looked at in terms of compliance with GMPs.
Some other considerations when we are talking about the non-U.S. inspections: There is a site master file that is required in the EU. Such a document has not been required for a number of years in FDA. The Type 1 drug master file is basically the same as a site master file. EMEA usually likes to see the site master file in advance before they actually come to the site.
I will talk a little bit about how technical agreements are very important to the EMEA. In cases where they have biologics, the separa-tion of pre and post viral inactivation activities is very important to the EMEA. Certainly certification of BSE/TSE-free materials. That
NOVEMBER/DECEMBER 2008 31

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
Global Harmonization Vision needed
In presentations at the PDA/FDA conference and at the ISPE annual meeting in Boca Raton, Florida in late October, CDER Director Janet Woodcock discussed the roles and responsi-bilities of regulators and industry in addressing the global supply chain concerns and why international regulatory harmonization is critical in supporting these efforts (see box on pp. 23–25).
She cited the increasingly global nature of the supply chain, driven in part by the expanding market share of generic drugs, as contributing to a greater potential for exploita-tion and a greater need for a cooperative and harmonized approach to prevent it.
Although significant progress has been made in interna-tional harmonization and the adoption of common standards through forums such as ICH, “the global regulatory system
unlikely is something that FDA will even ask about during an inspection for raw materials and so forth of animal origin. It is one of the top topics that comes out in non-U.S. inspections.
Job descriptions should contain specific GMP-related duties, which may or may not be the case in an FDA scenario. Training programs should be related to the job function and contain proficiency testing including periodic testing. For someone who has done the job for five or ten years, the EMEA believes they should be periodically checked to make sure they are actually performing that job proficiently and in compliance with the operating procedures that they are using.
The Europeans are concerned with good distribution practices. Basically when the product is shipped out of the drug manufacturer in the U.S., FDA’s overt attention is lost. They may go to drug distributors and so forth, but they don’t ask about [details of how you] assure the supply chain and distribution of your materials once they leave your company. However, the Europeans are very interested in that.
I will talk a little bit here about technical agreements – quality agreements, GMP agreements, and so forth. The Europeans want to see these agreements in place for every contracted operation, whether it is laboratory, packaging operations, API manufacture, whatever it might be. They look at these very closely and comment on them. Certainly from a business perspective, there should be an agreement between the outsourced company and the sponsor. But FDA is not really looking for these technical agreements. They may say that quality has not provided proper oversight over outsourced operations because of whatever the problems were. And certainly FDA would like to see the quality agreements, GMP agreements, whatever, but they don’t actually ask for them and inspect them, whereas the Europeans do. In the EUDRALEX Volume 4, which is their GMPs, they talk about the contract giver, the contract acceptor. And because it is in their GMP document, this makes those types of agreements necessary…. A little bit more on inspection comparison: In Europe, the final product release responsibility lies with the Qualified Person and there is no U.S. equivalent. So if you are attending to the EU, you certainly have to have the proper provisions for having a QP in Europe to release the product and manage that. There is a whole annex that is part of EUDRALEX Volume 4 that talks about the responsibilities for the QP. So that is certainly something that you need to be concerned about.
In general, many traditional QA responsibilities are handled by production in Europe, but this will not necessarily cause a real prob-lem [in U.S. inspections] as long as it is being done correctly.
Europe does not issue ‘483s,’ but they do send post-inspection letters that list the problems they have found during the inspec-tion. They were under discussion at the end of the inspection, and then sometime later you will get a report and a letter. The inspection report comes to the company for correction of inaccuracies. At that point, any of the issues that are brought up can be responded to. But it is not the same process as FDA where you have a 483, you respond to the 483. You may have a warning letter and then respond to the warning letter. It is a less formal. Again it is inspector-driven in Europe, because that letter and the inspection report and its conclusions are really written by the inspection team. There is no real supervisory review and higher level authority review of that inspection report and the conclusions and the decisions based on that report. So again, it is a lot less formal in Europe.
