Embed Size (px)
Citation preview

…in an academic collaboration with
ISRCTN 51125379ISRCTN 51125379
www.dtu.ox.ac.uk/4-Twww.dtu.ox.ac.uk/4-T
4-T Design4-T Design Collaborative academic and pharmaceutical study
Three-year, multi-centre trial of addition of anlogue insulin to oral hypoglycaemic agents in 700 patients with Type 2 diabetes
Open-label, three arm comparison of:
Basal insulin, given once (or twice) daily
Prandial insulin, given three times daily
Biphasic insulin, given twice daily
50 secondary-care based UK clinical centres
Funded by Novo Nordisk
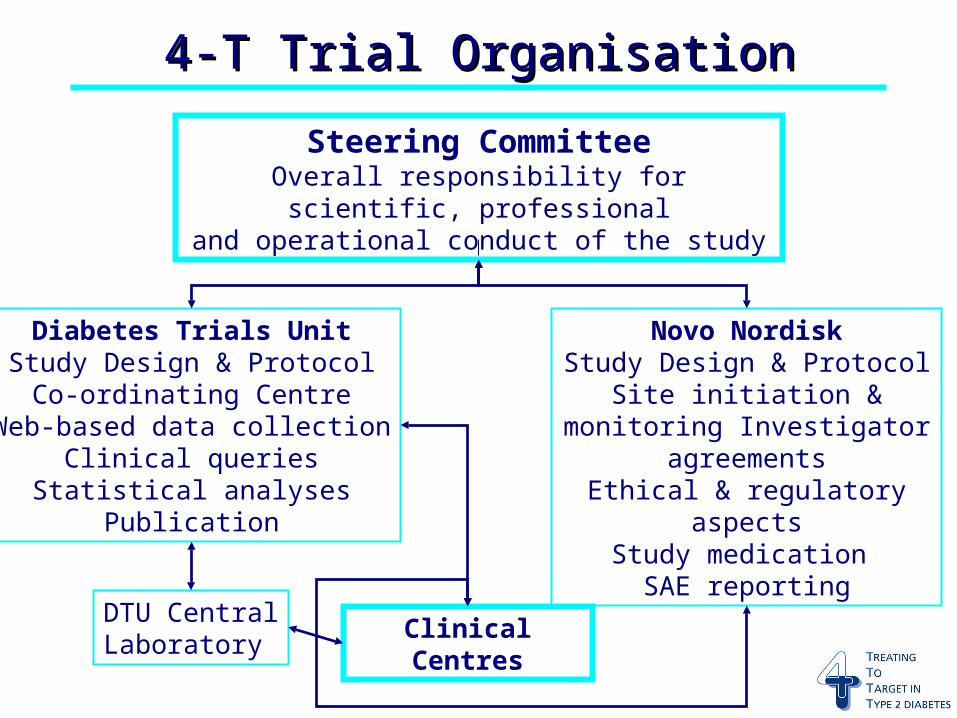
Steering CommitteeOverall responsibility for scientific, professional
and operational conduct of the study
Diabetes Trials UnitStudy Design & Protocol
Co-ordinating CentreWeb-based data collection
Clinical queriesStatistical analyses
Publication
Novo NordiskStudy Design & Protocol
Site initiation & monitoring Investigator agreements
Ethical & regulatory aspectsStudy medication
SAE reporting
DTU CentralLaboratory
Clinical Centres
4-T Trial Organisation4-T Trial Organisation
Steering Committee RemitSteering Committee RemitMain decision-making body of the Study
Responsible for protocol design
Ensure overall scientific, professional and operational conduct
Review performance of clinical centres, co-ordinating centre, central laboratory and centre monitors on a monthly basis
Steering Committee MembershipSteering Committee Membership Professor Rury Holman (Chair) Dr Jonathan Levy (Co-chair) Dr Andrew Farmer (Academic GP) Ms Joanne Keenan (DTU Project Manager)
Dr Melanie Davies (Independent Diabetologist) Mr George Nelson (Patient Representative)
Dr Alan McDougall (Novo Nordisk) Dr Henrik Schou (Novo Nordisk) Dr Mari-Anne Gall (Novo Nordisk)
