Embed Size (px)
Citation preview
AUGUST 2014�CANCER DISCOVERY | 889
Infl ammatory Myofi broblastic Tumors Harbor Multiple Potentially Actionable Kinase Fusions Christine M. Lovly 1 , Abha Gupta 2 , Doron Lipson 3 , Geoff Otto 3 , Tina Brennan 3 , Catherine T. Chung 4 , Scott C. Borinstein 5 , Jeffrey S. Ross 3,6 , Philip J. Stephens 3 , Vincent A. Miller 3 ,and Cheryl M. Coffi n 7
RESEARCH BRIEF
ABSTRACT Infl ammatory myofi broblastic tumor (IMT) is a neoplasm that typically occurs in
children. The genetic landscape of this tumor is incompletely understood and thera-
peutic options are limited. Although 50% of IMTs harbor anaplastic lymphoma kinase ( ALK) rearrange-
ments, no therapeutic targets have been identifi ed in ALK-negative tumors. We report for the fi rst time
that IMTs harbor other actionable targets, including ROS1 and PDGFRβ fusions. We detail the case of
an 8-year-old boy with treatment-refractory ALK-negative IMT. Molecular tumor profi ling revealed
a ROS1 fusion, and he had a dramatic response to the ROS1 inhibitor crizotinib. This case prompted
assessment of a larger series of IMTs. Next-generation sequencing revealed that 85% of cases evalu-
ated harbored kinase fusions involving ALK, ROS1, or PDGFRβ. Our study represents the most compre-
hensive genetic analysis of IMTs to date and also provides a rationale for routine molecular profi ling of
these tumors to detect therapeutically actionable kinase fusions.
SIGNIFICANCE: Our study describes the most comprehensive genomics-based evaluation of IMT to
date. Because there is no “standard-of-care” therapy for IMT, the identifi cation of actionable genomic
alterations, in addition to ALK, is expected to redefi ne management strategies for patients with this
disease. Cancer Discov; 4(8); 889–95. ©2014 AACR.
See related commentary by Le and Doebele, p. 870.
1 Department of Medicine, Vanderbilt University, Nashville, Tennessee. 2 Division of Hematology/Oncology, The Hospital for Sick Children, Uni-versity of Toronto, Toronto, Canada. 3 Foundation Medicine, Cambridge, Massachusetts. 4 Division of Pathology, The Hospital for Sick Children, Uni-versity of Toronto, Toronto, Canada. 5 Department of Pediatrics, Vanderbilt University, Nashville, Tennessee. 6 Albany Medical College, Albany, New York. 7 Department of Pathology, Microbiology, and Immunology, Vanderbilt University, Nashville, Tennessee.
Note: Supplementary data for this article are available at Cancer Discovery Online (http://cancerdiscovery.aacrjournals.org/).
Corresponding Author: Christine M. Lovly, Vanderbilt University School of Medicine, 2220 Pierce Avenue South, 777 Preston Research Building, Nashville, TN 37232-6307. Phone: 615-936-3457; Fax: 615-343-2973; E-mail: [email protected]
doi: 10.1158/2159-8290.CD-14-0377
©2014 American Association for Cancer Research.
INTRODUCTION
Infl ammatory myofi broblastic tumor (IMT) is a rare mes-
enchymal tumor that can occur at any age, but has a predi-
lection for children, adolescents, and young adults ( 1 ). An
estimated 150 to 200 new cases are diagnosed annually in
the United States ( 2 ). These soft-tissue tumors can occur at
multiple anatomic sites, but most commonly involve the lung,
abdomen/pelvis, and retroperitoneum. The mainstay of
treatment for IMT is surgical resection; however, treatment
on July 7, 2018. © 2014 American Association for Cancer Research. cancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst May 29, 2014; DOI: 10.1158/2159-8290.CD-14-0377

890 | CANCER DISCOVERY�AUGUST 2014 www.aacrjournals.org
Lovly et al.RESEARCH BRIEF
options are limited for patients with unresectable and/or
advanced disease.
IMTs are diagnosed pathologically using criteria estab-
lished by the World Health Organization (WHO; ref. 3 ).
These tumors are characterized histologically by a spindle
myofi broblastic cell proliferation with a lymphoplasmacytic
infl ammatory infi ltrate ( 4 ). Approximately 50% of IMTs are
positive for anaplastic lymphoma kinase (ALK) expression
by IHC. The most common mechanism of ALK expression
and activation involves structural rearrangements in the ALK
gene, leading to the formation of a chimeric fusion protein.
Several ALK fusion partners have been identifi ed retrospec-
tively ( 5 ), as tumor sequencing is not yet the standard of care
for IMTs. ALK fusions have been validated as a therapeutic
target. A patient with a RANBP2–ALK- positive IMT had a
partial response to the ALK tyrosine kinase inhibitor (TKI)
crizotinib, whereas a patient whose IMT lacked an ALK fusion
did not respond to this agent ( 6 ).
In contrast, actionable genomic alterations have not yet
been described in the 50% of IMT samples that are negative
for ALK by IHC. ALK-negative IMTs may be more aggres-
sive with a higher frequency of metastasis compared with
ALK-positive IMT ( 7 ). Little is known on the genomic level
about potential oncogenic drivers in this subset of IMTs and,
as such, there are no targeted therapies available for these
patients.
