Embed Size (px)
Citation preview
All Rights Reserved © 2016
Valley Health System & Dearborn Advisors, LLC®
Improving Patient Care with Meaningful Medication Therapy Alerts: A CASE STUDY IN ALERT FATIGUE REDUCTION
John Heeren, RPh, MSApplication Analyst, Pharmacy
David Troiano, RPh, MSIA, CPPSDirector of Service Development
All Rights Reserved © 2016
Session Description
2
Methodology used to analyze the initial state of alerts
Development of a program to address alerts
Approaches taken for each type of alert
Findings: quantitative and qualitative
Results achieved for each type of alert
Lessons Learned: adjustments made to the program
WE WILL COVER:
All Rights Reserved © 2016
Learning Objectives
3
IDENTIFY COMPONENTS
•
Describe the components of a successful Alert Fatigue Reduction Program including: •Governance•Analysis•Overall approach •Ongoing maintenance
IDENTIFY APPROACH
Describe the appropriate approach to analyze and address each type of alert
DEVELOP METHODOLOGY
Describe how MEDITECH and FDB product capabilities are employed to address each type of alert
All Rights Reserved © 2016
Valley Health System
4
Integrated Delivery Network
located in Ridgewood, NJ
451-bed Patient Centered Community Non-Profit hospital:
Valley Home Care
Valley Medical Group
Recipient of multiple awards:
J.D. Power and Associates Distinguished Hospital ProgramSM
– 9 years in a row
Magnet facility for nursing excellence since 2003
Leapfrog Top Hospital recipient with a Straight A Safety Score – 5 years in a row

All Rights Reserved © 2016
Dearborn Advisors, LLC®
5
Founded in 2001 Advisory Services
Focused on adoption by Clinicians to achieve the benefits of clinical systems investments