32 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
is still highly fragmented,” Woodcock pointed out at the ISPE conference. Noting the negative impact of the diverse inspec-tion and review practices and expectations, she stressed the need for “standardization and uniformity” – for doing “things the same way all the time.”
The challenge is to harmonize the standards, but also to make sure that the implementation is harmonized; “in other words, where the rubber meets the road – every application, every establishment doing things the same way.” Within CDER it is hard to assure this consistency, she said, so “developing more consistent approaches around the globe… is going to be tough.”
What is needed, Woodcock stressed, is “a vision for a fully harmonized international platform, both for review and inspection for quality.”
“This has to be our long term goal,” she maintained. “It is not going to work otherwise in my opinion. We have to have a standard approach to quality. Compared to clinical, this looks like a picnic. But it isn’t. It is tremendously difficult.”
Given the challenges involved, Woodcock said, “we won’t get there unless we understand where we need to go. This has been discussed a couple of times in ICH. We probably need to discuss it in a broader venue. And then develop an action plan for continued progress. Because right now we are in the phase of trying to implement what we have already standardized, and that is good. But we need to also start thinking about how we get to the next level.”
The globalization of manufacturing is a challenge “for indus-try and regulators alike,” she emphasized in her conclusion at the IPSE meeting. “We want to do the best for our custom-ers, the people that take these medicines. They deserve and they expect a uniform high level of quality.”
The heparin situation “brought home the need for
vigilance” in addressing the global supply chain,
Woodcock maintained.
“For the regulatory agencies around the world, heparin was a wake up call and it should be a wake up call to all profes-sionals who are working in the pharmaceutical quality area. We had up to 30% contamination of the finished widely-used drug product – worldwide contamination, present in many APIs, present in many finished products distributed to many countries.”
Woodcock elucidated the moral of the story, echoing the call made at the PDA/FDA supply chain conference for a coordi-nated global action plan.
“Much progress has been made over the past few years in har-monizing standards for submissions, harmonizing what we think for GMPs. But recent events have demonstrated an urgent need for continued progress, including involving all nations and involving the industries in the plan to move forward. We need an action plan to be developed, and we really have to think very seriously about in what venue we would develop that plan.”
CDeR’s WooDCoCK on InDUstRY/ReGULAtoR RoLes AnD GLoBAL HARMonIZAtIon
At the recent PDA/FDA and ISPE annual meetings, CDER Director Janet Woodcock discussed the roles and respon-sibilities of regulators and industry in addressing the quality of the global supply and why international regula-tory harmonization is critical in supporting these efforts. The following is excerpted from the two presentations.
We have to recognize that FDA and other regulators cannot inspect quality into the global drug supply. Inspection is only one important
component. The U.S. Congress is very focused on inspections – that we do more inspections – and that isn’t a bad thing. We would like
to be able to do more inspections around the globe. However, that is not going to be the way we ensure quality.
The manufacturers, the importers, the brokers and the distributors are going to have to take primary responsibility for maintaining the
quality of pharmaceuticals throughout the supply chain. And the reason is just like any other quality issue – it is the people on the ground,
the people managing that product that have to have primary responsibility for quality.
NOVEMBER/DECEMBER 2008 33

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
The regulators can try to set up systems. We can also work of course with the criminal investigation side because some of the threats
are from criminal activity, and we can help try to deal with that. But really as far as quality overall, you all have to take charge of that.
Training personnel and training regulators in countries that are emerging as manufacturing centers is just critical. This is an urgent need.
And these groups often are hungry for this kind of training. That is where professional societies like you who have a huge number of
members who are experts in these different areas can really help…..
As I said, manufacturers are primarily responsible for the pharmaceutical quality and for supply chain integrity. And I think most people
would agree with that. The regulator job is to promulgate or adopt quality standards, and we have been pushing on doing this as much as
possible. We need to ensure that the standards are met. But our job is really to audit rather than being the people responsible for quality.
We have to take action against poor quality, whether it is criminal-type behavior or other types of quality problems that we may see.
We need at the same time to enable continuous improvement so that we are not putting some type of structure in place around the world
that keeps people from innovating in this space and actually improving the outcomes, making it more efficient.
