Embed Size (px)
Citation preview
Improving Patient Flow Through Applying Lean Concepts to
Emergency Department
Hossam Elamir, MSc.HCM, PGDip.TQM, MBBCh, CPHQQuality & Accreditation Directorate, MOH, Kuwait
UNIVERSITY OF TORONTOToronto, OntarioSeptember 7- 8, 2017
Outline
• What is Quality?• The Global Situation of EDOC• The Local Problem• Causes of EDOC• Lean Management• Evidence-based Solutions
What is Quality?
• Don’t kill me (no needless deaths)
• Do help me & don’t hurt me (no needless
pain)
• Don’t make me feel helpless
• Don’t keep me waiting
• Don’t waste resources - mine or anyone
else’s
Berwick, D. M. (2005)
The Global SituationFor the past two decades or more, emergency department
(ED) overcrowding (OC) and increased ED length of stay
(LOS) have been attracting increasing attention globally, as
they create serious clinical and financial repercussions as
well as threatening quality and safety. EDOC is a situation
where institutional resources available are insufficient to
meet the basic service needs of emergency patients.
Prolonged EDLOS was defined as 4 hours in the UK, 4-6
hours in Canada and 8 hours in Australia.
Some negative EDOC outcomes • LWBS (Left Without Being Seen) rates
• Patient mortality (7-day mortality, 10-day mortality, 30-day mortality)
• Adverse cardiac outcomes, e.g., dysrhythmias, cardiac arrest, etc.
• Care compromise rated by nurses, physicians, and patients
• Transport delays
• Treatment delays
• Low patient satisfaction
• Ambulance diversion/ Negative financial effect
The Local Problem: Snapshots• This situation continues
for days at the moment.
• According to one of ED
senior physicians: “What
is the meaning of
quality! The patient
died! We would save her live if she was transferred a little bit
earlier to inpatient.”
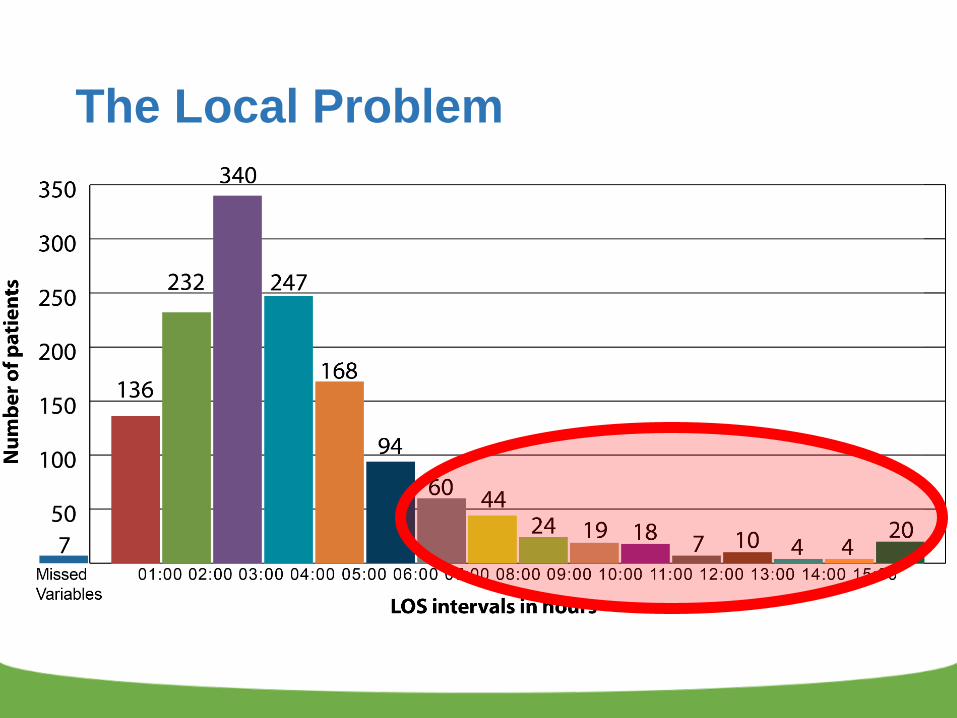