Here, we describe the case of an 8-year-old boy with
treatment-refractory ALK-negative IMT. Targeted next-gener-
ation sequencing (NGS)–based genomic profi ling identifi ed
the presence of a ROS1 kinase fusion within his tumor. On
the basis of this fi nding, he was treated with the ROS1/ALK/
MET TKI, crizotinib, and experienced rapid symptomatic
improvement and signifi cant decrease in his tumor burden.
This case prompted us to perform genomic analysis on a
larger series of this rare tumor. Our data show for the fi rst
time that kinase fusions are found in the majority of IMTs.
These data not only offer insight into this disease but also
provide a rationale for routine molecular profi ling to detect
therapeutically actionable kinase fusions and thereby offer
patients rational therapeutic strategies with existing TKIs
based on the genomic profi le of the tumor.
RESULTS Case Report
A 6-year-old boy presented with a 1-year history of cough
and fatigue. Imaging demonstrated the presence of a large
left-sided chest mass. Biopsy of the mass revealed IMT, nega-
tive for ALK expression by standard clinical IHC and for
ALK rearrangement by break-apart FISH. The tumor was
deemed unresectable due to its intimate association with the
pulmonary vein, aorta, and esophagus. At the time of diag-
nosis, his laboratory parameters were indicative of a micro-
cytic anemia and an infl ammatory state. Several treatment
regimens were administered, including anti-infl ammatory
agents (naproxen, corticosteroids, and indomethacin) as well
as cytotoxic chemotherapy (methotrexate–vinorelbine), over
the course of 24 months (Supplementary Fig. S1), with
no antitumor response and minimal improvement of his
anemia. While he was receiving methotrexate–vinorelbine,
we performed targeted NGS-based genomic profi ling of his
tumor using formalin-fi xed and paraffi n-embedded (FFPE)
tissue and surprisingly detected a TFG–ROS1 fusion ( Fig. 1A ).
ROS1 TKIs, such as crizotinib, have proven to be an effec-
tive therapeutic strategy in lung cancers harboring ROS1
kinase fusions ( 8, 9 ). Therefore, he was treated with crizotinib
(250 mg), obtained through a compassionate access program,
twice daily orally. He experienced grade 1 diarrhea and visual
disturbance, both of which resolved with no dose reduction.
Within 3 cycles of crizotinib therapy, he symptomatically
felt better, with decreased cough and signifi cantly increased
energy. Imaging studies revealed, for the fi rst time since diag-
nosis, a decrease in the size of his tumor mass ( Fig. 1B ). Nota-
bly, his hemoglobin (Hgb) and mean corpuscular volume
(MCV) rapidly increased and his erythrocyte sedimentation
rate (ESR) decreased ( Fig. 1C and Supplementary Table S1).
He has now been on crizotinib for 4 months with excellent
tolerance, improved quality of life, and continued decrease in
his tumor burden.
Patient and Tumor Characteristics In an effort to further characterize cases of both ALK-