Services to address the continuum of needs throughout the lifecycle of clinical systems
Transformation for Value®
Clinical
Strategy and Value
Project Management
Implementation
All Rights Reserved © 2016
Presenter Backgrounds
6
John HeerenRPh, MS
Years CPOE Implementation/Support
Application Analyst, Pharmacy
Valley Health
Years with EHR Vendor
David TroianoRPh, MSIA, CPPS
Years with EHR Vendor
Years of Healthcare Consulting
Director of Service Development
Dearborn Advisors, LLC
All Rights Reserved © 2016
Background
7
“Upgrade” from MEDITECH Magic to 6.14 on 5/30/2015
Change of drug interaction DB from MediSpan To FDB
Go-Live went well but with numerous physician complaints about alerts
Pre Go-live Preparation: All controls within MEDITECH used:
• Suppressed alerts within order sets• Limited duplicate checking to individual items• Providers received only level 1,2 Severity, Pharmacists Level 1,2,3• Home Meds- DI checking for 2 days• Dose checking - Fully Utilized FDB Content to replace In-House version• Dc’d Orders- DI checking for 1 day
All Rights Reserved © 2016
Summary Of Med Alerts
8
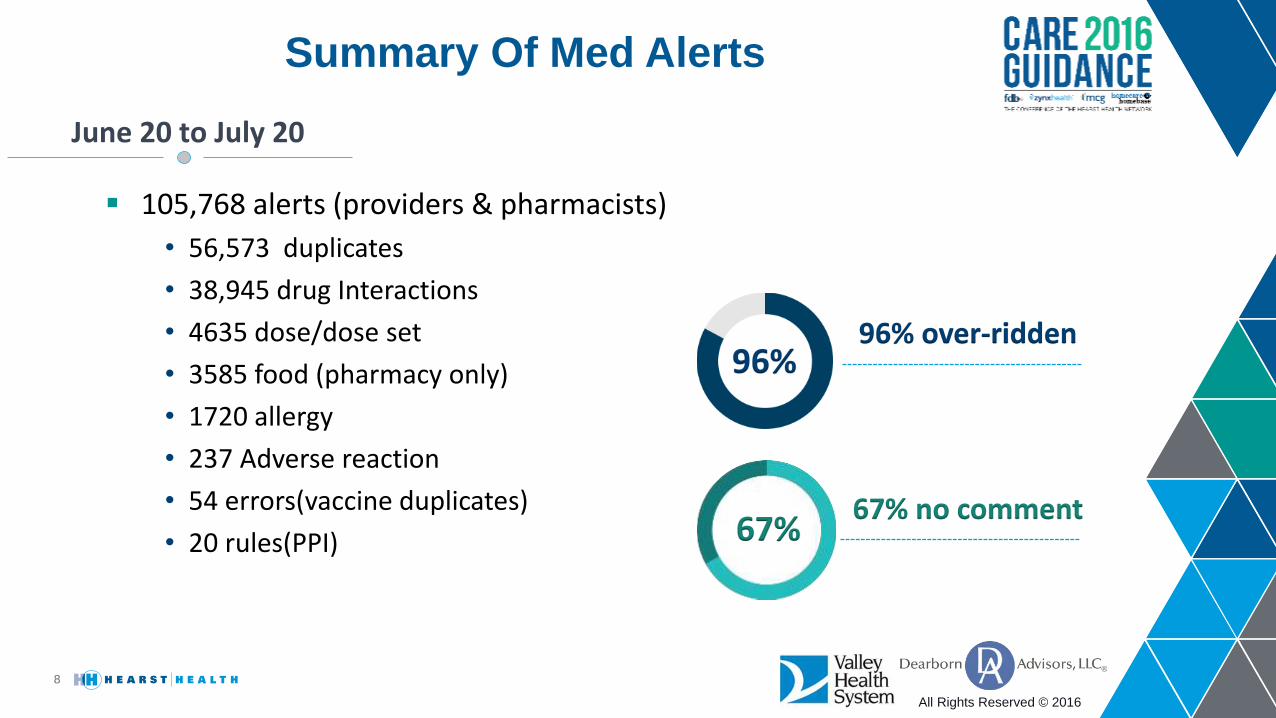
105,768 alerts (providers & pharmacists)
• 56,573 duplicates
• 38,945 drug Interactions
• 4635 dose/dose set
• 3585 food (pharmacy only)
• 1720 allergy
• 237 Adverse reaction
• 54 errors(vaccine duplicates)
• 20 rules(PPI)
June 20 to July 20
96% over-ridden
67% no comment
96%
67%
All Rights Reserved © 2016
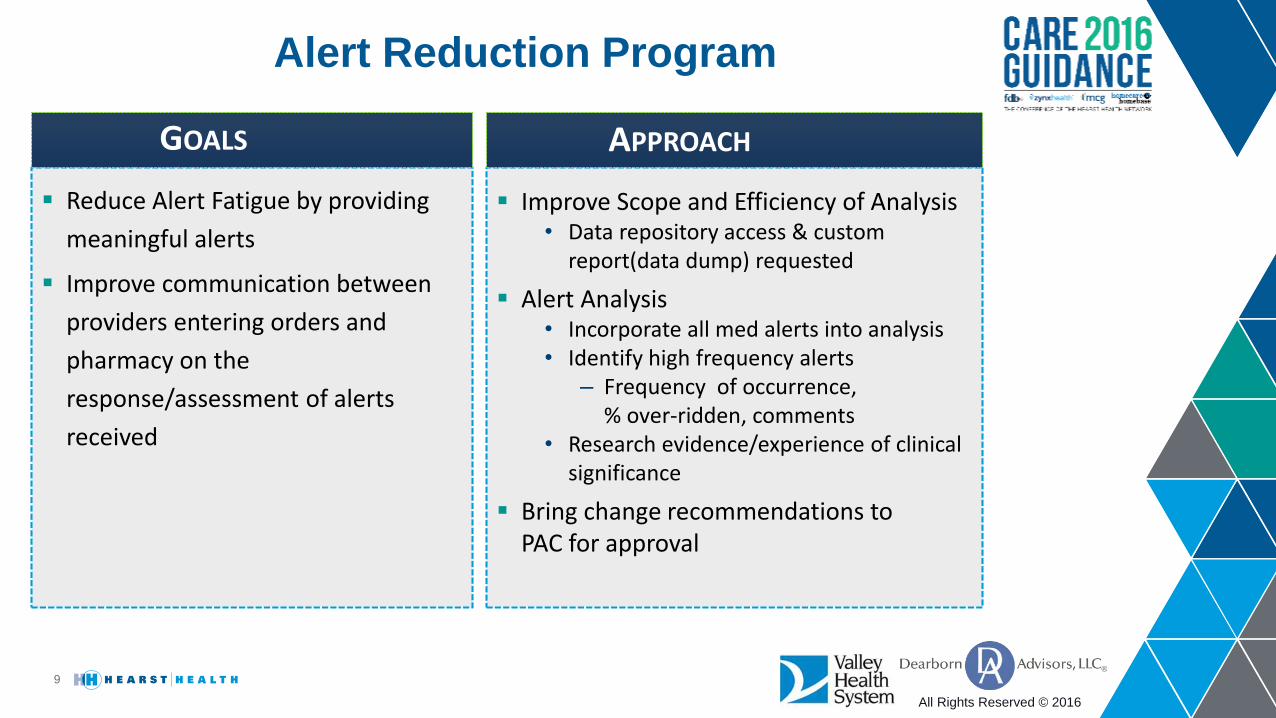
Alert Reduction Program
9
Reduce Alert Fatigue by providing
meaningful alerts
Improve communication between