The Local Problem• Observation of all patients visited ED during 7 days
(27 Nov. – 3 Dec. 2014)• Design Capacity Total time=
35 X 7 = 245 bed days
245 X 24 hours = 5880 bed hours
The Local Problem
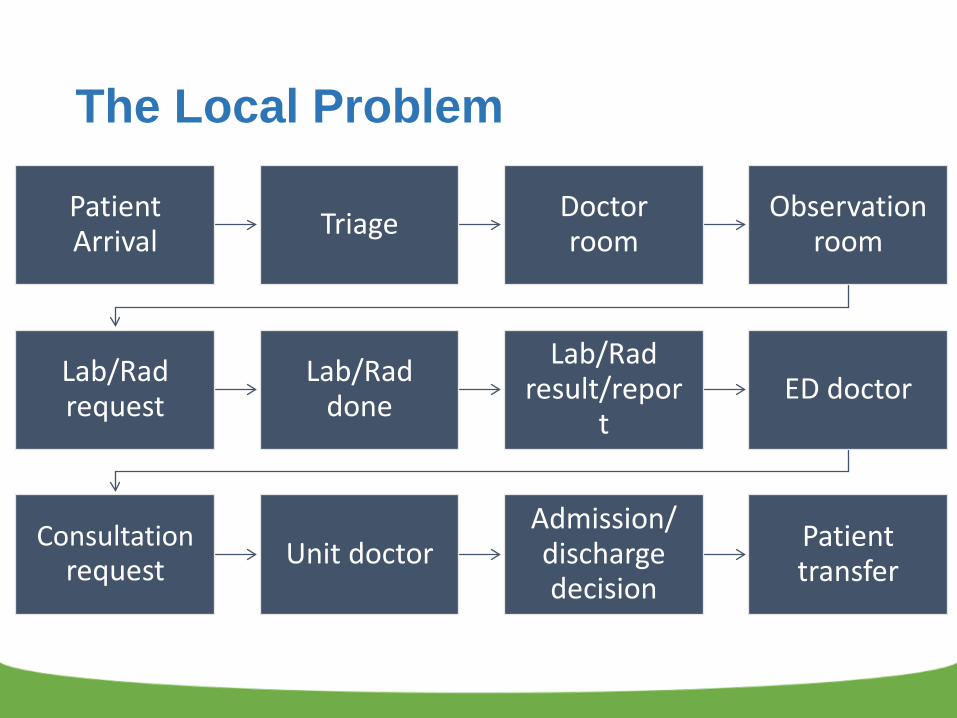
Patient Arrival Triage Doctor
roomObservation
room
Lab/Rad request
Lab/Rad done
Lab/Rad result/repor
tED doctor
Consultationrequest Unit doctor
Admission/ discharge decision
Patient transfer
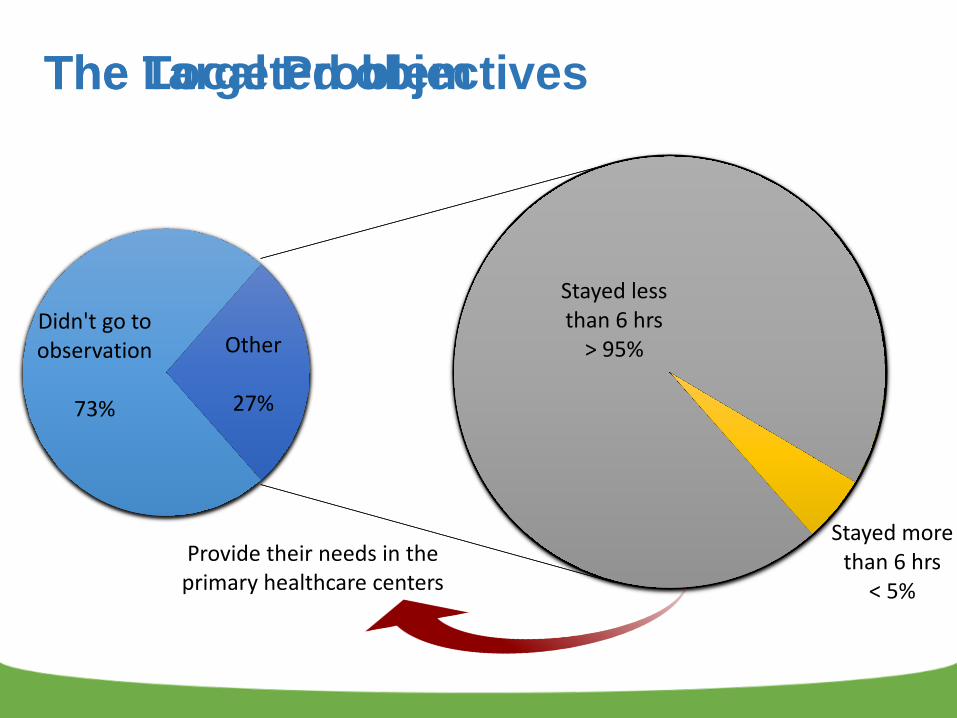
Total visits toED in 7 days
6383100%
Didn't go to observation
463373%
Shouldn't goto observation
31618%
Stayed lessthan 6 hrs
122470%
Stayed morethan 6 hrs
21012%
Other175027%
Didn't go to observation
73%
Stayed lessthan 6 hrs
> 95%
Stayed morethan 6 hrs
< 5%
Other
27%
Provide their needs in the primary healthcare centers
The Targeted objectivesThe Local Problem
The Local Problem
The Local Problem
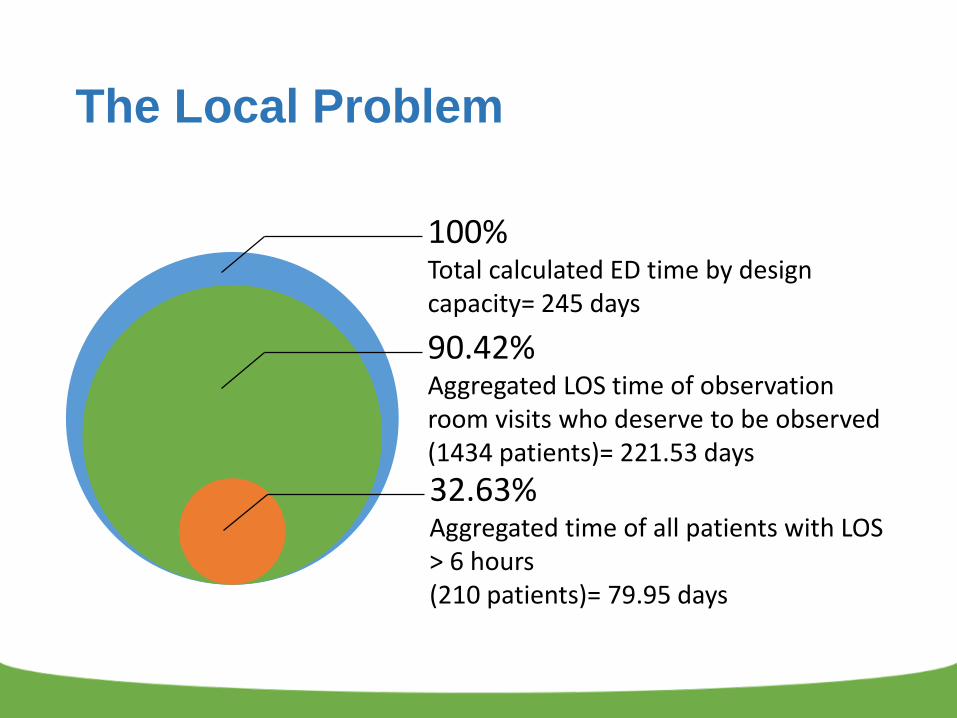