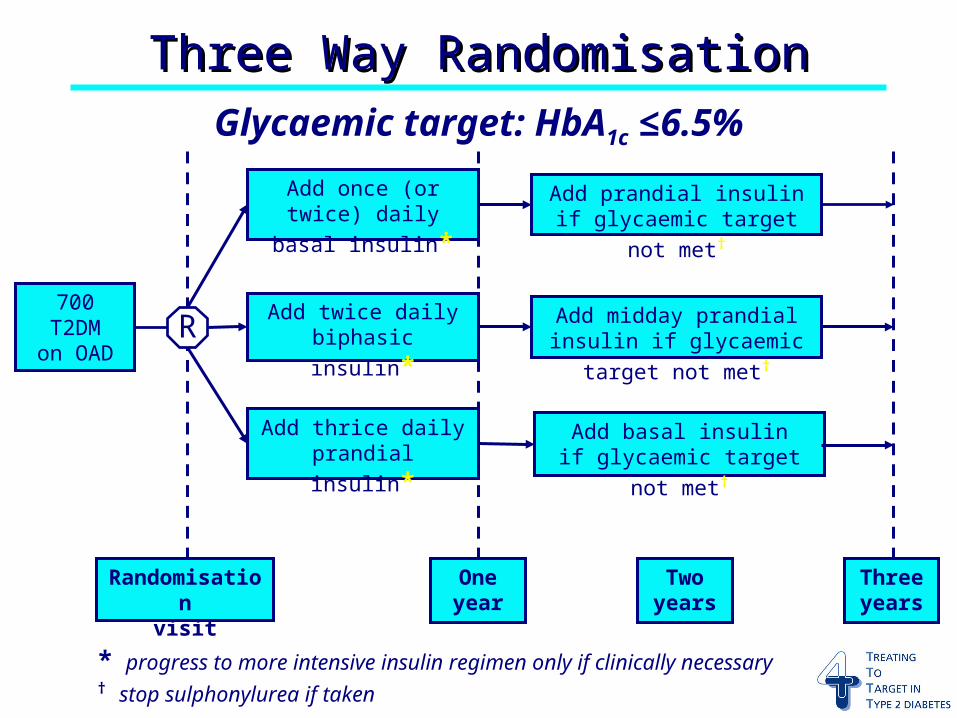
Three Way RandomisationThree Way Randomisation
700 T2DMon OAD
Add twice daily
biphasic insulin*
Add once (or twice)
daily basal insulin*
Add thrice daily
prandial insulin*
Randomisationvisit
Oneyear
* progress to more intensive insulin regimen only if clinically necessary† stop sulphonylurea if taken
Glycaemic target: HbA1c ≤6.5%
R Add midday prandial insulin
if glycaemic target not met†
Add prandial insulin
if glycaemic target not met†
Add basal insulin
if glycaemic target not met†
Twoyears
Threeyears
4-T Main Study Objectives4-T Main Study ObjectivesImpact of adding a single insulin preparation to OHA
Ability of the three different analogue insulin preparations to achieve good glycaemic control, defined as HbA1C levels ≤ 6.5 %, evaluated over 12 months
Need for more complex insulin regimensLonger term efficacy and durability of the three insulin preparations, as well as the need for a second analogue insulin preparation to be added in order to achieve good glycaemic control, evaluated in the second and third years of the study
Insulin dose calculatorStudy data will be used to derive algorithms that estimate individual insulin requirements, starting doses and titration steps
Major Inclusion CriteriaMajor Inclusion Criteria Aged ≥18 years, male and female
Type 2 diabetes for at least 12 months
On maximal tolerated doses of metformin and sulphonylurea for at least four months
Body mass index ≤40 kg/m2
HbA1c 7.0 % to 10.0 % inclusive
Written informed consent
Major Exclusion CriteriaMajor Exclusion Criteria Taking insulin therapy
Taking oral antidiabetic therapy other than sulphonylurea and/or metformin