providers entering orders and
pharmacy on the
response/assessment of alerts
received
GOALS
Improve Scope and Efficiency of Analysis• Data repository access & custom
report(data dump) requested
Alert Analysis• Incorporate all med alerts into analysis• Identify high frequency alerts
– Frequency of occurrence, % over-ridden, comments
• Research evidence/experience of clinical significance
Bring change recommendations to PAC for approval
APPROACH
All Rights Reserved © 2016
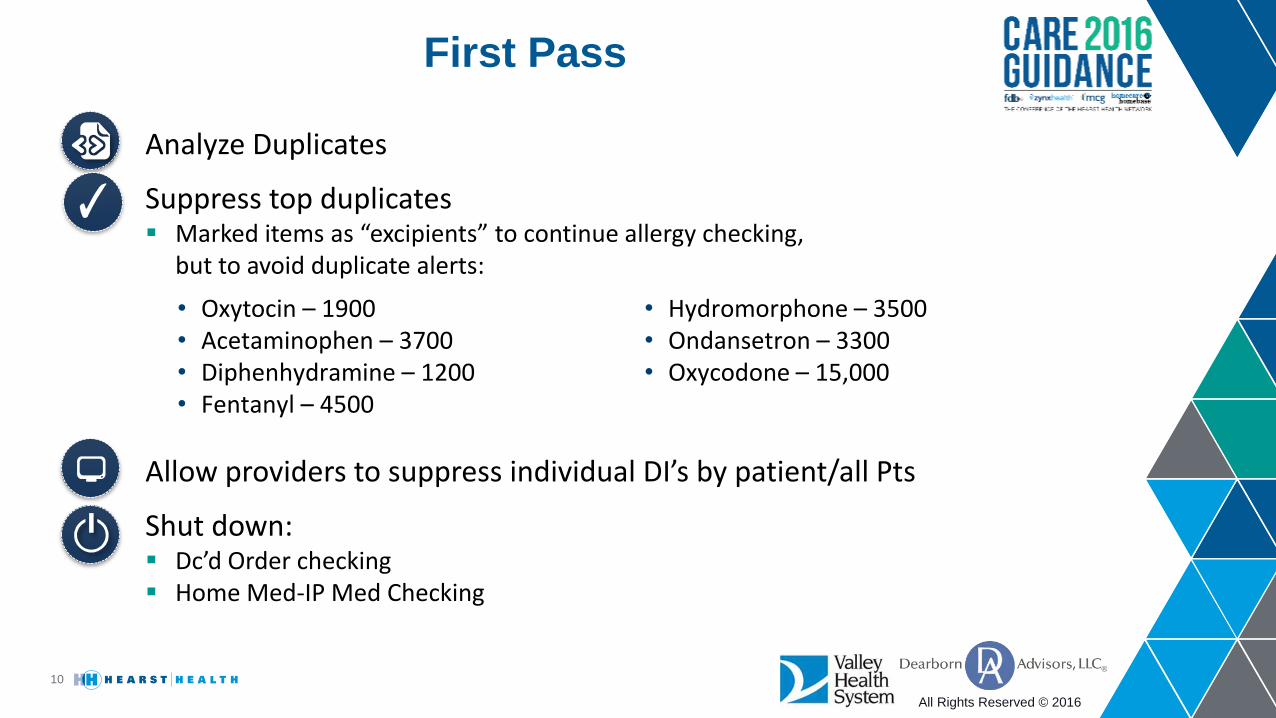
First Pass
10
Allow providers to suppress individual DI’s by patient/all Pts
Shut down: Dc’d Order checking Home Med-IP Med Checking
Analyze Duplicates
Suppress top duplicates Marked items as “excipients” to continue allergy checking,
but to avoid duplicate alerts:
• Oxytocin – 1900• Acetaminophen – 3700• Diphenhydramine – 1200• Fentanyl – 4500
• Hydromorphone – 3500• Ondansetron – 3300• Oxycodone – 15,000
All Rights Reserved © 2016
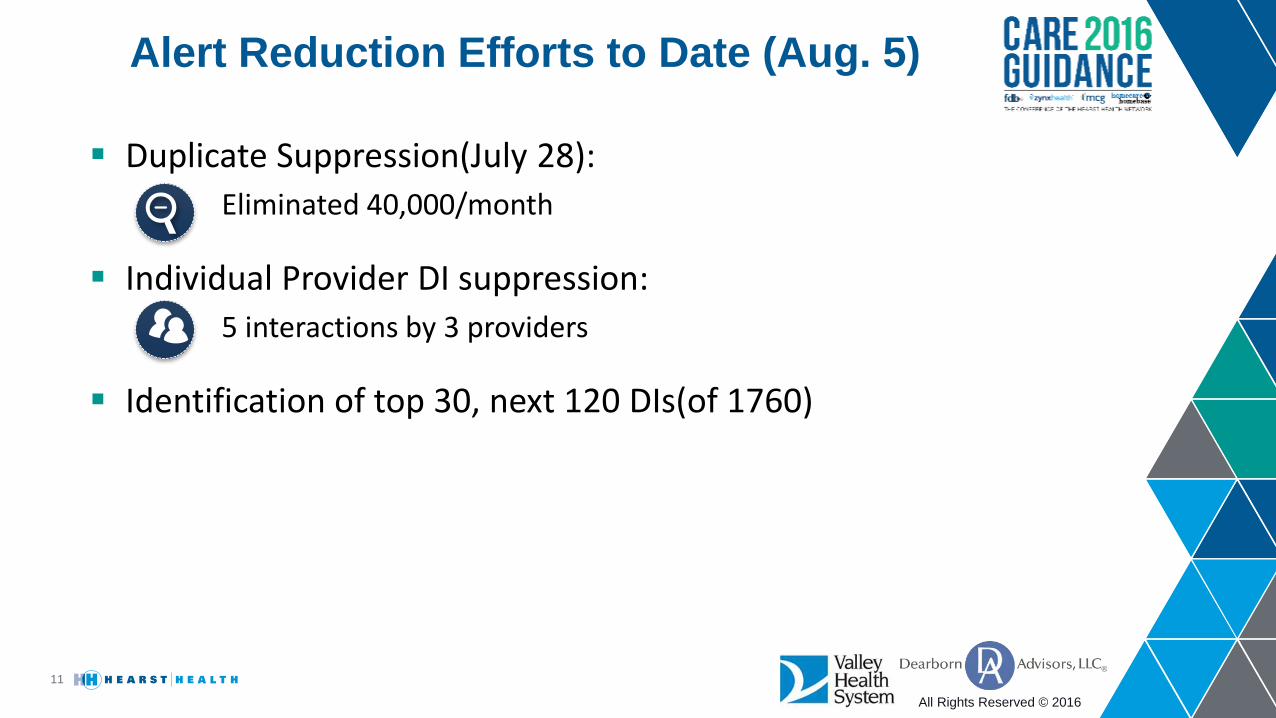
Alert Reduction Efforts to Date (Aug. 5)
11
Duplicate Suppression(July 28):
Eliminated 40,000/month
Individual Provider DI suppression:
5 interactions by 3 providers
Identification of top 30, next 120 DIs(of 1760)
All Rights Reserved © 2016
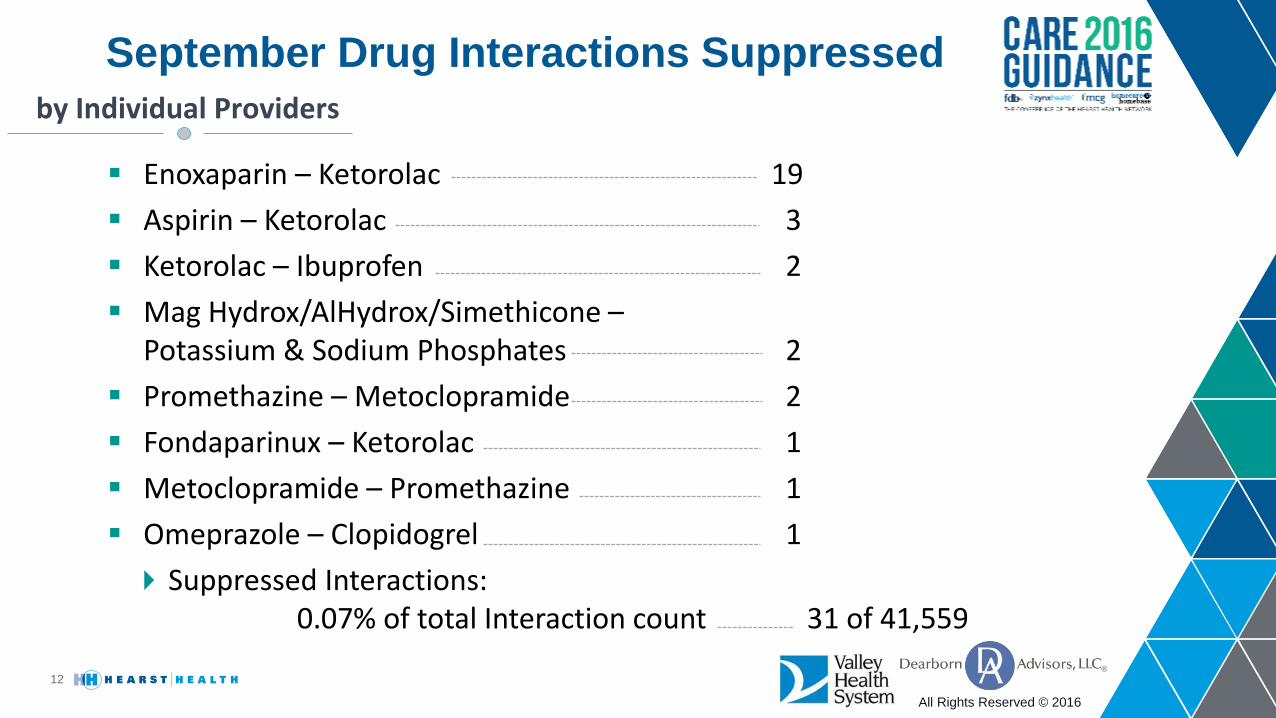
September Drug Interactions Suppressed
12
Enoxaparin – Ketorolac 19
Aspirin – Ketorolac 3
Ketorolac – Ibuprofen 2
Mag Hydrox/AlHydrox/Simethicone –Potassium & Sodium Phosphates 2
Promethazine – Metoclopramide 2
Fondaparinux – Ketorolac 1
Metoclopramide – Promethazine 1
Omeprazole – Clopidogrel 1
Suppressed Interactions:0.07% of total Interaction count 31 of 41,559
by Individual Providers