90.42%Aggregated LOS time of observation room visits who deserve to be observed(1434 patients)= 221.53 days
100%Total calculated ED time by designcapacity= 245 days
32.63%Aggregated time of all patients with LOS > 6 hours (210 patients)= 79.95 days
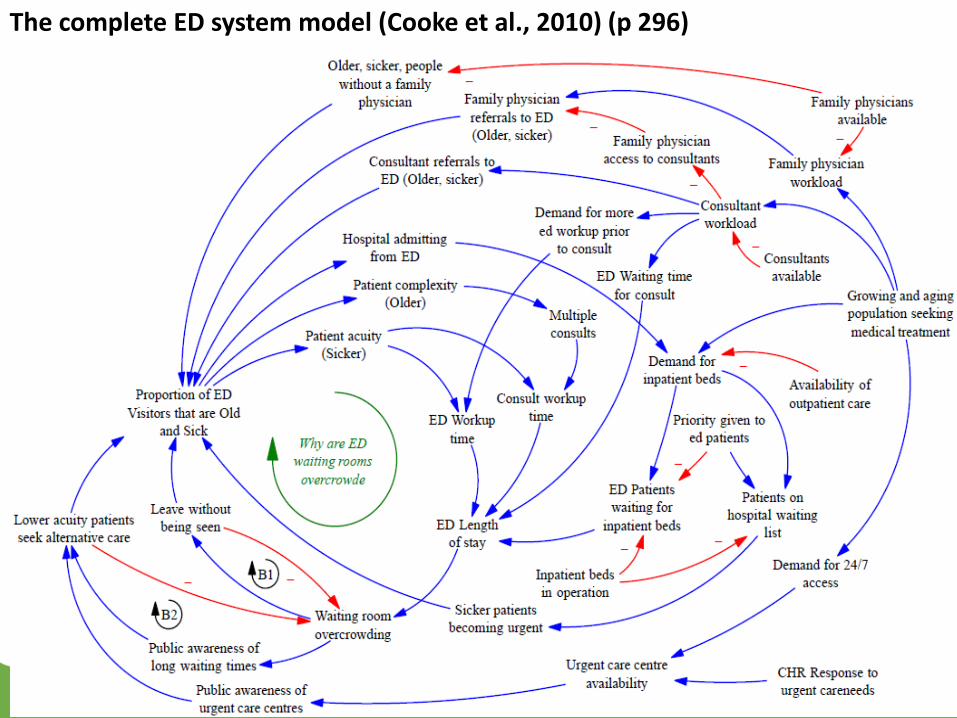
The complete ED system model (Cooke et al., 2010) (p 296)
Invaluable words
“For every complex problem,there’s a solution that issimple, neat, and wrong”
H L Mencken
Need Beds? Add Beds!
Current Beds Number
Beds number after expansion
Access block
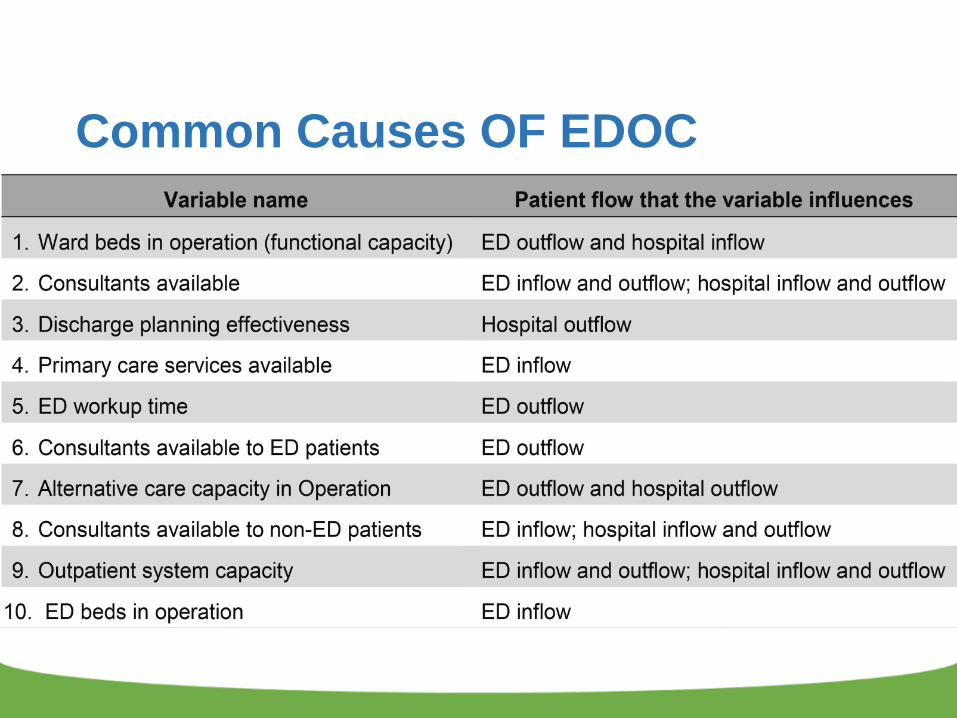
Common Causes OF EDOC
Lean Management (LM)
• LM: “……a management practice based on the
philosophy of continuously improving processes by
either increasing customer value or reducing non-
value adding activities (Muda), process variation
(Mura), and poor work conditions (Muri).” (p.365)
Radnor et al. (2012)
What is lean?
Vs
How does being lean affect your performance?