But professional and technical societies and standard-developing organizations need to participate in developing global technical stan-
dards. For many of these, the regulators do not need to set these standards. They can be set by technical groups, standard-developing
organizations and referred to by the regulators. This is often preferable because there is more agility in the standard developing world
than the regulators have. We need the professional groups to disseminate these standards and provide global education opportunities. The
professional and technical societies really need to widen the circle and develop a global professional community that is working on this.
Now what is happening in the U.S.? We are trying to focus on international regulatory harmonization. I believe that is one of the very
important things that we can do. If we can lay out and resolve some of our remaining differences and have a global platform on quality
that everyone understands and implement that uniformly, we will have gone a long way. Then we can have one message to all the rest
of the world that wants to join this effort.
FDA is also engaged in international outreach. We have been doing that for a long time. The new initiative is called “FDA Beyond Our
Borders.” We also are improving our information technology to keep track of the inventory that is in the U.S. and coming into the U.S.
We are going to continue the Pharmaceutical Quality for the 21st Century initiative. Because at the end of the day I believe that the
advancement of science and the application of science and technology to pharmaceutical manufacturing is one of the most important
things for resolving many of these issues.
So what do we need to have in international harmonization?
• aseemless,effective,globalregulatorycollaboration– a sort of world-wide safety net. We need to have regulators in all countries
be part of this global safety net. I think we all realize now that where one region or country goes, there we all go. It has to be across
the world. We can’t just sit in our citadel in FDA and say we will make sure that everything that gets in this country is okay. It is not
going to happen that way.
• increasetheeffectivenessofinspectorates, or even their presence, in these developing countries – countries that are developing
a pharmaceutical manufacturing sector.
• fullyharmonizedqualitystandardsfor ICH and non-ICH regions. We need to work for example, on implementation of ICH Q10 and
qualification of suppliers, etc. We need to consider, do we need to extend the principles of GMPs, say to excipients?
34 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
UsP’s Horizon Is expanding
While expanded inspection coverage by regulators is impor-tant, Woodcock stressed in her recent presentations that it is only one of the components that needs attention in the inter-national cooperation and harmonization effort.
Another key component, she points out, is the participation of standards developing organizations (SDOs) and support-ing associations in advancing global technical standards, which can then be referenced by regulators.
As in the case of the regulatory agencies, pharmacopeial cooperation and harmonization is being driven by the global nature of the standards issues needing to be addressed and the limited resources individual pharmacopeias have avail-able to address them.
At the PDA/FDA annual meeting and at the USP Annual Scientific Meeting in Kansas City in late September, USP CEO Roger Williams gave a high-level view of the challenges and opportunities in the advancement and harmonization of pharmacopeial standards.
Williams noted that the harmonization process with the European and Japanese Pharmacopeias (EP/JP) through
the ICH adjunct Pharmacopeial Discussion Group (PDG) has been relatively successful in the excipient area, both for monographs and general chapters. He gave IPEC and its three regional organizations “a lot of the credit for that. The TriPECs stepped up to the plate and sort of told PDG what they wanted, and that kind of vigorous interaction I think was very helpful to PDG.”
PDG “may be on the lip of a new way of thinking about working together,” Williams said. Notably missing from the process in the past, he pointed out, have been the Chinese and Indian Pharmacopeial Commissions. “It doesn’t make too much sense to me to exclude countries that have between a third and a half of the world’s population” from pharmaco-peial harmonization. He added that the pharmacopeias pay attention to units of production – a category in which India and China together dwarf the U.S.
Williams highlighted the global effort to address the heparin problem, and the coordination between the USP, EP and their respective regulatory authorities, in particular.
Another facet of the USP/EP cooperative effort is a prospec-tive bilateral harmonization pilot involving four key drug substances (monolukast, rizatriptan, celecoxib, and sildena-fil). The pilot involves submissions of information and ref-erence material for the designated molecules by the pioneer
• continuemanufacturingmodernizationand make sure that it is implemented within these global regulatory agreements – that
we don’t harmonize down to the lowest common denominator and hold back the field. Modernization will also help us be capable of
detecting what is going on in a better way.