positive and ALK-negative IMT, we obtained 37 samples from
33 patients with this rare disease ( Table 1 ). Patients ranged
in age from infancy (less than 1 year old) to age 41. As is
typical for IMT, the tumors arose at multiple anatomic loca-
tions, including thorax, mesentery, peritoneum, and bladder.
The pathologic diagnosis was established based on criteria
according to the WHO classifi cation ( 3 ). ALK IHC was com-
pleted on each sample as part of the standard pathologic
evaluation (Supplementary Methods). Eleven of 37 (30%) of
the cases were ALK IHC negative and 26 of 37 (70%) of the
cases were ALK IHC positive.
Targeted NGS Identifi ed ALK, ROS1, and PDGFRb Tyrosine Kinase Fusions in a Collection of IMT Samples
We hypothesized that further insight into the biology of
known fusions as well as discovery of novel kinase fusions
would provide new therapeutic targets to treat patients with
IMT. To address this hypothesis, we analyzed genomic DNA
from all 37 IMT samples using a targeted NGS-based assay
(FoundationOne), which assesses 3,769 exons of 287 cancer
genes and 47 introns of 19 commonly rearranged genes,
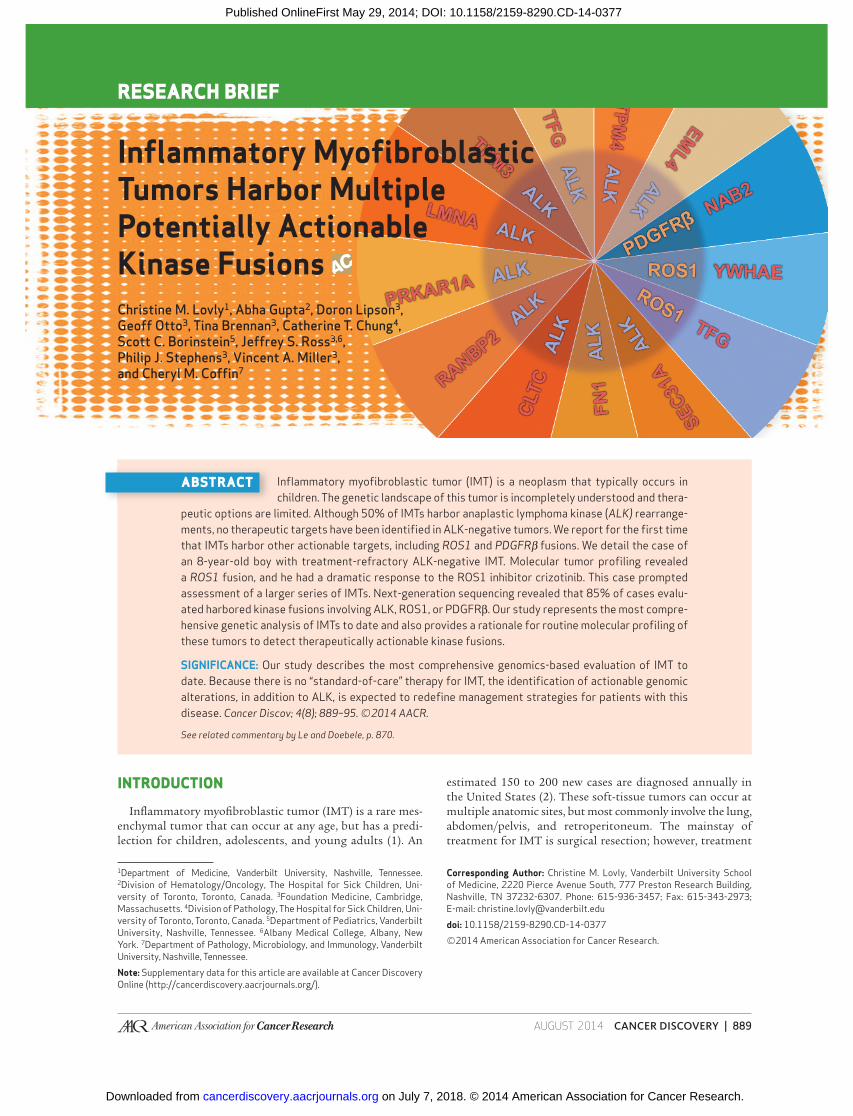
Figure 1. Response to crizotinib in an 8-year-old boy with refractory IMT harboring a TFG–ROS1 fusion. A, schematic representation of the TFG–ROS1 fusion. ROS1 is located on chromosome 6q22 and TFG is located on 3q12. The breakpoint occurs in-frame between exon 4 of TFG and exon 36 of ROS1 . B, CT scans before the initiation of crizotinib (left) and after 3 cycles of crizotinib (right) showing dramatic reduction in the tumor mass within the left lung. C, changes in Hgb, MCV, and ESR over the course of the patient’s treatments. Arrows below the graphs, initiation of the indicated therapies. The high (H) and low (L) limits of normal for each measured parameter are indicated on the blue graphs.
on July 7, 2018. © 2014 American Association for Cancer Research. cancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst May 29, 2014; DOI: 10.1158/2159-8290.CD-14-0377
AUGUST 2014�CANCER DISCOVERY | 891
Multiple Actionable Kinase Fusions in IMT RESEARCH BRIEF
Pre-crizotinib After 3 cycles of crizotinib
Hemoglobin (g/L)
MCV (fL)
ESR (mm/hr)
TFG (chr3)
ROS1 exons 35-43
ROS1 (chr6)
TFG exons 1-4
TFG–ROS1 fusion
ATG
ATG
ATG
5
35
chr4: 1,808,677
chr6: 117,643,755
A
B
C
g/L
fLm
m/h
162.5
150.0
137.5
125.0
112.5
100.0
87.575.0
100959085807570656055
125
100
75
50
25
0Jul Oct Jan 12 Jul Oct Jan 14Apr Jul Oct Jan 13 Apr
Steroid
pulse
Methotrexate
+ vinorelbine
Crizotinib
(11/20/2013)
on July 7, 2018. © 2014 American Association for Cancer Research. cancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst May 29, 2014; DOI: 10.1158/2159-8290.CD-14-0377
892 | CANCER DISCOVERY�AUGUST 2014 www.aacrjournals.org
Lovly et al.RESEARCH BRIEF
Sample ID Age (years) Gender Tumor site Tumor size (cm) ALK IHC Kinase fusion detected Coverage
L1 14 F Mesentery 7 Neg No fusion detected 252