Plasma creatinine >130 µmol/L
ALT ≥2x upper limit of normal
Life threatening cardiovascular disease
Participation in a clinical drug trialwithin the last three months
Lactating or potentially pregnant females
Primary Outcome and Sample SizePrimary Outcome and Sample Size The primary objective is to compare the HbA1c
levels achieved by the three insulin regimens Formal analyses will be performed at one year
and at three years, without adjustment for multiple comparisons, as the two phases of the study are regarded as separate experiments
4-T has 95% power to show equivalence between groups at the 5% level of significance if 233 patients per group are randomised, assuming an HbA1c standard deviation of 1.1 and a dropout rate that does not exceed 15%
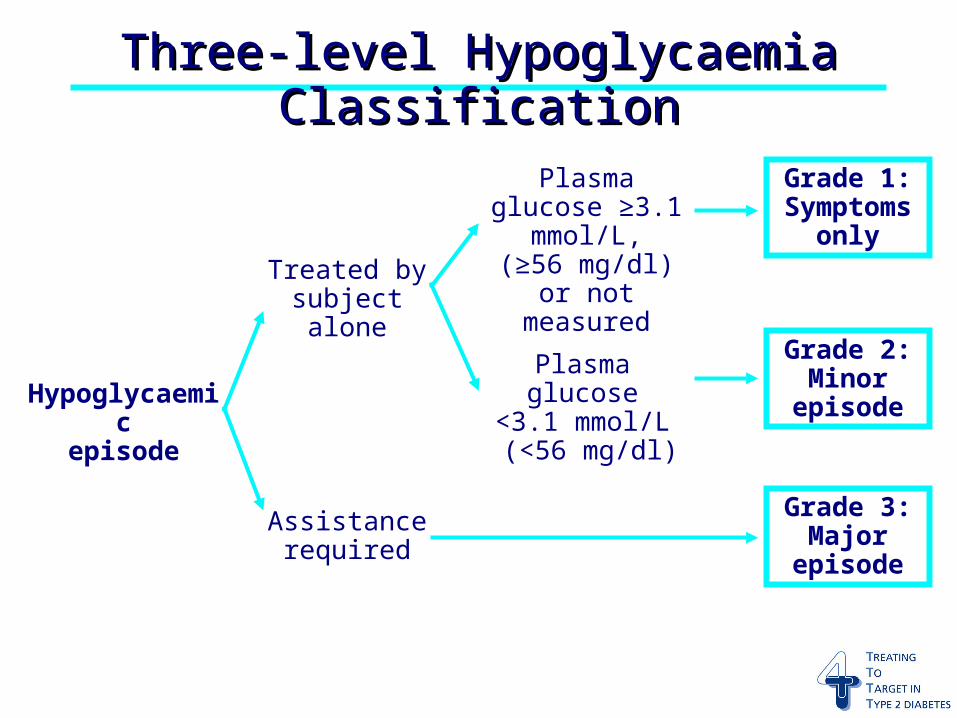
Three-level Hypoglycaemia ClassificationThree-level Hypoglycaemia Classification
Hypoglycaemicepisode
Plasma glucose ≥3.1 mmol/L,(≥56 mg/dl)
or not measured
Grade 1:Symptoms
onlyTreated by
subject alone
Grade 3:Major
episode
Assistancerequired
Plasma glucose<3.1 mmol/L (<56 mg/dl)
Grade 2:Minor
episode
Safety AssessmentsSafety Assessments Incidence of major hypoglycaemic episodes
Incidence of unexpected and/orserious adverse events (SAEs)
Plasma ALT, creatinine and lipid levels
Stop metformin if plasma creatinine ≥150 µmol/L
Blood pressure
The study commenced 1st November 2004
50 UK centres have been enrolled
18 patients per centre will be recruited
One year results expected in 2007
Three year results expected in 2009
ScheduleSchedule
Co-ordinating CentreCo-ordinating Centre
First point of contact/triage for all queries
Email: [email protected]
Phone: 01865 857 239
Fax: 01865 857 248
Web site: www.dtu.ox.ac.uk/4-T