• harmonizedpharmacopeialstandards. That is a tall order I know, but every time we have fragmentation, we are creating more bar-
riers around the world for effective regulation and effective maintenance of quality.
• agreeduponstandardsforsupplychainsecurityandintegrity. So that if there is a hand-off from one country to another, from one
region to another, everyone agrees that they are operating off the same standards for security.
• betterautomationandstandardizationfortheglobalinventory, because we have these products moving all around the globe and
we can use better IT to keep track of them.
• ongoingtrainingbothofregulatorsandofpersonnelin countries that are emerging as manufacturing centers is just critical. This
is an urgent need. And these groups often are hungry for this kind of training.
• developavisionfor what a fully harmonized international platform for both review and inspection would look like, because I don’t
think we have done that exercise.
• developanactionplanfor further continued progress – not just an FDA action plan, but a global action plan. And we really have to
think very seriously about in what venue we would develop that plan.
NOVEMBER/DECEMBER 2008 35

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
companies. Working through the different pharmacopeial structures and procedures – in the EP/EDQM case involving 36 member states plus the EU – the pilot’s goal is “the elab-oration of a final good monograph with physical reference material,” Williams explained.
Reflecting the expanding global pharmaceutical supply chain and marketplace for drug substances and drug products, USP has also significantly strengthened its relationships and interactions with other pharmacope-ial commissions, including those of China and India, and with the WHO.
USP has opened laboratory sites in Hyderabad, India, Shanghai, China and Brazil, and is working collaboratively on testing of reference standards, monograph elaboration, and other standards-setting activities. There is consider-able enthusiasm for these cooperative efforts, Williams com-mented, “because at the end of the day pharmacopeial resources are truly constrained.”
He pointed out that USP has “a very well-articulated series of [public] meetings now throughout the world,” including meetings in China, the Middle East region, India, south Asia, Europe and Latin America, that continue the global dialogue from its annual scientific meeting in the U.S.
USP has also been globalizing the makeup of its Council of Experts. “There are certain penalties for not being a ministe-rial pharmacopeia [government run],” Williams commented, “but one of the privileges is that we have no barrier for reach-ing into any part of the world for membership in our expert committees. And it is truly a privilege to see scientists from all parts of the globe help us set our standards.”
Williams emphasized that a significant force driving pharmacopeial evolution is the rapid advance in mea-surement science, which has not emanated mainly “from either the regulatory agencies or the pharmacopeias, but rather more the national metrology institutes and ISO.”
He anticipates that USP and the other pharmacopeias as well as the regulatory agencies will work increasingly closely with the national metrology institutes and their global parent body, the International Bureau of Weights and Measures (VIPM) located outside Paris. Involvement will likewise be increasing with ISO “by virtue of their guidances and other documen-tary standards.” The USP CEO sees “huge opportunities for us in working with ISO and VIPM and their allied bodies.”
An indication of this tightening relationship, Williams pointed out, is FDA’s GMPs for the 21st Century as well as ICH’s qual-
ity system guideline Q10, which have a “strong linkage to ISO fundamentals.” He noted that both FDA and USP labo-ratories have been ISO 17025 certified, and that USP is also certified to ISO 9001. USP’s hiring of William Cook from the U.S.’s metrology institute, the National Institute of Standards and Technology (NIST), to head the pharmacopeia’s metrol-ogy effort, will further this interlinking process.
Like the alliance between national metrology institutes and the parent organization VIPM, ISO is allied to professional associations for standard-setting bodies, which in the U.S. is the American National Standards Institute (ANSI). The U.S. has a “grassroots” approach to standards, Williams noted, with about 600 standard-setting organizations, about half of which are ANSI-accredited.
The ANSI-ASQ National Accreditation Board was the body that accredited USP’s certified reference material (CRM) pro-gram, which is now getting off the ground. A key goal of USP’s certification program is to lesson the contribution ref-erence standards make to the uncertainty around regulatory acceptance criteria and release specifications. The pharma-copeia announced the release of its first CRM, dextrometho-rphan hydrobromide, in September.