L2 16 F Mesentery 3 Neg No fusion detected 102
L3 22 F Buttock 10 Neg YWHAE–ROS1 a 497
L4 22 F Pelvis Unknown Neg YWHAE–ROS1 a 676
L5 38 F Lung 3 Neg EML4–ALK 607
L6 8 M Mesentery 6 Neg TFG–ROS1 179
L7 12 F Peritoneum >10 Neg NAB2–PDGFRβ 424
L8 5 M Lung 5 Neg No fusion detected 383
L9 41 M Nasopharynx 5 Neg TPM3–ALK 460
L10 12 F Peritoneum Unknown Neg NAB2–PDGFRβ a 147
L11 6 M Omentum 14 Pos RANBP2–ALK 475
L12 7 F Mesentery 11 Pos LMNA–ALK 461
L13 2 F Mesentery 10 Pos TPM3–ALK 121
L14 3 F Mesentery 8 Pos TPM4–ALK 211
L15 29 M Mesentery 18 Pos TPM4–ALK 602
L16 36 F Lung 7 Pos No fusion detected 598
L17 13 M Lung 3 Pos Fail
L18 2 M Bladder 5 Pos No fusion detected 341
L19 11 F Lung 2 Pos EML4–ALK 485
L20 7 M Mesentery 14 Pos TPM3–ALK 569
L21 20 F Mesentery 8 Pos TPM3–ALK 491
L22 1 M Mesentery 2 Pos Fail
L23 6 F Lung 2 Pos SEC31A–ALK a 1,008
L24 4 M Mesentery 10 Pos Fail
L25 14 M Pelvis 8 Pos TFG–ALK a 844
L26 26 F Bladder 3 Pos FN1–ALK a , b 511
L27 26 F Bladder 7 Pos CLTC–ALK 459
L28 14 M Mesentery 41 Pos CLTC–ALK 326
L29 8 F Bladder 3 Pos FN1–ALK a , b 1,235
L30 10 M Mesentery 8 Pos Fail
L31 9 F Lung Unknown Pos CLTC–ALK 822
L32 4 F Lung Unknown Pos CLTC–ALK 781
L33 4 F Lung Unknown Pos CLTC–ALK 721
L34 4 F Lung Unknown Pos CLTC–ALK 915
L35 <1 F Shoulder Unknown Pos PRKAR1A–ALK 813
L36 9 F Lung Unknown Pos CLTC–ALK 849
L37 6 M Lung 10.1 Neg TFG–ROS1 660
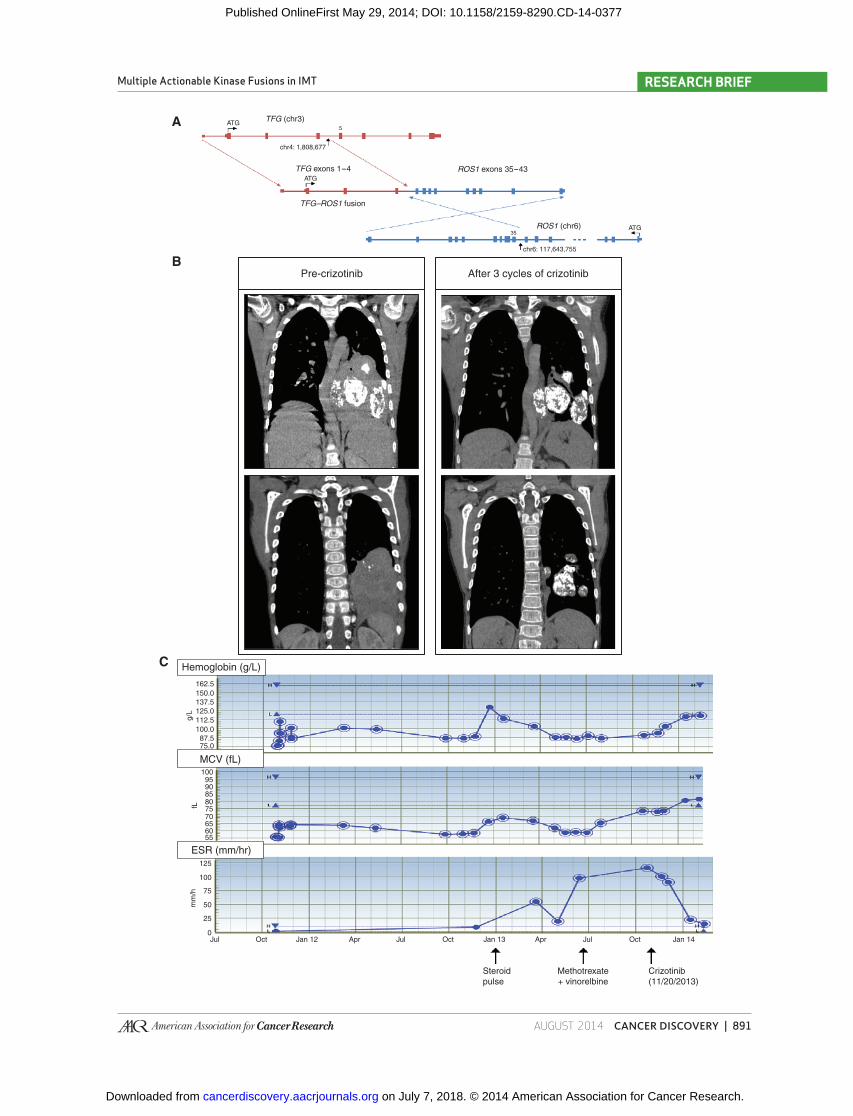
NOTE: A total of 37 FFPE tumor samples from 33 different patients with IMT were included in the analysis. The following samples were obtained from the same patient at different times in his/her disease course: L3/L4, L7/L10, L31/L36, L32/L33/L34. There was 100% concordance in the kinase fusions detected across multiple samples from the same patient. a Suffi cient material was available to verify these kinase fusions with RNA sequencing. b Initial results from the FoundationOne genomic DNA analysis were negative. The FN1–ALK fusion, which harbors an atypical breakpoint within intron 18 of ALK , was detected by RNA sequencing.
Table 1. Summary of clinical characteristics and targeted NGS results for the study cohort
on July 7, 2018. © 2014 American Association for Cancer Research. cancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst May 29, 2014; DOI: 10.1158/2159-8290.CD-14-0377
AUGUST 2014�CANCER DISCOVERY | 893
Multiple Actionable Kinase Fusions in IMT RESEARCH BRIEF
including 8 tyrosine kinases (Supplementary Table S2). This
platform has been previously described and successfully used
in several large genomic studies of various tumor types
( 10–12 ). In each case, tumor DNA was isolated from FFPE
tissue. Average coverage was 543×. Targeted NGS was success-
fully performed in 22 of 26 ALK-positive and 11 of 11 ALK-
negative specimens ( Table 1 and Supplementary Fig. S2). In
cases in which there was suffi cient tumor material available,
the kinase fusions were verifi ed with RNA sequencing.