All Rights Reserved © 2016
DI Review – First Effort
13
Compared FDB severities with Micromedex to identify DIs not needed
Reviewed all >1600 DIs
Downgraded 180 from severity 2 to 3
Removed from Physician view, still seen by pharmacy
All Rights Reserved © 2016
Sample of Interactions Downgraded
14
Acitretin/Ethyl Alcohol
Amifampridine/Possible QT Prolonging Agents
Amphotericin B/Corticosteroids; Corticotropin (ACTH)
Antidiabetic Agents/Gymnema
Aspartame; Phenylalanine; Tyrosine/Nitisinone
Bevacizumab/Sunitinib
Bortezomib/Ascorbic Acid (Vitamin C)
Certolizumab/Rituximab
Cisapride/Stiripentol
Colistimethate/Cephalothin
Contraceptives/Chloramphenicol
Cyclosporine/Sulfonamides
Dapsone/Didanosine
All Rights Reserved © 2016
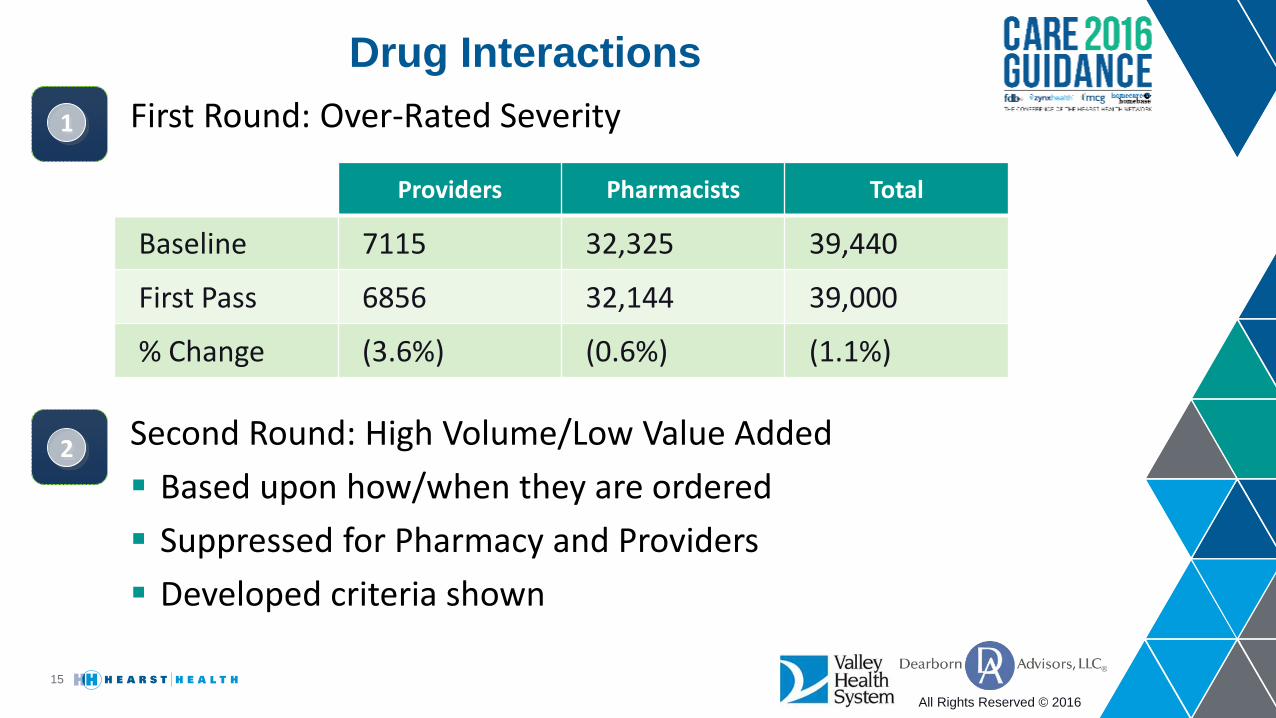
First Round: Over-Rated Severity
Drug Interactions
15
Second Round: High Volume/Low Value Added
Based upon how/when they are ordered
Suppressed for Pharmacy and Providers
Developed criteria shown
Providers Pharmacists Total
Baseline 7115 32,325 39,440
First Pass 6856 32,144 39,000
% Change (3.6%) (0.6%) (1.1%)
1
2
All Rights Reserved © 2016
16
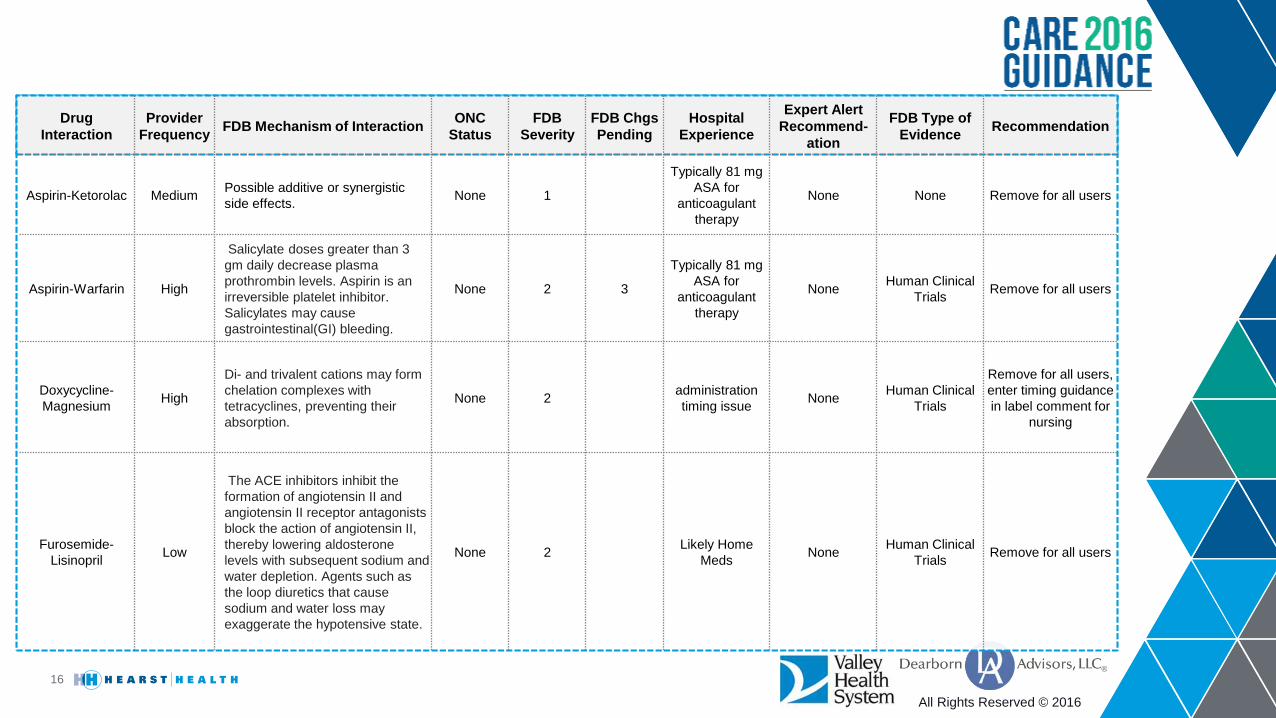
Drug
Interaction
Provider
FrequencyFDB Mechanism of Interaction
ONC
Status
FDB
Severity
FDB Chgs
Pending
Hospital
Experience
Expert Alert
Recommend-
ation
FDB Type of
EvidenceRecommendation
Aspirin-Ketorolac MediumPossible additive or synergistic
side effects.None 1
Typically 81 mg
ASA for
anticoagulant
therapy
None None Remove for all users
Aspirin-Warfarin High
Salicylate doses greater than 3
gm daily decrease plasma
prothrombin levels. Aspirin is an
irreversible platelet inhibitor.