Another potential catalyst for more rapid harmoniza-tion is the growing pharmacopeial interest in perfor-mance-based standards.
“We are just beginning to come to grips with some of the pos-sibilities for performance-based standards,” Williams said, noting that they are “much more common in other indus-tries” and helped Europe overcome the obstacles to regula-tory harmonization in the food area.
In the drug pharmacopeial context, he explained, a format for a monograph could be created that would not include the procedures themselves, but would allow for any procedure as long as the acceptable criteria were met. He pointed out that the default criteria currently in the USP are 98-102% for the drug substance and 90-110% for the drug product. ICH, in turn, provides impurity limit defaults. The criteria or limits could be referred to as “monograph design space,” Williams suggested – “that if you stayed within them, in terms of your procedure, you would be okay.”
The performance-based approach “gives you what I might call compendial flexibility,” he said. “You could use any pro-cedure you want as long as it met the criteria.” The approach would ally with the “equivalent or better” concept incorpo-rated in FDA and USP policy.
36 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
Under William’s vision, USP would have “very good methods” in its mandatory general chapters. “They would be very clear, very well organized, very simple,” providing “about 150 or 200 methods that you would use in your measurement studies.”
The performance-based monograph, in turn, “would not specify the procedure, but allow you the flexibility to choose a procedure as long as it was an adequate procedure.” To sup-port the evolution into this flexible monograph approach, he commented, “we understand clearly that the procedure must have a reference material, and our current view is that that reference material should be a certified reference material.”
Williams sees “great hope with this opportunity… in many ways. I think one way is that it actually promotes very rapid global harmonization. And to me, if we could do that, we would move past a lot of the fussing that has gone on over the last 100 years or more about how you harmonize the pharmacopeias.”
It would also draw the pharmacopeias more closely to the national metrology institutes, Williams said, which could assist in doing “key comparisons.”
The key comparison concept derives from the 1999 interna-tional treaty calling for transparency at the national metrol-ogy level “about just how well they are doing with their measurements” – effectively placing the results in the public domain. While USP is not a national metrology institute, VIPM has allowed USP to participate in two key comparison pilot studies, including one on digoxin. Williams remarked that USP laboratories “showed up pretty well compared to other national metrology institutes.”
The USP CEO pointed to the growing influence of the world-wide intergovernmental organizations as helping bolster the harmonization process in the pharmaceutical area. Along with the WHO, these include the World Trade Organization, which has oversight of the VIPM and is the international equivalent of the U.S. Department of Commerce, and the World International Property Organization, equivalent to the U.S. Patent and Trademark office.
Heavy Metals Present Hard Issues
Two areas that are drawing particular attention in the effort to improve and harmonize global standards are heavy metals and residual solvents.
The challenge and opportunity as well as the importance of the harmonization process are writ large in the standard-set-ting effort on the two classes of contaminants.
The USP and EP along with the FDA and EMEA have been focusing on the complex issues around developing viable analytical specifications given the breadth of manufactur-ing, product and usage variables and toxicology uncertain-ties involved.
A forum for the discussion of the issues around heavy metals testing in pharmaceuticals as well as dietary supplements and food ingredients was held in late August by the National Academy of Sciences’ Institute of Medicine (IOM).
USP asked IOM to convene the workshop to help in the pro-cess of revising the standards in the heavy metals general chapter of the pharmacopeia (Chapter <231>). At the forum were national and international experts in metal measure-ment and toxicity. The forum committee sought to include representatives from the EC and Japan with the goal of work-ing towards common specifications for metals testing among the USP, EP and JP.
As noted in the summary prepared by USP on the workshop, the consensus supported the starting premise that the old wet chemistry procedure in the current USP <231> is no longer suitable and should be replaced by instrumental methods of greater specificity and sensitivity for a wide range of metals of interest.