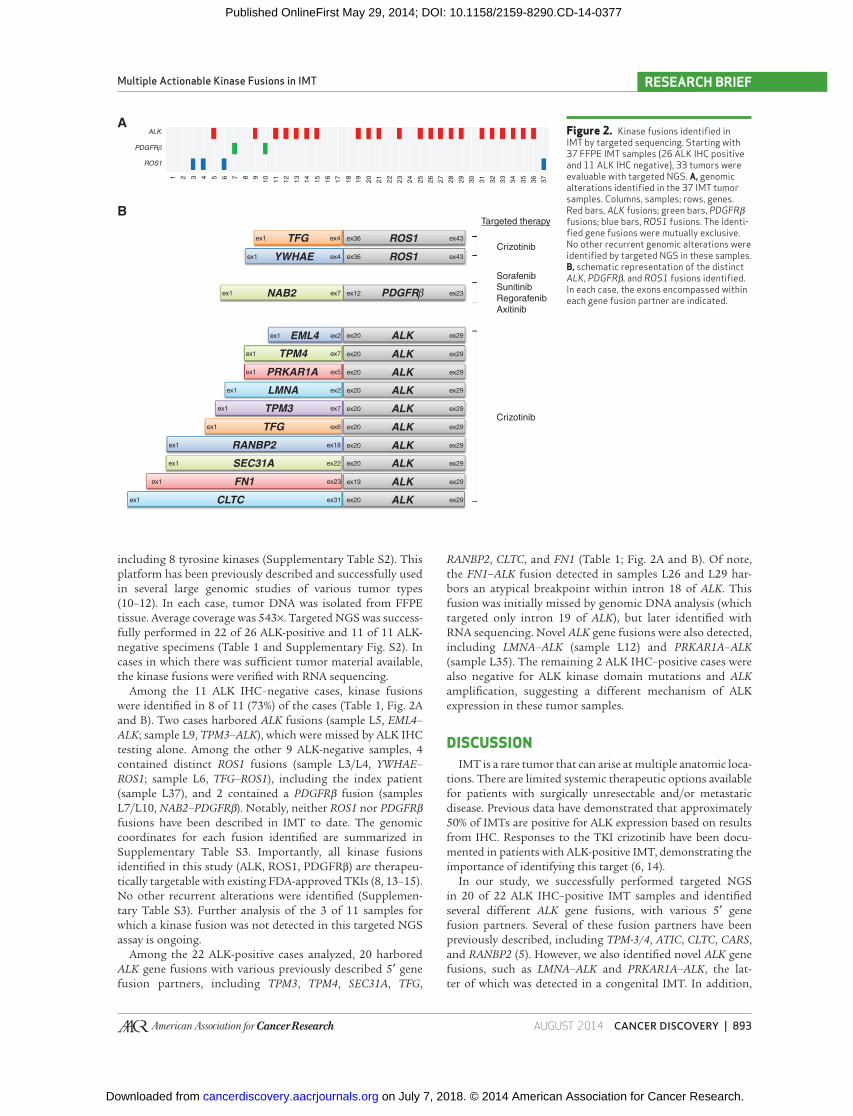
Among the 11 ALK IHC–negative cases, kinase fusions
were identifi ed in 8 of 11 (73%) of the cases ( Table 1 , Fig. 2A
and B ). Two cases harbored ALK fusions (sample L5, EML4–
ALK ; sample L9, TPM3–ALK ), which were missed by ALK IHC
testing alone. Among the other 9 ALK-negative samples, 4
contained distinct ROS1 fusions (sample L3/L4, YWHAE–
ROS1 ; sample L6, TFG–ROS1 ), including the index patient
(sample L37), and 2 contained a PDGFRβ fusion (samples
L7/L10, NAB2–PDGFRβ ). Notably, neither ROS1 nor PDGFRβ fusions have been described in IMT to date. The genomic
coordinates for each fusion identifi ed are summarized in
Supplementary Table S3. Importantly, all kinase fusions
identifi ed in this study (ALK, ROS1, PDGFRβ) are therapeu-
tically targetable with existing FDA-approved TKIs ( 8 , 13–15 ).
No other recurrent alterations were identifi ed (Supplemen-
tary Table S3). Further analysis of the 3 of 11 samples for
which a kinase fusion was not detected in this targeted NGS
assay is ongoing.
Among the 22 ALK-positive cases analyzed, 20 harbored
ALK gene fusions with various previously described 5′ gene
fusion partners, including TPM3 , TPM4 , SEC31A , TFG ,
RANBP2 , CLTC , and FN1 ( Table 1 ; Fig. 2A and B ). Of note,
the FN1–ALK fusion detected in samples L26 and L29 har-
bors an atypical breakpoint within intron 18 of ALK . This
fusion was initially missed by genomic DNA analysis (which
targeted only intron 19 of ALK ), but later identifi ed with
RNA sequencing. Novel ALK gene fusions were also detected,
including LMNA–ALK (sample L12) and PRKAR1A–ALK
(sample L35). The remaining 2 ALK IHC–positive cases were
also negative for ALK kinase domain mutations and ALK
amplifi cation, suggesting a different mechanism of ALK
expression in these tumor samples.