• One of the fittest athletes in the world
• His body fat is 3% less than supermodels
= 16
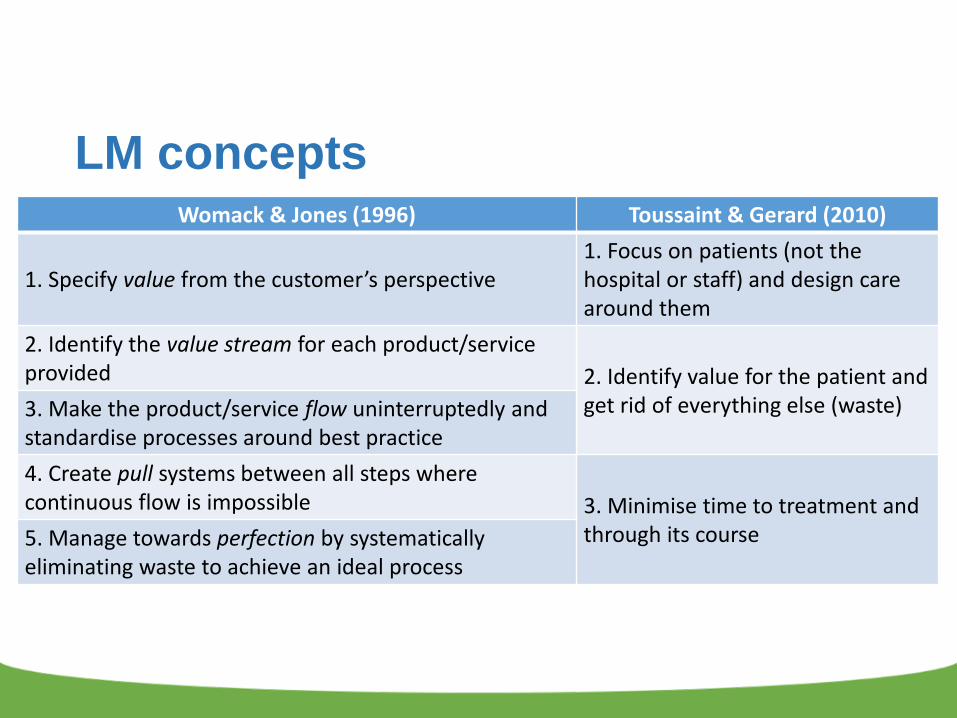
LM conceptsWomack & Jones (1996) Toussaint & Gerard (2010)
1. Specify value from the customer’s perspective1. Focus on patients (not the hospital or staff) and design care around them
2. Identify the value stream for each product/service provided 2. Identify value for the patient and
get rid of everything else (waste)3. Make the product/service flow uninterruptedly and standardise processes around best practice4. Create pull systems between all steps where continuous flow is impossible 3. Minimise time to treatment and
through its course5. Manage towards perfection by systematically eliminating waste to achieve an ideal process
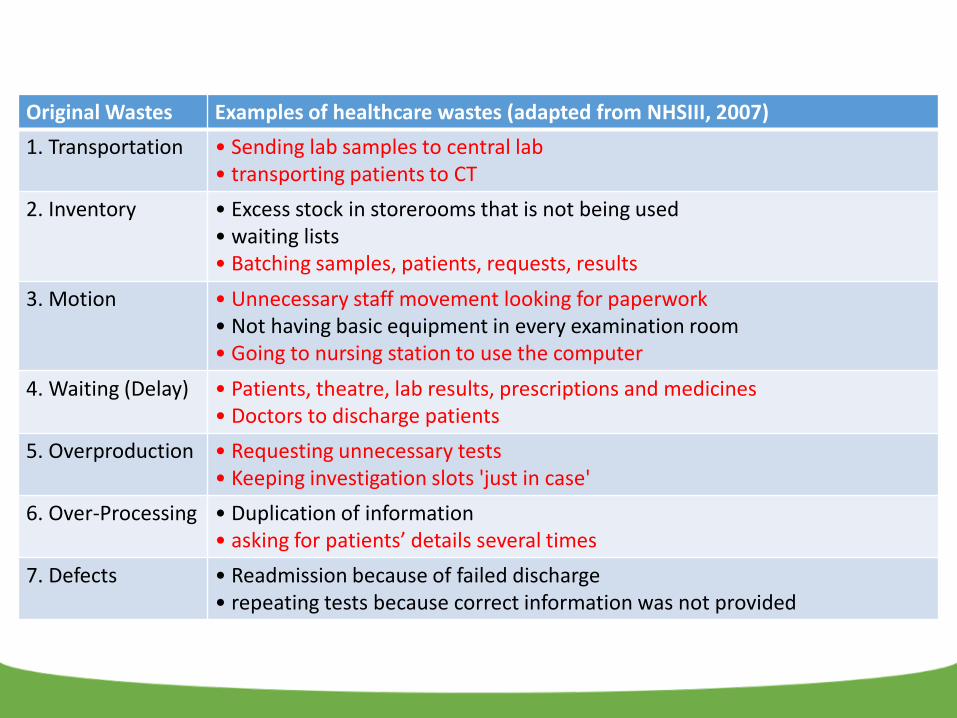
Original Wastes Examples of healthcare wastes (adapted from NHSIII, 2007)1. Transportation • Sending lab samples to central lab