Salicylates may cause
gastrointestinal(GI) bleeding.
None 2 3
Typically 81 mg
ASA for
anticoagulant
therapy
NoneHuman Clinical
TrialsRemove for all users
Doxycycline-
Magnesium High
Di- and trivalent cations may form
chelation complexes with
tetracyclines, preventing their
absorption.
None 2administration
timing issueNone
Human Clinical
Trials
Remove for all users,
enter timing guidance
in label comment for
nursing
Furosemide-
Lisinopril Low
The ACE inhibitors inhibit the
formation of angiotensin II and
angiotensin II receptor antagonists
block the action of angiotensin II,
thereby lowering aldosterone
levels with subsequent sodium and
water depletion. Agents such as
the loop diuretics that cause
sodium and water loss may
exaggerate the hypotensive state.
None 2Likely Home
MedsNone
Human Clinical
TrialsRemove for all users
All Rights Reserved © 2016
Home Med/Prescription Alerts
17
805 duplicate alerts
245 Drug Interaction alerts
Checking is done with both IP and Home/RX Meds
• Only if convert IP to home med w/o change then no checking with itself
• Any change results in all checking with ALL IP & Home Meds
‒ IV-PO, change dose, change form
Shut off duplicate checking for providers not working in purely ambulatory settings
Monitor DI checking
REVIEW – 1 WEEK OF DATA ACTIONS
All Rights Reserved © 2016
Anticoagulant – Antibiotic
18
Reflex INR order from anticoagulant order
Receive P&T approval & structure program for pharmacy to order/monitor INR
• Pharmacy currently has approval to order baseline INR
• Provide monitoring mechanism: report/dashboard of patients on anticoag without INR and with INR out of range