DISCUSSION IMT is a rare tumor that can arise at multiple anatomic loca-
tions. There are limited systemic therapeutic options available
for patients with surgically unresectable and/or metastatic
disease. Previous data have demonstrated that approximately
50% of IMTs are positive for ALK expression based on results
from IHC. Responses to the TKI crizotinib have been docu-
mented in patients with ALK-positive IMT, demonstrating the
importance of identifying this target ( 6 , 14 ).
In our study, we successfully performed targeted NGS
in 20 of 22 ALK IHC–positive IMT samples and identifi ed
several different ALK gene fusions, with various 5′ gene
fusion partners. Several of these fusion partners have been
previously described, including TPM-3/4 , ATIC , CLTC , CARS ,
and RANBP2 ( 5 ). However, we also identifi ed novel ALK gene
fusions, such as LMNA–ALK and PRKAR1A–ALK , the lat-
ter of which was detected in a congenital IMT. In addition,
Figure 2. Kinase fusions identifi ed in IMT by targeted sequencing. Starting with 37 FFPE IMT samples (26 ALK IHC positive and 11 ALK IHC negative), 33 tumors were evaluable with targeted NGS. A, genomic alterations identifi ed in the 37 IMT tumor samples. Columns, samples; rows, genes. Red bars, ALK fusions; green bars, PDGFRβ fusions; blue bars, ROS1 fusions. The identi-fi ed gene fusions were mutually exclusive. No other recurrent genomic alterations were identifi ed by targeted NGS in these samples. B, schematic representation of the distinct ALK , PDGFRβ , and ROS1 fusions identifi ed. In each case, the exons encompassed within each gene fusion partner are indicated.
A
B
1
ALK
ROS1
PDGFRβ
2 3 4 5 6 7 8 9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
Targeted therapy
Crizotinib
Sorafenib
Sunitinib
Regorafenib
Axitinib
Crizotinib
TFGex1 ex4 ex36 ex43
ex36 ex43
ex12 ex23
ex20 ex29
ex20 ex29
ex1 ex4
ex1
ex1
ex1
ex1
ex1
ex1
ex1
ex1
ex1
ex1
ex1 ex31
ex23
ex22
ex18
ex6
ex7
ex2
ex5
ex7
ex2
ex7
ROS1
ROS1
ALK
ALK
ex20 ex29ALK
ex20 ex29ALK
ex20 ex29ALK
ex20 ex29ALK
ex20 ex29ALK
ex20 ex29ALK
ex19 ex29ALK
ex20 ex29ALK
PDGFRβ
YWHAE
NAB2
EML4
LMNA
TPM4
TPM3
TFG
CLTC
FN1
RANBP2
SEC31A
PRKAR1A
on July 7, 2018. © 2014 American Association for Cancer Research. cancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst May 29, 2014; DOI: 10.1158/2159-8290.CD-14-0377

894 | CANCER DISCOVERY�AUGUST 2014 www.aacrjournals.org
Lovly et al.RESEARCH BRIEF
we identifi ed ALK fusions with noncanonical fusion break-
points. FN1–ALK , which has previously been described in
ovarian cancer, has a breakpoint in intron 18 of the ALK gene,
whereas most fusions have a breakpoint in ALK intron 19
( 16 ). Because patients with tumors harboring intron 1 (exon
19) ALK fusions can derive clinical benefi t from ALK inhibi-
tor therapy ( 17 ), there is a need to incorporate these atypical
but recurrent fusions into NGS-based diagnostic platforms.
Notably, we also detected ALK fusions in 2 of 11 IMT samples
that tested negative for ALK expression by IHC. Therefore,
the possibility of targeted therapy with an ALK inhibitor
would have been missed for these patients with ALK testing
by IHC alone.
In contrast, there are currently no data about potential
oncogenic “drivers” in the ALK-negative subset of IMTs. We
identifi ed actionable kinase fusions in 8 of 11 ALK-negative
IMT tumors analyzed by targeted NGS, including ROS1 and
PDGFRβ kinase fusions, which have not yet been described in
this disease. PDGFRβ kinase fusions have been described in
myeloproliferative disorders ( 18 ). ROS1 kinase fusions have
been detected in a variety of malignancies, including lung
cancer, glioblastoma, cholangiocarcinoma, and Spitz tumors
(reviewed in ref. 19 ). Crizotinib, which is FDA approved for
the treatment of ALK fusion–positive lung cancer, is also a
potent ROS1 inhibitor. Preliminary results from the phase I
clinical trial of crizotinib in ROS1 fusion–positive lung cancer
demonstrated an objective response rate of 56% ( 9 ). However,
responses in other ROS1 fusion–positive cancers have not
yet been documented. Here, we report that a young boy with
ROS1 fusion–positive IMT responded to crizotinib. This was
the fi rst antitumor response this patient has experienced
since his initial diagnosis more than 2 years before starting
crizotinib; his tumor previously did not respond to four dif-
ferent lines of therapy, including cytotoxic chemotherapy or
anti-infl ammatory agents. His tumor mass decreased in size,
his paraneoplastic anemia improved, and he felt better symp-
tomatically. This case clearly illustrates the need for improved
diagnostic and therapeutic paradigms in this disease.
Overall, our data show for the fi rst time that kinase fusions
are found in the majority of IMTs (85% in our series). To our
knowledge, this study represents the largest genomic analy-
sis of this tumor type to date, and our results redefi ne this
heterogeneous disease as being largely a kinase fusion–driven
neoplasm. These data not only provide insight into this rare
disease but also offer rational targeted therapeutic strate-
gies with existing FDA-approved TKIs based on the genomic
profi le of the tumor. Critical to successful deployment of
this evolving therapeutic paradigm is incorporation of test-
ing with highly sensitive NGS platforms capable of detecting
both known and novel fusions in multiple oncogenes from a
single tumor specimen.