At the same time, it was acknowledged that with the current state-of-the-art spectrometry methods, metals can be detected at levels much below that of any clinical or toxicological importance. The challenge in developing appropriate testing standards and limits, the workshop summary notes, is the cou-pling of method capability, risk assessment and likelihood of presence of metals with toxicity concern in a manner that best protects the public health and is viable in industry practice.
Wrestling with the complicated issues around which metals should be monitored and to what level of detection, the work-shop attendees concurred that further consideration of these issues and the limits for various metals would be required as part of the USP <231> revision process.
neW FDA Q&A on IMPoRtInG BIoLoGICs
In November, FDA’s Center for Biologics Evaluation and Research released a document addressing “frequently asked questions” about importing CBER-regulated products into the U.S. The questions addressed on the seven-page FAQ relate to: • what standards apply • FDA’s role • product coding, and • responsibilities and information needed for biological specimens/tissues.
NOVEMBER/DECEMBER 2008 37

www.IPQPubs.com
InternatIonal PharmaceutIcal QualIty
The focus should be on arsenic, cadmium, lead and mercury due to their high potential for clinical toxicity and risk for presence in the ingredients, the experts concurred. Other metals used in manufacture or present in starting materials will need to be considered using a risk-based approach. It was generally felt that testing for catalysts and reagents used in a specific process may be appropriate, with potentially a limit for the specific metals involved depending on the toxic-ity concern.
The suggested risk-based approach is in line with EMEA’s recently released “Guideline on the Specification limits for Residues of Metal Catalysts,” which played into the discussions.
Complicating the consideration of metals testing and limit setting is that the form of the metal, such as for mercury and arsenic, can significantly affect its toxicity, making a regu-latory standard based on total content potentially inappro-priate. The suggestion emerged that a reasonable approach might involve developing pharmacopeial specifications for the total amount of an individual metal at a worst-case limit, and requiring manufacturers to use speciation to justify a higher limit. Other toxicity issues that need to be consid-ered include patient population and condition, dosage form, duration of exposure, and other environmental contributions to the toxic load.
The workshop addressed the suitability of the newer spec-trometry methods and the need for reference materials to establish suitability and detection limits, particularly when several technologies may be used to produce acceptable results.
The participants concluded that USP should make a major effort to advance the metals testing in pharmaceutical ingre-dients, dietary supplements and food ingredients, and urged that this effort encompass harmonizing the approaches across the major pharmacopeia.
Also providing a foundation for the IOM/USP meeting discussions was the work of USP’s Ad Hoc Advisory Panel on Inorganic Impurities and Heavy Metals, which was appointed by the General Chapters Expert Committee to assist in the revision of <231>.
The ad hoc panel published a “stimuli to the revision process” article in the September/October issue of the Pharmacopeial Forum (PF) proposing a new chapter with pro-cedures that “rely on modern analytical technology” and “limits that are based on toxicity and exposure levels for the selected metals.”
The proposed chapter includes a table (#1) that provides limits for 31 metals in oral and parenteral materials. The pro-posal stresses that the table represents only a “first approxi-mation” by the ad hoc panel and that the limits and metals included “are under active discussion internationally.” Some of the limits were calculated using the EMEA’s new guide-line, the table notes.
The deadline for public comment on the PF proposal is December 15. USP’s current timeline calls for a draft chapter on heavy metals to be published for comment in the summer of 2009, with a final chapter targeted for about a year later. A generous implementation phase will follow.
The proposed chapter exemplifies USP CEO Williams’ comments at the annual scientific meeting on the phar-macopeial movement toward more performance-based standards and the flexible monograph.
The proposed chapter explains how and why the perfor-mance-based approach would be applied in the heavy metal setting: “The selection of an instrumental technique and a procedure for the evaluation of the inorganic impurities specified in Table 1 requires the evaluation of a large number of variables including, among others, sensitivity, precision, accuracy, compatibility, time, and cost. The method selected may include plasma spectroscopy, atomic absorption spec-troscopy, or any other method that displays requisite accu-racy (trueness and uncertainty) and established sensitivity and specificity.”
To demonstrate this compliance, the selected procedure must provide measurement values within 20% of the certified con-centration for each element using the USP reference standard. The proposed chapter defines the default approach if another procedure is not selected or the performance criteria is not met.