• transporting patients to CT2. Inventory • Excess stock in storerooms that is not being used
• waiting lists• Batching samples, patients, requests, results
3. Motion • Unnecessary staff movement looking for paperwork• Not having basic equipment in every examination room• Going to nursing station to use the computer
4. Waiting (Delay) • Patients, theatre, lab results, prescriptions and medicines• Doctors to discharge patients
5. Overproduction • Requesting unnecessary tests• Keeping investigation slots 'just in case'
6. Over-Processing • Duplication of information • asking for patients’ details several times
7. Defects • Readmission because of failed discharge • repeating tests because correct information was not provided
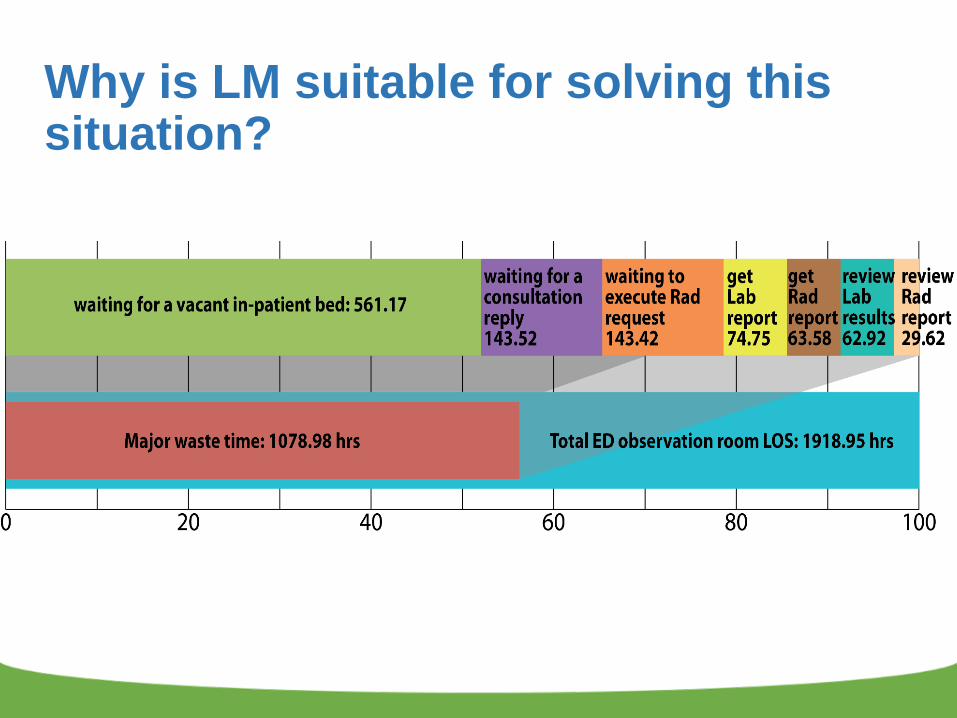
Why is LM suitable for solving this situation?