METHODS Patients and Tumor Samples
IMT samples and associated patient characteristics were analyzed
with an Institutional Review Board–approved protocol (#090572).
All clinical data were obtained and maintained according to Health
Insurance Portability and Accountability Act (HIPAA) standards. All
unique identifi ers have been removed before publication.
Genomic DNA Sequencing and Analysis DNA was extracted from FFPE samples. Sequencing was performed
for 3,769 exons of 287 cancer genes and 47 introns of 19 commonly
rearranged genes, including 8 tyrosine kinases (FoundationOne Panel;
Supplementary Table S2) as previously described ( 10 ). Tumor con-
tent was assessed by hematoxylin and eosin staining before analy-
sis; no micro/macro dissection tissue enrichment was performed.
Sequencing was performed on the HiSeq2000 instrument (Illumina)
with 40-bp paired reads to an average depth of 543X. Resultant
sequences were analyzed for base substitutions, insertions, deletions,
copy-number alterations, and select gene fusions ( 10 ). Additional
information about the analytic validation of this assay as well as the
sequencing of RNA is provided in the Supplementary Methods.
Disclosure of Potential Confl icts of Interest C.M. Lovly reports receiving a commercial research grant from
AstraZeneca, has received speakers’ bureau honoraria from Qiagen
and Abbott Molecular, and is a consultant/advisory board mem-
ber for Pfi zer. D. Lipson is director of and has ownership interest
(including patents) in Foundation Medicine. J.S. Ross is medical
director of, reports receiving a commercial research grant from, and
has ownership interest (including patents) in Foundation Medicine.
P.J. Stephens has ownership interest (including patents) in Founda-
tion Medicine, Inc. V.A. Miller is CMO of and has ownership interest
(including patents) in Foundation Medicine. No potential confl icts
of interest were disclosed by the other authors.
Authors’ Contributions Conception and design: C.M. Lovly, D. Lipson, J.S. Ross, C.M. Coffi n
Development of methodology: C.M. Lovly, D. Lipson, G. Otto,
T. Brennan, J.S. Ross, V.A. Miller, C.M. Coffi n
Acquisition of data (provided animals, acquired and managed
patients, provided facilities, etc.): C.M. Lovly, A. Gupta, C.T. Chung,
S.C. Borinstein, J.S. Ross, C.M. Coffi n
Analysis and interpretation of data (e.g., statistical analysis,
biostatistics, computational analysis): C.M. Lovly, D. Lipson,
J.S. Ross, P.J. Stephens, V.A. Miller, C.M. Coffi n
Writing, review, and/or revision of the manuscript: C.M. Lovly,
D. Lipson, C.T. Chung, S.C. Borinstein, J.S. Ross, P.J. Stephens,
V.A. Miller, C.M. Coffi n
Administrative, technical, or material support (i.e., reporting or
organizing data, constructing databases): C.M. Lovly, T. Brennan,
J.S. Ross, C.M. Coffi n
Study supervision: C.M. Lovly, C.M. Coffi n
Acknowledgments The authors thank Drs. Mace Rothenberg and Keith Wilner for
their assistance in obtaining crizotinib for the patient, Drs. William
Pao and Jeff Sosman for their critical review of this article, and Abudi
Nashabi for administrative assistance.
Grant Support This work was supported by the Richard and Valerie Aronsohn
Memorial Research Award from the Sarcoma Foundation of America
and by the Joyce Family Foundation. C.M. Lovly was additionally
supported by an NIH K12 training grant (K12 CA9060625) and a
Damon Runyon Clinical Investigator Award.
The costs of publication of this article were defrayed in part by
the payment of page charges. This article must therefore be hereby
marked advertisement in accordance with 18 U.S.C. Section 1734
solely to indicate this fact.
Received April 9, 2014; revised May 21, 2014; accepted May 21,
2014; published OnlineFirst May 29, 2014.
on July 7, 2018. © 2014 American Association for Cancer Research. cancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst May 29, 2014; DOI: 10.1158/2159-8290.CD-14-0377

AUGUST 2014�CANCER DISCOVERY | 895
Multiple Actionable Kinase Fusions in IMT RESEARCH BRIEF
REFERENCES 1. Gleason BC , Hornick JL . Infl ammatory myofi broblastic tumours:
where are we now? J Clin Pathol 2008 ; 61 : 428 – 37 .
2. Tothova Z , Wagner AJ . Anaplastic lymphoma kinase-directed ther-
apy in infl ammatory myofi broblastic tumors . Curr Opin Oncol
2012 ; 24 : 409 – 13 .
3. Coffi n CM , Fletcher JA . Infl ammatory myofi broblastic tumor . WHO
Classifi cation of Tumours of Soft Tissue and Bone . Lyon: IARC ;
2013 .
4. Coffi n CM , Patel A , Perkins S , Elenitoba-Johnson KS , Perlman E ,
Griffi n CA . ALK1 and p80 expression and chromosomal rearrange-
ments involving 2p23 in infl ammatory myofi broblastic tumor . Mod
Pathol 2001 ; 14 : 569 – 76 .