At the USP scientific meeting in Kansas City, USP advi-sory panel member Nancy Lewen (Bristol-Myers Squibb) explained that her panel decided against mandating specific analytical approaches “to provide analysts with greater flex-ibility and eliminate the need to purchase equipment they might not have.”
She also explained that the intent was not for manufactur-ers to have to test all 31 of the metals in the current table. It was expected that the number on the list would be pared down, she explained, and that USP would provide guidance to help manufacturers “test only for those elements that are pertinent to their products.” She also recognized that there was limited toxicological data on most metals, and that the IOM meeting discussions showed that getting toxicologists
38 NOVEMBER/DECEMBER 2008

InsIde The Global ReGulaToRy dIaloGue™
InternatIonal PharmaceutIcal QualIty
to agree on limits or safe levels is “very difficult.” Further, she noted, the limits can and will need to change as more knowl-edge is gained.
Recognizing the uncertainties and differing opinions around heavy metal toxicology and safe limits, USP committee members have been considering hold-ing an international conclave of the regulatory bodies involved to move the dialogue forward.
During the wrap-up session at the annual scientific meeting, Williams expressed support for the idea, noting that “with-out that, I think we are going to be hard-pressed to move forward to something official.” USP Chief Science Officer Darrell Abernethy concurred that “this has to be a collabora-tive activity that we are involved in.” He confirmed that it will “be an open process,” and USP will seek “the fullest par-ticipation” of all stakeholders in the dialogue.
Industry consultant Dennis Runser, an adjunct faculty member at the University of Wisconsin and active on USP committees, cautioned on the need for the pharmacopeia and FDA in establishing standards for any contaminants to be very mindful of the impact on the “entire world popula-tion.” The decisions need to be “transparent” based on the best safety and efficacy information available rather than on technology capabilities so that they are clearly understood and can be applied globally, he asserted.
USP General Chapters VP Anthony DeStefano responded that USP fully appreciates this point, stressing that the “guid-ing principle is not how low can one get, because that does in fact lead us down a very bad path.”
Along with heavy metals, the dialogue on progress-ing other impurity standards also continued at USP’s Kansas City meeting. Separate sessions of the two-day impurities track focused on: • degradation products and impurity control in APIs and drug products • the compendial and regulatory implications of the hepa-rin, melamine and glycerin adulterations • and the cur-rent issues and developments around residual solvents and • genotoxic impurities.
Addressing the first breakout session on impurity control, Eli Lilly expert Mark Argentine explained how quality by design (QbD) is being used in methods development, from very broad screening methods to tightly controlled QC lab methods (IPQ Sept./Oct. 2008).
The “broad issue” that Argentine’s presentation raised, DeStefano commented in summarizing the session, is “what actually gets submitted to USP. If it is a very narrow control method rather than a broader screening method, what is its applicability to other companies when they pick it up and go to verify it?” The dilemma for USP, he explained, is that “the tighter the method is focused on the process, the more work that it takes to verify that it will work across processes. The broader the screening method is, the more likely it is that it will work in a formulation different from the one for which it was originally intended.”
The impurity control discussions at the meeting, in general, highlighted the question of “how much verification is needed when applying USP methods for new uses.”
As USP develops performance-based monographs and chap-ters, DeStefano stressed, “this is going to be more and more of an issue… that we will obviously need to deal with – just what safe harbor does a USP method give you and how do you interpret that safe harbor?” The issue of verification of methods will need to be closely considered with industry help in the effort to make the expectations clearer, he said.
Implementation of Concern For solvents
Verification issues have been very alive in the context of implementing USP’s new standards on residual solvents.
The residual solvent dialogue has underscored the point that the challenge is not just developing inter-nationally acceptable standards but assuring their common interpretation and implementation by regu-lators in both their marketing application and GMP review processes.