Evidence-based Solutions
• Inputs Solutions:• Ambulance diversion
• 1ry Healthcare centers to manage non-urgent cases (e.g.: catheter change, blood collection)
• Closed ED area with security
• Close the ED pharmacy
• Proper triaging
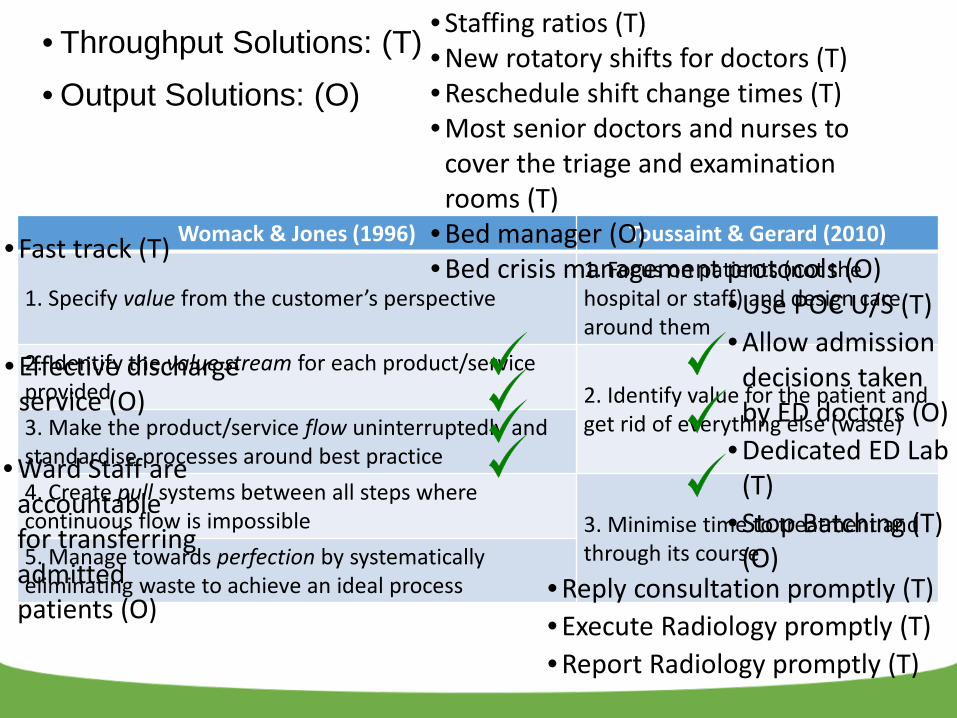
Womack & Jones (1996) Toussaint & Gerard (2010)
1. Specify value from the customer’s perspective1. Focus on patients (not the hospital or staff) and design care around them
2. Identify the value stream for each product/service provided 2. Identify value for the patient and
get rid of everything else (waste)3. Make the product/service flow uninterruptedly and standardise processes around best practice4. Create pull systems between all steps where continuous flow is impossible 3. Minimise time to treatment and
through its course5. Manage towards perfection by systematically eliminating waste to achieve an ideal process • Reply consultation promptly (T)
• Execute Radiology promptly (T)• Report Radiology promptly (T)
• Use POC U/S (T)• Allow admission
decisions taken by ED doctors (O)
• Dedicated ED Lab (T)
• Stop Batching (T) (O)
• Staffing ratios (T)• New rotatory shifts for doctors (T)• Reschedule shift change times (T)• Most senior doctors and nurses to
cover the triage and examination rooms (T)
• Bed manager (O)• Bed crisis management protocols (O)
• Effective dischargeservice (O)
• Fast track (T)
• Ward Staff are accountable for transferring admitted patients (O)
• Throughput Solutions: (T)• Output Solutions: (O)
Performance measures:
• EDLOS < 6 hrs
• Wait times < 20% of total EDLOS
• No patient boarded in ED > 45 mins
• Initiation of crisis protocols should be zero
• No increase in LWBS rates
• No increase in readmission rates
Bottom Line
• “Every system is perfectly designed
to get the results it gets.”
• "If we keep doing what we have
been doing, we'll keep getting
what we've always gotten"—an
expensive, high-tech, inefficient
health-care system.
P. Batalden
D. Berwick
References• Berwick, D. M. (2005), My right knee, Annals of Medicine
• ACEM. (2013) Policy on Standard Terminology. Melbourne, Australia: The Australasian College for Emergency Medicine
• Blum et al. (2006) Report From a Roundtable Discussion: Meeting the Challenge of Emergency Department Overcrowding/ Boarding. Washington, DC, USA: American College of Emergency Physicians
• Horwitz et al. (2010) US Emergency Department Performance on Wait Time and Length of Visit. Ann Emerg Med
• Radnor et al. (2012) Lean in healthcare: The unfilled promise? Soc Sci Med
References• Affleck et al. (2013) Emergency department overcrowding and
access block. CJEM
• Cooke et al. (2010) A dynamic model of the systemic causes for patient treatment delays in emergency departments. Journal of Modelling in Management
• Guttmann et al. (2011) Association between waiting times and short term mortality and hospital admission after departure from emergency department: population based cohort study from Ontario, Canada. BMJ.