5. Takeuchi K , Soda M , Togashi Y , Sugawara E , Hatano S , Asaka R , et al.
Pulmonary infl ammatory myofi broblastic tumor expressing a novel
fusion, PPFIBP1-ALK: reappraisal of anti-ALK immunohistochem-
istry as a tool for novel ALK fusion identifi cation . Clin Cancer Res
2011 ; 17 : 3341 – 8 .
6. Butrynski JE , D’Adamo DR , Hornick JL , Dal Cin P , Antonescu CR ,
Jhanwar SC , et al. Crizotinib in ALK-rearranged infl ammatory myofi -
broblastic tumor . N Engl J Med 2010; 363 : 1727 – 33 .
7. Coffi n CM , Hornick JL , Fletcher CD . Infl ammatory myofi broblastic
tumor: comparison of clinicopathologic, histologic, and immunohis-
tochemical features including ALK expression in atypical and aggres-
sive cases . Am J Surg Pathol 2007 ; 31 : 509 – 20 .
8. Bergethon K , Shaw AT , Ou SH , Katayama R , Lovly CM , McDonald
NT , et al. ROS1 rearrangements defi ne a unique molecular class of
lung cancers . J Clin Oncol 2012 ; 30 : 863 – 70 .
9. Ou S , Bang YJ , Camidge DR , Riely GJ , Salgia R , Shapiro G , et al.
Effi cacy and safety of crizotinib in patients with advanced ROS1-
rearranged non-small cell lung cancer (NSCLC) . J Clin Oncol 2013 ;
31 (suppl; abstr 8032) .
10. Lipson D , Capelletti M , Yelensky R , Otto G , Parker A , Jarosz M , et al.
Identifi cation of new ALK and RET gene fusions from colorectal and
lung cancer biopsies . Nat Med 2012 ; 18 : 382 – 4 .
11. Vignot S , Frampton GM , Soria JC , Yelensky R , Commo F , Brambilla
C , et al. Next-generation sequencing reveals high concordance of
recurrent somatic alterations between primary tumor and metas-
tases from patients with non-small-cell lung cancer . J Clin Oncol
2013 ; 31 : 2167 – 72 .
12. Drilon A , Wang L , Hasanovic A , Suehara Y , Lipson D , Stephens P ,
et al. Response to cabozantinib in patients with RET fusion-positive
lung adenocarcinomas . Cancer Discov 2013 ; 3 : 630 – 5 .
13. Kwak EL , Bang YJ , Camidge DR , Shaw AT , Solomon B , Maki RG ,
et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung
cancer . N Engl J Med 2010 ; 363 : 1693 – 703 .
14. Mosse YP , Lim MS , Voss SD , Wilner K , Ruffner K , Laliberte J , et al.
Safety and activity of crizotinib for paediatric patients with refractory
solid tumours or anaplastic large-cell lymphoma: a Children’s Oncol-
ogy Group phase 1 consortium study . Lancet Oncol 2013 ; 14 : 472 – 80 .
15. David M , Cross NC , Burgstaller S , Chase A , Curtis C , Dang R , et al.
Durable responses to imatinib in patients with PDGFRB fusion gene-
positive and BCR-ABL-negative chronic myeloproliferative disorders .
Blood 2007 ; 109 : 61 – 4 .
16. Ren H , Tan ZP , Zhu X , Crosby K , Haack H , Ren JM , et al. Identifi ca-
tion of anaplastic lymphoma kinase as a potential therapeutic target
in ovarian cancer . Cancer Res 2012 ; 72 : 3312 – 23 .
17. Doebele RC , Pilling AB , Aisner D , Kutateladze TG , Le AT , Weickhardt AJ ,
et al. Mechanisms of resistance to crizotinib in patients with ALK gene
rearranged non-small cell lung cancer . Clin Cancer Res 2012 ; 18 : 1472 – 82 .
18. Cross NC , Reiter A . Fibroblast growth factor receptor and platelet-
derived growth factor receptor abnormalities in eosinophilic myelo-
proliferative disorders . Acta Haematol 2008 ; 119 : 199 – 206 .
19. Davies KD , Doebele RC . Molecular pathways: ROS1 fusion proteins
in cancer . Clin Cancer Res 2013 ; 19 : 4040 – 5 .
on July 7, 2018. © 2014 American Association for Cancer Research. cancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst May 29, 2014; DOI: 10.1158/2159-8290.CD-14-0377
2014;4:889-895. Published OnlineFirst May 29, 2014.Cancer Discovery Christine M. Lovly, Abha Gupta, Doron Lipson, et al. Actionable Kinase FusionsInflammatory Myofibroblastic Tumors Harbor Multiple Potentially
Updated version
10.1158/2159-8290.CD-14-0377doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerdiscovery.aacrjournals.org/content/suppl/2014/06/03/2159-8290.CD-14-0377.DC1
Access the most recent supplemental material at:
Cited articles
http://cancerdiscovery.aacrjournals.org/content/4/8/889.full#ref-list-1
This article cites 17 articles, 9 of which you can access for free at:
Citing articles
http://cancerdiscovery.aacrjournals.org/content/4/8/889.full#related-urls
This article has been cited by 13 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerdiscovery.aacrjournals.org/content/4/8/889To request permission to re-use all or part of this article, use this link
on July 7, 2018. © 2014 American Association for Cancer Research. cancerdiscovery.aacrjournals.org Downloaded from
Published OnlineFirst May 29, 2014; DOI: 10.1158/2159-8290.CD-14-0377