Turn off for pharmacy and providers when INR monitoring program is in place
Alert Recommendations
All Rights Reserved © 2016
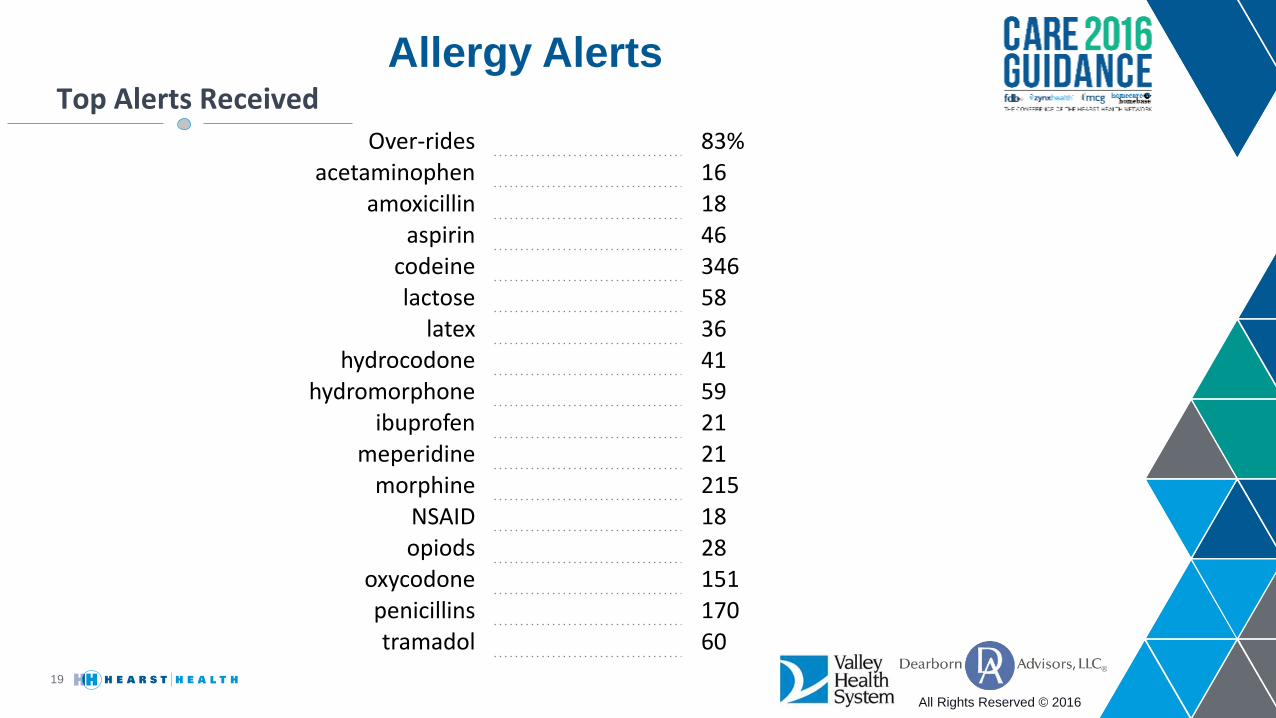
Allergy Alerts
19
Over-rides 83%acetaminophen 16
amoxicillin 18aspirin 46
codeine 346lactose 58
latex 36hydrocodone 41
hydromorphone 59ibuprofen 21
meperidine 21morphine 215
NSAID 18opiods 28
oxycodone 151penicillins 170tramadol 60
Top Alerts Received
All Rights Reserved © 2016
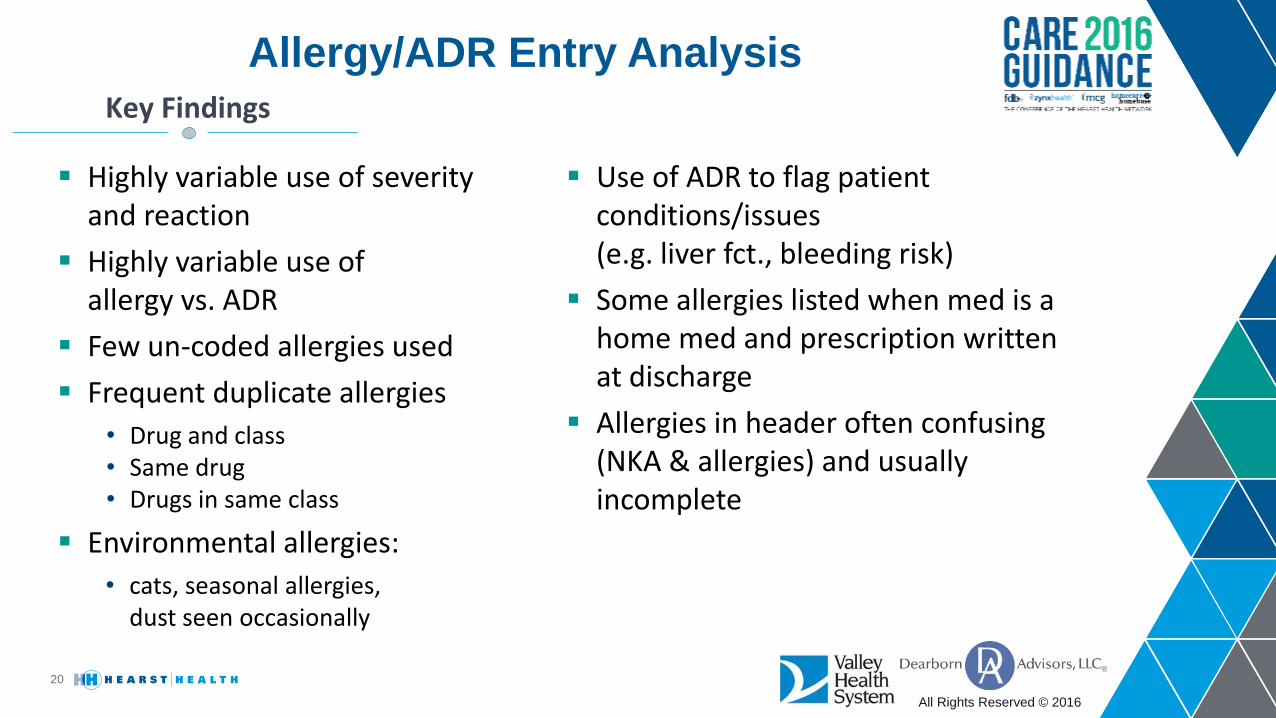
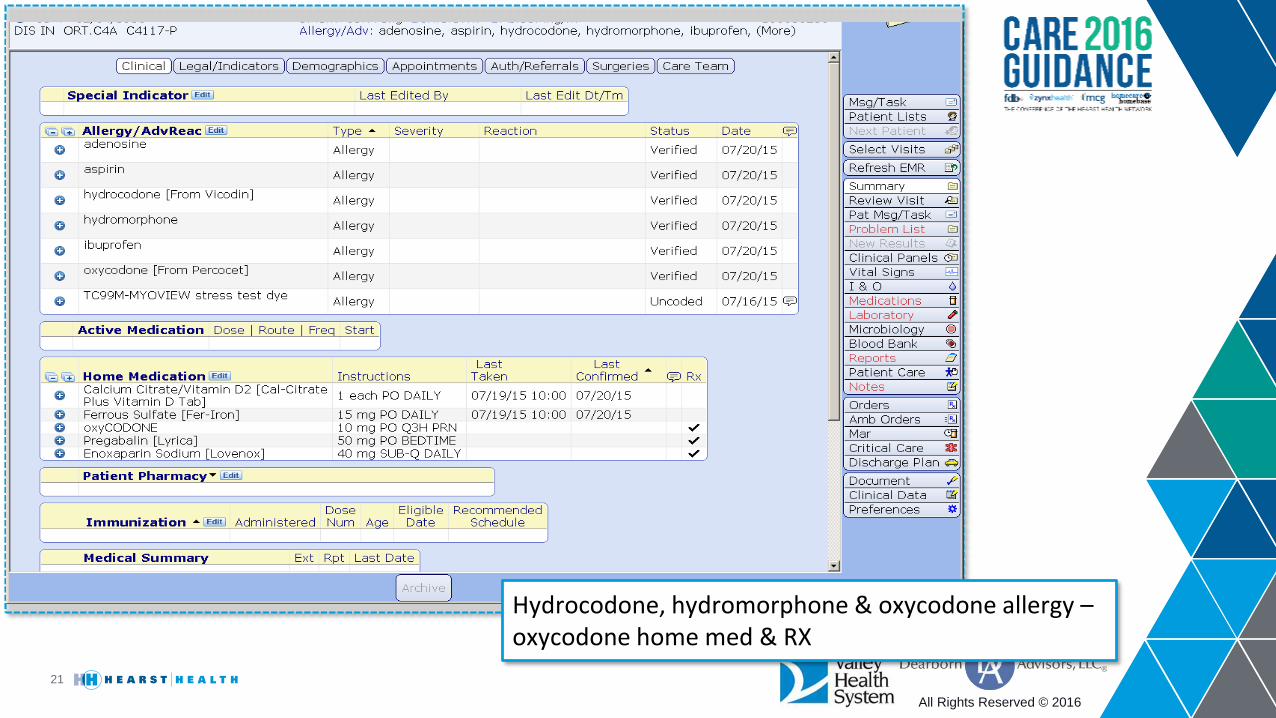
Allergy/ADR Entry Analysis
20
Highly variable use of severity and reaction
Highly variable use of allergy vs. ADR
Few un-coded allergies used
Frequent duplicate allergies
• Drug and class• Same drug • Drugs in same class
Environmental allergies:
• cats, seasonal allergies, dust seen occasionally
Key Findings
Use of ADR to flag patient conditions/issues (e.g. liver fct., bleeding risk)
Some allergies listed when med is a home med and prescription written at discharge
Allergies in header often confusing (NKA & allergies) and usually incomplete
All Rights Reserved © 2016
21
Hydrocodone, hydromorphone & oxycodone allergy –oxycodone home med & RX
All Rights Reserved © 2016
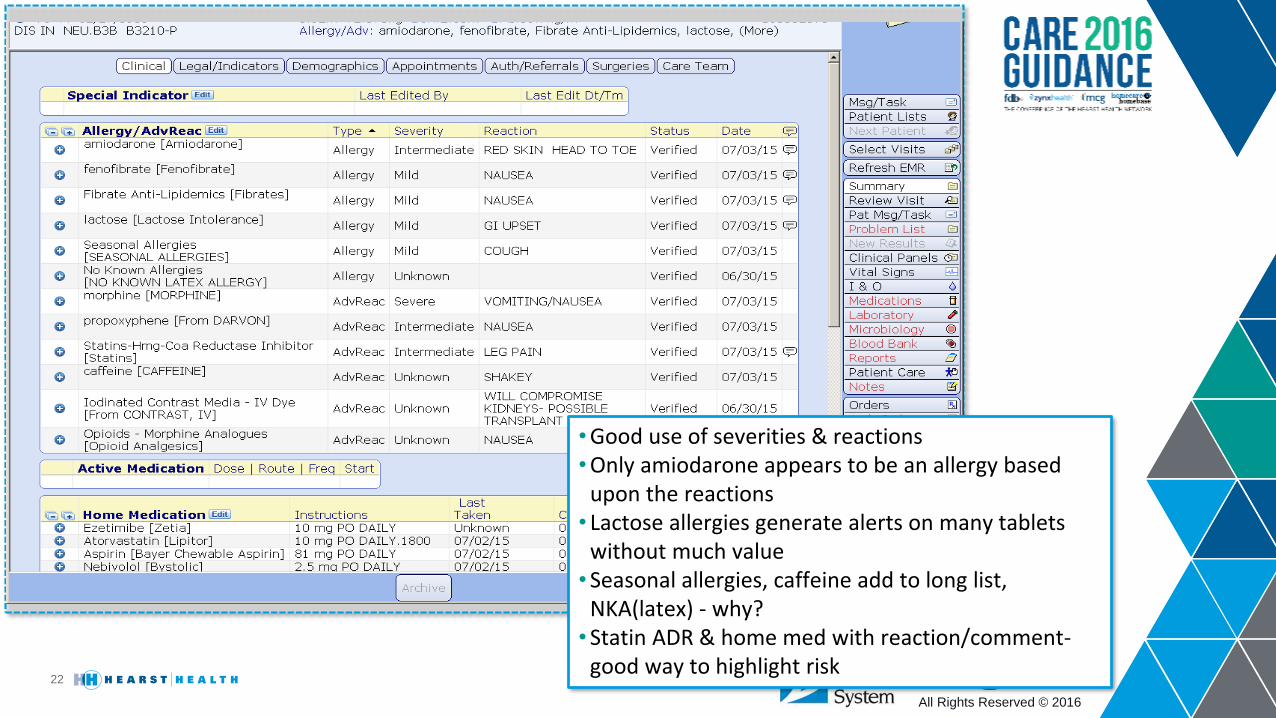
22
•Good use of severities & reactions•Only amiodarone appears to be an allergy based
upon the reactions• Lactose allergies generate alerts on many tablets
without much value•Seasonal allergies, caffeine add to long list,
NKA(latex) - why?•Statin ADR & home med with reaction/comment-
good way to highlight risk
All Rights Reserved © 2016
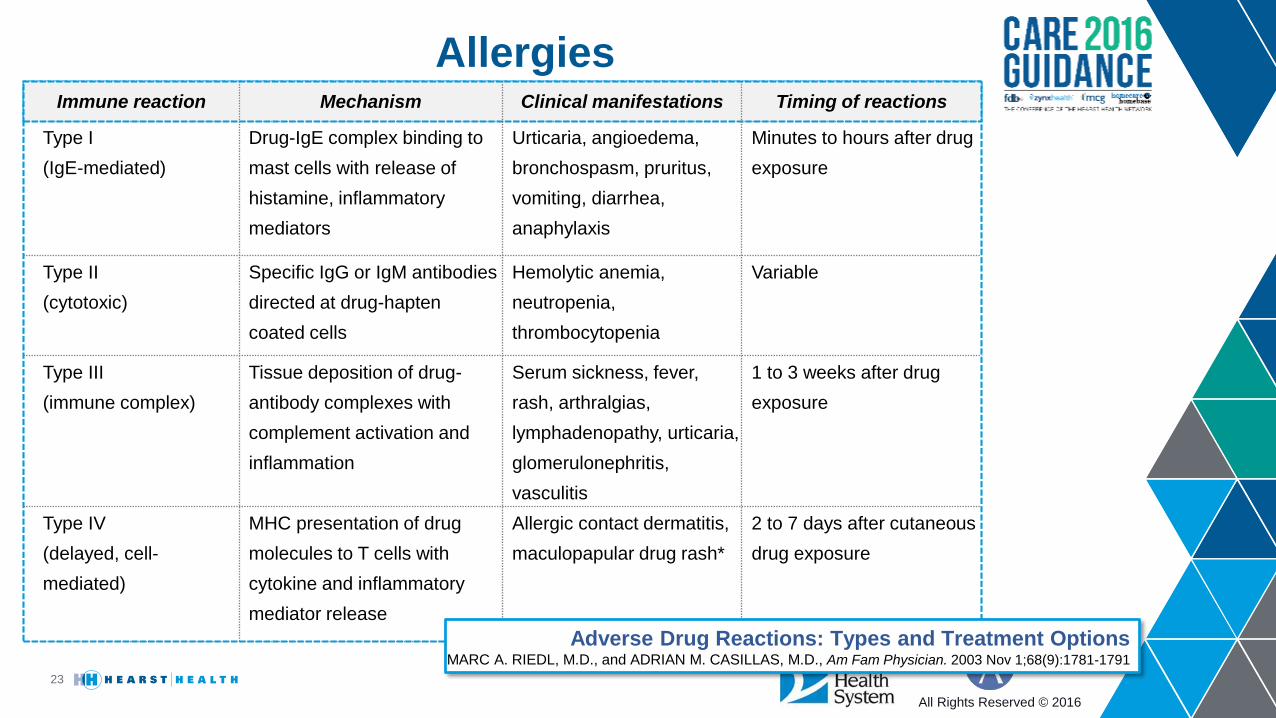
Allergies
23
Immune reaction Mechanism Clinical manifestations Timing of reactions