After a careful and lengthy vetting process through the inter-national stakeholder community, USP’s new chapter <467> on residual solvents became official in July 2008. The chapter incorporates the concepts and three-tier classification system based on solvent toxicity provided in ICH’s 1997 residual sol-vent guideline Q3C. The chapter applies to drug substances, excipients and products, and states that it is only necessary to test for solvents used in the course of the manufacture or purification of one of these.
In August, FDA issued additional guidance on the application of <467> in NDA and ANDA filings. Problems surfaced when the Office of Generic Drugs (OGD) began rejecting applica-tions that reviewers maintained did not contain enough data on lower risk residual solvents or did not adequately verify
NOVEMBER/DECEMBER 2008 39

InternatIonal PharmaceutIcal QualIty
www.IPQPubs.com
the supplier statements or certificates of analysis regarding compliance with the new USP chapter.
Feeling that the USP standards were being misapplied, industry quickly formed a coalition of associations to respond to the problem. The group submitted written com-ments and met with the agency on October 10.
OGD responded quickly to the industry concerns. In late October, “after carefully considering these com-ments and suggestions,” OGD issued a Q&A paper, in which it provided “clarifications” and a “flexible, stepwise approach to the application of USP <467> to ANDAs.”
Supplier qualification was a key industry concern – what type of “verification” information was needed and how much should be included in applications. Taking a more QbD/quality systems perspective, the industry coalition maintained generally that the focus should be on the con-trols that are used as opposed to testing, and that “the information to demonstrate compliance should typically be kept at the drug manufacturing site and assessed by FDA through GMP inspections rather than have to be filed with regulatory submissions.”
OGD’s response to the verification question in its Q&A paper is reflective of the industry point of view (see box at right). Other of the industry concerns addressed in the Q&A are: • the information that should be submitted to demonstrate compliance with USP <467> • what the excip-ient manufacturer’s statement should contain, and • how the requirements are applicable depending on when the ANDA or supplement was/is being submitted.
InTeRnaTIonal PhaRmaceuTIcal QualITy™ (ISSN 1937-6898) is published by IPQ
six times per year with the support of PDA.
For subscription information, please visit us on the web at www.ipqpubs.com
© 2008. All rights reserved. Parenteral Drug Association, Inc., 4350 East West
Hwy., Suite 150, Bethesda, MD, 20814. content cannot be photocopied, stored
or transmitted by magnetic or electronic means. Authorization to photocopy
items for internal or personal use is granted by IPQ when the fee of $2.00
(U.S.) per copy of each page is paid directly to Copyright Clearance Center,
222 Rosewood Dr., Danvers, MA 01923, USA (+1 978-750-8400). Violation of
copyright will result in legal action, including civil and/or criminal penalties,
and suspension of service.
InTeRnaTIonal
PhaRmaceuTIcal
QualITy
Editor-in-ChiefBill [email protected]
IPQ7920 Norfolk Ave., Ste. 900Bethesda, MD 20814
HoW CAn An AnDA sPonsoR VeRIFY eXCIPIent MAnUFACtUReR stAteMents on ResIDUAL
soLVents?
In its recent Q&A on residual solvent expectations for ANDA applicants, the Office of Generic Drugs clarified how an ANDA sponsor can verify excipient manufacturer statements as follows:
For each drug product excipient, an ANDA sponsor can choose either of two approaches:
1. The ANDA sponsor tests the residual solvents as a part of the complete testing protocol in order to demonstrate the capa-bility to perform the tests and to verify the excipient manu-facturer’s data for each identified residual solvent. Once the excipient manufacturer’s data is validated and verified, the ANDA sponsor can implement a valid vendor validation pro-gram as per 21 CFR 211.84(d)(2). The ANDA sponsor should submit complete COAs for all excipients, including residual solvent data, in ANDAs and applicable supplemental submis-sions to demonstrate verification and compliance with USP <467>.
2. As an alternative, excipient manufacturers or ANDA sponsors can submit evidence that the level of understanding and con-trol of the manufacturing process are sufficient to conclude that the acceptance criteria will always be met provided the process is run within the range of the critical parameters.
An excipient manufacturer’s statement that solvents are not used does not require the ANDA sponsor’s verification.