Type I
(IgE-mediated)
Drug-IgE complex binding to
mast cells with release of
histamine, inflammatory
mediators
Urticaria, angioedema,
bronchospasm, pruritus,
vomiting, diarrhea,
anaphylaxis
Minutes to hours after drug
exposure
Type II
(cytotoxic)
Specific IgG or IgM antibodies
directed at drug-hapten
coated cells
Hemolytic anemia,
neutropenia,
thrombocytopenia
Variable
Type III
(immune complex)
Tissue deposition of drug-
antibody complexes with
complement activation and
inflammation
Serum sickness, fever,
rash, arthralgias,
lymphadenopathy, urticaria,
glomerulonephritis,
vasculitis
1 to 3 weeks after drug
exposure
Type IV
(delayed, cell-
mediated)
MHC presentation of drug
molecules to T cells with
cytokine and inflammatory
mediator release
Allergic contact dermatitis,
maculopapular drug rash*
2 to 7 days after cutaneous
drug exposure
Adverse Drug Reactions: Types and Treatment OptionsMARC A. RIEDL, M.D., and ADRIAN M. CASILLAS, M.D., Am Fam Physician. 2003 Nov 1;68(9):1781-1791
All Rights Reserved © 2016
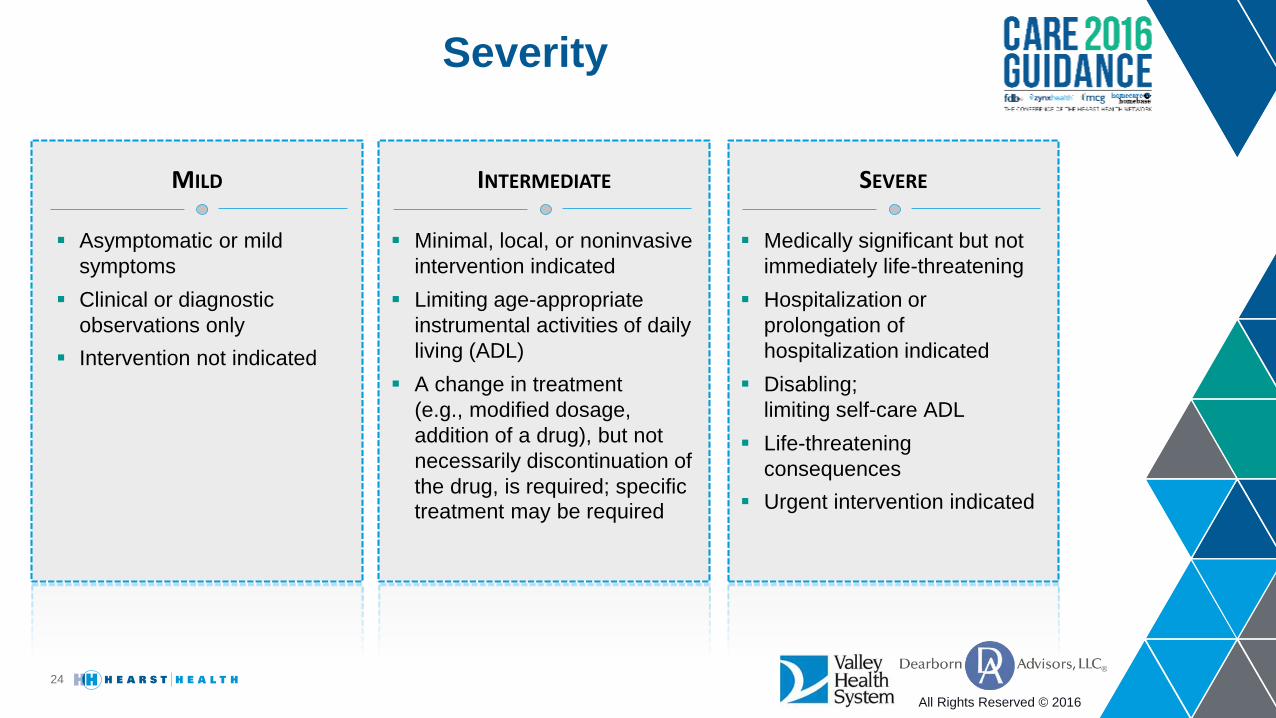
MILD
Severity
24
Asymptomatic or mild
symptoms
Clinical or diagnostic
observations only
Intervention not indicated
INTERMEDIATE
Minimal, local, or noninvasive
intervention indicated
Limiting age-appropriate
instrumental activities of daily
living (ADL)
A change in treatment
(e.g., modified dosage,
addition of a drug), but not
necessarily discontinuation of
the drug, is required; specific
treatment may be required
SEVERE
Medically significant but not
immediately life-threatening
Hospitalization or
prolongation of
hospitalization indicated
Disabling;
limiting self-care ADL
Life-threatening
consequences
Urgent intervention indicated
All Rights Reserved © 2016
P&P Change Summary
25
Use drug class when appropriate rather than multiple drugs in class
Enter environmental allergies (dust, pets) into pt history
Officially sanction the use of ADR for patient conditions
Non-licensed staff to enter unverified allergies
Enter lactose as ADR not allergy
Enter single ingredient entries not combination product allergies/ADRs
Integration with ADR reporting is needed
All Rights Reserved © 2016
Dose Checking
26
Utilized Alternate FDB Units to
correct for Salt vs Base for many
products. Identified products where
Dose Range Check units of measure
did not match Drug File.
Compared FDB data to NeoFax and
other references to adjust as issues
noted.
June 289 changes
July 228 changes
August 12 changes
September 31 changes
October 9 changes
MONTHLY CHANGES SINCE GO-LIVE:
All Rights Reserved © 2016
Review of Approach
27
• Alert Fatigue Work Group Approved• Analysis of Alerts• Turned off selected high volume duplicates
• Classification of drug interactions: Over-rated severity: Removed from Provider View Nuisance alerts: meds used correctly, interaction irrelevant Drug-food interactions: nonspecific so turned off Allowed providers to turn off individual alerts for patient, their pts
• Drug Allergy/ADR Identified poor use of allergy field, internal work group formed to resolve
• Dose Checking Researched dose alerts for applicability
‒ Finding mismatched units, appropriate alerts
Responded to Provider Complaints
All Rights Reserved © 2016
28
QUESTIONS COMMENTS
David Troiano, RPh, MSIA, CPPS
John Heeren, RPh, MS
Wrap-Up – Thank You